april 2016 vol. 34, no. 2 - welcome to bcps 34(2) - 2016 bcps j.pdfprofessor md. abul kashem...
TRANSCRIPT

April 2016
Vol. 34, No. 2

Chairman
Dr. Quazi Tarikul Islam
Editor-In-Chief
Dr. Khan Abul Kalam Azad
Editors
Dr. Zafar Ahmed Latif
Dr. A. N. M. Zia-ur-Rahman
Dr. Emran Bin Yunus
Dr. Parveen Fatima
Dr. U. H. Shahera Khatun
Dr. Syed Atiqul Haq
Dr. Fakhruddin Mohammad Siddiqui
Dr. Syeda Afroza
Dr. Md. Ridwanur Rahman
Dr. Nooruddin Ahmed
Dr. Khwaja Nazim Uddin
Dr. Md. Abdul Hamid
Dr. A.H.M. Rowshon
Dr. Tapan Kumar Saha
Dr. A.B.M. Bayezid Hossain
Dr. Md. Titu Miah
Dr. Tripti Rani Das
Dr. Dipi Barua
Dr. Rubina Yasmin
Dr. Mohammad Robed Amin
Dr. S.M. Anwar Sadat
Dr. (Col) Md. Abdur Rab
Dr. Shariff Asfia Rahman
Dr. S.M. Quamrul Akther
Dr. Aparna Das
Dr. Syed Ghulam Mogni Mowla
Dr. Tanveer Ahmed
Dr. Khan Abul Kalam Azad
on behalf of the Bangladesh College
of Physicians and Surgeons
Asian Colour Printing
130 DIT Extension Road
Fakirerpool, Dhaka-1000
Tk. 400/- for local and US$ 40 for
overseas subscribers
Professor Md. Sanawar HossainProfessor Kanak Kanti BaruaProfessor Md. Ruhul Amin Professor A.B.M. Muksudul AlamProfessor T.I.M. Abdullah-Al-FaruqProfessor Shahana Akhter Rahman Professor Md. Abdul Jalil ChowdhuryProfessor Md. Azizul KahharProfessor Abdul Kader KhanProfessor Sayeba Akhter Professor Md. Abul Kashem KhandakerProfessor Mohammod ShahidullahProfessor Quazi Deen Mohammad Professor Kohinoor BegumProfessor Quazi Tarikul IslamProfessor Choudhury Ali KawserProfessor Iffat AraProfessor Nazmun Nahar Professor Major Gen. (Retd.) Md. Ali Akbar Professor Shamsuddin Ahmed
Editorial StaffAfsana HuqMohammed Ibrahim
The Journal of Bangladesh College
of Physicians and Surgeons is a
peer reviewed Journal. It is
published four times a year,
(January, April, July and October).
It accepts original articles, review
articles, and case reports.
Complimentary copies of the
journal are sent to libraries of all
medical and other relevant
academic institutions in the
country and selected institutions
abroad.
While every effort is always made
by the Editorial Board and the
members of the Journal Committee
to avoid inaccurate or misleading
information appearing in the
Journal of Bangladesh College
of Physicians and Surgeons,
information within the individual
article are the responsibility of its
author(s). The Journal of Bangladesh
College of Physicians and Surgeons,
its Editorial Board and Journal
Committee accept no liability
whatsoever for the consequences
of any such inaccurate and misleading
information, opinion or statement.
ADVISORY BOARD
PUBLISHED BY
PRINTED AT
ANNUAL SUBSCRIPTION
EDITORIAL BOARD
ADDRESS OF CORRESPONDENCEEditor-in-Chief, Journal of Bangladesh College of Physicians and Surgeons, BCPS Bhaban, 67, Shaheed Tajuddin Ahmed Sarani
Mohakhali, Dhaka-1212, Tel : 8825005-6, 8856616, 9884189, 9884194, 9891865 Ext. 124, Fax : 880-2-8828928,
E-mail : <[email protected]> Editor’s e-mail: [email protected]
Official Journal of the Bangladesh College of Physicians and Surgeons
BCPS Bhaban, 67 Shaheed Tajuddin Ahmed Sarani
Mohakhali, Dhaka-1212, Bangladesh
Vol. 34, No. 2, April 2016 EDITORIAL
ORIGINAL ARTICLES
REVIEW ARTICLE
CASE REPORTS
IMAGES IN MEDICAL PRACTICE
LETTER TO THE EDITOR
COLLEGE NEWS
FROM THE DESK OF THE EDITOR IN CHIEF
OBITUARY
CONTENTS
JOURNAL OF BANGLADESH COLLEGE
OF PHYSICIANS AND SURGEONS
Vol. 34, No. 2, Page 53-125 April 2016
116
118
124
125
Hepatic Steatosis among Obese Children and Adolescents 57
R Shelim, F Mohsin, T Begum, MA Baki, S Mahbuba, R Islam
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes and Outcome of Burrhole 64
Aspiration after Urokinase Mediated Clot Lysis
MN Hossain, S Nabi, SS Hossain
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular 76
Chemotherapy according to National Tuberculosis Guideline of Bangladesh
DN Sarkar, R Amin, H Mohammed, MN Royt, MA Azhar, MA Faiz
Intramuscular Loading dose versus Combined Intravenous & Intramuscular Loading dose of 85
Magnesium Sulphate in the Management of Eclampsia in a Tertiary Level Hospital of Bangladesh
S Rouf, S Ahmed, A Afrin
Editorial
Review Article
Case Reports
Proboitics and their Role in GI Diseases 92
S Perveen, MA Ahmed
The Netlike Skin Lesion -Cutis Marmarota 115
MR Islam, MR Amin
Malignant Nodular Hidradenoma: Isolated Case Report and Review of Literature 100
SA Khan, AAA Ali, S Ferdousi, M Riyad, AAH Mahmud
Pseudotumor cerebri : A Rare Presentation of Systemic Lupus Erythematosus 104
A Das, JC Das, AA Ahmad, MA Kahhar
Accidental Intramuscular Isoprenaline in Early Pregnancy: The Effects, Management 108
and Outcome
M Mostafi, MA Rahman, MT Mollick, MN Haq, A Rafi
Testicular Tuberculosis with Tuberculoma of Brain in an HIV Negative Patient 112
M Khanom
Childhood TB: Situation Analysis and the Potential Solutions 53
Md. Abid Hossain Mollah
Image 114
Leter to the editor 115
college news 117
FROM THE DESK OF EDITOR in CHIEF 123
Obituary 124

Journal of Bangladesh College of Physicians and Surgeons (JBCPS)
INFORMATION FOR AUTHORS
MANUSCRIPT PREPARATION AND SUBMISSIONGuide to AuthorsThe Journal of Bangladesh College of Physician andSurgeons, provides rapid publication (quarterlypublication) of articles in all areas of the subject. The Journalwelcomes the submission of manuscripts that meet thegeneral criteria of significance and scientific excellence.
Papers must be submitted with the understanding thatthey have not been published elsewhere (except in theform of an abstract or as part of a published lecture, review,or thesis) and are not currently under consideration byanother journal published by INTERNATIONALRESEARCH JOURNALS or any other publisher.
The submitting (Corresponding) author is responsiblefor ensuring that the article’s publication has beensigned approved by all the other coauthors. It is alsothe authors’ responsibility to ensure that the articlesemanating from a particular institution are submittedwith the approval of the necessary institutionalrequirement. Only an acknowledgment from the editorialoffice officially establishes the date of receipt. Furthercorrespondence and proofs will be sent to thecorresponding author(s) before publication unlessotherwise indicated. It is a condition for submission ofa paper that the authors permit editing of the paper forreadability. All enquiries concerning the publication ofaccepted papers should be addressed to -
Editor-in-Chief(Presently Prof. Khan Abul Kalam AzadBCPS Bhaban67 Shaheed Tajuddin SaraniMohakhali, Dhaka 1212,BANGLADESHPhone: +8802-8825005 +8802-8825005Fax: +88002-8828928
Electronic submission of manuscripts is stronglyencouraged, provided that the text, tables, and figuresare included in a single Microsoft Word file (preferablyin Arial font).
Submit manuscripts as e-mail attachment to the editorialoffice at: [email protected]
A manuscript number will be mailed to the correspondingauthor within two working days.
The cover letter should include the correspondingauthor’s full address and telephone/fax numbers andshould be in an e-mail message sent to the editor, withthe file, whose name should begin with the first author’ssurname, as an attachment.
The Journal of Bangladesh College of Physicians andSurgeons will only accept manuscripts submitted as e-mail attachments or triplicate Hard copy with a soft copy
Article TypesFIve types of manuscripts may be submitted:
Editorials: It will be preferably written invited only andusually covers a single topic of contemporary interest.
Original Articles: These should describe new andcarefully confirmed findings, and experimentalprocedures should be given in sufficient detail for othersto verify the work. The length of a full paper should bethe minimum required to describe and interpret the workclearly.
Short Communications: A Short Communication issuitable for recording the results of complete smallinvestigations or giving details of new models orhypotheses, innovative methods, techniques , imagesin clinical practice, letter to editors, short reports orapparatus. The style of main sections need not conformto that of original article . Short communications are 2 to4 printed pages (about 6 to 12 manuscript pages) inlength.
Reviews: Submissions of reviews and perspectivescovering topics of current interest are welcome andencouraged. Reviews should be concise and no longerthan 4 to 6 printed pages (about 12 to 18 manuscriptpages). It should be focused and must be up to date.Reviews are also peer-reviewed.
Case Reports: This should cover uncommon and/orinteresting cases with appropriate confirmation process.
Review Process:All manuscripts are initially screened by editor andsent to selective reviewer. Decisions will be made as

rapidly as possible, and the journal strives to returnreviewers’ comments to authors within 3 weeks. Theeditorial board will re-review manuscripts that areaccepted pending revision. The JBCPS editorial boardwill try to publish the manuscript as early as possiblefulfilling all the rigorous standard journal needs.
I. A. Preparing a Manuscript for Submission to JBCPSEditors and reviewers spend many hours readingmanuscripts, and therefore appreciate receivingmanuscripts that are easy to read and edit. Much of theinformation in this journal’s Instructions to Authors isdesigned to accomplish that goal in ways that meeteach journal’s particular editorial needs. The followinginformation provides guidance in preparing manuscriptsfor this journal.
Conditions for submission of manuscript:• All manuscripts are subject to peer-review.
• Manuscripts are received with the explicitunderstanding that they are not under simultaneousconsideration by any other publication.
• Submission of a manuscript for publication impliesthe transfer of the copyright from the author to thepublisher upon acceptance. Accepted manuscriptsbecome the permanent property of the Journal ofBangladesh College of Physicians and Surgeons andmay not be reproduced by any means in whole or inpart without the written consent of the publisher.
• It is the author’s responsibility to obtain permissionto reproduce illustrations, tables etc. from otherpublications.
Ethical aspects:• Ethical aspect of the study will be very carefully
considered at the time of assessment of themanuscript.
• Any manuscript that includes table, illustration orphotograph that have been published earlier shouldaccompany a letter of permission for re-publicationfrom the author(s) of the publication and editor/publisher of the Journal where it was published earlier.
• Permission of the patients and/or their families toreproduce photographs of the patients where identityis not disguised should be sent with the manuscript.Otherwise the identity will be blackened out.
Preparation of manuscript:Criteria: Information provided in the manuscript areimportant and likely to be of interest to an internationalreadership.
Preparation:1. Manuscript should be written in English and typed
on one side of A4 (290 x 210cm) size white paper.
2. Margin should be 5 cm for the header and 2.5 cmfor the remainder.
3. Style should be that of modified Vancouver.
4. Each of the following section should begin onseparate page :o Title pageo Summary/abstracto Texto Acknowledgemento Referenceso Tables and legends.
Pages should be numbered consecutively at the upperright hand corner of each page beginning with thetitle page
I. A. 1. a. General Principles• The text of observational and experimental articles
is usually (but not necessarily) divided into thefollowing sections: Introduction, Methods, Results,and Discussion. This so-called “IMRAD” structureis a direct reflection of the process of scientificdiscovery.
• Long articles may need subheadings within somesections (especially Results and Discussion) toclarify their content. Other types of articles, such ascase reports, reviews, and editorials, probably needto be formatted differently.
• Electronic formats have created opportunities foradding details or whole sections, layeringinformation, crosslinking or extracting portions ofarticles, and the like only in the electronic version.
• Authors need to work closely with editors indeveloping or using such new publication formatsand should submit supplementary electronic materialfor peer review.
• Double-spacing all portions of the manuscript—including the title page, abstract, text,acknowledgments, references, individual tables, and

legends—and generous margins make it possible foreditors and reviewers to edit the text line by line andadd comments and queries directly on the paper copy.
• If manuscripts are submitted electronically, the filesshould be double-spaced to facilitate printing forreviewing and editing.
• Authors should number on right upper all of thepages of the manuscript consecutively, beginningwith the title page, to facilitate the editorial process.
I. A. 1. b. Reporting Guidelines for Specific StudyDesignsResearch reports frequently omit important information.Reporting guidelines have been developed for a numberof study designs that JBCPS journals ask authors tofollow. Authors should consult the Information forAuthors of this journal. The general requirements listedin the next section relate to reporting essential elementsfor all study designs. Authors are encouraged also toconsult reporting guidelines relevant to their specificresearch design. A good source of reporting guidelinesis the EQUATOR Network (http: //www.equator-network.org/home/) or CONSORT network (http://www.consort-statement.org ).
I. A .2. Title PageThe title page should have the following information:
1. Article title. Concise titles are easier to read thanlong, convoluted ones. Titles that are too shortmay, however, lack important information, such asstudy design (which is particularly important inidentifying type of trials). Authors should includeall information in the title that will make electronicretrieval of the article both sensitive and specific.
2. Authors’ names and institutional affiliations.
3. The name of the department(s) and institution(s)to which the work should be attributed.
4. Disclaimers, if any.
5. Contact information for corresponding authors. Thename, mailing address, telephone and fax numbers,and e-mail address of the author responsible forcorrespondence about the manuscript .
6. The name and address of the author to whomrequests for reprints should be addressed or aStatement that reprints are not available from theauthors.
7. Source(s) of support in the form of grants,equipment, drugs, or all of these.
8. A short running head or footline, of no more than40 characters(including letters and spaces).Running heads are published and also used withinthe editorial office for filing and locatingmanuscripts.
9. The number of figures and tables. It is difficult foreditorial staff and reviewers to determine whetherhe figures and tables that should have accompanieda manuscript were actually included unless thenumbers of figures and tables are noted on the titlepage.
I. A. 3. Conflict-of-Interest Notification PageTo prevent potential conflicts of interest from beingoverlooked or misplaced, this information needs to bepart of the manuscript. The ICMJE has developed auniform disclosure form for use by ICMJE memberjournals (http://www.icmje.org/coi_disclosure.pdf) andJBCPS has accepted that.
I. A. 4. Abstract• Structured abstracts are essential for original research
and systematic reviews. structured abstract meansintroduction, methods, results and conclusion inabstract
• Should be limited to 250 words
• The abstract should provide the introduction of thestudy and blinded state and should state the study’spurpose, basic procedures (selection of studysubjects or laboratory animals, observational andanalytical methods), main findings (giving specificeffect sizes and their statistical significance, ifpossible), principal conclusions. It should emphasizenew and important aspects of the study orobservations. Articles on clinical trials shouldcontain abstracts that include the items that theCONSORT group has identified as essential (http://www.consort-statement.org ).
• Because abstracts are the only substantive portionof the article indexed in many electronic databases,and the only portion many readers read, authorsneed to be careful that they accurately reflect thecontent of the article

I. A. 5. Introduction• Provide a context or background for the study (that
is, the nature of the problem and its significance). Itshould be very specific, identify the specifyknowledge in the aspect, reasoning and what thestudy aim to answer.
• State the specific purpose or research objective of,or hypothesis tested by, the study or observation;the research objective is often more sharply focusedwhen stated as a question.
• Both the main and secondary objectives should beclear.
• Provide only directly pertinent primary references,and do not include data or conclusions from thework being reported.
I. A. 6. MethodsThe Methods section should be written in such way
that another researcher can replicate the study.
I. A. 6. a. Selection and Description of Participants• Describe your selection of the observational or
experimental participants (patients or laboratoryanimals, including controls) clearly, includingeligibility and exclusion criteria and a description ofthe source population. Because the relevance of suchvariables as age and sex to the object of research isnot always clear, authors should explain their usewhen they are included in a study report—forexample, authors should explain why onlyparticipants of certain ages were included or whywomen were excluded. The guiding principle shouldbe clarity about how and why a study was done in aparticular way. When authors use such variables asrace or ethnicity, they should define how theymeasured these variables and justify their relevance.
I. A. 6. b. Technical Information• Identify the methods, apparatus (give the
manufacturer’s name and address in parentheses),and procedures insufficient detail to allow others toreproduce the results. Give references to establishedmethods, including statistical methods (see below);provide references and brief descriptions formethods that have been published but are not well-known; describe new or substantially modifiedmethods, give the reasons for using them, andevaluate their limitations. Identify precisely all drugs
and chemicals used, including generic name(s),dose(s), and route(s) of administration.
• Authors submitting review article should include asection describing the methods used for locating,selecting, extracting, and synthesizing data. Thesemethods should also be summarized in the abstract.
I. A. 6. c. Statistics• Describe statistical methods with enough detail to
enable a knowledgeable reader with access to theoriginal data to verify the reported results. Whenpossible, quantify findings and present them withappropriate indicators of measurement error oruncertainty (such as confidence intervals).
• Avoid relying solely on statistical hypothesistesting, such as P values, which fail to conveyimportant information about effect size. Referencesfor the design of the study and statistical methodsshould be to standard works when possible (withpages stated).
• Define statistical terms, abbreviations, and mostsymbols.
• Specify the computer software used.
I. A. 7. Results• Present results in logical sequence in the text, tables,
and illustrations, giving the main or most importantfindings first. Please keep the result the sequence ofspecific objective selected earlier.
• Do not repeat all the data in the tables or illustrationsin the text; emphasize or summarize only the mostimportant observations. Extra or supplementarymaterials and technical detail can be placed in anappendix where they will be accessible but will notinterrupt the flow of the text, or they can be publishedsolely in the electronic version of the journal.
• When data are summarized in the Results section,give numeric results not only as derivatives (forexample, percentages) but also as the absolutenumbers from which the derivatives were calculated,and specify the statistical methods used to analyzethem.
• Restrict tables and figures to those needed to explainthe argument of the paper and to assess supportingdata. Use graphs as an alternative to tables with manyentries; do not duplicate data in graphs and tables.

• Avoid nontechnical uses of technical terms instatistics, such as “random” (which implies arandomizing device), “normal,” “significant,”“correlations,” and “sample.” Where scientificallyappropriate, analyses of the data by such variablesas age and sex should be included.
I. A. 8. Discussion• Emphasize the new and important aspects of the
study and the conclusions that follow from them inthe context of the totality of the best availableevidence.
• Do not repeat in detail data or other informationgiven in the Introduction or the Results section.
• For experimental studies, it is useful to begin thediscussion by briefly summarizing the main findings,then explore possible mechanisms or explanationsfor these findings, compare and contrast the resultswith other relevant studies, state the limitations ofthe study, and explore the implications of the findingsfor future research and for clinical practice.
• Link the conclusions with the goals of the studybut avoid unqualified statements and conclusionsnot adequately supported by the data. In particular,avoid making statements on economic benefits andcosts unless the manuscript includes the appropriateeconomic data and analyses. Avoid claiming priorityor alluding to work that has not been completed.State new hypotheses when warranted, but labelthem clearly as such.
I. A. 9. References
I. A. 9. a. General Considerations Related to
References• Although references to review articles can be an
efficient way to guide readers to a body of literature,review articles do not always reflect original workaccurately. Readers should therefore be providedwith direct references to original research sourceswhenever possible.
• On the other hand, extensive lists of references tooriginal work of a topic can use excessive space onthe printed page. Small numbers of references to keyoriginal papers often serve as well as more exhaustivelists, particularly since references can now be addedto the electronic version of published papers, and
since electronic literature searching allows readersto retrieve published literature efficiently.
• Avoid using abstracts as references. References topapers accepted but not yet published should bedesignated as “in press” or “forthcoming”; authorsshould obtain written permission to cite such papersas well as verification that they have been acceptedfor publication.
• Information from manuscripts submitted but notaccepted should becited in the text as “unpublishedobservations” with written permission from thesource.
• Avoid citing a “personal communication” unless itprovides essential information not available from apublic source, in which case the name of the personand date of communication should be cited inparentheses in the text. For scientific articles, obtainwritten permission and confirmation of accuracy fromthe source of a personal communication. Some butnot all journals check the accuracy of all referencecitations; thus, citation errors sometimes appear inthe published version of articles. To minimize sucherrors, references should be verified using either anelectronic bibliographic source, such as PubMed orprint copies from original sources.
• Authors are responsible for checking that none ofthe references cite retracted articles except in thecontext of referring to the retraction. For articlespublished in journals indexed in MEDLINE, theICMJE considers PubMed the authoritative sourcefor information about retractions.
I. A. 9. b. Reference Style and Format• References should be numbered consecutively in
the order in which they are first mentioned in thetext.
• Identify references in text, tables, and legends byArabic numerals in superscript.
• References cited only in tables or figure legendsshould be numbered in accordance with thesequence established by the first identification inthe text of the particular table or figure.
I. A. 10. Tables• Tables capture information concisely and display it
efficiently.

• Use tables /fig that are relevant to study
• Try to limit the number of tables/figure
• Type or print each table with double-spacing on aseparate sheet of paper. Number tables consecutivelyin the order of their first citation in the text and supplya brief title for each.
• Do not use internal horizontal or vertical lines. Giveeach column a short or an abbreviated heading.Authors should place explanatory matter infootnotes, not in the heading. Explain all nonstandardabbreviations in footnotes, and use the followingsymbols, in sequence:*, †, ‡, §, _, ¶, **, ††, ‡‡, §§, _ _, ¶¶, etc.
• Identify statistical measures of variations, such asstandard deviation and standard error of the mean.
• Be sure that each table is cited in the text. If you usedata from another published or unpublished source,obtain permission and acknowledge that source fully.
I. A. 11. Illustrations (Figures)• Figures should be either professionally drawn and
photographed, or submitted as photographic-qualitydigital prints. In addition to requiring a version ofthe figures suitable for printing,(for example, JPEG / GIF)
• Authors should review the images of such files on acomputer screen before submitting them to be surethey meet their own quality standards. For x-ray films,scans, and other diagnostic images, as well aspictures of pathology specimens orphotomicrographs, send sharp, glossy, black-and-white or color photographic prints, usually 127 _173 mm (5 _ 7 inches)
• Letters, numbers, and symbols on figures shouldtherefore be clear and consistent throughout, andlarge enough to remain legible when the figure isreduced for publication.
• Photographs of potentially identifiable people mustbe accompanied by written permission to use thephotograph. Figures should be numberedconsecutively according to the order in which theyhave been cited in the text.
• If a figure has been published previously,acknowledge the original source and submit writtenpermission from the copyright holder to reproducethe figure. Permission is required irrespective of
authorship or publisher except for documents in thepublic domain.
• For illustrations in color, JBCPS accept colouredillustration but when it seems essential. This Journalpublish illustrations in color only if the author paysthe additional cost. Authors should consult thejournal about requirements for figures submitted inelectronic formats.
I. A. 12. Legends for Illustrations (Figures)
• Type or print out legends for illustrations usingdouble spacing, starting on a separate page, withArabic numerals corresponding to the illustrations.
• When symbols, arrows, numbers, or letters are usedto identify parts of the illustrations, identify andexplain each one clearly in the legend. Explain theinternal scale and identify the method of staining inphotomicrographs.
I. A. 13. Units of Measurement• Measurements of length, height, weight, and volume
should be reported in metric units (meter, kilogram,or liter) or their decimal multiples.
• Authors should report laboratory information inboth local and International System of Units (SI). .
• Drug concentrations may be reported in either SI ormass units, but the alternative should be providedin parentheses where appropriate.
I. A. 14. Abbreviations and Symbols• Use only standard abbreviations; use of nonstandard
abbreviations can be confusing to readers.
• Avoid abbreviations in the title of the manuscript.
• The spelled-out abbreviation followed by theabbreviation in parenthesis should be used on firstmention unless the abbreviation is a standard unitof measurement.
I. B. Sending the Manuscript to the Journal• If a paper version of the manuscript is submitted,
send the required number of copies of the manuscriptand figures; they are all needed for peer review andediting, and the editorial office staff cannot beexpected to make the required copies.
• Manuscripts must be accompanied by a cover letter,conflicts of interest form, authorship and declaration,proforma of which is available in JBCPS web site.

Editing and peer review: All submitted manuscripts aresubject to scrutiny by the Editor in-chief or any memberof the Editorial Board. Manuscripts containing materialswithout sufficient scientific value and of a priority issue,or not fulfilling the requirement for publication may berejected or it may be sent back to the author(s) forresubmission with necessary modifications to suit oneof the submission categories. Manuscripts fulfilling therequirements and found suitable for consideration aresent for peer review. Submissions, found suitable forpublication by the reviewer, may need revision/modifications before being finally accepted. EditorialBoard finally decides upon the publishability of thereviewed and revised/modified submission. Proof ofaccepted manuscript may be sent to the authors, andshould be corrected and returned to the editorial officewithin one week. No addition to the manuscript at thisstage will be accepted. All accepted manuscripts areedited according to the Journal’s style.
Submission Preparation ChecklistAs part of the submission process, authors are requiredto check off their submission’s compliance with all ofthe following items, and submissions may be returnedto authors that do not adhere to these guidelines.
Check ListsFinal checklists before you submit your revised articlefor the possible publication in the Journal of BangladeshCollege of Physicians and Surgeons:
1. Forwarding/Cover letter and declaration form
2. Authorship and conflicts of interest form
3. Manuscript
o Sample of the above documents is available inthe following links: http://www.bcpsbd.org(registration required for download)
o If you have submitted mention document (1, 2,3 ) above, when you first submitted your articlethen you don’t need to re-submit but if there ischange in the authorship or related then youhave to re-submit it.
• General outline for article presentation and formatD Double spacingD Font size should be 12 in arialD Margins 5 cm from above and 2.5 cm from rest
sides.
D Title page contains all the desired information(vide supra)
D Running title provided (not more than 40characters)
D Headings in title case (not ALL CAPITALS,not underlined)
D References cited in superscript in the textwithout brackets after with/without comma (,)or full stop (.)
D References according to the journal’sinstructions – abide by the rules of Vancouversystem. Use this link to get into the detail ofVancouver system.
• Language and grammarD Uniformity in the languageD Abbreviations spelt out in full for the first timeD Numerals from 1 to 10 spelt outD Numerals at the beginning of the sentence spelt
out
• Tables and figuresD No repetition of data in tables/graphs and in
textD Actual numbers from which graphs drawn,
providedD Figures necessary and of good quality (colour)D Table and figure numbers in Arabic letters (not
Roman)D Labels pasted on back of the photographs (no
names written)D Figure legends provided (not more than 40
words)D Patients’ privacy maintained (if not, written
permission enclosed)D Credit note for borrowed figures/tables
providedD Each table/figure in separate page
If you have any specific queries please use atwww.bcps.com
Manuscript Format for Research Article• Title
D Complete title of your articleD Complete author informationD Mention conflict of interest if any

• AbstractD Do not use subheadings in the abstractD Give full title of the manuscript in the Abstract
pageD Not more than 200 words for case reports and
250 words for original articlesD Structured abstract (Including introduction,
methods, results and discussion, conclusion)provided for an original article and(Introduction, results and discussion ,conclusion) for case reports.
D Key words provided – arrange them inalphabetical order (three – five )
• IntroductionD Word limit 150 -200 wordsD Pertinent information only
• Material and MethodsD Study DesignD Duration and place of studyD Ethical approvalD Patient consentD Statistical analysis and software used.
• ResultD Clearly present the dataD Avoid data redundancyD Use table information at the end of the
sentence before full stop between the smallbracket
• DiscussionD Avoid unnecessary explanation of someone
else work unless it is very relevant to the studyD Provide and discuss with the literatures to
support the studyD Mention about limitation of your study
• ConclusionD Give your conclusionD Any recommendation
• AcknowledgementD Acknowledge any person or institute who have
helped for the study
• ReferenceD Abide by the Vancouver styleD Use reference at the end of the sentence after
the full stop with superscript
• LegendsD TableD Figures
Journal of Bangladesh College of Physicians andSurgeons ISSN: 1015-0870
Indexed on HINARI, EMSCO, DOAJ, Index Copernicus,Ulrichs Web, Google Scholar, CrossRef, ProQuest,Scientific Common.
BanglaJOL is supported by IN

Chairman
Dr. Quazi Tarikul Islam
Editor-In-Chief
Dr. Khan Abul Kalam Azad
Editors
Dr. Zafar Ahmed Latif
Dr. A. N. M. Zia-ur-Rahman
Dr. Emran Bin Yunus
Dr. Parveen Fatima
Dr. U. H. Shahera Khatun
Dr. Syed Atiqul Haq
Dr. Fakhruddin Mohammad Siddiqui
Dr. Syeda Afroza
Dr. Md. Ridwanur Rahman
Dr. Nooruddin Ahmed
Dr. Khwaja Nazim Uddin
Dr. Md. Abdul Hamid
Dr. A.H.M. Rowshon
Dr. Tapan Kumar Saha
Dr. A.B.M. Bayezid Hossain
Dr. Md. Titu Miah
Dr. Tripti Rani Das
Dr. Dipi Barua
Dr. Rubina Yasmin
Dr. Mohammad Robed Amin
Dr. S.M. Anwar Sadat
Dr. (Col) Md. Abdur Rab
Dr. Shariff Asfia Rahman
Dr. S.M. Quamrul Akther
Dr. Aparna Das
Dr. Syed Ghulam Mogni Mowla
Dr. Tanveer Ahmed
Dr. Khan Abul Kalam Azad
on behalf of the Bangladesh College
of Physicians and Surgeons
Asian Colour Printing
130 DIT Extension Road
Fakirerpool, Dhaka-1000
Tk. 400/- for local and US$ 40 for
overseas subscribers
Professor Md. Sanawar HossainProfessor Kanak Kanti BaruaProfessor Md. Ruhul Amin Professor A.B.M. Muksudul AlamProfessor T.I.M. Abdullah-Al-FaruqProfessor Shahana Akhter Rahman Professor Md. Abdul Jalil ChowdhuryProfessor Md. Azizul KahharProfessor Abdul Kader KhanProfessor Sayeba Akhter Professor Md. Abul Kashem KhandakerProfessor Mohammod ShahidullahProfessor Quazi Deen Mohammad Professor Kohinoor BegumProfessor Quazi Tarikul IslamProfessor Choudhury Ali KawserProfessor Iffat AraProfessor Nazmun Nahar Professor Major Gen. (Retd.) Md. Ali Akbar Professor Shamsuddin Ahmed
Editorial StaffAfsana HuqMohammed Ibrahim
The Journal of Bangladesh College
of Physicians and Surgeons is a
peer reviewed Journal. It is
published four times a year,
(January, April, July and October).
It accepts original articles, review
articles, and case reports.
Complimentary copies of the
journal are sent to libraries of all
medical and other relevant
academic institutions in the
country and selected institutions
abroad.
While every effort is always made
by the Editorial Board and the
members of the Journal Committee
to avoid inaccurate or misleading
information appearing in the
Journal of Bangladesh College
of Physicians and Surgeons,
information within the individual
article are the responsibility of its
author(s). The Journal of Bangladesh
College of Physicians and Surgeons,
its Editorial Board and Journal
Committee accept no liability
whatsoever for the consequences
of any such inaccurate and misleading
information, opinion or statement.
ADVISORY BOARD
PUBLISHED BY
PRINTED AT
ANNUAL SUBSCRIPTION
EDITORIAL BOARD
ADDRESS OF CORRESPONDENCEEditor-in-Chief, Journal of Bangladesh College of Physicians and Surgeons, BCPS Bhaban, 67, Shaheed Tajuddin Ahmed Sarani
Mohakhali, Dhaka-1212, Tel : 8825005-6, 8856616, 9884189, 9884194, 9891865 Ext. 124, Fax : 880-2-8828928,
E-mail : <[email protected]> Editor’s e-mail: [email protected]
Official Journal of the Bangladesh College of Physicians and Surgeons
BCPS Bhaban, 67 Shaheed Tajuddin Ahmed Sarani
Mohakhali, Dhaka-1212, Bangladesh
Vol. 34, No. 2, April 2016 EDITORIAL
ORIGINAL ARTICLES
REVIEW ARTICLE
CASE REPORTS
IMAGES IN MEDICAL PRACTICE
LETTER TO THE EDITOR
COLLEGE NEWS
FROM THE DESK OF THE EDITOR IN CHIEF
OBITUARY
CONTENTS
JOURNAL OF BANGLADESH COLLEGE
OF PHYSICIANS AND SURGEONS
Vol. 34, No. 2, Page 53-125 April 2016
116
118
124
125
Hepatic Steatosis among Obese Children and Adolescents 57
R Shelim, F Mohsin, T Begum, MA Baki, S Mahbuba, R Islam
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes and Outcome of Burrhole 64
Aspiration after Urokinase Mediated Clot Lysis
MN Hossain, S Nabi, SS Hossain
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular 76
Chemotherapy according to National Tuberculosis Guideline of Bangladesh
DN Sarkar, R Amin, H Mohammed, MN Royt, MA Azhar, MA Faiz
Intramuscular Loading dose versus Combined Intravenous & Intramuscular Loading dose of 85
Magnesium Sulphate in the Management of Eclampsia in a Tertiary Level Hospital of Bangladesh
S Rouf, S Ahmed, A Afrin
Editorial
Review Article
Case Reports
Proboitics and their Role in GI Diseases 92
S Perveen, MA Ahmed
The Netlike Skin Lesion -Cutis Marmarota 115
MR Islam, MR Amin
Malignant Nodular Hidradenoma: Isolated Case Report and Review of Literature 100
SA Khan, AAA Ali, S Ferdousi, M Riyad, AAH Mahmud
Pseudotumor cerebri : A Rare Presentation of Systemic Lupus Erythematosus 104
A Das, JC Das, AA Ahmad, MA Kahhar
Accidental Intramuscular Isoprenaline in Early Pregnancy: The Effects, Management 108
and Outcome
M Mostafi, MA Rahman, MT Mollick, MN Haq, A Rafi
Testicular Tuberculosis with Tuberculoma of Brain in an HIV Negative Patient 112
M Khanom
Childhood TB: Situation Analysis and the Potential Solutions 53
Md. Abid Hossain Mollah
Image 114
Leter to the editor 115
college news 117
FROM THE DESK OF EDITOR in CHIEF 123
Obituary 124

EDITORIAL
Tuberculosis (TB) is one of the leading causes ofmorbidity and mortality of children in tuberculosis-endemic areas1. Based on vital registration data, WorldHealth Organization (WHO) in 2014, estimated that 1million children (<15 years) suffer from TB worldwideand 140,000 die each year, representing 10% and 9% ofglobal caseload and mortality, respectively2. This“merciless disease” exists in the shadow of adult TB andchildren particularly those under 5 years of age, whocame in contact with smear positive adult TB cases andwho suffers from malnutrition and HIV infection are themost vulnerable group to acquire tuberculosis3. ChildhoodTB (CTB) remains a neglected aspect of the TB epidemic,despite its contribution to 20% or more of the TB case-load in many countries with high TB incidence2. Amongthe 4,452,860 new cases reported in 2010 by the 22 highestTB burden countries, only 157,135, i.e. 3.5% (range, 0.1 to15.0), were reported as CTB4. However, the best estimatessuggest that children (under 15 years of age) account forapproximately 11% of the total TB burden,reflecting thatjust over 332,000 (7.5%) of CTB went undiagnosed orunreported in these countries4-5.
In light of these facts we can assume that, the actualburden of CTB is likely higher, but is not reflected indata because of challenges in diagnosing the cases.The barriers of diagnosis are related to not obtaininghigh quality specimens, pauci-bacillary nature of thedisease in young children and lack of mycobacterialculture facilities in settings where TB and malnutritionare endemic, even when available, the longtime delay ingetting results of culture and sensitivity [6]. Although,the gene X-pert MTB/RIF assay (Cepheid, Sunnyvale,CA, USA) is a new, rapid diagnostic test for the detectionof M tuberculosis than culture it is demonstratingencouraging results in the diagnosis of pulmonary TBespecially with greater sensitivity. Still, the sensitivityis less than 70% compared to culture in children6-8.
Reviewing the previous data, we can also postulate thatpoor ascertainment and reporting of TB casesis another
limitation and actually it prevents accurate estimationand true picture of the global burden of CTB9. Many atimes, deaths of HIV-infected children with TB isrecorded as death due HIV and not as TB 10. Similarly, inendemic settings, TB is commonly found in childrendying with pneumonia and reported as death frompneumonia not from TB6, 11, 12.
Despite all these limitations, evidence indicates thatglobal case detection of TB is improving, and it is mainlydue to intensified case finding following WHOguideline, notification through a harmonized bridgingbetween government and non-governmentorganizations, scrupulous adherence to national TBguideline, and implementation of DOTs program in manyTB-endemic countries2,13,14. However, the scenario isnot the same in many TB-endemic countries includingBangladesh where under-estimation of childhood TB isstill prevailing.
Bangladesh stands 7th amongst the 22 high TB burdencountries in the world. As in many high-Tb burdencountries, childhood tuberculosis (CTB) is also grosslyunder-detected in Bangladesh15. In 2007, BangladeshNational Tuberculosis Programme (BNTP) reportedincidence of childhood TB as 9 per 100 000 [16]. In 2011,of the total 155,673 newly reported TB cases, only 4,672(3%) cases occurred in childrenunder15 years17. TheNational incidence of CTB among 0-14 years old childrenwere 9 per 100,000 reported by the NTP in 2007 and 8.6per 100,000 reported by the Damien Foundation in200918. However, extrapolating data of best estimate(CTB;11% of total case load), the estimated incidenceand prevalence of CTB is likely to be 25/100,000 and 45/100,000 respectively in Bangladesh19.A surveyconducted by ICDDR,B in 2008-09 in Madhupur, Tangail,showed incidence of CTB as 52 per 100,000 among 0-14year children which is about 6 times higher than BNTPdata20. TB prevalence among adults in the same areawas estimated at 207/100 000 population, with childrenrepresenting approximately 20% of all cases identified.
Childhood TB: Situation Analysisand the Potential Solutions

Although, this does not represent national incidence ofCTB, it definitely indicates a gap between reported andactual disease burden in the communities. Using thesenumbers, it is estimated that around 21, 000 childrenwith TB remain undetected each year in Bangladesh.The plausible reasons behind this underestimation maybe i) poor awareness about childhood TB ii) difficultiesin access to TB diagnosis and care iii) clinical similaritieswith other common childhood diseases iv) Treatmentof CTB outside the national TB program v) lack of routinerecording and reporting of the cases and mostimportantly vi) lack of systematic screening for TBamong children living in the same households affectedby TB19. In addition, recommendations of INH preventivetherapy (IPT) for children, under 5 years of age is rarelyimplemented20.
The delay in diagnosis or under-diagnosis of TB amongchildren leave them in jeopardy and often results inserious consequences and fatal outcome21. Any childliving in a setting where there are people with infectiousTB can become ill with TB, even if they are vaccinated.Current TB vaccine protects young children againstthe most severe forms of TB, such as meningitis anddisseminated TB disease, but prevention of transmissionfrom an infectious contact is variable. We do not knowthe extent to which TB is a cause of childhood deathsbecause many of them are reported in global statisticsas deaths due to HIV, pneumonia, malnutrition ormeningitis, but the number is likely to be substantial2.
Therefore, to alleviate this situation, strengtheningTBcase detection as well as reporting is very important. Itis possible through orientation &training on TBof healthworkers to understand and improve their clinical skill ofTB diagnosis, masspeople awareness through advocacy,counseling and social mobilization, active contact searchand mandatory reporting of the cases. In addition,diagnosis and early initiation of treatment of childrenwith TB having associated comorbidities will help toreduce TB related deaths. We need to move beyond thetraditional approach of TB care by workingsynergistically across the entire health system andpartnering with communities to reach the goal of zeroTB deaths in children.
To achieve that, we need determined leadership, politicalcommitment at all levels, joint efforts by all the
stakeholders involved in TB care, relentless and robustresearch on CTBand of course mobilization of increasedresources and this is the demand of time.
[Acknowledgement: Dr. Jobayer Chisti ICDDRB,Dr.Mehdi Parvez SBMC,DrZohoraJameela Khan DMC]
(J Bangladesh Coll Phys Surg 2016; 34: 53-55)
Prof. Md. Abid Hossain MollahProfessor of PediatricsDhaka Medical College
References:1. Graham SM, Sismanidis C, Menzies HJ, Marais BJ, Detjen
AK, Black RE. Importance of tuberculosis control toaddress child survival. Lancet. 2014;383:1605-7.
2. World Health Organization. Global tuberculosis report2015. Geneva, Switzerland: World Health Organization;2015.
3. World Health Organization. Roadmap for ChildhoodTuberculosis”. Geneva: World Health Organization; 2013.
4. Perez-Velez CM, Marais BJ. Tuberculosis in children. NEngl J Med. 2012;367:348-61.
5. Nelson LJ, Schneider E, Wells CD, Moore M.Epidemiology of childhood tuberculosis in the UnitedStates, 1993-2001: the need for continued vigilance.Pediatrics. 2004;114:333-41.
6. Chisti MJ, Graham SM, Duke T, Ahmed T, Ashraf H,Faruque AS, et al. A Prospective Study of the Prevalenceof Tuberculosis and Bacteraemia in Bangladeshi Childrenwith Severe Malnutrition and Pneumonia Including anEvaluation of Xpert MTB/RIF Assay. PloS one.2014;9:e93776.
7. Bates M, O’Grady J, Maeurer M, Tembo J, Chilukutu L,Chabala C, et al. Assessment of the Xpert MTB/RIF assayfor diagnosis of tuberculosis with gastric lavage aspiratesin children in sub-Saharan Africa: a prospective descriptivestudy. The Lancet infectious diseases. 2013;13:36-42.
8. Rachow A, Clowes P, Saathoff E, Mtafya B, Michael E,Ntinginya EN, et al. Increased and expedited case detectionby Xpert MTB/RIF assay in childhood tuberculosis: aprospective cohort study. Clin Infect Dis. 2012;54:1388-96.
9. Graham SM, Cuevas LE, Jean-Philippe P, Browning R,Casenghi M, Detjen AK, et al. Clinical Case Definitionsfor Classification of Intrathoracic Tuberculosis inChildren: An Update. Clin Infect Dis. 2015;61Suppl3:S179-87.
10. World Health Organization.Stop TB partnership. Annualmeeting of the Childhood TB Subgroup. Kuala Lumpur,Malaysia,: World Health Organization; 2012.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
54

11. Nantongo JM, Wobudeya E, Mupere E, Joloba M,Ssengooba W, Kisembo HN, et al. High incidence ofpulmonary tuberculosis in children admitted with severepneumonia in Uganda. BMC Pediatr. 2013;13:16.
12. Oliwa JN, Karumbi JM, Marais BJ, Madhi SA, Graham SM.Tuberculosis as a cause or comorbidity of childhoodpneumonia in tuberculosis-endemic areas: a systematicreview. The Lancet Respiratory medicine. 2015;3: 235-43.
13. Oshi DC, Chukwu JN, Nwafor CC, Meka AO, Madichie NO,Ogbudebe CL, et al. Does intensified case finding increasetuberculosis case notification among children in resource-poor settings? A report from Nigeria. International journalof mycobacteriology. 2016;5:44-50.
14. Aketi L, Kashongwe Z, Kinsiona C, Fueza SB,Kokolomami J, Bolie G, et al. Childhood Tuberculosis ina Sub-Saharan Tertiary Facility: Epidemiology and FactorsAssociated with Treatment Outcome. PloS one.2016;11:e0153914.
15. Rashid MM. Tuberculosis and Malaria Control Programmein Bangladesh.: World Bank Group. Public PrivateDialogue. 8th PPD Workshop. 2015.
16. National Tuberculosis Control Programme. Tuberculosiscontrol Increasing child TB detection in Bangladesh.
Annual report 2008. Dhaka, Bangladesh: . DirectorateGeneral of Health Services. 2008.
17. National Guideline for the Management of Tuberculosisin Children. Second ed2016.
18. National Guideline for the Management of Tuberculosisin Children. First ed2012.
19. Bangladesh National Tuberculosis programe. ChildhoodTuberculosis: A training manual for medical doctors. 2013.
20. Ahmed T, Rahman AS, Islam R. Results from field: noveldiagnostics in children 41st World Conference on LungHealth of the International Union Against Tuberculosis andLung Disease (The Union), 11– 15 November 2010. Berlin,Germany: Int J Tuberc Lung Dis; 2010. p. S34–S5.).
21. Yan I, Korenromp E, Bendavid E. Mortality changes aftergrants from the Global Fund to Fight AIDS, tuberculosisand malaria: an econometric analysis from 1995 to 2010.BMC public health. 2015;15:977.
22. Chisti MJ, Ahmed T, Pietroni MA, Faruque AS, Ashraf H,Bardhan PK, et al. Pulmonary tuberculosis in severely-malnourished or HIV-infected children with pneumonia:a review. Journal of health, population, and nutrition.2013;31:308-13.
Childhood TB: Situation Analysis and the Potential Solutions Md. Abid Hossain Mollah
55

Summary:Background: Chronic liver disease, known as non- alcoholicfatty liver disease (NAFLD) is a metabolic complication ofobesity. Hepatic steatosis is an entity in the spectrum ofNAFLD, ranges from simple steatosis to advanced fibrosisand cirrhosis. Objective: To identify prevalence of hepaticsteatosis and to assess correlation between hepatic steatosisand anthropometry, SGPT and metabolic abnormalities ofobese children and adolescents. Methodology: This crosssectional study included 50 obese children and adolescents,attending the Endocrine OPD of Dept. of Paediatrics inBIRDEM from June 2009 to December 2009. BMI e” 95th
centile for age and sex was used as an anthropometric markerto diagnose obesity. Obesity with any dismorphism, endocrineor chromosomal abnormalities were excluded. Fasting bloodsamples were collected for measurement of SGPT, bloodglucose, lipid profile, FT4 &TSH. Sonographic findings offatty liver include increased echogenicity of liver, blurring
of vascular margins and increased acoustic attenuation.Results: Mean age of the children was 11.24 (8-18) years.High SGPT level was prevalent among 36% of obesechildren. The most prevalent abnormal lipid profile washigh TG (78%) followed by high cholesterol level (68%).The prevalence of hepatic steatosis was 36% with malepredominance (M 72.2%, F 27.8%). Mild hepatic steatosiswas 72% followed by moderate 28%. High SGPT, highcholesterol and LDL were more prevalent in children withhepatic steatosis in comparison to children without steatosis(P <0.004, <0.05 and <0.04 respectively). Conclusion:Hyperlipidemia with raised SGPT are important signs ofliver dysfunction in obese children with hepatic steatosis.Prevention of obesity and identification of children with anincreased risk of NAFLD are important steps in preventingirreversible liver damage.
Key words: Obesity, Non alcoholic fatty liver disease,Steatosis, SGPT, Hyperlipidemia.
(J Bangladesh Coll Phys Surg 2016; 34: 57-63)
Hepatic Steatosis among Obese Childrenand Adolescents
R SHELIMa, F MOHSINb, T BEGUMc, MA BAKId, S MAHBUBAe, R ISLAMf
ORIGINAL ARTICLES
a. Dr. Rumana Shelim, Assistant Professor, Dept. of Paediatrics,East- West Medical College Hospital.
b. Dr. Fauzia Mohsin, Associate professor, Dept of Paediatrics,BIRDEM.
c. Prof. Tahmina Begum, Professor & Head of the Department,Dept. of Paediatrics, BIRDEM.
d. Dr. MA Baki, Registrar, Dept of Paediatrics, BIRDEM.e. Dr. Sharmin Mahbuba, Senior Medical Officer, Dept of
Paediatrics, BIRDEM.f. Dr. Rubaiya Islam, Medical Officer, Dept of Paediatrics,
BIRDEM.Address of Correspondence: Dr. Rumana shelim, AssistantProfessor, Dept. of Paediatrics, East- West Medical CollegeHospital, Mobile: 01720504577, Email: rumanashelim@gmaReceived: 18 February, 2014 Accepted: 12 February, 2016
Introduction:Obesity is a global nutritional concern. The increasingprevalence of overweight, obesity and its consequencesprompted the WHO to designate obesity as a globalepidemic.1 Based on data from the 1999-2000 NationalHealth and Nutrition Examination Survey (NHANES IV)in United States, in all ranges prevalence of obesity has
increased compared with that in the previous report(1988-1994) and the most change, from 11% to 15%,occurred among 6 to 19 years of age group.2 Theprevalence of obesity and overweight in affluent schoolchildren in Dhaka was found to be 17.9% and 23.6%respectively.3 Obesity plays a central role in the insulinresistance syndrome, which includes hyperinsulinemia,hypertension, hyperlipidemia, and type 2 diabetesmellitus (DM).4Important health problems related toobesity are obstructive sleep apnea, degenerative jointdisease, cholecystitis, depression, reproductivecancers and infertility.4
A less well recognized association with childhoodobesity is chronic liver disease, known as nonalcoholicfatty liver disease (NAFLD). This disorder was firstdescribed in adults in the late 1970s and in children inthe mid 1980s.5 NAFLD represents fatty infiltration ofthe liver in the absence of alcohol consumption and isconsidered to be a hepatic consequence of metabolicsyndrome. According to the American Association for

the Study of Liver Diseases (AASLD), NAFLD isdefined as fat accumulation in the liver exceeding 5% to10% by weight, determined by the percentage of fat-laden hepatocytes on light microscopy. 6The prevalenceof NAFLD in obese children has been reported to rangefrom 20% to 77%.7 Most cases of NAFLD occur inpreadolescent and adolescent age group with malepredominance. Certain ethnic groups such as Hispanicand Asian may be more susceptible.5
The clinicopathologic spectrum of NAFLD ranges fromsteatosis or fatty liver, a reversible disorder to steatosiswith inflammation and fibrosis- nonalcoholicsteatohepatitis (NASH) to cirrhosis or hepatocellularcarcinoma.8 The progression of steatosis tosteatohepatitis is two hit process, proposed by Dayand James in 1998.9 Fat accumulation in the liver is thefirst hit; a consequence of the imbalance betweentriglyceride accumulation on one hand and lipid beta-oxidation and export on the other. Insulin resistance iswidely implicated in the initiation of NAFLD. Insulinresistance leads to hepatic steatosis, lipolysis andhyperinsulinemia. Lipolysis increases circulating freefatty acid and while increase uptake of FFA by liverleads to mitochondrial beta-oxidation overload andtherefore leading to accumulating fat in the liver.Hyperinsulinemia increases synthesis of fatty acid inthe liver by glycolysis and favouring hepaticaccumulation of triglyceride by decreasing Apo-Bproduction. Fat in the liver makes it vulnerable to thesecond hit. Factors involved in delivering the secondhit are thought to include oxidative stress andsubsequent lipid per oxidation, proinflammatorycytokines and adipocytokines. Increased hepatic FAoxidation can generate reactive oxygen radicals (ROS)that may promote mitochondrial dysfunction, lipidperoxidation and/or cytokine secretion. Cytokines arecapable of producing all the classical histologicalfeatures of NASH resulting in hepatocyte injury,inflammation and fibrosis. 10
The gold standard of diagnosis is liver biopsy but thisinvestigation is not frequently performed in the paediatricpopulation. In the absence of liver biopsy, presumedNAFLD is conventionally diagnosed by classicalultrasonographic hepatic appearances together with anelevated serum level of alanine aminotransferase (SGPT).7
Identification of children with an increased risk ofNAFLD is an important step in preventing irreversibleliver damage. This study will help us in early detectionof steatosis in obese children and adolescents and to
provide early intervention strategies to prevent furtherprogression of hepatic steatosis to its complications.
Aims and Objectives:The aims of our study were: (1) to determine theprevalence of hepatic steatosis among obese childrenand adolescents (2) to assess the correlation betweenultrasonographic hepatic steatosis and anthropometry,SGPT and metabolic abnormalities.
Methods:This was a cross sectional study done in BIRDEM fromJune 2009 to December 2009. Obese children andadolescents, 8 to 18 years of age, attending Paediatricendocrine outpatient department were included in ourstudy. Body mass index was used as an anthropometricmarker to diagnose obesity. According to official centersfor disease control (CDC), children with BMI e” 95th forage and sex were diagnosed as obese.11 Obese childrenhaving any dismorphism, endocrine or chromosomalabnormalities or diagnosed case of chronic hepatitisdue to metabolic, infectious or autoimmune cause wereexcluded from study. A predesigned data collectionsheet was used for each subject and informationregarding history, clinical examination andinvestigations were recorded.Weight was measured by spring scale in kilogram to thenearest 100 gram; standing height was measured bystadiometer to nearest 0.1 cm.The Body mas index (BMI)was calculated as weight in kilogram divided by squareof height in meter. Waist circumference was measuredat the level midway between the lower rib margin andthe iliac crest, at level of umbilicus (in centimeter) withthe person breathing out gently and hip circumferencewas measured at the maximum width over the buttocksat the level of greater trochenter by measuring tape (incentimeter).All subjects had blood samples taken in the morning,after an overnight fast, for the estimation of bloodglucose (by OGTT), SGPT, lipid profile, FT4 & TSH.During OGTT, fasting glucose 6.1-7.0 mmol/L, 2 hrplasma glucose <11.1mmol/L but >7.8 mmol/L signifiedIGT and fasting blood glucose >7mmol/L or 2-hr plasmaglucose e”11.1 mmol/L was considered as DM.12 In 8-15 years of age group, triglyceride (TG) level e”100 mg/dl was considered high while in 15-18 years of age groupTG >125 mg/dl was considered high.Hypercholesterolemia was defined as serum cholesterol>170mg/dl. SGPT >35 U/L was defined as high SGPT.12
Real-time abdominal USG examination was performedto rule out fatty liver by 3.5 MHz curvilinear transducer
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
58

using SONO ACE 8000 and Sonoline Antares ultrasoundmachine following 6-hours fast. In USG, ahyperechogenic (bright liver) indicated steatosis.Informed consent was taken from the parents. SPSS,version 12.0 for Windows software was used for datarecording and analysis. Chi-square test and Students t-test were used for comparing group ratios and groupaverages respectively. A P value less than 0.05 wasconsidered significant.Operational definitions:a) Hepatic Steatosis:Hepatic steatosis is a pathological conditioncharacterized by abnormal excessive accumulation oflipids mainly triglyceride in liver.9
b) Degree of fatty infiltration was graded as mild,moderate and severe according to ultrasonic appearanceof liver echotexture. The severity of echogenesity wasgraded as follows:mild steatosis - slight, diffuse increase in fine echoes inliver parenchyma with normal visualization of diaphragmand intrahepatic vessel borders.Moderate steatosis - moderate, diffuse increase in fineechoes with slightly impaired visualization ofintrahepatic vessels and diaphragm.Severe steatosis - marked increase in fine echoes withpoor or nonvisualization of the intrahepatic vessel borders,diaphragm, and posterior right lobe of the liver.13
Results:A total of 50 obese children and adolescents wereenrolled in the study. This was comprised of 30 boysand 20 girls of 8-18 years of age. 33 children (66%)belonged to 8-12 years age group while 17 children (34%)belonged to 13-18 years age group. The mean age of thesubjects was 11.24 years. Male: Female ratio was 1.5:1.Mean weight of the children was 55.79±17.62 kg, meanheight was 144.45±11.84 cm, mean BMI was 29.88±6.06kg/m2, mean Waist circumference (cm) was 69.77±31.79,mean Hip circumference (cm) was 60.36±39.36, meanwaist: hip ratio was 0.93:1. Among biochemicalparameters, mean level of SGPT was 35.93±19.56 U/L,triglyceride (TG) 165.80±58.07 mg/dl, cholesterol181.58±30.73 mg/dl, low density lipoprotein (LDL)111.0±30.53, high density lipoprotein (HDL) 37.18±9.34,fasting blood glucose 4.83±0.50, 2 hours after glucose7.39±1.49.The most prevalent abnormal lipid profile was highTG and that was detected in 78% children followed byhigh cholesterol level (68%) and high LDL (50%). High
SGPT was prevalent among 36% of obese children asshown in table-I.
Table-I
Metabolic abnormalities among obese childrenand adolescents (n=50)
Metabolic abnormalities Percentage (%)
High Triglyceride (TG) 78 %High Cholesterol 68 %High Low Density lipoprotein (LDL) 50 %CholesterolLow High Density Lipoprotein (HDL) 36 %CholesterolDiabetes Mellitus (DM) 6 %Impaired Glucose Tolerance (IGT) 12 %High SGPT 36 %In total, 18 obese children had ultrasonographicevidence of hepatic steatosis. The prevalence of hepaticsteatosis was 36% which is shown in figure-I
Fig.-1: Distribution of the patients according topresence of hepatic steatosis.
Thirteen children (72%) were found to have mild steatosiswhile five (28%) had moderate hepatic steatosis. Therewas no evidence of severe degree of hepatic steatosis.Out of twenty girls, five had hepatic steatosis as didthirteen boys. Prevalence of steatosis was high amongmale (72.2%) compared to female (27.8%).The mean ageof children having steatosis was 11.67 years. There is nostatistically significant difference in age (P=0.34) andanthropometric measurement including BMI (P=0.29) andWaist: Hip ratio (P=0.46) between children with or withouthepatic steatosis as shown in table- II.
The mean level of SGPT in obese children with hepaticsteatosis was 49.07(± 23.81) while 28.53(± 11.72) in
Hepatic Steatosis among Obese Children and Adolescents R Shelim et al.
59

children without steatosis.The mean level of triglycerideswas 186.39(± 42.24) in obese children with hepaticsteatosis and154.22 (± 62.99) in children withoutsteatosis. The mean level of cholesterol in children withor without steatosis was 191.56 (± 28.57) and 175.97(±30.89) respectively shown in table III
Table-IV: showed comparison of metabolic abnormalitiesin between these two groups. A correlation was evidentbetween High SGPT, cholesterol, LDL and hepaticsteatosis. High SGPT, high cholesterol and LDL weresignificantly common in obese children with hepaticsteatosis than children without steatosis (P <0.004,<0.05 and <0.04 respectively).
Table-II
Comparison of mean of age and anthropometric measurements in obese children and adolescentswith and without hepatic steatosis.
Anthropometric Hepatic Steatosis P value Measurements (Mean) Yes No
(n=18) (n=32)Age 11.67 11.0 0.34
(± 2.25) (±2.37)Height 148.32 142.28 0.08
(±8.78) (±12.88)Weight 61.78 52.42 0.07
(±16.78) (±17.44)BMI 31.08 29.20 0.29
(±42.73) (±6.15)Waist circumference 72.98 67.97 0.59
(±33.79) (±31.01)Hip circumference 57.40 62.02 0.69
(±42.73) (±37.095)Waist-Hip ratio 0.93 0.92 0.46
(±0.05) (±0.06)
Table -III
Mean biochemical parameters in obese children and adolescents with and without hepatic steatosis.
Biochemical parameters Hepatic steatosis
Yes No(n=18) (n=32)
SGPT 49.07 28.53(±23.81) (±11.72)
TG 186.39 154.22(±42.24) (±62.99)
Cholesterol 191.56 175.97(±28.57) (±30.89)
LDL 119.33 106.31(±33.25) (±28.35)
HDL 34.77 39.97(±5.78) (±10.85)
FBG 4.93 4.77(±0.51) (±0.49)
2HAG 7.62 7.27(±1.59) (±1.44)
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
60

Discussion:Liver disease is a serious complication of childhood obesity.Although much to be learned about NAFLD, it is alreadyevident that children with NAFLD, having high risk ofprogressive liver damage.5 In recent years, physicians havebecome increasingly interested in childhood obesity andaccompanying steatohepatitis, and many studies havebeen published about these topics.5,14,15
Male preponderance in obesity has been reported inmost of the studies in Bangladesh and in neighboringcountries.3,16,17 In the present study, male: female ratiowas found 1.5:1 which was similar to the previous studydone in BIRDEM, showing male: female ratio 1.3:1 andalso with other studies. 3, 16, 17 Among 50 obese childrenand adolescents, the most prevalent abnormal lipidprofile was high TG followed by high cholesterol andLDL level. All these figures were much higher than theprevious record in BIRDEM.17 In our study, prevalenceof IGT was 12% which was consistent with 17.1% and11.2% in different studies done in Bangladesh17 andabroad.18 The prevalence of diabetes mellitus was 6%,this figure was also consistent with other studies whereit was 4%.19
In present study, the prevalence of high SGPT amongobese children was 36%. The prevalence of high SGPTwas 25%, 48% and 47.1%, found in different studiesdone abroad.15, 20, 21The Third National Health andNutrition Examination Survey data have shown that 6%of overweight and 10% of obese adolescents haveelevated ALT levels.22
The exact prevalence of NAFLD is not wellestablished. Information on its prevalence amongchildren is scanty. In our study, the prevalence ofhepatic steatosis was 36%. Pooling data from studiesperformed mainly in tertiary medical centers- theprevalence of NAFLD in obese children has beenreported to range from20-77%.6 In an Italianmulticentric study, 53% obese children had radiologicalfatty liver.15 In one study of school-aged children innorthern Japan, overall prevalence of fatty liver was2.6% and increased to 10-35% in obese children.14
Study conducted among Chinese obese childrenshowed 77% had evidence of hepatic steatosis onsonography.23 In a small epidemiological study inIndia, prevalence of fatty liver was found 24%. 24
Table-IV
Comparison of metabolic abnormalities in obese children and adolescents withand without hepatic steatosis.
Metabolic Hepatic steatosis Odd ratio P valueAbnormalities Yes No
(n=18) (n=32) High SGPT 11 7 5.61 0.004
(61.1%) (21.9%) (1.58-19.87)
High Cholesterol 15 19 3.42 0.05(83.9%) (59.4%) (0.82-14.24)
High TG 16 23 3.13 0.09(88.9%) (71.9%) (0.59-16.45)
High LDL 12 13 2.92 0.04(66.7%) (40.6%) (0.87-9.78)
Low HDL 7 11 1.21 0.38(38.9%) (34.4%) (0.37-4.02)
DM 2 1 3.88 0.17(11.1%) (3.1%) (0.33-46.05)
IGT 2 4 0.87 0.45(11.1%) (12.5%) (0.14-5.32)
Hepatic Steatosis among Obese Children and Adolescents R Shelim et al.
61

In one study in Pakistan and Iran, 7.52% and 2.3% ofobese children had hyperechogenic fatty liverrespectively.25,21In present study 72% had mild, 28%had moderate hepatic steatosis, while no patient wasidentified to have severe steatosis. This finding iscomparable to study done by Madana et al.21 amongIranian obese children and by DFY Chan et al.23 amongChinese obese children and adolescents, based onultrasound score of fatty liver.
There had been male predominance (M 72.2%, F 27.8%)of hepatic steatosis found in our study with mean ageof 11.67±2.25 years. In the studies of Franzese et al.15
and Tominaga et al.14 there was no difference betweenfatty liver prevalence between boys and girls. However,male predominance and younger age at presentationwere postulated in different previous studies.23, 21
In ou study, when anthropometric measurements werecompared among obese children and adolescents withor without hepatic steatosis, there was no significantdifference between these two groups. This result wasnot similar to other study. Mandana Rafeey et al.21 andDFY Chan et al.23 showed in their studies, hepaticsteatosis was positively correlated with BMI, waist andhip circumference, triglyceride and insulin resistance,indicate that higher adiposity may lead to a greater degreeof fatty acid accumulation in the hepatocytes.
In the present study, high SGPT, high cholesterol andhigh LDL were more prevalent in children with hepaticsteatosis in comparison to children without steatosisbut there was no significant difference in TG, HDL andblood sugar level between these two groups. Nur Arslanet al.26 found a significant relationship between SerumTG and fatty liver in a study conducted among Turkishobese children. In another study among Iranian obesechildren and adolescents, total cholesterol and SGPTwere significantly higher among hepatic steatosis groupwhich is consistent with our findings.21
The best enzyme marker for hepatic steatosis appearsto be SGPT with a high sensitivity and specificity.Kawasaki et al.27 used SGPT as the predictor of fattyliver and found the correlation with of obesity to be thethird best as compared to immunoreactive insulin andserum triglyceride. The strong association between thedegree of steatosis and elevation of SGPT suggeststhat the greater degree of steatosis, the higher the chance
for inflammatory change and possible development ofmore progressive disease.23
Limitation of the study:In our study we did not make correlation betweenpredictors like socioeconomic status, exercise, dietarypattern or family history of dyslipidemia, DM,hypertension or fatty liver and hepatic steatosis whetherthese predictors resulted in steatosis in some obesechidren not in others. Sample size was small and durationof study was short. Patients with fatty liver did notundergo detailed evaluation for infective, metabolic andautoimmune hepatitis. In case of designing futureresearches in this field, special attention should be givento the above mentioned limitations.
Conclusion:Our study concludes that hyperechogenic (bright) liveron USG with hyperlipidemia and raised SGPT areimportant signs of liver dysfunction in obese childrenwith hepatic steatosis. In this study we attempted tofind out the obese children having hepatic steatosisand related metabolic abnormalities so that we couldmake necessary affords for helping children avoid theseserious liver problems as obesity with liver disease canget overlooked among the plethora of adverse outcomesrelated to childhood obesity. This may be helpful in thedevelopment of protocols designed to screen at- riskchildren and adolescents.
References:1. WHO consultation on obesity. Special issues in the
management of obesity in childhood and adolescence. InObesity Preventing and Managing the Global Epidemic,WHO, Geneva, 1998, pp.231-47.
2. Lustig RH, Preeyasombat C, Velasquez-MieyerPA.Childhood Obesity. In: Pes covitz OH, Eugster EA, editors.Pediatric Endocrinology Mechanisms, Manifestations andManagement. 1st ed. Philadelphia (PA) P: Lippincott,Williams& Wilkins; 2004: 682-714.
3. Mohsin F, Tayyeb S, Baki A, Zabeen B, Sharker S, BegumT, et al. Prevalence of obesity among affluent schoolchildren in Dhaka. Mymensingh Medical Journal 2010;19: 549-54.
4. Pinhas-Hamiel O, Dolan LM, Daniels SR. Increasedincidence of non-insulin dependent diabetes mellitusamong adolescents. J Pediatrics 1996; 128(5): 608-15.
5. Rashid M, Roberts EA. Nonalcoholic steatohepatitis inchildren. J Pediatr Gastroenterol nutr 2000; 30: 48-53.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
62

6. Neuschwandre-Tetri BA, Caldwell SH. Nonalcoholicsteatohepatitis summary of an AASLD Single TopicConference Hepatology 2003; 37(5): 1202-19.
7. Prashant Mathur, Manoja K das and Narendra K Arora.Non-alcoholic fatty liver disease and childhood obesity.Indian J of Pediatrics 2007;74: 401-407.
8. Clare Nugent, Zobair M Younossi. Evaluation andmanagement of obesity related Nonalcoholic fatty liverdisease. Gastroenterology and Hepatology 2007; 4(8):432-41.
9. Day CP, James OF. Steatohepatitis: A tale of two hits?Gastroenterology 1998; 114: 842-45.
10. Pessayre D, Berson A, Fromentry B. Mitichondria insteatohepatitis. Semin Liver Dis 2001; 21: 57-69.
11. Kuczmerski RJ, Ogden CL, Grummer- Strawn LM. 2000CDC growth charts; United States. Washington DC: Centerfor Disease Control and Prevention/National Center forHealth Statistics. Advance data314: 1-28.
12. Skelton JA, Rudolph CD. Overweight and obesity. In:Kliegman RM, Jenson HB, Behrman RE, Stanton BF,editors. Nelson Textbook of Pediatrics. 18th ed.
13. S Saadeh, Z M younossi, E M Remer, T Gramlich, J POng, et al. The utility of radiological imaging innonalcoholic fatty liver disease. Gastroenterology 2002;123: 745-750.
14. Tominaga K, Kurata JH, Chen YK, et al. Prevention offatty liver in Japanese children and relationship toobesity: an epidemiological ultrasonographic survey. DigDis Sci 1995; 40:2002-9.
15. Franzese A, Vajro P, Argenziono A, Puzziello A, IannucciMP, Saviano MC, et al. Liver involvement in obesechildren. Ultrasonography and liver enzyme levels atdiagnosis and during follow-up in an Italian population.Dig Dis Sci 1997; 42(7): 1428-32.
16. Kapil U, Singh p, Dwivedi SN, Bhasin S. Prevalence ofobesity among affluent adolescent school children inDelhi. Indian Pediatrics 2002; 39: 449-52.
17. Prevalence of Impaired Glucose Tolerance among Childrenand Adolescents with Obesity. Mohsin F, Mahbuba S,
Begum T, Azad K, Nahar N. Mymenshing Med J 2012;21(4): 648-90.
18. Brufani C, Ciampalini P, Grossi A, Flori R, Fintini D,Tozzi A,et al. Glucose tolerance status in 510 childrenand adolescents attending an obesity clinic in central Italy.Pediatr Diabetes 2009; 5: 416-20.
19. Third report of the National Education Program Expertpanel on Detection, Evaluation and treatment of HighBlood cholesterol in adults (Adult Treatment Panel ø):Exicutive Summary. Bethesda, MD: National Institutesof Health, 2001. NIH Publication No 01-3670.
20. Engelmann G, Lenhartz H, Grulich-Henn J. Obesity andmetabolic syndrome in children and adolescents. N Engl JMed 2004; 351(11): 1146.
21. Mandana R, Fakhrossadat M, Nafiseh M, GhergherehchiR, Shamsi G, Alka H. Fatty liver in children. Therapeuticsand Clinical Risk Management; 5: 371-74.
22. Strauss RS, Barlow SE, Dietz WH. Prevalence of abnormalserum aminotransferases values in overweight and obeseadolescents. J Pediatrics 2000; 136: 727-33.
23. Chan DFY, Li AM, Chu WCW, Chan MHM, Wong EMC,Liu EKH, et al. Hepatic steatosis in obese Chinese children.Int J Obes relat Metab Disord 2004; 28: 1257-63.
24. Singh SP, Nayak S, Swain M. Prevalence of nonalcoholicfatty liver disease in coastal eastern India: a preliminaryultrasonographic survey. Trop Gastroenterol 2004; 25:76-9.
25. M Ramzan, I Ali, A Matin. Sonographic assessment ofhepatic steatosis (fatty liver) in school children of DeraIsmail Khan City (NWFP) Pakistan. Pakistan Journal ofNutrition2009; 8(6): 797-99.
26. Arslan N, Buyukgebiz B, Ozturk Y, Cakmakci H. Fattyliver in obese children : prevalence and correlation withanthropometric measurements and hyperlipidemia. TheTurkish Journal of Pediatrics 2005; 47: 23-27.
27. Kawasaki T, Hashimoto N, Kikuchi T, Takahashi H,Uchiyama M. The relationship between fatty liver andhyperinsulinemia in obese children. J Pediatr Gastro Nutr1997; 24: 317-21.
Hepatic Steatosis among Obese Children and Adolescents R Shelim et al.
63

Summary:Background: Treatments of intracerebral hematoma (ICH)are controversial and surgical interventions in spontaneousICH are required and more accepted. Although advantageof neurosurgical intervention conservative treatment of ICHhas not been established, recent reports have suggestedfavourable effects of blood clot removal after liquefactionby means of urokinase. Objectives: To study the interventionby and out come in without or with complications ofBurrhole aspiration treatment after urokinase mediatedclot lysis; Study Design : Prospective interventional study.Place and Duration of Study: Departments of Neurosurgeryand Radiology & Imaging ,Dhaka Medical CollegeHospital, Dhaka, Bangladesh from July 2010 to December2010; Materials &Methods: A total of 30 Bangladeshipatients with spontaneous ICH (Age range: 40-75yrs,Meanage ±SD:59.1±11.52 years, Gender : 22 males, 8 females)full filling the criteria for spontaneous ICH were includedin the study. The desired information relevant to theobjectives were obtained and recorded carefully using astructured questionnaire; The Patients were treated withBurrhole aspiration after urokinase mediated lysis , evaluatedfor out come , complications and death and statisticallyanalyzed ; Results: The results on delays of intervention,types of intervention, doses of urokinase, post-operative
changes in haematoma volume, outcome with Glasgowoutcome scale(GOS) and GOS at follow–up, complicationsand death were presented with statistical analyses andsignificance .The outcome and death were compared withvarious variables such as hypertension (p <0.05), diabetesmellitus (p< 0.05) primary GOS (P<0.05),site of hematoma(p<0.05),volume of haematoma (p<0.05),ventricularextension of hematoma (p<0.05) and delay from ictus tointervention (p<0.05). Conclusion : It was observed thatearly treatment (within 24 hours of occurance) by usingminimally invasive technique and clot removal by urokinasemediated lysis can improve the consequences especially thosewith haematoma volume < 40 ml, lobar haematoma andwithout ventricular extension. Bad prognostic factors wereincrease of blood pressure, diabetes mellitus, GOS level <8,haematoma in the basal ganglia , ventricular extension ofthe haematoma volume> 40 ml and delay in intervention.However, the present was conducted with 30 patients onlyand therefore, studies with larger number of patients arerequired to draw more meticulous and more definitiveconclusions.
Key words: Intracerebral Haematoma, Burrhole Aspiration,Clot Lysis.
(J Bangladesh Coll Phys Surg 2016; 34: 64-75)
Journal of Bangladesh College of Physicians and SurgeonsVol. 34, No. 2, April 2016
Spontaneous Intracerebral Haematoma-II:Post-OperativeChanges and Outcome of Burrhole Aspiration after
Urokinase Mediated Clot LysisMN HOSSAINa, S NABIb, SS HOSSAINc
a. Dr. Mohammad Nazrul Hossain, Registrar, Dept. ofNeurosurgery, Apollo Hospitals, Bashundhara ResidentialArea, Dhaka, Bangladesh
b. Dr. Shahryar Nabi, Assistant Professor of Radiology andImaging, Dept of Radiology & Imaging, Dhaka MedicalCollege Hospital, Dhaka, Bangladesh
c. Prof. Dr. Sk. Sader Hossain, Professor and Head ofDepartment, Department of Neurosurgery, Dhaka MedicalCollege Hospital, Dhaka, Bangladesh
Address of Correspondence: Dr. Mohammad Nazrul Hossain,Registrar, Dept. of Neurosurgery, Apollo Hospitals, BashundharaResidential Area, Dhaka-1229, Bangladesh. Mobile: 01819496333,Email: [email protected]: 19 March, 2014 Accepted: 10 February, 2016
Introduction:Literature on spontaneous intracerebral hematoma (ICH)have been reviewed in our preceeding article where age,gender distribution, precipitating factors, clinical
presentations, neurological observations and CT scanfindings in our patients with spontaneous ICH weredocumented. Although treatments of ICH arecontroversial, surgical interventions in spontaneous ICHare required and more accepted1. Haematomas about 3cm diameter and those causing hydrocephalus generallyrequire surgical evacuation. The detailed account ofback ground scientific literature was not repeated here,as it has been stated in our preceding article.2-21 Theprocedure of intervention by, and outcome of, BurrholeAspiration after urokinase mediated clot lysis constitutethe contents of the present article, i.e. Part- II of our study.
Materials and Methods:Place & period of study, subjects of study, inclusion &exclusion criteria and data collection procedures were

stated and explained in our preceding article1. ICHDiameter was measured from maximum diameter of axialsection of CT scan; ICH Volume of haematoma wasmeasured by modified ellipsoid formula by ð/6 ABCwhich practically amounts to ½ ABC as described 22.
The procedure of catheter placement was determinedby the site of hematoma. Status of the patient during 3rd
post operative day (POD), at discharge and follow up(30th POD) were recorded. Outcome was measuredaccording to the modified Glasgow outcome scale (GOS)as suggested 23. Favorable: GOS 3-5 Unfavourable: GOS1 and 2. The flow chart of the patients presenting withfeatures of spontaneous ICH has been stated below :
Statistical AnalysisData were analyzed with descriptive statistics, Chi-squared () test and bi-variate analysis using computeraided statistical software SPSS win-17.The p value d”0.05 was used as the level of significance.
Results:InterventionsThe results on delays of intervention, types ofintervention and doses of urokeinase are presented inTable-1, Table-2, and Table-3 respectively. The post -operative changes in haematoma volume and GOS andGOS at follow up are presented in Table-4,Figure-1 &Table 5 respectively. The post- operative outcome(over all) complications, time of death and haemorrhageand death are stated in Figure-2 ,Table 6, Table-7 andTable-8 respectively.
The results on comparison of variables and outcome suchas hypertension & outcome, diabetes mellitus (DM) &death, GOS & outcome, site of haematoma and outcome,haematoma volume and outcome, ventricular extensionand outcome and finally delay, site of haematoma andoutcome are reported in Table 9a & 9b, Table-10, Table-
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
65

11a & 11b, Table-12a & 12b, Table 13a & 13b, Table 14a &14b, and Table-15a & 15b respectively.Delay: Table -1 shows that, on an average the delayfrom ictus to intervention was 41:43 hours with a rangefrom 7.00 to 72.00 hours.
Table -I
Distribution of the patients by their delay fromoccurrence to intervention
Time( Hours) Frequemncy Percent
<24:00 14 46.724:00 – 48:00 3 10.048:00 – 72:00 13 43.3Total 30 100.0
Mean ± SD, 41.34 ± 20.09 Hours, Mode 48:00 Hours,Range 7:00 to 72:00 HoursType of intervention: Table- 2 illustrate that catheterwas inserted in the Ventricle in 2 (6.6%) patients, in thecentre of haematoma in 23 (76.7%) patients and in bothin 5 (16.7%) patients..
Table-II
Distribution of the patients by thetypes of intervention
Intervention Frequency PercentCatheter in the centre of 23 76.7haematomaCatheter in the Ventricle 2 6.7Catheter in Both 5 16.7Total 30 100.0
Dose: Table- 3 shows that, on an average the patientsreceived 5.7 doses (instillation and aspiration) ofurokinase with a range from 2 to 10 times; Most of them(14,46.7%) received 4 to 6 doses.
Table-III
Distribution of the patients by the doses of urokinase
Dose Frequency Percent<3 6 20.04 -6 14 46.7> 7 10 33.3Total 30 100.0
Mean ± SD: 5.70 ± 2.38, Mode :4 ,Range: 2 to 10 times
Post-operative changesChange in haematoma :Table- 4 shows that, averagehaematoma volume on 3rd POD was 7.67 ml. Only in asingle patient, the volume in ventricle had increased.
Table-IV
Distribution of the patients by their changes inhaematoma volume
Volume of Ventricular extension Totalhaematoma Yes Nod” 5 ml 6 4 105 -10 ml 4 5 9> 10 ml 2 2More blood in ventricle 1 1Total 10 12 22
Mean ± SD: 7.67 ± 4.531, Mode: 10, Range :2 to 20 m
Change in GOS: Figure-1 explains that, more than one-fourth of the patients (8, 26.67%) died before 3rd POD(the first day for post-operative assessment of changesachieved through intervention). In a single (3.33%)patient GOS decreased. Out of the remaining 21 cases,GOS increased 1 to 5 points.
Fig.-1: Distribution of the cases by the change in GOSon 3rd POD.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
66

GOS at follow up :Table 5 shows that, among the livepatients, the GOS level had increased, i.e. on admissionthe level ranged from 6 to 11 and on 30th POD the lowestlevel was 10.GCS and also, the average of GCS hadincreased from 8.00 (On admission) to 13 (On 30th POD).There is positive correlation between the changes ofGCS level among the alive cases.
Outcome, Complications & Death Outcome of intervention overall : Figure-2 explainsthat near about three-fourth (22, 73.33%)] of the patientshad unfavourable outcome; 14 (46.67%) ‘Death’ and 8(26.67%) ‘Severe disability’. The remaining 8 hadfavourable outcome; 5 (16.67%) ‘Moderate disability’and 3 (10.0%) ‘Good recovery’.
Complications: Table - 6 illustrates that Iatrogenicpneumocephalous was the most (5, 16.7%) occurringcomplication;. 15 (50%) of the interventions wereuncomplicated.
Time and cause of death: Table -7 shows that respiratorydistress’ was the cause of most (7, 23.33%) deaths.
Haemorrhage and death :Table- 8 shows thatinvolvement of different areas of the cerebral hemispherehad strong association in outcome, when only deathwas considered; i.e. only 14.3% patients with corticalhaematoma died, on the contrary 85.7% patients withICH in the basal ganglia with ventricular extension (3 ormore ventricles) died.
Table-V
Distribution of alive cases by the GOS at follow - ups
GOSFollow up 6 - 8 9 - 12 13 - 15 Total Mean ± SDOn 3rd POD 3 14 5 22 10.95 ± 2.535At discharge 1 9 7 17 12.18 ± 1.879On 30th POD 4 12 16 13.44 ± 1.548
Correlation [GOS (on admission and on 3rd POD)], R = 0.724 R = 0.740 p = 0.001Correlation [GOS (on admission and at discharge)],R = 0.846 R = 0.846 p = 0.000Correlation [GOS (on admission and on 30th POD)],R = 0.787 R = 0.641 p = 0.002
Fig.-2: Distribution of the patients by their outcome (according to GOS).
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
67

Variables and OutcomeHypertension and outcome: Table -9a shows , an inverserelation of blood pressure with outcome ,i.e. with theincrease of BP (both systolic and diastolic) GOSdecreases’. Table-9b shows that atthough all the deathswere among those with high blood pressure, thedifference in death in respect of hypertension was notstatistically significant( x2 = 22.969, p > 0.05).
GOS and Outcome: Table 11a shows that outcomeachieved depended on initial GOS (on admission). Theincidence of death was higher in patients with lowerGOS level group. All of the patients with ‘goodrecovery’ had a GOS of 9 to 12 and patients with‘moderate disability’ had initial GOS more than 6. Table-11b shows the incidence of death among patient withprimary GOS; it was significantly higher in patients withlower GOS on admission (X2=3.519, p < 0.05).
Table-VI
Distribution of the cases by their postoperative complications
Complications Frequency Percent
No complication 15 50.0Pneumocephalous 5 16.7Accidental catheter withdrawal 2 6.7Aspiration pneumonia 2 6.7Chest pain 2 6.7Others (Meningitis, Re-stroke, Re-bleeding, Psychosis) 4 13.3
Total 30 100.0
Table-VII
Distribution of the cases by their time and cause of death
Cause of death Time of death TotalBefore Before Before3rd POD discharge 30th POD
Respiratory distress then death 7 7Sudden chest pain, then death 3 3Meningitis 1 1Aspiration pneumonia 1 1Re-bleeding 1 12nd stroke 1 1Total 8 5 1 14
Table-VIII
Distribution of the cases by their ICH and of death
Area of ICH Number (n) Death Percentage (%) Fraction of deathCerebral cortex 7 1 14.3 7.15Basal ganglia without ventricular extension 6 3 50.0 21.43Basal ganglia ventricular extension (<3 ventricle) 10 4 40.0 28.57Basal ganglia ventricular extension (e”3 ventricle) 7 6 85.7 42.85Total 30 14 46.7 100
Com
plic
atio
ns
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
68

Table- IX a
Distribution of the cases by hypertension and outcome
Outcome TotalDeath Persistent Severe Moderate Good
vegetative disability disability recoverystate
Mild hypertension 6 5 3 14Moderate hypertension 6 1 7Severe hypertension 8 1 9Total 14 8 5 3 30
Table-IX b
Distribution of the cases by hypertension and death
hypertension Outcome TotalDead Alive
Mild 0 14 14Moderate to severe 14 2 16Total 14 16 30
c2 = 22.969, df= p<0.05DM and death; Table-10 shows that all the 7 (23.33%) DM patients suffering from spontaneous ICH died.
Table -X
Distribution of the patients by DM and death
DM Death TotalYes No
Yes 7 0 7No 0 0 0Total 7 0 7
Table -XI a
Distribution of the patients by their primary GOS and outcome
GOS Outcome TotalDeath Persistent Sever Moderate Good
vegetative disability disability recoverystate
6 to 8 11 4 1 169 to 12 3 4 4 3 14Total 14 8 5 3 30
Hyp
er-
tens
ion
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
69

Site of haematoma and outcome :Table-12a shows thatoutcome of haematoma in the basal ganglia was notgood, as out of 23 (76.67%) haematoma 13 (43.33%)died. All 3 ‘good recovery’ had cortical haematoma.Table- 12b shows that the death rate was higher inpatients with haematoma in the basal ganglia which wasstatistically significant( p = 0.05).Hematoma volume and outcome: Table-13a indicatesthat outcome of large haematoma was not good; deathrate was high among patients with larger haematoma.All 3 ‘good recovery’ was with smaller haematoma.Table- 13b shows that, the difference between deathand haematoma volume was statistically significant(c2 = 0.117, p<0.05).
Ventricular extension and outcome :Table-14a showsthat the ratio of death was higher among patients with
ventricular extension of the haematoma as 10 (33.33%)died out of 18 (60.0%) patients were with ventricularextension. All the patients with ‘good recovery’ did nothave any ventricular extension of the haematoma.Table14b shows that the difference in death amongpatients with ventricular extension of haematoma wasstatistically significant (p < 0.05)Delay, site haematoma and outcome: Table 15a explainsthat the cortical haematoma showed time dependantoutcome, ‘the earlier the intervention the better therecovery. The single death in patient suffering from ICHin the cortex, had a 72 hours delay from incidence tostart of intervention. Table -15b shows that there wasstatistically significant difference in death and intervalbetween ictus and intervention (p < 0.05); Better resultswere shown with early intervention
Table- XI bDistribution of the patients by their primary GCS and death
Outcome TotalDead Alive
GCS 6 6 2 8> 6 8 14 22
Total 14 16 30
c2 = 3.519 df=1 p=0.05
Table- XII aDistribution of the cases by their site of haematoma and outcome
Location of Outcome Totalhaematoma Death Persistent Sever Moderate Good
vegetative state disability disability recoveryBasal ganglia 13 7 3 23Cortical 1 1 2 3haematomaTotal 14 8 5 3 30
Table -XII bDistribution of the cases by the location of haematoma and death
Outcome TotalDead Alive
Basal ganglia 13 10 23
Cortex 1 6 7
Total 14 16 30
c2 = 3.846 , df = 1 p= 0.05
Loca
tion
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
70
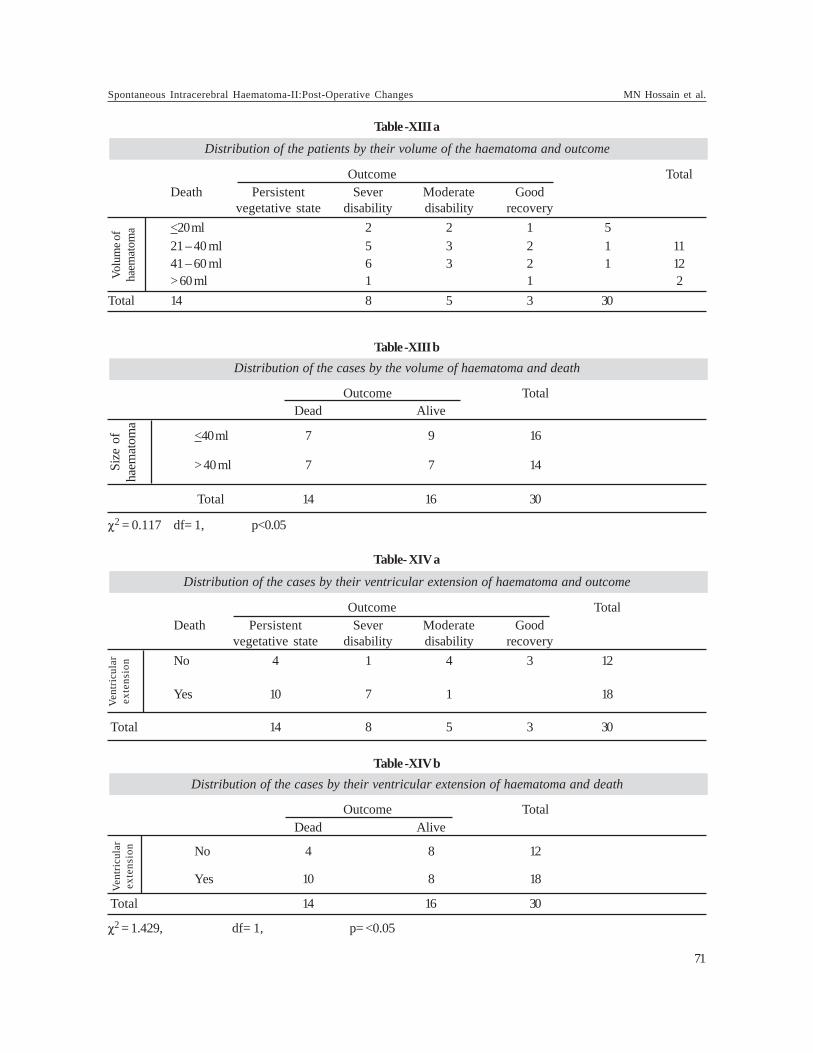
Table -XIII aDistribution of the patients by their volume of the haematoma and outcome
Outcome TotalDeath Persistent Sever Moderate Good
vegetative state disability disability recovery<20 ml 2 2 1 521 – 40 ml 5 3 2 1 1141 – 60 ml 6 3 2 1 12> 60 ml 1 1 2
Total 14 8 5 3 30
Table -XIII bDistribution of the cases by the volume of haematoma and death
Outcome TotalDead Alive
<40 ml 7 9 16
> 40 ml 7 7 14
Total 14 16 30
c2 = 0.117 df= 1, p<0.05
Table- XIV a
Distribution of the cases by their ventricular extension of haematoma and outcome
Outcome TotalDeath Persistent Sever Moderate Good
vegetative state disability disability recoveryNo 4 1 4 3 12
Yes 10 7 1 18
Total 14 8 5 3 30
Table -XIV bDistribution of the cases by their ventricular extension of haematoma and death
Outcome TotalDead Alive
No 4 8 12
Yes 10 8 18
Total 14 16 30
c2 = 1.429, df= 1, p= <0.05
Size
of
haem
atom
aVe
ntri
cula
rex
tens
ion
Vent
ricu
lar
exte
nsio
nVo
lum
e of
haem
atom
a
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
71

Discussion:The age – gender information, precipitating factors ,clinical presentations , neurological observation andCT scan findings in spontaneous ICH were presentedand discussed in our previous article (Part-I )1.In thepresent article (Part -II), the surgical intervention by,and outcome of, Burrhole aspiration after urokeniasemediated clot lysis were presented and discussed aspart –II of our study findings.On an average, the delay from ictus to intervention was41:43 hours with a range from 7:00 to 72:00 hours. Amongour patients, 47(49%) were operated within 24 hours, 21(22%) between 24 to 48 hours, 14 (15%) between 48 to72 hours and 13 (14%) between 3 to 7 days. Only 01patient was operated beyond 7 days after ictus24. Our27(67.50%) patient’s presented within 2 days and13(32.50%) patients attended after 2 days.)19,25.
Catheter in the Ventricle was inserted in 2 (6.6%) patients.Catheter was placed in the centre of the haematoma in
23 (76.7%) patients and the remaining 5 (16.7%)] werebenefited by both centre of haematoma and ventricleprocedures. On an average, the patients received about6 doses (instillation & aspiration) of urokinase with arange from 2 to 10 times. Most of them [14 (46.7%)]received 4 to 6 doses. Out of total 40 patients with ICH,in 25(62.5%) patients Burrhole aspiration of haematomawas done, in 8(20.00%) patients external ventriculardrainage, in 5( 12.50%) patients craniectomy anddecompression, in 2 patients (5.0%) cranicctomy andevacuation of haematoma was done 19,26 Out of total 29patients with ICH, in 8(27.56%) patients externalventricular drainage, in 7( 24.13%) patient’s craniectomyand decompression, in 14(48.27%) patient’s craniotomyand evacuation of haematoma was done27 .Out of total30 patients with ICH, in 13 (43.3%) patients craniotomyand evacuation of haematoma was done, in 13 (43.3%)patients Burrhole aspiration of haematoma was done, in3 (10%) patients craniectomy and evacuation of
Table -XV a
Distribution of the patients by their outcome with site of haematoma and delay from ictus to intervention
Table -XV b
Distribution of the cases by their delay and death
Outcome TotalDead Alive
Delay < 24 hrs 6 8 14> 24 hrs 8 8 16
Total 14 16 30
c2 = 0.153, df= 1, p<0.05
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
72

haematoma was done, in 1 (3.3%) patient externalventricular drainage (EVD) was done 28,29.
Average haematoma volume on 3rd POD was 7.67 ml.Only in 1(one) patient, the volume in ventricle hadincreased. a mean ICH volume of 65.4 ml (SD 28.1 ml) onday 1, 47.5 ml (SD 30 ml) on day 3, and 44.4 ml (SD 30.7ml) on day730.The average haematoma volume afteroperation was 7.60 ml. With each dose of urokinase theaverage haematoma volume decrease varied inindividuals from as less as 2.0 ml to 15.0 ml. . In a single(3.33%) patient GOS decreased. Out of the remaining 21cases, GOS increased 1 to 5 points. In most cases [9(30.0%)], the increase was by 3 points, followed by 2points in 7 (23.33%) cases and 4 in 3 (10.0%) cases.Motor strength of all the live patients gradually increasedexcept only a single case who eventually died.
More than one-fourth of the patients [8 (26.67%)] diedbefore 3rd POD (the first day for post-operativeassessment of changes achieved through intervention).In a single (3.33%) patient GOS decreased. Out of theremaining 21 cases, GOS increased 1 to 5 points. Again,among the live patients the GOS level had increased, i.e.on admission the level ranged from 6 to 11 and on 30th
POD the lowest level was 10. GOS and also, the averageof GOS, had increased from 8.00 (On admission) to 13.44(On 30th POD). There is positive correlation betweenthe changes of GOS level among the alive cases.{Correlation [GOS (on admission and on 3rd POD)] =0.724; R = 0.740 (p = 0.001); Correlation [GOS (onadmission and at discharge)] = 0.846; R = 0.846 (p =0.000) and Correlation [GOS (on admission and on 30th
POD)] = 0.787; R = 0.641 (p = 0.002)}.
About three-fourth [22 (73.33%)] of the patients hadunfavourable outcome; 14 (46.67%) ‘Death’ [among them1 (7.14%) patient from lobar haematoma, 3 (21.42%)patients from basal ganglia without ventricularextension, 4 (28.57%) patients from basal ganglia withless than three ventricular extension and remaining 6(42.82) patients from basal ganglia with more than threeventricular extension and 8 (26.67%) ‘Sever disability’[’(one from lobar(12.5%), six from basal ganglia withless than three ventricle extension (75.0%) and one frombasal ganglia with more than three ventricleextension(12.5%)]. The remaining 8 had favourableoutcome; 5 (16.67%) ‘Moderate disability’ [two fromlobar (40.0%) and 3 (60.0%) basal ganglia without
ventricular extension] and 3 (10.0%) ‘Good recovery’(allfrom lobar haematoma). In basal ganglia mortality is 25%,severe disability was 50% and moderate disability was25%31. In lobar haematoma mortality was 41.2%, severedisability was 35.5% and moderate disability was 23.5%.In Basal ganglia with ventricular extension, mortalitywas 100% and lobar haematoma with ventricularextension mortality was 71.4 %.
Of the interventions 50% (15) were uncomplicated.Iatrogenic pneumocephalous was the most [5 (16.7%)]occurring complications, 2 (6.7%) individuals each had‘accidental catheter withdrawal’, aspiration pneumoniaand chest pain. Other complications like, meningitis, re-stroke, re-bleeding, psychosis accounted for a single(3.3%) case. Near about half [14 (46.67%)] of the patientsdied. Out of the deaths, most [8 (26.67%)] occurredbefore 3rd POD (1st date for assessment of outcome).‘Respiratory distress’ was cause of 7(50.0%) deaths.Myocardial infraction was responsible for 3 (21.48%)deaths. Re-bleeding, meningitis, aspiration pneumoniaand re-stroke were the cause of remaining 4 (28.52%)deaths. Jin et al reported that nine patients (16.9%) diedbefore hospital discharge (one from cardiac problemsand eight from respiratory failure).18
Involvement of different areas of the cerebral hemispherehad strong association in outcome when only deathwas considered, i.e. only 14.3% patients with corticalhaematoma died. On the contrary, 85.7% patients withICH in the basal ganglia with ventricular extension (3 ormore ventricles) died. An inverse relation of bloodpressure with outcome, ie ‘with the increase of BP (bothsystolic and diastolic) GOS decreased. Although all thedeaths were among those with ‘moderate to high bloodpressure’, the difference in death in respect ofhypertension was not statistically significant ( p > 0.05).All the 7 (23.33%) diabetic patients suffering fromspontaneous ICH died. Outcome achieved dependedon initial GCS (on admission). The ratio of death washigher in patients with lower GOS level group. All of thepatients with good recovery had a GOS of 9 to 12 andpatients with ‘moderate disability’ had initial GOS morethan 6. Death rate was higher in patients with lowerGOS on admission; the difference was statisticallysignificant (p < 0.05). Outcome of haematoma in thebasal ganglia was not good, as out of 23 (76.67%)haematoma 13 (43.33%) died. All 3 good recovery hadcortical haematoma. Although the death rate was higher
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
73

in patients with haematoma in the basal ganglia, thedifference was not statistically significant; (p > 0.05).Outcome of large haematoma volume was not good;death rate was high among patients with largerhaematoma (>40 ml). All 3 good recovery was with smallvolume of haematoma (<40 ml). The difference wasstatistically significant between death and haematomavolume.( p < 0.05). The ratio of death was higher amongpatients with ventricular extension of the haematoma as10 (33.33%) died out of 18 (60.0%) patients withventricular extension. On the contrary, only 4 (13.33%)died among the 12 (40.0%) cases without ventricularextension. The death rate was 1.67 times higher inpatients with ventricular extension. All the patients withgood recovery did not have any ventricular extensionof the haematoma. The difference in death amongpatients with ventricular extension of haematoma wasstatistically significant; p < 0.05. The cortical haematomashowed time dependant outcome, ‘the earlier theintervention the better was the recovery’. The singledeath in patient suffering from ICH in the cortex had a72 hours delay from incidence to start of intervention.There was statistically significant difference in deathand interval between ictus and intervention indicatingbetter results with early intervention (p<0.05). Outcomeof study by Jin et al, was - at discharge, 25 patients(47%) had achieved good recovery (17patients GOS 3, 6patients GOS 4 and 2 patients GOS 5), and 19 patients(35.8%) remained vegetative (GOS 2)18,32,33. At 6 monthsfollow up, 29 patients (55%) had achieved good recovery(17 patients GOS 3, 8 patient GOS 4, and 4 patients GOS5) and 15 patient ,(28.3%) remained vegetative (GOS 2).
However the current study was conducted among 30patients only, not a large study to draw a definitneconclusion. Study of Spontaneous ICH in theperspective of the objective of the study was rare,causing difficulty to compare the findings to otherresearch findings. Patients came from all corners of thecountry after referral from local primary and secondaryhospitals, even from some tertiary hospitals. So, thedelay in occurrence to intervention took its toll as deathof the patients or severe disability. Patients had theirlast follow up on 30th POD, very short duration toovercome neurological deficits. If the duration werelonger, the condition of the live patients would havebeen better ideally. It meant that larger study includingmore patients with longer postoperative follow-up and
minimal delay between the occurrence of ICH andintervention should be done to draw more definitiveconclusion.
In Conclusion, early treatment (within 24 hours ofoccurrence) by using minimally invasive technique andclot removal by urokinase mediated clot lysis canimprove the consequences especially those withhaematoma volume <40 ml, lobar haematoma and withoutventricular extension. Bad prognostic factors wereincrease of BP (both systolic and diastolic), diabetesmellitus, GOS level <8, haematoma in the basal ganglia,ventricular extension of the haematoma volume >40 mland delay in intervention.
Acknowledgements:The authors would like to thank and gratefullyacknowledge Dr. K. A. Jhuma for valuable suggestionsand help during preparation of the manuscript.
References:1. Hossain MN, Hossain SS, Nabi S .Spontaneous intracerebral
Haematoma-I; Socioeconomic information, precipitatingfactors, clinical presentations, neurological observationsand CT scan findings. J of the College of Physicians andSurgeons Pakistan; 2013 (submitted).
2. Ojemann RG & Heros RC. Spontaneous brain hemorrhage.Stroke1983; 14(4): 468-75.
3. Siddique MS & Mendelow AD. Surgical treatment ofintracerebral hemorrhage. Br Med Bull 2000; 56(2):444-56.
4. Lejeune JP &Thines L. Neurosurgical management ofspontaneous cerebral hemorrhage. J Neuroradiol 2003;30(5): 332-5.
5. Escosa BM & Sola RG. Surgical indications in nontraumatic intracerebral hemorrhage. Rev Neurol 2001;32(11): 1060-2.
6. Unwin DH, Batjer HH and Greenlee RGJR. Managementcontroversy: medical versus surgical therapy forspontaneous intracerebral hemorrhage. Neurosurg Clin NAm 1992; 3: 533–537.
7. Kingman TA, Mendelow AD, Graham DI & Teasdale GM. Experimental intracerebral mass: description of model,intracranial pressure changes and neuropathology. JNeuropathol Exp Neurol 1988; 47: 128–137.
8. Chambers IR, Banister K& Mendelow AD. Intracranialpressure within a developing intracerebral haemorrhage.Br J Neurosurg 2001; 15: 140–141.
9. Zazulia AR, Diringer MN, Videen TO, Adams RE, YundtK, Aiyagari V, Grubb RLR, & Powers WJ, Hypoperfusionwithout ischemia surrounding acute intracerebral
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
74

hemorrhage. J Cereb Blood Flow Metab .2001 ;21:804–810.
10. Zazulia AR, Diringer MN, Derdeyn CP& Powers WJ.Progression of mass effect after intracerebral hemorrhage.Stroke 1999; 30: 1167–1173.
11. Lee KR, Kawal N, Kim S, Sagher O& Hoff JT.Mechanisms of edema formation after intracerebralhemorrhage: effects of thrombin on cerebral blood flow,blood-brain barrier permeability and cell survival in a ratmodel. J Neurosurg 1997; 86: 272–278.
12. Prasad K& Shrivastava A. Surgery for primarysupratentorial intracerebral haemorrhage. CochraneDatabase Syst Rev2000; 2: CD000200.
13. AuerLM, Ascher PW, Heppner F, Ladurner G, Bone G&Lechner H. Does acute endoscopic evacuation improvethe outcome of patients with spontaneous intracerebralhemorrhage? Eur Neurol 1985; 24: 254–261.
14. Zucacrello M, Andaluz N& Wagner KR. Minimallyinvasive therapy for intracerebral hematomas. NeurosurgClin N Am 2002; 13(3): 349-54.
15. MillerDW, Barnett GH, Kormos DW& Steiner CP.Stereotactically guided thrombolytic of deep cerebralhemorrhage: preliminary results. Cleve Clin J Med 1993;60: 321–324.
16. Montes JM, Wong JH, Fayad PB & Awad IA. Stereotacticcomputed tomographic-guided aspiration andthrombolysis of intracerebral hematoma: protocol andpreliminary experience. Stroke 2000; 31: 834–840.
17. Rohde V, Rohde I, Reinges MH, Mayfrank L& GilsbachJM. Frameless stereotactically guided catheter placementand fibrinolytic therapy for spontaneous intracerebralhematomas: technical aspects and initial clinical results.Minim Invasive Neurosurg 2000; 43: 9–17.
18. Jin SC, Hwang SK, Cho DS, Kim SH& Park DB. . UrokinaseThrombolysis for Nonaneurysmal SpontaneousIntraventricular Hemorrhage. J Korean Neurosurg Soc2005;38 : 281-286.
19. Das S. MS (Neurosurgery thesis). Role of surgery inprimary spontaneous intracerebral haemorrhage- AnalysisOf early outcome of surgery in relation to site and size ofhaemorrhage; BSMMU, Dhaka, Bangladesh; April 2004.
20. Rahman A. MS(Neurosurgery thesis) To compare theoutcomes between surgical and medical treatment ofspontaneous supratentorial intracerebal haemorrahge andalso to compare the outcomes according to Glasgow ComaScale (GCS), Glasgow outcome scale (GOS), Modified
Rankin Scale (MRS) and mortality between two groups;CMC,Chittagong, Bangladesh, June 2008.
21. ISLAM, T.K.M. MS(Neurosurgery thesis) Analysis Ofearly outcome of surgery in relation to preoperativeGlasgow coma scale (GCS) score and volume of haematoma;DMC, Dhaka, Bangladesh; sep 2010
22. Urokinase. http://en.wikipedia.org/wiki/urokinase(modified on 24 september 2010 at 23.10)
23. Manno EM, Atkinson JLD, Fulgham JR & WijdicksEFM.Emerging medical and surgical management strategiesin the evaluation and treatment of intracerebralHemorrhage, Symposium on cerebrovascular Disease.Mayo clin proc.2005 march; 80: 420-433. URL:http://enotes.tripod.com/ich 2005.htm
24. PAI SB, Varma RG, Parthiban JKBC.. Keyhole craniotomyin the surgical management of spontaneous intracerebralhematoma. Neurology Asia 2007;12: 21 – 27.
25. Kazui S, Minematsu K, Yamamoto H, Sawada T, YamaguchiT. Predisposing factors to enlargement of spontaneousintracerebral hematoma. Stroke.1997; 28: 2370-5.
26. Kazul S, Naritomi H, Yamamoto H, Sawada T& YamaguchiT. Enlargement of spontaneous intracerebral hemorrhage:incidence and time course. Stroke 1996; 27:1783-7.
27. Mayer SA, Sacco RL, Shi T& Mohr JP. Neurologicdeterioration in noncomatose patients with supratentorialintracerebral hemorrhage. Neurology1994; 44:1379-84.
28. Mutlu N, Berry RG& Alpers BJ,.Massive cerebralhemorrhage: clinical and pathological correlations. ArchNeurol 1963;8 :644-61.
29. Nath FP, Jenkins A, Mendlow AD, Graham DI & TeasdaleGM. 1986. Early hemodynamic changes in experimentalintracerebral hemorrhage. J Neurosurg 1986;65:697-703.
30. Teernstra OPM, Evers SMAA, Lodder J,& Leffers P.Stereotactic Treatment of Intracerebral Hematoma byMeans of a Plasminogen Activator. Stroke.2003; 34:968-974.
31. Tanaka A, Yoshinaga S, Nakayama Y, Kimura M &Tomonaga M. Cerebral blood flow and clinical outcomein patients with thalamic hemorrhages: a comparison withputaminal hemorrhages. J Neurol Sci 1996 ;144:191-7.
32. Wagner KR, Xig G, Hua Y, et al. Lobar intracerebralhemorrhage model in pigs: rapid edema development inperihematomal white matter. Stroke 1996;27:490-7.
33. Ropper AH & Gress DR Computerized tomography andclinical features of large cerebral hemorrhages. CerebrovascDis 1991; 1:38-42.
Spontaneous Intracerebral Haematoma-II:Post-Operative Changes MN Hossain et al.
75

Summary:Back ground: Abdominal tuberculosis is common inBangladesh and there is a national guide line for itsmanagement, which includes six months course of antitubercular therapy (ATT). This study was done to evaluatethe treatment outcome of abdominal tuberculosis followingnational guide line. Materials and Methods: This prospectivestudy of descriptive nature was done between November 2009to October 2010 at the department of Medicine, SirSalimullah Medical College, Mitford hospital, Dhaka,Bangladesh. Total 6 months ATT was given to the selective50 patients of abdominal tuberculosis following nationalguide line and out come measurement was done aftercompletion of treatment. Result: Five patients died out of50 patients during the course of treatment. The range ofage was 13-70 years and mean ± SD = 33.2 ± 14.77 andmale female ratio was o.72:1.
Out of 50 patients 17(34%) patients had Intestinal TB,24(48%) had Peritoneal TB, 2(4%) had abdominal lymphnode TB, and 7(14%) had other types. Three patients ofperitoneal TB patient died while rest 2 patients died werediagnosed as intestinal TB. Out of 45 patients who survived,43(95.6%) improved and 2(4.4%) did not improve. Out of15(33.3%) intestinal TB patients, 14(31.1%) improved and1(2.2%) did not improved. Out of total 21(46.7%) peritonealTB, 20(44.4%) improved and 1(2.2%) did not improve.Remaining 2(4.4%) abdominal lymph node TB, all wereimproved. In other variety cases (15.6%), all improved.Conclusion: Total 6 months regimen of ATT recommendedby national guide line is proved as a complete and effectivetreatment course of abdominal tuberculosis.
Key words: Abdominal tuberculosis, Treatment out come,National guide line.
(J Bangladesh Coll Phys Surg 2016; 34: 76-84)
Treatment Outcome in Patients of Abdominal Tuberculosisreceiving Antitubercular Chemotherapy according to
National Tuberculosis Guideline of BangladeshDN SARKARa, R AMINb, H MOHAMMEDc, MN ROYT d, MA AZHARe, MA FAIZf
a. Dr. Devendra Nath Sarkar, Associate Professor of Medicine,Rangpur Medical College
b. Dr. Robed Amin, Associate Professor of Medicine, DhakaMedical College, Dhaka
c. Dr. Hanif Mohammed, Associate Professor of Medicine,Mymensingh Medical College
d. Prof. Monidra Nath Roy, Professor of Bio Chemistry, SirSalimullah Medical College. Dhaka
e. Prof. MA Azhar, Professor and Head, Department ofMedicine and Principal, Sir Salimullah Medical College andMitford Hospital, Dhaka
f. Prof. MA Faiz, Professor of Medicine (Retired) SirSalimullah Medical College, Dhaka
Address of Correspondence: Dr .Md. Robed Amin, AssociateProfessor of Medicine, Department of Medicine, Dhaka MedicalCollege, Dhaka .Bangladesh.Apt-C-2, House no-76, Road-5, Block-F, Bonani, Dhaka, Bangladesh. e.mail: [email protected]
Received: 13 August, 2014 Accepted: 7 February, 2016
Introduction:Tuberculosis can involve any organ system in the body.While pulmonary tuberculosis is the most commonpresentation, extra-pulmonary tuberculosis (EPTB) is
also an important clinical problem1.2.3. Abdominal TB iscommon in Bangladesh and other tropical countries andposes a significant health hazards4.There is no extensivestudy done in our country regarding abdominaltuberculosis. One retrospective study done by RoufHMA in general Hospital. Sirajgonj.5 He showed that 16cases presented with acute surgical emergencies out of43 cases, 12 of them presented with intestinal obstruction(25%), and rest 27% had chronic symptoms. Faiz M Adid another retrospective study in 1989 in IPGM&R onextra- pulmonary tuberculosis6. He found intestinaltuberculosis in five cases out of 47 patients having extra-pulmonary tuberculosis6 The diagnosis ofgastrointestinal tuberculosis is often delayed,increasing the morbidity associated with this treatablecondition7 . Abdominal TB has a good prognosis ifpromptly diagnosed and treated8. A high clinical indexof suspicion and judicious use of diagnostic procedurecan certainly help in timely diagnosis and treatment andthus reduce the mortality of this curable but potentiallylethal disease9. Marshal et al and Anond et al also

recommend clinical trial in endemic countries 9,10.
Management of all patients with abdominal tuberculosisshould be given standard full course of antituberculartherapy (ATT). Duration of treatment is different indifferent canters. Treatment with three drug regimen fornine month was also used as anti tuberculosis treatment.
Successful treatment of abdominal tuberculosis for oneto one and a half year11 is also the recommendation byKilmach et al, Quorian et al and Schfield et al.12,13,14.Previously 18-24 months regime was popular, then 1year regime and now six months of total duration isconsidered sufficient for chemotherapy15,16,17.
In Bangladesh, there is a national guide line for treatmentof all kinds of TB patients. It is recommended total sixmonths ATT for the treatment of abdominal tuberculosispatients18. All patients of abdominal tuberculosis shouldreceive conventional anti-tubercular therapy for at leastsix months including initial two months of rifampicin,isoniazide, pyrazinamide, ethambutol and next fourmonths of rifampicin and isoniazide18.
There is still contradiction in the treatment of abdominaltuberculosis about its duration of treatment. Most ofthe clinician and specialist are still continuing theprevious duration of treatment. There has been noattempt before to see the outcome of national guidelinebased treatment before.
So, this study was done in the department of Medicine,SSMC & Mitford Hospital to evaluate the treatmentoutcome of abdominal tuberculosis following nationalguide line.
Materials and Methods:This prospective study of descriptive nature was donebetween November 2009 to October 2010 in thedepartment of Medicine, Sir Salimullah Medical College,Mitford hospital, Dhaka, Bangladesh. Total 50 patientswere purposively selected, after screening andconsidering inclusion and exclusion criteria. All patientsaged more than 13 to 70 years, both male and female.and diagnosed as abdominal tuberculosis and gettinganti-TB drugs following National guide line wereincluded in the study. The patients, getting anti-TB-drugs on the basis of clinical suspicion (not confirmedcases), patients getting anti-TB drugs not followingnational guide line, patients getting other drugs whichreduce the effectiveness of anti-TB drugs and patient,
taking anti-TB drugs irregularly and not giving consentwere excluded from the study.
The detailed clinical history was obtained from patientadmitted with suspected abdominal tuberculosisattending in the department of medicine,gastroenterology and surgery of SSMC & MitfordHospital or other teaching hospitals in Dhaka city. Thesuspected case was sought and screened from focusedhistory and examination. In taking history certain pointswere undertaken as screening part. These are: 1) Historyof contact with TB. Patient, 2) History of smoking ornon smoking tobacco,3) History of alcohol intake 4)History of hypertension 5) History of diabetes mellitus6) Past history of tubercular iinfectiton and 7) Historyof relevant symptoms-
Abdominal pain, fever, weight loss, anorexia, diarrhea,constipation, nausea/vomiting, night sweating, melaena,haematochezia. Thorough physical examination was
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular DN Sarkar et al.
77

done in all cases, which includes especially for abdominalexamination –abdominal tenderness, ascites,hepatomegaly, splenomegaly, abdominal mass, intestinalobstruction, intestinal perforation, abdominallymhadenopathy. After screening procedure, 5 ml bloodwas taken from every patients and sent to SSMCpathological laboratory for total count (TC), differentialcount(DC) of white blood cell (WBC), ESR, Hb &peripheral blood film ( ESR > 50 mmHg was consideredas high ESR) , urine-routine microscopic examination,fasting Blood sugar, CXR PA view (evidence of activepulmonary tuberculosis was observed). Hundred andfifty ml ascitic fluid was drawn whenever patientpresented with this sign and sent for cytology(Lymphocyte predominance in a total cell countexcessive of 150 was searched), biochemistry ( proteinraised was searched) and bacteriology for AFB wassearched in every case. The standard laboratoryprocedure for ascetic fluid study was performed. Anultasonography of whole abdomen by an expert singlehanded radiologist was done in every case. Thosefulfilling criteria for other diagnosis from ultasonographywere excluded from the study.
Mantoux test (> 10 mm indurations was considered aspositive) was done in every case. In selected cases fewinvasive Investigation was done like Peritoneal fluidanalysis, Adenosine deaminase (ADA) for ascitic fluid(> 37 IU/L is diagnostic of abdominal TB), colonoscopyand biopsy (presence of granulation tissue withcaseation necrosis), CT-scan (if needed, laparoscopicbiopsy (Presence of granulation tissue with caseationnecrosis).The diagnosis of tuberculosis was confirmed byfulfilling one or more of the following four criteria alongwith high clinical index of suspicion —• Histological evidence of tubercle with caseation
necrosis.• Histological demonstration of acid fast bacilli in a
lesion.• Culture of suspected tissue resulting in growth of
M. tuberculosis.• Increased ADA (Adenosine deaminase) in ascitic
fluid (> 37IU/L)
Treatment:All diagnosed patient with abdominal TB were undertreatment of anti tubercular therapy (ATT) cat-1 for sixmonths as per national guide line in which rifampicin,INH, ethambutol and pyrazinamide were given in first
two months and after that rifampicin and INH for nextfour months according to index dose. But no one wasunder treatment by ATT cat-2.The isoniazid dose was 300 mg/day for those under 50kg in body weight and 400 mg/day for those 50 kg andover. The rifampin dose was 450 mg/day for patientsunder 50 kg and 600 mg/day for those 50 kg and above.The ethambutol (15 to 20 mg/kg of body weight) andpyrazinamide doses (20 to 30 mg/kg) were 1,000 mg/dayand 1,250 mg/day, respectively, for those under 50 kgand 1,200 mg/day and 1,500 mg/day for those 50 kg andover. All patients were advised to take medicine fromdirectly observed treatment (DOT) corner, nearby theirresidence.Follow-up: All enrolled patients were followed upfulfilling the criteria below:(1) Follow up was given two months after ATT and six
months completion of ATT.(2) Treatment oucome was assessed by comparing the
symptoms and signs, before starting ATT and aftersix months of ATT.
(3) TC, DC, ESR & Hb% of blood was done aftercompletion of ATT to compare with the same asdone before ATT for treatment outcomemeasurement
(4) Body weight before and after ATT was measuredin all cases.
Treatment outcome measurement:Treatment completed: After completing of full treatmentcourse, a patient is declared “treatment completed”
Cured: Completed six months treatment of ATT anddisappearance of all symptoms and signs and absenceof acid fast bacilli and caseation in lesion and normalADA in ascitic fluid. Improved: Completed six months treatment of ATT anddisappearance of all symptoms and signs.
Not improved: Persistent of symptoms and signs aftersix months ATT and presence of caseation necrosisafter six months ATT and presence of acid fast bacilli inlesion after six months ATT and Increased ADA inascitic fluid after six months ATT
Death: Patient who died for any reason during the courseof treatment
Data collection and statistical analysis: Statisticalanalysis related with this study was performed by use ofSPSS 16.0 package program ( SPSS -16 package Chicago
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
78

Illionois).The data gathered was expressed by descriptivestatistical methods ( frequency distribution, percentage,mean & standard deviation) as applicable. Comparisonbetween groups was done by standard statistical test,example: Student’s paired ‘t’ test. Result of this studywas shown by different tables, chart and diagram etc.
Ethical issue: The study protocol was approved by theInstitutional review board of SSMC, Dhaka. Informedconsent was obtained from each subject. In every stepsof methodology ethical consideration was followedstrictly (e.g- blood collection, biopsy, peritoneal fluidsaspiration, consent proceedings etc). Data was collectedin an approved data collection form.
Results:During the period of November 2009 to October 2010total 50 patients were selected as per inclusion andexclusion criteria for treatment outcome measurement.Out of 50 patients 45 patients completed total treatmentcourse of anti tubercular therapy (six months ) and 5patients died on the course of treatment and were notable to complete the treatment course
Table-1
Socio demographic status (n=50)
Parameters Patient Percentangenumber (%)
Age (years) Mean ± SD 33.2 ± 14.77Range 13-70
Sex Male 21 42Female 29 58M:F(Ratio) 0.72:1
Occupation House wife 22 44Student 6 12Service holder 7 14Business man 8 16cultivator 7 14
Marital status Married 38 76Unmarried 12 24
Total number of patient is 50 with a range of 13-70 yearsand mean ± SD =33.2 ± 14.77. 21 (42%) patients weremale, 29 (58%) patients were female and male & femaleratio is o.72 : 1.Out of total 50 patients 2(4%) patients had pasthistory of TB infection, 7(14%) had history of TBcontact, 8(16%) had history of smoking, 6(12%) hadhistory of tobacco chewing and 1(2%) had historyof alcohol intake.
Table-II
Type of clinically diagnosed abdominal TB (n=50)
Type Patient number Percentage (%)
Intestinal TB 17 34
Peritoneal TB 24 48Abdominal lymph node TB 2 4Others (Other abdominal organ 7 14TB or combination ofother types)
Table-III
Frequency of symptoms of patientsat presentation (n=50).
Symptoms Patient Percentagenumber (%)
Abdominal pain 47 94Fever 48 96Anorexia 47 94Diarrhoea 7 14Constipation 4 8Vomiting 41 82Night sweating 41 82Melaena 0 0Haematochezia 1 2
Among the total 50 patients 47(94%) patients presentedwith abdominal pain ,48(96%) with fever and 47 (94%)with anorexia.
Table-IV
Distribution of signs of patientsat presentation (n=50)
Signs Patient Percentagenumber (%)
Abdominal tenderness 45 90Ascites 29 58Hepatomegaly 4 8Splenomegaly 0 0Abdominal mass 20 40Intestinal obstruction 6 12Intestinal perforation 1 2Abdominal lymphadenopathy 1 2
Among the total 50 patients, abdominal tenderness wasrecorded on 45(90%), ascites on 29(58%) and Abdominalmass on 20(40%).
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular DN Sarkar et al.
79
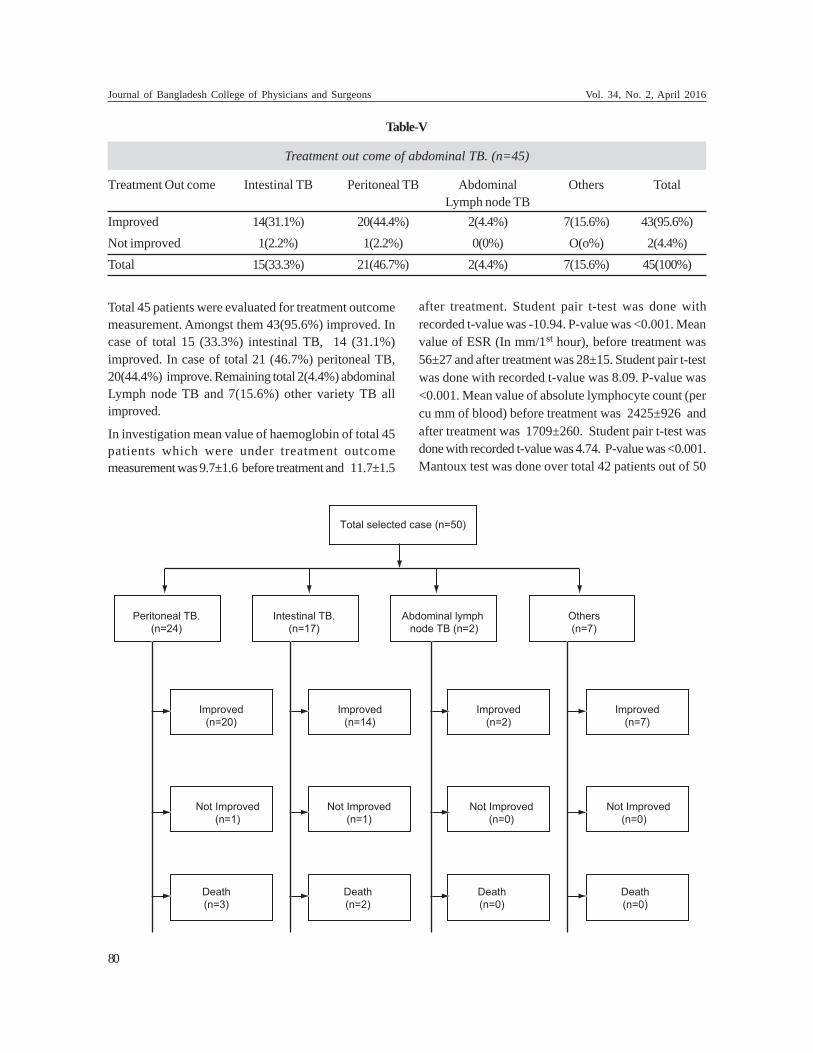
Total 45 patients were evaluated for treatment outcomemeasurement. Amongst them 43(95.6%) improved. Incase of total 15 (33.3%) intestinal TB, 14 (31.1%)improved. In case of total 21 (46.7%) peritoneal TB,20(44.4%) improve. Remaining total 2(4.4%) abdominalLymph node TB and 7(15.6%) other variety TB allimproved.
In investigation mean value of haemoglobin of total 45patients which were under treatment outcomemeasurement was 9.7±1.6 before treatment and 11.7±1.5
after treatment. Student pair t-test was done withrecorded t-value was -10.94. P-value was <0.001. Meanvalue of ESR (In mm/1st hour), before treatment was56±27 and after treatment was 28±15. Student pair t-testwas done with recorded t-value was 8.09. P-value was<0.001. Mean value of absolute lymphocyte count (percu mm of blood) before treatment was 2425±926 andafter treatment was 1709±260. Student pair t-test wasdone with recorded t-value was 4.74. P-value was <0.001.Mantoux test was done over total 42 patients out of 50
Table-V
Treatment out come of abdominal TB. (n=45)
Treatment Out come Intestinal TB Peritoneal TB Abdominal Others TotalLymph node TB
Improved 14(31.1%) 20(44.4%) 2(4.4%) 7(15.6%) 43(95.6%)Not improved 1(2.2%) 1(2.2%) 0(0%) O(o%) 2(4.4%)Total 15(33.3%) 21(46.7%) 2(4.4%) 7(15.6%) 45(100%)
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
80

patients. MT-positive 37(88%) and MT-Negative 5(11.9%). Out of 50 patients 24 (48%) were diagnosed onthe basis of increased ADA level (In ascitic fluid) and 26(52%) on the basis of Tissue biopsy (histopathology)along with high index of clinical suspicion.
Discussion:Abdominal tuberculosis can be presented in differentform and outcome can be also vary according to variablesite involvement. Although there may be many variableswhich can alter the outcome of disease (age,nutrition,demography etc) the ATT usually overcome all thevariables to have a better outlook of the disease if thetreatment taken through DOTS strategy18.
In this study out of total 50 patients 34% patients hadintestinal TB, 48% had Peritoneal TB, 14% had otherabdominal organ TB or combination of other types. Thisfinding is consistent with other studies whereperitoneum was the common site of involvement inabdominal tuberculosis.19.
Among the patients with intestinal involvement, ileo-cecal region were the common site in our series. It isconsistent with studies done by Palmar et al. andJakubosky et al.20 In contrast jejunum and ileum werethe predominant site of involvement according to otherstudies.12,21
Five patients died during the course of treatment of thisseries. One of the patient died within threee days ofATT and interestingly he had AFB positive in his asciticfluid. The other two patients who had raised ADA alsodied at one month in one case and other one at 2nd
months of treatment. The iliocaecal TB cases who diedwere also were within treatment schedule. One of thepatient died as a complication of intestinal obstructionand died after operation done in SSMCH for hisobstruction. The other case that died was havingadvanced disease with severe malnutrition.
The survivied 45 patients were evaluated for treatmentoutcome measurement. Amongst them 95.6% improvedand 4.4% had no improvement. In case of intestinal TB,93.3% had improved. In case of peritoneal TB, 95.6 %shown improvement. Remaining total two (4.4%)abdominal lymph node TB and 7 (15.6%) other varietyTB all improved. This study is consistent with anotherstudy where all tuberculosis patients improved with thesame regimen of 6-months duration22,23.
This study was undertaken to test whether a six monthregimen is effective in eliminating abdominal TB or not.To date, increasing evidence suggests that 6- to ninemonth regimens that include isoniazid and rifampin areindeed effective in this regard.24,25 However, fewproperly randomized trials of extrapulmonary diseasetreatment, featuring appropriate clinical end points, havebeen conducted, except for reports on tuberculouslymphadenitis (6–8) and spinal TB patients26,27,28
Two patients out of 45 did not improve. They hadpersistent previous symptoms and signs even treatmentcompleted. The cause of which may be non-compliancewith ATT , MDR-TB or HIV infection. It deserves furtherstudy whether extension of ATT duration required ornot. So they were referred to respective higher centre toexclude MDR-TB or concomitant HIV infection and forfurther management. These two patients were lost tofollow up and so the ultimate outcome could not bemeasured.
There are few studies in Bangladesh on clinical aspectsof abdominal tuberculosis. It was seen in this studythat highest number of cases were recorded in youngerage group. Abdominal tuberculosis can occur at anyage, but most commonly in young age. The mean age of33.2 years in the present study reflects the observationsof various studies.29,30 Age distribution of this studydoes not coincide with other studies.31,32 The meanage of presentation in their study was 6-11yrs. Becausetheir study was among the children. Male-female ratiowas 0.72:1. In another study, the disease was observedwith female predominance, which co-insides with thisstudy33. Moreover, in this study, age of the patientswas not in the same age group but it was also observedin the later part of second decade with a femalepreponderance and the numbers of female patients weremore than other series. Sheldon et al also observedsimilar age distribution in Bangladeshi migrants in EastLondon.34
Non-specific abdominal pain, low grade fever, anorexiaand night sweating are common symptom in this studywhich coincides with the studies of Tanrikulu AC etal.35, Demir k et al36, Talwar BS et al37. Though abdominaldistension, ascites and anorexia have also been reportedas the common presenting symptoms in somestudies.32,38 Present study revealed abdominaltenderness, ascites , abdominal mass as common sign
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular DN Sarkar et al.
81

while organomegaly and intestinal obstruction orperforation and abdominal lymphadenopathy were notvery common. This data is consistent with other studies.13,21,,39 These signs were not co-insides with the findingsof Bernhard JS et al7. Peripheral lymphadenopathy wasuncommon findings in patients with intestinal orperitoneal tuberculosis. It was not reported in the earlierstudies as well.39,.
Routine laboratory investigations although non-specificbut were helpful in this study to suspect the possibilitiesof abdominal tuberculosis. ESR was raised in all casesand mean value of ESR (In mm/1st hour), before treatmentwas 56 and after treatment was 28. Raised ESR has beenreported in 50-100% of patients in earlier studies.13,19,33
Total and differential count of WBC were non-specificin our series, other studies had similar findings. Butmean value of absolute lymphocyte count (per cu mmof blood) before treatment was 2425 and after treatmentwas 1709, which is consistent with earlier studies.13,19,33
In this study Mantoux test was done over total 42patients out of 50 patients. MT-positive was in 88%case. These findings are similar with the report of a 10-year review by Gilinsky NH et al.19 In other studies,tuberculin test was positive in 70-80% patients.13,21,39
Patents with abdominal tuberculosis may have anegative tuberculin test and a normal ESR.13,19,33,39 Onestudy has reported high ESR in 60% and positiveMantoux test in 24% of cases.41 In areas where TB ishighly endemic, positive Mantoux test neither confirmsnor excludes the diagnosis. 35,42,43 In this study, 48%were diagnosed on the basis of increased ADA level (inascitic fluid) and 52% were on the basis of tissue biopsy(histopathology) along with high index of clinicalsuspicion. In other studies ascitic fluid ADA has beenconsidered to be a useful screening test with ATB, whichare consistent with this study.44,45. Bacteriologicaldiagnosis by culture of AFB was not possible due tolack of facilities. Other studies have also faced similardifficulties in the microbiological confirmation of thedisease; most of them relied on histopathologicaldiagnosis. 13,46,47.
Previously there was longer duration of treatmentschedule of ATT in the treatment of abdominaltuberculosis. Now six months treatment of four drugsATT is recommended . But there is still contradictionamong the physicians. The evidence in this study notonly evaluate the national guideline but also shows its
effectiveness as 96% cases showed improvement in thisseries. A short course of ATT is justified for any form ofabdominal tuberculosis in Bangladesh. The strength ofthis study was 52 % had tissue diagnosis and 48% hadADA raised status which indicates its importance indiagnosing tuberculosis in extrapulmonary sites.
There was many limitations in this study. ADA was doneduring the time of diagnosis but ADA was not possibleto measure after completion of treatment during lastfollow up. It was due to non availability of ascetic fluidto perform ADA test. Some patients were diagnosedafter laparotomy and some were after colonoscopyfollowed by biopsy. But all of them did not agree to dothe same procedure after clinical improvement. So, ‘cure’was not possible to declare to that group of patients.Sampling was random and in an urban medical collegehospital. So that it may not be a representative ofcommunity or country. So, large scale study is requiredwhich should include private hospital and privatechambers of specialist doctors, which may give realreflection of the country. HIV screening and MDR-TBscreening were not done due to financial constrains.Culture of AFB was not done due to limited finance &availability.
Conclusion:Short course six months regimen was found to besufficient for treatment of abdominal TB, which wereintroduced by national guideline of tuberculosis control.Though there is much evidence of improvement ofabdominal TB by nine months treatment or twelvemonths treatment or more time consuming treatment,but improvement by minimum time duration is costeffective and beneficial to increased compliance.
Though there is negligible failure of the regimen it canbe concluded that six months regimen of ATT can berecommended for routine use of treatment of abdominalTB. Further large scale double blind trial to evaluatevalidation of this study is recommendation.
References:1. Fanning A. Tuberculosis: 6. Extrapulmonary disease. CMAJ
1999; 160 : 1597-603.
2. Iscman MD. Tuberculosis in relation to humanimmunodeficiency virus and acquired immunodeficiencysyndrome. In: Iseman MD, editor. A clinician’s guide totuberculosis. Philadelphia: Lippincott Williams andWilkins; 2000 p. 199-252.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
82

3. Dutt AK, Stead WW. Epidemiology. In: Schlossberg D,editor.Tuberculois and nontuberculous mycobacterialinfection. Philadelphia: W.B. Saunders Company; 1999p.3-16
4. Cartwell MF. Suider DEJ. Cauthen GM. Epidemiology ofTuberculosis in United States. 1985 through 1992. JAMA,1994;17;272(2):535-9
5. Rouf HMA. Intestinal tuberculosis in Bangladesh - study43 cases. Journal of Bangladesh College of Physicians andSurgeons. 1990; Vol 7, No.2: 38-44.
6. Faiz MA, Das KK, Khondaker AK, Tahir M.Extrapulmonary tuberculosis in Bangladesh - A Review of47 cases. Journal of Bangladesh College of Physiciansand Surgeons, 1990; Vol. 17, No.2:1-7.
7. Bernhard JS, Bhatia G, Knauer CM. GastrointestinalTuberculosis Jclin Gastrenterol 2001; 1 : 397-402
8. Hass WH. Mycobacterium tuberculosis. In: Mandell GL,Bennett JE, Dolin R, eds. Principles and Practice ofInfectious Diseases. Philadelphia: Churchill Livingstone,2000:2576±607.
9. Marshall JB. Tuberculosis of the Gastrointestinal tractand peritoneum. Am J Gastroenterol 1993; 88:989-99.
10. Anond BS, Nanda R, Sachdev GK. Response of tuberculosisstricture to antituberculous treatment. Gut 1988;29:62-9.
11. Findlay JM. Medical management of gastrointestinaltuberculosis. J R Soc Med 1982; 75:583-4.
12. Klimach OE, Prmerod LP. gastrointestinal tuberculosis.A retrospective review of 109 cases in a district of GeneralHospital. Q J Med 1985; 56:569-78.
13. Al-Quorain, et al. Abdominal tuberculosis in Saudi Arabia:A clinical pathological study of 65 cases. Am JGastroenterol 1993; 88:75-79.
14. Schofield PF. Abdominal tuberculosis. Gut 1985;1275-1278.
15. Channa GA. Abdominal Tuberculosis: continuation ofsurgical scourge. J CPSP 2008; 18:393-6.
16. Sharma MP, Bhatia V. Abdominal Tuberculosis. Indian Jof Med Res 2004; 120:305-15.
17. Balasurbramaniam R, Nagarajan M, Balambal R, TripathySP, Sundaraman R, Venkatesan P, et al. randomizedcontrolled clinical trial ofshort course chemotherapy inabdominal tuberculosis: a five year report. Int J TubercLung Dis 1997;1:44-51.
18. National Guidelines and Operational Manual forTuberculosis Control. 4th ed. National TuberculosisControl Programme. Directorate General of HeathServices, Dhaka, Bangladesh.
19. Gilinsky NH, Marks IN, Kottler RE, et al . Abdominaltuberculosis; A 10- year review. S Afr Med J 1983; 64:849-57.
20. Jakubowski A, Elwood RK, Enarso DA. Clinical featuresof abdominal tuberculosis. J Infect Dis 1988; 687-92.
21. Bhargava DK, Shrinwas, Chawla TC et al. Intestinaltuberculosis. Bactorological study of tissue obtained bycolonoscopy and during surgery. J Trop Med Hygiene1985; 88:249-52.
22. Sherman S, Rohweddr JJ, Ravikrishnan KP, et al.Tuberculous enterits and peritonitis: Report of 36 generalhospital cases. Arch Intern Med 1980; 140: 506-8.
23. Sang Hyoung Park, Suk-Kyun Yang,* Dong-Hoon Yang,Kyung Jo Kim, Soon Man Yoon, Jae Won Choe, ByongDuk Ye, Jeong-Sik Byeon, Seung-Jae Myung, and Jin-HoKim. Prospective Randomized Trial of Six-Month versusNine-Month Therapy for Intestinal Tuberculosis.Antimicrobial agents and chemotherapy,American Societyfor Microbiology Oct. 2009, Vol. 53, No. 10 : 4167–4171.
24. American Thoracic Society. 1992. Control of tuberculosisin the United States. Am. Rev. Respir. Dis. 146:1623–1633.
25. .Dutt, A. K., D. Moers, and W. W. Stead. 1986. Short-course chemotherapy for extrapulmonary tuberculosis.Nine years’ experience. Ann. Intern. Med. 104:7– 12.
26. Medical Research Council Working Party on Tuberculosisof the Spine. 1999. Five-year assessment of controlledtrials of short-course chemotherapy regimens of 6, 9 or18 months’ duration for spinal tuberculosis in patientsambulatory from the start or undergoing radical surgery.Fourteenth report of the Medical Research CouncilWorking Party on Tuberculosis of the Spine. Int. Orthop.23:73–81.
27. Medical Research Council Working Party on Tuberculosisof the Spine. 1993 Controlled trial of short-courseregimens of chemotherapy in the ambulatory treatmentof spinal tuberculosis. Results at three years of a study inKorea. Twelfth report of the Medical Research CouncilWorking Party on Tuberculosis of the Spine. J. BoneJoint Surg. Br. 75:240–248.
28. Parthasarathy, R., K. Sriram, T. Santha, R. Prabhakar, P. R.Somasundaram, and S. Sivasubramanian. 1999. Short-coursechemotherapy for tuberculosis of the spine. A comparisonbetween ambulant treatment and radical surgery—ten yearreport. J. Bone Joint Surg. Br. 81:464–471.
29. .Baloch NA, Anees S, Baber M, Maingal M et al. Abdominaltuberculosis, A review of 68 cases. J Surg Pak. 2002;7:12-4.
30. Channa GA, Khan MA. Abdominal tuberculosis: Surgeons’perspective J Surg Pak 2003; 8:18-22
31. Tzoanopoulos D, Mimidis K, Giaglis S, Ritis K, Kartalis G.The usefulness of PCR amplification of the IS6110insertion element of M. tuberculosis complex in asciticfluid of patients with peritoneal tuberculosis. Eur J InternMed 2003; 14:367-71.
Treatment Outcome in Patients of Abdominal Tuberculosis receiving Antitubercular DN Sarkar et al.
83

32. Gürkan F, Ozates M, Bosnak M, et al. Tuberculousperitonitis in 11 children: clinical features and diagnosticapproach. Pediatr Int 1999; 41:510-3.
33. Sing V, Jain AK, Agarwal AK, Gupta S, Khannas, WhonnaAK, Gupta J Clinicopathological profile of abdominaltuberculosis. BJCP 1985; 49; 1:22-24.
34. Sheldon CD, Probert CSJ, Cock H, King K, Rompton DS,Barnes NC, Mayberry JF. Incidence of abdominaltuberculosis in Bangladeshi migrants in East London.Tubercle and Lung disease 1993; 74:12-15
35. Tanrikulu AC, Aldemir M, Gurkan F, et al. Clinical reviewof tuberculous peritonitis in 39 patients in Diyarbakir,Turkey. J Gastroenterol Hepatol 2005; 20:906-9
36. Demir K, Okten A, Kaymakoglu S, et al. Tuberculousperitonitis— reports of 26 cases, detailing diagnostic andtherapeutic problems. Eur J Gastroenterol Hepatol2001;13:581-5.
37. Talwar BS, Talwar R, Chowdhary B, Prasad P. Abdominaltuberculosis in children: an Indian experience. J TropPediatr 2000; 46:368-70.
38. Chavalittamrong B, Talalak P. Tuberculous peritonitis inchildren.Prog Pediatr Surg 1982; 15:161-7
39. Manohar A, Simjee AE, Haffejee AA, et al. Symptomsand investigative findings in 145 patients with tuberculousperitonitis diagnosed by Peritoneoscopy and biopsy overa five year period. Gut 1990; 31: 1130-2.
40. Lingenfelser T, Zak J, Marks IN et al. Abdominaltuberculosis: still a potentially lethal disease. Am JGastroenterol 1993; 88:744-50.
41. Yilmaz T, Sever A, Gür S, Killi RM, Elmas N. CT findingsof abdominal tuberculosis in 12 patients. Comput MedImaging Graph 2002; 26:321-5.
42. Lin YS, Huang YC, Chang LY, Lin TY, Wong KS. Clinicalcharacteristics of tuberculosis in children in the north ofTaiwan. J Microbiol Immunol Infect 2005; 38:41-6.
43. Ibrahim M, Osoba AO. Abdominal tuberculosis. On-goingchallenge to gastroenterologists. Saudi Med J 2005;26:274-80.
44. Tzoanopoulos D, Mimidis K, Giaglis S, Ritis K, Kartalis G.The usefulness of PCR amplification of the IS6110insertion element of M. tuberculosis complex in asciticfluid of patients with peritoneal tuberculosis. Eur J InternMed 2003; 14:367-71.
45. Voigt MD, Kalvaria I, Trey C, et al. Diagnostic value ofascites adenosine deaminase in tuberculous peritonitis.Lancet 1989; 1:751- 4.
46. Pfaller MA. Application of new technology to the detection,identification, and antimicrobial susceptibility testing ofmycobacteria. Am J Clin Pathol 1994; 101:329-37.
47. Uygur-Bayramicli O, Dabak G, Dabak R. A clinical dilemma:abdomin tuberculosis. World J Gastroenterol 2003;9:1098-101.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
84

Journal of Bangladesh College of Physicians and SurgeonsVol. 34, No. 2, April 2016
Summary:Background:Intramuscular loading dose of MagnesiumSulphate could be a suitable alternative for communityintervention of the management of severe Pre- Eclampsiaand Eclampsia. Objective: To compare the efficacy of theloading total IM regime of injection Magnesium Sulphate(MgSO4) with the standard loading combined IV and IMregime for termination & prevention of recurrent convulsionsin the treatment of Eclampsia. Methods: Total 200 patientswere studied at Dhaka Medical College Hospital, Bangladeshfrom October 2012 to May 2013 where 100 patients were treatedwith loading IM regime (Case group) and 100 patients receivedstandard loading combined IV & IM regime (Control Group).The efficacy of both regimes was measured by the rate ofrecurrent convulsions. Results: No significant differenceswas observed in both groups in terms of age (23.03±3.90vs 23.34±4.63 years), parity (64% vs 63% primi),gestational age (36.39±3.64 vs 36.13±3.95 weeks),no of
convulsions (5.28±3.21 vs 5.35±3.31 times), mean diastolicblood pressure (98.74±17.22 vs 104.25±15.43 mmHg) andGlasgow Coma Scale (e”8, 96% vs<8, 92%). Nosignificant differences observed between the two groupsin mean convulsion to treatment interval (5.16±3.71 vs4.95±3.12 hr) and convulsion to delivery interval(13.26±8.8 vs 13.95±8.46 hr). The recurrent convulsionrate was almost same in both groups (3% vs 5%, ð2 =0.521, P> 0.05ns). Case fatality was 2% in case group and3% in control group (P > 0.05ns). Conclusions: Loadingtotal IM regime of MgSO4 is found as effective as the loadingcombined IV and IM regime in terms of control of convulsionsand prevention of recurrent fits in Eclampsia. So it could beused by the field level workers before referral.
Key words: Magnesium sulphate, Pre-Eclampsia, Eclampsiamanagement
(J Bangladesh Coll Phys Surg 2016; 34: 85-91)
Intramuscular Loading dose versus Combined Intravenous& Intramuscular Loading dose of Magnesium Sulphate in
the Management of Eclampsia in a TertiaryLevel Hospital of Bangladesh
S ROUFa, S AHMEDb, A AFRINc
a. Prof. Salma Rouf, Professor of Obs and Gynae, DhakaMedical College and Hospital
b. Dr. Shatil Ahmed, Indoor Medical Office, Department ofObs and Gynae, Dhaka Medical College and Hospital
c. Ms. Ashiana Afrin, Management Trainee, UniMed andUniHealth Ltd.
Address of Correspondence: Prof. Salma Rouf, Professor ofObs and Gynae, Dhaka Medical College and Hospital, E-mail:[email protected]: 11 October, 2014 Accepted: 23 October, 2015
Introduction:Maternal mortality is a great concern for a developingcountry like Bangladesh. Bangladesh has to reach MDG-5 by reducing the MMR to 1.47 / 1000 by 20151. The factis that the current MMR in Bangladesh is 1.94 / 1000live births as on 2010,2 is still one of the highest insouth Asia. Near about 12000 to 15000 women die everyyear from maternal health related complications.3
Severe Pre Eclampsia (PE) and Eclampsia (E) are seriousand relatively frequent complications of pregnancy and
is a major cause of poor pregnancy outcome, with ahigh maternal and perinatal mortality and severeobstetric morbidity in our country. Severe Pre-Eclampsia,often called a silent killer is characterized by high bloodpressure accompanied by a high level of protein in theurine but without attention often go undetected anduntreated and develops in to Eclampsia – the final andmost severe phase of PE causing seizures, coma andeven death of the mother and baby.
It is estimated that every year Eclampsia is associatedwith about 50,000 maternal deaths worldwide, predictablyagain most of which occur in the developing countries2. The current incidence of Eclampsia are 0.04% to 0.1%in the United states and United kingdom, on the contrarywith a much high rate in developing countries as greatas 15% in some parts of Asia, Africa and LatinAmerica.4Eclampsia is the second most important causeof maternal death in Bangladesh contributing 20% of all

maternal deaths due to obstetric complications2. Everyday four mothers die due to Eclampsia contributing to1500 maternal deaths / year.2In resource poor developingcountries the incidence of Eclampsia varies from 1 in100 to 1 in 1700.5
The BIRPERHT survey 6 of maternal morbidity showedthat national incidence of convulsion in pregnancy andpuerperium was 7.9% and over 100000 women developEclampsia each year in Bangladesh.7A number of studieshave shown that case fatality of Eclampsia was veryhigh in hospitals and is mainly due to delay in referraland management, long interval between onset ofconvulsion and reaching the hospitals.8
In many developing countries PE / Eclampsia is theleading cause of maternal mortality often claiming asmany women’s lives as Post Partum Hemorrhage (PPH),sometimes more. Unlike PPH prevention, managementof Eclampsia still did not get priority in public and privatehealth agenda due to lack of awareness and scarcity ofclear policy and guidelines at the national level.Till nowthe management of Eclampsia is solely institutional basedand there is no community level intervention. In theeffort to detect all the Pre-Eclampsia before it becomelife threatening one approach is to take testing forhypertension (measuring BP) and proteinurea (checkingurine for protein) in women in their homes rather thandepending entirely on them to reach facilities .
In Bangladesh 71% of total deliveries happen in homeby unskilled birth attendants and only 23% of womendeliver under medical supervision9 and the rest have noaccess to obstetric care.9 Only 23.4% women inBangladesh complete the recommended 4 ANC visits,48.9% have irregular ANC visits and 28.7% do not seekany ANC during their entire pregnancies.2So, there is alarge unmet need for early detection of PE / E and manymissed opportunities. According to nationaldemographic surveys (DHS) unmet need for checkingBP in pregnancy ranges from 13.9% in Indonesia to53.1% in Bangladesh.10As a result most Pre-Eclampsiaremaining unrecognized until severe complications suchas Eclampsia occur.
More over lack of availability of anticonvulsant drug-injection Magnesium Sulphate (MgSO4) at communityand rural level, cost of Inj. MgSO4, lack of training ofhealth care providers and supportive supervision alsoact as a barrier to ensure availability of Eclampsia
prevention and management services throughout thenation. That is why mortality associated with Pre-Eclampsia and Eclampsia shows little decline in morethan 75% in low resource countries like Bangladesh.10Itis the need of the time that a national guideline on usingMagnesium Sulphate putting a loading dose at thelowest level by the field level health workers- FWV/FWA (Family Welfare Visitor & Family WelfareAssistant) at home before transferring women to facilitiesis very much required and is equally important inmanagement perspective. If the patients could receiveloading dose at home, this will prevent convulsion insevere PE and subsequent recurrent fits in Eclampsiaduring transfer to facilities and thereby decreases thechance of development of seizure related complications-CVA, pulmonary oedema, unconsciousness, abruptionetc.
Among the many anti convulsants Inj. MagnesiumSulphate topped the list and is recommended asanticonvulsant of choice after the Eclampsia trial in199511.
There are 3 regimes of Magnesium Sulphate availablefor practicing. The popular one is combined IV and IMregime (Prichard) 12 which is being used in Bangladesh,Intravenous regime (Zuspanregime) 13 and Intramuscularregime 14. Intramuscular regime is not being practicedin our country.
In Bangladesh Magnesium Sulphate was firstintroduced in 199615 at Dhaka medical college hospital(DMCH) the largest tertiary Government teachinginstitute which has a separate Eclampsia ward with anaverage yearly admission of 700 – 800Eclampsiapatients.After the two published pilot studiesdone at the same institute, 15,16a guideline was publishedby the Eclampsia working group in January 1998 17 andMagnesium Sulphate has been used routinely from thebeginning of 1998, after the commencement of itsproduction locally . According to the published guidelinereduced dose schedule is recommended which is almosthalf of the dose described by the CollaborativeEclampsia trial.11As the weight of the averageBangladeshi young women is light, this curtail doseappears to control convulsions effectively. Even it wasfound in a randomized controlled trial that only the initialloading dose was sufficient to arrest convulsions andprevent subsequent recurrences.18
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
86

It is very difficult to train the field level workers tocalculate and prepare this IV and IM loading doses.Moreover they need to develop the skill of putting onIV cannulation. To remove the constrains of preparingand using IV and IM loading doses of MgSO4 at thecommunity and rural level (by the field workers), weplanned to conduct a case control study to compare theefficacy of loading IM regime and standard IV and IMregime of injection Magnesium Sulphate for Eclampsiato terminate convulsions and prevent its recurrence.
Methods:This case control Quasi experimental study wasconducted at the Eclampsia unit of Dhaka MedicalCollege Hospital (DMCH) from October 2012 to May2013. Dhaka Medical College hospital is one of the wellreputed tertiary care teaching and training institutelocated at the centre of the capital. It has got a separateEclampsia unit with round the clock emergency andintensive care facilities. The average yearly admissionof Eclampsia patient is 700-800. During the study perioda total of 200 patients were enrolled by purposivesampling.All the consecutive 100 antepartum andpostpartum Eclampsia patients admitted in unit IV(Researcher’s Unit) were taken as study population(Group A) and received 10gm IM loading dose of Inj.Magnesium Sulphate according to the followingprotocol.
All the consecutive 100 antepartum and postpartumEclampsia patients admitted in other units were takenas control group (group-B) and received 10 gm IV andIM loading dose (4 gm IV + 6 gm IM) of Inj. MagnesiumSulphate according to the following protocol.
Patients of both groups received an additional dose of2.5 gm MgSo4 IV in diluted form if there was convulsionafter ½ an hour of loading dose which was consideredas recurrent convulsion and put on maintenance therapyfor 24 hours. The schedule of maintenance therapy was2.5 gm IM in alternate buttock at 4 hourly interval.Besides anticonvulsants patients of both groups weremanaged by the same protocol of Eclampsia managementprepared by Eclampsia working group of Bangladesh.17
The efficacy of both regimes was measured by the rateof recurrent convulsions.
Patients who received any anticonvulsants before handfrom out-side were excluded from the study. The studywas approved by departmental review board and ethicalclearance was taken from the institutional ethicalcommittee.
Results were expressed as incidence, mean ± SD andproportion. Comparison between two groups was madewith x2 analysis, t test as appropriate. P values of < 0.05was considered significant.
Fig.-1: Group A (study cases) Inj. MgS04IM regime
Fig.-2: Group B (Control cases) Inj. MgSO4 IV and IM regime
Intramuscular Loading dose versus Combined Intravenous & Intramuscular S Rouf et al.
87

Results:The study was conducted to compare the efficacy ofthe loading total IM regime of Injection MagnesiumSulphate with the standard loading combined IV andIM regime for termination of convulsion and preventionof its recurrence in the treatment of Eclampsia. A total of200 patients were studied out of which 100 patients hadreceived the loading total IM regime (Group-A or cases)and 100 patients were treated with the standard loadingcombined IV and IM regime (Group-B or controls). Socio-demographic characteristics of the patients, patients’profile, severity of the disease, patients’ outcome andpregnancy outcome (both maternal and foetal) afterrecieving the loading dose of Magnesium Sulphate ofboth case and control groups were recorded. After datacollection, processing and analysis, the followingobservations were obtained:
Table 1 described the characteristics of the patients andseverity of the disease.In both the groups patients’profiles were almost the same. The average age of thecase group was 23.03 ± 3.90 years and the control groupwas 23.34 ± 4.63 years. Most of the parameters whichindicate severity of the disease on admissionrevealedno significant differences. The mean number of
convulsions before admission was 5.28 ± 3.21 and 5.35± 3.31 among the case and control groups respectivelyand other parameters like mean diastolic blood pressure(98.74±17.22 vs 104.25±15.43 mm.Hg) and Glasgow ComaScale (e”8, 96% vs<8, 92%) were almost the same.
No significant difference was observed in convulsionto treatment and convulsions to delivery intervalsbetween the two groups (Table 2). The mean convulsionto treatment interval was 5.16 ± 3.71 hr in case groupand 4.95 ± 3.12 hr in the control group. The meanconvulsion to delivery interval was 13.26 ± 8.80 hr and13.95 ± 8.46 hr respectively in the case and controlgroups. The recurrent convulsion rate was 3% in casegroup and 5% in the control group without anysignificant difference being observed (ð2 =0.521significance 0.718). Table.3 showed the maternaland foetal outcome and the maternal death rate was 2%in the case group and 3% in the control group (P> 0.05ns).
Table 3 also described the maternal outcome in relationto mode of delivery and faetal outcome. The rate ofvaginal delivery (55% vs 53%), cesarean delivery (32%vs 42%), live birth (77% and 79%) and still birth (2% vs21%) were found consistent among the two groups.
Table-I
Patients’ characteristics
Regime IM RegimeIV & IM(n = 100) (n = 100)
Parametre Percentage/ Mean ± SD Percentage/ Mean±SD SignificanceAge ( in years) 23.03 ± 3.90 23.34 ± 4.63 P > 0.05ns
Parity 0 64 631-5 36 37 P > 0.05ns
Type of eclampsia Antepartum & 71 86 P < 0.05*
IntrapartumPostpartum 29 14
Gestational age (in weeks) 36.39 ± 3.64 36.13 ± 3.95 P > 0.05ns
No. of convulsions before hospitalization 5.28±3.21 5.35±3.31 P > 0.05ns
^DBP ( in mm of Hg) 98.74 ±17.22 104.25 ± 15.43 P < 0.05*Edema Nil 29 12 P < .01**
Present 71 88Albuminuria Nil 14 9 P > 0.05ns
Present 86 91#GCS >8 96 92 P < 0.05*
<8 4 8
*/**: Significant ^DBP :Diastolic Blood Pressurens : Not significant #GCS :Glasgow Coma ScaleSD : Standard deviation
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
88
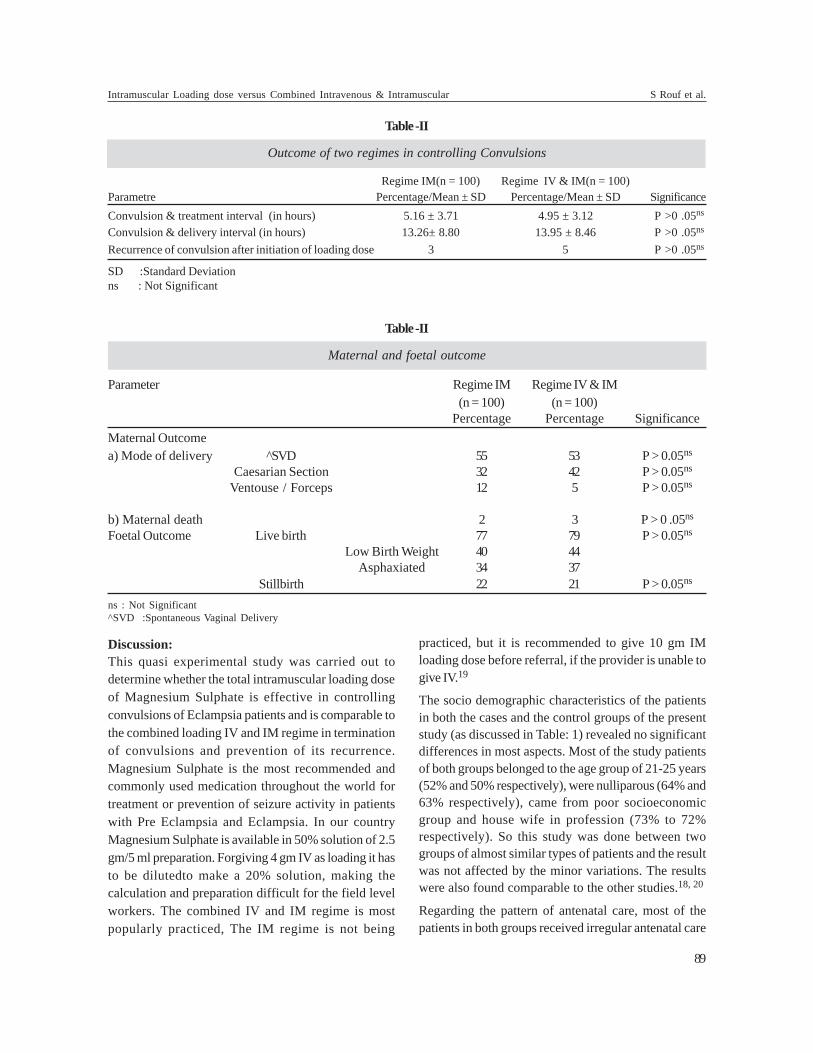
Discussion:This quasi experimental study was carried out todetermine whether the total intramuscular loading doseof Magnesium Sulphate is effective in controllingconvulsions of Eclampsia patients and is comparable tothe combined loading IV and IM regime in terminationof convulsions and prevention of its recurrence.Magnesium Sulphate is the most recommended andcommonly used medication throughout the world fortreatment or prevention of seizure activity in patientswith Pre Eclampsia and Eclampsia. In our countryMagnesium Sulphate is available in 50% solution of 2.5gm/5 ml preparation. Forgiving 4 gm IV as loading it hasto be dilutedto make a 20% solution, making thecalculation and preparation difficult for the field levelworkers. The combined IV and IM regime is mostpopularly practiced, The IM regime is not being
practiced, but it is recommended to give 10 gm IMloading dose before referral, if the provider is unable togive IV.19
The socio demographic characteristics of the patientsin both the cases and the control groups of the presentstudy (as discussed in Table: 1) revealed no significantdifferences in most aspects. Most of the study patientsof both groups belonged to the age group of 21-25 years(52% and 50% respectively), were nulliparous (64% and63% respectively), came from poor socioeconomicgroup and house wife in profession (73% to 72%respectively). So this study was done between twogroups of almost similar types of patients and the resultwas not affected by the minor variations. The resultswere also found comparable to the other studies.18, 20
Regarding the pattern of antenatal care, most of thepatients in both groups received irregular antenatal care
Table -II
Outcome of two regimes in controlling Convulsions
Regime IM(n = 100) Regime IV & IM(n = 100)Parametre Percentage/Mean ± SD Percentage/Mean ± SD SignificanceConvulsion & treatment interval (in hours) 5.16 ± 3.71 4.95 ± 3.12 P >0 .05ns
Convulsion & delivery interval (in hours) 13.26± 8.80 13.95 ± 8.46 P >0 .05ns
Recurrence of convulsion after initiation of loading dose 3 5 P >0 .05ns
SD :Standard Deviationns : Not Significant
Table -II
Maternal and foetal outcome
Parameter Regime IM Regime IV & IM(n = 100) (n = 100)
Percentage Percentage SignificanceMaternal Outcomea) Mode of delivery ^SVD 55 53 P > 0.05ns
Caesarian Section 32 42 P > 0.05ns
Ventouse / Forceps 12 5 P > 0.05ns
b) Maternal death 2 3 P > 0 .05ns
Foetal Outcome Live birth 77 79 P > 0.05ns
Low Birth Weight 40 44Asphaxiated 34 37
Stillbirth 22 21 P > 0.05ns
ns : Not Significant^SVD :Spontaneous Vaginal Delivery
Intramuscular Loading dose versus Combined Intravenous & Intramuscular S Rouf et al.
89

(49% and 37% respectively) and a significant proportionhad none (23% and 24%). This is consistent with thenational findings which states that 28.7% women ofBangladesh do not seek any ANC, 26% complete atleast 4 ANC visits and the rest 45% of women haveirregular ANC visits.9
The distribution of pattern of referral and the personnelwho referred the patients to DMCH showed thatmajority of the patients came directly from home in bothgroups (49% and 35 % respectively), whereas quite alarge number were also referred from district hospitalsand private clinics (41% and 46% respectively) and asignificant number were attended by doctors beforebeing referred to DMCH (41% and 57%). This is muchhigher than the national findings which states that only23% of births are attended by medical personnels.9Thiscould be explained by the fact that DMCH is the largest,most renowned and the most easily accessible tertiarylevel government institute of the country. So it receivescomplicated cases from all over the countries, usuallyreferred by doctors. So training of the field level workers(like SBA, FWV and nurses) is urgently needed for earlydetection of PE/E cases at home as well as offeringloading dose of MgSO4 in convulsive women or severePE cases at home or at lower facilities before transferring.
Table 1 also describes the parameters which indicateseverity of the disease and has shown very subtle andnegligible differences between the cases and the controlgroups. The mean number of convulsion beforeadmission was 5.28 ± 3.21 in the case and 5.35 ± 3.31 inthe control group. These findings were also foundconsistent with other studies.18, 20
Table 2 shows the outcome of patients after receivingthe loading dose in terms of recurrence of convulsions.The mean (± SD) time required to initiate treatment inthe cases and control groups were 5.55 ±5.07 and 4.95±3.12 hours and to deliver after the onset of convulsionswas 13.26±8.80 and 13.95±8.46 hours respectivelybetween the two groups without any significantdifference. In another prospective study carried out atDMCH, no significant difference was observed amongthe groups (group 1 only loading dose n = 202 andgroup 2 standard regime n = 199) in mean fit andtreatment interval ( 6.88 ±5.26 vs 7.12 ± 4.29 hr) and fitand delivery interval (11.35 ± 10.22 vs 11± 6.69 hr)18. Sothe present study findings were consistent andcomparable with the previous study findings.
Regarding the recurrence of convulsions after receivingthe loading dose, 3 patients of cases group (3%) and 5patients of control group (5%) developed recurrentconvulsions after initiation of the loading dose. Thedifference is not found statistically significant. Moreoverrecurrent convulsion rate was also found similar to thestudy done for comparing the efficacy of loading doseversus standard regime of Magnesium Sulphate18. Sothe loading total intramuscular regime appears to beequally effective like the loading combined IV and IMregime in preventing recurrence of convulsions in thetreatment of Eclampsia.
Table 3 shows the case fatality and 2 patients of casegroup (2%) and 3 patients of control group (3%) diedand among the 2 patients of case group 1 patient diedundelivered. The case fatality rate was also comparableto the previous prospective comparativestudy18. As thedifference is not statistically significant, the loading totalintramuscular regime appears to be equally effectivelike the loading combined IV and IM regime in preventingmaternal deaths in Eclampsia.
Regarding the maternal outcome in relation to mode ofdelivery and foetal outcome (live births and still births)in both ‘cases’ and ‘control’ groups of the present studyobserved no significant differences (Table.3).
From these above perspective it can be inferred that theloading total intramuscular regime is found as effectiveas the loading combined IV and IM regime in terms ofcontrol of convulsions and prevention of recurrenceand seems to be at least equally effective in terms ofmanaging pregnancy outcome and preventing casefatality if not better than IV and IM combined regime.
The strength of the study is that, this is the first studyin Bangladesh which has been carried out to evaluatewhether total intramuscular loading dose of MagnesiumSulphate is effective in controlling convulsions andprevention of its recurrence and is comparable tocombined IV and IM regime. Though IV dose iscomfortable for the patients and has immediate action,IM dose will be easy to administer for health workers ofgrassroot level.
Study shows that severe PE/E patients who receivedthe loading doses before referral had reduced numberof convulsions, more effective control of convulsions,shorter time to regain full consciousness, reducedmaternal mortality and still birth rates21. So it is
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
90

recommended to use loading doses at peripheral facilitiesand homebirths19, 21.Considering theclinicaleffectiveness demonstrated by the present study, easeof administration, ease of monitoring, easier availabilityand cost effectiveness, the loading total IM regime ofMagnesium Sulphate appears to be equally preferablespecially for the root level workers who will attend theEclampsia patients or severe PE at home and can offerthis treatment before referral. This will prevent furtherrecurrence in Eclampsia and prevent development offits in severe PE and thereby greatly improves theoutcome by reducing convulsion treatment intervalandpreventing seizure related complications. On thebasis of the findings, integrated with the understandingfrom available literature, it will be recommended that anational guideline will be constructed for putting aloading total IM dose of Magnesium Sulphate at thelowest level by the field level workers before referral.
References:1. Millennium Development Goals Midterm Bangladesh
Progress Report 2007. Planning Commission GOB
2. Bangladesh Maternal Mortality and Health care survey2010.
3. Millennium Development Goals Bangladesh ProgressReport 2008. Planning Commission GOB
4. Regmi MC, Aggarwal A, Pradhan T, Rijal P, Subedi A andDuprety. Loading dose versus Standard regimen ofMagnesium Sulphate in Eclampsia – a randomized trial.Nepal Med Coll J 2010; 12 (4): 244 — 247
5. Crowther CA. Eclampsia at Harare maternity hospital,an epidemiological study. S Aft. Med j 1985; 68: 927 –929.[PubMed : 4081926]
6. The Bangladesh Institute of Research for promotion ofEssential and Reproductive Health and Technologies (BIRPERHT ). Proceedings of Dessiminassion workshopon maternal morbidity study. Hotel Sheraton, Dhaka,1994.
7. Yasmin HA, Rahman MH, Chowdhury FK et al. Baselinesurvey for assessment of Emergency obstetric care servicesin Bangladesh. BIRPERHT, March 1995 ; 10
8. Begum K, Hossain F. A study of 447 cases of eclampsiaadmitted in Dhaka Medical college Hospital. XV AsianOceanic Cong obstetric gynaecol 1995 : 169 – 73
9. Bangladesh health and Demographic Survey 2011
10. Intervention for impact in essential obstetric and Newborncare. African Regional Meeting Report. 21 – 25 Feb.2011,Addis Abasa Ethiopia.
11. The Eclampsia Trial Collaborative group-Which anticonvulsant for women with eclampsia? Evidence fromthe collaborative Eclampsia trial. Lancet 1995 : 345 ;1455 – 1463
12. Pritchard JA, Cunningham FG, Pritchard SA. The ParklandMemorial Hospital protocol for treatment of Eclampsia:Evaluation of 245 cases. Am J ObstetGynecol 1984; 148:951-963.
13. Zuspan FP. Treatment of severe Pre Eclamsia andEclampsia, ClinObstetGynecol 1996; 9: 945- 971.
14. Royal College of Obstetricians &Gynaecologists. LifeSaving Skills Manual. Essential Obstetrics and NewbornCare, Leverpool School of Tropical Medicine, WorldHealth Organization, LATH 2007;22(ISBN 978-19047552-28-8)
15. Rouf S, Shamsuddin L. Khan JH. Magnesium Sulphateversus Diazepum in the management of eclampsia.Bangladesh J Obstet&gynaecol 1996 ;Vol 11,1 : 1-14
16. L. Shamsuddin, S. Rouf. JH khan et al. Magnesium Sulphateversus Diazepam in the management of eclampsia.Bangladesh Medical Research Council Bulletin Aug 1998;Vol 24, 2: 43-8.
17. Eclampsia working group. Eclampsia in Bangladesh. Areview and guideline Bangladesh J obstetriesGynaecology1997, 12 No:1: 1- 27.
18. Begum M R, Begum A, Quadir E. Loading dose versusstandard regime of Magnesium Sulphate in the managementof Eclampsia ; A randomized trial . J. Obstet.Gynacol.Research June 2002; Vol. 28, No.3; 154-159.
19. WHO, UNFPA, UNICEF, The World Bank Group;Integrated Management of Pregnancy, Child birth,Postpartum and New born Care: A Guide for EssentialPractices. WHO, Geneva 2006, 2nd edition ( WQ 175)
20. Sultana N, Begum A, Begum K: Single loading dose ofMagnesium Sulphate for control of Convulsion inEclampsia. Journal of Bangladesh College of Physiciansand Surgeons. May 2003, Vol 21, No-2, P 63-68
21. Begum MR, Begum A,Quadir E, Akhter S, L.Shamsuddin:Eclampsia: Still a Problem in Bangladesh. MedGenMed.MedScape General Medicine2004; 6(4):52. file:///L: /Journal SR.
Intramuscular Loading dose versus Combined Intravenous & Intramuscular S Rouf et al.
91

Summary:Objective: To evaluate role of probiotics in human physiology,metabolism, health, immunity and GI disorders.It is importantfor gastroenterologists to improve their understanding of themechanisms of probiotics and the evidence that support theiruse in clinical practice.
Data Sources: A medline search (1948-December 2014) wasconducted using GI diseases and probiotics as terms foridentifying pertinent studies. Search limits includedEnglish language. Additional information was obtainedfrom bibliographies.
Data Selection And Data Extraction: The informationprovided is based on review of primary literature fromrandomized controlled trials (RCTs), meta-analyses, expertconsensus panel recommendations and society-based practicerecommendations. References are provided for more readingand figure summarizes key information about theirmechanism of action.
Data Synthesis: The need for objective, evidence-basedguidance on the role of probiotics is becoming increasingly
important as public awareness grows. This consensus isintended as a practical reference to help physicians makeappropriate, evidence-based recommendations to patientswho might benefit from probiotic treatment. Overall, therandomised, placebo-controlled trials included in thisarticle support, with a high evidence level, the therapeuticeffects of probiotic agents for several disorders includingantibiotic or Clostridium difficile-associated diarrhea,irritable bowel syndrome, and the inflammatory boweldiseases. Although probiotic research is a rapidly evolvingfield, there are sufficient data to justify a trial of probioticsfor treatment or prevention of some of these conditions.However, the capacity of probiotics to modify diseasesymptoms is likely to be modest and varies among probioticstrains and not all probiotics are right for all diseases. Thegoal of this review is to provide clinicians with an overviewof the rationale and data which support or refute the role ofprobiotics for treating commonly encounteredgastrointestinal disorders.
(J Bangladesh Coll Phys Surg 2016; 34: 92-99)
Proboitics and their Role in GI DiseasesS PERVEENa, MA AHMEDb
REVIEW ARTICLES
a. Colonel (Dr) Shaila Perveen, Classified Medical Specialistand Gastroenterologist, CMH Jessore.
b. Dr. Colonel Mir Azimuddin Ahmed, Classified MedicalSpecialist and Gastroenterologist, CMH Jessore
Address of Correspondence: Colonel (Dr) Shaila Perveen,Classified Medical Specialist and Gastroenterologist, CMH Jessore.
Received: 22 March, 2015 Accepted: 30 March, 2016
Introduction:Our gut is home to an estimated 100 trillionmicroorganisms representing more than1000 differentbacterial species, 400 of which are estimated to be ofprobiotic species1.There is growing recognition of therole of diet and other environmental factors inmodulating the composition and metabolic activity ofthe human gut microbiota, which in turn can impacthealth.Up to 10% of an individual’s daily energy needscan be derived from the by products of bacterialfermentation. Gastrointestinal microbiota are also criticalfor normal immune system development.2 Intestinal
bacteria weigh up to 1 kg and bacterial cells outnumberhuman cells by 10:1. The bacterial genome or DNA mayoutnumber the human genome by 100:1.The physiologicimpact mediated by these resident microbes is importantenough to be labeled as “other organ” or “ hiddenmetabolic organ”
Probioticsare defined as ‘live microorganisms’ whichwhen administered in adequate amounts confer a healthbenefit on the host’.3 There is plentiful evidence thatprobiotics( pro and biota meaning ‘for life’ ) impact themicrobiome and benefit human health4. Probiotics aredistinct from prebiotics (dietary substances such asindigestible oligosaccharides including bananas,whole grains, honey, garlic and onions) that provide ahealth benefit by selectively promoting the growth ofbeneficial bacteria in the gut and synbiotics (productscontaining a synergistic combination of prebiotics andprobiotics ).
Although research on the microbiome is emerging,scientists have already made tremendous progress in

understanding the microbial makeupand associatingmicrobiome diversity with human physiology,health anddisease. It is likely that much of this impact is mediatedthrough diet. What we eat and drink influences themicrobiome and the microbiome in turn converts dietarycontent into biological signals providing enzymaticmachinery thus influencing what the human host is ableto extract from its diet including energy.5
Probiotics and the Immune SystemHumans and their trillions of intestinal microorganismscoevolve to form a largely beneficial symbiosis. Humangut microbiome is acquired during the last trimester ofpregnancy6. Unlike the human genome, the humanmicrobiome is acquired . Vaginally born babies acquiredifferent microbiomes than babies born by cesareansection7. Gastrointestinal microbiota are critical fornormal immune system development8. The intestinalmucosa comprising the largest surface area of the body,is constantly exposed to a vast array of microbes, foodantigens, and toxins. The intestinal epithelium must‘tolerate’ the commensal flora that maintain mucosalhomeostasis by controlling inflammatory responses aswell as sensing danger signals of potentially harmfulpathogens.
Probiotics can down regulate the effects of luminalbacteria in initiating and sustaining an intestinalinflammatory response particularly important inulcerative colitis. It is becoming increasingly clear thatthe intestinal microbiota composition, the intestinalbarrier and the mucosal immune system plays pivotalroles in the development of a variety of allergic andautoimmune diseases.
Types of ProbioticsMost of the probiotics are bacteria, some arefungus(yeast) and some contain mixture.Lactobacillusacidophilus is the “friendly” bacteria and mostcommonly used probiotic. Such healthy bacteria inhabitthe intestines and protect against the entrance andproliferation of pathogens. Since the mid 1990s, clinicalstudies have established that probiotic therapy can helptreat several gastrointestinal illnesses.9
Lactobacillus acidophilus, Lactobacillus casei bothconvert lactose into lactic acid helping in lactoseintolerance. Lactobacillus bulgaricus(discovered byBulgarian doctor) can be found inmany yogurts andsoft cheese.Itis helpful for those who are lactoseintolerant L. Acidophilus may also be helpful in reducingcholesterol levels.Lactobacillus rhamnosus GG means
the genus is Lactobacillus, the species is rhamnosusand the strain is GG.10
Bifidobacteria is a family of bacteria that has beenstudied for its ability to prevent and treat variousgastrointestinal disorders, including infections, irritablebowel syndrome and constipation. In addition to makinglactic acid, it also makes some important short-chainfatty acids that are then absorbed and metabolized bythe body. Certain bifidobacteria may actually protectthe host from carcinogenic activity of other intestinalflora.Saccharomyces boulardii is the only yeast probiotic.Some studies have shown that it is effective in preventingand treating diarrhea associated with the use ofantibiotics and to reduce side effects of H. pyloritherapy, traveler’s diarrhea,Crohn’s disease.Probiotic mixture (VSL#3 )consisting of 8 strains oflive freeze-dried lactic acid bacteria. Each sachet contains450 billion live probiotic bacteria .Streptococcusthermophilus, Bifidobacterium breve, B longum, Binfanti, Lactobacillus acidophilus, L plantarum, Lparacasei, L bulgaricus.11
Probiotic therapy may also help people with Crohn’sdisease and irritable bowel syndrome. Clinical trial resultsare mixed, but several small studies suggest that certainprobiotics may help maintain remission of ulcerativecolitis and prevent relapse of Crohn’s disease and therecurrence of pouchitis (a complication after surgeryfor ulcerative colitis). Because these disorders are sofrustrating to treat, many people are giving probiotics atry even before all the evidence is in for the particularstrains. More research is needed to find out which strainswork best for what conditions.
Mechanism of Action of ProbioticsProbiotics work by several different mechanisms. Thesecommensal microorganisms contribute energy andcellular precursors in the form of short-chain fatty acids,prevent infections and modulate and train the hostimmune system.12 They act as a barrier by lining theintestinal tract close to the brush border. Throughcompetitive inhibition, they prevent other luminalbacteria stimulating the mucosal immune system. Theyenhance mucus production so that patients will have athicker mucus layer, which protects against invasivebacteria. Probiotics influence the mucosal immunesystem to secrete protective immunoglobulins (Ig) suchas secretory IgA and protective defensins andbacteriocins into the lumen (Fig I). Finally, probioticsalter the function of the mucosal immune system to make
Proboitics and their Role in GI Diseases S Perveen & MA Ahmed
93

dendritic cells more anti-inflammatory and less pro-inflammatory so that they are slightly less responsiveand less reactive to luminal bacteria in initiating andsustaining an intestinal inflammatory response whichis particularly important in ulcerative colitis.13
Indications of ProbioticsAltough still being studied, probiotics may help severalspecific illnesses. In 2011, experts at Yale Universityreviewed the research studies. They concluded thatprobiotics are best case in the treatment of diarrhea.Controlled trials have shown that Lactobacillus GGcan shorten the course of infectious diarrhea in infantsand children (but not adults). Although studies arelimited and data are inconsistent, two large reviews,taken together, suggest that probiotics reduce antibiotic-associated diarrhea by 60% when compared with a
placebo. Probiotics can improve intestinal function andmaintain the integrity of the intestinallining and helpfight bacteria that cause diarrhea. In childhooddiarrheain the pediatric population, rotavirus has beenthe most common cause of infectious diarrhea. Datasuggests that the benefit of probiotics in preventingacute infectious diarrhea is modest.14
In treating necrotizing enterocolitis, a type of infectionand inflammation mostly seen in infants Lactobacillusrhamnosus GG (LGG) is the most effective probioticreported to date, reducing both severity and durationof diarrhea by ~1 day.15 The American Academy ofPediatrics supports the recommendation of LGG earlyin the course of acute infectious diarrhea to reducesymptom duration.
Fig.-1: Diagrammatic representation of mechanism of action of Proboitics
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
94

For antibiotic associated diarrhea incuding thosereceiving Helicobacter pylori eradication therapy andviral gastroenteritis supporting data are strong forprobiotics (L. rhamnosusGG, Saccharomycesboulardii)are among the few treatment modalitiesavailable. However, the duration of symptoms in theseconditions is typically short regardless of probiotic use.Patients given the higher dose of probiotic concurrentwith antibiotics ( for 5 days afterward) had feweroccurrences of AAD (15.5 vs. 44.1%).As a secondaryendpoint these studies also showed a reduction indevelopment of C. difficile-associated diarrhea16.
Diarrhea caused by C. difficile bacteria is a commonnosocomial and community-based medical condition.C difficile sickens half a million Americans and killsmore than approximately 14,000 people a year in theUnited States.17 Antibiotic therapy with metronidazole,oral vancomycin and now fidaxomicin makeup thecurrent treatment regimen but recurrence remains aclinical problem.
Recently, In patients with recurrent CDAD the fecalcommunities were highly variable in bacterialcomposition and were characterized by markedlydecreased diversity. Preservation and restoration of themicrobial diversity could represent novel strategies forprevention and treatment of recurrent CDAD.18
Fecal microbiota transplants (FMTs), also known asstool transplants from healthy donors have emerged asan effective means of stopping infections and succeededin 91% of patients with recurrent CDI.Patients whounderwent colonoscopic FMT found it so effective thatmore than half (53%) said that a fecal microbiotatransplant would be their top choice if they contractedCDI again.19,20
Typically, patients receive the fecal transplants byenema, colonoscopy or a nasal tube.As a potentiallyless costly and less invasive alternative, researchersmade fecal pill.Dr. Louie first created a fecal transplantpill when a C difficile infection persisted in one patientwho could not tolerate a nasal tube.[21]Currently, it isapproved only for recurrent C difficile infections,
After the patients ingested the capsules, the researchersfound significantly increased numbers of Bacteroides,C coccoides, C leptum, Prevotella, Bifidobacteria,andDesulfovibrio and significantly decreased numbersofEnterobacteriaceaeandVeillonella. They found noC difficile in the intestines.
Symptoms of irritable bowel syndrome (IBS) and otherfunctional GI disorders (FGID) frustrate people withoverlapping symptoms and exhaust them with prolongedconventional medications having considerable adverseeffects.22 They can be treated with foods andsupplements containing probiotics.
The first practical consensus on the role of probioticsin the management of GI symptoms in adultsrecommendspecific probiotics in the management of some IBSsymptoms and can also be used as an adjunct toconventional treatment.23 For overall symptoms andabdominal pain in IBS, probiotics(BifidobacteriumbifidumMIMBb75,Escherichia coliDSM17252) hasstrong supportive evidence for benefit and should betried.In overall symptoms in IBS-D(B. longum subsp.infantis 35624), improving the frequency and/orconsistency of bowel movements and bloating/distension (B. animalis subsp. lactis DN-173 010 -Activia) probiotics could be tried.In overall symptomsin IBS-C(B. animalis -Activia) probiotics may beconsidered.Flatus in IBS has currently no evidence tosupport use of probiotics. No probiotic alleviates thefull range of symptoms in IBS.24 Though it has shownimprovement in some aspects of health-related qualityof lifethere is need for more research.This consensuspublication with new research and input from patientgroups is intended to be updated in 3 years.
The need for objective, evidence-based guidance onthe role of probiotics is becoming increasingly importantas public awareness for probiotics grows. Thisconsensus is intended as a practical reference to helpphysicians make appropriate, evidence-basedrecommendations to patients who might benefit fromprobiotic treatment. Overall, the randomised, placebo-controlled trials included with a high evidence level, arole for specific probiotics in the management of overallsymptoms and abdominal pain in patients with IBS.Preventing or reducing diarrhoea in patients receivingantibiotics or H. pylori eradication triple therapy. Thetrials support, with a moderate evidence level, a role forspecific probiotics in managing overall symptoms inpatients with IBS-D; improving bowel movements andbloating/distension in patients with IBS; and improvingsome aspects of health-related quality of life.25
The lack of consensus on the role of probiotics in themanagement of constipation is consistent with theWorld Gastroenterology Organisation guideline on
Proboitics and their Role in GI Diseases S Perveen & MA Ahmed
95

prebiotics and probiotics, which recommends certainprebiotics but not probiotics, for the treatment ofconstipation.26
Inflammatory bowel disease (IBD) e g Crohn’s disease,ulcerative colitis and pouchitis(after ileal pouch analanastomosis in ulcerative colitis patients) are oftenrefractory to standard therapy. The rational to useprobiotics and its beneficial efficacy in the treatment ofchronic inflammatory bowel disease (IBD) isincreasingly scrutinized.The role of probiotics forinducing and maintaining remission especially regardinginduction of remission for ulcerative colitis has shownbreakthroughs.27
A relationship between immune response andgastrointestinal microbials appears to be involved inthe mechanism of ulcerative colitis (UC). AlternativeIBD treatment approaches aimed at modifying thecomposition of the intestinal microbiota in order toovercome gut dysbiosis have become a subjectof majorinterest in recent years. There is also some evidencethat probiotics may facilitate and stabilize clinicalremission.28
Changes in the relative abundance of the familiesEnterobacteriaceae and Lachnospiraceae in UCpatients provide useful diagnostic indications of clinicalresponse after FMT.29 Randomized, placebo-controlledtrials with larger cohorts will be necessary to establishcause–effect relationships for the successfullytransmitted donor phylotypes such as F. prausnitzii, B.ovatus, and R. faecis.
Trial results comparing the probiotic(Escherichia coliNissle1917) tomesalazine have reported equivalent ratesof UC relapse. Treatment with Lactobacillus rhamnosusGGstrain alone or in combination with mesalazineresulted in a nonsignificant odds ratio decrease forrelapse and a significant increase in time to relapsecompared to treatment with mesalazine alone.Additionally, bifidobacteria fermented milksupplemented patients had significant reductions in UCexacerbations when compared to nonsupplementedpatients. Probiotics were well tolerated, with adverseevent rates similar between treatments. One study of 90volunteers found significantly higher remission rates inpeople with ulcerative colitis who were given thebeneficial bacteria E. coli Nissle. The higher the dose,the longer their remission.30
It is suggested that patients with ulcerative colitisbenefit by using bacterial therapies and patients withCrohn’s disease from S. boulardii, an yeast.31
Chronic or recurrent pouchitis is an importantcomplication occurring in ~10–20% of UC patients afterileal anal pouch formation surgery. VSL#3 was shownbeneficial in prophylaxis against pouchitis onset aftersurgical take-down and in maintaining clinical remissionafter antibiotic induction.Clinical expert guidelinesconcur that probiotics (VSL#3) can be effective forpreventing recurrence of pouchitis.32,33
Diverticulosis is present in approximately two thirds ofthe elderly population and a large majority of thoseaffected remain entirely asymptomatic. However, anestimated 20% of patients may develop ‘diverticulardisease’ with time. Change in the colonic microflora,resulting in a decrease in healthy flora and an increasein pathogenic bacteria, may be detected in patients withdiverticular disease. This may allow chronic inflammationand epithelial cell proliferation in and around thediverticula.34 Probiotics, restoring the colonicmicroenvironment, have been proposed to treat thosepatients.35
The most recently published RCT in Diverticulosiscompared mesalazine or mesalazine plusBifidobacterium infantis 35624 for 12 weeks andfollowed up for nine additional months. Global symptomscores were assessed over the 52 weeks of follow-up.Mesalamine demonstrated a consistent trend inreducing symptoms. Addition of probiotic did notincrease mesalamine efficacy.36
Another Multicentre Double-blind, Randomised,Placebo-Controlled Study showed both cyclicmesalazine and L. casei subsp. DG 24 billion/day appearto be better than placebo for maintaining remission insymptomatic uncomplicated diverticular disease (SUDD)especially when used in combination. Moreover, bothtreatments alone or in combination are significantlybetter than placebo in preventing occurrence of acutediverticulitis in SUDD patients.37
Alcoholic liver disease is characterized by fatty liver(steatosis), which may progress to alcoholic hepatitis,fibrosis, and cirrhosis.38 Intestinal bacterial overgrowthis common in patients with alcoholic liver disease. Inalcoholics, translocation of bacteria and bacterialproducts into the circulation contributes to liver disease.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
96

Treatment with prebiotics partially restored gutmicrobiome, reduced bacterial overgrowth and lessenedalcoholic steatohepatitis. Disbiosis (disruption ordysregulationof intestinal antimicrobial molecules)contributed to changes in the enteric microbiome leadingto alcoholic steatohepatitis in mice.39
Role in Metbolic disease or obesity shows comparisonsof the distal gut microbiota of genetically obese andlean human volunteers revealing that obesity isassociated with changes in the relative abundance ofthe two dominant bacterial divisions, theBacteroidetesand the Firmicutes. Obese microbiome hasan increased capacity to harvest energy from the diet.40
Gut microbiota is an additional contributing factor tothe pathophysiology of obesity.41 Studies in mice haveassociated the phylum Firmicutes with obesity and thephylum Bacteroidetes with weight loss.42
There is clear evidence that the intestinal microbiotainfluences the host through its effect on body weight,bile acid metabolism, proinflammatory activity and insulinresistance, and modulation of gut hormones43. Asynergism between role ofmicroflora, aberrant intestinalmicrobiota(either quantitatively or qualitatively), a“leaky” gut mucosal barrier and altered mucosalimmunity contributing to type 1 diabetes has begun toevolve. Changes in gut microbiota and thus cell wallcomponents are involved in the epigenetic regulationof inflammatory reactions. An improved diet targeted toinduce gut microbial balance and epigenetic changes ofpro-inflammatory genes may be effective in theprevention of metabolic syndrome.44
Precautions about ProbioticsProbiotics preparations are generally considered as foodnot drug. They are already present in a normal digestivesystem and therefore safeand may cause few sideeffects.In the USA, formulations of probiotics are medicalfoods and must be used under medical supervision.In asystematic review of studies, rate of side effects wassame in probiotics users as in those taking mesalazine.Noserious side effects have been associated withprolonged use of probiotics in ulcerative colitis.45
Probiotics have enjoyed an impeccable safety reputationbut immune compromise (including a debilitated stateor malignancy) has been identified as a risk factor forrare cases of bacteraemia or fungaemia in patients takingcertain probiotics (most commonly Saccharomyces
boulardii).46 No serious adverse events attributed toFMT were observed.47
One high profile multicenter placebo controlled DutchRCT examining probiotic supplementation in severeacute pancreatitis found a higher incidence of mesentericischemia and death in the treatment group.48 This is theonly trial supporting the concept that probiotics shouldbe avoided in critically ill patients.
Probiotic ingredients should be clearly marked on thelabel. There’s no way to judge the safety of unidentifiedmixtures.Probiotics are food particles andthey arerapidly washed awaywithin days, although strain-specific differences occur.49 For a chronic GI problem, itis critically important that the product is taken inadequate doses on a regular basis (e.g. just before ameal) for a reasonable period of time, which should beat least a month, unless it cannot be tolerated for anyreason. In order to get the full benefits of probiotics,dose selection should be based on available evidenceand manufacturers’ recommendations. Some yogurtscontain the friendly bacteria but as they are sensitive tooxygen, light and dramatic temperature changesso whenheat-treated or pasteurized, they lose thesevaluable”liveand active cultures.”.
Despite their long history, wide availability andsubstantial publication record, the clinical role ofprobiotics are in general, inadequately characterised andremains ill-defined. Probiotic research are complicatedby the wide variety of probiotic strains obtained withone strain notapplicable to others. According to ageand health status of the target group effects of probioticsmay vary.
The variable range of formulations (capsules, sachets,yoghurts and fermented milks or fruit drinks), differindose and the presence of supporting substrates addfurther sources of variation.50
Conclusion:Despite widespread use of natural therapies by patientsallured by advertisesments, health care providers maybe unfamiliar with probiotics as a treatmentmodality.Many patients consume probiotic products inattempts to manipulate the intestinal microbiota forhealth benefit. Questions regarding optimal probiotic,dosing, specific patient populations and placement intherapy are to be answered by large, randomized,
Proboitics and their Role in GI Diseases S Perveen & MA Ahmed
97

controlled trials conducted before probiotics can beroutinely recommended.Evidence supports a role forconsidering the recommendation of conventionalprobiotics for some clinical conditions. Probiotic strainselection should focus on quality tested products withclinically demonstrated benefit for the given disorder.Patients and physicians should expect modest effectsand consider using probiotics as a supplement ratherthan a replacement for conventional therapy.[51]
Probiotic research is evolving rapidly and this articlereflect physicians’ rather than patients’perspectives.Future clinicians will have the opportunityto use directed selection of a probiotic or probioticderived product to specifically address a unique diseasecausing physiologic or genetic defect.Thoughchallenges exist, ongoing investigations offer greatpromise for the future.
Some patients have interest in probiotics and theirpotential and they may take probiotics (or productsincorrectly identified as probiotics) to reduce theirsymptoms before consulting their physician. Therefore,educational materials for the general public are alsoneeded to improve their understanding and to ensureappropriate use of probiotics.
References:1. Macpherson AJ, Harris NL, Interactions between
commensal intestinal bacteria and the immune system.Nat Rev Immunol. 2004; 4(6):478-85.
2. Conlon MA, Bird AR. The Impact of Diet and Lifestyleon Gut Microbiota and Human Health. Nutrients.2014;7(1):17-44.
3. FAO/WHO Working Group. Guidelines for the evaluationof probiotics in food. Report of a joint FAO/WHOworking group on drafting guidelines for the evaluationof probiotics in food. London, Ontario, Canada 2002.Available at: ftp://ftp.fao.org/es/esn/food/wgreport2.pdf.Accessed 2013.
4. Sanders ME. Impact of probiotics on colonizing microbiotaof the gut. Journal of Clinical Gastroenterology.2011;45:115–119.
5. Thomas CM, Versalovic J. Probiotics-host communication:Modulation of signaling pathways in the intestine. GutMicrobes. 2010;1(3):148–163.
6. Koenig JE, Spor A, Scalfone N, Fricker AD, Stombaugh J,Knight R, Angenent LT, Ley RE. Succession of microbialconsortia in the developing infant gut microbiome. PNAS.2011;108(Suppl 1):4578–4585.
7. Dominguez-Bello MG, Costello EK, Contreras M, MagrisM, Hidalgo G, Fierer N, Knight R. Delivery mode shapesthe acquisition and structure of the initial microbiotaacross multiple body habitats in newborns. PNAS.2010;107(26):11971–11975.
8. Macpherson AJ, Harris NL. Interactions betweencommensal intestinal bacteria and the immune system.Nat Rev Immunol. 2004; 4(6):478-85.
9. R Fuller. Probiotics in human medicine. Gut1991;32(4):439–442.
10. H.M. Timmerman, C.J.M. Koningb, L. Mulderc, F.M.Romboutsd, A.C. BeynenaMonostrain. multistrain andmultispecies probiotics—A comparison of functionalityand efficacy.International Journal of Food Microbiology.2004; 96(3):219–233.
11. Elizabeth C. Verna. Use of probiotics in gastrointestinaldisorders: what to recommend? TherapAdvGastroenterol.2010; 3(5): 307–319.
12. Borchers AT, Selmi C, Meyers FJ, Keen CL, Gershwin ME.Probiotics and immunity. Gut 2010; 59(3):325-32.
13. Richard N. Fedorak. Probiotics in the Management ofUlcerative Colitis. GastroenterolHepatol (N Y). 2010;6(11): 688–690.
14. Thomas DW, Greer FR, American Academy of PediatricsCommittee on Nutrition, Review Probiotics and prebioticsin pediatrics. Pediatrics. 2010; 126(6):1217-31
15. Allen SJ, Martinez EG, Gregorio GV, Dans LF, ReviewProbiotics for treating acute infectious diarrhoea.Cochrane Database Syst Rev. 2010;10 (11):CD003048
16. Issa I, MoucariR.Probiotics for antibiotic-associateddiarrhea: Do we have a verdict? World JGastroenterol.2014 ;20(47):17788-17795.
17. Floch MH, Walker WA, Madsen K, Sanders ME,Macfarlane GT, Flint HJ, Dieleman LA, Ringel Y,Guandalini S, Kelly CP, Brandt LJ, Recommendations forprobiotic use-2011 update. ClinGastroenterol. 2011;45:S168-71.
18. Chang JY, Antonopoulos DA, Kalra A, Tonelli A, KhalifeWT, Schmidt TM, Young VB. Decreased diversity of thefecal microbiome in recurrent clostridium difficile-associated diarrhea. Journal of Infectious Diseases.2008;197(3):435–438
19 . Dr. Mellow, Dr. Schiller, and Dr. Kenneley.AmericanCollege of Gastroenterology (ACG) 2011 Annual ScientificMeeting and Postgraduate Course; President’s PlenarySession II. Presented 2011.
20. Brandt LJ, Borody TJ, Campbell J. Endoscopic fecalmicrobiota transplantation: “first-line” treatment forsevere Clostridium difficile infection? J ClinGastroenterol2011; 45: 655-657.
21. Dr. Kamepalli, Dr. Louie, and Dr. Moore ID Week 2013.Abstract 89. Presented 2013.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
98

22. Drossman DA. The functional gastrointestinal disordersand the Rome III process. Gastroenterology 2006; 130:1377–90.
23. Moayyedi P, Ford AC, Talley NJ, Cremonini F, Foxx-Orenstein AE, Brandt LJ, Quigley EM .The efficacy ofprobiotics in the treatment of irritable bowel syndrome: asystematic review. J Gastroenterol. 2009; 44(1):26-46.
24. P Moayyedi, A C Ford, N J Talley, F Cremonini, A E Foxx-Orenstein, L J Brandt, E M M Quigley. The efficacy ofprobiotics in the treatment of IBS. Gut 2010; 59:325-332.
25. A. P. S. Hungin, C. Mulligan, B. Pot, P. Whorwell, L.Agrèus, P. Fracasso, C. Lionis, J. Mendive, J.-M. Philippartde Foy, G. Rubin, C. Winchester, N. de Wit. Probiotics inthe Management of Lower Gastrointestinal Symptomsin Clinical Practice. Aliment PharmacolTher. 2013;38(8):864-886.
26. Guarner F, Khan AG, Garisch J, et al. Probiotics andprebiotics. 2011. Available at: http://www.worldgastroenterology.org/probiotics-prebiotics. html.Accessed 2013
27. Meijer BJ, Dieleman LA. Probiotics in the treatment ofhuman inflammatory bowel diseases: update 2011. JClinGastroenterol. 2011; 45:139-44.
28. Khan KJ, Ullman TA, Ford AC et al,Antibiotic therapy ininflammatory bowel disease: a systematic review and meta-analysis. Am J Gastroenterol. 2011;106:661–73.
29. SieglindeAngelberger MD, Walter Reinisch MD,AthanasiosMakristathis PhD, Cornelia Lichtenberger etal, Temporal Bacterial Community Dynamics Vary AmongUlcerative Colitis Patients After Fecal MicrobiotaTransplantation Am J Gastroenterol. 2013;108(10):1620-1630
30. Naidoo K, Gordon M, Fagbemi AO, Thomas AG, AkobengAK. Probiotics for maintenance of remission in ulcerativecolitis. Cochrane Database Syst Rev. 2011;(12):CD007443.
31. Cain AM, KarpaKD Clinical utility of probiotics ininflammatory bowel disease AlternTher HealthMed.2011;17(1):72-79.
32. Floch MH, Walker WA, Madsen K, Sanders ME,Macfarlane GT, Flint HJ, Dieleman LA, Ringel Y,Guandalini S, Kelly CP, Brandt LJ, Recommendations forprobiotic use-2011 update J ClinGastroenterol. 2011; 45(3):168-71.
33. Pardi DS, D’Haens G, Shen B, Campbell S, Gionchetti P,Clinical guidelines for the management of pouchitis inInflamm Bowel Dis. Gut 2009;15(9):1424-31.
34. Humes DJ. Changing epidemiology: does it increase ourunderstanding? J DigDis 2012; 30: 6–11.
35. Tursi A. Antibiotics and probiotics in the treatment ofdiverticular disease. J ClinGastroenterol. 2011; 45(12):46–52 .
36. Stollman N, Magowan S, Shanahan F, Quigley EM. Arandomized controlled study of mesalamine after acutediverticulitis: results of the DIVA trial. JClinGastroenterol2013; 47: 621–9.
37. Tursi A, G. Brandimarte, W. Elisei, M. Picchio et al,Mesalazine and/or Probiotics in Maintaining Remission
of Symptomatic Uncomplicated Diverticular Disease.Aliment PharmacolTher. 2013;38(7):741-751.
38. Bataller R, Brenner DA. Liver fibrosis. J Clin Invest.2005;115:209–218.
39. Yan AW, Fouts DE, Brandl J, Starkel P, Torralba M, SchottE, Tsukamoto H, Nelson KE, Brenner DA, Schnabl B.Enteric dysbiosis associated with a mouse model ofalcoholic liver disease. Hepatology. 2011;53(1):96–105.
40. Murphy EF, Cotter PD, Hogan A, O’Sullivan O, Joyce A,Fouhy F, Clarke SF, Marques TM, O’Toole PW, StantonC et al, Divergent metabolic outcomes arising from targetedmanipulation of the gut microbiota in diet-induced obesity.Gut.2013; 62(2):220-6.
41. Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, MardisER, Gordon JI. An obesity-associated gut microbiome withincreased capacity for energy harvest. Nature. 2006;444(22):1027–1031.
42. Million M, Lagier JC, Yahav D, Paul M. Gut bacterialmicrobiota and obesity.ClinMicrobiol Infect.2013;19(4):305-13.
43. Han J, Lin H.Intestinalmicrobiota and type 2 diabetes:From mechanism insights to therapeutic perspective.World J Gastroenterol. 2014;20(47):17737-17745.
44. Remely M, Aumueller E, Jahn D, Hippe B, Brath H,Haslberger AG.MicrobiotaHYPERLINK “http://www.ncbi.nlm.nih.gov/pubmed/24533976” and epigeneticregulation of inflammatory mediators in type 2 diabetesand obesityHYPERLINK “http://www.ncbi.nlm.nih.gov/pubmed/24533976”.Benef Microbes. 2014;5(1):33-43.
45. Naidoo K, Gordon M, Fagbemi AO, Thomas AG, AkobengAK. Probiotics for maintenance of remission in ulcerativecolitis. Cochrane Database Syst Rev.2011; (12):CD007443.
46 Sanders ME, Akkermans LM, Haller D, et al. Safetyassessment of probiotics for human use. Gut Microbes2010;1:164–85.
47. Ilan Youngster, George H. Russell, Christina Pindar,Tomer Ziv-Baran et al, Oral, Capsulized, Frozen FecalMicrobiota Transplantation for Relapsing Clostridiumdifficile Infection. JAMA. 2014;312(17):1772-1778.
48. Besselink MG, van Santvoort HC, Buskens E, BoermeesterMA et al, Probiotic prophylaxis in predicted severe acutepancreatitis: a randomised, double-blind, placebo-controlled trial Dutch Acute Pancreatitis Study GroupLancet. 2008; 23(13):651-9.
49. O’Connell Motherway M, Zomer A, Leahy SCetal,Functional genome analysis of BifidobacteriumbreveUCC2003 reveals type IVb tight adherence (Tad) pili asan essential and conserved host-colonization factor.ProcNatlAcadSci USA 2011; 108: 11217–22.
50. FAO/WHO Expert Consultation. Health and nutritionalproperties of probiotics in food including powder milkwith live lactic acid bacteria. Report of a joint FAO/WHOexpert consultation on evaluation of health andnutritional properties of probiotics in food includingpowder milk with live lactic acid bacteria, 2001. Cordoba,Argentina. Accessed 2012.
51. Ciorba MA. A gastroenterologist’s guide to probiotics.ClinGastroenterolHepatol. 2012; 10 (9):960-8.
Proboitics and their Role in GI Diseases S Perveen & MA Ahmed
99

CASE REPORTS
Summary:Malignant Nodular Hidradenoma is an infrequent highlymalignant, primary skin tumor derived from eccrine sweatglands. It has an aggressive course, with high recurrence,high rate of metastases and has very poor prognosis. It hasbeen described as an “orphan”neoplasm. The tumor issimilar to its benign counterpart but had additional featuressuch as surface ulceration, numerous mitotic figures andinfiltrative growth pattern. Pre-operative diagnosis is difficult
by the fine needle aspiration cytology. Malignant nodularhidradenoma of chest wall in 35 years old women, whopresented to us with a recurrent rapidly growing swellingover chest wall that grew rapidly over two months after firstexcision. Tissue diagnosis of first excised specimen waseccrine poroma that was similar to its benign counterpart.
Key words: sweat gland tumor, malignant hidradenoma,eccrine poroma, spiradenoma.
(J Bangladesh Coll Phys Surg 2016; 34: 100-103)
Malignant Nodular Hidradenoma: Isolated Case Reportand Review of Literature
SA KHANa, AAA ALIb, S FERDOUSIc, M RIYADd, AAH MAHMUDe
Intoduction :Malignant tumors of the sweat glands represent rareoncological entites, characterized by non-specificclinical presentation and equivocal pathologicalfeatures. Their precise diagnosis and histologicalclassification can be very difficult. It is an extremely raretumor with less than 50 cases reported1.
Hidradenomas arise as intradermal nodules from eccrinesweat glands. Ultrastructural and enzyme histochemicalstudies have shown nodular hidradenomas to beintermediate between eccrine poroma and eccrinespiradenoma2. The histology of the malignanthidradenoma resembles of it’s benign counterpart. The
a. Dr. Sadia Armin Khan, Assistant Professor, Department ofSurgery, Ad-din Women’s Medical College Hospital
b. Professor Abu Ahmed Ashraf Ali, Professor of Surgery, Ad-din Women’s Medical College Hospital
c. Dr. Shamima Ferdousi, Associate Professor, Departmentof Pathology, Ibrahim Medical College Hospital
d. Dr. Mahmud Riyad, Associate Professor, Department ofSurgery, Ad-din Women’s Medical College Hospital
e. Dr. Ahmed-Al-Hasan Mahmud, Registar, Department ofSurgery, Ad-din Women’s Medical College Hospital.
Address of Correspondence: Dr. Sadia Armin Khan, AssistantProfessor, Department of Surgery, Ad-din Women’s MedicalCollege Hospital, Mobile: 01720809726, e-mail: [email protected]
Received: 30 September, 2014 Accepted: 29 November, 2015
criteria for malignancy include poor circumscription,presence of nuclear atypia, mitotic activity, presence ofpredominantly solid cell islands, infiltrative growthpattern, necrosis, and angio-lymphatic permeation3-5 .We report a case of malignant nodular hidradenoma ina middle aged woman who presented with a recuurentswelling in right side of lower chest wall.
Case report :A 35 years old female presented to us with swellingover right side of chest wall. The swelling was excisedand sent for histopathology. The report was ecccrineproroma. But it recurred after two months. The swellingwas rapidly increasing in size over the last one and halfmonths. The mass became significantly prominent overthe last 15 days prior to presentation resulting indiscomfort.
Physical examination revealed a large lobulated massabout 20 cmx15cm in size, without ulceration. It washard, non-mobile, non-fluctuant and adherent to theold scar. The draining area showed no palpablelymphnode. General examination including lungs andliver were normal. Per-operatively, a hard fibrous tumorwas observed to infiltrate the muscle but not tounderlying ribs. Wide local excision with 1 cm marginalclearance of healthy surrounding tissue was performedalong with primary closure. Biopsy was sent topathological examination.

Pathological findings :GROSS : Partly skin covered with grayish yellow massmeasuring 18x11x7cm. Skin surface shows a part of oldincision mark measuring 5.5 cm in length. The cut surfaceshows a grey brown lobulated tumor with area of cysticchange.
Microscopic description : The dermis presents amalignant tumor with infiltrating border made ofpolygonal cells showing mild to moderatepleomorphism. Mitotic figures are frequent. Areas ofnecrosis are seen. The deep resection margin andperipheral resection margins are free from tumor. Thetumor exhibited infiltrative growth pattern. A diagnosisof malignant nodular hidradenoma was made.
Discussion :The recognition of hidradenoma as a distinct entity wasfirst reported in 1941 by Mayer, whereas the term “clearcell hidradenoma” was proposed in 1954 by Keasbyand Hadley6. The malignant form of hidradenoma isextremely rare, with less than 50 cases ever reported inthe literature. All these cases were characterized by asignificant rate of locoregional recurrence. Some patientsdeveloped distant metastatic spread as well 7-8.
The disease is usually expressed as a small intradermalmass which remains inactive for a long period of timebefore increasing in size. Its aggressive behavior is moreapparent after each local relapse with faster growth andinvasion of the surrounding tissues. In most cases, noepidermal participation is encountered. Hidradenomausually affects middle-aged women, although itsmalignant form shows no age or gender predilection 9-11.
Malignant hidradenoma is usually found in the scalp,face or anterior surface of the trunk. These lesions tendto metastasized and may cause death12.
Although there is insufficient evidence in the literature,the recurrence rate may be estimated at about 50% andmetastasis rate is about 60% including metastasis toregional nodes, bone, viscera and skin 12.
Histologically, clear cell hidradenoma seems to originatefrom the ductal epithelium of the sweat glands, whereashistogenetically it appears to represent a transitionaltumor, sharing features of eccrine poroma and eccrinespiradenoma 9.
Malignant nodular hidradenoma are usually larger,asymmetrical, and show invasion into surrounding
Per-operative view showing large mass adhere tooverlying scar mark and surrounding tissue
Microscopical image of the clear cell hidradenomaarising from the anterior abdominal wall. A) Elementsof tubular and solid neoplastic configuration arisingin the vicinity of a hair follicle. B) Malignant cellswith clear, transparent cytoplasm and round nucleus.
Malignant Nodular Hidradenoma: Isolated Case Report SA Khan et al.
101

tissue. In addition, there may be angio-lymphaticinvasion. Mitosis are usually easily detected, and somemay be atypical. Tumor necrosis, areas of highcellularity, and focal and diffuse areas of markedcytological atypia in which differentiated elements areunrecognizable are present in some examples. In somecases of Malignant nodular hidradenomas, nuclearanaplasia may be only slight to moderate or even absentin the both primary tumors and the metastasis. Nuclearanaplasia , if present, may be limited to the clear cells oraffect both the polyhedral and clear cells12.
The recognition of the eccrine origin of a malignanthidradenoma may be accomplished through specificimmunohistochemical techniques, a positive PAS stain,as well as with the presence of lobules with epidermaldifferentiation 8, 13.
Sweat-glands neoplasms generally arise from the eccrinecellular lineage, they exhibit cellular growth patternsthat may further influence the neoplasm’s architecture.Hidradenoma may exhibits both cystic and solid featuresand that is why it enters on differential diagnosis withapocrine tumors; in fact there are divergent opinions onthe primitive cellular lineage . The issue is complicatedby the coexistence of eccrine and apocrine cells insidecutaneous hamartomas or inside adnexal tumors withmixed differentiation (follicular and sebaceous) 14,15.
Malignant clear cell hidradenoma usually develops denovo and invades the dermis and subcutaneous tissue.Surprisingly, it might share significant histopathologicalfeatures with its benign form. The mitotic index may notbe representative or may affect only a small cellularsubpopulation. Thereafter, the diagnosis of malignancythrough standard pathological examination may proveextremely difficult 16.
In our case, it was interesting to note that, in contrast tothe final diagnosis, previous pathology reports hadascertained the presence of an eccrine poroma. The latteris a benign tumor of the sweat glands with similar clinicalpresentation and equivocal enzyme reactions, whichpose tremendous diagnostic dilemmas 17. Because ofthe rarity of these oncological entities, as well as theirhistopathological similarity, it is almost impossible todefine whether a malignant clear cell hidradenoma hadbeen developed from a benign eccrine poroma or wasthe correct diagnosis from the beginning.
The most recent reports support the fact that malignantclear cell hidradenoma should be considered as a distinctentity rather than the result of a malignant transformationof its benign type, underlining the importance of aprecise initial diagnosis 18,19. Rosen et al.20 presenteda case of a clear cell hidradenoma of the eyelidcomplicated by multiple recurrences and invasion ofnearby structures. Histologically, no atypia or increasednuclear mitoses were found. The precise identificationof a benign or malignant hidradenoma, based onpathological examination, was not possible. Similarfindings were noted in other case reports of clear cellhidradenoma 21-26.
Surgical excision remains the therapeutic modality ofchoice. Wong et al.8 supported wide surgical resectionwith a least 2 cm of clear margins for both primary diseaseand local recurrences. Elective regionallymphadenectomy after lymphoscintigraphy should alsobe performed. The role of sentinel lymph node biopsyin the treatment of malignant hidradenoma iscontroversial. Locoregional recurrence even after widesurgical excision has been reported in more than 50% ofcases, although overall and disease-free survival ratesare hard to determine as the result of the very limitednumber of reported cases 27. Adjuvant chemotherapyand radiotherapy have no impact in local control orsurvival 28.
The use of Mohs micrographic surgery with superiorevaluation of surgical margins has been utilized morerecently as the primary treatment modality29. The use ofsentinel lymph node biopsy also has been reported tobe useful, especially given the propensity for themetastatic spread29.
Immunohistochemitry revealed strong positivity forEpithelial Membrane Antigen (EMA), Estrogen andProgesterone Receptors (EPR) and CEA. P63, CFDP-15and C-erbB2 were negative. Ki67 decorated 40% ofneoplastic cells, which has been sparked interest intreatment with hormone therapy. Schrçder et al30 reportedthe use of tamoxifen as adjuvant therapy for an estrogenreceptor positive metastatic sweat gland adenocarcinoma.Further study has also been going on.
Conclusion: Malignant clear cell hidradenoma is a rare oncologicalentity, with no particular clinical or histopathologicalfeatures. It should be included in the differential
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
102

diagnosis of dermal lesions with an aggressive behaviorand multiple recurrences, despite aggressive surgicaltreatment.
References:I. E. Liapakis, D.P. Korkolis, A. Koutsoumi, A. Fida, G.
Kokkalis and P.P. Vassilopoulus: Malignant Hidradenoma:A Report of Two Cases and Review of the Literature.ANTICANCER RESEARCH 26: 2217-2220 (2006)
2. Agarwala NS, Rane TM, Bhaduri AS. Clear cell hidradenomaof the eyelid: A case report. Indian J Pathol Microbiol.1999;42:361–3. [PubMed]
3. Headington JT, Niederhuber JE, Beals TF. Malignant clearcell acrospiroma. Cancer. 1978;41:641–7. [PubMed]
4. Mehregan AH, Hashimoto K, Rahbari H. Eccrineadenocarcinoma: A clinicopathologic study of 35 cases.Arch Dermatol. 1983;119:104–14. [PubMed]
5. Volmar KE, Cummings TJ, Wang WH, Creager AJ, TylerDS, Xie HB. Clear cell hidradenoma: A mimic of metastaticclear cell tumors. Arch Pathol Lab Med. 2005;129:e113–6. [PubMed]
6. Keasby LE and Hadley GG: Clear cell hidradenoma. Cancer7: 934-951, 1954.
7. AshJey J, Smith-Reed M and Chernys A: Sweat glandcarcinoma. Case report and review of the literature.Dermatol Surg 23: 129-133, 1997.
8. Wong TY, Suster S, Nogita T, Duncan LM, Dickersin RGand Mihm MC: Clear cell eccrine carcinomas of the skin.A clinicopathologic study of nine patients. Cancer 73:1631-1643, 1994.
9. Lever WF and Schaumburg-Lever G: Histopathology ofthe Skin. 6th Edition. JB Lippincot, Philadelphia, pp.557-585, 1983.
10. Lopez-Burbano LF, Cimorra GA, Gonzalez-Peirona E andA/Faro J: Malignant clear-cell hidradenoma. PRS 80: 300-303, 1986.
11. Champion RH, Burton JL and Ebling FJG (eds.): Rook/Wílkinson/Ebling. Textbook of Dermatology, 5thEdition,Blackwell Scientific Publications, Oxford pp.1515-1518, 1992.
12. David E Elder: Lever’s Histopathology of the Skin, 9th
Edition,907.
13. Johnson BI and Helwig EB Jr: Eccrine acrospiroma. Cancer23:641-657, 1969.
14. Groben PA, Hitchcock MG, Leshin B, White WL (1999)Apocrine poroma: a distinctive case in a patient withnevoid basal cell carcinoma syndrome. Am JDermatopathol 21: 31-33.
15. Harvell JD, Kerschmann RL, LeBoit PE (1996) Eccrineor apocrine poroma? Six poromas with divergent adnexaldifferentiation. Am J Dermatopathol 18: 1-9.
16. Hernandez-Perez E and Cruz FA: Clear cellhidradenocarcinoma:report of an unusual case.Dermatologica 153: 249-252, 1976.
17. Hashimofo K, Di Bella RJ and Lever WF: Clear cellhidradenoma. Arch Dermatol 96: 18-38, 1967.
18. Lopez-Burbano LF, Cimorra GA, Gonzalez-Peirona E andA/Faro J: Malignant clear-cell hidradenoma. PRS 80: 300-303, 1986.
19. Ohta M, Hiramoto M, Fujii M and Togo T: Nodularhidradenocarcinoma on the scalp of a young woman: casereport and review of literature. Dermatol Surg 9: 1265-1268, 2004.
20. Rosen Y, Kim B and Yermakov V: Eccrine sweat glandtumor of clear cell origin involving the eyelids. Cancer36: 1034-1041, 1975.
21. Harada T, Muraoka M, Ishii M and Wakasa K: Malignantclearcell hidradenoma associated with pseudoepithelio-matous hyperplasia on the forehead. Ann Plast Surg 4:443-444, 2003.
22. Yildirim S, Akoz T, Apaydin I, Ege GA and Gideroglu K:Malignant clear cell hidradenoma with giant metastasisto the axilla. Ann Plast Surg 1: 102, 2000.
23 Grossniklaus HE and Knight SH: Eccrine acrospiroma(clear cell hidradenoma) of the eyelid.Immunohistochemical and ultrastructural features.Ophthalmology 98: 347-352, 1991.
24. Herzberg AJ, Elenitsas R and Strohmeyer CR: An unusualcase of early malignant transformation in a spiradenoma.Dermatol Surg 21: 731-734, 1995.
25. Biernat W and Biernat S: Cutaneuous adnexal carcinomaarising within a solitary cylindroma-spiradenoma. Am JDermatopathol 18: 77-82, 1996.
26. ltoh T, Yamamoto N and Tokunaga M: Malignant eccrinespiradenoma with smooth muscle cell differentiation:histological and immunohistochemical study. Pathol Int46: 887-893, 1996.
27. Touma D, Laporte M, Goosens A and Ledoux M:Malignant clear cell hidradenoma. Dermatology 186: 284-286, 1993.
28. Stromberg BV, Thorne S, Dimino-Emme L, Katz DA andRouse JW: Malignant clear cell hidradenoma: a case reportand literature review. Nebr Med J 76: 166-170, 1991.
29. Tolland JP, Brenn T, Guldbakke KK, et al. Mohsmicrographic surgery and sentinel lymph node mappingand estrogen receptor analysis for the treatment ofmalignant nodular hidradenoma. Dermatol Surg.2006; 32:1294-1301.
30. Schrçder U, Driers V, Klussmann JP, et al. Successfuladjuvant tamoxifen therapy for estrogen receptor positivemetastasizing sweat gland adenocarcinoma: need a clinicaltrial? Ann Otol Rhinol Laryngol. 2004; 113(3, pt 1):242-244.
Malignant Nodular Hidradenoma: Isolated Case Report SA Khan et al.
103

Journal of Bangladesh College of Physicians and SurgeonsVol. 34, No. 2, April 2016
Summary:Raised intracranial pressure in the absence of an intracranialmass or hydrocephalus (BIH or pseudotumor cerebri) hasbeen described in association with many conditions includingSLE. Several pathogenic pathways tie BIH with SLE asthrombotic obliteration of cerebral arteriolar and venoussystems and immune complex deposition within the arachnoidvilli that are responsible for cerebrospinal fluid (CSF)
absorption. The diagnosis of BIH was confirmed by increasedintracranial pressure in the absence of any abnormalradiological findings of the brain. We report a young womanwith SLE complicated by BIH which resolved withcorticosteroid therapy and osmotic diuretics.
Key wards: Pseudotumour cerebri, Systemic lupus erythematosus
(J Bangladesh Coll Phys Surg 2016; 34: 104-107)
a. Dr. Aparna Das, Asso. Prof.Dept. of Medicine, DhakaMedical College
b. Dr. Jiban Chandra Das, IMO, Dept. of Medicine, DhakaMedical College
c. Dr. Abdullah Al Ahmad , HMO, Dept. of Medicine, DhakaMedical College
d. Prof. Md Azizul Kahhar, Professor. Dept. of Medicine,Dhaka Medical College
Address of Correspondence: Dr. Aparna Das, Asso. Prof.,Dept. of Medicine, Dhaka Medical College.
Received: 30 September, 2014 Accepted: 20 December, 2015
Pseudotumor Cerebri : A Rare Presentation of SystemicLupus Erythematosus
A DASa, JC DASb , AA AHMADc, MA KAHHARd
Introduction:Systemic lupus erythematosus (SLE) is a multisystemautoimmune disease characterized by diversemanifestations encompassing almost all organ systemsand the finding of antibodies in the blood directedagainst one or more components of cellnuclei¹.Neuropsychiatric manifestations can occur inup to two-thirds of patients with SLE2 . Pseudotumourcerebri (PTC) is an exceedingly rare manifestation ofneuropsychiatric lupus and one of the causes ofheadache in SLE patients 2. It is characterized by anelevated intracranial pressure (papilloedema withoccasional abducent nerve palsy) in the absence ofspace occupying lesion or ventricular enlargement, bio-chemical and cytological abnormalities, in alert andoriented patients3,4. Pseudotumour cerebri (PTC) maypresent as unremitting headache 3. If this condition isnot treated promptly it can even lead to blindness. Sincethe first case of Bettman et al 5, there have been sporadicreports of concomitant SLE and PTC in adults. Here, wedescribe a case of 22-year-old lady presenting withprolonged fever and headache as the main features of
her disease who showed a dramatic response to oralsteroids.
Case Report:A 22-year-old lady presented with 1-year and 6-monthsduration of low-grade fever, headache, episodic jointpain and hair fall. She lost 8 kg of her body weight overthe course of her illness and developed an ulcer in oralcavity 5 days prior to admission at our hospital. Herheadache was unilateral, throbbing, predominantlyoccurring on awaking from sleep without otheraggravating and relieving factors. Apart from malaise,nausea and occasional dizziness on standing, she deniesany vomiting, blurring of vision, diplopia, reduction inurinary volume, alteration of consciousness. Review ofother systems was negative other than the abovementioned symptoms. She had an unremarkable pastmedical and family history. She does not smoke, drinkalcohol and have never used intravenous drugs.
With these complaints she had visited two physicians1-year back and had been admitted once at a tertiarylevel hospital one month ago where she was diagnosedwith urinary tract infection and was given some insightabout the possibility of SLE. Having been not cured offever she got admitted at a secondary hospital whereher fever was attributed to urinary tract infection. Hermedication included occasional use of paracetamol,naproxen sodium for headache, oral cefuroxime,intravenous levofloxacin for urinary tract infection andhad been transfused with 2 units of fresh human wholeblood. She denies taking any other medications includingoral contraceptives. On admission, examination revealeda thin, ill-looking young woman with a temperature of
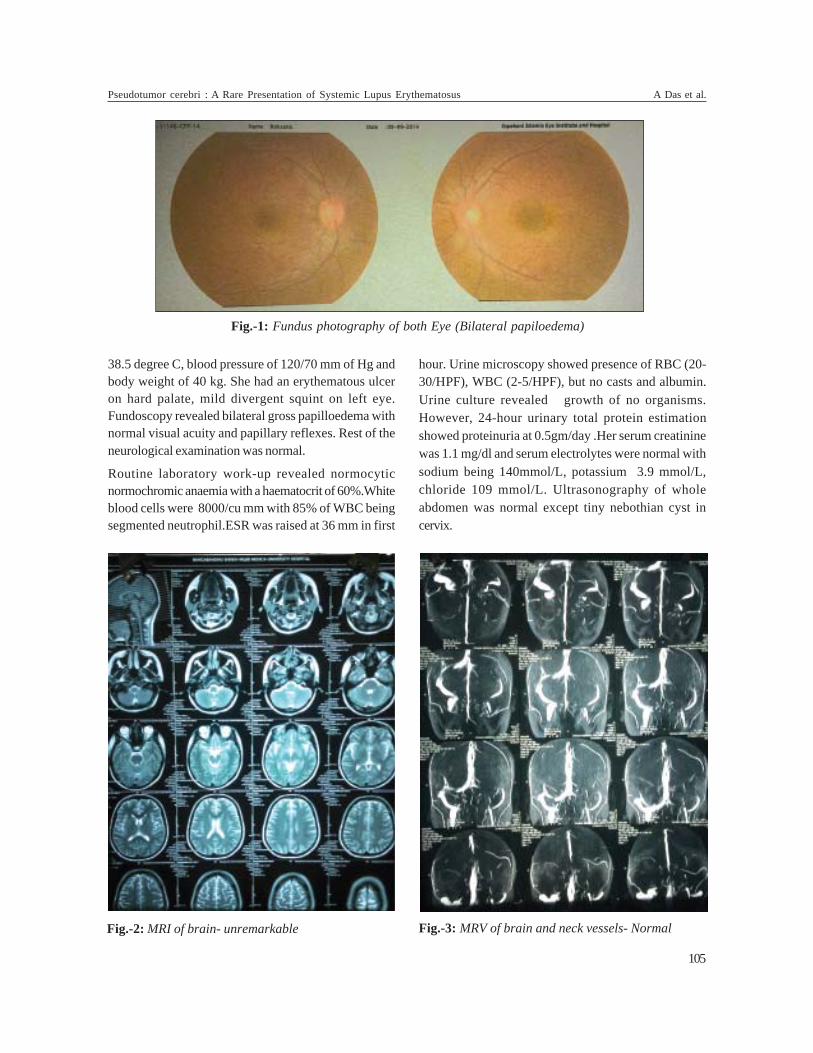
38.5 degree C, blood pressure of 120/70 mm of Hg andbody weight of 40 kg. She had an erythematous ulceron hard palate, mild divergent squint on left eye.Fundoscopy revealed bilateral gross papilloedema withnormal visual acuity and papillary reflexes. Rest of theneurological examination was normal.
Routine laboratory work-up revealed normocyticnormochromic anaemia with a haematocrit of 60%.Whiteblood cells were 8000/cu mm with 85% of WBC beingsegmented neutrophil.ESR was raised at 36 mm in first
hour. Urine microscopy showed presence of RBC (20-30/HPF), WBC (2-5/HPF), but no casts and albumin.Urine culture revealed growth of no organisms.However, 24-hour urinary total protein estimationshowed proteinuria at 0.5gm/day .Her serum creatininewas 1.1 mg/dl and serum electrolytes were normal withsodium being 140mmol/L, potassium 3.9 mmol/L,chloride 109 mmol/L. Ultrasonography of wholeabdomen was normal except tiny nebothian cyst incervix.
Fig.-1: Fundus photography of both Eye (Bilateral papiloedema)
Fig.-3: MRV of brain and neck vessels- NormalFig.-2: MRI of brain- unremarkable
Pseudotumor cerebri : A Rare Presentation of Systemic Lupus Erythematosus A Das et al.
105

Further work-up revealed highly positive anti-nuclearantibodies (ANA),with a titre at 37 U/ml, with coarsespeckled; anti double-stranded DNA (ds-DNA) with titreat 136.7U/ml(normal<2U/ml).Serum C3 and C4 werereduced at 0.286g/L and 0.087g/L respectively.Antiphospholipid antibody was negative.Rheumatoidfactor was negative. Neuro-imaging of brain with MRIshowed no abnormality and magnetic resonancevenography (MRV) was normal with no evidence ofcerebral venous sinus thrombosis. Subsequently, alumber puncture revealed an opening pressure of 42 cmof H2O with a normal haemato-cytological and chemicalcomposition with WBC being 02/cu mm, plenty of RBC,protein concentration of 3 mg/dl and glucose level at2.8 mmol/L and it was negative on Gram and Z-N staining.
Discussion:According to the revised American College ofRheumatology (ACR) criteria 6 our patient wasdiagnosed with SLE with her oral ulceration, history ofepisodic joint pain, positive result for ANA and anti ds-DNA, microscopic haematuria (detected on RME) andproteinuria (detected on 24-hour urinary total proteinestimation).
Headache is a common symptom in SLE patients.Different types of headache may occur in SLE due tovarious underlying conditions. Pseudotumour cerebri(PTC) is a rare manifestation of neuropsychiatric SLEbut commonly presents with headache. Early detectionand treatment is important since it can lead to permanentvisual impairment ranging from 6 to 24 % of cases 7
(Data varies among different studies).
This patient fulfilled the modified Dandy criteria 4 forthe diagnosis of Pseudotumour cerebri (PTC) with signsof raised intracranial pressure (headache, bilateralpapilloedema); no localized findings on neurologicalexamination; normal neuro-diagnostic studies(brain MRIand MR venography) with no evidence of venousobstructive disease; raised intracranial pressuremeasured by lumber puncture (42 cm H2O); normalchemical and cytological composition of CSF; and noabnormality in consciousness leve l(alert and awakepatient) . Certain drugs (vitamin A, tetracyclines, nalidixicacid, nitrofurantoin, sulpha derivatives, lithium,phenytoin, indomethacin, oral contraceptive pills, andsteroids), endocrinological abnormalities (hypo- andhyperthyroidism, hypoparathyroidism, adrenal
insuffiency, Cushing’s syndrome) and hypertension areknown causes of Pseudotumour cerebri. She was noton above mentioned antibiotics and vitamins and didnot use oral contraceptive pills. Our patient did not haveany endocrinopathies.. She has never had hypertension(we also found normal blood pressure since admissionat our hospital). Corticosteroid therapy could not beimplicated because she was not receiving prednisoloneat the time of diagnosis of Pseudotumour cerebri.Therefore, we had to think of SLE as the cause of PTC inour patient.
However, the association of SLE and intracranialhypertension is still unclear. The proposed mechanismsinclude immune-mediated injury within the arachnoidvilli and consequent reduction in CSF absorption orprobable hypercoagulable state without overt vascularthrombosis giving rise to micro-obliteration of cerebralarteriolar and venous systems 8,9,10. Young females withserologically active lupus, severe form renal lesions,past history of arterial or venous thrombosis, andlaboratory evidence of procoagulant activity appearsto be at increased risk of raised intracranial pressure11.
Our patient had mild renal disease (RBC 20-30/HPF, 24-hour urinary total protein 0.5gm/day, no casts).She hadno past history of thrombosis. The antiphospholipidantibody (Ig M and Ig G) work-up was also negative.Therefore, Pseudotumour cerebri in this patient wasconsidered as a manifestation of neuropsychiatric SLE.Our patient, similar to other patients with SLE-associated pseudotumour cerebri 8, respondeddramatically to steroids (40 mg of oral prednisolone)with remission from her headache, resolution of bilateralpapilloedema, which is quite atypical for idiopathicintracranial hypertension.
Conclusion:In conclusion, we described a woman with SLE whopresented to us with fever and headache. Headache is acommon symptom in patients with neuropsychiatric SLE.Sometimes it can be the only presenting symptom.Therefore, Pseudotumour cerebri should be consideredin the differential diagnosis of headache in patients withSLE, and work-up of Pseudotumour cerebri shouldinclude screening for connective tissue diseases.
References:1. Mills JA. Systemic lupus erythematosus. New England
Journal of Medicine 1994; 330: 1871–9
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
106

2. Guwani Liyanage,H M D Herath.Pseudo tumour cerebri insystemic lupus erythemaosus.Srilanka Journal of ChildHealth 2008;37:59-60
3. Kesler A, Fattal-Valevski A. Idiopathic intracranialhypertension in the pediatric population. J Child Neurol2002; 17: 745-748.
4. Wall M. Idiopathic intracranial hypertension. Neurol Clin1991; 9: 73-95.
5. Bettman JW, Daroff RB, Sanders MD, Joyt WF.Papilledema and asymptomatic intracranial hypertensionin systemic lupus erythematosus. A fluoresceinangiographicstudy of resolving papilloedema. Arch Ophthalmol1968;80:189-93.
6. Tan EM, Cohen AS, Fries JF, et al. The 1982 revisedcriteria for the classification of systemic lupuserythematosus. Arthritis Rheum 1982; 25: 1271-1277.
7. Biousse V,Bruce BB, Newman NJ .Update on thepathophysiology and management of idiopathicintracranial hypertension. J Neurol Neurosurg Psychiatry.2012;83(5):488-94. doi: 10.1136/jnnp-2011-302029
8. Green L, Vinker S, Amital H, Amir T, Bar-Dayan Y, LeviY, et al. Pseudotumor cerebri in systemic lupuserythematosus. Semin Arthritis Rheum 1995;25:103-8.
9. Horoshovski D, Amital H, Katz M, ShoenfeldY.Pseudotumor cerebri in SLE. Clin Rheumatol1995;14:708-10.
10. Parnass SM, Goodwin JA, Patel DV, Levinson DJ, ReinhardJD. Dural sinus thrombosis: A mechanism for pseudotumorcerebri in systemic lupus erythematosus. J Rheumatol1987;14:152-5.
11. Nampoory MR, Johny KV, Gupta RK, Constandi JN, NairMP, al-Muzeiri I. Treatable intracranial hypertension inpatients with lupus nephritis. Lupus 1997;6:597-602.
Pseudotumor cerebri : A Rare Presentation of Systemic Lupus Erythematosus A Das et al.
107

Journal of Bangladesh College of Physicians and SurgeonsVol. 34, No. 2, April 2016
Summary:Isoprenaline is a beta-adrenergic agonist, used for the treatmentof cardiovascular emergencies like hypotensive shock or severbradycardia. This drug is not indicated to use in bolus form eitherintramuscularly or intravenously. Accidentally a 22 year oldpregnant woman was given an intramuscular injection of two
mg Isoprenaline. It was a lethal dose, fortunately the patientsurvived. This article narrated the events, the ECG changes,management and outcome of the patient and pregnancy.
Key words: Isoprenaline, overdose, side effects, treatment.
(J Bangladesh Coll Phys Surg 2016; 34: 108-111)
Accidental Intramuscular Isoprenaline inEarly Pregnancy: The Effects, Management
and OutcomeM MOSTAFIa, MA RAHMANb, MT MOLLICKc, MN HAQd, A RAFIe
a. Brig Gen Prof Mamun Mostafi, Head, Dept. of Medicine,Rangpur Medical College & CMH.
b. Maj Md AnisurRahman, Combined Military Hospital(CMH), Rangpur Cantonment, Rangpur.
c. Lt Col Md Torab Mollick, Combined Military Hospital(CMH), Rangpur Cantonment, Rangpur.
d. Lt Col Md Naimul Haq, Combined Military Hospital (CMH),Rangpur Cantonment, Rangpur.
e. Lt Col Ahmed Rafi, Combined Military Hospital (CMH),Rangpur Cantonment, Rangpur.
Address of Correspondence: Brig Gen Prof Mamun Mostafi,Head, Department of Medicine, Rangpur Army Medical Collegeand CMH Rangpur, E-mail: [email protected]: 19 October, 2014 Accepted: 7 February, 2016
Introduction:Isoprenaline is a synthetic sympathomimetic amine thatis structurally related to epinephrine. It is used for thetreatment of bradycardia, heart block, hypotensiveconditions and rarely for asthma. It is a non-selectivebeta-adrenergic agonist, used as intravenous infusion,oral, intranasal or subcutaneous. Therapeutic dose ofisoprenaline varies depending on indication of use. Theplasma half-life for isoprenaline is approximately twohours. Usually it is given in a dose of IV infusion 5 ìg/min initially, then doses of 2-20 ìg/min based on patient’sresponse. The lethal dose of isoprenaline is 10-50 ìg/kgbody weight (in animal). Overdose of isoprenaline maycause tachycardia, palpitations, angina, Adams-Stokesattacks, pulmonary edema, hypertension, hypotension,ventricular arrhythmias, dyspnea, nervousness,headache, dizziness, nausea, visual blurring, flushingof the skin, sweating, tremor, weakness, and pallor. Cardiotoxicity causing fatal outcome are ventriculartachycardia, ventricular fibrillation and cardiac asystole1.
However, lethal effects of isoprenaline toxicity can beminimized by propranolol infusion2.
Case report:A 22 old woman, wife of a soldier of Bangladesh Army,was admitted to Combined Military Hospital (CMH),Rangpur through emergency and casualty department,with 14 weeks’ history of amenorrhea, per vaginalbleeding and abdominal pain for three hours followingsexual intercourse. She also had symptoms of earlypregnancy like morning sickness. Clinically an averagebuilt lady weighing 48 kg, anxious, pale, pulse 96 beats/min, blood pressure 100/60 mm Hg, respiration 20breaths/min, temperature 980 F. Abdominal examinationshowed mild lower abdominal tenderness and per vaginalbloody discharge. She was diagnosed as a case ofthreatened abortion and subsequently it was confirmedby urine analysis and ultrasound of pelvic organs. Shewas managed by physical rest, intravenous fluid,sedatives and injection progesterone (proluten depot)intramuscular weekly (total 10 doses). On third day ofadmission she was advised discharge from the hospitalafter first dose of weekly injection progesterone.
Instead of injection progesterone, injection isoprenalineone ml (2 mg, about 41 ìg/kg weights) was givenintramuscular mistakenly by the duty nurse. It wasdiscovered by identifying the used ampoule ofisoprenaline injection.
Immediately after the injection, patient developedpalpitation, chest pain, breathlessness, profuse sweats,tremor, agitation, and restlessness. There was headache,dizziness, nausea, vomiting and visual blurring followedby drowsiness. Examination revealed cloudiness ofconsciousness, tachycardia with gallop; lungs wereclear. Patient was immediately shifted to intensive care

unit (ICU); her heart rate was 190 beats/min, bloodpressure 40/30 mm Hg, respiration 40 breaths/min therewas central cyanosis.12 lead electrocardiogram (ECG) could not be donebecause of restlessness, however she was on
continuous cardiac monitor and ECG tracings were availableinstantly. creatine phosphokinase (CPK), CK-MB and allother relevant investigations were conducted includingrandom blood sugar, serum electrolytes, renal function andliver function test, all of them were normal.
A- Isoprenaline and proluten depot injection vials; B, C, D, & E- ECG changes after intramuscular isoprenaline; F– ECG tracing after 12 hours.
Fig. Isoprenaline injection and ECG changes
Accidental Intramuscular Isoprenaline in Early Pregnancy, the Effects, Management M Mostafi et al.
109

She was advised intravenous propranolol, but couldnot be provided because of nonavailability in the localmarket. Oral Propranolol was started, 40 mg stat andtwo hourly. She was also treated with carotid massage,intravenous fluid, sedatives and intravenous omeprazolealong with high flow oxygen. She was on continuouscardiac monitoring and pulse oxymeter. Other parameterswere followed up continuously minute to minute. Patientdeveloped different types of ECG abnormalities (atrialtachycardias and VPC) as shown in the picture whichfinally returned to normal sinus rhythm.
After about four hours, patient’s blood pressureimproved (BP-70-90/30-50 mmHg), Pulse 130-100 beats/min, patient felt better, consciousness regained and chestwas clear. Patient gradually settled over 6-8 hours. Thereafter patient was stable heamodynamically and on fifthday patient was discharged from hospital without anyadverse outcome. Later on the patient had a normalvaginal delivery with a healthy male child.
Discussion:Isoprenaline is a non-selective beta-adrenergic agonist,by activating â1-receptors on the heart, it inducespositive chronotropic, dromotropic, and inotropiceffects. Isoprenaline’s effects on the cardiovascularsystem (non-selective) relate to its actions on cardiacâ1 receptors and â2 receptors on smooth muscle withinthe tunica media of arterioles. It has positive inotropicand chronotropic effects on the heart. Beta2-adrenoceptor stimulation in arteriolar smooth muscleinduces vasodilation. It’s inotropic and chronotropiceffects elevate systolic blood pressure, while itsvasodilatory effects tend to lower diastolic bloodpressure. The overall effect is to decrease mean arterialpressure due to the â2 receptor’s vasodilation3.
Isoprenaline toxicity has a historical background. Anepidemic of deaths within a group of individuals whowere being treated for asthma was detected between1963 and 1968 in Europe, and Australia. This was laterfound to be largely attributed to isoprenaline inhalerswhich were being used at five times the dose used inUSA and Canada. Shortly after realizing overdose ofthe drug was causing many deaths, the medication waswithdrawn and the number of asthmatics dying wasquickly decreased4. The exact cause of this increased
mortality was not known but it may be related to theexcessive use of aerosols containing isoprenaline5.Analysis of individual cases has shown that patientshave died suddenly and unexpectedly. Descriptions oftheir clinical state before death were understandablyscanty but found a marked tachycardia in their eightpatients; in one an electrocardiogram showed multipleectopic beats6-7.
The acute toxicity of isoprenaline cause a striking dropin blood pressure, and repeated large doses may resultin cardiac enlargement and focal myocarditis. Accidentaloverdosage of isoprenaline is evidenced mainly bytachycardia or other tachyarrhythmias, palpitations,angina, hypotension or hypertension1.
The effects of the intravenous injection of isoprenalineon heart rate and arterial pressure have been studied inanimals. The fatal dose of isoprenaline (10-50 ìg/kg)reduced arterial and pulse pressures. Ventricularfibrillation did not occur; death occurred from cardiacasystole. Death was produced in a similar way in animalswith hypoxaemia by giving four or five doses ofisoprenaline (2·5 ìg/kg) at five minutes intervals or bytwo doses of 25 ìg/kg. The final reduction in arterialpressure during a fatal response resulted from areduction in cardiac contractility9.
In case of accidental toxicity of isoprenaline patientshould be closely observed with cardiac rhythmmonitoring by ECG, monitoring of pulse, blood pressure,respiration, consciousness and arterial oxygensaturation by pulse oxymetry. The lethal effects ofisoprenaline could be prevented by intravenouspropranolol. The cardiac toxic effects of isoprenalinemay be potentiated by hypoxia. Intensive oxygentherapy is also required. It is not known whetherisoprenaline is dialyzable or not9.
In the reported patient the administered dose was veryhigh; about 41 ìg/kg, which is a lethal dose theoretically.It could be easier if injectable propranolol was available.In spite of that the success was possibly because ofyoung otherwise healthy heart, immediate attention andsubsequent management.
Extensive search in internet showed no case reportrelevant to accidental parental isoprenaline toxicity. Toour best knowledge it is the first published case reportof such toxicity in Bangladesh and probably in the world.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
110

Conclusion:Accidental drug overdose or toxicity is not uncommonin the medical institutions; human error is always there.A confession of the mistake, detecting the used drugsand an immediate appropriate intervention can save thelife in this dangerous and precarious situation.
References:1. Current medication information; Isoproterenol
Hydrochloride; The Daily Med; The US National Libraryof Medicine; ’http://dailymed.nlm.nih.gov/dailymed;Revised: 3/2013
2. Shanks, R.G. The effect of Propranolol, the cardiovascularresponses to isoprenaline, adrenaline and nor-adrenalinein the anaesthetized dog. Brit J. Pharmaco 26:322:1966
3. B. G. Katzung; Adrenoceptor activating & othersympathomimetic Drugs; Katzung Pharmacology, 9th
edition; Section II, Chapter 9; page 169- 199.
4. Pierce, Neil and Hensley, Michael J. “EpidemiologicStudies of Beta Agonists and Asthma Deaths”.Epidemiologic Studies 20 (2):1998.
5. Speizer. E.E, Heaf. P, Doll, R and Strange L,B. Observationon recent increase in mortality from asthma; Brith medjournal 1, 335-39; 30 October,1968
6. Greenberg MJ, Pines A. Pressurized Aerosols in Asthma.Br Med J. 1967 Mar 04;1(5539):a563–563
7. Investigation into use of drugs preceding death fromasthma, British med journal 1, 339-43, 30 October, 1968.
8. Harris, Wallard, Clyde D, Schoenfeld, Arnold M. Weisseren:Effects of adrenergic receptor activation and blockade onthe systolic pre-ejection period, heart rate and arterial pressurein man: The jourl of clini. invest, vol- 46, no- 11, 1967.
9. J. M. Collins, D. G. Mc Devitt, R. G. Shanks, and J. G.Swanton; The cardio-toxicity of isoprenaline duringhypoxia; British Journal of Pharmacology Volume 36,Issue 1, published online: 19 July 2012.
Accidental Intramuscular Isoprenaline in Early Pregnancy, the Effects, Management M Mostafi et al.
111

Summary:Isolated testicular tuberculosis without renal or pulmonaryinvolvement has not been reported much earlier. The case ofa young HIV negative patient with testicular tuberculosisand tuberculoma of brain has been presented. A 32 years oldnormotensive, non-diabetic farmer presented to emergencyfacility with sudden onset of severe headache, vertigo andvomiting that developed over 24 hours and mild pain,swelling of right hemiscrotum associated with low gradefever for last one month. On examination, patient wasconscious, oriented, pulse rate was 72/min, blood pressurewas recorded 130/80 mm Hg, body temperature was 99 degreeF, genital examination revealed swelling of righthemiscrotum with enlarged, firm and mildly tender righttestis. He refused full neurological examination due to severe
Journal of Bangladesh College of Physicians and SurgeonsVol. 34, No. 2, April 2016
headache and vertigo. MRI of brain revealed multiple, hyper-intense, ring-enhancing lesions over right cerebellarhemisphere and corpus callosum. Aspiration of scrotal fluidrevealed about 50 ml of yellowish pus, microbiologyconfirmed presence of few acid-fast-bacilli and plenty ofpus cells. FNAC from right testicular mass revealed presenceof granuloma and caseation necrosis. His chest X-ray andCSF analysis were normal, ESR was 20, USG of abdomen,hepatic and renal work-up was normal. Soon the patientwas started with category I antituberculosis drug along withintravenous steroids. An excellent symptomatic improvementdeveloped on 5th day of initiating drug therapy, he was closelymonitored and followed up after discharge. This case reportwas prepared with his full consent.
(J Bangladesh Coll Phys Surg 2016; 34: 112-114)
Testicular Tuberculosis with Tuberculoma of Brainin an HIV Negative Patient
M KHANOM
Address of Correspondence: Dr. Mehrunnissa Khanom,Assistant Professor, Department of Medicine, Southern MedicalCollege and Hospital, Chittagong.Received: 22 January, 2015 Accepted: 10 January, 2016
Introduction:Tuberculosis is one of the major health problems inBangladesh. Although genitourinary tuberculosis wasthe most common subtype of extra-pulmonarytuberculosis in the past, it has recently been reported toaccount for less than 0.5% of all patient with extra-pulmonary tuberculosis and 1.5% of pulmonarytuberculosis1, 2. 15% to 20% of extrapulmonarytuberculosis involves the CNS3. CNS involvementmanifests as meningitis, cerebritis, tuberculousabscesses or tuberculomas. Intracranial tuberculomasare a rare complication of tuberculosis occurring throughhematogenous spread from an extracranial source.Testicular tuberculosis with only intracranial spread isan even rarer finding and to the best of our knowledge,only one previous case has been reported in theliterature4.
Male genital TB can present as a testicular mass that isdifficult to differentiate from malignancy. Again,misdiagnosis of scrotal TB may lead to otherwiseavoidable epididymo-orchiectomy4. Clinical suspicionor recognition and prompt diagnosis are important
because early treatment can prevent patientdeterioration and lead to clinical improvement.
Case Report:A 32 years old normotensive, non-diabetic farmerpresented to emergency department with thecomplaints of sudden onset of severe headache,vertigo and vomiting that developed over preceding24 hours and rendered the patient unwilling to move.On close questioning, he mentioned about mild painand swelling of right hemiscrotum associated with lowgrade fever for last one month. There was no historyof cough, haemoptysis or abnormal urethral discharge.He was non-smoker, non-alcoholic and there was nohistory of substance abuse or high risk sexual behavior,he was happily married and had two children. Onexamination, patient was conscious, oriented, pulserate was 72/min, blood pressure was recorded 130/80mm Hg, body temperature was 99 degree F, genitalexamination revealed swelling of right hemiscrotumwith enlarged, firm and mildly tender right testes. Herefused full neurological examination due to severeheadache and vertigo, however, there was no neckstiffness, reflexes and fundus were normal. MRI ofbrain revealed multiple, smallring-like lesions over rightcerebellar hemisphere and corpus callosum (Fig. 1).USG of scrotum showed presence of fluid at right

hemiscrotum and multiple hypo-echoic lesions insideright testis (Fig. 2). Aspiration of scrotal fluid revealedabout 50 ml of yellowish pus, microbiology confirmedpresence of few acid-fast-bacilli and plenty of pus cells.FNAC from right testicular mass confirmed presenceof granuloma and central caseation necrosis (Fig. 3).His chest X-ray was normal. CSF analysis revealedtwo lymphocytes/high power field with normal protein,sugar levels and ADA level 3 IU/L. ESR was 20, USG ofabdomen, hepatic and renal work-up was normal, HIVstatus was negative. Serum levels of beta-HCG, AFP,LDH and PSA were normal. A diagnosis of testicular
tuberculosis with tuberculoma of brain was made. Soonthe patient was started with antituberculosis drugcategory I regimen according to national guideline fortuberculosis as well as intravenous steroids. Anexcellent symptomatic improvement developed on 5th
day of initiating drug therapy, he was discharged on9th day, when he was able to move independently. Hisfollow-up visit was on 20th day of initiating drug, itwas uneventful and revealed normal neurologicalfindings with decreased size of testicular lump. Patientwas re-assured and advised to continue anti-TB drug,the intravenous steroid was switched to oral to be
Fig.-1: MRI of brain showing multiple, hyper-intense ring-enhancing lesions at right cerebellar hemisphere andgenu of corpus callosum.
Fig.-2: USG of right testis (Arrows indicate outline of hypo-echoic lesions).
Testicular Tuberculosis with Tuberculoma of Brain in an HIV Negative Patient M Khanom et al.
113
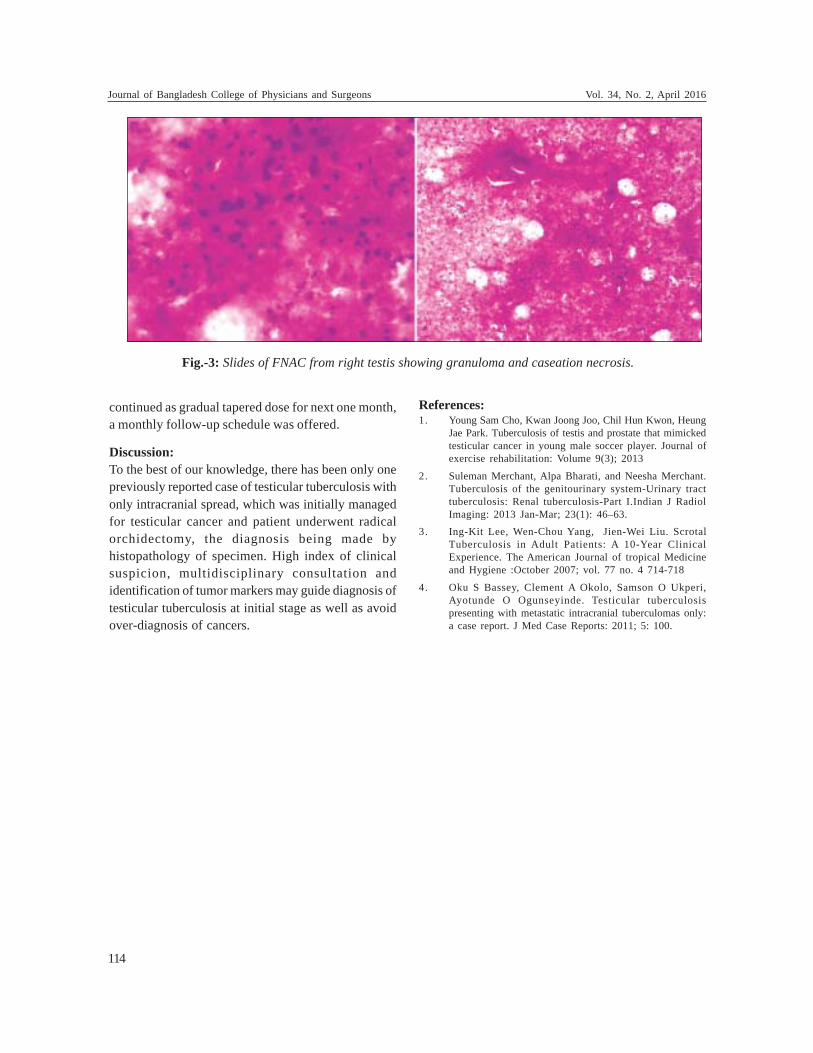
continued as gradual tapered dose for next one month,a monthly follow-up schedule was offered.
Discussion:To the best of our knowledge, there has been only onepreviously reported case of testicular tuberculosis withonly intracranial spread, which was initially managedfor testicular cancer and patient underwent radicalorchidectomy, the diagnosis being made byhistopathology of specimen. High index of clinicalsuspicion, multidisciplinary consultation andidentification of tumor markers may guide diagnosis oftesticular tuberculosis at initial stage as well as avoidover-diagnosis of cancers.
Fig.-3: Slides of FNAC from right testis showing granuloma and caseation necrosis.
References:1. Young Sam Cho, Kwan Joong Joo, Chil Hun Kwon, Heung
Jae Park. Tuberculosis of testis and prostate that mimickedtesticular cancer in young male soccer player. Journal ofexercise rehabilitation: Volume 9(3); 2013
2. Suleman Merchant, Alpa Bharati, and Neesha Merchant.Tuberculosis of the genitourinary system-Urinary tracttuberculosis: Renal tuberculosis-Part I.Indian J RadiolImaging: 2013 Jan-Mar; 23(1): 46–63.
3. Ing-Kit Lee, Wen-Chou Yang, Jien-Wei Liu. ScrotalTuberculosis in Adult Patients: A 10-Year ClinicalExperience. The American Journal of tropical Medicineand Hygiene :October 2007; vol. 77 no. 4 714-718
4. Oku S Bassey, Clement A Okolo, Samson O Ukperi,Ayotunde O Ogunseyinde. Testicular tuberculosispresenting with metastatic intracranial tuberculomas only:a case report. J Med Case Reports: 2011; 5: 100.
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
114

IMAGES IN MEDICAL PRACTICE
This 24 years old gentleman presented with A netlike,arborizing pattern on the anterior thighs and buttocksdefined by violaceous, erythematous streaks resemblinglightning. The skin within the erythematous areas waspale. On exposure to cold, lesions becomes morepronounced but never fades completely on warming1.There was no ulceration. There were no other physicalsymptoms and signs. There was no history ofdyslipidaemia or cardiovascular complication and hencesneddons syndrome is excluded.2 The investigationsruled out the connective tissue disease, vasculitis orhaematological diathesis. There was no drugs exposure
The Netlike Skin Lesion -Cutis Marmarota MR ISLAMa, MR AMINb
a. Dr. Mohammad Rafiqul Islam, Assistant Professor ofMedicine, Dhaka Medical College.
b. Dr. Md. Robed Amin, Associate Professor of Medicine,Dhaka Medical College.
Address of Correspondence: Dr. Mohammad Rafiqul Islam,Assistant Professor of Medicine, Dhaka Medical College.
Fig 1and 2: mottled bluish (livid) discoloration of the skin that occurs in a netlike pattern
like quinine or amantadine. The patient was diagnosedas a case of Idiopathic Livedo Reticularis3. The skincondition is also known as cutis marmorata3.Management is keep from chilling, Pentoxifylline (400mg PO three times a day), low-dose aspirin, and heparin.The patient was discharged without any complicationin hospital.
References:1. Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L.
(2007). Dermatology: 2-Volume Set. St. Louis: Mosby.p. 1615. ISBN 1-4160-2999-0.
2. Sneddon, I. B. (April 1965). “Cerebro-Vascular LesionsAnd Livedo Reticularis”. British Journal of Dermatology77 (4): 180–5. doi:10.1111/j.1365-2133. 1965. tb14628.x.PMID 14278790.
3. Klaus Wolff, Richard Ellen Johnson (2009).FitzpatricksColor atlas and synospsis of clinical dermatology, SixthEdition. Mcgraw Hill.p374.ISBN 978-0-07-163342-0
(J Bangladesh Coll Phys Surg 2016; 34: 115)

LETTER TO THE EDITOR(J Bangladesh Coll Phys Surg 2016; 34: 116-117)
ToEditor -in –ChiefJournal of Bangladesh College of Physicians andSurgeons.
Subject: A letter to the Editor on an article titled ‘MetabolicSyndrome in Bangladeshi Menopausal Women.’
Dear Sir,
I would like to thank you for publishing the article‘Metabolic Syndrome in Bangladeshi MenopausalWomen. -A Cross Sectional Study’ in your journal. I ama regular reader and analyzer of the journal ofBangladesh College of Physicians and Surgeons.Reading , analyzing and understanding of a journalarticle keeps us updated to the recent development inthe field of medicine. It also helps us to learn about thestandard format of scientific journal publication. Withthis aim I have gone through the above mentioned article.
I must thank and appreciate the authors for this crosssectional study on ‘Metabolic Syndrome in BangladeshiMenopausal Women’ because it is not very uncommonin Bangladeshi population and menopausal women areparticularly vulnerable to atherosclerosis due tometabolic syndrome leading to increased risk ofcoronary artery disease and cerebro- vascular accident.As I read this topic, I have experience some sorts ofdeficiencies in the study which I like to share with youand the authors. The topics of the study and objective,method, result analysis and conclusion were written inproper scientific way with a few deficiencies. Theintroduction was properly written.In the heading ofobjectives instead of ‘to assess the factors of metabolicsyndrome’ it may be appropriate to write ‘to assess thecomponents of metabolic syndrome’.
In the diagnostic criteria section in addition to thementioned five components of metabolic syndromethere are other components of metabolic syndrome,namely hyperurecemia, prothrombotic state withincreased levels of plasminogen activator inhibitor type1(PAI-1)and pro-inflammatory state, were not at allconsidered in this study. In the discussion section, theresults were compared with the international studies
very nicely and appropriately but whether any of thestudied patients have ever developed coronary arterydisease and cerebro-vascular accidents were notmentioned in the study.
In the end, I must thank and appreciate the authorsbecause of their hard work and appropriate way ofanalysis of the results of this study. The study is verymuch informative and give us updated knowledge tomanage this groups of patients. I would like to requestthem to be generous to accept my soft criticism on thetopic.
With regards
Dr. Md. Hafiz SarderAssociate ProfessorDepartment of MedicineDhaka Medical College
ToEditor -in –ChiefJournal of Bangladesh College of Physicians andSurgeons.
Subject: Response to the letter “to the Editor on anarticle titled ‘Metabolic Syndrome in BangladeshiMenopausal Women.’”
Dear sir,
This is very much appreciating that aforementionedarticle was reviewed by one of your regular readers. Wewant to thank him for his nice critic on the article.
Every study has some limitation which enables us toconduct further study to reduce the gaps going throughthe limitations. We wanted to compare the factors thatcould be associated with the metabolic syndrome. Indoing so we followed the National Cholesterol EducationProgram (NCEP) Adult Treatment Panel (ATP) III criteriafor diagnosing Metabolic Syndrome (MetS). In thatcriteria, it was written that presence of whether any threeof five risk factors would enable a person designated asa candidate of MetS. Because our criteria was todiagnose MetS according to NCEP ATPIII criteria, we

didn’t include other components for the diagnosis. Andthis is also the reason we didn’t write ‘components ofmetabolic syndrome’ instead of factors related withmetabolic syndrome.
In the discussion, development of coronary heartdisease and cerebro-vascular accident were notmentioned because it was not also our objective of study.But nonetheless it can be called a limitation of ourresearch. We really value the comment of our eruditereader which will lead us to carefully work with thescientific aspects of this kind of research work.
The other comments on deficiencies could not beaddressed as those were not specific.
Thanking again for the valuable comments. We lookforward to learn more from the expert comments.
Best regards.
Dr. Muna Shalima JahanAssociate ProfessorDepartment of Gynae and ObsSSMC
Letter to the Editor
117

COLLEGE NEWS(J Bangladesh Coll Phys Surg 2016; 34: 118-123)
College news Examinations news: Results of FCPS Part-I, Part-II and MCPS examination held in January are givenbellow:4377 candidates appeared in FCPS Part-I, examinatin held in Januuary, 2016 of which 465 candidates came outsuccessful.Subject wise results are as follows:Result of FCPS Part-I Examination (January, 2016)
Roll No. Name Subject From where graduated
The following candidates satisfied the Board of Examiners and are declared to have passed the FCPS - II Examinationsheld in January, 2016 subject to confirmation by the council of Bangladesh College of Physicians and Surgeons
SL. No. Subject January-16
Total Candidate Total Passed Percentage
1. Anaesthesiology 152 14 9.212. Biochemistry 8 1 12.503. Dentistry 286 63 22.034. Dermatology & Venereology 56 3 5.365. Family Medicine 4 0 0.006. Haematology 15 2 13.337. Histopathology 26 3 11.548. Medicine 1316 39 2.969. Microbiology 24 3 12.5010. Obst. & Gynae 874 41 4.6911. Ophthalmology 126 13 10.3212. Otolaryngology 135 3 2.2213. Paediatrics 462 73 15.8014. Physical Medicine & Rehabilitation 32 13 40.6315. Psychiatry 16 2 12.5016. Radiology & Imaging 51 4 7.8417. Radiotherapy 46 9 19.5718. Surgery 748 179 23.93 Total 4377 465 10.62
110005 Mizanur Rahman Anaesthesiology Faridpur Medical College,Faridpur110007 Sultan Reza Anaesthesiology Jahurul Islam Medical College, Bajitpur110010 Mohammad Ashrafur Rahman Anaesthesiology Sir Salimullah Medical College, Dhaka110011 Zikrul Bashir Anaesthesiology Rangpur Medical College,Rangpur110012 Md. Nazmul Islam Anaesthesiology Chittagong Medical College, Chittagong150001 Dr. Md. Abdul Hannan Sheikh Conservative Dentistry and Endodontics Dhaka Dental College,Dhaka150002 Kamrun Nahar Conservative Dentistry and Endodontics City Dental College, Dhaka150004 Shamima Afroz Conservative Dentistry and Endodontics City Dental College, Dhaka160001 Meher Afsun Dermatology and Venereology Sir Salimullah Medical College, Dhaka
Roll No. Name Subject From where graduated
College News
119
160004 Dr. Muhammed Ashraful Dermatology and Venereology Chittagong Medical College, ChittagongAlam Bhuiyan
160005 Md. Shahjahan Siraj Dermatology and Venereology Mymensingh Medical College,Mymensingh
160009 Dhrubajyoti Roy Chowdhury Dermatology and Venereology Sher-E-Bangla Medical College, Barisal160010 Nandita Ghosh Dermatology and Venereology Rangpur Medical College, Rangpur160011 Parimal Kumar Sen Dermatology and Venereology Sher-E-Bangla Medical College, Barisal200001 Muhammad Kamruzzaman Haematology Sher-E-Bangla Medical College, Barisal200002 A.K.M Mynul Islam Haematology Chittagong Medical College, Chittagong200003 Muhammad Nurul Farhad Haematology MAG Osmani Medical College, Sylhet200007 Mohammad Abdullah Az Haematology Dhaka Medical College, Dhaka
Zubayer Khan200009 Tangia Muquith Haematology Sir Salimullah Medical College, Dhaka220001 Mohammad Sowkat Hossain Histopathology Comilla Medical College, Comilla240036 Ferdaus Ahammed Medicine Comilla Medical College, Comilla240051 F.M. Monjur Hasan Medicine Dhaka Medical College,Dhaka240064 Md. Maniruzzaman Sarkar Medicine Sir Salimullah Medical College, Dhaka240076 Md. Emran Hossain Medicine University of Science & Technology
Chittagong (USTC)240101 Md. Zahid Amin Medicine Dhaka Medical College, Dhaka240111 Md Yeanur Hossain Medicine Dhaka Medical College, Dhaka240120 Sayra Monir Medicine Dhaka Medical College, Dhaka240124 Quazi Tamjidul Islam Medicine Ibrahim Medical College, Dhaka240127 Dr. Muhammad Mustafa Faysal Medicine Mymensingh Medical College,
Mymensingh240131 Md Merazul Islam Shaikh Medicine Rajshahi Medical College, Rajshahi240133 Mohammad Shafiqullah Akbar Medicine MAG Osmani Medical College, Sylhet240155 Golam Sagir Medicine Rangpur Medical College, Rangpur240193 Mohammad Rashidul Hasan Medicine Sir Salimullah Medical College, Dhaka240216 Md. Shahadat Hossain Medicine Chittagong Medical College, Chittagong240229 Liton Kumar Roy Medicine Sher-E-Bangla Medical College, Barisal240244 Md Jubaidul Islam Medicine Rangpur Medical College, Rangpur240261 Mohammad Fakhrul Alam Medicine Dhaka Medical College, Dhaka240275 Abdullah-Al- Mamun Medicine Sir Salimullah Medical College, Dhaka240289 Mohammed Amdad Ullah Khan Medicine Sher-E-Bangla Medical College, Barisal240295 Subrata Kumar Paul Medicine Mymensingh Medical College,
Mymensingh240304 Md. Ashrafuzzaman Medicine Sir Salimullah Medical College, Dhaka240319 Md. Enamul Hoq Medicine MAG Osmani Medical College, Sylhet240325 Mohammed Masudul Medicine Khulna Medical College, Khulna
Hassan Khan240343 Md.Monoarul Alam Medicine Faridpur Medical College, Faridpur240431 Mohammad Shayekh Abdullah Medicine Dhaka Medical College, Dhaka240438 Dilruba Alam Medicine Chittagong Medical College, Chittagong240465 Md. Nazmul Islam Medicine Mymensingh Medical College,
Mymensingh300009 Mossammat Kulsum Akter Obst and Gynae Chittagong Medical College, Chittagong300018 Nahid Sultana Obst and Gynae MAG Osmani Medical College, Sylhet300054 Razia Parvin Obst and Gynae MAG Osmani Medical College, Sylhet300104 Sharmin Akhter Obst and Gynae Dhaka Medical College,Dhaka300105 Ashutosh Deb Sharma Obst and Gynae Mymensingh Medical College,
Mymensingh

Roll No. Name Subject From where graduated
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
120
300111 Lubna Jahan Obst and Gynae Bangladesh Medical College, Dhaka300127 Dr. Amina Khatun Obst and Gynae Rajshahi Medical College, Rajshahi300128 Snigdha Chakraborty Obst and Gynae Sher-E-Bangla Medical College, Barisal300130 Tahmina Sharmin Obst and Gynae Mymensingh Medical College,
Mymensingh300145 Murshida Khatun Obst and Gynae Dhaka Medical College, Dhaka300192 Jesmeen Akhtar Obst and Gynae Z.H. Sikder Women’s Medical College,
Dhaka300201 Tania Noor Obst and Gynae Medical College for Women and
Hospital, Dhaka300224 Sabnam Sultana Obst and Gynae Sher-E-Bangla Medical College, Barisal300229 Khadija Mannan Obst and Gynae Mymensingh Medical College,
Mymensingh300262 Atisha Rabbi Obst and Gynae Sir Salimullah Medical College, Dhaka300286 Aklima Zakaria Zinan Obst and Gynae Dhaka Medical College, Dhaka300290 Shahina Akther Obst and Gynae MAG Osmani Medical College, Sylhet300291 Nasrin Sultana Obst and Gynae Sir Salimullah Medical College, Dhaka300304 Mst. Wazira Shefat Jahan Obst and Gynae Dinajpur Medical College, Dinajpur300334 Luna Farhana Hoque Obst and Gynae Dhaka Medical College, Dhaka300352 Dr. Farzana Rahman Obst and Gynae Shaheed Ziaur Rahman Medical
College, Bogra300379 Shahnaz Akhtar Obst and Gynae Dhaka Medical College, Dhaka300384 Naznin Begum Obst and Gynae Rangpur Medical College, Rangpur300386 Dr. Tamanna Chowdhury Obst and Gynae Rajshahi Medical College, Rajshahi300393 Raffat Sultana Obst and Gynae Rangpur Medical College, Rangpur300397 Amatus Slam Nimmi Obst and Gynae Mymensingh Medical College,
Mymensingh300398 Fahmida Chowdhury Obst and Gynae Dinajpur Medical College, Dinajpur300400 Alif Laila Obst and Gynae Dhaka Medical College,Dhaka300413 Nasrin Sultana Obst and Gynae Mymensingh Medical College,
Mymensingh300430 Tahsin Islam Obst and Gynae Dhaka Medical College, Dhaka300431 Surayea Bul-Bul Obst and Gynae Dhaka Medical College, Dhaka300442 Jesmin Ara Obst and Gynae Shaheed Ziaur Rahman Medical
College, Bogra310001 Shamim Ara Yeasmin Ophthalmology Rajshahi Medical College, Rajshahi310002 Muliha Rahman Ophthalmology Chittagong Medical College, Chittagong310003 Dr. Nasima Aktar Ophthalmology Sir Salimullah Medical College, Dhaka310004 Mohammad Rashedul Hasan Ophthalmology Dhaka National Medical College, Dhaka310006 Nusrat Shahrin Ophthalmology MAG Osmani Medical College, Sylhet310007 Sattyajit Mondal Ophthalmology Rangpur Medical College, Rangpur310008 Ahsanul Huq Ophthalmology Rajshahi Medical College, Rajshahi310011 Tasmia Tahmid Ophthalmology Chittagong Medical College, Chittagong310012 Sujit Kumar Sarker Ophthalmology Sher-E-Bangla Medical College, Barisal310015 Md.Ibrahim Khalilullah Ophthalmology Rangpur Medical College, Rangpur310017 Anisur Rahman Khan Ophthalmology Rajshahi Medical College, Rajshahi310019 Sheikh Md. Arafat Rahman Ophthalmology Rajshahi Medical College, Rajshahi310020 Md. Zakir Hossain Ophthalmology Sir Salimullah Medical College, Dhaka310021 Klaara Salmin Sattar Ophthalmology Rajshahi Medical College, Rajshahi310022 Mohammad Mazharul Islam Ophthalmology Rajshahi Medical College, Rajshahi310024 Rumana Tussie Ophthalmology Rajshahi Medical College, Rajshahi

Roll No. Name Subject From where graduated
College News
121
310025 Umme Qulsum Ophthalmology MAG Osmani Medical College, Sylhet310026 Md. Linkon Akhter Ophthalmology Rangpur Medical College, Rangpur310032 Tanima Roy Ophthalmology Chittagong Medical College, Chittagong320004 Shaikh Ahmed Oral and Maxillofacial Surgery Chittagong Medical College, Chittagong320011 Aminul Haque Oral and Maxillofacial Surgery Sappro Dental College, Dhaka330001 Imtiaz Ershadul Haque Orthodontics and Dentofacial Orthopaedics Dhaka Dental College, Dhaka330005 S. M. Omar Faruk Orthodontics and Dentofacial Orthopaedics Dhaka Dental College, Dhaka330006 Kohinur Akther Orthodontics and Dentofacial Orthopaedics Pioneer Dental College, Dhaka330011 Kazi Mafruhah Orthodontics and Dentofacial Orthopaedics Dhaka Dental College, Dhaka330015 Muhammad Mahdee Hasan Orthodontics and Dentofacial Orthopaedics Dhaka Dental College, Dhaka330016 Nazmul Hasan Chowdhury Orthodontics and Dentofacial Orthopaedics City Dental College, Dhaka350004 Md. Baha Uddin Otolaryngology Dhaka Medical College,Dhaka350007 Nazmul Hossain Chowdhury Otolaryngology Bangladesh Medical College, Dhaka350008 Muhammad Saleh Akram Otolaryngology Armed Forces Medical College, Dhaka350010 Mohammad Anamul Haque Otolaryngology Rangpur Medical College, Rangpur350015 Mohammad Harun-Or-Rashid Otolaryngology Rangpur Medical College, Rangpur350016 K.M. Reza-Ul-Haq Otolaryngology Community Based Medical College,
Mymensingh350017 Bhuiyan A.R.M. Shoyeb Otolaryngology Jahurul Islam Medical College, Bajitpur350021 Md. Khaled Shahrear Otolaryngology Khulna Medical College, Khulna350023 Mohammed Sirazul Islam Otolaryngology Sir Salimullah Medical College, Dhaka350025 Muhammad Mozammal Haque Otolaryngology Rajshahi Medical College, Rajshahi390002 Mohammad Saiful Islam Paediatrics Chittagong Medical College, Chittagong390012 Ferdousi Hossain Poly Paediatrics Dhaka Medical College, Dhaka390055 Syeda Nafisa Islam Paediatrics Rangpur Medical College, Rangpur390060 Mahmuda Begum Paediatrics Sher-E-Bangla Medical College, Barisal390065 Md. Humayun Shahed Paediatrics Sher-E-Bangla Medical College, Barisal390068 Simul Mazumder Paediatrics Mymensingh Medical College,
Mymensingh390070 Kamrun Nahar Paediatrics Chittagong Medical College, Chittagong390086 Mohammed Jamal Uddin Paediatrics MAG Osmani Medical College, Sylhet390088 Md. Ashfaque Ahemmed Khan Paediatrics Sher-E-Bangla Medical College, Barisal390102 Farhana Haque Paediatrics Sir Salimullah Medical College, Dhaka390104 Dr. Nazma Parvin Shammy Paediatrics Sher-E-Bangla Medical College, Barisal390112 Anita Sarker Paediatrics Rajshahi Medical College, Rajshahi390124 Rashidul Hasan Paediatrics Sher-E-Bangla Medical College, Barisal390131 Gulshan Nigar Chaudhury Paediatrics Dhaka Medical College, Dhaka390133 Debabrata Roy Paediatrics Sher-E-Bangla Medical College, Barisal390136 Asma Akter Paediatrics Mymensingh Medical College,
Mymensingh390143 Md. Ramzan Ali Paediatrics Faridpur Medical College, Faridpur390165 Navila Ferdous Paediatrics Sher-E-Bangla Medical College, Barisal390168 Tahmina Ferdaus Paediatrics Sher-E-Bangla Medical College, Barisal390188 Dr. Md. Rokibul Islam Paediatrics Chittagong Medical College, Chittagong390195 Mohammad Kamruzzaman Paediatrics MAG Osmani Medical College, Sylhet390198 Dr Rifat Zaman Paediatrics Shaheed Ziaur Rahman Medical College,
Bogra400006 Mohammed Ahsanul Hoque Physical Medicine & Rehabilitation MAG Osmani Medical College, Sylhet400008 Asiful Haque Physical Medicine & Rehabilitation Shaheed Ziaur Rahman Medical College,
Bogra

Roll No. Name Subject From where graduated
Journal of Bangladesh College of Physicians and Surgeons Vol. 34, No. 2, April 2016
122
410003 Zaman Ummay Humayra Plastic and Reconstructive Surgery Dhaka Dental College, Dhaka420001 Dr. Md. Tariquzzaman Prosthodontics Rangpur Dental College, Rangpur420002 Shahnaj Begum Prosthodontics Mymensingh Medical College,
Mymensingh430002 Md Faruk Hossain Psychiatry Rangpur Medical College, Rangpur450001 Shamsun Nahar Radiology & Imaging Armed Forces Medical College, Dhaka450006 Tasnova Zerin Iqbal Radiology & Imaging Mymensingh Medical College,
Mymensingh450009 Shahedur Rahman Radiology & Imaging Sher-E-Bangla Medical College, Barisal460005 Anannya Sarkar Radiotherapy Rangpur Medical College, Rangpur460009 Md. Shariful Islam Radiotherapy Rajshahi Medical College, Rajshahi480010 Mst. Jesmen Nahar Surgery Sir Salimullah Medical College, Dhaka480061 Mohammad Saiful Islam Sharif Surgery MAG Osmani Medical College, Sylhet480072 Kalyan Kumar Saha Surgery Mymensingh Medical College,
Mymensingh480090 Mohammad Mustafizur Rahman Surgery Dhaka Medical College, Dhaka480091 Dr. Md. Rajibul Huque Surgery Dhaka Medical College,Dhaka480098 Subarna Islam Surgery Chittagong Medical College, Chittagong480100 Sultan Mahmud Surgery Rajshahi Medical College, Rajshahi480165 Md. Maniruzzaman Surgery Sir Salimullah Medical College, Dhaka480179 Golam Mustafa Surgery Rangpur Medical College, Rangpur480181 Md. Rezaul Alam Surgery Armed Forces Medical College, Dhaka480184 Sanjeeda Saad Surgery Rajshahi Medical College, Rajshahi480241 Md Rezwonul Haque Surgery Rajshahi Medical College, Rajshahi480251 Suzon Kumar Mazumder Surgery Sir Salimullah Medical College, Dhaka500007 Md. Towhid Belal Urology Dhaka Medical College, Dhaka560001 Jannatul Ferdous Gynaecological Oncology Medical College for Women and
Hospital, Dhaka370001 Farhana Jalil Paediatric Nephrology Sir Salimullah Medical College, DhakaThe following candidates satisfied the Board of Examiners and are declared to have passed the MCPS Examinations held in January,2016 subject to confirmation by the council of Bangladesh College of Physicians and Surgeons
Roll No. Name Subject From where graduated
110004 Ilias Ahammad Anaesthesiology Mymensingh Medical College,Mymensingh
110006 Gobinda Kumar Saha Anaesthesiology Sher-E-Bangla Medical College, Barisal110008 Md.Waliullah Anaesthesiology Rangpur Medical College, Rangpur910001 Md. Husenuzzaman Chowdhury Clinical Pathology Armed Forces Medical College, Dhaka910002 Sharmin Akter Clinical Pathology Armed Forces Medical College, Dhaka910003 Umme Hani Clinical Pathology Armed Forces Medical College, Dhaka930003 Suraiya Islam Dina Dental Surgery Dhaka Dental College, Dhaka930004 K. S. M. Bayazid Dental Surgery Dhaka Dental College, Dhaka160004 Rokeya Begum Dermatology and Venereology MAG Osmani MedicalCollege, Sylhet160008 Armin Hasan Dermatology and Venereology Chittagong Medical College, Chittagong160009 Jannatun Nayeem Dermatology and Venereology Rajshahi Medical College, Rajshahi160010 Sharmin Jahan Dermatology and Venereology Sir Salimullah Medical College, Dhaka160016 Mohammad Saiful Islam Dermatology and Venereology Dhaka Medical College, Dhaka180001 Mohammad Refatul Islam Family Medicine Shaheed Ziaur Rahman Medical College,
Bogra920004 Jannatun Naiem Forensic Medicine Bangladesh Medical College, Dhaka
College News
123
920005 Sharmin Sultana Forensic Medicine Medical College for Women andHospital, Dhaka
240016 Mostofa Kamal Chowdhury Medicine Dhaka Medical College, Dhaka240037 Md. Reaz Uddin Chowdhury Medicine Sher-E-Bangla Medical College, Barisal240072 Issa Muhammad Baker Medicine Shaheed Ziaur Rahman Medical College,
Bogra240133 Pritish Tarafder Medicine Khulna Medical College, Khulna240151 S.M. Sajjadul Haq Medicine Rangpur Medical College, Rangpur240218 Tapan Seal Medicine Chittagong Medical College, Chittagong300023 Mousumi Majid Obst and Gynae Dhaka Medical College, Dhaka300034 Umme Rehnuma Tarannum Obst and Gynae Chittagong Medical College, Chittagong300046 Dr. Swapna Biswas Joy Obst and Gynae Dhaka Medical College, Dhaka300050 Shahnaz Mizan Obst and Gynae Chittagong Medical College, Chittagong300116 Tahura Akter Obst and Gynae Sher-E-Bangla Medical College, Barisal310002 S M Rejwan Raju Ophthalmology Dhaka Medical College, Dhaka310003 Most. Sanjida Akter Ophthalmology Rajshahi Medical College, Rajshahi310005 Sharah Rahman Ophthalmology MAG Osmani Medical College, Sylhet310015 Jannatul Ferdousy Ophthalmology Armed Forces Medical College, Dhaka350006 Munjure Khoda Md.Doulatullah Otolaryngology Dhaka Medical College, Dhaka350007 Dr. Nazmul Islam Otolaryngology Chittagong Medical College, Chittagong350009 Md. Azizul Hoque Manik Otolaryngology Mymensingh Medical College,
Mymensingh390008 Khaleda Begum Paediatrics Sir Salimullah Medical College, Dhaka390010 Nasren Akter Paediatrics Khulna Medical College, Khulna390023 Mohammad Abdur Rahman Paediatrics Sher-E-Bangla Medical College, Barisal430002 Bushra Sultana Psychiatry Dhaka Medical College, Dhaka450002 Taqarrob Abu Jafar Radiology & Imaging Armed Forces Medical College, Dhaka450003 Mohammad Sabbirul Huq Radiology & Imaging Armed Forces Medical College, Dhaka450006 Umme Iffat Siddiqua Radiology & Imaging Faridpur Medical College, Faridpur480026 U Than Kyow Surgery Dinajpur Medical College, Dinajpur480033 Eliza Sultana Surgery Rajshahi Medical College, Rajshahi480048 Khandaker Mominul Islam Surgery Rajshahi Medical College, Rajshahi480053 Kazi Mazharul Islam Surgery Dhaka Medical College, Dhaka110004 Ilias Ahammad Anaesthesiology Mymensingh Medical College,
Mymensingh110006 Gobinda Kumar Saha Anaesthesiology Sher-E-Bangla Medical College, Barisal110008 Md.Waliullah Anaesthesiology Rangpur Medical College, Rangpur910001 Md. Husenuzzaman Chowdhury Clinical Pathology Armed Forces Medical College, Dhaka910002 Sharmin Akter Clinical Pathology Armed Forces Medical College, Dhaka910003 Umme Hani Clinical Pathology Armed Forces Medical College, Dhaka930003 Suraiya Islam Dina Dental Surgery Dhaka Dental College, Dhaka930004 K. S. M. Bayazid Dental Surgery Dhaka Dental College, Dhaka
Roll No. Name Subject From where graduated

FROM THE DESK OF EDITOR in CHIEF(J Bangladesh Coll Phys Surg 2016; 34: 124)
Dear Fellows,
AssalamuAlaikum. We are stepping forward with timelypublication of our beloved journal. I am truly thankfulto the authors, the reviewers, the members of the editorialboard, the office staffs, the press and all concerned.Our endeavor for further improvement continues and Iwould request our honored reviewers to help us withtheir comments within time. So that we would be able togive feedback to the authors in time and they would beencouraged to produce high quality articles. Meanwhile
the editorial board is putting all out efforts to co-ordinatethe whole process to make accurately timed publicationof JBCPS. I am sure to have all your support thankfully.
Thank you.
Prof. Khan Abul Kalam AzadEditor-in-ChiefJournal of BCPS

The Fellows who died in 2016
(J Bangladesh Coll Phys Surg 2016; 34: 125)
Professor Rashiduddin Ahmed
Professor Rashiduddin Ahmed died on 19th March, 2016. He own FCPS withoutExamination in Neurosurgery in 1990 .
Professor A.N.M. Atai Rabbi
Professor A.N.M. Atai Rabbi died on 28thMay, 2016. He passed fellowship in Surgeryin July1972.