arc ureteral stones
DESCRIPTION
ureteral stone managementTRANSCRIPT
Clinical Practice Guidelines
The American Urological AssociationUreteral Stones Clinical Guidelines Panel
The Managementof Ureteral Calculi
Report onReport on
The Managementof Ureteral CalculiArchived Document—
For Reference Only
Ureteral Stones Clinical Guidelines Panel Members and Consultants
The Ureteral Stones Clinical Guidelines Panel consists of board-certified urologists who are ex-perts in stone disease. This Report on the Management of Ureteral Calculiwas extensively reviewedby nearly 50 urologists throughout the country in January 1997. The panel finalized its recommenda-tions for the American Urological Association (AUA) Practice Parameters, Guidelines and StandardsCommittee, chaired by Joseph W. Segura, M.D. in July 1997. The AUA Board of Directors approvedthese practice guidelines in August 1997.
The Summary Report also underwent independent scrutiny by the Editorial Board of the Journalof Urology, was accepted for publication in July 1997 and appeared in its November 1997 issue. ADoctor’s Guide for Patients and Evidence Working Papershave also been developed; both are avail-able from the AUA.
The American Urological Association expresses its gratitude for the dedication and leadershipdemonstrated by the members of the Ureteral Stones Clinical Guidelines Panel in producing thisguideline.
Members Consultants
ISBN 0-9649702-4-4
Joseph W. Segura, M.D., F.A.C.S.(Panel Chairman)The Carl Rosen Professor of UrologyDepartment of UrologyThe Mayo ClinicRochester, Minnesota
Glenn M. Preminger, M.D., F.A.C.S.(Panel Facilitator)Professor, Department of UrologyDuke University Medical CenterDurham, North Carolina
Dean G. Assimos, M.D., F.A.C.S.Associate Professor of Surgical SciencesDepartment of UrologyThe Bowman Gray School of MedicineWake Forest UniversityWinston-Salem, North Carolina
Stephen P. Dretler, M.D., F.A.C.S.Clinical Professor of SurgeryHarvard Medical SchoolDirector, Kidney Stone CenterMassachusetts General HospitalBoston, Massachusetts
Hanan S. Bell, Ph.D. (Consultant in Methodology)Seattle, Washington
Patrick M. Florer(Database Design andCoordination)
Dallas, Texas
Curtis Colby(Editor)Washington, D.C.
Robert I. Kahn, M.D., F.A.C.S.Chief of EndourologyCalifornia Pacific Medical CenterSan Francisco, California
James E. Lingeman, M.D., F.A.C.S.Director of ResearchMethodist Hospital Institute for Kidney Stone Disease
Associate Clinical Instructor in UrologyIndiana University School of MedicineIndianapolis, Indiana
Joseph N. Macaluso, Jr., M.D., F.A.C.S.Managing DirectorThe Urologic Institute of New OrleansAssociate Professor of Clinical UrologyLouisiana State University Medical Center School of Medicine
New Orleans, Louisiana
Archived Document— For Reference Only
Page iCopyright © 1997 American Urological Association, Inc.
Advances over the past two decades in urologic technology and interventionaltechniques have dramatically increased the available choices for management ofureteral calculi. As a consequence, however, questions have arisen regarding the se-lection of particular treatment modalities, taking into consideration such factors asthe size, location and composition of the stone and the presence or absence of infec-tion. To help clarify treatment issues, the American Urological Association (AUA)convened the Ureteral Stones Clinical Guidelines Panel and charged it with the taskof producing practice recommendations based primarily on outcomes evidence fromthe treatment literature. The result of the panel’s efforts is this Report on theManagement of Ureteral Calculi.
Recommendations in this report are to assist physicians specifically in treatmentof solitary stones within the ureter. Ureteral calculi present serious problems becausethey can cause severe flank pain (ureteral colic) and possible obstruction of the col-lecting system. They account for the majority of emergency room visits due to painfrom urinary tract stone disease. Therapeutic goals are to treat urinary tract infectionif present, to remove all stone material and to relieve obstruction without causingureteral damage.
The choice of treatment can be a source of controversy given the range of alterna-tive modalities now available, each with advantages and disadvantages—whichmakes ureteral calculi an especially appropriate subject for evidence-based recom-mendations. A summary of this report has been published in the Journal of Urology(November 1997). A Doctor’s Guide for Patientsand Evidence Working Papersareavailable for purchase through the AUA.
Introduction
Archived Document— For Reference Only
Page iiiCopyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Production and layout by
Joyce BrownLisa EmmonsTracy Kiely
Suzanne Boland PopeBetty Wagner
Copyright © 1997American Urological Association, Inc.
Archived Document— For Reference Only
To develop recommendations for treatment ofureteral calculi, the Ureteral Stones ClinicalGuidelines Panel reviewed the literature on ureter-al stones from 1966 to January 1996 and extractedand meta-analyzed all relevant data to estimate asaccurately as possible both desirable and undesir-able outcomes of alternative treatment modalities.The panel followed an explicit approach to the de-velopment of practice policy recommendations(Eddy, 1992). This approach emphasizes the useof scientific evidence in estimating outcomes. Ifthe evidence has limitations, the limitations areclearly stated. When panel opinion is necessary,the explicit approach calls for an explanation ofwhy it is necessary and/or discussion of the fac-tors considered. For a full description of themethodology, see Chapter 1.
Ureteral calculi are stones that usually form inthe renal collecting system, then progress downthe ureter. They tend to become lodged at siteswhere the ureter narrows. The three most commonentrapment sites are at the ureteropelvic junction,over the iliac vessels and at the ureteral meatus.
The composition of ureteral calculi varies, butmost stones are composed of calcium salts such ascalcium oxalate monohydrate and calcium oxalatedihydrate. Less common materials include cys-tine, uric acid and struvite. In size, stones varyfrom less than 2 mm to greater than 2 cm in diam-eter. The majority of stones are less than 4 mm inwidth, small enough to pass spontaneously inmost patients. A stone’s size is an important fac-tor—together with symptom severity, degree ofobstruction, the presence or absence of infectionand level of renal function—in deciding whetherto manage the stone initially by observation,awaiting spontaneous passage, or to intervene ac-tively.
Accepted alternatives for treating patients withureteral calculi can be grouped into five generalcategories:• Observation (also termed “expectant manage-
ment” and “watchful waiting”);
• Shock wave lithotripsy (SWL);
• Ureteroscopy (URS);
• Percutaneous nephrolithotomy (PNL); and
• Open surgery (referring to any method of opensurgical exposure of the ureter and removal ofstones).In addition, laparoscopy is used as a salvage
procedure in special circumstances, and there isthe traditional treatment alternative of blind bas-keting. However, as practiced with modern tech-niques using guide wires and fluoroscopic control,blind basketing is no longer “blind.”
ObservationAs noted above, the majority of ureteral stones
are small enough to pass spontaneously with acontrollable degree of patient discomfort. Forthese stones, observation is an obvious treatmentchoice. Drugs used to manage ureteral colic in theinterim before passage include narcotic analgesicsand nonsteroidal anti-inflammatory agents.
In deciding initially for or against active inter-vention, the size and location of the stone may beprime factors. Stones with a width of 5 mm orless have perhaps a 50 percent chance of sponta-neous passage if in the proximal ureter and asomewhat better chance if in the distal ureter.Accurate estimation of size may be a problem be-cause often a radiograph overestimates actualstone size and may also (about 15 percent of thetime) underestimate size (Otnes and Sandnes,1978).
However, size may not be the most importantfactor. If a patient is experiencing excruciating
Treatment methods
Background
Methodology
Page 1 Executive SummaryCopyright © 1997, American Urological Association, Inc.
Executive Summary –Report on the management of ureteral calculi
Archived Document— For Reference Only
Page 2 Executive Summary Copyright © 1997, American Urological Association, Inc.
pain, active intervention may be appropriate re-gardless of stone size. If urinary tract infection ispresent, the kidney is at risk for development ofpyelonephritis and/or pyonephrosis. Urgent inter-vention is indicated, again regardless of stonesize.
Another factor is degree of obstruction. At oneextreme, a patient with an asymptomatic stone inthe distal ureter not causing obstruction may beobserved for a year or more before the stone final-ly passes or a decision is made to choose an ac-tive treatment. At the other extreme—total ob-struction—renal function starts to deteriorate intwo weeks (Gillenwater, 1996). Also, a patientwith a solitary kidney and/or transplant kidneys orwith borderline renal function may not be able totolerate any degree of obstruction.
Shock wave lithotripsyShock wave lithotripsy (SWL) has become the
most frequently utilized method for active man-agement of calculi in the urinary tract (AppendixD, page 64). SWL is based on the principle that ahigh-pressure shock wave will release energywhen passing through areas of differing acousticimpedance. Shock waves generated outside thebody can be focused on a stone using a variety ofgeometric techniques. The shock wave passesthrough the body and releases its energy as itpasses into the stone. Thousands of such shockwaves may be required. The goal is to reduce thestone to particles small enough to pass withoutsignificant pain.
Shock wave lithotripsy has few short-termcomplications, its noninvasive nature has muchappeal and the technique is widely available.SWL does have disadvantages for management ofhard, dense stones not easily fragmented, such asthose made of calcium oxalate monohydrate.Also, because multiple treatments may be needed,SWL may not provide the required frequency ofservice if only mobile SWL is available and ancil-lary procedures may be necessary for manage-ment of fragments. Certain characteristics of indi-vidual patients, such as obesity or orthopedicproblems, may make these patients poor candi-dates for SWL.
UreteroscopyThe advent of ureteroscopy in the 1980s dra-
matically altered the management of symptomatic
ureteral calculi. Rigid ureteroscopy has been usedin conjunction with ultrasonic lithotripsy, electro-hydraulic lithotripsy (EHL), laser lithotripsy andpneumatic lithotripsy to successfully fragmentureteral calculi. Also, many stones can be re-moved with basket extraction under direct visionafter dilation of the intramural ureter.
Currently the three most commonly employedmethods for intracorporeal lithotripsy of ureteralstones, via the flexible, semirigid or rigid uretero-scope, are EHL, laser lithotripsy and pneumaticlithotripsy. Ultrasonic lithotripsy is occasionallyused for lower ureteral calculi, but its use hasbeen supplanted to a large extent by the abovethree methods.
Percutaneous stone removalPercutaneous nephrolithotomy (PNL), which
became popular as a primary technique for stoneremoval in the early 1980s, can theoretically beused for all stones. In practice, shock wavelithotripsy (SWL) and ureteroscopy (URS) arenow used in the majority of situations where PNLwas once employed to remove ureteral calculi.However, large stones or complex, impactedstones in the proximal ureter are often best man-aged by PNL.
PNL has unquestioned advantages: (1) If thestone can be seen, it can almost always be de-stroyed. (2) The ureter may be directly inspectedso that small fragments may be identified and re-moved. (3) The process is rapid, with success orfailure being obvious immediately.
One disadvantage is that the expertise requiredfor this operation is not as widely available as itonce was, because a greater number of urologytraining programs are focusing less on PNL andmore on shock wave lithotripsy and ureteroscopyfor stone management.
Open surgeryA variety of specific operations may be per-
formed in order to remove a ureteral calculus.Depending on anatomy and stone location, aureterolithotomy may be performed either througha flank, dorsal or anterior skin incision. However,standard ureterolithotomy is rarely performed to-day, except in cases of complex patient anatomyor large volume ureteral calculi. As of 1996, theincidence of open surgery for the treatment of all
Archived Document— For Reference Only
Page 3 Executive SummaryCopyright © 1997, American Urological Association, Inc.
stones was about 1 to 2 percent. In most cases, thesurgery was used to treat renal staghorn calculi.
Panel recommendations for the treatment ofureteral calculi apply to standard and nonstandardpatients as delineated by the following criteria:
The standard patient is defined as a nonpreg-nant adult:• who has a solitary ureteral stone composed of
material other than cystine or uric acid;
• who has not been previously treated for thisstone;
• whose medical condition, including renalfunctional status, body habitus and urinarytract anatomy, permit performance of any ofthe accepted active treatment modalities in-cluding use of anesthesia;
• whose situation is such that all acceptedmodalities are available and that permits useof any of these modalities.Nonstandard patientsare defined as prepu-
bescent children and other patients who do notmeet the above criteria delineating the standardpatient. For nonstandard patients, the choice ofavailable treatment options may be limited.
The terms “standard,” “guideline” and “op-tion,” as used in the panel’s recommendations, re-fer to the three levels of flexibility for practicepolicies defined in Chapter 1 (page 8). A standardis the least flexible of the three, a guideline moreflexible and an option the most flexible. Optionscan exist because of insufficient evidence or be-cause patient preferences are divided. In the lattercase particularly, the panel considered it importantto take into account likely preferences of individ-ual patients when selecting from among alterna-tive interventions.
The first three of the following recommenda-tions apply to both proximal and distal ureteralstones. Subsequent recommendations are catego-rized, first, by whether the stone is located in theproximal or distal ureter and, second, by whetherthe stone is 1 cm or less in diameter or greaterthan 1 cm in diameter. The proximal or upperureter is divided from the distal or lower ureter atthe point where the ureter narrows as it curvesover the iliac vessels.
Recommendation: For stones withlow probability of spontaneous passage
The decision that a stone has a low probabilityof spontaneous passage is based on both the factsof the case and professional experience. Factorsthat weigh in the decision are the size of thestone, the shape of the stone, the patient’s internalanatomy and the history of previous stone pas-sage. In general, patients whose stones are 0.5 cmor less in diameter have a good chance of sponta-neous passage, whereas the chance of sponta-neous passage for larger stones diminishes consid-erably.
Although, as a practical matter, it is evidentthat the availability of equipment and the exper-tise of an individual practitioner may affect thechoice of a treatment intervention, it is unaccept-able to withhold certain treatments from the pa-tient and not offer them as alternatives because ofpersonal inexperience or unfamiliarity with one ofthe accepted treatment modalities or because ofthe local unavailability of equipment or expertise.
Recommendation: For stones withhigh probability of spontaneouspassage
Guideline● In a patient who has a newly diagnosed
proximal or distal ureteral stone with ahigh probability of spontaneous passage,and whose symptoms are controlled, obser-vation with periodic evaluation is recom-mended for initial treatment.
Standard● A patient who has a ureteral stone with a
low probability of spontaneous passagemust be informed about the existing activetreatment modalities, including the relativebenefits and risks associated with eachmodality.
Treatment recommendations
(continued on page 6)
Archived Document— For Reference Only
Page 4 Executive Summary Copyright © 1997, American Urological Association, Inc.
Recommendations
For stones with low probability of spontaneous passage
Standard
A patient who has a ureteral stone with a low probability of spontaneous pas-sage must be informed about the existing active treatment modalities, includingthe relative benefits and risks associated with each modality.
For stones with high probability of spontaneous passage
Guideline
In a patient who has a newly diagnosed proximal or distal ureteral stone with ahigh probability of spontaneous passage, and whose symptoms are controlled,observation with periodic evaluation is recommended for initial treatment.
For treatment by shock wave lithotripsy
Guideline
Routine stenting to increase efficiency of fragmentation is not recommended aspart of shock wave lithotripsy.
For stones of 1 cm or less in proximal ureter
Standard
Open surgery should not be the first-line active treatment.
Guideline
Shock wave lithotripsy is recommended as first-line treatment for most patients.
(continued on next page)
Archived Document— For Reference Only
Page 5 Executive SummaryCopyright © 1997, American Urological Association, Inc.
Recommendations (continued)
For stones greater than 1 cm in proximal ureter
Guideline
Open surgery should not be the first-line treatment for most patients.
Option
Shock wave lithotripsy, percutaneous nephrolithotomy and ureteroscopy are allacceptable treatment choices.
For stones of 1 cm or less in distal ureter
Standard
Open surgery should not be the first-line treatment.
Guideline
Blind basketing without fluoroscopy and guide wire cannot be encouraged as atreatment choice.
Option
Shock wave lithotripsy and ureteroscopy are both acceptable treatment choices.
For stones greater than 1 cm in distal ureter
Standard
Blind basketing is not recommended as a treatment choice.
Guideline
Open surgery should not be the first-line treatment for most patients.
Option
Shock wave lithotripsy and ureteroscopy are both acceptable treatment choices.
Archived Document— For Reference Only
Page 6 Executive Summary Copyright © 1997, American Urological Association, Inc.
Up to 98 percent of stones less than 0.5 cm indiameter, especially in the distal ureter, may be ex-pected to pass spontaneously. How long until pas-sage occurs, over what period of time passagetakes place and the degree of colic or other symp-toms are all unpredictable and often bear heavilyon the decision to intervene in such patients. In thepanel’s opinion, for most of these patients the highprobability of spontaneous passage justifies obser-vation as the initial treatment. However, difficul-ties in tolerating pain, multiple trips to the emer-gency room or other factors may mandate treat-ment in a patient whose stone might otherwise beexpected to pass.
Recommendation: For treatment byshock wave lithotripsy
It has become common practice to place aureteral stent, usually a double-J stent, for moreefficient fragmentation of ureteral stones usingSWL. The data analyzed by the panel did not sup-port the routine use of such stents when the goal isto improve the stone-free results of SWL. The datashowed no improved fragmentation with stenting.Routine stenting may be justifiable for other pur-poses such as management of symptoms associat-ed with the passage of stones.
Recommendation: For stones of 1 cmor less in proximal ureter
Although open surgery will usually be success-ful, relatively longer hospitalization and greaterpostoperative morbidity with open surgery meanthat SWL should be the first-line treatment formost patients. Ureteroscopy and PNL are accept-
able choices in situations where SWL may not beappropriate or as salvage procedures for failedSWL.
Recommendation: For stones greaterthan 1 cm in proximal ureter
Treatment results for large stones in the upperureter are less predictable than for small stones.Shock wave lithotripsy, PNL and URS are all ac-ceptable options in the upper ureter, but URS maybecome less appropriate as the stones encounteredbecome larger. Open surgery, despite the excellentstone-free results, should not be the first-line treat-ment in most patients with large stones. The rea-sons are the same as for patients with small stones:relatively greater postoperative morbidity andlonger hospitalization. Open surgery may well beappropriate for nonstandard patients and is certain-ly an acceptable alternative as a salvage measure.
Recommendation: For stones of 1 cmor less in distal ureter
Blind basketing refers to basket manipulationof distal ureteral stones as practiced prior to theadvent of ureteroscopy and fluoroscopy around1981. The high success rates attending uretero-scopic stone removal utilizing fluoroscopic con-trol, the availability of fluoroscopy as an adjunc-tive measure and the lack of training in the vast
Standard: Open surgery should not be thefirst-line treatment.
Guideline: Blind basketing without fluo-roscopy and guide wire cannot be encouragedas a treatment choice.
Option: Shock wave lithotripsy andureteroscopy are both acceptable treatmentchoices.
Guideline: Open surgery should not bethe first-line treatment for most patients.
Option: Shock wave lithotripsy, percuta-neous nephrolithotomy and ureteroscopy areall acceptable treatment choices.
Standard: Open surgery should not be thefirst-line active treatment.
Guideline: Shock wave lithotripsy is rec-ommended as first-line treatment for most pa-tients.
Guideline: Routine stenting to increaseefficiency of fragmentation is not recom-mended as part of shock wave lithotripsy.
Archived Document— For Reference Only
Page 7 Executive SummaryCopyright © 1997, American Urological Association, Inc.
majority of programs in the technique of blindbasket extraction mean that blind basketing with-out fluoroscopy and safety guide wire cannot beencouraged as a treatment choice. The data fromthe literature suggest that blind basketing canachieve a 73-percent success rate. Nevertheless,the panel’s expert opinion is that guided stone ma-nipulation (concomitant use of fluoroscopy andsafety guide wire) or ureteroscopic basketingwould be a considerably safer and more effica-cious option.
Shock wave lithotripsy and URS are each ef-fective for management of distal ureteral stones.Each has advantages and disadvantages. Shockwave lithotripsy is minimally invasive and can of-ten be performed either without anesthesia or un-der intravenous sedation, but may require multipleprimary treatments for adequate fragmentationand is more likely to require ancillary treatment.
Ureteroscopy has a higher success rate, withthe least risk of requiring multiple treatments andthe least risk of an ancillary procedure, but ismore invasive than SWL. Although not studied bythe panel, cost issues will bear on the patient’s de-cision as to which treatment method is more ap-propriate. Availability is also a factor. Ureter-oscopy is widely available in the current era, as isSWL, although the availability of SWL will vary
according to whether practitioners are dependenton a mobile machine.
Recommendations: For stonesgreater than 1 cm in distal ureter
Large stones in the ureter must be fragmentedprior to ureteroscopic extraction, and SWL mustfragment large stones into passable fragments.Such stones will likely require more SWL treat-ments than will smaller stones, and URS may bepreferable when such cases can be anticipated.Given the high success rates using SWL andURS, open surgery should not be the first-linetreatment in most patients; but open surgery maybe preferable for certain very large ureteral stonesor in special situations.
Standard: Blind basketing is not recom-mended as a treatment choice.
Guideline: Open surgery should not bethe first-line treatment for most patients.
Option: Shock wave lithotripsy andureteroscopy are both acceptable treatmentchoices.
Archived Document— For Reference Only
Page 8 Copyright © 1997 American Urological Association, Inc.
The Ureteral Stones Clinical Guidelines Paneldeveloped the recommendations in this Report onthe Management of Ureteral Calculi utilizing anexplicit approach (Eddy, 1992), as opposed to anapproach relying solely on panel consensus with-out open description of the evidence considered.
The explicit approach attempts to arrive atpractice policy recommendations through mecha-nisms that systematically take into account rele-vant factors for making selections between alter-native interventions. Such factors include estima-tion of the outcomes from the interventions,consideration of patient preferences and assess-ment when possible of the relative priority of theinterventions for a share of limited health care re-sources. In estimating the outcomes of interven-tions, emphasis is placed on the use of scientificevidence. When panel opinion is necessary, theexplicit approach calls for explaining why it wasnecessary and/or discussion of the factors consid-ered.
To develop the recommendations in this report,the panel reviewed the literature on ureteral stonesand made an extensive effort to estimate as accu-rately as possible the outcomes of alternativetreatment modalities. For considering patient pref-erences, the panel members themselves served aspatient proxies.
The review of the evidence began with a litera-ture search and extraction of data as subsequentlydescribed on this page and on page 9. The dataavailable in the literature were displayed in evi-dence tables. From these tables, with referenceback to the original articles when necessary, thepanel developed estimates of outcomes for the fol-lowing treatment modalities: shock wave lithotrip-sy, percutaneous stone removal, open removal,blind basketing, ureteroscopy and observation.Other treatment alternatives such as chemolysiswere considered, but available evidence was insuf-ficient to yield outcome estimates. The panel usedthe FAST*PRO meta-analysis software packagedescribed on page 9 to combine the evidence from
the various studies. The resulting outcome esti-mates were arrayed for comparison in the out-comes balance sheet tables on pages 18–21.
The panel generated its recommendationsbased on the outcomes shown in the balance sheettables and on expert opinion. These recommenda-tions were graded according to three levels offlexibility as determined by strength of evidenceand the expected amount of variation in patientpreferences. The three levels of flexibility are de-fined as follows (Eddy, 1992):• Standard: A treatment policy is considered a
standard if the health and economic outcomesof the alternative interventions are sufficientlywell-known to permit meaningful decisionsand there is virtual unanimity about which in-tervention is preferred.
• Guideline: A policy is considered a guidelineif (1) the health and economic outcomes of theinterventions are sufficiently well-known topermit meaningful decisions and (2) an appre-ciable but not unanimous majority agree onwhich intervention is preferred.
• Option: A policy is considered an option if (1)the health and economic outcomes of the inter-ventions are not sufficiently well-known topermit meaningful decisions, (2) preferencesamong the outcomes are not known, (3) pa-tients’ preferences are divided among the alter-native interventions and/or (4) patients are in-different about the alternative interventions.A standard obviously has the least flexibility. A
guideline has significantly more flexibility, andoptions are the most flexible. As noted in theabove definition, options can exist because of in-sufficient evidence or because patient preferencesare divided. In the latter case particularly, the pan-el considered it important to take into accountlikely preferences of individual patients with re-gard to health outcomes when selecting fromamong alternative interventions. For this report,the panel did not consider economic outcomes.
Chapter 1 – Methodology
Archived Document— For Reference Only
Page 9Copyright © 1997 American Urological Association, Inc.
Three literature searches were performed usingthe MEDLINE database, the first one in Januaryof 1994. Retrieved were all articles related to uri-nary tract calculi published from 1966-1993. Twoupdate searches were performed, one in January1995 and the second in January 1996. These threesearches yielded a total of 1,698 articles. For rea-sons of practicality and validity, the panel decidedthat only English-language articles from peer-re-viewed journals would be used in the analysis. Allof the articles were imported into a Papyrus Bibli-ography System database (Research SoftwareDesign, Portland, Oregon).
The panel as a group then reviewed the ab-stracts and selected for data extraction the articlesrelevant to treatment of ureteral calculi. A total of526 were selected for extraction. The panel de-vised a comprehensive data extraction form tocapture as much pertinent information as possiblefrom each article. A sample of this form is inAppendix C.
The selected articles were divided among pan-el members, who reviewed the actual articles andtranscribed the data onto the forms. Each articlewas independently reviewed by two panel mem-bers who then consulted to reconcile any differ-ences. At this stage, 199 articles were rejected forreasons such as the following: (1) inadequatemethods, (2) lack of relevant data, (3) duplicationof data in a later article from the same source, (4)article not published in a peer-reviewed English-language publication, (5) lack of primary data (asin a review article). The net result was 327 articleswith acceptable outcomes data. All data were en-tered into an Access database (Microsoft, Red-mond, Washington). Entries were double-checkedat a later time.
The bar graph in Figure A-1 on page 47 cate-gorizes by year of publication the number of arti-cles retrieved from the literature, the number re-jected and the number accepted for data extrac-tion. Most articles used were published after 1986.The graph in Figure A-2 categorizes the articlesby source. The majority came from the Journal ofUrology, Urology, The Journal of EndourologyandThe British Journal of Urology.
The data resulting from the above processwere combined to generate the outcome probabili-ty estimates for alternative interventions displayedin the balance sheet tables on pages 18–21. Com-bining outcomes evidence from the literature inorder to generate probability estimates can be per-formed in a variety of ways depending on the na-ture and quality of the evidence. For example, ifthere were one good randomized controlled trial,the results of that one trial alone may be used inthe balance sheet. Other studies of significantlylesser quality may be ignored. For ureteral stones,however, none of the available randomized trialswas considered of sufficient quality to stand alonein the analysis.
If there are no studies of satisfactory qualityfor certain balance sheet cells or if the studiesfound are not commensurable, expert opinion maybe used to fill in those cells, they may be leftblank or “No data” may be indicated.
If a number of studies report data relevant to aparticular cell or cells, meta-analytic methods maybe used to combine the data from these studies toderive an overall estimate. Different specific meth-ods are available depending on the nature of theevidence. For this report, the panel elected to usethe Confidence Profile Method (Eddy 1989; Eddy,Hasselblad and Shachter, 1990), which allowsanalysis of data both from randomized controlledtrials and from single-arm studies that are not con-trolled. The FAST*PRO computer software pack-age (Eddy and Hasselblad, 1992) was used in theanalysis.
Although there are some randomized con-trolled trials for ureteral stones, none could beused in that form for this report because of prob-lems with the quality of the data. Therefore,FAST*PRO was used to combine the single armsfrom various clinical series to estimate outcomesfor each intervention. Frequently, the series thatwere combined showed very different results, im-plying site-to-site variations that may be causedby differences in patient populations, in how theintervention was performed or in the skill of thoseperforming the intervention. Because of the differ-ences, a random effects or hierarchical model wasused to combine studies for most outcomes.
Evidence combinationLiterature search, articleselection and data extraction
Archived Document— For Reference Only
Page 10 Copyright © 1997 American Urological Association, Inc.
Where outcomes were infrequent or if all serieshad comparable results, a fixed effects Bayesianmodel was used.
A random effects model assumes that for eachsite there is an underlying true rate for the out-come being assessed. It further assumes that thisunderlying rate varies from site to site. This site-to-site variation in the true rate is assumed to benormally distributed. The method of meta-analysisused in analyzing the ureteral stones data attemptsto determine this underlying distribution, which isused to estimate the effect on the population as awhole. In a fixed effects model, no site-to-sitevariation is assumed, and the studies are combinedto estimate the effect for the population as awhole.
The results of the Confidence Profile Methodare probability distributions. These can be de-scribed using a mean or median probability with aconfidence interval. In this report, the 95-percentconfidence interval (95% CI) is that interval suchthat the probability (Bayesian) of the true valuebeing outside the interval is 5 percent.
The results presented in this report have sever-al limitations. As mentioned previously, there arefew randomized controlled trials for ureteralstones. The data come mostly from uncontrolledclinical series. Because of wide variety in stonesize, composition and position, patient selectionbias is a major potential problem when using datafrom clinical series. Even when studies report theresults of several different interventions, the likeli-hood is high that the patients who received one in-tervention differed significantly from those whoreceived another intervention.
Another difficulty is negative publication bias.Studies with poor results are less likely to be pub-lished, either because they are never submitted forpublication or because they are rejected later.Consequently, analyses such as this one, based onpublished data, may be overestimating treatmentefficacy. On the other hand, in the case of newerinterventions, such as ureteroscopic techniques,the majority of the papers describe the authors’initial set of cases using the new technique.Because these papers represent early experience,
they may underestimate current efficacy as thetechniques have matured.
Variation in reporting complications presentsanother difficulty. Authors define and record com-plications differently. Some authors report eventhe most minor complications. Other authors failto report complications at all. If a complication israre and the panel analyzes only those papers thatreport the complication, the result will be a signif-icant overestimation of the frequency of that com-plication. The panel dealt with this problem by at-tempting to determine more appropriate denomi-nators for rare complications, but the possibility ofoverestimation still exists.
The potential exists for both overestimationand underestimation when individual complica-tions are combined into a category, such as the“significant” and “less significant” categories inthe tables on page 20, and probability estimatesare generated for the category. If multiple compli-cations occur in single patients and these compli-cations become part of the source data, the proba-bility estimate generated for that category will bean overestimation. If the source data come fromstudies in which authors did not report all thecomplications that occurred, therefore omittingsome that would be included in the category, theprobability estimate for that category will be anunderestimation.
Another problem stems from the fact that al-though authors group patients with ureteral stonesaccording to stone size, different authors use dif-ferent size categories. For example, one authormay divide patients into groups according towhether the stone is greater or less than 0.5 cm indiameter. Another author may use a different pointof division. Thus, studies could not always be reliably combined because their patient popula-tions differed based on the sizes included. Be-cause of such differences in reporting, it was notpossible to include all the relevant studies in a sin-gle meta-analysis. The problem was accentuatedwhen the panel attempted to determine the proba-bility of spontaneous passage for stones of varioussizes and location. Not only were stone sizes re-ported with different division points, but the timepoints for calculation of passage also varied. As aresult, the panel was unable to combine the resultsof spontaneous passage studies. (See further dis-cussion of limitations on pages 16–17 of Chapter3.)
LimitationsArchived Document— For Reference Only
Page 11Copyright © 1997 American Urological Association, Inc.
Chapter 2 – Ureteral calculi and their management
Ureteral calculi are stones that usually form inthe renal collecting system, then progress downthe ureter. They tend to become lodged at siteswhere the ureter narrows. The three most commonentrapment sites are at the ureteropelvic junction,over the iliac vessels and at the ureteral meatus.
With regard to stone location for the purposeof treatment, the ureter used to be divided intothirds. An upper section was demarcated from theureteropelvic junction to the upper edge of thesacrum, a middle section from the upper edge ofthe sacrum to the pelvic brim and a lower sectionfrom the pelvic brim to the ureteral orifice. Thisthree-part division was consistent with the differ-ent surgical approaches required to remove thestone—for example, a flank incision or a Foleymuscle-splitting incision for a stone in the upperureter or a high Gibson incision for a stone in themiddle section.
Today, however, open surgery is seldom per-formed to remove ureteral stones, except in spe-cial cases, surgery having given way to treatmentmethods such as extracorporeal shock wave litho-tripsy, ureteroscopy and percutaneous nephrolith-otomy. As a result, the ureter is now generally di-vided into two sections: the proximal or upperureter (combining the former middle and uppersections) and the distal or lower ureter. The pointof division is where the ureter curves over the ili-ac vessels and narrows, creating an impedimentfor the ureteroscope. Two-part division of theureter into proximal and distal sections is the sys-tem used in this report.
The composition of ureteral calculi varies, butmost stones are composed of calcium salts such ascalcium oxalate monohydrate, calcium oxalate di-hydrate and calcium phosphate. Less commonmaterials include cystine, uric acid and struvite.
A stone’s composition is one of the factors—together with location, size, degree of impaction,
shape, surface contour and other considerations—that may influence choice of treatment. A cystinecalculus in the distal ureter, for example, is usual-ly fragmented more effectively using an intracor-poreal endoscopic method than with extracorpore-al shock wave lithotripsy. Intracorporeal lithotrip-sy devices such as electrohydraulic lithotripsy,pneumatic lithotripsy and certain lasers (e.g.,Holmium and Alexandrite lasers) are effective infragmenting cystine. Coumarin green laserlithotripsy is ineffective because the translucentcystine does not absorb light. However, Tasca,Cecchetti, Zattoni, et al. (1993) used pulsed dyelaser lithotripsy to fragment cystine stones bycoating the stone with rifamycin, a red dye thatincreases the light absorption.
Some types of stone materials may be difficultto fragment into small passable pieces by anymethod. A notable example is calcium oxalatemonohydrate, which is both hard and dense. Fortreatment of distal stones made of such materials,ureteroscopic extraction with basket or forcepsmay be more effective than attempts at fragmenta-tion. By contrast, a calcium oxalate dihydratestone fragments easily and is usually a good can-didate for extracorporeal shock wave lithotripsy orany form of intracorporeal lithotripsy.
Ureteral calculi vary in size from less than 2mm to greater than 2 cm in diameter. The majori-ty of stones are less than 4 mm in width, smallenough to pass spontaneously in most patients. Astone’s size is an important factor—together withsymptom severity, degree of obstruction, the pres-ence or absence of infection and level of renalfunction—in deciding whether to manage thestone initially by observation, awaiting sponta-neous passage, or to intervene actively.
Accepted alternatives for treating patients withureteral calculi can be grouped into five generalcategories:
Treatment methods
Background: Stone location,composition and size
Archived Document— For Reference Only
• Observation (also termed “expectant manage-ment” and “watchful waiting”);
• Shock wave lithotripsy (SWL);
• Ureteroscopy (URS);
• Percutaneous nephrolithotomy (PNL); and
• Open surgery (referring to any method of opensurgical exposure of the ureter and removal ofstones)In addition, laparoscopy has recently been
used as a salvage procedure in special circum-stances (Fahlenkamp, Schonberger, Liebetruth, etal., 1994; Gaur, Agarwal, Purohit, et al., 1994).
There is also the traditional treatment alterna-tive of blind basketing. However, as practicedwith modern methods using guide wires and fluo-roscopic control, blind basketing is no longer“blind” and comparatively not the most effica-cious therapeutic choice. In the past, some excel-lent outcomes were achieved with blind basketingin expert hands. Today, other treatment methodsare available, especially SWL and URS, that inthe panel’s opinion are more efficacious and saferthan blind basketing even when the basket re-moval is augmented by fluoroscopy and guidewires.
Management by observationAs noted previously, the majority of ureteral
stones are small enough to pass spontaneouslywith a controllable degree of patient discomfort.For these stones, observation is an obvious treat-ment choice. Drugs used to manage ureteral colicin the interim before passage include narcoticanalgesics and nonsteroidal anti-inflammatoryagents.
Pharmacologic agents have also been used tofacilitate stone passage itself. In one randomized,double-blind, placebo-controlled study (Borghi,Meschi, Amato, et al., 1994), a calcium antagonist(nifedipine) was used together with a corticos-teroid (methylprednisolone) to facilitate sponta-neous ureteral stone passage. Engelstein, Kahanand Servadio (1992), in another randomized con-trolled study, used a terpenic essential oil prepara-tion, Rowatinex™, to facilitate spontaneous pas-sage. (Rowatinex™ has not been FDA approvedfor use in the United States.) The potential sideeffects of such medications are an important con-sideration if this kind of adjunctive therapy is uti-lized.
In deciding initially for or against active inter-vention, the size and location of the stone may beprime factors. Stones with a width of 5 mm orless have perhaps a 50-percent chance of sponta-neous passage if in the proximal ureter and asomewhat better chance if in the distal ureter.Accurate estimation of size may be a problem be-cause often a radiograph overestimates actualstone size and may also (about 15 percent of thetime) underestimate size (Otnes and Sandnes,1978).
However, size may not be the most importantfactor. If a patient is experiencing excruciatingpain, active intervention may be appropriate re-gardless of stone size. If urinary tract infection ispresent, the kidney is at risk for development ofpyelonephritis and/or pyonephrosis. Urgent inter-vention is indicated, again regardless of stonesize.
Another factor is degree of obstruction. At oneextreme, a patient with an asymptomatic stone inthe distal ureter not causing obstruction may beobserved for a year or more before the stone final-ly passes or a decision is made to choose an ac-tive treatment. At the other extreme—total ob-struction—renal function starts to deteriorate intwo weeks (Gillenwater, 1996). Also, a patientwith a solitary kidney and/or transplant kidneys orwith borderline renal function may not be able totolerate any degree of obstruction.
The patient’s employment could be a factor.For example, if a patient frequently travels longdistances or spends much time in foreign coun-tries, active treatment may be indicated for evenan asymptomatic ureteral stone.
Shock wave lithotripsyShock wave lithotripsy (SWL) has become the
most frequently utilized method for active man-agement of calculi in the urinary tract (AppendixD, page 64). SWL is based on the principle that ahigh-pressure shock wave will release energywhen passing through areas of differing acousticimpedance. Shock waves generated outside thebody can be focused onto a stone using a varietyof geometric techniques. The shock wave passesthrough the body and releases its energy as itpasses into the stone. Thousands of such shockwaves may be required. The goal is to reduce thestone to particles small enough to pass withoutsignificant pain.
Page 12 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 13Copyright © 1997 American Urological Association, Inc.
Many types of shock wave machines are avail-able today. Although they are all based on thesame general principle, they have significant dif-ferences with regard to treatment of ureteral cal-culi. The original machine, the Dornier HM-3,probably the most common machine throughoutthe world, has the largest focal point and, in itsunmodified version, the highest power of all cur-rent devices. However, with this machine, visual-izing stones in certain parts of the ureter is oftendifficult. In an effort to facilitate ureteral stonetargeting and reduce anesthesia requirements,newer machines were developed with smaller fo-cal points and improved fluoroscopic imaging.The trade-off is that stones treated with these“second-generation” and “third-generation” ma-chines often require more procedures to achievethe same result produced with fewer proceduresby other devices. Obviously, for large or hardstones, multiple treatments may be required.
Shock wave lithotripsy has few short-termcomplications, its noninvasive nature has muchappeal and the technique is widely available.SWL does have disadvantages as noted previouslyfor management of hard, dense stones not easilyfragmented such as those made of calcium oxalatemonohydrate. Also, because multiple treatmentsmay be needed, SWL may not provide the re-quired frequency of service if only mobile SWL isavailable and ancillary procedures may be neces-sary for management of fragments. Certain char-acteristics of individual patients, such as obesityor orthopedic problems, may make these patientspoor candidates for SWL.
Concerns have been raised too regarding theuse of SWL to treat distal ureteral calculi inwomen of childbearing age because of the theo-retical possibility that unfertilized eggs and/orovaries may be damaged. To date, no objectiveevidence has been discovered to support such con-cerns, but many centers require that women age40 or younger be fully informed of the possibilityand give their consent before treatment with SWL(Carrol and Shi, 1986; Chaussy and Fuchs, 1987;Erturk, Herrman and Cockett, 1993; Miller,Bachor and Hautmann, 1988; Vieweg, Weber,Miller, et al., 1992).
UreteroscopyThe advent of ureteroscopy in the 1980s dra-
matically altered the management of symptomaticureteral calculi. Rigid ureteroscopy has been used
in conjunction with ultrasonic lithotripsy, electro-hydraulic lithotripsy (EHL), laser lithotripsy andpneumatic lithotripsy to successfully fragmentureteral calculi (Beck, Vaughan and Sosa, 1989;Denstedt, Eberwein and Singh, 1992; Dretler,1990; Preminger and Roehrborn, 1989; Schulze,Haupt, Piergiovanni, et al., 1993). Also, manystones can be removed with basket extraction un-der direct vision after dilation of the intramuralureter.
Improvements in fiberoptics and irrigation sys-tems have fostered the use of smaller semirigidureteroscopes (6.9 to 8.5 F.). The introduction ofthe semirigid miniscope (Dretler and Cho, 1989)and the flexible deflectable ureteroscopes havemade access to the upper ureter and intrarenal col-lecting system a safer and less tedious procedure(Beck, Vaughan, and Sosa, 1989; Huffman, 1989;Preminger and Roehrborn, 1989). However, theextremely small working channel of the semirigidand flexible instruments, which ranges from 2.4 to4.0 F., has limited the size and usefulness of in-struments that can be passed through these ureter-oscopes and used for stone removal. Indeed, forlarger stones in the proximal ureter, the 3 F. bas-ket or grasping forceps are often inadequate to ac-complish successful stone extraction. The limita-tion of available instrumentation and the dangerof avulsion have prompted use of intracorporeallithotripsy for the management of larger upperureteral and intrarenal calculi.
Currently the three most commonly employedmethods for intracorporeal lithotripsy of ureteralstones, via the flexible, semirigid or rigid uretero-scope, are EHL, laser lithotripsy and pneumaticlithotripsy. Ultrasonic lithotripsy is occasionallyused for lower ureteral calculi, but its use hasbeen supplanted to a large extent by the abovethree methods. Although the choice of which typeof intracorporeal lithotripsy to employ is frequent-ly based on the location and composition of thestone to be treated, more often the experience ofthe clinician and availability of equipment dictatethis choice. (Intracorporeal lithotripsy methodsare described in detail on pages 67-69 ofAppendix D.)
Percutaneous stone removalPercutaneous nephrolithotomy (PNL), which
became popular as a primary technique for stoneremoval in the early 1980s (Appendix D, page69), can theoretically be used for all stones. In
Archived Document— For Reference Only
Page 14 Copyright © 1997 American Urological Association, Inc.
practice, shock wave lithotripsy (SWL) andureteroscopy (URS) are now used in the majorityof situations where PNL was once employed toremove ureteral calculi. However, large stones orcomplex, impacted stones in the proximal ureterare often best managed by PNL.
The procedure may be divided into two parts,access and stone removal. To achieve percuta-neous access, the urologist or radiologist places asmall flexible guide wire, under fluoroscopic con-trol, through the patient’s flank into the kidneyand down the ureter. Care is taken to optimize theapproach to the kidney through an upper or mid-dle calyx access position so that the best approachto the ureter is obtained. Once access is achieved,the tract is dilated to 24-30 F. and a rigid or flexi-ble nephroscope or ureteroscope is introduced.Under direct vision, the stone may be removed in-tact or broken up (with some form of intracorpo-real lithotripsy) and the pieces removed.
PNL has unquestioned advantages: (1) If thestone can be seen, it can almost always be de-stroyed. (2) The ureter may be directly inspectedso that small fragments may be identified and re-moved. (3) The process is rapid, with success orfailure being obvious immediately.
Hospitalizations are usually 3 to 5 days, withmost patients returning to light activity after 1 to2 weeks. Transfusion rates for PNL in treatingureteral calculi vary from 2 to 6 percent. Retreat-ment rates, that is, the rate at which the instru-ment must be reinserted through the tract to re-move residual stones, vary from 10 percent insimple situations to 40-50 percent for more com-plicated problems. Stone-free rates of 75-90 per-cent are regularly achievable using PNL.
One disadvantage of PNL is that the expertiserequired for this operation is not as widely avail-
able as it once was, because a greater number ofurology training programs are focusing less onPNL and more on shock wave lithotripsy andureteroscopy for stone management.
Open surgeryA variety of specific operations may be per-
formed in order to remove a ureteral calculus.Depending on anatomy and stone location, aureterolithotomy may be performed either througha flank, dorsal or anterior skin incision. However,standard ureterolithotomy is rarely performed to-day, except in cases of complex patient anatomyor large volume ureteral calculi.
Hospitalization in current practice ranges from2 to 7 days. Average postoperative disability is 4to 6 weeks, based on the fact that a typical inci-sion has regained about 80 percent of its preoper-ative strength by then; but recent investigationsuggests that months may pass before many pa-tients feel completely normal (Assimos, Wrenn,Harrison, et al., 1991). As of 1996, the incidenceof open surgery for the treatment of all stones wasabout 1 to 2 percent. In most cases, the surgerywas used to treat renal staghorn calculi.
StentingAlthough not a major treatment option, ureter-
al stenting may play an important adjunctive rolein overall management of patients with ureteralstones. For example, patients with sepsis and as-sociated obstruction may require internal drainage(using a stent) or external drainage (using percuta-neous nephrostomy). Stents may also provide a“bail out” option in difficult interventions, as incases of impacted stones.
Archived Document— For Reference Only
Page 15Copyright © 1997 American Urological Association, Inc.
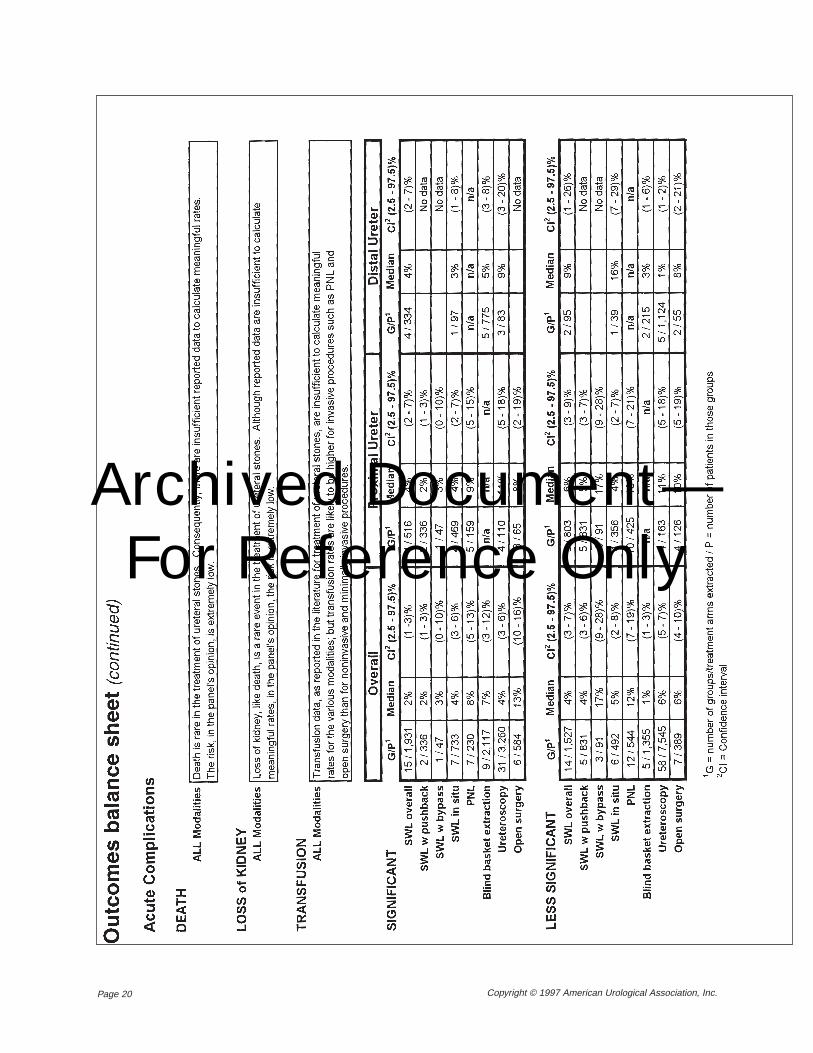
For purposes of comparative analysis, out-comes of a therapeutic medical intervention canbe categorized as either beneficial or harmful(Eddy, 1990, 1992). The Ureteral Stones ClinicalGuidelines Panel analyzed in detail available out-comes data for the main potential benefit (beingstone free) and the main potential harms (possiblecomplications) of alternative approaches to treat-ing ureteral stones. The panel also analyzed out-comes data for the number of primary and sec-ondary procedures per patient with each approach.
Results of the panel’s analysis are summarizedas probability estimates in the outcomes balancesheet tables on pages 18–21 and in the more de-tailed outcomes balance sheet tables on pages 48-62 of Appendix B. The data extraction and evi-dence combination processes that produced theprobability estimates are described on pages 9–10of Chapter 1. The evidence tables showing theraw data are available in the Evidence WorkingPapers for this report.
The outcomes balance sheet tablesThe term “balance sheet,” as applied to the
display of outcomes information, refers to a tableor tables that list “beneficial and harmful healthoutcomes and their magnitudes, including a rangeof uncertainty for each” (Eddy, 1992). This formof summary display, Eddy notes, allows the “si-multaneous consideration of all the important out-comes.”
The outcomes balance sheet tables on pages18–21 summarize results following ConfidenceProfile (FAST*PRO) meta-analyses of combinedoutcomes data from the ureteral calculi treatmentliterature. The meta-analytic process used is de-scribed in Chapter 1. Results are displayed in thetables as outcome probability estimates in theform of percentages. In most cases, a 95-percentconfidence interval (95% CI) is reported along
with a median probability. It should be noted that“median” in these tables is the median of theprobability distribution resulting from FAST*PROmeta-analysis (Eddy, Hasselblad and Shachter,1990). It is not the median of an array of individ-ual study results. A table’s G/P columns show thenumber of patient groups (G) for a given outcomeand the total number of patients (P) in thosegroups. A cell marked “No data” indicates insuffi-cient extractable data for a given outcome.
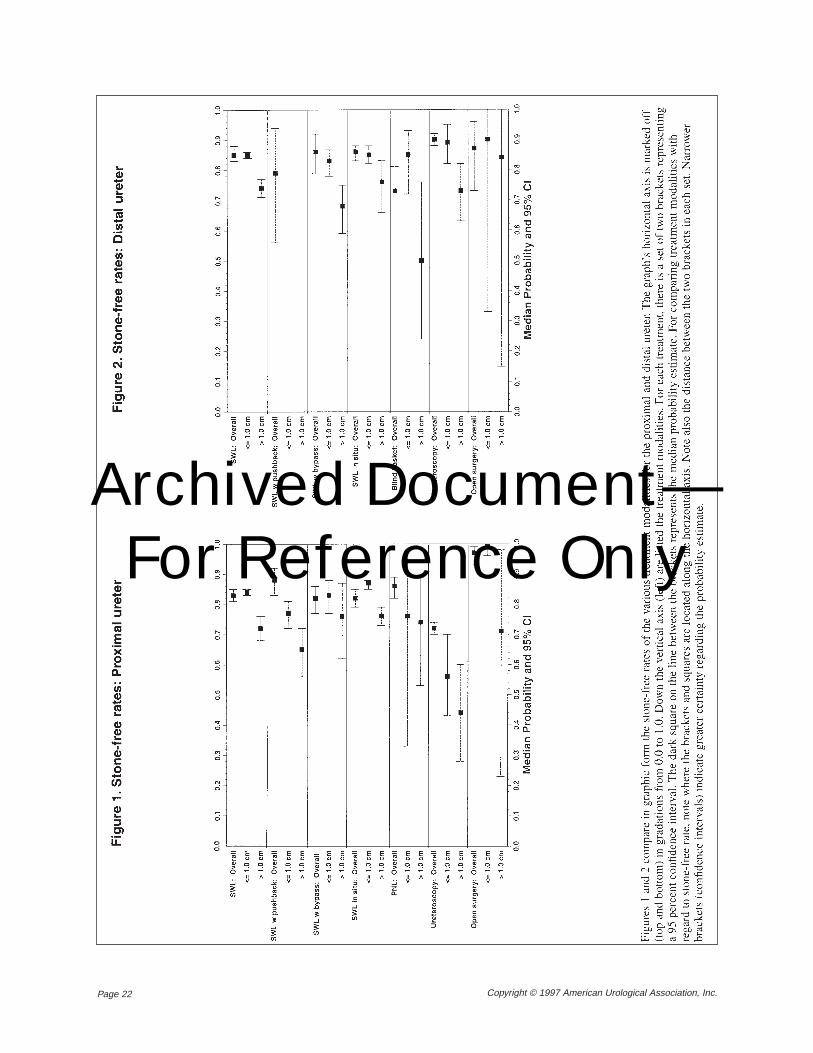
The three major types of probability estimatesin the tables mirror the three types of outcomesanalyzed by the panel: stone-free rate, number ofprimary and secondary procedures per patient andtreatment complications. The panel stratified alloutcomes by stone location in either the proximalor the distal ureter (see page 11 for definition).The tables therefore display probability estimatesseparately for the proximal ureter and the distalureter, either in separate tables or in two separatesets of columns within a table. Stone-free ratesand numbers of procedures per patient are furtherstratified in the tables by two categories of stonesize: less than or equal to 1.0 cm and greater than1.0 cm in diameter. Stone-free rates are also rep-resented graphically in Figures 1 and 2 on page22, stratified by both location and size. A third setof columns in each of the outcomes balance sheettables displays unstratified outcome probabilityestimates under the heading “Overall.”
The outcomes balance sheet tables provideoutcome probability estimates for the followingtreatment alternatives:• Extracorporeal shock wave lithotripsy (SWL);
• Ureteroscopy (URS);
• Percutaneous nephrolithotomy (PNL);
• Blind basket extraction;
• Open surgery; and
• Observation.The outcome estimates for blind basket extrac-
tion, in the tables for the distal ureter, are basedon data for basket manipulation of distal stoneswithout use of guide wires and fluoroscopic con-
Combined outcomes data
Chapter 3 – Outcomes analysis for ureteral calculitreatment alternatives
Archived Document— For Reference Only
Page 16 Copyright © 1997 American Urological Association, Inc.
trol. The panel does not recommend such “trulyblind” blind basketing (see pages 12 and 28).However, published data for basket extractionwith guide wires and fluoroscopy were insuffi-cient to generate outcome estimates for the bal-ance sheet.
There are also no outcome estimates in theoutcomes balance sheet tables for blind basketmanipulation of stones in the proximal ureter.Because of the high risk of morbidity, blind bas-keting is seldom used to extract proximal stonesand few data are available for this procedure. Forsimilar reasons, the balance sheet also omits out-come estimates for PNL in the distal ureter. PNLis rarely used to remove distal stones. The proce-dure has been used only in special circumstancessuch as for patients who have failed both SWLand URS or patients with a ureteral stricture distalto the stone that impedes passage of fragments orthe introduction of a ureteroscope.
For SWL, the panel stratified the outcome esti-mates by three specific treatment methods: (1)pushback (stone manipulation back into the renalcollecting system); (2) bypass of the stone with anexternalized or internalized stent; (3) in situ (withno ureteral manipulation). Estimates are displayedin the balance sheet’s SWL tables with a separaterow for each of these three methods. A fourth rowshows combined results for all methods.
URS results could not be stratified by type ofmethod—stone retrieval or intracorporeal litho-tripsy—because the designs of most URS studieswith extractable data would not permit such anal-ysis. Open surgery could not be stratified by inci-sional approach because the approach was too of-ten not specified. Laparoscopic ureterolithotomywas not included as a treatment alternative be-cause of the paucity of reported cases and thesmall number of urologists who routinely performlaparoscopic procedures. Similarly, only the re-sults from treating patients with single ureteralstones could be analyzed because of the paucityof data on treatment of patients with multiplestones.
SWL stone-free rates in the outcomes balancesheet tables are based on combined results fromboth mobile and fixed lithotripters. Studies byCass and by Mobley, Myers, Jenkins, et al. pro-duced results for the largest numbers of treatedpatients (see Table A-1 in Appendix A, Papyrusnumbers 3114, 3546, 3889, 5023 and 5369).These results were achieved by a large number oftreating physicians who performed SWL using
mobile lithotripters. Because of the large num-bers, the panel performed an analysis to assesswhether results reported in the Cass and Mobleystudies were different from results reported byother studies in which fixed lithotripsy sites wereused. The panel found overlap in most instancesand therefore decided to combine the data. Thepanel was unable to determine relative efficacy ofdifferent lithotripters, even though studies report-ing results employed a variety of devices, becausethe design of these studies did not permit a validcomparison.
Data regarding acute and long-term SWLcomplications were, for the most part, not report-ed from mobile sites. The panel therefore usedonly SWL data from fixed sites to generate proba-bility estimates for complications. Data wereavailable from mobile sites regarding primary andsecondary procedures per patient. However, theretreatment rate was significantly lower in the mo-bile site data as compared to the data from fixedsites. The panel felt this lower rate was the resultof the limited, intermittent availability of the mo-bile sites and decided to use only data from fixedsites in analyzing primary and secondary proce-dures per patient.
General limitations to combiningoutcomes data
Those outcome estimates in the outcomes bal-ance sheet tables with wide confidence intervalssuggest considerable uncertainty in the medicalknowledge base. One reason may be data limita-tions because of relatively few studies of a giventreatment alternative or because of few studies re-porting a given outcome directly. The short dura-tion of many studies introduces uncertainty aswell.
Two major reasons for outcome estimates withwide confidence intervals are: (1) wide variationsfrom study to study in reported incidence of cer-tain outcomes (such as acute complications) and(2) the wide variability in how studies have re-ported treatment data. For example, the definitionof ureteral calculi may differ significantly amongvarious investigators, and some of the reports donot specify such factors as the size of the stones.Thus, not all studies may be comparing treatmentoutcomes for stones of similar size, compositionor location within the ureter. In these cases, thepanel attempted to extrapolate from existing infor-mation to equate the treatment outcomes.
Archived Document— For Reference Only
Page 17Copyright © 1997 American Urological Association, Inc.
The combined analysis may be weakened tooby the quality of individual studies. As noted pre-viously, there are currently few randomized, con-trolled trials for treatment of ureteral calculi.Therefore, most of the data analyzed by the panelcame from clinical series. The limitations of in-cluding these types of studies are obvious. (Seethe discussion of limitations on page 10 of Chap-ter 1.) Yet, if clinical series were not included, lit-tle could be said about the benefits and harms ofvarious treatments for ureteral stones.
It should also be remembered that manage-ment of patients with ureteral stones is unique inthat the majority of patients with a “disease” (asymptomatic stone) are spontaneously “cured”(the stone passes). This fact and the fact that it isnot always possible to predict the behavior of thestone mean that the results of treatment could beinadvertently biased. In an extreme example,treatment with SWL of a series of stones less than4 mm in diameter would yield spectacular butmeaningless results.
Despite such limitations, the panel believesthat the confidence intervals contain the true prob-ability of a given outcome for most study sites.Better estimates, narrower confidence intervalsand greater certainty about treatment differencescan be obtained through large, well-controlledstudies that test different treatments in the samepatient population. However, until these types ofoutcome studies are completed, guidance can stillbe given to the physicians and patients who needto make decisions at the present time.
The following sections discuss the analysisused to generate the outcome probability esti-mates in the outcomes balance sheet tables. Theinformation is organized in relation to major typesof outcomes, beginning with stone-free rates. Asnoted previously (page 15), additional tables arecontained in Appendix B (pages 48-62) and in theEvidence Working Papers. These additional tablesinclude FAST*PRO analysis tables.
Stone-free rateIn the panel’s expert opinion, the stone-free
rate provides an objective outcome measure forevaluating the efficacy of treatment. Stone-freestatus is especially important for patients withureteral stones because residual fragments aremuch less likely to remain “clinically dormant” inthe ureter than are most fragments (other thanstruvite) remaining in the kidney.
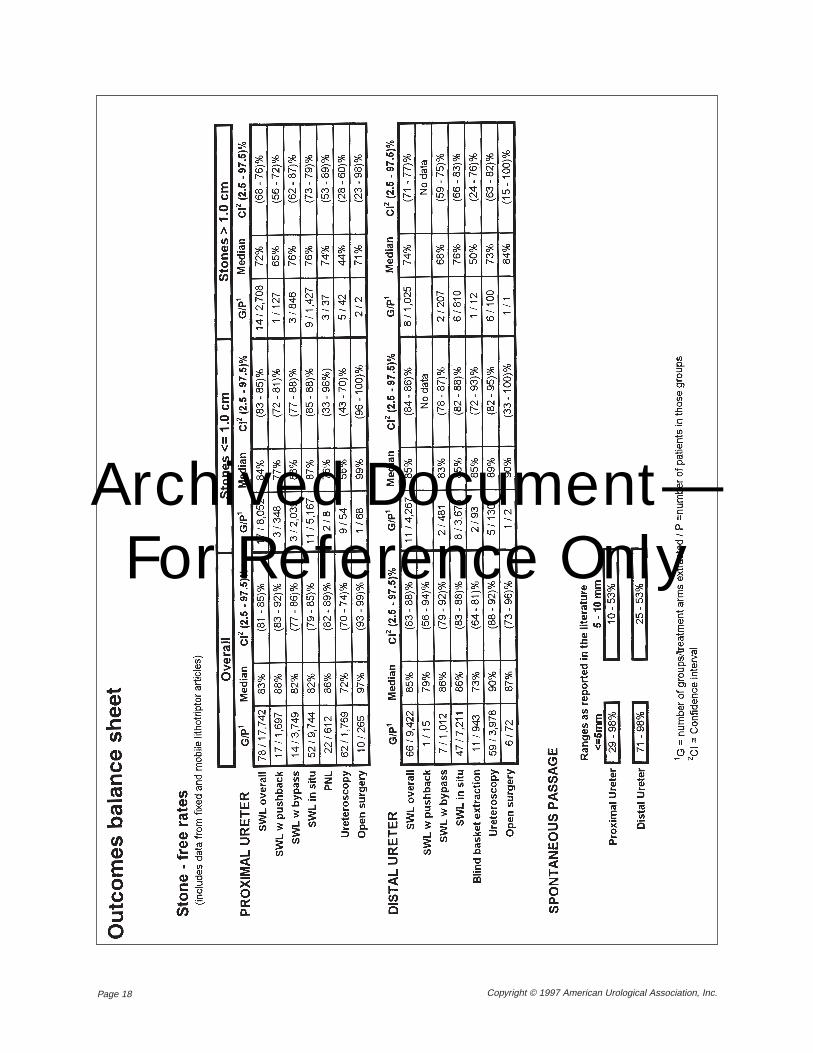
Estimated probabilities of being stone free af-ter SWL, URS, PNL, blind basket extraction andopen surgery are displayed in two balance sheettables on page 18, one for the proximal ureter andone for the distal ureter. The reported stone-freerates may be slightly overestimated because themajority of studies in the present analysis utilizedonly a plain abdominal radiograph (KUB) to as-sess stone-free status. This radiographic methodmay underestimate the incidence of residual frag-ments in the ureter. The degree of error, however,is not so high as when a KUB is used to detect re-nal fragments.
Each of the two balance sheet tables on page18 contains three categories of stone-free rates.Two of the categories stratify rates by stone size(≤ 1.0 cm and > 1.0 cm). The third is an “Overall”category that displays stone-free rates unstratifiedby stone size. The data used to generate stone-freerates in the “Overall” category came from manysources. These sources include the studies thatprovided stone-free data for the two size cate-gories, but they include many other studies aswell. This is evident from the much larger num-bers in the G/P column under “Overall.” Thus, thestone-free rates in the “Overall” category, basedpartly on different data, should be considered in-dependently from the stone-free rates categorizedby stone size.
To determine likelihood of being stone freewith management by observation rather than ac-tive intervention, the panel sought to combineavailable data on spontaneous passage and devel-op probability estimates in relation to such factorsas stone size and location. Unfortunately, becauseof differences in how results have been reportedin various studies, the available data were incom-patible and could not be combined. The studiesdiffered, for example, not only in their groupingsof patients by stone size, but in their time framesfor spontaneous passage.
Analysis of outcomes inbalance sheet tables
(continued on page 23)
Archived Document— For Reference Only
Page 18 Copyright © 1997 American Urological Association, Inc.
outcomes balance sheet starts on this page
Archived Document— For Reference Only
Page 19Copyright © 1997 American Urological Association, Inc.
outcomes balance sheet continues on thispage
Archived Document— For Reference Only
Page 20 Copyright © 1997 American Urological Association, Inc.
outcomes balance sheet continues on thispage
Archived Document— For Reference Only
Page 21Copyright © 1997 American Urological Association, Inc.
outcomes balance sheet continues on thispage
Archived Document— For Reference Only
Page 22 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 23Copyright © 1997 American Urological Association, Inc.
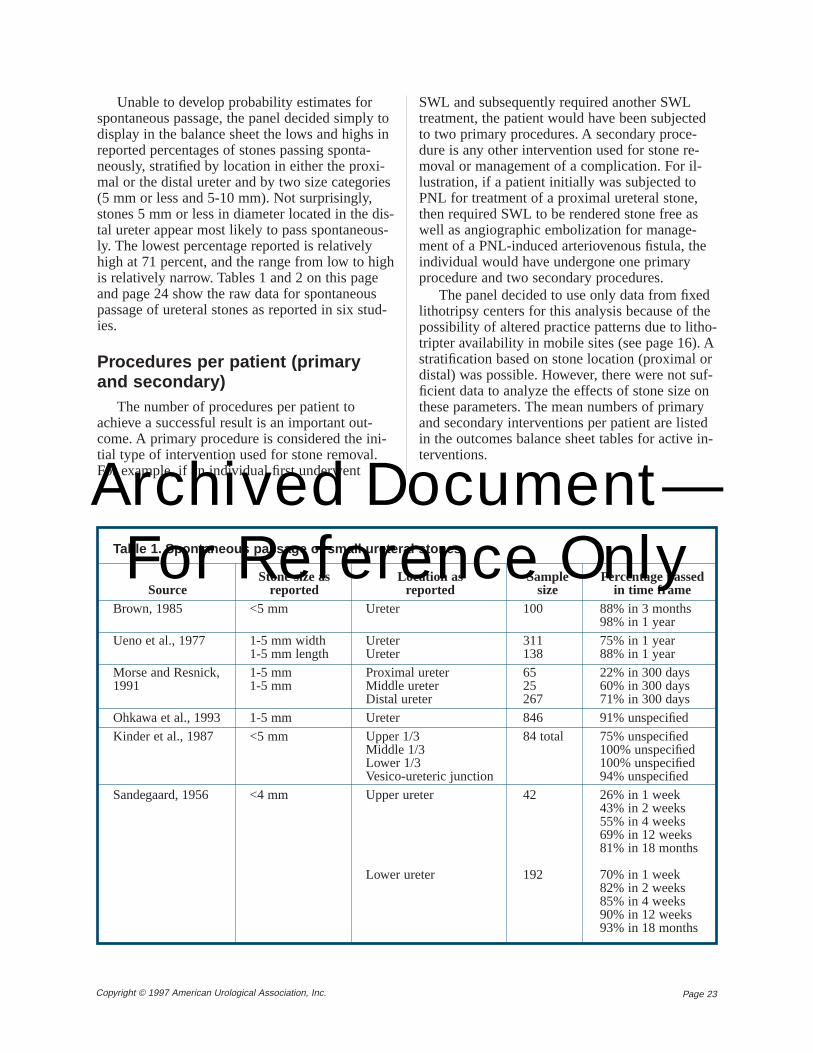
Unable to develop probability estimates forspontaneous passage, the panel decided simply todisplay in the balance sheet the lows and highs inreported percentages of stones passing sponta-neously, stratified by location in either the proxi-mal or the distal ureter and by two size categories(5 mm or less and 5-10 mm). Not surprisingly,stones 5 mm or less in diameter located in the dis-tal ureter appear most likely to pass spontaneous-ly. The lowest percentage reported is relativelyhigh at 71 percent, and the range from low to highis relatively narrow. Tables 1 and 2 on this pageand page 24 show the raw data for spontaneouspassage of ureteral stones as reported in six stud-ies.
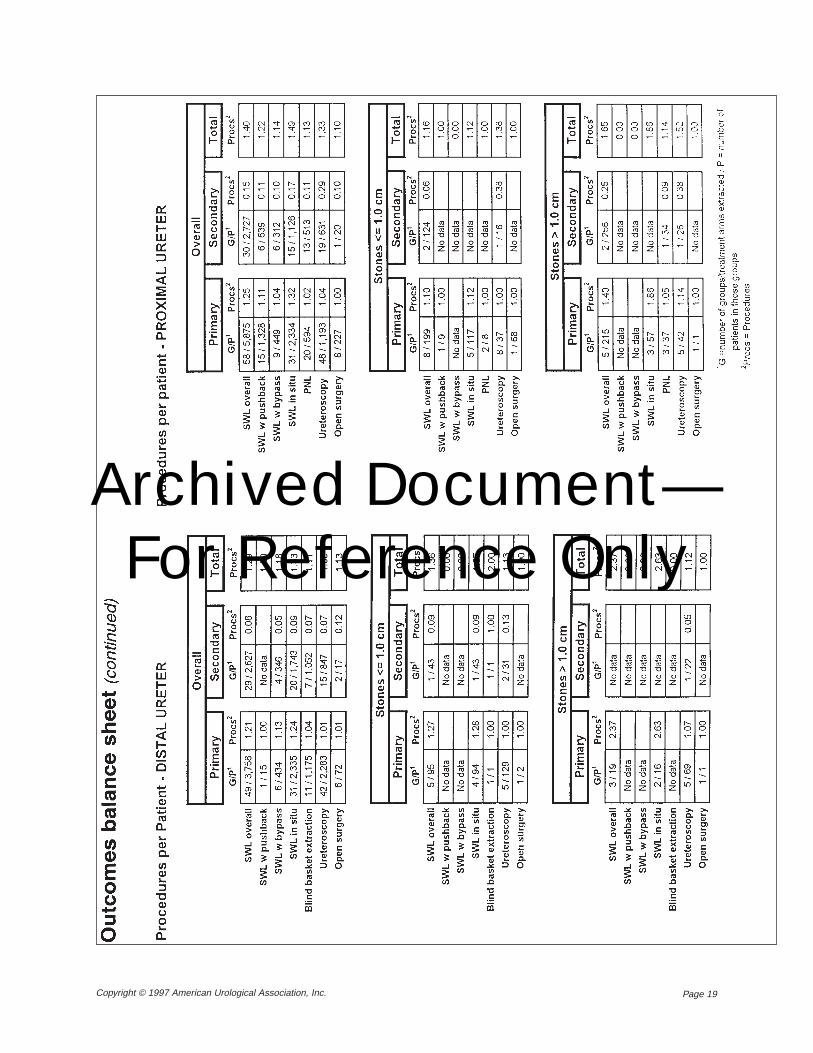
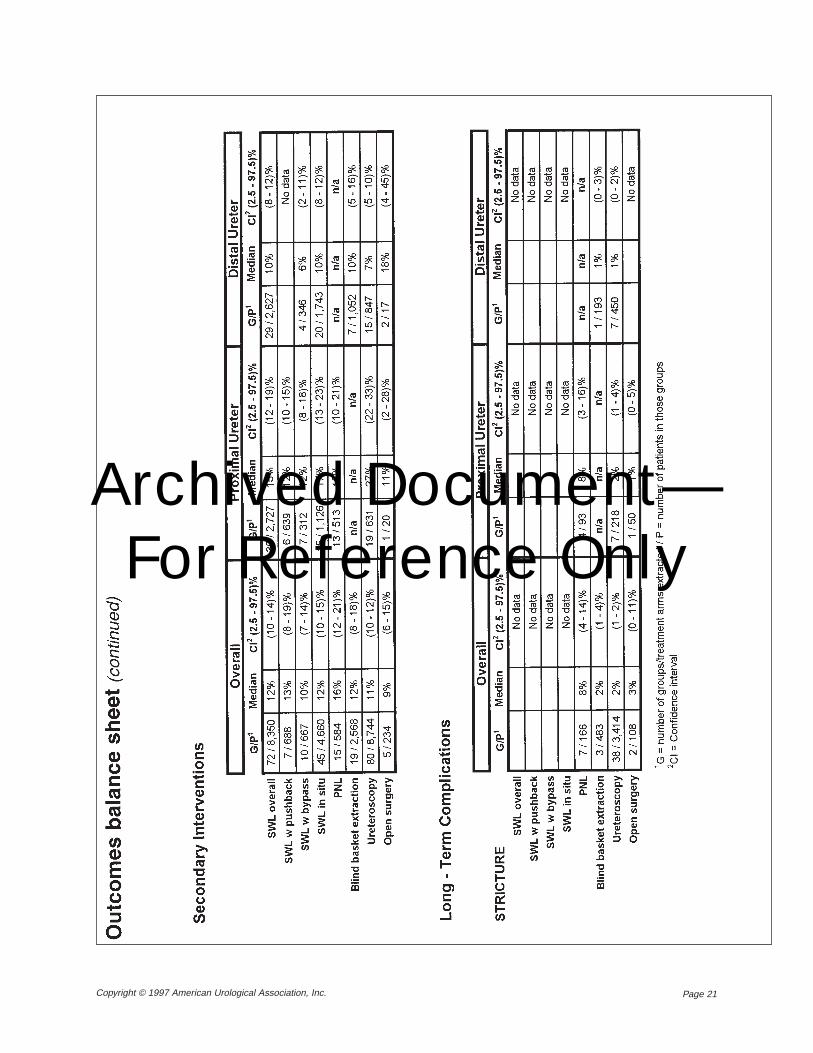
Procedures per patient (primaryand secondary)
The number of procedures per patient toachieve a successful result is an important out-come. A primary procedure is considered the ini-tial type of intervention used for stone removal.For example, if an individual first underwent
SWL and subsequently required another SWLtreatment, the patient would have been subjectedto two primary procedures. A secondary proce-dure is any other intervention used for stone re-moval or management of a complication. For il-lustration, if a patient initially was subjected toPNL for treatment of a proximal ureteral stone,then required SWL to be rendered stone free aswell as angiographic embolization for manage-ment of a PNL-induced arteriovenous fistula, theindividual would have undergone one primaryprocedure and two secondary procedures.
The panel decided to use only data from fixedlithotripsy centers for this analysis because of thepossibility of altered practice patterns due to litho-tripter availability in mobile sites (see page 16). Astratification based on stone location (proximal ordistal) was possible. However, there were not suf-ficient data to analyze the effects of stone size onthese parameters. The mean numbers of primaryand secondary interventions per patient are listedin the outcomes balance sheet tables for active in-terventions.
Table 1. Spontaneous passage of small ureteral stones
SourceBrown, 1985
Ueno et al., 1977
Morse and Resnick,1991
Ohkawa et al., 1993
Kinder et al., 1987
Sandegaard, 1956
Location asreported
Ureter
UreterUreter
Proximal ureterMiddle ureterDistal ureter
Ureter
Upper 1/3Middle 1/3Lower 1/3Vesico-ureteric junction
Upper ureter
Lower ureter
Samplesize
100
311138
6525267
846
84 total
42
192
Stone size asreported
<5 mm
1-5 mm width1-5 mm length
1-5 mm1-5 mm
1-5 mm
<5 mm
<4 mm
Percentage passedin time frame
88% in 3 months98% in 1 year
75% in 1 year88% in 1 year
22% in 300 days60% in 300 days71% in 300 days
91% unspecified
75% unspecified100% unspecified100% unspecified94% unspecified
26% in 1 week43% in 2 weeks55% in 4 weeks69% in 12 weeks81% in 18 months
70% in 1 week82% in 2 weeks85% in 4 weeks90% in 12 weeks93% in 18 months
Archived Document— For Reference Only

Page 24 Copyright © 1997 American Urological Association, Inc.
Acute complicationsIn the panel’s opinion, patients would be most
concerned about the risks of four acute complica-tions: (1) death, (2) loss of kidney, (3) transfusionrequirement and (4) the need for unplanned sec-ondary interventions. Therefore, information re-garding these outcomes is provided separately inthe balance sheet.
The data extraction form (Appendix C) lists anumber of other acute complications. These werecategorized as either significant or less significantcomplications for the outcomes balance sheet ta-bles on page 20. More detailed tables are onpages 48-62 of Appendix B. Significant complica-tions include ureteral avulsion, visceral injury,sepsis, vascular injury, hydro- or pneumothorax,pulmonary embolism and urinoma. Avulsion is apotential major complication of URS for proximalureteral stones. Reported data were limited, butthe panel believes the risk is less than 1.0 percent.Examples of less significant complications areureteral perforation, perirenal hematoma, ileus,
steinstrasse, wound infection, UTI and stent mi-gration.
Because complications were not reportedbased on stone size in any of the series, risks forcomplications are stratified in the outcomes bal-ance sheet tables only by stone location in eitherthe proximal or the distal ureter.
The majority of the articles abstracted did notmention mortality risks. Therefore, the risk forthis complication is listed as very low in the bal-ance sheet for all treatment options. The same istrue for the risk of kidney loss. Regarding transfu-sion, data reported for all treatment alternatives(including PNL and open surgery) were too limit-ed to calculate meaningful probability estimates.In the panel’s opinion, however, the risks areclearly greater for PNL and open surgery.
For distal stones, the data are sparse regardingdevelopment of significant acute complications af-ter SWL and after open surgical removal. The es-timated risk for in situ SWL calculated byFAST*PRO analysis was 3.0 percent (95% CI
Table 2. Spontaneous passage of large ureteral stones
SourceBrown, 1985
Ueno et al., 1977
Morse and Resnick,1991
Ohkawa et al., 1993
Kinder et al., 1987
Sandegaard, 1956
Location asreported
Ureter
UreterUreter
Distal ureter
UreterUreterUreterUreter
Upper 1/3Middle 1/3Lower 1/3Vesico-ureteric junction
Upper ureter
Lower ureter
Samplesize
16
199359
8
1080845176178
32 total
51
39
Stone size asreported
5-7 mm
6-9 mm width6-35 mm length
6 mm
6-10 mm11-15 mm16-20 mm>20 mm
≥6 mm
4-6mm
Percentage passedin time frame
44% in 1 year
19% in 1 year41% in 1 year
25% in 300 days
53% unspecified10% unspecified2% unspecified0% unspecified
10% unspecified14% unspecified40% unspecified45% unspecified
2% in 1 week2% in 2 weeks2% in 4 weeks2% in 12 weeks12% in 18 months
18% in 1 week23% in 2 weeks26% in 4 weeks33% in 12 weeks46% in 18 months
Archived Document— For Reference Only
Page 25Copyright © 1997 American Urological Association, Inc.
1.0-8.0 percent), but the estimated risks for by-pass and pushback techniques could not be deter-mined from the available data. However, the esti-mated overall risk of significant complications af-ter SWL (for distal calculi) using any of thesetechniques was 4.0 percent (95% CI 2.0-7.0 per-cent). In the panel’s opinion, this estimate is ap-plicable to SWL of distal stones using stent by-pass or pushback as it is somewhat higher thanthe in situ rate and reflects the more invasive na-ture of these treatments. An estimated risk for de-velopment of significant acute complications afteropen surgical removal of distal calculi could notbe generated with the FAST*PRO technique. Inthe panel’s opinion, the risk would be equivalentto the risk after open surgical removal of proximalureteral calculi.
Long-term complicationsThe development of ureteral stricture was the
only long-term complication reported with suffi-cient extractable data for any of the treatment op-tions. Stricture is not always secondary to the in-tervention, but may be induced by an inflammato-ry reaction from the stone, especially whenimpacted. The actual risk of stricture is probably
higher than reported for some treatments since de-velopment of this problem is often clinically silentand many patients are not routinely subjected topostoperative upper urinary tract radiographicstudies. However, with ureteroscopic removal, thecurrent stricture rate may be lower since many ofthe data for this therapeutic approach were fromearlier series when surgeons had neither the tech-nical experience they have today nor the smallersemirigid and flexible ureteroscopes and array ofintracorporeal lithotripsy devices available today.
The estimated risk for stricture after treatmentof proximal ureteral stones, as determined byFAST*PRO analysis, was 8.0 percent (95% CI3.0-16.0 percent) for PNL, 2.0 percent (95% CI1.0-4.0 percent) for ureteroscopic removal and 1.0percent (95% CI 0-5.0 percent) for open surgery.No data were available for SWL. The relativelyhigh estimated risk after treatment by PNL (8.0percent) may reflect the selection for PNL oflarge, hard, impacted or multiple proximal stonesthat have failed other treatments.
The estimated risk for stricture after removalof distal ureteral stones was 1.0 percent (95% CI0-2.0 percent) for ureteroscopy. Data were notsufficient to generate distal stone probability esti-mates for SWL, blind basketing or open surgery.
Archived Document— For Reference Only
Page 26 Copyright © 1997 American Urological Association, Inc.
The Ureteral Stones Clinical Guidelines Panelgenerated the recommendations in this chapterbased primarily on outcome estimates derivedfrom data reported in the literature. Where report-ed data were insufficient, the panel added its ex-pert opinion in making recommendations. Themethodology is described in Chapter 1.
The panel concluded from reviewing the litera-ture and analyzing the data that the following out-come probabilities are the most significant in set-ting forth recommendations for management ofureteral calculi:• the probability of being stone free following
treatment;
• the probability of undergoing more than oneprimary procedure;
• the probability of undergoing secondary, un-planned procedures; and
• the probability of having complications or oth-er morbidity associated with treatment.There are six methods for primary manage-
ment of ureteral stones: (1) shock wave lithotripsy(SWL); (2) ureteroscopy (URS); (3) percutaneousremoval of ureteral stones (PNL); (4) open surg-ery; (5) blind basket extraction; and (6) observa-tion.
Most stones in the United States are managedby either endourology or shock wave lithotripsy,and most training programs in the U.S. and Can-ada emphasize nonsurgical approaches. As notedon page 12, oral pharmacologic agents have alsobeen used in an effort to optimize stone passage(Borghi, Meschi, Amato, et al., 1994; Engelstein,Kahan and Servadio, 1992).
In the panel’s opinion, open surgery should notbe the first-line treatment in most standard pa-
tients (see panel recommendations below). Thisopinion is grounded in the fact that, in most pa-tients, hospitalization and postoperative morbidityare significantly less with SWL and endourologythan with any open surgical technique.
Shock wave lithotripsy is the least invasive op-tion available, but also the most likely to requiremultiple primary treatments and secondary inter-ventions in both the proximal and distal ureter.
Ureteroscopy, particularly in the distal ureter,has the highest stone-free rates but is more inva-sive than SWL.
Although PNL is theoretically an effectivetreatment modality for any ureteral stone, on apractical basis it is almost always used as a sal-vage procedure for unsuccessful SWL or URS orin special situations such as large proximal im-pacted ureteral calculi.
Panel recommendations for the treatment ofureteral calculi apply to standard and nonstandardpatients as delineated by the following criteria:
The standard patient is defined as a nonpreg-nant adult:• who has a solitary ureteral stone composed of
material other than cystine or uric acid;
• who has not been previously treated for thisstone;
• whose medical condition, including renalfunctional status, body habitus and urinarytract anatomy, permit performance of any ofthe accepted active treatment modalities in-cluding use of anesthesia;
• whose situation is such that all acceptedmodalities are available and that permits useof any of these modalities.Nonstandard patientsare defined as prepu-
bescent children and other patients who do not
Standard andnonstandard patients
Panel conclusions fromliterature review and
data analysis
Chapter 4 – Ureteral calculi treatment recommendations
Archived Document— For Reference Only
Page 27Copyright © 1997 American Urological Association, Inc.
meet the above criteria delineating the standardpatient. For nonstandard patients, the choice ofavailable treatment options may be limited.
The terms “standard,” “guideline” and “op-tion,” as used in the panel’s recommendations, re-fer to the three levels of flexibility for practicepolicies defined in Chapter 1 (page 8). A standardis the least flexible of the three, a guideline moreflexible and an option the most flexible. Optionscan exist because of insufficient evidence or be-cause patient preferences are divided. In the lattercase particularly, the panel considered it importantto take into account likely preferences of individ-ual patients when selecting from among alterna-tive interventions.
The first three recommendations below applyto both proximal and distal ureteral stones.Subsequent recommendations are categorized,first, by whether the stone is located in the proxi-mal or distal ureter and, second, by whether thestone is 1 cm or less in diameter or greater than 1cm in diameter. The proximal or upper ureter isdivided from the distal or lower ureter at the pointwhere the ureter narrows as it curves over the iliacvessels.
Recommendation: For stones withlow probability of spontaneous passage
The decision that a stone has a low probabilityof spontaneous passage is based on both the factsof the case and professional experience. Factorsthat weigh in the decision are the size of thestone, the shape of the stone, the patient’s internalanatomy and the history of previous stone pas-sage. In general, patients whose stones are 0.5 cm
or less in diameter have a good chance of sponta-neous passage, whereas the chance of sponta-neous passage for larger stones diminishes consid-erably.
Although, as a practical matter, it is evidentthat the availability of equipment and the exper-tise of an individual practitioner may affect thechoice of a treatment intervention, it is unaccept-able to withhold certain treatments from the pa-tient and not offer them as alternatives because ofpersonal inexperience or unfamiliarity with one ofthe accepted treatment modalities or because ofthe local unavailability of equipment or expertise.
Recommendation: For stones withhigh probability of spontaneous passage
Up to 98 percent of stones less than 0.5 cm indiameter, especially in the distal ureter, may beexpected to pass spontaneously. How long untilpassage occurs, over what period of time passagetakes place and the degree of colic or other symp-toms are all unpredictable and often bear heavilyon the decision to intervene in such patients. Inthe panel’s opinion, for most of these patients thehigh probability of spontaneous passage justifiesobservation as the initial treatment. However, dif-ficulties in tolerating pain, multiple trips to theemergency room or other factors may mandatetreatment in a patient whose stone might other-wise be expected to pass.
Recommendation: For treatment byshock wave lithotripsy
Guideline: Routine stenting to increase ef-ficiency of fragmentation is not recommendedas part of shock wave lithotripsy.
Guideline: In a patient who has a newlydiagnosed proximal or distal ureteral stonewith a high probability of spontaneous pas-sage, and whose symptoms are controlled, ob-servation with periodic evaluation is recom-mended for initial treatment.
Standard: A patient who has a ureteralstone with a low probability of spontaneouspassage must be informed about the existingactive treatment modalities, including the rel-ative benefits and risks associated with eachmodality.
Panel recommendations
Archived Document— For Reference Only
Page 28 Copyright © 1997 American Urological Association, Inc.
It has become common practice to place aureteral stent, usually a double-J stent, for moreefficient fragmentation of ureteral stones usingSWL. The data analyzed by the panel did not sup-port the routine use of such stents when the goalis to improve the stone-free results of SWL. Thedata showed no improved fragmentation withstenting. Routine stenting may be justifiable forother purposes such as management of symptomsassociated with the passage of stones.
Recommendations: For stones of1 cm or less in proximal ureter
Although open surgery will usually be suc-cessful, relatively longer hospitalization andgreater postoperative morbidity with open surgerymean that SWL should be the first-line treatmentfor most patients. Ureteroscopy and PNL are ac-ceptable choices in situations where SWL maynot be appropriate or as salvage procedures forfailed SWL.
Recommendations: For stonesgreater than 1 cm in proximal ureter
Treatment results for large stones in the upperureter are less predictable than for small stones.Shock wave lithotripsy, PNL and URS are all ac-ceptable options in the upper ureter, but URS maybecome less appropriate as the stones encounteredbecome larger. Open surgery, despite the excellentstone-free results, should not be the first-linetreatment in most patients with large stones. The
reasons are the same as for patients with smallstones: relatively greater postoperative morbidityand longer hospitalization. Open surgery maywell be appropriate for nonstandard patients andis certainly an acceptable alternative as a salvagemeasure.
Recommendations: For stones of1 cm or less in distal ureter
Blind basketing refers to basket manipulationof distal ureteral stones as practiced prior to theadvent of ureteroscopy and fluoroscopy around1981. The high success rates attending uretero-scopic stone removal utilizing fluoroscopic con-trol, the availability of fluoroscopy as an adjunc-tive measure and the lack of training in the vastmajority of programs in the technique of blindbasket extraction mean that blind basketing with-out fluoroscopy and safety guide wire cannot beencouraged as a treatment choice. The data fromthe literature suggest that blind basketing canachieve a 73-percent success rate. Nevertheless,the panel’s expert opinion is that guided stone ma-nipulation (concomitant use of fluoroscopy andsafety guide wire) or ureteroscopic basketingwould be a considerably safer and more effica-cious option.
Shock wave lithotripsy and URS are each ef-fective for management of distal ureteral stones.Each has advantages and disadvantages. Shockwave lithotripsy is minimally invasive and can of-ten be performed either without anesthesia or un-der intravenous sedation, but may require multipleprimary treatments for adequate fragmentationand is more likely to require ancillary treatment.
Ureteroscopy has a higher success rate, withthe least risk of requiring multiple treatments andthe least risk of an ancillary procedure, but ismore invasive than SWL. Although not studied by
Standard: Open surgery should not be thefirst-line treatment.
Guideline: Blind basketing without fluo-roscopy and guide wire cannot be encouragedas a treatment choice.
Option: Shock wave lithotripsy andureteroscopy are both acceptable treatmentchoices.
Guideline: Open surgery should not bethe first-line treatment for most patients.
Option: Shock wave lithotripsy, percuta-neous nephrolithotomy and ureteroscopy areall acceptable treatment choices.
Standard: Open surgery should not be thefirst-line active treatment.
Guideline: Shock wave lithotripsy is rec-ommended as first-line treatment for most pa-tients.
Archived Document— For Reference Only
Page 29Copyright © 1997 American Urological Association, Inc.
the panel, cost issues will bear on the patient’s de-cision as to which treatment method is more ap-propriate. Availability is also a factor. Ureter-oscopy is widely available in the current era, as isSWL, although the availability of SWL will varyaccording to whether or not a practitioner is de-pendent on a mobile machine.
Recommendations: For stonesgreater than 1 cm in distal ureter
Large stones in the ureter must be fragmentedprior to ureteroscopic extraction, and SWL mustfragment large stones into passable fragments.Such stones will likely require more SWL treat-ments than will smaller stones, and URS may bepreferable when such cases can be anticipated.Given the high success rates using SWL andURS, open surgery should not be the first-linetreatment in most patients; but open surgery maybe preferable for certain very large ureteral stonesor in special situations.
The relatively recent development of small(7.5 to 10.5 F.), actively deflectable, flexibleureteroscopes has improved endoscopic access tothe upper ureter. Meanwhile, intracorporeallithotripsy devices have become more powerfulwith the introduction of the Holmium laser(Ho:YAG). Recent articles suggest that this lasercan effectively fragment virtually any type of uri-nary calculus (Bagley and Erhard, 1995; Erhardand Bagley, 1995; Grasso, 1996; Shroff, Watson,Parikh, et al., 1996). Moreover, because the laserlight can be carried through small, flexible quartz
fibers, Holmium lasers are particularly well suitedfor use with small-diameter flexible ureteroscopesin the upper ureter. The use of flexible uretero-scopes in combination with the Holmium lasermay allow the efficacy of ureteroscopy in the up-per ureter to approach the efficacy achieved in thelower ureter. However, the numbers of cases re-ported as of this writing are still too small to sig-nificantly alter the stone-free rates displayed inthe outcomes balance sheet tables (e.g., 72 per-cent overall for ureteroscopy in the proximalureter).
Although shock wave lithotripsy machineshave improved in ease of localization of ureteralstones, and the requirement for anesthesia has de-creased, there has been no increase in power oreffectiveness over the original Dornier HM-3. Im-provements in the fragmentation ability, andtherefore the efficacy, of shock wave machinesawait further advances in the understanding ofshock waves, their generation and their stone andtissue interactions.
Three major challenges in stone research are:1. Stone prevention:Any kidney stone is poten-
tially preventable. The symptoms, the risks oftreatment and the trauma of the stone eventcould in theory be prevented by appropriatemetabolic evaluation and treatment of identi-fied problems. Such prevention research,which could eventually result in savings ofhundreds of millions of dollars each year,would require a high degree of physician-pa-tient cooperation.
2. A uniform system of stone reporting:Lackof such a system has hampered the panel indeveloping both the Report on the Manage-ment of Ureteral Calculiand the previousReport on the Management of Staghorn Cal-culi. Mr. David Tolley and colleagues have de-vised a uniform system of reporting which, ifaccepted by the major journals, would go along way toward standardizing the reportingof stone results and thus making comparisonof stone results easier and more practical(Tolley, Wallace and Tiptaft, 1991).
3. Ability to predict the response of a stone toshock wave lithotripsy: Ureteral stone man-agement would be optimized if the degree towhich a given stone could be fragmented werepredictable. At present, such prediction is pos-sible only in the most general way.
Current trends andrecommendations for
further research
Standard: Blind basketing is not recom-mended as a treatment choice.
Guideline: Open surgery should not bethe first-line treatment for most patients.
Option: Shock wave lithotripsy andureteroscopy are both acceptable treatmentchoices.
Archived Document— For Reference Only
Page 30 Copyright © 1997 American Urological Association, Inc.
Alken P. Percutaneous ultrasonic destruction of renalcalculi. Urol Clin North Am 1982;9:145-51.
Assimos DG, Boyce WH, Harrison LH, McCulloughDL, Kroovand RL, Sweat KR. The role of openstone surgery since extracorporeal shock wavelithotripsy. J Urol 1989;142:263-7.
Assimos DG, Wrenn JJ, Harrison LH, McCulloughDL, Boyce WH, Taylor CL, Zagoria RJ, Dyer RB. Acomparison of anatrophic nephrolithotomy and per-cutaneous nephrolithotomy with and without extra-corporeal shock wave lithotripsy for management ofpatients with staghorn calculi. J Urol 1991;145:710-4.
Beck EM, Vaughan ED, Jr., Sosa RE. The pulsed dyelaser in the treatment of ureteral calculi. Semin Urol1989;7:25-9.
Bagley D, Erhard M. Use of the holmium laser in theupper urinary tract. Tech Urol 1995;1(1):25-30.
Bagley DH, Huffman JL, Lyon ES. Combined rigidand flexible ureteropyeloscopy. J Urol 1983;130:243-4
Begun FP, Jacobs SC, Lawson RK. Use of a prototype3F electrohydraulic electrode with ureteroscopy fortreatment of ureteral calculous disease. J Urol 1988;139:1188-91.
Blandy JP, Singh M. The case for a more aggressiveapproach to staghorn stones. J Urol 1976;115:505-6.
Borghi L, Meschi T, Amato F, Novarini A, Giannini A,Quarantelli C, Mineo F. Nifedipine, methylpred-nisolone in facilitating ureteral stone passage: a ran-domized, double-blind, placebo-controlled study. JUrol 1994;152:1095-8.
Brown RB. A success and cost analysis study of themethods of managing impacted lower ureteric cal-culi. Aust N Z J Surg 1985;55:51-4.
Brown, RD, Preminger, GM. Changing surgical aspectsof urinary stone disease. [Review]. Surg Clin NorthAm 1988;68:1085-1104.
Carrol PR, Shi RY. Genetic toxicity of high energyshockwaves: assessment using the induction of muta-tions or micronuclei in chinese hamster ovary. J Urol1986;135:292A.
Chaussy CG, Fuchs GJ. Extracorporeal shock wavelithotripsy of distal-ureteral calculi: is it worthwhile?.J Endourol 1987;1(1):1-8.
Chaussy C, Schmiedt E, Jocham D, Brendel W,Forssmann B, Walther V. First clinical experiencewith extracorporeally induced destruction of kidneystones by shock waves. J Urol 1982;127:417-20.
Coptcoat MJ, Ison KT, Watson G, Wickham JEA.Lasertripsy for ureteral stones: 100 clinical cases. JEndourol 1987;1:119-22.
Denstedt JD, Clayman RV. Electrohydraulic lithotripsyof renal and ureteral calculi. J Urol 1990;143:13-7.
Denstedt JD, Eberwein PM, Singh RR. The Swisslithoclast: a new device for intracorporeal lithotripsy.J Urol 1992;148:1088-90.
Dretler SP. An evaluation of ureteral laser lithotripsy:225 consecutive patients. J Urol 1990;143:267-72.
Dretler SP. Laser photofragmentation of ureteral cal-culi: analysis of 75 cases. J Endourol 1987;1:9-14.
Dretler SP. Modes of intracorporeal lithotripsy. In kid-ney stones and medical and surgical management.Coe FL, ed. Philadelphia (PA): Lippincott/Raven;1995
Dretler SP, Cho G. Semi-rigid ureteroscopy: a newgenre. J Urol 1989;141:1314-6.
Dretler SP, Watson G, Parrish JA, Murray S. Pulseddye laser fragmentation of ureteral calculi: initialclinical experience. J Urol 1987;137:386-9.
Dretler SP, Bhatta KM. Clinical experience with highpower (140 mj.), large fiber (320 micron) pulsed dyelaser lithotripsy. J Urol 1991;146:1228-31.
Eddy DM. The confidence profile method: A Bayesianmethod for assessing health technologies. Oper Res1989;37(2):210-28.
Eddy DM. Clinical decision making: from theory topractice. Comparing benefits and harms: the balancesheet. JAMA 1990;263:2493-2505.
Eddy DM. A manual for assessing health practices &designing practice policies: the explicit approach.Philadelphia (PA): American College of Physicians1992;126 p.
Eddy DM, Hasselblad V. FAST*PRO. Software formeta-analysis by the confidence profile method. SanDiego (CA): Academic Press, Inc. Harcourt BraceJovanovich; 1992. 196 p.
Eddy DM, Hasselblad V, Shachter R. A Bayesianmethod for synthesizing evidence: the confidenceprofile method. Int J Technol Assess Health Care1990;6:31-55.
References*
_________________*Includes articles cited in text. See Table A-1 in Appendix A for a complete listing of articles extracted for analysis.
Archived Document— For Reference Only
Page 31Copyright © 1997 American Urological Association, Inc.
Engelstein D, Kahan E, Servadio C. Rowatinex for thetreatment of ureterolithiasis. J D Urol 1992;98:98-100.
Erhard MJ, Bagley DH. Urologic applications of theholmium laser: preliminary experience. J Endourol1995;9(5): 383-6.
Erturk E, Herrman E, Cockett AT. Extracorporealshock wave lithotripsy for distal ureteral stones. JUrol 1993;149:1425-6.
Fahlenkamp D, Schonberger B, Liebetruth L, LindekeA, Loening SA. Laparoscopic laser ureterolithotomy.J Urol 1994;152:1549-51.
Feagins BA, Wilson WT, Preminger GM. Intracor-poreal electrohydraulic lithotripsy with flexibleureterorenoscopy. J Endourol 1990;4:347-51.
Gaur DD, Agarwal DK, Purohit KC, Darshane AS,Shah BC. Retroperitoneal laparoscopic ureterolitho-tomy for multiple upper mid ureteral calculi. J Urol1994;151:1001-2.
Gillenwater JY, Grayhack JT, Howards SS, DuckettJW: Adult and pediatric urology, 3rd ed. St.Louis(MO): Ann S. Patterson 1996; Chapter 21;973-98.
Grasso M, Bagley DH. Endoscopic pulsed-dye laserlithotripsy: 159 consective cases. J Endourol1994;8:25-7.
Grasso M. Experience with the holmium laser as anendoscopic lithotrite. Urology 1996;48(2): 199-206.
Green DF, Lytton B. Early experience with direct vi-sion electrohydraulic lithotripsy of ureteral calculi. JUrol 1985;133:767-70.
Higashihara E, Horie S, Takeuchi T, Kameyama S,Asakage Y, Hosaka Y, Honma Y, Minowada S, Aso Y.Laser ureterolithotripsy with combined rigid andflexible ureterorenoscopy. J Urol 1990;143:273-4.
Hofmann R, Hartung R. Use of pulsed Nd:YAG laserin the ureter. Urol Clin North Am 1988; 15:369-75.
Huffman JL. Early experience with the 8.5 F compactureteroscope. Surg Endoscopy 1989; 3:164-6.
Kinder RB, Osborn DE, Flynn JT, Smart JG.Ureteroscopy and ureteric calculi: how useful? Br JUrol 1987;60:506-8.
McCullough D,Yeaman LD, Bo WJ, Kroovand RL,Assimos DG, Griffin AS. Experimental effects of ex-tracorporeal shock waves on the rat ovary and fetus.In Shock wave lithotripsy: state of the art. LingemenJE, Newman DM, eds. New York(NY): PlenumPress; 1988:pp 327-9.
Miller K, Bachor R, Hautmann R, Extracorporealshock wave lithotripsy in the prone position: tech-nique, indications, results. J Endourol 1988;2:113-5.
Mobley TB, Myers DA, Jenkins JM, Grine WB, JordanWR. Effects of stents on lithotripsy of ureteral cal-culi: treatment results with 18,825 calculi using theLithostar lithotriptor. J Urol 1994;152:53-6.
Morgentaler A, Bridge SS, Dretler SP. Management ofthe impacted ureteral calculus. J Urol 1990;143:263-6.
Morse RM, Resnick MI. Ureteral calculi: natural histo-ry and treatment in an era of advanced technology. JUrol 1991;145:263-5.
Ohkawa M, Tokunaga S, Nakashima T, Yamaguchi K,Orito M, Hisazumi H. Spontaneous passage of upperurinary tract calculi in relation to composition. UrolInt 1993;50:153-8.
Otnes B, Sandnes H. Comparison of radiologic mea-surement and actual size of ureteretal calculi. ScandJ Urol 1978; 12:155-6.
Patel VJ. The coagulum pyelolithotomy. Br J Surg1973;60:230-6.
Perez-Castro Ellendt E, Matinez-Pineiro JA.Transurethral ureteroscopy: a current urologic proce-dure. Arch Esp Urol 1980;33:445-60
Preminger GM, Sonographic piezoelectric lithotripsy:more bang for your buck. J Endourol 1989;3:321-7.
Preminger GM, Roehrborn CG. Special applications offlexible deflectable ureterorenoscopy. Semin Urol1989;7:16-24.
Preminger GM, Schultz S, Clayman RV, Curry T,Redman HC, Peters PC. Cephalad renal movementduring percutaneous nephrostolithotomy. J Urol1987;137:623-25.
Raney AM. Electrohydraulic lithotripsy: experimentalstudy and case reports with the stone disintegrator. JUrol 1975;113:345-7.
Raney AM, Handler J. Electrohydraulicnephrolithotripsy. Urology 1975;6:439-42.
Resnick MI. The craft of urologic surgery:pyelonephrolithotomy for removal of calculi fromthe inferior renal pole. Urol Clin North Am 1981;8:585-90.
Reuter HJ, Kern, E. Electronic lithotripsy of ureteralcalculi. J Urol 1973;110:181-83.
Sandegård E, Prognosis of Stone in the Ureter. ActaChirurgica Scandinavica, Stockholm, 1956,Berlingska Boktryckeriet, Lund, 1956; supplemen-tum 219:1-67.
Schulze H, Haupt G, Piergiovanni M, Wisard M,NiederHausern W, Senge T. The Swiss lithoclast: anew device for endoscopic stone disintegration. JUrol 1993;149:15-8.
Segura JW, Preminger GM, Assimos DG, Dretler SP,Kahn RI, Lingeman JE, Macaluso JN Jr.Nephrolithiasis Clinical Guidelines Panel: report onthe management of staghorn calculi. Baltimore(MD):American Urological Association, Inc., 1994.
Segura JW, Patterson DE, LeRoy AJ, Williams HJ Jr,Barrett DM, Benson RC Jr, May GR, Bender CE.Percutaneous removal of kidney stones: review of1,000 cases. J Urol 1985;134:1077-81.
Archived Document— For Reference Only
Page 32 Copyright © 1997 American Urological Association, Inc.
Shroff S, Watson GM, Parikh A, Thomas R,Soonawalla PF, Pope A. The holmium: YAG laser forureteric stones. Br J Urol 1996;78:836-9.
Tasca A, Cecchetti W, Zattoni F, Pagano F.Photosensitization of cystine stones to induce laserlithotripsy. J Urol 1993;149:709-12.
Thorwald J. The century of the surgeon. NewYork(NY): Pantheon Books; 1957.
Tolley DA, Wallace DMA, Tiptaft RC. First UKConsensus Conference on LithotriptorTerminology—1989. Br J Urol 1991;67:9-12.
Ueno A, Kawamura T, Ogawa A, Takayasu H. Relationof spontaneous passage of ureteral calculi to size.Urology 1977;10:544-6.
Vieweg J, Weber HM, Miller K, Hautmann R. Femalefertility following extracorporeal shock wavelithotripsy of distal ureteral calculi. J Urol1992;148:1007-10.
Weber HM, Miller K, Ruschoff J, Gschwend J,Hautmann RE. Alexandrite laser lithotripter in exper-imental and first clinical application. J Endourol1991;5:51-5.
Yiu MK, Liu PL, Yiu TF, Chan AY. Clinical experiencewith holmium: YAG Laser lithotripsy of ureteral cal-culi. Lasers Surg Med 1996;19(1):103-106.
Young HH. Treatment of calculus of the lower end ofthe ureter in the male. Am Med 1902;4:209.
Archived Document— For Reference Only
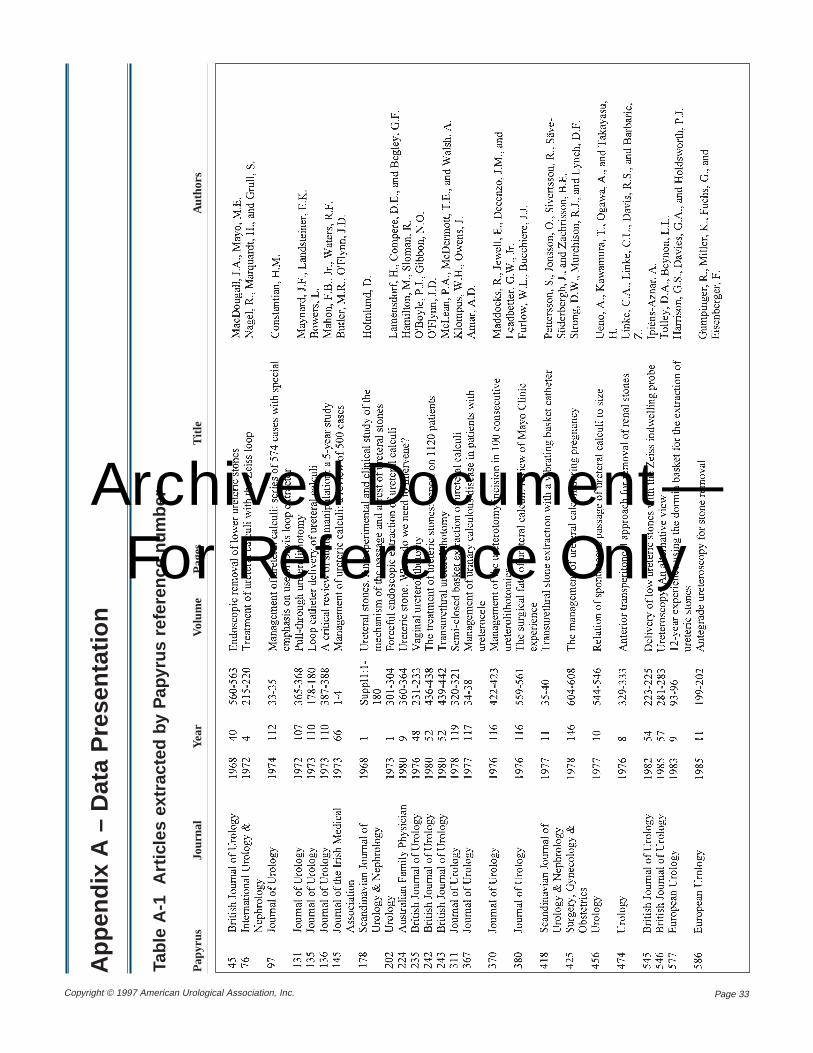
Page 33Copyright © 1997 American Urological Association, Inc.
App
endi
x A
– D
ata
Pre
sent
atio
n
Tabl
e A
-1
Art
icle
s ex
trac
ted
by P
apyr
us r
efer
ence
num
ber
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
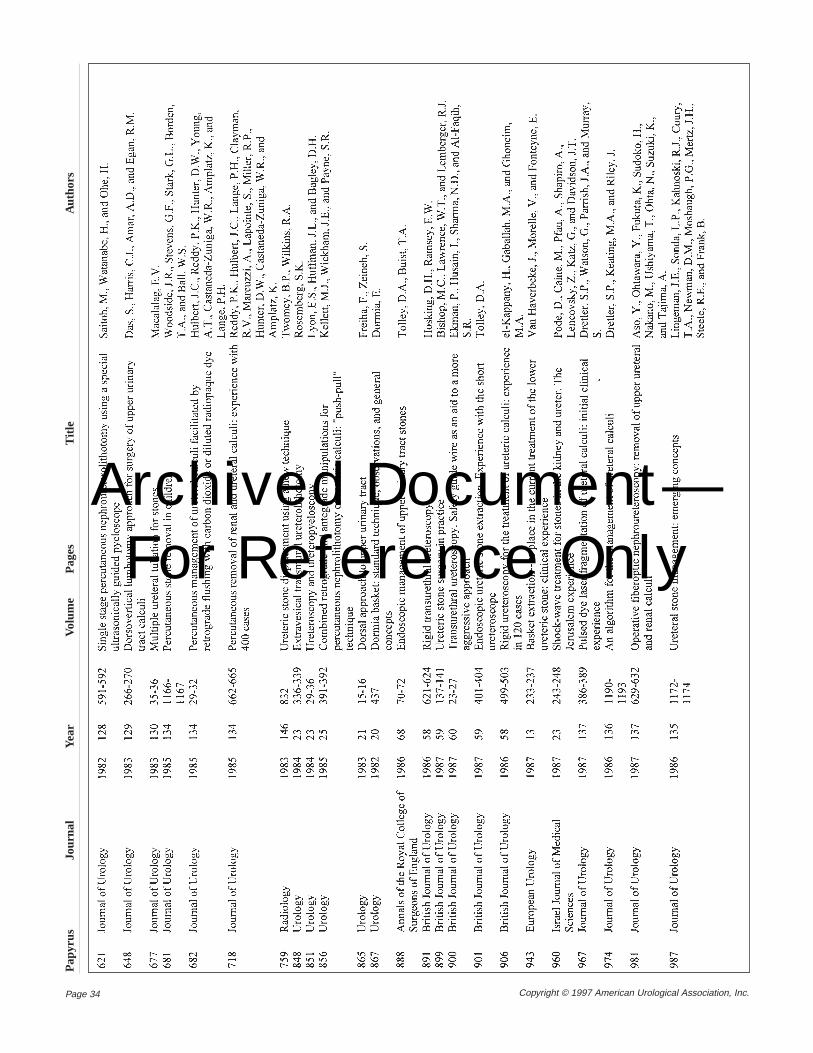
Page 34 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
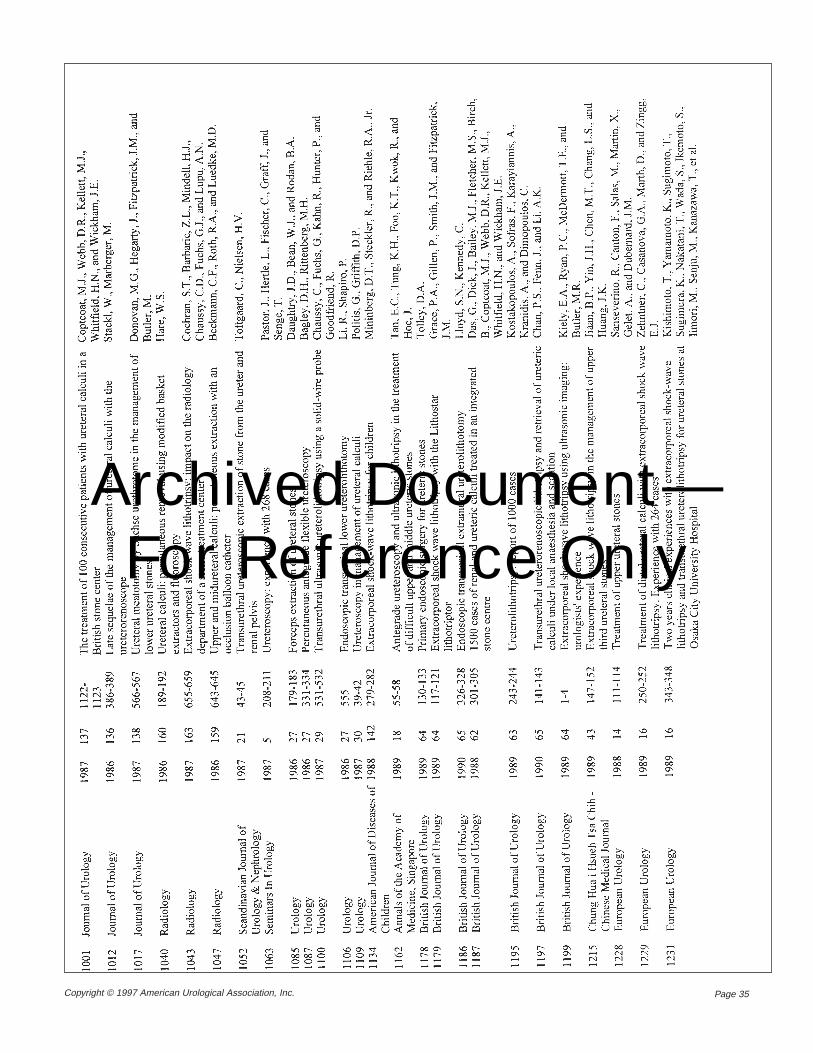
Page 35Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
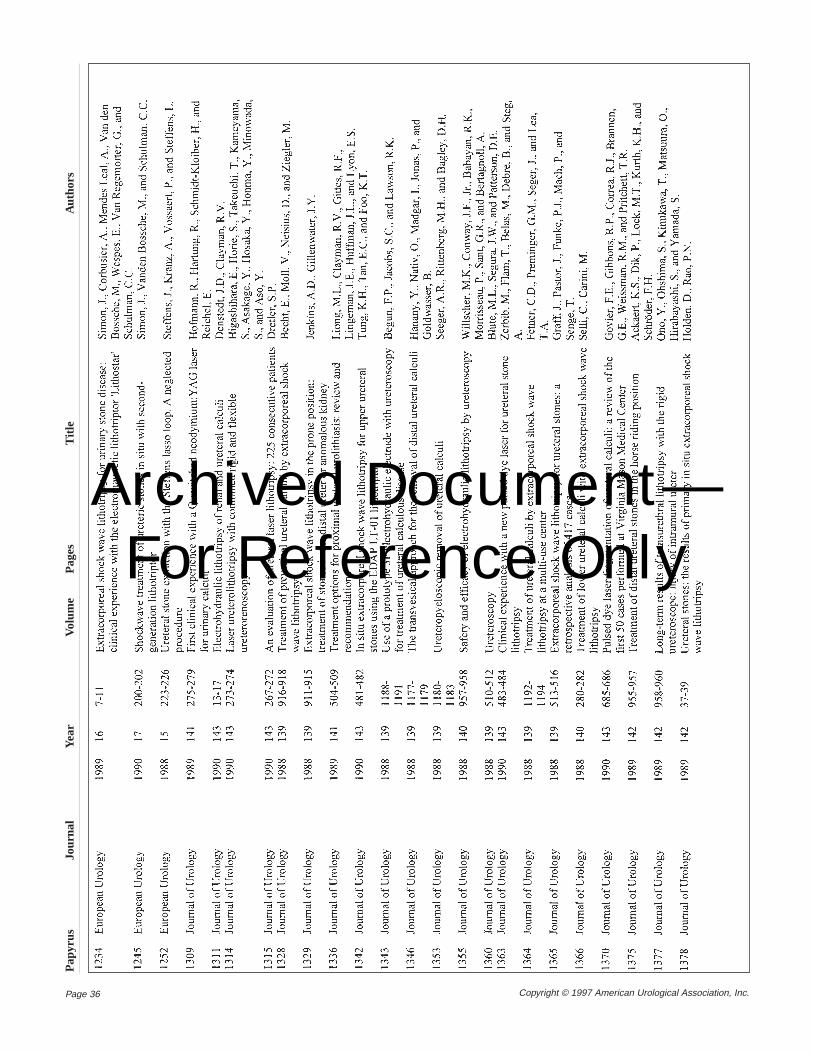
Page 36 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
Page 37Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 38 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
Page 39Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 40 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
Page 41Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 42 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
Page 43Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 44 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
Page 45Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
Page 46 Copyright © 1997 American Urological Association, Inc.
Pap
yrus
Jour
nal
Year
Volu
me
Pag
esT
itle
Aut
hors
Archived Document— For Reference Only
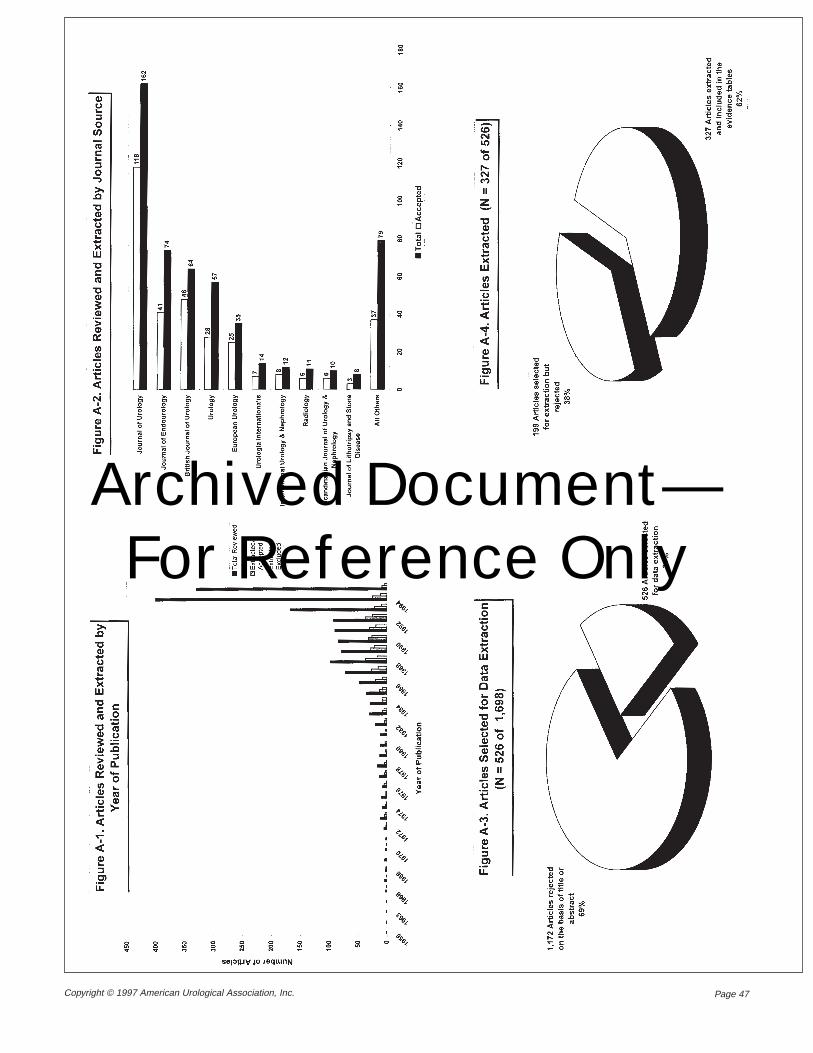
Page 47Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
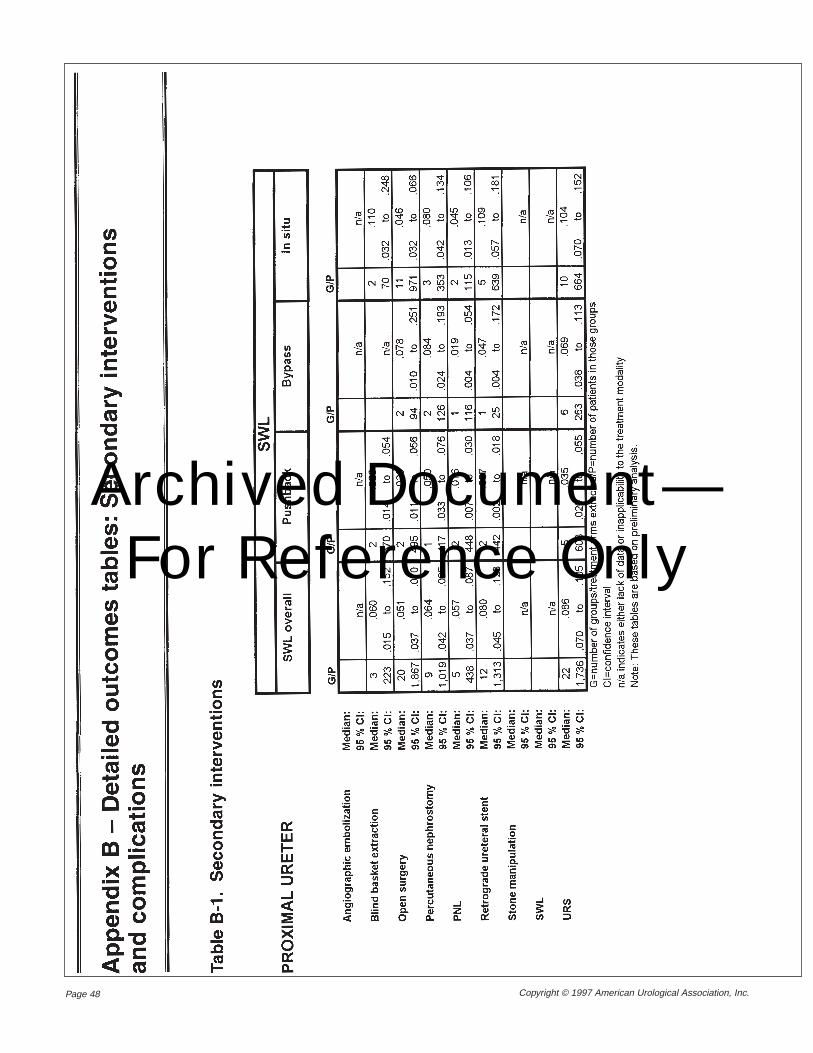
Page 48 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
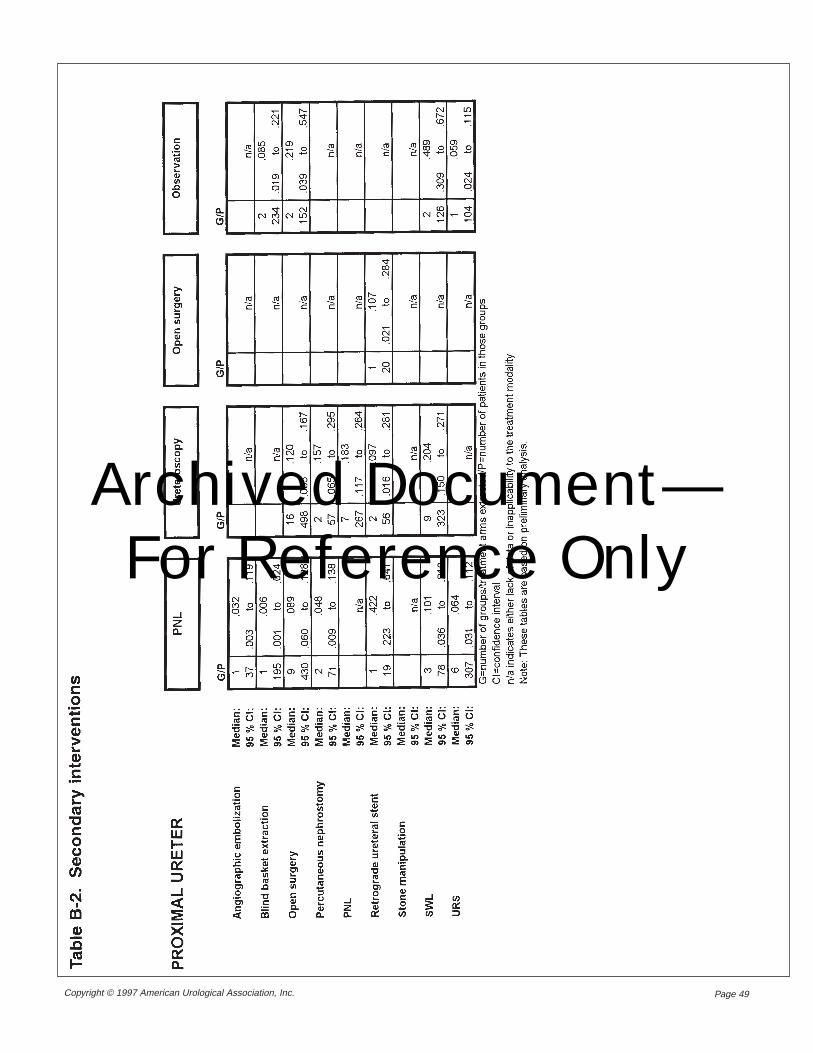
Page 49Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
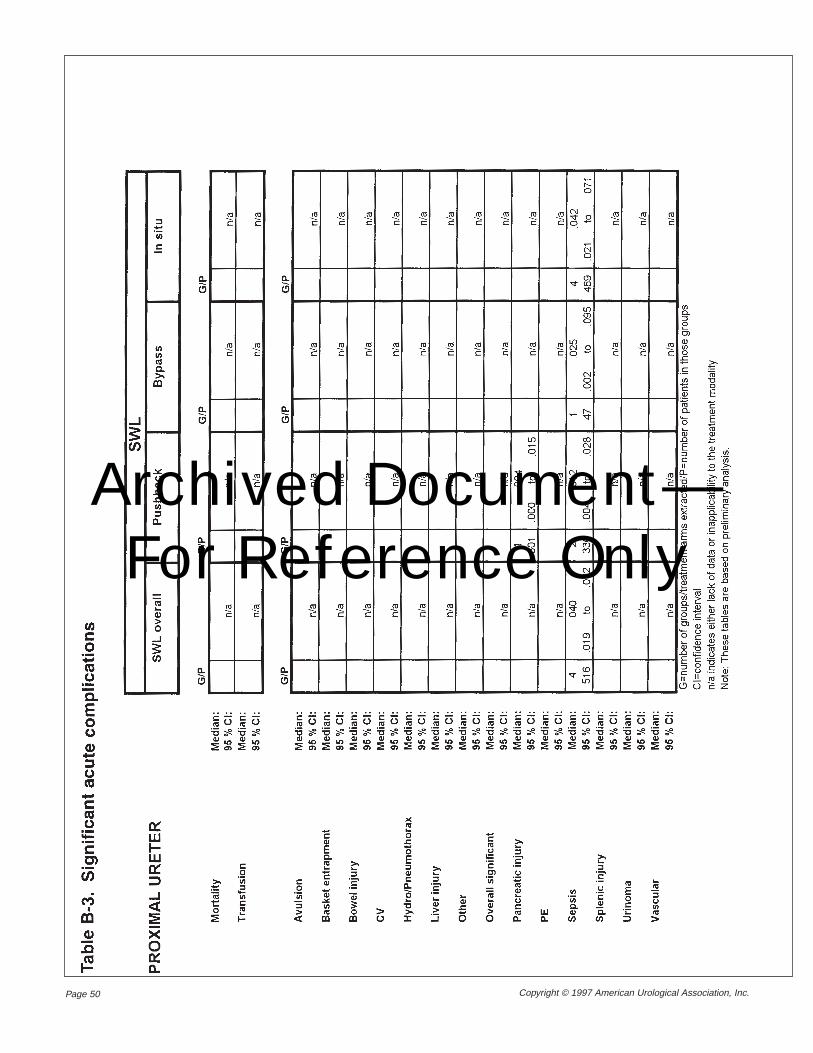
Page 50 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
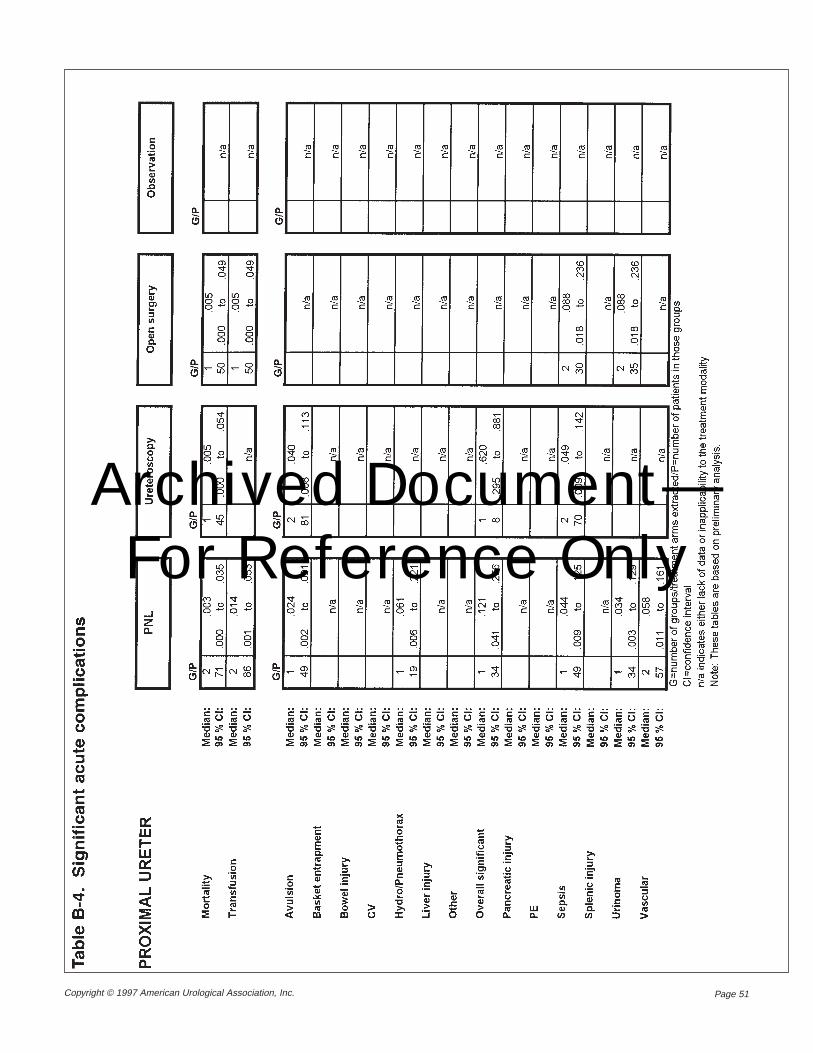
Page 51Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
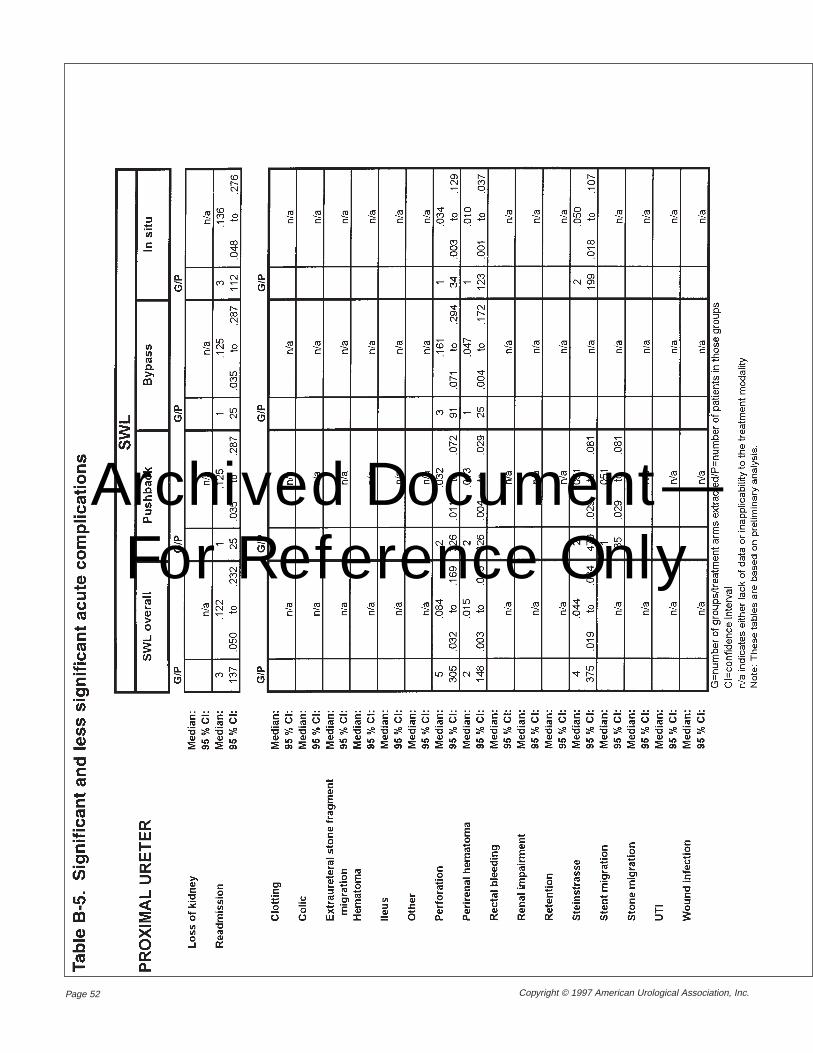
Page 52 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
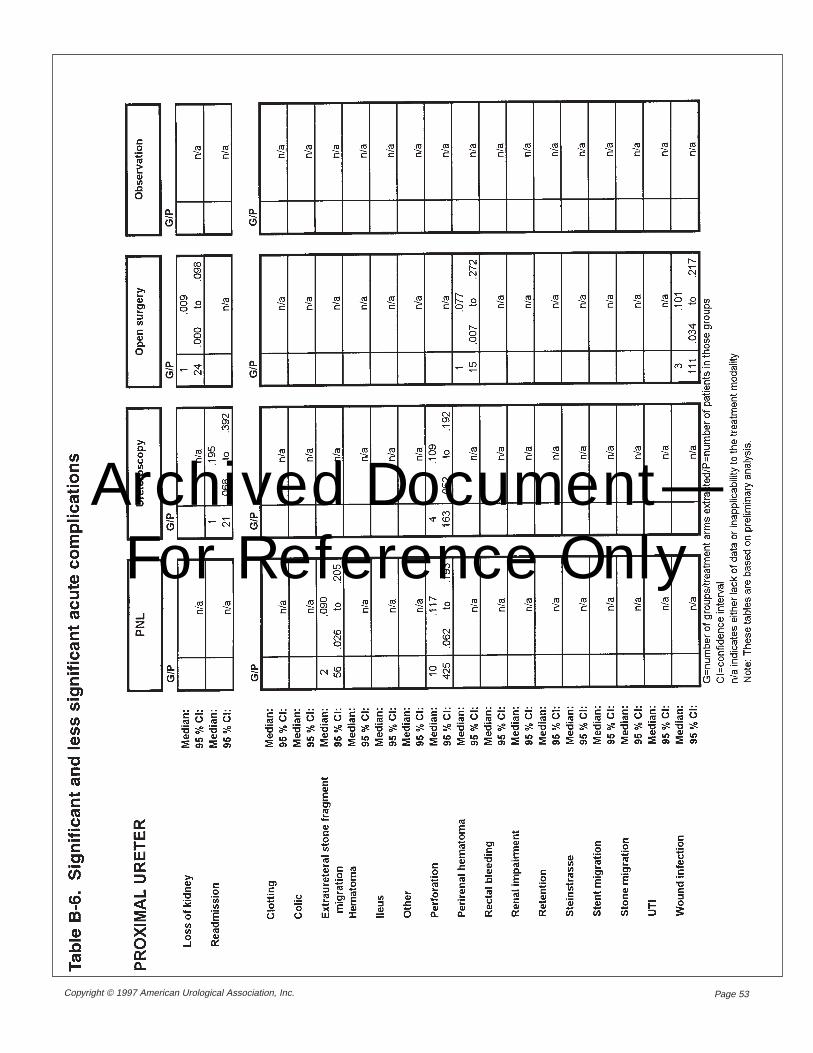
Page 53Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
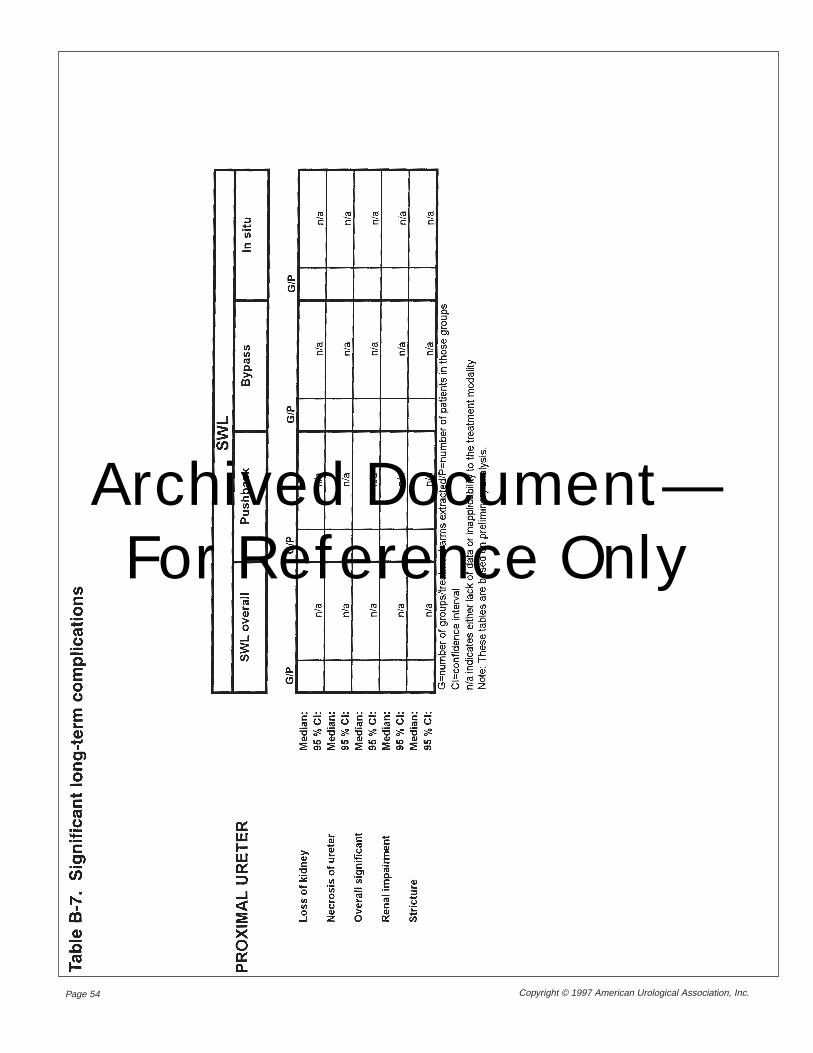
Page 54 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
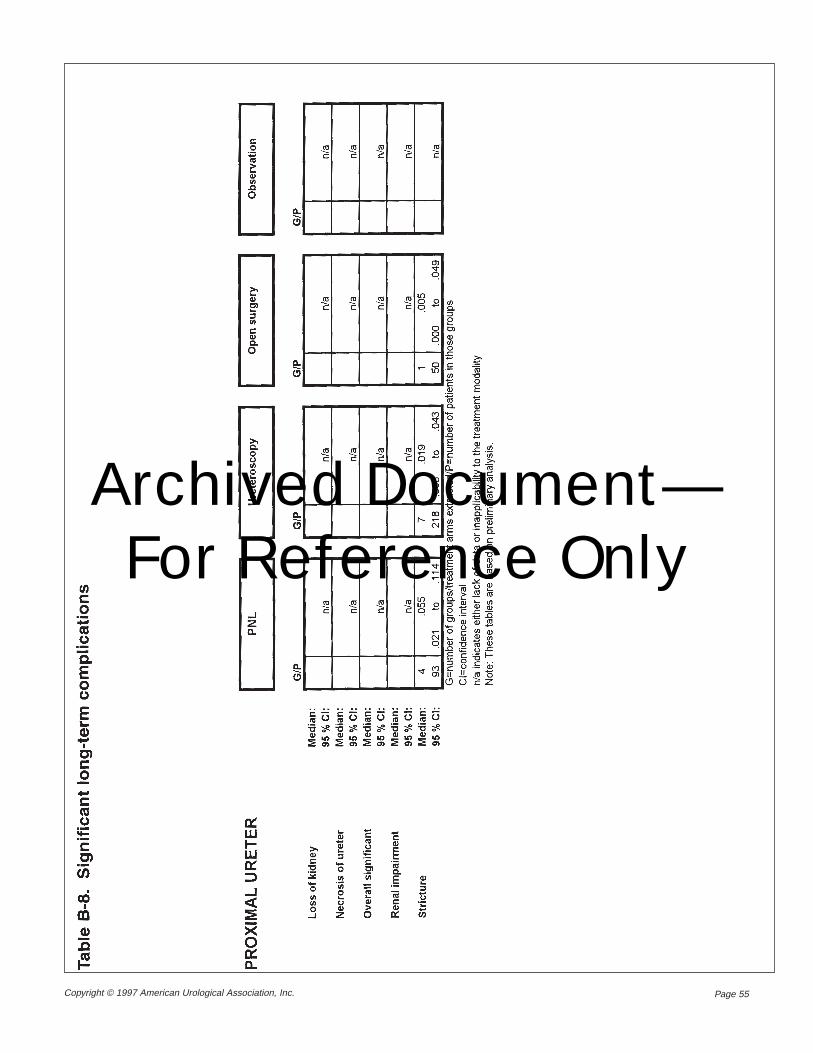
Page 55Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
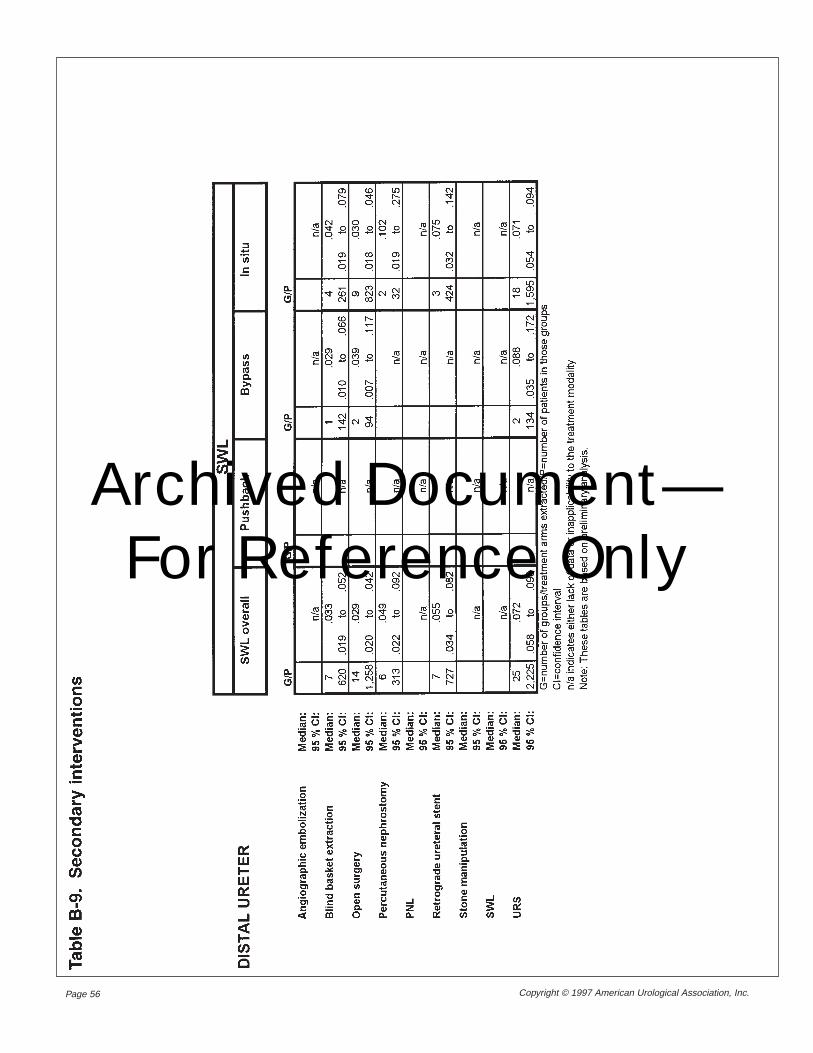
Page 56 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
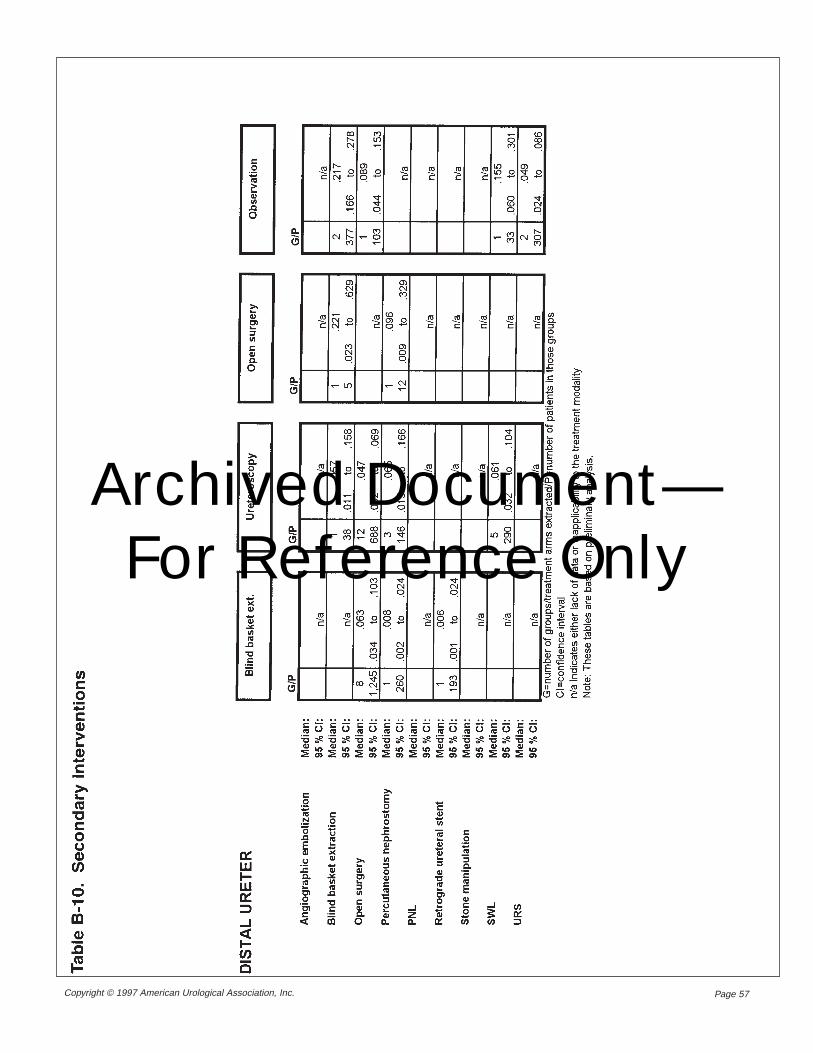
Page 57Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
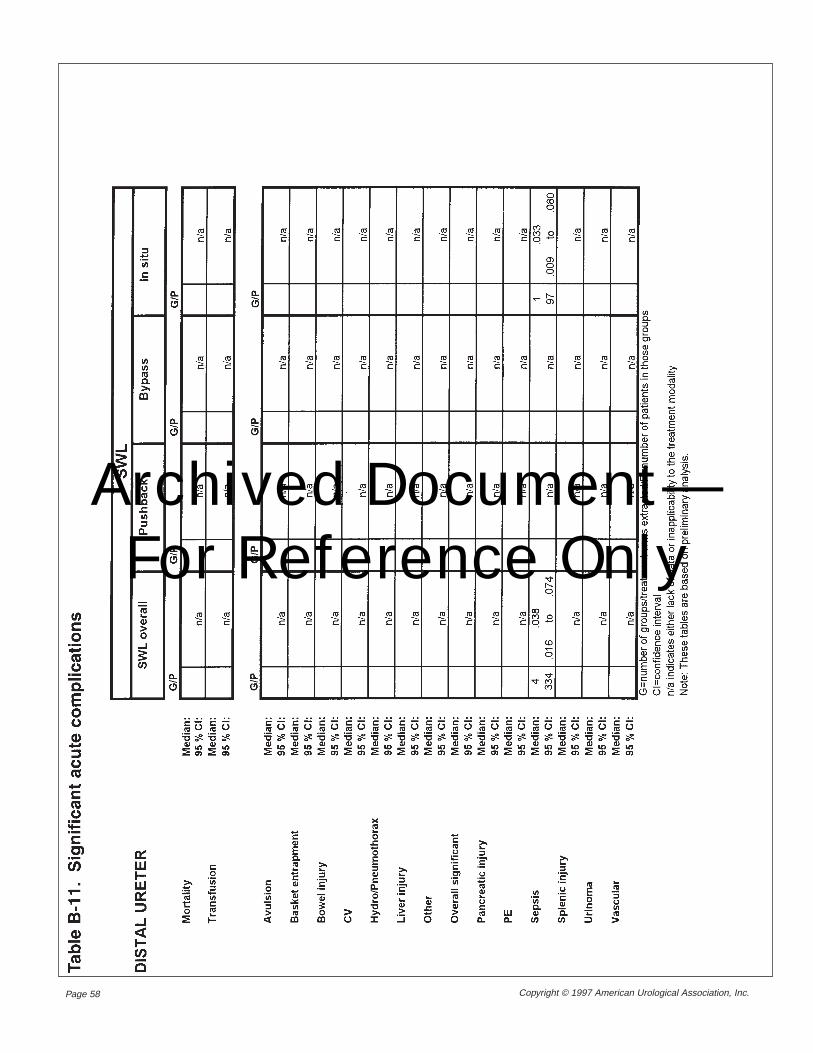
Page 58 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
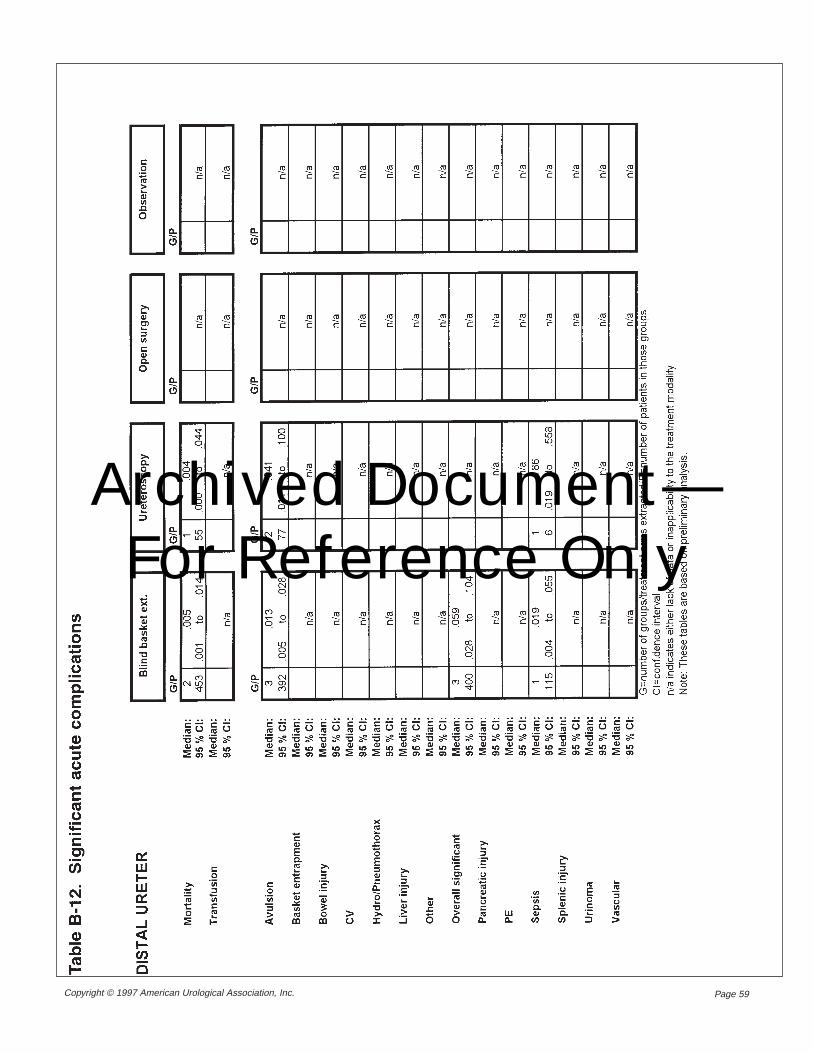
Page 59Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
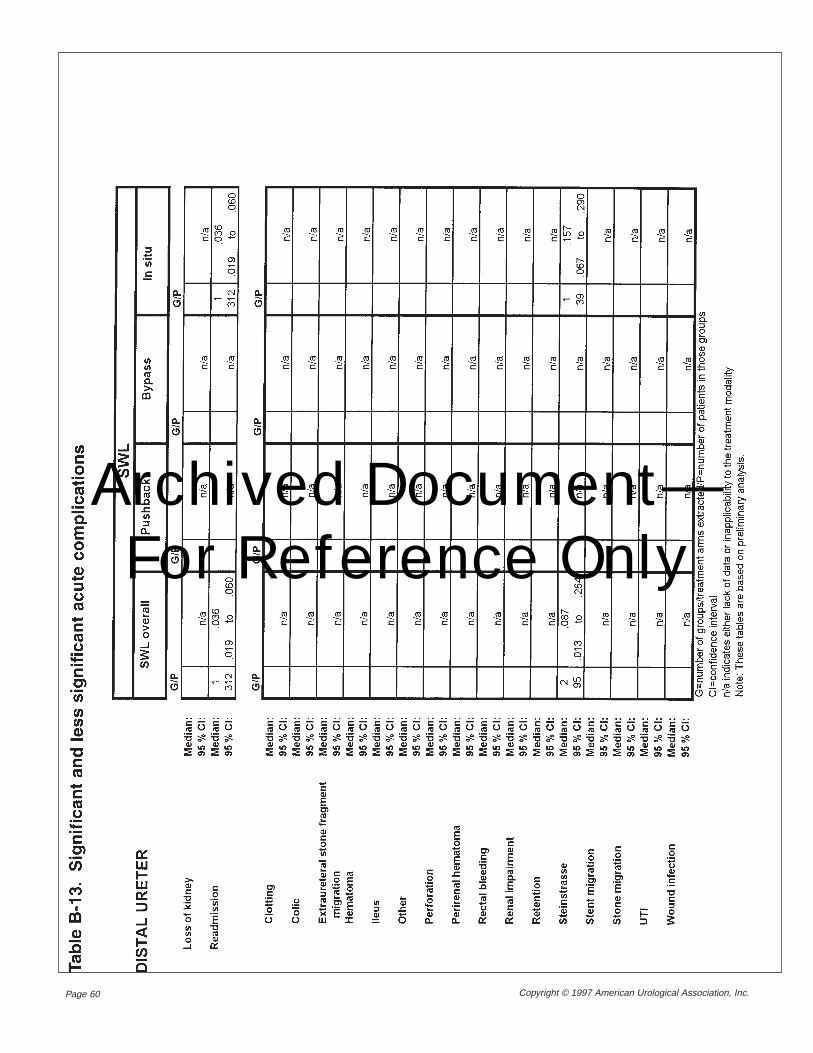
Page 60 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
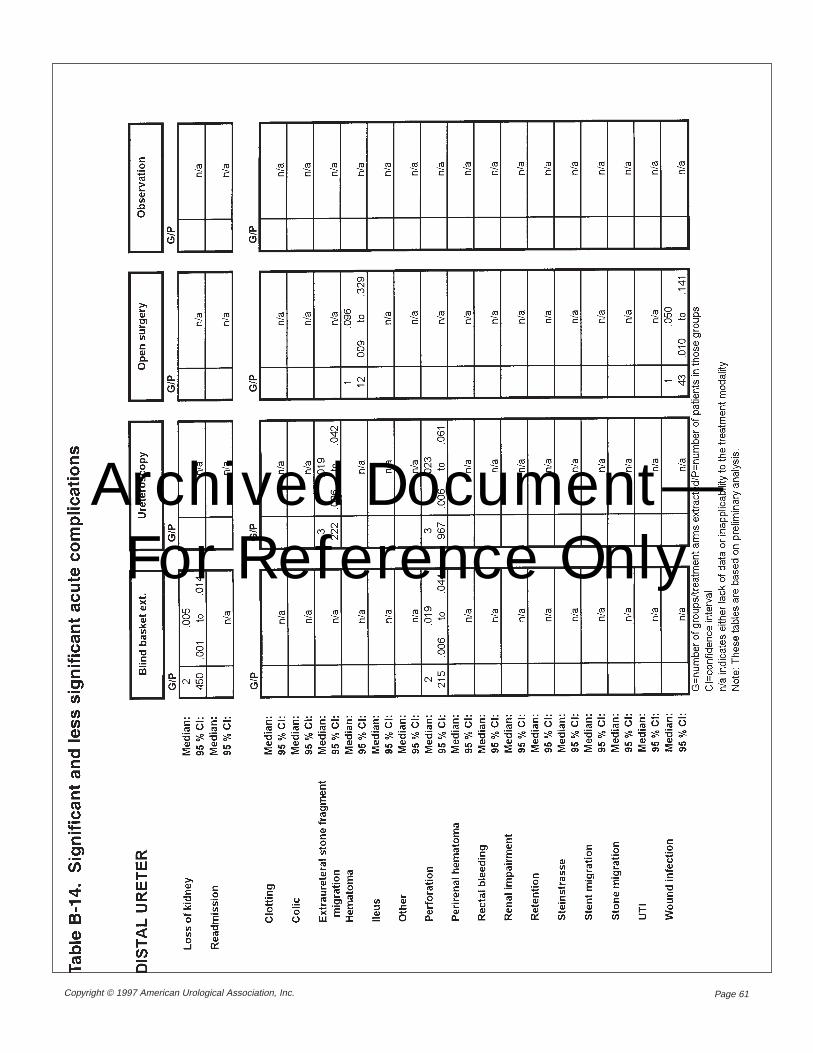
Page 61Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
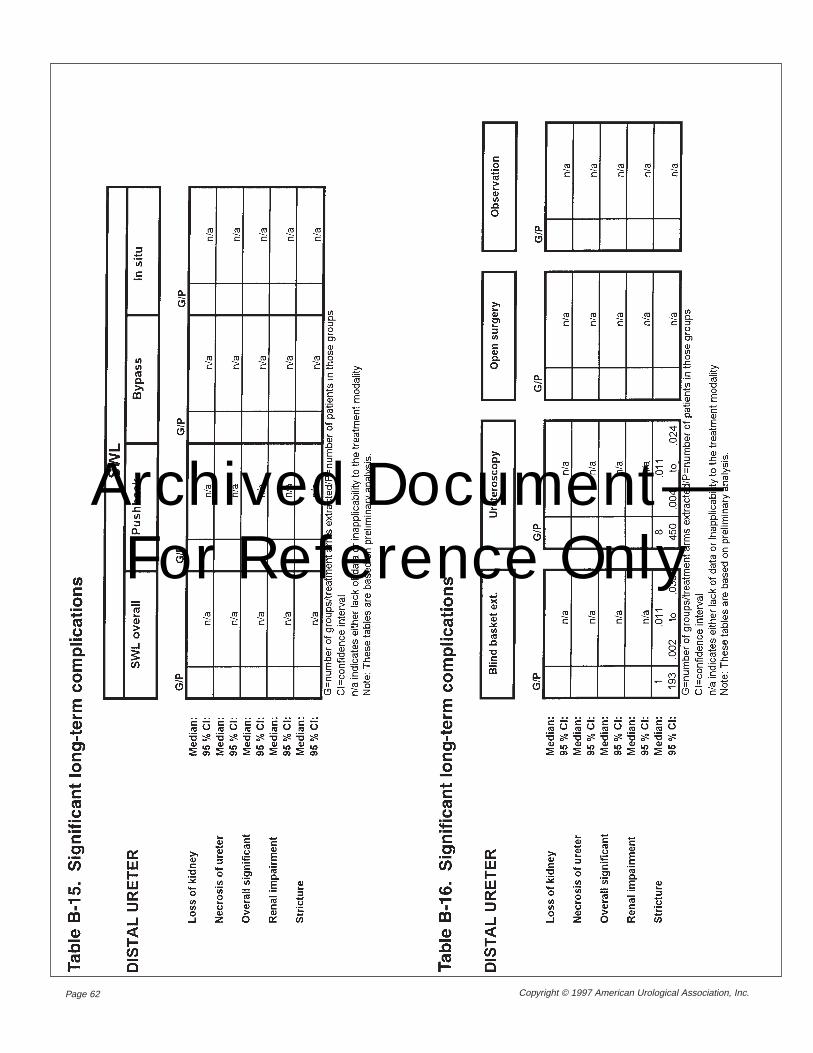
Page 62 Copyright © 1997 American Urological Association, Inc.
Archived Document— For Reference Only
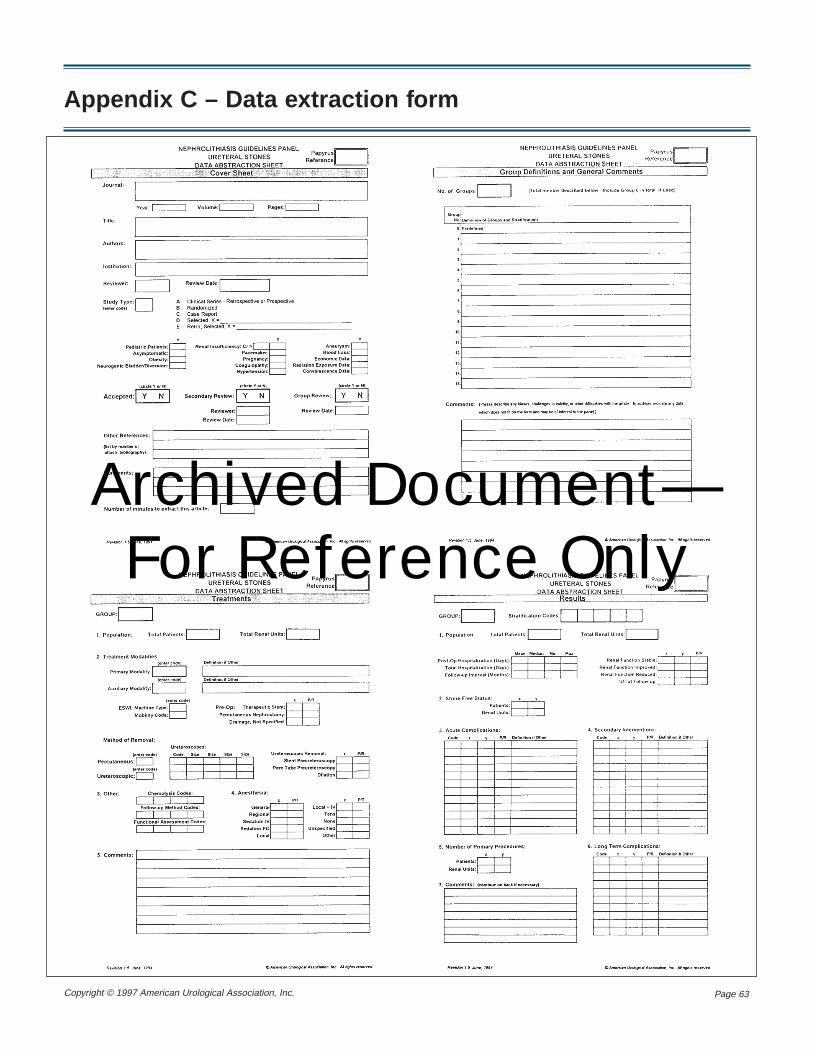
Page 63Copyright © 1997 American Urological Association, Inc.
Appendix C – Data extraction form
Archived Document— For Reference Only
Page 64 Copyright © 1997 American Urological Association, Inc.
Appendix D – Techniques for managing urinary calculi
Recorded attempts to treat patients with uri-nary tract stone disease date back to ancient Egypt(Dretler, 1995). For bladder stones, the Egyptiansattached a diamond to the end of a hollow reedwith gum and inserted it through the urethra intothe bladder. The goal was to fragment the stonewith the diamond as the patient walked around.
In the first century, A.D., perineal lithotomywas used by Roman physicians to treat patientswith bladder stones. Perineal lithotomy remainedthe accepted method for bladder stone removaluntil the 19th century. The stone was crushedand/or extracted with a forceps through the per-ineal incision. The procedure, without anesthesia,required four or five strong men to hold the pa-tient down. Without sterilized instruments, sepsiswas a common complication. Also common weresevere bleeding, perforated rectum and urinary fis-tulae—and frequently the patient died.
Surgery under such conditions was obviouslysomething to be avoided if possible. In Luchnow,India, in 1782, a Colonel Martin, who was also aphysician, faced the lithotomist’s knife himselfbecause of a bladder stone that would not pass.Having exhausted all the nonsurgical remedies ofhis day—including bladder instillation of a pow-dered mixture of lye and pigeon dung—thecolonel was desperate. Finally, he created a filethat could be inserted through his urethra into hiswater-filled bladder. By leaning forward so thatthe stone was above the bas-fond, he could gentlyfile the stone—which he did three times a day fornearly seven months. The stone disintegrated atlast, and he voided the fragments (Thorwald,1957).
Advances in the 19th century included amethod of intracorporeal lithotripsy invented bythe French surgeon Civiale. A three-prong forcepscould be inserted into the bladder and opened totrap the stone, which was then crushed by tighten-
ing an adjusting screw. There were other advancesin the 19th and early 20th centuries, includingsuch landmarks as the development of generalanesthesia and the invention of the cystoscope.Young (1902) reported the first ureteral dilationfor successful manipulation of ureteral stones.However, the major advances in treatments forstone disease have come just in the last fewdecades. Extracorporeal shock wave lithotripsy,ureteroscopy and percutaneous nephrolithotomy,along with newer methods of intracorporeallithotripsy such as laser lithotripsy, have truly rev-olutionized the management of urinary calculi.
Ever since the first patient with a renal calcu-lus was successfully treated with shock wavelithotripsy in 1980, this form of stone therapy hasrapidly gained widespread acceptance to becomethe treatment of choice for the majority of renaland ureteral calculi. Worldwide clinical serieshave documented the efficacy of shock-wavelithotripsy (Chaussy, Schmiedt, Jocham, et al.,1982; Brown and Preminger, 1988).
Shock waves are high-energy amplitudes ofpressure generated in the air or water by an abruptrelease of energy in a small space. They propagateaccording to the physical laws of acoustics andare transmitted through media with low attenua-tion. When a shock wave encounters a boundarybetween substances of differing acoustic imped-ance (density), compressive stresses are generatedthat may overcome the tensile strength of that ob-ject. Shock waves travel through water and thesoft tissues of the body with low attenuation be-cause these materials have similar densities.
However, when kidney or ureteral stones ofany composition are contacted by a shock wave ofsufficient energy, a compression wave is induced
Extracorporeal shockwave lithotripsy
Historical background
Archived Document— For Reference Only
Page 65Copyright © 1997 American Urological Association, Inc.
along the front face of the stone. As a result, thestone surface facing the shock wave begins tocrumble. As a shock wave crosses the oppositesurface of the stone, part of the energy is reflect-ed, creating tensile stress and fragmentation.Repeated shock waves eventually reduce the stoneto small fragments, ideally 2 mm or less in diame-ter, which may be passed spontaneously.
Extensive clinical testing has determined thatthe compression tensile wave phenomenon resultsin an implosion rather than an explosion of thefragments and that the total kinetic energy of allfragments can be minimized by using a largenumber of relatively low-energy shock wavesrather than fewer shocks of higher energy.
Although the basic principles of shock wavelithotripsy have not changed, a myriad of techno-logical advances and modifications in the current-ly available lithotripters have significantly ex-panded the clinical applications.
Lithotripter instrumentationAll lithotripters share four main features: an
energy source, a focusing device, a couplingmedium and a stone-localization system. Theoriginal Dornier HM-3 design utilizes a sparkplug energy generator with an elliptical reflectorfor focusing the shock waves. A water bath or wa-ter-filled cushion transmits the shock waves to thepatient with stone localization provided by bipla-nar fluoroscopy. Modifications of the four basiccomponents of the HM-3 lithotripter have nowprovided a new class of lithotripters of which tenmachines are currently either available commer-cially or undergoing clinical trials. This section onnew instrumentation reviews the features andprincipal differences between these lithotripterswith regard to shock wave generation, focusing,patient coupling and stone localization.
Shock wave generation
The two basic types of energy sources for gen-erating shock waves are point sources and extend-ed sources. The electrohydraulic devices (Dornier,Direx, Medstone, Northgate and Technomed) uti-lize point sources for energy generation, whereasextended sources are incorporated in the piezo-electric devices (Diasonics, EDAP and Wolf) andthe electromagnetic devices (Siemens).
The electrohydraulic shock wave generator islocated at the base of a water bath and produces
shock waves by an electric spark-gap of 15,000 to25,000 volts of one microsecond duration. Thehigh-voltage spark discharge produces rapid evap-oration of water, which generates a shock wave byexpanding the surrounding fluid at the first focalpoint (F1). This electrohydraulic generator is lo-cated within an ellipsoidal reflector that concen-trates the reflected shock waves at the second fo-cal point (F2).
Multiple, repeated electrohydraulic shockwaves from a first-generation machine producepain at the skin level and within the focal region,thus requiring general or regional anesthesia dur-ing lithotripsy.
Anesthesia-free second-generation electrohy-draulic lithotripters have been developed bywidening the aperture of the ellipse and decreas-ing the overall energy intensity of the shock wavegenerator. However, some form of analgesia, se-dation or local anesthesia is usually required withthe majority of second-generation electrohydrauliclithotripters.
Piezoelectric shock waves are generated by thesudden expansion of ceramic elements excited bya high-frequency, high-voltage energy pulse. Themotion of the piezoceramic elements generates anultrasonic wave which in turn produces a shockwave directed to the focal point. The shock waveis then propagated through either a water-filledbag (EDAP and Diasonics) or basin (Wolf). Thespherical focusing mechanism of the piezoelectriclithotripters provides a wide region of shock waveentry at the skin’s surface and a very small focalregion (4 x 8 mm in the Wolf lithotripter). Thecombination of a wide aperture of the focusingsphere, a larger skin-entry zone, a small focal re-gion and lower peak pressures generated by thepiezoelectric machines has provided an anesthe-sia-free form of lithotripsy.
In the electromagnetic device (Siemens),shock waves are generated when an electrical im-pulse moves a metallic membrane that is housedwithin a shock tube. The resulting shock waveproduced in the water-filled shock tube cylinder isfocused by an acoustic lens and coupled to thebody surface with a water cushion. Some form ofsedation and/or local anesthesia is usually re-quired during treatment with this electromagneticlithotripter due to the smaller aperture and moder-ate peak pressures generated. The Dornier DLCCompact lithotripter also utilizes an electromag-netic generator and is currently undergoing clini-cal trials in the United States.
Archived Document— For Reference Only
Page 66 Copyright © 1997 American Urological Association, Inc.
Shock wave focusing
Once shock waves are generated, they must befocused on the target calculus. The method of fo-cusing is dictated by the type of shock wave generation. Machines that utilize point sources,such as the electrohydraulic lithotripters, generateshock waves that travel in an expanding circularpattern and require ellipsoidal reflectors for fo-cusing the shock waves at the second focal point.The array of piezoceramic elements is positionedon a spherical disc, which allows focusing at avery small focal region, whereas the vibratingmetal membranes of the electromechanicallithotripter produce an acoustical wave that re-quires a lens for focusing the shock wave.
Coupling of the shock wave
The coupling media currently utilized by thedifferent lithotripters ranges from a 1,000-literwater bath to an enclosed water cushion. The wa-ter bath requires unique positioning of the patientin the tub so that the calculus is at the second fo-cal point. Modifications in the patient gantry sys-tem of the first-generation Dornier HM-3lithotripter now allow the treatment of children aswell as distal ureteral calculi.
Second-generation machines have adopted de-signs for coupling that minimize the space re-quirements as well as the physiological and func-tional disadvantages of a large water bath.Current models use either an enclosed watercushion, a small exposed pool of water or a total-ly contained shock tube. The water-filled cush-ions and shock tubes contain the shock wavesource, conditioned water and a coupling mem-brane to allow simplified positioning and drylithotripsy. However, the direct water-skin inter-face utilized by two units (Technomed and Wolf)is believed by some to offer improved shockwave coupling.
Stone localization
Stone localization during lithotripsy is accom-plished with either fluoroscopy or ultrasonogra-phy. Fluoroscopy provides the urologist with afamiliar modality and has the added benefits ofeffective ureteral stone localization. Moreover,fluoroscopy facilitates the use of contrast materialto help delineate the anatomy of the collectingsystem. However, fluoroscopy requires morespace and carries the inherent risk of ionizing ra-diation to both the patient and medical staff. Yet,
fluoroscopy remains the preferred method of lo-calizing ureteral calculi.
Ultrasonography is becoming an increasinglyimportant modality for the urologist.Sonography-based lithotripters offer the advan-tages of stone localization with continuous moni-toring and effective identification of radiolucentstones, without radiation exposure (Preminger,1989). Additionally, ultrasound has been docu-mented to be effective in localizing stone frag-ments as small as 2 mm. The major disadvan-tages of ultrasound stone localization include theneed for basic mastery of ultrasonic techniquesby the urologist and the difficulty in localizingureteral stones.
Instrumentation for newerlithotripters
Currently there are a number of lithotripters inclinical trials that attempt to incorporate many ofthe characteristics of an ideal lithotripter.
The basic design of the newer machines in-cludes dual-imaging capabilities as well as vari-able shock wave power. Among these machinesare the Dornier MFL 5000 (HM5), Dornier MPL9000X, EDAP LT-02, Siemens Lithostar Plus,Storz, Modulith SL-20 and Wolf Piezolith 2500.
Dual imaging
Dual-imaging capabilities entail having bothfluoroscopic and sonographic localization sys-tems available in the same machine. Such a de-sign has the advantage of utilizing fluoroscopyfor imaging stones within the ureter, while havingthe option to use sonography for identifying radi-olucent calculi. Moreover, sonographic capabili-ties allow one to initially target a stone using flu-oroscopy and then switch over to ultrasound toavoid an excessive amount of ionizing radiation.Having fluoroscopy capabilities may also lessenthe learning curve for many urologists who areunfamiliar with sonographic stone-localizationprocedures.
Interestingly, whereas the Dornier, Siemensand Storz machines have all added ultrasound ca-pabilities to provide dual imaging, none of thesesystems provides in-line imaging for both the flu-oroscopic or sonographic localization devices.For example, with the Dornier and Siemens de-vices, one can utilize sonography to target a radi-olucent or biliary tract calculus; yet the patientmust be moved blindly to the fluoroscopy unitwhich is in line with the shock wave generator.
Archived Document— For Reference Only
Page 67Copyright © 1997 American Urological Association, Inc.
Alternatively, it is possible to utilize the fluoro-scopic localization system with the Storz ma-chine, but only the ultrasound is in line with theshock wave generator.
Of these devices, only the Wolf Piezolith 2500and EDAP LT-02 at this time have both the fluo-roscopy and sonography in line with the piezo-electric shock wave generator. This design permitsrapidly changing from fluoroscopic to sonograph-ic stone localization without moving the patientoff the treatment dish.
Variable power
All six of the aforementioned third-generationdevices have variable power shock wave genera-tors that allow the operator to apply the appropri-ate amount of shock wave energy for a particularstone. One can turn down the generator power toprovide significantly reduced anesthesia/analgesiarequirements with the Dornier, EDAP, Siemensand Storz machines, as well as to provide totallyanesthesia/analgesia-free lithotripsy with the Wolfdevice. Moreover, the shock wave intensity can beincreased with all four machines to allow ade-quate fragmentation of extremely hard or largecalculi. However, when using these lithotripters inthe high-power mode, various forms of anesthe-sia/analgesia are necessary.
Thus, no one has yet developed the ultimateshock wave which allows totally anesthesia-freelithotripsy with maximum efficiency. Yet, by vary-ing the shock wave energy, one can administer ahighly efficient shock wave with the need foranesthesia/analgesia when high shock wave pres-sures are indicated. On the other hand, with asmall or soft stone, the shock wave energy can besignificantly decreased to provide minimal-anes-thesia lithotripsy.
Ureteroscopic stone removal was first reportedin 1980 (Perez-Castro-Ellendt and Martinez-Pineiro, 1980). It quickly replaced blind basketingand open surgery for removing stones in the lowerureter and today is SWL’s chief rival as a treat-ment choice for these stones. URS allows removalof stones by basket extraction or with grasping
forceps under direct vision after ureteral dilation.URS is often the method of choice (rather thanPNL) for fragmenting stones using one of fourmethods of intracorporeal lithotripsy describedbelow: ultrasonic lithotripsy, electrohydrauliclithotripsy, laser lithotripsy or pneumatic lithotrip-sy.
Ultrasonic lithotripsy (UL)Ultrasonic lithotripsy was first described by
Alken in 1982. He had used PNL to fragment kid-ney stones. Commercially available units consistof a power generator and an ultrasound transducerand a probe, both forming the sonotrode. A piezo-ceramic element in the handle of the sonotrode isstimulated to resonate, and this converts electricalenergy into ultrasound waves (with a frequency of23,000-27,000 Hz) which then are transmittedalong the hollow metal probe to create a vibratingaction at its tip. When the vibrating tip is broughtin contact with the surface of a stone, the calculuscan be disintegrated.
The probe must be rigid because sound wavescannot be transmitted without energy loss alongflexible probes. The probes come in sizes of 10 F.and 12 F. and are passed through the straightworking channel of a rigid ureteroscope ornephroscope. Suction tubing can be connected tothe end of the sonotrode probe, thus convertingthe unit into a vacuum cleaner for stone frag-ments. Normal saline at body temperature shouldbe used as irrigant.
Ultrasonic lithotripsy is generally used forfragmentation of large stones. However, some uricacid, calcium oxalate monohydrate or cystinestones may not break up easily, thereby necessi-tating EHL.
Besides the risk for perforation and extravasa-tion of irrigant, UL is associated with noise levelsof around 90 dB several inches from the transduc-er. For lengthy UL sessions, ear plugs are recom-mended. Depending on the location of the stones,retained fragments are seen in 3-35 percent of allcases treated with ultrasonic lithotripsy. This can-not be considered a failure in many cases becausethe UL is often performed for the debulking oflarge stones, to be followed by shock wave litho-tripsy as part of a planned two-stage procedure.
Electrohydraulic lithotripsy (EHL)The principles of electrohydraulic lithotripsy
(EHL) were described and developed by a
Ureteroscopy (URS)
Archived Document— For Reference Only
Page 68 Copyright © 1997 American Urological Association, Inc.
Russian engineer in 1950. This technology hasbeen used extensively for the destruction of blad-der stones, and in 1975 reports were published onits use for the fragmentation of kidney stones(Raney and Handler, 1975)]. The EHL unit has aprobe, a power generator and a foot pedal. Theprobe consists of a central metal core and two lay-ers of insulation with another metal layer betweenthem. Probes are flexible and available in multiplesizes to be used through rigid and flexible nephro-scopes.
Commercially available EHL units are manu-factured with power up to 120 volts. The electri-cal discharge is transmitted to the probe where itgenerates a spark at the tip. The intense heat pro-duction in the immediate area surrounding the tipresults in a cavitation bubble which produces ashock wave that radiates spherically in all direc-tions. Collapse of the bubble causes a secondshock wave. These shock waves, repeated at a fre-quency of 50-100 per second, result in destructionof the stone.
EHL will effectively fragment all kinds of uri-nary calculi including the very hard cystine, uricacid and calcium oxalate monohydrate stones.Since the probes are small and flexible, they canbe used through flexible nephroscopes andureteroscopes to fragment stones in calyces inac-cessible by UL through a rigid instrument. Theprimary disadvantage of EHL is its inability to ef-ficiently remove the stone fragments. All particleshave to be either washed out during intraoperativeirrigation or grasped with forceps. It is advanta-geous to fragment the stone into the smallestnumber of particles that allow extraction withgrasping devices (usually < 1 cm). There is novirtue in transforming a large stone into hundredsof small particles, or even sand-like material, be-cause a significant amount of time is required toremove the debris. Overall, EHL should be thesecond choice for routine stone fragmentation inthe kidney, but may be the procedure of choice inthe ureter.
The first experience with electrohydrauliclithotripsy in the ureter entailed a 6 F. EHL probethat was fluoroscopically guided to the obstructingcalculus (Reuter and Kern, 1973). The most com-mon cause of failure in this early experience wassecondary to the operator’s inability to pass theprobe to the level of the stone. An additional earlyexperience using EHL within the ureter describedthe use of a 9 F. probe which provided excellentfragmentation of the stone. However, 40 percent
of the patients had ureteral extravasation follow-ing the lithotripsy procedure (Raney, 1975). Thishigh complication rate was attributed to the largeprobe size. The use of a smaller 5 F. EHL probethrough the rigid ureteroscope was compromisedby decreased stone visualization because theprobe occupied most of the working channel ofthe rigid ureteroscope (Green and Lytton, 1985).
The development of a smaller 3 F. EHL probe,used through a flexible ureteroscope, was reportedin 1988 (Begun, Jacobs and Lawson, 1988). Morerecently, a 1.9 F. EHL probe has been developed.It has been quite successful in fragmenting ureter-al and intrarenal stones. An additional benefit ofthese small-caliber probes is improved visualiza-tion through the flexible ureteroscope, as a largerportion of the working channel is available for ir-rigation (Denstedt and Clayman, 1990; Feagins,Wilson and Preminger, 1990).
Laser lithotripsyLaser lithotripsy was originally developed for
the management of ureteral calculi; and signifi-cant advances in laser fibers and power-generationsystems have made laser lithotripsy, in many prac-titioners’ hands, the treatment of choice for frag-mentation of ureteral stones (Dretler, 1987).
The pulsed dye laser delivers short one-mi-crosecond pulsations at 5-10 Hz produced from acoumarin green dye. A plasma is formed at thestone surface, resulting in a highly localizedshock wave. The 504-nanometer wave length pro-duced by the dye laser is selectively absorbed bythe stone and not the surrounding ureteral wall.Because the energy is delivered in short pulses,the heat generated is minimal, thus protecting theureter (Coptcoat, Ison, Watson, et al., 1987;Dretler, 1987; Dretler, Watson, Parrish, et al.,1987).
Initial experience has yielded fragmentationrates from 64 to 95 percent (Hofmann andHartung, 1988; Higashihara, Horie, Takeuchi, etal., 1990; Morgentaler, Bridge and Dretler, 1990).Failures have been related to equipment malfunc-tion (4 to 19 percent) or more often to stone com-position. Also, the use of EHL and/or basketinghas been necessary as an adjunctive measure withthe laser in some cases of successful stone re-moval. Use of the pulsed dye laser in the ureter inall series appears to be safe. No significant intra-operative or postoperative complications havebeen noted.
Archived Document— For Reference Only

Page 69Copyright © 1997 American Urological Association, Inc.
Continued development of laser technologyhas yielded larger diameter laser fibers able tofragment hard calculi more effectively. Newer300- and 320-micrometer fibers are superior to the200-micrometer fibers in fragmentation of calci-um oxalate monohydrate and cystine stones(Dretler and Bhatta, 1991). Fragmentation rates ofgreater than 90 percent have been obtained withthe newer fibers.
As the field continues to advance, new lasers(Alexandrite, q-switched YAG and Holmium) arenow being used as sources for laser lithotripsyunits (Weber, Miller, Rüschoff, et al., 1991).Initial reports of clinical experience with theHolmium laser (Ho:YAG) have been especiallyfavorable (Bagley and Erhard, 1995; Erhard andBagley, 1995; Grasso, 1996; Shroff, Watson,Parikh, et al., 1996; Yiu, Liu, Yiu, et al., 1996).The reported results indicate that the Ho:YAG ef-fectively fragments all types of urinary calculi,wherever they are located and whatever theircomposition, including cystine stones.
The Ho:YAG produces light of 2,100 nm, withtissue penetration of less than 0.5 mm. It is also apulsed laser. Various low-water-density, quartz-fiber delivery systems and various combinationsof endoscopes and laser fibers have been devel-oped for specific applications. In combinationwith the actively deflectable, flexible uretero-scope, the Ho:YAG has proven ideally suited forfragmenting stones in the upper ureter (Bagleyand Erhard, 1995). Potential complications of theHo:YAG, when used to fragment ureteral stones,include stricture and possible perforation of theureteral wall (Shroff, Watson, Parikh, et al.,1996). This laser can also be used to cut or ablatesoft tissue, such as bladder neck contracture,ureteral and urethral strictures and prostate tissue.
Pneumatic lithotripsyPneumatic lithotripsy uses a device (frequently
called a lithoclast), in which a compressed air sys-tem is connected to a pressure box which is con-nected to a metal rod. Air pulses in the pressurebox drive a metallic bullet that strikes the end ofthe rod, driving it against the stone to be frag-mented. Each air pulse has a pressure of three at-mospheres, and pulsation frequency is 12-16Hertz (Schulze, Haupt, Piergiovanni, et al., 1993).Rods are 2.4 F. to 6 F. in diameter. They can beused with nephroscopes and cystoscopes for frag-
menting renal or bladder stones and with semi-rigid or rigid ureteroscopes for fragmentingureteral stones.
Pneumatic lithotripsy has at least three advan-tages (Dretler, 1995). One, it effectively fragmentseven the hardest large stones (Denstedt, Eberweinand Singh, 1992). Two, it is relatively inexpen-sive. Three, it is relatively safe, with only an occa-sional perforation of the ureter. Its disadvantagesare that it cannot be used through a flexibleureteroscope and that it tends to push the stonecephalad.
Percutaneous endoscopic manipulation ofstones in the renal collecting system, in its devel-opment, has no precedent in the history of urolog-ic surgery. The technique evolved, within adecade, from a procedure undertaken by a fewphysicians to a procedure performed routinely bythousands of urologists worldwide—only to thenbe forced into the background by an even morerevolutionary procedure for stone treatment,namely extracorporeal shock wave lithotripsy.
The PNL procedure begins with a percuta-neous nephrostomy tract, which needs to be estab-lished in order to gain access to the intrarenal col-lecting system. The access tract should enter thekidney through a posterior calyx, which is usuallyfacilitated by positioning the patient at 30 degreeson the fluoroscopy table. In most cases, the loweror middle pole calyces may be accessed below the12th rib, but occasionally a supracostal approachis necessary to optimally reach the targeted stone(Segura, Patterson, LeRoy, et al., 1985). Oneshould anticipate possible cephalad renal move-ment during nephrostomy access placement,which may alter the proposed approach(Preminger, Schultz, Clayman, et al., 1987).
The nephrostomy tract is formed by dilatingthe skin, fascia, muscles and renal tissues over aguide wire. Nephrostomy tract dilatation can beperformed using graduated dilators or a ballooncatheter. After the nephrostomy tract has been di-lated up to a 30 F. (10 mm diameter) size, a hol-low plastic sheath is placed into the renal pelvis.A variety of endoscopic instruments may then be
Percutaneousnephrolithotomy (PNL)
Archived Document— For Reference Only

Page 70 Copyright © 1997 American Urological Association, Inc.
passed directly into the renal collecting system toperform various manipulations.
Endoscopy is begun by performing rigid orflexible nephroscopy. Although specially designednephroscopes with a 30-degree side-arm viewingsystem are available, a traditional panendoscopeof 24 F. is equally well suited for rigidnephroscopy and allows visualization and manip-ulation inside the renal collecting system. Oncethe renal pelvis and those calyces that are accessi-ble to a rigid nephroscope have been visualizedand the surgeon is familiar with the intrarenalanatomy, flexible nephroscopy can be performedto inspect individual calyces that may not be with-in reach of the rigid instrument. With the help ofthese flexible instruments, the entire collectingsystem can be visualized by taking advantage ofthe tip deflection and rotating the instrument in-side the kidney.
The internal diameter of the working sheath isusually 30 F., which equals about 1 cm. Stones upto this size can be extracted intact through thesheath. For fragmentation of stones inside the re-nal collecting system or ureter that are too large tobe extracted (greater than 1 cm), the four intracor-poreal lithotripsy modalities are available: ultra-sonic lithotripsy (UL), electrohydraulic lithotripsy(EHL), laser lithotripsy and pneumatic lithotripsy.
Whereas shock wave lithotripsy, ureteroscopyand percutaneous nephrolithotomy have becomewidely embraced as treatments of choice for themajority of renal and ureteral calculi, the indica-tions for open surgery have decreased dramatical-ly. Assimos, Boyce, Harrison, et al. (1989) found
that, of 893 stone procedures performed since theintroduction of lithotripsy at their institution, 4.1percent required open surgery for renal calculi.The most common indication for open surgerywas failure of lithotripsy or percutaneousnephrolithotomy.
Morbidly obese patients often require opensurgery. Their body habitus precludes fluoroscopicor sonographic localization or effective treatmentof renal calculi because the shock waves becomeattenuated in the excess tissue. Also, the largeamount of adipose tissue in the flank may preventplacement of an Amplatz sheath into the renalpelvis during percutaneous nephrostolithotomy.
Stones in a collecting system with distal ob-struction may require open surgery with concomi-tant pyeloplasty. In addition, obstructed or scarredcalyceal infundibula can be repaired with calyor-rhaphy or calycoplasty after removal of the stone(Resnick, 1981). Coagulum pyelolithotomy maybe helpful in patients with many small stones inmultiple calyces. This procedure could also be ofbenefit for clearing small residual calculi in pa-tients who have undergone anatrophicnephrolithotomy (Patel, 1973).
For branched renal calculi, surgical proceduresbeyond simple open pyelolithotomy may be nec-essary for stone removal. Anatrophic nephrolitho-tomy is based on the blood supply to the kidney,using the relatively avascular plane of Brodel’sline for the lateral renal parenchymal incision pri-or to entering the collecting system. This ap-proach permits wide exposure of the renal pelvisenabling en bloc removal of the branched calculiwith minimal residual calculi (Blandy and Singh,1976). Patients with complex stones or evidenceof parenchymal loss may benefit from either par-tial or complete nephrectomy for stone disease(Assimos, Boyce, Harrison, et al., 1989).
Open surgery
Archived Document— For Reference Only
Page 71Copyright © 1997 American Urological Association, Inc.
Index
AAlexandrite lasers, 11Avulsion, 13, 24
BBalance sheet
definition and description of, 15tables, 18-21
Basket extractionand distal ureteral stones, 5, 6, 17, 25, 28, 29and proximal ureteral stones, 16, 17and ureteroscopy, 2, 6-7, 11, 13, 29blind, 1, 5, 6, 7, 12, 15-16, 17, 26, 28, 29definition and description of, 6-7, 28outcomes of, 8, 15-16, 25recommendations for, 5, 6, 7, 12, 28, 29
CCalcium monohydrate and dihydrate calculi, 1, 2, 11Calcium phosphate calculi, 11Complications of treatment, 2, 13, 16, 24-25. See also
specific complications.Confidence profile method, 9-10, 15Cystine calculi, 1, 3, 11, 26
DDeath, 24Distal ureteral stones, definition of, 3, 11, 27Dornier HM-3 shock wave machine, 13, 29Drugs. SeePharmacologic agents.
EElectrohydraulic lithotripsy (EHL), 2, 13
FFAST*PRO meta-analysis software package, 8, 9, 15,
17, 24, 25Fluoroscopy, 1, 5, 6-7, 12, 14, 15-16, 28
HHolmium lasers, 11, 29Hospitalization, 6, 14, 26, 28Hydrothorax, 24
IIntracorporeal lithotripsy, 11, 13, 16, 29
KKidney, loss of, 24
LLaparoscopy, 1, 12, 16Laser lithotripsy, 2, 11, 13, 29Lithotripters, fixed and mobile, 2, 16, 23
MMortality, seeDeath.
OObservation
and distal ureteral stones, 1-2, 3-4, 6, 23, 24and proximal ureteral stones, 1-2, 3-4, 6, 23, 24as treatment option, 1-2, 12, 26factors in deciding against intervention, 1-2, 3, 6, 11,
17outcomes of, 8, 15,17recommendations for, 3, 6, 27
Obstruction, 2, 12, 14Open surgery
and complications, 24-25and distal stones, 5, 6, 7, 17, 24, 28, 29and proximal stones, 4, 5, 6, 17, 25, 28, 29as treatment option, 1, 2-3, 4, 11, 12, 26outcomes of, 15, 25recommendations for, 4, 5, 6, 7, 26, 28, 29
Outcomes. See Outcomes under specific treatmentmethods.
PPain, 1-2, 6, 12, 27Patient
complications most concerned about, 24informing about treatment options, 3, 27standard and nonstandard, 3, 26-27
Percutaneous nephrolithotomy (PNL)and complications, 24and distal ureter, 16and proximal ureter, 2, 5, 6, 17, 25, 26
Archived Document— For Reference Only
Page 72 Copyright © 1997 American Urological Association, Inc.
as outcome, 8, 15, 17, 23as treatment option, 1, 2, 11, 12, 13-14, 26recommendations for, 5, 6, 26, 28
Pharmacologic agents, 1, 12, 26Pneumatic lithotripsy, 2, 13Pneumothorax, 24Primary and secondary procedures, 15, 16, 23, 26Proximal ureteral stones, definition of, 3, 11, 27Pulmonary embolism, 24
RRadiographic assessment (KUB), 1, 12, 17Rifamycin, 11Rowatinex™, 12
SSecondary, unplanned procedures, 23, 26Sepsis, 14, 24Shock wave lithotripsy (SWL)
and complications, 2, 13, 16, 24-25and distal stones, 5, 6, 7, 17, 24-25, 28, 29and proximal stones, 5, 6, 17, 25, 28as treatment option, 1, 2, 4, 11, 12-13, 14, 26outcomes of, 8, 15, 16, 17, 23, 24-25recommendations for, 4, 5, 6, 7, 26, 27-28, 28-29used to treat women of childbearing age, 13
Spontaneous passageand distal stones, 1, 4, 6, 12, 23, 27and oral pharmacologic agents, 1, 12and proximal stones, 1, 3, 4, 12, 23, 27as outcome, 10, 17, 23of large ureteral stones (Table 2), 24of small ureteral stones (Table 1), 23recommendations relating to, 3, 4, 6, 27
Stents, 4, 6, 14, 27-28Stone-free rates
and open surgery, 6, 16, 17, 28and percutaneous nephrolithotomy (PNL), 14, 16, 17
and shock wave lithotripsy (SWL), 6, 16, 17and ureteroscopy (URS), 17, 29as outcome, 15-17, 23, 29
Stones, seeUreteral calculi.Stricture, 16, 25
TTransfusions, 14, 24
UUltrasonic lithotripsy, 2, 13Ureteral calculi
composition of as related to treatment, 1, 3, 11, 16definition of, 1, 11greater than 1 cm, 5, 6, 7, 15, 17, 28, 29less than or equal to 1 cm, 4, 5, 6, 15, 17, 28-29location of as related to treatment, 1, 2, 11, 12, 14,
16, 17, 27Size of as related to treatment, 1-2, 3, 10, 11, 12, 16,
17, 23, 27struvite, 1, 17
Ureteral stricture. SeeStricture.Ureteroscopes, 13, 14, 25, 29Ureteroscopy (URS)
and basket extraction, 2, 6-7, 11, 13, 29and complications, 25and distal stones, 5, 6-7, 17, 26, 29and proximal stones, 5, 6, 17, 25, 29as treatment option, 1, 2, 11, 12, 13, 14, 26in conjunction with types of lithotripsy, 2, 13outcomes of, 8, 15, 16, 25, 26recommendations for, 5, 6, 7, 26, 28, 29
Uric acid calculi, 3, 11, 26Urinary tract infection, 2, 12, 24Urinoma, 24
VVascular injury, 24Visceral injury, 24
Archived Document— For Reference Only
Megan CohenHealth Policy Director
Suzanne Boland PopeGuidelines Manager
Julie BowersGuidelines Assistant
Joyce BrownGuidelines Assistant
Kim HagedornHealth Policy Projects Coordinator
American Urological Association, Inc.
This report on the Management of Ureteral Calculi was developed by the Female Stress Urinary UreteralStones Guidelines Panel of the American Urological Association, Inc.
This report is intended to furnish to the skilled practitioner a consensus of clear principles and strategies forquality patient care, based on current professional literature, clinical experience, and expert opinion. It does notestablish a fixed set of rules or define the legal standard of care, pre-empting physician judgment in individualcases.
An attempt has been made to recommend a range of generally acceptable modalities of treatment, taking in-to account variations in resources and in patient needs and preferences. It is recommended that the practitionerarticulate and document the basis for any significant deviation from these parameters.
Finally, it is recognized that conformance with these guidelines cannot ensure a successful result. The para-meters should not stifle innovation, but will, themselves, be updated and will change with both scientific knowl-edge and technological advances.
Board of Directors (1997 – 1998)
Practice Parameters, Guidelines and Standards Committee (1997 – 1998)
Health Policy Department Staff and Consultants
Roy J. Correa, Jr., MD*William R. Turner, Jr., MD*Jack W. McAninch, MDMartin I. Resnick, MD*Winston K. Mebust, MD*Brendan M. Fox, MDThomas P. Ball, Jr. MD*
Joseph W. Segura, MD, ChairIan M. Thompson, Jr., MD, Vice ChairRodney A. Appell, MDRoy J. Correa, Jr., MD, Ex OfficioRoger R. Dmochowski, MDJack S. Elder, MDThomas C. Fenter, MD, ConsultantJohn B. Forrest, MDCharles E. Hawtrey, MD, Consultant
Gerald P. Hoke, MDStuart S. Howards, MDJohn D. McConnell, MD, ConsultantWinston K. Mebust, MD, Ex OfficioSharron L. Mee, MDGlenn M. Preminger, MDMartin I. Resnick, MD, Ex OfficioClaus G. Roehrborn, MD, FacilitatorLinda D. Shortliffe, MD, Consultant
Joseph A. Smith, Jr., MD, ConsultantDatta C. Wagle, MDHanan Bell, PhD, Methodology
ConsultantCurtis Colby, Medical Editor
ConsultantPatrick M. Florer, Database
Consultant
Robin HudsonHealth Policy Projects Assistant
Theresa LincolnHealth Policy Projects Clerk
Lisa EmmonsHealth Policy Manager
Tracy KielyHealth Policy Analyst
Betty WagnerHealth Policy Assistant
Scott ReidGovernment Relations Policy Analyst
Roger WoodsGovernment Relations Assistant
Randolph B. FenningerWashington Liaison
William GlitzPublic Relations Consultant
Dennis J. Card, MD*Joseph C. Cerny, MD*Joseph N. Corriere, Jr., MDH. Logan Holtgrewe, MDLawrence W. Jones, MD*David L. McCullough, MD*Harry C. Miller, Jr., MD*
Gerald Sufrin, MD*Robert S. Waldbaum, MD*G. James GallagherMelanie H. Younger
*Voting member
Archived Document— For Reference Only
American Urological Association, Inc.1000 Corporate BoulevardLinthicum, Maryland 21090
ISBN 0-9649702-4-4
Septem
ber 1997R
eport on the Managem
ent of Ureteral C
alculi
Archived Document— For Reference Only