arterial blood pressure response to heavy resistance exercise · arterial blood pressure response...
TRANSCRIPT

Arterial blood pressure response to heavy resistance exercise
J. D. MAcDOUGALL, D. TUXEN, D. G. SALE, J. R. MOROZ, AND J. R. SUTTON Departments of Physical Education and Medicine, McMaster University, Hamilton, Ontario L&S 4K1, Canada
MACDOUGALL, J. D., D. TUXEN, D. G. SALE, J. R. MOROZ, AND J. R. SUTTON. Arterial blood pressure response to heavy resistance exercise. J. Appl. Physiol. 58(3): 785-790, 1985.- The purpose of this study was to record the blood pressure response to heavy weight-lifting exercise in five experienced body builders. Blood pressure was directly recorded by means of a capacitance transducer connected to a catheter in the brachial artery. Intrathoracic pressure with the Valsalva ma- neuver was recorded as mouth pressure by having the subject maintain an open glottis while expiring against a column of Hg during the lifts. Exercises included single-arm curls, overhead presses, and both double- and single-leg presses performed to failure at 80, 90, 95, and 100% of maximum. Systolic and diastolic blood pressures rose rapidly to extremely high values during the concentric contraction phase for each lift and de- clined with the eccentric contraction. The greatest peak pres- sures occurred during the double-leg press where the mean value for the group was 320/250 mmHg, with pressures in one subject exceeding 480/350 mmHg. Peak pressures with the single-arm curl exercise reached a mean group value of 255,’ 190 mmHg when repetitions were continued to failure. Mouth pressures of 30-50 Torr during a single maximum lift, or as subjects approached failure with a submaximal weight, indicate that a portion of the observed increase in blood pressure was caused by a Valsalva maneuver. It was concluded that when healthy young subjects perform weight-lifting exercises the mechanical compression of blood vessels combines with a po- tent pressor response and a Valsalva response to produce extreme elevations in blood pressure. Pressures are extreme even when exercise is performed with a relatively small muscle mass.
weight-lifting exercise; blood pressure; static contraction; small versus large muscle mass; Valsalva maneuver
SEVERAL STUDIES HAVE NOW demonstratedthatregular resistance training or weight lifting is associated with ventricular wall hypertrophy (11, 12, 14, 20). Such find- ings are considered to be a normal adaptation to a systemic pressure overload induced by such exercise. Although a number of investigators have recorded marked elevations in blood pressure in response to sub- maximal static exercise (2, 9, 10, 17), changes in blood pressure during maximal dynamic contractions, as in weight lifting, are not known. The purpose of this study was to directly record the hemodynamic response in experienced body builders to a typical weight-training session. A secondary purpose was to examine the effects
of exercises involving different active muscle masses upon the magnitude of this response.
METHODS
Five healthy male volunteers (22-28 yr) served as subjects. All were experienced body builders and were fully informed of the purposes of the study and the associated risks in accordance with the institution’s eth- ics committee.
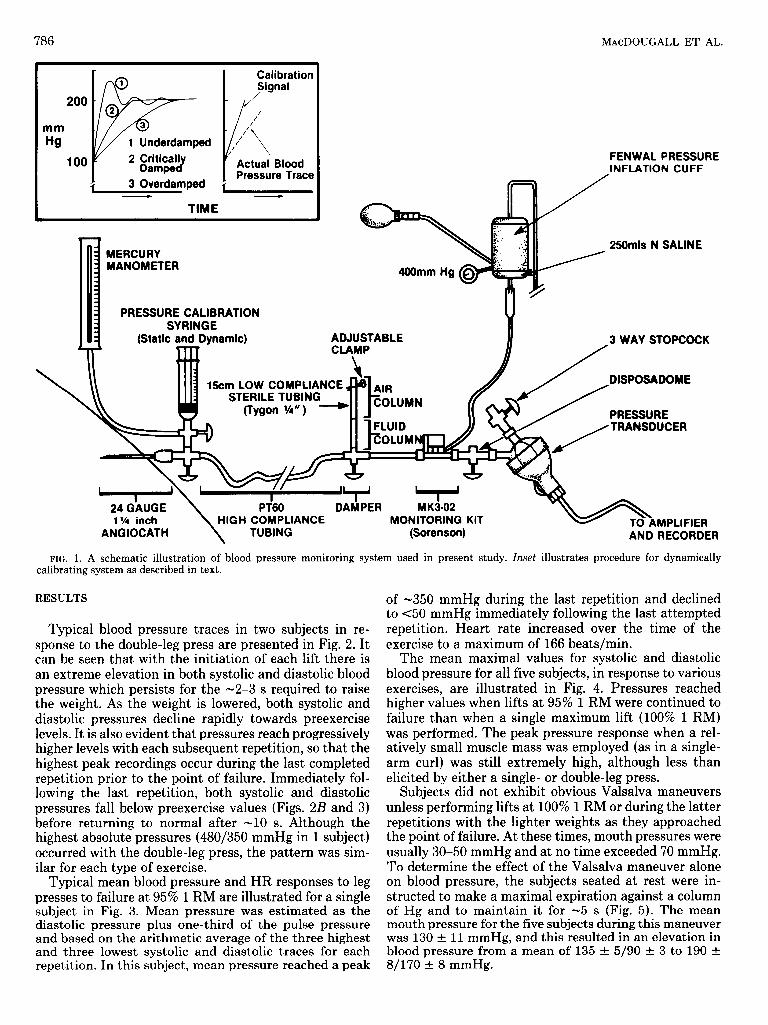
The left brachial artery of each subject was cannulated under local anesthesia with a 24-gauge Angiocath that was connected to a pressure transducer (Bell and Howell, Pasadena, CA) as illustrated in Fig. 1. The response of the transducer was verified to be linear within the range O-500 mmHg, and the system was statically calibrated against an Hg manometer by means of a calibration syringe. In addition, the system was dynamically cali- brated by using square-wave pressure signals that were rapidly switched into the arterial line. These signals were then critically damped by adjusting the height of an air column in a section of low-compliance tubing inserted into the line (Fig. 1). Arterial blood pressure was con- stantly recorded on a strip chart for each subject through- out 90 min of heavy weight training. For each exercise, the height of the pressure transducer was adjusted to midsternum level. Heart rate (HR) was derived from the systolic pressure traces.
Since it was anticipated that possible Valsalva maneu- vers would affect blood pressure results, intrathoracic pressure was recorded as mouth pressure during the lifts. This was accomplished by teaching the subjects to exhale through a modified mouthpiece against a column of Hg instead of completely closing their glottises.
Among the weight-lifting exercises which subjects per- formed were single-arm curls and overhead presses with the noncatheterized arm and both double- and single-leg seated leg presses. The curl exercise was done with free weights on a curl pedestal that supported the upper arm, whereas the other exercises were performed on a Univer- sal Gym apparatus. In each exercise, repetitions were performed to the point of concentric contraction failure in successive sets with 80, 90, 95, and 100% of the maximum single lift (1 RM) as determined on a previous occasion. A recovery period of 2 min was allowed after each set.
0161-7567/85 $1.50 Copyright 0 1985 the American Physiological Society 785
786 MAcDOUGALL ET AL.
mm Hg
100
1 Underdamped
3 Overdamped w
TIME
Calibration
Pressure Trace
MERCURY MANOMETER
PRESSURE CALIBRATION SYRINGE
(Static and Dynamic) ADJUSTABLE CLAMP
\ + 15cm LOW COMPLIANCE
STEP II c TIIDIU~ PL II
FENWAL PRESSURE INFLATION CUFF
2SOmls N SALINE
3 WAY STOPCOCK
/
PRESSURE
24 G’AUGE
\
DAMPER M KS-02 1 %a inch HIGH COMPLIANCE MONITORING KIT
AklOCkTH MD1 ICICD
I TUBING (Sorenson) AND RECORDE :R
FIG. 1. A schematic illustration of blood pressure monitoring system used in present study. Inset illustrates procedure for dynamically calibrating system as described in text.
RESULTS
Typical blood pressure traces in two subjects in re- sponse to the double-leg press are presented in Fig. 2. It can be seen that with the initiation of each lift there is an extreme elevation in both systolic and diastolic blood pressure which persists for the -2-3 s required to raise the weight. As the weight is lowered, both systolic and diastolic pressures decline rapidly towards preexercise levels. It is also evident that pressures reach progressively higher levels with each subsequent repetition, so that the highest peak recordings occur during the last completed repetition prior to the point of failure. Immediately fol- lowing the last repetition, both systolic and diastolic pressures fall below preexercise values (Figs. 2B and 3) before returning to normal after -10 s. Although the highest absolute pressures (480/350 mmHg in 1 subject) occurred with the double-leg press, the pattern was sim- ilar for each type of exercise.
Typical mean blood pressure and HR responses to leg presses to failure at 95% 1 RM are illustrated for a single subject in Fig. 3. Mean pressure was estimated as the diastolic pressure plus one-third of the pulse pressure and based on the arithmetic average of the three highest and three lowest systolic and diastolic traces for each repetition. In this subject, mean pressure reached a peak
of -350 mmHg during the last repetition and declined to ~50 mmHg immediately following the last attempted repetition. Heart rate increased over the time of the exercise to a maximum of 166 beats/min.
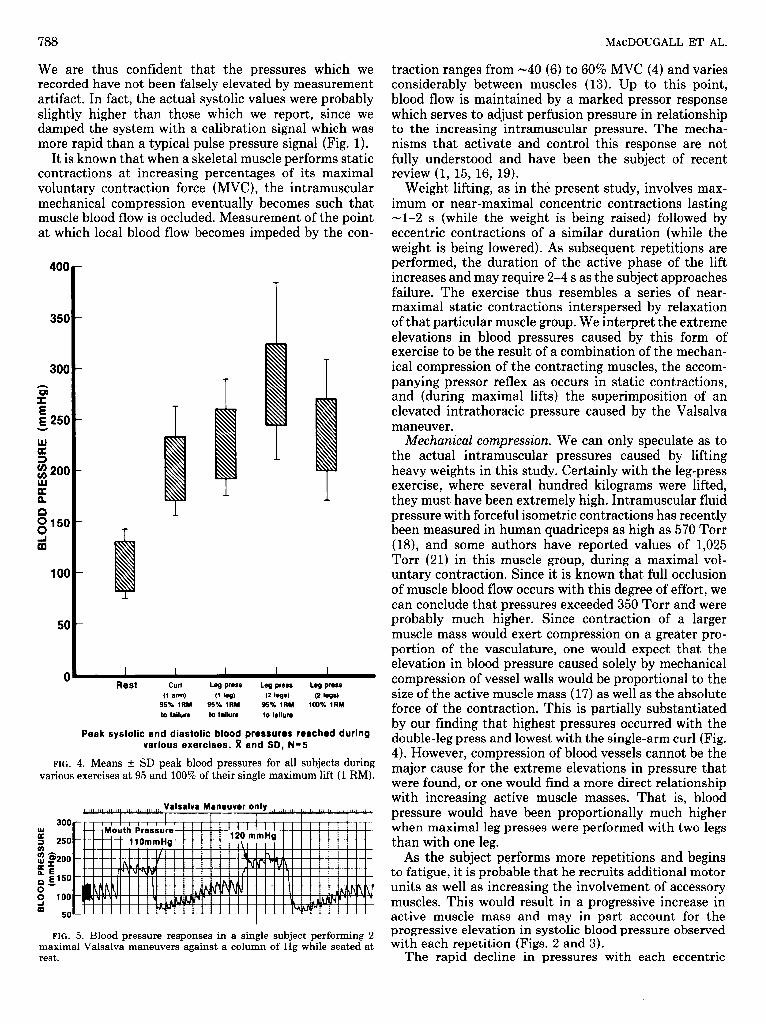
The mean maximal values for systolic and diastolic blood pressure for all five subjects, in response to various exercises, are illustrated in Fig. 4. Pressures reached higher values when lifts at 95% 1 RM were continued to failure than when a single maximum lift (100% 1 RM) was performed. The peak pressure response when a rel- atively small muscle mass was employed (as in a single- arm curl) was still extremely high, although less than elicited by either a single- or double-leg press.
Subjects did not exhibit obvious Valsalva maneuvers unless performing lifts at 100% 1 RM or during the latter repetitions with the lighter weights as they approached the point of failure. At these times, mouth pressures were usually 30-50 mmHg and at no time exceeded 70 mmHg. To determine the effect of the Valsalva maneuver alone on blood pressure, the subjects seated at rest were in- structed to make a maximal expiration against a column of Hg and to maintain it for -5 s (Fig. 5). The mean mouth pressure for the five subjects during this maneuver was 130 t 11 mmHg, and this resulted in an elevation in blood pressure from a mean of 135 t 5/90 t 3 to 190 t 8/170 t 8 mmHg.

BLOOD 1 ‘RESSURE AND WEIGHT LIFTING
A lea press 90% 1 RM
787
17 Reps to failure
FIG. 2. Actual traces of blood pressure response of 2 subjects performing double-leg presses to failure at 90% of their single maximum RM). Total elapsed time in A is 58 s and in B is 42 s.
lift (1
Double leg press 95%1 RM (9 reps to failure)
350
G 300 I E g 250
E z 200
cn ; 150 n
f 100
E 50 / /
t 5
’ \ / \
1’ \ \
I FIG. 3. Heart rate and estimated mean blood pres-
sure response for a single subject performing leg presses at 95% of his single maximum lift (1 RM). Mean pressure was estimated as diastolic pressure plus
r I I I I I I I I I I one-third of pulse pressure.
170
E 150 P
2; 130 2 a 110
k a 90
2 70
-
- *-
I i
Pre 1 2 3 4 5 6 7 a 9 + exercise REPETITIONS Failure
HR ranged from -102 beats/min between sets to peak values of -170 beats/min during actual lifting. The av- erage HR for the five subjects over the -90-min session was estimated to be 110 beats/min. Over this same time the average mean blood pressure was estimated to be -131 mmHg.
diastolic systemic blood pressures. To our knowledge, values of this magnitude have never before been recorded.
The accuracy of direct blood pressure measurement using a fluid-filled transducer-tubing system has been recently investigated (5). Such variables as the compli- ance of the system, the inertance of the fluid moving in the system, and the friction between the tubing and the fluid moving in it can combine to cause an underdamped system. For this reason we utilized a damping device (Fig. 1) so that the system could be critically damped.
DISCUSSION
Our results indicate that lifting of heavy weights re- sults in up to a fourfold elevation in both systolic and
788 MAcDOUGALL ET AL.
We are thus confident that the pressures which we recorded have not been falsely elevated by measurement artifact. In fact, the actual systolic values were probably slightly higher than those which we report, since we damped the system with a calibration signal which was more rapid than a typical pulse pressure signal (Fig. 1).
It is known that when a skeletal muscle performs static contractions at increasing percentages of its maximal voluntary contraction force (MVC), the intramuscular mechanical compression eventually becomes such that muscle blood flow is occluded. Measurement of the point at which local blood flow becomes impeded by the con-
400
350
300
@ E ~250 w w a 3 $200 W
E
0 $50
d
100
50
0 Rest curl Leg press Leg press WI PSS
(1 am) (1 WI) (2 hs) (2 @Is) 95% 1RM 95% 1RM 95% 1RM 100% 1RM to failure to failure to failure
Peak systolic and diastolic blood pressures reached during various exercises. x and SD, N=5
FIG. 4. Means & SD peak blood pressures for all subjects during various exercises at 95 and 100% of their single maximum lift (1 RM).
300
ii
: 250
2 s200 ax rLE 0 El50
s 100 $ -1 50
I I I I I I I I I I t I I 1
.’ Mouth Pressurq I i I I I I-, ” ” ” ”
1-f 11OmmHa’ I I 120 mmHg __
I\1 1 1 I
FIG. 5. Blood pressure responses in a single subject performing 2 maximal Valsalva maneuvers against a column of Hg while seated at rest.
traction ranges from -40 (6) to 60% MVC (4) and varies considerably between muscles (13). Up to this point, blood flow is maintained by a marked pressor response which serves to adjust perfusion pressure in relationship to the increasing intramuscular pressure. The mecha- nisms that activate and control this response are not fully understood and have been the subject of recent review (1, 15, 16, 19).
Weight lifting, as in the present study, involves max- imum or near-maximal concentric contractions lasting -1-2 s (while the weight is being raised) followed by eccentric contractions of a similar duration (while the weight is being lowered). As subsequent repetitions are performed, the duration of the active phase of the lift increases and may require 2-4 s as the subject approaches failure. The exercise thus resembles a series of near- maximal static contractions interspersed by relaxation of that particular muscle group. We interpret the extreme elevations in blood pressures caused by this form of exercise to be the result of a combination of the mechan- ical compression of the contracting muscles, the accom- panying pressor reflex as occurs in static contractions, and (during maximal lifts) the superimposition of an elevated intrathoracic pressure caused by the Valsalva maneuver.
h4echanicaZ compression. We can only speculate as to the actual intramuscular pressures caused by lifting heavy weights in this study. Certainly with the leg-press exercise, where several hundred kilograms were lifted, they must have been extremely high. Intramuscular fluid pressure with forceful isometric contractions has recently been measured in human quadriceps as high as 570 Torr (US), and some authors have reported values of 1,025 Torr (21) in this muscle group, during a maximal vol- untary contraction. Since it is known that full occlusion of muscle blood flow occurs with this degree of effort, we can conclude that pressures exceeded 350 Torr and were probably much higher. Since contraction of a larger muscle mass would exert compression on a greater pro- portion of the vasculature, one would expect that the elevation in blood pressure caused solely by mechanical compression of vessel walls would be proportional to the size of the active muscle mass (17) as well as the absolute force of the contraction. This is partially substantiated by our finding that highest pressures occurred with the double-leg press and lowest with the single-arm curl (Fig. 4). However, compression of blood vessels cannot be the major cause for the extreme elevations in pressure that were found, or one would find a more direct relationship with increasing active muscle masses. That is, blood pressure would have been proportionally much higher when maximal leg presses were performed with two legs than with one leg.
As the subject performs more repetitions and begins to fatigue, it is probable that he recruits additional motor units as well as increasing the involvement of accessory muscles. This would result in a progressive increase in active muscle mass and may in part account for the progressive elevation in systolic blood pressure observed with each repetition (Figs. 2 and 3).
The rapid decline in pressures with each eccentric

BLOOD PRESSURE AND WEIGHT LIFTING 789
phase of the lift is interesting, since one would expect the absolute force of contraction to be the same when lowering the weight as when raising it. However, since it is known that muscles are stronger when contracting eccentrically, the degree of muscle excitation during this phase of the lift would be smaller than during the con- centric phase (3). It is thus apparent that the blood pressure response is more dependent on the degree of effort or percent of MVC than on the absolute mechan- ical force developed.
sponse to weight lifting.
Finally, the degree to which possible contractions in the catheterized arm might have affected results is not known. We thus recognize that measurement of arterial pressure at this site may not accurately reflect pressures throughout the systemic circuit. However, since subjects were not allowed to grasp any part of the apparatus with the nonactive hand, we feel that even if such contractions occurred they would not have been forceful enough to have a major effect on our results. This conclusion is supported by the fact that the pressure traces indicate well-preserved waveforms; this would probably not have been the case had they been falsely elevated by compres- sion or spasm within the brachial artery.
The rapid drop in blood pressure immediately after exercise (Figs. 2 and 3) is probably caused by the sudden perfusion of a large vasodilated muscle mass which was previously occluded, as well as by a transient pressure undershoot initiated by baroreceptor and cardiopulmo- nary reflexes responding to the extreme elevation in pressure with the last repetition. This is the likely cause of the temporary feelings of faintness or dizziness that subjects often experience immediately following heavy lifting.
Pressor response. The immediate increase in blood pressure which occurs with a forceful static contraction is largely the result of an increased cardiac output (Qc) and to a lesser extent a reflex vasoconstriction in vas- cular beds other than those of the exercising muscles (2, 15, 19). The increase in &c with static contractions is thought to be exclusively due to increased HR, since stroke volumes (SV) tend to decrease with this form of exercise (2, 10, 19), presumably due to an impaired venous return.
A second plausible explanation for this condition is that it is due to a cerebral vasoconstriction accompanying the hypocapnia caused by hyperventilation during the exercise. We investigated this possibility by monitoring end-tidal CO2 partial pressure (Pco~) in four subjects during the leg-press movement. Our data (Fig. 6) indi- cated that although the subjects did hyperventilate dur- ing the lifting (with end-tidal PCO~ ~30 Torr in some subjects), 2 s after completion of the exercise they were actually hypercapnic, with end-tidal PCO~ reaching al- most 50 mmHg after 20 s of recovery. We thus conclude that the faintness commonly experienced by weight lif- ters 5-10 s postexercise is not caused by cerebral vaso- constriction because of hypocapnia.
The authors accept that the general relationship be- tween the magnitude of the pulse pressure and SV may not apply under such extreme conditions as in the pres- ent study. However, if it does, inspection of pulse pres- sures during contraction (Figs. 2 and 4) suggest that SV is considerably higher than at rest in spite of large increases in peripheral resistance. This is not the case for a prolonged static contraction or with the Valsalva maneuver alone (Fig. 5). One interpretation could be that the forceful contractions interspersed with a relative relaxation in this form of exercise provide a powerful muscle pump which serves to enhance ventricular filling pressures and venous return. The extreme increases in blood pressure with weight lifting may thus also be due to an increase in both HR and SV as well as vasocon- triction in nonexercising areas. The progressive increase in HR which is seen as subsequent repetitions are per- formed probably also contributes to the progressive in- crease in blood pressure found with each repetition (Figs. 2 and 3).
Vdsalua maneuuer. The validity of using buccal pres- sure (with glottis open) as a measure of intrathoracic pressure has been previously established in subjects per- forming a strain or cough type of maneuver (7). Again, however, we do not know whether this relationship holds during the weight-lifting exercise in the present study. Despite this, our results show that the Valsalva maneu- ver alone can produce substantial rises in systemic blood pressure (Fig. 5). It is thus evident that a portion of the increase in blood pressure that occurs when a subject performs a single maximal contraction or lifts a submax- imal weight to failure can be directly attributed to the increased intrathoracic pressure generated by the Val- salva maneuver.
It has been shown that this increase in intrathoracic pressure with the Valsalva maneuver is directly trans-
Recovery
The possible involvement of a reflex pathway that originates in skeletal muscle and chemically effects the pressor response to forceful isometric contractions has been suggested by some authors (17). The magnitude of the change in blood pressure in the present study and the rapidity by which the response occurs and then declines with the eccentric phase of the lift suggest a minimal role for such a mechanism in the nressor re-
4-1 ’ ’ ’ I I I 1 I
min min 0 10s 20s 30s 40s 50s
’ !I+ 60s 120s
(x,*SD) N=4
FIG. 6. Means t SD end-tidal CO2 partial pressure (Pco~) for 4 subjects performing double-leg presses to failure at 90% of their single maximum lift.

790 MAcDOUGALL ET AL.
mitted to the cerebrospinal fluid so that cerebrospinal pressure increases to match that in the thorax and ab- domen (7). This may represent an important protective mechanism by reducing transmural pressures across cerebral vessels and thus reducing the risk of vascular damage under the extremes of pressure encountered with this form of exercise. It is also probable that the cardiac compression caused by a rise in intrathoracic pressure would assist the heart in maintaining or augmenting SV despite extreme peripheral resistance. Unlike the situa- tion where the Valsalva maneuver is performed at rest (Fig. 5), the powerful muscle pump provided by this form of exercise is apparently sufficient to overcome this pressure and provide adequate diastolic filling. Thus, although some of the increase in blood pressure which occurs when lifting heavy weights is caused by the subject performing brief Valsalva maneuvers, the process may serve an important protective function for the heart and
REFERENCES
1. ABBOUD, F. M., A. L. MARK, AND M. D. THAMES. Modulation of the somatic reflex by carotid baroreceptors and by cardiopulmonary afferents in animals and in humans. Circ. Res. 48, Suppt. I: 131- 137,198l.
2. BEZUCHA, G. R., M. C. LENSER, P. G. HANSON, AND F. J. NAGLE. Comparison of hemodynamic responses to static and dynamic exercise. J. Appl. Physiol. 53: 1589-1593, 1982.
3. BIGLAND, B., AND 0. C. J. LIPPOLD. The relation between force, velocity and integrated electrical activity in human muscles. J. Physiol. London 123: 214-224, 1954.
4. BONDE-PETERSEN, F., A. L. MBRK, AND E. NIELSEN. Local muscle blood flow and sustained contractions of human arms and back muscles. Eur. J. Appl. Physiol. Occup. Physiol. 34: 43-50, 1975.
5. BOUTROS, A., AND S. ALBERT. Effect of the dynamic response of transducer-tubing system on accuracy of direct blood pressure measurement in patients. Crit. Cure Med. 11: 124-127, 1983.
6. HALL-JURKOWSKI, J., J. R. SUTTON, AND R. J. DUKE. Subarach- noid hemorrhage in association with weightlifting (Abstract). Can. J. Appl. Sports Sci. 8: 210, 1983.
7. HAMILTON, W. F., R. A. WOODBURY, AND H. T. HARPER, JR. Arterial, cerebrospinal, and venous pressures in man during cough and strain. Am. J. Physiol. 141: 42-50, 1944.
8. HUMPHREYS, P. W., AND A. R. LIND. The blood flow through active and inactive muscles of the forearm during sustained hand- grip contractions. J. Physiol. London 166: 120-135, 1963.
9. KILBOM, A., AND T. BRUNDIN. Circulatory effects of isometric muscle contractions, performed separately and in combination with dynamic exercise. Eur. J. Appl. Physiol. Occup. Physiol. 36: 7-17, 1976.
10. LIND, A. R., S. H. TAYLOR, P. W. HUMPHREYS, B. M. KENNEALLY, AND K. W. DONALD. The circulatory effects of sustained voluntary muscle contraction. Clin. Sci. 27: 229-244, 1964.
11. LONGHURST, J. C., A. R. KELLY, W. J. GONYEA, AND J. H. MITCHELL. Echocardiographic left ventricular masses in distance runners and weight lifters. J. Appl. Physiol. 48: 154-162, 1980.
12. MENAPACE, F. J., W. J. HAMMER, T. F. RITZER, K. M. KESSLER,
vessels of the brain. Weight lifting is a relatively safe sport with few in-
stances where the excessive elevations in blood pressure, demonstrated in this paper, are known to result in injury. We have, however, recently reported a case of brain stem ischemia (22) and a case of subarachnoid hemorrhage (6) that occurred during weight lifting.
In summary, when healthy young subjects perform heavy weight-lifting exercises, the mechanical compres- sion of blood vessels with each contraction combines with a potent pressor response and a Valsalva response to produce extreme elevations in systolic and diastolic pressures. These elevations are extreme even when ex- ercise is performed with a relatively small muscle mass.
This study was supported by a grant from Engineering Research Council of Canada.
the Natural Sciences and
Received 19 December 1983; accepted in final form 5 October 1984.
H. F. WARNER, J. F. SPANN, AND A. A. BOVE. Left ventricular size in competitive weight lifters: an echocardiographic study. Med. Sci. Sports Exercise 14: 72-75, 1982.
13. MITCHELL, J. H., F. C. PAYNE, B. SALTIN, AND B. SCHIBYE. The role of muscle mass in the cardiovascular response to static con- tractions. J. Physiol. London 309: 45-54, 1980.
14. MORGANROTH, J., B. J. MARON, W. HENRY, AND S. E. EPSTEIN. Comparative left ventricular dimensions in trained athletes. Ann. Intern. Med. 82: 521-524, 1975.
15. NUTTER, D. O., AND C. W. WICKLIFFE. Regional vasomotor re- sponses to the somatopressor reflex from muscle. Circ. Res. 48, Suppl. I: 98-103,198l.
16. ROWELL, L. B., P. R. FREUND, AND S. F. HOBBS. Cardiovascular responses to muscle ischemia in humans. Circ. Res. 48, Suppl. I: 37-47,198l.
17. SEALS, D. R., R. A. WASHBURN, P. G. HANSON, P. L. PAINTER, AND F. J. NAGLE. Increased cardiovascular response to static contraction of larger muscle groups. J. Appl. Physiol. 54: 434-437, 1983.
18. SEJERSTED, 0. M., A. R. HARGENS, K. R. KARDEL, P. BLOM, 0. JENSEN, AND L. HERMANSEN. Intramuscular fluid pressure during isometric contraction of human skeletal muscle. J. Appl. Physiol. 56: 287-295, 1984.
19. SHEPHERD, J. T., C. G. BLOMQVIST, A. R. LIND, J. H. MITCHELL, AND B. SALTIN. Static (isometric) exercise. Retrospection and introspection. Circ. Res. 48, Suppt. I: 179-188, 1981.
20. SNOECKX, L. H., H. F. ABELING, J. A. LAMBREGTS, J. J. SCHMITZ, F. T. VERSTAPPEN, AND R. S. RENEMAN. Echocardiographic di- mensions in #athletes in relation to their training programs. Med. Sci. Sports Exercise 14: 428-434, 1982.
21. SYLVEST, O., AND N. HVID. Pressure measurements in human striated muscles during contraction. Acta Rheumatol. Stand. 5: 216-222,1959.
22. TUXEN, D. V., J. SUTTON, D. MACDOUGALL, AND D. SALE. Brain- stem injury following maximal weight lifting attempts (Abstract). Med. Sci. Sports Exercise 15: 184, 1983.