asia & near east operations research and … res materials fr... · related literature 3 ... bc...
TRANSCRIPT

1
FACTORS THAT CONTRIBUTE TO THE VARYING PERFORMANCE OF
BSPOs AND BHWs IN THE DELIVERY OF FAMILY PLANNING SERVICES
IN ILOILO CITY
PHILIPPINES
Fely David Fely Chin
Final Report
Subcontract Number C193.43A
SOCIAL SCIENCE RESEARCH INSTITUTE CENTRAL PHILIPPINE UNIVERSITY
THE POPULATION COUNCIL
ASIA & NEAR EAST OPERATIONS RESEARCH ANDTECHNICAL ASSISTANCE PROJECT
October 1994

2
TABLE OF CONTENTSList of Tables iiList of Tables in Apendix A iiiAcronyms ivExecutive Summary vSection I - INTRODUCTION 1
Background and Rationale of the Study 1Problem Statement 2Hypotheses of the Study 2Related Literature 3Ultimate Objective of the Study 5Immediate Objective of the Study 5Variables of the Study and their Operational Definitions 5
A. Dependent Variable 6B. Independent Variables 6
Study Design 7Sampling Procedure 7Data Collection 8
Survey of the BHWs and BSPOs 9In-depth interviews with key informants 9Focus Group Discussion (FGD) 10Examination of office and clinic records/documents 10Observation 11
Data Processing and Analysis 11Research Utilization Workshop 11Limitations of the Study 12
Section II - THE STUDY AREA AND ITS FAMILY PLANNING PROGRAM 13Setting of the Study 13Health and Family Planning Service Facilities in the City 13The Population/Family Planning Program of Iloilo City 16The Beginnings of the Family Planning Program of Iloilo City 16Problems and Difficulties Encountered in FP Program Implementation 17Recent Developments in the Family Planning Program of Iloilo City 18
A. Functions and Responsibilities of the City Population Office 18B. Functions and Responsibilities of the City Health Office 19
The BSPOs and BHWs: Their Roles and Responsibilitiesin the Family Planning Program of Iloilo City 21A. The BSPOs' Prescribed Functions and Responsibilities 21B. The BHWs' Prescribed Functions and Responsibilities 21
Section III - THE BSPOS AND BHWS AND THEIR WORK 23Profile of the BSPOs and BHWs of Iloilo City 23Selection Process 23Training 26

3
The Actual Work of BSPOs and BHWs 28Other Activities Involved in by Volunteers 30Incentives and Other Benefits Received by the Volunteers 31Other Benefits Received By the Volunteers 34Supervision of Volunteers 34The Work of the BSPOs and BHWs: Interest and Commitment
and Satisfaction 38Family Planning Supplies 39KAP among the BSPOs and BHWs 42
Knowledge 42Attitudes 43FP Practices 44
BSPOs' and BHWs' FP Performance 47Number of clients served 47Time spent in FP activities 47FP clients motivated 49FP clients referred 49FP clients counselled 49FP clients provided with FP supplies 51
Factors Influencing Volunteers' FP Performance 51Attendance in FP training 51Time spent on FP functions 51Knowledge and attitudes towards FP 52Interest and commitment 52Involvement in community/livelihood projects 52Supervision and FP performance 53Position/designation 53Supervisor Ratings and Satisfaction with Incentives 53
Section IV - THE BSPOS AND THE BHWS: VIEWS FROM THECOMMUNITY AND OTHER FP WORKERS 55
The BSPOs and the BHWs: The Community's View 55On Volunteers' Interaction with the Community 56On Attributes of an Effective FP Volunteer 56Some Suggestions on How to Improve Volunteers FP Performance 57The BSPOs and the BHWs: the FP Workers' Views 57
On the Volunteers' Role in Family Planning 57On Attributes of an Effective Volunteer 58On Volunteers' Interaction with the FP Workers 59On How to Improve Volunteers' FP Performance 59Research Utilization 60
Section V - SUMMARY, CONCLUSIONS AND RECOMMENDATIONSSummary of Findings 61Conclusions 64Policy Implications and Recommendations 65

4
Appendix A 67Bibliography
LIST OF TABLES
Table 1 Sample Distribution of Respondents by Area 8Table 2 Distribution of In-depth Interview Key Informants by Area 10Table 3 Number of FGDs Conducted by Number of
Participants by Type and by Area 11Table 4 Profile of the Study Area 15Table 5 Distribution of BSPOs and BHWs by Demographic Characteristics 24Table 6 Distribution of BSPOs and BHWs by Economic Characteristics 25Table 7 Distribution of BSPOs and BHWs according to How They Were
Recruited by Designation 27Table 8 Distribution of BSPOs and BHWs by Trainings Attended 28Table 9 Distribution of BSPOs and BHWs by Family Planning
Activities Actually Performed 30Table 10 Distribution of BSPOs and BHWs by Other Functions
Actually Performed by Them in the Past Six Months 32Table 11 Distribution of BSPOs and BHWs by Involvement in
Livelihood Projects 33Table 12 Distribution of Respondents According to Designation 35Table 13 Distribution of BSPOs and BHWs by Incentives and Other
Benefits Received by Designation 35Table 14 Distribution of BSPOs and BHWs by Supervision 36Table 15 Distribution of BSPOs and BHWs by Supervision 37Table 16 Distribution of BSPOs and BHWs by Work Experience 40Table 17 Distribution of Volunteers by Supplies Received,
by Sources of Supplies and Designation 41Table 18 Distribution of BSPOs and BHWs by Knowledge and
Attitude on Family Planning 45Table 19 Distribution of BSPOs and BHWs by Family Planning Practice 46Table 20 Distribution of BSPOs and BHWs by Number of Clients Served,
Number of FP Cases Attended, and, Time Spent in FP by Designation 48
Table 21 Distribution of BSPOs and BHWs by Performance 50Table 22 Correlation Values Between Performance and Selected Variables 54

5
LIST OF TABLES IN APPENDIX A
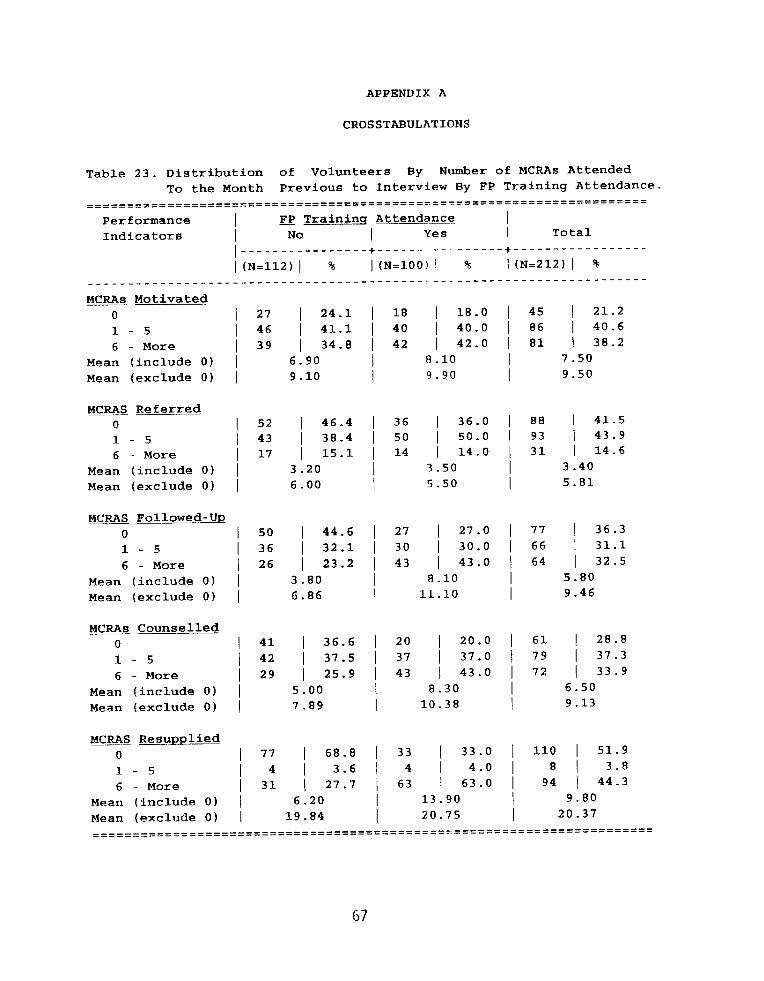
Table 23 Distribution of Volunteers By Number of MCRAsServed by FP Training Attendance 67
Table 24 Distribution of Volunteers By Number of MCRAs Served by Knowledge on Family Planning 68
Table 25 Distribution of Volunteers By Number of MCRAs Served by Attitude on Family Planning 69
Table 26 Distribution of Volunteers By Number of MCRAs Served by Relationship with Supervisor in Terms of Supervisors' Rating
70Table 27 Distribution of Volunteers By Number of MCRAs
Served by Number of Hours Spent on FP Functions 71Table 28 Distribution of Volunteers By Number of MCRAs
Served by Interest and Commitment in termsof Number of Years in Active Service 72
Table 29 Distribution of Volunteers By Number of MCRAsServed by Satisfaction with Incentives 73
Table 30 Distribution of Volunteers By Number of MCRAsServed by Involvement in Community Projects 74
Table 31 Distribution of Volunteers By Number of MCRAsServed by Number of Meetings with Supervisor 75
Table 32 Distribution of Volunteers By Number of MCRAs Servedby Number of Hours Spent by Supervisor per Visit 76
Table 33 Distribution of Volunteers By Number of MCRAsServed by Designation 77

6
ACRONYMS
ARI - Acute Respiratory InfectionBC - Barangay CaptainBHS - Barangay Health Station BHW - Barangay Health WorkerBNS - Barangay Nutrition ScholarBSPO - Barangay Service Point OfficerCHO - City Health OfficeCPO - City Population OfficeCPU - Central Philippine UniversityDOH - Department of HealthFGD - Focus Group DiscussionFP - Family PlanningFPOP - Family Planning Organization of the PhilippinesIMCH - Integrated Maternal Child HealthIMH - Iloilo Mission HospitalLGU - Local Government UnitMCH - Maternal Child HealthMCRA - Married Couple of Reproductive AgeNGO - Non-Government OrganizationNFP - Natural Family PlanningPTB - Pulmonary TuberculosisSSRI - Social Science Research InstituteTFR - Total Fertility RateTIDA - Total Integrated Development ApproachUNICEF - United Nation International Children's Emergency FundUSAID - United States Agency for International DevelopmentWHO - World Health OrganizationWVSU - West Visayas State University

7
EXECUTIVE SUMMARY
Background of the Study
In 1992, the Population Council established the Family Planning Operation Researchand Training (FPORT) Program in Philippines. Its mandate included bringing togetherprogram managers and regional researchers to identify problem areas which may benefitfrom operations research. From Western Visayas (Region VI), the City Population Office(CPO) of Iloilo City in collaboration with Social Science Research Institute (SSRI) of theCentral Philippine University (CPU), identified a problem concerning the poor performanceof volunteer FP workers and undertook to study the problem. The study focused on theBarangay Service Point Officers (BSPO) who assist in the delivery of FP services under thesupervision of the CPO; and Barangay Health Workers (BHW) who concentrate on maternaland child care but have minimal involvement in FP and are supervised by the City HealthOffice.
The objective of the study was to determine and compare the FP activities andperformance of the BSPOs and BHWs in Iloilo City and determine the factors that influencetheir performance. The study sample consisting of 106 BSPOs and 106 BHWs wererandomly selected for interview, using systematic sampling with a random start. Qualitativetechniques included 29 in-depth interviews with key informants consisting of health andpopulation officers, family planning coordinators, physicians, nurses and midwives; 13Focus Group Discussions (FGD) with FP workers and clients; observation of actual field andclinic activities of FP volunteers.
Summary of Findings
1. The BSPOs and the BHWs of Iloilo City were mostly female, 46 years oldon the average, high school-educated, and married with 4 to 5 children on the average. Thegainfully employed volunteers (58.5 percent) were mostly engaged in part-time small scalebusiness and were earning a monthly median income of P1,000. Their median total monthlyhousehold income was P3,000.
2. Only a few of the volunteers (both BSPOs and BHWs) were able to attenda formal FP training. Most of the BSPOs, but only 29.2 percent of the BHWs had receivedinformal training or orientation on their roles and functions from their immediatesupervisors.
3. Although most of the volunteers were reportedly active in their work andFP-related functions, many were still not involved in FP motivation, referral, follow-up,

8
counselling and distribution of FP supplies. With their functions focused on MCH care, theBHWs' involvement in FP activities were limited.
4. Volunteers were able to serve an average of 11 FP clients per week, theBSPOs spending an average of 5 hours per week in FP work, while the BHWs, 3 hours perweek. Some volunteers were also involved in community/livelihood projects.
5. PPOs directly supervised the BSPOs, while the PHNs and RHMs supervisedthe BHWs. Volunteer-supervisor interactions were limited to an average of 2 to 3 times amonth. These interactions were more frequent and lasted longer among the BHWs thanamong the BSPOs.
6. Both the BSPOs and the BHWs favorably appraised their supervisors in termsof: approachability, supportiveness, helpfulness, flexibility, consideration, dedication to andknowledge about their job.
7. The volunteers' monthly incentive of P 200. has served as a motivating factorin improving FP performance. However, the delay in its release and the fact that somevolunteers (those holding dual roles) were receiving more than the others had negativelyaffected FP performance.
8. The majority of the volunteers were interested and committed to their workas indexed by their long years of continued active service (aaverage of 8 years) and theirintention to continue working "as long as they are able", an indication of their commitmentto their work.
9. The most common FP supplies distributed by the volunteers to their clientswere pills and condoms which they usually obtain from their respective supervisors or fromthe health clinic/stations or the CPO.
10. Most of the Barangay Captains were acquainted with the BSPOs and BHWs
in their barangay. Some BSPOs/BHWs, however, were not known to many MCRAs in thecommunity due to limited volunteer-community interaction. To meet their health/FP needs,some mother go directly to the health clinic ot opt not to seek any help.
11. The involvement of men either as FP targets or as volunteer motivators, wasobviously minimal. The FGDs and in-depth interview participants argued that, since themen play a major role in FP decision-making, they must also be involved in the FP program.
12. The FP performance of the BSPOs was significantly better than that of theBHWs. Those holding dual functions both as BSPOs and BHWs also performed better thanthose who were BHWs alone, but not better than those serving as BSPOs exclusively.
13. The volunteers' FP performance is significantly influenced by their attendance

9
in FP training, the amount of time they spent in FP activities, their interest and commitmentto their work, and the amount of time spent by their supervisor with them.

10
CONCLUSIONS
1. While the delivery of FP services is a major function of the BSPOs, thisis only one of the many responsibilities of the BHWs. More BSPOs than BHWs handlereferrals, follow-up and resupplying current FP users with contraceptives.
2 Close supervision and monitoring of the health volunteers by theirsupervisors was perceived to help improve volunteers' FP performance. This enablesthe supervisor to follow-up the progress of the volunteers' work and to assist them inaddressing whatever problems/difficulty they may encounter.
3. Although the quantitative analysis did not show significant correlationbetween the volunteers' FP performance and their relationship with supervisors, this hasbeen unanimously recognized by the volunteers themselves and the FP workers as animportant ingredient in improving delivery of FP services.
4. The volunteers' incentive was perceived as a motivating factor for FPvolunteers to perform well, however, the delay in its release, and the fact that somevolunteers (both BSPOs and BHW) receive more than the others had bred indifferenceamong them, and admittedly influenced their performance.
5. The data support the hypotheses that the volunteers' FP performance issignificantly influenced by various personal and external factors, such as trainingattendance, amount of time spent on FP tasks, supervision, volunteers' interest andcommitment to their work, and their participation in community activities.
6. Volunteers trained on FP tend to perform better than those who had notundergone training.
7. The amount of time spent by the volunteers on their FP tasks also positivelyaffects their performance. The more time the volunteers spent on his FP work, thebetter his/her performance.
8. Supervision is proven as an important component of FP programimplementation. The closer the volunteers are supervised and the more time thesupervisors spent with them the better the FP performance of the volunteers.
9. Volunteers who were involved in community activities, performed better thanthose who were not and the more activities they were involved in, the better their FPperformance.

11
10. Despite the fact that husbands play a major role in family decision-making, theirparticipation in FP program is very minimal. Moreover, like many other programs, IloiloCity's FP program is still very female oriented.
POLICY IMPLICATIONS AND RECOMMENDATIONS
1. A training which will address the immediate knowledge and skills needs of thevolunteers needs to be conducted. Before any training is conducted, however, a trainingneeds assessment should be done, so that the specific training needs of the volunteers canbe immediately addressed.
2. The perceived poor relationship between some CPO and CHO personnel andbetween their respective volunteers and its admitted negative influence on FP performancesuggests the inclusion in the proposed training of a reorientation on the roles andresponsibilities of all those involved in the FP program.
3. To allow the PPOs more time to monitor, guide and assist their BSPOs, thenumber of PPOs must be increased and the coverage of each supervisor be reduced.
4. There is a need for the immediate resolution of conflicts and strained relationshipbetween some CPO and CHO personnel and volunteers. The present initiative to bridgethe gap and resolve the problems between the CPO and CHO through a coordinativesystem that defines their respective roles and tasks must be pursued and given the chanceto work. This requires regular consultation and dialogue and close coordination betweenthe CPO and CHO.
5. There is also a need to train the volunteers on some simple visual diagnosticprocedures to enable them to detect "warning signs" or symptoms that would requireimmediate termination of contraceptive use or referral of a client to a clinic.
6. There is need to identify and define common indicators of FP performancewhich the CHO and the CPO could use in the evaluation of the FP performance of theirvolunteers.
7. The fact that husbands often make the final decision in FP practice makes theirinvolvement in FP programs imperative, both as targets and motivators. The CHO andCPO can start this by recruiting male BSPOs and BHWs.
8. Since volunteer work needs time, interest and commitment, these should begiven priority among the criteria to be considered in the recruitment and selection ofvolunteers.
13
SECTION I
INTRODUCTION
Background and Rationale of the Study
Iloilo City's population, which has grown at an annual rate of 2.4 percent in the lastdecade, was estimated to include about 335,000 persons in 1993. Planners and socialscientists predict that, given geophysical, economic and social limitations, the presentpopulation growth rate may put the city at a high risk of suffering from more seriouseconomic and social problems in the future.
Attending to Iloilo City's population-related concerns and problems are two localgovernment offices, each tasked with specific but related roles. Serving as the bad agencyin the implementation of the city's population development-related programs, includingFamily Planning, is the City Population Office (CPO). The other is the City Health Office(CHO) whose major concern is the delivery of basic health services. Although FamilyPlanning is also included under basic health services in Iloilo City. The CPO leads theimplementation of FP services.
In order to make their services more accessible to the people especially in areas withno health or FP facilities, both the CPO and the CHO maintain a network of communityvolunteer workers who assist in the delivery of health services directly at the grassrootslevel. The volunteers for the CPO are called the Barangay Service Point Officers (BSPOs),while the volunteers for the CHO are the Barangay Health Workers (BHWs).
The BSPOs and the BHWs have their specific prescribed functions. The BSPOs focuson population development and FP promotion, while the BHWs concentrate on health care,including FP. In relation to FP, they share common responsibilities including: motivationof FP potential clients, follow-up of potential or current users (CUs), referral of potential andcurrent users, and counselling and resupplying FP users with contraceptives. In addition,the volunteers are also involved in community organizing activities and other communityactivities through which FP and health care are further promoted.
In Iloilo City, the BSPOs and the BHWs have played important roles in theimplementation of the city's FP program and have been recognized as instrumental in thecity's successful FP accomplishments in the past. When the CPO was awarded the mostoutstanding population office in Region VI from 1977 to 1980, the BSPOs were given thecredit for the CPO's good performance. One BSPO in the city was awarded "one of themost outstanding BSPOs in the country." The city's FP accomplishment in terms of number

14
of FP acceptors reached a high record of 18,000 in 1981.
This achievement was not sustained through the 1980s, however. From themid-1980s to the beginning of the 1990s, a decline in FP accomplishment was noted. Thenumber of FP users in the city decreased while the drop-out rate increased and the numberof new acceptors declined (CPO Report). The DOH Annual Reports from 1989 to 1991further confirmed this low performance of Iloilo City as compared with other cities inRegion VI.
Iloilo City's poor FP performance in the early nineties has been attributed to severalfactors, two of which were the changes in the national FP program and in the citygovernment's leadership especially during the second half of the 1980s. Despite the setbackssuffered by the FP program, the network of community volunteers remained in place andthe city government continued to subsidize their monthly allowances. Despite this, however,the CPO and the CHO felt that the city's poor record in FP may be linked to the performanceof their respective volunteers. While some volunteers remained active and continued toreach and serve FP clients, others failed to properly perform their FP functions.
Family Planning accomplishment maybe gauged by several indicators, mostespecially the number of current FP acceptors. Since the BSPOs and BHWs are amongthose directly responsible for this accomplishment, it is important to determine what factorsinfluence the volunteers' varying FP performance. It is in this context that this diagnosticstudy was conducted.
Problems Statement
The considerations discussed above therefore lead us to pose the following researchquestion: What factors contribute to the generally low and varying performance of theBSPOs and the BHWs in the delivery of FP services in Iloilo City?
Hypotheses
Related literature, pre-existing theories and the experiences of population programimplementors suggest several possible answers to the above problem. These include: lackof training, lack or inadequate supervision, lack of knowledge about FP, heavy workload,poor relationship with supervisors, volunteer dissatisfaction over incentives
and/or other benefits received, lack of interest and commitment to their work as BSPO orBHW, and inavailability or lack of FP supply available to the volunteer workers fordistribution to their clients.

15
Since training is assumed to prepare the volunteers to perform their roles andfunctions, it is predicted that trained BSPOs and BHWs would perform better than thosewho had not been trained. In a similar vein, adequate supervision is expected to improveperformance. BSPOs and BHWs who meet with their supervisors more frequently andregularly are therefore expected to perform better than those who have lesser contact.
Volunteers involved in community organizing. Faithful performance of this roleshould give them many opportunities to talk to couples about FP. It can be hypothesized,therefore, that volunteers involved in community projects will perform better than those whohave no involvement at all.
The BSPOs' and the BHWs' relationship with their supervisors is also expected toinfluence their performance. Those who relate well with their supervisors are expected toperform in a superior fashion.
It is also assumed that the volume of work a volunteer handles would affect hisperformance. A volunteer who performs multiple functions will generally not be able toperform as well as one who has fewer responsibilities. It is thus expected that a volunteerwho is functioning as either a BSPO or only as a BHW may perform better than one whois handling both roles.
Another possible determinant of performance is the volunteer's level of interest andcommitment to the program. If this were true, the more interested or committed theBSPOs/BHWs are to their FP responsibilities, the better their performance.
Two other factors which are predicted to influence the volunteers' performance are(1) satisfaction with incentives and benefits received and (2) availability of FP supplies. Itis hypothesized that BSPOs or BHWs who are satisfied with the incentives and otherbenefits they receive will be better performers than those who are partially satisfied oraltogether unsatisfied. Finally, when FP supplies are available to the volunteers, this shouldfacilitate their efforts to extend contraceptive services to the people of Iloilo City.
Related Literature
Previous studies on community volunteers' performance in terms of their overallfunctions, whether conducted in Region VI, in other parts of the country or in othercountries, reveal that their FP performance is influenced by various factors. Among thesewe may include: 1) the various personal characteristics of the volunteers (social,economic and attitudinal), 2) environmental characteristics, and 3) the volunteers' interactionwith their clients and co-workers.
A study on "BSPO Volunteerism" in Region VI in the early 1980s (Laconico, et al.:1981) revealed significant relationships between the BSPOs' participation in the Outreach

16
Project as correlated with their socioeconomic status and their frequency of communityinvolvement. The study of Chin and Cuevas (1992) on BHW performance in Iloilo, on theother hand, did not find any significant relationship between performance and selectedsociodemographic characteristics of the BHWs, such as age, sex, educational attainment andincome. However, she found that commitment and interest are positively related withperformance.
Based on the concept that a favorable interaction process between a client and an FPworker can influence to the clients to accept contraception, Raymundo and others (1991)conducted a study on client-FP worker interaction. The study revealed that a favorableinteraction process between the clients and FP workers can be attributed to the workers'favorable relationship with their clients. This was manifested in the clients' positiveevaluation of the FP workers' effectiveness. The cooperativeness they exhibited towards theFP workers was also another manifestation of the favorable interaction between the twogroups.
A study conducted in Taiwan (as cited by Raymundo, et. al., 1991) also revealed thatsome personal characteristics of the FP workers improve client-worker interaction and theworkers' effectivity in promoting contraceptive acceptance. This study further showed thatthe Taiwanese prefer FP workers who are: 1) emotionally mature, 2) married, 3) withchildren, 4) contraceptive users, 5) educated, 6) at ease during discussions, and 7)indigenous. Preference is given to FP workers who are contraceptive users themselvesbecause they are perceived as better role models. This is expected to improve theirefficiency in recruiting FP acceptors.
Miralao's study (1973) noted that FP acceptors tended to judge FP workers in termsof their ability to get along with people. When asked to identify the positive and desirablecharacteristics they were looking for in a community FP worker, the majority expressed thatthey want a worker with "good public relation" and/or similar attributes of "sociability."Corroborating Miralao's findings, Lacson's (1977) study also revealed that FP acceptorscharacterized an FP motivator as one who has a pleasing personality, proper communicationand motivation skills and proper attitude towards his or her job. The acceptors alsopreferred young female FP workers who have at least a college background or at least a highschool education.
The importance of interpersonal communication in FP promotion was also noted ina Taiwanese the study conducted by Kenny, et al. (1970). This study showed that morehome visits by FP motivators resulted in more monthly IUD acceptors. FP motivators,usually carry out house to house visits, sip tea, and engage in face to face interaction withprospective FP clients to recruit them to accept the program.
While the above studies provide some basis for explaining the performance ofcommunity FP volunteers the work and inconsistent correlations obtained would appear toindicate that much of the variation in the volunteers' performance is still left unexplained.

17
There are also many factors whose influence on performance has not been examined. Thisindicates the need for further investigation on this subject.
Ultimate Objective of the Study:
This study's ultimate objective is to provide FP program managers, service providers,and policy makers with information that will help them improve FP program planning andimplementation. It is important that the people who have a
stake in the implementation of the FP program understand the strengths and weaknesses ofactual FP program implementation, especially in the local level, so that they can makeappropriate actions to address emerging program concerns.
Immediate Objective of the Study
The Social Science Research Institute (SSRI) of Central Philippine University (CPU)in cooperation with the Population Office of Iloilo City conducted this diagnostic study in1993 to determine and compare the FP activities and performance of BSPOs and BHWs inIloilo City and to determine the factors which influence their performance most strongly.
Variables of the Study and their Operational Definitions
The dependent variable of the study is the BSPOs' and the BHWs' performance inthe delivery of FP services. It is assumed that the volunteers' performance is influenced byboth internal (personal) and external (structure or system) factors; these have therefore beentreated as the independent variables of the study. The internal factors considered are: 1)attendance in training, 2) knowledge about their FP functions, 3) perceptions regarding theirrelationship with their supervisors, 4) time allotted for FP tasks, 5) interest and commitmentto their tasks, 6) level of satisfaction with the incentives and benefits, and, 7) involvementin IGP and community activities. The external factors, on the other hand, are: 1)supervision time provided to them by their supervisors, 2) availability of supply, and 3)FP-related positions and other tasks/activities. The operational definitions of these variablesare presented below.
A. Dependent Variable
1. Performance in FP service delivery. This refers to the number of MCRAsmotivated, followed-up, counselled and/or provided FP supplies by theBSPO/BHW in the last six months.

18
B. Independent Variables
Internal/Personal Factors
1. Training attendance. This refers to the number and type of trainings attended byBSPO/BHW, particularly on FP service delivery as well as the type of trainingattended.
2. Knowledge about FP. This was measured in terms of the number of questionsanswered correctly among the five items on FP which were included in thesurvey instrument.
3. Relationship of BSPOs/BHWs with their supervisor. This refers to thevolunteers' qualitative assessment of some attributes of their immediatesupervisors. Using a Lickert Scale of 1 (lowest) to 5 (highest), they were askedto rate their supervisors in terms of "approachability", "supportiveness","helpfulness", etc.
4. Time allotted for FP activities. This was measured in terms of the number ofhours spent per week by each volunteer on FP service delivery during the last sixmonths.
5. Interests and commitment. This refers to the volunteers' number of years ofcontinuous service as BSPOs/BHWs. The period only includes the time whenthey were active or had outputs (e.g. attended meetings, made reports, etc.)
6. Satisfaction with incentives received. This pertains to the volunteers' assessmentof their satisfaction with the incentive they receive from the city governmentbased on a scale of 1 (lowest satisfaction) to 5 (highest satisfaction).
7. Involvement in livelihood projects. In this study this refers to the number ofcommunity/livelihood projects the volunteers were involved in during the last sixmonths prior to the survey.
External Factors
1. FP-related position. This refers to the position/s held by the BSPO/BHW,whether they were functioning as: a) BSPO only, b) BHW only, or c) bothBSPO/BHW.
2. Supervision received. This refers to the number of meetings/contacts theBSPOs/BHWs had with their supervisors in the last six months prior to the studyand the amount of time spent by their supervisor with them.

19
3. Availability and source of FP supply. Availability refers to the amount of FPsupplies requested, received and distributed by the volunteers, while sourcerefers to where the volunteers get their FP supplies (DOH, CHO, CPO, or NGO).
Study Design
This study was designed as a diagnostic assessment of the performance of the BSPOsand BHWs in Iloilo in the delivery of FP services. Using both quantitative and qualitativeapproaches, it attempted to examine the prevailing situation of the FP program in Iloilo Cityalong with the roles and functions performed by the BSPOs and the BHWs in programimplementation. It assumed that there will be variations in the volunteers' performance oftheir respective functions; as such, a major study question becomes that of determiningwhich factors contribute to these variations. Discussed below are the procedures employedby the study with regard to sampling, data collection and data analysis.
Sampling Procedure
The target population of this study consists of the BSPOs and the BHWs assignedin 158 barangays of Iloilo City. There were actually 165 barangays in Iloilo City as of theend of 1992; however, the subdivision (housing estates) barangays were not includedbecause there are no regular BSPOs assigned in these areas. In each of the 158 remainingbarangays, there was one BSPO along with two BHWs. Both groups of health volunteersare provided cash incentives of P200 each per month by the Iloilo City Local Government.
Based on a total population of 474 (316 BHWs and 158 BSPOs), and samplingformula (Parel, et al, 1985) illustrated below, the desired sample size for the proposed studyis 212. This sample was allocated equally to BSPOs and BHWs. The subsamples thereforeconsist of 106 BSPOs and 106 BHWs.
NZ . p (1-p)2
n = ------------------------Nd + Z . p (1-p)2 2
where: n = the desired sample sizeN = total populationZ = Confidence level (1.96 for a 95 percent level)d = sampling error (.05)p = estimated proportion of respondents possessing certain characteristics (0.50)

20
Systematic sampling with a random start was used to draw the elementary sample. Asampling frame was prepared by listing separately in alphabetical order all the BSPOs andthe BHWs supported by the Iloilo City Government in the 158 barangays covered by thestudy. The names were then numbered consecutively.
For each list, the sampling interval was determined by dividing the total number ofBSPO/BHWs by the desired sample size for each group. From a random start, the sampleBSPOs/BHWs were drawn using the sampling interval. Table 1 presents the samplingdistribution of the survey respondents.
Table 1.Sample Distribution of Respondents by Designation and Area
District BSPO BHW TOTAL
N % N % N %
Arevalo 10 9.4 7 6.6 17 8.0Jaro 22 20.8 30 20.3 52 24.5Lapaz 25 23.6 19 17.9 44 20.8Mandurriao 5 4.7 5 4.7 10 4.7Molo 15 14.2 19 17.9 34 16.0City Proper 29 27.4 26 24.5 55 25.9
Total 106 100 106 100 212 100
Data Collection
A combination of quantitative and qualitative techniques was used to collect the dataneeded for this study: 1) Personal interviews of BSPOs and BHWs; 2) In-depth interviewsof CPO, CHO and Barangay Health Station (BHS) personnel and some barangay leaders;3) Focus group discussions (FGD) with MCRAs, RHWs and some BHWs not included inthe survey; 4) Actual observation of BHW and BSPO activities at the health centers and inthe field; and 5) Examination of CPO and CHO or clinic records/documents including theaccomplishment reports of the community volunteers.
Survey of the BHWs and BSPOs. The BSPOs and the BHWs were the main surveyrespondents of this study. They were interviewed using a structured interview schedule

21
which was prepared in consultation with the CPO and CHO. The survey solicitedinformation on: the BSPOs'/BHWs' background; FP trainings attended and their knowledgeabout their FP functions; the amount and type of supervision they have received from theirsupervisors; the time they allot to their FP functions; their involvement in communityprojects and activities; their perception regarding their relationship with their supervisors;their satisfaction with the incentives and benefits they have received; and their interest andcommitment to their work.
The survey instrument which was prepared in English was translated to Ilonggo, thelanguage of the target population. The Ilonggo translation was then back-translated toEnglish to check on consistency and correctness of the translation. An independent socialscience researcher was asked to comment on the instrument.
The translated instrument was pre-tested with five BHWs and five BSPOs who were notpart of the sample. Based on the results of this process, the instrument was further revised.
Interviews were conducted by trained interviewers. Fieldwork, was undertaken incoordination with the CPO and the CHO and was closely monitored by field supervisors andthe principal investigator.
In-depth interviews with key informants. In-depth interviews with CPO and CHOpersonnel, Barangay Nutrition Scholars (BNS), and Barangay Captains (BC) wereconducted to solicit their views regarding the FP program of Iloilo City, the role played bythe volunteers in program implementation and FP accomplishments, and their perceptionsregarding the factors that make a volunteer perform satisfactorily or poorly. The interactionof the volunteers with the community and the health system was also examined using thein-depth interview results. The qualitative data also served to validate some of the surveyresults. A total of 29 key informants were carried out. This included 7 PHNs, 5 RHMs, 5PPOs, 1 CPO, 1 CHO, 2 FP Coordinator, 5 BCs, and 3 BNS. Table 2 presents the sampledistribution of the key informants by type and area.

22
Table 2. Distribution of Key Informants by Type and Area.
District PH RH PP CP CH FP BC BN TON M O O O C S T
Arevalo 1 1 0 0 0 0 0 0 2Jaro 2 1 1 0 0 0 1 0 5Lapaz 2 1 1 0 0 1 1 0 6Mandurria 1 0 1 0 0 1 1 1 5oMoloCity Prop
0 0 1 0 0 0 1 1 31 2 1 1 1 0 1 1 8
Total 7 5 5 1 1 2 5 3 29
Focus Group Discussion FGDs with MCRAs, BHWs and selected RHMs were alsoconducted to further validate the survey data and determine other external factors that mayhave influenced the volunteers' performance. Discussed by the MCRAs were theirmotivations to practice or not to practice FP and how they regard the BHWs/BSPOs as FPservice providers. FGDs with midwives and BHWs focused on their perceptions regardingthe volunteers' involvement in community projects and activities, the availability of supplies,problems in FP service delivery and other external factors that may hamper the volunteers'performance.
The FGDs were conducted in five geographically different barangays in Iloilo city:agricultural, coastal, commercial, slum, and residential. It was assumed that the barangaylocation could influence the volunteers' performance and other people's perception ofthe volunteers' roles and functions. The FGD areas were drawn at random from among thebarangays under each category. An FGD guide was used as a common reference for allFGDs.
A total of 13 FGDs were conducted involving a total of 92 participants. Table 3presents the distribution of FGD participants by type and by area.
Examination of office and clinic records/documents. Clinic records andBSPOs/BHWs accomplishment reports were also examined to get further information aboutthe volunteers' performance and their other activities.

23
Table 3. Number of FGDs Conducted by Number of Participants by Type and byArea.
District No. RHM/ BHW MCRAs Totalof PHN
FGD
Jaro 3 8 6 6 20
Lapaz 3 7 8 8 23
Mandurriao 2 0 9 9 18
Molo 2 0 5 10 15
City Proper 3 7 5 4 16
Total 13 22 33 37 92
Observation. Observations of BSPOs' and BHWs' clinic and field activities focusedon the volunteers' actual activities at the health center/station or in the field, the number ofMCRAs they attended to and the services they provided. The clinic observations wereconducted on a regular clinic day, while the field observations were done on a randomlychosen day in a week. Trained nurses conducted the observations.
Data Processing and Analysis.
Survey data were processed using DBASE III for data management and SPSS PC+for statistical analysis. Descriptive analysis mainly utilized frequency distribution andmeasures of central tendencies. The existence and extent of relationships involving FPperformance of the volunteers and their hypothesized determinants were determined usingappropriate statistical tools. This was supplemented by qualitative information from thein-depth interviews, FGDs, clinic and field observations and information taken from officialdocuments.
Research Utilization Workshop
To immediately feedback the study results to program managers and other end-usersof the study for reaction and possible action, a Research Utilization (RU) Workshop wasconducted upon the study's completion. The workshop was

24
conducted in January 1994 and attended by 46 participants representing the DOH, theNational Economic and Development Authority (NEDA), POPCOM, USAID, ThePopulation Council, Family Planning Organization of the Philippines (FPOP), the CHO; theCPO; CPU; and selected BSPOs and BHWs.
During the open forum that followed the presentation of the study's major findings,issues concerning FP program implementation and volunteers' FP performance pointed outby the study were discussed. The participants then examined and reacted on the researchers'recommendations and gave additional recommendations to improve the city's FP program. In the action planning that followed, CPO and CHO staff and volunteers, summarized theissues and recommendations and specified the planned actions on these. The workshopoutputs were then presented for reaction during the plenary.
Limitations of the Study
This study covers Iloilo City only and included only BSPOs and BHWs receiving monthly support from the City Government. Only 158 of the 162 city barangayswere covered because some did not have regular BSPOs or BHWs.
Insofar as the volunteers' FP performance was the main concern of this study, theinquiry focused mainly on the volunteers' FP-related activities and accomplishments. TheFP performance index used was number of FP clients motivated, followed-up, referred,counseled or provided FP supplies based on CHO and CPO records. In case of absence ofor incomplete records, data were collected from the volunteers or their supervisors.

25
SECTION II
THE STUDY AREA AND ITS FAMILY PLANNING PROGRAM
This section describes Iloilo City, the setting of this diagnostic study and its FPprogram.
Setting of the Study
`Iloilo City, is a chartered city in the Province of Iloilo, one of six provinces inRegion VI (Western Visayas). As of the latest census (NSO, 1990), Iloilo City had a totalpopulation of 309,505 persons, distributed in a land area of 6,852.198 hectares. With anannual growth rate of 2.4 percent, the city's total population as of the time of the study isestimated at approximately 332,329 persons. The city has 56,617 households (NSO, 1990),with an average of 5.4 members. The city's population is young, with 35 percent being lessthan 15 years old.
"Hiligaynon," is the language of the "Ilonggos," the local name for Iloilo natives.Although there are some clusters of small ethnic groups residing in the city, the city'spopulation consists basically of "Ilonggos". Some of the ethnic groups in the city includeMuslim traders from Mindanao, and a few "aetas," a nomadic group of Filipino natives,who sometimes come to the city from reserve settlements or the uplands to beg. There arealso individual migrants from other parts of the country who have established their residencein the city.
Iloilo City has 180 barangays which are distributed in its six political districts asfollows: Arevalo, 13; City Proper, 45: Jaro, 42: lapaz, 37: Mandurriao, 18: and Molo, 25.
Jaro has the most number of households among the six districts, (14,642, as of 1990census), followed by Lapaz (12,242), then City Proper (10,774). Each of the three otherdistricts has less than 10,000 households.
Health and Family Planning Service Facilities in the City
Iloilo City has five hospitals, two of which are run by the government while the otherthree are private. One of the government hospitals is located in the Mandurriao District,while the other is located in Lapaz. One of the private hospitals is located in Jaro, while thetwo others are located in the City Proper.

26
The City Health Office (CHO) operates seven main health centers and 20 BarangayHealth Stations. Manning these health centers and stations are 9 physicians, 28 nurses, 10regular midwives, and 25 contractual midwives (CHO Documents). The CHO, likewise,coordinates 360 BHWs all over the city who are mobilized to assist the health personnel inpromoting and implementing the various health programs of DOH including FP.
All the health clinics of the CHO provide FP services. FP supplies, such as condomsand pills, are available in the clinics and health stations. Trained FP personnel conductphysical examinations and evaluate the medical history of prospective and current FP users,conduct pap smear tests for referred current FP users and carry out IUD insertions.
Also providing FP services in the city are three privately-run FP clinics, the ArevaloFamily Planning Clinic, the West Visayas State University (WVSU) Family Planning Clinicin Lapaz and the Family Planning of the Philippines (FPOP) clinic at the Iloilo MissionHospital (IMH) in Jaro. These clinics provide FP supplies such as condom and pills, conductphysical examination of FP clients and IUD insertion, and perform vasectomy and ligation.There are also several private medical clinics located in the various districts in the city whichprovide FP services. These are usually run by private medical practitioners who specializein Family Medicine or Obstetrics and Gynecology.
Although the CPO does not have a clinical facility, it maintains a network of BSPOswho are engaged in the recruitment of FP clients and in the maintenance of FP current users,aside from resupplying their clients with pills and condoms. By the end of 1993, the CPOhad 175 BSPOs.
Table 4 provides detailed information on the distribution of the variables discussedabove, as they are found within the major districts of the city.

27
Table 4. Profile of the Study Area by District
Character- Districtsistics
Arevalo City Jaro Lapaz Mandur MoloProper riao
Total
Area (has.) 506.25 289.18 2987.1 1148.6 1469.5 451.59 6852
No. of Brgys. 13 45 42 37 18 25 180
Population 24,100 56,924 79,829 66,248 30,877 51,527 309,505
AnnualGrowth Rate 3.8 0.4 3.5 1.6 4.1 2.6 2.4
No. of Households 4,581 10,774 14,642 12,242 5,237 9,141 56,617
No. of DayCare Center. 12 17 16 22 6 16 89
No. ofHealth Clinic 1 6 10 7 3 3 30
No. of FPClinics 1 0 1 1 0 0 3
No. ofBHWs 24 9 82 77 37 50 360
No. ofBSPOs 14 51 45 46 19 27 202
The Population/Family Planning Program of Iloilo City
In order to understand and appreciate the roles and functions of the BSPOs and the BHWs in thedelivery of FP services in Iloilo City it would be useful to first examine the city's population/FP program.A brief history of the city's FP program is presented in this section along with the problems and difficultiesencountered in program implementation and some recent program developments.
The Beginnings of the Family Planning Program of Iloilo City
The FP program of Iloilo City started in 1976 as a result of the implementation of the PhilippineGovernment's National Population and Family Planning Outreach Project (NPFPOP), a USAID-fundedproject, managed by the Population Commission (POPCOM). To implement and manage the program at

28
the city level, the CPO was created by the city government through a City Ordinance passed by theSangguniang Panglungsod (City Legislative Council). USAID, through POPCOM, provided contraceptivesupplies, technical support, financial assistance for personnel services and travelling expenses of theoutreach personnel, then called Full-time Outreach Workers (FTOWs). As its counterpart, the citygovernment provided office space, financial assistance for the administrative support staff and officesupplies.
Adopting a phase-in-phase-out scheme, the funding institution and the city government agreed thatthe latter would gradually absorb all financial obligations of the project within a period of eight years. Thiscondition was met by the City Government in 1985, when it assumed full responsibility for the project byabsorbing all CPO personnel as regular permanent employees.
The CPO implemented the project using the Total Integrated Development Approach (TIDA)wherein FP was coordinated with other sectoral concerns. It was community-based and supported by anetwork of volunteer workers, namely the BSPOs. These volunteers were guided and supervised by theCPOs field personnel and the FTOWs, later called the Population Program Officers (PPOs). The BSPOs'major functions included: 1) FP and health, 2) community organization and development, 3) recordkeeping, and 4) participation in community activities. Relative to FP, the BSPOs were tasked to: 1)motivate and remotivate married couples of reproductive age to practice FP, 2) follow up current users,3) make referrals to service centers, and 4) provide contraceptive supplies to users. (CPO Documents).
During the first five years of program implementation, Iloilo City's Population Program meritednational recognition. FP acceptance in Iloilo reached a high record of 18,000 FP acceptors in the early1980's (CPO Records). Owing to this, the CPO was judged as the most outstanding office in Region VI.One of its BSPOs was also chosen as one of the most outstanding BSPOs in the country.
Problems and Difficulties Encountered in FP Program Implementation
In the mid-eighties, some changes in the National FP Program occurred. In particular, managementof the national FP program was transferred at this time from POPCOM to the Department of Health. Asa result, the management of the city's FP program was also delegated to the CHO. Family planninglogistics were also transferred from POPCOM to DOH both for the nation as a whole and within IloiloCity. In point of fact, the CHO had already been providing FP services for some time the concentrationof its services had really been on health. Coordination of the FP program and distribution of FP supplieswere responsibilities had been handled for the most part by the CPO.
Concurrent with these developments were a number of political changes. There was a turnover inthe city government's leadership which resulted in new program priorities and emphases, Family Planningwas now relegated to the "back seat". The CPOs field operations were discontinued and most of CPOpersonnel, including its office head and the PPOs, were detailed in various offices of the city governmentand told to perform various tasks ranging from clerical to technical. The CPO was not abolished outrightbut only three personnel were left to take charge of all administrative functions of the office.
Even so, the CPO's outreach program and its network of BSPOs remained intact. The volunteersreportedly continued to function in the field, even with minimal or no supervision at all. The CPO was ableto continue its operations, thanks to financial assistance from other funding agencies, like the UNICEF. In1988, it was tapped by the UNICEF-Assisted Urban Basic Services Project to organize another group of

29
volunteer workers (the Community Organization Volunteers or COVs) who were tasked with mobilizingthe community for socioeconomic projects. Since they were already in place, the BSPOs were tapped toparticipate as community volunteers. They were thus able to continue performing their FP related functions.
In 1989, the CPO was reactivated. The city government recalled all the CPO staff to their formerpositions. The office resumed field operations and the BSPOs who had become inactive were reactivated.Nevertheless, since the national FP program was already being managed by DOH, the CHO continued toplay a major role in the implementation of the FP program.
The collaboration of the CHO and the CPO in the implementation of the FP program of Iloilo City,has not been without problems. Lack of clear definition of their respective roles in the program, and somemiscommunication problems have reportedly strained relationship between the personnel and volunteersof the two offices. These developments have adversely affected FP program implementation, andconsequently, FP service delivery in the city.
Recent Developments in the Family Planning Program of Iloilo City
With the implementation of the Local Government Code (LGC) and with FP program regainingattention both at the national and at the local level, Iloilo city's FP program has once again been given focusand attention. In 1993, the City Government through an Administrative Order No. 4 Series of 1993 issuedby the Local Executive, designated the CPO as lead agency and over-all coordinator of thePopulation/Family Planning Program of the City of Iloilo (Section 1) and the CHO as a participating agency(Section 3). To improve program coordination the directive specifically defined the functions andresponsibilities of each office in the implementation of the FP program. These functions andresponsibilities are summarized below.
A. Functions and Responsibilities of the City Population Office
The CPO has been designated to perform the following functions and responsibilities:
1. Formulate and implement yearly and/or midterm plans for Family Planning and PopulationDevelopment Program as well as monitor and evaluate the progress/accomplishment of the plannedactivities;
2. Set targets for various FP activities, based on approved standards, as well as the accomplishmentof such targets;
3. Implement IEC activities;
4. Manage logistics and information services;
5. Provide storage facilities for FP supplies and delivers these supplies to all FP providers outlets;
6. Implement referral system. The following clients must be referred to health clinics for completephysical examination and medical history evaluation:
a. All new acceptors b. All high risk or problematic clientsc. All gynecological problems d. All clients needing a yearly pap smear.

31
7. Utilize the BSPOs in dispensing FP supplies to current users, as well as in the motivation andfollow-up of new acceptors, current users, and/or drop-outs;
8. Conduct pre-marital counseling sessions to all MCRAs desiring to be married;
9. Be responsible for all training activities, including: formulation of training designs, budgetpreparation, selection of resource persons and participants, and securing of technical and financialsupport for the training;
10. Gather, consolidate, and submit forms from all FP outlets for the purpose of programreports;
11. Coordinate with different participating agencies concerned with FP;
12. Formulate and implement various livelihood projects in response to opulation and developmentprograms.
B. Functions and Responsibilities of the City Health Office
The CHO, on the other hand, has been given the following functions and responsibilities:
1. The Family Planning Coordinator, in behalf of the CHO, coordinates with the CPO field officersconcerning FP activities, especially on the resupply for New Acceptors and on trainings;
2. All trained FP personnel are expected to perform the following:
a. Conduct complete physical examination and medical history evaluation of all new acceptors andcurrent users referred to the clinic and record these in appropriate forms;
b. Dispense the initial dose or first pack of pills to all new acceptors and explain to them themechanism of action, advantages and disadvantages, side effects, adverse reactions, druginteractions, and most especially the characteristics of the FP method desired by the client, as wellas their follow-up schedule;
c. Conduct physical assessment and medical history evaluation of all prospective IUD clients andexplain to them the mechanism of action, advantages and disadvantages, side effects, adversereactions, procedures of insertion; then do the insertion; warn them of the danger signs and theexpected menstrual changes after insertion.
d. Attend to all referred current users as well as gynecological patients;
e. Conduct a gynecological examination; treat STDs identified, refer complicated cases and thoserequiring surgical intervention.
3. Integrate FP motivation in Pre-partum and post-partum visits of clients including those attendedto by the BHWs and BNS;
4. Make a FP consultation clinic schedule weekly in each BHS/catchment area where there is a trainedpersonnel on FP.
5. Continue motivational activities with all prospective FP clients or MCRAs;
6. Receive all kinds of FP acceptors; whether walk-in or referred cases;

32
7. Make a file record of all FP clients served in the clinic;
8. Be responsible for the storage and dispensing of all FP supplies (pills, condoms) in their respectivedesignated catchment areas; and
9. Coordinate with their respective BSPOs and PPOs assigned in their catchment areas for FP updatesand/or problems.
The BSPOs and BHWs: Their Roles and Responsibilities in the Family Planning Program of IloiloCity
As already mentioned earlier, the functions of the BHWs concentrate on MCH care, while those of theBSPOs focus on FP. Since FP is also a component of maternal health, the BHWs are also expected toperform FP functions similar to those performed by the BSPOs. Described below are the functions andresponsibilities prescribed for the BSPOs and the BHWs.
A. The Functions and Responsibilities of the BSPOs
The functions and responsibilities prescribed for the BSPOs include the following:
1. Collect necessary data and information from the barangay; 2. Motivate MCRAs to practice FP; 3. Follow-up new acceptors and remotivate defaulters; 4. Refer clients to the Barangay Health Clinic; 5. Resupply current users with pills or condoms; 6. Store and keep FP supplies (pills and condoms) and reading materials relating to FP; 7. Conduct an information and education campaign on FP;8. Prepare and keep records;9. Prepare and report number of new acceptors and number of defaulters;
10. Participate in activities/projects of BSPOs such as meetings, seminars or workshops; 11. Support any special project of the CPO regarding population and development.
B. The Functions and Responsibilities of the BHWs
While the functions prescribed for BSPOs tend to be FP-focused, those prescribed for the BHWsencompass a broader sphere of responsibilities. The following are the roles and functions expected of aBHW:
1. As a motivator/counsellor, they are expected to generate acceptors for health services and motivatepeople to practice a healthy lifestyle;
2. As a community organizer, they are expected to provide leadership in organizing/mobilizing thecommunity towards self reliance and to establish or strengthen linkages involving communitymembers, the DOH, the LGU and NGOs;
3. As a health care provider, they must assist in the effective and efficient delivery of health services;
4. As a facilitator, they should assist the community in providing immediate access to health resourcesand provide learning opportunities about health for the community members;
5. As data gatherer/reporter/recorder, they are expected to provide information on health,accomplishments, problems and needs of the community.

33
The BHWs' FP-related tasks include: a) motivation of MCRAS to plan their families, b) referrals ofFP acceptors to the barangay health clinic for their first supply of FP needs, and 3) follow-up FP users anddefaulters. The BHWs are also expected to introduce FP acceptors to the BSPO who will provide themwith additional supplies as needed.
The above information indicates that, relative to FP, the prescribed roles and functions of the BSPOsand the BHWs are more or less the same. As mentioned earlier, the BSPOs and the BHWs play commonroles in the promotion of the FP program in Iloilo City. They are both involved in motivation, follow-up,referrals, counseling and providing FP supplies to the FP clientele. The success of the FP program istherefore dependent on their respective performance.
A recent review of the accomplishment reports of the BSPOs in Iloilo City by the CPO revealedvariations in the BSPOs' performance in the delivery of FP services. While some BSPOs are performingquite well, others are not. Records show that there are BSPOs who had consistently motivated, and referredFP acceptors and users despite the difficulties they have encountered. On the other hand, DOH and CHOstaff members feel likewise about the BHWs' performance. They have noted varying performance on thepart of the BHWs and attribute this to several factors which affect either the volunteers themselves or theirenvironment.

35
SECTION III
THE BSPOS AND BHWS AND THEIR WORK-Profile of the BSPOs and BHWs of Iloilo City
Table 5 presents background information on the two groups analyzed in this study. The BSPO andBHWs in Iloilo City were mostly female (98 percent), with an average age of 46 years. The BSPOs wereslightly older than the BHWs, on the average (49 years old vs. 43 years old). The majority of both groupswere married (84 percent and 83 percent, respectively).
All of the volunteers had attended school, with the majority (86.2 percent) having at least reachedhigh school. About one-third (33 percent) were able to reach college. This latter pattern was a little morecommon among the BSPOs.
The majority of the married volunteers had four or more children (68.8 percent), the average, beingabout five (4.7). Comparatively, the BSPOs' and the BHWs' mean number of children did not differ much,their averages being 5.01 and 4.49, respectively.
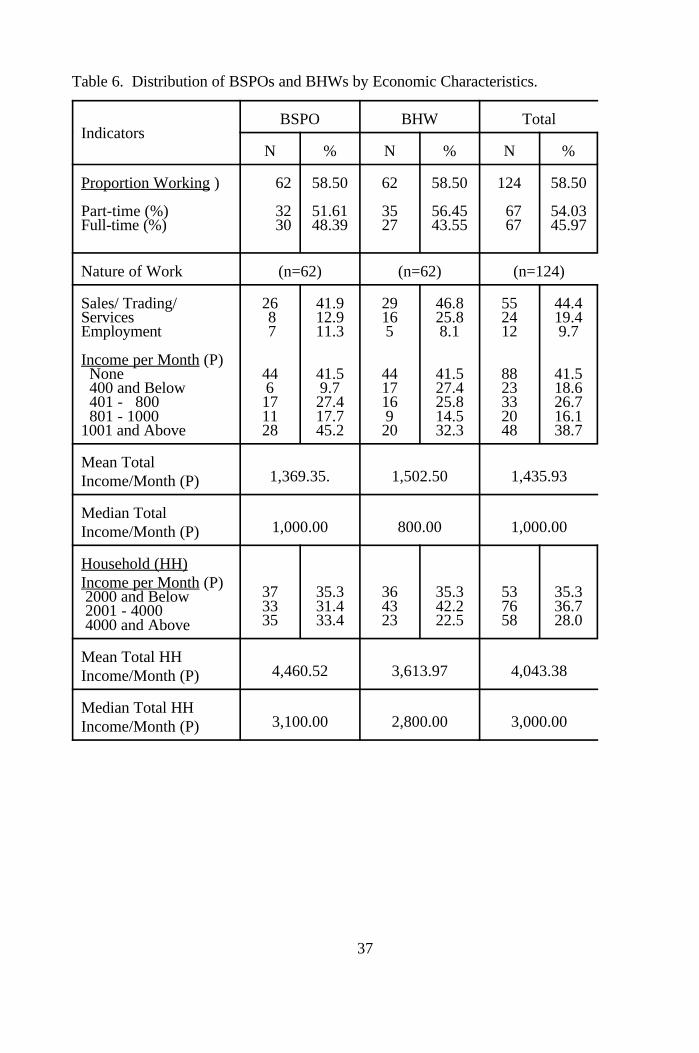
At the time of the survey, slightly more than half of both the BHWs and BSPOs were gainfullyworking (both 58.6 percent), most of whom were engaged in sales/trading/small scale business on a parttime basis (BSPO, 41.94 percent; BHWs 46.77 percent). Table 6 shows that on the average, the workingBHWs were earning P 1501.50 per month, while the working BSPOs were earning a monthly average ofP 1369.65. The BSPOs' household monthly income was posted at P 4460.52, which is more than that ofthe BHWs' (P 3,613). The difference implies that the other working members of the BSPOs' householdsmay be earning more than the working household members of the BHWs.

36
Table 5. Distribution of BSPOs and BHWs by Demographic Characteristics.
Indicators BSPO BHW Total
N % N % N %
Total Respondents 106 100 106 100 212 100Sex: Male 2 2.0 2 2.0 4 2.0 Female 104 98.0 104 98.0 208 98.0
Age in Years: 25 and below 3 2.8 9 8.5 12 5.7 26 - 35 8 7.5 14 13.2 22 10.4 36 - 45 29 27.4 37 34.9 66 31.1 46 - 55 34 32.1 34 32.1 68 32.1 56 - 65 27 25.5 11 10.4 38 17.9 66 and above 5 4.7 1 0.9 6 2.8
Mean Age ( years) 49.35 43.30 46.34
Highest Educ.Attain..: Elementary High School College Others
Civil Status: Single Married Widowed/Separated
No. of Children: None 1 - 3 4 - 6 7 - 9 10 - 20 Not applicable
Mean No. of Children Ever Born
14 13.2 14 13.2 28 13.243 40.6 57 53.8 100 47.243 40.6 27 25.5 70 33.06 5.7 8 7.5 14 6.6
6 5.7 11 10.4 17 8.089 84.0 88 83.0 177 83.511 10.4 7 6.6 18 8.5
1 0.9 4 3.8 5 2.431 29.2 30 28.3 61 28.82 39.6 43 40.6 85 40.1
20 18.9 18 17.0 38 17.96 5.7 0 0.0 6 2.86 5.7 11 10.4 17 8.0
5.01 4.49 4.76(99) (91) (190)
37
Table 6. Distribution of BSPOs and BHWs by Economic Characteristics.
IndicatorsBSPO BHW Total
N % N % N %
Proportion Working ) 62 58.50 62 58.50 124 58.50
Part-time (%) 32 51.61 35 56.45 67 54.03Full-time (%) 30 48.39 27 43.55 67 45.97
Nature of Work (n=62) (n=62) (n=124)
Sales/ Trading/ 26 41.9 29 46.8 55 44.4Services 8 12.9 16 25.8 24 19.4Employment 7 11.3 5 8.1 12 9.7
Income per Month (P) None 44 41.5 44 41.5 88 41.5 400 and Below 6 9.7 17 27.4 23 18.6 401 - 800 17 27.4 16 25.8 33 26.7 801 - 1000 11 17.7 9 14.5 20 16.11001 and Above 28 45.2 20 32.3 48 38.7
Mean TotalIncome/Month (P) 1,369.35. 1,502.50 1,435.93
Median TotalIncome/Month (P) 1,000.00 800.00 1,000.00
Household (HH)Income per Month (P) 2000 and Below 2001 - 4000 4000 and Above
37 35.3 36 35.3 53 35.333 31.4 43 42.2 76 36.735 33.4 23 22.5 58 28.0
Mean Total HHIncome/Month (P) 4,460.52 3,613.97 4,043.38
Median Total HHIncome/Month (P) 3,100.00 2,800.00 3,000.00

38
Selection Process
The community plays an important role in the recruitment and selection of BSPOs
and BHWs in Iloilo City. Based on CPO and CHO records, both groups of volunteers are
recruited through the recommendations of community residents and/or their barangay
leaders, particularly the Barangay Captain. Although the CHO does not use any specific
criteria when selecting their BHWs, preference is given to volunteers who are willing and
committed to serve and those who have time volunteer work. A community leader or a
barangay official, should vouch for the volunteer's willingness and commitment through a
recommendation or endorsement.
A similar recommendation is also a prerequisite for the selection of BSPOs. Among
the community folk who are encouraged to recommend a new volunteer is an active BSPO
or a BSPO resigning or retiring from his/her work. According to CPO personnel, preference
is given to a BSPO volunteers is: 1) willing and committed, 2) availability of time, and 3)
current or former practice of FP.
When the FP program was still under the management of POPCOM, it was a
standard procedure for FTOWs to approach volunteers so as to ask for their help on the
project. The most likely candidates for this position were first determined by means of a
social investigation. Replacements for BSPOs who resign or retire were also recruited in
this case by asking advice from the person stepping down from the job. The respondents' report on how they were recruited confirmed the information
provided by the CHO and the CPO staff regarding the selection of their respective
volunteers. Table 7 shows that most of the BSPOs were reportedly "appointed" (40.6
percent), while most of the BHWs, "volunteered" (37.7 percent) for their posts. The
second most popular means of recruiting the BSPOs was through "recommendation" (34
percent). The BHWs who were directly "appointed" constitute 29.2 percent, while those
who had been "recommended" constitute 25.5 percent.
Political intervention in the recruitment of BSPOs and BHWs was also reported.
Qualitative data revealed that some Barangay Captains and city officials have recommended
individuals not that they were interested or qualified, but because they were politically

39
active and had supported them during the elections. The CHO and the CPO staff claimed
that some of their inactive volunteers were political recommendees.
Table 7. Distribution of BSPOs and BHWs According to How They Were Recruited by Designation.
Indicators BSPO BHW Total
N % N % N %
How volunteers wereselected: Volunteered
Invited
Recommended
Appointed
Others
18 17.0 40 37.7 58 27.4
5 4.7 5 4.7 10 4.7
36 34.0 27 25.5 63 29.7
43 40.6 31 29.2 74 34.9
4 3.8 3 2.8 7 3.3
Total 106 100 106 100 212 100
Training
Training for the BSPOs and BHWs has been either provided by POPCOM, DOH, the
CPO or the CHO staff. When the FP program in Region VI was still being coordinated by
POPCOM, some BSPOs of Iloilo City were selected to undergo POPCOM-conducted
trainings. In the absence of training records, the CPO estimated that about 45-50 BSPOs.
These trainings which focused on leadership skills, FP methods, and motivation processes.
The CPO reported that many of the "original" BSPOs who had undergone formal
training, had already resigned from their posts. Additional recruits, however, have been
provided informal (on-the-job) training by their respective supervisors on their roles and
responsibilities as BSPOs. The PPOs, admitted, however, that these orientation sessions were
limited and may not adequately prepare the volunteers for the performance of their functions.
To remedy this limitation, they have reportedly been providing reinforcements by means of
follow-up instructions during meetings and field visits.

40
The CHO has not provided any formal training to the BHWs. As in the case of the
BSPOs though, this office has been providing a basic orientation on their roles and
responsibilities to this group. A few BHWs have also been selected to attend DOH-sponsored
health-related trainings in the past. It should be pointed out at this juncture, though that the
orientation given the BHWs emphasizes MCH care insofar as this is the main focus of their
community involvement. In general, FP represents only one of the many components
subsumed under MCH.
When queried regarding their training experiences, a big majority of the BSPOs (89.6
percent) attested that they had attended at least one training (Table 8). In comparison, only
29.2 percent of the BHWs had been trined. All the BSPOs reported that the training they had
attended included topics on FP, while 58.1 percent of the trained BHWs reported the same.
MCH was the focus of most trainings attended by the BHWs. The data further disclosed that
at least one of two trainings attended by the volunteers was on FP.
Table 8. Distribution of BSPOs and BHWs by Trainings Attended.
Indicators BSPO BHW TOTAL
N % N % N %
Volunteers whohad attendedtrainings
TYPES OF
TRAININGS
ATTENDED:
Family Planning 2 2 Hilot 4 4 Maternal Care 10 5 BSPO/BHW Trng. 7 5 Others
95 89.6 31 29.2 126 59.4
(N=95 (N=31 (N=126)) )
95 18100.0 58.0 115 91.3 2.1 6.4 4 3.2 4.2 12.9 8 6.3 10.5 16.1 15 11.9
7.4 16.1 12 9.5
Mean Total No. ofTrainings Attended 2.00 1.80 1.91
Mean No. of FPTrainings Attended 1.24 1.10 1.2

41
The Actual Work of BSPOs and BHWs
To determine what tasks the BSPOs and the BHWs actually perform in the field, they
were asked to enumerate work-related activities which they performed in the six months prior
to the interview. Although the volunteers have other tasks aside from those which are FP
related, only the FP related ones were assessed in this study.
The data in Table 9 reveal that the majority of the BSPOs have been performing
almost all of their prescribed FP-related tasks. The most common FP task reportedly
performed by them during the six months prior to interview was "counseling MCRAs on FP"
(86.79 percent). This was closely followed by "motivating MCRAs to practice FP" (84.9
percent), "resupplying current users with contraceptives" (82.02 percent), and "following
up defaulters/drop-outs" (80.19 percent). The least reported among the FP-related activities
was "referrals of MCRAs to health clinic". But even this was also reportedly done by more
than two-thirds of the BSPOs. (This finding was confirmed by the key informants and FGD
participants.)
In addition to their FP activities, the BSPOs were also involved in some other types
of health-related activities. For example, more than one-third of them were involved in data
collection (34.9 percent). This can be attributed to a 1992 effort by the CPO to conduct a
baseline survey of household to establish a benchmark data for the city's population/FP
program. Others were involved in the conduct of home visits (14.2 percent), mother's class
(11.3 percent) and pre-natal referrals (13 percent). Activities which were performed by only
a few (less than 10 percent) of the BSPOs were: preparing reports, assisting during
immunization, collecting laboratory specimen and promoting sanitation (see Table 10).
Turning now to the BHWs, we find this group to be mostly involved in assisting the
health clinic personnel provide MCH care whether in the clinics or in the field (97 percent).
These health care services they provided include: immunization, weighing of children, and
pre- and post-natal counseling. In addition, they were also involved in the health information
drives which accompanied mothers'classes and house visits.

42
Table 9 shows that the most commonly performed FP tasks by the BHWs during the
specified period were: 1) motivating MCRAs to practice FP (72.6 percent) and 2) counseling
them on FP (55.7 percent). Referrals, follow-up of defaulters and resupply of contraceptives
were also being performed, but by only less than half of the BHWs. The least performed FP
task of the BHWs was "resupply of contraceptives to current users" with a mere 13.6 percent.
Comparatively then, it would seem that more BSPOs than BHWs were doing each one of the
five FP-related functions.
As already mentioned, the BHWs' responsibilities concentrated on health care, which
also includes FP. Table 10 shows the variety of health-related activities performed by the
BHWs, in the last six month prior to interview. The three most common activities involved
in by the volunteers were: to assist during immunization day (47.2 percent), to collect
laboratory specimen (34.9 percent), and to refer pre-nataland TB patients (34.3 percent).
Many were also involved in data collection (27.4 percent), as were the BSPOs. Other
activities participated in by more than 20 percent of the BHWs, other than those already
mentioned were: conduct of mothers class (22.7 percent), home visits (23.6 percent), and
assisting at the RHU (20.8 percent).
The reported activities of the BHWs were confirmed by the participants in the
in-depth interviews and FGDs. These same respondents also pointed out that the BHWs
performed other activities which did not come out too strongly in the above listing, namely:
1) to assist in taking vital signs of the clinic clients; 2) to provide post-partum care to mother;
3) to conduct health and sanitation campaigns and 4) to run errands.

43
Table 9. Distribution of BSPOs and BHWs by Family Planning Activities Actually Performed.
FP Activities BSPO BHW TOTAL
N % N % N %
Motivation 90 84.90 77 72.64 167 78.77
Referral 75 70.75 49 46.22 124 58.49
Follow-up 85 80.19 50 47.17 135 63.68
Counsel 92 87.79 59 55.66 151 71.22
Resupply 88 83.01 14 13.20 102 48.11
Table 10. Distribution of BSPOs and BHWs by Other Functions Actually Performed by Them in the Past Six Months.
ACTIVITIES BSPO BHW TOTAL
N % N % N %
Assisted during 8 7.5 50 47.2 58 27.36 immunization
Collected laboratory 6 5.7 37 34.9 43 20.28 specimen
Promoted Sanitation 5 4.7 5 4.7 10 4.72
Weighed Children/ 0 0.0 18 17.0 18 8.49 Feeding
Assisted at the RHU 4 3.8 22 20.8 26 12.26
Prepared Reports 9 8.5 11 10.4 20 9.43
Conducted Data 37 34.9 29 27.4 66 31.13 Collection
Followed Up 0 0.0 17 16.0 17 8.02EPI/TB Patients
Conducted Home Visits
Conducted Mother's Class
Made Referrals for Natal/TB etc.
Others
15 14.2 25 23.6 40 18.87
12 11.3 24 22.7 36 16.98
33 31.1 47 34.3 80 37.74
11 10.4 16 15.1 27 12.74

44
Other Activities Involved in by Volunteers
The volunteers were also involved in community projects and/or activities. It will be
recalled that one of their tasks related to organizing mothers for community development
and/or livelihood projects. Interviews with the PPOs and the supervising nurses and midwives
revealed that the health volunteers did participate in these activities. Volunteers were likewise
encouraged to engage in their own income generating projects for the welfare of their own
families.
An inquiry on this subject revealed that 50 percent of the BSPOs and 21 percent of
the BHWs were involved in livelihood projects during the time of the survey (Please see Table
11). In general, volunteers were involved most heavily in sanitaion/beautification projects,
mothers' classes, the sonstruction of footwalks and capital assistance projects. Interviews
with key informants and FGDs with MCRAs did not fully confirm this picture, though. For
the most part, these respondents stressed the FP-related and helath-related activities of the
volunteers, possibly because they were must acquianted with these functions.

45
Table 11. Distribution of BSPOs and BHWs by Involvement in Livelihood Projects.
Indicators BSPO BHW Total
N % N % N %
Involvement with (n=106 (n=10 (n=212CommunityProjects Not involved 53 84 137 Involved 53 22 75
) 6) )50.0 79.2 64.650.0 20.8 35.4
Mean No. of (n=53) (n=22) (n=75)Livelihood Projects 1.87 1.27 1.69
Types of ProjectsInvolved In
AnimalDispensing
Capital Assistance
Food Processing
Compost Pit Making
Day Care Center/ Mother's Class 19 35.8 10 45.5 29 38.7
Environmental Sanitation
Footwalk/ Construction
Others
4 7.5 1 4.5 5 6.7
2 3.8 9 40.9 11 14.7
2 3.8 0 0.0 2 2.7
0 0.0 2 9.1 2 2.7
19 35.8 6 27.3 25 33.3
11 20.8 13 59.1 24 32.0
0 0.0 3 13.6 3 4.0
Incentives and Other Benefits Received by the Volunteers
As mentioned earlier, the city government provides a monthly incentive of P200.00
to at least one BSPO and two BHWs in every barangay in Iloilo City. In some barangays
where there are more than two BHWs, the P400 allotted for this purpose is reportedly shared
by the active BHWs. In other instances, the BHWs take turns in receiving the incentive.

46
According to the key informants, this monetary incentive was first provided in 1989.
The BSPOs and the BHWs confirmed that they were indeed receiving P200 monthly
as an allowance for their expenses. Table 12 shows that only one of the respondents, a BSPO
who had been in service for only six months, was not receiving any monthly allowance during
the survey period. It was noted however, that some volunteers were receiving more than
P200 a month as indicated by the average monthly receipt of P258.57 for the BSPOs and
P207.62 for the BHWs. This is possible insofar as some volunteers were holding dual roles,
that of a BSPO and BHW at the same time and were receiving the P400 allotted for both
positions every month. Table 13 shows that 18.9 percent of the volunteers included in the
study were holding two functions. All volunteers were aware that this incentive was being
provided by the city government.
When asked whether or not they were contented with their monthly incentives, more
than two-thirds of each group said they were not (74.3 percent, respectively). This
discontented ones expressed that the amount was too small to even cover their field expenses.
Their supervisors and the barangay captains shared the same sentiment. They all agreed that
increasing the incentive would encourage volunteers to work harder to improve their
performance. There were some, however, who believed that even without the BSPOs and
BHWs would still be largely willing and dedicated to continue serving, since they were
volunteers. Most of the volunteers affirmed this view but they also said that they would
welcome an increase in their monthly allowance.
Some CHO personnel expressed concern over different aspects of the incentive
question. They noted, for example, the bigger amount received by those workers who held
dual roles others pointed to the suggestion from some sectors that the incentive be

47
withdrawn. Concerning the first issue, it was noted that some of those who were holding only
single post, and therefore receiving only P200, tended to harbor "resentment" towards their
colleagues who were receiving twice as much. Given this attitude, they expect those
receiving more incentives to do more work than they. This feeling, was also expressed by
some volunteers during the in-depth interviews and FGDs. It was alleged, in fact, that this
has affected the volunteers' performance. Regarding the second question, a CHO official
suggested that, since the incentive issue has created controversies among the volunteers, it
might be more practical to suspend it. He recalled that, in the past, even without incentives,
community volunteers had consistently performed well, even when they were not given
incentives. The typical consequence of the "incentive issue" has thus been a strained
relationship among volunteers, which may also hamper performance. The suggestion to
eliminate all incentives, though, generated strong objections from the volunteers as well as
from some supervisors.
Other Benefits Received By the Volunteers
Some of them reportedly received other additional benefits. Table 13 shows that the
three most common additional benefits received by the BSPOs were: free supplies and some
clothing (32.1 percent), free education (8.5 percent) and money (6.6 percent), free hospital
services, livelihood projects, money and insurance were also received by a few others.
The BHWs also received free education (5.7 percent), and free supplies and clothing (2.8
percent), but the additional benefit received by the most number of them was free hospital
services (16 percent).
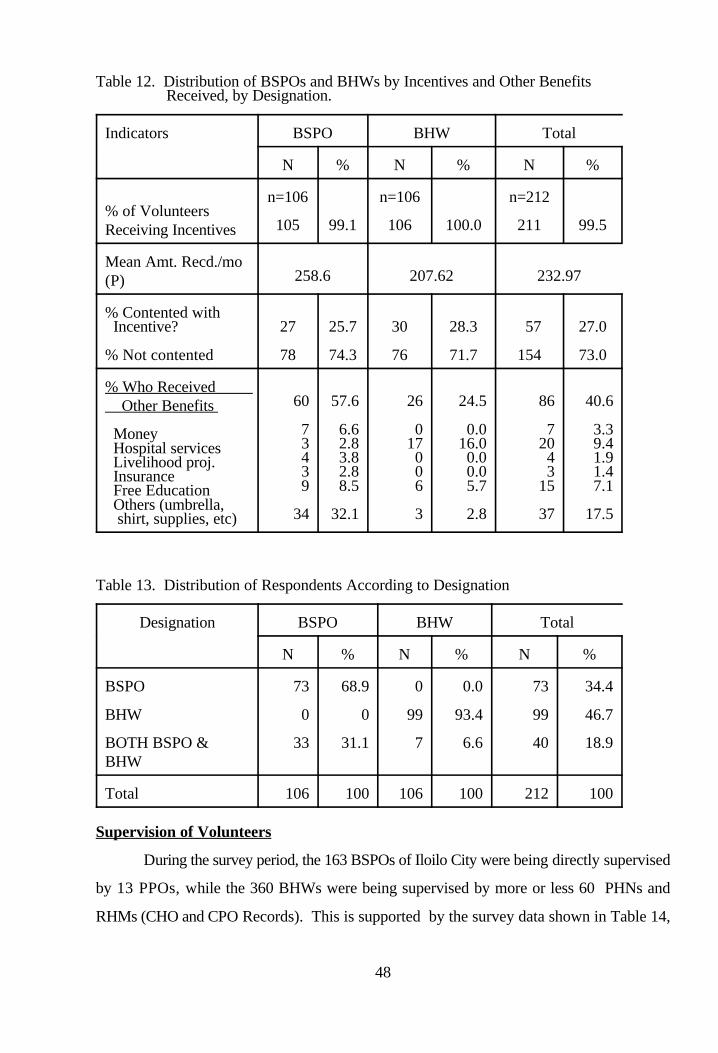
48
Table 12. Distribution of BSPOs and BHWs by Incentives and Other Benefits Received, by Designation.
Indicators BSPO BHW Total
N % N % N %
% of VolunteersReceiving Incentives
n=106 n=106 n=212
105 99.1 106 100.0 211 99.5
Mean Amt. Recd./mo(P) 258.6 207.62 232.97
% Contented with Incentive? 27 25.7 30 28.3 57 27.0
% Not contented 78 74.3 76 71.7 154 73.0
% Who Received Other Benefits
Money Hospital services Livelihood proj. Insurance Free Education Others (umbrella, shirt, supplies, etc)
60 57.6 26 24.5 86 40.6
7 6.6 0 0.0 7 3.33 2.8 17 16.0 20 9.44 3.8 0 0.0 4 1.93 2.8 0 0.0 3 1.49 8.5 6 5.7 15 7.1
34 32.1 3 2.8 37 17.5
Table 13. Distribution of Respondents According to Designation
Designation BSPO BHW Total
N % N % N %
BSPO 73 68.9 0 0.0 73 34.4
BHW 0 0 99 93.4 99 46.7
BOTH BSPO & 33 31.1 7 6.6 40 18.9BHW
Total 106 100 106 100 212 100
Supervision of Volunteers
During the survey period, the 163 BSPOs of Iloilo City were being directly supervised
by 13 PPOs, while the 360 BHWs were being supervised by more or less 60 PHNs and
RHMs (CHO and CPO Records). This is supported by the survey data shown in Table 14,

49
which reveal that a big majority of both BSPOs and the BHWs were indeed being directly
supervised by their respective supervisors (92.5 percent and 95.3 percent respectively). Some
BSPOs who were holding dual posts identified the PHNs/RHMs as their supervisor.
Similarly some of the BHWs who were in the same situation reported their supervisors to be
the PPOs.
The data further confirmed that the community volunteers were being monitored by
their respective supervisors through field visits and meetings. The volunteer-supervisor
interaction or meetings during the month prior to interview averaged two meetings for the
BSPOs and three meetings for the BHWs. Only 23.6 percent of the BSPOs were able to meet
with their supervisors three or more times during the period, as against the 54.7 percent
BHWs who did so. On the other hand, the majority of the BSPOs had met with their
supervisors only twice or even less (76.4 percent) while only 45.3 percent of the BHWs had
met with their supervisors the same number of times. All of the BHWs had reportedly been
visited by their supervisors in the field within the month prior to interview. Except for four,
all the other BSPOs were also visited in the field by their PPOs. The PPOs' visits lasted for
1.77 hours on the average, while those of the PHNs/RHMs lasted more than two hours.
Most of the volunteer-supervisor interactions were initiated by the supervisors, except
for a few which were volunteer-initiated (BSPOs, 20.4 percent; BHWs, 27.6 percent).
Within the week prior to interview, most of the volunteers had had meeting/s with their
supervisors (BHWs, 64.8 percent, BSPOs 50.5 percent). Some BSPOs (10.7 percent) and
BHWs (3.8 percent), however, were not able to meet with their supervisors at all (Table 15).
The rare volunteer-supervisor interaction for some has been attributed to the latter's
work overload. The PPOs admitted that their supervision activities have been usually
constrained by large area coverage and their numerous office-based responsibilities, such as
marriage counseling, report preparation and other related tasks. They lamented that with
each having more than 10 BSPOs to monitor and supervise, they could hardly cope with their
responsibilities. This sentiment was shared by the BSPOs themselves as well as the FGD
participants. The latter reported that they seldom see the PPOs in the community.
Despite the limited volunteer-supervisor interactions, the volunteers still positively
appraised their supervisors in terms of "approachability", "supportiveness", "helpfulness",

50
"flexibility", "consideration", "dedication in their job" and "knowledge of their job". Using
a scale of 1 (lowest) to 5 (highest), the BSPOs gave their PPOs favorable ratings, averaging
between 4.68 (Dedication) and 4.78 (Supportiveness). Similarly, the BHWs gave their
supervisors high ratings, the averages ranging from 4.7 (Consideration) to 4.82 (knowledge
of job). Comparatively, however, the BHWs gave their supervisors slightly higher ratings
than the BSPOs did theirs.
Table 14. Distribution of BSPOs and BHWs by Supervision.
Indicators BSPO BHW Total
N % N % N %
Imm. Supervisor'sDesignation RHM PPO PHN
No. of TimesSupervised /Month No Answer 1 - 2 3 - 4 5 - 6 7 & above
Mean No. of TimesSupervised /Month
No. of Hrs. Spent bySupervisor /Visit No Answer Less than 1 hr. 1 hr-1 hr & 59 min 2 hr-2 hrs & 59 min 3 or more hrs.
Mean No. ofHrs/Visit
Who Initiated the mtg. 0 0.0 7 6.7 7 3.4 PHN/RHM 68 64.1 2 1.9 70 32.7 RHP 22 20.4 29 27.6 51 24.0 PPO 7 6.8 21 20.0 28 13.2 Self 2 1.9 1 1.0 3 1.4 Both Sup. & Self Others
98 2.8 51 48.1 54 25.55 92.5 5 4.7 103 48.6
3
4 3.8 0 0.0 4 1.977 72.6 48 45.3 125 59.021 19.8 47 44.3 68 32.12 1.9 6 5.7 8 3.82 1.9 5 4.7 7 3.3
2.0 3.22 2.6
4 3.8 0 0.0 4 1.99 8.5 6 5.7 15 7.1
50 47.2 41 38.7 91 42.926 24.5 31 29.2 57 26.917 16.1 28 26.4 45 21.2
1.77 2.10 1.94
7 6.8 45 42.9 52 25.0
4.7 50 47.2 55 25.9

51
Table 15. Distribution of BSPOs and BHWs by Supervision.
Indicators BSPO BHW Total
N % N % N %
Recd. Instructionfrom Sup. Last Wk. No Yes
Latest Mtg. withSupervisor:*W/in a wk. prior to interview*1 to 2 wks prior 22 20.4 22 21.0 44 20.7to interview*2 to 4 wks priorto interview*More than 4 wks prior to inter.
Mean Rating ofSupervisor's: Approachability 4.75 4.78 4.77
Supportiveness 4.75 4.74 4.75
Helpfulness 4.70 4.70 4.70
Flexibility 4.68 4.79 4.74
Consideration 4.74 4.82 4.78
Dedication to job
Knowledge of job
35 33.0 17 16.2 52 24.571 67.0 89 83.8 160 75.5
54 50.5 69 64.8 123 57.7
20 18.4 11 10.5 31 14.4
11 10.7 4 3.8 15 7.2
4.71 4.72 4.71
4.78 4.75 4.77

52
The BSPOs' and the BHWs' Interest and Commitment and Satisfaction with their Work.
Considering length of service as the index of interest and commitment, the BSPOs
and BHWs in Iloilo fared quite well in these attributes. This is evidenced by the data in Table
16 which show that the majority of the BSPOs (75.6 percent) and the BHWs (60.4
percent) have been in active service for more than five years. Comparatively, the BSPOs
have been in service longer than the BHWs (9.88 years vs 7.01 years on the average). More
BSPOs than BHWs have served as volunteers for nine years or more (61.4 percent vs.
38.7 percent).
The volunteers' interest and commitment is further demonstrated by the majority's
desire to continue working as volunteers (98.6 percent). Only two BSPOs and one BHW
expressed plan to quit. More BSPOs than BHWs expressed r intention to continue their
volunteer work "until they are able" (51.9 percent and 47.6 percent), respectively). Some
even said they intend "to stay on for life" (24 percent and 23 percent, respectively), while
others said they would work "until their services are needed" (16 percent, and 18 percent,
respectively).
The volunteers' satisfaction with their work is another evidence of their interest and
commitment. Most of them, despite complains about their work, appeared to be quite satisfied
with their work. Using a scale of 1 (lowest) to 5 (highest), they obtained good self-
ratings for "liking their job," the BSPOs, with an average self-assessment of 4.6, and the
BHWs, 4.7. All the volunteers, except one BHW expressed contentment with their work and
rated themselves favorably on this (4.59).

53
Table 16. Distribution of BSPOs and BHWs by Work Experience.
Indicators BSPO BHW Total
N % N % N %
No. of Yrs. inActive Service Less than 1 yr. 1 - 2 3 - 4 5 - 8 9 - 12 13 or more
Mean No. of Yrs.in Active Service
Intends to ContinueWorking 2 1.9 1 0.9 3 1.4 No 104 98.1 105 99.1 209 98.6 Yes
Until When? 55 51.9 50 47.6 105 49.8 Until able 25 24.0 24 22.9 49 23.4 Until alive 17 16.3 19 18.1 36 17.2 Until needed 1 1.0 0 0.0 1 0.5 Two years more 1 1.0 0 0.0 1 0.5 Ten years more 2 1.9 1 1.0 3 1.4 Until year ends 0 0.0 5 4.8 5 2.4 Cannot tell 1 1.0 1 1.0 2 1.0 Until I like it 3 2.9 5 4.8 8 3.8 Others
Mean Rating of 4.54 4.67 4.60Liking the Job
Mean Rating of JobContentment
2 1.9 2 1.9 4 1.921 19.8 26 24.5 47 22.23 2.8 14 13.2 17 8.0
15 14.2 23 21.7 38 17.920 18.9 25 23.6 45 21.245 42.5 16 15.1 61 28.8
9.88 7.01 8.45
4.55 4.64 4.59

54
Family Planning Supplies
It was mentioned earlier that in the early years of the FP program in Iloilo City, the
CPO was the distribution channel of FP supplies. With the transfer of FP management to
DOH, the responsibility of storing and distributing FP supplies was also transferred to the
CHO. This arrangement continued until the implementation of Administrative Order No. 4,
which has designated the CPO to be the distribution channel again of the FP. In 1992 and
1993 when this study was conducted, FP logistics in Iloilo City was still being handled by the
CHO. The FP supplies most commonly distributed by the volunteers were pills and condoms
(See Table 17). The data further reveal that the BSPOs distributed more FP supplies than the
BHWs did. The data further revealed that the FP supplies distributed by the volunteers
were mostly obtained from the CPO or the PPOs. This were true for both the BSPOs and the
BHWs who engaged in contraceptive resupply. It is interesting to note that only a few
volunteers obtained FP supplies directly from the CHO. This confirms the earlier claim of the
CPO personnel and their volunteers that it was difficult to obtain FP supplies from the CHO.
The same claim was reiterated by the volunteers and the CPO personnel during the in-depth
interviews.
To provide the BSPO enough and timely FP supplies, the PPOs reportedly requested
for FP supplies from FPOP clinic who ironically also obtained their supplies from DOH. The
difficulty of sourcing FP supplies from the CHO was attributed by some BSPOs to
antagonistic attitudes of some CHO personnel towards them. This perception was also
shared by some of the PPOs.

60
From the point of view of the CHO personnel, however, they were not aware
or conscious that they were being perceived by the BSPOs as such. Nevertheless,
they also expressed some misgivings regarding the failure of some BSPOs to refer
to the health clinic their FP clients. Cases of new clients having been provided their
first dose of pills by the BSPOs without prior referral to a clinic for examination as
required, were reported. Moreover, the clinic personnel also attested that many of
their FP clients are "walk-in" rather than "referred" ones.
These somewhat tense interactions between the CHO and the CPO volunteers
and personnel have been blamed for the strained relationship prevailing among some
FP workers of both the CHO and the CPO. This has been attributed to lack of clear
definition of the respective roles and functions of the CHO and CPO personnel and
volunteers in the FP program implementation. To counteract the adverse effects of
this relationship problems on FP program implementation the CHO and the CPO
have tried to discuss and resolve the problem. Although as of the conduct of the
study, no concrete results have yet been realized, the consultations are expected to
lessen the problem with the implementation of the Administrative Order No. 4 of the
City Government which clearly stipulates the respective functions and
responsibilities of the CHO and the CPO in the implementation of the city's FP
program. Moreover, with the strict implementation of the FP "Referral System"
(see Appendix E), it is expected that similar problems can be prevented.

61
Table 17. Distribution of Volunteers by Supplies Received by Sources of Supplies and Designation.
Supplies Sources of Supplies
CPO PPO FPOP CHO Total
Received by BSPOs Pills 89 84.0 14 13.2 1 0.9 1 0.9 105 56.1
Condom 66 62.2 12 11.3 1 0.9 0 0.0 79 42.2
IUD 1 0.9 1 0.9 1 0.9 0 0.0 3 1.6
Received by BHWs Pills 6 5.7 0 0.0 0 0.0 0 0.0 6 33.3
Condom 9 8.5 0 0.0 0 0.0 2 1.8 11 61.1
IUD 1 0.9 0 0.0 0 0.0 0 0.0 1 5.6
Received by AllVolunteers Pills 95 44.8 14 6.6 1 0.5 2 0.9 112 54.9
Condom 75 35.5 12 5.7 1 0.5 1 0.5 89 43.6
IUD 2 0.9 1 0.5 0 0.0 0 0.0 3 1.5
The BSPOs' and BHWs' Family Planning Knowledge Attitudes and Practices
Discussed below are the volunteers' FP knowledge, attitudes and practices.
Knowledge. The volunteers' knowledge about family planning was gauged
in terms of their agreement or disagreement to five statements used to measure
knowledge. These include:
1. Sterilization/ligation will make a woman weak.
2. A woman's health suffers more from pregnancy than possible side effectsof using family planning method.

62
3. Male sterilization/vasectomy affects sexual performance.
4. The oral pill can cause cancer.
5. The easiest time for a woman to get pregnant i (given period relative tomenstruation).
The responses to the above statements revealed that both the BSPOs and the BHWs
have "good" knowledge about family planning. The majority of the BSPOs and BHWs
negated three of the most common misconceptions about family planning: 1)
Sterilization/Ligation will make a woman weak"; 2) "Male sterilization/Vasectomy affects
sexual performance"; and 3) "Oral pills can cause cancer." Less than 10 percent of both
groups accepted these three statements (See Table 18).
On the other hand, most of them agreed that: 1) "A woman's health suffers more from
pregnancy than from the effects of using family planning"; and 2) "The easiest time for a
woman to get pregnant is when she engages in sex seven to ten days after menstruation."
More than half of both groups, (but with a higher proportion of the BSPOs) concurred to the
two statements. Comparatively, the BSPOs seemed to be more knowledgeable about FP than
the BHWs.
Attitudes. The volunteers' attitude towards FP planning was measured in terms of their
reaction to the following statements:
1. The best way to plan a family is to have all the children you want as soon aspossible and then stop.
2. People in my village are much too ignorant to really learn how to use

63
contraceptives.
3. I feel comfortable talking about contraceptives.
4. Using contraceptives is against my religion.
5. The best time between the birth of two children is about two years ormore. (Three choices were given.)
The volunteers' responses to the statements indicate that on the whole, the
BSPOs and the BHWs have an open and favorable attitude towards family planning,
especially in the use of contraceptives. The data show that 96 percent of the BSPOs
and 93.4 percent of the BHWs "feel comfortable talking about contraceptives".
Moreover, a big majority of both groups agreed that "two births must be spaced by
two or more years".
Another indication of the volunteers' open attitude towards FP is their
hesitance to admit that, their religion is against the use of contraceptives. Despite the
fact that most of them were Roman Catholics and that the Roman Catholic Church
is openly campaigning against the use of contraceptives, less than 20 percent of
both the BSPOs and the BHWs admitted that: "Using contraception is against their
religion."
The data also imply the influence of culture on the Filipinos' attitudes towards
having children immediately after marriage. The fact that the majority of the BSPOs
and BHWs supported the statement that: "The best way to plan a family is to have
all the children you want as soon as possible and then stop," demonstrates the high
value they give to children and their sexual status.
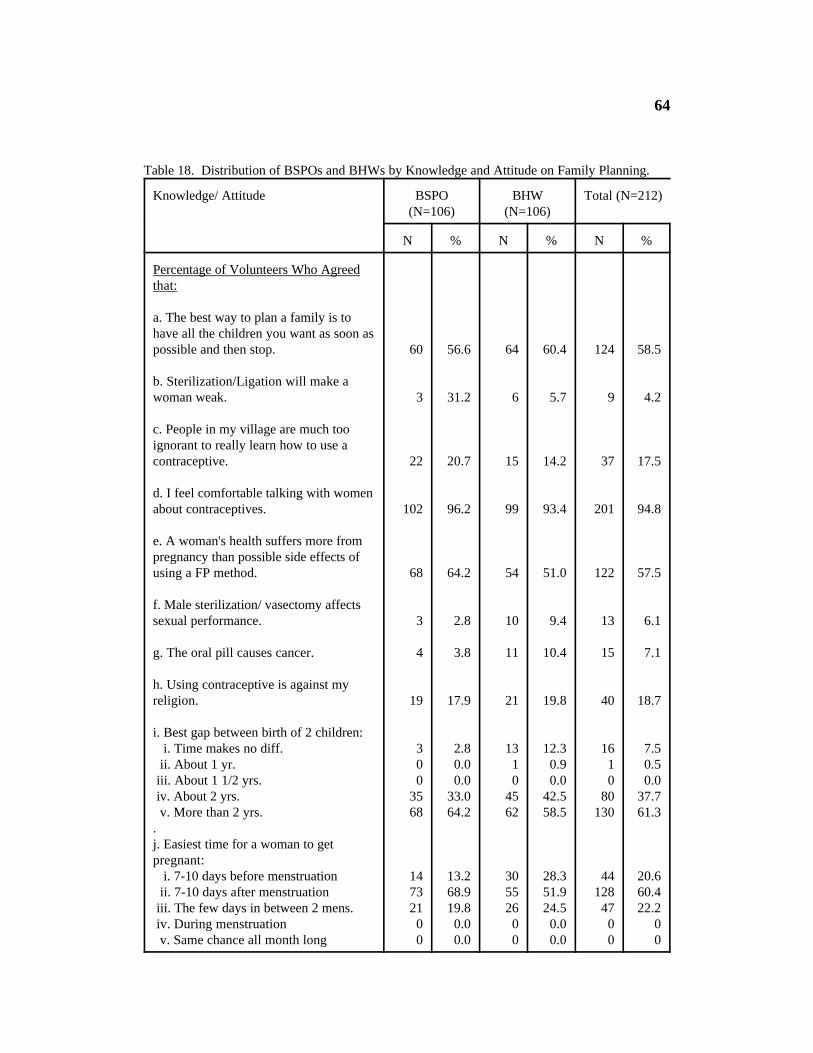
64
Table 18. Distribution of BSPOs and BHWs by Knowledge and Attitude on Family Planning.
Knowledge/ Attitude BSPO BHW Total (N=212)(N=106) (N=106)
N % N % N %
Percentage of Volunteers Who Agreedthat:
a. The best way to plan a family is tohave all the children you want as soon aspossible and then stop. 60 56.6 64 60.4 124 58.5
b. Sterilization/Ligation will make awoman weak. 3 31.2 6 5.7 9 4.2
c. People in my village are much tooignorant to really learn how to use acontraceptive. 22 20.7 15 14.2 37 17.5
d. I feel comfortable talking with womenabout contraceptives. 102 96.2 99 93.4 201 94.8
e. A woman's health suffers more frompregnancy than possible side effects ofusing a FP method. 68 64.2 54 51.0 122 57.5
f. Male sterilization/ vasectomy affectssexual performance. 3 2.8 10 9.4 13 6.1
g. The oral pill causes cancer. 4 3.8 11 10.4 15 7.1
h. Using contraceptive is against myreligion. 19 17.9 21 19.8 40 18.7
i. Best gap between birth of 2 children: i. Time makes no diff. 3 2.8 13 12.3 16 7.5 ii. About 1 yr. 0 0.0 1 0.9 1 0.5 iii. About 1 1/2 yrs. 0 0.0 0 0.0 0 0.0 iv. About 2 yrs. 35 33.0 45 42.5 80 37.7 v. More than 2 yrs. 68 64.2 62 58.5 130 61.3.j. Easiest time for a woman to getpregnant: i. 7-10 days before menstruation 14 13.2 30 28.3 44 20.6 ii. 7-10 days after menstruation 73 68.9 55 51.9 128 60.4 iii. The few days in between 2 mens. 21 19.8 26 24.5 47 22.2 iv. During menstruation 0 0.0 0 0.0 0 0 v. Same chance all month long 0 0.0 0 0.0 0 0

65
FP Practices. Table 19 indicates that of the 100 BSPOs and 95 BHWs who
were or had been married, the majority (73.7 percent) and 73 percent, respectively)
had practised or were practising FP. A little over one-fourth of both groups have
never practised FP.
The most common FP methods used by those who had practiced or were
practising family planning among the BSPOs and BHWs was the pill
(31.1 percent for both). IUD ranked second for the BSPOs (19.8 percent), while for
the BHWs, Natural Family Planning (NFP) emerged the second most popular
method (21.7 percent). NFP ranked third for the BSPOs (19.8 percent), while IUD
had the same priority among the BHWs. Both male and female sterilization
(vasectomy and ligation) and condom were quite unpopular among the volunteers.
Comparatively, however, there were more BSPOs (11 percent) than BHWs
(6.3 percent) who had been ligated. The husband of one BSPO, has been
vasectomized, but there was none among the BHWs' husbands.
At the time of the study, the majority of the currently married community
volunteers were not practicing FP. Only slightly more than one-third of both groups
were currently FP users, 33.7 percent of the BSPOs and 36.4 percent of the BHWs.
Among the three most popularly used FP by the volunteers at the time of the
survey were ligation, NFP, and pills for both groups, but not in the same order of
popularity. Among the BSPOs, the most popular method was ligation (36.7 percent),
while NFP was the most popular among the BHWs (31.2 percent). Pills which

66
ranked third among the BSPO family planning users (16.7 percent), emerged as the
second most popular methods used among the BHWs. Ligation among the BHWs
came as a close third (18.8 percent). Vasectomy and the use of condom still
remained unpopular among the volunteers.
From the data above, it is quite evident that many of the former contraceptive
users among the volunteers have either "graduated" because they are not anymore
reproductive, or have dropped out. Although the number of current NFP users is
lower than those who used this method before, the current users of this method
among the married volunteers is still proportionately higher than the NFP users
before.

67
Table 19. Distribution of BSPOs and BHWs by Family Planning Practice.
Characteristics BSPO BHW Total
N % N % N %
Civil Status n=106 n=106 n=212 Single 6 5.7 11 10.4 17 8.0 Married 89 84.0 88 83.0 177 83.5 Widowed/ 11 10.4 7 6.6 18 8.8 Separated
FP Practice n=100 n=95 n=195 Ever Used 73 73.0 70 73.7 143 73.3 Never Used 27 27.0 25 26.3 52 26.7
FP Method Ever n=73 n=70 n=143Used: Pills 33 31.1 33 31.1 66 31.1 Condom 14 13.2 10 9.4 24 11.3 Ligation 7 7.5 4 4.2 11 5.2 NFP/Rhythm 19 17.9 23 21.7 42 19.8 IUD 21 19.8 13 12.3 34 16.0 Vasectomy 1 1.1 0 0.0 1 0.5
Present FP Practice n=89 n=88 n=177
Using 30 33.7 32 36.4 62 35.0 Not Using 59 66.3 56 63.6 115 65.0
FP Method Used
Pills 5 16.7 7 21.9 12 19.4 Condom 2 6.7 4 12.5 6 9.7 Ligation 11 36.7 6 18.8 17 27.4 NFP/Rhythm 9 30.0 10 31.2 19 30.6 IUD 1 3.3 4 12.5 5 8.1 Vasectomy 1 3.3 0 0.0 1 1.6 Both Condom & NFP 1 3.3 1 3.1 2 3.2
n=30 n=32 n=62

68
BSPOs' and BHWs' FP Performance
As operationally defined earlier, performance in the delivery of FP services
in this study is measured in terms of the number of MCRAs motivated, referred,
followed-up, counseled and provided FP supplies. While the volunteers have many
other functions other than the FP-related ones, only their performance in the area of
FP was appraised.
It is important to reiterate that the original plan was to measure FP
performance in terms of number of FP clients reached or attended to relative to
targets, however, this was not realized because, as learned only during the data
collection stage, the CPO and the CHO did not have officially established FP targets
during the period covered by the study. Likewise, most of the volunteers did not also
have targets. Although some respondents specified their targets when asked about
them, their supervisors cautioned that these may not be accurate. This prompted the
change in the indicator of FP performance to number of FP clients motivated,
followed-up, referred, counseled and provided FP supplies. Table 20 and 21 show
the data on the volunteers' performance in the delivery of FP services.
Number of clients served. Table 20 indicates that on the average, the
volunteers taken as a whole were able to serve about 11 clients a week within the
month prior to interview. The BSPOs notably registered a better accomplishment
(12.09) than the BHWs (9.36) in terms of number of FP clients served. This was
consistent with their performance the week immediately prior to interviews, during

69
which they had attended to an average of 11 and 6 FP clients, respectively.
Time spent in FP activities. The BSPOs spent an average of 5 hours a week
on their FP functions, during their three-day week volunteer work. The BHWs, on
the other hand, being more preoccupied with health-related functions, spent an
average of 3 hours per week on FP activities during the same period.
With regards to how active they were in their jobs, on a scale of 1 (lowest) to
5 (highest), the BSPOs and BHWs rated themselves positively. They obtained an
average of 4.29 and 4.46, respectively, the BSPOs giving themselves a lower rating
than the BHWs did themselves.
The BSPOs worked slightly longer the week prior to interview (mean of
3.54 days) than the BHWs did (3.11 days). This is probably why the BSPOs were
also able to attend to more FP cases (11.76 on the average) than the BHWs did (7.73,
on the average).
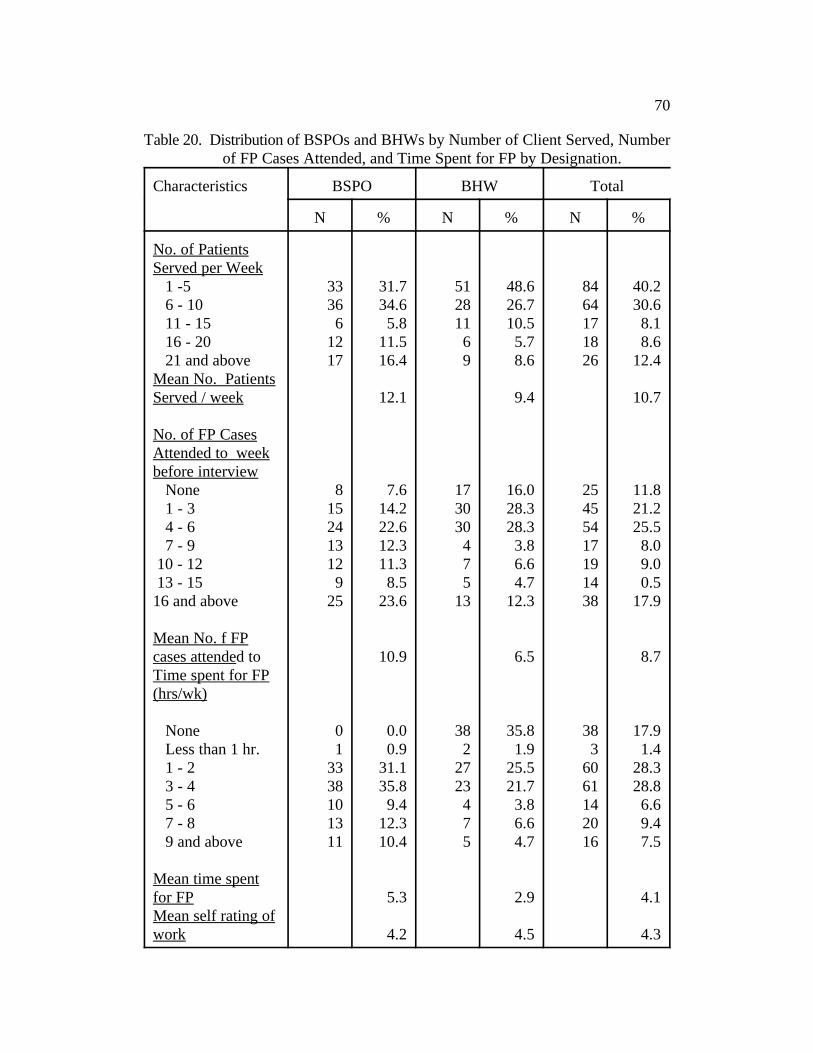
70
Table 20. Distribution of BSPOs and BHWs by Number of Client Served, Number of FP Cases Attended, and Time Spent for FP by Designation.
Characteristics BSPO BHW Total
N % N % N %
No. of PatientsServed per Week 1 -5 33 31.7 51 48.6 84 40.2 6 - 10 36 34.6 28 26.7 64 30.6 11 - 15 6 5.8 11 10.5 17 8.1 16 - 20 12 11.5 6 5.7 18 8.6 21 and above 17 16.4 9 8.6 26 12.4Mean No. PatientsServed / week 12.1 9.4 10.7
No. of FP CasesAttended to weekbefore interview None 8 7.6 17 16.0 25 11.8 1 - 3 15 14.2 30 28.3 45 21.2 4 - 6 24 22.6 30 28.3 54 25.5 7 - 9 13 12.3 4 3.8 17 8.0 10 - 12 12 11.3 7 6.6 19 9.0 13 - 15 9 8.5 5 4.7 14 0.516 and above 25 23.6 13 12.3 38 17.9
Mean No. f FPcases attended to 10.9 6.5 8.7Time spent for FP(hrs/wk)
None 0 0.0 38 35.8 38 17.9 Less than 1 hr. 1 0.9 2 1.9 3 1.4 1 - 2 33 31.1 27 25.5 60 28.3 3 - 4 38 35.8 23 21.7 61 28.8 5 - 6 10 9.4 4 3.8 14 6.6 7 - 8 13 12.3 7 6.6 20 9.4 9 and above 11 10.4 5 4.7 16 7.5
Mean time spentfor FP 5.3 2.9 4.1Mean self rating ofwork 4.2 4.5 4.3

71
Table 21 presents the volunteers' FP performance in terms of number of FP
clients motivated, followed-up, referred, counseled and provided FP supplies by the
volunteers during the month prior to interview.
FP clients motivated. The data show that 90 of the 106 BSPOs and only 77
of the 106 BHWs interviewed were able to motivate potential or current FP users
during the previous month. On the whole, all the volunteers were able to motivate
an average of 9.5 FP clients, with the BSPOs registering a higher accomplishment,
(13, on the average) than the BHWs (6 on the average). This confirms the
volunteers' and their supervisors' report that the BHWs, being involved in mostly
health-related functions usually do not put so much priority on their FP functions.
FP clients referred. The number of volunteers who were able to make FP
referrals to the health clinics was much fewer than those who had motivated and
followed-up FP clients. Only 75 BSPOs and 45 BHWs were able to do so. The
number of clients whom they were able to refer averaged 5 for the BSPOs and 6 for
the BHWs. It was noted that the BHWs were able to refer one more FP case (6) than
the BSPOs did (5).
FP clients followed-up. The data further show that while most (85 out of the
106) of the BSPOs were able to follow-up FP clients, either potential users or
defaulters, during the previous month, only 50 of the BHWs were able to do so. The
BSPOs averaged six FP follow-ups, while the BHWs averaged only five. This is
another indication of the better FP performance of the BSPOs than the BHWs.

72
FP clients counseled. The majority of the BSPOs (92 of the 106), but only
59 of the BHWs were able to provide FP counseling. Those who did among the
BSPOs were able to advise an average of 11 FP clients, while those who did among
the BHWs were able to reach only an average of 6 mothers.
FP clients provided with FP supplies. Distributions of FP supplies to clients
was more popular among the BSPOs than among the BHWs as indicated in Table
21. The data show that while 88 BSPOs were able to provide FP supplies to their
clients, only a mere 14 BHWs were able to do so. Within the six month period prior
to interview, the BSPOs distributed FP supplies to an average of 21 contraceptive
users, while the few BHWs who did so, resupplied only an average of 14 users.

73
Table 21. Distribution of BSPOs and BHWs by Performance.
FP Activities BSPO BHW Total
N % N % N %
No. of volunteersinv.in motivation
Mean no. of clientsmotivated
No. of volunteers inv.in referral
Mean no. of clients 6.1 5.3 5.8referred
No. of volunteers inv.in follow-up
Mean no. of clientsfollowed-up
No. of volunteers inv.in counsel.
Mean no. of clientscounseled
No. of volunteers inv.in resupply 21.4 13.6 20.4
Mean no. of clientsprovided FP supplies
90 84.9 77 72.6 167 78.8
75 70.8 49 46.2 124 58.5
85 80.2 50 47.2 135 63.7
92 87.8 59 55.7 151 71.2
88 83.0 14 13.2 102 48.1
12.7 5.8 9.5
11.2 5.8 9.2
11.0 6.3 9.2
74
Factors Influencing Volunteers' FP Performance
As earlier hypothesized, FP performance of the volunteers may be influenced
by a number of factors, such as: attendance in FP training, knowledge and attitudes on
FP, relationship between volunteers and supervisors, time spent by volunteers on FP
activities, interest and commitment, satisfaction with incentives, supervision received
and designation/position held by the volunteers. The results of the correlation analysis
between these variables and the volunteers FP performance are presented in Table 22
.
Attendance in FP training. Table 22 shows that attendance in FP training is
significantly correlated with FP performance. This is indicated by significant positive
correlations between number of FP trainings attended by the volunteers and the
number of FP clients they had followed-up (r = .24), counseled (r =.22), and provided
FP supplies (r = .35). The positive influence of training on performance is further
demonstrated in Table 23 (Appendix) that shows that volunteers who had attended FP
training performed better than those who had not. Similarly, those who had attended
three or more trainings were able to motivate, refer, follow-up, counsel and provide
FP supplies to more clients than those who had attended only one or two FP trainings.
This means that training indeed improves performance.
Time spent on FP functions and FP performance. The results of the
correlation analysis also proved that the amount of time spent by the volunteers on
FP activities impinges on their FP performance. Significant positive correlation
was found between the predictor variable and the volunteers' FP performance as

75
measured by number of FP clients motivated (r = .21), referred (r =.14), followed-up
(r = .19), counseled (r = .19), and provided FP supplies (r = .24). The
crosstabulation (See Table 27 in Appendix A) supports the positive influence of
time spent on FP functions on FP performance, as indicated by the greater number
of FP clients motivated, referred, followed-up, counseled, and provided FP supplies
by those who have spent more than three hours a week on FP functions than those
who spent less time on them. This means that the volunteers' FP performance will
improve if they allot more time to their FP responsibilities.
Knowledge and attitudes towards FP and FP performance. The correlation
values between FP knowledge and number of FP clients motivated (r = .01),
referred (r = .11), followed-up ( r = .08), counseled (r =.06) and provided FP
supplies (r = .06) were all not statistically significant. This means that knowledge
on FP as measured by the indicators used in this study does not have significant
bearing on the volunteers' FP performance. The volunteers' attitudes towards FP
was not also found to be significantly correlated with FP performance, all correlation
values being negligible and not significant at five percent level (See Table 22). The
crosstabulation of the determinant variable and FP performance presented in Table
25 further attest to this. This data, however, should be treated and interpreted with
caution, since knowledge and attitudes of the volunteers did not vary very much,
most of them exhibiting good FP knowledge and favorable FP attitudes.
Interest and commitment. The volunteers' interest and commitment to their
work as gauged by their length of active service as volunteers was found to

76
significantly contribute to the improvement of their FP performance. The correlation
values between the FP performance and number of MCRAs referred (r =.18),
followed-up (r = .14), counseled (r = .16), and provided FP supplies (r = .28)
were all significant at 5 percent level. The crosstabulation between the two target
variables further demonstrates the positive contribution of length of service or
experience to FP performance. This is manifested by the higher proportions of
volunteers who have motivated, referred, followed-up, counseled and provided FP
supplies to more than five FP clients among those who had been in active service for
more than five years than those who have served for a shorter period of time. The
average number of MCRAs served under each length of service category
corroborates the correlation findings. This can be further interpreted as: FP
performance or the volunteer's performance improves as one stays longer in the
service.
Involvement in community/livelihood projects. It was earlier argued that
involvement in community project by the volunteers would give them the chance to
interact with the people in the community and in effect make them more acquainted
with the people and their needs. The results of the correlation analysis tended to
support this position, since most of the correlation values between involvement in
community projects and number of FP clients referred (r = .19), followed-up
(r = .15), counseled (r = .13), and provided FP supplies (r = .27) were all significant
at 5 percent level. Furthermore, the crosstabulation between the two target variables
clearly shows that those involved in community activities/livelihood projects were

77
able to motivate, follow-up, refer, counsel and provide FP supplies to more FP clients
than those who were not involved in any community project (see also mean number of
clients served under each project involvement category. Based on this, it can be deduced
that a greater interaction with the -community makes a volunteer a more effective FP
worker.
Supervision and FP performance. To reiterate, supervision in this study is indicated
by the number of meetings a volunteer had with his/her supervisors and the amount of
time spent by a supervisor with the volunteer during their meetings/visits. While
number of meetings with the supervisors was found to have no significant bearing on the
volunteers' performance, the amount of time spent by the supervisors with the volunteers
was found to significantly influence all the indicators of FP performance, except the
number of clients provided with FP supplies. This implies that the number of
volunteer-supervisor interaction may not be as important as the amount of time spent in
the interaction or probably the quality of supervision.
An interesting pattern was also noted in the crosstabulation. While in most cases,
the number of FP clients served increased with the increase in time spent by the
supervisors during meetings or visits, some volunteers who were never visited by their
supervisors, and therefore had zero interaction with them performed consistently. This
may be a case of volunteers who have been in service for a long time already and may
already be so efficient so as not to need any supervision anymore. PPO supervisors have
mentioned that they have a number of BSPOs, who even during the time that the field

78
operations of the CPO was paralyzed, still functioned effectively. In most cases, those
who have been in service for a long time, do not seem to need any supervision anymore.
Reports on such cases were made by PPOs during in-depth interviews. It will be
recalled that when the CPO field operation was stopped in the early eighties, some
volunteers were reported to have continued to be active even with minimal or no
supervision at all.
Position/designation and FP performance. The hypothesis that number or type of
position/s held by the volunteers has significant bearing on their performance finds
support in this study. Table 33 shows that the BSPOs performed better than the BHWs,
and volunteers who served both as BSPO and BHW also performed better than the
BHWs.

79
Table 22. Correlation Values Between Performance and Selected Variables.
Independent PerformanceVariables
Motiv Referred Followe Coun- Resupated- selled pliedd-up
FP TrainingAttendance
KnowledgeTowards FP
AttitudeTowards FP
Relation withSupervisors(rating)
Time Spent in FP
Interest andCommitment
Satisfaction w/Incentive
Involvement inLive. Proj.
No. of Mtg. w/Superv.
0.07 0.05 0.24* 0.22* 0.35*
0.01 0.11 0.08 0.06 0.06
0.11 0.01 0.01 0.03 0.07
-0.06 0.05 0.04 0.02 0.02
0.21* 0.14* 0.19* 0.19* 0.24*
0.06 0.18* 0.14* 0.16* 0.28*
-0.001 -0.04 0.07 0.01 0.04
0.04 0.19* 0.15* 0.13* 0.27*
-0.02 0.13* 0.13* 0.07 -0.25*
*Significant at 5% level.

80
SECTION IV
THE BSPOS AND THE BHWS: VIEWS FROM THE
COMMUNITY AND OTHER FP WORKERS
This section presents views of the community and other FP workers
regarding the BSPOs and the BHWs, most especially their role and performance in
the FP program. Based largely on qualitative data generated from in-depth interviews
and FGDs with community folk and other FP workers, this section delves into: 1)
the volunteers' role in he FP program, 2) their interaction with the community or
other FP workers, 3) the attributes of an effective FP volunteer, and 4) suggestions
on how to improve the FP performance of volunteers. The community viewpoint is
brought out in this case by Barangay Captains (BCs), mothers and Barangay
Nutrition Scholars (BNS; while the FP workers is based on comments frrom CPO
and CHO office/clinic and field personnel consisting of office heads, FP
Coordinators, PHNs, RHMs, and PPOs.
The BSPOs and the BHWs: The Community's View
On the BSPOs' and the BHWs' Role in the FP Program
The community folks acknowledged the important contribution of the BSPOs
and the BHWs in the promotion of health and FP in the barangays. The BCs,

81
mothers and BNS all recognized that the volunteers have helped disseminate FP
information, motivate and follow-up FP users, advise mothers on FP, and distribute
FP supplies. Between the two groups of volunteers, the BSPOs were viewed by the
community as more active in FP promotion and implementation. They concurred
that the BSPOs are really FP workers, while the BHWs are basically health workers,
who are involved in FP promotion as part of their health care functions While they
see the BSPOs mainly as FP motivators, FP counselors and FP supply distributors,
they see the BHWs as the connecting link between the DOH and the community in
the area of health service delivery.
The key informants vividly recalled that the BHWs assist in the health
clinics, help during immunization, attend or conduct mothers' classes, weigh
children, promote the DOH health programs, and promote sanitation in the
barangays. FP activities of the BHWs remembered by the key informants include:
attending to FP clients during clinic days or in the field when they make house visits
and provide FP advice to mothers or couples, especially when mothers seek pre-natal
or post-natal care or advice. They stressed however, that the volunteers' work is
concentrated on health care and their FP involvement is only minimal. This
information corroborates the report of the BHWs and the BSPO on their actual
activities.
The BCs, BNSs and mothers agreed that most of the BSPOs and BHWs are
active. The BCs estimated that around 75-90 percent of the volunteers are active.
The BNS and the mothers, however, gave a more conservative estimates of active

82
volunteers placing this figure at 50-75 percent. Even though community key
informants, emphasized that there are some inactive volunteers who are not serious
about their work, they favorably assessed the volunteers' performance in
accomplishing their respective functions.
On Volunteers'Interaction with the Community
Almost all of the BCs and the BNS were acquainted with a BSPO or a BHWs
in their barangay. The BCs confirmed the earlier report about on the selection of
volunteers by saying that they have recommended or endorsed BSPOs and BHWs
for appointment. One BC, however, did not know the BSPO in his barangay. He
said that the barangay does not have one. The BNS in the same barangay also made
the same report.
Although most of the mothers knew a BSPO or a BHW in their barangay,
there were also those who were not familiar with any volunteer. Those who were
not, had reportedly heard about BSPOs and BHWs and what they do, but claimed
that they have not yet met any of them, nor do they know where they live.
The BCs, BNSs and mothers expect the volunteers to constantly interact with
the people in the community, especially with the mothers and their children. A few
mothers lamented that some volunteers do not conduct house visits. Instead, they
"just wait for their clients to go to them." Since they have less contact with the
people in the community, many people do not know them and therefore they cannot
be of help.

83
Both the BCs and the mothers say that active BSPOs and BHWs are generally
popular in the community. They said that the active ones are involved not only in
health and FP activities, but also in community projects and activities. Two BCs
reported that their community volunteers sometimes attend barangay meetings or
assemblies and participate in the discussion of barangay concerns, such as
population, health and the like. The BNS (who are involved in the promotion of the
community nutrition program) also reported that the active volunteers assist them in
the collection of nutrition and health data.
On Attributes of an Effective FP Volunteer
For the community folks, an effective BSPO/BHW is one who: conducts
home visits, concerned with her clients, committed to her job, possessed of good
public relations, active in the health or FP information campaign, and helpful to the
clients. The BNSs added that an effective BHW updates and regularly prepares
reports, attends meetings regularly and assists the health personnel during clinic
days. As for the mothers their idea of a good BSPO as someone who is responsive
to their needs, easily able to identify potential FP acceptors, and a good motivator.
Even while admitting that the community volunteers have contributed much
to the FP program in their barangay, the key informants acknowledged that some of
the volunteers could not effectively perform their FP functions and responsibilities.
According to this view, the volunteers lack training and encouragement from their
supervisors. They also have to contend with the negative attitudes that some clients

84
hold towards them. Financial constraints, family problems, and delay in the release
of incentives were also blamed for the poor performance of some volunteers. The
key informants also expressed preference for volunteers who can effectively
communicate and relate to the people. They agreed that volunteers who possess good
communication skills can effectively motivate people to accept and practice FP to
improve their health practices. For this group, volunteers who can relate well to the
people in the community are generally more acceptable, thereby bocoming more
effective.
Some key informants noted that only very few men are involved in FP
promotion. They expressed that men can be effective FP motivators if given the
responsibility and the right training. The mothers believed that since men usually
make the final decision, especially on critical matters, like family planning practice,
they should be actively involved in the family planning program, not only as targets
but also as motivators. They believed that men could be more convincing than
women in motivating other men to practice FP.
Some Suggestions on Improving the FP Performance of Volunteers
The BCs, mothers, and the BNSs agreed that volunteers should be closely
supervised to further improve their performance. They also agreed that an increase
in their incentives can further encourage them to be more active. Further training
on FP according to them can improve their work. The BNS added that it might help
if the volunteers were to be provided with their own kits and health or FP supplies.

85
The BCs also suggested that giving due recognition to the volunteers who perform
well will further enhance their performance. They added that it would also help if
the volunteers could be provided health insurance so they can be protected. They are
convinced that the volunteers' performance can be improved if the clients improve
their attitude towards them. Good relationship between volunteers and supervisors
was also mentioned as another facilitating factor in improving volunteer
performance.

85
SECTION IV
THE BSPOS AND THE BHWS: VIEWS FROM THECOMMUNITY AND OTHER FP WORKERS
This section presents views of the community and other FP workers regarding theBSPOs and the BHWs, most especially their role and performance in the FP program. Basedlargely on qualitative data generated from in-depth interviews and FGDs with community folkand other FP workers, this section delves into: 1) the volunteers' role in he FP program, 2)their interaction with the community or other FP workers, 3) the attributes of an effective FPvolunteer, and 4) suggestions on how to improve the FP performance of volunteers. Thecommunity viewpoint is brought out in this case by Barangay Captains (BCs), mothers andBarangay Nutrition Scholars (BNS; while the FP workers is based on comments frrom CPOand CHO office/clinic and field personnel consisting of office heads, FP Coordinators, PHNs,RHMs, and PPOs.
The BSPOs and the BHWs: The Community's ViewOn the BSPOs' and the BHWs' Role in the FP Program
The community folks acknowledged the important contribution of the BSPOs and theBHWs in the promotion of health and FP in the barangays. The BCs, mothers and BNS allrecognized that the volunteers have helped disseminate FP information, motivate andfollow-up FP users, advise mothers on FP, and distribute FP supplies. Between the twogroups of volunteers, the BSPOs were viewed by the community as more active in FPpromotion and implementation. They concurred that the BSPOs are really FP workers, whilethe BHWs are basically health workers, who are involved in FP promotion as part of theirhealth care functions While they see the BSPOs mainly as FP motivators, FP counselors andFP supply distributors, they see the BHWs as the connecting link between the DOH and thecommunity in the area of health service delivery.
The key informants vividly recalled that the BHWs assist in the health clinics, helpduring immunization, attend or conduct mothers' classes, weigh children, promote the DOHhealth programs, and promote sanitation in the barangays. FP activities of the BHWsremembered by the key informants include: attending to FP clients during clinic days or in thefield when they make house visits and provide FP advice to mothers or couples, especiallywhen mothers seek pre-natal or post-natal care or advice. They stressed however, that thevolunteers' work is concentrated on health care and their FP involvement is only minimal.This information corroborates the report of the BHWs and the BSPO on their actualactivities.
The BCs, BNSs and mothers agreed that most of the BSPOs and BHWs are active.The BCs estimated that around 75-90 percent of the volunteers are active. The BNS and themothers, however, gave a more conservative estimates of active volunteers placing this figureat 50-75 percent. Even though community key informants, emphasized that there are someinactive volunteers who are not serious about their work, they favorably assessed thevolunteers' performance in accomplishing their respective functions.

86
On Volunteers'Interaction with the Community
Almost all of the BCs and the BNS were acquainted with a BSPO or a BHWs in theirbarangay. The BCs confirmed the earlier report about on the selection of volunteers by saying thatthey have recommended or endorsed BSPOs and BHWs for appointment. One BC, however, didnot know the BSPO in his barangay. He said that the barangay does not have one. The BNS inthe same barangay also made the same report.
Although most of the mothers knew a BSPO or a BHW in their barangay, there were alsothose who were not familiar with any volunteer. Those who were not, had reportedly heard aboutBSPOs and BHWs and what they do, but claimed that they have not yet met any of them, nor dothey know where they live.
The BCs, BNSs and mothers expect the volunteers to constantly interact with the peoplein the community, especially with the mothers and their children. A few mothers lamented thatsome volunteers do not conduct house visits. Instead, they "just wait for their clients to go tothem." Since they have less contact with the people in the community, many people do not knowthem and therefore they cannot be of help.
Both the BCs and the mothers say that active BSPOs and BHWs are generally popular inthe community. They said that the active ones are involved not only in health and FP activities,but also in community projects and activities. Two BCs reported that their community volunteerssometimes attend barangay meetings or assemblies and participate in the discussion of barangayconcerns, such as population, health and the like. The BNS (who are involved in the promotionof the community nutrition program) also reported that the active volunteers assist them in thecollection of nutrition and health data.
On Attributes of an Effective FP Volunteer
For the community folks, an effective BSPO/BHW is one who: conducts home visits,concerned with her clients, committed to her job, possessed of good public relations, active in thehealth or FP information campaign, and helpful to the clients.
The BNSs added that an effective BHW updates and regularly prepares reports, attends meetingsregularly and assists the health personnel during clinic days. As for the mothers their idea of agood BSPO as someone who is responsive to their needs, easily able to identify potential FPacceptors, and a good motivator.
Even while admitting that the community volunteers have contributed much to the FPprogram in their barangay, the key informants acknowledged that some of the volunteers couldnot effectively perform their FP functions and responsibilities. According to this view, thevolunteers lack training and encouragement from their supervisors. They also have to contend withthe negative attitudes that some clients hold towards them. Financial constraints, family problems,and delay in the release of incentives were also blamed for the poor performance of somevolunteers. The key informants also expressed preference for volunteers who can effectivelycommunicate and relate to the people. They agreed that volunteers who possess good

87
communication skills can effectively motivate people to accept and practice FP to improve theirhealth practices. For this group, volunteers who can relate well to the people in the communityare generally more acceptable, thereby bocoming more effective.
Some key informants noted that only very few men are involved in FP promotion. Theyexpressed that men can be effective FP motivators if given the responsibility and the right training.The mothers believed that since men usually make the final decision, especially on critical matters,like family planning practice, they should be actively involved in the family planning program, notonly as targets but also as motivators. They believed that men could be more convincing thanwomen in motivating other men to practice FP.
Some Suggestions on Improving the FP Performance of Volunteers
The BCs, mothers, and the BNSs agreed that volunteers should be closely supervised tofurther improve their performance. They also agreed that an increase in their incentives can furtherencourage them to be more active. Further training on FP according to them can improve theirwork. The BNS added that it might help if the volunteers were to be provided with their own kitsand health or FP supplies. The BCs also suggested that giving due recognition to the volunteerswho perform well will further enhance their performance. They added that it would also help ifthe volunteers could be provided health insurance so they can be protected. They are convincedthat the volunteers' performance can be improved if the clients improve their attitude towards them. Good relationship between volunteers and supervisors was also mentioned as anotherfacilitating factor in improving volunteer performance.
The BSPOs and the BHWs: the FP Workers' ViewsOn the Volunteers' Role in Family Planning
The FP workers in the community, particularly the CHO and the CPO field/clinic personnelin Iloilo City recognized the BSPOs and BHWs as their partners in health and FP promotion. TheBHWs, in particular, were viewed by the CHO personnel as their link to the community. Theyadmitted that there is health manpower shortage in the city and many people could not availofhealth services because they do not have access to them. They agreedthat the BHWs have helpedfill the gap and made health services more accessible to the people. They also added that thepresence of volunteers and their assistance can reduce the workload of the health personnel.
In the promotion of FP, the CHO personnel stressed that the BSPOs are more effectivethan the BHWs because BSPOs concentrate on FP-related functions. Although the BHWs are alsoexpected to attend to FP clients, they counld not spend as much time on this as the BSPOs sincetheir functions and responsibilities are concentrated on health care.
In appraising the FP performance of the BSPOs and the BHWs, the FP workers gave the volunteers a generally favorable rating. Some CPO workers, however, rated theBHWs slightly lower than they did the BSPOs. Correspondingly, some CHO workers also ratedthe BSPOs lower than they did the BHWs.
Although FP is one of the major concerns of the CHO, the health personnel admitted thattheir office in general and its field volunteers in particular could not effectively attend to FP asmuch as they would want to because of their many other responsibilities. They expressed a needfor the BSPOs to make more referrals of FP users to the health clinics for a physical examination

88
before they are first given contraceptives. They recognized that, through the BSPOs, theprospective FP clients in the community could gain better access to FP information and services.
The FP workers echoed the report from the community folk to the effect that BHWs areindeed assisting the health personnel during clinic days. They also viewed them as promotingDOH health programs, assisting during immunization, conducting child weighing, motivating andfollowing-up FP clients, and refering potential FP users to the health clinic.
On the Attributes of an Effective Volunteer.
The FP workers of both the CHO and the CPO shared the view that, in order forvolunteers to be effective, they must be active, sincere, persistent, approachable, industrious,patient and hardworking. They also emphasized that it is important for volunteers to possess goodcommunication skills so that they can effectively convince clients to accept FP use and properhealth care practices. The RHMs added that an effective volunteer knows how to relate to peoplein the community so that they will be accepted. They expressed that some community folk seennot to trust them and would go directly to the clinic, tation than approaching a BSPO/BHW foradvice or FP supplies. This will sometimes happen even when it means spending more money andtime.
They also agreed that the volunteers should be able to visually detect signs of abnormalitiesamong their clients, so that they can immediately refer them to clinics. They believed, however,that in order for the volunteers to do this, they should have adequate training on this aspect.
The CHO and the CPO workers also shared the opinion that an active BSPO or BHW isone who consistently motivates and follows-up her clients, advises or refers FP clients to the healthclinic and regularly provides FP services. They also expect them to conduct regular house visits.In general, they prefer volunteers who are helpful, cooperative, diligent and dependable.
On Volunteers' Interaction with the FP Workers
Recognizing that the CPO is the lead agency in the implementation of the FP program,most of the CHO FP personnel believed that the CPO staff and volunteers should have greaterparticipation in the implementation of the FP program than the CHO personnel and volunteers.As such, they expect the BSPOs and their supervisors to concentrate their efforts on FP. On theother hand since the CHO still provides the clinic-based FP services, they also expect the BSPOsto closely coordinate with CHO personnel.
The CHO FP workers favorably assessed the performance of the CPO and their volunteers,but admitted that coordination problems, especially concerning referral system, have hampered FPprogram implementation. While the BSPOs and the BHWs are expected to refer clients to clinics, the CHO FP workersreported that only few cases are being referred to the clinics by the volunteers. The clinic personnelthus claimed that the clinics have mainly been attending to walk-in clients.
The CPO staff and BSPOs, however, argue, that many of the cases that they refer to theclinics either go to other government clinics or private FP estabishments in the city. The BSPOsalso declared that some of their referred cients fail to bring their referral slips to the clinic and arethus, considered as walk-ins.

89
On How to Improve Volunteers' FP Performance
The CPO and the CHO FP workers are convinced that the FP performance of thevolunteers can be further improved if they could be given: 1) increased incentives, 2) furthertrainings, 3) close supervision, 4) due recognition, 5) additional benefits, such as insurance. Theyalso advocated for an improvement of relationships between the volunteers themselves (i.e. theBSPOs and the BHWs) as well as with the communities and the volunteers supervisors.
They also echoed the BCs' and BNs' suggestion that volunteers be provided more trainingon communication and motivation skills and FP techniques in order to improve their competenceand efficiency in motivating potential FP acceptors. These trainings, according to them, will makethe volunteers more competent and effective in motivating potential FP acceptors.
Along with the BCs it was asserted that close supervision and monitoring of the volunteers'activities will help them improve their performance. Believing that the incentive "improves thevolunteers' self-esteeem," they suggested that this be increased. Like the BCs, the CPO and theCHO supervisors were convinced that high performing volunteers should be given due recognitionso that they will be encouraged to work harder.
Research Utilization
After the RU Workshop, more consultation meetings and dialogues between theresearchers and city health and population officers were held, during which the CPO's and CHO'sactions on the research results and recommendations were discussed. Both offices recognized thevalue of the research findings on their FP program. The impact of the diagnostic assessment onthe city's FP program implementation is best summarized in the City Population Officer's reportto the Iloilo City Mayor submitted by the City Population Officer City in August 1994 which incapsule described the study's major findings and the actions taken by the CPO and the CHO inresponse to the study results and recommendations. The actions/activities reported were:
1) 169 BSPOs were trained on Community Organization and basic FP;
2) All BSPOs were provided sign boards to facilitate identification.
3)Dialogues and team building sessions and monthly conferences between the CPO andCHO staff and their volunteer workers were conducted to improve coordination and workingrelationship between the two offices and their staff.
4)A referral system jointly prepared by the CHO and the CPO to facilitate provision ofappropriate FP services was put in place.
5) An FP Management and Supervision Course for Population Program Officers and CHOclinic personnel has been proposed for 1995.
Confirming the above report, the City Health Officer also added that a common indicatorof the volunteers' FP performance has already been identified, used, which is the number ofacceptors referred to the clinic relative to target.

90
SECTION V
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
This study was conducted in order to determine and compare the FP activities andperformance of the BSPOs and BHWs in Iloilo City and find out what factors influence theirperformance.
The study sample consisted of 106 BSPOs and 106 BHWs who were selected usingsystematic sampling with a random start. To collect the data needed to answer the studyobjectives, a combination of quantitative and qualitative techniques were used namely: 1) personalinterviews of BSPOs and BHWs; 2) in-depth interviews of CPO, CHO and BHS personnel, BNS,and some BCs; 3) FGDs with BHWs, RHMs and MCRAs; 4) actual observation of BHW andBSPO activities at in health stations and the field; and 5) an examination of CPO and CHO orclinic records/documents including the accomplishment reports of the community volunteers.
Trained interviewers conducted the interviews using structured questionnaires translatedto Ilonggo, the language of the target population. The in-depth interviews and FGDs wereconducted or facilitated by the investigators themselves, while trained nurses did the clinic and fieldobservations.
Summary of Findings
The results of this study may be summarized as follows:
1. The BSPOs and the BHWs of Iloilo City were mostly female (98 percent), in their mid40's, high-school educated, married, and have 4 to 5 children. A little more than half weregainfully employed. In most cases this was part-time work, predominantly engaged in sales/tradingor vending, with a monthly median income P1000. Their median total monthly household incomewas P3000.
2. The BSPOs and the BHWs were selected as based on the recommendation orendorsement of barangay officials and/or respected community leaders. In their selection,preference was given to volunteers who were interested, committed and those who have time todo volunteer work.
3. Only a few of the volunteers (both BSPOs and BHWs) were able to attend a formal FPtraining. Most of the BSPOs, but only 29.2 percent of the BHWs had received informal trainingor orientation on their roles and functions from their immediate supervisors.
4. Although most of the volunteers were reportedly active in their work and involved inFP-related functions, some of them were still not involved in FP motivation, referral, follow-up,counseling and distribution of FP supplies. With their functions focused on MCH care, the BHWs'involvement in FP activities were limited. A majority of this group was involved in motivation(72.64 percent) and counseling (55.66 percent), but fewer than half were doing follow-ups,referrals, and contraceptive resupplies.

91
5. Volunteers engaged in FP activities, were able to serve an average of 11 FP clients perweek in the six months prior to the interview, with the BSPOs having served more than theBHWs.
6. The volunteers, on the whole, spent an average of 3 days a week on volunteer work,with the BSPOs allotting an average of five hours, and the BHWs 3 hours on FP functions. Someof both groups were also involved in community/livelihood projects.
7. The PPOs of the CPO directly supervised the BSPOs, while the PHNs and RHMs ofthe CHO supervised the BHWs. Volunteer-supervisor interactions were limited, about two tothree times a month. Comparatively speaking, the volunteer-supervisor interactions were morefrequent for the BHWs than for the BSPOs. These also lasted longer for the BHWs than for theBSPOs.
8. The volunteer-supervisor interactions for both groups had generally transpired the weekprior to interview and were mostly initiated by the supervisors. They were usually situated at thehealth clinic/station (BHWs) or at the CPO Office (BSPOs).
9. Both the BSPOs and the BHWs favorably appraised their supervisors in terms of:approachability, supportiveness, helpfulness, flexibility, consideration, dedication to andknowledge about their job. They gave them ratings ranging from 4.70 to 4.78 for each qualitybased on a scale of 1 (lowest) to 5 (highest).
10. The Iloilo City government provides a monthly subsidy of P200 for travelling andother expenses to BSPOs and BHWs in every barangay. Those holding dual roles receive P400monthly. The majority of them were discontentment with their allowance and would welcomean increase.
11. The majority of the volunteers were interested and committed to their work as indexedby their long years of continued active service (average of 8 years) and their intention tocontinue working "as long as they are able," "alive" or "needed". Their interest and commitmentmay probably have been sustained because they also liked and were contented with their work.
12. The most common FP supplies distributed by the volunteers to their clients were pillsand condoms which they usually obtained from their respective supervisors, from the healthclinic/stations or the Population Office.
13. Being a recommending person for the volunteers, most of the BCs were acquaintedwith the BSPOs and BHWs in their barangay. Some BSPOs/BHWs, however, were not knownto many MCRAs in the community due to limited volunteer-community interaction. To meettheir health/FP needs, some mothers go directly to the health clinic or opt not to seek any help.
14. BCs, BNs, MCRAs and the other FP workers (PPOs, PHNs, RHMs, and BNSs)acknowledged the important role played by the volunteers in the promotion and implementationof the FP program. They recognized that the volunteers serve as a link between the health andpopulation offices with the community and help to make health/FP services more accessible tothe people, especially to those in remote barangays.
15. The FP performance of the BSPOs was significantly better than that of the BHWs.Those holding dual functions both as BSPOs and BHWs also performed better than those whowere BHWs alone, but not better than those serving as BSPOs alone.

92
16. Although quantitative data failed to support the hypothesis that FP performance isinfluenced by quantity of supervision, there is sufficient qualitative evidence to show thatamount of time spent by the supervisor with the volunteers influences their FP performance. Themajority of the volunteers, their supervisors, as well as the other key informants of this studyattributed the volunteers' difficulty or failure to accomplish their FP functions to lack ofsupervision. They all felt that closer supervision will improve the volunteers' performance.
17. The absence of a relationship between FP performance and volunteers relationshipwith supervisors, may have been due to the very high ratings the volunteers gave to theirsupervisors. The correlation analysis did not yield significant results for this variable, but thequalitative data again revealed that the failure of some volunteers to accomplish theirresponsibilities,has been blamed on the poor relationship existing between volunteers and theirsupervisors.
18. The volunteers' lack of understanding of the CPOs' and the CHOs' respective rolesin the implementation of the FP program has also been perceived to have affected the volunteersFP performance. With the BHWs' work focused on MCH care, their time for FP activities isusually limited. The CHO staff concurred that FP is not a priority of the BHWs. The CHOexpect the CPO personnel and the BSPOs to perform FP functions. This has apparently createdsome friction between some CPO and CHO staff and volunteers, and has affected coordinationand implementation of both the FP program and the volunteers' FP performance.
19. The involvement of men either as FP targets or as volunteer motivators, wasobviously very minimal. The FGDs and in-depth interview participants argued that, since themen play a major role in FP decision-making, they must also be involved in the FP program.They noted that male-oriented FP methods are more difficult to promote than female orientedones.
Conclusions
1. The performance of the volunteer health workers in the delivery of FP services in IloiloCity still leaves much to be desired. Despite the incentives they receive, many are still not doingtheir FP functions as expected.
2. While the delivery of FP services is a major function of the BSPOs, this is only one ofthe many responsibilities of the BHWs. More BSPOs than BHWs handle referrals, follow-up andresupplying current FP users with contraceptives, because the latter have concentrated on MCHcare thereby giving less emphasis to their FP-related functions.
3. Close supervision and monitoring of the health volunteers by their supervisors cancontribute to help improve the FP performance of volunteer workers. This enables thesupervisor to follow-up the progress of the volunteers' work and to assist the volunteers inaddressing whatever problems/difficulty they may encounter. In comparison, present patternsof supervision donot seem to be having much impact onthe performance factor.
4. Although the quantitative analysis did not show a significant correlation between FPperformance and relationship with supervisors, a good standing in this regard was nonethelessunanimously recognized as an important ingredient in improving the delivery of FP services.Both community members and the FP workers agreed that a good relationship between the

93
BHWs and the BSPOs and their respective supervisors is quite important. In a collaborativework, the actors' clear understanding of their roles and responsibilities is a must.
5. The volunteers' incentive was generally perceived as a motivating factor for FPvolunteers to perform well. However, the delay in its release, and the fact that some volunteers(both BSPOs and BHW) receive more than the others had bred some indifference among themand has probably had a detrimental influenced on their performance.
6. The volunteer workers still lack training on FP promotion and service delivery. Manywere performing FP functions which they have not been trained to do. Others would ratherrefuse to perform some of their prescribed functions due to lack of knowledge and skills.
7. Despite the fact that FP practice is a husband-wife function, when conflict indecision-making arises, the husband's decision usually prevails. Nevertheless, Iloilo City's FPprogram, like many others, is still very female-oriented.
Policy Implications and Recommendations
1. The fact that lack of training, communication and motivation skills have all contributedto the poor performance of some volunteers suggests that a training which will improve theimmediate knowledge and skills of the volunteers along these dimensions needs to be conducted.Before this is undertaken, however, a training needs assessment should be made, so as topinpoint the specific weaknesses of the volunteers.
2. The perceived poor relationship between some CPO and CHO personnel as well asbetween their respective volunteers suggests that a reorientaion on the roles and responsibilitiesof all those involved in the FP program should be included in the proposed training. Valuesreorientation also seems to be an obvious training necessity. This should include a reorientationon "voluntarism", "cooperativism," and "smooth interpersonal relations" as well as on othervalues.
3. The CPO field supervisors (PPOs) will not be able to provide their BSPOs withadequate supervision unless their workload becomes manageable. To allow the PPOs more timeto monitor, guide and assist their BSPOs, the number of PPOs must be increased and theircoverage reduced.
4. The conflict and strained relationships existing between some CPO and CHOpersonnel and also between their volunteers has admittedly hampered the implementation of theFP program. This will pose more problems if it is left unresolved. The present initiative to bridgethe gap between these two offices through a coordinative system that defines their respectiveroles and tasks must be pursued and given the chance to work. In the process, the CPO andCHO must continue regular consultation and sharings of experiences.
5. There is also a need to train the volunteers on some simple visual diagnosticprocedures. Although they are expected to refer FP problem cases to a clinic, they should knowhow to detect "warning signs" of FP side effects, or "symptoms" that could probably warranttermination of contraceptive use or immediate referral of a client to a clinic. Many times,symptoms of FP side effects or indications of possible termination of contraceptive use areignored not only by the client but also by the FP worker because they are both unfamiliar withthe "risk signs".

94
6. The lack of consensus among the FP service providers regarding the definition of FPperformance makes it difficult to systematically assess the CPO's and the CHO's as well aspersonnel's or volunteer's accomplishments. This suggests the need to identify and definecommon indicators of FP performance which both offices should use in their performanceevaluation.
7. The fact that husbands often make the final decision in FP practice, makes theirinvolvement in FP programs imperative, both as targets and motivators. The CHO and CPO canstart this by recruiting male BSPOs and BHWs.
8. Since volunteer work needs time, interest and commitment, these should be givenpriority among the criteria to be considered in the recruitment and selection of volunteers. Theirmotivation to be volunteers must also be examined and before they are appointed they must bemade to clearly understand their roles and responsibilities as volunteers, what they are expectedto do, and what they should expect and what not to expect from their involvement in theprogram. Awareness of all these can prevent frustrations and dissatisfaction on the part of thevolunteers, and in effect minimize program implementation problems.