arvs and art – looking to the future sharon r lewin professor and head, department of infectious...
TRANSCRIPT

ARVs and ART – looking to the future
Sharon R LewinProfessor and Head, Department of Infectious Diseases, Monash University and Alfred HospitalCo-head, Centre for Biomedical Research, Burnet Institute, Melbourne, Australia
7th IAS Conference on Pathogenesis, Treatment and Prevention, Kuala Lumpur, 30th June – 3rd July, 2013

ARV and ART: looking to the future
Better antiretrovirals–Reduce cost–Reduce toxicity–Enhance durability of control
Reduce long term morbidity
The very distant future

cheaper and better antiretrovirals

Strategies to reduce cost of current ARVsOptimising the active pharmaceutical
ingredient (API)– Optimise material sourcing– Change in manufacturing process– Improve bioavailability
Pharmaco-enhancementExtension of shelf-lifeReduce dose
Crawford et al., Lancet Infect Dis 2012; 12:550; Conference on Antiretroviral Dose Optimisation (CADO), 2010

New source of raw material Mg tert-butoxide reduces cost of TDF
Similar strategies currently being evaluated for efavirenz, ATZ/r, DRV/r
Crawford et al., Lancet Infect Dis 2012; 12:550

Lower doses can be effective, reduce toxicities…and reduce cost
Drug Doses studied Outcome Study
NNRTI
Efavirenz 600mg vs 400mg vs 200mg
No difference in %<400 c/ml
Hicks
Riplivarine 150mg vs 75 mg vs 25mg
All doses non inferior to EFV
Pozniak
Protease inhibitors
LPV/r 400/100 vs 200/100 mg
Improved outcomes for low dose
Murphy
Integrase inhibitors
Raltegravir 600 vs 400 vs 200 vs 100 mg
HIV RNA < 50 c/ml in 85%, 83%, 88% and 88%
Markowitz

New ARVs in development
NRTI NNRTI PI Entry Inh InSTI
Phase 3 TAF cenicriviroc dolutegravir
Phase 2 apricitabine DAPD dexelvucitabinefestinavir
BILR 355 MK-1439
BMS-663068 ibalizumab PF-232798
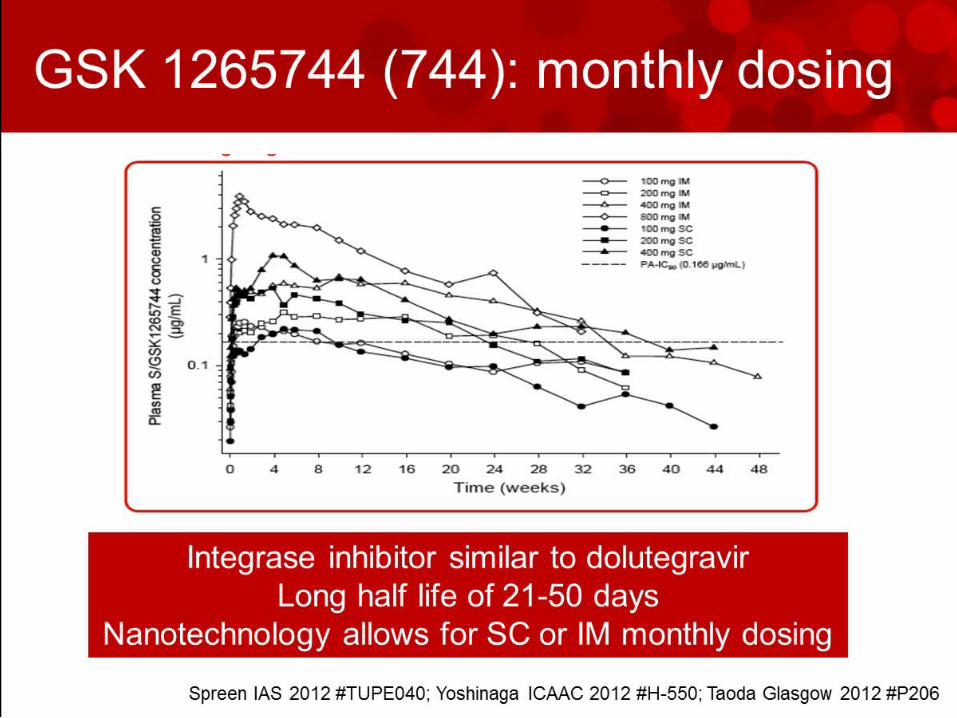
GSK744
Phase 1/2 amdoxovir elvucitabine
TMC 310911
HGS004
Phase 1 RDEA 806 CTP-298 CTP-518 PPL-100 SPI-256
SCH532706 VIR-576
BI 224436 INH-1001
Gulick, 20th CROI, Atlanta, GA, March 2013

Tenofovir alenofenamide (TAF): reduced renal toxicity and cost
Zolopa CROI 2013, Atlanta, GA # 99LB
0102030405060708090
100
2 4 8 12 16 24
% H
IV-1
RN
A <
50 c
/mL
Time (Weeks)
TAF/FTC/EVG/c 88% (n=112)
TDF/FTC/EVG/c 90% (n=58)
Change in serum creatinine at Week 24TAF +0.07 mg/dL
TDF +0.12 mg/dL (p=0.02)
TAF/FTC/EVG/COBI
Rx-naïve, VL >5000, CD4 >50 (N=170)


New technologies for delivery of ARVsNanotechnology
– Efavirenz 300mg – Pediatric LPV/r in development
Injectables, implants, slow release– GSK744 + rilpivarine LA– GSK744 + 2NRTI (Latte study)– Vaginal rings e.g., dapivirine / maraviroc
Multipurpose prevention technologies– HIV + STI + pregnancy

Long and short term priorities to improve ARVs First-line
– fixed-dose combination regimens that are equally or more potent and more durable and affordable than TDF/XTC/EFV
Post Treatment –failure – fixed dose boosted, dose-optimized darunavir in replacing atazanavir or
lopinavir as the protease inhibitor of choice– A one pill once daily second-line regimen.– Studies of reduced-dose darunavir/ritonavir (DRV/r),
Enhancing Trial Participant Criteria– including girls and women of reproductive age, TB co-infection, and
comorbidities (such as hypertension).
Longer Term Research Priorities– oral and injectable long-acting drugs (including GSK744 and TMC278)
as well as nano-formulations and implantable devices.
CADO2 report, South Africa, April 2013

reduce long term
morbidity

Increased age-related complications on ART
Frieberg et al., JAMA Internal Med 2013
Increased risk of AMI in HIV compared to HIV uninfectedHR = 1.48 (CI = 1.27 – 1.72)
Further increase HR if CD4<200 or HIV RNA>500
Mea
n A
MI
even
ts p
er 1
000
pers
on y
ears
40-49 years 50-59 years 60-69 years0
1
2
3
4
5
6
2
3.9
5
1.52.2
3.3
HIV+ HIV-
N=82,459; Veterans Ageing Cohort Study Virtual Cohort

HIV and aging in Africa
Mills et al., N Engl J Med 2012; 366:14
In 2040, the number of persons over 50 years of age living with HIV is expected to be 9 million

Lifestyle
Etiology of non-AIDS-related events
Non-AIDS-related events are more common in HIV disease, even after adjustment for age, cART exposure and traditional risk factors
Deeks SG, Phillips AN. Br Med J 2009;338:a3172
cARTtoxicity
Persistentinflammation(immune activation)
Non-AIDS events
(e.g. smoking)

Prevention of non AIDS events needs a different model of care Lifestyle modifications
– Reduce smoking, healthy diet, exercise
Reduce modifiable risk factors– Assessment of blood pressure, glucose and
lipids
Counselling and screening for common cancers
Enhance CD4 recovery and reduce inflammation

the very distant future

HIV cure is rare and possible – but a very long term goal
THE VISCONTI PATIENTS The Mississippi
baby
The Berlin Patient

Acknowledgements
The Alfred Hospital, Melbourne– Julian Elliott – Jennifer Hoy– Edwina Wright
Elsewhere– Steve Deeks– Diane Havlir– Trip Gulich– Judith Currier– Andrew Ball– Adeeba Kamarulzaman
