asco 2016 gu review
TRANSCRIPT
ASCO 2016 GU review JonathanRosenberg,MDAssociateAttendingPhysicianEnnoErcklentzChairGenitourinaryOncologyService

Prostate cancer • #5005and5006:Initialchemotherapyinprostatecancer
• #5008:Dosingofcabazitaxel2ndline• #5004:QOLonCHAARTED• #5001:AdjuvanttherapyafterRP• #5009:GermlinefindingsinCRPC
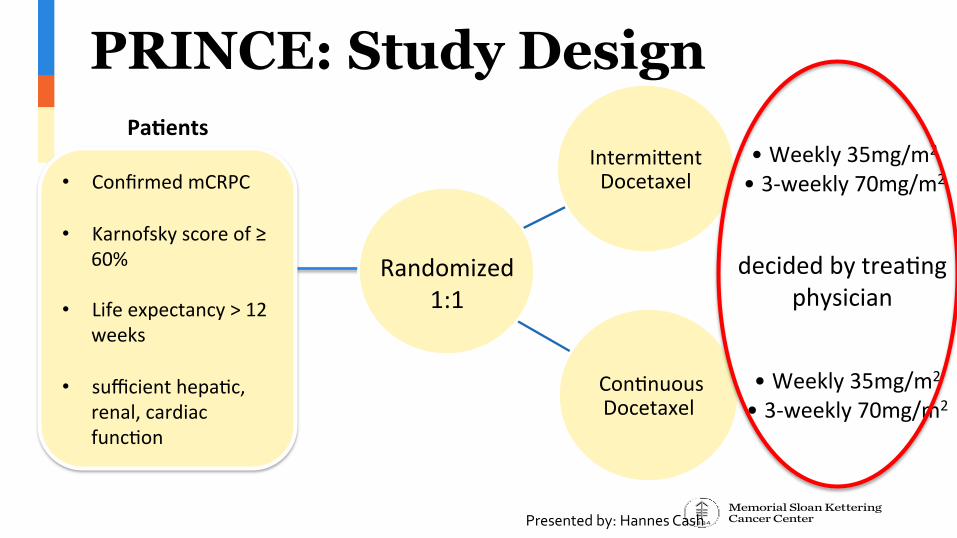
PRINCE: Study Design
Intermi(entDocetaxel
• Weekly35mg/m2• 3-weekly70mg/m2
Con>nuousDocetaxel
• Weekly35mg/m2• 3-weekly70mg/m2
Randomized1:1
Pa#ents
decidedbytrea>ngphysician
• ConfirmedmCRPC
• Karnofskyscoreof≥60%
• Lifeexpectancy>12weeks
• sufficienthepa>c,renal,cardiacfunc>on
Presentedby:HannesCash

PRINCE: Study Design Intermittent Docetaxel
12 week sequence 3-weekly: 4 cycles Weekly: 3 cycles
Treatment Holiday until disease progression
Intermittent Docetaxel
12 week sequence 3-weekly: 4 cycles Weekly: 3 cycles
DiseaseProgression:50%PSAincrease(atleast>4ng/ml)ofPSAnadira2ercon#nuingdocetaxelRadiologicalprogression(RECIST)Symptoma>cprogression
Presentedby:HannesCash

Study Objectives Primaryoutcomemeasures:• One-yearoverallsurvivalPrimaryhypothesis
• Non-inferiorityanalysisofintermittentvs.continuoustreatment
Presentedby:HannesCash

Poor enrollment • Expectedpatientnumber:424with247events
• Expectedpower:80%at1-sided97.5%CI
• Poorrecruitment:187(<45%ofplanned)patientsrandomizedbetweenAugust2005andMay2008
• IncludedinITT-Analysis:156patients,91events• Achievedpower:39%
Presentedby:HannesCash
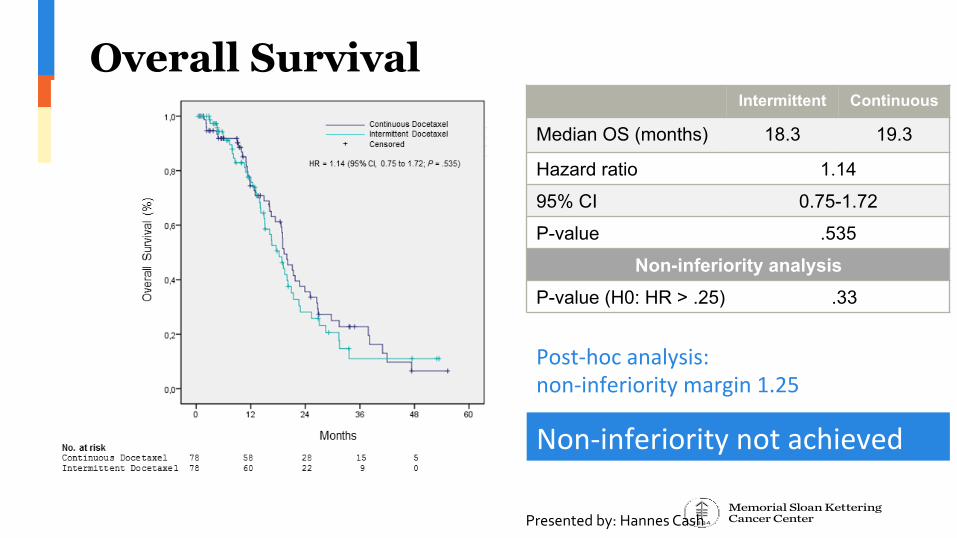
Overall Survival Intermittent Continuous
Median OS (months) 18.3 19.3
Hazard ratio 1.14
95% CI 0.75-1.72
P-value .535
Non-inferiority analysis P-value (H0: HR > .25) .33
Post-hocanalysis:non-inferioritymargin1.25
Non-inferioritynotachieved
Presentedby:HannesCash
Summary: Intermittent Docetaxel
• Outcomes:– Non-inferiorityat1-yearsurvival– Non-inferioritynotachievedforOS– Nodifferencesintoxicity– NoQoLdata
• Significantlyunderpoweredtodrawconclusions• However,peoplearedoingthisintherealworldandfinditavalidmanagementstrategy
Presentedby:HannesCash


Presentedby:
Docetaxelremainsfront-linestandard
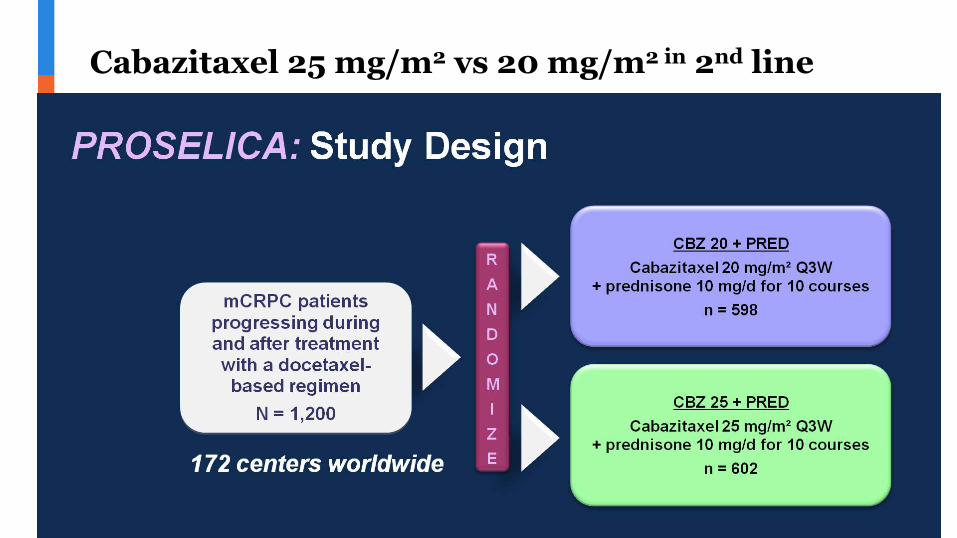
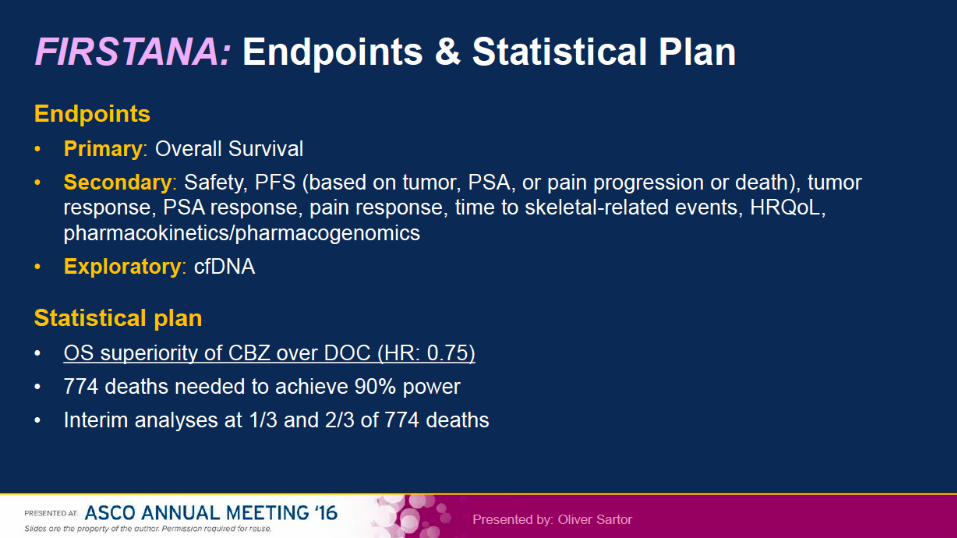
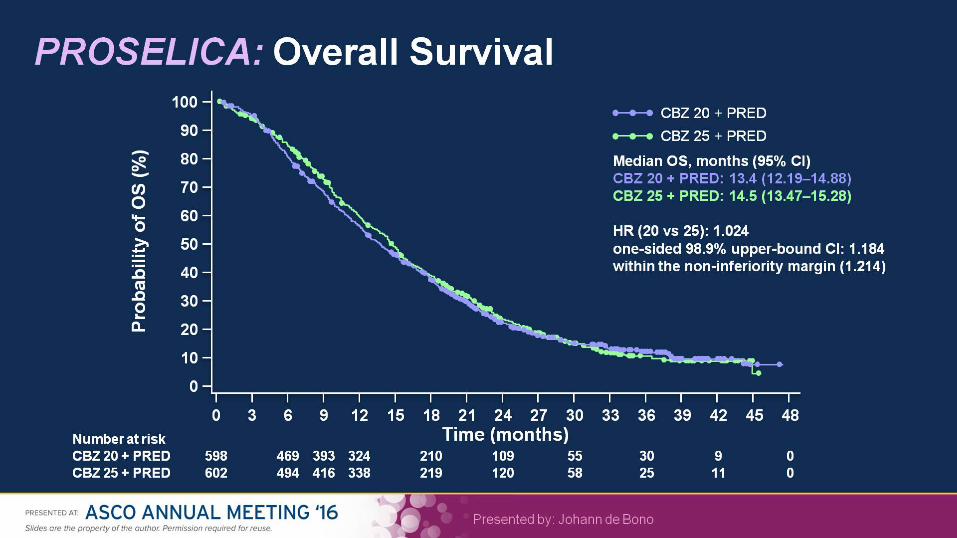
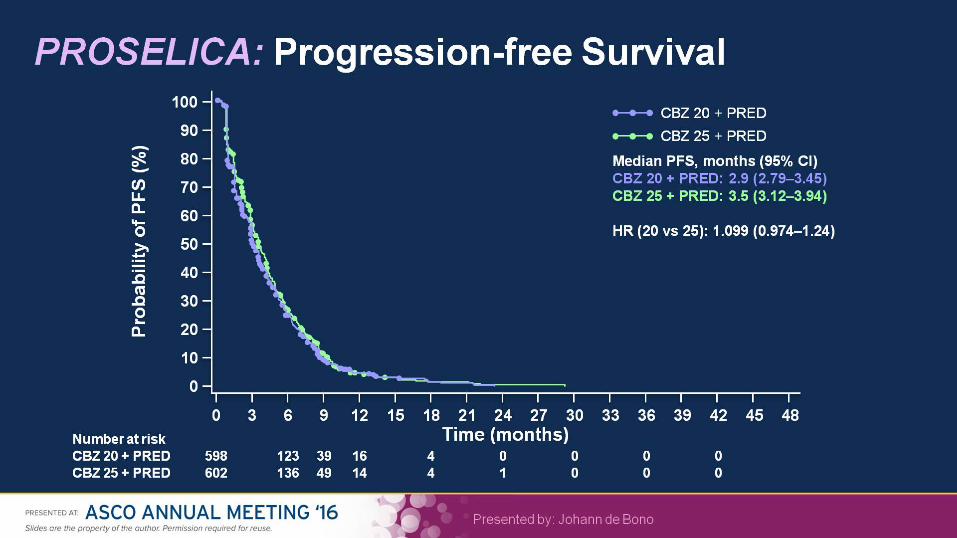
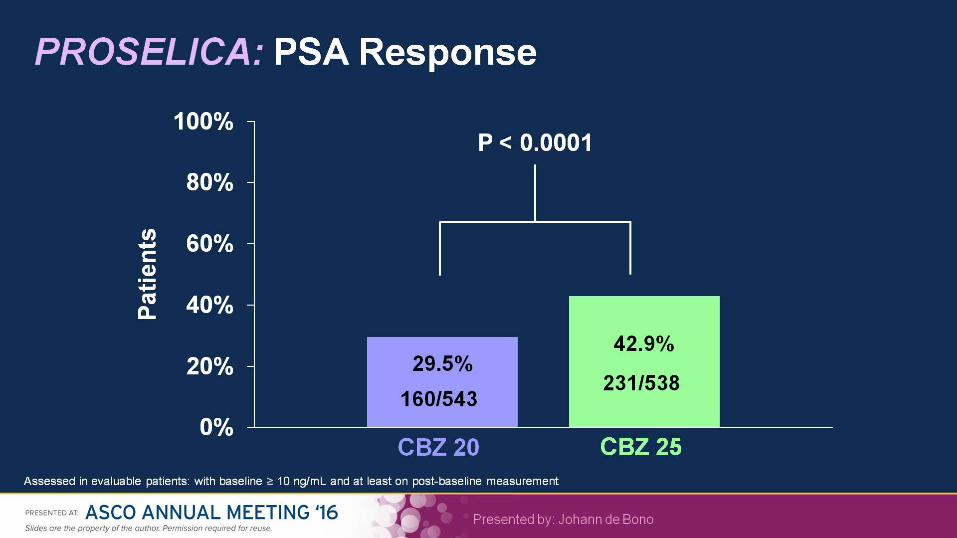
Cabazitaxel 25 mg/m2 vs 20 mg/m2 in 2nd line



Cabazitaxel in prostate cancer
• Dosereductionin2nd-linesettingdoesnotworsenoutcomes
• Front-linetherapywithdocetaxelremainsstandard
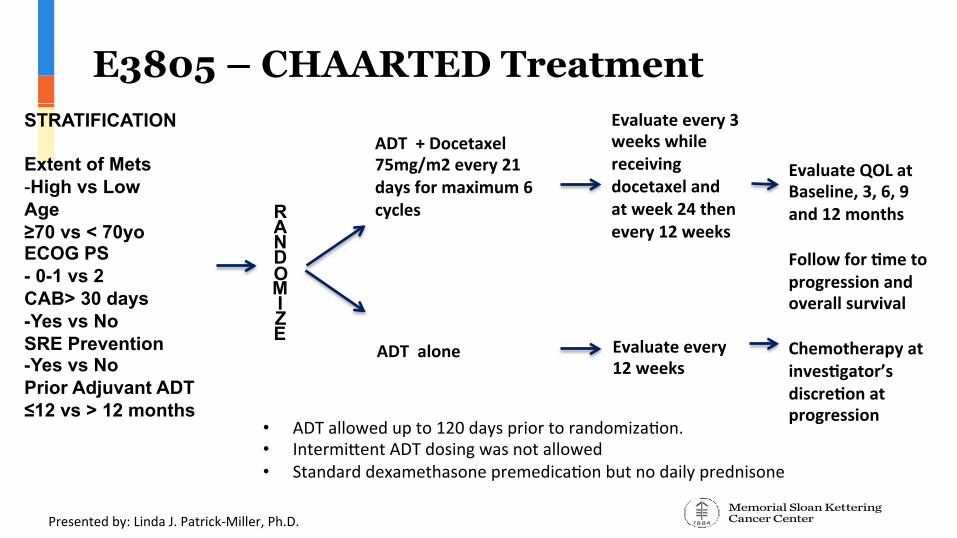
E3805 – CHAARTED Treatment STRATIFICATION Extent of Mets - High vs Low Age ≥70 vs < 70yo ECOG PS - 0-1 vs 2 CAB> 30 days -Yes vs No SRE Prevention -Yes vs No Prior Adjuvant ADT ≤12 vs > 12 months
RANDOMIZE
ADT+Docetaxel75mg/m2every21daysformaximum6cycles
ADTalone
Evaluateevery3weekswhilereceivingdocetaxelandatweek24thenevery12weeks
Evaluateevery12weeks
EvaluateQOLatBaseline,3,6,9and12monthsFollowfor#metoprogressionandoverallsurvivalChemotherapyatinves#gator’sdiscre#onatprogression
Presentedby:LindaJ.Patrick-Miller,Ph.D.
• ADTallowedupto120dayspriortorandomiza>on.• Intermi(entADTdosingwasnotallowed• Standarddexamethasonepremedica>onbutnodailyprednisone
QOL Endpoints • PrimaryEndpoint:OverallQOL
– FunctionalAssessmentofCancerTherapy-Prostate(FACT-P).Self-reportmeasureofgeneralanddisease-specificqualityoflife8.Thesumof5subscales:
1 Physical2 Social3 Emotional4 Functionalwell-being5 Concernsspecifictoprostatecancer
• HigherscoresindicatebetterQOL.
Presentedby:LindaPatrick-Miller,Ph.D.
8Esper,P.etal.AdultUrology,1997.
Overall QOL • Patientstreatedwithdocetaxel+ADTreportadecrementinoverallQOL(FACT-P)whileontreatment
• HOWEVER:QOLreturnstobaselineat12months:significantlybetterthanpatientstreatedwithADTalone
• SupportschangeinpracticebasedonSTAMPEDEandCHAARTED
• Clinicalbenefitdemonstrated,nowsupportedbyQOLdata• Docetaxelx6+ADTisastandardofcare
Presentedby:LindaPatrick-Miller,Ph.D.
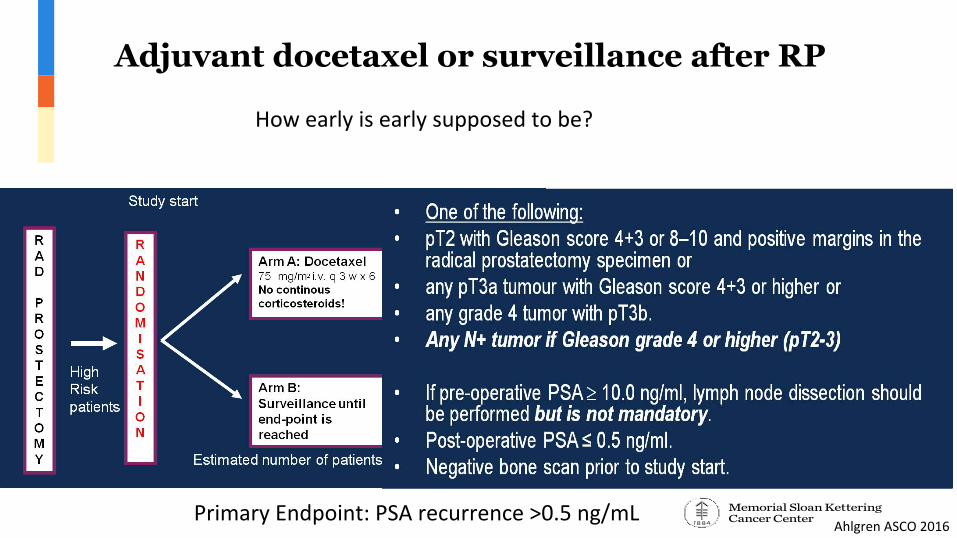
PrimaryEndpoint:PSArecurrence>0.5ng/mL
Adjuvant docetaxel or surveillance after RP
AhlgrenASCO2016
Howearlyisearlysupposedtobe?

Adjuvant docetaxel (no steroids) does not improve bPFS: No role at this time
Twiceasmanydeathsinthedocetaxelarm(6vs3)
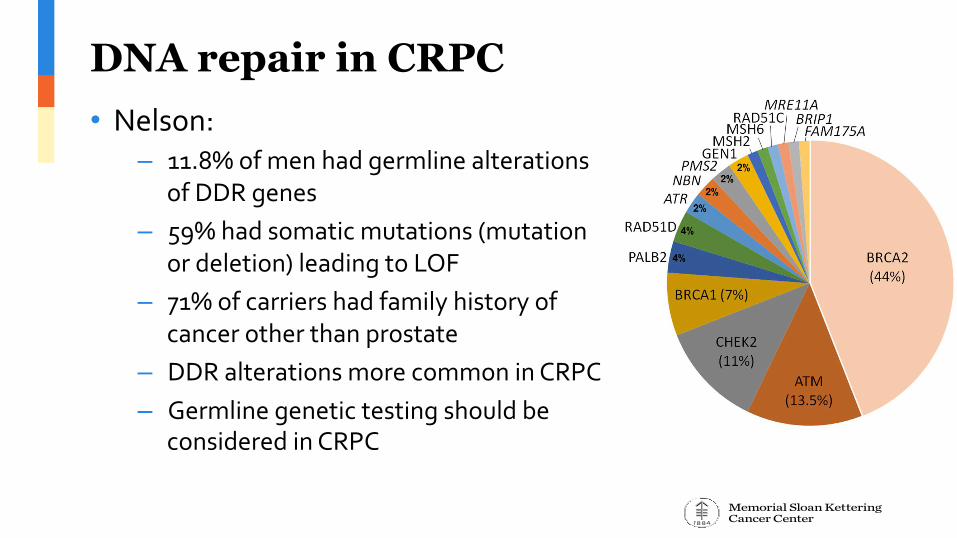
DNA repair in CRPC • Nelson:
– 11.8%ofmenhadgermlinealterationsofDDRgenes
– 59%hadsomaticmutations(mutationordeletion)leadingtoLOF
– 71%ofcarriershadfamilyhistoryofcancerotherthanprostate
– DDRalterationsmorecommoninCRPC– Germlinegenetictestingshouldbe
consideredinCRPC
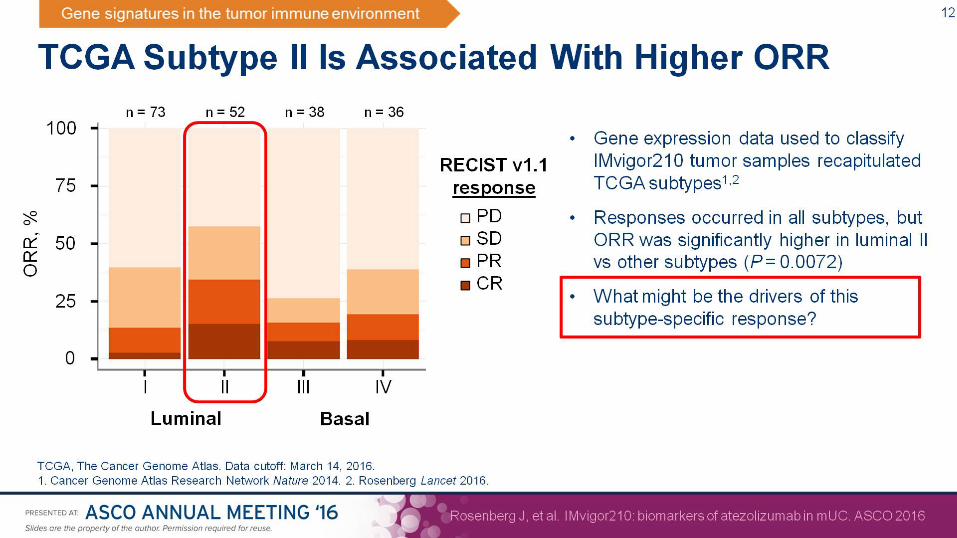
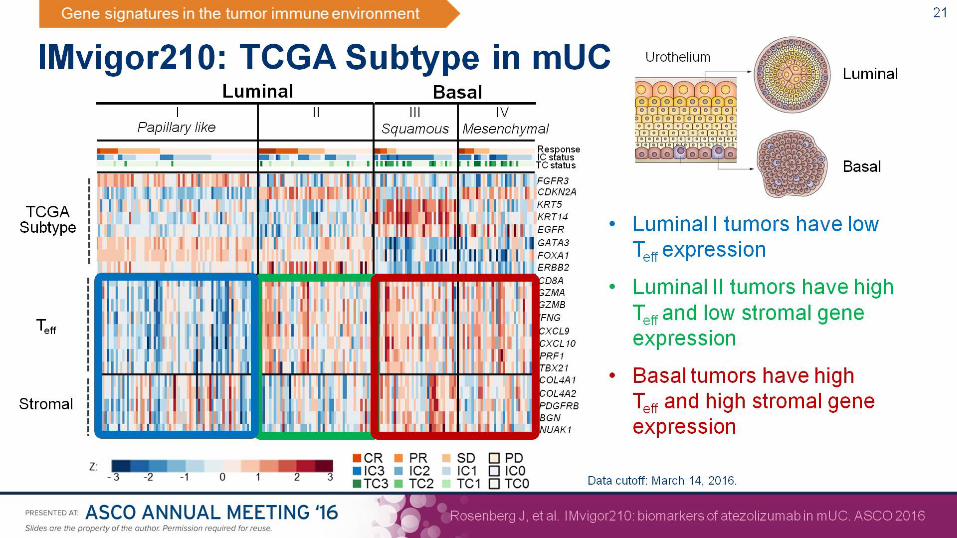
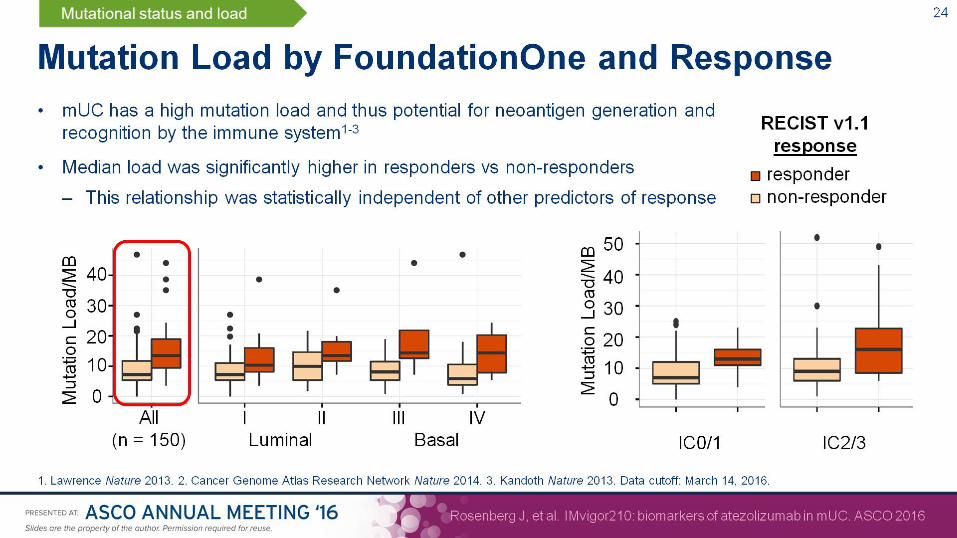
Bladder cancer • #4502:DurvalumabphaseI• #4501:NivolumabphaseI/II• #LBA4500Atezolizumab1stline• #4515Atezolizumab2ndline• #104Atezolizumabbiomarkers• #5011DDRgenealterationsandcisplatinresponse
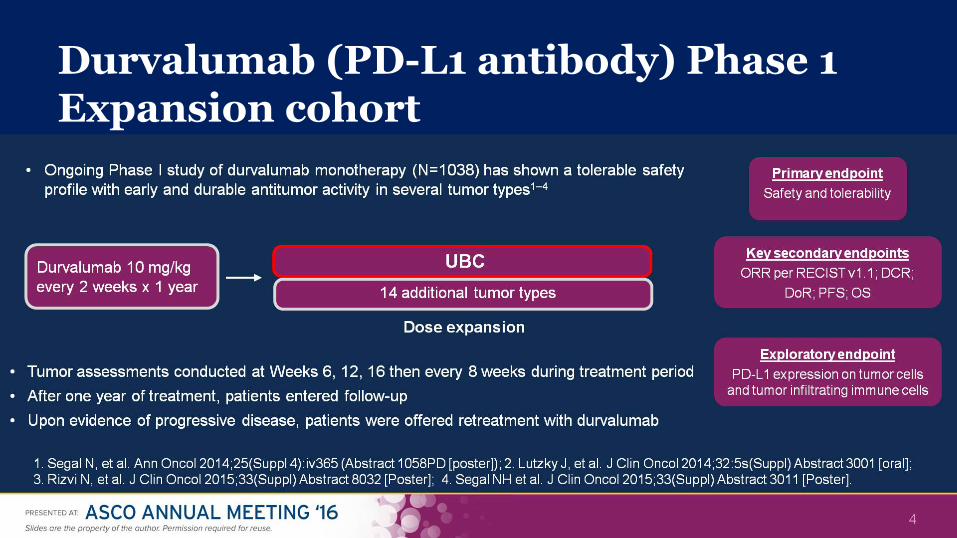
Durvalumab (PD-L1 antibody) Phase 1 Expansion cohort
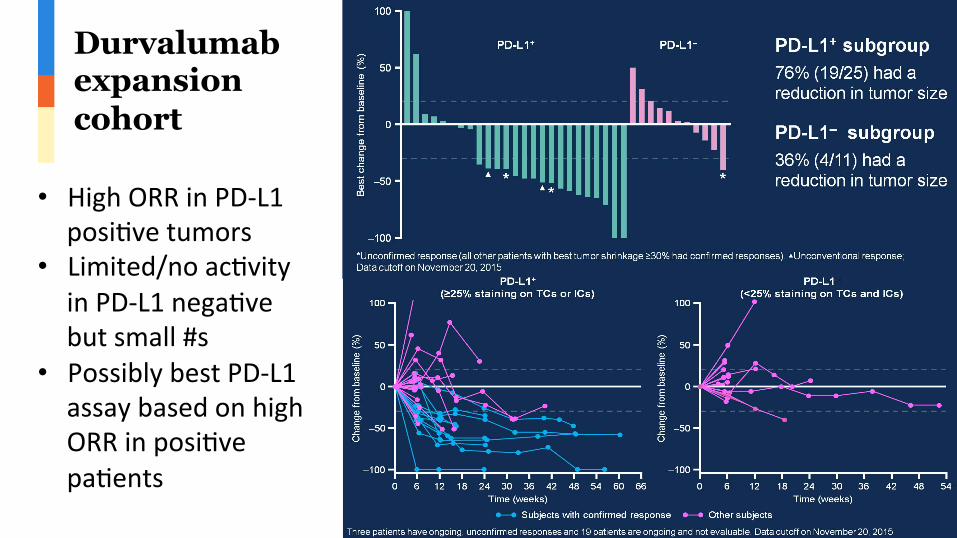
Durvalumab expansion cohort
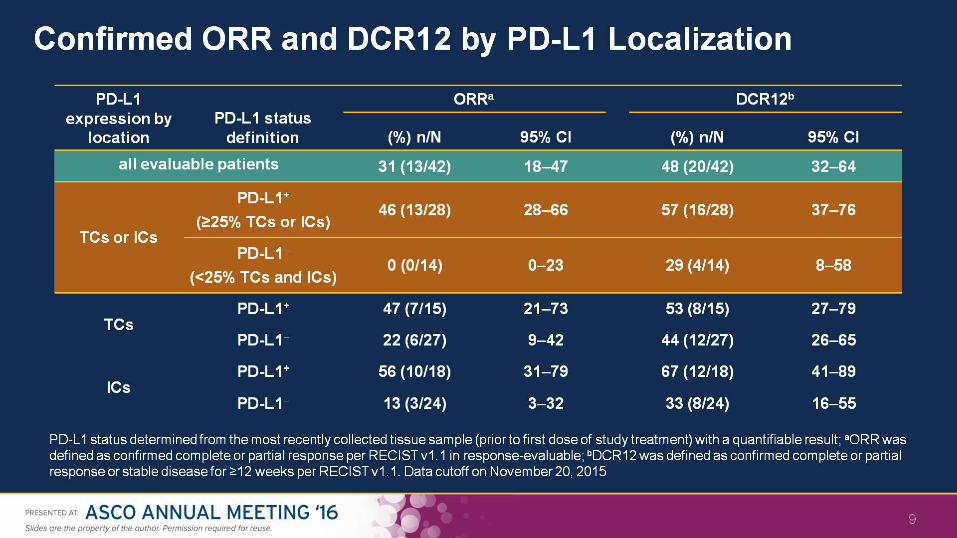
• HighORRinPD-L1posi>vetumors
• Limited/noac>vityinPD-L1nega>vebutsmall#s
• PossiblybestPD-L1assaybasedonhighORRinposi>vepa>ents

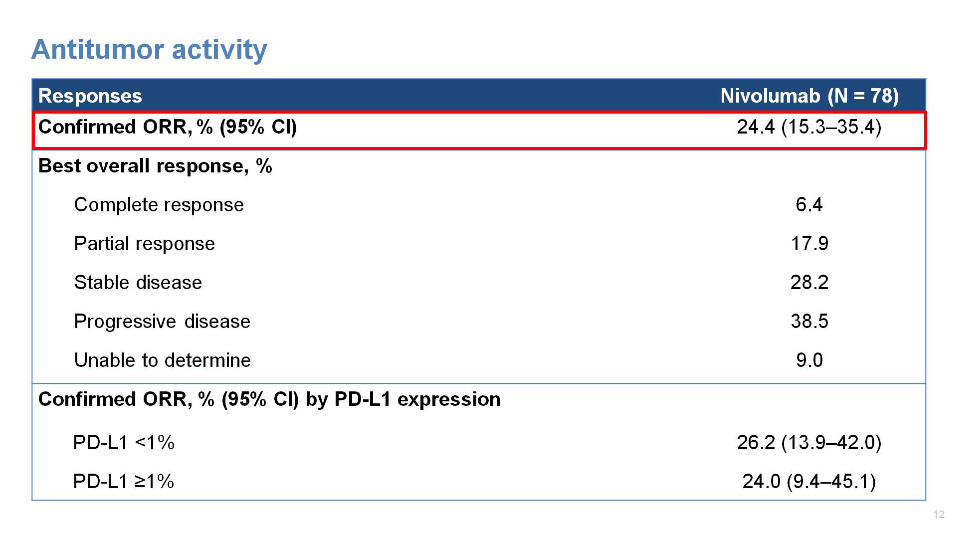
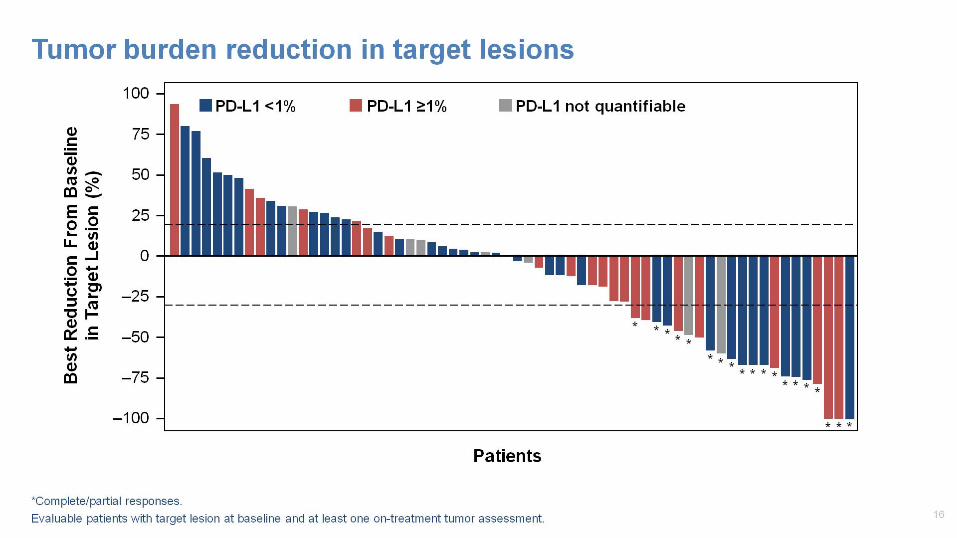
Nivolumab in urothelial carcinoma
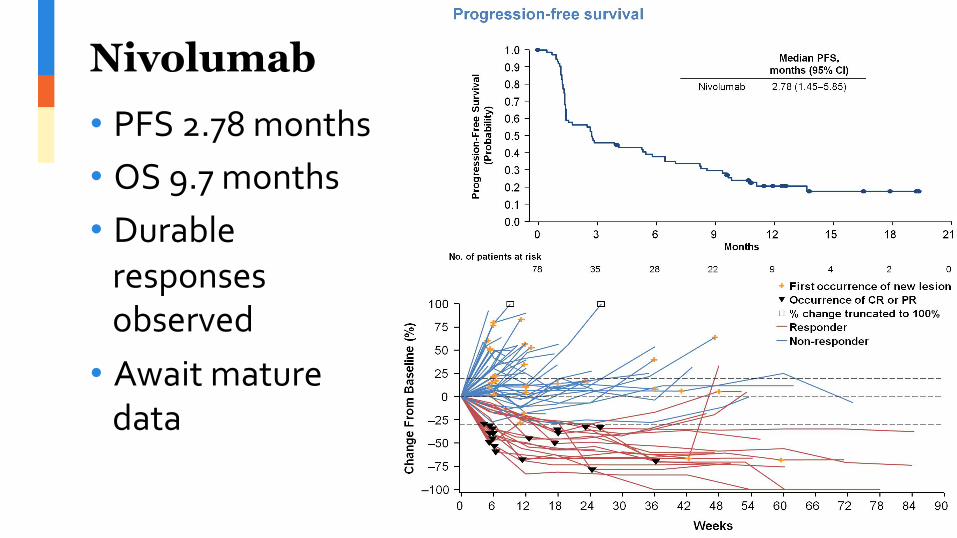
Nivolumab • PFS2.78months• OS9.7months• Durableresponsesobserved
• Awaitmaturedata

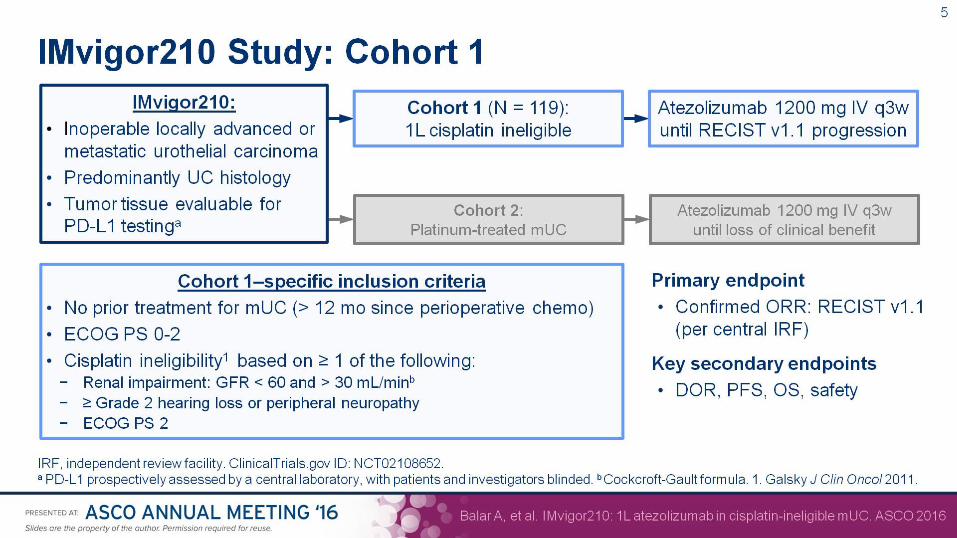
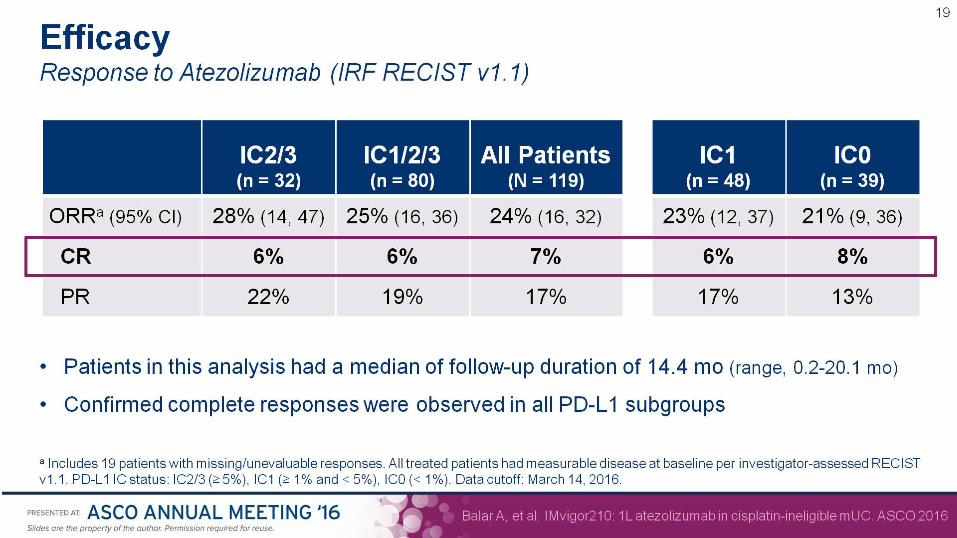
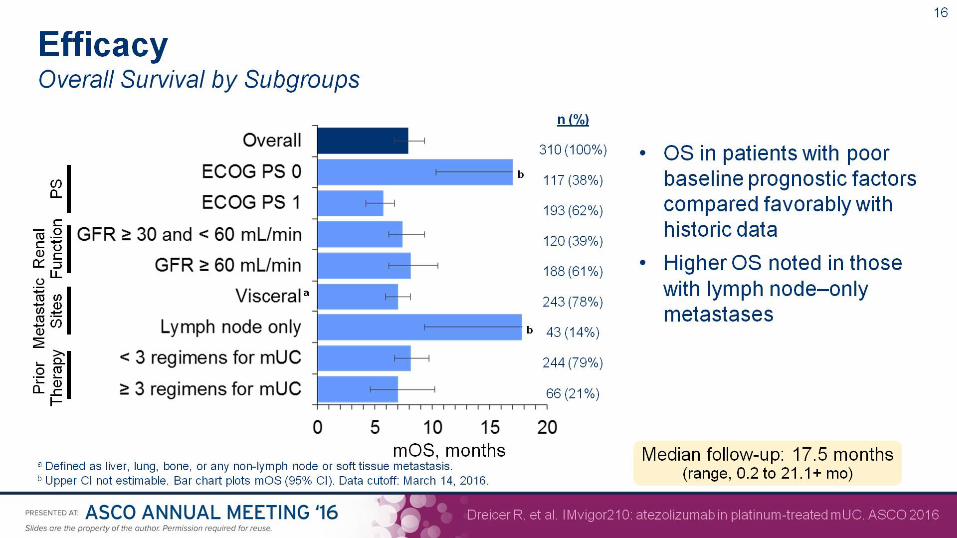
Atezolizumab in cisplatin-ineligible bladder cancer • No“standard”thoughgemcitabineandcarboplatiniscommunitystandard
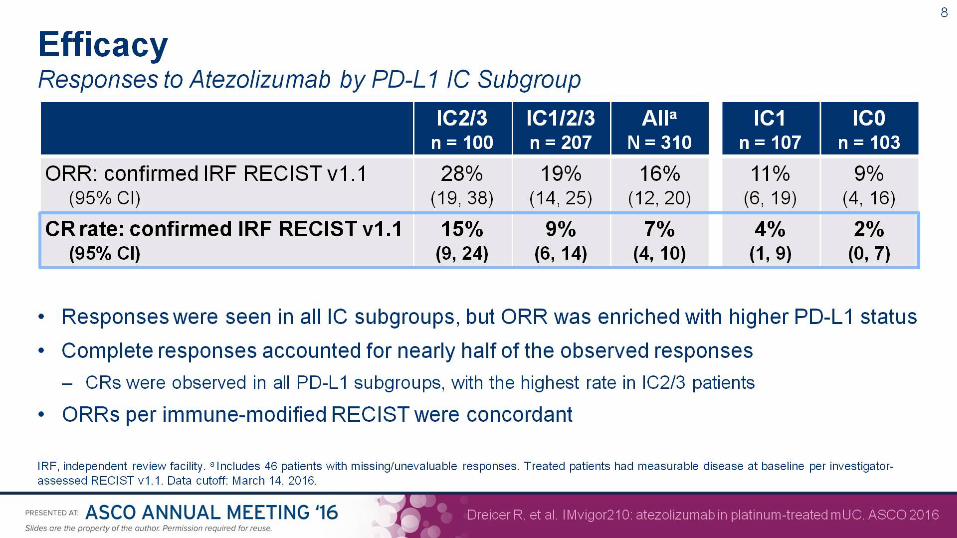
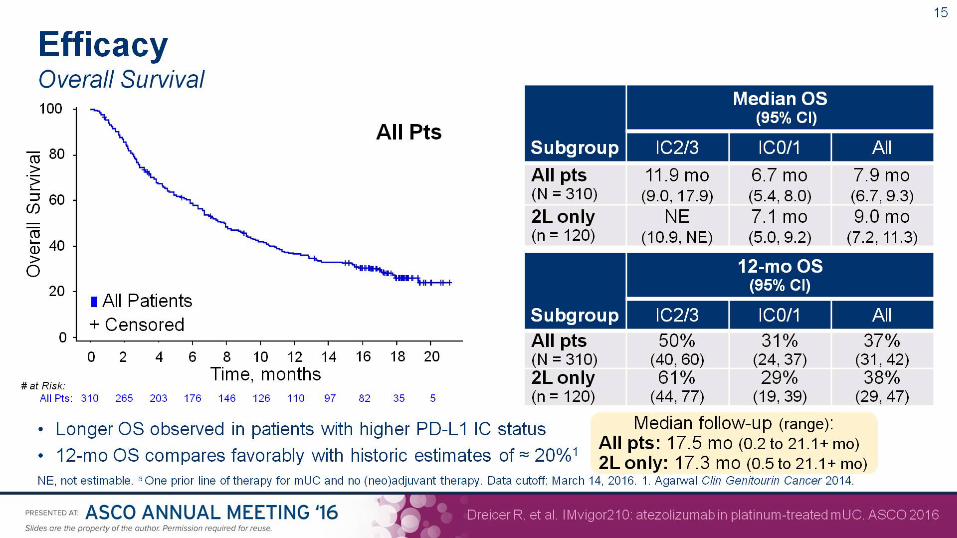
• MedianOS9.3monthsinphaseIIItesting• AtezolizumabisfirstFDA-approvedPD-L1inhibitor
– Approvedforlocallyadvancedormetastaticurothelialcarcinomapreviouslytreatedwithplatinum-basedchemotherapy






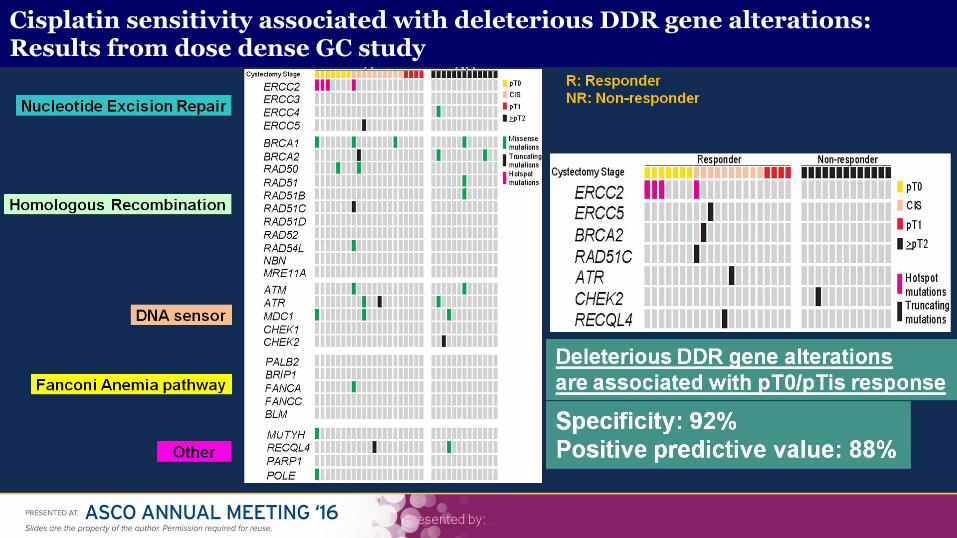
Cisplatin sensitivity associated with deleterious DDR gene alterations: Results from dose dense GC study

Kidney cancer
• #4506:OverallSurvivalwithcabozantinibvs.everolimus
• #4507:Long-termsurvivalwithnivolumabphaseIandIIstudies
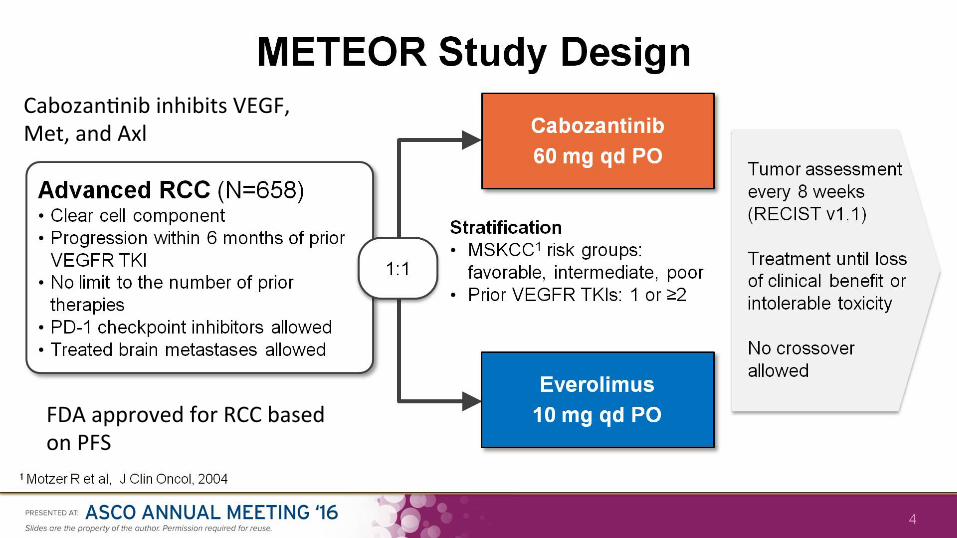
Cabozan>nibinhibitsVEGF,Met,andAxl
FDAapprovedforRCCbasedonPFS


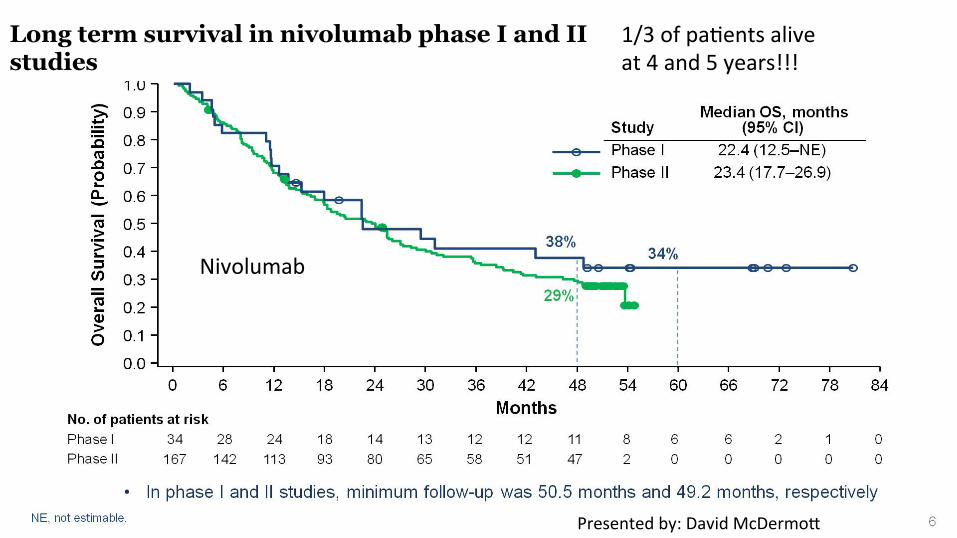
Nivolumab
1/3ofpa>entsaliveat4and5years!!!
Long term survival in nivolumab phase I and II studies
Presentedby:DavidMcDermo(
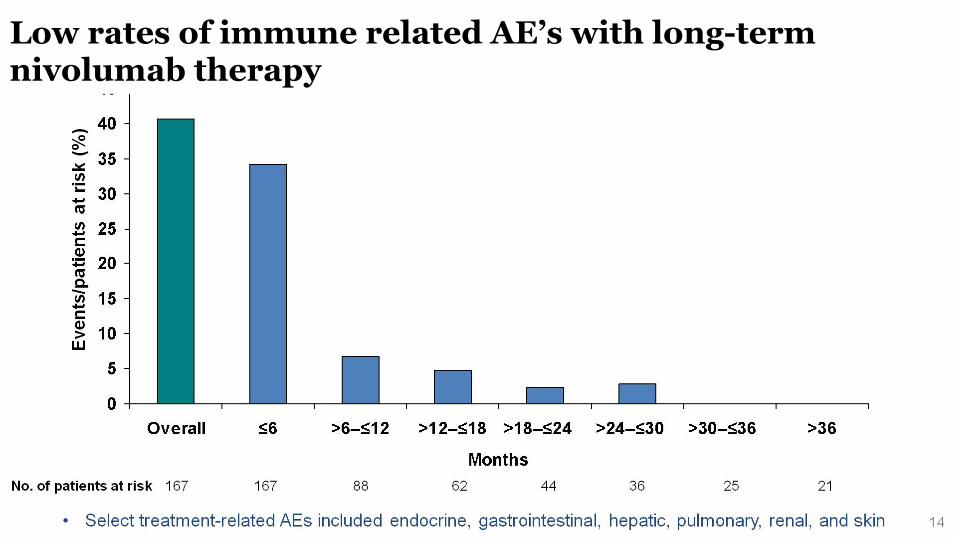
Low rates of immune related AE’s with long-term nivolumab therapy

Take-home points: Kidney • CabozantinibhasOSimprovement2nd-linesetting
– PFSadvantageinfront-linesetting(Cabo-SunAlliancetrial)
• Wenowhave5yearsurvivaldataforRCCthatisunprecedented
– 10drugs(plusIL-2)approvedforccRCCallowingsequentialtherapytoprolonglife

Sehng Paradigm1 Paradigm2
First-line,suitableforTKI
Suni>nibor
Pazopanib
Suni>nibor
Pazopanib
Second-line Nivolumab
Axi>nib,Cabozan>niborLenva>nib+Everolimus
Third-line Axi>nib,Cabozan>nib
orLenva>nib+Everolimus
Nivolumab
Treatment Paradigm for Most Clear-cell mRCC Patients

Acknowledgments
• RobDreicer• OliverSartor• JoaquimBellmunt• BobMotzer