approach to lung nodule - southern kentucky...
TRANSCRIPT
5/10/2016
1
Approach to Lung NoduleAHEC Summer Conference
July/2016
Ashish Maskey, MDPulmonary, Critical Care, Interventional Pulmonology
Disclosure
• None
Objective
• Who should you screen for lung cancer• Benign vs Malignant pulmonary nodule• What is the best modality to biopsy
pulmonary nodules
5/10/2016
2
Case• HPI
– 62 female active smoker– CT chest was performed for lung cancer screening
• PMH:• COPD on home oxygen
– GERD, HTN,
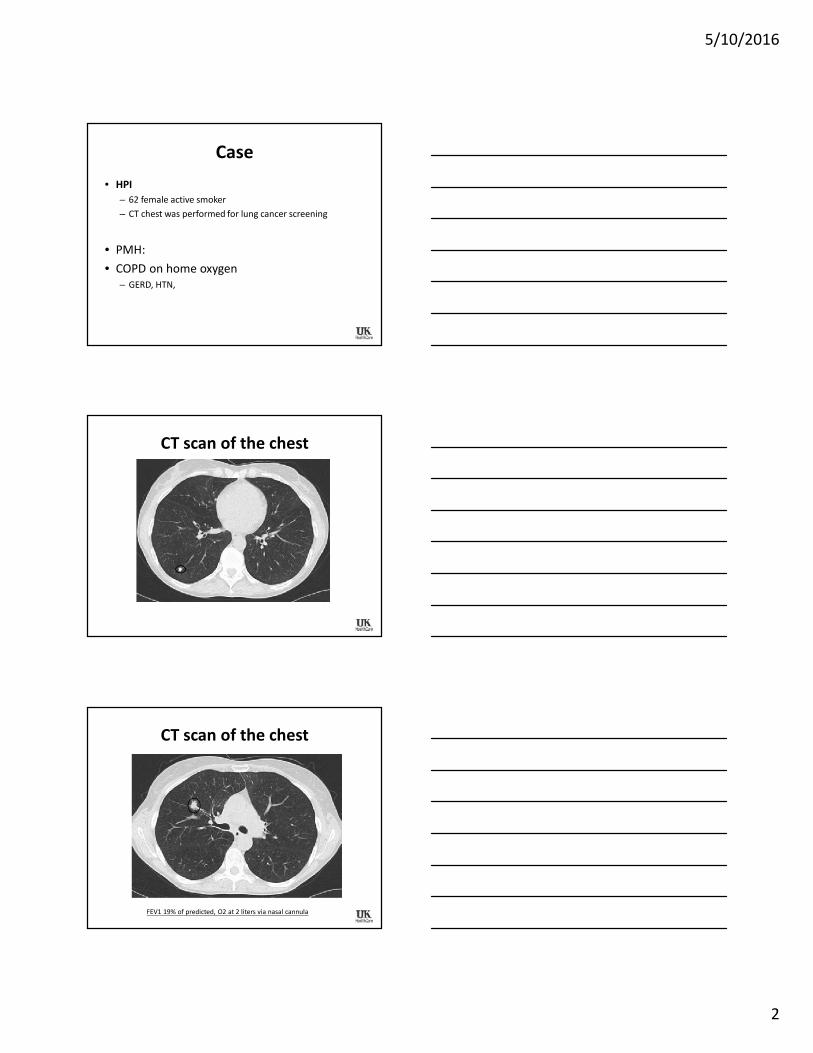
CT scan of the chest
CT scan of the chest
FEV1 19% of predicted, O2 at 2 liters via nasal cannula
5/10/2016
3
Question?
• Benign or Malignant
• Frequency of follow up imaging
• Biopsy or not to biopsy
• Method of biopsy
• VATS lobectomy
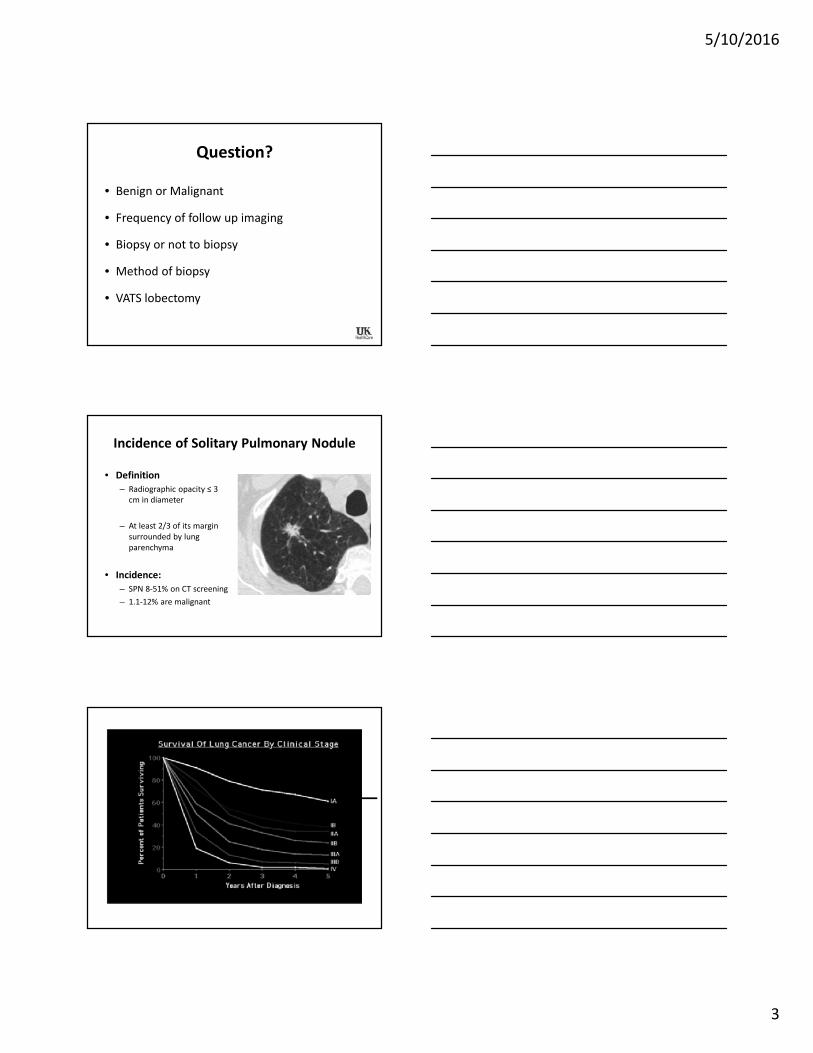
Incidence of Solitary Pulmonary Nodule
• Definition– Radiographic opacity ≤ 3
cm in diameter
– At least 2/3 of its marginsurrounded by lungparenchyma
• Incidence:– SPN 8-51% on CT screening– 1.1-12% are malignant
5/10/2016
4
Differential Diagnosis of Solitary Pulmonary Nodules
NeoplasticMalignantLung cancerPrimary pulmonary carcinoid Solitary metastasisTeratomaLeiomyoma
BenignHamartoma Chondroma Fibroma LipomaNeural tumor (Schwannoma, neurofibroma) Sclerosing hemangiomaPlasma cell granuloma Endometriosis
InfectiousTB (tuberculoma)Round pneumonia, organizing pneumonia Lung abscessFungal: aspergillosis, blastomycosis, cryptococcosis, histoplasmosis, coccidioidomycosisParasitic: amoebiasis, echinococcosis, Dirofilaria immitis (dog heartworm) MeaslesNocardiaAtypical mycobacteriaPneumocystis jiroveciSeptic embolus
Differential Diagnosis of Solitary Pulmonary Nodules
• Vascular• Arteriovenous malformation• Pulmonary infarct• Pulmonary artery aneurysm• Pulmonary venous varix• Hematoma
• Congenital• Bronchogenic cyst• Lung sequestration• Bronchial atresia with mucoid impaction
• Inflammatory• Rheumatoid arthritis• Granulomatosis with polyangiitis (Wegener)• Microscopic polyangiitis• Sarcoidosis
• Lymphatic• Intrapulmonary or subpleural lymph node• Lymphoma
• Outside lung fields• Skin nodule• Nipple shadows• Rib fracture• Pleural thickening, mass or fl uid
(pseudotumor)
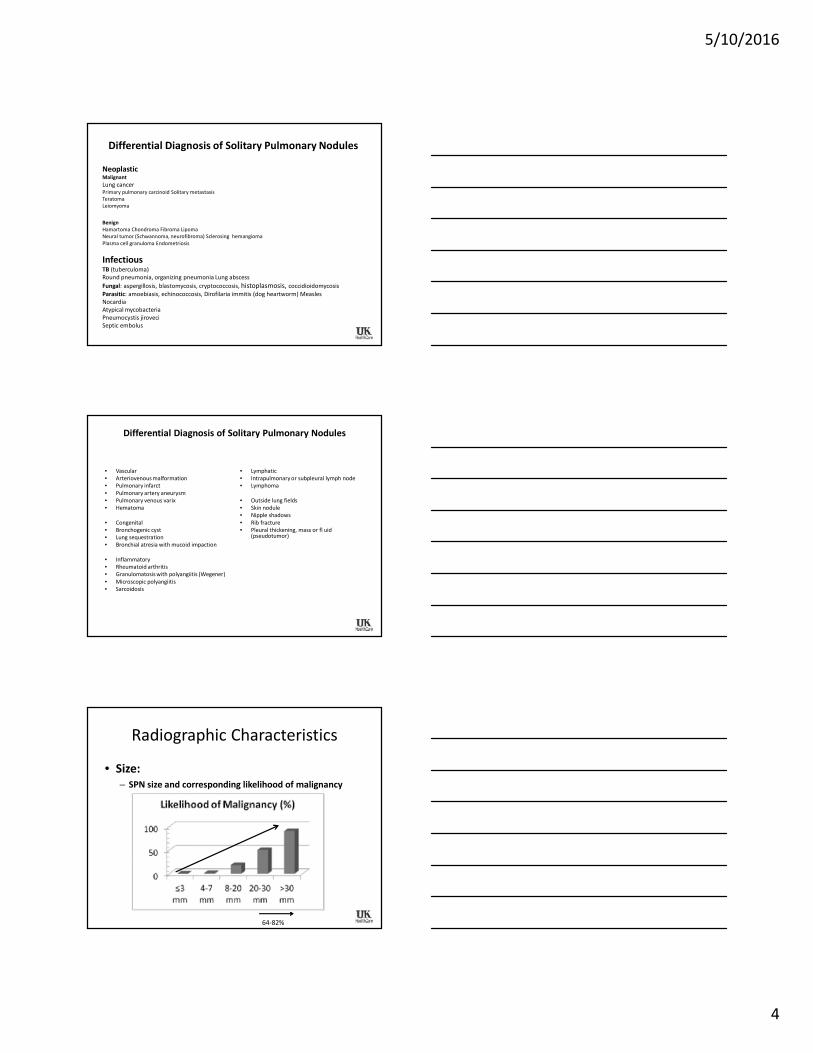
Radiographic Characteristics
• Size:– SPN size and corresponding likelihood of malignancy
64-82%
5/10/2016
5
Radiographic Characteristics• Margins
– Smooth 1/3 malignant
– Lobulated PPV 80% malignant
– Spiculated PPV 88-94%
– Polygonal Benign
– Ragged lepidic pattern of adenocarcinoma
– Halo aspergillus, kaposi, wegener
– Notched adenocarcinoma
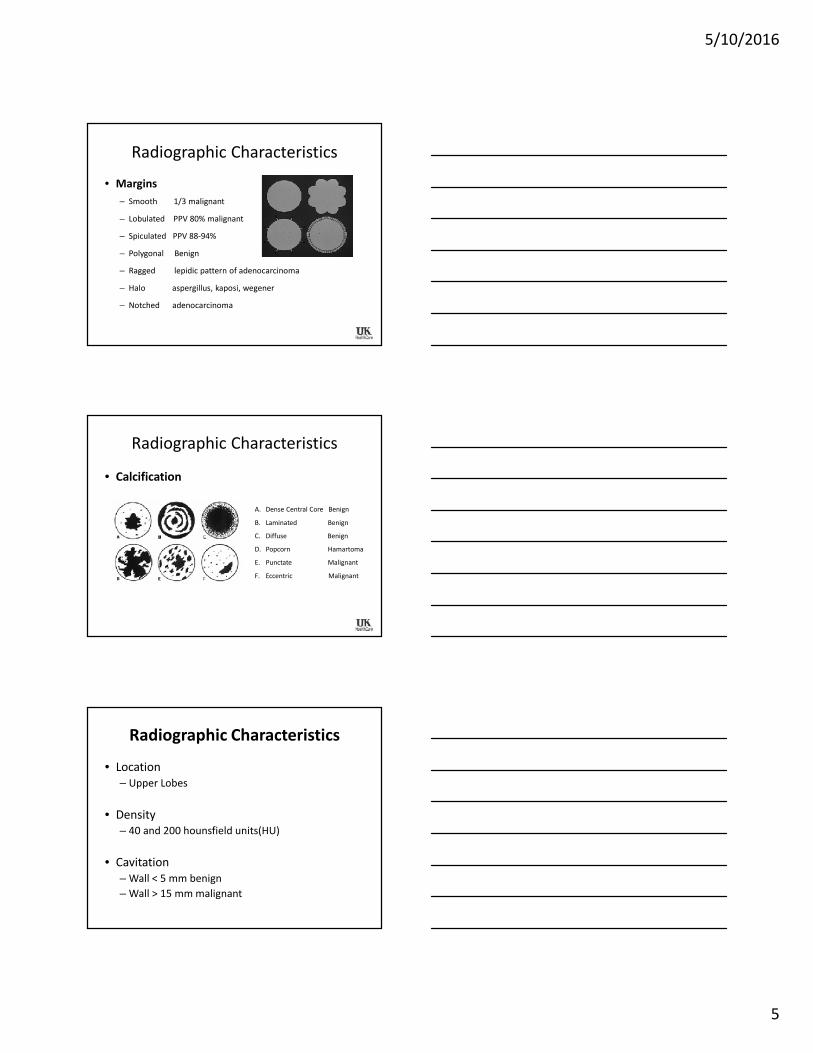
Radiographic Characteristics
• Calcification
A. Dense Central Core Benign
B. Laminated Benign
C. Diffuse Benign
D. Popcorn Hamartoma
E. Punctate Malignant
F. Eccentric Malignant
Radiographic Characteristics
• Location– Upper Lobes
• Density– 40 and 200 hounsfield units(HU)
• Cavitation– Wall < 5 mm benign– Wall > 15 mm malignant
5/10/2016
6
Radiographic Characteristics
• Growth rate:– volume doubling time 20-400 days ( average 100 days)
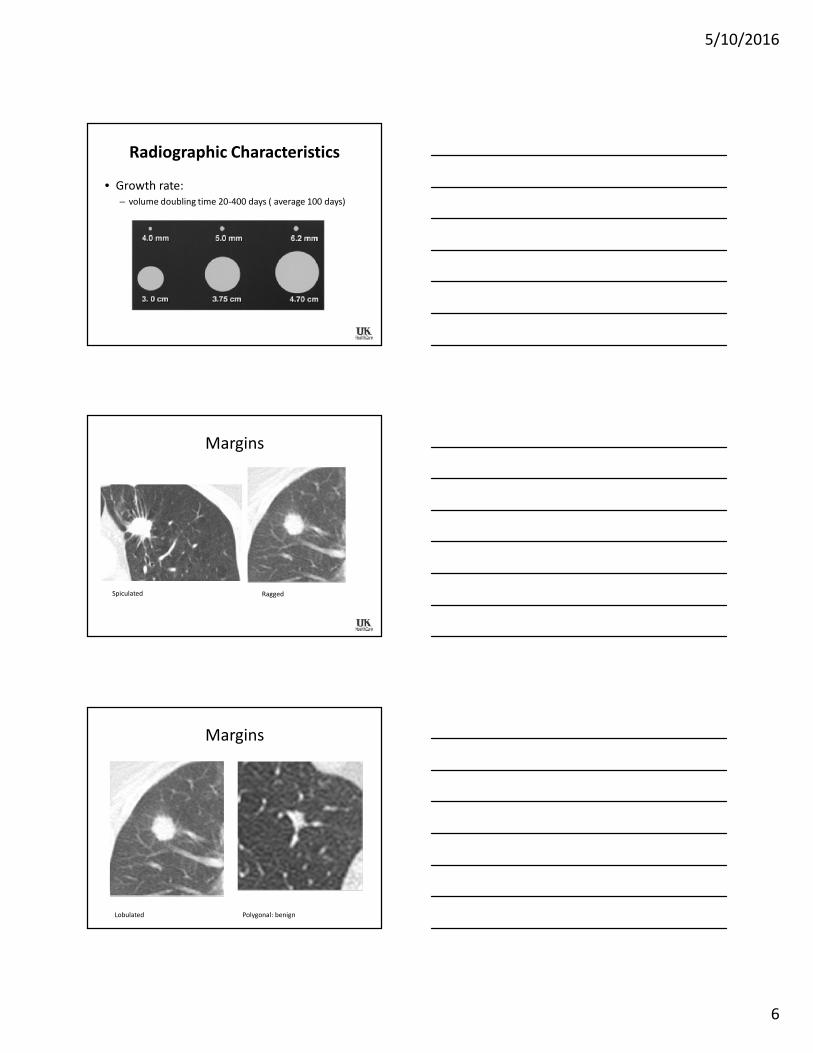
Margins
Spiculated Ragged
Margins
Lobulated Polygonal: benign
5/10/2016
7
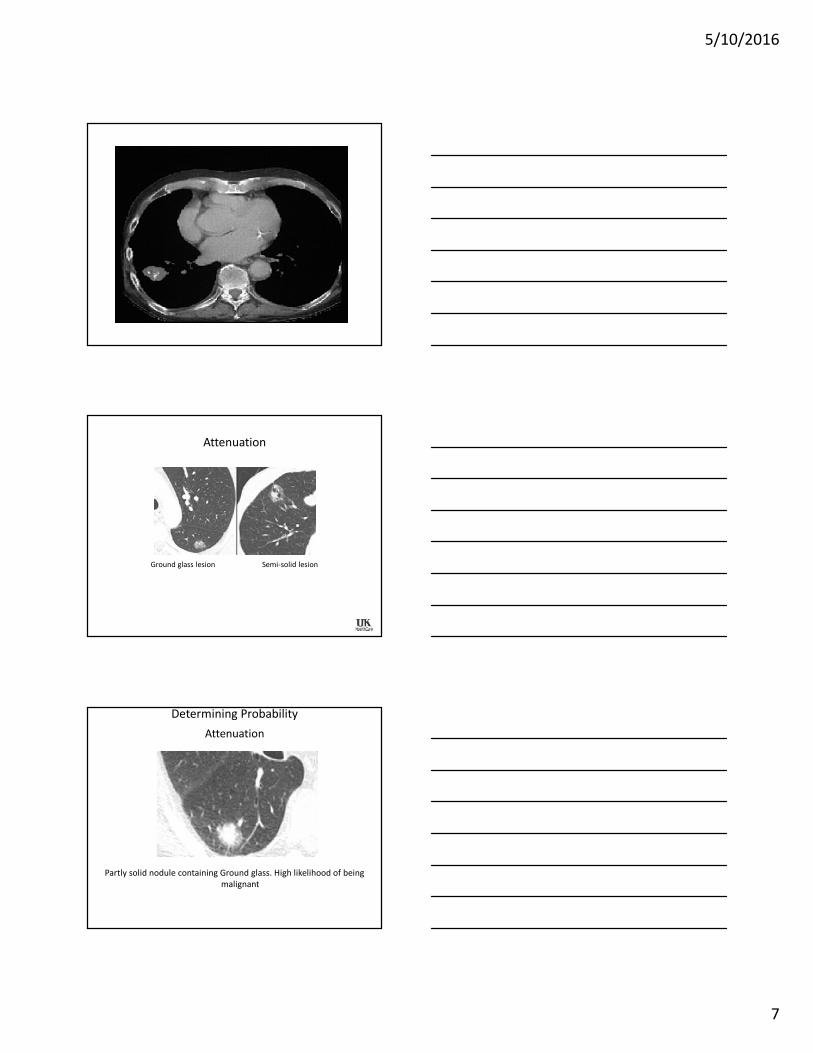
Attenuation
Ground glass lesion Semi-solid lesion
Attenuation
Partly solid nodule containing Ground glass. High likelihood of beingmalignant
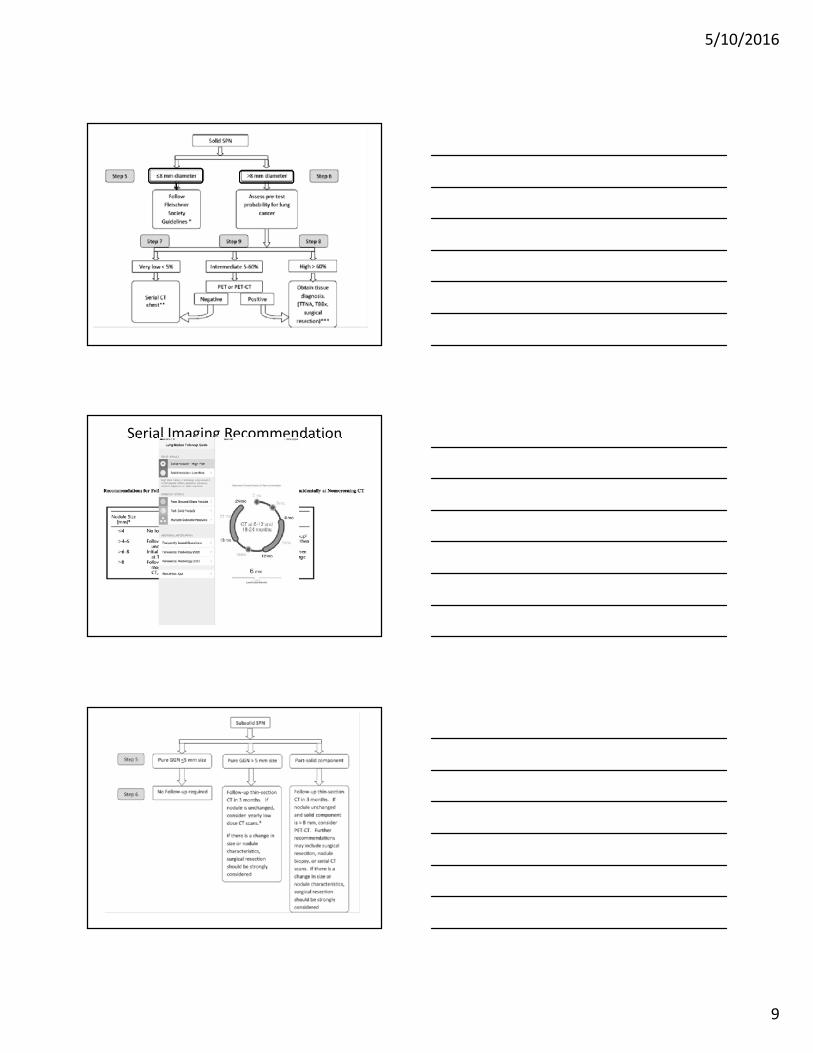
Determining Probability
5/10/2016
8
Pre-test Probability
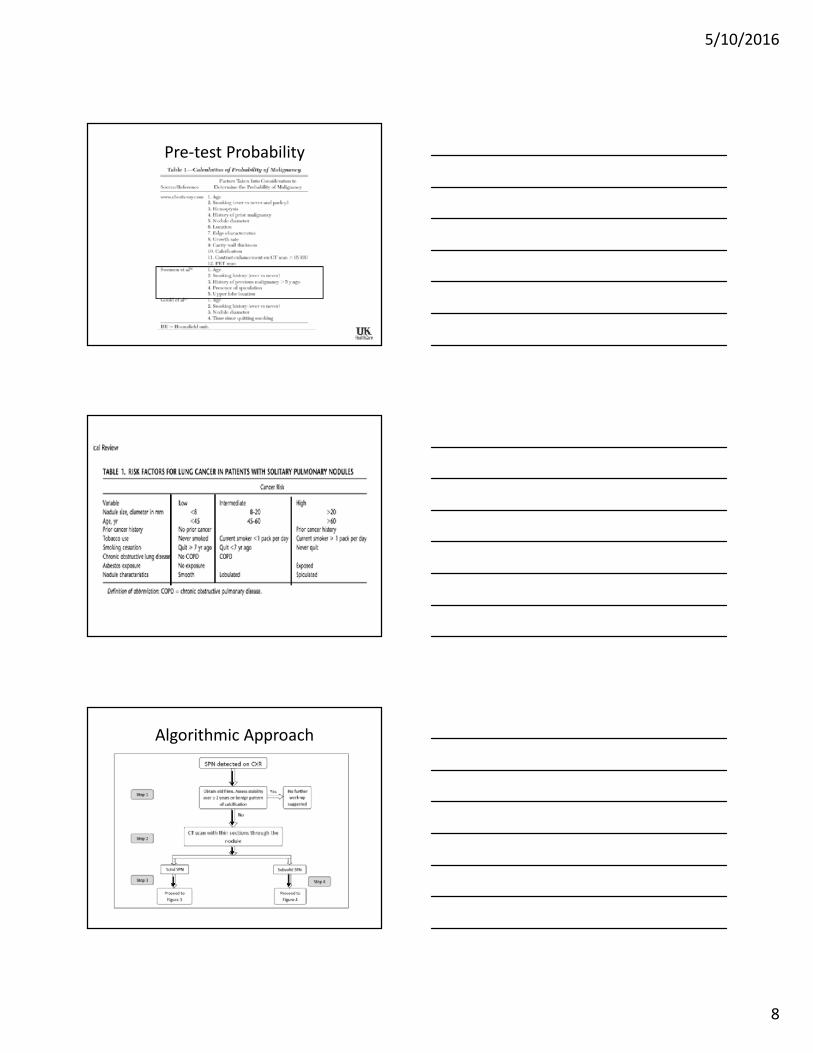
Algorithmic Approach
5/10/2016
9
Serial Imaging RecommendationFleischner Society
5/10/2016
10
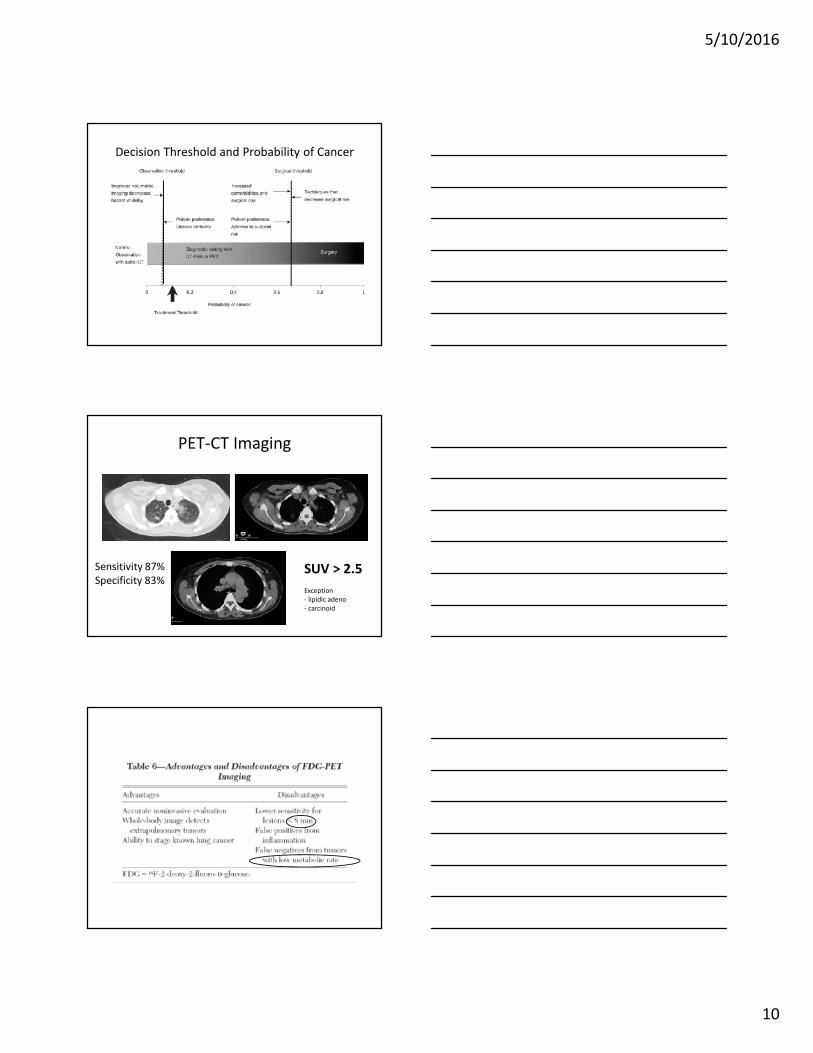
Decision Threshold and Probability of Cancer
PET-CT Imaging
SUV > 2.5Exception- lipidic adeno- carcinoid
Sensitivity 87%Specificity 83%

5/10/2016
11
CT guided transthoracic needle aspirationDiagnosis rate: 65-94%%
Complication:pneumothorax 15-43%(27%)• chest tube 4-18%HemorrhageAir embolism
RiskSmaller lesionDeeper lesionEmphysemaLateral punctureProximity o fissureLow entry angle to pleura
Bronchoscopy with Transbronchial Biopsy
• Diagnosis rates• < 2 cm 33% (10-50%)• >3 cm 63%
Rivera et al. Initial diagnosis of lung cancer. Chest 2007:132:131S-148S
5/10/2016
12
New modalities in Bronchoscopy
• Ultrathin bronchoscopy• Guide sheath• Radial Endobronchial Ultrasound• Virtual bronchoscopy• Electromagnetic navigation bronchoscopy
• Combination of the different modalities.
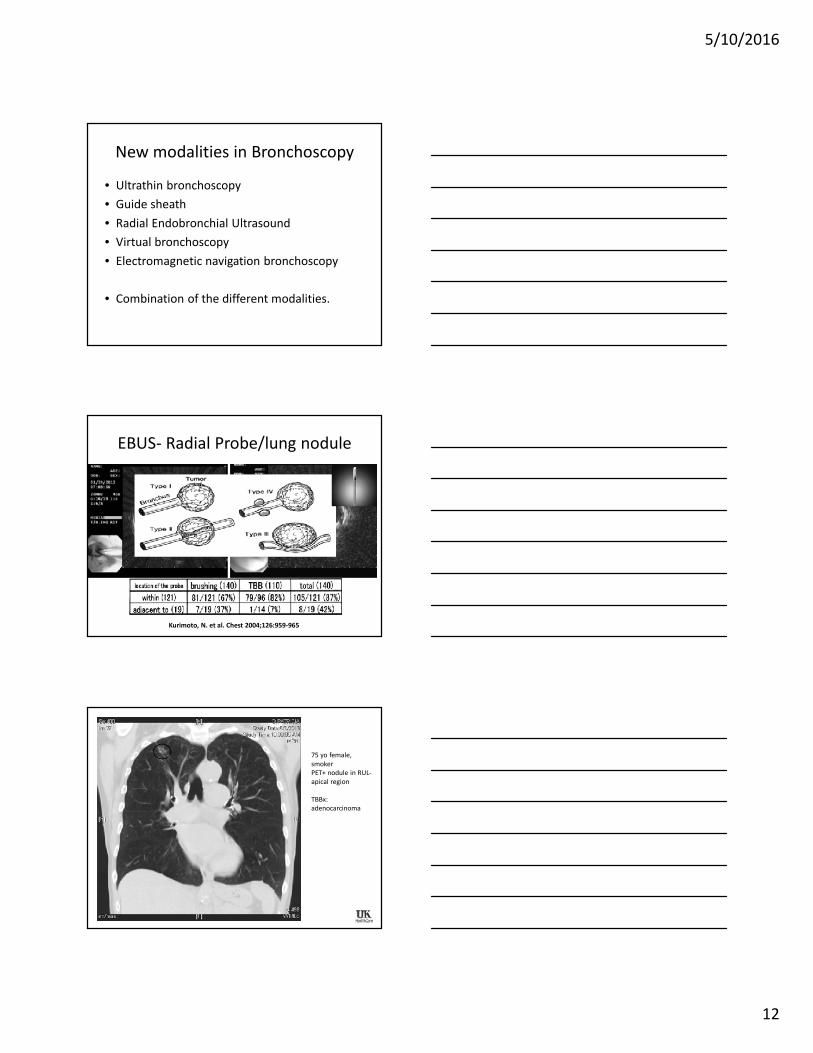
EBUS- Radial Probe/lung nodule
Kurimoto, N. et al. Chest 2004;126:959-965
• 75 yo female, smoker• PET+ nodule in RUL-apical region• TBBx: adenocarcinoma
75 yo female,smokerPET+ nodule in RUL-apical region
TBBx:adenocarcinoma
5/10/2016
13
Video Assisted Thoracoscopy
• Wedge Resection– Diagnosis rate 90-95%– Complication: 0.5%
• Lobectomy– Complication: 4%
• Conversion to thoracotomy is 12 %
National Lung Screening Trial• 53,454 high risk patients
– Age 55-74– > 30 pack year History of smoking– Quit < 15 years
– 26,722 had a low dose helical CT
– Positive screening 24.2 %– False positive 94.5%– Incidence of cancer 645/100,000
NEJM 2011: 365:395-409

5/10/2016
14
The National Lung Screening Trial
• Low dose CT 1.5 mSv vs 8 mSv
• The diagnosis were made with Bronschoscopy,Needle biopsy, Mediastinoscopy, thoracotomy
• Relative risk reduction 20.0%• Number needed to screen 320
NEJM 2011: 365:395-409
US Preventive Services Task Force recommendation statement onScreening for lung Cancer (July 30, 2013):
“Based on available evidence, the Task Force recommendsscreening people who are at high risk for lung cancer withannual low dose CT scans, which can prevent substantialnumber of lung cancer-related deaths occurring in people age55 or older.”
“…you can reach a reasonable balance of benefits and harms byscreening people who are 55 to 80 years old and have a 30pack year or greater history of smoking, who are currentsmokers or have quit in the past fifteen years.”
Public Health Perspective
Questions
5/10/2016
15
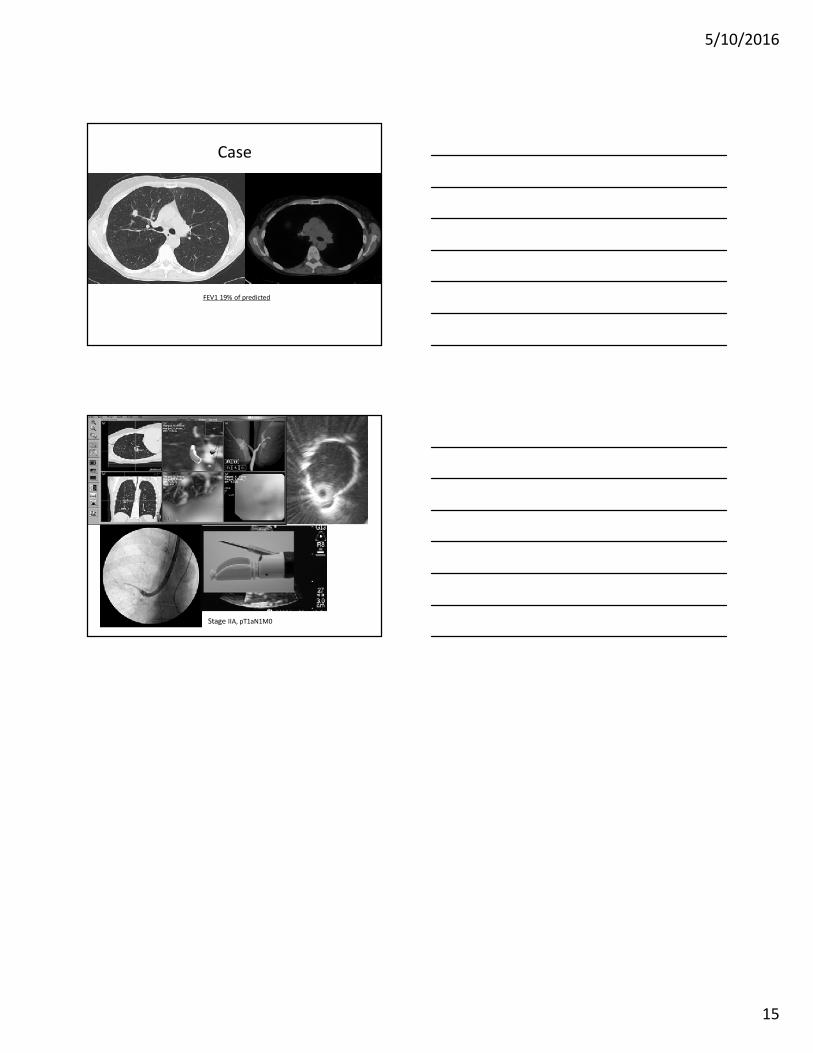
Case
FEV1 19% of predicted
Stage IIA, pT1aN1M0