approaches towards decrypting ischemic strokes of unknown ... · athens stroke registry (2000)64...
TRANSCRIPT
10/3/2017
1
Approaches towards decrypting ischemic strokes of unknown causes
(Cryptogenic ischemic strokes)
Deb Mojumder MD PhD
Neurology/Neurocritical care
3rd October 2017
Disclosures
None to disclose
10/3/2017
2
https://www.nbcnews.com/http://www.nbcnews.com/slideshow/cartoons-credit-crunch-31409267
Decoding
Objectives
10/3/2017
3
Ischemic Stroke
678,000/yr in the US1
1 Mozzafarian D, et al. Circulation. 2015;131:e29-e322.
10/3/2017
4
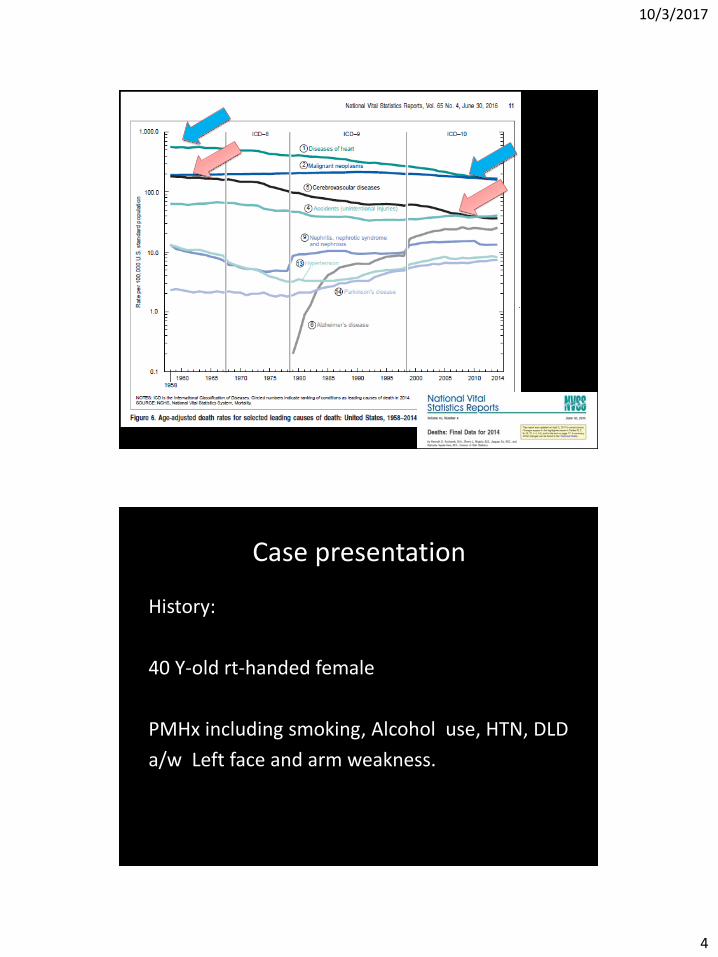
Case presentation
History:
40 Y-old rt-handed female
PMHx including smoking, Alcohol use, HTN, DLD
a/w Left face and arm weakness.
10/3/2017
5
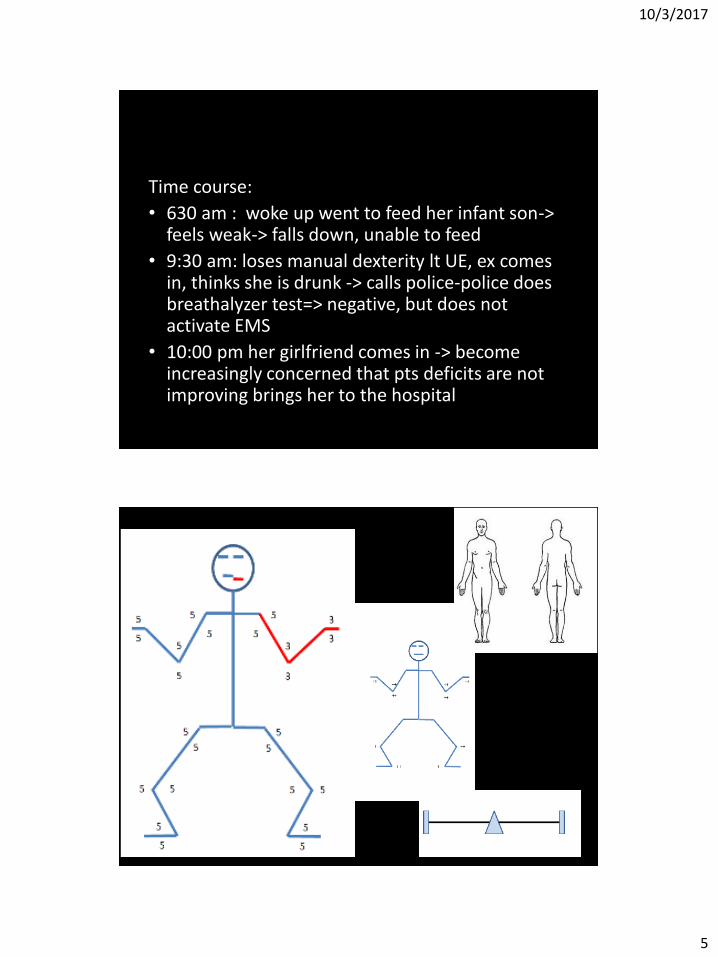
Time course:
• 630 am : woke up went to feed her infant son-> feels weak-> falls down, unable to feed
• 9:30 am: loses manual dexterity lt UE, ex comes in, thinks she is drunk -> calls police-police does breathalyzer test=> negative, but does not activate EMS
• 10:00 pm her girlfriend comes in -> become increasingly concerned that pts deficits are not improving brings her to the hospital
10/3/2017
6
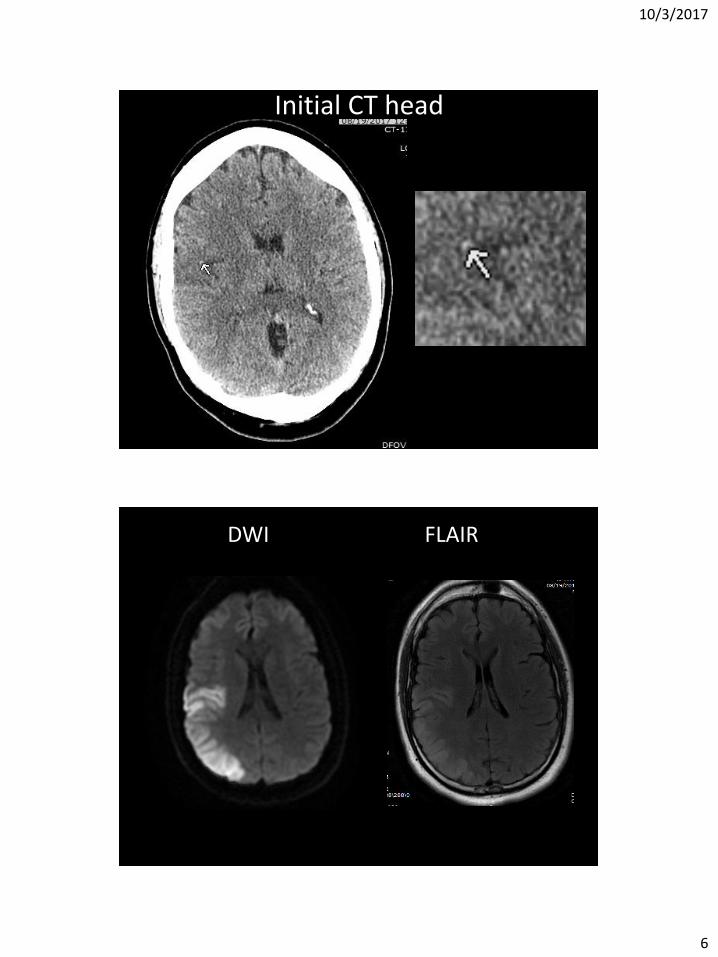
Initial CT head
DWI FLAIR
10/3/2017
7
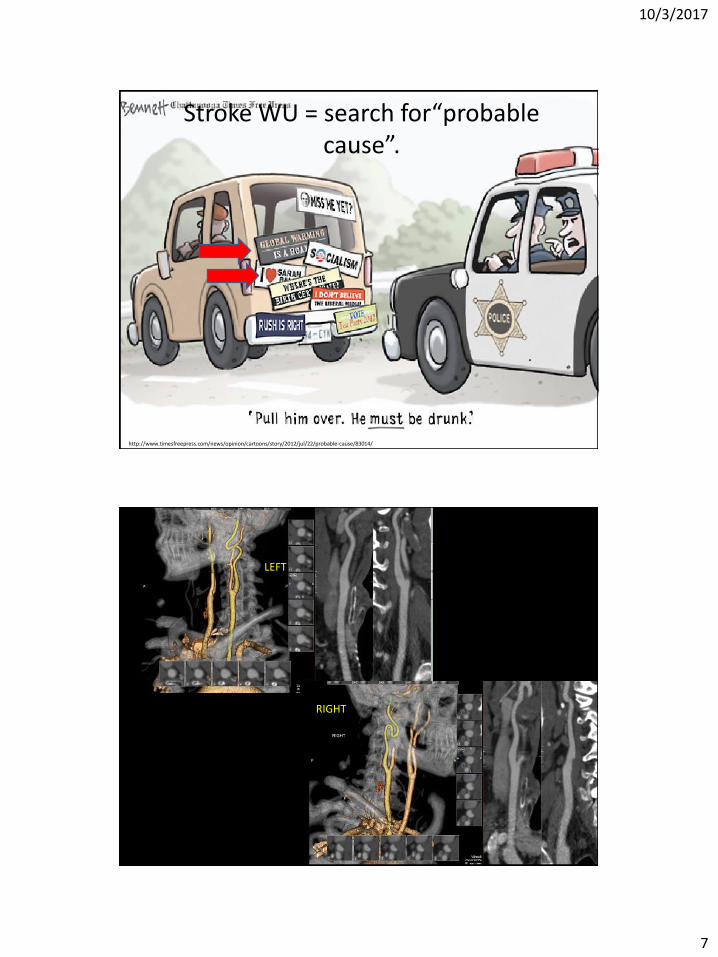
http://www.timesfreepress.com/news/opinion/cartoons/story/2012/jul/22/probable-cause/83014/
Stroke WU = search for“probable cause”.
LEFT
RIGHT
10/3/2017
8
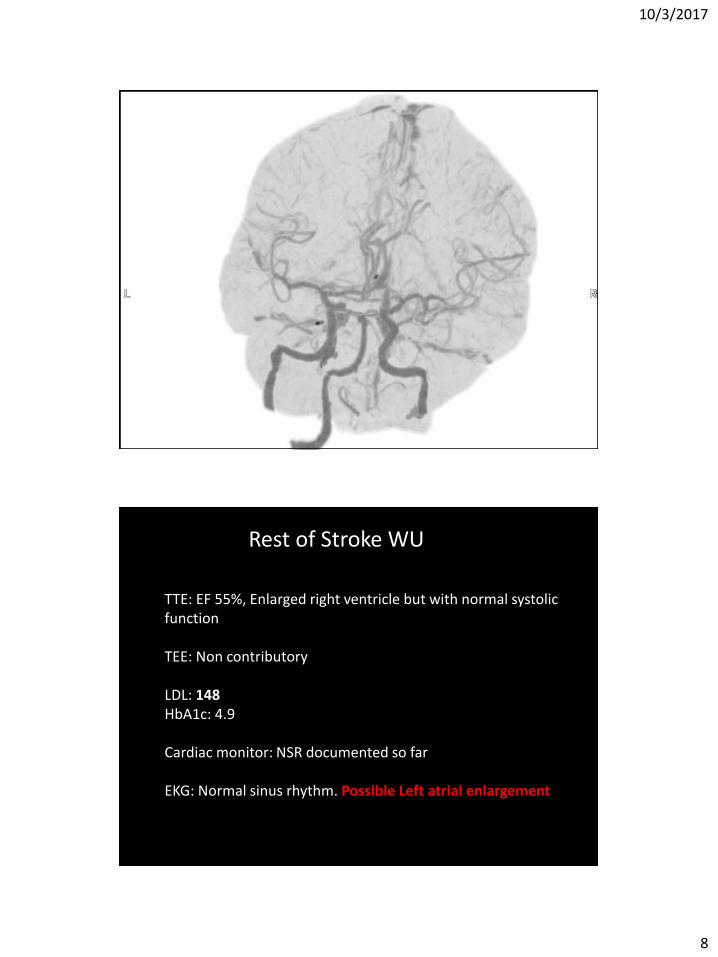
TTE: EF 55%, Enlarged right ventricle but with normal systolic function TEE: Non contributory LDL: 148 HbA1c: 4.9 Cardiac monitor: NSR documented so far EKG: Normal sinus rhythm. Possible Left atrial enlargement
Rest of Stroke WU
10/3/2017
9
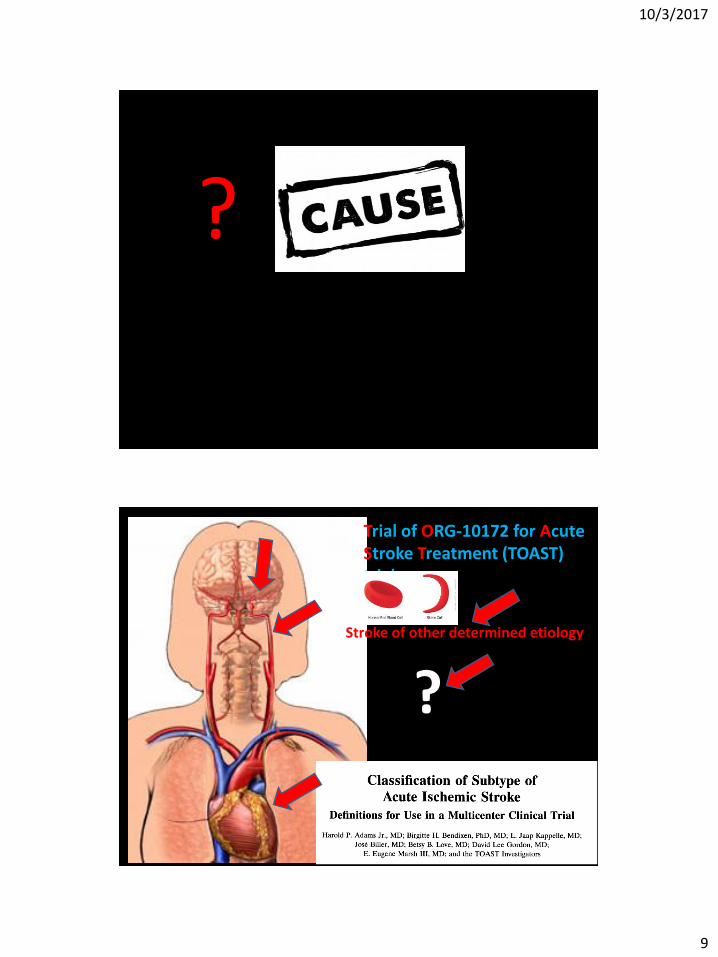
?
Trial of ORG-10172 for Acute Stroke Treatment (TOAST) trial
Stroke of other determined etiology
?
10/3/2017
10
“Unknown” implies considering full workup:
• Neuroimaging: topographical features
• Imaging of large vessels,
• Cardiac rhythm monitoring
• Imaging of the heart,
• Serological studies
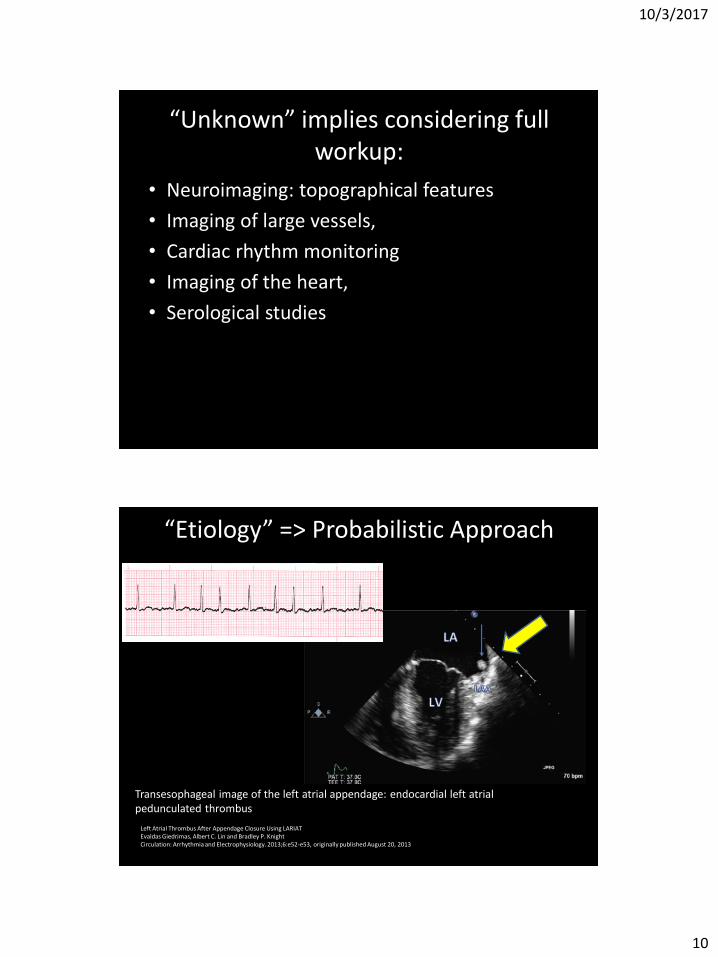
“Etiology” => Probabilistic Approach
Left Atrial Thrombus After Appendage Closure Using LARIAT Evaldas Giedrimas, Albert C. Lin and Bradley P. Knight Circulation: Arrhythmia and Electrophysiology. 2013;6:e52-e53, originally published August 20, 2013
Transesophageal image of the left atrial appendage: endocardial left atrial pedunculated thrombus
10/3/2017
11
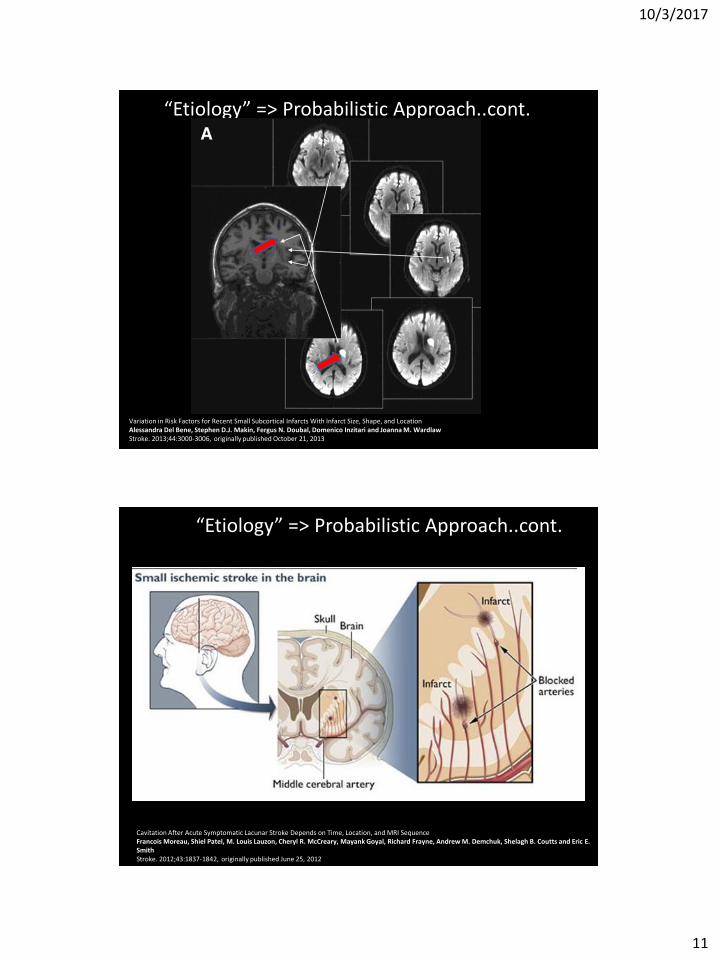
“Etiology” => Probabilistic Approach..cont.
Variation in Risk Factors for Recent Small Subcortical Infarcts With Infarct Size, Shape, and Location Alessandra Del Bene, Stephen D.J. Makin, Fergus N. Doubal, Domenico Inzitari and Joanna M. Wardlaw Stroke. 2013;44:3000-3006, originally published October 21, 2013
“Etiology” => Probabilistic Approach..cont.
Cavitation After Acute Symptomatic Lacunar Stroke Depends on Time, Location, and MRI Sequence Francois Moreau, Shiel Patel, M. Louis Lauzon, Cheryl R. McCreary, Mayank Goyal, Richard Frayne, Andrew M. Demchuk, Shelagh B. Coutts and Eric E. Smith Stroke. 2012;43:1837-1842, originally published June 25, 2012
10/3/2017
12
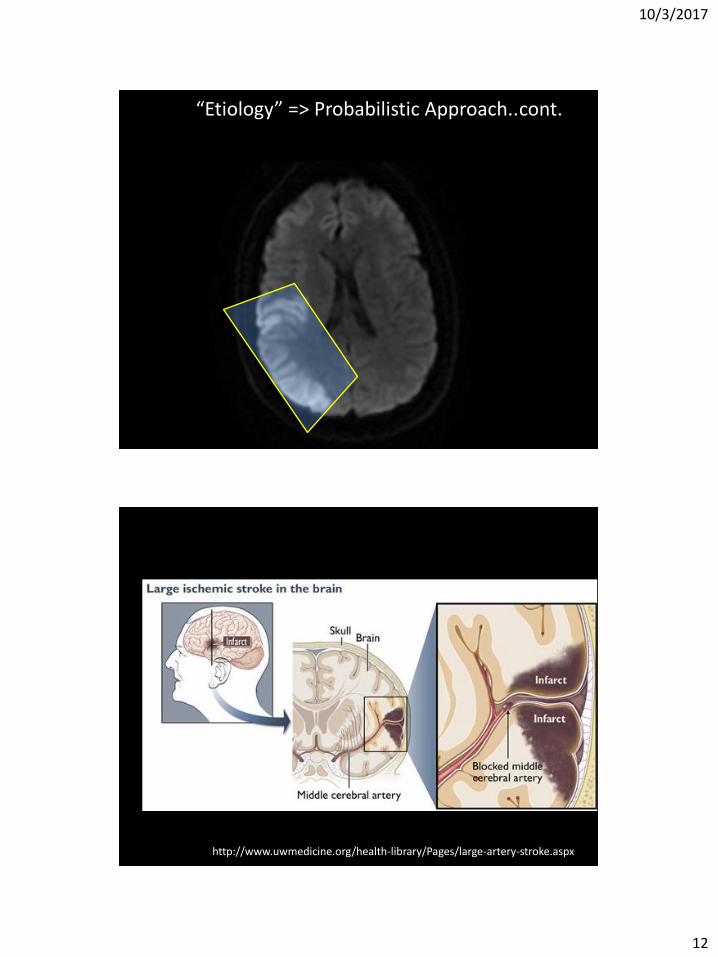
“Etiology” => Probabilistic Approach..cont.
http://www.uwmedicine.org/health-library/Pages/large-artery-stroke.aspx
10/3/2017
13
Co-existance of more than one mechanism
“Etiology” => Probabilistic Approach..cont.
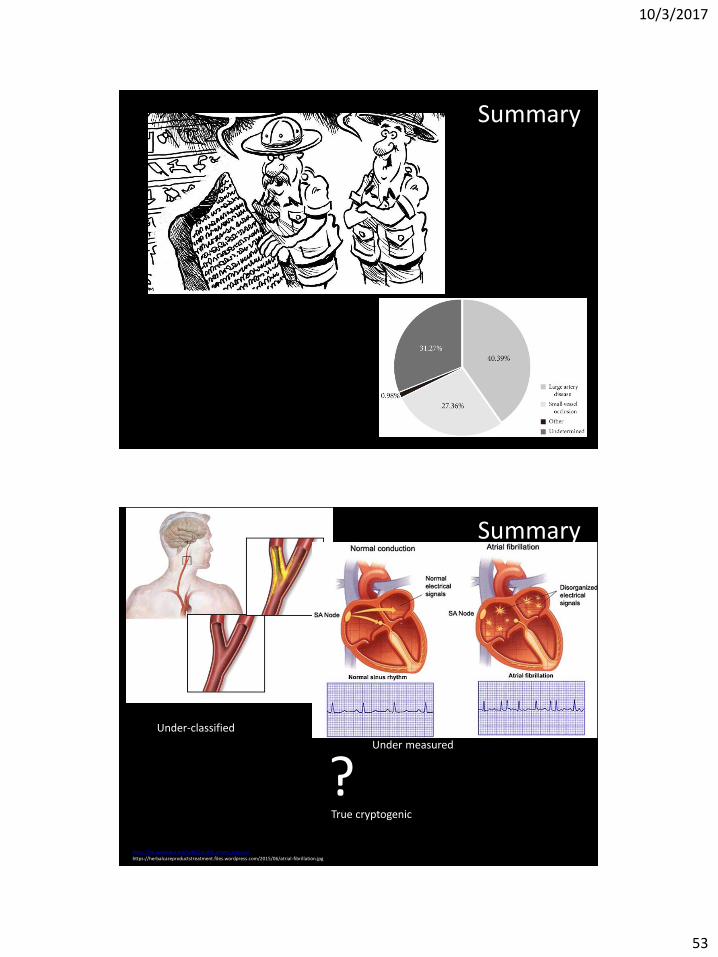
Epidemiology of cryptogenic stroke

10/3/2017
14
Geun Oh, Hyung & Rhee, Eun-Jung & Kim, Tae-Woong & Bok Lee, Kyung & Park, Jeong-Ho & Yang, Kwang & Jeong, Dushin & Park, Hyung-Kook. (2011). Higher Glycated Hemoglobin Level Is Associated with Increased Risk for Ischemic Stroke in Non-Diabetic Korean Male Adults. Diabetes & metabolism journal. 35. 551-7. 10.4093/dmj.2011.35.5.551.
Reference Study Design Sample Size Mean Age (years) Criteria for
Cryptogenic Stroke Frequency of Cryptogenic
Stroke
Besancon Stroke Registry (2000)63 Prospective registry 1776 71 Study-specific 18%
Athens Stroke Registry (2000)64 Prospective registry of first-ever strokes 885 70 Not specified 21%
German Stroke Data Bank (2001)65 Prospective registry 5017 66 Modified TOAST criteria 23%
WARSS (2001)66 Randomized trial 2206 63 TOAST criteria 26%
Erlangen Study (2001)67 Population-based 583 73 TOAST criteria 32%
Ankara (2002)68 Prospective registry 264 66 TOAST criteria 33%
Suwon (2003)69 Prospective registry 204 62 TOAST criteria 18%
TULIPS (Japan) (2004)70 Prospective registry 831 72 NINDS SDB 23%
Perugia (2006)71 Prospective stroke unit 358 NR TOAST criteria 17%
PRoFESS (2008)72 Randomized trial 20,332 66 TOAST criteria 16%
Bern (2008)73 Prospective registry 1288 NR TOAST criteria 39%
Buenos Aires (2010)74 Retrospective case series 155 67 TOAST criteria 27%
ASTRAL (2010)75 Prospective inpatient registry 1633 73 Modified TOAST
criteria 12%
North Dublin (2010)8 Population-based registry 381 NR Causative Classification System 26%
VITATOPS (2010)76 Randomized trial 8164 63 Study-specific 14%
PERFORM (2011)77 Randomized trial 19,100 67 Study-specific 22%
Mannheim Stroke Center (2012)78 Prospective case series 103 69 TOAST criteria 30%
Hebi, China (2012)79 Retrospective case series 425 65 TOAST criteria 16%
South Korea (2012)80 Prospective hospital-based registry 3278 64 TOAST criteria 21%
Miami/Mexico City (2012)81 Prospective registry of Hispanics 671 NR Modified TOAST criteria 17%
Santiago, Chile (2012)82 Prospective stroke unit 380 66 TOAST criteria 20%
Barcelona (2012)83 Prospective stroke unit 274 NR TOAST criteria 32%
Santiago de Compostela (2013)84 Prospective case series 1050 NR TOAST criteria 35% Bavaria (2013)85 Prospective stroke unit 393 62 TOAST criteria 17%
NR = not reported. TIA = transient ischemic attack. NINDS SDB = National Institute of Neurological Disorders and Stroke Data Bank
Frequency of Cryptogenic Ischemic Stroke Varies According to Study Design, Age, and Diagnostic Criteria for Cryptogenic Stroke Adapted from Hart RG, Diener H-C, Coutts SB, Easton JD, Granger CB, O’Donnell MJ, Sacco RL, Connolly SJ, for the Cryptogenic Stroke/ESUS International Working Group, with permission.
10/3/2017
15
Factors influencing prevalence
• Classification scheme:
– TOAST
– Causative Classification Scheme (CCS)
• supra-aortic large-vessel disease, cardioaortic embolism, small-vessel occlusion, other uncommon causes, or undetermined
• evident, probable, or possible
• Undetermined: unknown-cryptogenic embolism, unknown-other cryptogenic, unclassified, and incomplete evaluation
• lowest proportion classified as undetermined (26% versus 39% for TOAST in the North Dublin Stroke Study, n = 381
Factors influencing prevalence
• Population characteristics
– Age: younger cohorts
– Sex: ᴓ
– Race: AA and Hispanic
– Vascular risk factors: particularly hypertension: lower proportions (more than controls though)
10/3/2017
16
Factors influencing prevalence..cont.
• Diagnostic testing:
– Large vessel: Intracranial and intracranial: MRA, CTA and catheter based angio better than US
– Small vessel: Imaging : MRI, Clinical stroke syndrome: clinician
– Cardio-embolic: TEE>TTE
Proposed etiologies
• Common risk factors shared by small vessel, large vessel, or cardiac cause: HTN, smoking, DLD, Obesity, DM
• Conceptual framework:
– Under-classified,
– under-measured
– true cryptogenic
10/3/2017
17
https://en.wikipedia.org/wiki/Carotid_artery_stenosis https://herbalcareproductstreatment.files.wordpress.com/2015/06/atrial-fibrillation.jpg
? Classification (Under-classified)
Measurement (Under measured)
True cryptogenic
Case presentation 1 (Under-Measured Cryptogenic)
• 62-year-old female
• H/o hypertension and obesity
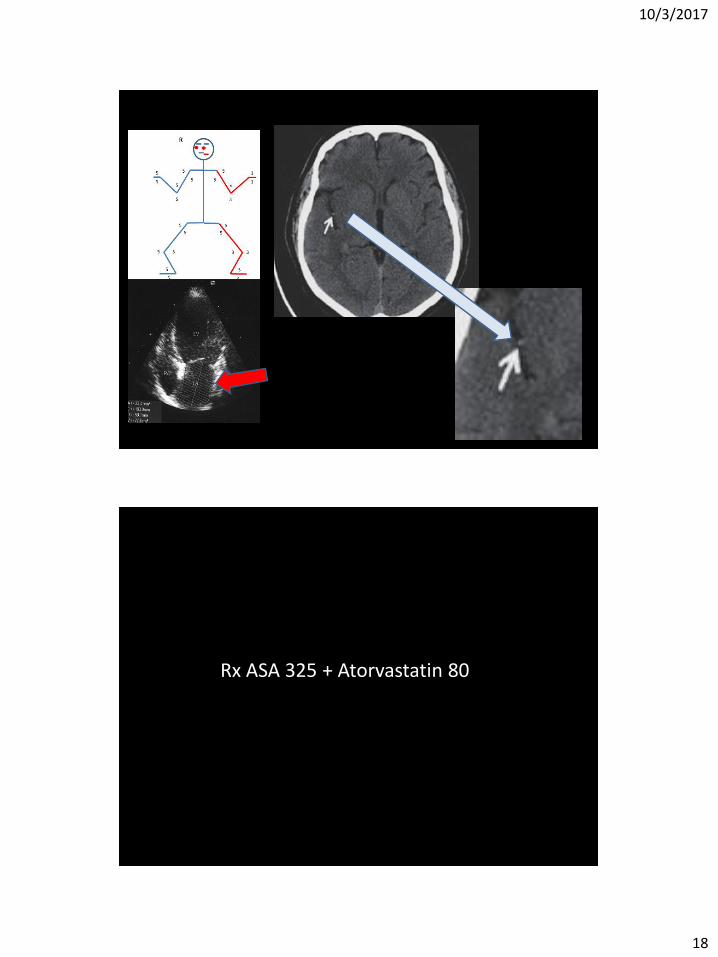
10/3/2017
18
Rx ASA 325 + Atorvastatin 80
10/3/2017
19
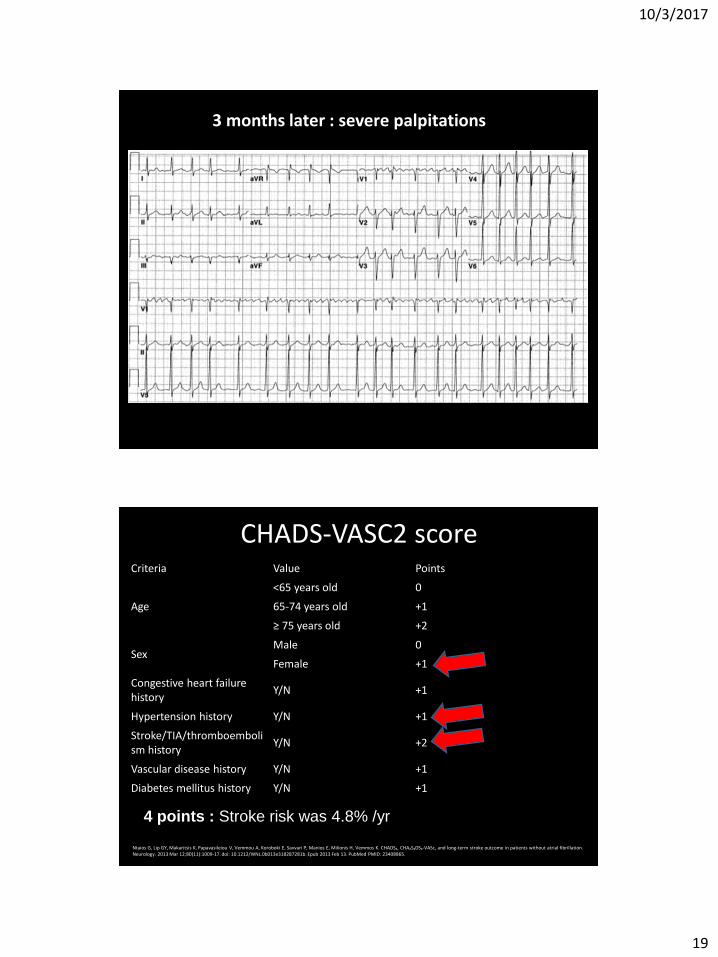
3 months later : severe palpitations
CHADS-VASC2 score
4 points : Stroke risk was 4.8% /yr
Criteria Value Points
Age
<65 years old 0
65-74 years old +1
≥ 75 years old +2
Sex Male 0
Female +1
Congestive heart failure history
Y/N +1
Hypertension history Y/N +1
Stroke/TIA/thromboembolism history
Y/N +2
Vascular disease history Y/N +1
Diabetes mellitus history Y/N +1
Ntaios G, Lip GY, Makaritsis K, Papavasileiou V, Vemmou A, Koroboki E, Savvari P, Manios E, Milionis H, Vemmos K. CHADS₂, CHA₂S₂DS₂-VASc, and long-term stroke outcome in patients without atrial fibrillation. Neurology. 2013 Mar 12;80(11):1009-17. doi: 10.1212/WNL.0b013e318287281b. Epub 2013 Feb 13. PubMed PMID: 23408865.
10/3/2017
20
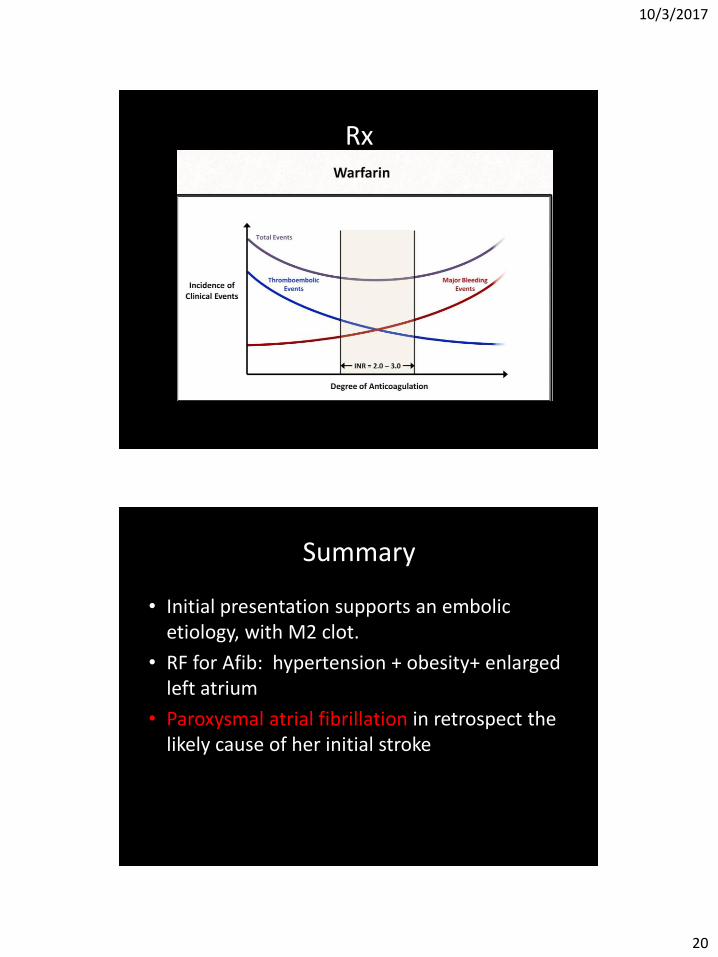
Rx
Summary
• Initial presentation supports an embolic etiology, with M2 clot.
• RF for Afib: hypertension + obesity+ enlarged left atrium
• Paroxysmal atrial fibrillation in retrospect the likely cause of her initial stroke
10/3/2017
21
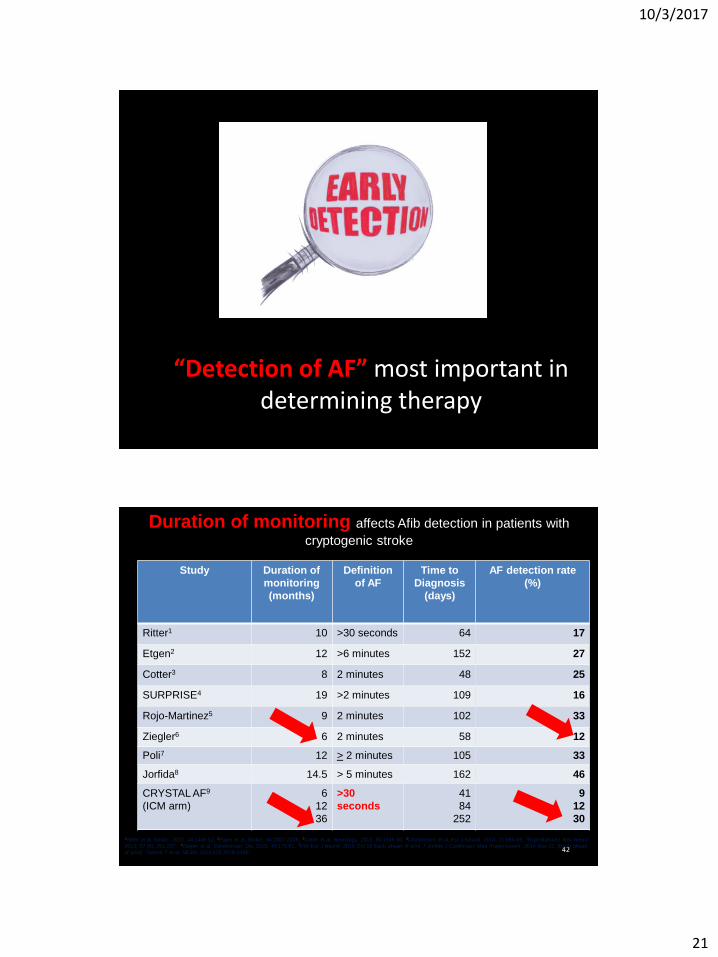
“Detection of AF” most important in determining therapy
42
Duration of monitoring affects Afib detection in patients with
cryptogenic stroke
Study Duration of
monitoring
(months)
Definition
of AF
Time to
Diagnosis
(days)
AF detection rate
(%)
Ritter1 10 >30 seconds 64 17
Etgen2 12 >6 minutes 152 27
Cotter3 8 2 minutes 48 25
SURPRISE4 19 >2 minutes 109 16
Rojo-Martinez5 9 2 minutes 102 33
Ziegler6 6 2 minutes 58 12
Poli7 12 > 2 minutes 105 33
Jorfida8 14.5 > 5 minutes 162 46
CRYSTAL AF9
(ICM arm)
6
12
36
>30
seconds
41
84
252
9
12
30
1Ritter et al, Stroke. 2013, 44:1449-52; 2Etgen et al, Stroke. 44:2007-2009; 3Cotter et al, Neurology. 2013, 80:1546-50; 4Christensen et al, Eur J Neurol. 2014, 21:884-89; 5Rojo-Martinez Rev Neurol
2013; 57 (6): 251-257; 6Ziegler et al, Cerebrovasc Dis. 2015, 40:175-81. 7Poli Eur J Neurol. 2015 Oct 16 Epub ahead of print ;8 Jorfida J Cardiovasc Med (Hagerstown). 2014 Nov 15. [Epub ahead
of print] 9Sanna T et al, NEJM. 2014;370:2478-2486;

10/3/2017
22
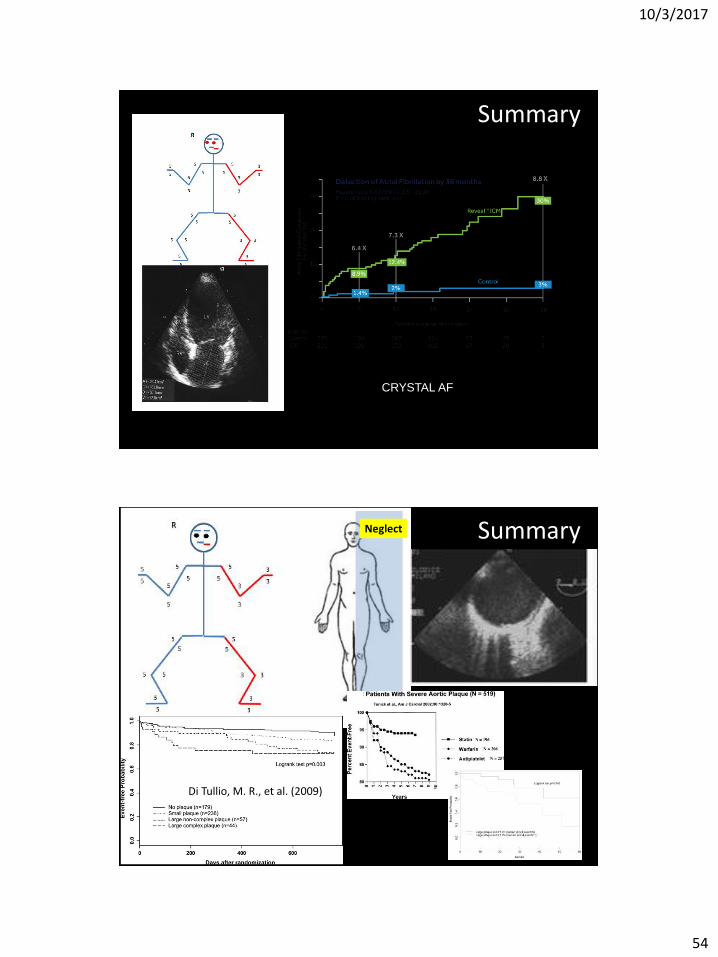
Detection of AF is most important in determining therapy, how long the heart is monitored is important: CRYSTAL-AF trial (2014)
CRYSTAL AF = CRYptogenic STroke and underlying. AtriaL Fibrillation
10/3/2017
23
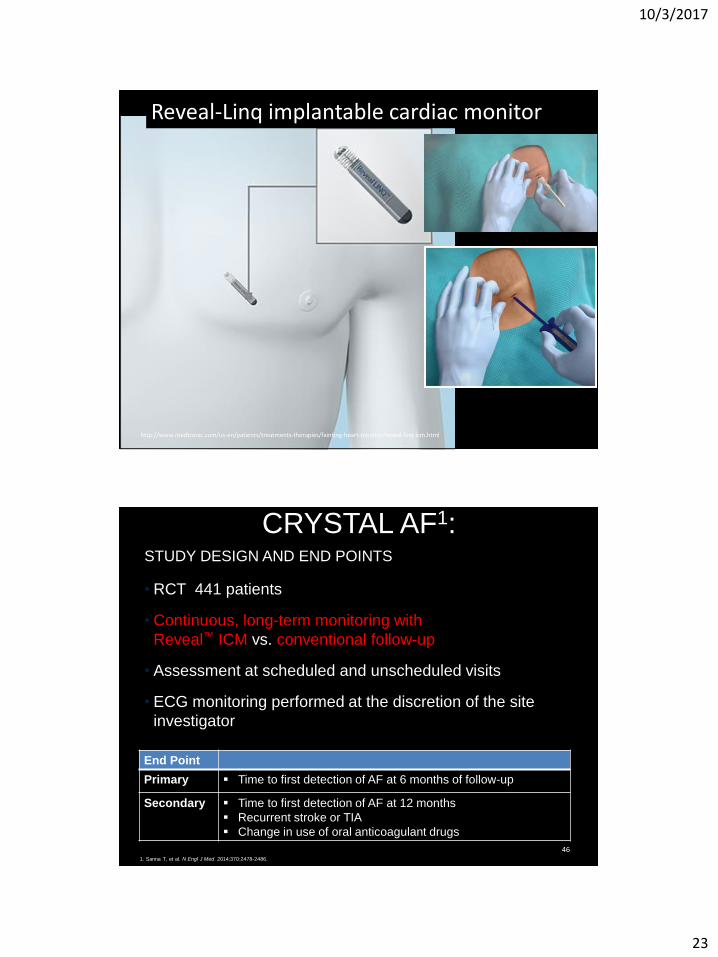
http://www.medtronic.com/us-en/patients/treatments-therapies/fainting-heart-monitor/reveal-linq-icm.html
Reveal-Linq implantable cardiac monitor
46
CRYSTAL AF1:
STUDY DESIGN AND END POINTS
• RCT 441 patients
• Continuous, long-term monitoring with
Reveal™ ICM vs. conventional follow-up
• Assessment at scheduled and unscheduled visits
• ECG monitoring performed at the discretion of the site
investigator
20%
15%
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
End Point
Primary Time to first detection of AF at 6 months of follow-up
Secondary Time to first detection of AF at 12 months
Recurrent stroke or TIA
Change in use of oral anticoagulant drugs
10/3/2017
24
47
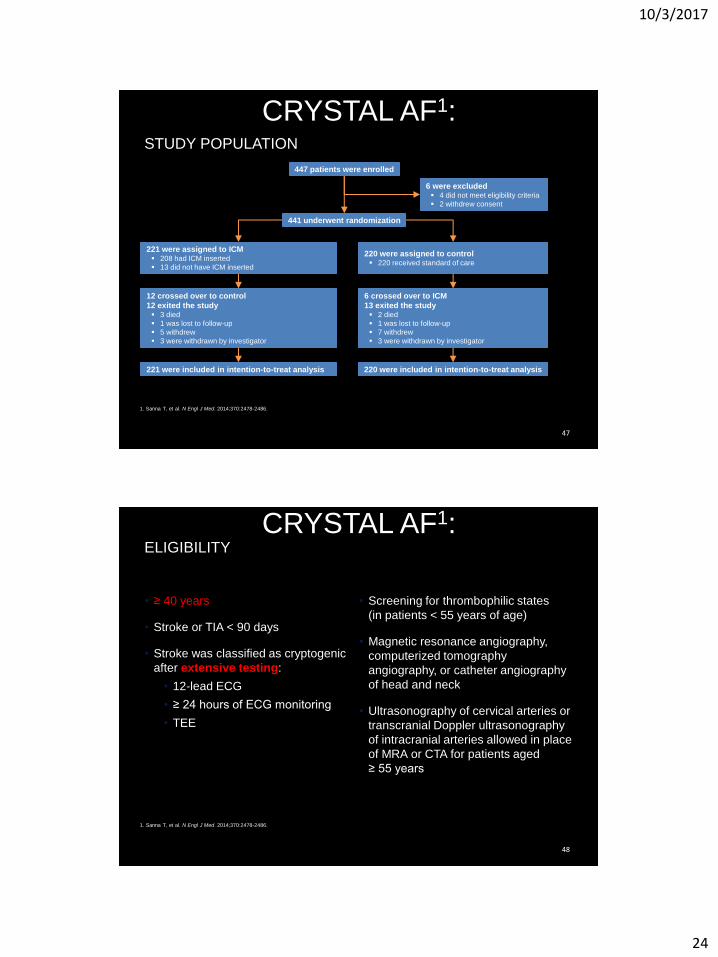
CRYSTAL AF1:
STUDY POPULATION
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
447 patients were enrolled
6 were excluded 4 did not meet eligibility criteria
2 withdrew consent
441 underwent randomization
221 were assigned to ICM 208 had ICM inserted
13 did not have ICM inserted
220 were assigned to control 220 received standard of care
12 crossed over to control
12 exited the study 3 died
1 was lost to follow-up
5 withdrew
3 were withdrawn by investigator
6 crossed over to ICM
13 exited the study 2 died
1 was lost to follow-up
7 withdrew
3 were withdrawn by investigator
221 were included in intention-to-treat analysis 220 were included in intention-to-treat analysis
48
CRYSTAL AF1:
ELIGIBILITY
• ≥ 40 years
• Stroke or TIA < 90 days
• Stroke was classified as cryptogenic
after extensive testing:
• 12-lead ECG
• ≥ 24 hours of ECG monitoring
• TEE
• Screening for thrombophilic states
(in patients < 55 years of age)
• Magnetic resonance angiography,
computerized tomography
angiography, or catheter angiography
of head and neck
• Ultrasonography of cervical arteries or
transcranial Doppler ultrasonography
of intracranial arteries allowed in place
of MRA or CTA for patients aged
≥ 55 years
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
10/3/2017
25
49
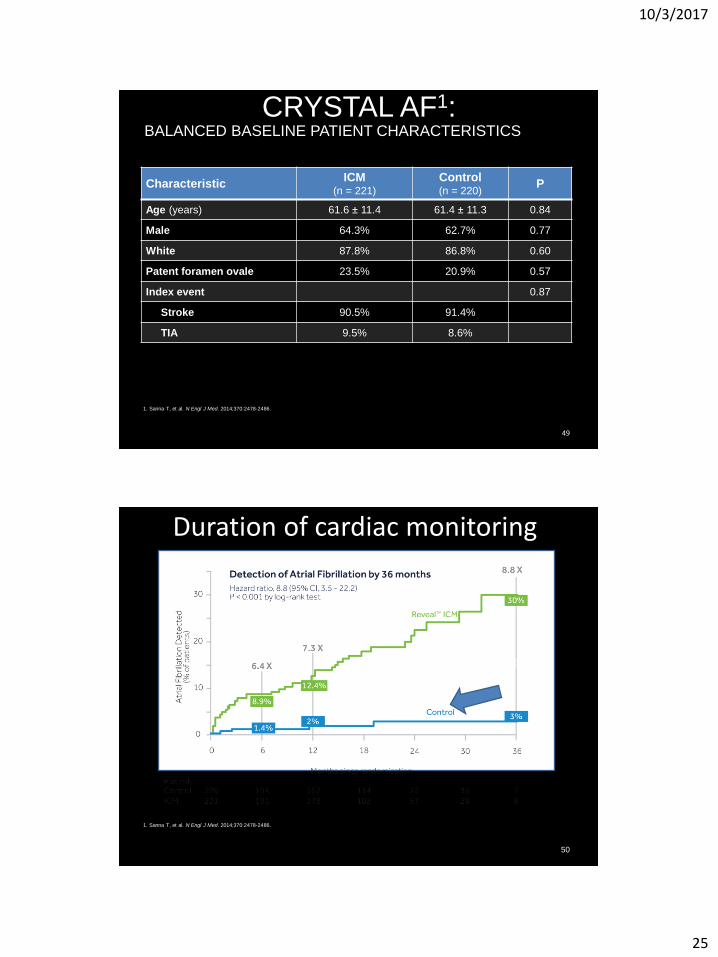
CRYSTAL AF1:
BALANCED BASELINE PATIENT CHARACTERISTICS
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
Characteristic ICM
(n = 221)
Control (n = 220)
P
Age (years) 61.6 ± 11.4 61.4 ± 11.3 0.84
Male 64.3% 62.7% 0.77
White 87.8% 86.8% 0.60
Patent foramen ovale 23.5% 20.9% 0.57
Index event 0.87
Stroke 90.5% 91.4%
TIA 9.5% 8.6%
50
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
Scheduled and unscheduled EKG monitoring
Duration of cardiac monitoring

10/3/2017
26
51
CRYSTAL AF:
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
12 months
97% of patients in whom AF was detected received oral anticoagulants
52
CRYSTAL AF:
MEDIAN TIME TO DETECTION OF AF
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
84 Days in the ICM group (range 18 to 265 days)
53 Days in control group (range 17 to 212 days)
10/3/2017
27
53
CRYSTAL AF1:
SAFETY
•2.4% removed due to infection or pocket
erosion
•Most common adverse events:
•Infection (1.4%)
•Pain (1.4%)
•Irritation or inflammation (1.9%)
Note: Reveal™ XT used in this study.
1. Sanna T, et al. N Engl J Med. 2014;370:2478-2486.
• Under-Measured Cryptogenic: Paroxysmal atrial fibrillation
• Detection makes a difference in treatment
• New evidence on monitoring duration

10/3/2017
28
Case presentation 2 : under-classified
• 71-year-old man
• h/o MI and PVD
CT angiography of carotids reports 40% stenosis bilaterally. Cardiac monitoring and transthoracic echocardiogram are normal. Transesophageal echocardiogram reveals non-significant atherosclerosis of aortic arch (<4 mm)
Neglect
10/3/2017
29
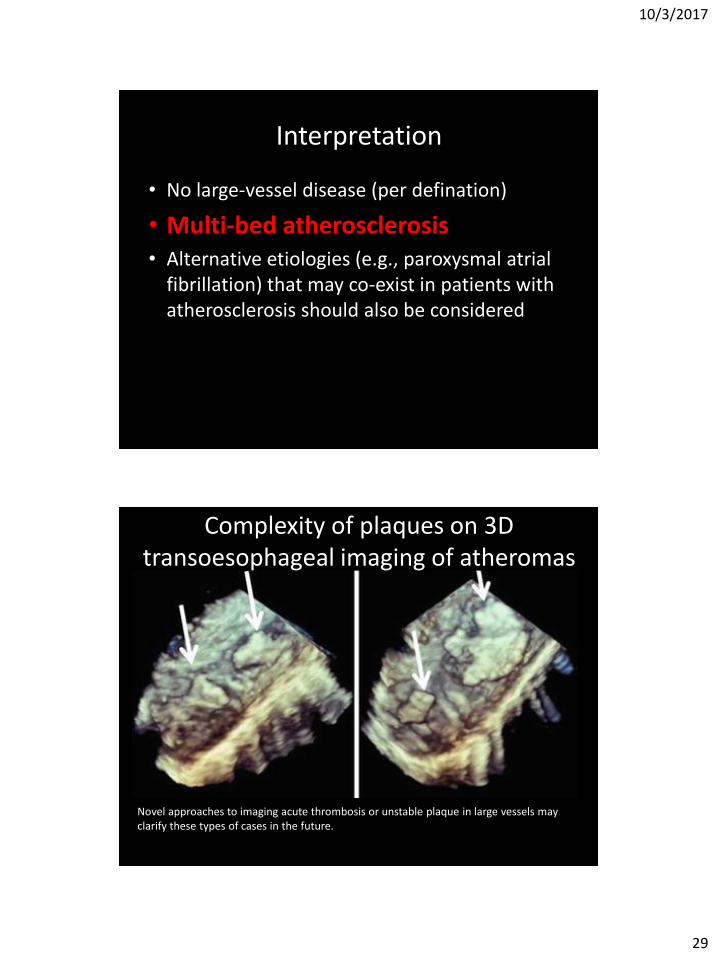
Interpretation
• No large-vessel disease (per defination)
• Multi-bed atherosclerosis • Alternative etiologies (e.g., paroxysmal atrial
fibrillation) that may co-exist in patients with atherosclerosis should also be considered
Novel approaches to imaging acute thrombosis or unstable plaque in large vessels may clarify these types of cases in the future.
Complexity of plaques on 3D transoesophageal imaging of atheromas
10/3/2017
30
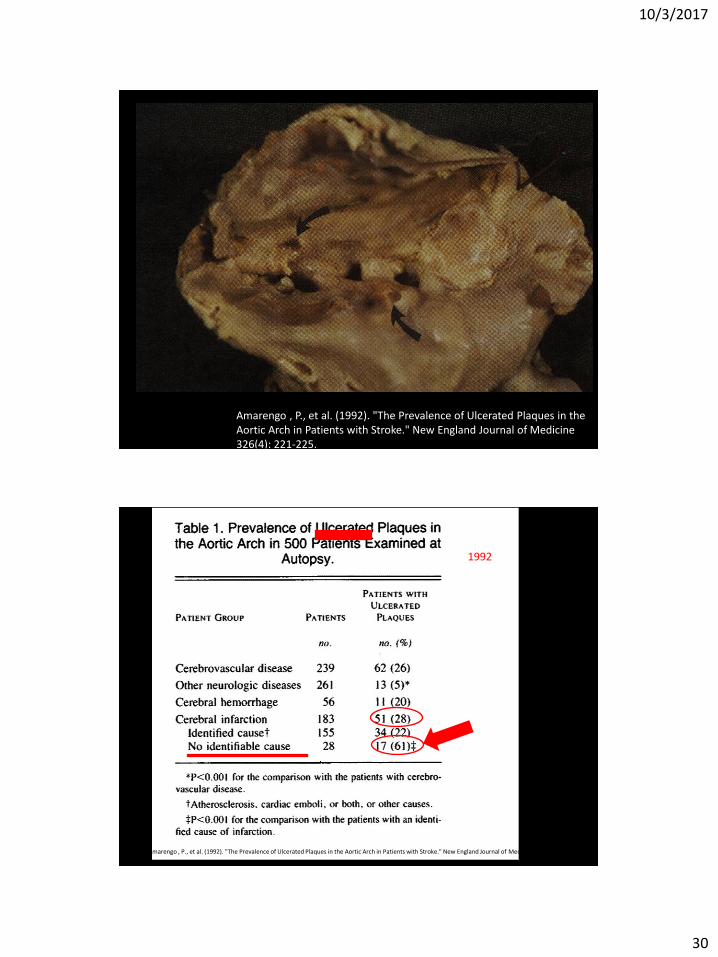
Amarengo , P., et al. (1992). "The Prevalence of Ulcerated Plaques in the Aortic Arch in Patients with Stroke." New England Journal of Medicine 326(4): 221-225.
Amarengo , P., et al. (1992). "The Prevalence of Ulcerated Plaques in the Aortic Arch in Patients with Stroke." New England Journal of Medicine 326(4): 221-225.
1992
10/3/2017
31
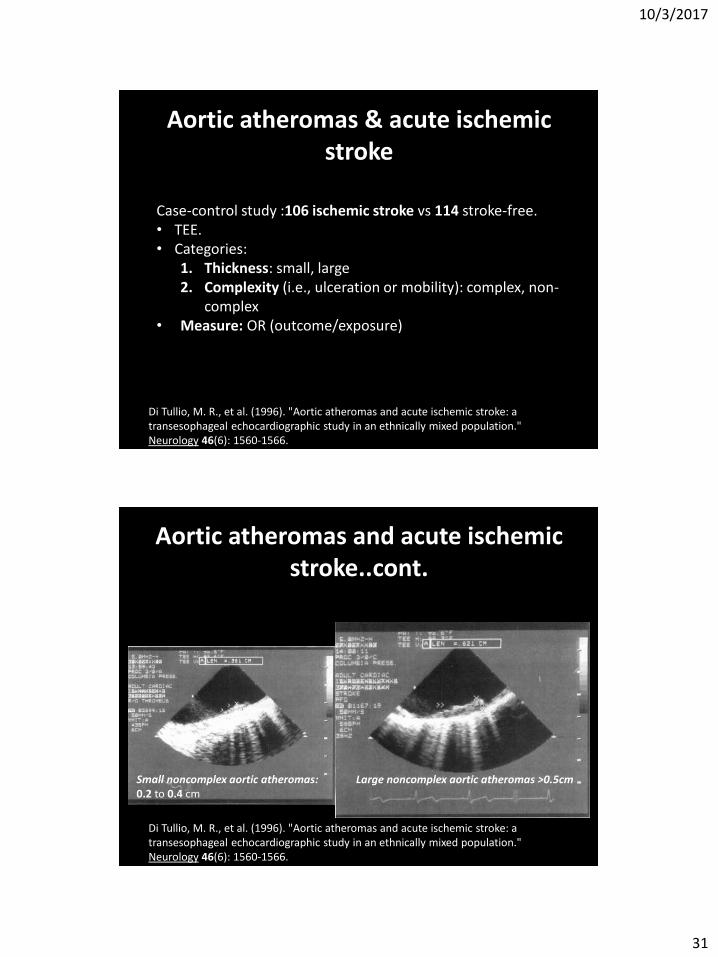
Aortic atheromas & acute ischemic stroke
Di Tullio, M. R., et al. (1996). "Aortic atheromas and acute ischemic stroke: a transesophageal echocardiographic study in an ethnically mixed population." Neurology 46(6): 1560-1566.
Case-control study :106 ischemic stroke vs 114 stroke-free. • TEE. • Categories:
1. Thickness: small, large 2. Complexity (i.e., ulceration or mobility): complex, non-
complex • Measure: OR (outcome/exposure)
Large noncomplex aortic atheromas >0.5cm
Aortic atheromas and acute ischemic stroke..cont.
Di Tullio, M. R., et al. (1996). "Aortic atheromas and acute ischemic stroke: a transesophageal echocardiographic study in an ethnically mixed population." Neurology 46(6): 1560-1566.
Small noncomplex aortic atheromas: 0.2 to 0.4 cm
10/3/2017
32
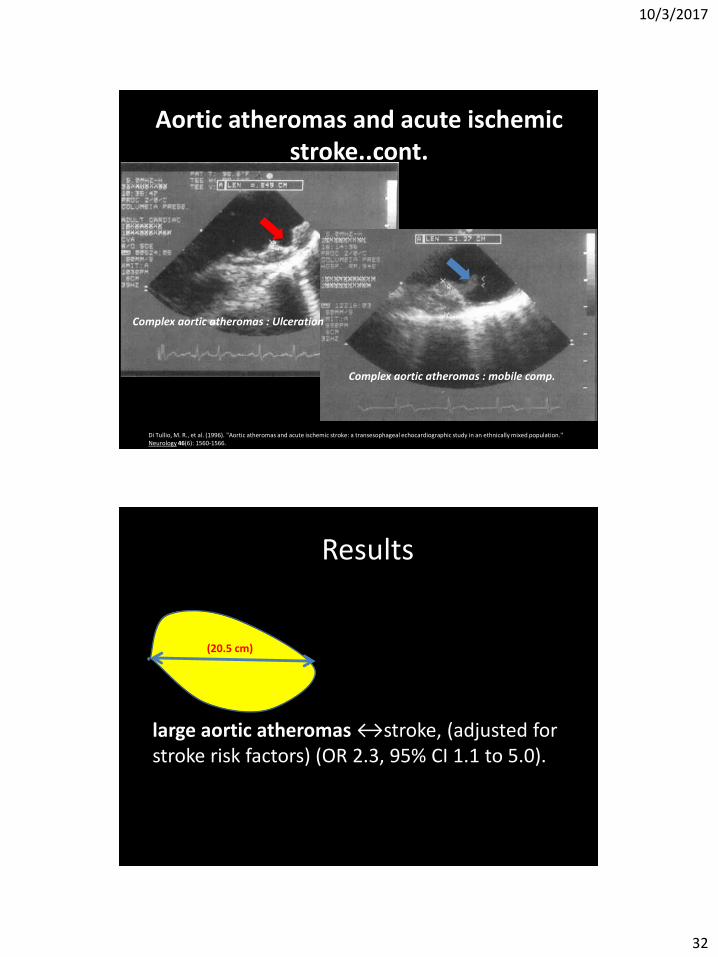
Aortic atheromas and acute ischemic stroke..cont.
Di Tullio, M. R., et al. (1996). "Aortic atheromas and acute ischemic stroke: a transesophageal echocardiographic study in an ethnically mixed population." Neurology 46(6): 1560-1566.
Complex aortic atheromas : Ulceration
Complex aortic atheromas : mobile comp.
Results
large aortic atheromas ↔stroke, (adjusted for stroke risk factors) (OR 2.3, 95% CI 1.1 to 5.0).
(20.5 cm)
10/3/2017
33
Frequency of Ulcerated or mobile plaque in >60 yr olds with cryptogenic stroke vs controls
>60 years
? 22% 8%;
OR 3.4,
95% CI 1.1 to 11.21,
14%
Summary
• While considering aortic arch atheroma one must consider the size as well as the complexity as a risk factor for cryptogenic stroke
10/3/2017
34
Secondary prevention: Aortic Arch Plaques
Treatment With Warfarin or Aspirin:
RCT 0 to 85 years of age 516 patients TEE Aspirin in 325-mg tablets vs Warfarin :INR of 1.4 to 2.8 Vs identical placebo. FU 2 years Di Tullio MR, Russo C, Jin Z, Sacco RL, Mohr JP, Homma S. Aortic Arch Plaques and Risk of Recurrent Stroke and Death. Circulation. 2009;119(17):2376-2382. doi:10.1161/CIRCULATIONAHA.108.811935.
Primary end-points (2 yrs)
10/3/2017
35
• Two-year incidence of recurrent stroke/death was similar between the warfarin-treated (43 of 256, 16.4%) and aspirin-treated (41 of 260, 15.8%; P=0.43) groups.
• The incidence of major hemorrhagic events was low and similar between the warfarin and aspirin groups (0.88 versus 2.16 per 100 patient-years; P0.13).
• Minor hemorrhagic events were more frequent in the warfarin group (26.76 versus 10.0 per 100 patient-years; P0.001).
10/3/2017
36
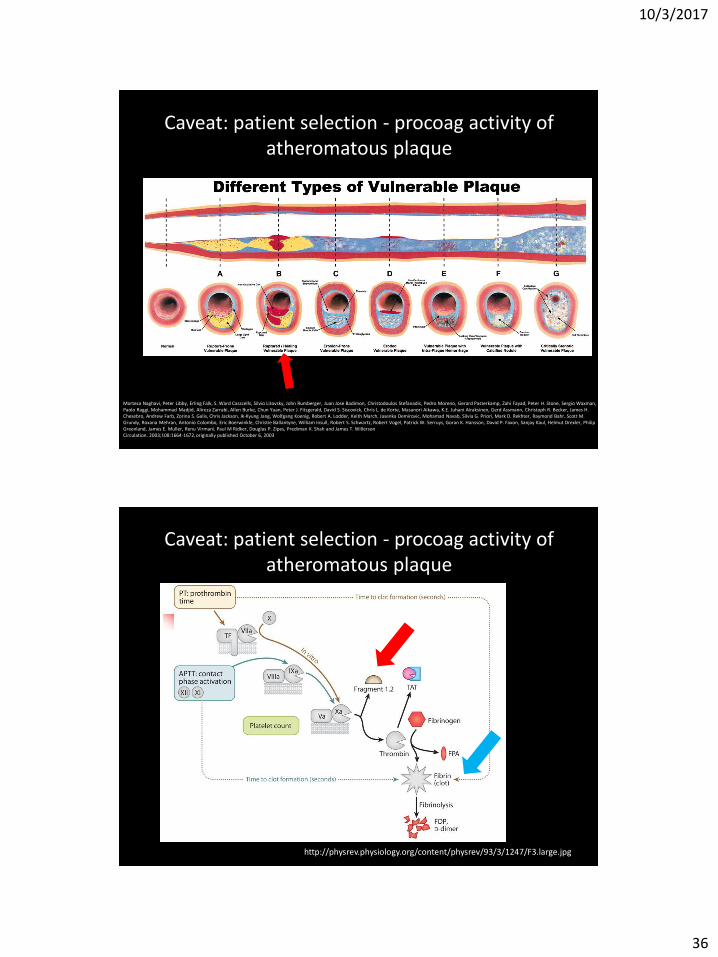
Caveat: patient selection - procoag activity of atheromatous plaque
Morteza Naghavi, Peter Libby, Erling Falk, S. Ward Casscells, Silvio Litovsky, John Rumberger, Juan Jose Badimon, Christodoulos Stefanadis, Pedro Moreno, Gerard Pasterkamp, Zahi Fayad, Peter H. Stone, Sergio Waxman, Paolo Raggi, Mohammad Madjid, Alireza Zarrabi, Allen Burke, Chun Yuan, Peter J. Fitzgerald, David S. Siscovick, Chris L. de Korte, Masanori Aikawa, K.E. Juhani Airaksinen, Gerd Assmann, Christoph R. Becker, James H. Chesebro, Andrew Farb, Zorina S. Galis, Chris Jackson, Ik-Kyung Jang, Wolfgang Koenig, Robert A. Lodder, Keith March, Jasenka Demirovic, Mohamad Navab, Silvia G. Priori, Mark D. Rekhter, Raymond Bahr, Scott M. Grundy, Roxana Mehran, Antonio Colombo, Eric Boerwinkle, Christie Ballantyne, William Insull, Robert S. Schwartz, Robert Vogel, Patrick W. Serruys, Goran K. Hansson, David P. Faxon, Sanjay Kaul, Helmut Drexler, Philip Greenland, James E. Muller, Renu Virmani, Paul M Ridker, Douglas P. Zipes, Prediman K. Shah and James T. Willerson Circulation. 2003;108:1664-1672, originally published October 6, 2003
http://physrev.physiology.org/content/physrev/93/3/1247/F3.large.jpg
Caveat: patient selection - procoag activity of atheromatous plaque
10/3/2017
37
Aortic Plaques and Risk of Ischemic Stroke
Caveat: patient selection - procoag activity of atheromatous plaque (APRIS
trial)
Di Tullio MR, Homma S, Jin Z, Sacco RL. Aortic Atherosclerosis, Hypercoagulability and Stroke: the Aortic Plaque and Risk of Ischemic Stroke (APRIS) Study. Journal of the American College of Cardiology. 2008;52(10):855-861. doi:10.1016/j.jacc.2008.04.062.
Transesophageal echocardiography in 255 patients with first acute ischemic stroke Vs 209 control subjects matched by age, sex and race-ethnicity. The association between arch plaques and hypercoagulability, and its effect on the stroke risk, was assessed with a case-control design
10/3/2017
38
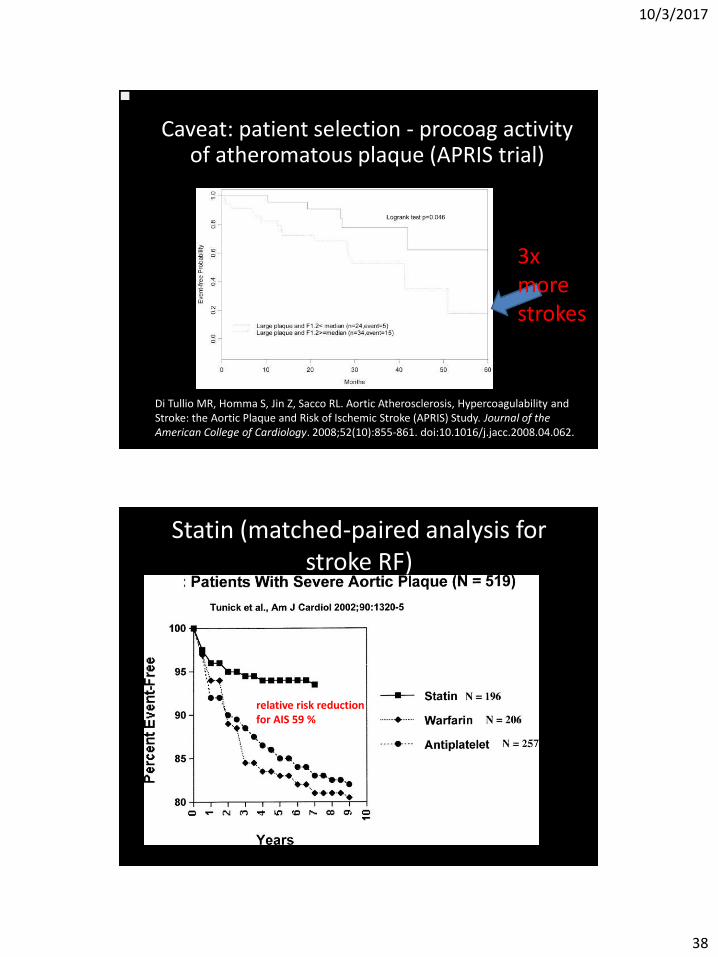
Di Tullio MR, Homma S, Jin Z, Sacco RL. Aortic Atherosclerosis, Hypercoagulability and Stroke: the Aortic Plaque and Risk of Ischemic Stroke (APRIS) Study. Journal of the American College of Cardiology. 2008;52(10):855-861. doi:10.1016/j.jacc.2008.04.062.
Caveat: patient selection - procoag activity of atheromatous plaque (APRIS trial)
3x more strokes
Statin (matched-paired analysis for stroke RF)
relative risk reduction for AIS 59 %
10/3/2017
39
• Under-classified Cryptogenic: Aortic arch atheroma
• ASA~Warfarin in general
• Untested potential for Warfarin in hypercoagulable states
• Statins highly effective in risk reduction
Case presentation 3: True cryptogenic
• 38-year-old woman
• ᴓ PMHx
• ᴓ traditional risk factors for ischemic stroke,
• ᴓ medical co-morbidities,
• ᴓ systemic illness
• ᴓ FH of premature stroke.
10/3/2017
40
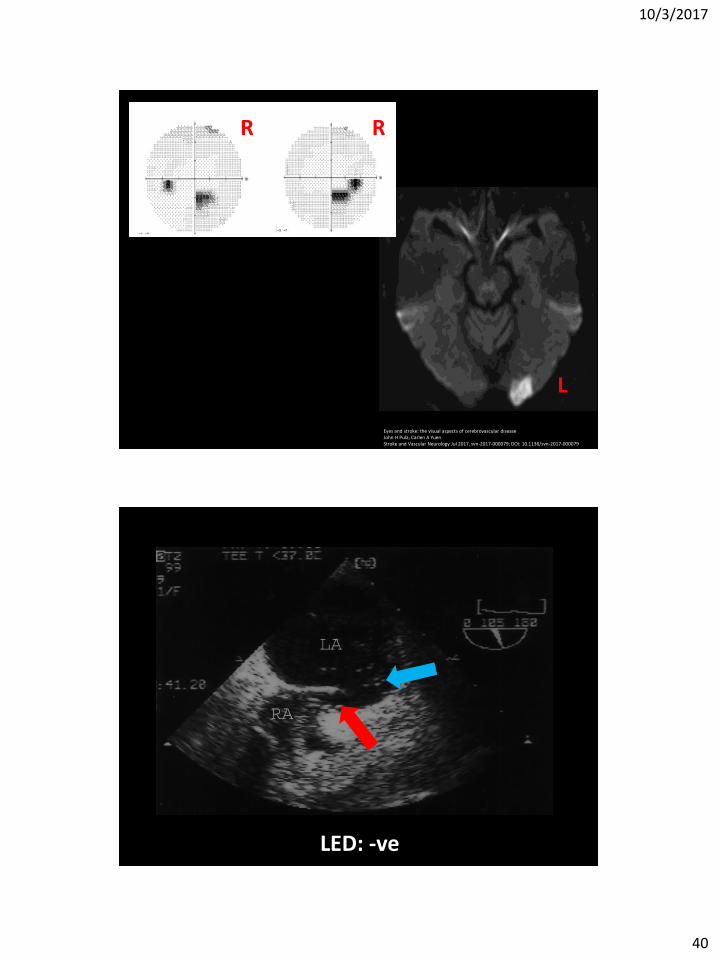
Eyes and stroke: the visual aspects of cerebrovascular disease John H Pula, Carlen A Yuen Stroke and Vascular Neurology Jul 2017, svn-2017-000079; DOI: 10.1136/svn-2017-000079
R R
L
LED: -ve
10/3/2017
41
• Five-day Holter monitor: WNL
• CT angio H&N: WNL
• MRV: WNL
• Thrombophilic screen: WNL
Notes on true cryptogenic stroke
http://www.mayoclinic.org/diseases-conditions/patent-foramen-ovale/symptoms-causes/dxc-20345732 https://www.slideshare.net/Rajeswaran1990/cardio-vascular-diseases
?
10/3/2017
42
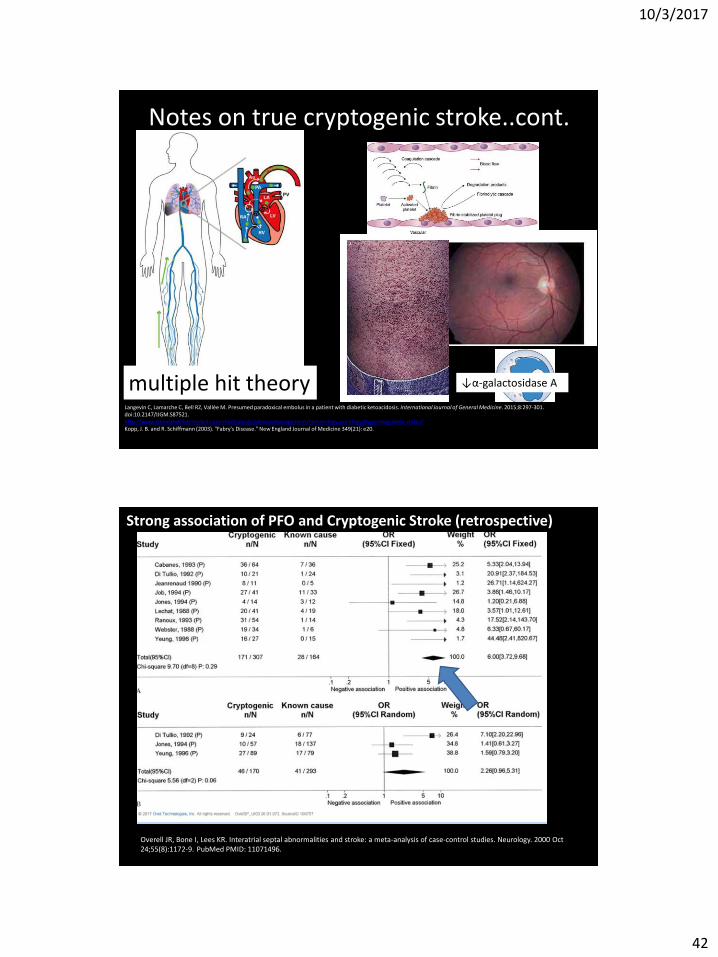
Notes on true cryptogenic stroke..cont.
multiple hit theory Langevin C, Lamarche C, Bell RZ, Vallée M. Presumed paradoxical embolus in a patient with diabetic ketoacidosis. International Journal of General Medicine. 2015;8:297-301. doi:10.2147/IJGM.S87521. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hematology-oncology/hypercoagulable-states/ Kopp, J. B. and R. Schiffmann (2003). "Fabry's Disease." New England Journal of Medicine 349(21): e20.
↓α-galactosidase A
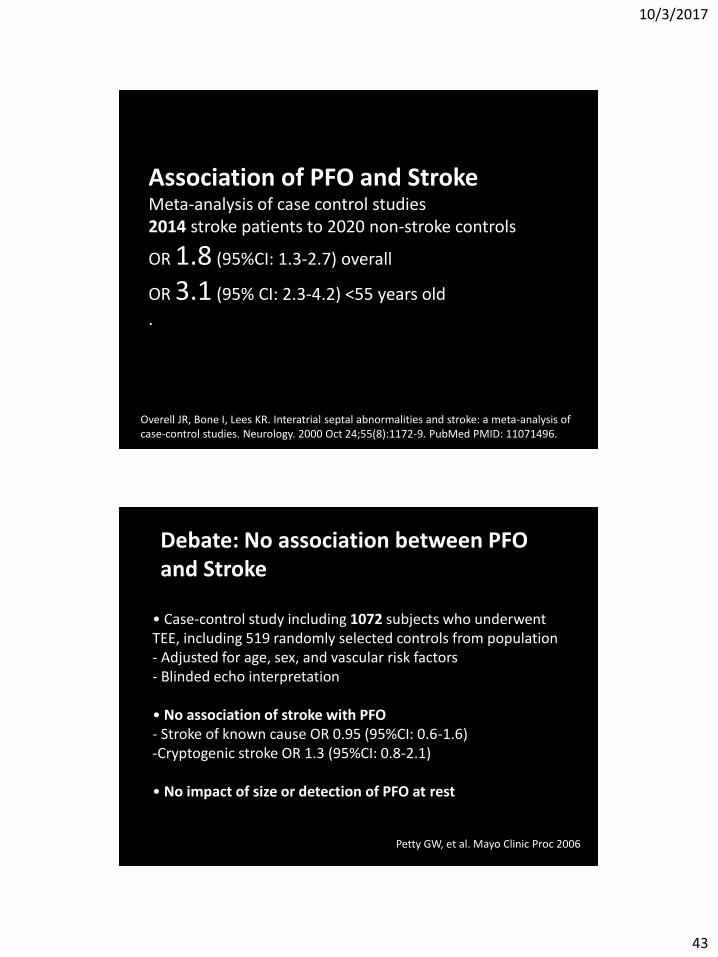
Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology. 2000 Oct 24;55(8):1172-9. PubMed PMID: 11071496.
Strong association of PFO and Cryptogenic Stroke (retrospective)
10/3/2017
43
Association of PFO and Stroke Meta-analysis of case control studies 2014 stroke patients to 2020 non-stroke controls
OR 1.8 (95%CI: 1.3-2.7) overall
OR 3.1 (95% CI: 2.3-4.2) <55 years old
.
Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology. 2000 Oct 24;55(8):1172-9. PubMed PMID: 11071496.
• Case-control study including 1072 subjects who underwent TEE, including 519 randomly selected controls from population - Adjusted for age, sex, and vascular risk factors - Blinded echo interpretation • No association of stroke with PFO - Stroke of known cause OR 0.95 (95%CI: 0.6-1.6) -Cryptogenic stroke OR 1.3 (95%CI: 0.8-2.1) • No impact of size or detection of PFO at rest
Petty GW, et al. Mayo Clinic Proc 2006
Debate: No association between PFO and Stroke
10/3/2017
44
PFO in Cryptogenic Stroke Study (PICSS)
PFO in (recurrent) Cryptogenic Stroke (PICSS): secondary prevention
• 42-center study that evaluated transesophageal echocardiographic findings in patients randomly assigned to warfarin or aspirin
• 630 stroke patients
– 312 (49.5%) warfarin
– 318 (50.5%) aspirin.
• Of these, 265 patients experienced cryptogenic stroke and 365 experienced known stroke subtypes
Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP; PFO in Cryptogenic Stroke Study (PICSS) Investigators. Effect of medical treatment in stroke patients with patent foramen ovale: patent foramen ovale in Cryptogenic Stroke Study. Circulation. 2002 Jun 4;105(22):2625-31. PubMed PMID: 12045168.
10/3/2017
45
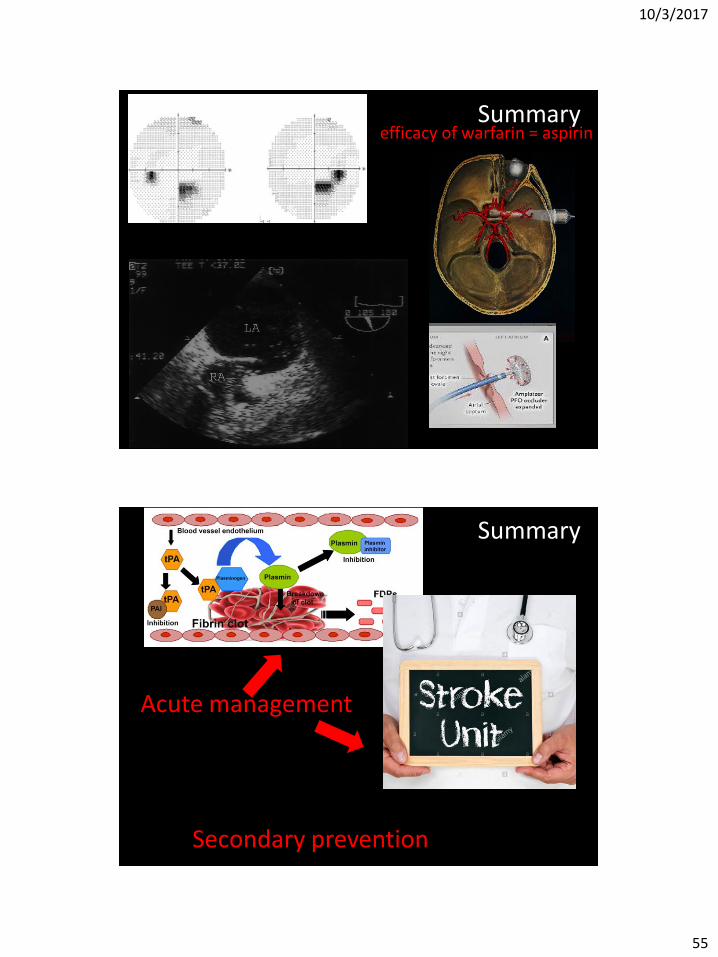
Primary end-points (2 yrs)
efficacy of warfarin ~ aspirin
Medical management:
=
https://acphospitalist.org/archives/2008/02/expert.htm
10/3/2017
46
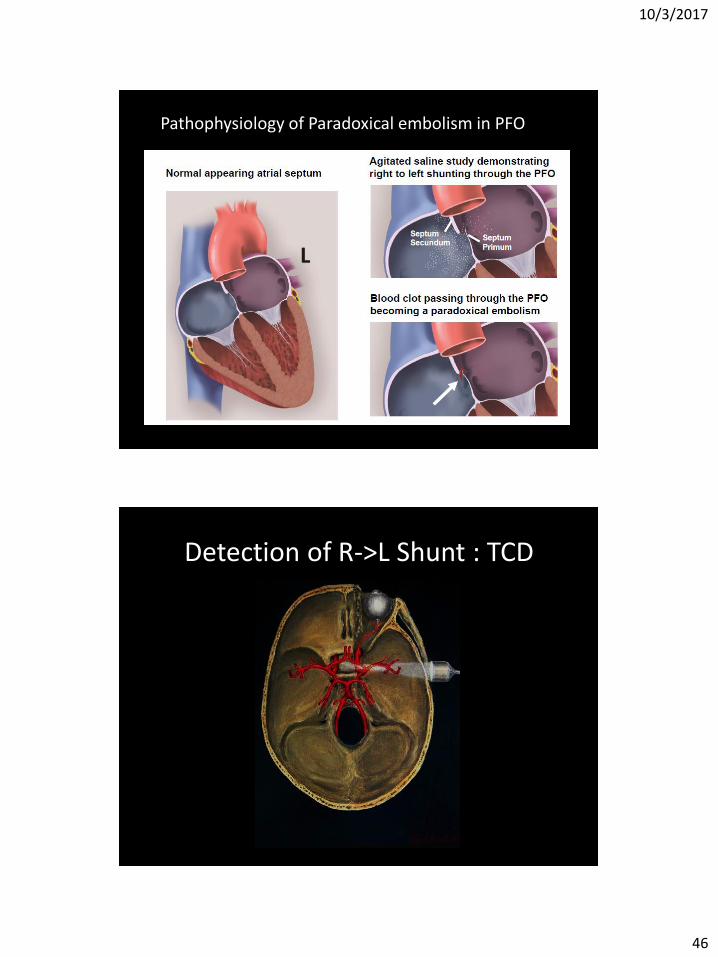
Pathophysiology of Paradoxical embolism in PFO
L
Detection of R->L Shunt : TCD
10/3/2017
47
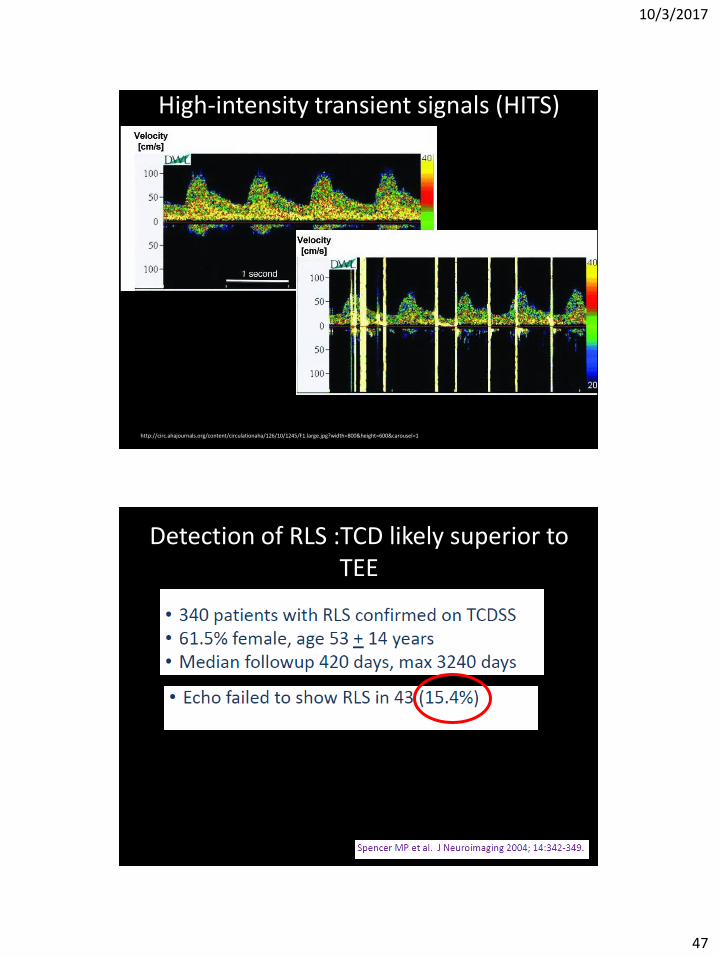
High-intensity transient signals (HITS)
http://circ.ahajournals.org/content/circulationaha/126/10/1245/F1.large.jpg?width=800&height=600&carousel=1
Detection of RLS :TCD likely superior to TEE
10/3/2017
48
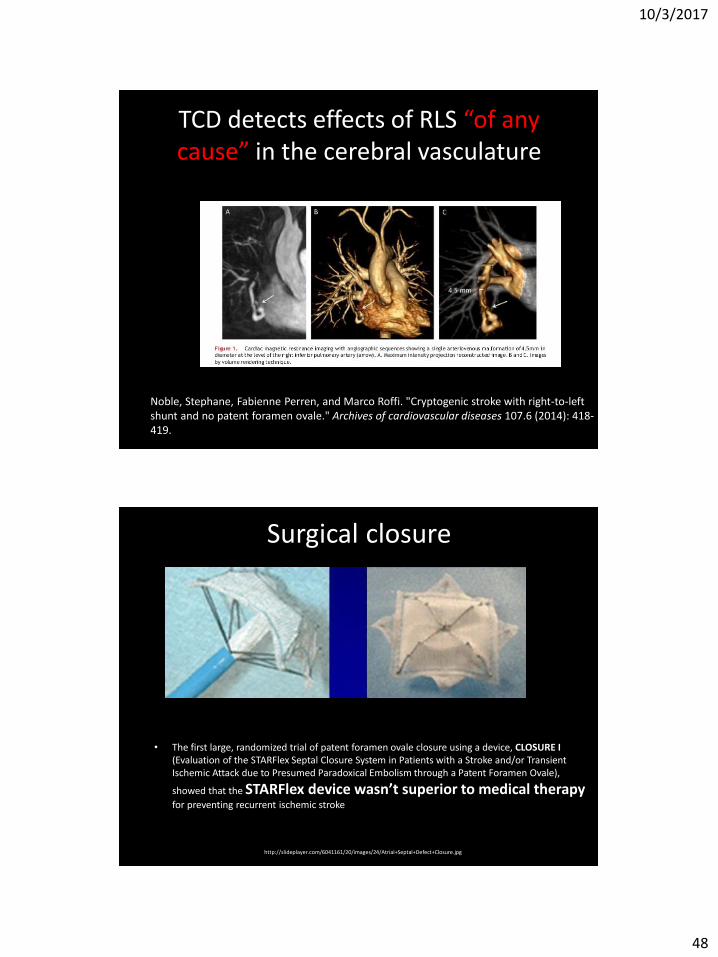
TCD detects effects of RLS “of any cause” in the cerebral vasculature
Noble, Stephane, Fabienne Perren, and Marco Roffi. "Cryptogenic stroke with right-to-left shunt and no patent foramen ovale." Archives of cardiovascular diseases 107.6 (2014): 418-419.
Surgical closure
• The first large, randomized trial of patent foramen ovale closure using a device, CLOSURE I (Evaluation of the STARFlex Septal Closure System in Patients with a Stroke and/or Transient Ischemic Attack due to Presumed Paradoxical Embolism through a Patent Foramen Ovale),
showed that the STARFlex device wasn’t superior to medical therapy
for preventing recurrent ischemic stroke
http://slideplayer.com/6041161/20/images/24/Atrial+Septal+Defect+Closure.jpg
10/3/2017
49
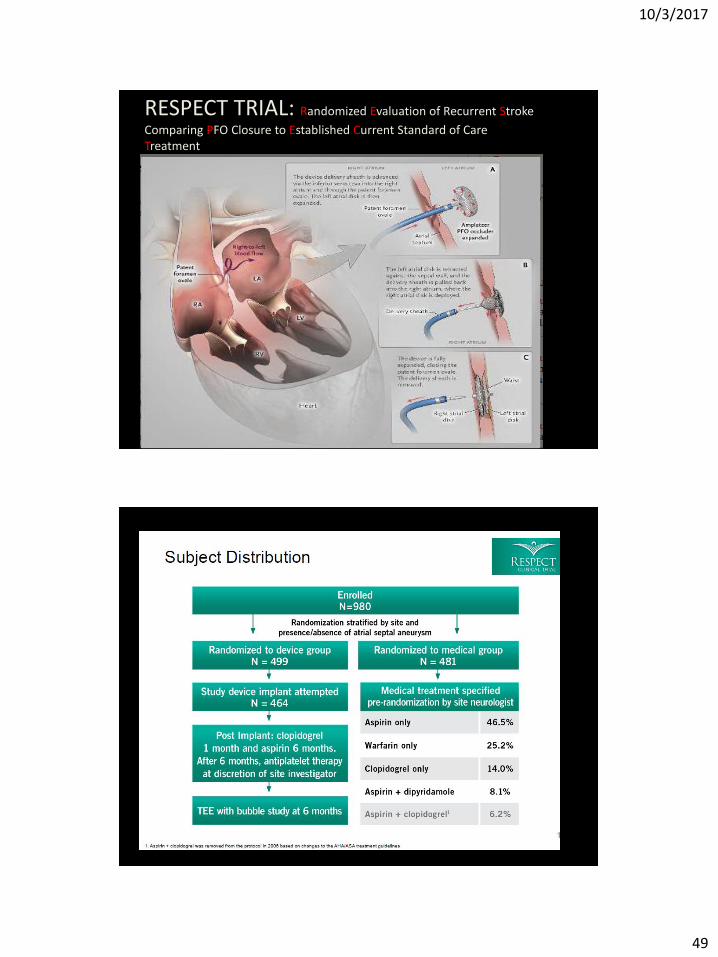
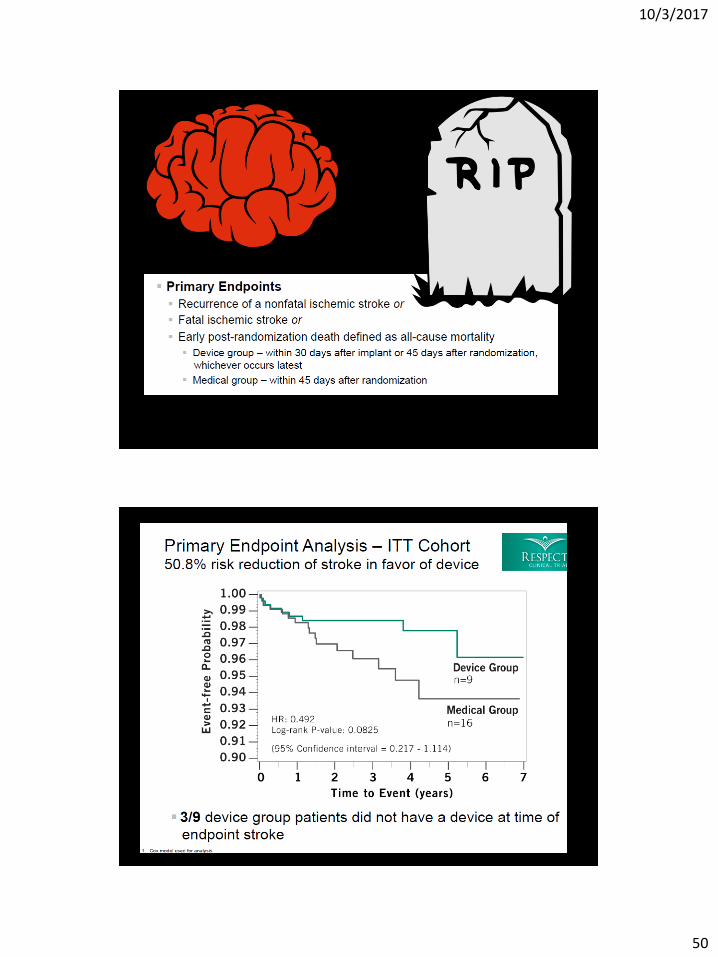
RESPECT TRIAL: Randomized Evaluation of Recurrent Stroke
Comparing PFO Closure to Established Current Standard of Care Treatment
10/3/2017
50
10/3/2017
51
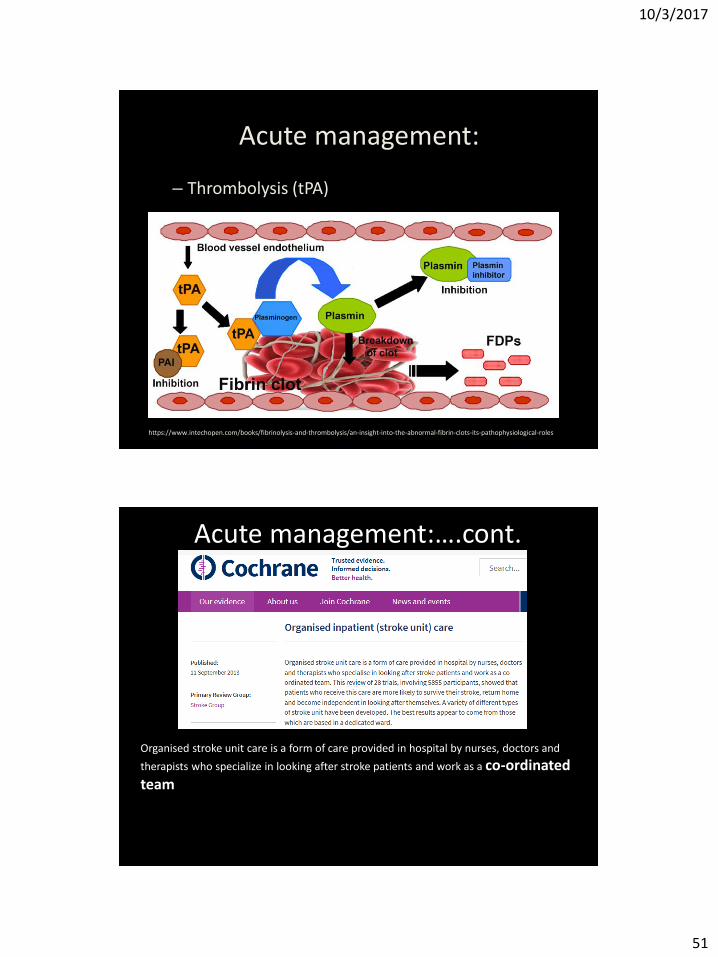
Acute management:
– Thrombolysis (tPA)
– Stroke unit care (organized inpatient care)
https://www.intechopen.com/books/fibrinolysis-and-thrombolysis/an-insight-into-the-abnormal-fibrin-clots-its-pathophysiological-roles
Organised stroke unit care is a form of care provided in hospital by nurses, doctors and
therapists who specialize in looking after stroke patients and work as a co-ordinated team
Acute management:….cont.
10/3/2017
52
• 28 trials, 5855 participants: – more likely to survive their stroke,
– return home
– become independent in looking after themselves.
• A variety of different types of stroke units.
Best results : dedicated ward.
Management implications…cont
• Secondary prevention:
– Lifestyle modifications
– Anti-HTN treatment
– Statin
– Anti-thrombotic (debate)
10/3/2017
53
Summary
https://en.wikipedia.org/wiki/Carotid_artery_stenosis https://herbalcareproductstreatment.files.wordpress.com/2015/06/atrial-fibrillation.jpg
? Under-classified
Under measured
True cryptogenic
Summary
10/3/2017
54
CRYSTAL AF
Summary
Neglect
Di Tullio, M. R., et al. (2009)
Summary
10/3/2017
55
efficacy of warfarin = aspirin Summary
Secondary prevention
Summary
Acute management
10/3/2017
56
Thank you
Questions?