aseptic technique infection control
TRANSCRIPT
Aseptic technique: evidence-basedapproach for patient safety
AbstractThe fact that there is a relationship between the standards of aseptic techniqueperformance and the rise in hospital infection rates has heen suggested by theDepartment of Heath's (DoH's, 2004) Winning Ways document. This literature reviewconsiders how the aseptic technique is performed in the UK, and examines the natureof ritualistic and evidence-based practice underpinning this skill-based procedure.The findings have identified an emerging glove culture and continuing poorhand-hygiene practices. The alternative 'clean technique' is also adopted widely inclinical practice which confuses the aseptic theory-practice gap. While it is hard topinpoint an actual time or event that causes infection, it is unlikely nurses will everbecome involved in litigation as a result of a poorly performed aseptic technique.However, the review concludes that nurses should not become too complacent. It brieflyconsiders how performance of the aseptic technique can be improved, through creativeeducational strategy, applied risk assessment and clinical audits of nurses' practices.Key words: • Infection control • Nursing: role • Patients: welfare
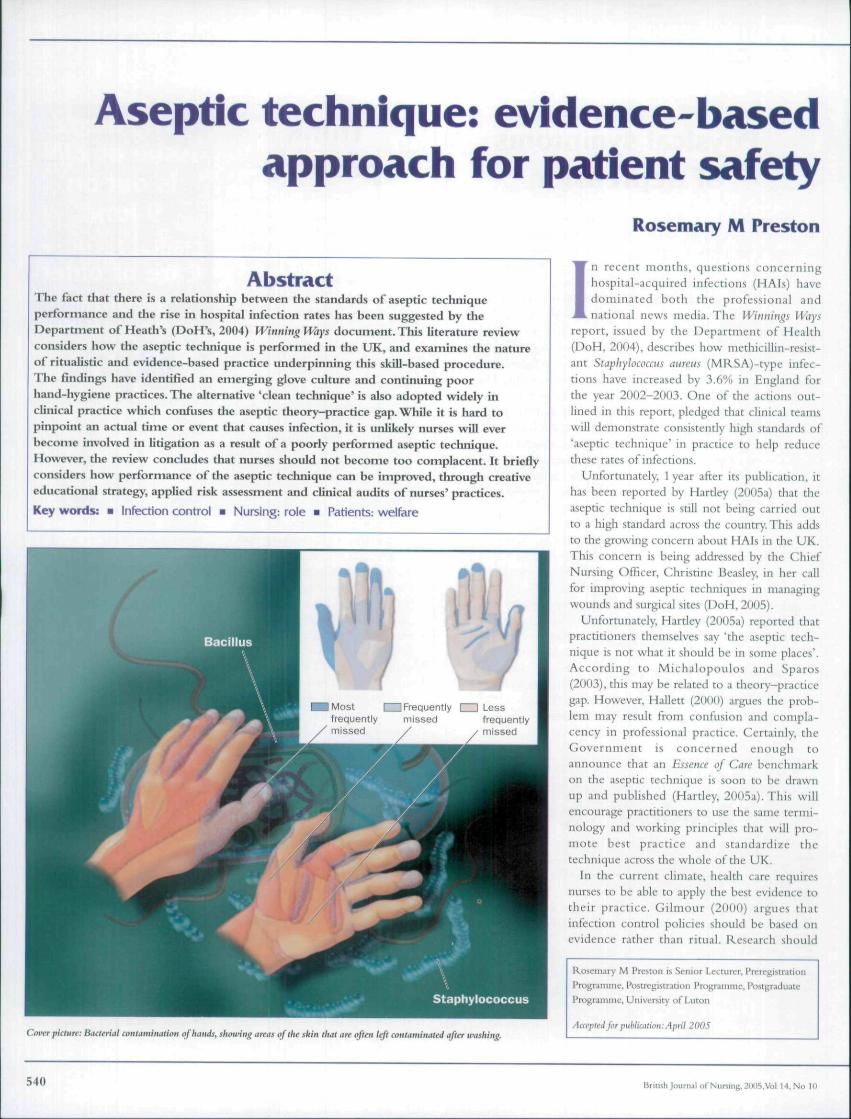
Most I I Frequently I I Lessfrequently missed frequentlymissed / ^ missed
Rosemary M Preston
I n recent months, questions concerninghospital-acquired infections (HAIs) havedominated boEh the professional andnational news media. The Witniings Ways
report, issued by the Department of Health(DoH, 2004), describes how methicillin-resist-ant Sfaphylococcus atireus {MRSA)-type infec-tions have increased by 3.6% in England forthe year 2002-2003. One of the actions out-lined in this report, pledged that clinical teamswill demonstrate consistently high standards of'aseptic technique' in practice to help reducethese rates of infections.
Unfortunately, 1 year after its publication, ithas been reported by Hartley (2()05a} that theaseptic technique is still not being carried outto a high standard across the country, This addsto the growing concern about HAIs in the UK.This concern is being addressed by the ChiefNursing Officer, Christine Beasley, in her callfor improving aseptic techniques in managingwounds and surgical sites (DoH, 2005).
Unfortunately, Hartley {2005a) reported thatpractitioners themselves say 'the aseptic tech-nique is not what it should be in some places'.According to Michalopoulos and Sparos(2003), this may be related to a theory-practicegap. However, Hallett (2000) argues the prob-lem may result from confusion and compla-cency in professional practice. Certainly, theGovernment is concerned enough toannounce that an Essence of Care benchmarkon the aseptic technique is soon to be drawnup and published (Hartley, 2005a). This willencourage practitioners to use the same termi-nology and working principles that will pro-mote best practice and standardize thetechnique across the whole of the UK.
In the current climate, health care requiresnurses to be able to apply the best evidence totheir practice. Gilmour (2000) argues thatinfection control policies should be based onevidence rather than ritual. Research shoiiki
Cover piclure: Bacterial contamination of hands, showing areas of the skin that an often left contaminated after washing.
Roseniary M Preston i Senior Lecturer. Prerej;! strati onProgramme, Postregistrarion Prtigramme, PostgraduateProgramme. Univtrsity of Liicon
Aat'ptfii for piihliiittion: April 2005
540 British Joum.ii of Nuning. 211(15.Vo! 14, No in

INFECTION CONTROL NURSING
promote the practice of risk assessment tominimize the incidence of cross-infection.However, if general principles of asepsis are notbeing practised to a high enough standard(Hartley, 2nO5a), is there evidence to suggestwhy this might be happening? This review ofthe literature examines ritualistic and evi-dence-based practice in relation to the educa-tion and practice of the aseptic technique, aswell as its impHcations for patient safety.
Principles of the 'aseptic technique'The aim of the aseptic technique is to preventthe transmission of microorganisms to wounds,or other susceptible sites, to reduce the risk ofinfection (Bree-Williams and Waterman, 1996;Xavier, 1999). However, pathogenic microhialcontamination continues to be identified as aproblem when practitioners carry out aseptic-type procedures (Ward, 2(){H); Michalopoulosand Sparos, 2UU3; Myatt and Langley, 2003). Ina survey conducted in two major hospitals \nGreece, nurses demonstrated a sound knowl-edge of the aseptic principle when questioned.but 15.6% of nurses were found to have con-taminated their hands during the procedure(Michalopouios aiid Sparos, 2003).
Bree-Williams and Waterman (1996) andHailett (2000) have both observed that a failureto use the aseptic technique correcdy could heresponsible for problematic and intractable infec-tions such as MRSA. For example, Bree-Williams and Waterman (1996), in theirobservational study, found that 33% of nursescontaminated their hands and equipment duringthe aseptic tachnique procedure. This was foundto be a result of a number of factors, rangingfrom making the procedure more complicatedthan required, to poor skill in handwashing,glove technique and use of non-touch principlesin handling sterile equipment and instruments.
In assessing attitudes towards the aseptictechnique, Hailett (2000) found that nurses dis-cussed the concept of aseptic technique in'fatalistic' terms. This was a small qualitativestudy involving community nurses, whoexpressed a belief that 'asepsis' was virtuallyimpossible to achieve in reality. While thisresult may only have significance in a commu-nity setting, Hatlet (2000) was concernedabout the degree of ambivalence and uncer-tainty around infection control in wound care,particularly as it could be related to how prac-titioners are originally taught the aseptic tech-nique, combined with a failure to adopt newskills and techniques safely as they emerge inprofessional practice. As Hailett (2000) con-cluded, if there is no research evidence to sup-port the aseptic procedure then it is not
surprising if the practice is becoming obsoletefor some nurses.
Therefore, is the aseptic technique alwaysnecessary? According to Gilmour (2000) andWeaver (2004), performing an aseptic tech-nique requires sterile equipment, gloves andfluids, and 'non-touch' actions of the nurse.This will help to minimize spread of potentialpathogens to other sites, wounds or selt. It isalso important for nurses to be able to accountfor their actions at all times. This means beingable to demonstrate a sound knowledge andpractice in maintaining a sterile field(Gilmour. 1999; Xavier, 1999; Nursing andMidwifery Council (NMC). 2002; Weaver,
political factors that may impinge on theireveryday working environments and expectedworking practices.
Teaching clean technique vs aseptictechnique?Over the past 10 years, a move tovrards a cleantechnique has heen identified (Gilmour, 1999;Williams, 1999; Michalopoulos and Sparas, 2(K)3).A clean technique adopts the same aims as theaseptic technique but uses clean rather than sterilegloves. It is also less ritualistic and relies on lesshand-washing intraprocedure, but continues toutilize sterile equipment and fluids as appropriatefor individual patients' needs (Gilmour. 2000).
Table 1. Exercising universal principles when performing an aseptic technique forwound care
Assess risks of cross infection and sele^T^ja&^snd size of sterile gloves needed
Don a clean apron LWash hands at start of procedure and a^ny time contamination occursOpen, dispense and transfer sterile equipment and fluids without contaminating themRemove soiled dressing if present with hand gloved in sterile waste bagTurn the bag inside out without contaminating your hands and continue to use for waste items
Apply sterile gloves as per Table 3 guidelinesAssess, cleanse if needed, and re-apply new dressingUse non-touch actions when manipulating gauze swabs or irrigation, to avoid contaminating gloved hands.the patients other susceptible sites, bed or general environmentRemove gloves from hands using guidelines from Table 3Discard sterile field and waste bag into yellow plastic sack without contaminating your handsRemove apron and discard into a yellow sackWash hands
Contominatedwaste Adapted from Baillie (2005}
2004). Gilmour (2000) goes on to argue thatdespite its ritualistic nature (of being a formalprocedure that is followed consistently), theaseptic technique {Table 1), is an effectiveinfection control strategy.
However, in an observational study ofhealthcare practitioners in two accident andemergency departments, Al-Damouk et al(2004) found that there was poor compliancewith good-practice guidelines for the aseptictechnique. This study was conducted in theUK and New Zealand and it showed UK doc-tors' rate of compliance to be as low as 27%.Although it was accepted that a compromise instandards of asepsis in very sick patients wouldbe likely to occur, this low figure contrastedsharply with New Zealand's doctors whoscored 58%. This result could imply that bothnurses and doctors in the UK may havebecome confused and complacent about theterm aseptic in their everyday practice. It mayalso be the result of the differences in howprofessional practitioners are trained in theUK, combined with other sociocultural and
Parker (2000) observed that the clean tech-nique was an alternative approach when dealingwith some chronic wounds using non-sterilesolutions such as tap water for irrigation {Riyatand Quinton, 1997; Hollinworth and Kingston,1998). Therefore, it must be asked whether thenurses in Hallett's study (2000) believed theywere doing the 'best they could' when adoptingthis alternative approach. For example, one F-grade sister in the study commented she 'didn'treally believe in this clean-aseptic procedure —she did the best she could'. This may be whyshe and her colleagues felt the aseptic techniquehad become virtually obsolete in their commu-nity practice. If so, it could be a reason whynurses in other practice areas are similarly con-fused about when to apply the clean or asepticapproaches for a range of'aseptic-type' proce-dures (Table 2).
Reinforcing aseptic techniquepracticesThe complex issues surrounding the acceptablestandard for performing the aseptic technique
British Journal ofNursmg,2IKJ5.Vol U. No Hi 541

L-ontinues to pose a challenge for all professionalhealthcare practitioners. Evidence-based practice(.'an be difficult to implement in infection con-trol as most professionals tend to base their prac-tice on experience or 'expert opinion' (Ward,2002). It is usual to find nurses and doctors whohave both a lack of knowledge of the evidence.ivaihble and an unwillingness to change theirbehaviour based on new evidence {Davey, 1997;Ward, 2()()(); Myatt and Langley, 2003).
The aseptic technique is one area of profes-sional practice in which ritual can be recog-nized from when to wash hands and dongloves, to opening the sterile packages, andperforming procedures such as care of intra-venous cannulae (Dougherty, 2000), or wound
Table 2. Clinical procedures requiringrisk assessment for an aseptictechnique approach
Redressing all acute woundsRedressing some chronic woundsUrinary cathetcrization '
Redressing dr.Injection of meaicaiion^nncludmg intravenous,intramuscular, subcutarjeous and intra-dermalroutes ^Instillation of eye dropsrBladder washouts/irrigjtionsBlood-glucose ;••!"•" ' • vVenepunctureCannulationCare of central Imas (including Hickman lines)
Ad Im Baillie (2005)
care (Wilson, 2003). Successive studies onwound care (Filetoth, 2003; Michalopoulosand Sparos. 2003). hand hygiene (Patel, 2004:Rickard. 2004) and glove use (Ross, 1999)Iiave been well reported in the last 5 years.
For example, botb Filetoth (2003) andMiclialopoulos ;tnd Sparos (2003) reported onthe need to improve aseptic technique practicein wound care to reduce the rates of woundinfection. In handwashing practices, both Patel(2004) and Rickard (2004) have reviewed thevarious factors which inhibit good handwashingtechniques and have otfered suggestions on howprofessionals can be helped to improve theirperformance. In glove selection and technique,Ross (1999) reported on an audit that identifiedthat practitioners were using gloves inappropri-ately and that latex sensitivity was becoming aproblem for healthcare workers. This report alsohighlighted the importance of risk assessmentfor glove use in the healthcare setting.
The motivation to look at research andexplore new methods to improve skill-basedcare is recognized to be a focus for ongoingpostregistration education (Ford and Koehler,2001; NMC, 2002; Preston, 2004). In maintain-ing good standards for the aseptic technique, thisshould involve revisiting the skills of handwash-ing, glove selection and technique, maintaining asterile field with use of non-touch principlesand developing risk-assessment protocols thatencompass safety issues for both the professionalpractitioner and patient (Bree-Williams andWaterman, 1996; Ford and Koehler et al, 2001;Michalopoulos and Sparos, 2003).
Learning to visualize 'mkrobialfallout*As suggested by Rickard (2004), one of thereasons for non-compliance in the aseptictechnique is because the individual cannot seethe microorganisms with the naked eye. Therelationship between contamination, coloniza-tion and infection is not easy for the averageprofessional to perceive in practice, and it cantake many days for an infection to develop(Wilson, 2003). This makes it harder to pin-point the actual time, occasion or event thatcaused the infection. To help overcome thislack of awareness in practice. Ford and Koehler(2001), for example, provided an educationalsession for their staff that used colourful pom-poms with parachutes to represent microbialfallout. This helped staff to realize the locationof contamination on their equipment, thepatient and their hands while performing theaseptic technique. Talcum powder or pillowfeathers have been used in a similar way.
Another visual aid useful for raising aware-ness of'microbial fallout' is to follow a 'simplehand-hygiene exercise' as reported by Aspockand Roller (1999). This involves using acreamy-coloured dye whicb is applied togloved hands and which are then washed withsoap and running water and dried using stan-dard paper towels. The aim is to see the distri-bution of dye on the gloves following thisbandwash procedure. Parts of the hands thatare frequently left contaminated with the soapydye (Griffiths, 2002) are the palms, betweenthe fingers and outer edge of the thumb. Thistype of exercise can allow practitioners torefine their handwashing technique to a higherstandard of performance.
Learning to wash hands effectivelyThe relationship between poor hand hygieneand infection risks has been well documented(Merchant, 2001; GrifFiths, 2002; Rickard,2004). Hartley (2005b) reported intensive care
unit (ICU) nurses would need to wash theirhands every 3 minutes to ensure patient safety.This was based on an observational study con-ducted at the University College LondonHospital and the Royal Free Hospital, London.This study identified 534 handwashing oppor-tunities in a 26-hour observation period, i.e. oneevery 3 minutes. It was interesting to note thatthe nurses scored a low 29% for handwash com-pliance for the total number of opportunitiesobserved.The findings also conveyed the impor-tance of washing hands when moving betweendifferent parts of the patient's body and ventila-tor, e.g. so that colonization and spread ofMRSA was kept to a minimum. Although ICUis a specialist area, the issue of handwashingtechniques, as well as timing and frequency, isoften viewed as the major causal link in HAIs(Dunford, 1997; Rotter, 2001; Weaver, 2(K)4).
In relation to the aseptic technique, effectivehandwashing practice is essential even if glovesare worn at some stage in the procedure. Swales(2003) identified that hands should be washedbefore and after wound care, and also afterremoval of gloves if worn. Pittet (2001) notesthat nurses often forget to do handwashing atthese times or devote too little time to washand dry their hands in an appropriate manner.
Bree-Williams and Waterman (1996) high-lighted that contamination of gloves occurredbecause hands were still wet when attempting toapply the gloves. Further, good quality soap, toweland wash-basin facilities continues to be a prob-lem in ensuring compliance (Hampton, 2003).
When undertaking handwashing as part ofthe aseptic procedure how many units still haveno "elbow* or foot-controlled taps? This meansnurses cannot safely mix hot and cold waterand turn the taps off without recontaminatingtheir washed hands. It would also be interestingto investigate if practitioners use the foot ped-als on waste bins or lift the bin hds with theirhands instead as this may pose a risk activityleading to higher rates of HAIs. Clearly, thereis a need for all practitioners to conduct riskassessments of the facihties they have available.Any concerns raised by practitioners, such asthe risks posed by poor design, should beheeded and action taken as a matter of highpriority in the healthcare setting.
Alcohol gelsThe use of hand gels and alcohol rubs are anadditional aid to promoting hand hygiene(Rickard, 2004).These have proved to be effec-tive in reducing the time it takes to effectdecontamination of the hands compared withusing soap, water and paper towels (Jones et al,2000; Bissett, 2002; Pittet, 2002; Patel, 2004).
542 British JoiirnjlofNiir5ing.2()0S,VDl 14, No

l^ickard (2004) discovered that in an average8-hour shift, nurses could spend a total of45mmLites, or 15% of their work activities,devoted to hand-hygiene practices. The use ofalcohol, waterless-base ruhs reduces the timespent on this activity.
However, inservice education emphasizes thatthese rubs are only effective on hands that haveno visible signs of sailing (Bissett, 2002; Patel,2004). Further, the efficacy of these rubs werequestioned by Kramer (2002), who found thatwhere the apphcation time was 8—16 seconds,this would increase the likelihood of cross-con-tamination. In this study, the researchers testedthe antimicrobial efficacy of If) gels and fourrinses on the contaminated hands of 15 volun-teers. This showed that a rub time of at least30 seconds is needed to meet acceptable stan-dards for successful hand decontamination.
Rickard (2004) also reported other reasonsfor poor hand decontamination. He high-lighted issues involving hoth complacency andavoidance factors related to skin problems,workload and lack of time, poor facilities andmaterials and disagreement with hospital pro-tocol and training regulations.
Traditionally, it has been accepted thatincreasing the amount of training and educationis the best strategy to take if compliance in handhygiene is to improve. Unfortunately, writerslike (lould (2000) have found that despite manyinnovative strategies being forwarded in educa-tional programmes, hand- hygiene behaviourcontinues to be poorly applied. As Rickard(2004) concludes, fliture strategies could involveempowering patients to question practitioners'hand-hygiene practice, improve hand-hygienefacilities, and create local ownership of anyproblems identified. These problems can beassessed locally through regular risk assessment,research, and feedback of infection rates.
Learning to select clean or sterilegloves using a risk-assessmentprotocolNurses are now expected to wear gloves for allprocedures to protect not only the patient, butalso themselves from infection (Hampton,2002; Yip and Cacioli, 2002). Unfortunately,this practice has promoted a distinct behav-ioural culture, where nurses use gloves inap-propriately for a number of tasks such asconducting clinical observations and assistingpatients with feeding, where risks to eitherpatients or themselves are not identified(Infection Control Nurses Association, 1999;Raybould. 2001). In the Health and SafetyCommission (1999) report. Control ofSubstances Hazardous to Health Regulations:
Table 3. Applying a safe glove technique
A. To don sterile gloves
Open outer glove wrapping without touching the gloves insideEnsure gloves are positioned in front of you:R -glove to your right and L- glove to your left with the fingers furthest away from your bodyPick up the edge of the cuff of the L-glove with your right thumb and index fingerLift the glove and insert the fingers of your left handPuli the cuff to the wrist of your left hand and release the left cuff edge smoothly, leaving the cuff of the glo\folded IPoint and insert fingers 2 5 of now gloved left hand into the folded cuff of the right gioveLift right glove from surface and insert fingers of right hand into the glove, taking care not to touch eithergloves sterile surfacesPuli the right glove over the right hand, and rotate folded cuff part over the right wrist as you so doInsert fingers 2 5 of now gloved right hand back into fold of left glove and rotate fold over the left wrist as yoso doAssess whether gloves were contaminated during their application and then proceed with procedure
B. To remove soiled gloves
Move to waste bag or a foot pedal binPick up the edge of the left glove sleeve on the wrist end with the thumb and index finger of your gloved righihandHook your third finger underneath and invert the glove as you gently pull off the left glove using your glovedright hand to control its drop into the waste bag/binInsert the thumb of your now ungloved left hand into the glove cuff on the right wristPeel right glove carefully down right hand inverting glove as you so doDrop glove into waste bag/binBoth gloves should be fully inverted (turned inside out) when discarded, if correct procedure is carried outDo not forget to wash your hands
Adapted from Aspock and Koller (1999)
Approifed Codes of Practice, it is suggested thatrisk assessment should follow specific guide-lines related to the barrier efficacy for the typeof gloves selected. Unfortunately, this is an areawhere the theory-practice gap is well docu-mented (Gould and Chamberlain, 1997;Curran, 2000; Rourke et al, 2001).
For example, Curran (2000) reported on rea-sons for an outbreak of the hepatitis B infec-tion in a group of patients who were alldiabetic. Practitioners were found to be usinggloves to protect themselves from blood-borneinfections when conducting blood glucosemonitoring. However, it was discovered thatthese practitioners had failed to understand therisk posed to their patients by not changingtheir gloves between each procedure. This washow successive diabetic patients were found tohave become infected.
In addition, Hampton (2002) has highlightedthe lack of understanding in relation to thehealth risk of developing latex sensitivity,assessing permeability (virus leaking) risks ofboth polyvinyl and latex gloves material, andrecognizing the high costs and wastageinvolved when using gloves inappropriately inthe healthcare setting.
In the case of acute wound care and urinarycatheterization, for example, Hampton andCollins (2002) and Haberstich (2002) advocatethat sterile gloves should always be worn.However, they also acknowledge that there aresome practice environments where the risk isassessed as low for some chronic wounds, suchas chronic leg ulcers when managed in thepatients' home, as well as other sterile proce-dures. Both O'Toole (1997) and Gottrup et al(2001) support this view of adapting the asep-tic procedure to a clean technique for these sit-uations and of using clean non-sterile glovesand sterile equipment and fluids (but includingtap water when applicable).
Unfortunately, the technique for safelyapplying sterile gloves has been shown to be ofa low standard. In relation to applying cleangloves, there appears to be no research on tech-niques for their application and it is left to thepractitioner to adapt the technique taken forapplying sterile gloves to minimize the risk ofcontamination. Aspock and Koiler (1999) givea clear explanation of how to apply andremove sterile gloves correctly in their simplehand-hygiene exercise (Table 3). This is animportant skill, as Bree-Williams and
544 Uritish Journal orNiir5iiij(.2IK)5,Vol 14. No 10

INFECTION CONTROL NURSING
Waterman (1996) found 33% of nurses putgloves on incorrectly, which could have led toglove contamination. Further, nurses oftenselected the wrong glove size and some triedto apply gloves while hands were still wet.
In a different study, Davey (1997) found therewas also some confusion relating to whengloves should be applied in the aseptic proce-dure. Some nurses did not know that thewound dressing could be removed with thesterile wastage bag to avoid contaminating theirhands, thus reducing the need for an extra pairof gloves or forceps (see Table 1). Parker (2000)supported the need for hands to be washedafter glove removal. This will remove any bacte-rial growth from the hands that might haveoccurred during glove use or on their removal.
Hampton (2002) also considers that it is pos-sible for virus particles to leak through latexand polyvinyl gloves. For example, whilenurses are performing wound care the amountof exposure to exudates and blood can behigh, even in chronic wounds. It is, therefore,important that even with gloves, non-touchprinciples are used when assessing, cleansingand redressing wounds (see Table 1). Gloves canbecome perforated or the permeability alteredif they come into contact with chemical agentslike alcohol-hand gels.
As Jones et al (2000) argued, these gels havenot been tested on latex material, only humanskin. Therefore, the culture behaviour observedin some nurses, who apply hand gels to disin-fect gloves during the aseptic procedure, oreven between patients, as reported by Curran(2000), is not recommended. If gloves becomesoiled or contaminated, they should beremoved, hands washed or disinfected with analcohol rub, and dried well before fresh glovesare applied. Only in this way can the nurseensure patient safety is maintained.
Aseptic technique: improving patientsafety?It was reported in the DoH (2004) docu-ment. Winning Ways, that the UK has one ofthe highest HAl rates in Europe. Urinary-tract infections are reported at 23%, withwound infections 9% and blood infections at6% (DoH, 2004). Certainly from the patient'sperspective, this equates to an alarming riskto his/her safety, ranging from posing a threatto his/her life, to a longer stay in hospitalwith increased NHS costs, loss of personalearnings and, for some, long-term disability(Myatt and Langley, 2003).
According to Myatt and Langley (2003),MRSA colonization and infection is consid-ered to be endemic in NHS hospitals, with
critical care units identified as the highest riskareas. However, in all clinical environments,this review has highlighted the need to ques-tion basic aseptic principles when performinga range of clinical procedures, whether theseare involving wound care, administration ofdrugs, urinary catheterization or blood-glu-cose monitoring.
In practice, both the clean and aseptic tech-nique (Gilmour, 2000; Parker 2000) appear tobe used synonymously, but often withoutrecourse to risk assessment. Poor handhygiene, incorrect glove selection and tech-nique and a failure to use non-touch actionswhen manipulating sterile equipment are areaswhich need most attention. Such failures indi-cate a problematic theory—practice gap thatwas identified by Michalopoulos and Sparos(2003). However, this is further compoundedby an observed rise in glove culture (Hallett,2000; Raybould 2001).
Risk assessment is not routinely carried outbefore glove usage, and it has been observed byCurran (2000) that some nurses wear the samepair of gloves for multiple tasks. For example,some nurses do not always change glovesbetween patients when performing some cleanprocedures such as blood-glucose monitoring(Curran, 2000; Rourke et al, 2001). Regularaudits of practice behaviour and educationalsupport programmes are needed to resolvesome of these behavioural issues. Action plansshould be drawn up for nurses to follow ifstandards of performance are found to be poor.
While the introduction of alcohol-based handdisinfectants has significantly reduced hand-con-tamination risks (Patel, 2004), poor practice inits application can negate its efficacy. Nursesshould recognize that this practice only meetsliigh enough standards if they apply the disin-fectants for at least 30 seconds (Kramer, 2002).Applying hand disinfectants to gloved hands isnot recommended (Jones et al, 2000) as thesechemicals have not been tested on latex or syn-thetic glove material, only human skin. Riskassessments on type of gloves (latex orpolyvinyl), equipment, lotions and exposure riskto blood and wound exudates, should be com-pleted as a universal precaution for all asepticprocedures (Weaver, 2004). This should guideuurses to adopt safer principles when usinggloves and to enhance hand-hygiene practice.
It should be noted that aprons and uniformsare easily contaminated and can be a reservoirfor cross-infection. Callaghan (1998) andPearson et al (2001) have both concluded thatplastic aprons should be changed betweenpatients and always before performing an asep-tic or clean procedure. It is also recommended
(Callaghan, 1998) that uniforms are changeddaily and, if laundered at home, should bewashed at a high temperature of bO^C. From apersonal observation, the wearing of rings,including wedding bands, should be considereda source of pathogenic contamination if wornduring aseptic-type procedures.
ConciusionPatient safety when performing the aseptictechnique is of the highest importance.Considering the relationship between contami-nation, colonization and infection is not easyfor the nurse to perceive in practice. This makesit harder to pinpoint the actual time, occasionor event that caused the infection. While drugerrors are more easily identified (Preston,2004), errors in applying the aseptic techniqueare more difficult to prove in law. Therefore, it isunlikely that nurses will be involved in someform of litigation as a result of a poor perform-ance leading to HAI (Oxtoby, 2003).
However, nurses should not be complacentabout this area of their practice. It is recom-mended that all nurses use risk-assessment pro-tocols, attend educational updates, and conductregular audits in their practice areas. Suchstrategies should promote ownership of theproblems identified in their practice andimprove the standard of aseptic technique per-formance. This will not only have benefits inpromoting the safety and wellbeing of thepatients, but also provide a safe environment forstudent uurses to learn and practice this skill ina safe and competent manner. ISD
M-Daiiiouk M, Fudiiey E, Bleetnian A (2()(:)4) Hand hygieneand aseptic technique in the emergency department. _/Hoip Infect 56(2yAi7^\
Aspock C. Koller W (1999} A simple hand hygiene (practiceforum). AmJ Infect Conlwl 27(4): 370-2
Baillie L, ed (2005) Dmeloping Practical Nursing Skills. 2ndedn.Arnold, London: HI-7, 214-5
Bissett L (2002) Can alcohol hand rubs increase compliancewith hand hygiene? Br j Nurs ll(l(i}: 1072-7
KEY POINTS
• The practice of aseptic technique is causing
concern for patient safety.
• Giove culture is emerging as a threat
to controlling infection risks.
• Poor hand hygiene practices continue
to be observed.
• Hand disinfectants are oniy effective
if applied for longer than 30 seconds.
• Risk assessment should precede ali aseptic
technique procedures.
• Education strategies are needed
to visualize microbiai fallout.
Urinshjtjurnal of Nursing. 2(Ht5.Vol 14 ,NQ HI 545

lirL'e-WiUi;mts FJ, Waterman H (19%) An examination of nurses' practices when pertbrming a.septictfihiiiques for wound dressings./,-liii' Ntm 23{1): 48-54
I \ill.igii.iti I (! WH) Bai teri.il contamination of nurses' uniforms: a study. Niirs Slaitd 13(1): 37-42C_!iirran ET (200(1) Hcpatim U virus: cmss-infecrion ii) one-exposure prone procedure. Br J Nun
9(6): 344-5HavtyJ (1997) Discovering nursing students' understandings about aseptic teclmique. InlJ.Wirs Israel
3(2): 105-10I )c(H (2004) PHiiHiH^ Ways: H rfeiVi? Thgetlwr to Reduce Healtitcare Associated Infection in England. DoH.
London (iutp://www.dh.gov.Lik/PublicatioiisAndStatistics/Publications/PubUcationsl'olic\AndC;uidance/fi/en) (accessed 11 May 2005)
I )oH (2005) Chief Nursing Officer — hospitals must spread best practice on reducing MRSA. DoH,London (http;//\vvv\v.tJh.g(.)V.iik/PublicdtionsAndStatistics/PressReleascs/PressReleasesNocices/6/cn?CONTENTJD=410l750&chk=jRqaqu) (accessed 11 May 2005)
[ 'ouglierty L (2(KX)) Care of peripheral intrawnous canmila. JVHR Ttities 96(5): 51—21 timfonl C (1997) Mechicillin-resistant SiiipliYlocoaus aureui. Nurs Smnd 11(25): 58-62Kiietoth Z (2003) Hospital-Acquired Itifeciion: Cause and Control. Whurr Publishers, London.
PhiladelphiaFord D, Koehier S (20(H) A creative process for reinforcing aseptic technique practices (rfsean.'h/edu-
cation)..-lOKN/73(2); 44(i-!>0Cilmour O (I9')9) Redefining xseptic technique.^ Cominimity Nurs 13(7):22-f>(_lilniour D (2U'>0) Is the aseptic tecimique always necessary? / CMnmiiiiiiy Nurs 14(4): 32—5(lottrup F, Mullcr K. Bergmark S. Norrej^iard S (2001) I'owder free, non-sterile gloves as.sessed in
wound healing centre. HurJ .S'lirg 167(8): 625—7Griffiths E (2002) How to keep your hand'; clean. Practice Niming 13(20): K2(lould D (2000) Innovations in hand hygiene: Manugel from SSL Inter national. Br I i\'urs 9(20):
2175-80Ciould D, Chamberlain A (1997) The use of a wani-based educational teaching package to enhance
nui^scs'compliance with infection control procedures. Infeci CoiUrnl Hosp Epidt-miol 17(1): 5,V-8OHaberetich N | (2(Nl2) Protecting cathetcrized patients firtm infection. Nursitig and Residential Cart
4(1(1): 482-4Hailett C (2000) Infection control in wound care: a study ot fatalism in conimunity nursing._/ Clin
.\>(R 9(1): 103-91 lanipton S (2002) The appropriate use of gloves to reduce allet^es and infection. Br j Nurs 11(17):
1120-4ilimpton S (2003) Nurses' inappropriate use of gloves in caring for patients. Br / Nurs 12(17):
1024-7I lampton S, Collins F (2(102) A Comprehensive Gmde lo Tissue Viability. Whurr Publishers, LondonI lardeyj (2(X15a) Aseptic technique to be part of essence of care guidance. NursTiitm 101(4): 6Hartley I (2lMI5b) Hand washing needed every 3 minutes in ICU. NimTimes 101(2): 71 le.ikh and SafeC)' C'odimissjon (1999) Coiirrol of Sukirances Hazardous lo Hcalili Regulations: Appwtml
Codes ofl'r.Klin. He;dth and Safety E.\t'cuti\'L- Books, Londont loUinu'orth H. Kingston J (1998) Usitig a non-sterile technique in wound care.J Community Nurs
13(4): 226-9Infection Control Nurses As.sociation (1999) Glove Usage Guidelines. ICNA and Regent Medical,
Londonlones R.Jamp.iin H, Mulberry C!, Rizer R (2000) Moisturizing alcohol-hand gcU for sui^cal hand
preparation (research/education). AORNJ 71(3): 584, 587. 589-90,592,594-5.597-9Kramer A (2002) Alcohol-based gels have litnited efficacy. .4i«( NIITSJ 10(1): 18.Merchant R (2001) Maint;iin good hand hygsene. Nursing and Residential Care 3(3): 136-7Michaiopoulos A, Sparos L (20(13) Postoperative wound infections. Nurs Stand 17(44): 53—4, 56, 3H,
60Myatt R, Langley S (2(K)3) Changes in infection contriil practice to a-ducc MRSA infection. BrJ
Nurs 12(1 \y.075-f\NMC: (2002) Code of I'rofcssioml Conduct. NMC. LondonOxToby K (2{X)3) Right side of tlie law .Vur^ViHia 99(24):22-6O'Toole S (1997) Dispo.wble gloves. PnfNursi-13(3): 184-90I'.irkfr I. (2000) Applying the principles of infection control to wound care. Br_/Nwrr 9(7): 394—404l'.itfl S (2(M)4) The efficacy of alcohol-based disinfectant products. Nurs Times 100(23): 32I'earson A, Baker H.Walsh K. Fitzgerald M (2001) Contemporary nurees'uniforms: history and tr.iiii-
tions._/ Nurs \ Umag 9(3): 147-56Pittet D (2001) Improving adherence to hand hygiene practice: a multidisciplinary approach. Eme<^
hifixtDisl(2):\~\5Pittet D (20<l2) Prttmotion of hand liygiene: magic, hype or scientific challenge. Infect Control Hosp
E H / 2 3 ( 3 ) l l 8 9Preston RM (2(H)4) Drug error and patient safety: the need for a change in practice. Brf Nurs 13(2):
72-8Kaybould LM (2fKll) Disposable non-sterile gloves: a policy for appropriate usage. BrJ Nurs 10(17):
11.15-41Hickani NAS (2Ol>4) Hand hygiene: promoting compliance among nurses and health workers. BrJ
,V(iw 13(7): 404-10Riyat MS, Quinton DN (1997) Tap water as a vraund cleansing agent in accident and emei^ncy.J
Accid Emerf' Med 14: 165-fikoss S (1999) Rationalizing the purch.use and use of gloves in health care. Br/A/Hw 8(5): 279-87liotter ML (2001) Arguments for alcohol hand disinfection. / Hasp hifva 48(Suppl A): 54-8Kourke C. Bates C. Read R C (2(X)1) Poor hospital infection fontn>l practice in venepunctUR' and
use of courniquets.J Hosp /H/ivr 49(1): 59-61Sw-ales J (2003) Why hand washing is flindamental to good practice. Nursing and Residential Care 5(9):
424-7Ward 1) (2000) Haiidwa.shing facilities in the clinical area: a litemture review. BrJ \'\irs 9(2): 82-6Ward D (2002) Conimunity infection control: what is the evidence? BrJ Community Nurs 7(6):
304-8Weaver D (2004) Efficient management of clinical practice. Nursing and Residential Care 6(9): 420-5Williatns C (1999) Wound irrigation techniques: new Steripod normal saline. BrJ Nurs 8(21):
1460-2Wilson J (200.3) Infection Control in Clitiiml Practice. 2nd edn. BalliereTindall, LondonXavier C (1999) AsepsLs. Nurs Stmd 13(36): 49-53Yip E. Cacioli P (2002) The manufacture of gloves from natural rubber latex._/ Allcijiy Clin Immiuiol
YLNTREVL* (DULOXETINE) ABBREVUTED PRESCRIBING INFORMATION.Presentation Hard gas tro-re sis ram capsules, 20mg or 40mg ol diiloxeune Also containssucrose. Uses Indicated tor wcimen kir iht- trcatmtTii cA moderate to severe stress tirinar>-lncotiunence (5UI). Dosage and Administration 40mg twice daily without regard tomeals. Reassess after 2-4 weeks. If trouhlcsomi: adverse events continue beyond 4 weeks,reduce to 20nig twice daily. Comhinadon with pelvic lloor muscle training may be mureeffective than either ireatment alone. Caution when treating iht elderiy. \\'hendiscontinuing after more than 1 week of therapy, the dose should he tapered o\xr 1weeks. Contra-indkations Hi-pereensitivic)' to any of the components. Pregnancy andlactation. Combination wiih montamint oxida.se inliibnoni (MAOIs) IJver diseasea-suliing in hepaiic impalrmetit. Use wiih potent inhihirors of CYP1A2. e.g. [luvoxamineor ciprofloxacin. (^ecautions Use with caution in patients with a hLsiory of mania,bipolar disorder, or seizures. ExercLse caution when using in combinati(3n withatiiideprcssants. Cannon in patients with increased intra-ocular pressure, or ihose at nskol acute narrow-angle glaucoma. Caution in pauents taking aniicoagulams or productsknown to affect platelet function and thost with blei-drng tendencies. Since ircatmenimay be associated with sedation, patients should be cautioned ahoui their ability' lo drivea car or operate hazardous machinery. Hypnnatraemia ha.s heen reported rarely in theelderly As wirh oiher dnigs with similar pharmacological action, iscilau'd cases of suicidalideation or behavioiira have been reponed during therapy or early after discontinuaiion:encourage patients lo report any distressing thoughts or feelings. Interacdons In rarecases, serotonin s>Tidrome has been reponed in patients using SSRIs coticomitantly withserotoncrgic products. Caution is adMsabte il duloxetine is used concomuancly withscrotonergic antidepressants like SSRIs, tricyelics, venlafaxinu, or tnptanS. tramadol andtrjptnphan. Caution LS ad\ised when taken in comhmation with other centrally actingdru^ or substances, including alcohol and sedatives. EJ/ecli oj duloxtlirte on olhcr dm^\Oiution is advised if duioxetine is eo-administered lvith products that are pa'dominantiymetabolised by CYP2D6 if they have a narrow thcrapeutit indra. Undesirable EffectsThe majont)' of adveise events typically occun-ed in the first week, were mild lomoderate, and resolved within a month. Very common (» 10%): Nausea, dry mouih,faugue, insomnia, and constipation. Common f* l%and <10%): Anorexia, appetiiedecreased, thirst, sleep disorder, anxiety, libido decreased, anorgasmia, headache,dizziness (except vertigo), somnolence, tremor, blurred vision, nervousness, diarrhoea,vomiting, dyspepsia, sweating increased, leihargy, pruritus, and weakness. Uncommim{i 0.1% and <1%): Loss of libido. Dizziness (x 5%) was also reponed asaaimmonadverse event upon discontinuation. In trials, treatment was a.s.sociated with smail,transient increases in ALT AST and creatinine phosphokinase. F-or funher information seeSiimmar)' of Product CharHeterisiics, which is available at htip://eme.medicines.org.uti/,Legal Category POM. Marketing Authorisation Numbers I:U/1A14/28O/OOI,i;U/l'04/280/003. Basic NHS Cost i:30 80 pei pack of 56 x 20mg capsules; L3O.aO perpack I'f 1(1 X 40tng capsules Dale of Preparation or Last Review Augusi 2004. FullPrescribing Information is Available h'rom Eli Lilly and Compaii)- Lmited, filly Hou.sc,Priestle)' Road, Basingstoke. Hampshire RG24 9NL Ielephone: Basingstoke (01256) il5Q99. "YENTREVE (duloxetine) Ls a trademark of Eli UUy and Compao); References: 1.Hampe! C ti al Eiir Vrol 1997: 32(5uppl 2):3-12. 2. Hunskaar S d al BjV InrL-nuiti.mci)2004; 93:324-330. 3. Sand\-ik H et alj Chn Epidenwol 1995; 48(3):33Q-M_V 4. WeidnerAC el ill. Am J ObsUi Gynccoi 2001; 184:20-27. 5. Yencreve Summary of ProductCharacteristics. 6. Bump RC « al Worldwide efficacy of duloxetine after 12 weeks andone year in women with SUl; a 4-study meta analysis. Rjster preserited at InternationalContinence Society (ICS), Florence. Italy, October 2003. SUD29P August 2004.
dulDxetine
546 British Journal of Numng,20()5,Vol 14, No 10
