are susceptible to infection by human immunodeficiency virus type
TRANSCRIPT

JOURNAL OF VIROLOGY, May 1994, p. 3041-305()0022-538X/94/$04.00+0Copyright © 1994, American Society for Microbiology
Two Subpopulations of Human Triple-Negative Thymic CellsAre Susceptible to Infection by Human Immunodeficiency
Virus Type 1 In VitroHELENE VALENTIN,' MARIE-THERESE NUGEYRE,' FRANQOISE VUILLIER,2LAURENCE BOUMSELL,3 MICHEL SCHMID,3 FRANQOISE BARRE-SINOUSSI,'*
AND ROSEMARIE A. PEREIRA4
Unite de Biologie des R&trovirus' and Laboratoire d'Inmmuno-HInmatologie/Immunlo-Pathologie,2 Institult Pasteur;75724 Paris Cedex 15, and Institut de Recherche slir les Maladies dii Sang, INSERM U93, Centre Hayem, HopitalSaint-Louis, 75475 Paris Cedex 10,3 France, and Institute of Medical and Veterinary Science, Adelaide, Australia4
Received 20 May 1993/Accepted 24 January 1994
Some infants infected with human immunodeficiency virus type I (HIV-1) rapidly develop a fatal diseasecharacterized by a severe lymphopenia. To explain the immune dysfunction, we proposed a mechanism bywhich a nongeneration of CD4+ T cells is caused by HIV-1 infection of thymic cells. To examine this hypothesis,we infected primary triple-negative (TN; phenotypically CD3- CD4- CD8-), CDla- TN, or CDla+ TNthymic cell subsets. Our data indicate that by flow cytometry, TN, CDla - TN, and CDla+ TN cells remain CD4negative throughout the culture period. We demonstrated that TN and CDla+ TN thymic cell subsets are
susceptible to HIV-1 as is the entire thymic cell population, whereas CDla- TN cells are not. A limited numberof infected TN cells are expressing HIV-1 but the level of transcription is very high in permissive cells, as
detected by in situ hybridization. We then performed blocking experiments on TN cells to examine themechanism of HIV-1 entry into these cells. CD4 (OKT4a) monoclonal antibody blocks their infection. Finally,infection experiments on two subpopulations ofTN cells (CD2+ CD7+ and CD2 - CD7 -) indicate that infectedTN cells may correspond to both immature thymocytes and thymic dendritic cells. These data are of particularinterest since infection of thymic stromal cells might result in an impairment of T-cell differentiation, whichmay explain a nongeneration of functional CD4+ T-cell population in the thymus. This phenomenon may playa role in AIDS pathogenesis, in particular in infants born from seropositive mothers.
Clinical and immunological manifestations of AIDS are
known to be associated with human immunodeficiency virus(HIV) infection. However, the mechanisms responsible for thephenomenon that leads to the dramatic and ultimately fataldysfunctions of the immune system are not well defined yet.HIV-1 is known to infect cells expressing the CD4 molecule,including helper T cells (27), monocytes/macrophages (20),follicular dendritic cells (DC) (4), and brain microglial cells(12). The T-cell dysfunctions and quantitative depletion ofCD4+ cells have been thought to occur by any of a wide rangeof distinct mechanisms. Originally, the loss of CD4+ T cellsduring the course of infection was thought to be a direct resultof HIV- cytopathic effects in vitro (26). However, the propor-tion of CD4+ cells that express viral mRNA is very low, as
judged by in situ hybridization (ISH) experiments with cellsfrom patients with AIDS and AIDS-related complex (24). Incontrast, it has been shown by PCR technology that manyCD4+ circulating lymphocytes from patients with AIDS andAIDS-related complex may carry the provirus (45). Recentdata obtained by PCR ISH confirmed that the low percentageof cells producing HIV-1 is opposed to the high number oflatently infected cells (16).
Other mechanisms have been suggested to explain a part ofthe dramatic loss of CD4+ cells in patients with AIDS and thepathogenesis of AIDS, such as host-mediated cytotoxic activi-ties (42), T-cell dysfunction (reviewed in references 33, 34, and
Corresponding author. Mailing address: Unite de Biologie desR6trovirus, Institut Pasteur, 25, rue du Dr. Roux, Bt. Roux, 75724Paris Cedex 15, France. Phone: (33-1) 45 68 87 33. Fax: (33-1) 45 68 8957.
41), and cell death by apoptosis (22, 23). Programmed celldeath is a physiological response to stimulation that normallyoccurs during thymopoiesis. In HIV-infected individuals, cir-culating T cells have been reported to undergo a rapidprogrammed cell death.
Additional possible mechanisms have been proposed toaccount for the T-cell defects observed in patients with AIDS.For example, infection of the bone marrow precursors of Tcells has been suggested by in vivo studies in seropositiveindividuals (14, 46). However, in vitro HIV-1 infection of bonemarrow precursors was reported (18, 31) but is still controver-sial (17). Infection of T-cell precursors, such as mature andimmature thymocytes, by HIV-1 has also been described (15,44, 49) and could explain their failure to become maturefunctional CD4+ T cells. Authors have previously demon-strated that fresh human unfractionated and immature CD4+thymic cells are permissive in vitro to HIV-1 infection andproduce infectious virions (15, 44, 49). Indeed, de Rossi et al.have also shown that immature CD4+ CD8+ (double-positive)thymocytes are susceptible to viral infection and replication(15). Furthermore, intermediates of T-cell differentiation, in-cluding CD4+ CD8+, CD3- CD4'-lw+ CD8-, and CD16+thymic clones, are shown by PCR analysis to be susceptible toHIV-1 infection (44), whereas thymic clones entirely lackingthe CD4 molecule at their surface are described as resistant.Finally, to explain why some neonates with congenital HIV-1infection exhibit immune dysregulation, Tanaka et al. haveshown that human fetal unfractionated thymocytes, most ofwhich are CD4+, are permissive to HIV-1 in vitro and produceinfectious virions (48).
Recent studies on the SCID-hu mouse model suggested that
3041
Vol. 68, No. 5
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

3042 VALENTIN ET AL.
infected thymic cells were more apparent in the medulla thanin the cortex and that both human CD4+ CD8+ double-positive and CD4+ and CD8+ single-positive thymocytes maybe a target for HIV-1 infection (1, 8, 37, 47). Others studiesusing simian immunodeficiency virus-infected macaques indi-cated that the thymic involution was at least partially due to aloss of thymocytes observed 8 weeks postinfection (7).
All of the foregoing observations suggest a role for thethymus in the pathophysiology of AIDS. However, at whatstage of differentiation T cells become susceptible to infectionand how HIV-1 can alter T-cell differentiation remain unclear.Here, we propose that HIV-1 infection of the human triple-negative (TN; CD3- CD4- CD8-) thymic cell subset couldresult in an impairment of the immune system. To investigatethis hypothesis, we have initiated in vitro studies on thesusceptibility to HIV-1 infection of separated subsets of TNthymic cells. Our results indicate that both immature corticalthymocytes and residual thymic DC may be targets for HIV-1.
MATERIALS AND METHODS
MAbs and culture cell lines. Mouse anti-human monoclonalantibodies (MAbs) were used. They include IOT6 (CDla),IOTlla and OTlIla-fluorescein isothiocyanate (FITC) (CD2),10T3 (CD3), IOT7 and IOT7-FITC, IOT8 (CD8), and ION16(CD16) (Immunotech, Marseille, France); OKT4 and OKT4a(CD4) (Ortho Diagnostic Systems Inc., Raritan N.J.); anti-human T-cell receptor (TCR) 8/Iy-1 (Becton Dickinson & Co.,Mountain View, Calif.); 12-FITC (HLA-DR class II) andT6-RD1 (CDla) (Coulter, Hialeah, Fla.); BMA031 (anti-human TCR ac4) (Behring AG, Marburg, Germany); andCD2-phycoerythrin (PE), CD3-FITC, T4-FITC, T4-PE, T8-FITC, CD14-PE, and anti-interleukin 2 (IL-2) receptor(CD25) (Dako, Glostrup, Denmark). M232 (CD18), CD3x3,and CD8x8 were kindly provided by A. Bernard (Nice,France). 13B8.2 and biotin-conjugated L544 (CDla) MAbswere kind gifts of D. Olive (Marseille, France) and L. Boum-sell, respectively. Immunoglobulin G2a (IgG2a) (Immunotech)was used for immunodepletion and for negative control ofimmunofluorescence.CEM and NIH 3T3 cell lines were resuspended in culture
medium RPMI 1640 (Whittaker, Walkersville, Md.) supple-mented with 10% fetal calf serum (Labsystem S.A., Les Ulis,France), 2 mM L-glutamine (GIBCO Laboratories, GrandIsland, N.Y.), 50 ,ug of penicillin-streptomycin per ml, and 100,ug of neomycin (GIBCO) per ml.Preparation of thymic cell populations. Thymic tissue was
obtained from 1- to 24-month-old HIV-seronegative infantsundergoing cardiac surgery. Tissue was teased, and erythro-cytes were removed by Ficoll-Hypaque density gradient cen-trifugation (Eurobio, Les Ulis, France). Most adherent cellswere removed by allowing cells to adhere to 150-cm2 plastictissue culture flasks (Falcon) at a concentration of 0.5 x 107 to1 X 107 cells per ml in culture medium containing RPMI 1640plus 5% fetal calf serum overnight at 37°C in a humidifiedatmosphere containing 5% CO2.
Subsets of thymic cells were obtained by magnetic beaddepletion. Briefly, each depletion cycle consisted of incubationwith MAbs for 30 min at 4°C with gentle agitation followed bywashes and addition of goat anti-mouse IgG-coated magneticbeads (Dynabeads, M450; Dynal, Oslo, Norway) for 30 min at4°C with constant gentle shaking. The magnetic beads (cellbound or cell free) were removed with a strong magnet.Purification of CDla - TN and TN thymic cell subsets requiresthree cycles of depletion involving incubation with CD3 andCD4 MAbs (cycle 1), with CD3, CD4, and CD8 MAbs (cycle
2), and with CD4, CD8, and CDla MAbs or with CD4 andCD8 MAbs and IgG2a (cycle 3). Erythrocytes, residual mag-netic beads, and dead cells were then eliminated by Ficoll-Hypaque density gradient centrifugation. The final cell yieldwas consistently 0.5 to 1% of the initial number of the entirethymic cell population.From TN thymic cells, CD2+ CD7+ and CD2- CD7- or
CDla+ and CDla- thymic cells were sorted with a FACStarmicrofluorometer (Becton Dickinson). Two-color immunoflu-orescence experiments were performed by incubating the cellssimultaneously during 30 min with an FITC-conjugated CD7MAb (IOT7) and PE-conjugated CD2 MAb (IOTlla). One-color immunofluorescence experiments were done after incu-bation during 30 min with CDla MAb (IOT6) and washedbefore addition of an appropriate amount of goat F(ab')2anti-mouse FITC-conjugated IgG antibody (Immunotech).The cells were then washed and resuspended in phosphate-buffered saline. After cell sorting, the cell populations werereanalyzed for purity.The same four subsets of TN cells were also obtained after
positive or negative selection by using the magnetic beadsystem. The positive-selected TN cells were detached from themagnetic beads (DETACHaBEAD; Dynal) as instructed bythe manufacturer during 60 min at room temperature withconstant and gentle shaking.
Phenotypic analysis. The phenotypes of cell populations atthe beginning of the culture and/or throughout the cultureperiod were determined by indirect immunofluorescence.Briefly, cells were incubated with predetermined saturatedconcentrations of mouse MAb during 30 min at 4°C and thenwashed before addition of goat anti-mouse IgG-FITC during30 min at 4°C. Labeled cells were analyzed by cytofluorometryusing an EPICS 752 cell sorter (Coulter) or a FACScan(Becton Dickinson).
In vitro infection with HIV-1 and cell culture. Virus con-taining supernatants from CEM cells releasing high levels ofHIV-1(LAI) were used for infectivity studies. Fresh preparedthymic cell populations were infected with cell-free HIV-1(LAI) at multiplicities of infection ranging from 0.1 to 1 for 60min at 37°C in a 5% CO2 atmosphere. A heat-inactivated (60min at 56°C) virus solution was also incubated with thymic cellpopulations as a control. Infected cells were washed exten-sively to remove unbound virus and subsequently resuspendedat 106 cells per ml in a fresh culture medium consisting ofRPMI 1640 supplemented with 10% fetal calf serum, 10%semipurified IL-2 (Biotest, Frankfurt, Germany), 2 ,ug ofPolybrene (Sigma Chemical Co., St. Louis, Mo.) per ml, 1 U ofsheep anti-human alpha interferon serum (Boehringer-Mann-heim, Meylan, France) per ml, L-glutamine, and antibiotics.The cells were then activated for 3 days with 7.5 ,ug ofphytohemagglutinin P (PHA; Difco, Detroit, Mich.) per ml.Activation was performed at that time in order to limit T-celldifferentiation before addition of HIV-1. All cultures wereincubated at 37°C in a humidified atmosphere containing 5%CO2.
Reverse transcriptase (RT) assays were carried out as pre-viously described (5). Viral p25 antigen (Ag) expression wasmeasured by a capture immunoassay as instructed by themanufacturer (ELAVIA Ag I kit; Diagnostics Pasteur, MarnesLacoquette, France). Culture supernatants and cells weresampled every 3 to 4 days for RT activity and viral Ag, for ISHto detect viral mRNA, and for PCR analysis. On day 9 afterviral inoculation, an aliquot of infected thymic cells wascocultivated at a ratio of 1:3 with PHA-stimulated humanperipheral blood lymphocytes (PBL) from one HIV-seroneg-ative donor. The cocultures were maintained at 106 cells per ml
J. VIROL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.
HIV-1 INFECTION OF TWO HUMAN THYMIC CELL SUBSETS 3043
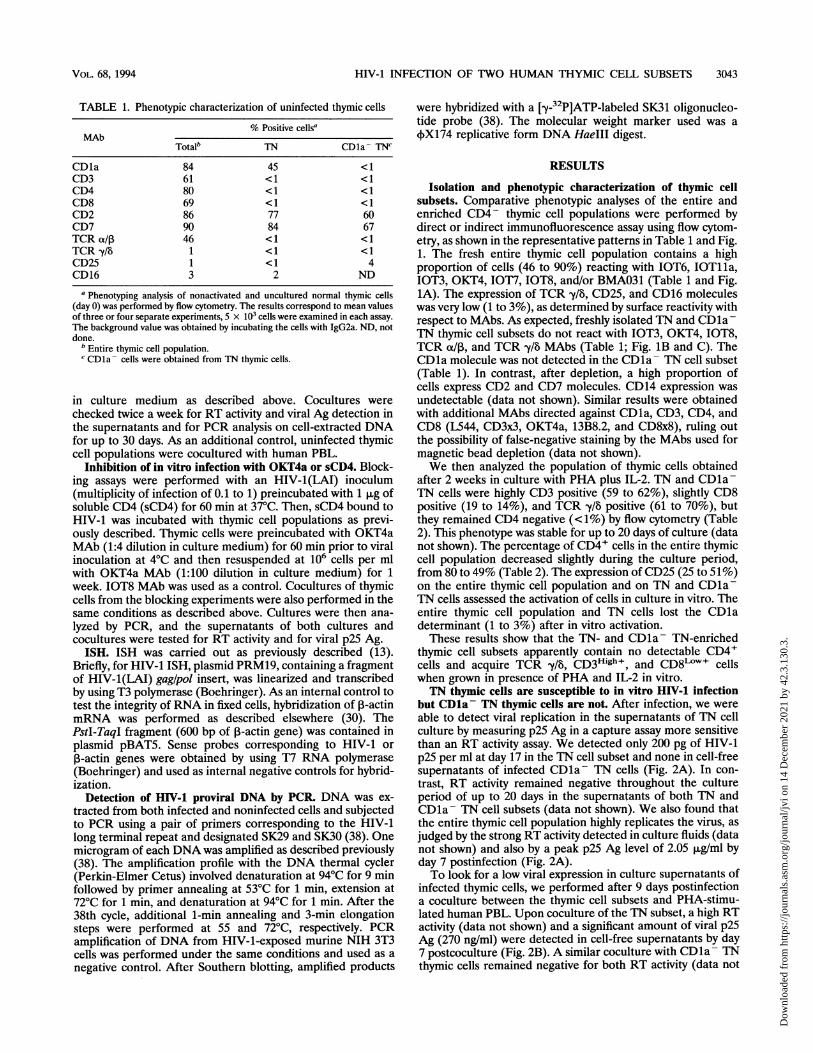
TABLE 1. Phenotypic characterization of uninfected thymic cells
% Positive cellsaMAb
Totalb TN CDla- TNC
CDla 84 45 <1CD3 61 <1 <1CD4 80 <1 <1CD8 69 <1 <1CD2 86 77 60CD7 90 84 67TCR t/ 46 < 1 <1TCR -y/8 1 < 1 < 1CD25 1 < 1 4CD16 3 2 ND
a Phenotyping analysis of nonactivated and uncultured normal thymic cells(day 0) was performed by flow cytometry. The results correspond to mean valuesof three or four separate experiments, 5 x 103 cells were examined in each assay.The background value was obtained by incubating the cells with IgG2a. ND, notdone.
b Entire thymic cell population.c CD1a - cells were obtained from TN thymic cells.
in culture medium as described above. Cocultures werechecked twice a week for RT activity and viral Ag detection inthe supernatants and for PCR analysis on cell-extracted DNAfor up to 30 days. As an additional control, uninfected thymiccell populations were cocultured with human PBL.
Inhibition of in vitro infection with OKT4a or sCD4. Block-ing assays were performed with an HIV-1(LAI) inoculum(multiplicity of infection of 0.1 to 1) preincubated with 1 ,ug ofsoluble CD4 (sCD4) for 60 min at 37°C. Then, sCD4 bound toHIV-1 was incubated with thymic cell populations as previ-ously described. Thymic cells were preincubated with OKT4aMAb (1:4 dilution in culture medium) for 60 min prior to viralinoculation at 4°C and then resuspended at 106 cells per mlwith OKT4a MAb (1:100 dilution in culture medium) for 1week. IOT8 MAb was used as a control. Cocultures of thymiccells from the blocking experiments were also performed in thesame conditions as described above. Cultures were then ana-lyzed by PCR, and the supernatants of both cultures andcocultures were tested for RT activity and for viral p25 Ag.
ISH. ISH was carried out as previously described (13).Briefly, for HIV-1 ISH, plasmid PRM19, containing a fragmentof HIV-1(LAI) gag/pol insert, was linearized and transcribedby using T3 polymerase (Boehringer). As an internal control totest the integrity of RNA in fixed cells, hybridization of 1-actinmRNA was performed as described elsewhere (30). ThePstI-TaqI fragment (600 bp of ,B-actin gene) was contained inplasmid pBAT5. Sense probes corresponding to HIV-1 or,B-actin genes were obtained by using T7 RNA polymerase(Boehringer) and used as internal negative controls for hybrid-ization.
Detection of HIV-1 proviral DNA by PCR. DNA was ex-tracted from both infected and noninfected cells and subjectedto PCR using a pair of primers corresponding to the HIV-1long terminal repeat and designated SK29 and SK30 (38). Onemicrogram of each DNA was amplified as described previously(38). The amplification profile with the DNA thermal cycler(Perkin-Elmer Cetus) involved denaturation at 94°C for 9 minfollowed by primer annealing at 53°C for 1 min, extension at72°C for 1 min, and denaturation at 94°C for 1 min. After the38th cycle, additional 1-min annealing and 3-min elongationsteps were performed at 55 and 72°C, respectively. PCRamplification of DNA from HIV-1-exposed murine NIH 3T3cells was performed under the same conditions and used as anegative control. After Southern blotting, amplified products
were hybridized with a [-y-32P]ATP-labeled SK31 oligonucleo-tide probe (38). The molecular weight marker used was a(X174 replicative form DNA HaeIII digest.
RESULTS
Isolation and phenotypic characterization of thymic cellsubsets. Comparative phenotypic analyses of the entire andenriched CD4- thymic cell populations were performed bydirect or indirect immunofluorescence assay using flow cytom-etry, as shown in the representative patterns in Table 1 and Fig.1. The fresh entire thymic cell population contains a highproportion of cells (46 to 90%) reacting with IOT6, IOT1la,IOT3, OKT4, IOT7, IOT8, and/or BMA031 (Table 1 and Fig.1A). The expression of TCR -y/l, CD25, and CD16 moleculeswas very low (1 to 3%), as determined by surface reactivity withrespect to MAbs. As expected, freshly isolated TN and CDla -TN thymic cell subsets do not react with IOT3, OKT4, IOT8,TCR ot/,B, and TCR y/8 MAbs (Table 1; Fig. 1B and C). TheCD1a molecule was not detected in the CD1a - TN cell subset(Table 1). In contrast, after depletion, a high proportion ofcells express CD2 and CD7 molecules. CD14 expression wasundetectable (data not shown). Similar results were obtainedwith additional MAbs directed against CDla, CD3, CD4, andCD8 (L544, CD3x3, OKT4a, 13B8.2, and CD8x8), ruling outthe possibility of false-negative staining by the MAbs used formagnetic bead depletion (data not shown).We then analyzed the population of thymic cells obtained
after 2 weeks in culture with PHA plus IL-2. TN and CDla-TN cells were highly CD3 positive (59 to 62%), slightly CD8positive (19 to 14%), and TCR -y/l positive (61 to 70%), butthey remained CD4 negative (<1%) by flow cytometry (Table2). This phenotype was stable for up to 20 days of culture (datanot shown). The percentage of CD4+ cells in the entire thymiccell population decreased slightly during the culture period,from 80 to 49% (Table 2). The expression of CD25 (25 to 51%)on the entire thymic cell population and on TN and CDla-TN cells assessed the activation of cells in culture in vitro. Theentire thymic cell population and TN cells lost the CDladeterminant (1 to 3%) after in vitro activation.These results show that the TN- and CDla- TN-enriched
thymic cell subsets apparently contain no detectable CD4+cells and acquire TCR /y, CD3High+, and CD8"'w+ cellswhen grown in presence of PHA and IL-2 in vitro.TN thymic cells are susceptible to in vitro HIV-1 infection
but CDla- TN thymic cells are not. After infection, we wereable to detect viral replication in the supernatants of TN cellculture by measuring p25 Ag in a capture assay more sensitivethan an RT activity assay. We detected only 200 pg of HIV-1p25 per ml at day 17 in the TN cell subset and none in cell-freesupernatants of infected CDla- TN cells (Fig. 2A). In con-trast, RT activity remained negative throughout the cultureperiod of up to 20 days in the supernatants of both TN andCDla- TN cell subsets (data not shown). We also found thatthe entire thymic cell population highly replicates the virus, asjudged by the strong RT activity detected in culture fluids (datanot shown) and also by a peak p25 Ag level of 2.05 ,ug/ml byday 7 postinfection (Fig. 2A).To look for a low viral expression in culture supernatants of
infected thymic cells, we performed after 9 days postinfectiona coculture between the thymic cell subsets and PHA-stimu-lated human PBL. Upon coculture of the TN subset, a high RTactivity (data not shown) and a significant amount of viral p25Ag (270 ng/ml) were detected in cell-free supernatants by day7 postcoculture (Fig. 2B). A similar coculture with CDla- TNthymic cells remained negative for both RT activity (data not
VOL. 68, 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

CD4
LIIR~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'F-.
U .~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
CONTROL
.1 1 1e lee ieee
OVERLAY:SINGLE PARAMETER__________ __
C
w4tCD
t
.1 1 18±eee ieee
LOG FLUORESCENCE INTENSiTY'FIG. 1. Determination of CD4 molecule expression in uncultured entire thymic cell populations (A), TN cells (B), and CDla- TN cells (C)
by flow cytometric analysis (5,000 cells counted). In each panel, the dark line correspond to the background, while the dotted line shows CD4expression.
3044
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

HIV-1 INFECTION OF TWO HUMAN THYMIC CELL SUBSETS 3045
TABLE 2. Phenotypic characterization of infected and uninfectedthymic cells
% Positive cells'MAb T btlh Total + TN + CDla- CDla- TNTotal HIV-1 HIV-1 TNc + HIV-1
CDla 3 7 1 <1 1 <1CD3 84 79 59 59 62 61CD4 49 1 <1 <1 <1 <1CD8 72 91 19 19 14 12CD2 90 95 75 75 75 NDCD7 94 95 83 82 79 NDTCR os/, 73 65 2 1 4 3TCR y/l 2 5 61 55 70 62CD25 51 35 46 50 25 NDCD16 < 1 1 14 17 ND ND
a Phenotyping analysis was performed as described for Table 1 but on eitherinfected or noninfected 15-day cultured cells. ND, not done.
b Entire thymic cell population.c CDla- cells were obtained from TN thymic cells.
shown) and viral p25 Ag during up to 25 days of the cocultureperiod (Fig. 2B). As expected, no virus replication was ob-served in the entire thymic cell population, either noninfectedor exposed to heat-inactivated virus (Fig. 2).These results suggested that only CDla+ TN cells may be
sensitive to HIV-1. However, to evaluate their permissivity to
I*a
tQ
.:>
0 3 7 10 13 17 20 24 30
Time after culture (days)
the virus, we highly purified the CDla+ subset (93%) from theTN population (Table 3). After 8 days postinfection, the cellsreplicate the virus, as judged by the detection of viral p25 Agin the culture supernatants (Table 3).These data suggest that the TN thymic cell subset and in
particular CDla+ TN cells are susceptible to HIV-1 infectionand that, in contrast, CDla- TN thymic cells are not.Only a few CDla+ TN thymic cells express HIV-1 mRNA as
detected by ISH. In a third set of experiments, the frequencyand level of HIV-1 expression in infected TN thymic cellsubsets was evaluated by ISH. Figure 3 shows a representativefield obtained with either the entire or the TN thymic cellpopulation, 9 days postinfection, after hybridization with a35S-labeled HIV-1 probe. Our results consistently demon-strated that up to 30% of the entire infected thymic cellpopulation expressed HIV-1 mRNA (Fig. 3B), whereas a lowpercentage (between 0.2 to 0.5%) of TN cells was positive byISH (Fig. 3C). However, in this low percentage of positive TNcells, a large number of silver grains were observed, suggestinga very high level of expression of HIV-1 gag/pol transcripts inthese infected cells. In contrast, the inoculated CDla- TNthymic cells were negative (Fig. 3D). The percentage ofpositive TN cells was consistently low, with no significantvariation at days 4, 7, 9, 13, 15, and 21 postinfection (Fig. 3C,Table 3, and data not shown).The specificity of ISH was assessed by using several controls.
As expected, the noninfected entire thymic cell population was
CaPu
:>
1051
410
103
102
101I
..-0
0 3 7 10 2014 17
Days after coculture with activated PBL
FIG. 2. (A) p25 detection by a capture enzyme-linked immunosorbent assay in culture supernatants of the entire noninfected thymic cell
population (EJ), the entire thymic cell population infected by HIV-1 (LAI) (-), the entire thymic cell population infected by heat-inactivatedHIV-1 (0), infected TN thymic cells (A), and infected CDla- TN cells (A). The sensitivity limit of the p25 Ag assay used is 50 pg/ml, as indicated
(----). (B) p25 detection in coculture supernatants of total noninfected thymic cells (O), the entire thymic cell population infected byheated-inactivated HIV-1 (0), infected TN thymic cells (A), and infected CDla- TN cells cocultured with stimulated PBL (A).
B
VOL. 68, 1994
0----
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

3046 VALENTIN ET AL.
TABLE 3. Infected TN thymic cells seem to correspond toimmature thymocytes and residual stroma cells
% Positive cellsb Viral % HIV-1Thymic populationa p25 Ag mRNA
CD4 CDla CD2 CD7 (ng/ml)c by ISHd
Expt 1TN <1 45 77 84 14.4 0.3CDla- TN <1 <1 60 67 <0.005 NDCDla+ TN <1 93 90 95 6.8 0.8
Expt 2TN <1 51 90 95 0.49 0.5CD2+ CD7+ TN <1 60 90 93 0.9 0.3CD2- CD7- TN 3 17 3 3 12.7 10a TN designates the CD3- CD4+ILow CD8 thymic cells. CDla+, CDla-,
CD2+ CD7+, and CD2- CD7- cells were obtained from TN thymic cells asdescribed in Materials and Methods.
b Labeling of thymic cell subsets was obtained by direct or indirect immuno-fluorescence at day 0.
c In culture supernatant of HIV-1-infected thymic cells at day 8 postinfection.The sensitivity limit of the p25 Ag assay is 0.05 ng/ml.
d Detection of HIV-1 transcripts by ISH was carried out at day 5 postinfection.ND, not detected.
negative for HIV-1 mRNA expression (Fig. 3A). All CDla-TN thymic cells exposed to HIV-1 (Fig. 3E) as well asuninfected entire and TN thymic cell populations (data notshown) were positive by ISH with use of the 1-actin probe,indicating the integrity of thymic cell mRNA. In comparison,we noticed a significant decrease in 3-actin hybridization signalin the entire infected thymic cell population, suggesting thatHIV-1 may modulate P-actin expression (data not shown). Asan internal control, the sense HIV-1 and 1-actin riboprobeswere tested at the same specific activities as the antisenseprobes, and no significant background was observed underidentical exposure conditions (data not shown).These results further support the observation that a very
limited number of cells in TN and CDla+ TN thymic cellsubsets replicate the virus, but each positive cell expresses avery high level of HIV-1 mRNA.
HIV-1 infection does not affect cell surface molecule expres-sion in the TN thymic cell subset. To determine whether theexpression of HIV-1 transcripts in the entire and TN thymiccell populations modulates the expression of a variety of cellsurface molecules, flow cytometry analysis of HIV-1-infectedthymic cells was performed by day 15 postinfection (Table 2).The infected entire thymic cell population exhibited a declineof CD4 expression to undetectable levels (<1%; Table 2).Moreover, HIV-1 infection of the entire thymic cell populationalso resulted in a decrease of CD25 expression (51%, com-pared with 35% in infected cells). These effects correspondedto the peak of RT activity and were probably due to the knowneffects of HIV-1 for CD4+ lymphoid cells and to the decreaseof cell activation after infection (5, 27). The same results wereobtained by days 8, 21, and 30 postinfection. In contrast, suchflow cytometry analysis revealed no phenotypic change of TNand CDla- TN thymic cells infected with HIV-1.OKT4a MAb blocks HIV-1 infection ofTN thymic cells. The
foregoing results indicated that TN cells were CD4 negative byflow cytometry (Fig. 1B and Table 2). To examine whetherHIV-1 enters the TN cells via the CD4 receptor, we performedblocking experiments using CD4-specific MAb. To detect anyminimal viral expression, the OKT4a-treated cells were cocul-tured on day 9 after infection with PHA-stimulated PBL. Ourresults indicate that OKT4a MAb inhibited viral p25 Agproduction in supernatants of the TN thymic cell subsetcocultured with activated PBL (Fig. 4A). Similar results were
obtained with sCD4. In contrast, CD8 (IOT8) MAb was unableto block HIV-1 infection of TN thymic cells, as judged by thepresence of viral p25 Ag in coculture supernatants (Fig. 4A).Similar results were observed in the RT activity assay (data notshown).
Because we were unable to detect viral p25 Ag in coculturesupernatants of the blocking experiments, the presenceof HIV-1 long terminal repeat sequences was examined bygene amplification of DNA from TN cells infected and treatedwith OKT4a MAb or sCD4 (Fig. 4B). Based on PCR anal-ysis, OKT4a MAb and sCD4 appeared to totally abrogateHIV-1 infection in TN cell subset (Fig. 4B, lanes 9 and 10).This result suggests that HIV-1-permissive cells in this subsetwere CD4+/I"w, i.e., probably very low according to theundetectable cell surface CD4 expression by flow cytometry.Specificity of PCR signals was assessed by using severalcontrols. Negative controls were including samples withoutDNA or DNAs from the entire thymic cell population, eithernoninfected or infected with heat-inactivated virus. DNA fromHIV-1-exposed NIH 3T3 was also included as a negativecontrol. No proviral sequence was detected in DNA from thosecells (Fig. 4B, lanes 1 to 3 and 5) or in DNA from the entirethymic cell population exposed to HIV-1 pretreated with sCD4(Fig. 4B, lane 6). Positive controls consisted of DNA frominfected entire and TN thymic cell populations with or withoutIOT8 preincubation prior to HIV-1 exposure (Fig. 4B, lanes 4,7, and 8).
In conclusion, our results strongly suggest that HIV-1 infec-tion of TN thymic cells is mediated via the CD4 molecule,although the expression of CD4 is very low, i.e., not detectableby flow cytometry. According to these, data HIV-1-permissivecells found in the TN thymic cell subset should be renamedCD3- CD4+'L/w CD8-.
Infected TN thymic cells correspond to both immaturethymocytes and thymic stroma cells. We have shown that theminor subpopulation of TN cells sensitive to HIV-1 infectionexpress the CDla molecule. In the thymus, two cell popula-tions constitutively express CDla: cortical immature thymo-cytes and thymic DC (6, 9). To determine the nature ofinfected CDla+ TN cells, we performed magnetic bead deple-tion or cell sorting experiments with CD2 and CD7 MAbs. Asshown in Table 3, the phenotypic characterization of the CD2+CD7+ (90 to 93% of double positive) and CD2- CD7- (97%of double negative) fractions from TN cells indicates that theyare highly enriched. CD4 molecule expression was not detect-able on the surface of uncultured CD2+ CD7+ TN cells butwas at a low level (3%) on CD2- CD7- TN cells. CD2+CD7+ and CD2- CD7- fractions expressed 60 and 17%,respectively, of CDla molecules.
Surprisingly, on day 8 postinfection, we were able to detectviral p25 Ag in the supernatant of both CD2+ CD7+ andCD2 - CD7 - fractions (Table 3). Finally, we also found HIV-1mRNA expression in those fractions by ISH (Table 3). Only avery limited number of CD2+ CD7+ TN cells were HIV-1positive (0.3%) as found for TN cells, whereas a higher numberwas identified in the CD2- CD7- fraction (10%). The pre-dominant population infected by HIV-1 in the TN cells maythus be the CD2 - CD7 - TN subset.These data strongly suggest that there are two populations
of cells in the TN (CD3 - CD4+'L/°w CD8 -) subset thatsupport HIV infection: cortical thymocytes (CD2+ CD7+CD4+/I"w) and residual thymic stroma cells (CD2- CD7-CD4+/Low).
J. VIROL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

HIV-1 INFECTION OF TWO HUMAN THYMIC CELL SUBSETS 3047
vft' B
at . 'A- 44, f* ft -. 4. 'ft ft. iS -.
V * 2W rj4. j.
ftft.ftS.. .' '4 -
- A
Al~~~~~~~~~~~~~~~~~~~~.t
9 4'
C- 'ft ft 'I
ft ft
ft. 0
5 ft tftftft *,ft .k w .. -ft ft 'ft ft
* ft. ft
* 1 ft 'ft -,¶ ft9. ft ft ft4 'ft A ft ft
5 ft ft ft. ft. 7 ft
ft.> ft ft 4, ft
ft ft.' ft
ft - / . . S . *. £ft ft.. ;k.' ft ft ft S j ft
ftlfrA '' ., ft ft
ft 4 *5 ft,ft.
.4* .1
* ~ ~~ ' *..t1 4.. -$5*
# '~ at'
*.~~~~~~~AY * 0 0 s
L98. * '
F~~~a-z aA,.t , e,..3LFIG. 3. Expression of HIV-1 transcripts by ISH in infected entire and TN thymic cell populations. Subsets of thymic cells were submitted to
ISH using a "S-labeled antisense riboprobe corresponding to HIV-1(LAI) gag/pol sequences. Infected and uninfected cells were examined after9 days of culture; the exposure time of the autoradiographs was 8 days. (A) Entire noninfected thymic cell population; (B) positive control [entirethymic cell population infected with HIV-1(LAI)]; (C) infected TN thymic cells; (D) CDla- TN cells exposed to HIV-1; (E) internal controlcorresponding to infected CDla- TN cells hybridized with a "S-labeled antisense P-actin riboprobe.
DISCUSSION
The human thymus is an active organ in the T-lymphoidsystem during the perinatal period. Multipotential hemopoi-etic precursors migrate into the thymus, where they differen-tiate into Ag-reactive T cells before being released into thecirculation (10). This maturation correlates with the expressionof membrane molecules (21) in parallel with immunocompe-tent functions such as helper, killer, and suppressive functions.Immunopathological events associated with infectious diseases
are often linked with abnormal immune responses and/oralterations of lymphopoiesis or thymopoiesis. In AIDS patho-genesis, T-cell precursors that express either low or high levelsof the CD4 receptor were reported to be permissive to HIV-1(15, 44, 49). In the present study, we investigated the possibilitythat immature CD4 - thymic subsets of T-cell lineage are
susceptible to HIV-1 infection. We show that TN thymic cells,as defined by flow cytometry, are clearly sensitive to infectionby HIV-1 (Fig. 2). Using ISH experiments, we found that only
VOL. 68, 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

3048 VALENTIN ET AL.
105
104
103
210 -
1021:
3 7 10
Days after coculture with activ
1 2 3 4 5 6 7 8
FIG. 4. Blocking of HIV-1 infection of TI(OKT4a) MAb. (A) p25 Ag detection in ce
PHA-stimulated human PBL cocultured with iipreincubated with CD8 MAb (IOT8) (A), inpreincubated with CD4 MAb (OKT4a) (A).infected with HIV-1 preincubated with sCD4sensitivity of the assay. (B) Detection of HIV-DNA extracted from 9-day cultures of cells treLanes: 1, no-DNA PCR control; 2, uninfecpopulation; 3, NIH 3T3 cells exposed to HI'entire thymic cell population; 5, entire thymiclated with heated HIV-1; 6, entire thymic cellHIV-1 treated with sCD4; 7, infected TN thymcell population preincubated with IOT8 and thTN thymic cells preincubated with OKT4a an(thymic cells inoculated with sCD4-treated HI
a small percentage of TN thymic cells areinfection but express high levels of HIV-and may thus serve as a reservoir for virinfection of TN cells might occur thrcintrathymic cells such as thymocytes or th
by extrathymic cells such as those circ
migrating then from other tissues.Flow cytometry assays of the TN cell
MAb failed to show any detectable CD4 (
surface, compared with that of the entiretion (Fig. 1; Tables 2 and 3). However, 4that HIV-1 entry into TN cells depend
expression. First, with the PCR technology after reverse tran-
A scription, we found CD4 mRNA expression in TN cells (datanot shown). Second, the infection of TN cells was blocked byMAb directed to the CD4 epitope (OKT4a) recognized byHIV-1 gpl2O (Fig. 4). According to Chapel et al. (11), HIV-1-permissive cells in the TN subset probably express a sufficientamount of CD4 molecules on their surface to allow infection.Thus, they might be an intermediate between CD3- CD4-CD8- and CD3- CD4+ CD8+ thymocytes, as has alreadybeen described in the literature (3, 19, 43). However, weprovide no evidence that our primary TN cell population issimilar to CD3 - CD4+II'w thymic clones found to be sensitiveto HIV-1 by Schnittman et al. (44), since CD4 expression wasnever detected in our cell subset by flow cytometry (Fig. 1B).Based on blocking experiments, we also cannot entirely ex-clude that HIV-1 enters TN thymic cells through an alternativepathway. Possible allosteric effects of the CD4-OKT4a MAbcomplex may interfere with the ability of HIV-1 to bind to areceptor other than CD4.To identify the CD3 - CD4+L°w CD8 - subpopulation of
.----------------.TN cells that is sensitive to HIV-1, we first purified CDla+ andCDla- cells from TN cells. When CDla+ cells are removedfrom the TN thymic cell subset, the remaining cell populationis resistant to HIV-1 infection, as judged by the sensitive viralAg capture assay performed on culture and coculture super-natants and by ISH experiments on HIV-1-exposed CDla-TN cells (Fig. 2 and 3; Table 3). In addition, HIV-1 does not..... ....
seem to penetrate into CDla- TN thymic cells, since no14 17 20 HIV-1 proviral sequence is detected by PCR in DNA extracted
from those infected cells (data not shown). Several hypothesiszatedPBL may explain why TN thymic cells, but not CDla- TN cells, are9 10 B susceptible to HIV-1, even though both subsets express CD4
mRNA (data not shown). The mechanism of regulation ofCD4 molecule expression is still unknown, and thus it is
* 105 bp possible that most immature intrathymic T cells, like CDla-TN cells, express CD4 mRNA but no CD4 surface molecule, orat least not enough to be infected. Moreover, CDla- TN cells
N thymic cells by CD4 may lack other molecules possibly involved as coreceptors on11-free supernatants of their surface, in contrast to their expression on TN cells.nfected TN thymic cells CDla - TN cells are probably more immature thymocytes thanifected TN thymic cells TN cells. This hypothesis, in agreement with other studies (2,, and TN thymic cells 19, 29, 43), implies that CD1 is expressed earlier than CD3,*1 sequences by PCR in CD4, or CD8 during T-cell differentiation. In this case, it isated or not with MAb. likely that HIV-1 infection occurs only at this stage of T-cellted entire thymic cell differentiation, since the CDla+ TN fraction was found toV-1; 4, HIV-1-infected replicate the virus (Table 3).cell population inocu- However, in the thymus, there are two populations of cellspopulation exposed to that express CDla: cortical immature thymocytes and thymic
iic cells; 8, entire thymic DC. We therefore could not exclude from our results thatien infected; 9, infected HIV-1-sensitive CDla+ TN cells are either one or both ofd then infected; 10, TN those two thymic cell populations. We thus studied both CD2+
*1 CD7+ and CD2- CD7- fractions, obtained from the TNsubset, and showed that both are able to replicate HIV-1, asevidenced by viral mRNA expression and virus production
susceptible to HIV-1 (Table 3). These results strongly suggest that both CD2+1 transcripts (Fig. 3) CD7+ cortical immature TN thymocytes and CD2 - CD7-ral spreading. HIV-1 residual thymic stroma cells are permissive to HIV-1 in vitro.ugh either infected The level of CDla expression in the CD2- CD7- TN fractionymic stromal cells or (17%) does not allow us to reach a conclusion as to the thymiculating in blood or DC origin of those cells (Table 3). However, we have indirect
evidence that HIV-1-permissive CD2- CD7- thymic stromaI subset with OKT4 cells are thymic DC. First, CD2 - CD7 - TN cells do notexpression at the cell express the CD14 monocyte/macrophage marker. In contrast,thymic cell popula- they express a high level of HLA-DR but a low level of thymic
several data indicate fibroblast (TE-7) and epithelial (TE-3) molecules. In addition,Is on CD4 molecule we show that human purified thymic fibroblasts and epithelial
J. VIROL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

HIV-1 INFECTION OF TWO HUMAN THYMIC CELL SUBSETS 3049
cells do not support HIV-1 replication in vitro (unpublisheddata). According to these data, the only stromal cells that maybe a target for HIV-1 remain thymic DC. Recent studies ofHIV-1-seropositive children and of simian immunodeficiencyvirus-infected monkeys in vivo indicate an atrophy of thethymus with alterations of thymic stroma cells (7, 25, 35, 36).DC from various origins were described as a potential reservoirfor HIV-1 in blood and lymph nodes (28, 32, 39, 40). A recentreport on early thymic precursors in mice indicates that DCand thymocytes may originate from a common low-CD4precursor (3). With regard to our study, this result is ofinterest, suggesting the presence of this precursor in our TNsubset. Whatever their origin, DC or other thymic stroma cellsare known to play a major role in the intrathymic differentia-tion of T cells (10). Thus, any disorders of thymic stroma cellfunctions that might be induced by HIV-1 may lead to anabnormal selection of T cells in the thymus. In our opinion,such a process should be considered in AIDS pathogenesis ininfants, although most probably, multiple and complex mech-anisms are involved.
ACKNOWLEDGMENTS
We thank Robert Bassin (Bethesda, Md.), Alan Rein, Dave Ott,Jacqueline London, Daniel Cefai, Daniel Scott, and Patrice Debre(Paris, France) for helpful discussions and critical comments. We arevery grateful to F. Leca (Paris, France) for providing thymus fromcardiac surgery in infants. We are also indebted to Rosemay Vazeuxfor plasmid PRM19, Fawzia Louache for plasmid pBAT5, GabrielGras and Guillaume Dighiero for flow cytometry analysis, Luc d'Au-riol and Nicole Monplaisir for selecting or synthesizing oligonucleotideprimers and probes, and David Klatzmann for sCD4. Finally, we aregrateful to Raymond Whitham for corrections of the English.
This work was supported by the Agence Nationale de Recherche surle SIDA, by the Fondation pour la Recherche Medicale, and by theFrench Ministry of Foreign Affairs.
REFERENCES1. Aldrovandi, G. M., G. Feuer, L. Gao, B. Jamieson, M. Kristeva,
I. S. Y. Chen, and J. A. Zack. 1993. The SCID-hu mouse as amodel for HIV-1 infection. Nature (London) 363:732-736.
2. Alvarez-Vallina, L., A. Gonzalez, F. Gambon, M. Kreisler, and F.Diaz-Espada. 1993. Delimitation of the proliferative stages in thehuman thymus indicates that cell expansion occurs before theexpression of CD3 (T cell receptor). J. Immunol. 150:8-16.
3. Ardavin, C., L. Wu, C.-L. Li, and K. Shortman. 1993. Thymicdendritic cells and T cells develop simultaneously in the thymusfrom a common precursor population. Nature (London) 362:761-763.
4. Armstrong, J. A., and R. Horne. 1984. Follicular dendritic cells andvirus-like particles in AIDS-related lymphadenopathy. Lancetii:370-372.
5. Barre-Sinoussi, F., J. C. Chermann, F. Rey, M. T. Nugeyre, S.Chamaret, C. Axler-Blin, F. Vesinet-Brun, C. Rouzioux, W. Roze-baum, and L. Montagnier. 1983. Isolation of a T lymphotropicretrovirus from a patient at risk for acquired immune deficiencysyndrome (AIDS). Science 220:868-870.
6. Barthelemy, H., M. Pelletier, D. Landry, M. Lafontaine, C.Perreault, C. Tautu, and S. Montplaisir. 1986. Demonstration ofOKT6 antigen on human thymic dendritic cells in culture. Lab.Invest. 55:540-545.
7. Baskin, G. B., M. Murphey-Corb, L. N. Martin, B. Davison-Fairburn, F.-S. Hu, and D. Kuebler. 1991. Thymus in simianimmunodeficiency virus-infected rhesus monkeys. Lab. Invest.65:400-407.
8. Bonyhadi, M. L., L. Rabin, S. Salimi, D. A. Brown, J. Kosek, J. M.McCune, and H. Kaneshima. 1993. HIV induces thymus depletionin vivo. Nature (London) 363:728-732.
9. Boumsell, L. 1989. Cluster report: CD1, p. 251-258. In W. Knapp(ed.), Leucocyte typing IV. White cell differentiation antigens.Oxford University Press, Oxford.
10. Boyd, R. L., and P. Hugo. 1991. Towards an integrated view ofthymopoiesis. Immunol. Today 12:71-78.
11. Chapel, A., A. Bensussan, E. Vilmer, and D. Dormont. 1992.Differential human immunodeficiency virus expression in CD4+cloned lymphocytes: from viral latency to replication. J. Virol.66:3966-3970.
12. Chiodi, F., S. Fuerstenberg, M. Gidlund, B. Asjo, and E. M. Fenyo.1987. Infection of brain-derived cells with the human immunode-ficiency virus. J. Virol. 61:1244-1247.
13. David, F. J. E., B. Autran, H. C. Tran, E. Menu, M. Raphael, P.Debre, B. L. Hsi, T. G. Wegman, F. Barre-Sinoussi, and G.Chaouat. 1992. Human trophoblast cells express CD4 and are
permissive for productive infection with HIV-1. Clin. Exp. Immu-nol. 88:10-16.
14. Davis, B. R., D. H. Schwartz, J. C. Marx, C. E. Johnson, J. M.Berry, J. Lynding, T. C. Merigan, and A. Zander. 1991. Absent or
rare human immunodeficiency virus infection of bone marrow
stem/progenitor cells in vivo. J. Virol. 65:1985-1990.15. de Rossi, A., M.-L. Calabro, M. Panozzo, D. Bernardi, B. Caruzo,
G. Tridente, and L. Chieco-Banchi. 1990. In vitro studies of HIV-1infection in thymic lymphocytes: a putative role of the thymus inAIDS pathogenesis. AIDS Res. Hum. Retroviruses 6:287-297.
16. Embretson, J., M. Zupancic, J. L. Ribas, A. Burke, P. Racz, K.Tenner-Racz, and A. T. Haase. 1993. Massive covert infection ofhelper T lymphocytes and macrophages by HIV during theincubation period of AIDS. Nature (London) 362:359-362.
17. Folks, T. M. 1991. Human immunodeficiency virus in bone mar-
row: still more questions than answers. Blood 77:1625-1626.18. Folks, T. M., S. W. Kessler, J. M. Orenstein, J. S. Justement, E. S.
Jaffe, and A. S. Fauci. 1988. Infection and replication of HIV-1 inpurified progenitor cells of normal human bone marrow. Science242:919-922.
19. Galy, A., S. Verma, A. Barcena, and H. Spits. 1993. Precursors ofCD3+CD4+CD8+ cells in the human thymus are defined byexpression of CD34. Delineation of early events in human thymicdevelopment. J. Exp. Med. 178:391-401.
20. Gartner, S., P. Markovits, D. M. Markovits, M. H. Kaplan, R. C.Gallo, and M. Popovic. 1986. The role of mononuclear phagocytesin HTLVIII/LAV infection. Science 233:215-219.
21. Gelin, C., L. Boumsell, J. Dausset, and A. Bernard. 1984. Theheterogeneity and functional capacities of human thymocyte sub-populations. Proc. Natl. Acad. Sci. USA 81:4912-4916.
22. Gougeon, M.-L., R. Olivier, S. Garcia, D. Guetard, T. Dragic, C.Dauguet, and L. Montagnier. 1991. Mise en evidence d'un pro-cessus d'engagement vers la mort cellulaire par apoptose dans leslymphocytes de patients infect6s par le VIH. C.R. Acad. Sci. ParisSer. III 312:529-537.
23. Groux, H., G. Torpier, D. Monte, Y. Mouton, A. Capron, and J.-C.Ameisen. 1992. Activation-induced death by apoptosis in CD4+ Tcells from human immunodeficiency virus-infected asymptomaticindividuals. J. Exp. Med. 175:331-340.
24. Harper, M. E., L. M. Marselle, R. C. Gallo, and F. Wong-Staal.1986. Detection of lymphocytes expressing human T-lymphotropicvirus type III in lymph nodes and peripheral blood from infectedindividual by situ hybridization. Proc. Natl. Acad. Sci. USA83:772-776.
25. Joshi, V. V., J. M. Oleske, S. Saad, C. Gadol, E. Connor, R. M.Bobila and A. B. Minnefoz. 1986. Thymus biopsy in children withacquired immunodeficiency syndrome. Arch. Pathol. Lab. Med.110:837-842.
26. Klatzmann, D., E. Champagne, S. Chamaret, J. Gruest, D. Gue-tard, T. Hercend, J. C. Gluckman, and L. Montagnier. 1984.T-lymphocytes T4 molecule behaves as the receptor for humanretrovirus LAV. Nature (London) 312:767-768.
27. Klatzmann, Q., F. Barre-Sinoussi, M.-T. Nugeyre, C. Dauguet,J.-C. Chermann, and L. Montagnier. 1984. Selective tropism oflymphoadenopathy associated virus (LAV) for helper-inducer Tlymphocytes. Science 225:59-63.
28. Langhoff, E., E. F. Terwilliger, H. J. Bos, K. H. Kalland, M. C.Poznansky, 0. M. L. Bacon, and W. A. Haseltine. 1991. Replica-tion of human immunodeficiency virus type 1 in primary dendriticcell cultures. Proc. Natl. Acad. Sci. USA 88:7998-8002.
29. Lanier, L. L., J. P. Allison, and J. H. Phillips. 1986. Correlation of
VOL. 68? 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.

3050 VALENTIN ET AL.
cell surface antigen expression on human thymocytes by multi-color flow cytometric analysis: implications for differentiation. J.Immunol. 137:2501-2507.
30. Louache, F., A. Bettaieb, A. Henri, E. Oksenhendler, J.-P. Farcet,P. Bierling, M. Seligmann, and W. Vainchenker. 1991. Infection ofmegakaryocytes by human immunodeficiency virus in seropositivepatients with human thrombocytopenic purpura. Blood 78:1697-1705.
31. Lunardi-Iskandar, Y., M.-T. Nugeyre, V. Georgoulias, F. Barre-Sinoussi, C. Jasmin, and J.-C. Chermann. 1989. Replication ofhuman immunodeficiency virus 1 and impaired differentiation of Tcells after in vitro infection of bone marrow immature T cells. J.Clin. Invest. 83:610-615.
32. Macatonia, S. E., R. Lau, S. Patterson, A. J. Pinching, and S. C.Knight. 1990. Dendritic cell infection, depletion and dysfunctionin HIV-infected individuals. Immunology 71:38-45.
33. Matsuyama, T., K. Nobayashi, and N. Yamamoto. 1991. Cytokinesand HIV infection: is AIDS a tumor necrosis factor disease? AIDS5:1405-1417.
34. Miedema, F., M. Tersmette, and R. A. W. van Lier. 1990. AIDSpathogenesis: a dynamic interaction between HIV and the im-mune system. Immunol. Today 11:293-296.
35. Muller, J. G., V. Krenn, S. Czub, C. Stahl-Henning, C. Coulibaly,G. Hunsmann, C. Kneitz, T. Kerbau, A. Rethwilm, V. terMeulen,and H. K. Muller-Hermelink. 1993. Alteration of thymus corticalepithelium and interdigitating dendritic cells but no increase ofthymocyte cell death in the early course of simian immunodefi-ciency virus infection. Am. J. Pathol. 143:699-713.
36. Muller, J. G., V. Krenn, S. Czub, C. Stahl-Henning, C. Coulibaly,G. Hunsmann, and H. K. Muller-Hermelink. 1993. The thymicepithelial reticulum and interdigitating cells in SIV-induced thy-mus atrophy and its comparison with other forms of thymusinvolution. Res. Virol. 144:93-98.
37. Namikawa, R., H. Kaneshima, M. Lieberman, I. L. Weissman, andJ. M. McCune. 1988. Infection of the SCID-hu mouse by HIV-1.Science 242:1684-1686.
38. Ou, C.-Y., S. Kwok, S. W. Mitchell, D. H. Mack, J. J. Sninsky, J.Krebs, P. Feorino, D. Warfield, and G. Schochetman. 1988. DNAamplification for direct detection of HIV-1 in DNA of peripheralblood mononuclear cells. Science 239:295-297.
39. Pantaleo, G., C. Graziosi, L. Butini, P. A. Pizzo, S. M. Shnittman,D. P. Kotler, and A. S. Fauci. 1991. Lymphoid organs function asa major reservoirs for human immunodeficiency virus. Proc. Natl.Acad. Sci. USA 88:9838-9842.
40. Patterson, S., and S. C. Knight. 1987. Susceptibility of humanperipheral blood dendritic cells to infection by human immuno-deficiency virus. J. Gen. Virol. 68:1177-1181.
41. Pinching, A. J., and K. E. Nye. 1990. Defective signal transduction.A common mechanism for cellular dysfunction in HIV infection?Immunol. Today 11:256-259.
42. Plata, F., B. Autran, L. Pedroza, S. Wain-Hobson, M. Raphael, C.Mayaud, M. Denis, J.-M. Guillon, and P. Debre. 1987. AIDSvirus-specific cytotoxic T lymphocytes in lung disorders. Nature(London) 328:348-351.
43. Schmitt, C., S. Ktorza, S. Sarun, C. Blanc, R. De Jong, and P.Debre. 1993. CD34 expressing human thymocyte precursors pro-liferate in response to IL7 but have lost myeloid differentiationpotential. Blood 82:3675-3685.
44. Schnittman, S. M., S. M. Denning, J. J. Greenhouse, J. S.Justement, M. Baseler, J. Kurtzberg, B. F. Haynes, and A. S.Fauci. 1990. Evidence for susceptibility of intrathymic T-cellprecusors and their progeny carrying T-cell antigen receptorphenotypes TCRcx+ and TCRy8b to human immunodeficiencyvirus infection: a mechanism for CD4+ (T4) lymphocyte depletion.Proc. Natl. Acad. Sci. USA 87:7727-7731.
45. Schnittman, S. M., M. C. Psallidopoulos, H. C. Lane, L. Thomp-son, M. Baseler, F. Massari, C. H. Fox, N. P. Salzman, and A. S.Fauci. 1989. The reservoir for HIV-1 in human peripheral blood isa T cell that maintains expression of CD4. Science 245:305-308.
46. Stanley, S. K., S. W. Kessler, J. S. Justement, S. M. Schnittman,J. J. Greenhouse, C. C. Brown, L. Musongela, K. Musey, B.Kapita, and A. Fauci. 1992. CD34+ bone marrow cells are infectedwith HIV in a subset of seropositive individuals. J. Immunol.149:689-697.
47. Stanley, S. K., J. M. McCune, H. Kaneshima, J. S. Justement, M.Sullivan, E. Boone, M. Baseler, J. Adelsberger, M. Bonyhadi, J.Orenstein, C. H. Fox, and A. S. Fauci. 1993. Human immunode-ficiency virus infection of the human thymus and disruption of thethymic microenvironment in the SCID-hu mouse. J. Exp. Med.178:1151-1163.
48. Tanaka, K. E., W. C. Hatch, Y. Kress, R. Soeiro, T. Calvelli, W. K.Rashbaum, A. Rubinstein, and W. D. Lyman. 1992. HIV-1 infec-tion of human fetal thymocytes. J. Acquired Immune Defic. Syndr.5:94-101.
49. Tremblay, M., K. Numazaki, H. Goldman, and M. Wainberg. 1990.Infection of human thymic lymphocytes by HIV-1. J. AcquiredImmune Defic. Syndr. 3:356-360.
J. VIROL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
vi o
n 14
Dec
embe
r 20
21 b
y 42
.3.1
30.3
.