article type: review article algorithms for managing ... · article type: review article algorithms...
TRANSCRIPT
Acc
epte
d A
rtic
le
This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/apa.12962 This article is protected by copyright. All rights reserved.
Article Type: Review Article
Algorithms for managing infant constipation, colic, regurgitation and cow’s milk allergy in formula-fed infants
Vandenplas Y1, Alarcon P2, Alliet P3, De Greef E1, De Ronne N4, Hoffman I5,
Van Winckel M6, Hauser B1.
1UZ Brussel, Vrije Universiteit Brussel, Brussels, Belgium;
2 National Institute of Child Health, Lima-Peru
3 Jessaziekenhuis, Pediatrics, Hasselt, Belgium
4 Kind en Gezin, Brussels, Belgium
5 UZ Gasthuisberg, KUL, Leuven, Belgium
6 UZ Gent, RUG, Ghent, Belgium
Short title: Algorithms for gastrointestinal symptoms
Key-words: algorithms, constipation, colic, cow’s milk protein allergy, regurgitation
Address for correspondence: Yvan Vandenplas, UZ Brussel, Laarbeeklaan 101, 1090 Brussels,
Belgium.
e-mail: [email protected]; Tel + 3224775780; Fax: +3224775783

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Abstract
Gastrointestinal symptoms, such as constipation, regurgitation and infant colic, occur in about
half of infants. These symptoms are often functional, but they may also be caused by cow’s milk
protein allergy. We developed three algorithms for formula-fed infants, which are consensus
rather than evidence-based due to the limited research available in the existing literature.
Conclusion. We believe that these algorithms will help primary healthcare practitioners to
recognise and manage these frequent gastrointestinal manifestations in infants.
Key Notes
• Gastrointestinal symptoms, such as constipation, regurgitation and infant colic, frequently
affect infants and these can be functional or caused by cow’s milk protein allergy.
• The authors developed three algorithms for formula-fed infants, which are consensus
rather than evidence-based due to the limited research available in the existing literature.
• We believe that these algorithms will help primary healthcare practitioners to recognise
and manage these frequent gastrointestinal manifestations in infants.
Conflict of Interest: Yvan Vandenplas is a consultant for Biocodex and United Pharmaceuticals.
The other authors have no conflicts of interest relevant to this article to disclose.
Abbreviations:
CMPA: cow’s milk protein allergy
GORD: gastro-oesophageal reflux disease
IgE: immunoglobulin E

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Introduction
About 50% of infants present with functional gastrointestinal symptoms, such as colic,
regurgitation and constipation, and many infants experience a combination of these symptoms
(1). Each of these three conditions account for roughly 20 to 25% of all cases (1). The Rome III
criteria propose diagnostic criteria for these symptoms, but do not propose management
techniques (2). These symptoms are almost never a reason to stop breastfeeding, but functional
GI symptoms very frequently lead to formula changes by parents and healthcare providers. A
descriptive study published 30 years ago quantified this frequency, by showing that these
moderate digestive problems led to formula changes in 35% of cases (3) and these findings have
repeatedly been confirmed.
Most algorithms propose different approaches for each separate functional GI symptom, but
many infants present with a combination of these problems (1). Cow’s milk protein allergy
(CMPA) is not a functional gastrointestinal problem, but it is a similar condition since symptoms
of CMPA are unspecific and functional. CMPA in infants presenting with gastrointestinal
manifestations, is normally non-Immunoglobulin E (IgE) mediated. Therefore, laboratory tests
such as specific IgE tests, skin prick tests and patch tests are not helpful as they are, at best,
indicative of a diagnosis of IgE mediated CMPA (4) and the management of IgE and non-IgE
mediated allergy is identical.
This study presents state-of-the-art practical algorithms for the management of these functional
gastrointestinal symptoms, providing a follow-up to the algorithms that were published in 2013
(5). The goal was to further simplify the proposed approach. Like guidelines or
recommendations, they need to be challenged and adapted over time. The authors met face-to-

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
face twice and held email discussions to reach a consensus. They didn’t receive any financial
contribution or other kind of help.
Constipation
Feeding plays a key role in the stool pattern of infants younger than four months. Healthy breast-
fed babies may defecate as frequently as seven times per day or as infrequently as once a week
(2,5,6). Extremes of up to 12 times a day or once in three or four weeks have even been reported
(2,6). Hard stools occur in only 1% of exclusively breast-fed infants, compared to 9.2% in
standard formula-fed infants, without prebiotic or probiotic supplementation (7). Firm or hard
stools are often seen when breast milk is switched to infant formula or after the introduction of
solids. Harder stools are frequent in infants fed with formulas containing palm olein oil or palm
oil as the main source of fat (8).
Diagnosis
A thorough medical history and physical examination are the cornerstones for establishing the
diagnosis and aetiology of infant constipation. Failure to pass meconium during the 24 to 48
hours after birth should raise suspicion of Hirschsprung’s disease or cystic fibrosis (6,9).
Functional constipation is constipation without an underlying causal organic disease.
It is important that healthcare professionals are aware of the normal defecation pattern of infants
so that they can differentiate between abnormal and normal defacation, educate and advise
parents adequately and avoid unnecessary treatment. It is crucial to understand what parents
mean when they use the term constipation. Information should be gathered regarding the
duration of the condition, the frequency of bowel movements, the consistency and size of the

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
stools, whether defecation is painful and the presence of pain and blood. This information will
help to make the distinction between functional constipation and constipation due to organic
disease. The Amsterdam stool scale may provide a more objective description of stool
consistency (10). The definition proposed by Biggs et al for infant constipation - of “difficult or
rare defecation lasting for at least two weeks” - has been well accepted and recommended by
experts (9). No laboratory or radiographic testing is necessary if there are no reasons to suspect
an organic cause (6). The younger the infant, the higher the risk of an anatomical or organic
cause, although functional constipation remains the most frequent condition at any age.
Anorectal examination should evaluate perianal sensitivity, anal position and tone, the size of the
rectum and the presence of an anal wink (5,6). Specific tests must be performed if other clinical
data are present, such as failure to thrive, intermittent diarrhoea or abdominal distension (6).
Although CMPA has been shown to be a cause of constipation in a subset of children, the exact
proportion is unclear and the pathophysiological mechanisms have remained elusive (6).
Management
The first step in managing functional constipation is to educate and reassure the parents by
addressing the myths and fears around constipation and pointing out that functional constipation
is one of the most common manifestations in infants (1,5,6). Infantile dyschezia - crying and
straining during defecation - is considered to be normal behaviour in young infants and should
not be medicalised (2). Dietary recommendations may help. If the probability of an organic
condition is low, reassurance and close follow up should be sufficient. In some regions, it is
common to use magnesium-rich mineral water to prepare infant formula. However, there is no
evidence to support this practice and mineral intake will be above the recommended limit if only
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
this water is used (6). Juices containing sorbitol, such as prune, pear and apple juices, can
decrease constipation, but the risk is that infants may drink more fruit juice than formula and,
therefore, become malnourished. Glycerine suppositories can be helpful if rectal emptying is
necessary to provide acute relief. However, evidence does not support the use of mineral oil,
which could lead to a risk of lipoid pneumonia due to aspiration, or enemas such as phosphates,
in young infants. Infant formulas offer a good alternative for managing functional constipation if
they contain partially or extensively hydrolysed proteins, fortified with prebiotics and, or,
probiotics, and do not contain palm oil as the main source of fat in the oil blend (11,12). There
are some formulas advertised as anti-constipation formulas, but some of them have a high
magnesium content, albeit within the regulatory limits (13). An Italian study suggested that
Lactobacillus reuteri (L. reuteri ) was effective in preventing constipation (14). The literature
about the efficacy of probiotics in infant constipation is very limited, since only one trial has
been performed that shows encouraging results (15), but supplementing infant formulas with
probiotics and prebiotics is regarded as safe. Several studies have been performed with a partial
hydrolysate, supplemented with a prebiotic and ȕ-palmitate, and this showed some beneficial
results (16,17).
Regurgitation
The prevalence of daily regurgitation in three to four-month-old infants is estimated to be around
50 to 60% (5,18). More than four episodes of regurgitation per day, which occurs in about 20%
of all infants, is considered to be troublesome by parents and leads them to seek medical help
(18-21).

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Diagnosis
Regurgitation is the passage of refluxed contents into the pharynx or mouth or from the mouth.
Vomiting is defined as a central nervous system reflex involving both autonomic and skeletal
muscles. Most episodes of gastro-oesophageal reflux and regurgitation occur during the post-
prandial period and cause few or no symptoms (18). According to the Rome III criteria, the
diagnosis of regurgitation in a healthy infant between the age of three weeks and 12 months
should include: regurgitation two or more times per day for at three weeks or more and absence
of nausea, haematemesis, aspiration, apnoea, failure to thrive, difficulty in feeding or swallowing
and abnormal posture (2). More than 50% of all infants fit these criteria and we feel that there
needs to be a stricter definition. In our view, infants should present with at least four episodes of
regurgitation a day for at least two weeks and, according to the epidemiologic data, this
corresponds to 20% of all infants (5,18). Gastro-oesophageal reflux disease (GORD) is a
condition in which the reflux of gastric contents causes a decreased quality of life and, or,
complications (18). The management of GORD, which is seldom used in this age group, includes
lifestyle changes as well as pharmacological therapy - mainly acid reducing medication - and, in
few cases, surgery (5,18,22). In infants younger than three weeks and older than six months, the
differential diagnoses should be more strictly excluded, since physiologic regurgitation rarely
starts before the age of three weeks or after the age of six months.
Management
Regurgitation is physiological in this age group and occurs in normal healthy infants. However, a
complete medical history and physical examination are warranted in infants with troublesome
and frequent regurgitation involving more than four episodes a day, to rule out organic disease.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Since physiological regurgitation should not be diagnosed in an infant with vomiting and poor
weight gain (5,18), anthropometry is of major importance. The management of regurgitation
starts with reassuring the parents and providing information on the natural history of
regurgitation, correct formula preparation and how overfeeding may exacerbate regurgitation. In
infantile regurgitation, thickened formula or anti-regurgitation formula decreases the frequency
and the volume of regurgitation, but does not decrease gastro-oesophageal reflux (18). The prone
anti-Trendelenburg position cannot be recommended because of the risk of sudden infant death
syndrome (23). An anti-regurgitation bed with an angle of 40 or 50 degrees has been studied
(24). Sleeping the infant on their side has also been recommended (25), but this sleeping
position is associated with an intermediate risk for sudden infant death syndrome between prone
and supine sleeping positions. Many studies have failed to show any benefits of anti-secretory
drugs or prokinetic agents in this situation (5,18,22). A subset of infants with therapy resistant
regurgitation may suffer from CMPA (4,5,22,22) as detailed in the CMPA algorithm.
The nutritional management of regurgitation consists of correcting the frequency and volume of
feeds if necessary (5,18,22,28). Because of its increased viscosity, thickened anti-regurgitation
formula reduces both the volume and frequency of regurgitation and crying and improves sleep
and supports weight gain (5,18,22). The commercial anti-regurgitation formulas contain different
thickening agents, such as processed rice, corn or potato starch, guar gum or locust bean gum
(5,18,22). In-vitro laboratory tests have found that bean gum has a negative effect on the
absorption of vitamins and minerals (26), but this has not been confirmed in clinical trials (27). If
a commercial anti-regurgitation formula is not available, a thickening product may be added to
the formula. Cereals increase the caloric intake, possibly inducing excessive weight gain, and

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
locust bean gum does not increase the calorific density, but may cause gassiness. Home-
thickening of a regular formula always increases the osmolarity, which may induce reflux and
regurgitation by increasing the number of lower oesophageal sphincter relaxations. This may
induce reflux and regurgitation. Infants with persistent regurgitation or vomiting should be
referred to a paediatric specialist (18).
There is limited literature suggesting that some specific probiotics (L. reuteri DSM 17938) and
prebiotics prevent functional GI symptoms such as regurgitation (14,17). L. reuteri may
accelerate gastric emptying (28). CMPA should be suspected in an infant with persistent and
recurrent regurgitation and, or, vomiting, particularly if this is associated with other
manifestations of allergic disease, such as eczema and, or, wheezing, as seen in the CMPA
algorithm. There are also studies that need to be replicated that suggest that formulas that do not
contain palm olein or palm oil as the main source of fats in the oil blend are associated with less
regurgitation (29) or that a thickened partial hydrolysate formula may be slightly more effective
than a thickened standard infant formula (30), possibly because it is easier to digest partial
hydrolysates (31). Partial hydrolysates empty the stomach faster than standard protein, which
may contribute to a decrease in regurgitation (32).
Infantile colic
Infantile colic was originally defined by Wessel in 1954 as crying lasting three or more hours a
day, at least three days a week and for at least three weeks (33). In 2006, the Rome III criteria
defined it as “episodes of irritability, fussing, or crying that begin and end for no apparent reason
and last at least three hours a day, at least three days a week, for at least one week” (2). The
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
incidence of infantile colic varies between 5 and 30% (34,35) and it is reported to occur equally
frequent in breast and bottle-fed infants and in both sexes. The aetiology of colic is multi-
factorial and is unknown. Multiple hypotheses have been proposed, including altered
gastrointestinal function, food intolerance, transient low lactase activity, CMPA, gastro-
oesophageal reflux and intestinal microflora imbalance. (5). Parents being able to cope is of
major importance for reporting and managing colic, more so than in any other functional
gastrointestinal manifestation.
Diagnosis
The cardinal manifestation of infantile colic is excessive and persistent loud crying, mostly late
in the afternoon. During each episode the child appears irritable, distressed and fussy and
contracts the legs, becomes red-faced and has frequent episodes of borborygmi. CMPA and
GORD should be considered in patients with severe colic. Very limited literature suggests that a
transient low lactase activity could also cause excessive crying (36,37).
Attention should always be focused on how the parents are coping, including their anxiety levels,
signs of depression, the absence of mother–child reciprocity and the risk of child abuse.
Management
There are no uniform criteria for a specific therapeutic approach. The first recommended step is
to look for potential symptoms that indicate a possible organic disease (see algorithm). If these
are not present, the feeding technique should be evaluated and the parents should be reassured
and supported. Parents should be informed about how to recognise signs of hunger and fatigue
and how they can offer their infant offering structure, regularity and a calm environment.
General advice emphasising the self-limiting nature of the condition is important. Clinicians

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
should advise mothers who are breastfeeding to continue doing so. If there are reasons to
consider CMPA, advising the mother to avoid cow’s milk proteins for a minimum of two weeks
can be considered. The most validated treatment for infant colic is to substitute cow’s milk with
an extensively hydrolysed formula in a highly selected population of infants (5). In formula-fed
infants, eliminating CMP and replacing it with an extensively hydrolysed protein formula has
been reported as an effective treatment (5,35). However, this information is mainly derived from
studies in highly selected patients from tertiary care level centres. Experience, but not evidence,
has shown that partially hydrolysed formulas can be a useful option when extensive hydrolysate
would be too expensive and CMPA is not a potential cause of infant colic (31,35). In many
cases, these formulas have reduced lactose or are lactose free and have added prebiotics or
probiotics and this results in a reduction in the number of crying episodes per week and total
crying time with varying levels of evidence (31). However, the role of lactose can be questioned,
as soy formula has not been associated with any benefits (34). According to one review (36), soy
formulas seemed to be effective, but soy milk can induce allergy and is, therefore, not
recommended. In a recent meta-analysis, which included data from 40 studies, the weighted
prevalence of soy allergies was no more than zero to 0.5% in the general population (38). But the
negative results of studies evaluating the efficacy of lactase strongly suggest that low lactase
activity can cause infant colic (36). Patient selection is likely to be a major bias in these studies.
Several studies have been performed with proton pump inhibitors in distressed infants, but they
all failed to show any benefit (39). Allopathic drugs, such as simethicone and lactase, have not
proved to be effective and some of them, such as dicyclomine, can cause potentially serious
adverse reactions (36,40). Fennel extract and sucrose solutions have shown some benefit (36).
Medications such as dicycloverine or cimetropium have also been tested in infant colic.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Cimetropium has shown a high rate of lethargy, motion sickness and, or, somnolence. Other
randomised controlled trials have studied glucose or saccharose solutions, showing varying
effects on crying time (41). In a double-blind, placebo-controlled trial, a partial hydrolysate with
high ȕ-palmitate and a specific prebiotics mixture with galacto and fructo-oligosaccharides,
resulted in a significant decrease in colic within one week of intervention (42). One clinical trial
demonstrated the safety and efficacy of L. reuteri in preventing infant colic (14). Two
randomised double- blind trials showed that L. reuteri effectively reduced crying time in breast-
fed infants (43,44). A recent study with the same probiotic strain, L. reuteri DSM 17938, in a
community sample of breast-fed and formula-fed infants with infant colic failed to show any
benefit (45). In fact, at one-month-old, the probiotic group actually cried or fussed 49 minutes
more than the placebo group (95% confidence interval eight to 90 minutes, P=0.02) (45).
Studies have evaluated the role of additional family support, counselling therapies, car rides
during colic episodes, reduced stimulating actions, such as changing nappies, spinal massages by
chriropractors and even the use of herbal options. None of these trials has been of sufficient
methodological quality to allow any recommendation (22,36,40). There is also insufficient
evidence to systematically recommend swaddling, although the technique has been reported to
be of some benefit in infants younger than eight-weeks-of-age (46).
Infant colic is a multi-factorial condition and it is, therefore, unlikely that a single intervention
will reduce it significantly in an unselected patient population. According to all the systematic
reviews to date, there is some evidence of a beneficial effect of hydrolysed formula in patients
with infant colic due to CMPA.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Cow’s milk protein allergy (CMPA)
Cow’s milk is the most common cause of food allergy in infants and occurs in 3-5% of formula-
fed infants and in 0.5% of breast-fed infants (4). CMPA often presents with gastrointestinal
manifestations, such as regurgitation, vomiting and abnormal defecation. Avoiding cow’s milk
protein can resolve the symptoms. However, dietary restrictions and elimination diets need to be
avoided if they are not needed because they may induce impaired growth or malnutrition and
cause unnecessary costs for the family.
Classification and clinical features
According to the definition proposed by the World Allergy Organization, CMPA is a
hypersensitivity reaction caused by specific immunological mechanisms to one or more of the
proteins in cow’s milk (4). CMPA can be classified in different categories: IgE-mediated, non-
IgE mediated and a mixture of IgE-mediated /non-IgE-mediated.
IgE-mediated CMPA is caused by an immediate hypersensitivity to CMP, which is often
associated with atopic conditions such as atopic eczema, asthma and, or, allergic rhinitis.
Gastrointestinal symptoms, such as regurgitation, vomiting, colic and diarrhoea, accompany
systemic manifestations of the skin, such as urticaria and angioedema, and respiratory tract
symptoms such as rhinitis, wheezing and stridor. Symptoms such as pallor or flaccidity
(hypotension) also occur soon after allergen exposure, usually within an hour. Anaphylaxis is the
most serious manifestation of IgE-mediated CMPA, but is rare (4). Mixed IgE/non-IgE-mediated
CMPA and non-IgE-mediated CMPA constitute a mixed group of disorders that have been well
defined clinically, although their immunological mechanisms are not well understood. In
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
individual infants, it may be very difficult to distinguish reflux from CMPA symptoms. The
conditions that might be caused by CMPA are not confined to CMPA and may also be triggered
by other food allergens.
Diagnosis and management
The central principle in managing patients with food allergies is avoiding the food known to
cause the reaction. In some parts of the world there is a tendency for medical practitioners to
over-diagnose CMPA and prescribe elimination diets that are not adequately supervised. In other
parts there is a tendency to under diagnose CMPA. Both practices could have an adverse impact
on the child’s growth (47). An elimination diet should be recommended for infants with
symptoms that suggest an IgE-mediated reaction. Skin prick or specific IgE tests can be
performed, but are not recommended (4) and atopy patch testing is not a recommended
procedure (48). Recently, the Cow's Milk Related Symptom Score was developed as an
awareness tool to facilitate appropriate diagnosis of CMPA (49). Total IgE has a poor specificity
for the diagnosis of CMPA, but does provide information on the prognosis: the higher the IgE,
the longer it will take to develop tolerance. (50). A cow’s milk challenge is the diagnostic gold
standard, but does not provide proof that the immune system is involved. IgE sensitisation
without a clinical history does not conclusively show CMPA.
Children with CMPA should also be monitored for the development of tolerance. Most children
with IgE-mediated CMPA will ultimately achieve tolerance (51) and children that have an IgE
negative allergy become tolerant at a younger age. However, our knowledge of the natural

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
evolution of CMPA is likely to be biased since most data has come from tertiary care level
centres and focused on the most severe cases.
Regarding formula replacement, all guidelines recommend an extensive hydrolysate as the first
option (4). There is limited evidence that the addition of prebiotics or probiotics to an extensive
hydrolysate offer any additional benefit (50,52). An open study suggested that probiotics induced
a more rapid tolerance (50). Soy is the second option, when the extensive hydrolysate is not
available, too expensive or if the child refuses to drink it (4). Rice hydrolysates, which are on
the market in a growing number of countries, will soon play a role in these recommendations
since the evidence of their efficacy is growing (53,54). Extensively hydrolysed rice protein
formulas are free of CMP allergens, and thus have a low residual allergenicity, and they are
cheaper than extensive cow’s milk-based hydrolysates. The World Allergy Organization
Diagnosis and Rationale for Action against CMPA (WAO-DRACMA) guidelines recommend
amino acid-based formulas rather than extensive hydrolysates for infants at high risk of
anaphylactic reactions (55). WAO-DRACMA recommends extensive hydrolysates over soy
formula in IgE-mediated CMPA, but stresses the need for more data by stating that “there is very
sparse evidence suggesting a possible benefit from using eHF compared to soy formula”.
Although soy protein has been used in infant feeding for more than 100 years, the popularity of
soy infant formula varies substantially in different parts of the world. The world is divided into
those countries where is it popular, such as the USA, and those where it is avoided, such as
France (56). The Agence Française de Sécurité Sanitaire des Aliments has underlined the limited
knowledge and uncertainties regarding the presence of isoflavones in soy formulas (57).
However, a recent meta-analysis concluded that soy infant formula was safe (58).
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
A literature review by The American Academy of Pediatrics concluded that about 10% to 14%
of infants with CMPA will become sensitised to soy and that this happens more frequently in
non-IgE mediated CMPA (59). In a prospective cohort study of 13,019 infants by Katz et al, the
incidence of IgE-mediated CMPA was 0.5%. Interestingly, none of the 66 had a documented
allergy to soy and 64 of these infants could tolerate soy (60). A recent meta-analysis found that
the prevalence of allergy to soy and IgE sensitisation to soy infant formula was less than reported
and that there was insufficient evidence to hypothesise that the risk would be increased in infants
younger than six months (59, 60).
Conclusion
Infants presenting with functional gastrointestinal problems often go through a series of
unnecessary investigations and medical treatments. The practical algorithms presented in this
paper will help general practitioners and paediatricians to diagnose and manage these functional
disorders and CMPA, focusing on reassurance, education and dietary intervention. The diagnosis
and management of CMPA is challenging because there is no specific symptom or diagnostic
test other than exclusion or provocation. Overall, medication has failed to provide significant
improvements in these conditions. Although there is some evidence that functional
gastrointestinal disorders and CMPA may be accompanied by dysbiosis, the proof on the
efficacy of therapeutic interventions with prebiotics and probiotics is very limited.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
References
1. Iacono G, Merolla R, D'Amico D, Bonci E, Cavataio F, Di Prima L, et al; Paediatric Study
Group on Gastrointestinal Symptoms in Infancy. Gastrointestinal symptoms in infancy: a
population-based prospective study. Dig Liver Dis 2005; 37:432-8.
2. Hyman PE, Milla PJ, Benninga MA, Davidson GP, Fleisher DF, Taminiau J. Childhood
functional gastrointestinal disorders: neonate/toddler. Gastroenterology 2006; 130:1519-26.
3. Forsyth BW, McCarthy PL, Leventhal JM. Problems of early infancy, formula changes, and
mothers' beliefs about their infants. J Pediatr 1985; 106:1012-7.
4. Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S, et al. . Diagnostic
approach and management of cow’s milk protein allergy in infants and children: a practical
guideline of the GI-committee of ESPGHAN. J Pediatr Gastroenterol Nutr 2012; 55:221-9.
5. Vandenplas Y, Gutierrez-Castrellon P, Velasco-Benitez C, Palacios J, Jaen D, Ribeiro H, et al.
Practical algorithms for managing common gastrointestinal symptoms in infants. Nutrition 2013;
29:184-94.
6. Tabbers MM, Dilorenzo C, Berger MY, Faure C, Langendam MW, Nurko S, et al. Evaluation
and Treatment of Functional Constipation in Infants and Children: Evidence-Based
Recommendations From ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr 2014;
58:265-81.
7. Tunc VT, Camurdan AD, Ilhan MN, Sahin F, Beyazova U. Factors associated with defecation
patterns in 0-24-month-old children. Eur J Pediatr 2008; 167:1357-62.
8. Lloyd B, Halter RJ, Kuchan MJ, Baggs GE, Ryan AS, Masor ML. Formula tolerance in
postbreastfed and exclusively formula-fed infants. Pediatrics 1999; 103: E7
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
9. Biggs WS, Dery WH. Evaluation and treatment of constipation in infants and children. Am
Fam Physician 2006; 73:469-77.
10. Ghanma A, Puttemans K, Deneyer M, Benninga M, Vandenplas Y. Amsterdam infant stool
scale is more useful for assessing children who have not been toilet trained than Bristol stool
scale. Acta Paediatr 2014; 103:e91-2.
11. Koo WW, Hockman EM, Dow M. Palm olein in the fat blend of infant formulas: effect on
the intestinal absorption of calcium and fat, and bone mineralization. J Am Coll Nutr 2006;
25:117-22.
12. Moro G, Mosca F, Miniello V, Fanaro S, Jelinek J, Stahl B, et al. Effects of a new mixture of
prebiotics on faecal flora and stools in term infants. Acta Paediatr 2003; 91 (Suppl441): 77-9.
13. Chao HC, Vandenplas Y. Therapeutic effect of Novalac-IT in infants with constipation.
Nutrition 2007; 23:469-73.
14. Indrio F, Di Mauro A, Riezzo G, Civardi E, Intini C, Corvaglia L, et al. . Prophylactic use of
a probiotic in the prevention of colic, regurgitation, and functional constipation: a randomized
clinical trial. JAMA Pediatr 2014; 168:228-33.
15. Coccorullo P, Strisciuglio C, Martinelli M, Miele E, Greco L, Staiano A. Lactobacillus
reuteri (DSM 17938) in infants with functional chronic constipation: a double-blind, randomized,
placebo-controlled study. J Pediatr 2010; 157:598-602.
16. Bongers ME, de Lorijn F, Reitsma JB, Groeneweg M, Taminiau JA, Benninga MA. The
clinical effect of a new infant formula in term infants with constipation: a double-blind,
randomized cross-over trial. Nutr J 2007; 6:8.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
17. Savino F, Maccario S, Castagno E, Cresi F, Cavallo F, Dalmasso P, et al. Advances in the
management of digestive problems during the first months of life. Acta Paediatr 2005;
94(Suppl449):120-4.
18. Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric
gastroesophageal reflux clinical practice guidelines: joint recommendations of the North
American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) and
the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN). J
Pediatr Gastroenterol Nutr 2009; 49:498-547.
19. Hegar B, Dewanti NR, Kadim M, Alatas S, Firmansyah A, Vandenplas Y. Natural evolution
of regurgitation in healthy infants. Acta Paediatr 2009; 98:1189-93.
20. Martin AJ, Pratt N, Kennedy JD, Ryan P, Ruffin RE, Miles H, Marley J. Natural history and
familial relationships of infant spilling to 9 years of age. Pediatrics 2002; 109:1061-7.
21. Nelson SP, Chen EH, Syniar GM, Christoffel KK. Prevalence of symptoms of
gastroesophageal reflux during infancy. A pediatric practice-based survey. Pediatric Practice
Research Group. Arch Pediatr Adolesc Med 1997; 151:569-72.
22. Lightdale JR, Gremse DA; Section on Gastroenterology, Hepatology, and Nutrition.
Gastroesophageal reflux: management guidance for the pediatrician. Pediatrics 2013;
131:e1684-95.
23. Moon RY, Task force on Sudden Infant Death Syndrome. SIDS and other sleep-related
infant deaths: expansion of recommendations for a safe infant sleeping environment. Pediatrics
2011; 128:1030-9.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
24. Vandenplas Y, De Schepper J, Verheyden S, Devreker T, Franckx J, Peelman M, et al. A
preliminary report on the efficacy of the Multicare AR-Bed in 3-week-3-month-old infants on
regurgitation, associated symptoms and acid reflux. Arch Dis Child 2010; 95:26-30.
25. Loots C, Smits M, Omari T, Bennink R, Benninga M, van Wijk M. Effect of lateral
positioning on gastroesophageal reflux (GER) and underlying mechanisms in GER disease
(GERD) patients and healthy controls. Neurogastroenterol Motil 2013; 25:222-9, e161-2.
26. Bosscher D, Van Caillie-Bertrand M, Deelstra H. Do thickening properties of locust bean
gum affect the amount of calcium, iron and zinc available for absorption from infant formula? In
vitro studies. Int J Food Sci Nutr 2003; 54:261-8.
27. Levtchenko E, Hauser B, Vandenplas Y. Nutritional value of an "anti-regurgitation" formula.
Acta Gastroenterol Belg 1998; 61:285-7.
28. Indrio F, Riezzo G, Raimondi F, Bisceglia M, Filannino A, Cavallo L, et al. Lactobacillus
reuteri DSM 17938 accelerates gastric emptying and improves regurgitation in infants. Eur J
Clin Invest 2011; 41:417-22.
29. Alarcon PA, Tressler RL, Mulvaney A, Lam W, Comer GM. Gastrointestinal tolerance of a
new infant milk formula in healthy babies: an international study conducted in 17 countries.
Nutrition 2002; 18:484-9.
30. Vandenplas Y, Leluyer B, Cazaubiel M, Housez B, Bocquet A. Double-blind comparative
trial with 2 antiregurgitation formulae. J Pediatr Gastroenterol Nutr 2013; 57:389-3.
31. Vandenplas Y, Cruchet S, Faure C, Lee H, Di Lorenzo C, Staiano A, et al. When should we
use partially hydrolysed formulae for frequent gastro-intestinal symptoms and allergy
prevention? Acta Paediatr 2014; 103:689-95.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
32. Billeaud C, Guillet J, Sandler B. Gastric emptying in infants with or without gastro-
oesophageal reflux according to the type of milk. Eur J Clin Nutr 1990; 44: 577-83.
33. Wessel MA, Cobb JC, Jackson EB, Harris GS Jr, Detwiler AC. Paroxysmal fussing in
infancy, sometimes called “colic.” Pediatrics 1954; 14:421-35.
34. Critch J. Infantile colic: is there a role for dietary interventions? Paediatr Child Health 2011;
116:47-9.
35. Shergill-Bonner R. Infantile colic: practicalities of management, including dietary aspects. J
Fam Health Care 2010; 20:206-9.
36. Bruyas-Bertholon V, Lachaux A, Dubois JP, Fourneret P, Letrilliart L. Which treatments for
infantile colics? Presse Med 2012; 41:e404-10.
37. Cohen-Silver J, Ratnapalan S. Management of infantile colic: a review. Clin Pediatr 2009;
48:14-17
38. Katz Y, Gutierrez-Castrellon P, González MG, Rivas R, Lee BW, Alarcon P. A
comprehensive review of sensitization and allergy to soy-based products. Clin Rev Allergy
Immunol 2014; 46:272-81.
39. Gieruszczak-Bia!ek D, Konarska,Z, Skórka A, Vandenplas Y, Szajewska H. No effect of
proton pump inhibitors on crying and irritability in infants: systematic review of randomized
controlled trials. J Pediatr (in press)
40. Metcalf TJ, Irons TG, Sher LD, Young PC. Simethicone in the treatment of infant colic: a
randomized, placebo-controlled, multicenter trial. Pediatrics 1994; 94: 29–34.
41. Akçam M, Yilmaz A. Oral hypertonic glucose solution in the treatment of infantile colic.
Pediatr Int 2006; 48:125-7.
42. Savino F, Palumeri E, Castagno E, Cresi F, Dalmasso P, Cavallo F, et al. Reduction of crying
episodes owing to infantile colic: a randomized controlled study on the efficacy of a new infant
formula. Eur J Clin Nutr 2006; 60:1304-10.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
43. Savino F, Cordisco L, Tarasco V. Lactobacillus reuteri DSM 17938 in infantile colic: a
randomized, placebo trial. Pediatrics 2010; 126:e526-33.
44 Szajewska H, Gyrczuk E, Horvath A. Lactobacillus reuteri DSM 17938 for the management
of infantile colic in breastfed infants: a randomized, double-blind, placebo-controlled trial. J
Pediatr 2013; 162:257-62.
45. Sung V, Hiscock H, Tang ML, Mensah FK, Nation ML, Satzke C, Heine RG, Stock A, Barr
RG, Wake M. Treating infant colic with the probiotic Lactobacillus reuteri: double blind,
placebo controlled randomised trial. BMJ 2014; 348:g2107.
46. van Sleuwen BE, L'hoir MP, Engelberts AC, Busschers WB, Westers P, Blom MA, et al..
Comparison of behavior modification with and without swaddling as interventions for excessive
crying. J Pediatr 2006; 149:512-7.
47. Kirby M, Danner E. Nutritional deficiencies in children on restricted diets. Pediatr Clin N
Am 2009; 56:1085-103.
48. Boyce JA, Assa'ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. NIAID-
Sponsored Expert Panel. Guidelines for the diagnosis and management of food allergy in the
United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol 2010;
126:1105-18.
49. Vandenplas Y, Dupont C, Eigenmann P, Host A, Kuitunen M, Ribes-Konick C, et al. A
workshop report on the development of the Cow's Milk-related Symptom Score awareness tool
for young children. Acta Paediatr 2015; DOI: 10.1111/apa.12902
50. Berni Canani R, Nocerino R, Terrin G, Frediani T, Lucarelli S, Cosenza L, et al. Formula
selection for management of children with cow's milk allergy influences the rate of acquisition of
tolerance: a prospective multicenter study. J Pediatr 2013; 163:771-7.e1.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
51. Skripak JM, Matsui EC, Mudd K, Wood RA. The natural history of IgE-mediated cow’s milk
allergy. J Allergy Clin Immunol 2007; 120:1172–7.
52. Moro G, Arslanoglu S, Stahl B, Jelinek J, Wahn U, Boehm G. A mixture of prebiotic
oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age.
Arch Dis Child 2006; 91:814-9.
53. Vandenplas Y, De Greef E, Hauser B; Paradice Study Group. Safety and tolerance of a new
extensively hydrolyzed rice protein-based formula in the management of infants with cow's milk
protein allergy. Eur J Pediatr 2014; 173:1209-16
54. Vandenplas Y, De Greef E, Hauser B; Paradice Study Group. An extensively hydrolyzed rice
protein-based formula in the management of infants with cow’s milk protein allergy: preliminary
results after 1 month. Arch Dis Childh 2014; 99:933-6.
55. Fiocchi A, Schünemann HJ, Brozek J, Restani P, Beyer K, Troncone R, et al. Diagnosis and
Rationale for Action Against Cow's Milk Allergy (DRACMA): a summary report. J Allergy Clin
Immunol 2010; 126:1119-28.
56. Vandenplas Y, De Greef E, Devreker T, Hauser B. Soy infant formula: is it that bad? Acta
Paediatr 2011; 100:162-6
57. www.afssa.fr; March 2005
58. Vandenplas Y, Castrellon PG, Rivas R, Gutiérrez CJ, Garcia LD, Jimenez JE, Anzo A, Hegar
B, Alarcon P. Safety of soya-based infant formulas in children. Br J Nutr 2014; 111:1340-60.
59. Bhatia J, Greer F, American Academy of Pediatrics Committee on Nutrition. Use of soy
protein-based formulas in infant feeding. Pediatrics 2008; 121:1062-8.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
60. Katz Y, Rajuan N, Goldberg MR, Eisenberg E, Heyman E, Cohen A, Leshno M. Early
exposure to cow’s milk protein is protective against IgE-mediated cow’s milk protein allergy J
Allergy Clin Immunol 2010; 126:77-82.
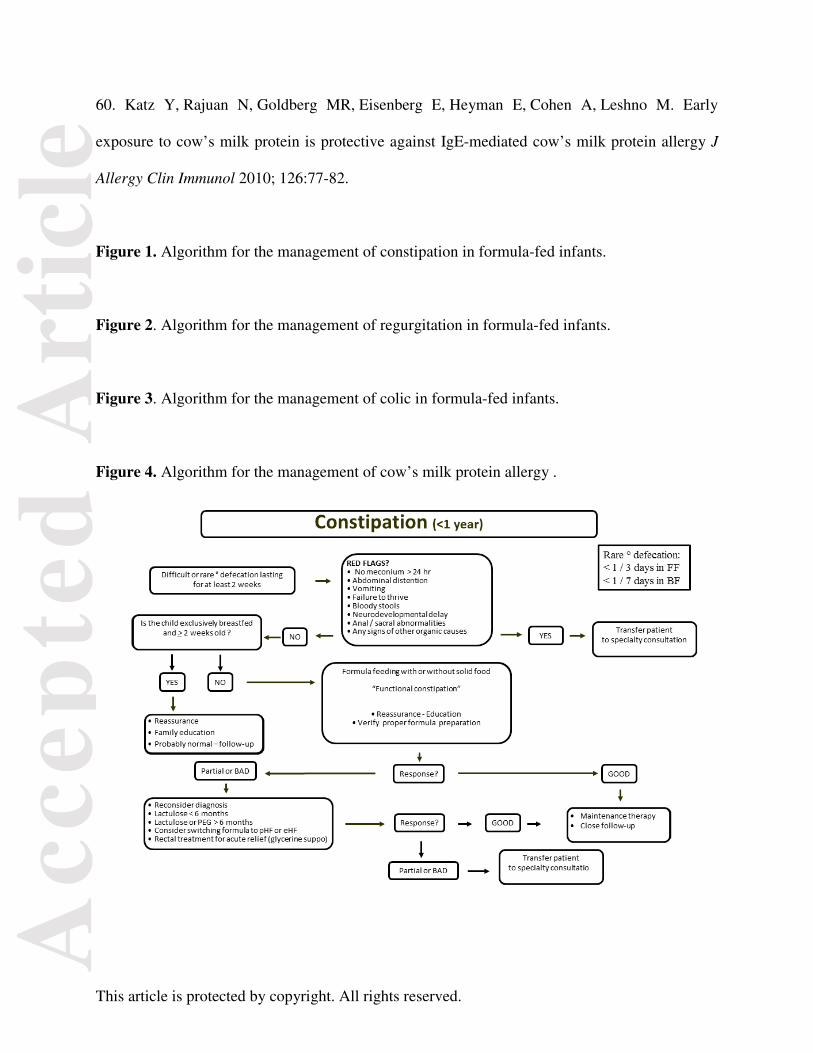
Figure 1. Algorithm for the management of constipation in formula-fed infants.
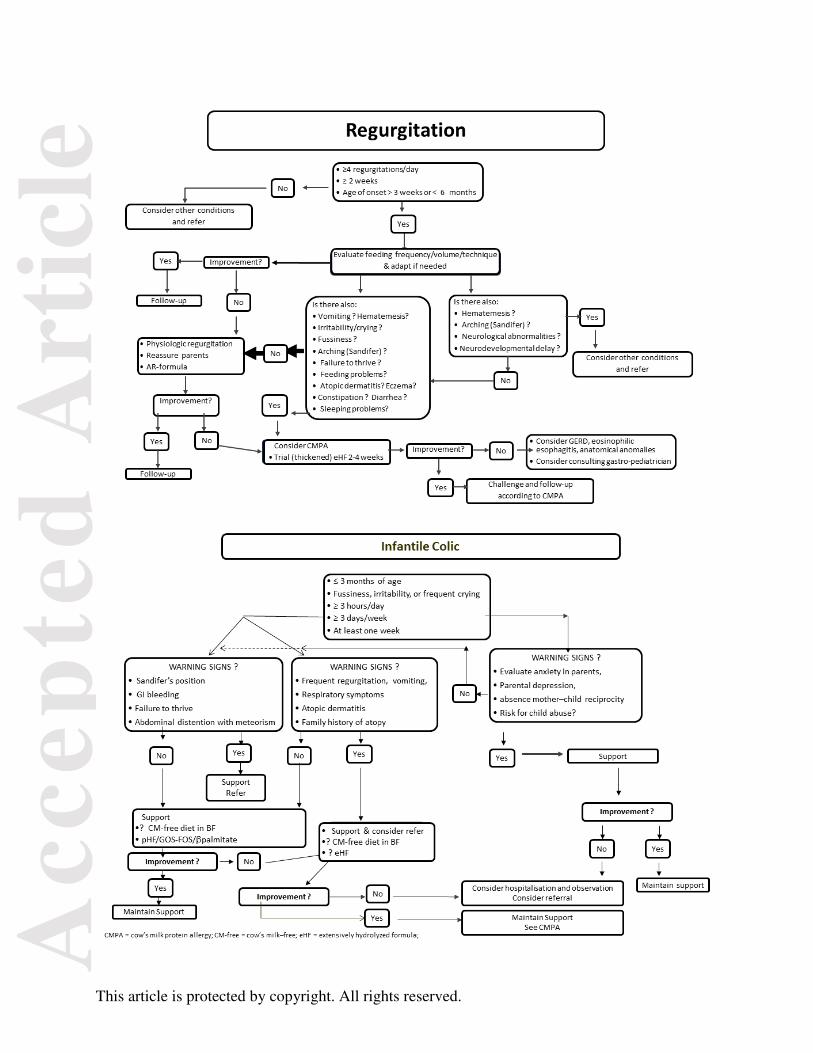
Figure 2. Algorithm for the management of regurgitation in formula-fed infants.
Figure 3. Algorithm for the management of colic in formula-fed infants.
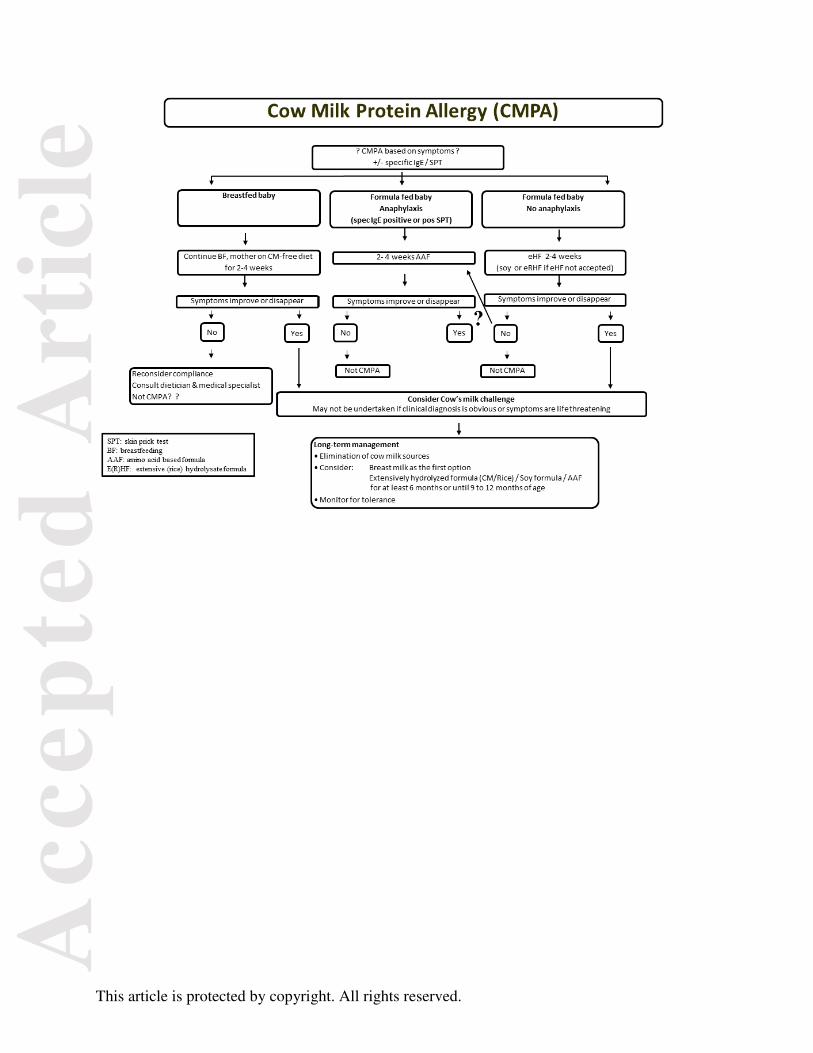
Figure 4. Algorithm for the management of cow’s milk protein allergy .
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.