as parents opt out of getting shots for their children ...€¦ · web viewdescribe how access to...
TRANSCRIPT

STUDENT CASE STUDY—SINGER-FREEMAN
MMR VACCINE AND AUTISM: SCIENTIFIC INQUIRY, ETHICS, AND EVIDENCE-BASED PROBLEM SOLVING
CASE STUDY FOR THE AACU STIRS PROGRAM
Karen Singer-Freeman, Associate Professor of Psychology, Purchase College, State University of New York
STUDENT CASE
Learning ObjectivesThrough participation in this case study, students should be able to:
Part One Describe how vaccines function to protect individuals and society. Describe how access to vaccines differs in different parts of the world. Describe the symptoms and complications associated with vaccine-preventable diseases. Verbally interpret the meaning of data presented visually.
Part Two Explain basic ethical principles used in scientific research. Use evidence presented in this case to illustrate how deductive logic can be used to generate
conclusions from data. Use evidence presented in this case to illustrate how inductive logic can be used to generate
hypotheses from data. Explain how experiments, population comparisons, case control studies, time-trend analysis
studies, and cohort studies contribute to establishing cause and effect. Verbally interpret the meaning of data presented visually.
Part Three Describe the different choices countries can make to protect themselves against vaccine-
preventable diseases. Describe how individual choices can affect public health. Discuss how this case illustrates the evidence-based, problem-solving approach. Describe the importance of accurate media coverage of scientific research.
Part OnePreparatory Materials
Review the information on autism available at this website: http://www.ninds.nih.gov/disorders/autism/detail_autism.htm
Review the information on vaccines available at this website:

STUDENT CASE STUDY—SINGER-FREEMAN
o http://www.cdc.gov/vaccines/pubs/parents-guide/downloads/parents-guide-part3.pdf
Read the case study through Question 5.
Note: You will also need to prepare for Part Two before you discuss in class. See the beginning of Part Two for these preparatory materials.
Understanding the ProblemIn 1998, Dr. Andrew Wakefield and colleagues published a paper in the Lancet reporting that eight out of twelve children they had seen for stomach problems developed autism shortly after receiving the Measles, Mumps, and Rubella (MMR) vaccine (Wakefield et al. 1998). They hypothesized that this combination vaccine might cause one form of autism in which a normally developing child loses cognitive and language abilities. The paper received a great deal of media attention. In the months and years following the report, the Daily Mail, a popular British newspaper, published articles with these headlines: “MMR Killed My Daughter"; "MMR Fears Gain Support"; "New Evidence 'Shows MMR Link to Autism'"; "MMR Safe? Baloney. This Is One Scandal That's Getting Worse"; "Scientists Fear MMR Link To Autism"; and "Why I Wouldn't Give My Baby The MMR Jab" (Greenslade 2013). MMR immunization rates in the United Kingdom dropped from 94 percent in 1998 to 75 percent in 2002 (Offit and Coffin 2003). As media reports of the study spread in the United States, immunization rates fell here as well and diseases that were nearly eradicated returned (Centers for Disease Control 2014). To combat the prevailing doubts about the safety of vaccinations, scientists have conducted and published increasingly sophisticated analyses of epidemiological data (Dales, Hammer, Smith 2001; Farrington, Miller, and Taylor 2001; Rao and Andrade 2011; Taylor et al. 1999). However, despite consensus among scientists that the MMR vaccine is safe and that the vaccine preservative thimerosal is safe (Parker et al. 2004), there continue to be reports in non-scientific sources suggesting that vaccines or thimerosal cause autism (Rao and Andrade 2011). These reports have caused some parents to delay vaccinating their children (Gust et al. 2004; Omer et al. 2009) and have allowed diseases such as measles to reappear in the United States (Parker et al. 2006).
Understanding Vaccination FBefore considering research that tests the safety of vaccines, we must understand how vaccines work to protect us from diseases. Please refer to the Guide to Vaccine Safety you read to prepare for this case study and review Figure 1 below in order to answer the questions below. If you would like to learn more about how vaccines build immunity you can go to this site: http://www.historyofvaccines.org/content/how-vaccines-work.
Figure 1. Vaccination (see right). Retrieved from: http://www.cdc.gov/vaccines/parents/vaccine-decision/prevent-diseases.html .

STUDENT CASE STUDY—SINGER-FREEMAN
Key Questions1) What is immunity?2) How do vaccines create immunity without creating disease?3) What can we conclude from looking at Figure 2?4) Describe one personal, one community, and one future benefit of vaccinating all eligible
children for measles.5) Who is ineligible for vaccination? How can we protect these individuals from disease?
Figure 1. Cases of Measles in the United States. Retrieved from: http://www.cdc.gov/vaccines/pubs/parents-guide/downloads/parents-guide-part3.p.
Herd ImmunityWhen a large percentage of a community is vaccinated against a disease, even the unvaccinated are protected from this disease. This is known as herd immunity (Centers for Disease Control 2014). The percentage of people that must be vaccinated in order to protect the community is different for different diseases, depending on the contagiousness of the disease. For example, at least 80–86 percent of a population must be vaccinated to protect against polio (historyofvaccines.org). However, because measles is highly contagious, more than 94 percent of the population must be vaccinated in order to establish measles herd immunity (Ochoche and Gweryina 2014)
In Figure 3, an outbreak of a disease occurs in three communities with different levels of vaccination coverage. Herd immunity is important because in some instances vaccines can fail to provide immunity and because some people cannot be vaccinated (including children under six months, pregnant women, and individuals with compromised immune systems). If an increasing number of parents chose not to vaccinate their children, those who cannot be vaccinated, those for whom the vaccine did not provide immunity, and those who were voluntarily left unvaccinated are all at an increased risk of becoming sick with the disease compared to if there was a sufficient level of vaccination in the community.

STUDENT CASE STUDY—SINGER-FREEMAN
Figure 2. An Outbreak of a Disease Occurs in Three Different Communities. In the top community no one is immunized. In the middle community, some are immunized but not enough to produce herd immunity. In the bottom community, a critical minimum portion of the population is immunized, protecting community members who are not vaccinated. Retrieved from: http://www.niaid.nih.gov/topics/pages/communityimmunity.aspx .
Key Questions6) Explain herd immunity in your own words.7) Explain how an individual who chooses not to be vaccinated can potentially harm an individual
who was vaccinated.
Vaccine-Preventable DiseasesLearn more about some of the diseases that vaccines prevent by reviewing Figure 4 below and the Appendix at the end of this case.

STUDENT CASE STUDY—SINGER-FREEMAN
Figure 4. Summary of Vaccine-Preventable Diseases. Retrieved from: http://www.healthyfamiliesnow.net/arkansas-healthy-children-handbook/chapter-4-childrens-health-histories-physical-exams-and.

STUDENT CASE STUDY—SINGER-FREEMAN
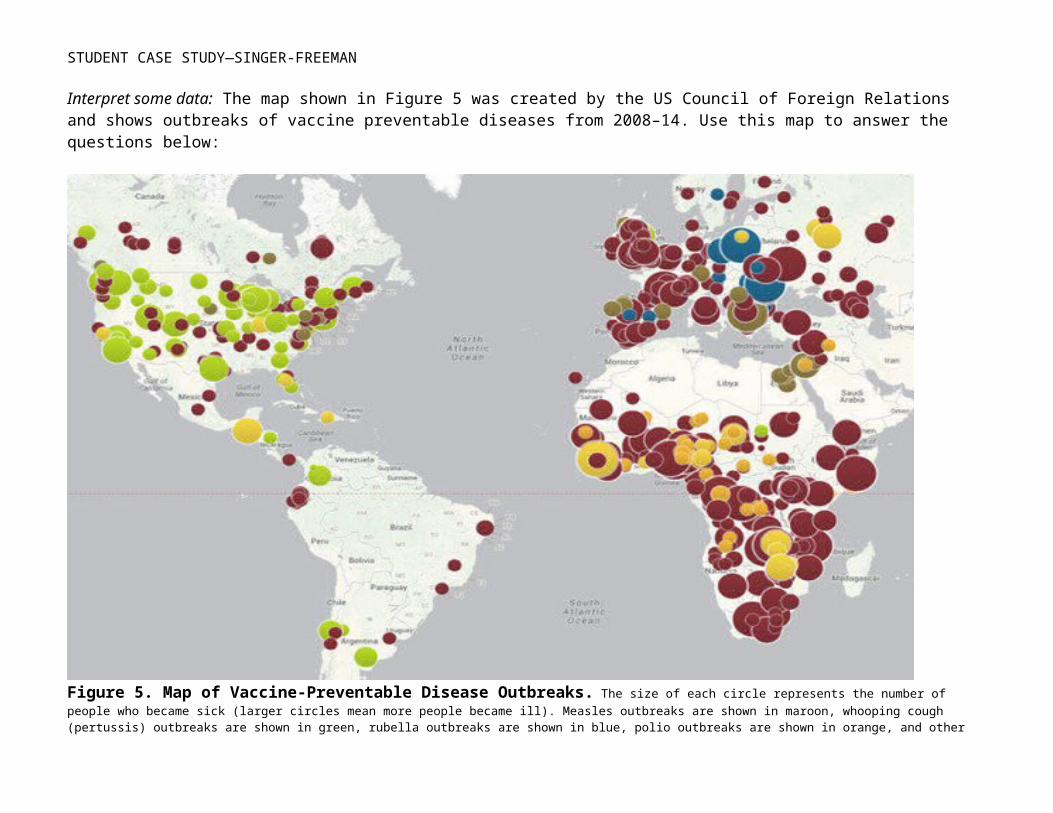
Interpret some data: The map shown in Figure 5 was created by the US Council of Foreign Relations and shows outbreaks of vaccine preventable diseases from 2008–14. Use this map to answer the questions below:
Figure 5. Map of Vaccine-Preventable Disease Outbreaks. The size of each circle represents the number of people who became sick (larger circles mean more people became ill). Measles outbreaks are shown in maroon, whooping cough (pertussis) outbreaks are shown in green, rubella outbreaks are shown in blue, polio outbreaks are shown in orange, and other vaccine preventable disease outbreaks are shown in yellow. Retrieved from: http://www.cfr.org/interactives/GH_Vaccine_Map/#map On March 28, 2014.

STUDENT CASE STUDY—SINGER-FREEMAN
Key Questions8) Which vaccine-preventable diseases list death as a possible complication in Figure 4?9) Which continents have the highest number of cases for measles, whooping cough, rubella, and
polio? 10) Suggest explanations for why so many people in these areas get these diseases and consider
the information you would need to gather to support your answers to determine if your proposed explanation is correct.
A Closer Look at Vaccination Coverage in the United StatesFigure 6 depicts changes in US vaccination coverage, by state, between 2006 and 2011, and reports the coverage needed to maintain adequate herd immunity for each preventable disease. Vaccination coverage has decreased in states listed on the left side of the figure and increased or remained the same in states on the right side of the figure. Red lines indicate when coverage levels in 2011 were below the level needed for herd immunity for one or more of the vaccine-preventable diseases. States in gray bars had adequate herd immunity in 2006. However, many states have lost this level of protection. For example, by looking at the column for New York, you can see that coverage has dropped for both the DTP vaccine (top) and the MMR vaccine (bottom) because the bar for this state is on the left side of both the top and bottom figure. You can see that New York had adequate herd immunity for measles, mumps, and rubella in 2006 because the bottom bar for New York is colored gray. However, the red lines at the top of each bar indicate that in 2011 it was below the ideal level of protection for measles, diphtheria, and pertussis.
STUDENT CASE STUDY—SINGER-FREEMAN
Figure 6. Change in DTP and MMR Vaccination Coverage, 2006–11. Red lines indicate states that have fallen below the herd immunity threshold for Pertussis (top) or Measles (bottom). Retrieved from: http://www.scientificamerican.com/article/too-many-children-go-unvaccinated/.
Key QuestionsUse the figure above to answer the following key questions.
11) What levels of vaccination coverage are required to maintain adequate herd immunity for Pertussis, Diptheria, Measles, Mumps, and Rubella?
12) Describe two possible consequences of reduced herd immunity for people living in the area.

STUDENT CASE STUDY—SINGER-FREEMAN
13) Select one state other than New York from the left side of the figure. Tell us what you can determine about the State’s vaccine coverage in 2006 and 2011.
The loss of herd immunity is causing resurgence of diseases like measles and pertussis (whooping cough) (Parker et al. 2006). As outbreaks become more common in the United States, the importance of vaccinating children is beginning to receive more media coverage.
“Doctors See Chinks in Vaccination Armor,” by Amanda Mascarelli, August 5, 2011, Los Angeles Times. Retrieved from: http://articles.latimes.com/2011/aug/05/health/la-he-vaccines-herd-immunity-20110801/2.
As parents opt out of getting shots for their children, diseases such as whooping cough and measles make a comeback when 'herd immunity' crumbles. . . . As immunization rates have dropped in certain pockets of the United States— due largely to parents' unfounded concerns about vaccine safety—some of the most contagious diseases are making a comeback. . . . In addition to the rise in whooping cough, the CDC has received reports of 12 outbreaks of measles this year that have sickened more than 170 people, the highest number since 1996. One cluster involved 21 people in a Minnesota community that included many children who skipped the MMR vaccine for measles, mumps, and rubella because their parents had doubts about its safety, the CDC says. "This is an ominous trend in our country," says Dr. James Campbell, a pediatrician in Golden, Colo. . . . Currently, about 20 states allow parents to forego vaccinations due to "conscientious objections" or "personal belief exemptions." A 2004 study in Pediatrics found that states allowing philosophical exemptions from vaccines have significantly higher rates of unimmunized children. Those kids tended to come from affluent families with parents who had doubts about the safety of vaccines.
“Remembering How to Fight Measles,” by Paul Offit, March 27, 2014, New York Times.Retrieved from: http://www.nytimes.com/2014/03/28/opinion/remembering-how-to-fight-measles.html.
The measles vaccine is a victim of its own success. In 1963, when the vaccine first came into existence, measles virus infected about three million people a year in the United States, hospitalized 48,000, and killed 500. By the turn of the 21st century, however, measles infections had been virtually eliminated. Unfortunately, because some parents are choosing not to vaccinate their children, measles is coming back. Last year, nearly 200 cases were reported. This year, the numbers appear to be even worse, with cases in more than half a dozen states already . . . Clinicians and parents have forgotten how terrifying measles can be. Earlier this month, Kristin Cavallari, a former reality-show star, and the wife of the Chicago Bears quarterback Jay Cutler, told a national television audience that she had decided not to vaccinate her children. “I’ve read too many books about autism,” she said, though the link between vaccines and autism has been thoroughly disproved. Ms. Cavallari’s cavalier attitude teaches us that not only have we largely eliminated measles; we’ve eliminated the memory of the disease. Measles, however, can be deadly. In February 1991, I witnessed an outbreak of measles in Philadelphia that centered on two faith-healing churches. Five children died in one month. The city was in a panic. We’re approaching a precipice. If we remain on our current path, measles cases will continue to grow. When we get to about 600 cases of measles a year, we could again

STUDENT CASE STUDY—SINGER-FREEMAN
see measles deaths, most likely among children. But everyone who isn’t immune is vulnerable, including those who can’t be vaccinated for medical reasons and rely on the rest of us for protection.
Reflect on what you have learned in this section of the case study by considering some final questions.
Key Questions14) What do you believe are the three most important reasons for parents to vaccinate their
children?15) Of the vaccine-preventable diseases you have learned about, which one seems the most
dangerous to public health? Explain your answer by discussing the extent to which the disease is contagious as well as the possible complications for the disease.
Part Two A: Fighting Rumors with SciencePreparatory Materials
Register for and complete this one- to two-hour workshop that introduces you to ethics in research with human subjects. The training is available at: http://phrp.nihtraining.com/.
Read Part Two A of the case study Read an Introduction to Evidence-Based Problem Solving (available at:
http://www.aacu.org/stirs/casestudies/index.cfm) Watch three brief lectures on randomized controlled trials (available at:
https://www.youtube.com/watch?v=7ybuE39BpQ8), case control and cohort studies (available at: https://www.youtube.com/watch?v=J3GHTYa-gZg) and time trend studies (available at: https://www.youtube.com/watch?v=GUq_tO2BjaU)
In 2010, because of doubts about the findings, Lancet retracted the original Wakefield article that had suggested a link between the MMR vaccine and the development of autism. In 2004, ten of the twelve authors publically said they disagreed with the paper’s findings and Dr. Wakefield has had his medical license revoked for ethical misconduct (Burns 2010). There were four primary problems with the way that Wakefield implemented and reported his study: 1) He received money from lawyers who were currently suing vaccine manufacturers; 2) Although he said that the twelve patients in the study entered his practice consecutively, in fact, he had selected the group of patients for the study from a larger group of patients that he did not include; 3) He completed invasive tests on the children in the study without obtaining approval that the inclusion of these tests was necessary or ethical; and 4) He misreported the children’s symptoms in ways that supported his hypothesis (Godlee, Smith, and Marcovitch 2011; Miller 2003).
Key Questions16) Why is it a problem that Wakefield received payments from lawyers representing families who
were suing vaccine manufacturers? How might this have influenced his choice of research subjects?
17) Why are the results of his research less likely to be correct if he selected the patients that he included instead of including all of his current patients?

STUDENT CASE STUDY—SINGER-FREEMAN
18) Why is it unethical to conduct painful tests on children without the approval of a committee that oversees the ethical conduct of research? (You may wish to review the NIH training workshop to help you answer this question (http://phrp.nihtraining.com/ ).
Unfortunately, the retraction of Wakefield’s original article has had little effect on the beliefs of some parents that vaccines cause autism. Scientists are now convinced that vaccines do not cause autism (Centers for Disease Control 2014). However, the damage from this one “bad study” continues to be felt in terms of lowered vaccination rates and the return of preventable diseases (Greenslade 2013). Today it is your job to learn about the research that has convinced scientists that there is no association between MMR vaccine and autism. You will be asked to consider ways that you could improve the safety of the public by increasing MMR vaccination rates.
Research DesignBy the end of this section of the case study you will be able to explain why scientists believe that vaccines are safe and, in fact, save lives. In order to do this you will have to learn a little about research design. Research design describes the decisions that we make when we design research experiments. Scientists wish to learn the causes of disease. In order to know for certain that exposure to one thing (like a vaccine) causes another thing (like autism), conducting an experiment is essential.
The experiment: Experiments rely on randomized controlled trials. One group of participants is selected in such a way that the group represents a larger population. This group is randomly divided into two or more groups. It is important to randomly assign the participants into two groups in order to avoid accidentally putting more of the healthy children in the group we expect to get a particular treatment. We also must include a large number of participants so we are not unduly influenced by individual differences. We test both groups to see if they have the condition we are interested in before the treatment. This is called a pre-test. Because we would probably choose to test one-year-olds (who have not yet received the MMR vaccine) it is unlikely that any children will have been diagnosed with autism when our experiment begins (autism is not generally diagnosed until age two at the earliest). However, it is important to check as a way of making sure that the two groups are similar before receiving the treatment.
After we have determined that the groups are equivalent, one group receives an experimental treatment (like the MMR vaccine) that is hypothesized to cause something (like autism or disease immunity). We call this group the treatment group. The other group—called the control group—does not receive the experimental treatment. The control group may receive the standard treatment (if there is one), no treatment, or a sham treatment called a “placebo.”1We then follow both groups to see whether more children who received MMR vaccines develop autism (or disease immunity) than
1 A placebo is something that seems similar to the experimental treatment—for example, a saline injection lacking the important active ingredient—the vaccine. Placebos are used in many experimental studies because the belief that one is receiving treatment can be enough to cause improvement of symptoms; this is known as the “placebo effect.” In the experiment described above, a placebo might not be necessary since the development of autism in a very young child is unlikely to be influenced by the placebo effect. On the other hand, administration of a placebo could affect the parents’ perception of a child’s risk of developing autism.

STUDENT CASE STUDY—SINGER-FREEMAN
children who did not receive vaccines. Figure 7 summarizes the key features of experimental design, with a placebo administered to the control group.
Figure 7. The Key Features of Experimental Design.
If we conducted this experiment and found that substantially more children who received the MMR vaccine developed autism than did children who received the saline injection, we would have strong evidence that the MMR vaccine was dangerous. How would we decide whether the rates of autism in the two groups were different enough to reach this conclusion? Scientists use statistical analyses to decide whether the differences between groups that we observe in an experiment are large enough to indicate that our treatment caused the difference. These tests measure the difference between groups and the difference within groups to determine the likelihood that the treatment had the anticipated effect on the outcome. Experiments allow us to make causal conclusions because we have made sure that everything except our treatment is the same in the two groups. If the difference between the groups was large enough (given the variability within each group), we would have found some support for the hypothesis that the MMR vaccine causes autism.
If the difference between the groups was too small (given the variability within each group) to support the hypothesis that the MMR vaccine causes autism, we would still be unable to conclude that the MMR vaccine does not cause autism. All we would be able to conclude is that we did “not find evidence that vaccines cause autism.” This is because although an experiment includes conditions that allow scientists to find support for a causal relationship between a treatment and a disease, proof that a relationship does not exist is impossible, especially from a single study.
The experiment described above has never been done. You have already learned about the ethics that are involved in decisions about research design. As a reminder, the three primary ethical guidelines that are explained in the Belmont Report are: Respect for People, Beneficence, and Justice. All research must conform to these guidelines and be approved by a committee of impartial experts before data is collected.
The population of all 1-year-old
children in the United States
Representative group of 10,000
1-year-old children
Treatment Group 5,000 receive
vaccine (autism rates
measured)
Autism rates
measured
Control Group 5,000 receive saline
(autism rates measured)
Autism rates
measured

STUDENT CASE STUDY—SINGER-FREEMAN
Key Questions19) Use your own words to describe the three key ethical principles laid out in the Belmont Report. 20) Which principle(s) of the Belmont Report would be violated by this experiment? Explain your
answer.21) If we were able to conduct this experiment, what could we conclude and what would we be
unable to conclude? Explain your answer.22) Propose and describe another way we could study this question that would not violate any of
the ethical principles outlined in the Belmont Report. Complete answers should include the population that would be studied, the information that would be collected, and the possible conclusion that could be drawn.
Part Two B: How Can We Study the Effects of Potentially Dangerous Treatments? Methods Used in the Study of Vaccines and AutismOnce your group has answered Question 22, please see your instructor for guidance on next steps for this section of the case study.
Concluding Part Two B—Summing It All UpReflect on what you have learned in this section of the case study by considering some final questions.
Key Question40) Of the three study designs that you reviewed, which do you believe offers the most convincing
evidence that vaccinations are unrelated to the development of autism? Explain your answer.
Part Three: How Do We Protect our Children through Public Policy?You are now aware of the dangerous effects of vaccine avoidance. Currently in the United States, all states allow parents to petition for an exemption from vaccinations for their children. Some states only accept religious beliefs and medical conditions as reasons for vaccine exemption whereas other states also allow philosophical exemptions. In some states, the number of parents seeking vaccine exemptions is rising. For example, in New York State, the average religious exemption rate nearly doubled over the past ten years, rising from 0.23 percent in 2000 to 0.45 percent in 2011 (Imdad et al. 2013).
Lawmakers, doctors, and parents are becoming increasingly concerned about the risk unvaccinated children create for the community. On June 24, 2014, a Brooklyn Federal District Court judge upheld a New York City policy that bars unimmunized children from attending public school when another child has a vaccine-preventable illness (Mueller 2014). In his ruling the judge cited a 1905 Supreme Court ruling that upheld a the right of a the State of Massachusetts to issue a $5 fine to a man who disobeyed an order to be vaccinated during a smallpox outbreak. The judge ruled that although a family has a right to refuse vaccination for religious reasons, the state has a right to limit an unvaccinated child’s access to school because the child’s presence could threaten public health. This case is thought to establish the government’s right to require immunizations as a matter of public health.

STUDENT CASE STUDY—SINGER-FREEMAN
There are three different approaches to encouraging vaccination:i. Education and Encouragement—Parents receive information about the importance of vaccination, the dangers of the diseases vaccines prevent, and the safety of vaccines. Vaccination is provided at little or no cost. It is left to parents to decide what is best for them and their children. If you select this position be sure to explain how you will limit the effects of sensationalistic media coverage.ii. Make Vaccinations a Legal Requirement but Allow Parents to Opt Out—This policy is currently used in much of the United States. Although parents must show evidence of vaccinations in order to enroll children in public schools or camps they are exempt from this requirement if they complete a form. Rules vary in each state. All 50 states allow exemption if an individual is medically unable to be vaccinated, 47 states allow exemptions for religious reasons, and 19 states allow exemptions for philosophical reasons. Individual state exemptions can be seen at: http://www2a.cdc.gov/nip/schoolsurv/schImmRqmtReport.asp.iii. Tighten Vaccine Requirements—Only allow vaccine exemptions for medical (or medical and religious) reasons.
It is time for you to take a stand. In the next class we will have a debate discussing these three options. Before class you must do the following:
41) Select a position from one of the above and write a paragraph explaining why you believe it is the best option for your state.42) For each of the other two positions, write a paragraph in which you explain two possible problems with the position.
In each of these paragraphs be sure to consider the role of the media in communicating scientific research to the public. Come to class ready to share your views.
ReferencesBurns, J. F. 2010. “British Medical Council Bars Doctor Who Linked Vaccine with Autism,” New York Times, May 24. Retrieved from: http://www.nytimes.com/2010/05/25/health/policy/25autism.html?_r=0.
Centers for Disease Control and Prevention. 2014. “Vaccines and Immunizations.” Last modified December 16. http://www.cdc.gov/vaccines/.
Dales L., S. Hammer, and N. J. Smith. 2001. “Time Trends in Autism and in MMR Immunization Coverage in California.” Journal of the American Medical Association, 285(9): 1183–85. DOI: 10.1001/jama.285.9.1183.
Editors of Lancet. 2010. “Retraction—Ileal-lymphoid-nodular Hyperplasia, Non-specific colitis, and Pervasive Developmental Disorder in Children.” Lancet, 375(9713): 445. DOI: 10.1016/S0140-6736(10)60175-4.

STUDENT CASE STUDY—SINGER-FREEMAN
Farrington, C., E. Miller, and B. Taylor, B. 2001. “MMR and Autism: Further Evidence Against a Causal Association.” Vaccine, 19(27): 3632–35.
Godlee, F., J. Smith, and H. Marcovitch. 2011. “Wakefield’s Article Linking MMR Vaccine and Autism Was Fraudulent.” British Medical Journal, 342: c7452.
Greenslade, R. 2013. “The Story behind the MMR scare.” Guardian, April 24. Retrieved from: http://www.theguardian.com/society/2013/apr/25/mmr-scare-analysis .
Gust, D. A., T. W. Strine, E. Maurice, P. Smith, H. Yusuf, M. Wilkinson, and B. Schwartz. 2004. “Underimmunization among Children: Effects of Vaccine Safety Concerns on Immunization Status.” Pediatrics, 114(1): e16–e22.
Hertz-Picciotto, I., and L. Delwiche. 2009. “The Rise in Autism and the Role of Age at Diagnosis.” Epidemiology, 20(1): 84–90.
Imdad, A., B. Tserenpuntsag, D. S. Blog, N. A. Halsey, D. E. Easton, and J. Shaw. 2013. “Religious Exemptions for Immunization and Risk of Pertussis in New York State, 2000–11.” Pediatrics. Retrieved from: http://pediatrics.aappublications.org/content/early/2013/05/29/peds.2012-3449.
Kaye, J. A., M. del Melero-Montes, and H. Jick. 2001. “Mumps, Measles, and Rubella Vaccine and the Incidence of Autism Recorded by General Practitioners: A Time Trend Analysis.” British Journal of Medicine, 322(7284): 460–63. Retrieved from: http://www.bmj.com/content/322/7284/460 .
Mueller, B. 2014. “Judge Upholds Policy Barring Unvaccinated Students During Illness.” New York Times, June 22. http://www.nytimes.com/2014/06/23/nyregion/judge-upholds-policy-barring-unvaccinated-students-during-illnesses.htm.
Ochoche, J. M., and R. I. Gweryina. 2014. “A Mathematical Model of Measles with Vaccination and Two Phases of Infectiousness.” IOSR Journal of Mathematics, 10(1): 95–105. Retrieved from: http://iosrjournals.org/iosr-jm/papers/Vol10-issue1/Version-4/R0101495105.pdf.
Omer, S. B., D. A. Salmon, W. A. Orenstein, M. P. deHart, and N. Halsey. 2009. “Vaccine Refusal, Mandatory Immunization, and the Risks of Vaccine-preventable Diseases.” New England Journal of Medicine, 360(19): 1981–88.
Ouellette-Kuntz, H., H. Coo, M. Lam, M. M. Breitenbach, P. E. Hennessey, P. D. Jackman, and A. M. Chung. 2014. “The Changing Prevalence of Autism in Three Regions of Canada.” Journal of Autism and Developmental Disorders, 44(1): 120–36.
Parker, S. K., B. Schwartz, J. Todd, and L. K. Pickering. 2004. “Thimerosal-containing Vaccines and Autistic Spectrum Disorder: A Critical Review of Published Original Data.” Pediatrics, 114(3): 793–804.

STUDENT CASE STUDY—SINGER-FREEMAN
Parker, A. A., W. Staggs, G.H. Dayan, I. R. Ortega-Sánchez, P. A. Rota, L. Lowe, P. Boardman, R. Teclaw, C. Graves, and C. W. LeBaron. 2006. “Implications of a 2005 Measles Outbreak in Indiana for Sustained Elimination of Measles in the United States.” New England Journal of Medicine, 355(5): 447–55.
Rao, T. S., and C. Andrade. 2011. “The MMR Vaccine and Autism: Sensation, Refutation, Retraction, and Fraud.” Indian Journal of Psychiatry, 53:95–6. Retrieved from: http://www.indianjpsychiatry.org/text.asp?2011/53/2/95/82529 .
Stanovich, K. E., R. F. West, and M. E. Toplak. 2013. “Myside Bias, Rational Thinking, and Intelligence.” Current Directions in Psychological Science, 22(4): 259–64. DOI: 10.1177/0963721413480174.
Taylor, B., E. Miller, C. Farrington, M. C. Petropoulos, I. Favot-Mayaud, J. Li, and P. A. Waight. 1999. “Autism and Measles, Mumps, and Rubella vaccine: No Epidemiological Evidence for a Causal Association. Lancet, 353(9169): 2026–29.Wakefield, A. J., S. H., Murch, A. Anthony, J. Linnell, D. M. Casson, M. Malik, M. Berelowitz et al. 1998. “Ileal-lymphoid-nodular Hyperplasia, Non-specific Colitis, and Pervasive Developmental Disorder in Children.” Lancet, 351(9103): 637–41.
About the AuthorProfessor Singer-Freeman is an associate professor of psychology at Purchase College, State University of New York. She developed this case study to be part of her introductory class in Child Development as well as her upper-level class in Experimental Psychology. Singer-Freeman’s research examines analogical reasoning in young children. She has experience in curriculum development, general education, assessment, and mentoring. She is currently a co-investigator on an National Science Foundation (NSF) Transforming Undergraduate Education in Science (TUES) grant, which is funding her work adapting the Passion Driven Statistics curriculum from Wesleyan University for use at Purchase College. Professor Singer-Freeman serves on the campus Educational Policies Committee and serves as the associate director of the Baccalaureate and Beyond Program, which supports the success of underrepresented minority and first generation students from community colleges. Professor Singer-Freeman recently established the Interpersonal Relationships Improve Student Success (I-RISE) mentoring program with the help of a CEMRRAT grant for ethnic minority recruitment, retention, and training from the American Psychological Association and utilized funds from an AAC&U Bringing Theory to Practice grant to establish Social Action Learning Communities for transfer students. In recognition of her work with students, she received the Guiding Light award from Purchase College Student Affairs in 2006 and the SUNY Chancellor’s Award for Excellence in Teaching in 2013.

STUDENT CASE STUDY—SINGER-FREEMAN
Appendix: Descriptions of Vaccine-Preventable Diseases Retrieved from the Centers for Disease Control, 2014
Measles causes fever, runny nose, cough, and a rash all over the body. About one out of ten children with measles also gets an ear infection, and up to one out of twenty gets pneumonia. About one out of one thousand gets encephalitis (an inflammation of the brain that can lead to convulsions, and can leave the child deaf or mentally retarded), and one or two out of one thousand die. While measles is almost gone from the United States, it still kills an estimated 164,000 people each year around the world. Measles can also make a pregnant woman have a miscarriage or give birth prematurely.(Retrieved from: http://www.cdc.gov/measles/about/overview.html. Accessed March 28, 2014.)
Mumps is a contagious disease that is caused by the mumps virus. Mumps typically starts with a few days of fever, headache, muscle aches, tiredness, and loss of appetite and is followed by swelling of salivary glands. Anyone who is not immune from either previous mumps infection or from vaccination can get mumps. Mumps is best known for the swelling of the cheeks and jaw that it causes, which is a result of swelling of the salivary glands. People who show symptoms usually recover after a week or two, but mumps can occasionally cause serious complications. The most common complication is inflammation of the testicles (orchitis) in males who have reached puberty; rarely does this lead to fertility problems. Other rare complications include: inflammation of the brain and/or tissue covering the brain and spinal cord (encephalitis/meningitis); inflammation of the ovaries (oophoritis) and/or breasts (mastitis) in females who have reached puberty; and deafness. (Retrieved from: http://www.cdc.gov/mumps/about/disease-overview.html. Accessed March 28, 2014.)
STUDENT CASE STUDY—SINGER-FREEMAN
Rubella is an acute viral disease that causes fever and rash. Complications include at least a twenty percent chance of damage to the fetus if a woman is infected early in pregnancy, deafness, cataracts, heart defects, mental retardation, and liver and spleen damage. (Retrieved from: http://www.cdc.gov/rubella/index.html. Accessed March 28, 2014.)
Pertussis (whooping cough) can cause serious illness in infants, children, and adults. The disease usually starts with cold-like symptoms and maybe a mild cough or fever. After one to two weeks, severe coughing can begin. Unlike the common cold, pertussis can become a series of coughing fits that continues for weeks. In infants, the cough can be minimal or not even there. Infants may have a symptom known as "apnea." Apnea is a pause in the child's breathing pattern. Pertussis is most dangerous for babies. About half of infants younger than one year of age who get the disease are hospitalized. Pertussis can cause violent and rapid coughing, over and over, until the air is gone from the lungs and you are forced to inhale with a loud "whooping" sound. This extreme coughing can cause you to throw up and be very tired. The "whoop" is often not there and the infection is generally milder (less severe) in teens and adults, especially those who have been vaccinated. Early symptoms can last for one to two weeks and usually include: runny nose; low-grade fever (generally minimal throughout the course of the disease); and mild, occasional cough. Because pertussis in its early stages appears to be nothing more than the common cold, it is often not suspected or diagnosed until the more severe symptoms appear. Infected people are most contagious up to about two weeks after the cough begins. Antibiotics may shorten the amount of time someone is contagious.
“Would You Know Pertussis?”Hear how the cough may sound at: http://www.cdc.gov/pertussis/materials/everyone.html#pertussis-sounds. It is important to know that not everyone with pertussis coughs or "whoops."
As the disease progresses, the traditional symptoms of pertussis appear and include: Paroxysms (fits) of many, rapid coughs followed by a high-pitched "whoop"; vomiting; and exhaustion after coughing fits. The coughing fits can go on for up to ten weeks or more. In China, pertussis is known as the "100-day cough."
Although you are often exhausted after a coughing fit, you usually appear fairly well in-between. Coughing fits generally become more common and severe as the illness continues and can occur more often at night. The illness can be milder (less severe), and the typical "whoop" absent in children, teens, and adults who have been vaccinated with a pertussis vaccine. Recovery from pertussis can happen slowly. The cough becomes less severe and less common. However, coughing fits can return with other respiratory infections for many months after pertussis started. (Retrieved from: http://www.cdc.gov/pertussis/about/signs-symptoms.html. Accessed March 28, 2014.)
Pertussis (whooping cough) can cause serious and sometimes life-threatening complications in infants and young children, especially those who are not fully vaccinated. In infants younger than one year of

STUDENT CASE STUDY—SINGER-FREEMAN
age who get pertussis, about half are hospitalized. The younger the infant, the more likely treatment in the hospital will be needed. Of those infants who are hospitalized with pertussis about:
1 in 4 (23%) get pneumonia (lung infection) 1 or 2 in 100 (1.6 %) will have convulsions (violent, uncontrolled shaking) Two-thirds (67%) will have apnea (slowed or stopped breathing) 1 in 300 (0.4%) will have encephalopathy (disease of the brain) 1 or 2 in 100 (1.6%) will die
The photograph above shows an infant being treated for severe pertussis infection. She received extracorporeal membrane oxygenation (ECMO), a procedure that can take over the work of the lungs and heart. She also received dialysis to help her kidneys keep working. (Retrieved from: http://www.cdc.gov/pertussis/about/photos.html. Accessed March 28, 2014.)
Teens and adults can also get complications from pertussis. They are usually less serious in this older age group, especially in those who have been vaccinated with a pertussis vaccine. Complications in teens and adults are often caused by the cough itself. For example, you may pass out or fracture a rib during violent coughing fits. In one study, less than five percent of teens and adults with pertussis were hospitalized. Pneumonia (lung infection) was diagnosed in two percent of those patients. The most common complications in another study of adults with pertussis were: weight loss (33%), loss of bladder control (28%), passing out (6%), and rib fractures from severe coughing (4%). (Retrieved from: http://www.cdc.gov/pertussis/about/complications.html Accessed March 28, 2014.)