article factors that influence the provision of good ...clok.uclan.ac.uk/19717/1/19717.pdf ·...
TRANSCRIPT
Article
Factors that influence the provision of goodquality routine antenatal services: a qualitative evidence synthesis of the views and experiences of maternity care providers [Protocol]
Downe, Soo, Finlayson, Kenneth William, Tunçalp, Özge and Gülmezoglu, A Metin
Available at http://clok.uclan.ac.uk/19717/
Downe, Soo, Finlayson, Kenneth William, Tunçalp, Özge and Gülmezoglu, A Metin (2017) Factors that influence the provision of goodquality routine antenatal services: a qualitative evidence synthesis of the views and experiences of maternity care providers [Protocol]. Cochrane Database of Systematic Reviews .
It is advisable to refer to the publisher’s version if you intend to cite from the work.http://dx.doi.org/10.1002/14651858.cd012752
For more information about UCLan’s research in this area go to http://www.uclan.ac.uk/researchgroups/ and search for <name of research Group>.
For information about Research generally at UCLan please go to http://www.uclan.ac.uk/research/
All outputs in CLoK are protected by Intellectual Property Rights law, includingCopyright law. Copyright, IPR and Moral Rights for the works on this site are retained by the individual authors and/or other copyright owners. Terms and conditions for use of this material are defined in the http://clok.uclan.ac.uk/policies/
CLoKCentral Lancashire online Knowledgewww.clok.uclan.ac.uk
Cochrane Database of Systematic Reviews
Factors that influence the provision of good-quality routine
antenatal services: a qualitative evidence synthesis of the
views and experiences of maternity care providers (Protocol)
Downe S, Finlayson K, Tunçalp Ö, Gülmezoglu AM
Downe S, Finlayson K, Tunçalp Ö, Gülmezoglu AM.
Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and experiences
of maternity care providers.
Cochrane Database of Systematic Reviews 2017, Issue 8. Art. No.: CD012752.
DOI: 10.1002/14651858.CD012752.
www.cochranelibrary.com
Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iFactors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Qualitative Protocol]
Factors that influence the provision of good-quality routineantenatal services: a qualitative evidence synthesis of theviews and experiences of maternity care providers
Soo Downe1 , Kenneth Finlayson1 , Özge Tunçalp2 , A Metin Gülmezoglu2
1Research in Childbirth and Health (ReaCH) unit, University ofCentral Lancashire, Preston, UK. 2UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development andResearch Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization,Geneva, Switzerland
Contact address: Soo Downe, Research in Childbirth and Health (ReaCH) unit, University of Central Lancashire, Preston, PR1 2HE,UK. [email protected].
Editorial group: Cochrane Effective Practice and Organisation of Care Group.Publication status and date: New, published in Issue 8, 2017.
Citation: Downe S, Finlayson K, Tunçalp Ö, Gülmezoglu AM. Factors that influence the provision of good-quality routine antenatalservices: a qualitative evidence synthesis of the views and experiences of maternity care providers. Cochrane Database of SystematicReviews 2017, Issue 8. Art. No.: CD012752. DOI: 10.1002/14651858.CD012752.
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
This is a protocol for a Cochrane Review (Qualitative). The objectives are as follows:
- To identify the factors influencing the provision of quality ANC according to health care providers
- To explore how these factors relate to, and help to explain the findings of, the related Cochrane intervention reviews
B A C K G R O U N D
There has been widespread and continuing concern about ratesof maternal and neonatal deaths and serious morbidity across theworld (UN 2015). Antenatal care (ANC) offers the promise ofscreening women and their fetuses for actual and potential prob-lems as the pregnancy progresses, and for treating any complica-tions that arise. Antenatal care is therefore a core component ofmaternity care provision in most contexts around the world. Themain measures for the adequacy of ANC provision are the timeof the first visit and the number of antenatal sessions attended(WHO 2002). Current World Health Organization (WHO) rec-ommendations for routine ANC for women with no existing orhistorical health problems are a four-session programme during
pregnancy, starting before 16 weeks gestation, with specific inter-ventions and activities at each visit (WHO 2002). This is termedFocused Antenatal Care (FANC). The number of visits and thecontent of each visit are based on the WHO Antenatal Care Trialpublished in 2001 (Villar 2001).
Although the percentage of women who attend ANC early inpregnancy and who go on to attend at least three more sessions isrising, it is still very low in some countries, particularly in Sub-Sa-haran Africa (Hogan 2010). Evidence suggests that when servicesare provided in central locations and transportation is infrequent,expensive or non-existent, this is a clear barrier to attendance, es-pecially in cultures where women do not have the autonomy to de-cide to attend and/or to pay for transportation (Campbell 2006).
1Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

However, more recent data suggest that, even when services aremore accessible and affordable, women do not always use them,especially if they are members of marginalised population groups(Downe 2009; Finlayson 2013). This observation holds true inboth high- and low-income settings. These studies also note thatthe biomedical assumptions supporting formal ANC might notfulfil the needs of all pregnant women, especially in cultures wherea more psychosocial approach is culturally normative. A recentreview of what women want and need during pregnancy revealsthat antenatal care needs to provide social support and tailoredinformation as well as monitoring well-being and providing inter-ventions and therapies where these are required (Downe 2016).This review informed a framework for future ANC provision com-prising three equally important domains, each provided by prac-titioners with good clinical and interpersonal skills within a high-quality health system: clinical practices (interventions and tests),relevant and timely information, and psychosocial and emotionalsupport. The recent, revised WHO ANC guidelines for a positivepregnancy experience highlight the importance of the provider,shifting the terminology from ANC ’visit’ to ’contact’ to reflectthe significance of the relationship between woman and provider(WHO 2016). The growing recognition of the degree to whichwomen are subject to disrespect and abuse by caregivers in formalmaternity care systems also provides an insight as to why womenmay not attend ANC, or why they may attend just once (Bohren2015; White Ribbon Alliance 2011).
Alongside the narratives of pregnant and postnatal women, quali-tative data is emerging from maternity service providers suggestingthat in some settings, staff are also exposed to disrespect and abuse(Bowser 2010), from vertical or horizontal bullying in the work-place (Khalil 2009), or from threats of physical or sexual assaultduring their commute (Wilson 2016). Studies have documentedthese experiences in countries of all income brackets. More pro-saically, staff may face barriers to providing good-quality antena-tal care (or any antenatal care at all) because of a lack of essen-tial resources, equipment and drugs (Matsuoka 2010). This limitsstaff capacity to ensure that facilities are attractive and clean, andthat they can provide an adequate response to both routine needsand emergencies (Sharma 2015). Beyond this, provision of carein rural locations is limited by understaffing when professionalswho might be interested in working in these locations are put offfrom doing so by lack of good-quality housing or schooling fortheir children (Lehmann 2008). In high-income countries, too,staff and resource shortages influence the provision of quality an-tenatal care (RCM 2015), but even when resources are sufficient,problems may arise due to the increasingly technical content ofcare and especially the extent to which this hinders positive inter-personal interaction between healthcare providers and pregnantwomen and their companions (Nyman 2013). These issues canhave a negative influence on staff morale and a subsequent impacton the quality of care provided (Smith 2009).
The same psychosocial factors identified as important by womenattending ANC also appear to affect staff morale and job satisfac-tion. Maternal health professionals cite the opportunity to developauthentic, woman-centred relationships as an integral componentof quality ANC (Carolan 2007; Everett-Murphy 2010). Alterna-tive models of care delivery, such as midwife-led care (incorporat-ing continuity of care) or group-based approaches (e.g. CenteringPregnancy; Manant 2011) may be more conducive to the type ofrelationship-based care that women and staff desire. In terms ofclinical outcomes, a Cochrane Review comparing different mod-els of maternity care supports this view, reporting that midwife-led models of care produced better maternal and infant outcomescompared to other models of antenatal care (Sandall 2016). Whilethe combination of clinical surveillance and woman-centred con-tinuity of care appears to be associated with positive outcomes andmutual satisfaction, it is still not clear how this approach can beadopted and/or adapted in different contexts, particularly in low-income settings where resources may be scarce.
Qualitative research is the ideal vehicle for answering questionsof acceptability and for exploring subjective factors that mightframe delivery of ANC programmes. Data arising from qualitativestudies can indicate how staff can be encouraged and supportedto design and provide better-quality ANC that is more effective,acceptable and accessible. Qualitative data can inform individualstudies and reviews of effectiveness by suggesting outcomes that arerelevant to staff, by generating hypotheses that can be tested out infuture subgroup analyses, and by providing possible explanationsfor results of individual studies and reviews. In addition, thesemethods can inform guidelines by answering questions around theacceptability and feasibility of implementing different aspects ofANC in policy and practice.
By synthesising the findings from relevant qualitative studies us-ing meta-ethnographic techniques (Noblitt 1988), and by utilis-ing a pre-determined framework approach (based on the theoryof reasoned behaviour; Fishbein 2010), we may identify a widerange of potential factors relating to health system, behavioural,sociocultural and political dimensions.
This review is designed to provide insights to further developguidelines and care provision in the future, serving as a comple-ment to the existing Cochrane Reviews of ANC provision (Catling2015; Dowswell 2015).
Description of the topic
Antenatal care has been defined as the routine care that all healthywomen can expect to receive during their pregnancy (NICE 2008).Globally, there is wide variation in the number and content ofroutine ANC sessions provided, including a greater or lesser degreeof technical monitoring and testing (Dowswell 2015). Generally,the central purpose is prophylactic, through the monitoring and
2Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

support of whole populations of pregnant women and of theirbabies to maximise the health and well-being of the majority andto identify, treat and/or refer the minority who develop actual orpotential complications as the pregnancy progresses.There is little theoretical research that is directly focused on theviews and experiences of healthcare provision, though there is awide spectrum of research on components like knowledge, under-standing of and beliefs about benefits, and design features, suchas the AAAQ (available, accessible, acceptable, appropriate and ofgood quality) model (Potts 2008). The review team jointly chosethe Reasoned Action Approach (RAA) as the theoretical underpin-ning for the review (Fishbein 2010), as it is widely used in health-care behavioural research and appeared, a priori, to have a goodpotential explanatory power for the phenomenon of interest. Inaccordance with recent guidance on choosing theories for use insystematic reviews (Noyes 2016), we made this decision only afterexploring a number of other theories, including organisational the-ories such as Donabedian’s Structure and Process Outcome Theory(or derivatives) and Webers Theory of Bureaucracy (Donabedian2003; Weber 1964), as well as motivational behavioural theoriessuch as the Health Belief Model (Strecher 1997). However, fromour professional and research knowledge of the field, we believedthat the relevant factors for healthcare professionals in general andfor antenatal care in particular (across settings and cultures) wouldprobably combine both structural/organisational/resource issuesas well as human motivation and behaviour. We therefore selectedthe RAA theory, as it amends the original purely behavioural model
of the theory of planned behaviour/reasoned action, adding inbackground factors including individual, social and informationalvariables. Logic models based on this theory should include in-put factors relating to attitudes, subjective norms and behaviouralcontrol. These input factors are hypothesised to lead to the outputof intended behaviour. In the right context, intended behavioursthen result in actual behaviours. The RAA further states that theinput factors are, themselves, preceded by three psychosocial do-mains relating to behavioural, normative and control beliefs. Basedon this, we hypothesise that the degree to which staff actually pro-vide good-quality ANC services is mediated by their intentions(or lack thereof ) to do so. These intentions are themselves mod-erated by pre-existing attitudes and beliefs about the capacity toprovide services, which are in turn mediated by local social normsaround the philosophy and ideal content of ANC and the degreeof control that staff have over enacting those beliefs and norms,for example, through autonomy in practice and easy access to theresources needed to carry out their duties. Figure 1 presents theproposed logic model based on the RAA. We will initially examinethe studies included in the review to establish emerging themesand determine their fit with the initial theoretical logic model. Wewill then construct amended logic model(s) to take account of allthe findings, as a basis for informing future quantitative reviews,practice guidelines, and implementation in policy and practice. Arelated review will look at the views of pregnant women in termsof factors influencing their uptake of antenatal care.
Figure 1. Theory of Reasoned Action
3Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Description of the phenomenon of interest
The phenomena of interest for this review are the factors thatinfluence the provision of high-quality antenatal care from theperspective of healthcare providers.
Why is it important to do this review?
Given the low levels of uptake of ANC in some countries andamong some population groups, it is important to determine howANC can be rendered more acceptable and accessible so that itcan fulfill its promise of benefiting women and babies. A recentqualitative review of what matters to women in the context ofANC highlights effective interventions, supportive relationships,and technically competent and caring staff as integral componentsof the service (Downe 2015). Service providers play a key role inimplementing and delivering ANC and are likely to offer valuableinsights into their ability to deliver a high-quality service that isacceptable and accessible to women.
The beneficiaries of this review will be the staff providing ANCand the women (and their offspring) using it, provided that pol-icy makers, funders and health workers use the findings alongsidethe existing quantitative Cochrane Reviews to design, fund andprovide ANC that is better aligned with health providers’ needsand expectations. The review will complement an existing reviewlooking at the factors associated with the delivery of intra-partumand postpartum care from the perspective of skilled birth atten-dants (Munabi-Babigumira 2015), plus existing qualitative andquantitative reviews related to the uptake and delivery of ANC, asdescribed in Table 1.
O B J E C T I V E S
- To identify the factors influencing the provision of quality ANCaccording to health care providers
- To explore how these factors relate to, and help to explain thefindings of, the related Cochrane intervention reviews
M E T H O D S
Criteria for considering studies for this review
Types of studies
This is a systematic review of qualitative primary studies. Accord-ing to Merriam, “qualitative researchers are interested in under-standing the meaning people have constructed, that is, how peoplemake sense of their world and the experiences they have in theworld”. (Merriam 2009). To achieve this, the review will include
studies using qualitative designs and approaches, such as ethnog-raphy, phenomenology, case studies, grounded theory, observa-tional studies and mixed methods. These studies will use appro-priate methods of data collection for the methodology employed,including interviews, focus groups, open-ended survey questions,diaries and other narrative data collection methods. We will ex-clude studies that collect data using qualitative methods but donot perform a qualitative analysis (for example, where qualitativedata are only reported using descriptive statistics). We will includemixed methods studies where it is possible to extract findings de-rived from qualitative research. We will include studies regardlessof whether they have been carried out alongside studies of effec-tiveness of ANC, so long as they are of an appropriate standard ac-cording to our chosen quality appraisal tool (Downe 2007; Walsh2006).
Types of participants
We will include studies that report the views and experiences ofstaff based in primary, secondary and tertiary care settings, who areemployed by public, private or charity funders to provide routineantenatal care services. Our definition of clinical staff includesskilled birth attendants who fulfil the WHO 2004 definition of askilled birth attendant, i.e. an “accredited health professional suchas a midwife, doctor or nurse that is trained to proficiency andhas the necessary skills to manage a normal pregnancy, childbirthand provide postnatal care as well as the skills to detect, manageand refer any complications in the mother and neonate” (WHO2004).We will also include any studies that collect data from managersof healthcare facilities and other providers who may work withskilled birth attendants as part of the team at a facility. Theseproviders work closely with skilled birth attendants and may haveviews and experiences of factors that influence the provision ofantenatal care.We will include studies among auxiliary cadres such as auxiliarynurse midwives and associate clinicians (non-physician clinicians)if these staff are employed at the health facility, work independentlyor as part of a team, and are recognised within that setting as skilledbirth attendants. Although auxiliary cadres do not currently meetthe international definition of skilled birth attendants, we willinclude them in this review, for settings where they are recognisedas skilled providers of care. We will include studies that documentstudent nurses’ or midwives’ attitudes and experiences withoutusing hypothetical scenarios only if the students are participantsalongside skilled birth attendants and we cannot distinguish theirviews from those of other participants. We will exclude studies inwhich only students participate, as we are concerned with factorsaffecting the delivery of care in routine settings rather than inteaching settings.In some instances, we may not be able to tell if health providersfit our definition of skilled birth attendants. In these instances, we
4Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

will contact the authors of the study for more information andinclude these studies as long as the health providers are recognisedas skilled birth attendants in that particular setting.We will also include lay health workers where they are paid directlyor indirectly to provide ANC.We will exclude studies that focus exclusively on trained or un-trained traditional birth attendants, as they lie outside the defini-tion of skilled birth attendants and do not tend to provide ’rou-tine’ ANC in health facilities. We will not include staff who arecommenting on their experiences and views of delivering or pro-viding specialist antenatal services for women/babies with specificconditions (such as HIV, malaria, or in -utero interventions formalformation), as this review is designed to complement reviewsof routine antenatal care for healthy women and babies. In addi-tion, we will not include papers if they only report on what serviceproviders think about the views and experiences of women receiv-ing ANC. We are interested in provider perceptions of routineANC from their own perspective rather than their views on whatwomen may or may not think about the service.
Setting
The review will include any setting where routine ANC is provided(e.g. outpatient/antenatal clinics or antenatal wards in hospitals,birth centres, local health centres, community centres, children’scentres, and/or the woman’s home or other local venue).
Types of interventions
We will include studies about routine antenatal care provision forhealthy women and babies. We define antenatal care as routinecare provided for healthy women during their pregnancy. We willinclude studies exploring the views and experiences of any or allof the following components of ANC.
• Content of care: consultations, tests, treatments,information, advice, and support related to maintaining andmonitoring a healthy pregnancy and helping women to preparefor birth and parenting, where these are provided as part ofpublicly or privately funded, formal ANC provision for thewoman/fetus without complications.
• How care is provided: including the perceived attitudes andbehaviours of staff as well as the biomedical, psychosocial,relational and other approaches to care provision.
The review will not include:• ANC programmes/interventions designed for women and
babies with specific complications; or• programmes/interventions that are only about antenatal
education (for childbirth and/or for parenting). Theseprogrammes do not include clinical care, tests, and treatments,and they are not usually provided routinely to whole populationsof women.
Phenomena of interest
The phenomena of interest for this review, therefore, are the factorsinfluencing the delivery of good-quality routine antenatal care,based on the views and experiences of healthcare providers.
Search methods for the identification of studies
Electronic searches
We will search PDQ-Evidence (www.pdq-evidence.org) for relatedreviews in order to identify eligible studies for inclusion, as well asthe following electronic databases.
• MEDLINE - OvidSP• Embase - OvidSP• CINAHL Complete - EbscoHost• PsycINFO - EbscoHost• AMED - EbscoHost• LILACS - Virtual Health Library• AJOL (African Journals Online)• Social Science Citation Index - EbscoHost
We chose these databases based on exploratory searches and weanticipate that they will provide the highest yieldof results. We will use text word searches utilizing title, abstractand keyword functions and will include index terms relating tohealth personnel and qualitative research. Where possible we willalso include database specific limiters to identify qualitativeresearch utilizing the ‘best balance of sensitivity and specificity’function. An example of a MEDLINE search strategy isshown in Appendix 1.We will include eligible studies published between 1 January 2000and the date the search is run. This date range is intended tocapture provider views and experiences of care provision since theintroduction of focused antenatal care programmes.We will not impose any language or geographic restrictions.
Searching other sources
We will handsearch the reference lists of included papers and per-form forward citation tracking to identify additional referencesthat may be relevant. We will then subject these papers to the sameinclusion/exclusion and quality-checking criteria as those identi-fied from the search terms above.We will check the contents pages of over 50 relevant journals asthey are issued through Zetoc alerts, over the period the review isundertaken. We want to ensure that we pick up any studies thatare published as the review is progressing to ensure we capture asmuch of the data as possible.We will not include Conference abstracts or PhD and Masterstheses.
5Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data collection and analysis
Selection of studies
Assessing abstracts and full text according to the inclusion
criteria
We will collate records identified from different sources into onedatabase and remove duplicates. Two members of the team (SD,KF) will independently assess each abstract to determine eligibilityagainst the inclusion criteria. The authors will then retrieve andindependently assess the full text of all the abstracts that have beenassessed as potentially relevant and then agree on the final list ofincluded studies. In the event of continuing lack of agreementfor a particular study, a third team member (OT) will adjudicate.Where appropriate, we will contact the study authors for furtherinformation.
Translation of non-English language papers
For papers in a language other than those understood by the reviewauthors (English, French, Spanish, Portuguese, Turkish), we willinitially have the abstract translated through open source software(Google Translate). If this indicates inclusion, or if the translationis inadequate to make a decision, we will ask members of themultilingual networks associated with the research teams of thereview authors to translate the full text. If we cannot do this for astudy in a particular language, we will list the study as ’awaitingclassification’, to ensure transparency in the review process.Conceptual translation between languages and cultures is a recog-nised issue in both qualitative and quantitative research (Al Amer2015; Stevelink 2013). Regmi 2010 discuss the issues of transla-tion (a direct and literal word-for-word process) and transliteration(a process of translating meaning that may not be word for word)in undertaking qualitative research in different language and cul-tural groups. They use the term ’elegant free translation’ (Birbili2000), which is an approach that, in Birbilis analysis, can help thereader to ’know what is going on’ even if it is less faithful to theoriginal text. Regmi 2010 see this as a process involving transcrip-tion of only the key themes or few quotes along with a descriptionof the context (via a kind of transliteration). They recognise thatthis process risks the loss of some precision and meaning but seeit is a pragmatic solution to the complexity and resource demandsof full translation in primary qualitative research.Given that the current review did not aim to be philosophicallyphenomenological, and that the key aims are about the relativelybroad concept of influencing factors, we have taken the prag-matic decision to use the ’elegant free translation’ approach tothe transliteration of our included studies, rather than translatingthem word for word. We will apply this approach both at the stageof decisions about inclusion, and for data extraction and analysis.
Potential sampling from the included studies
Large numbers of studies can threaten the quality of the analysisin qualitative evidence syntheses. In addition, syntheses of quali-tative studies aim for greater variation in concepts as opposed toan exhaustive sample that aims to avoid bias. To allow for thebroadest possible variation within the included studies, if morethan 30 studies are included following our search, we will considerusing maximum variation purposive sampling to select from theeligible studies (Benoot 2016). Key areas of variation that we mayconsider will include the cadre of healthcare worker, the type ofANC provision and the geographical setting. Once these variableshave been determined, we will create a sampling frame and mapall eligible studies onto the frame. We will then review the numberof studies in each frame and reach a decision regarding how manystudies in each cell we will include in the review.
Recording of study characteristics
We will record study characteristics using a form designed specifi-cally for this review. The study characteristics form will record de-tails of first author, date of publication, language, country of study,context (urban/rural), participant group (parity, sociodemograph-ics), type of ANC received (caregiver group, location, focused an-tenatal care (FANC) or other), theoretical/conceptual perspectiveof the study, research methods, sample size, method of analysis,and key themes (as recorded by the authors in each case).
Assessing quality and risk of bias of included studies
Our inclusion criteria specify that to be included a study must haveused qualitative methods for both data collection and data analysis.This criterion constitutes a basic quality threshold, and we willdiscard studies that do not meet this standard. In addition, to assessthe methodological quality of included studies, one author willapply a quality appraisal framework to each study. A second authorwill check for discrepancies. We will resolve disagreements throughdiscussion or by consulting a third reviewer. We will use the A-D grading of Downe and colleagues and the criteria of Walsh andDowne (Downe 2007; Walsh 2006). This includes an assessmentof the study scope and purpose, design, sampling strategy, analysis,interpretation, researcher reflexivity, ethical dimensions, relevanceand transferability; a number of other qualitative reviews haveused this approach successfully (e.g. Downe 2009; Finlayson 2013;Downe 2015). We will then grade studies against Lincoln andGuba’s summary criteria, as follows (Lincoln 1985).A. No, or few flaws. The study credibility, transferability, depend-ability and confirmability is high.B: Some flaws, unlikely to affect the credibility, transferability,dependability and/or confirmability of the study.C: Some flaws that may affect the credibility, transferability, de-pendability and/or confirmability of the study.D: Significant flaws that are very likely to affect the credibility,transferability, dependability and/or confirmability of the study.
6Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

We will analyse studies with a grading of C or more. We will liststudies that we grade as less than C, but we will not include themin the central analysis. As apparent from the summary criteriagiven above, grading a study as D in our taxonomy means that it isjudged to have ’significant flaws which are very likely to affect thecredibility, transferability, dependability, and/or confirmability ofthe study.’ We acknowledge that some qualitative researchers be-lieve that all qualitative data have potential value in understand-ing phenomenon of interest, but we have argued consistently thatincluding poor-quality studies in systematic reviews risks a misun-derstanding of the final phenomenon, which has potentially im-portant consequences if the findings are to be used in a practiceor policy context (Walsh 2006). However, given the global natureof the review we may be more lenient towards studies conductedin settings that would otherwise be under-represented in the finalanalysis (e.g. if there were relatively few studies from Africa) toensure the review incorporates provider experiences from as widea range of settings as possible. This is a similar approach to thatadopted by Glenton and colleagues in their review of lay healthworker programmes (Glenton 2013)
Data extraction and analysis
Following the principles of meta-ethnography (Noblitt 1988),data extraction and analysis will take place simultaneously for eachincluded study in turn. We will extract author-identified themesfrom the primary papers and log them onto an Excel spreadsheet.We will code the themes and use them to generate second-or-der concepts, recorded on the next page of the spreadsheet. Wewill examine emerging concepts for similarities and, where ap-propriate, collapse them into new themes (recorded on the finalpage of the spreadsheet). These final themes will form the basisfor the synthesis. Meta-ethnography uses an approach based onconstant comparative analysis, where the analysis is built up studyby study. The process requires the researcher to be open to theemergence of new themes, ensuring that unexpected phenomenacan be captured and examined by subjecting the initial assump-tions about what is in the data to both confirmation (’reciprocalanalysis’) and disconfirmation (’refutational analysis’) against eachstudy in turn. This ensures that the product of the review is con-tinually refined as each study is included. Using the principles offramework analysis (Gale 2013), this process will not start froma position of no knowledge but will be used to test and, wherenecessary, amend the original theoretically informed logic model(the ’framework’) given in Figure 1. This incorporates elementsof the ’best fit’ framework synthesis approach where ’new’ themesemerging from the synthesised data will be added to the a prioriconcepts in the framework as they arise (Carroll 2013).We will then use these findings to ratify and/or amend the com-ponents of the logic model iteratively. Two reviewers will under-take the analysis and resolve any disagreements on the thematic
structure/theory/amendments to the logic model by consensusthroughout the extraction and analysis process.Framework analysis is used when there are some existing theoriesabout what might be in the data. In the case of the current re-view, we had already determined that we were looking for factorsinfluencing the provision of quality antenatal care by healthcareproviders within the more general data on their views and experi-ences, and that the theory of reasoned behaviour might offer goodexplanatory power for the findings (as expressed in the logic modelgiven in Figure 1). In summary, our approach will incorporate thefollowing steps,
1. Choose the a priori theory for likely utility (the reasonedaction approach).
2. Undertake a meta-synthesis of the included papers.3. Map the metasynthesis themes and line-of-argument to the
a priori theory.4. Amend the a priori theory where necessary to ensure all the
data are accounted for.5. Draw up logic models (based on the line of argument) to
assess the fit of the new theory for the total data set and forsubgroups in the data set.
Planned subanalysis
Providing there is sufficient data to work with we also plan to per-form a subanalysis according to income levels in the study settingby comparing studies conducted in high income countries (HICs)against studies conducted in low- and middle-income countries(LMICs). We believe that differences in resource levels (equip-ment, staff and infrastructure) may affect the provision of good-quality antenatal care.
Reflexive note
In keeping with quality standards for rigour in qualitative research,the review authors considered their views and opinions on antena-tal care as possible influences on the decisions made in the designand conduct of the study, and, in turn, on how the emerging re-sults of the study influenced those views and opinions. SD believedat the outset that staff motivation for providing maternity carein general, and antenatal care in particular, varied from completevocational commitment to a simple need to earn enough incometo pay for everyday costs of living. She also believed that manystaff working in this area are highly committed to providing good-quality care, but that, for others, gender, power, and hierarchy is-sues, together with resourcing problems, have resulted in lack ofmotivation and burn-out for some staff working in this area, witha consequent lack of concern for the well-being of women andbabies using ANC. KF believed that staff were generally drawnto maternity care because of a desire to provide a comprehensivearray of clinical expertise, hands-on care and emotional and psy-chological support to pregnant women and babies.
7Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

We will therefore use refutational analytic techniques to minimisethe risk that these pre-suppositions would skew the analysis andthe interpretation of the findings.Given the rapidly evolving nature of this area of research, we willalso note our reflections on some of the methodological and the-oretical issues that arise during the course of this review.
Appraisal of the confidence in the review findings
We will use the GRADE-CERQual tool (Confidence in the Ev-idence from Reviews of Qualitative research) to assess the confi-dence that the review findings merit (Lewin 2015). The GRADECERQual Project Group developed this approach in 2004, whichuses the following four concepts to assess confidence.
1. Methodological limitations: the extent to which there areproblems in the design or conduct of the primary studies thatcontributed evidence to a review finding.
2. Relevance: the extent to which the body of evidence fromthe primary studies supporting a review finding is applicable tothe context (perspective or population, phenomenon of interest,setting) specified in the review question.
3. Coherence: the extent to which the review findings are wellgrounded in data from the contributing primary studies andprovide a convincing explanation for the patterns found in thesedata.
4. Adequacy: an overall determination of the degree of richnessand quantity of data supporting a review finding.The above assessments will result in an overall assessment of ourconfidence in each individual review finding as either high, mod-erate, low or very low. We will conclude the appraisal of confidencein each review finding by drafting a table that will summarise thekey findings, level of confidence in each, and an explanation forour assessment of each finding.
Line of argument synthesis and final logic models
We will then synthesise the final thematic structure into a ’line ofargument’ synthesis. This is a phrase or statement that summarisesthe main findings of the study and the theoretical insights thatthey generate. A line of argument synthesis includes logical con-nections between concepts, and it will therefore reflect the finallogic model(s) that are constructed from the data. In the case of thecurrent review we will use the line of argument and the resultinglogic model(s) to explain what might underpin the ability of staff
to provide quality antenatal care, in terms of social, behaviouraland control beliefs, and organisational or contextual componentsthat interact with these factors to prevent the delivery of qualityantenatal care. These could be used to interpret the findings of ex-isting quantitative reviews in this field; to explain how and why theoutcomes identified in the accompanying ANC guideline ’work’,for who and in what context; and to identify areas for future ef-fectiveness research in this field. The models will also demonstratethe extent to which the RAA explains these factors on the basis ofthe data included in the review.
Using the synthesised qualitative findings to
supplement the Cochrane intervention reviews
As part of data synthesis, we plan to explore how the findings fromour review relate to and help explain the findings of the relatedCochrane intervention reviews (see Table 1). We will also look tocompare and contrast the findings from our review with those froma related review exploring healthcare professionals’ views on the de-livery of intrapartum and postpartum care (Munabi-Babigumira2015). The findings will also be used to inform panel judgementson the acceptability and value of proposed components and inter-ventions for new WHO ANC guidelines. In this review, we willbuild on the emerging experience of others in the field by usinga narrative approach to explore how the reviews relate, and howthe findings from the qualitative review inform the findings fromthe intervention reviews and vice versa. At least two reviewers willwork together to map our review findings in relation to the inter-vention reviews and to the ANC guideline development process.
A C K N O W L E D G E M E N T S
Claire Glenton and Simon Lewin of the Oslo satellite of theCochrane Effective Practice and Organisation of Care Group pro-vided guidance in developing the protocol.
The peer referees, Andrew Booth, Meghan Bohren and BrianMcKinstry, provided valuable input to improve the protocol.
The Norwegian Satellite of the Effective Practice and Organisa-tion of Care (EPOC) Group receives funding from the NorwegianAgency for Development Co-operation (Norad), via the Norwe-gian Institute of Public Health, to support review authors in theproduction of their reviews.
8Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
Additional references
Al Amer 2015
Al-Amer R, Ramjan L, Glew P, Darwish M, SalamonsonY. Translation of interviews from a source language to atarget language: examining issues in cross-cultural healthcare research. Journal of Clinical Nursing 2015;24(9-10):1151–62.
Benoot 2016
Benoot C, Hannes K, Bilsen J. The use of purposefulsampling in a QES. A worked example on sexual adjustmentto a cancer trajectory. BMC Medical Research Methodology
2016;16(21):1–12.
Birbili 2000
Birbili, M. Translating from one language to another. SocialResearch Update 2000;31:1–7.
Bohren 2015
Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK,Souza JP, et al. The mistreatment of women duringchildbirth in health facilities globally: a mixed-methodssystematic review. PLOS Medicine 2015;12(6):1–32.[e1001847. doi:10.1371/journal.pmed.1001847]
Bowser 2010
Bowser D, Hill K. Exploring evidence for disrespect andabuse in facility-based childbirth. www.tractionproject.org/sites/default/files/Respectful˙Care˙at˙Birth˙9-20-101˙Final.pdf (accessed 15 November 2015).
Campbell 2006
Campbell O, Graham W. Strategies for reducing maternalmortality: getting on with what works. Lancet 2006;368
(9543):1284–99.
Carolan 2007
Carolan M, Cassar L. Pregnancy care for African refugeewomen in Australia: attendance at antenatal appointments.Evidence Based Midwifery 2007;5(2):54–8.
Carroll 2013
Carroll C, Booth A, Leaviss J, Rick J. “Best fit”framework synthesis: refining the method. BMC Medical
Research Methodology 2013;13(1):1–16. [DOI: 10.1186/1471-2288-13-37.]
Catling 2015
Catling CJ, Medley N, Foureur M, Ryan C, Leap N, TeateA, Homer CS. Group versus conventional antenatal carefor women. Cochrane Database of Systematic Reviews 2015,Issue 2. [DOI: 10.1002/14651858.CD007622.pub3]
Donabedian 2003
Donabedian A. An Introduction to Quality Assurance in
Health Care. New York: Oxford University Press, 2003.
Downe 2007
Downe S, Simpson L, Trafford K. Expert intrapartummaternity care: a meta-synthesis. Journal of Advanced
Nursing 2007;57(2):127–40.
Downe 2009
Downe S, Finlayson K, Walsh D, Lavender T. ’Weighing upand balancing out’: a meta-synthesis of barriers to antenatalcare for marginalized women in high-income countries.British Journal of Obstetrics and Gynaecology 2009;16:518–29.
Downe 2015
Downe S, Finlayson K, Tuncalp , Metin GulmezogluA. What matters to women: a systematic scoping reviewto identify the processes and outcomes of antenatal careprovision that are important to healthy pregnant women.British Journal of Obstetrics and Gynaecology 2015;123:529–39. [DOI: 10.1111/1471–0528.13819]
Dowswell 2015
Dowswell T, Carroli G, Duley L, Gates S, Gülmezoglu AM,Khan-Neelofur D, Piaggio G. Alternative versus standardpackages of antenatal care for low-risk pregnancy. CochraneDatabase of Systematic Reviews 2015, Issue 7. [DOI:10.1002/14651858.CD000934.pub3]
Everett-Murphy 2010
Everett-Murphy K, Paijmans J, Steyn K, Matthews K,Emmelin M, Peterson Z. Scolders, carers or friends: SouthAfrican midwives’ contrasting styles of communicationwhen discussing smoking cessation with pregnant women.Midwifery 2011;27:517–24.
Finlayson 2013
Finlayson K, Downe S. Why do women not use antenatalservices in low- and middle-income countries? A meta-synthesis of qualitative studies. PLOS 2013;10(1):e1001373. [DOI: 10.1371/journal.pmed.1001373]
Gale 2013
Gale NK, Heath G, Cameron E, Rashid S, Redwood S.Using the framework method for the analysis of qualitativedata in multi-disciplinary health research. BMC MedicalResearch Methodology 2013;13:117.
Glenton 2013
Glenton C, Colvin C, Carlsen B, Swartz A, Lewin S, Noyes J,Rashidian A. Barriers and facilitators to the implementationof lay health worker programmes to improve access tomaternal and child health: qualitative evidence synthesis.Cochrane Database of Systematic Reviews 2013, Issue 10.[DOI: 10.1002/14651858.CD010414.pub2]
Hogan 2010
Hogan MC, Foreman KJ, Naghavi M, Ahn SY, WangM, et al. Maternal mortality for 181 countries, 1980-2008: a systematic analysis of progress towards MillenniumDevelopment Goal 5. Lancet 2010;375:1609–23.
Khalil 2009
Khalil D. Levels of violence among nurses in Cape Townpublic hospitals. Nursing Forum 2009;44(3):207–17. [doi:10.1111/j.1744–6198.2009.00144.x]
9Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lehmann 2008
Lehman U, Dielman M, Martineau T. Staffing remote ruralareas in middle- and low-income countries: a literaturereview of attraction and retention. BMC Health ServicesResearch 2008;8:19. [DOI: 10.1186/1472–6963–8–19]
Lewin 2015
Lewin S, Glenton C, Munthe-Kaas H, Carlsen B, ColvinCJ, Gülmezoglu M, et al. Using qualitative evidence indecision making for health and social interventions: anapproach to assess confidence in findings from qualitativeevidence syntheses (GRADE-CERQual). PLOS Medicine
2015;12(10):e1001895. [e1001895. doi:10.1371/journal.pmed.1001895]
Lincoln 1985
Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park,CA: Sage, 1985.
Matsuoka 2010
Matsuoka S, Aiga H, Rasmey LC, Rathavy T, Okitsu A.Perceived barriers to utilization of maternal health servicesin rural Cambodia. Health Policy 2010;95:255–63.
Merriam 2009
Merriam S. Qualitative Research: A Guide to Design and
Implementation. San Francisco, CA: Jossey-Bass, 2009.
Munabi-Babigumira 2015
Munabi-Babigumira S, Glenton C, Lewin S, FretheimA, Nabudere H. Factors that influence the provision ofintrapartum and postnatal care by skilled birth attendantsin low- and middle-income countries: a qualitative evidencesynthesis. Cochrane Database of Systematic Reviews 2015,Issue 2. [DOI: 10.1002/14651858.CD011558]
NICE 2008
National Institute for Health and Care Excellence.Antenatal care for uncomplicated pregnancies, 2008.www.nice.org.uk/guidance/CG62 (Accessed 15 November2015).
Noblitt 1988
Noblitt GW, Hare RD. Meta-Ethnography: SynthesizingQualitative Studies. Newbury Park, CA: Sage, 1988.
Noyes 2016
Noyes J, Hendry M, Chandler J, Lewin S, Glenton C,Garside R. Current use was established and Cochraneguidance on selection of social theories for systematicreviews of complex interventions was developed. Journal of
Clinical Epidemiology 2016;75:78–92. [DOI: 10.1016/j.jclinepi.2015.12.009]
Nyman 2013
Nyman V, Bondas T, Downe S, Berg M. Glancing beyondor being confined to routines: labour ward midwives’responses to change as a result of action research. Midwifery2013;29(6):573–8. [DOI: 10.1016/j.midw.2013.02.010]
Phillippi 2009
Phillippi JC. Women’s perceptions of access to prenatalcare in the United States: a literature review. Journal of
Midwifery & Womens Health 2009;54(3):219–25. [doi:10.1016/j.jmwh.2009.01.002]
RCM 2015
Royal College of Midwives. State of Maternity ServicesReport 2015. www.rcm.org.uk/sites/default/files/RCM%20State%20of%20Maternity%20Services%20Report%202015.pdf(accessed 15 November 2015).
Regmi 2010
Regmi K, Naidoo J Pilkington P. Understanding theprocesses of translation and transliteration in qualitativeresearch. International Journal of Qualitative Methods 2010;9(1):ejournals.library.ualberta.ca/index.php/IJQM/article/viewFile/6829/6473 (accessed 15 November 2015).
Sandall 2016
Sandall J, Soltani H, Gates S, Shennan A, Devane D.Midwife-led continuity models versus other modelsof care for childbearing women. Cochrane Database
of Systematic Reviews 2016, Issue 4. [DOI: 10.1002/14651858.CD004667.pub5]
Sharma 2015
Sharma G, Mathai M, Dickson KE, Weeks A, HofmeyrGJ, Lavender T, et al. Quality care during labour andbirth: a multicountry analysis of health system bottlenecksand potential solutions. BMC Pregnancy and Childbirth2015;15(Suppl 2):1–19. [http://www.biomedcentral.com/1471–2393/15/S2/S2]
Smith 2009
Smith AH, Dixon AL, Page L. Health care professionals’views about safety in maternity services. Midwifery 2009;25
(1):21–31.
Stevelink 2013
Stevelink SA, van Brakel WH. The cross-culturalequivalence of participation instruments: a systematicreview. Disability and Rehabilitation 2013;35(15):1256–68.
Strecher 1997
Strecher VJ, Rosenstock IM. The health belief model. In:Glanz K, Lewis FM, Rimer BK editor(s). Health Behaviorand Health Education: Theory, Research and Practice. 2ndEdition. San Francisco CA: Jossey-Bass Inc, 1997:41–59.
UN 2015
United Nations. Millennium Development Goals Report2015. www.un.org/millenniumgoals/2015˙MDG˙Report/pdf/MDG%202015%20rev%20(July%201).pdf (accessed15 November 2015).
Villar 2001
Villar J, Ba’aqeel H, Piaggio G, Lumbiganon P, Belizán JM,Farnot U, et al. WHO antenatal care randomised trial forthe evaluation of a new model of routine antenatal care.Lancet 2001;357:1551–64.
Walsh 2006
Walsh D, Downe S. Appraising the quality of qualitativeresearch. Midwifery 2006;22(2):108–19.
Weber 1964
Weber M. Theory of Social and Economic Organization.New York: The Free Press, 1964. [Edited and translated byTalcott Parsons]
10Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
White Ribbon Alliance 2011
The White Ribbon Alliance. Respectful maternitycare: the universal rights of childbearing women.whiteribbonalliance.org/wp-content/uploads/2013/10/Final˙RMC˙Charter.pdf (accessed 15 November 2015).
WHO 2002
WHO. WHO Antenatal Care Randomized Trial: Manual forthe Implementation of the New Model. Geneva: World HealthOrganization, 2002. [can–mnch.ca/french/wp–content/uploads/2013/11/WHO–Antenatal–Care–Randomized–Care–Trial–Manual–for–the–Implementation–of–the–
New–Model.pdf ]
WHO 2016
WHO. WHO Recommendations on Antenatal Care fora Positive Pregnancy Experience. Geneva: World HealthOrganization, 2016. [apps.who.int/iris/bitstream/10665/250796/1/9789241549912–eng.pdf?ua=1]
Wilson 2016
Wilson JL. An exploration of bullying behaviours innursing: a review of the literature. British Journal of Nursing2016;25(6):303–6. [DOI: 10.12968/bjon.2016.25.6.303.]
∗ Indicates the major publication for the study
A D D I T I O N A L T A B L E S
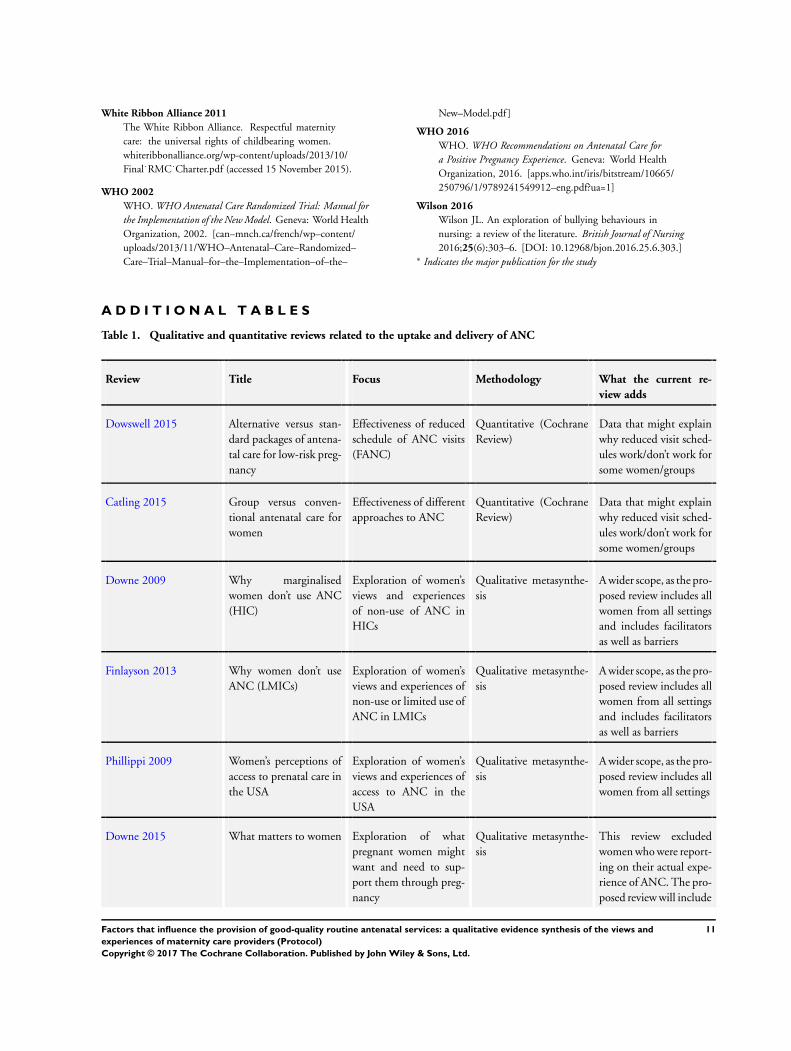
Table 1. Qualitative and quantitative reviews related to the uptake and delivery of ANC
Review Title Focus Methodology What the current re-
view adds
Dowswell 2015 Alternative versus stan-dard packages of antena-tal care for low-risk preg-nancy
Effectiveness of reducedschedule of ANC visits(FANC)
Quantitative (CochraneReview)
Data that might explainwhy reduced visit sched-ules work/don’t work forsome women/groups
Catling 2015 Group versus conven-tional antenatal care forwomen
Effectiveness of differentapproaches to ANC
Quantitative (CochraneReview)
Data that might explainwhy reduced visit sched-ules work/don’t work forsome women/groups
Downe 2009 Why marginalisedwomen don’t use ANC(HIC)
Exploration of women’sviews and experiencesof non-use of ANC inHICs
Qualitative metasynthe-sis
A wider scope, as the pro-posed review includes allwomen from all settingsand includes facilitatorsas well as barriers
Finlayson 2013 Why women don’t useANC (LMICs)
Exploration of women’sviews and experiences ofnon-use or limited use ofANC in LMICs
Qualitative metasynthe-sis
A wider scope, as the pro-posed review includes allwomen from all settingsand includes facilitatorsas well as barriers
Phillippi 2009 Women’s perceptions ofaccess to prenatal care inthe USA
Exploration of women’sviews and experiences ofaccess to ANC in theUSA
Qualitative metasynthe-sis
A wider scope, as the pro-posed review includes allwomen from all settings
Downe 2015 What matters to women Exploration of whatpregnant women mightwant and need to sup-port them through preg-nancy
Qualitative metasynthe-sis
This review excludedwomen who were report-ing on their actual expe-rience of ANC. The pro-posed review will include
11Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Qualitative and quantitative reviews related to the uptake and delivery of ANC (Continued)
these accounts
Munabi-Babigumira2015
Fac-tors that influence theprovision of intrapartumand postnatal care byskilled birth attendantsin low- and middle-in-come countries: a quali-tative evidence synthesis
Exploration of the at-titudes, views, experi-ences and behaviours ofskilled birth attendantsand those who supportthem, to identify fac-tors that influence thedelivery of intrapartumand postnatal care inlow- and middle-incomecountries
Qualitative evidencesynthesis
Data that might iden-tify the barriers and fa-cilitators associated withthe delivery of intra-partum and postpartumcare from the perspectiveof healthcare providers
A P P E N D I C E S
Appendix 1. MEDLINE search strategy
# Searches Results
1 Prenatal Care/ or Perinatal Care/ or Maternal Health Services/or Maternal-Child Health Services/
37806
2 (antenatal care or antenatal service? or antenatal support or pre-natal care or prenatal service? or prenatal support or antepar-tum care or antepartum service? or antepartum support or peri-natal care or perinatal service? or perinatal support or maternalcare or maternal service? or maternal health care or maternalhealthcare or maternal support or pregnancy care or pregnancyservice? or pregnancy support).ti,ab,kw
21772
3 1 or 2 49966
4 exp Health Personnel/ 446351
5 (Staff or provider$ or health care provider$ or nurs$ or mid-wife$ or midwives or physician$ or doctor$ or obstet$ or med-ical professional$ or clinician$ or skilled birth attendant$ orauxiliary or lay health worker$).ti,ab,kw
1213677
6 4 or 5 1449700
12Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
7 3 and 6 17809
8 qualitative research/ 33348
9 7 and 8 504
10 limit 7 to “qualitative (best balance of sensitivity and specificity)”
4640
11 9 or 10 4666
12 limit 11 to yr=“2000 -Current” 3668
C O N T R I B U T I O N S O F A U T H O R S
OT conceived of and commissioned the study. SD and KF drafted the protocol with revisions from OT. All authors read, amendedand approved the manuscript.
D E C L A R A T I O N S O F I N T E R E S T
All authors have contributed to the review of the WHO ANC guidelines (2015-2016): Soo Downe and Kenny Finlayson were fundedto undertake related reviews for the guideline team.
S O U R C E S O F S U P P O R T
Internal sources
• University of Central Lancashire (UCLan), UK.Infrastructure Funding
• World Health Organization (WHO), Switzerland.Infrastructure Support
External sources
• Bill and Melinda Gates Foundation, USA.Grant number OPP1084319
13Factors that influence the provision of good-quality routine antenatal services: a qualitative evidence synthesis of the views and
experiences of maternity care providers (Protocol)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.