arthrodesis of the foot and ankle
DESCRIPTION
ArthrodesisTRANSCRIPT

Arthrodesis plays an important role in reconstructivesurgery of the foot and ankle, enabling the surgeon tocreate a painless, stable, plantigrade foot. It is usedmost often to correct a painful joint secondary toarthrosis, chronic instability of the foot and ankle frommuscle dysfunction (e.g., posterior tibial tendon,poliomyelitis), or a deformity that has resulted in anonplantigrade foot.
Arthrodesis can greatly enhance a patient’s func-tional capacity, but it places increased stress on thejoints proximal and distal to the fusion site. After anankle or triple arthrodesis, approximately 30% ofpatients demonstrate arthroses distal or proximal tothe fusion site within 5 years. Although most of thesefindings are radiographic, their presence at 5 yearsdoes not bode well for what will occur at these joints20 to 30 years in the future.
Many factors probably affect the onset of this arthro-sis besides the increased stress. One factor is probablyrelated to the overall stiffness or laxity of the sur-rounding joints. The stiffer the surrounding joints, theless the patient is able to dissipate the increased stresscreated by the fusion compared with a patient who hasmore joint laxity. Because an arthrodesis is often per-
formed on a traumatized extremity, the adjacent joints,although not demonstrating arthrosis, might have sus-tained tissue damage at the time of the initial injurythat makes them more vulnerable to develop arthrosiswhen subjected to increased stress.
Although this chapter discusses arthrodesis of thejoints of the foot and ankle, the clinician shouldalways remember that, if possible, arthrodesis shouldbe avoided, particularly in patients younger than 50years. Often an osteotomy or a tendon transfer can beused to create a plantigrade foot without resorting toan arthrodesis. It is often more challenging to thesurgeon’s creativity to avoid an arthrodesis. If thesurgeon can offer the patient 5 to 10 years of improvedquality of life from a reconstructive procedure withoutusing an arthrodesis, this is the desired approach.
TECHNICAL CONSIDERATIONS
The two basic types of arthrodeses are an in situ fusionand one that corrects a deformity. In an in situ fusion,positioning the foot or ankle is usually not diffi-cult because no deformity is present. In a deformity-
Arthrodesis of the Foot and AnkleRoger A. Mann
1087
C H A P T E R
20
TECHNICAL CONSIDERATIONSSOFT TISSUE CONSIDERATIONSSURGICAL PRINCIPLES
COMPLICATIONSSPECIFIC ARTHRODESES (video clips 11-14)

1088 PART V Arthritis, Postural Disorders, and Tendon Disorders
correcting fusion, however, the surgeon must decide theprecise alignment that must be obtained to produce aplantigrade foot. To determine the alignment, thesurgeon first must evaluate the normal extremity. With the patient in a supine position, the patella isaligned to the ceiling, giving the surgeon a referencepoint from which all measurements are made. Thedegree of internal or external rotation, varus or valgus,and abduction or adduction is carefully noted. A particular arthrodesis is not always placed into a stan-dard alignment; rather, it must be individualized foreach patient. Using the patella as a reference pointmakes alignment at surgery much easier and moreprecise.
When evaluating the patient for an arthrodesis, thesurgeon must also carefully examine the adjacentjoints for range of motion and overall alignment.Because an arthrodesis places more stress on the sur-rounding joints, if one of these joints has mild arthro-sis, the prognosis for success is diminished. As anexample, when a double or triple arthrodesis needs tobe performed and there is mild arthrosis of the ankleor valgus or varus tilt of the talus in the ankle mortise,following a double or triple arthrodesis the ankle jointcan deteriorate more rapidly or become more symp-tomatic as a result of the increased stress. Therefore itis important to inform the patient who is about toundergo a triple or double arthrodesis in the presenceof early arthrosis of the ankle joint that although thefusion will create a painless hindfoot, it might alsoresult in rapid deterioration of the ankle. Similarly, ifthe patient has concomitant arthrosis of the tar-sometatarsal joints that is not symptomatic, it canbecome symptomatic after a triple or double arthrode-sis because of the added stress from the proximalfusion. In some cases when multiple joints areinvolved, it may be more desirable to treat the patientconservatively with an orthotic device such as anankle–foot orthosis (AFO) rather than carry out anarthrodesis.
Once a decision has been made to perform anarthrodesis, the next most critical factor is to establishthe proper alignment of the fusion site. To do this, thesurgeon must consider the entire lower extremity andnot just the foot. The position of the knee or the bowof the tibia, which can occur either naturally or as aresult of prior trauma, must be carefully examinedwhen planning the arthrodesis. The alignment of theextremity distal to the fusion site is also important tobe sure a plantigrade foot is created.
The biomechanics of the foot dictates its optimalalignment. When the subtalar joint is placed into aneverted (valgus) position, it creates flexibility of the trans-verse tarsal joint and results in a supple forefoot. Whenthe subtalar joint is in an inverted (varus) position, it
locks the transverse tarsal joint. This creates a rigidforefoot and increased stress under the lateral aspectof the foot. It is therefore important to align the sub-talar joint in 5 to 7 degrees of valgus when a fusion iscarried out in order to maintain flexibility of the fore-foot. When a talonavicular arthrodesis is performed,the surgeon must remember that motion in the sub-talar joint will no longer occur. Therefore the subtalarjoint must be aligned into 5 degrees of valgus, afterwhich the talonavicular joint is aligned while takinginto account abduction or adduction of the transversetarsal joint as well as correcting any forefoot varus thatmight be present. This complex alignment creates atechnically challenging situation for the surgeon. If the joints surrounding the talonavicular joint are not properly aligned, a plantigrade foot will not becreated.
When arthrodesing the tarsometatarsal joints, thesurgeon should always try to match the abnormal footto the normal foot by carefully evaluating the weight-bearing posture of both feet preoperatively. The mostcommon deformity is abduction and varying degreesof dorsiflexion. Any malalignment needs to be cor-rected. Once the first metatarsocuneiform joint is sta-bilized, the other joints need to be aligned, both in thetransverse and in the dorsoplantar direction. This willalign the metatarsal heads and prevent one from beingtoo prominent, which can result in an intractableplantar keratosis.
SOFT TISSUE CONSIDERATIONS
The soft tissue envelope of the foot and ankle oftencontains little or no fatty tissue. At times this lack ofsoft tissue padding has been further compromised byprevious surgery or trauma to the soft tissues, result-ing in adherence of the soft tissue to the underlyingbone. The surgical approach should be as precise aspossible to avoid placing undue tension on the skinedges. If significant realignment is to be achieved, itmust not be at the expense of proper wound approxi-mation. This occasionally occurs when attempting tocorrect a valgus deformity of the heel in which anopening lateral wedge osteotomy results in increasedtension on the lateral skin edges, which makes closuredifficult. Skin flaps should be made as full thickness aspossible to diminish the possibility of a skin slough.Creating an incision down to the bone, then retractingon the deep structures and not the skin edge, is prob-ably the best way to avoid a skin problem.
When making an incision, the surgeon must alwaysbe cognizant of the location of the cutaneous nervesabout the foot and ankle. Although cutaneous nervestend to lie in certain anatomic areas, great variation

CHAPTER 20 Arthrodesis of the Foot and Ankle 1089
exists. Therefore, as the incision is carried downthrough the subcutaneous tissues, it is important toalways look for an aberrant cutaneous nerve. The cuta-neous nerves can be quite superficial and easily tran-sected but sometimes become adherent within scartissue. If this occurs, a painful scar or dysesthesiasdistal to the injury can result in a dissatisfied patientdespite a satisfactory fusion.
Another unique problem after foot surgery is theimpact of footwear, which can rub against a subcuta-neous neuroma, further aggravating the problem.
If a nerve is inadvertently transected during a surgical approach, it should be carefully dissected to a more proximal level and the cut end buriedbeneath some fatty tissue or muscle so that it will notbecome symptomatic. Sometimes, although a nerve isnot cut, it can be stretched as a result of retraction,which can result in a transient loss of function.Patients must be made aware of the potential for nerve injury and the area where they can experiencenumbness.
SURGICAL PRINCIPLES
When carrying out an arthrodesis of the foot andankle, the following surgical principles should be care-fully observed:
• A well-planned incision of adequate length toavoid undue tension on the skin edges.
• An attempt should be made to create broad, con-gruent cancellous surfaces that can be placed intoapposition to permit an arthrodesis to occur.
• The arthrodesis site should be stabilized withrigid internal fixation. This sometimes dependson the surgeon’s ingenuity in creating a rigid construct, particularly if poor bone stock ispresent.
• When performing a fusion, the hindfoot must bealigned to the lower extremity and the forefoot tothe hindfoot to create a plantigrade foot.
After exposure of the fusion site, the soft tissues sur-rounding the joints are removed. This mobilizes thejoints, allowing the surgeon to realign the foot. Attimes, because of previous trauma or severe malalign-ment, mobilization of the joints is not possible andbone resection needs to be carried out. In my experi-ence, however, the majority of cases can be aligned,even when a significant deformity is present, by com-plete mobilization of the involved joints followed bymanipulation to create a plantigrade foot.
Once the joints have been mobilized and it is deter-mined that bone does not need to be removed, thearticular surfaces are meticulously debrided of their
articular cartilage and any fibrous tissue to subchon-dral bone. This is achieved with a curet or a small,sharp osteotome. A lamina spreader or a towel clip canfacilitate distraction of the articular surfaces, makingthe debridement easier, but this can damage the boneif it is soft.
Once the subchondral bone is exposed, the foot isonce again manipulated, placing it into the desiredalignment. If this is achievable, internal fixation can beinserted. If large amounts of bone need to be removedto create a plantigrade foot, this should be done beforeremoving the articular cartilage. The subchondral sur-faces are heavily feathered or scaled with a 4- or 6-mmosteotome, which creates a broader, bleeding cancel-lous surface required for successful fusion. The articu-lar surfaces to be arthrodesed are brought together andstabilized with provisional fixation. Then interfrag-mentary compression is achieved using appropriatedefinitive fixation.
By carrying out a fusion in this manner, broad bleed-ing surfaces of cancellous bone are brought together,which provides the best possible chance for a success-ful arthrodesis. In my experience, bone graft from theiliac crest is rarely necessary when carrying out anarthrodesis. Sometimes bone has been lost, making abone graft necessary, but in an in situ fusion, graftingis not usually required. If a small amount of bone isneeded, it can be harvested from the calcaneus, medialmalleolus, or proximal medial tibia without violatingthe iliac crest and causing its attendant morbidity.Likewise, bone substitutes or other materials are rarelyrequired if the bone preparation is carried out correctly.
For internal fixation, I prefer an interfragmentaryscrew that compresses the joint surfaces. At times apower staple, a plain staple, or a plate may be used.Although an external fixator can provide excellent fix-ation, if possible a closed system without an externalfixator is safer due to possible pin tract problems withprolonged immobilization. Because of soft bone orsoft tissue problems, however, it may become neces-sary to use an external fixator. Under these circum-stances this device provides excellent rigid fixation.
The skin closure after a fusion is very critical. Thesurgeon should always attempt, if possible, to obtaina soft tissue cover underneath the skin flaps, such asfat or muscle. This is important because if a superficialwound slough occurs, it will be over an underlying bedof soft tissue rather than bone. This is not always pos-sible, particularly on the dorsum of the foot, wherebone lies directly beneath the skin. If any tension isnoticeable on the skin edge, some type of a relaxingskin suture should be used. A drain is always useful ifprofuse bleeding is anticipated.
The initial postoperative dressing is very importantand should support the soft tissues as well as the

1090 PART V Arthritis, Postural Disorders, and Tendon Disorders
arthrodesis site. A heavy cotton gauze roll providesuniform compression about the extremity, supportedby plaster splints. A circumferential cast should beavoided during the immediate postoperative periodbecause it can result in undue pressure against theexpanding extremity, increasing pain and possiblyjeopardizing healing of the wound edges. The postop-erative dressing is used for approximately 10 to 14 daysbefore removing the sutures.
After most fusions, bupivacaine hydrochloride(bupivacaine) is instilled into the wounds to diminishthe initial postoperative pain. A popliteal block isused, which generally provides 18 to 36 hours of painrelief. The popliteal block may be repeated after 18 to24 hours if the patient has too much breakthroughpain. It is much easier to prevent postoperative pain than play catch-up after the pain cycle has beenestablished.
COMPLICATIONS
The main complications after an attempted arthrode-sis include infection, skin slough, nerve disruption orentrapment, nonunion, and malalignment.
The possibility of infection is always a postsurgicalconcern. During surgery, antibiotic irrigation as well asparenteral antibiotics can help minimize this compli-cation. Good surgical technique with careful handlingof the tissues, removal of devitalized tissue, and pre-vention of hematoma formation also play an impor-tant role in minimizing the possibility of infection. Ifan infection occurs, it is important to recognize andtreat it promptly with appropriate antibiotics.
A skin slough around the foot and ankle can presenta difficult management problem because of the lack ofadequate subcutaneous tissue. The potential for a skinslough can be minimized by creating full-thicknessskin flaps, making incisions of adequate length to min-imize tension on the skin edges, using postoperativedrainage when appropriate, and applying a firm com-pression dressing postoperatively. Placing a patientinto a cast without adequate padding is not advisable.When a skin slough occurs, it is important to treat itvigorously with local debridement and application ofwet-to-dry dressings to promote granulation tissue,followed by coverage with a split-thickness skin graft.Vacuum-assisted closure (wound-VAC) can be extremelyuseful to manage a wound slough. If the slough is toolarge, a plastic surgeon should be consulted.
Nerve disruption or entrapment around the foot andankle not only creates numbness but also can causechronic pain from footwear rubbing against theneuroma. A carefully planned surgical approach is thebest treatment, but if a symptomatic neuroma occurs,
it should be identified and resected into an area notsubject to pressure and then buried either beneathmuscle or into bone.
A nonunion of an attempted fusion site is always anunfortunate event. As a general rule, of the jointsaround the foot and ankle, the talonavicular probablyhas the highest incidence of nonunion. Its curved sur-faces make adequate exposure difficult, and prepara-tion of the joint surfaces may be inadequate. Evenwhen the bone surfaces have been adequately prepared, nonunion can occur if internal fixation isinadequate.
The vascularity of the bone plays an important rolein the development of a nonunion. Avascular necrosisof the talus from any cause creates a situation that isvery difficult to manage. When avascular bone ispresent, it is often not possible to obtain a fusion tothe dysvascular bone, and an attempt must be madeeither to bypass the avascular area or to determine theportions of the talus that still have adequate vascular-ity and attempt a fusion using these areas. The navic-ular can develop evidence of avascular changes eitherspontaneously or secondary to previous injury. Whenthis problem is encountered, the involved area needsto be resected and bone grafted. When dealing withdysvascular bone preoperatively, it is important toidentify the areas of potential problems and create asurgical plan that will help solve the problem. Recog-nizing a dysvascular problem also helps to predict theoutcome for the patient.
Occasionally an asymptomatic nonunion occursand can be treated with observation. After a triplearthrodesis the talonavicular joint occasionally doesnot fuse, but because of a successful fusion of the sub-talar and calcaneocuboid joints, it may not be a sourceof pain. If a nonunion is symptomatic, a revision ofthe fusion site needs to be considered. If the overallalignment of the nonunion is satisfactory, bone graft-ing by inlaying bone across the nonunion site oftenresults in a fusion if internal fixation is adequate. Atother times, if the nonunion site has resulted in lossof alignment, the area needs to be revised. This is doneby removing the internal fixation and the fibrous tissuebetween the bone ends, realigning the surfaces, per-forming a bone graft if necessary, and inserting rigidfixation.
Malalignment after a fusion is a problem that usuallycan be avoided by meticulous bone preparation andrigid internal fixation. Malalignment after a triplearthrodesis is seen most often. The usual malalign-ment following a triple arthrodesis is varus of the heeland adduction or supination (or both) of the forefoot.This requires the patient to walk on the lateral aspectof the foot, causing patient dissatisfaction. When afusion of the hindfoot is performed, it is important to

CHAPTER 20 Arthrodesis of the Foot and Ankle 1091
evaluate the entire lower extremity preoperatively andintraoperatively to reduce the risk of malalignment.After carefully observing the normal extremity, thesurgeon should always relate the foot alignment to thepatella. Once the joint surfaces have been preparedand provisionally stabilized, the alignment shouldagain be checked to be sure it is correct. Malalignmentcan only be prevented by careful observation of theextremity at surgery.
SPECIFIC ARTHRODESES
Much has been written about arthrodesis of the footand ankle. Many surgical approaches, site prepara-tions, and types of internal and external fixation havebeen proposed. This section presents the techniques Ihave evolved over time and that result in a satisfactoryoutcome with careful adherence to technique. Othertechniques may be equally effective, but reproduciblygood results have been achieved with subtalararthrodesis, talonavicular arthrodesis, double arthro-desis, triple arthrodesis, naviculocuneiform arthrode-sis, and tarsometatarsal arthrodesis.
SUBTALAR ARTHRODESIS
An isolated subtalar joint arthrodesis results insatisfactory correction of deformity and relief ofpain that enables the patient to regain theability to perform most activities. Of the hind-foot fusions, the patient’s ability to achieve ahigh level of function is greatest after a subtalararthrodesis. Biomechanically, the position of thesubtalar joint determines the flexibility of thetransverse tarsal (talonavicular–calcaneocuboid)joint, and therefore it is imperative that a sub-talar arthrodesis be positioned in about 5degrees of valgus to permit mobility of thetransverse tarsal joint. If it is placed in varus, thetransverse tarsal joint is locked, and the patienttends to walk on the lateral side of the foot. Theposture of the forefoot also needs to be con-sidered because if there is more than 10 to 12degrees of fixed forefoot varus, after a subtalararthrodesis the patient cannot compensate forthis deformity and walks on the lateral side ofthe foot, resulting in discomfort beneath thefifth metatarsal head or base, or both, and insevere stress on the lateral ankle ligaments.Occasionally the fixed forefoot varus can be cor-rected by carrying out a simultaneous naviculo-cuneiform fusion.
It was previously believed that an isolatedsubtalar arthrodesis should not be carried out,and that a triple arthrodesis would be the pro-cedure of choice when a hindfoot fusion wasindicated. The literature has demonstrated,however, that an isolated subtalar arthrodesisproduces a superior result with less stress on theankle joint than a triple arthrodesis.*
Indications
The most common indication for a subtalararthrodesis is arthrosis secondary to trauma,usually a calcaneal fracture, rheumatoid arthritis,primary arthrosis, or talocalcaneal coalition thatcannot be resected. It is also indicated for amuscle imbalance (e.g., loss of peroneal musclefunction) or posterior tibial tendon dysfunctionwith an unstable subtalar joint but normal trans-verse tarsal joint motion and a fixed forefootvarus deformity of less than 12 degrees. A sub-talar arthrodesis is indicated in patients with aneuromuscular disorder such as Charcot–Marie–Tooth disease, poliomyelitis, or nerve injury withinstability of the subtalar joint.
Although a subtalar fusion can have an excel-lent result, if the deformity can be corrected witha calcaneal osteotomy instead of a fusion, thisshould be strongly considered.
Position of Arthrodesis
The subtalar arthrodesis should be placed inapproximately 5 degrees of valgus. Varus shouldbe avoided because it results in increased sta-bility of the transverse tarsal joint. Conversely,too much valgus results in an impingementagainst the fibula and increased stress along themedial aspect of the ankle joint.
Surgical Technique
1. The patient is placed in a supine positionwith a support under the ipsilateral hip tofacilitate exposure of the subtalar joint(video clip 11).
2. A thigh tourniquet is applied.3. The skin incision begins at the tip of the
fibula and is carried distally toward the baseof the fourth metatarsal. When an isolatedsubtalar arthrodesis is carried out, the inci-sion usually stops at about the level of thecalcaneocuboid joint (Fig. 20–1A).
*References 1-4, 7, 8, 10, 11, and 14-16.

Fibula
IncisionCalcaneo-
cuboid joint
Base fourthmetatarsal
A2
A1
B C
D1 D2Figure 20–1 Subtalar joint fusion. A, Site of fusion. Incision is made from the tip of the fibula and extends toward the base ofthe fourth metatarsal so as to place it in the interval between a branch of the superficial peroneal nerve dorsally and the suralnerve plantarly. B, Exposure of subtalar joint with Weitlaner retractor. C, A lamina spreader placed within the sinus tarsi areaexposes the posterior and middle facets. D, When a screw is used for fixation of the subtalar joint, it is placed through the pos-terior facet into the neck of the talus. Circle in the posterior facet (PF) demonstrates where the tine of the guide is placed inorder to accurately place the screw. MF identifies the middle facet. The anterior cruciate guide is placed into the subtalar jointwith the tine in posterior facet, as marked on the model. The guide is then set on the heel, after which a guide pin is placedacross the subtalar joint. E, Preoperative and postoperative radiographs demonstrate subtalar fusion using a 7.0-mm screw. Thescrew begins off the weight-bearing area of the heel. F, Preoperative and postoperative radiographs demonstrate subtalararthrodesis after calcaneal fracture. Interpositional bone graft is used to reestablish the talocalcaneal relationship. Interpositionalbone graft is rarely required to obtain a satisfactory result. G, When lateral subluxation of the subtalar joint is present, the jointmust be reduced and not fused in situ. The lateral aspect of the calcaneus should line up with the lateral aspect of the talus. H,Example of in situ fusion with persistent lateral subluxation of the subtalar joint, resulting in subfibular impingement and per-sistent pain. I, Preoperative and postoperative radiographs demonstrating subtalar fusion in a patient with prior ankle fusion whodeveloped arthrosis of the subtalar joint.
1092

E1 E2
G H
F1 F2
I2I1Figure 20–1—cont’d
1093

1094 PART V Arthritis, Postural Disorders, and Tendon Disorders
4. While deepening the incision, the surgeonshould be cautious, because the anteriorbranch of the sural nerve may be crossingthe operative site.
5. The incision passes along the dorsal aspectof the peroneal tendon sheath and distallyalong the floor of the sinus tarsi.
6. The extensor digitorum brevis muscle originis detached and the muscle belly reflecteddistally, exposing the underlying sinus tarsi,subtalar joint, and calcaneocuboid joint(Fig. 20–1B). The fat pad is dissected out ofthe sinus tarsi and reflected dorsally.
7. A small elevator is passed along the lateralside of the posterior facet of the sub-talar joint. It is not necessary to strip the per-oneal tendons off the lateral side of the calcaneus unless a lateral impingementfrom a previous calcaneal fracture requiresdecompressing.
8. With a curet, the contents of the sinus tarsiand tarsal canal are removed.
9. A lamina spreader is inserted into the sinustarsi to visualize the posterior facet of thesubtalar joint (Fig. 20–1C). When lookingacross the sinus tarsi, the surgeon can seethe middle facet of the subtalar joint. If thesurgery is being carried out for severearthrosis or a talocalcaneal coalition, it isoften not possible to open the subtalar jointvery far. Under these circumstances, a smallcuret is used to remove the cartilage fromthe posterior facet. A thin wide elevatorthen can be inserted into the joint to pry itopen, after which a lamina spreader isinserted.
10. With a curet of appropriate size, all the articular cartilage is removed from the posterior and middle facets. Using a curet,a fairly safe instrument, reduces the pos-sibility of damaging the flexor hallucislongus tendon in the posterior aspect of the joint or the neurovascular bundle alongthe posteromedial aspect of the joint. When removing the articular cartilage fromthe middle facet, it is important not to inadvertently go too far distally and damagethe cartilage on the plantar aspect of thehead of the talus, which lies just in front ofit.
11. Once all the articular cartilage has beenremoved, the lamina spreader is removedand the alignment of the subtalar joint
observed. If no deformity is present, thesurgeon may proceed with feathering orscaling the articular surfaces. If a varusdeformity needs to be corrected, bone isremoved from the lateral aspect of the pos-terior facet to correct the deformity. It isunusual to remove more than 3 to 5 mm ofbone when correcting a deformity, althoughoccasionally more bone needs to beremoved.
12. If a previous calcaneal fracture is present inwhich the lateral wall needs to be decom-pressed, the peroneal tendons are elevatedfrom the lateral aspect of the calcaneus asfar posteriorly and plantarward as possible.The impinging lateral wall is removed sothat it is approximately in line with thelateral aspect of the talus. Sometimes, up to7 to 10 mm of bone needs to be resectedin severe cases.
13. The posterior and middle facets, along withthe bone in the base of the sinus tarsi, areheavily scaled. The dense bone in the floorof the sinus tarsi is deeply scaled and ismobilized so that it can be packed into thetarsal canal after the internal fixation hasbeen inserted. The bone along the lateralaspect of the calcaneus that forms the anterior process may be mobilized to withinabout 0.5 cm of the calcaneocuboid jointand used for bone graft. When a lateraldecompression has been carried out, evenmore bone is available to the surgeon.Rarely is bone harvested from the iliac crest.
14. After the bone surfaces have been scaled,the subtalar joint is manipulated and placedinto the desired position of 5 degrees ofvalgus.
Internal Fixation
Internal fixation is carried out with a fullythreaded 7.0-mm cannulated screw to obtainmaximum interfragmentary compression. Awasher is always used.
Screw patterns used for fixation of the subta-lar joint include placing the screw from the neckof the talus into the calcaneus, placing a screwfrom the calcaneus into the talus, and placingtwo screws between the calcaneus and the talus.In most cases a single fully threaded screwinserted through a glide hole in the calcaneus,
CHAPTER 20 Arthrodesis of the Foot and Ankle 1095
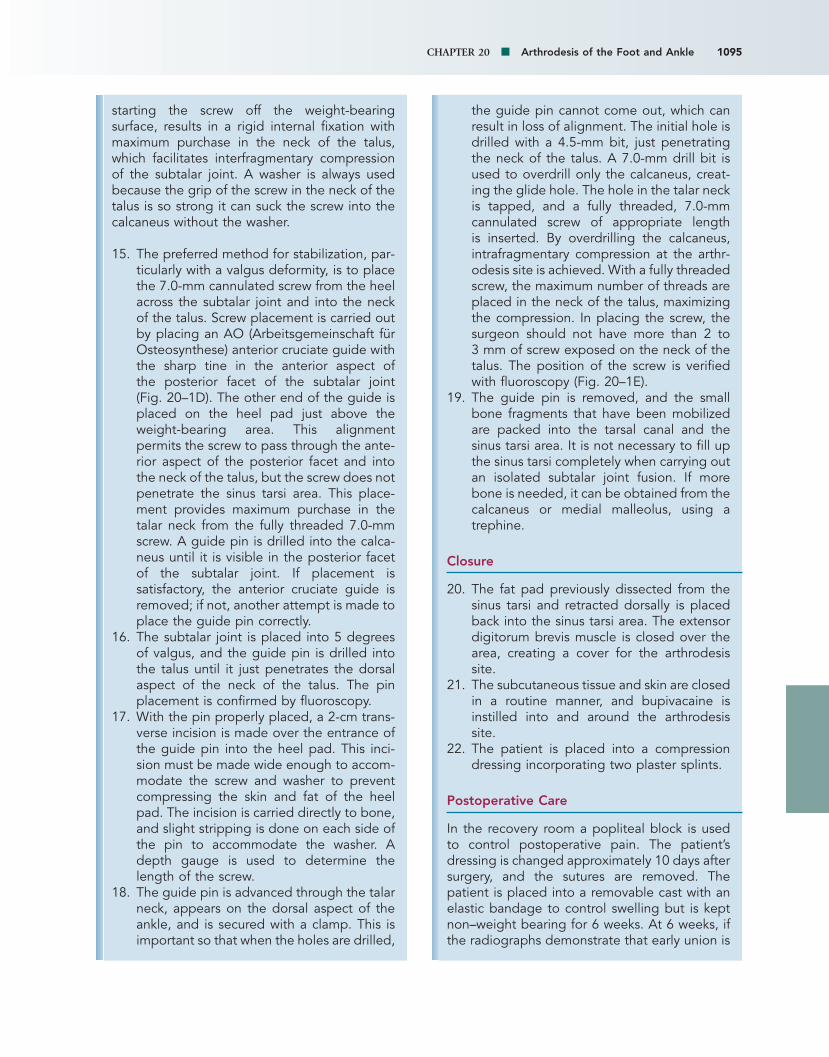
starting the screw off the weight-bearingsurface, results in a rigid internal fixation withmaximum purchase in the neck of the talus,which facilitates interfragmentary compressionof the subtalar joint. A washer is always usedbecause the grip of the screw in the neck of thetalus is so strong it can suck the screw into thecalcaneus without the washer.
15. The preferred method for stabilization, par-ticularly with a valgus deformity, is to placethe 7.0-mm cannulated screw from the heelacross the subtalar joint and into the neckof the talus. Screw placement is carried outby placing an AO (Arbeitsgemeinschaft fürOsteosynthese) anterior cruciate guide withthe sharp tine in the anterior aspect of the posterior facet of the subtalar joint (Fig. 20–1D). The other end of the guide isplaced on the heel pad just above theweight-bearing area. This alignmentpermits the screw to pass through the ante-rior aspect of the posterior facet and intothe neck of the talus, but the screw does notpenetrate the sinus tarsi area. This place-ment provides maximum purchase in thetalar neck from the fully threaded 7.0-mmscrew. A guide pin is drilled into the calca-neus until it is visible in the posterior facetof the subtalar joint. If placement is satisfactory, the anterior cruciate guide isremoved; if not, another attempt is made toplace the guide pin correctly.
16. The subtalar joint is placed into 5 degreesof valgus, and the guide pin is drilled intothe talus until it just penetrates the dorsalaspect of the neck of the talus. The pinplacement is confirmed by fluoroscopy.
17. With the pin properly placed, a 2-cm trans-verse incision is made over the entrance ofthe guide pin into the heel pad. This inci-sion must be made wide enough to accom-modate the screw and washer to preventcompressing the skin and fat of the heelpad. The incision is carried directly to bone,and slight stripping is done on each side ofthe pin to accommodate the washer. Adepth gauge is used to determine thelength of the screw.
18. The guide pin is advanced through the talarneck, appears on the dorsal aspect of theankle, and is secured with a clamp. This isimportant so that when the holes are drilled,
the guide pin cannot come out, which canresult in loss of alignment. The initial hole isdrilled with a 4.5-mm bit, just penetratingthe neck of the talus. A 7.0-mm drill bit isused to overdrill only the calcaneus, creat-ing the glide hole. The hole in the talar neckis tapped, and a fully threaded, 7.0-mm cannulated screw of appropriate length is inserted. By overdrilling the calcaneus,intrafragmentary compression at the arthr-odesis site is achieved. With a fully threadedscrew, the maximum number of threads areplaced in the neck of the talus, maximizingthe compression. In placing the screw, thesurgeon should not have more than 2 to 3 mm of screw exposed on the neck of thetalus. The position of the screw is verifiedwith fluoroscopy (Fig. 20–1E).
19. The guide pin is removed, and the smallbone fragments that have been mobilizedare packed into the tarsal canal and thesinus tarsi area. It is not necessary to fill upthe sinus tarsi completely when carrying outan isolated subtalar joint fusion. If morebone is needed, it can be obtained from thecalcaneus or medial malleolus, using atrephine.
Closure
20. The fat pad previously dissected from thesinus tarsi and retracted dorsally is placedback into the sinus tarsi area. The extensordigitorum brevis muscle is closed over thearea, creating a cover for the arthrodesissite.
21. The subcutaneous tissue and skin are closedin a routine manner, and bupivacaine isinstilled into and around the arthrodesissite.
22. The patient is placed into a compressiondressing incorporating two plaster splints.
Postoperative Care
In the recovery room a popliteal block is usedto control postoperative pain. The patient’sdressing is changed approximately 10 days aftersurgery, and the sutures are removed. Thepatient is placed into a removable cast with anelastic bandage to control swelling but is keptnon–weight bearing for 6 weeks. At 6 weeks, ifthe radiographs demonstrate that early union is

1096 PART V Arthritis, Postural Disorders, and Tendon Disorders
occurring, the patient is permitted to bearweight as tolerated in a removable cast. Approx-imately 12 weeks after surgery, radiographs areobtained, and if satisfactory union has occurred,the patient is permitted to ambulate with anelastic stocking.
Complications
Nonunion of the subtalar joint occurs infre-quently. The few nonunions that we haveencountered are usually in young patients aftera severe intraarticular calcaneal fracture in whichthe bone in the midportion of the calcaneusappears to be sclerotic and may be dysvascular.A nonunion should be repaired with bone graft-ing and further internal fixation.
Malalignment of the subtalar joint in too muchvarus results in locking of the transverse tarsaljoint and increased weight bearing on the lateralside of the foot. To accommodate this, thepatient often walks with the extremity in exter-nal rotation.
If the subtalar joint is placed into excessivevalgus, it can impinge against the fibula, causingpain over the peroneal tendons. It can also placeincreased stress along the medial aspect of theankle joint and pronation of the foot.
Sural nerve entrapment or laceration canoccur and may be bothersome to the patient.Unfortunately, the anterior branch of the suralnerve can pass next to the incision, making this complication almost unavoidable, but anattempt should be made to identify it andretract it if possible. If the neuroma is too both-ersome it requires resection to a more proximallevel.
Author’s Experience
We reviewed 101 of our subtalar arthrodesesusing the single lag screw method of fixation.The average time for arthrodesis was 12.3±3.4weeks. In the series, 99 of 101 fused (98%).6 Thepresence of a prior ankle fusion significantly prolonged the time to arthrodesis to 14.9±7weeks. Other factors including smoking, revi-sion surgery, patient age, or sex did not affecttime to arthrodesis. The fixation screw wasremoved in 13 (13%) of 101, at an average of8.8 months.
We reviewed another series of 48 subtalarfusions in 44 patients (26 women and 18 men;average age, 41.3 years; range, 13 to 75 years)
at an average of 60 months (range, 24 to 177months) after surgery.8 The preoperative diag-nosis was calcaneal fracture in 12 cases, talocal-caneal coalition in 11, subtalar joint arthrosiswithout calcaneal fracture in 12 (5 primary, 7post-traumatic), posterior tibial tendon dysfunc-tion in 11, subtalar joint instability in one, andpsoriatic arthritis in one case.
Fusion occurred in 47 of 48 arthrodeses, withthe one nonunion in a young patient after a cal-caneal fracture. This was successfully revisedusing iliac crest bone graft. Sixteen (33%) of the48 fusions underwent screw removal.
Forty-one patients (93%) were satisfied. Thethree dissatisfied patients (7%) had persistentpain; one foot was fused in 12 degrees of valgusand another in 7 degrees of varus. The patientsobserved a decrease in their pain from 3.7 out of 4.0 to 0.8 and a functional increase from3.4 out of 4.0 to 0.9. Using the AmericanOrthopaedic Foot and Ankle Society (AOFAS)scoring system,5 the patients averaged 89.3,which translated to 86% good and excellentresults, 7% fair, and 7% poor.
Functionally the patients did well, althoughhalf observed problems walking on unevenground and climbing steps and inclines. Seventypercent participated in recreational sports (e.g.,walking for pleasure, biking, skiing, swimming),and 14% were able to play sports that requiredrunning and pivoting (e.g., basketball, racquetsports). This is a much higher level of activitycompared with patients who have undergone atriple arthrodesis.3
Nine patients had work-related injuries; five ofthese had a fracture of the calcaneus with result-ant arthrosis. The two patients with bilateral frac-tures did not return to work, two were retrainedfor a sedentary job, and one retrained for a con-struction job. Of the four other patients, threereturned to work and one retired.
All patients wore normal shoes, and six usedan orthotic device.
The physical examination demonstrated thatthe alignment averaged 5.7 degrees of valgus,and the one patient with fusion in varus was dis-satisfied. The range of motion demonstrated anaverage of 9.8 degrees of dorsiflexion com-pared with 14.2 degrees on the uninvolved side,for a 30% loss of motion, and plantar flexionaveraged 47.2 degrees compared with 52.4degrees, for a 9.2% loss of motion. This resultedin a 14% loss of sagittal plane motion. The trans-
CHAPTER 20 Arthrodesis of the Foot and Ankle 1097
verse tarsal joint motion demonstrated 60% lossof abduction and adduction compared with theuninvolved side. Five feet had flexible forefootvarus with an average of 7 degrees, and six hadfixed forefoot varus with an average of 4.7degrees.
Final follow-up radiographs demonstrated anincrease in arthrosis of the ankle joint in 12 of33 patients; 11 of these had slight arthrosis (twohad mild symptoms), and one had moderatechanges and was symptomatic. Arthrosisincreased at the transverse tarsal joint in 13 of33 patients, 12 had slight arthrosis, and only onehad mild symptoms. New osteophyte formationalong the anterior aspect of the ankle was notedin 12 patients; five were slight (two sympto-matic), five moderate (all were symptomatic),and two severe (both symptomatic).
Evaluation of the subgroups demonstratedthat the 11 patients with a calcaneal fracture hadan AOFAS score of 83. Ten of the 11 underwentan in situ fusion with lateral wall decompression.One patient with severe collapse had a boneblock added to restore the height of the calca-neus. Based on our experience and that ofothers,9,12 it is not necessary to add a bone blockwhen carrying out an isolated subtalar fusionafter a calcaneal fracture unless severe impac-tion exists with greater than 1.5 cm loss ofheight (Fig. 20–1F).
The 10 patients who underwent a subtalararthrodesis for talocalcaneal coalition had anaverage AOFAS score of 93. Six of thesepatients had evidence of mild arthrosis of thetalonavicular joint at follow-up, but none weresymptomatic. Our study and another13 demon-strate that isolated subtalar fusion is the treat-ment of choice for a nonessential talocalcanealcoalition. A triple arthrodesis is not necessary toobtain a satisfactory result, even in the presenceof beaking of the talonavicular joint.
The eight patients with posterior tibial tendondysfunction had an AOFAS score of 88. This pro-cedure was used when the primary deformitywas in the hindfoot with hindfoot valgus andcalcaneal impingement against the fibula orwhen subtalar joint inversion was absent, pre-cluding the use of a tendon transfer. These
patients all had less than 12 degrees of fixedforefoot varus and no transverse tarsal jointhypermobility. A subtalar fusion is the procedureof choice for these patients, because a tendontransfer will fail owing to lack of subtalar inver-sion. A triple arthrodesis is not necessary andcreates a more rigid foot.
The five patients with primary arthrosis of thesubtalar joint that had not been previouslydescribed in the literature had an AOFAS scoreof 100. These patients did extremely well andhad essentially no limitations after their proce-dure. The other seven patients who had arthro-sis of the subtalar joint not associated with acalcaneal fracture but rather a talar fracture hadan AOFAS score of 86. This again demonstratesthat for an isolated subtalar joint problem, anisolated subtalar joint arthrodesis results in sat-isfactory correction, and that a more extensivefusion, with its increased long-term morbidity, isnot necessary.
Special Considerations
Occasionally in the patient with rheumatoidarthritis, severe subluxation occurs at the subta-lar joint (Fig. 20–1G and H). It is imperative thatthe clinician recognize this problem so thatwhen a subtalar arthrodesis is carried out, thecalcaneus is repositioned under the talus, restor-ing the normal weight-bearing alignment. If thesurgeon fails to recognize this malalignment andplaces a bone block into the lateral side of thesubtalar joint, wedging it open will not repo-sition the calcaneus into correct anatomic alignment.
Sometimes following an ankle arthrodesispatients develop arthrosis of the subtalar joint.In this situation we carry out our standard typeof fusion. The screw placement is a little simplerbecause there is no concern about penetratingthe ankle joint with the screw (Fig. 20–1I). Post-operatively these patients are placed into ashort-leg cast rather than a removable castbecause I believe better immobilization can beachieved. We have not had problems achievingan arthrodesis in this patient cohort, although itdoes take longer to occur.

1098 PART V Arthritis, Postural Disorders, and Tendon Disorders
TALONAVICULAR ARTHRODESIS
Although arthrodesis of the talonavicular jointinvolves only a single joint, biomechanically itresults in almost complete loss of motion in thesubtalar and transverse tarsal joints. This motionis lost because for the subtalar joint to invert andevert, the navicular must rotate over the talarhead. Thus, if talonavicular movement isrestricted, subtalar motion does not occur.19,22
An isolated talonavicular arthrodesis results ina satisfactory outcome, particularly in patientswho do not place a high demand on their foot,such as rheumatoid patients.18,20 In the high-demand patient or one working at a strenuousoccupation, it is probably advisable to add a calcaneocuboid joint arthrodesis. This creates adouble arthrodesis, resulting in increased stabil-ity of the transverse tarsal joint.17 The additionof the calcaneocuboid joint to the talonavicularfusion does not result in any further loss of hind-foot motion. Therefore, I usually carry out adouble arthrodesis instead of the isolated talo-navicular arthrodesis, except in the low-activitypatient.
Indications
The most common indication for an isolatedtalonavicular arthrodesis is primary arthrosis,arthrosis secondary to trauma,20 or rheumatoidarthritis.18 With instability of the talonavicularjoint secondary to dysfunction of the posteriortibial tendon or collapse of the talonavicularjoint from rupture of the spring ligament, an iso-lated talonavicular arthrodesis can be consid-ered. In these circumstances, however, I usuallycarry out a double or triple arthrodesis.
Alignment of the Fusion
The alignment of the normal foot is observed todetermine the alignment of the affected side.The positioning of an isolated talonaviculararthrodesis is very important, because the sub-talar and calcaneocuboid joint motion is greatlyrestricted after this arthrodesis. Therefore thehindfoot and forefoot must be aligned into aplantigrade position; if not, a nonplantigradefoot will be created and may be symptomatic.The subtalar joint should be placed into 5degrees of valgus, the talonavicular joint intoneutral, and the forefoot into 0 to 5 degrees offorefoot varus (Fig. 20–2A).
Surgical Technique
1. The patient is placed in the supine position,and a thigh tourniquet is applied. Becausethe extremity naturally falls into externalrotation, the patient does not requireturning.
2. The talonavicular joint is usually approachedthrough a longitudinal incision starting justdistal to the medial malleolus and carrieddistally 1 cm beyond the naviculocuneiformjoint (Fig. 20–2B). The incision can becurved slightly dorsally, particularly if a largedorsal osteophyte requires removal.
3. Using a periosteal elevator or a sharp,curved osteotome, the joint capsule is strip-ped from the dorsal, medial, and plantaraspects of the joint.
4. If dorsal osteophytes are present, they areremoved at this time, using an osteotomeor a rongeur.
5. Exposure of the talonavicular joint is facili-tated by placing a towel clip into the prox-imal medial portion of the navicular andapplying a distracting force in a medialdirection (Fig. 20–2C).
6. The articular surfaces of the talus and navicular are identified, and the articularcartilage is removed with an osteotome orcuret.
7. If the bone is hard enough, a small laminaspreader sometimes can be placed into themedial side of the joint to gain better visu-alization. This being a curved joint, visuali-zation of the lateral aspect is difficult butessential if satisfactory debridement is to beachieved.
8. The joint surfaces are heavily feathered, and the foot is manipulated into anatomicalignment.
9. The calcaneus is held in one hand, plac-ing the subtalar joint in approximately 5degrees of valgus. The talonavicular joint ismanipulated, bringing the transverse tarsaljoint into a few degrees of abduction andthe forefoot into a plantigrade position thatis perpendicular to the long axis of the tibia.If possible, the forefoot should not have aresidual of more than 5 to 7 degrees of fixedforefoot varus or valgus.
10. The type of internal fixation selecteddepends in part on the quality of the bone.Using two 4.0- or 4.5-mm cannulated screws

CHAPTER 20 Arthrodesis of the Foot and Ankle 1099
Flatfoot deformityLong axis of talus passesthrough first metatarsal
A2A1
B CFigure 20–2 Talonavicular arthrodesis. A, Radiograph and diagram demonstrate changes that occur in the talonavicular jointwith flatfoot deformity. The head of the talus deviates medially as the forefoot deviates laterally into abduction. The diagramdemonstrates abnormal alignment brought about by flatfoot deformity and its subsequent correction. The navicular is once againcentered over the head of the talus. B, Exposure of the talonavicular joint through a medial incision. The Freer elevator pointsto the naviculocuneiform joint. C, Access is gained to the talonavicular joint by distracting the joint with a towel clip.

1100 PART V Arthritis, Postural Disorders, and Tendon Disorders
Figure 20–3 Preoperative and postoperative radiographs demonstrate talonavicular arthrodesis using a 7.0-mm cannulatedscrew. Note the congenital hallux varus.
gives excellent fixation, and the profile ofthe screw head is low enough that fractur-ing the medial aspect of the navicular neednot be a concern. In a large person a 7.0-mm cannulated screw can be used. If thebone is very soft, multiple staples are useful.
11. With the surgeon holding the foot in correctalignment, a guide pin is placed startingalong the medial side of the navicular at the naviculocuneiform joint and drilledobliquely across the navicular into the headand neck of the talus.
12. The alignment of the foot is then once againcarefully verified, and if it is satisfactory, thepin placement is checked with fluoroscopy.A second parallel pin is inserted.
13. The navicular is overdrilled and a 40- to 50-mm, long-threaded cancellous screw isinserted. The smooth shank of the screwmust completely pass across the intendedfusion site. If the bone is soft, a washer isused.
14. After both screws have been inserted, thestability of the arthrodesis site is checked. Ifany significant motion is present, staplescan be used to increase stability. This issometimes necessary in the rheumatoidpatient or the elderly patient with poroticbone.
15. If the bone is too soft, four or five staplesare used for fixation. This is also useful if thenavicular fractures while inserting a screw(Fig. 20–3).
16. The wound is closed in layers, with the deepfascia being approximated over the arthro-desis site. The subcutaneous tissue and skin are closed in a routine manner. Thewound over the talonavicular joint rarelybreaks down.
17. Bupivacaine is injected into the wound toprovide postoperative analgesia.
18. The patient is placed into a compressiondressing incorporating two plaster splints.
Postoperative Care
In the recovery room a popliteal block is admin-istered to control postoperative pain. The post-operative dressing is changed in 10 to 14 days,sutures are removed, and the patient is placedinto a short-leg, removable cast with an elasticbandage to control swelling. Weight bearing is not permitted. Six weeks after surgery, radiographs are obtained, and if satisfactoryunion is occurring, the patient is permitted toambulate with weight bearing as tolerated in a short-leg cast. Three months after surgery, ifradiographic healing is evident, the patient is

CHAPTER 20 Arthrodesis of the Foot and Ankle 1101
permitted to ambulate without support as tolerated.
Complications
The nonunion rate of the talonavicular joint ismuch higher than that of the calcaneocuboid orsubtalar joint, partly because of the surgeon’sinability to gain adequate exposure of the entirejoint in preparation for the arthrodesis. The highnonunion rate can also result from the relativeavascularity of the navicular, particularly in post-traumatic cases. If a nonunion occurs and thealignment is satisfactory, carrying out a slot typeof bone graft into several areas around thetalonavicular joint usually results in satisfactoryunion.
Malalignment of the joint results in malposi-tion of the hindfoot and forefoot. The mostcommon malposition is a flatfoot deformity,which results from leaving the forefoot in toomuch abduction and the subtalar joint in valgus.This can only be corrected by revision to a triplearthrodesis.
DOUBLE ARTHRODESIS
The double arthrodesis as described byDuVries23 consists of a fusion of the talonavicu-lar and calcaneocuboid joints.17,24 It is based onthe biomechanical principle that if the motion inthe talonavicular and calcaneocuboid joints iseliminated, no motion occurs in the subtalarjoint. This results in the same degree of immo-bilization as a triple arthrodesis, but without the necessity of completing the subtalarportion. A double arthrodesis takes less timeand probably has less patient morbidity becausethe subtalar joint is not included in the fusionmass.
Indications
The double arthrodesis is indicated when themalalignment involves the transverse tarsal jointor forefoot, or both. It is most often carried out for patients with posterior tibial tendon dys-function who are not candidates for a ten-don reconstruction or subtalar fusion. In thesepatients, the subtalar joint is flexible and no subtalar disorder is present. There is also a
fixed forefoot varus, greater than 15 degrees,and abduction of the transverse tarsal joint is increased. A fusion of the talonavicular andcalcaneocuboid joints is sufficient to create a plantigrade foot without including the subtalar joint. If any arthrosis is present withinthe subtalar joint, a triple arthrodesis is indicated.
The double arthrodesis is also indicated inpatients with isolated arthrosis involving thetalonavicular joint who, because of their youngage or high level of activity, would be placinggreat stress on the foot. Although an isolatedtalonavicular arthrodesis is excellent for the lessactive patient (e.g., with rheumatoid arthritis), amore active person often has some pain in thefoot if the calcaneocuboid joint is not added tothe talonavicular fusion. Based on my experi-ence in large patients, rather than do a doublearthrodesis, a triple arthrodesis is a better pro-cedure, because when a double arthrodesis iscarried out, great stress is placed on the talon-avicular fusion site, which can result in fixationfailure and loss of alignment. When the subtalarjoint is added, creating a triple arthrodesis, itstabilizes the subtalar joint, relieving stress onthe talonavicular joint.
Position of Arthrodesis
The positioning of the foot for a doublearthrodesis is extremely critical. The subtalarjoint must be placed into 5 degrees of valgusand maintained there while the transverse tarsal joint is positioned into the same degreeof abduction or adduction as the normal foot.The forefoot is placed into a plantigrade position with little or no residual fixed forefootvarus. In many patients with dysfunction of the posterior tibial tendon, one of the maincomponents being corrected is the fixed fore-foot varus of greater than 15 degrees, whichprecludes performing an isolated subtalarfusion.
Surgical Technique
1. The patient is placed in a supine positionwith a support under the ipsilateral hip toallow easy access to the medial and lateralaspects of the foot (video clip 12).
2. A thigh tourniquet is applied.3. The skin incision is made along the lateral
aspect of the foot, starting at the base of

1102 PART V Arthritis, Postural Disorders, and Tendon Disorders
the fourth metatarsal, and extends proxi-mally toward the tip of the fibula, stoppingabout 1 cm short of the tip.
4. The incision is deepened to the extensordigitorum brevis muscle. Care is taken toidentify any anterior branch of the suralnerve that might be crossing the surgicalfield.
5. The capsule of the extensor digitorumbrevis is opened, its origin is released, andthe muscle is reflected distally about 1 cmdistal to the calcaneocuboid joint.
6. The calcaneocuboid joint is identified andthe soft tissue stripped plantarward anddorsally using a periosteal elevator.
7. The articular cartilage is removed from thecalcaneocuboid joint as thoroughly as pos-sible using a small, sharp osteotome orcuret.
8. Placing a deep retractor into the woundalong the dorsal aspect, the surgeon iden-tifies the lateral aspect of the talonavicularjoint opposite the calcaneocuboid joint and removes articular cartilage if possible.Usually, cartilage can be removed from thelateral third of the talar head and occasion-ally from the navicular, depending on howtight the foot is.
9. The medial approach is through a longitu-dinal incision, starting at the tip of themedial malleolus and carried distally 1 cmpast the naviculocuneiform joint (see Fig.20–2B).
10. The incision is deepened through the cap-sular tissues, after which the capsule andspring ligament are stripped from the nav-icular. An elevator is passed over the dorsalaspect of the talonavicular joint, completelyfreeing the joint.
11. Using a towel clip embedded into the prox-imal portion of the navicular, the surgeondistracts the talonavicular joint by pullingthe foot in an adducted position and longi-tudinally (see Fig. 20–2C). If the quality of the bone is adequate, a small laminaspreader is useful to gain exposure.
12. The articular cartilage is removed from thetalonavicular joint with an osteotome orcuret. Sometimes removing the cartilage isdifficult, and it is important to be sure thatthe joint capsule has been completelystripped from the talonavicular joint to facil-itate exposure.
13. The foot is manipulated into proper align-ment to determine whether any bone needsto be removed from the attempted fusionsite, which generally is not necessary. How-ever, it is important to be sure no gap iscreated at the calcaneocuboid joint when thefoot is brought into a plantigrade position.
14. To correct a severe forefoot varus deformity,the navicular must be plantar flexed on thehead of the talus. This is carried out byholding the hindfoot in one hand and rotat-ing the forefoot in such a way as to plantarflex the navicular on the head of the taluswhile simultaneously adducting the foot.This maneuver corrects the deformity andcreates a plantigrade foot.
15. With the foot held in a plantigrade posi-tion, the calcaneocuboid joint is observedbecause if it is distracted, some bone needsto be removed from the talar head. Thisdoes not occur often, but again, it is impor-tant that a gap is not created between thecalcaneus and cuboid.
16. Before placing the internal fixation, thebone ends are heavily scaled using a 4-mmosteotome. The talonavicular joint must bewell feathered from both medial and lateralsides to ensure that the greatest amount ofbone surface has been destroyed to helpprevent a nonunion.
17. Many ways are available to carry out internalfixation for a double arthrodesis. If adequatebone stock exists, two 4.0-mm cannulatedscrews across the talonavicular joint providesexcellent internal fixation. A single 7.0-mmscrew can be used in a large patient, but ina smaller person or a person with soft bone,it can result in a fracture of the medial sideof the navicular (Fig. 20–4A to C).
18. The foot is then manipulated into properalignment as described earlier; and theguide pin for the 4.0-mm cannulated screwis placed across the talonavicular joint.
19. The guide pin is started at the distal end ofthe navicular at the naviculocuneiform joint.If one starts at the midportion of the navic-ular, insufficient bone may be present alongthe medial side of the navicular, and a frac-ture of the medial aspect of the navicularcan occur. The surgeon should attempt toincorporate as much of the medial aspect of the navicular as possible with the screw.The placement is usually checked with

A
B3
C2
D2
B1
B2
C1
D1
Figure 20–4 A, Diagram of double arthrodesis. B, Preoperative and postoperative radiographs demonstrating arthrodesis using7-0 mm cannulated screws. C, Double arthrodesis using a cannulated screw for the talonavicular joint and power staples for thecalcaneocuboid joint. D, Double arthrodesis using power staples in both the talonavicular and calcaneocuboid joints. This isdone when the bone is soft, particularly in a patient with rheumatoid arthritis. Note the arrangement of staples around the jointto gain maximum stabilization. Continued
1103

1104 PART V Arthritis, Postural Disorders, and Tendon Disorders
E1 F1
F2
G3
G4
G1 G2
E2
Figure 20–4—cont’d E, Radiographs demonstrate failed double arthrodesis secondary to fracture of the talonavicular screw.F, Revision of double arthrodesis to a triple arthrodesis. G, Preoperative and postoperative radiographs demonstrate the cor-rection that can be obtained with double arthrodesis in a patient with an acquired flatfoot secondary to posterior tibial tendondysfunction.

CHAPTER 20 Arthrodesis of the Foot and Ankle 1105
fluoroscopy, and if placement is satisfactory,a parallel pin is inserted. The navicular isoverdrilled with a 4.0-mm drill bit, afterwhich 4.0-mm long threaded screws areinserted. It is important that the threadscross the joint surface. If the quality of boneis not good, washers should be employed.
20. The fixation of the calcaneocuboid joint is usually carried out using two 4.0-mm cannulated screws. As a general rule, thescrews can be brought from proximal todistal, starting in the anterior process area and brought obliquely across into thecuboid. At times, however, the bone align-ment is such that this is not possible, andthe screws are brought from the cuboid intothe calcaneus. Sometimes the bone is too soft, and a seam of staples is used (Fig. 20–4D).
21. The deep layers are closed, followed by thesubcutaneous tissues and skin.
22. The wounds are instilled with 0.25% bupi-vacaine, after which a compression dressingincorporating plaster splints is applied.
Postoperative Care
In the recovery room a popliteal block is admin-istered to control postoperative pain. The post-operative dressing is removed in approximately10 days, after which the patient is placed into aremovable cast with an elastic bandage tocontrol swelling. The patient is kept non–weightbearing for 6 weeks from the time of surgery. At6 weeks, radiographs are obtained. If satisfac-tory union is occurring, the patient is permittedto bear weight in a cast. Approximately 12weeks after surgery, radiographs again areobtained. If satisfactory union has occurred, thepatient is permitted to ambulate with an elasticstocking .
Author’s Experience
We reviewed our experience with 32 patients(19 women, 13 men) who had undergone adouble arthrodesis.25 The average age was 62years (range, 38 to 81 years), and averagefollow-up was 56 months (range, 24 to 162months). The diagnosis was posterior tibialtendon dysfunction in 20 patients, isolatedtalonavicular arthrosis in five, rheumatoid arthri-tis in five, talar neck nonunion in one, and anacquired flatfoot deformity after a spinal cordinjury in one.
The patients’ satisfaction rate was 92%, and8% were dissatisfied. Pain relief was the mainbenefit. The preoperative pain, assessed as 4.3of a possible 5, diminished postoperatively to1.4 (zero equals no pain). Functional capacityincreased from 3.6 of 4 preoperatively to 1.3postoperatively.
The fusion rate was 87.5% (28 of 32 cases).Four nonunions of the talonavicular jointoccurred, all of which had staple fixation. Threeof the four required a revision to a triplearthrodesis (Fig. 20–4E and F).
As a group, they noted maximum recovery atabout 8 months after surgery.
The patients’ level of activities demonstratedthat most could walk for pleasure, and five wereable to run short distances; 60% played golf,biked, hiked, and swam. Seventy-five percent ofthe patients noted some difficulty when walkingon uneven ground or inclines or when going upand down steps.
The physical examination demonstrated thatthe average hindfoot position was 5.8 degreesof valgus, the transverse tarsal joint had 4.4degrees of abduction, and the forefoot varuswas 9 degrees. The range of motion of the anklejoint decreased 11 degrees compared with theuninvolved side.
The radiographic evaluation demonstratedthat the anteroposterior (AP) talar–secondmetatarsal angle improved from 30 degrees(abduction) to 14 degrees, and the lateraltalar–first metatarsal angle improved from !16degrees (indicating dorsiflexion) to !7 degreespostoperatively (Fig. 20–4G).
The follow-up radiographs demonstrated aslight degree of ankle arthrosis in 53% ofpatients that was not present preoperatively,and 30% noted mild symptoms. Twenty percentdemonstrated evidence of arthrosis in the sub-talar joint, but none were symptomatic. The nav-iculocuneiform joint demonstrated an increasein arthrosis in 37% of patients, all of whom hadslight symptoms, except for one patient, whosesymptoms were severe. The tarsometatarsaljoints demonstrated a 22% increased incidence,but none were symptomatic.
Special Considerations
Complex problems involving the talonavicularjoint include its possible collapse secondary tofracture, avascular necrosis, or both. At othertimes, involvement of the forefoot distal to the

1106 PART V Arthritis, Postural Disorders, and Tendon Disorders
talonavicular joint occurs, with extension intothe naviculocuneiform and sometimes the tar-sometatarsal joints. In these situations a modi-fied double arthrodesis has been used toprovide stability.
In many of these cases the overall alignmentof the foot is satisfactory or at least adequate fora plantigrade foot. Rather than take down theinvolved areas and place a large bone graft, arectangular slot is cut from the talus to thecuneiforms or into the metatarsal bases, as indi-cated by the clinical circumstances (Fig. 20–5).The slot is cut all the way across the foot frommedial to lateral, after which a piece of iliac crestbone graft is inlaid into the slot. Fixation of thebone graft and surrounding bone is done withscrews or multiple staples. At the same time thecalcaneocuboid joint is arthrodesed to providestability to the lateral column. This is obviously
A B
C DFigure 20–5 Technique for slot graft to correct disruption of tarsal joints. A, Outline of slot graft extending from the talus intothe metatarsal bones. B, Preoperative and postoperative radiographs demonstrate placement of the bone block, which is heldin place with two 4.0-mm screws, and fusion of the calcaneocuboid joint to help reinforce the fusion site. Preoperative and post-operative anteroposterior (C) and oblique (D) radiographs demonstrate placement and incorporation of the bone block.
an extensive procedure and is only done undercertain circumstances when significant deformitywithin the midportion of the foot is present butno significant anatomic correction needs to becarried out. In a situation with marked destruc-tion of the midfoot and malalignment, this pro-cedure cannot be used. Then one would needto take down the involved area and either bonegraft it or possibly collapse the lateral column torealign the midfoot.
After the inlay bone graft procedure, thepatient is immobilized for a prolonged period.As a general rule, weight bearing is not permit-ted for 3 months, after which the patient is grad-ually started on progressive weight bearing overthe next 3 months. It is sometimes difficult tostate when union has occurred, and thereforethe surgeon should be very cautious in allowingpatients to bear weight.

CHAPTER 20 Arthrodesis of the Foot and Ankle 1107
A
B1
C1
D1
D3
B2
C2
D2 D4
Figure 20–6 Triple arthrodesis, methods of internal fixation. A, Diagram of triple arthrodesis. B, Postoperative radiographdemonstrating triple arthrodesis with anatomic restoration of foot posture. C, Triple arthrodesis using 7.0-mm cannulated screwsfor the subtalar and talonavicular joints and multiple power staples for the calcaneocuboid joint. D, Correction of severe hind-foot deformity secondary to long-standing posterior tibial tendon dysfunction with restoration of the longitudinal arch using a7.0-mm cannulated screw for the subtalar joint and power staples for the talonavicular and calcaneocuboid joints. Note that theheight of the longitudinal arch has been restored and severe abduction of the foot is corrected.
TRIPLE ARTHRODESIS
The triple arthrodesis consists of fusion of thetalonavicular, calcaneocuboid, and subtalarjoints (Fig. 20–6A). Initially the triple arthrodesiswas used to treat deformities of the foot secondary to paralysis, mainly poliomyelitis, in which severe anatomic distortion was pre-sent.33,35,38 To correct this abnormality, largebone wedges were resected to place the footinto a plantigrade position. Little or no internalfixation was used, and at times the patient wasreturned to surgery in the immediate postoper-
ative period to remanipulate the foot into betteralignment.
As the number of patients with deformed feet secondary to paralysis declined, the triplearthrodesis was performed less often. It is nowmost often carried out for residuals of trauma,rheumatoid arthritis, and long-standing poste-rior tibial tendon dysfunction in which the basicbone anatomy is present. Although distorted,significant bone resection is usually not neces-sary. This allows the procedure to be done byreleasing the contracted joint capsules, remov-ing the articular cartilage, scaling the exposed

1108 PART V Arthritis, Postural Disorders, and Tendon Disorders
bony surfaces, and using manipulation to createa plantigrade foot. It is not unusual to carry out a triple arthrodesis when no distortion of the anatomy exists, and an in situ fusion isachieved.32
The best way to carry out a triple arthrodesisis by meticulously releasing the joint capsules tomobilize the joint; removing the articular carti-lage; scaling or feathering the bone surfaces;aligning the foot into a plantigrade position;and securing the joints with rigid internal fixa-tion. By using these principles, a high fusion rateand a plantigrade foot can be achieved. In ourexperience, bone grafting from the iliac crest israrely necessary, but if bone graft is needed, itcan usually be obtained from the calcaneus,medial malleolus, or proximal tibia without violating the iliac crest and risking added morbidity.
Although the triple arthrodesis is a valuabletool for the orthopaedic surgeon, it is notwithout postoperative complications. The litera-ture points out that because of the added stress across the ankle joint as a result of a triple arthrodesis, approximately 30% of pa-tients demonstrate ankle degeneration at 5years.26-31,36-38 This reinforces the biomechanicsof the foot and ankle complex, demonstratingthat the ankle, subtalar, and transverse tarsaljoints are functioning together. When a triplearthrodesis is carried out, increased stress isplaced proximally on the ankle joint and distallyon the midfoot. Therefore it is imperative that amore limited arthrodesis always be consideredwhen feasible. Because of the possible anklejoint deterioration, when evaluating the patientpreoperatively for a triple arthrodesis, a weight-bearing AP radiograph of the ankle must beincluded to ascertain if preexisting arthrosis canpreclude the triple arthrodesis or at least topredict the future for the patient.
Indications
Arthrosis involving the subtalar joint and eitherthe talonavicular or the calcaneocuboid joint, orboth, is an indication for triple arthrodesis.Arthrosis of only the subtalar joint can usually betreated by an isolated subtalar joint fusion.
Triple arthrodesis can be used for the unsta-ble hindfoot secondary to neuromuscular disor-ders such as poliomyelitis, nerve injury, posteriortibial tendon dysfunction, or rheumatoid arthri-
tis in which the subtalar and transverse tarsaljoints are involved. Malalignment of the footsecondary to arthrofibrosis resulting from a compartment syndrome, crush injury, or severetrauma is an indication for a triple arthrodesis.In the patient with a symptomatic, unresectable,or previously resected calcaneonavicular coali-tion, a triple arthrodesis is indicated. It is important to appreciate, however, that thepatient with a talocalcaneal (subtalar) coalitioncan be treated with an isolated subtalar fusioneven if there is osteophyte formation on thedorsal aspect of the talar head. The patient with a severe symptomatic pes planus deformitythat is not amenable to other procedures, such as lateral column lengthening, calcanealosteotomy, or subtalar fusion, can also be con-sidered a candidate for a triple arthrodesis.
Whenever considering a triple arthrodesis,however, the surgeon must be mindful of theconsequences of the potential degeneration atthe ankle joint. If a younger person can betreated with an AFO or a more limited fusion,this may be a better method of treatment.
Position of Arthrodesis
The position of a triple arthrodesis is criticalbecause once an arthrodesis has been achieved,the foot is in a fixed position and cannot accom-modate to the ground. It is therefore essentialthat the hindfoot be placed in about 5 degreesof valgus, the transverse tarsal joint in 0 to 5degrees of abduction, and the forefoot in lessthan 10 degrees of varus. If accurate alignmentis not achieved, the patient will have a non-plantigrade foot, which can cause chronic painthat requires a revision.
Surgical Technique
1. The normal foot is examined and its alignment noted. Patients have a varyingdegree of forefoot adduction or abduction,and the surgeon should attempt to matchthis with the affected extremity (video clip14).
2. The patient is placed in a supine positionwith a support under the ipsilateral hip toimprove visualization of the lateral aspect ofthe hindfoot. (A detailed discussion of thisapproach is presented in the sections onsubtalar and double arthrodeses.)

CHAPTER 20 Arthrodesis of the Foot and Ankle 1109
3. The skin incision starts at the tip of the fibulaand is carried to the base of the fourthmetatarsal. Caution should be used whendeepening this incision, looking for the suralnerve and possibly an anterior branch (seeFig. 20–1A).
4. The extensor digitorum muscle is removedfrom its origin on the lateral side of the talusand calcaneus and retracted distally.
5. The subtalar and calcaneocuboid joints are visualized, and the articular cartilage isremoved.
6. Through the lateral incision, the lateralaspect of the talonavicular joint is identifiedand as much articular cartilage is removedas possible. (A detailed discussion of thisapproach is presented in the section ontalonavicular arthrodesis.)
7. The skin incision begins 2 cm distal to thetip of the medial malleolus in the midlineand is carried 1 cm distal to the naviculo-cuneiform joint (see Fig. 20–2B).
8. The incision is deepened to expose the jointcapsule, which is stripped from the talonav-icular joint.
9. Using a towel clip in the navicular, thesurgeon distracts the joint by pulling thefoot into an adducted position to enhancevisualization of the articular surfaces (seeFig. 20–2C). If the bone stock is adequate,a small lamina spreader is useful.
10. The articular cartilage is removed from thetalonavicular joint.
11. At times, some articular cartilage is alsoremoved through the lateral incision. Thisdepends on the flexibility of the foot.
12. The foot is manipulated, first by bringingthe subtalar joint into 5 degrees of valgus,then manipulating the transverse tarsal jointto eliminate the fixed forefoot varus. This isdone by rotating the navicular in a plantardirection on the head of the talus and simul-taneously bringing the transverse tarsal jointinto about 0 to 5 degrees of abduction. Thismaneuver usually creates a plantigradefoot. The foot cannot be manipulated if the joints have not been completely mobilized.
13. After the manipulation, it is important toinspect the articular surfaces to be surethere is good bone apposition. If the bonesare not properly apposed, it may be neces-sary to remove some bone, usually from the
head of the talus, to shorten the medialcolumn and close the calcaneocuboid joint.
14. Once alignment has been achieved, thejoint surfaces are heavily scaled or featheredin preparation for internal fixation.
15. The internal fixation is initially achieved inthe subtalar joint (see the section on subta-lar arthrodesis and Fig. 20–1D).
16. The anterior cruciate guide is placed intothe posterior facet of the subtalar joint andthen the back of the heel. A guide pin isinserted into the posterior facet and the AOguide is removed.
17. The calcaneus is manipulated into 5 de-grees of valgus, and the pin is advancedinto the neck of the talus. Its position is ver-ified by fluoroscopy.
18. The length of the screw is determined and the guide pin is drilled through topresent on the dorsal aspect of the anklejoint.
19. A 4.5-mm cannulated drill is used to makethe initial hole, which must pass through theanterior cortex of the talus, after which thecalcaneus is overdrilled with a 7.0-mm bit.The talar neck is tapped and a 7.0-mm fullythreaded cannulated screw with a washer isinserted. This fixes the subtalar componentof the triple arthrodesis in correct align-ment. In our experience, a single screw isadequate to stabilize the subtalar joint.
20. The transverse tarsal joint is manipulated tocorrect the forefoot malalignment. Once theappropriate alignment has been achieved,the talonavicular joint is fixed.
21. The fixation of the talonavicular joint isusually achieved with two 4.0-mm cannu-lated screws. The guide pin is insertedacross the talonavicular joint, starting at the naviculocuneiform joint, and is drivenobliquely into the neck of the talus. Twoguide pins are inserted and their position isverified radiographically.
22. The navicular is overdrilled with a 4.0-mmdrill bit, and a partially threaded cannulatedscrew of appropriate length is inserted; awasher may be used depending upon bonequality. The screws generally are about 45to 60 mm in length, but this varies frompatient to patient.
23. The calcaneocuboid joint is visualized andfixed with two 4.0-mm cannulated screws.The guide pin is placed from the calcaneus

1110 PART V Arthritis, Postural Disorders, and Tendon Disorders
into the cuboid, and two partially threadedscrews of appropriate length are used. If thebone is too soft, staples are used.
24. If the surgeon is not satisfied with the coap-tation of the bony surfaces, a bone graft canbe used if necessary.
25. The extensor digitorum brevis muscle isclosed over the lateral side of the wound,after which the subcutaneous tissue andskin are closed. On the medial side, thecapsular tissue is closed over the talonavic-ular joint, if possible, after which the subcu-taneous tissue and skin are closed.
26. Bupivacaine (0.25%) is instilled into thewound to provide initial postoperative analgesia.
27. A compression dressing incorporating twoplaster splints is applied.
Postoperative Care
In the recovery room, a popliteal block is admin-istered to control the immediate postoperativepain. The patient’s initial surgical cast is changed10 to 14 days after surgery, and the sutures areremoved if appropriate. The patient is placedinto a short-leg removable cast with an elasticbandage to control edema and is kept non–weight bearing for 6 weeks. Then radiographsare obtained, and if satisfactory union is occur-ring, the patient is permitted to bear weight astolerated in the removable cast.
Twelve weeks after surgery, radiographs areagain obtained, and if a fusion has occurred, the patient wears an elastic stocking and is permitted to bear weight as tolerated. If thefusion is somewhat tenuous, the patient is askedto walk around the house without the cast anduse it outside for another month (Fig. 20–6B to D).
Complications
The most frequent complication after a triplearthrodesis is a nonunion of one of the fusionsites, most often the talonavicular joint, proba-bly because its exposure is more difficult and thebone may be sclerotic. If a nonunion occurs andis not symptomatic, no treatment is indicated.Occasionally after a triple arthrodesis, if two ofthe three joints have fused, the joint with anonunion is asymptomatic. If a painful nonunionis present but the alignment of the extremity issatisfactory, some type of an inlay bone block
across the area of the nonunion, possibly alongwith reinforcement of the internal fixation,usually results in a satisfactory fusion. If the areaof the nonunion is symptomatic and the align-ment is unsatisfactory, revision of the arthrode-sis may be necessary.
The next most common complication ismalalignment. In my experience the most fre-quent malalignment is residual varus of the cal-caneus, followed by a fixed forefoot varus andthen adduction of the forefoot. A valgus defor-mity of the hindfoot, although not as commonas a varus deformity, is distressing for mostpatients and can result in an unsatisfactoryoutcome.31,35 In this situation the surgeon mightconsider a medial displacement calcaneal oste-otomy to correct the excessive valgus if the remainder of the forefoot alignment is satisfactory.
Entrapment of the sural nerve, particularly ananterior branch, giving rise to dysesthesias onthe lateral side of the foot, can annoy thepatient. This might need to be corrected by a neurolysis or resection of the nerve, thenburying the stump under soft tissues or intobone.
Occasionally after a triple arthrodesis in apatient with long-standing severe valgus defor-mity, although a plantigrade position of the footcan be achieved, the ankle cannot be broughtback to neutral position because of an Achillestendon contracture. When the triple arthrodesisis carried out, if the ankle cannot be broughtinto about 5 degrees of dorsiflexion, an Achillestendon lengthening or gastrocnemius slideshould be strongly considered. One must becautious, however, not to overlengthen thetendon, but the foot should not be left in an equinus posture. Adults recover theirstrength very slowly, if at all, after Achillestendon lengthening.
Revision for Malalignment
A plantigrade foot might not be achieved aftera triple arthrodesis. If the patient is sympto-matic, a revision of the triple arthrodesis may beindicated. Technically these are very difficultcases and need to be carefully planned preop-eratively to identify the precise nature anddegree of the malalignment and which compo-nents of the triple arthrodesis need to berevised.

CHAPTER 20 Arthrodesis of the Foot and Ankle 1111
If the hindfoot is malaligned and the forefootis in a plantigrade position, the hindfoot can becorrected without revising the forefoot. If a varusdeformity is present, a lateral closing wedgeDwyer procedure can be used. Occasionally a lateral displacement osteotomy with somerotation of the fragment from varus into val-gus can produce better alignment.
When the calcaneus is in too much valgus andthere is an impingement against the fibula, a calcaneal osteotomy displacing it in a medialdirection can be used to correct the deformity.However, rather than create a long obliqueosteotomy, as one would for a Dwyer proce-dure, the cut is made more perpendicular, justposterior to the posterior facet of the subtalarjoint. The osteotomy is then displaced mediallyabout 1 cm, and occasionally the posterior frag-ment can be rotated slightly on its long axis ifthe degree of valgus has a rotational compo-nent. Fixation of the osteotomy is usually donewith a cannulated 7.0-mm screw placed justlateral to the Achilles tendon and driven distallyacross the osteotomy site into the calcaneus. Ifone screw is not adequate for fixation, a Stein-mann pin is used for 4 weeks until the boneshave become sticky.
If the hindfoot is properly aligned and themain deformity is malalignment of the forefoot,usually from residual forefoot varus, the frontportion of the triple arthrodesis can be revisedand the hindfoot left intact. Besides the varusdeformity, an adduction deformity is also oftenpresent. This type of revision is carried outthrough a medial and lateral approach throughthe previous incisions. The soft tissues arestripped off the fusion mass around the trans-verse tarsal joint, which is osteotomized, and thefoot is realigned. The realignment is usuallycarried out by rotating the forefoot block ofbone into a more pronated position. If there isresidual adduction or possibly abduction in theforefoot, a lateral or medial closing wedge isremoved at the same time to achieve satisfac-tory alignment. Fixation after a revision canusually be achieved by using large screws, butif the bone is too soft, multiple staples can beuseful.
The postoperative regimen after revision of a triple arthrodesis is the same as for a triple arthrodesis, that is, non–weight bearingfor 6 weeks and then weight bearing for 6weeks.
Author’s Experience
We have reviewed two groups of patients aftertriple arthrodesis.30,34 The first group involved 29fusions in 27 patients (23 women, 4 men) fortreatment of posterior tibial tendon dysfunction.The average age was 62 years (range, 44 to 78years), and average follow-up was 55 months(range, 24 to 122 months). The preoperativeAOFAS score was 30, which improved postop-eratively to 80. One nonunion of the talonavic-ular joint occurred and was asymptomatic.
The AP radiographs demonstrated that thetalar–first metatarsal angle improved from 24 to 10 degrees postoperatively and thetalar–second metatarsal angle from 35 to 19degrees. In the lateral radiograph the talar–first metatarsal angle improved from 18 to 9degrees. In all cases the final correction wasgreater than the contralateral foot if it was notpathologic. The radiographs further demon-strated an increase in the arthrosis in the anklejoint in 10 of 29 cases (33%), in the naviculo-cuneiform joint in five (17%), and at the tar-sometatarsal joint in four (14%) (Fig. 20–7A and B).
A second group consisted of 17 patients (12women, 5 men) and 18 feet, with an averageage of 66 years (range, 52 to 80 years ). Theywere evaluated to determine the effect of atriple arthrodesis in the older age group,because no paper had previously addressed thisin the literature.30 The etiology was poste-rior tibial tendon dysfunction in 10 patients,rheumatoid arthritis in three (four feet), diabetesmellitus in one, poliomyelitis in one, trauma inone, and poststroke effects in one. The follow-up was 42 months (range, 27 to 156 months).The procedure was carried out because of pain,deformity, or both. The pain level preoperativelywas 4 on a scale of 5 and postoperatively was 1.
Fourteen patients (15 feet) were satisfiedbecause of the improved position and dimin-ished pain. Interestingly, however, 11 patientsstill thought they had some pain in the foot, but it was not sufficiently symptomatic for themto be dissatisfied with the procedure. Of thethree patients who were dissatisfied, two had a valgus alignment of the heel that resulted in pain. The patients observed that the timefrom surgery to maximum relief was about 10months.

1112 PART V Arthritis, Postural Disorders, and Tendon Disorders
A B
Figure 20–7 A, Mild valgus tilt of theankle joint 2 years after triple arthrode-sis. B, Moderate valgus tilt 3 years aftertriple arthrodesis.
The level of activities improved for ninepatients (10 feet). Seven reported no change intheir ambulatory capacity, and one believed thather ambulatory capacity was decreased. Theappearance of the foot improved for 13 of 17patients, and two were dissatisfied because ofthe valgus alignment of their heel. Twelvepatients (13 feet) could wear any shoe theywanted, but five had some problems withfootwear.
The range of motion demonstrated that dor-siflexion was equal on both feet, and plantarflexion on the affected side was 30 degreescompared to 44 degrees on the normal side, fora 32% loss.
Radiographs demonstrated that the APtalar–second metatarsal angle improved from36 to 16 degrees and the lateral talar–firstmetatarsal angle from 22 to 9 degrees, whichindicates plantar flexion of the first metatarsal.
Some evidence of arthrosis of the ankle jointwas seen preoperatively in 14 of the 18 anklesand progressed in seven (one grade in threeankles and greater than one grade in four).Seven patients demonstrated changes at thenaviculocuneiform and tarsometatarsal joints.
Three nonunions occurred, one at the talo-navicular joint, which was revised successfully,
and two at the calcaneocuboid joint, one requir-ing revision and one being asymptomatic.
In summary, the triple arthrodesis is an excel-lent procedure for correcting a fixed deformityof the foot, but it should be used judiciously,particularly in the younger patient, and onlywhen a lesser procedure cannot be used.
NAVICULOCUNEIFORM ARTHRODESIS
A naviculocuneiform arthrodesis is usuallycarried out for arthrosis of one or more of thearticulations as a result of primary arthrosis orsecondary to trauma. The other reason to carryout this arthrodesis is in the patient with poste-rior tibial tendon dysfunction and a fixed fore-foot varus deformity so that a more extensivehindfoot fusion can be avoided.
In the patient with a fixed uncorrectable forefoot varus deformity, a double or triplearthrodesis is indicated because an isolated sub-talar arthrodesis would cause the patient to walkon the lateral border of the foot. If the fixed fore-

CHAPTER 20 Arthrodesis of the Foot and Ankle 1113
foot varus can be corrected, however, patientswith this deformity can be treated with a sub-talar arthrodesis and a naviculocuneiformarthrodesis. This spares the transverse tarsaljoint, which leaves the forefoot more flexible.Approximately 15 to 20 degrees of fixed fore-foot varus can be corrected through the navicu-locuneiform joint, depending upon how rigidthe deformity is.
Indications
The most common indication is isolated navicu-locuneiform arthrosis secondary to trauma. Thenext most common indication is a fixed forefootvarus deformity secondary to posterior tibialtendon dysfunction.
Position of Arthrodesis
With arthrosis of the joint secondary to traumathere usually is little or no deformity of the fore-foot, and an in situ fusion can be carried out.Because this is a difficult articulation to obtainan isolated arthrodesis, the fusion mass shouldinclude the first and second and, if possible, the third naviculocuneiform joints. When thereis a fixed forefoot varus, the position of thearthrodesis depends upon the degree of defor-mity. Arthrodesis is usually carried out alongwith either a subtalar arthrodesis or a recon-struction of the posterior tibial tendon with anFDL transfer.
Surgical Technique
1. The patient is placed in the supine position,and a thigh tourniquet is applied. Becausethe extremity naturally falls into externalrotation, the patient does not requireturning.
2. The naviculocuneiform joint is approachedthrough a longitudinal incision starting justdistal to the medial malleolus and carrieddistally just dorsal to the posterior tibialtendon, distal enough to expose the firstmetatarsocuneiform joint.
3. The dissection is carried down to bone,using caution not to injure the posteriortibial tendon as it passes on the plantaraspect of the wound. As one proceeds dis-tally, the tibialis anterior tendon is obliquelycrossing the field and needs to be mobilizedso that it can be pulled somewhat distallyout of harm’s way.
4. By sharp and blunt dissection the jointcapsule is stripped from the medial, dorsal,and plantar aspects of the joint.
5. Using a small osteotome, the articular carti-lage is removed from the first, second, andthird cuneiform, as well as the correspon-ding surface of the navicular. Usually it is difficult to completely denude the third naviculocuneiform joint. A small laminaspreader does help facilitate exposure ofthese joints.
6. The articular surfaces are then featheredwith a 4-mm osteotome or perforated withmultiple drill holes.
7. The foot is corrected by rotating the distalportion of the foot into pronation or plantarflexion at the fusion site while holding thehindfoot in neutral position. Sometimes ittakes several manipulations in this mannerto gain the necessary correction. It is im-portant, however, that as this is carried out the hindfoot is held in neutral position,otherwise inadequate correction will beobtained. If correction of the deformityseems overly difficult, it is probably due tolack of adequate capsular stripping.
8. Once the foot is manipulated into satisfac-tory alignment, a 0.062-inch Kirschner wireis placed across the dorsal aspect of thejoint to stabilize it so that internal fixationcan be inserted.
9. Rigid fixation can be achieved by placingthe screws from the tubercle of the navicu-lar and proceeding distally into the first andsecond cuneiforms. A third screw passingfrom the first cuneiform back into the nav-icular can also be used with caution. Theproblem with the screw passing in this direc-tion is that all the threads have to passacross the fusion site and cannot enter thetalonavicular joint.
10. Usually one screw is passed from the navic-ular into the first cuneiform and the secondfrom the navicular into the second cunei-form. As a rule, it is not possible to get ascrew from the navicular into the thirdcuneiform.
11. The wound is closed in layers, with the deepfascia being approximated over the fusionsite. The subcutaneous tissue and skin areclosed in a routine manner. Wounds alongthe medial border of the foot usually healwell.
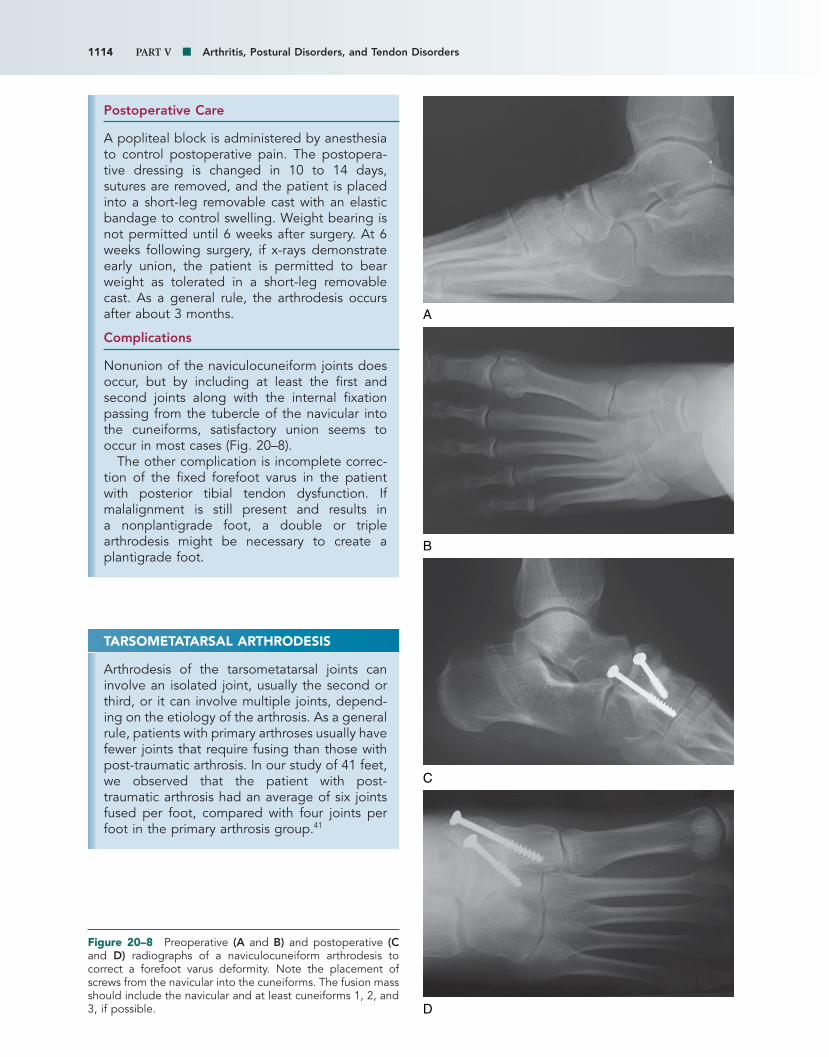
1114 PART V Arthritis, Postural Disorders, and Tendon Disorders
Postoperative Care
A popliteal block is administered by anesthesiato control postoperative pain. The postopera-tive dressing is changed in 10 to 14 days,sutures are removed, and the patient is placedinto a short-leg removable cast with an elasticbandage to control swelling. Weight bearing isnot permitted until 6 weeks after surgery. At 6weeks following surgery, if x-rays demonstrateearly union, the patient is permitted to bearweight as tolerated in a short-leg removablecast. As a general rule, the arthrodesis occursafter about 3 months.
Complications
Nonunion of the naviculocuneiform joints doesoccur, but by including at least the first andsecond joints along with the internal fixationpassing from the tubercle of the navicular intothe cuneiforms, satisfactory union seems tooccur in most cases (Fig. 20–8).
The other complication is incomplete correc-tion of the fixed forefoot varus in the patientwith posterior tibial tendon dysfunction. Ifmalalignment is still present and results in a nonplantigrade foot, a double or triplearthrodesis might be necessary to create aplantigrade foot.
A
D
B
C
Figure 20–8 Preoperative (A and B) and postoperative (Cand D) radiographs of a naviculocuneiform arthrodesis tocorrect a forefoot varus deformity. Note the placement ofscrews from the navicular into the cuneiforms. The fusion massshould include the navicular and at least cuneiforms 1, 2, and3, if possible.
TARSOMETATARSAL ARTHRODESIS
Arthrodesis of the tarsometatarsal joints caninvolve an isolated joint, usually the second orthird, or it can involve multiple joints, depend-ing on the etiology of the arthrosis. As a generalrule, patients with primary arthroses usually havefewer joints that require fusing than those withpost-traumatic arthrosis. In our study of 41 feet,we observed that the patient with post-traumatic arthrosis had an average of six jointsfused per foot, compared with four joints perfoot in the primary arthrosis group.41

CHAPTER 20 Arthrodesis of the Foot and Ankle 1115
The extent of the deformity is also variable.This depends on the number of joints involvedand whether the deformity results from primaryor traumatic arthrosis. The patient with primaryarthrosis tends to have more pronation and agreater degree of deformity. Usually, if a singlejoint is involved, particularly the second or third,little or no deformity is present and thereforeonly an in situ fusion is necessary. If a deformityis present, however, realignment of the foot isessential to obtain a satisfactory result.
Determining the extent of the fusion site issometimes difficult, particularly if it appears asthough only one joint is involved. Besides acareful physical examination and radiographicstudies consisting of weight-bearing radi-ographs, a computed tomography (CT) scanand bone scan may be useful in determining theextent of the arthrosis and which joints shouldbe included in the fusion mass. Even aftercareful physical and radiographic evaluation, ifany doubt exists regarding the presence ofarthrosis, the joint should be examined atsurgery to be sure that arthritis is not being overlooked. Arthrosis may be seen at surgerywhen, even in retrospect, the radiographappears to be normal. This is particularly true forthe medial naviculocuneiform joint and the thirdmetatarsocuneiform (MTC) joint. Although themost obvious arthrosis usually is present at thetarsometatarsal or intertarsal joints, the navicu-locuneiform joints must always be carefullyevaluated, particularly in the patient aftertrauma. If the naviculocuneiform joint doesappear to be involved, at least the two medialjoints should always be included in the fusionmass and, if necessary, the third. It is difficult toobtain an isolated fusion between the medialcuneiform and the navicular.
The question is often raised about whetherthe fourth and fifth metatarsocuboid articula-tions should be included in the fusion site or if they should undergo isolated fusion. As ageneral rule, the fourth and fifth metatar-socuboid articulations seem to be somewhatmore forgiving and tend to be less symptomaticthan the medial three MTC joints, despite thearthrosis. The reason may be that more flexibil-ity exists in the two lateral rays than in themedial three rays, which are more rigid. Motionalso occurs between the third cuneiform andcuboid, which results in more motion of the twolateral rays of the foot. If clinical examination
and radiographs show arthrosis at the fourth andfifth metatarsocuboid joints and a fusion is indi-cated, however, the cuboid should not be fusedto the lateral cuneiform so that some mobilitycan be maintained between the medial andlateral aspects of the longitudinal arch. Notfusing the cuboid to the lateral cuneiformappears to give the foot a little more flexibilityto adapt to the ground.
Indications
The main indication for arthrodesis of the tar-sometatarsal joints is arthrosis resulting in pain,deformity, or both. The arthrodesis can includea single joint or multiple joints.
Position of Arthrodesis
The arthrodesis site is positioned to correct anyforefoot abduction or adduction or dorsiflexion.At times a complex deformity from trauma, par-ticularly a crush injury, results in a deformityinvolving multiple planes, and it can be difficultto achieve a plantigrade foot. However, thesurgeon should attempt to obtain a foot as closeto plantigrade as possible.
Surgical Technique
1. The patient is placed in a supine position,and a tourniquet is used about the thigh(video clip 13).
2. The surgical approach varies, depending onwhich joints are being arthrodesed. For anisolated first tarsometatarsal arthrodesis, adorsomedial incision is used, centered overthe joint. This allows satisfactory visualiza-tion of the joint as well as access to thedorsum of the foot to insert screws for inter-nal fixation.
3. For an isolated second MTC arthrodesis, theincision is made just lateral to the midpor-tion of the joint. By placing the incisionhere, the neurovascular bundle is locatedmedial to the incision. Subperiosteal dis-section can safely mobilize and retract theneurovascular bundle medially.
4. The approach to the first, second, and thirdtarsometatarsal joints is carried out throughtwo longitudinal incisions. The first is cen-tered over the dorsomedial aspect of thefirst tarsometatarsal joint or possibly slightlytoward the midline, compared with the iso-lated fusion. The second incision is made
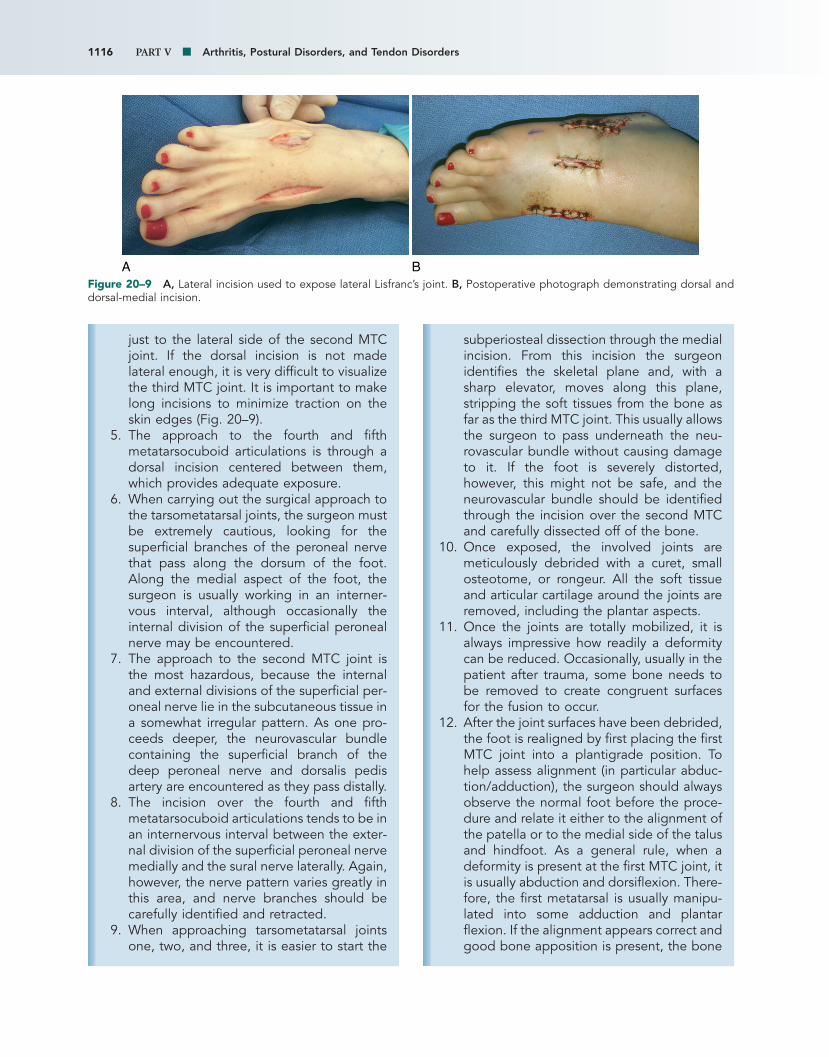
1116 PART V Arthritis, Postural Disorders, and Tendon Disorders
BAFigure 20–9 A, Lateral incision used to expose lateral Lisfranc’s joint. B, Postoperative photograph demonstrating dorsal anddorsal-medial incision.
just to the lateral side of the second MTCjoint. If the dorsal incision is not madelateral enough, it is very difficult to visualizethe third MTC joint. It is important to makelong incisions to minimize traction on theskin edges (Fig. 20–9).
5. The approach to the fourth and fifthmetatarsocuboid articulations is through adorsal incision centered between them,which provides adequate exposure.
6. When carrying out the surgical approach tothe tarsometatarsal joints, the surgeon mustbe extremely cautious, looking for thesuperficial branches of the peroneal nervethat pass along the dorsum of the foot.Along the medial aspect of the foot, thesurgeon is usually working in an interner-vous interval, although occasionally theinternal division of the superficial peronealnerve may be encountered.
7. The approach to the second MTC joint isthe most hazardous, because the internaland external divisions of the superficial per-oneal nerve lie in the subcutaneous tissue ina somewhat irregular pattern. As one pro-ceeds deeper, the neurovascular bundlecontaining the superficial branch of thedeep peroneal nerve and dorsalis pedisartery are encountered as they pass distally.
8. The incision over the fourth and fifthmetatarsocuboid articulations tends to be inan internervous interval between the exter-nal division of the superficial peroneal nervemedially and the sural nerve laterally. Again,however, the nerve pattern varies greatly inthis area, and nerve branches should becarefully identified and retracted.
9. When approaching tarsometatarsal jointsone, two, and three, it is easier to start the
subperiosteal dissection through the medialincision. From this incision the surgeonidentifies the skeletal plane and, with asharp elevator, moves along this plane,stripping the soft tissues from the bone asfar as the third MTC joint. This usually allowsthe surgeon to pass underneath the neu-rovascular bundle without causing damageto it. If the foot is severely distorted,however, this might not be safe, and theneurovascular bundle should be identifiedthrough the incision over the second MTCand carefully dissected off of the bone.
10. Once exposed, the involved joints aremeticulously debrided with a curet, smallosteotome, or rongeur. All the soft tissueand articular cartilage around the joints areremoved, including the plantar aspects.
11. Once the joints are totally mobilized, it isalways impressive how readily a deformitycan be reduced. Occasionally, usually in thepatient after trauma, some bone needs tobe removed to create congruent surfacesfor the fusion to occur.
12. After the joint surfaces have been debrided,the foot is realigned by first placing the firstMTC joint into a plantigrade position. Tohelp assess alignment (in particular abduc-tion/adduction), the surgeon should alwaysobserve the normal foot before the proce-dure and relate it either to the alignment ofthe patella or to the medial side of the talusand hindfoot. As a general rule, when adeformity is present at the first MTC joint, itis usually abduction and dorsiflexion. There-fore, the first metatarsal is usually manipu-lated into some adduction and plantarflexion. If the alignment appears correct andgood bone apposition is present, the bone
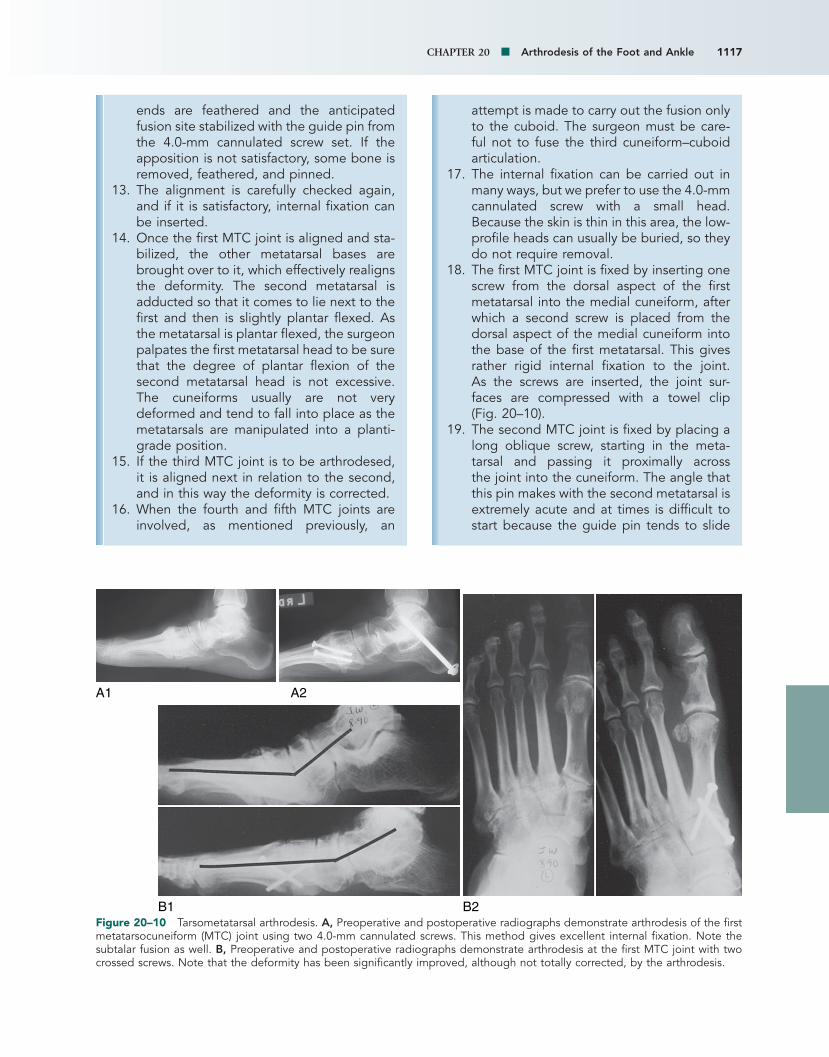
CHAPTER 20 Arthrodesis of the Foot and Ankle 1117
ends are feathered and the anticipatedfusion site stabilized with the guide pin fromthe 4.0-mm cannulated screw set. If theapposition is not satisfactory, some bone isremoved, feathered, and pinned.
13. The alignment is carefully checked again,and if it is satisfactory, internal fixation canbe inserted.
14. Once the first MTC joint is aligned and sta-bilized, the other metatarsal bases arebrought over to it, which effectively realignsthe deformity. The second metatarsal isadducted so that it comes to lie next to thefirst and then is slightly plantar flexed. Asthe metatarsal is plantar flexed, the surgeonpalpates the first metatarsal head to be surethat the degree of plantar flexion of thesecond metatarsal head is not excessive.The cuneiforms usually are not verydeformed and tend to fall into place as themetatarsals are manipulated into a planti-grade position.
15. If the third MTC joint is to be arthrodesed,it is aligned next in relation to the second,and in this way the deformity is corrected.
16. When the fourth and fifth MTC joints areinvolved, as mentioned previously, an
B1 B2
A2A1
Figure 20–10 Tarsometatarsal arthrodesis. A, Preoperative and postoperative radiographs demonstrate arthrodesis of the firstmetatarsocuneiform (MTC) joint using two 4.0-mm cannulated screws. This method gives excellent internal fixation. Note thesubtalar fusion as well. B, Preoperative and postoperative radiographs demonstrate arthrodesis at the first MTC joint with twocrossed screws. Note that the deformity has been significantly improved, although not totally corrected, by the arthrodesis.
attempt is made to carry out the fusion onlyto the cuboid. The surgeon must be care-ful not to fuse the third cuneiform–cuboidarticulation.
17. The internal fixation can be carried out inmany ways, but we prefer to use the 4.0-mmcannulated screw with a small head.Because the skin is thin in this area, the low-profile heads can usually be buried, so theydo not require removal.
18. The first MTC joint is fixed by inserting onescrew from the dorsal aspect of the firstmetatarsal into the medial cuneiform, afterwhich a second screw is placed from thedorsal aspect of the medial cuneiform intothe base of the first metatarsal. This givesrather rigid internal fixation to the joint. As the screws are inserted, the joint sur-faces are compressed with a towel clip (Fig. 20–10).
19. The second MTC joint is fixed by placing along oblique screw, starting in the meta-tarsal and passing it proximally across the joint into the cuneiform. The angle thatthis pin makes with the second metatarsal isextremely acute and at times is difficult tostart because the guide pin tends to slide
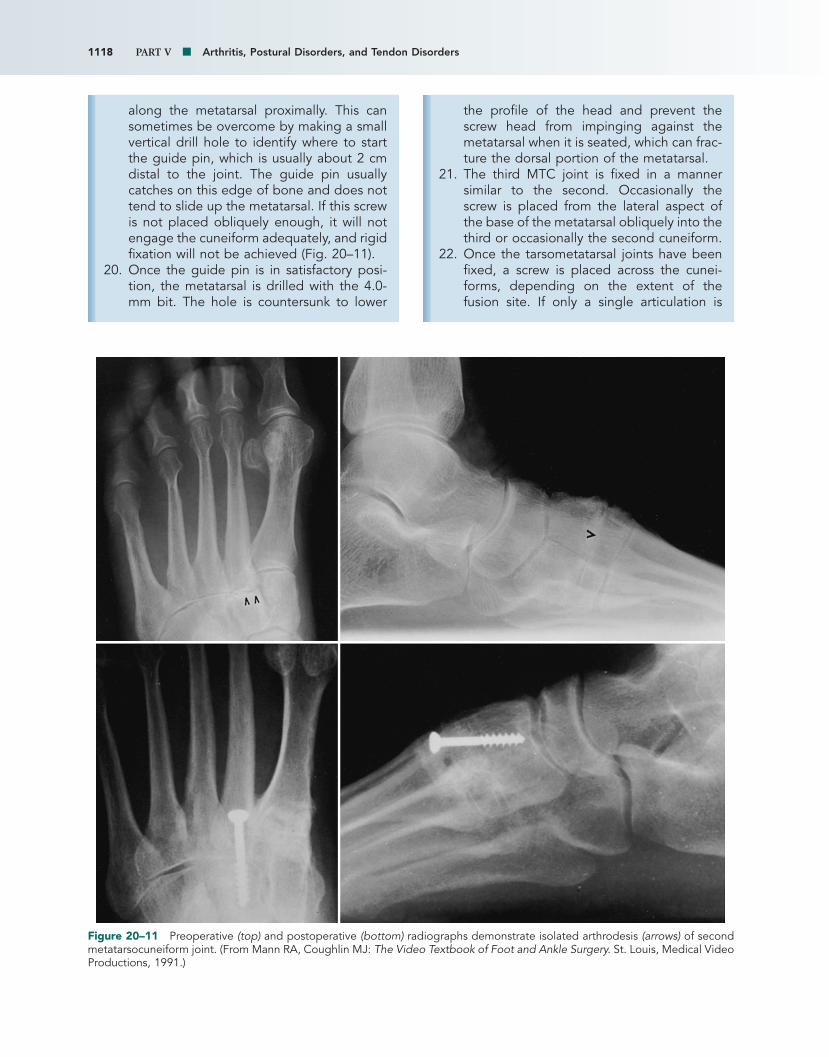
1118 PART V Arthritis, Postural Disorders, and Tendon Disorders
Figure 20–11 Preoperative (top) and postoperative (bottom) radiographs demonstrate isolated arthrodesis (arrows) of secondmetatarsocuneiform joint. (From Mann RA, Coughlin MJ: The Video Textbook of Foot and Ankle Surgery. St. Louis, Medical VideoProductions, 1991.)
along the metatarsal proximally. This cansometimes be overcome by making a smallvertical drill hole to identify where to startthe guide pin, which is usually about 2 cmdistal to the joint. The guide pin usuallycatches on this edge of bone and does nottend to slide up the metatarsal. If this screwis not placed obliquely enough, it will notengage the cuneiform adequately, and rigidfixation will not be achieved (Fig. 20–11).
20. Once the guide pin is in satisfactory posi-tion, the metatarsal is drilled with the 4.0-mm bit. The hole is countersunk to lower
the profile of the head and prevent thescrew head from impinging against themetatarsal when it is seated, which can frac-ture the dorsal portion of the metatarsal.
21. The third MTC joint is fixed in a mannersimilar to the second. Occasionally thescrew is placed from the lateral aspect ofthe base of the metatarsal obliquely into thethird or occasionally the second cuneiform.
22. Once the tarsometatarsal joints have beenfixed, a screw is placed across the cunei-forms, depending on the extent of thefusion site. If only a single articulation is

CHAPTER 20 Arthrodesis of the Foot and Ankle 1119
AFigure 20–12 Midfoot arthrodesis of multiple joints. A, Preoperative and postoperative radiographs of intertarsal arthrodesisfor degenerative arthrosis. Note that the screw pattern locks navicular to the cuneiforms; also note the intercuneiform screws. Ifthe tarsometatarsal joints are not involved, the arthrodesis does not need to include them. Continued
being fused, it is not necessary to fuse thecuneiforms to one another. If the first,second, and third MTC joints are beingfused, however, a screw is placed mediolat-erally across the cuneiforms to stabilizethem. Another screw is then placed from themedial aspect of the first metatarsal baseobliquely into the cuneiforms. This screwmay also cross the second MTC joint. Thisscrew helps to reinforce the fusion mass andensure that rigid fixation is achieved.
23. When the naviculocuneiform joints areincluded in the fusion mass, a screw can bepassed from the tip of the navicular into thecuneiforms, which usually provides excel-lent internal fixation. If the naviculocun-eiform joints are to be included in the fusionsite, it is imperative that at least the first and
second cuneiforms be involved because anisolated fusion of the medial cuneiform andthe navicular is difficult to achieve. Screwscan also be placed from the cuneiforms intothe navicular (Fig. 20–12).
24. Fixation of the metatarsocuboid joint isusually achieved by placing a screw from thedorsal aspect of the fourth metatarsal intothe cuboid. The fixation of the fifth metatar-socuboid joint is more difficult because theactual articulating surface is quite small. Anoblique guide pin may be placed percuta-neously from the lateral aspect of themetatarsal base into the cuboid and a screwinserted over it.
25. Proliferative bone over the dorsal aspect ofthe MTC joints is removed, morselized, andpacked into any existing spaces in the

1120 PART V Arthritis, Postural Disorders, and Tendon Disorders
B1
D1
B2
D2
C1
C2
E1
E2Figure 20–12—cont’d B and C, Preoperative (1) and postoperative (2) radiographs demonstrate arthrodesis of tarsometatarsaljoints 1, 2, and 3, along with cuneiforms using a four-screw pattern. Note the correction of deformity in both the anteroposte-rior and lateral planes. D and E, Preoperative (1) and postoperative (2) radiographs demonstrate arthrodesis of tarsometatarsaljoints 1, 2, and 3, along with intercuneiform joints using a six-screw pattern. The number of screws used depends on the sta-bility of fixation needed to obtain rigid fixation. Note the correction of deformity in both the anteroposterior and lateral planes.

CHAPTER 20 Arthrodesis of the Foot and Ankle 1121
fusion site. If the surgeon is not satisfiedwith the apposition of the bone surfaces, abone graft, generally from the calcaneus ormedial malleolus, can be used.
26. The skin closure is very important in thesecases. The skin is very fragile, and whenmultiple joints are arthrodesed, moderateswelling can occur.
27. The subcutaneous tissue is closed with 3-0plain sutures and the skin with a runninglongitudinal near-far/far-near suture, whichkeeps tension off the skin edges.
Postoperative Care
At the conclusion of the procedure, 0.25% bupi-vacaine is placed into the surgical field toprovide initial postoperative pain relief. A compression dressing consisting of fluffs and aheavy cotton bandage incorporating two plastersplints is applied. In the recovery room, apopliteal block is placed to control the initialpostoperative pain.
The patient is kept non–weight bearing in thepostoperative cast for approximately 12 to 14days, after which the cast is removed and thepatient placed into a short-leg removable castwith an elastic bandage to control swelling. Thepatient is keep non–weight bearing for 6 weeks.At 6 weeks radiographs are obtained, and ifearly union is occurring, weight bearing is per-mitted in the cast for another 6 weeks. Twelveweeks after surgery, radiographs are againobtained, and if satisfactory union has occurred,the patient is gradually permitted to work out ofthe removable cast and into a shoe. An elasticstocking is used to control swelling.
Complications
The three main complications that can occurafter a tarsometatarsal arthrodesis are skinslough, nonunion, and failure to correct amalalignment.
The skin on the dorsum of the foot often haslittle subcutaneous fat. Combined with postop-erative swelling and multiple incisions, this canlead to a skin slough. Therefore, meticulous caremust be taken at surgery to obtain a good sub-cutaneous closure followed by a skin closure,with a minimum amount of tension along theskin edge. I prefer a running, horizontal mattresssuture that keeps the tension off the skin edgesas much as possible. If a slough occurs, local
wound care usually is adequate to resolve theproblem, but sometimes a skin graft or even aflap is necessary. If the slough is not too large,vacuum-assisted wound closure (wound-VAC)maybe useful.
A nonunion of an attempted fusion site canoccur, although infrequently. With meticulouspreparation of the bone surfaces and rigid inter-nal fixation, the tarsometatarsal joints have ahigh fusion rate. We were able to obtain a fusionin 176 of 179 joints for a 98% fusion rate.41 If anonunion occurs and is symptomatic, the fibroustissue around the involved joint needs to beexcised, the bone surfaces once again scaled,the joint bone grafted if necessary, and internalfixation reapplied.
Malalignment of the foot can be a problem.The deformity usually present preoperatively isabduction and dorsiflexion, which results in alarge prominence on the plantar–medial aspectof the foot in the area of the first tarsometatarsaljoint. If the forefoot is not reduced by bringingthe first metatarsal into adduction and plantarflexion, this prominence remains and might con-tinue to be a source of pain for the patient. Withadequate reduction, this prominence does notstrike the ground, which usually provides relieffor the patient. Occasionally, malalignment of ametatarsal occurs by placing it into too muchdorsiflexion or plantar flexion, which can be cor-rected with an osteotomy and internal fixation ifnecessary.
A neuroma, particularly on the dorsum of thefoot, can also occur from entrapment or lacera-tion of one of the sensory nerves on the dorsum.Usually a small branch is involved, and althoughannoying to the patient, it usually is not a majorproblem. Occasionally, if one of the largerbranches of a superficial peroneal nerve is cut,a large, painful neuroma develops and is aggra-vated by footwear. If this occurs and is sympto-matic, the neuroma should be identified andburied either underneath the extensor digito-rum brevis muscle or into a hole in the bone.The dorsum of the foot being so devoid of fattytissue in some patients sometimes makes it dif-ficult to bury the nerve’s cut end adequately.
Author’s Experience
We reviewed a series of 40 patients (41 feet)who underwent surgery, with a follow-up of 6years (range, 2 to 17).41 The diagnoses wereprimary arthrosis in 21 patients (18 women, 3

1122 PART V Arthritis, Postural Disorders, and Tendon Disorders
REFERENCES
Subtalar Arthrodesis
1. Angus PD, Cowell HR: Triple arthrodesis: A long-term review. JBone Joint Surg Br 68:260-265, 1986.
2. Bennett GL, Graham CE, Mauldin DM: Triple arthrodesis inadults. Foot Ankle 12(3):138-143, 1991.
3. Graves SC, Mann RA, Graves KO: Triple arthrodesis in olderadults. J Bone Joint Surg Am 75:355-362, 1993.
4. Haritidis JH, Kirkos JM, Provellegios SM, Zachos AD: Long-termresults of triple arthrodesis: 42 cases followed for 25 years. FootAnkle 15(10):548-551, 1994.
5. Kitaoka HB, Alexander IJ, Adelaar RS, et al: Clinical ratingsystems for the ankle–hindfoot, midfoot, hallux and lesser toes.Foot Ankle 15(7):349-353, 1994.
6. Haskell A, Pfeiff C, Mann R: Subtalar joint arthrodesis using asingle lag screw. Foot Ankle Int 25:774-777, 2004.
7. Mann RA, Baumgarten M: Subtalar fusion for isolated subtalardisorders: Preliminary report. Clin Orthop Relat Res 226:260-265, 1988.
8. Mann RA, Beaman DN, Horton G: Isolated subtalar arthrode-sis. Foot Ankle Int 19(8):511-519, 1998.
9. Russotti GM, Cass JR, Johnson KA: Isolated talocalcanealarthrodesis: A technique using moldable bone graft. J Bone JointSurg Am 70:1472-1478, 1988.
10. Sangeorzan BJ, Smith D, Veith R, Hansen ST: Triple arthrodesisusing internal fixation in treatment of adult foot disorders. ClinOrthop Relat Res 294:299-307, 1993.
11. Southwell RB, Sherman FC: Triple arthrodesis: A long-term study with force plate analysis. Foot Ankle 2(1):15-24,1981.
12. Stephens HM, Sanders R: Calcaneal malunions: Results of aprognostic computed tomography classification system. FootAnkle Int 7(7):395-401, 1996.
13. Swiontkowski MF, Scranton PE, Hansen S: Tarsal coalitions:Long-term results of surgical treatment. J Pediatr Orthop 3:287-292, 1983.
14. Tenuta J, Shelton YA, Miller F: Longer-term follow-up of triplearthrodesis in patients with cerebral palsy. J Pediatr Orthop13:713-716, 1993.
15. Wetmore RS, Drennan JC: Long-term results of triple arthrode-sis in Charcot–Marie–Tooth disease. J Bone Joint Surg Am 71:417-422, 1989.
men) and 22 feet, post-trauma effects in 17 (9women, 8 men), and inflammatory arthritis intwo (one man, one woman). The age for theprimary arthrosis group was 60 years (range, 27to 75), for post-trauma group 40 years (range,30 to 67), and for arthritis group 44 and 70years. The patients noted symptoms for anaverage 2.8 years for the post-trauma group,10.9 years for the primary arthrosis group, and14 years for the arthritis group.
Preoperatively, all the patients complained ofpain, and 78% had a foot deformity that madewearing shoes difficult. The group with primaryarthrosis had a greater degree of deformity thanthe patients with traumatic arthrosis.
Using the technique described previously, wewere able to obtain union in 176 of 179 jointsfor a 98% union rate. Of the three nonunionsthat occurred, one required surgical repair.Patient satisfaction was 93% (38 of 41 feet).Postoperatively, five patients had a prominentmetatarsal head, although none developed acallus that required trimming. The prominenthead involved the second metatarsal twice,second and third metatarsals twice, and first andsecond metatarsals once. Three patients devel-oped a stress fracture of the second metatarsal,and all of them healed spontaneously. Threefeet demonstrated minimal neuritic symptomsalong one of the dorsal scars, but none requiredfurther treatment.
The preoperative radiographic findings demon-strated that the patients with primary arthrosishad more pronation than those with traumaticarthrosis. The deformity observed in the APradiograph was usually two times greater than that noted on the lateral radiograph. Theaverage correction obtained in the AP plane(i.e., abduction or adduction) was 9 degrees,which compares favorably to that of Horton andOlney,39 who obtained a 10-degree correction.In the lateral radiograph we obtained anaverage correction of 8 degrees, which wasapproximately half that reported by Horton andOlney. At follow-up, arthrosis not present pre-operatively was observed in adjacent joints inthree patients (five joints) in the post-traumagroup and eight patients (12 joints) in theprimary arthrosis group. None of these weresymptomatic.
Our failure rate of the procedure was 3 (7%)of 41, which was lower than that reported bySangeorzan et al,42 whose failure rate was 5
(31%) of 16, and Johnson et al,40 whose rate was2 (15%) of 13.
The primary differences between patientswith primary arthrosis and post-trauma arthrosiswere age (60 versus 41 years, respectively) andthe extent of the deformity, which was greaterin the primary arthrosis patients. These patientshad an average of six joints fused per foot,whereas the post-trauma patients had four jointsper foot.
After surgery, one patient continued to use anAFO, and 11 used some type of an orthoticdevice (e.g., Hapad, Spenco liner) in their shoe.No patient required custom-made footwear.

CHAPTER 20 Arthrodesis of the Foot and Ankle 1123
16. Wukich OK, Bowen RJ: A long-term study of triple arthrodesisfor correction of pes cavovarus in Charcot–Marie–Tooth disease.J Pediatr Orthop 9:433-437, 1989.
Talonavicular Arthrodesis
17. Clain MR, Baxter DE: Simultaneous calcaneal–cuboid andtalonavicular fusion: Long-term follow-up study. J Bone JointSurg Br 76:133-136, 1994.
18. Elbaor JE, Thomas WH, Weinfeld NS, Potter TA: Talonaviculararthrodesis for rheumatoid arthritis of the hindfoot. Orthop ClinNorth Am 7:821-826, 1976.
19. Elftman H: The transverse tarsal joint and its control. ClinOrthop Relat Res 16:41, 1960.
20. Fogel GR, Kato HY, Rand JA, Chao EY: Talonavicular arthrode-sis for isolated arthrosis: 9.5 year results and gait analysis. FootAnkle 3(2):105-113, 1982.
21. Harper MC, Tisdel CL: Talonavicular arthrodesis for the painfulacquired flatfoot. Foot Ankle Int 17(11):658-661, 1996.
22. O’Malley MJ, Deland JT, Lee K: Selective hindfoot arthrodesisfor the treatment of adult acquired flatfoot deformity: An invitro study. Foot Ankle Int 16(7):411-417, 1995.
Double Arthrodesis
23. DuVries HL: Surgery of the Foot. St Louis, Mosby, 1959, p 300.24. Inman VT (ed): DuVries’ Surgery of the Foot, ed 3. St Louis,
Mosby, 1973, pp 491-494.25. Mann RA, Beaman DN: Double arthrodesis for posterior tibial
tendon dysfunction. Clin Orthop Relat Res 365:74-80, 1999.
Triple Arthrodesis
26. Adelaar RS, Dannelly EA, Meunier PA, et al: A long-term studyin triple arthrodesis in children. Orthop Clin North Am 7:895-908, 1976.
27. Angus PD, Cowell HR: Triple arthrodesis: A critical long-termreview. J Bone Joint Surg Br 62:260-265, 1986.
28. Bennett GL, Graham CE, Mauldin DM: Triple arthrodesis inadults. Foot Ankle 12(3):138-143, 1991.
29. Drew AJ: The late results of arthrodesis of the foot. J Bone JointSurg Br 33:496-502, 1951.
30. Graves SC, Mann RA, Graves KO: Triple arthrodesis in olderadults: Results after long-term follow-up. J Bone Joint Surg Am75:355-362, 1993.
31. Haritdis JH, Kirkos JM, Provellegios SM, Zachos AD: Long-termresult of triple arthrodesis: Forty-two cases followed for twenty-five years. Foot Ankle Int 15(10):548-551, 1994.
32. Jahss MH, Godsick PA, Levin H: Quadruple arthrodesis withiliac bone graft. In Bateman JE, Trott AW (eds): The Foot andAnkle, New York, Thieme-Stratton, 1980, pp 93-102.
33. Lambrinudi C: New operation on drop-foot. Br J Surg 15:193-200, 1927.
34. Mann RA, Mann JA, Prieskorn D, Sobel M: Posterior tibialtendon dysfunction treated by fusion. Paper presented at the 18th Annual Verne T. Inman Lectureship, University of California, San Francisco, May, 1997.
35. Ryerson EW: Arthrodesing operations on the feet. J Bone JointSurg 5:453-471, 1923.
36. Smith RW, Shen W, DeWitt S, Reischl SF: Triple arthrodesis inadults with non-paralytic disease. J Bone Joint Surg Am 86:2707-2713, 2004.
37. Southwell RB, Sherman FC: Triple arthrodesis; a long-termstudy with force plate analysis. Foot Ankle 2(1):15-24, 1981.
37. Wetmore RS, Drennan JC: Long-term results of triple arthrode-sis in Charcot–Marie–Tooth disease. J Bone Joint Surg Am 71:417-422, 1989.
Tarsometatarsal Arthrodesis
39. Horton GA, Olney BW: Deformity correction and arthrodesis ofthe midfoot with a medial plate. Foot Ankle 14:493-499, 1993.
40. Johnson JE, Johnson KA: Dowel arthrodesis for degenerativearthritis of the tarsometatarsal (Lisfranc) joints. Foot Ankle6(5):243-253, 1986.
41. Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometa-tarsal arthrodeses for primary degenerative osteoarthrosis orosteoarthrosis after trauma. J Bone Joint Surg Am 78:1376-1385,1996.
42. Sangeorzan BJ, Veith RG, Hansen ST Jr: Salvage of Lisfranc’s tar-sometatarsal joint by arthrodesis. Foot Ankle 10(3):193-200,1990.