arterial blood gas analysis in respiratory disorders
TRANSCRIPT

ARTERIAL BLOOD GAS ANALYSIS IN RESPIRATORY DISORDERS
Dr.R.SelvakumarProfessor of AnaesthesiologyK.A.P.Viswanatham Govt Medical College,Trichy-Tamilnadu-India
A knowledge about basics and patient’s clinical historyis important in reading ABG.. just like ECG….
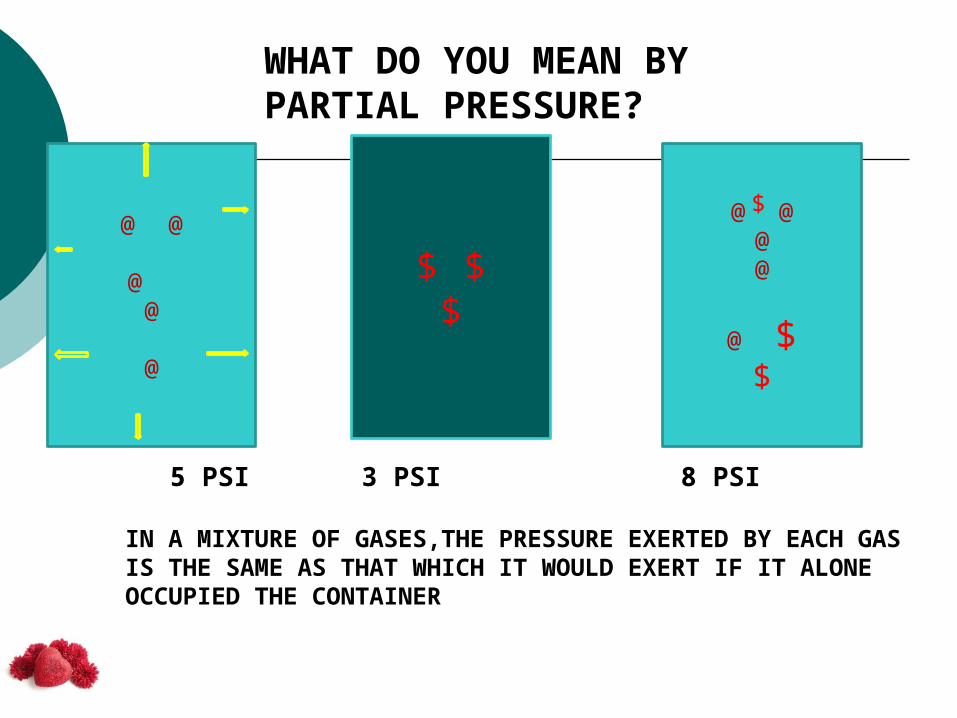
WHAT DO YOU MEAN BY PARTIAL PRESSURE?
@ @
@@
@
$ $$
@ @@@
@ $$
IN A MIXTURE OF GASES,THE PRESSURE EXERTED BY EACH GASIS THE SAME AS THAT WHICH IT WOULD EXERT IF IT ALONEOCCUPIED THE CONTAINER
$
5 PSI 3 PSI 8 PSI

DALTON’S LAW OF PARTIAL PRESSURE
THE PROPORTION OF THE PRESSURE EXERTED BY A GASIN THE TOTAL PRESSURE IS EQUATED WITH THE VOLUMEIT OCCUPIES
@ @@@
@
$$
$
PRESSURE OF @ GAS = 5 PSIPRESSURE OF $ GAS = 3 PSITOTAL PRESSURE = 8 PSI
What is the % contribution of pressure of @ gasin the total pressure?5/8 x 100 = 62.5%
So, gas @ will occupy62.5% of the total volume

Total atmospheric pressure -760 mm of Hg
Out of this 760, 78% is contributed byNitrogen and 21 % is contributedby Oxygen
21/100 x 760 = 160
Partial pressure of Oxygen in the atmosphere
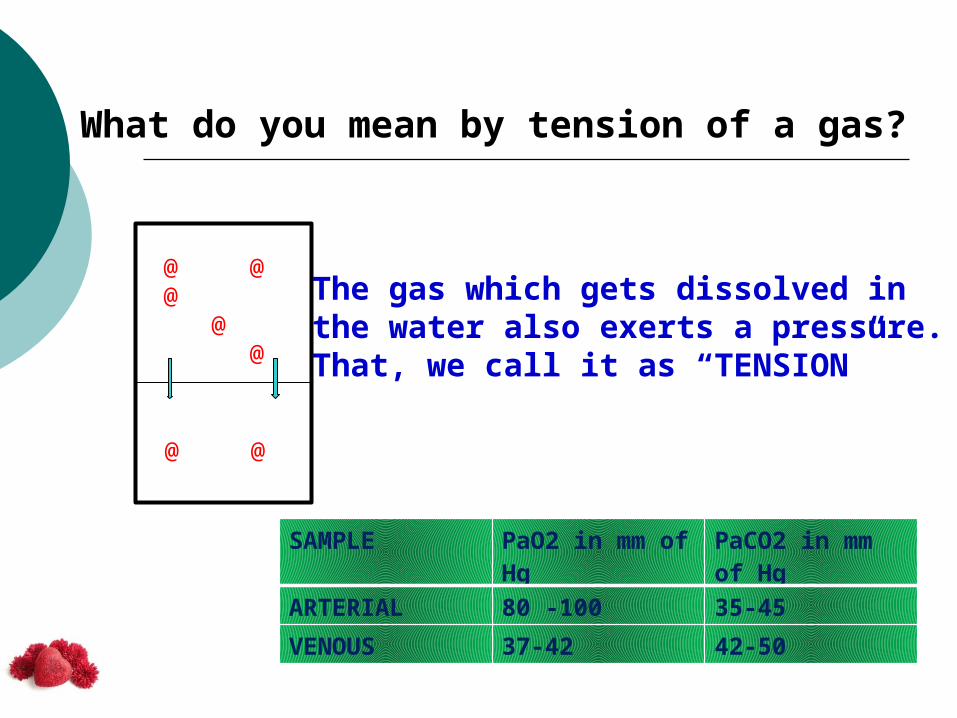
What do you mean by tension of a gas?
@ @@
@ @
@ @
The gas which gets dissolved in the water also exerts a pressure.That, we call it as “TENSION”
SAMPLE PaO2 in mm of Hg
PaCO2 in mm of Hg
ARTERIAL 80 -100 35-45VENOUS 37-42 42-50

What do you mean by FIO2?
• The % of O2 in the inspired gas mixture
• In room air , it is 21% or 0.21
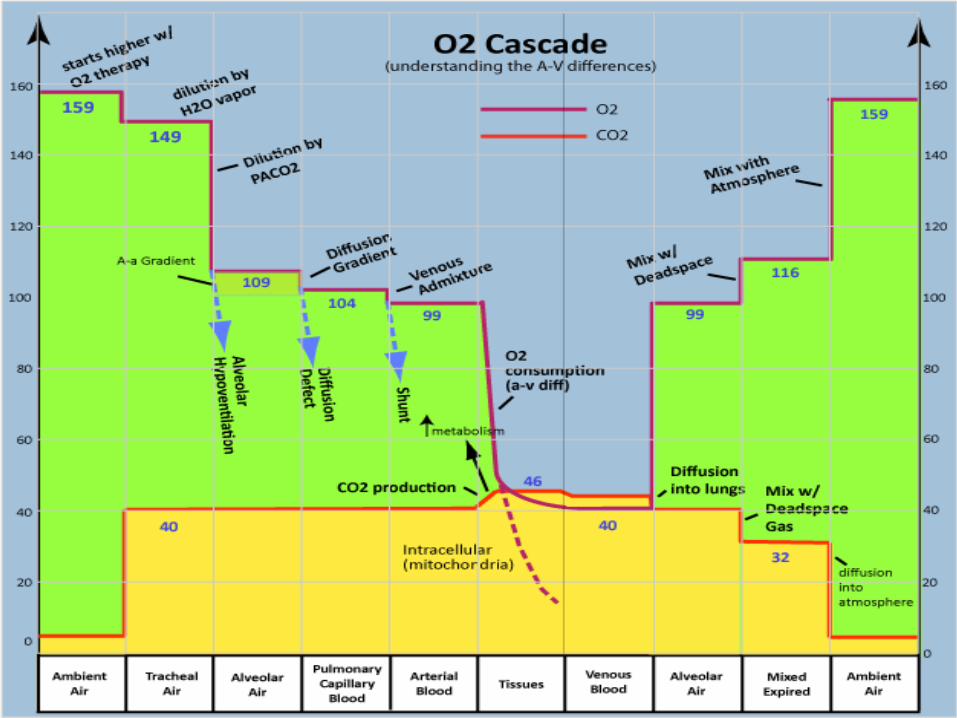
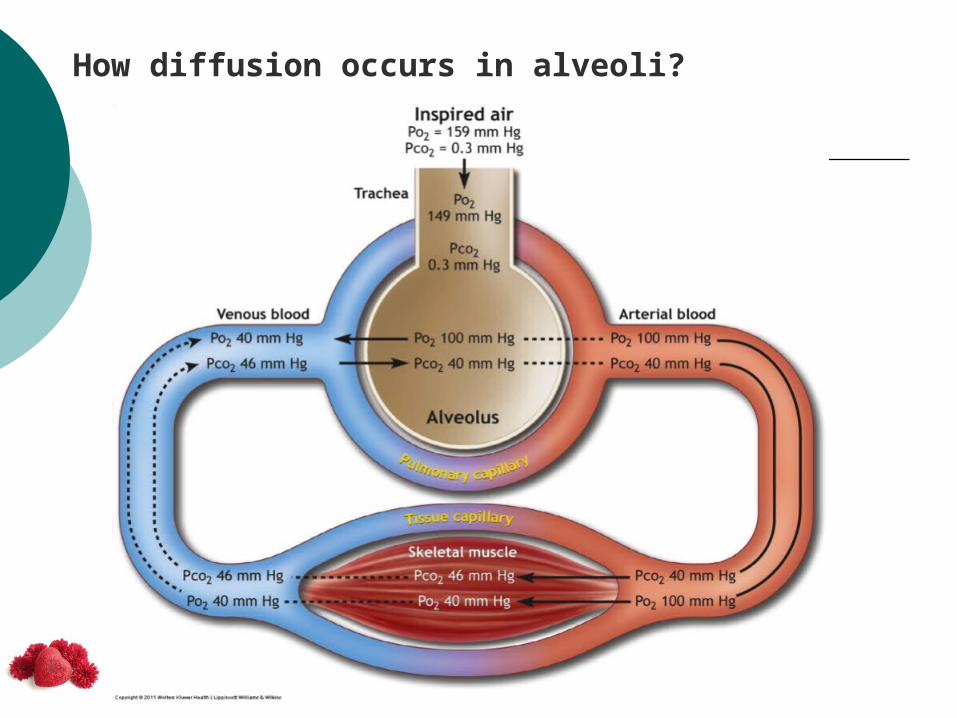
How diffusion occurs in alveoli?
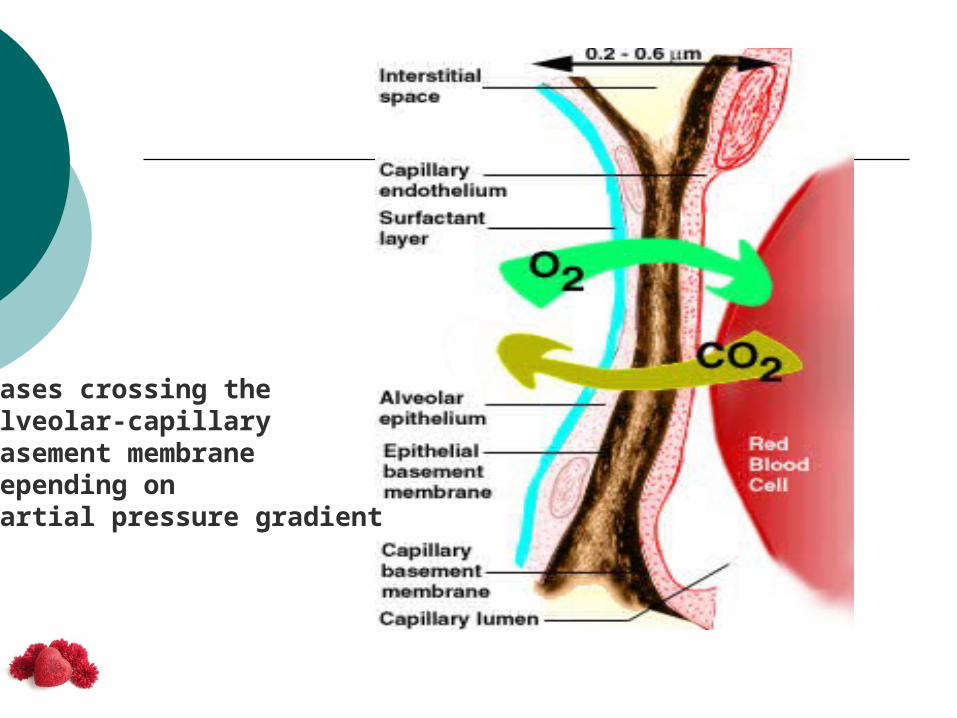
Gases crossing theAlveolar-capillaryBasement membranedepending onPartial pressure gradient

Do all alveoli participate in gaseous exchange?

What is the normal O2 content of the blood?
(Hb in gm% X 1.34 X SaO2) + ( 0.003 X paO2) = CaO2 = 20.1 ml
Oxygen in the blood combined with Hb + Oxygen dissolved in plasma as physical solution

How to increase the oxygen content of the blood?
(Hb in gm% X 1.34 X SaO2) + ( 0.003 X paO2) = CaO2 = 20.1ml
(15 X 1.34 X 99) + ( 0.003 X 100 ) = 20.1 ml%
(4 X 1.34 X 99) + (0.003 x 100 ) = 5.6 ml%
(15 X 1.34 x 99) + (0.003 x 600 ) = 21.6 ml%
Which is better?To give 100% O2 or increase the available Hb..?

What is the limitation of pulseoximetry?
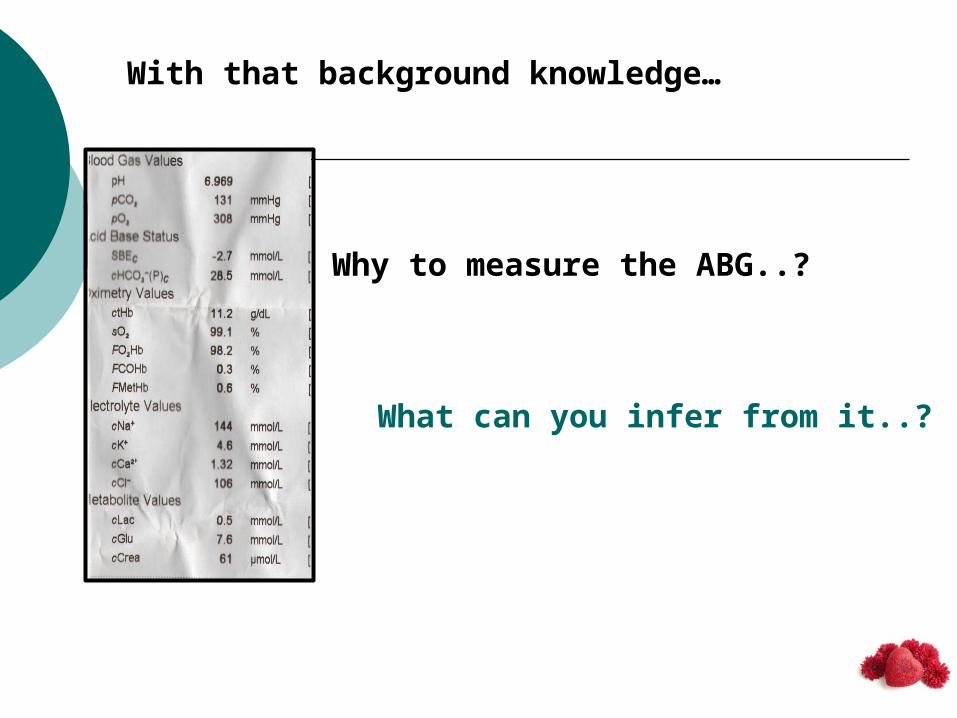
With that background knowledge…
Why to measure the ABG..?
What can you infer from it..?

ABG reflects
ALVEOLAR VENTILATION
OXYGENATION
ACID-BASE DISORDERS
ELECTROLYTE STATUS
ALVEOLAR VENTILATION
• CO2 level in the blood depends upon the production and excretion.• Excretion depends upon alveolar ventilation
• Alveolar ventilation depends upon many factorslike central respiratory drive , neuronal pathways,Anterior horn cells, respiratory muscle condition,Respiratory mechanics, intactness of airway and integrity of the pulmonary gas exchange system
If ventilation decreases, then CO2 level increases…..

OXYGENATION
ABG tells you about the status of oxygenation in the form of
paO2, SaO2, Oxygen Content, a/A ratio, (A-a)DO2
We can know the joint status of cardio-pulmonary system
ACID-BASE DISORDER
We can measure the pH, HCO3 level and Base excess/deficit
We can also know about the adequacy of compensatory mechanisms operating in the body.

COMPENSATORY MECHANISMS IN ACID-BASE DISORDERDUE TO RESPIRATORY PROBLEMS
If CO2 accumulates, due to Hypoventilation
CO2 + H2O = H2CO3 = H+ + HCO3
1 molecule of H+ and 1 molecule of HCO3is added to the circulation
But acidosis results….. How?

The impact of H+ increase is more, since the level of H+ in body is in nanomoles and HCO3 is in mmoles
How the body compensates for the addition of excess H+?
It retains HCO3 through kidney.
We call it as metabolic compensation

COMPENSATION RULE:
HCO3 increases by 1 meq/L for every 10 mm rise of CO2 in acute situations.
It increases by 3.5 meq/L for every 10 mm rise in chronic situations.
Memorize plz

COMPENSATION RULE:
If CO2 is washed out due to hyperventilation,HCO3 falls by 2 meq/L for every 10 mm fall in paCO2 in acute situations.
In chronic states, HCO3 falls by 5 meq/L for every10 mm fall of paCO2.
Memorize plz
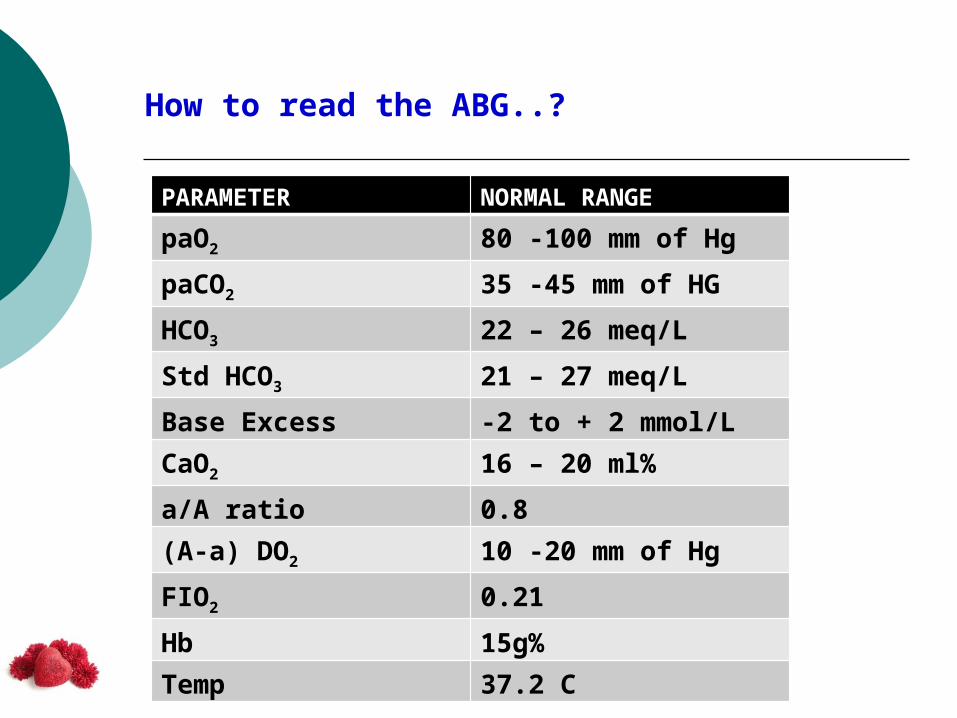
How to read the ABG..?
PARAMETER NORMAL RANGEpaO2 80 -100 mm of HgpaCO2 35 -45 mm of HGHCO3 22 – 26 meq/LStd HCO3 21 – 27 meq/LBase Excess -2 to + 2 mmol/LCaO2 16 – 20 ml%a/A ratio 0.8(A-a) DO2 10 -20 mm of HgFIO2 0.21Hb 15g%Temp 37.2 C
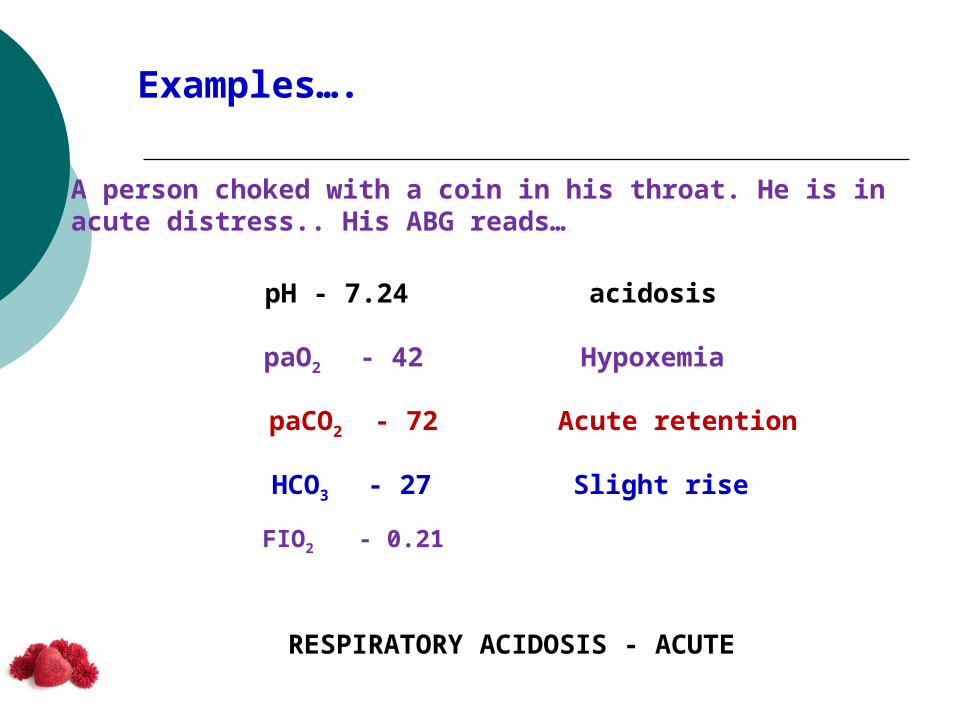
Examples….
A person choked with a coin in his throat. He is in acute distress.. His ABG reads…
pH - 7.24
paO2 - 42
paCO2 - 72
HCO3 - 27
acidosis
Hypoxemia
FIO2 - 0.21
Acute retention
Slight rise
RESPIRATORY ACIDOSIS - ACUTE
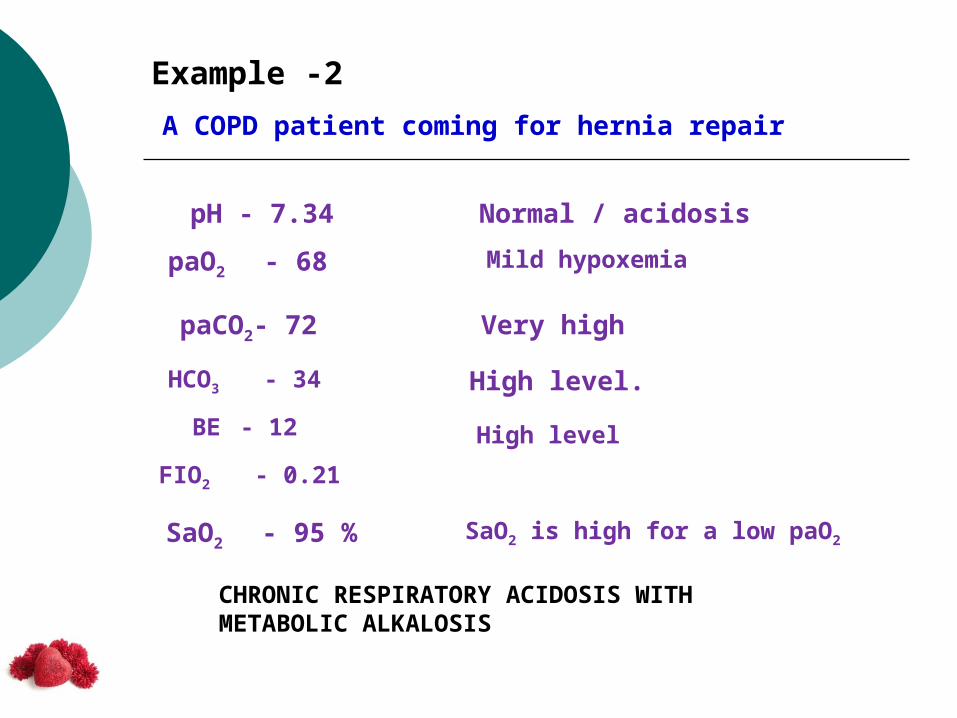
Example -2A COPD patient coming for hernia repair
pH - 7.34paO2 - 68
paCO2- 72
HCO3 - 34
FIO2 - 0.21
BE - 12
Normal / acidosisMild hypoxemia
SaO2 - 95 %
Very high
High level.
High level
SaO2 is high for a low paO2
CHRONIC RESPIRATORY ACIDOSIS WITH METABOLIC ALKALOSIS

pH 7.34paO2 68paCO2 72HCO3 34BE 12SaO2 95FIO2 0.21
• Why it is chronic?
• paO2 is 68, but SaO2 is 95%. How?
• Can it be chronic metabolic alkalosis with compensatory respiratory acidosis?

RULES YOU MUST NEVER FORGET….
pH drifts towards primary acid-base disorder
Compensation never overshoots….
pH 7.34paO2 68paCO2 72HCO3 34BE 12SaO2 95FIO2 0.21

Comment about oxygenation in the first ABG…
pH 7.24paO2 42paCO2 72HCO3 27SaO2 55%FIO2 0.21(A-a)DO2 75a/A ratio 0.38
Severe Hypoxia
Saturation very low
Normal -110 -90 = 20 So ,it is highNormal 90/110 = 0.8Very low.
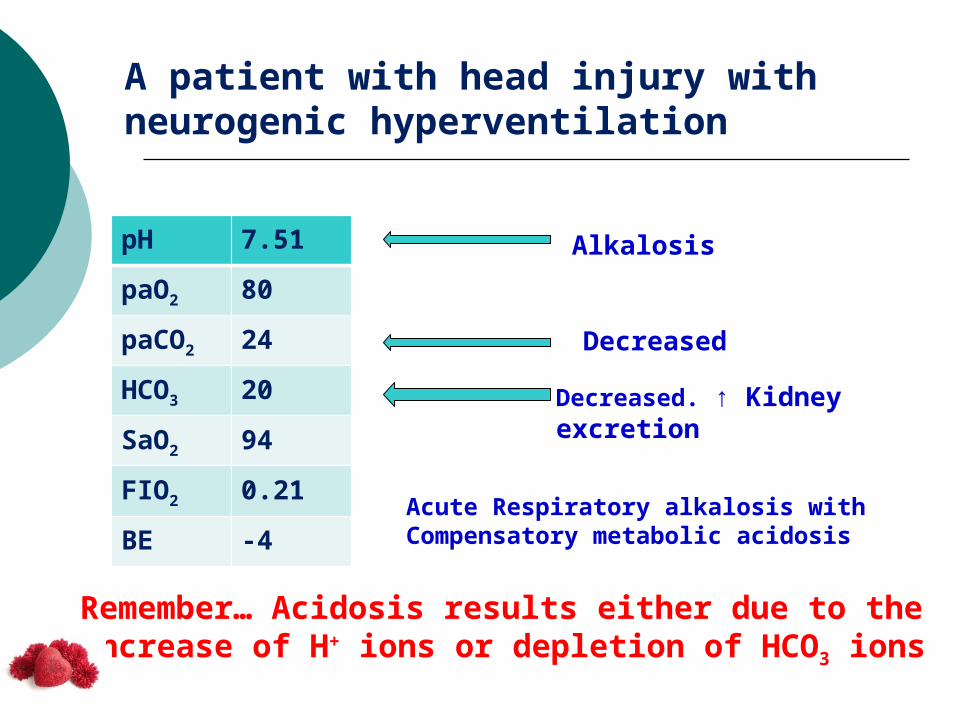
A patient with head injury with neurogenic hyperventilation
pH 7.51paO2 80paCO2 24HCO3 20SaO2 94FIO2 0.21BE -4
Alkalosis
Decreased
Decreased. ↑ Kidney excretion
Acute Respiratory alkalosis withCompensatory metabolic acidosis
Remember… Acidosis results either due to theIncrease of H+ ions or depletion of HCO3 ions

A patient living in high altitude region
pH 7.48
paO2 72
paCO2 24
HCO3 16
SaO2 96
FIO2 0.21
Mild alkalosis
Mild hypoxemia
Decreased level
Very low level. Kidney excreted much HCO3
For a paO2 of 72, saturation is high
Chronic respiratory alkalosiswith compensatory metabolic acidosis

Some more complicated ABGs…
pH 7.32
paO2 68
paCO2 69
HCO3 34
FIO2 0.21
pH 7.26
paO2 42
paCO2 78
HCO3 26
FIO2 0.40
COPD DEVELOPING LOBAR PNEUMONIA
More acidotic
Further lowered
Looks like normal
Chronic resp.acidosiswith compensatory met.alkalosis
Acute on Chronic resp.acidosiswith compensatory met.alkalosis
Increases further
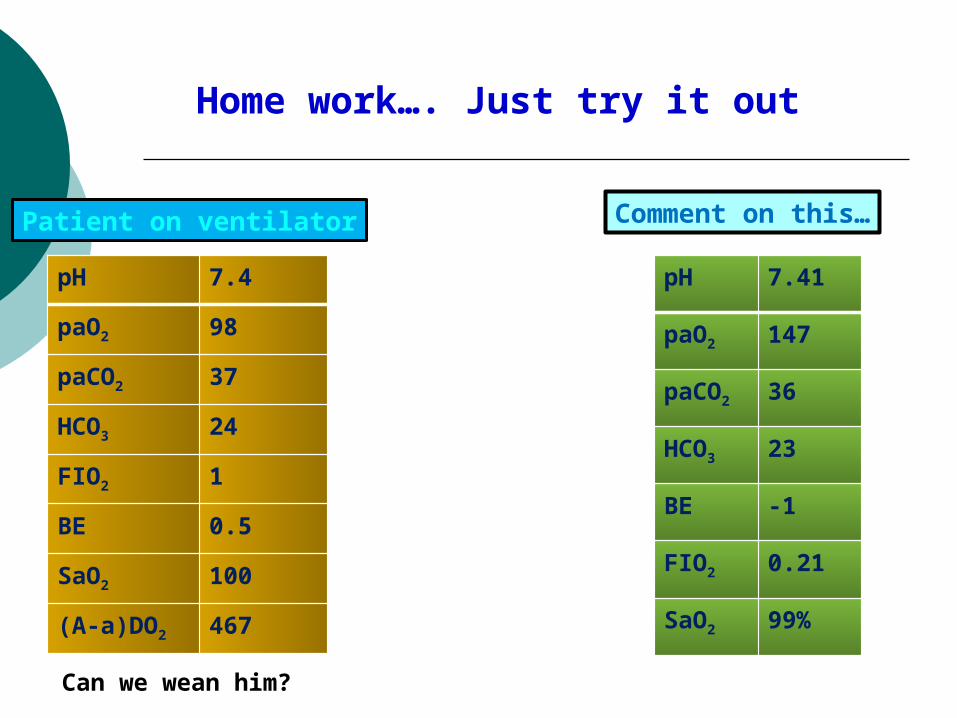
Home work…. Just try it out
pH 7.4
paO2 98
paCO2 37
HCO3 24
FIO2 1
BE 0.5
SaO2 100
(A-a)DO2 467
Patient on ventilator
Can we wean him?
pH 7.41
paO2 147
paCO2 36
HCO3 23
BE -1
FIO2 0.21
SaO2 99%
Comment on this…
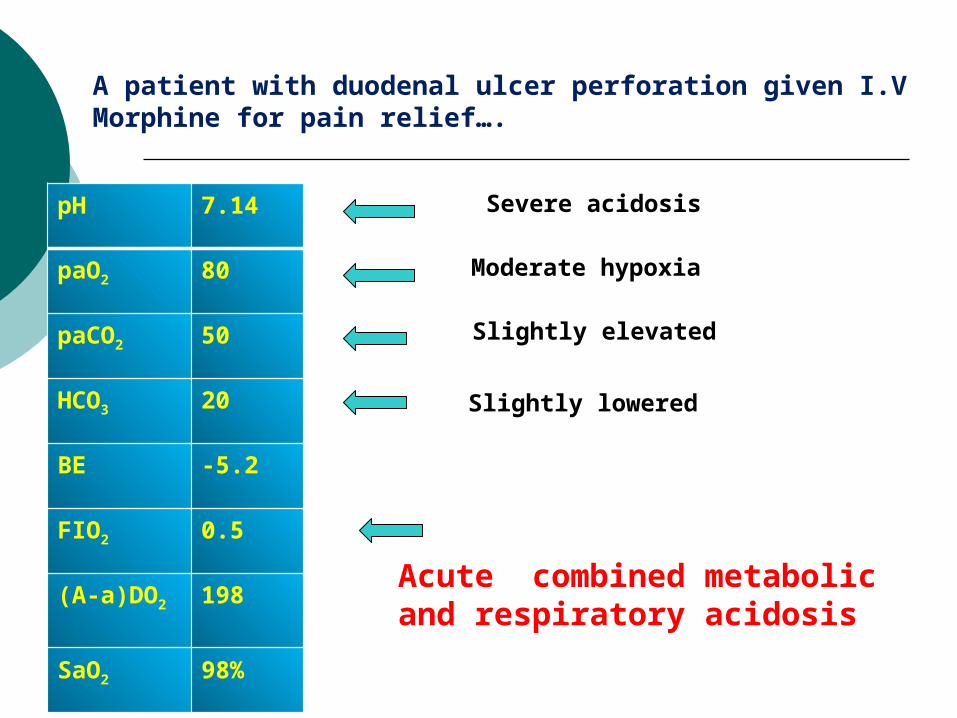
A patient with duodenal ulcer perforation given I.VMorphine for pain relief….
pH 7.14
paO2 80
paCO2 50
HCO3 20
BE -5.2
FIO2 0.5
(A-a)DO2 198
SaO2 98%
Severe acidosis
Moderate hypoxia
Slightly elevated
Slightly lowered
Acute combined metabolicand respiratory acidosis
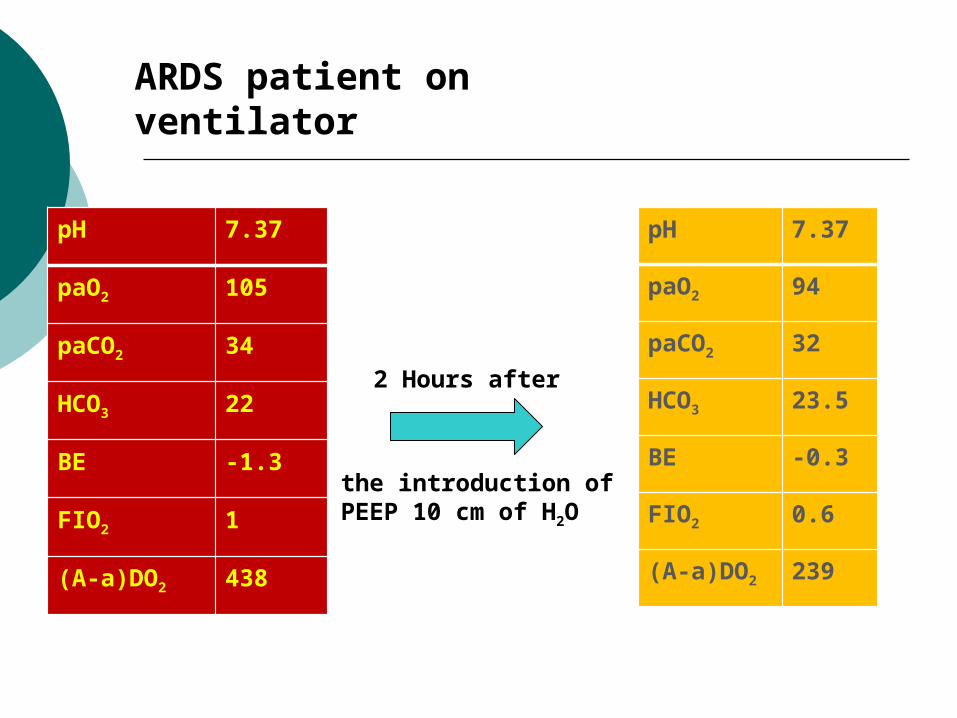
ARDS patient onventilator
pH 7.37
paO2 105
paCO2 34
HCO3 22
BE -1.3
FIO2 1
(A-a)DO2 438
2 Hours after
the introduction of PEEP 10 cm of H2O
pH 7.37
paO2 94
paCO2 32
HCO3 23.5
BE -0.3
FIO2 0.6
(A-a)DO2 239

Summary
Always remember the Basic physiology
Go through the clinical history and then try to read
pH sways to the primary acid-base disorder side
Compensatory phenomenon never overshoots

If you understand and remember the basic…
If you are methodical….
Reading ABG is a child’s play
Concluding……

dr.r.selvakumarprofessor of anaesthesiologyk.a.p.viswanatham govt medical collegetrichy
thank you