ashton_mph_thesis_fall2014
TRANSCRIPT
FEDERALLY QUALIFIED HEALTH CENTER TRANSFORMATION
TO THE PATIENT-CENTERED MEDICAL HOME MODEL:
A QUALITATIVE STUDY OF PROVIDER EXPERIENCES
by
DAVID WESLEY ASHTON, BA
APPROVED:
PAUL ROWAN, PHD, MPH
OSAMA MIKHAIL, PHD, MBA

Copyright by
David Wesley Ashton, BA, MPH 2014

DEDICATION
To Jeannie

FEDERALLY QUALIFIED HEALTH CENTER TRANSFORMATION
TO THE PATIENT-CENTERED MEDICAL HOME MODEL:
A QUALITATIVE STUDY OF PROVIDER EXPERIENCES
by
DAVID WESLEY ASHTON BACHELOR OF ARTS, THE UNIVERSITY OF TEXAS AT AUSTIN, 2006
Presented to the Faculty of The University of Texas
School of Public Health
in Partial Fulfillment
of the Requirements
for the Degree of
MASTER OF PUBLIC HEALTH
THE UNIVERSITY OF TEXAS SCHOOL OF PUBLIC HEALTH
Houston, Texas December, 2014

ACKNOWLEDGEMENTS
I sincerely wish to thank Dr. Paul Rowan for his experienced leadership and patience
throughout this project; and to Dr. Osama Mikhail for his valued guidance. Without their
continued support I would not have been able to bring this project to fruition. It is an honor
and pleasure to contribute original work to the scientific community to which I owe so much.

FEDERALLY QUALIFIED HEALTH CENTER TRANSFORMATION
TO THE PATIENT-CENTERED MEDICAL HOME MODEL:
A QUALITATIVE STUDY OF PROVIDER EXPERIENCES
David Wesley Ashton, BA, MPH The University of Texas
School of Public Health, 2014 Thesis Chair: Paul Rowan, PhD, MPH
A semi-structured interview was conducted with administrators within four separate
federally qualified health centers (FQHCs) that previously achieved level 3 patient-centered
medical home (PCMH) recognition from the National Committee for Quality Assurance
(NCQA). It was hypothesized that these organizations may be able to share valuable lessons
with other sites who are interested in pursuing NCQA-PCMH recognition. A qualitative
framework analysis was performed, revealing various themes and sub-themes including
reasons for seeking recognition, organizational performance improvements, diagnosis of
approach, effectiveness of approach and overall lessons learned. Difficulties reported
include interpretation of NCQA standards, data collection and reporting, patient engagement,
restructuring of personnel responsibilities and emphasizing the importance of gaining
participation throughout the organization.

TABLE OF CONTENTS
List of Tables ......................................................................................................................... viii
List of Figures .......................................................................................................................... ix
List of Appendices .....................................................................................................................x
Background ..............................................................................................................................11
Methods....................................................................................................................................14
Results ......................................................................................................................................18
Discussion ................................................................................................................................25
Conclusion ...............................................................................................................................27
Appendices ...............................................................................................................................31
References ................................................................................................................................42
LIST OF TABLES
Table 1: Semi-structured Interview Questions Organized by Framework Analysis Category ……………………………………………………………………………28
viii

LIST OF FIGURES
Figure 1: Structure for Identifying Barriers to Implementation of NCQA-PCMH Standards....................................................................................................................30
ix
List of Appendices
Appendix A: Script for Initial Contact………………………………………………31 Appendix B: Letter of Information………………………………….………………32 Appendix C: Baseline Questionnaire………………………………………………..33 Appendix D: Semi-structured Interview Questions…………………………………34 Appendix E: Coding Template (with quotes)……………………………………….36
x

BACKGROUND
The importance of delivering high quality, patient centered health care to the
underserved, chronically uninsured and underinsured is well understood. Complications
resulting from unmet medical needs in this population increase demand for care in hospital
emergency rooms, account for a high portion of uncompensated care for providers and is a
known driver of increasing costs for the entire population. One long-standing approach to
addressing the needs of uninsured and underinsured individuals in the U.S. is the availability of
grants and loan guarantees offered by the Health Resources and Services Administration (HRSA)
to organizations that qualify. In 2011, federally qualified health centers (FQHC) addressed
health care needs of more than 20 million patients (HRSA National Report, 2011). An
increasingly preferred model of primary care delivery is the patient-centered medical home
(PCMH) but implementation of this model in a FQHC is not as widespread in resource-
constrained provider organizations. The PCMH model offers an opportunity for primary care
providers to deliver a more integrated system of medical care that promises to reduce the number
of downstream emergency room visits, improve cost as well as quality of services delivered
while ultimately improving the health and well-being of the communities they serve
(Rittenhouse, 2009). The National Council of Quality Assurance (NCQA) is a leading
organization that offers this recognition to providers who can satisfy the criteria listed in their
guidelines. The transformational process may appear to be daunting for many who operate a
FQHC. Provider experiences can illuminate the process so that practical considerations can be
more comprehensively understood by other FQHC managers who are considering a similar
objective. One approach to addressing this problem is to qualitatively collect, analyze and
interpret information from administrative health professionals working in a FQHC who have
Page 11 of 43
overseen the transformation to a patient-centered medical home (PCMH) model of primary care
delivery. These essential lessons that a limited number of FQHC managers have thus far learned
can prove to be valuable to others who can most readily apply the knowledge gained from
transformational experiences. The overall goal of this study was to identify obstacles associated
with FQHC preparedness for PCMH evaluation by NCQA.
In order to obtain PCMH 2011 program recognition through NCQA a provider must
satisfy all 6 must-pass elements and achieve an overall score of 35–59 (level 1), 60–84 (level 2),
or 85–100 (level 3) (NCQA Standards and Guidelines, 2011). Must-pass elements include:
access during office hours, use of data for population management, care management, support
self-care processes, referral tracking & follow-up, and implementation of continuous quality
improvement. Overall there are 6 categories containing 27 standards/elements for a total
possible score of 100 points. The current fee structure varies, but can often start at $8,500 and
increases as necessary for discretionary reviews, annual renewals and reconsideration requests.
Reconsideration and reevaluation is an option although will invariably require additional
organizational resources. Because baseline preparedness for the NCQA specified criteria will
vary among provider applicants the internal investment of resources would appear to be unique
to each organization. One example of this is use of electronic health records and whether or not
the initial expense of implementation has previously been incurred or if it will be an added cost
that contributes to the overall burden of transformation.
Page 12 of 43

SPECIFIC AIMS: Interview FQHC administrators who have previously achieved
medical home recognition, gather valid guidance for FQHCs facing the challenge of achieving
this recognition with maximum efficiency. An overall research agenda structure was developed
(Figure 1) in order to delineate the aims of the present study from subsequent studies that could
build upon current findings. Future studies may either address individual needs of a unique
FQHC or any broadly identified barriers that pose a commonly perceived challenge to
implementation.
1. Sub-aim 1: Preparation: Determine what steps were taken by management in
preparation for NCQA evaluation. Identify:
a. Initial preparation steps.
b. How responsibilities and tasks were delegated within the organization.
c. If everything was handled within the organization, whether additional staff or an
outside consultant was hired for the process.
d. Information, materials, or resources gathered to plan.
2. Sub-aim 2: Evaluation: Determine what was successful or unsuccessful for NCQA
evaluation in the initial preparation. Assess:
a. Mistakes and successes
b. Usefulness of preparation materials provided by NCQA
c. Usefulness of outside resources (materials, consultants, publications)
3. Sub-aim 3: Recommendations: Experiences applicable to other FQHC managers who
are considering this challenge.
a. If someone were to repeat the process, what would have been done differently
b. Motives for pursuing recognition; achievement of expected benefits
Page 13 of 43

c. Any other lessons that can be shared
METHODS
A preliminary consultation was obtained from a manager of a local FQHC who was
preparing for NCQA recognition and was able to clarify specific and general concerns of an
organization in this position. The questions composed for the interview were developed in order
to address specific aims and themes identified as relevant to this project. A local administrative
staff person volunteered to review the interview for relevance and ease of comprehension.
Identification of recognized medical homes for interview: Potential sites were identified
in states where demand for care in community based clinics is expected to be greatest. Utilizing
Statehealthfacts.org, a resource maintained by the Kaiser Family Foundation, it was discovered
that the same 5 states contain the highest population of uninsured individuals while
simultaneously enrolling the greatest number of Medicaid beneficiaries – California, Florida,
Illinois, New York, and Texas (Statehealthfacts.org, 2012). These states would presumably have
the highest consistent demand and opportunity for efficient and comprehensive health services
offered in a community health center setting. NCQA publishes a list of providers who have
obtained PCMH recognition on their public website, www.ncqa.com. The providers were then
cross-referenced to the FQHC list published by HRSA, yielding 13 health organizations, most of
them operating multiple locations within the same state. For the purposes of this study, the goal
was to interview all 4 identified single site providers and up to 4 randomly chosen multi-site
providers, bringing the overall sample size between 4 and 8. The emphasis was on the single site
locations based on the rationale that experiences of a single site FQHC present a clearer picture
that should be relevant for a single site as well as an organization operating multiple sites. As
Page 14 of 43
the sample size for single site locations is relatively low, additional data from multi-site locations
may prove useful. Following identification of prospective interviewees, the organizations were
individually contacted via telephone so that an interview could be requested and scheduled.
The goal was to conduct the interview with an individual in each organization who
played a direct administrative role in preparing the submission materials, including interfacing
with upper management as well as other parties in the FQHC, and was substantially involved in
interacting with NCQA. Ideally, the interview would be conducted with the “lead” person, or
one of the “lead” people involved in this effort. Therefore, the websites of the selected
organizations were reviewed and whenever possible an administrator was identified who was in
this role, such as a chief operations officer or a quality improvement officer. When this
information was not available on the organization’s webpage, we identified either an
administrator who could readily identify this person or the chief executive officer/executive
director, and asked for the name of the most appropriate person. Of the websites that were
visited, it was more common to find a named chief executive officer rather than an expanded
listing of senior management and their respective responsibilities.
A phone script was devised for initial contact (see Appendix A). The goals for the initial
phone contact were: make contact; identify the best administrator for the interview; receive an
initial willingness; obtain an email address for sending informed consent information and further
contact information; and establish an interview date, if possible. Alternately, it was also
considered that at the time of phone contact, a potential interviewee might want to conduct the
interview at that moment or very soon, such as later that same day or the next day, so the plan
was made to have the phone consent information ready, and have the recording apparatus ready
at the time of any recruitment call.
Page 15 of 43

Upon contact, the potential interviewee was given a concise but thorough explanation of
what is being requested of them throughout participation in the study: a telephone appointment to
gather voluntary responses during a recorded 20-30 minute semi-structured interview;
preliminary background information about the organization; and consent to provide this
information for the current study. If verbal consent was obtained at that time an email address
was requested in order to send comprehensive information including an officially approved
consent form and preliminary baseline questions (Appendix C). General patient population
information was requested in the baseline questions (age, payer-mix, number of outpatient visits
in a given period) to describe the sites. In addition, it was necessary to understand the range of
services offered in each FQHC. Prior to concluding the recruitment phone call a time was
established to conduct the 20-30 minute semi-structured interview. A reminder email was sent
up to one week prior to the scheduled interview time in order to confirm the appointment
followed by another reminder one day in advance. The interviewee was asked if correspondence
should be coordinated directly with them or through an administrative assistant. Receipt of the
baseline questionnaire was monitored by the PI; if not received within one week, a weekly email
reminder was sent to the contact email address no more than a total of 3 times.
Composition of semi-structured interview: When phone contact is made the participant,
having received study information in advance was reminded that their participation is voluntary
and confidential. In addition, consent to be recorded was obtained prior to initiation of the
recording device, then again with recording rolling. It will be repeated that consent has been
delivered by email and reaffirmed at the present moment. A statement was gathered that the
interviewee has reviewed this information, and verbally agrees to participate. Interviews were
recorded on a password protected audio recording device that was kept in a locked office and
Page 16 of 43

transcribed with full anonymity by a professional medical transcriptionist who regularly works
with medical and legal data. Interviews were burned to an audio compact disk and archived by
the faculty advisor in a locked cabinet in a locked office at the institution at which this study was
performed. All other versions of the recordings were permanently deleted.
Questions were asked in the order listed (Appendix D). The interviewee was given
ample opportunity to expound upon their responses. Follow-up questions were developed to
delve further into topics that are believed to be of central relevance to the project. After all
questions have been asked the interviewer stated, “thank you, the interview is concluded” prior
to hanging up.
Data analysis plan: A qualitative framework analysis approach was employed as
described by Ritchie and Spencer which “involves a systematic process of sifting, charting and
sorting material according to key issues and themes” (1994). The five key stages of the analysis
process, noted here, were followed. (1) Familiarization, where the researcher acquires an
overview of the topic being examined. This has been done through becoming acquainted with
peer-reviewed literature on the subject (Coleman 2010, Crabtree 2011, Gilfman 2010, Jaen 2010,
Nutting 2011, Stange 2010) and meeting with a FQHC manager who is in the process of
pursuing NCQA PCMH recognition. (2) Identifying a thematic framework begins with
familiarization but culminates into identifying central themes that are in need of exploration and
development. For the most part, these themes are often known prior to the interview phase and
are used to guide the preparation of the questions in a semi-structured interview situation. After
the interviews have been conducted and transcribed the data are (3) indexed and (4) charted
according to the predetermined themes. This will be hierarchical in nature, containing
subcategories within the overarching themes. The chosen model for coding themes is template
Page 17 of 43

analysis, detailed by Nigel King (Symon & Cassell, 1998). This template coding approach
allows for the flexibility that is required as questions have been prepared beforehand but are
intentionally open-ended so that the interviewee is allowed ample opportunity to expound on the
themes believed to be of central relevance to the project. Finally, (5) mapping and interpretation
of the charts will be the substance of the results section following completion of the previous
four stages. It represents the end product of the qualitative analysis which details lessons learned
by FQHC managers who shared their valuable experiences with transforming a primary care
practice that serves a medically underserved population into a more comprehensive model of
health care delivery.
RESULTS
After attempts to recruit from several FQHCs, administrators at four sites agreed to be
interviewed, and these interviews were completed. Transcriptions were prepared from the audio
recordings and then, following the five steps of framework analysis, a coding template was
compiled. Responses were organized under the four major domains and sub-domains: 1)
Contextual/reasons for seeking recognition: three sub-domains; 2) Diagnostic/describe the
approach that was taken: two sub-domains; 3) Evaluative/how approach was effective or
problematic: one sub-domain with 3 subsequent areas; 4) Strategic/lessons learned: two sub-
domains. The full template is provided in Appendix E.
Contextual/reasons for seeking recognition: The first sub-domain relates to external
evaluation of the organization, either from the community, grantors or payors. Community
perception was of importance to all sites, mostly relating to improvement of their reputation
through marketing or word-of-mouth. Another motivation was to attract more insured patients,
Page 18 of 43

as stated, “[We wanted] to show that we are not just [serving the] homeless, that we can actually
provide care to insured patients.” Granting agencies such as the Health Resources and Services
Administration (HRSA) and the Department of Housing and Urban Development (HUD) as well
as industry sponsors (i.e.- General Electric) also factored into their decision scheme, either
through efforts to sustain current funding levels or to increase eligibility for additional
opportunities. Financial incentives from meaningful use reimbursements were equally relevant,
“in some areas, [satisfying] meaningful use is just staying 50 percent or greater and in most of
the areas, we are meeting above 80 percent and getting close to 100 percent in most of our
targeted areas.”
The next sub-domain that emerged was organizational performance. Sub-themes included
increasing the quality of patient care through treatment adherence (i.e.- medication use),
illustrated by this response: “[We are] better able to manage the patient's illnesses, so we are
decreasing the number of medications that we are having to give out; we are decreasing the
number of times that the patient might have to come in within a month.” Other improved aspects
of organizational performance included decreasing hospitalization rates/emergency room visits
as well as increased utilization of preventive care such as vaccinations for children. Additionally,
there were reports of their organization’s ability to increase the number of patients seen in a
given time period resulting in decreased waiting times and queuing on the street. “It is very hard
to see somebody who has been sitting out there for three hours and you are telling him, sorry, we
have three slots, we can refer you to an emergency room; and that's not what we were here for.
Our goal was focusing on the patient care and making sure that the patient left here with what
they needed.” There were also reports of better scheduling availabilities. “You would think that
a lot of providers are of the mind-set that if they spend additional time with the patient they will
Page 19 of 43

be able to see fewer patients, but it is through overall efficiencies that they have actually been
able to increase patient volume.” Consistency of operations was also important, either for
FQHCs operating single or multiple sites, allowing a single set of standards to dictate processes,
which was perceived to reduce variability among clinical teams.
Diagnostic/description of the approach that was taken: One sub-domain relates to the
determination of the approach beginning with development of an understanding of the NCQA
recognition process. All sites reported struggling with informational materials provided: “the
standards are open for interpretation…even with NCQA, their reviewers do not interpret the
same. So, we had some things that came back from one reviewer, ‘no you didn't get these
points,’ and the next reviewer turned around gave them to us. So, it’s more subjective.” There
were reports of gaining a clearer understanding by attending an NCQA conference with
workshops and by arranging an early site visit with representatives including question and
answer sessions.
Adding to the determination of the approach taken was assessment of their individual
readiness. It was important to evaluate the available resources for the planning process. One site
described applying for a grant to improve diabetes outcomes based on the PCMH model which
allowed them to hire an additional nurse dedicated solely to patient education, a critical
component of NCQA recognition. Prior accreditations/recognitions also influenced their
approach. This could include accreditations from other organizations, Joint Commission for
instance, or previous attempts at NCQA-PCMH recognition and falling short of points required
for level 3. Through these prior attempts some of the standards may have already been
implemented. One respondent stated, “It was important to look at the standards and how we
aligned it with our practices and our policies that we currently had. So, that gave us an idea as to
Page 20 of 43
what we needed to do, if we needed change anything.” It was a common theme for sites to
undergo a degree of trial and error throughout their respective organizations, building upon
experiences over time.
All respondents reported forming a team of at least two or more individuals, then
growing as the initiatives gained momentum. One site described participating in a network of
different FQHCs in their geographical area. Through that collaboration they were able to share
insights and also seek the assistance of a consultant who provided help to multiple sites more
efficiently. No other sites reported hiring a consultant for two primary reasons: lack of available
resources and also the unique characteristics that distinguish FQHCs from other types of
organizations or provider groups. One interviewee – drawing from personal experience – made
it clear that the differences between other private providers and FQHCs were very clear in his
organization and that many experiences did not translate well to more resource-constrained
FQHCs.
Formation of internal teams was essential to progress in meeting NCQA standards. One
specific site reported that it began as an initiative led by their executive officers and medical
directors but later realized the importance of participation across all departments. All of the
organizations interviewed discussed the importance of involvement from accounting departments
as well as information technology departments in large part due to the data tracking and
reporting requirements that are a notably burdensome component of NCQA reporting. There
was an aspect that included internal human resources representatives as well, including revisions
to job descriptions, duties and titles. Participation from case managers and clinical staff was
required as well. This extended to nurses and medical assistants as well as physicians. The
following quote points to the importance of including all personnel within the organization,
Page 21 of 43
“When we told them the importance of NCQA recognition, that our center would be better for all
these things, they bought into it. And the fact that they were each given something to do within
their department, that did a complete change within our company.”
The second sub-domain relates to defining the approach taken. A major theme was the
establishment of timelines and intermediate goals. Leading the system of prioritization was
imbedded within the NCQA standards. The six must-pass elements dictate that without meeting
those stated criteria, the effort dedicated to the process will not have yielded the desired results.
It was said:
…at our first three meetings, it was a lot of understanding the process, how it
works, and then going over each standard, not understanding them, but knowing
that we had the six standards and which one was the most important to meet and
what they imply... If you don't pass that mandatory standard, no matter whatever
else you have you lose all the points… So, that is what basically, the first three
meetings consisted of.
Once unmet standards were identified the plan to address them could be established.
Some examples include preclinical visits, patient education and family participation. The
standards that were already a part of the regular operations could be moved down the list.
Multiple sites reported implementing self-imposed deadlines to stay on schedule.
With a timeline and intermediate goals in place one major theme that was reported was
the training of personnel, establishing clinical teams comprised of a physician, nurse or medical
assistant and a patient service representative. Further cross training of personnel so that
assistance could be provided to other teams with a degree of interchangeability seemed to gain
importance. Examples include assisting other teams with data entry or patient contact as needed.
Page 22 of 43

Again, the various data collection, formatting and assimilation tasks were often a new
requirement that demanded considerable effort.
Evaluative/how approach was effective or problematic: One of the primary difficulties
reported includes the additional patient engagement and education requirements. Multiple sites
stated that their patient populations posed some challenges. Some FQHCs reported having a
high percentage of immigrant populations with varying levels of health and social literacy.
Another reported serving a large homeless population and the unique obstacles to patient
involvement that seemed to create. Receiving responses to patient satisfaction surveys did at
times delay the pre-established timelines and often needed more extensive follow up to obtain
survey results to the level specified by NCQA.
Another common recurring theme continued to be engagement and training of FQHC
personnel. It was stated:
one of the most difficult parts for our PCMH model was finding specific teams to
work with. As part of a PCMH model, they were requesting for you to have one
specific medical provider, with either a nurse or a medical assistant, and a patient
service representative be part of that team. So, when the patients are coming in,
they have that knowledge of, okay, [name] is the nurse that works with Dr.
[name] and this is my doctor and oh the service representative registering me
today is [name], so it would make it more of a friendly environment and he would
feel comfortable, especially with the type of population that we deal with.
Further difficulties included data gathering:
our patient services and our financial department play a big role for this
recognition. They tend to want to know exactly how many patients are seen, how
Page 23 of 43
many outpatient visits, how many people are coming in that are not compensated,
how many are coming in that are [covered through] Medicaid, and I think that is
the most difficult part to maintain.
Strategic/lessons learned: A recurring theme continued to be the interpretation of NCQA
standards. Because NCQA does not perform a site visit to verify satisfying the recognition
standards, everything must be compiled and reported in a certain manner that ultimately was not
clear enough to any of the sites interviewed. If interpretation of the standards is not aligned with
NCQA expectations it is very difficult to achieve level 3 recognition. Only through NCQA
related trainings, frequent communication with NCQA representatives and receiving feedback
could any of the sites meet the overall goal of obtaining level 3 recognition. One site reported
lapses in communication with their representative which led to considerable difficulties in
making progress, or they reported not being effectively informed that they were appointed a
different representative – again, creating barriers for them.
The term transformation is applied to the process because provider organizations are
required to truly transform the way patient care is delivered. This was a challenge for many, but
not all, of the sites that agreed to be interviewed. The operational changes are reportedly
burdensome for FQHC staff who are asked to alter the manner in which their duties are
performed. Another example continues to be the data intensive elements. All sites were
consistent in this. One stated, “getting to a level 3 without having significant ongoing data
analytics capabilities, I think would be difficult,” another clarified, “what we are doing is we are
running reports on a monthly basis, so that at the end of the year, whenever we have to report, we
are not pulling the report on 12-month data. We are just doing it month to month to make our
life much easier.”
Page 24 of 43

Participation at all levels is critical, continuous and resource intensive. The statement
below is illuminating:
When you first hear, create teams, create huddles, meet with the doctors and
nurses, improve your no-show rate, call the patient the day before, give them that
one-on-one, you know, that human touch… I was one of the ones that said these
teams are never going to work, what they are asking for is very difficult, but give
it a try. It really does work and it is beneficial.
DISCUSSION
Determination of gaps in readiness was truly a site-specific exercise. It may be difficult
to address this on a large scale because of the variation among FQHCs. Few of the sites reported
experiencing the same benefits of obtaining level 3 recognition. Two of the four sites reported
being considerably transformed, one was still looking for greater improvement in quality
measures, yet another site made it clear that they did not gain many benefits at all, that their
operational standards were already reflective of best practices and made no revisions to their
approach to the delivery of care. One influence may be the patient population that is served. It
may be important that the sites that reported greater difficulties as well as achieving greater
benefits of transformation also had higher rates of uncompensated care, ranging from 60-80% of
their overall payer mix. Further studies will likely prove beneficial.
All sites reported grappling with the documentation and reporting aspects however. They
all acknowledged that it is to the advantage of the FQHC to be able to develop their own
strategies and implementation processes, that it can’t be completely detailed by NCQA due to the
variability across sites. All sites were able to overcome the reporting challenges by increased
dialogue with NCQA representatives.
Page 25 of 43

The principal lesson that emerged was that interpretation of standards must be considered
from the NCQA perspective rather than based on any other assumptions or heuristics on which
one might rely upon when reviewing the materials. It appeared to be worthwhile to attend
NCQA sponsored conferences or workshops dedicated to this pursuit. Also, the level of
cooperation between FQHCs is not consistent. One site reported being contacted by another
FQHC, asking to review their standard operating procedures in preparation for their initial
attempt at recognition. This was not favorably received in part due to the amount of effort that
was spent to acquire these experiences and implement the changes, and so seemingly regarded as
proprietary knowledge that should be guarded. An organization belonging to an external FQHC
network also seemed to gain an advantage by sharing perspectives, insights and a consultant.
There was common agreement that the standards are beneficial, even if they are already
in practice. Most of the sites confirmed that their organization is providing a higher standard of
care within their respective communities after adopting the recommended processes. All
reported a sense of esteem from receiving level 3 recognition. Some thought recertification
would be difficult but others felt that the difficult aspects had already been addressed by the
initial process. One site noted, “I think that re-certification is going to be tough … mostly
because of the staff [who] may be doing a great job and we might find that, now, your great job
is just average and so now you have to do a better job.” Additionally, the importance of their
role in the community as a safety-net provider was widely perceived, “first of all, credentialing
and accreditation for any organization in the managed care world provides better be first rate…”
Page 26 of 43
CONCLUSION
Implementation of the patient-centered medical home model in federally qualified health
centers may be an important step toward improving the health of medically underserved
populations in this country. Gaining insight from administrators who have fostered their
organizations through the lengthy process of obtaining this recognition from NCQA can possibly
help others with the transformational process. We found that focusing greater attention on
interpretation of NCQA standards along with enhanced communication with representatives
could help organizations throughout this endeavor. Additionally, engaging both internal staff
and patients can present greater challenges than some may initially anticipate. The data intensive
nature of this undertaking is a remarkable hurdle as well. Further studies may be helpful in
addressing the following: expansion of the current sample size to further identify common or
widespread obstacles; examining the environment within FQHCs that have not endeavored to
implement the model; patient engagement in chronically underserved communities and barriers
within these sub-populations that may interfere with the type of engagement that is required by
NCQA; or evaluating the rationale behind FQHCs seeking certification from various accrediting
organizations. Reporting to NCQA is a resource-intensive endeavor regardless of current
practices. Many FQHCs can individually address site-specific barriers by simply initiating the
process within their organizations, learning from other sites as well as the experiences that are
unique to them. Efficient management of resources is a constant process for all organizations.
Developing a tailored approach to pursuing, obtaining and maintaining PCMH recognition with
added attention to lessons previously learned may help to facilitate adoption of these evidence-
based standards.
Page 27 of 43
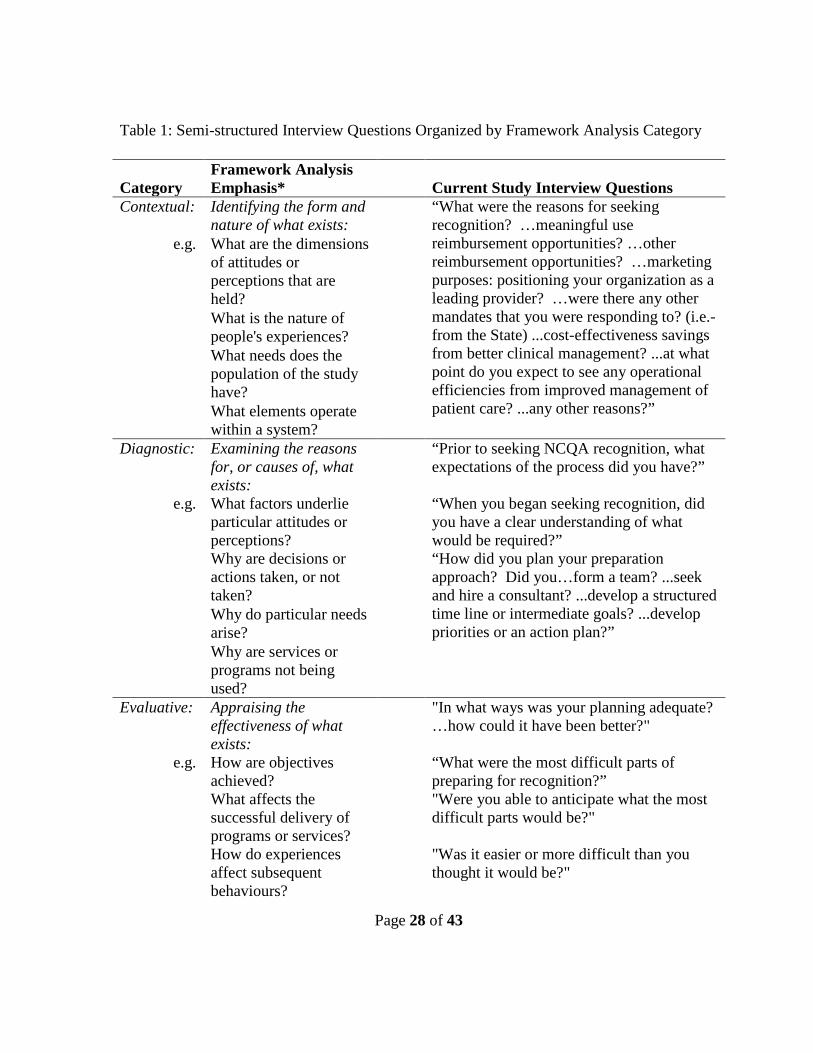
Table 1: Semi-structured Interview Questions Organized by Framework Analysis Category
Category
Framework Analysis Emphasis* Current Study Interview Questions
Contextual: Identifying the form and nature of what exists:
“What were the reasons for seeking recognition? …meaningful use reimbursement opportunities? …other reimbursement opportunities? …marketing purposes: positioning your organization as a leading provider? …were there any other mandates that you were responding to? (i.e.- from the State) ...cost-effectiveness savings from better clinical management? ...at what point do you expect to see any operational efficiencies from improved management of patient care? ...any other reasons?”
e.g. What are the dimensions of attitudes or perceptions that are held?
What is the nature of people's experiences?
What needs does the population of the study have?
What elements operate within a system?
Diagnostic: Examining the reasons for, or causes of, what exists:
“Prior to seeking NCQA recognition, what expectations of the process did you have?”
e.g. What factors underlie particular attitudes or perceptions?
“When you began seeking recognition, did you have a clear understanding of what would be required?”
Why are decisions or actions taken, or not taken?
“How did you plan your preparation approach? Did you…form a team? ...seek and hire a consultant? ...develop a structured time line or intermediate goals? ...develop priorities or an action plan?”
Why do particular needs arise?
Why are services or programs not being used?
Evaluative: Appraising the effectiveness of what exists:
"In what ways was your planning adequate? …how could it have been better?"
e.g. How are objectives achieved?
“What were the most difficult parts of preparing for recognition?”
What affects the successful delivery of programs or services?
"Were you able to anticipate what the most difficult parts would be?"
How do experiences affect subsequent behaviours?
"Was it easier or more difficult than you thought it would be?"
Page 28 of 43

What barriers exist to systems operating?
"Did you feel satisfied with the preparation information that was provided by NCQA?"
"What additional information would have assisted the planning process?"
“What aspects of seeking and maintaining recognition appear to require the greatest amount of resources from your organization?”
“Do you think overall quality of patient care has improved since obtaining recognition?”
“What will be the most challenging issues for recertification?”
Strategic: Identifying new theories, policies, plans or actions:
“Are there any lessons learned or further information that would be helpful for other FQHCs that are considering transformation to the medical home model?” e.g. What types of services
are required to meet needs?
What actions are needed to make programs or services more effective?
How can systems be improved?
What strategies are required or overcome newly defined problems?
*Quoted and paraphrased from Ritchie and Spencer, 1994. **Complete interview, in interview order, contained in Appendix.
Page 29 of 43
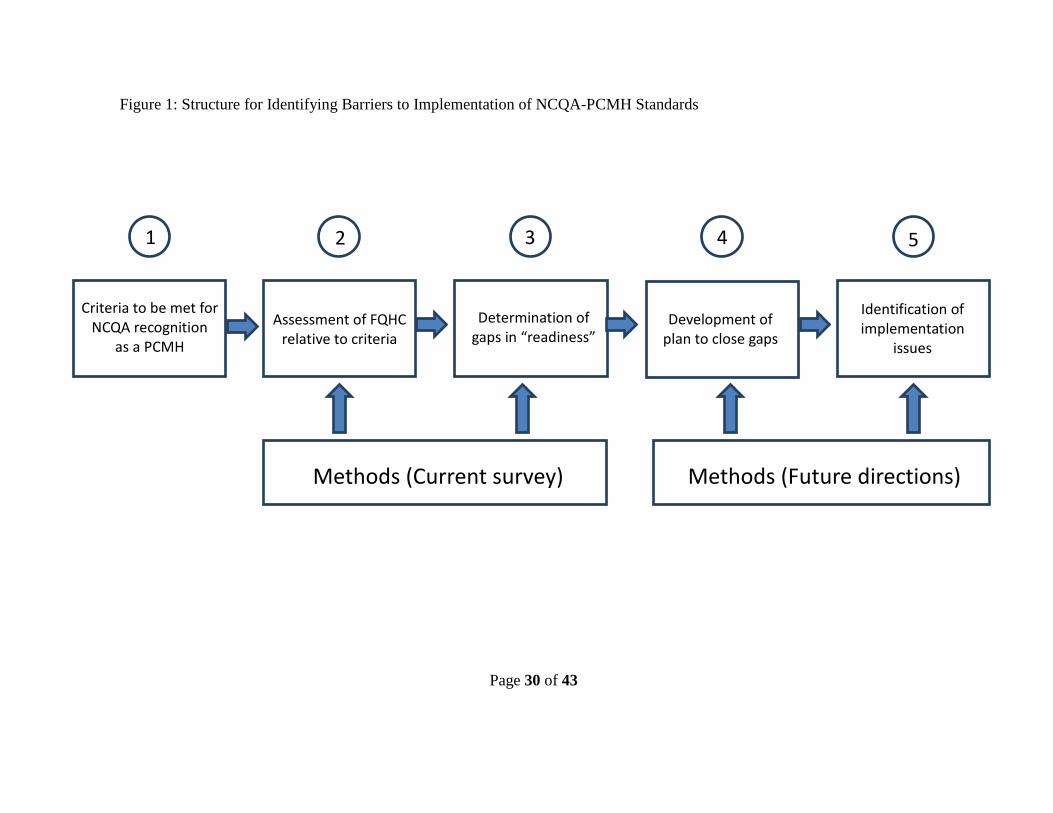
Figure 1: Structure for Identifying Barriers to Implementation of NCQA-PCMH Standards
Criteria to be met for
NCQA recognition as a PCMH
Assessment of FQHC relative to criteria
Determination of gaps in “readiness” Development of
plan to close gaps
Identification of implementation
issues
Methods (Current survey)
Methods (Future directions)
1 2 3 4 5
Page 30 of 43
APPENDICES
Appendix A: Script for Initial Contact
Hello,
I am a graduate student at the University of Texas School of Public Health and I am conducting a study about the medical home model in federally qualified health centers. Is there someone I could talk to about your organization’s experience with the transition? I am looking for an operations manager or someone who dealt with the majority of the transformational process.
[Requested contact person or voicemail]
[Hello, my name is David Ashton and I am a graduate student at the University of Texas School of Public Health…and I am conducting a study about implementation of the medical home model in federally qualified health centers. I am hoping to gather some information from someone who has overseen the transition process, perhaps an operations manager or whoever was principally responsible for implementation the new standards.]
My goal is to hold an interview for a period of 20 to 30 minutes and to gather some information regarding experiences throughout the transition and any lessons that you may have learned within your organization. Would it be possible to set up some time that works with your schedule? I can be as flexible as needed so that I don’t disrupt your workday.
If I have your consent to be interviewed, I would like to send an email containing letter of information and some preliminary baseline questions about your organization – is this acceptable to you?
May I have your contact information?
Name:
Title:
Phone:
Email:
Best time to call:
Preference for coordinating through administrative assistant:
Thank you very much.
Page 31 of 43

Appendix B: Letter of Information
LETTER OF INFORMATION
Federally Qualified Health Center Transformation to the Patient-Centered Medical Home Model: A Qualitative Study of Provider Experiences
HSC-SPH-13-0553
Date
Dear _________,
I am inviting you to take part in a research project I am conducting at the University of Texas Health Science Center called Federally Qualified Health Center (FQHC) Transformation to the Patient-Centered Medical Home (PCMH) Model: A Qualitative Study of Provider Experiences. Your decision to take part is voluntary. You may refuse to answer any questions asked at any time. This research project has been reviewed by the Committee for the Protection of Human Subjects (CPHS) of the University of Texas Health Science Center at Houston as HSC-SPH-13-0553.
The purpose of this research study is to gather information regarding transitional lessons that are relevant to FQHC administrators as they consider pursuing medical home recognition from the National Council on Quality Assurance (NCQA). There are many providers that can in turn apply this experience to enhance their own implementation processes in order to deliver a higher standard of health care to individuals in their respective communities.
I would like to ask you a series of questions to which you may respond with as much detail as is comfortable to you. These questions will focus on the experience of your institution during the certification process. This interview will take about 20 to 30 minutes. The only risk of being in this study is the possible loss of confidentiality, and there is no direct benefit to taking part in this study. Your decision to take part is voluntary. You may decide to stop taking part in the study at any time. If you withdraw from the study none of your information or answers will be used in any way. You will not be personally identified in any reports or publications that may result from this study. Any personal information about you that is gathered during this study will remain confidential to every extent of the law. A special number will be used to identify you in the study and only the investigator will know your name. If you have questions at any time about this research study, please feel free to contact me at (512) 669-0658. You can contact me to discuss problems, voice concerns, obtain information, and offer input in addition to asking questions about the research.
Thank you,
David Ashton Masters Candidate School of Public Health, University of Texas Health Science Center
This study (HSC-SPH-13-0553) has been reviewed by the Committee for the Protection of Human Subjects (CPHS) of the University of Texas Health Science Center at Houston. For any questions about research subject's rights, or to report a research-related injury, call the CPHS at (713) 500-7943.
Page 32 of 43

Appendix C: Baseline Questionnaire PRELMINARY/BASELINE INFORMATION
Provider organization/medical home: How many patients/enrollees in a given time period? How many outpatient visits per year? Ages by age group Preschool: Youth: Teens: Adults under 65: Adults 65+: Specialty services (YES or NO) Vision: YES or NO Dental: YES or NO Behavioral health: YES or NO Other: Payer mix (%) Uncompensated care: Medicaid: Medicare: Private coverage: Covered through additional special program funding (grant to serve specific need, such as Ryan White):
Page 33 of 43
Appendix D: Semi-structured Interview Questions
QUESTIONS (in order of interview)
1. “Prior to seeking NCQA recognition, what expectations of the process did you have?”
2. “When you began seeking recognition, did you have a clear understanding of what would be
required?”
3. “How did you plan your preparation approach? Did you…”
a. “Form a team?”
b. “Seek and hire a consultant?”
c. “Develop a structured timeline or intermediate goals?"
d. “Develop priorities or an action plan?”
4. “In what ways was that plan adequate?”
a. “How could the plan have been better?”
5. “What were the most difficult parts of preparing for recognition?”
a. “Were you able to anticipate what the most difficult parts would be?”
b. “Was it easier or more difficult than you thought it would be?”
6. “Did you feel satisfied with the preparation information that was provided by NCQA?”
a. “What additional information would have assisted the planning process?”
7. “What aspects of seeking and maintaining recognition appear to require the greatest amount
of resources from your organization?”
8. “Do you think overall quality of patient care has improved since obtaining recognition?”
9. “What will be the most challenging issues for recertification?”
10. “What were the reasons for seeking recognition?”
a. “Meaningful use reimbursement opportunities?”
Page 34 of 43
b. “Other reimbursement opportunities?”
c. “Marketing purposes: positioning your organization as a leading provider?”
d. “Were there any mandates that you were responding to? (i.e. - from the State)”
e. “Cost-effectiveness savings from better clinical management?”
i. “At what point do you expect to see any operational efficiencies from
improved management of patient care?”
f. “Any other reasons?”
11. “Are there any lessons learned or further information that would be helpful for other FQHCs
that are considering transformation to the medical home model?”
Page 35 of 43

Appendix E: Coding Template (with quotes)
1 Reasons for seeking recognition (Contextual) 1 External evaluation of organization
1 Community 1 Improve reputation (word of mouth/marketing)
We wanted to be on the forefront and to improve the relationship with the community
1 Attract more insured patients to show that we are not just [serving the] homeless, that we can actually provide care to insured patients
2 Grantors (HRSA, HUD, industry) 1 Sustain current funding levels The number one reason that we have continued to do NCQA, is we are involved in some of the HRSA projects and they require NCQA/PCMH.
2 Eligibility for additional opportunities 3 Payors (Medicare, Medicaid/CHIP, private)
1 Meaningful use in some areas, meaningful use is just staying 50 percent or greater and in most of the areas, we are meeting above 80 percent and getting close to 100 percent in most of our targeted areas.
2 Organizational performance 1 Increase quality of patient care
1 Tx/Rx adherence [We are] better able to manage the patient's illnesses, so we are decreasing the number of medications that we are having to give out; we are decreasing in the number of times that the patient might have to come in within a month
2 Decrease hospitalization rates, ER visits 3 Preventive care
1 Immunizations 2 Increase volume of patient care
1 Decrease wait times/queuing Page 36 of 43
it is very hard to see somebody who has been sitting out there for three hours and you are telling him, sorry, we have three slots, we can take and can refer you to an emergency room and that's not what we were here for. Our goal was focusing on the patient care and making sure that the patient left here with what they needed.
2 Better scheduling availabilities you would think that a lot of providers are of the mind-set that if they spend additional time with the patient they will be able to see fewer patients, but it is through overall efficiencies that they have actually been able to increase patient volume
3 Operational consistency 1 Single site because that sets the standards at a certain level and it says that if you are level 3 NCQA-recognized, you will have your standards
2 Multi-site 2 Diagnosis of how approach was taken (Diagnostic)
1 Determination of approach 1 Develop understanding of recognition process the standards are open for interpretation…even with NCQA, their reviewers do not interpret the same. So, we had some things that came back from one reviewer, “no you didn't get these points,” and the next reviewer turned around gave them to us. So, it’s more subjective.
1 NCQA conference/workshops 2 NCQA early site visit, Q&A We did have staff from the NCQA come to meet and they did tell us what would be required. They did have a question and answer session, which was very helpful, and then we went from there
3 NCQA website 2 Readiness preparation and assessment
1 Available budget/resources 1 Seek grant funding for additional personnel
Page 37 of 43
initially we had no budget and what I did is that I applied for a grant to improve diabetes outcomes based on the PCMH model, so that gave me some money to work with and dedicate the time to initiate the different logs and tracking information that is required
2 Prior accreditations (i.e.- Joint Commission) 1 Possibly meeting many standards it was important to look at the standards and how we aligned it with our practices and our policies that we currently had. So, that gave us an idea as to what we needed to do, if we needed change anything
3 Prior attempts for NCQA-PCMH recognition 1 Level 1 or 2 (trial and error)
3 Formation of team 1 External
1 FQHC network (i.e.- shared resources) 1 Multi-site consultant 2 Training sessions
2 Internal When we told them the importance of NCQA recognition, that our center would be better for all these things, they bought into it. And the fact that they were each given something to do within their department, that did a complete change within our company
1 Executive 2 Medical directors 3 Clinical staff
1 Nursing staff 2 Medical assistants 3 Case managers
4 Other departments 1 Billing/Finance
1 Data tracking 2 IT/Analytics
1 Patient portal 2 Data tracking/reporting
Page 38 of 43

3 Human Resources 1 Revision of job descriptions, change in focus
2 Approach to meeting NCQA standards 1 Establish timeline and goals at our first three meetings, it was a lot of understanding the process, how it works, and then going over each standard, not understanding them, but knowing that we had the six standards and which one was the most important to meet and what they imply... If you don't pass that mandatory standard, no matter whatever else you have you lose all the points… So, that is what basically, the first three meetings consisted of
1 Must-pass elements 2 Identify unmet standards (i.e.)
1 Preclinic visits 2 Patient education 3 Family participation
3 Triage standards already in process 4 Self-imposed deadlines to stay on schedule we set up target dates and timelines we tried to always go back and reassess and that kind of thing. The days became 12 and 14 hour days. And we had to set up some priorities and procedures and kept that in a log that we reviewed ahead of time
2 Training of personnel 1 Establish clinical teams
1 Physician 2 Nurse/MA 3 Patient service representative
2 Cross training 1 Assist other teams when needed
3 Data collection and assimilation 3 How was approach effective/problematic (Evaluative)
1 Difficulties 1 Patient engagement and education
1 Health or social literacy 2 % of uncompensated care
Page 39 of 43

1 Possible relation to challenges in patient engagement 2 Staff training and engagement one of the most difficult parts for our PCMH model was finding specific teams to work with. As part of a PCMH model, they were requesting for you to have one specific medical provider, with either a nurse or a medical assistant, and a patient service representative be part of that team. So, when the patients are coming in, they have that knowledge of, okay, [name] is the nurse that works with Dr. [name] and this is my doctor and oh the service representative registering me today is So-and-so, so it would make it more of a friendly environment and he would feel comfortable, especially with the type of population that we deal with.
3 Data gathering and reporting our patient services and our financial department play a big role for this recognition. They tend to want to know exactly how many patients are seen, how many outpatient visits, how many people are coming in that are not compensated, how many are coming in that are Medicaid, and I think that is the most difficult part to maintain. And, what we are doing is we are running reports on a monthly basis, so that at the end of the year, whenever we have to report, we are not pulling the report on 12-month data. We are just doing it month to month to make our life much easier.
4 Lessons learned (Strategic) 1 Interpretation of standards
1 Aligning FQHC interpretation of standards with NCQA expectations 1 Trainings offered 2 Frequent communication with assigned representatives from NCQA
1 Potentially problematic, occasional lapses reported 2 Operational challenges
1 Data gathering/tracking 1 Data intensive getting to a level 3 without having significant ongoing data analytics capabilities, I think would be difficult
1 Collection 2 Reporting
2 Review monthly
Page 40 of 43
2 Participation at all levels 1 Clinical teams 2 Group huddles 3 Training
1 Initial 2 Continuous When you first hear, create teams, create huddles, meet with the doctors and nurses, improve your no-show rate, call the patient the day before, give them that one-on-one, you know, that human touch… I was one of the ones that said these teams are never going to work, what they are asking for is very difficult, but give it a try. It really does work and it is beneficial.
Page 41 of 43
REFERENCES
1. Coleman K & Phillips K. (2010). Providing underserved patients with medical homes:
assessing the readiness of safety-net health centers. Issue Brief (Commonwealth Fund),
85, 1-14.
2. Crabtree BF, Chase SM, Wise CG, Schiff GD, Schmidt LA, Goyzueta JR, et al. (2011).
Evaluation of patient centered medical home practice transformation initiatives. Medical
Care, 49(1), 10-6.
3. Gilfillan RJ, Tomcavage J, Rosenthal MB, Davis DE, Graham J, Roy JA, et al. (2010).
Value and the medical home: effects of transformed primary care. American Journal of
Managed Care, 16(8), 607-14.
4. Health Resources and Serviced Administration. 2011 National
Data http://bphc.hrsa.gov/uds/view.aspx?year=2011 (accessed 4/7/2013).
5. Jaen CR, Crabtree BF, Palmer RF, Ferrer RL, Nutting PA, Miller WL, et al. (2010).
Methods for evaluating practice change toward a patient-centered medical home. Annals
of Family Medicine, 8 Suppl 1, S9-20; S92.
6. King, N. (1998). Template Analysis. pp. 118-134. Symon, G, Cassell, C, Qualitative
Methods and Analysis in Organizational Research, 1998. Thousand Oaks, CA: Sage
Publications.
7. Nutting PA, Crabtree BF, Miller WL, Stange KC, Stewart E & Jaen C. (2011).
Transforming physician practices to patient-centered medical homes: lessons from the
national demonstration project. Health Affairs, 30(3), 439-45.
Page 42 of 43

8. National Committee on Quality Assurance. (2011). Standards and Guidelines for
NCQA’s Patient-Centered Medical Home 2011.
9. Ritchie, J, Spencer, L. (1994). Qualitative data analysis for applied policy research. pp.
173-194. A. Bryman and R.G. Burgess [eds.] Analyzing qualitative data, 1994.
10. Rittenhouse DR, Shortell SM. (2009). The patient centered medical home: will it stand
the test of health reform? Journal of the American Medical Association. 2009;
301(19):2038-2040.
11. Stange KC, Miller WL, Nutting PA, Crabtree BF, Stewart EE & Jaen CR. (2010).
Context for understanding the National Demonstration Project and the patient-centered
medical home. Annals of Family Medicine, 8 Suppl 1, S2-8; S92.
12. Stange KC, Nutting PA, Miller WL, Jaen CR, Crabtree BF, Flocke SA, et al. (2010).
Defining and measuring the patient-centered medical home. Journal of General Internal
Medicine, 25(6), 601-12.
Page 43 of 43