asia pacific journal of health management - achsm · research articles and notes ... hok-cheung ma...
TRANSCRIPT

Asia Pacific Journal of Health ManagementVolume 1 Issue 2 – 2006 The Journal of the Australian College of Health Service Executives
• Reforminghealthsystems
• Regulatingtheprivatesector
• Improvingclientsafetyandsatisfaction
• Integratingservices
• Assessingemployeehealthstatus
...andmore
This issue proudly sponsored by:

EditorialExpectations of a Professional Journal: telling the truth 4 MaryHarris
in this issue 7
SPEcial FEaturE articlE a Model Health System for australia – Part 2: What should a (single) commonwealth funded public health system look like? 8 AndrewPodger
analytical riPoStE response to Podger’s Model Health System for australia (Part 1 and Part 2 articles) 15 JeffreyBraithwaite
rESEarcH articlES and notESregulation in the doldrums: reforming private health care sector legislation in Bangladesh 22 MRedwanurRahmanandSimonBarraclough
changing an incident reporting and Management Paradigm: the nSW Safety improvement Program 29 SarahMichael,MaureenRobinson,PaulDouglasandJeffreyBraithwaite
the impact of a continuous Quality improvement approach on Patient care in the ambulance Environment 39 RussellLinwood
centralised control and devolved responsibilities: personal experiences of senior health executives on the implementation of the area health management model in new South Wales,1990-1999 44 ZhanmingLiang,StephanieShort,PeterHowardandClaireBrown
Health Status of Employees: defining influences on health in the tertiary education industry 51 MaryDitton
ManagEMEnt PracticEintegrating diabetes Services: opportunities to build cultural bridges 61 HadleySlade-Jones,RodPerkinsandJohnWellingham
in ProFilE 67 JimBirch
Q’s and a’sPrinciples that should underpin a health financing system; improvements in quality of health careover the past five years; council of australian governments (coag) health workforce reforms 69 Experiencedhealthmanagersandeducatorsaddressthesequestions
Book rEviEWBeyond Patient Safety: managerial perspectives on error 74 ReviewedbyJeffreyBraithwaite
liBrary BullEtin 76
uPdatE on Journal activitiES 80
guidElinES For contriButorS 81
co n t E n t S
AsiaPacificJournalofHealthManagement2006;1:2 1

2 AsiaPacificJournalofHealthManagement2006;1:2
PuBliSHErAustralianCollegeofHealthServiceExecutives
EditorMary HarrisMPH,PhD,FCHSECHE
Editorial adviSory Boarddavid BriggsBHA,MHM(Hons),FCHSE,CHE,FHKCHSECo-ordinatorHealthManagementandGerontologyPrograms,UniversityofNewEngland,NewSouthWales,Australia
gwenda FreemanBA,GradDipBusMgt,MBA,FCHSE,CHEFundraisingOfficer–NorthWestRegion,AustralianRedCross,Victoria
Mary HarrisMPH,PhD,FCHSECHEEditor,AsiaPacificJournalofHealthManagement
godfrey isouardBScMHAPhDAFCHSECHEAFAIMAssociateProfessor,Head,SchoolofBiomedicalandHealthSciences,UniversityofWesternSydney,NewSouthWales,Australia
Hok-cheung MaMBBS,MHA,DCH,MRCP,FRCP,FRCP,FHKCP,FHKCCM,FHKAM(Med,)FHKAM(ComMed),FRACMA,FCHSE,CHEPresident,HongKongCollegeofHealthServiceExecutivesandChiefExecutive,RuttonjeeandTangShiuKinHospitals,HongKong
Judith MeppemPSM,RN,RM,BHA,COTM,FCN,MACORN,FINE,MNSWMA(Hon),MNUMS(Hon),FCHSE(Hon)FormerNewSouthWalesChiefNursingOfficer;Consultant,Nursing,MidwiferyandHealthCare
rod PerkinsBDS,MHA,PhD,FCHSE,CHESeniorLecturerinHealthManagement,HealthSystemsGroupandAssociate,CentreforHealthServicesResearch&Policy,SchoolofPopulationHealth,TheUniversityofAuckland,NewZealand
Mavis SmithBHA,MHA,FCHSE,CHE,FHKCHSE,FAICDChiefExecutiveOfficer,ACHSE,Director,MavisSmithHealthConsulting,Victoria,Australia
Editorial oFFicEMavis SmithBHA,MHA,FCHSE,CHE,FHKCHSE,FAICDProductionManagerandChiefExecutiveOfficer,ACHSE
rose EllisPhD,BA(Hons)Sub-Editor
australian college of Health Service ExecutivesPOBox341NorthRydeNSW1670AustraliaTelephone:+61298785088;Facsimile:+61298782272;Email:[email protected].
ISSN:1833-3818(Print)
Editorial coMMittEEJim BirchBHA,FCHSE,CHEConsultant,JimBirchManagementConsultancyPtyLtd
Jeffrey BraithwaiteBA,DipLR,MIR(Hons),MBA,PhD,FAIM,FCHSE,CHEAssociateProfessor,Director,CentreforClinicalGovernanceResearchinHealth,FacultyofMedicine,UniversityofNewSouthWales,Australia
robert cusackBHSM,FNIA,AFCHSE,CHEGeneralManager,PrinceofWalesPrivateHospital,NewSouthWales,Australia
Mary HarrisMPH,PhD,FCHSE,CHEEditor,AsiaPacificJournalofHealthManagement
grant lennoxBEc,BHA,AFCHSE,CHEChiefExecutiveOfficer,TasmanianAmbulanceService,DepartmentofHumanServicesandHealth,Tasmania,Australia
Janice lewisBSc,MBus,DBA,FCHSE,CHEProgramCoordinator,HealthPolicyandManagement,SchoolofPublicHealth,CurtinUniversity,WesternAustralia,Australia
nicola northPhD,MA,FCNADirectorofPostGraduateStudies,SchoolofNursing,FacultyofMedicalandHealthSciences,TheUniversityofAuckland,NewZealand
terry o’BryanMAdmin,BBus(Actg),FCHSE,CHE,FCPAChiefExecutiveOfficer,ISISPrimaryCare,Victoria,Australia
John rasaBA,MHP,FCHSE,CHE,FAIM,MAICD,FAHRIAssociateProfessor,Director,AustralianCentreforLeadershipDevelopment,Victoria,Australia
Stephanie ShortDipPhty,BA(Hons),MSc,PhD,FCHSE,CHEProfessor,Dean–TeachingandLearning(HealthGroup),Head,SchoolofPublicHealth,GriffithUniversity,Queensland,Australia
Sally torrRN,CM,BA,MHP,PhD,FCHSECHEPatientCareandServicesManager,GreaterWesternAreaHealthService,Bourke,NewSouthWales,Australia
Peter yuenPhD,BA,MBA,FCHSE(Hon),CHEProfessor,DepartmentofManagementandMarketing,theHongKongPolytechnicUniversity,Kowloon,HongKong
SuBMiSSion oF articlESContributions, including letters to the Editor, should besubmitted to the Editor, ACHSE APJHM journal@achse.org.auandshouldcomplywiththeGuidelinesforContributors.Theseguidelinesappearat theendof the journalandareavailableinelectronicformfromwww.achse.org.auorahardcopycanbeobtainedfromtheNationalOfficebyphoning+61298785088oremailingtheEditorAPJHMatjournal@achse.org.au.
aSia PaciFic Journal oF HEaltH
ManagEMEnt

MiSSion StatEMEntThemissionoftheAsiaPacificJournalofHealthManagementistoadvanceunderstandingofthemanagementofhealthandagedcareserviceorganisationswithintheAsiaPacificregion through the publication of empirical research,theoreticalandconceptualdevelopmentsandanalysisanddiscussionofcurrentmanagementpractices.
TheobjectiveoftheAsiaPacificJournalinHealthManage-ment is to promote the discipline of health managementthroughouttheregionby:• stimulatingdiscussionanddebateamongpracticing managers,researchersandeducators;
• facilitatingtransferofknowledgeamongreadersby wideningtheevidencebaseformanagementpractice;
• contributingtotheprofessionaldevelopmentofhealth andagedcaremanagers;and
• promotingACHSEandthedisciplinetothewider community.
ManagEMEnt PracticE articlESManagement practice papers are practitioner oriented with aviewtoreportinglessonsfromcurrentmanagementpractice.
rESEarcH articlES Anarticlereportingoriginalquantitativeorqualitativeresearchrelevanttotheadvancementofthemanagementofhealthandagedcareserviceorganisations.
rESEarcH notESShorterthanaresearcharticle,aresearchnotemayreporttheoutcomesofapilotstudyorthefirststagesofalargecomplexstudyoraddressatheoreticalormethodologicalissueetc.Inallinstancesit isexpectedtomakeasubstantivecontributiontohealthmanagementknowledge.
rEviEWSA careful analysis of a management or policy issue of currentinterest to managers of health and aged care serviceorganisations.
viEWPointSApractitionerorientedviewpoint/commentaryaboutatopicaland/orcontroversialhealthmanagementissuewithaviewtoencouragingdiscussionanddebateamongreaders.
lEttErS to tHE EditorApositiveorcriticalcommentabouttheJournaloraparticulararticleorperhapssomesuggestionsforfutureJournalthemesorsuggestionsforimprovingreaderinterestintheJournal.
SuBScriPtionSThe cost of subscription to the Journal is included in themembership dues for ACHSE members. For non-ACHSEmembersthesubscriptioncostis$80.
advErtiSingAll booking and enquiries concerning advertising in theJournal should be directed to the Production Manager(EditorialOffice)
coPyrigHt©AustralianCollegeofHealthServiceExecutives2006.
This publication is copyright. Subject to the Copyright Act 1968(Cth),nopartofthisJournalmaybereproducedbyanyprocess, without the written permission of the AustralianCollegeofHealthServiceExecutives.
articlE rEPrintS and PErMiSSionSReprintsareavailableinhardcopyoraselectronicdownloadswithpermissiontoprint.Reprintpricesareasfollows: 1–9copies $6.00each 10–49 $5.50 50–79 $5.00 80–99 $4.50100–499 $4.00(Minimumorder$10.00)
For inForMation or to ordEr:HealthPlanningandManagementLibraryPOBox341NORTHRYDENSW1670Phone:6129805-0125Fax: 61298893099Email: [email protected]
diSclaiMEr AllarticlespublishedinthisJournalincludingeditorialsaretheopinionsandviewsoftheauthorsanddonotnecessarilyreflect those of the Australian College of Health ServiceExecutivesunlessotherwisespecified.
AsiaPacificJournalofHealthManagement
AsiaPacificJournalofHealthManagement2006;1:2 3
Expectations of a Professional Journal: telling the truthM Harris
E d i to r i a l
A professional or ‘scholarly’ journal seeks to provide aspecific constituency of readers with information derivedpredominantly from research and experimentation oncurrentprofessionalandacademicissues.[1]Other‘journals’or periodicals of interest to a professional audience mayinclude the general interest, sometimes glossy, magazine,the‘popular’newsletter,andeventhe‘sensational’,frequentlyopinionated periodical. [1] This editorial explores somecharacteristicsofthescholarlydiscipline-basedjournal.
Since 1665, when the first two professional journals werefounded(ThePhilosophicalTransactionsoftheRoyalSocietyof London and the Journal des Savants) one overarchinggoal has influenced the contents of the now remarkablyproliferatedscholarlyJournal.[2,3]
Thisgoalistotrytotellthetruth.
Researchers, scholars, professionals are all interested tocontributetoaJournalthathasareputationfortruth-tellingandquality.Thereadership–professional,academicandlay–isinterestedtoreadaJournalthattriestosiftgrainfromchaff.
Well known strategies have been adopted by scholarlyand scientific Journals to improve the probability that thepublisherprintsandthereadershipreadstruthfulmaterialonissuesofcurrentimportance.Thesestrategiesincludepeerreview, identifying type of article and limiting publishingto research articles that adhere to the laws of scientificcommunication.[4]
Peer reviewThemostcommonlyusedstrategy is forallmaterial tobepeer-reviewed before acceptance for publication. Two orthree readers, with expertise in the field under scrutiny,read and critique an article that has been submitted forpublication. They may recommend to the editor that thearticleshouldbe1)acceptedforpublicationasis,2)acceptedonlyfollowingcertainchanges,or3)rejected.
Asindicatedbytherecentdisclosureoffraudulentpublishedresearch on stem cells in South Korea, peer-review is nota guarantee against the publication of false or misleadinginformation. [5] However, peer-review is widely regardedas the best available safeguard to publishers, contributorsand readers that each article meets the criteria for qualityestablishedbyexpertknowledgeofthefield.
identification of type of articleA second strategy applied by editorial staff to enhancequalityofarticlesandreducetheprobabilityofmisleadingthereadershipistoacceptanarticleforpublicationunderaclearlyidentifiedclassificationorheading.Headingsmayinclude original research, research notes, review articles,editorial or other comment on current issues, critiques ofpublishedresearchoropinion,letters,etc.[4]Inthiswaytheauthor/scanspecifywhatkindofarticletheybelievetheyare submitting, the editors and reviewers assess whetherthearticleseemstohavebeenappropriatelylabeled.
No reader is likely to consider him/herself misled if acontroversial point of view is presented with threadbarejustification in an article headed‘Opinion.’ In this instance,a reader typically begs-to-differ, and moves on – perhapsunimpressed,butbynomeansaffronted.
adherence with the laws of scientific communicationFinally, scholarly Journals insist that original researcharticles should adhere to the central laws of all scientificcommunication,namely:Quality,Propriety,Accuracy,andReproducibility.[6]
Thefirstthreeofthese lawsrequirethatthestructureandcontentofanarticleshoulddemonstrateobjectivity,utility,integrity and accuracy. In addition, to gain approval forpublicationanarticleshould‘accordwithprofessionalandethicalstandards,aswellasgenerallyacceptedstandardsofgoodtaste’.[6,p.2]
Reproducibility,demandsthatastudybereportedinsuchawaythatitcouldberepeatedbyqualifiedthirdparties.[6]Itfollowsthatthereshouldbe:
4 AsiaPacificJournalofHealthManagement2006;1:2

ExpectationsofaProfessionalJournal:tellingthetruth
• Aclearlystatedresearchquestion,issueorhypothesis.
• Methodsinsufficientdetailtopermitaninterested readerto:
• comprehendwhathasbeendonetogenerateand analysethedatareported;
• replicatethestudyifnecessary;and
• understandstrengthsandweaknessesofthe methodology.• Clearlyreportedresultsshowing‘wartsandall’.
• Acleardiscussiononthecontributionoftheresearch tothebodyofrelevantknowledgeand/orhealth managementpracticeandjustifiableconclusions.
• Fullandaccuratereferencingofallsourcesofinformation.
Naturally,noperfectresearcharticlehaseverbeenwritten.Descriptionsofhowresearchhasbeenconducted,analysisofdataanddiscussionoffindingsareallsubjecttocriticismand debate. This ferment makes the field so vital andinteresting.
As a consequence, this and other Journals maintain highstandardsforacceptanceofarticles,whilerecognisingthatsomeissuesinhealthmanagementareextremelycomplexanddifficulttoresearch.Itispointlesstoexpectthekindofexperimentalcontrol instudiesaboutthemanagementofhealth services that can be achieved by laboratory-basedbio-medicalresearchers.
Quantitative and qualitative methodsAccordingly this Journal acknowledges that current issuesin health service management may be appropriatelystudied by use of qualitative or quantitative methods andthat reports may be accepted for publication that useeither research model, or a mix of both models.What theJournal does expect is that the researcher demonstrates asoundunderstandingoftheirselectedmethodandadoptsarigorousapproachinapplyingandreportingit.
Policy makers and senior managers tend to favourquantitativestudiesbasedon‘probabilitysampling’inwhichthe findings can be readily generalised to the populationunder study. Characteristically, the approach to samplingispredetermineddependingontheresearchquestion,thesizeofthetargetpopulationandthesamplesizerequiredtoachieveastatisticallymeaningfulandunbiasedresult.[7,8]
While quantitative studies have obvious strengths ofgeneralisabilityandtransferability, theyarenotalwaysthebestmethodwhenseekingtogainagreaterunderstanding
ofhowahealthcareorganisationfunctions,orwhythingsarethewaytheyareortheeffectsofagiveninterventiononselectedclientgroups.ManyofourcontributorstothisissueoftheJournalhavechosenaqualitativeresearchapproachtoaddresssuchquestionsas‘Whathavebeentheeffectsofaninterventiontoimprovepatientsafety?’‘Howdidalarge-scalehealthreformaffectseniorhealthexecutivesinvolvedinits implementation?’‘Whatdeficienciescurrentlyexist inlegislationtocontroltheprivatesectorandwhatreformsarenecessary?’‘Whatarethebarriersandpossiblesolutionstoimprovedintegrationofservicesforpeoplewithdiabetes?’
Samplingmethodsusedbyqualitativeresearchersdifferinimportantwaysfromthoseusedbyquantitativeresearchers.Here the aim is to‘purposefully select’ participants from agiven population (ie those most able to provide relevantinformation). Frequently, the approach to sampling is notpredetermined, rather it is allowed to evolve as the needfor,andsourcesof,newinformationemerge,inwhichcasesampleselectionmaycontinueuntilnonewevidencerelatedtotheresearchquestionisapparent;asituationfrequentlyreferred to as ‘theoretical saturation’. [7, p. 334; 8, p. 177]The sample size is typically small in qualitative researchdue to the resource-intense nature of data collection andthe findings may be limited to a single‘case’, such as onecommunity health network of service providers.The mainchallenges then for qualitative research are replicabilityand generalisability. Some studies seek to address theselimitations through the careful maintenance of a researchdiary and the collection of data from multiple sourcesusingavarietyofmethods(eginterview,records,historicaldocuments,ethnography,observation,quantitativesurveys)tosupportandtestparticularemergingtheories;aprocessknownas‘triangulation’.[7,p.275]
AsanewlyestablishedprofessionalJournal,theAsiaPacificJournalofHealthManagementhasdevelopedqualitycontrolprocesses based on the criteria outlined above so that itmay publish articles that meet the scholarly expectationsof itsreadership. Timeandourcorrespondingreaderswilldeterminehowsuccessfulweareinthisendeavour.
Mary g HarrisMPH,PhD,FCHSE,CHEEditor
AsiaPacificJournalofHealthManagement2006;1:2 5

references1. OlinandUrisLibraries.Distinguishingscholarlyjournalsfromother periodicals.Available:http://www.library.cornell.edu/olinuris/ref/ research/skill20.html(Accessed13/09/06).
2. TheRoyalSociety.BriefhistoryoftheSociety;Thegreatestjournals inscience.Available:http://www.royalsoc.ac.uk/page.asp?id=2176 (Accessed19/09/06).
3. TheDibnerLibraryoftheHistoryofScienceandTechnology. TheAmsterdamprintingoftheJournaldesSavants.Available: http://www.sil.si.edu/libraries/Dibner/newacq_2000.htm (Accessed19/09/060).
4. NationalInstitutesofHealth(NIH).Guidelinesfortheconduct ofresearchintheIntramuralResearchProgramsatNIH. Available:http://www.nih.gov/news/irnews/guidelines.htm (Accessed13/09/06).
ExpectationsofaProfessionalJournal:tellingthetruth
6 AsiaPacificJournalofHealthManagement2006;1:2
5. NationalInstitutesofHealth(NIH).Recenteventsconcerningstem cellresearchfraudinSouthKorea.StatementofJFBattey,Chair, NIHStemCellTaskforce.TestimonybeforetheSubcommittee onCriminalJustice,DrugPolicyandHumanResourcesCommittee onGovernmentReform,UnitedStatesHouseofRepresentatives. Washington:NIH;March7,2006.
6. NationalInstitutesofHealth(NIH).NIHPolicyManual.1184 –ScientificandprofessionalinformationpresentedbyNIH employees:review,approval,anddistribution.Available:http:// www1.od.nih.gov/oma/manualchapters/management/1184/ main.html(Accessed13/09/06).
7. BrymanA.Socialresearchmethods.2nded.Oxford:Oxford UniversityPress;2004.
8. MinichielloV,SullivanG,GreenwoodK,AxfordR.Handbookfor researchmethodsinhealthsciences.Sydney:Addison-Wesley;1999.

Ambulance Service as a CQI model. He provides evidencethatsuggeststhatuseofthemodelhashadapositiveeffectonpatientandorganisationaloutcomes.
Usingaqualitativeresearchapproach,Ling,Short,HowardandBrownreporttheexperiencesofseniorhealthexecutivesduringtheimplementationoftheAreaHealthManagementModelinNewSouthWales.Theseresearchersconcludethatwhile senior executives initially held positive views aboutthe potential benefits of the model, only limited gainswere achieved due shortcomings during the early stagesofimplementation(eginadequateresourcestoimplementwide-scale change, job insecurity and instability for thosechargedwithimplementingthechangeandeffortsbythedepartmenttocentralisecontrol).
Thehealthstatusofuniversityemployeesisthefocusofanarticle by Ditton. Based on a survey of University of NewEngland staff, she concludes that the comparatively poormental health status of Australian university employeesposes a public health challenge for those concerned withmaintainingandpromotingthehealthofthisworkforce.
Slade-Jones,PerkinsandWellinghamreportfindingsfromaqualitativestudytoexplorewaysofovercomingbarrierstointegratedcareforpeoplewithdiabetes.Identifiedbarriersincludealackofcollaborativeskillsintheworkforce,alackofresourcesandalackoftimeforstakeholderstointegratecare. Three solutions to overcoming these barriers aredescribed.
InthefirstoftheJournal’sbookreviews,Braithwaiteprovidesaprécisofthebooktitled‘Beyondpatientsafety:managerialperspectivesonerror’.Heconcludesthatthebookisworthbuyingandreadingbecauseitcontainsimportantmessagesforhealthcarepolicymakers,executivesandmanagers.
Nineoriginalarticles, includingacommentaryandabookreview, are presented in this issue of the Journal togetherwithourotherregularfeatures:In-profile(JimBirch),Q’s&A’sandtheACHSELibraryBulletincompiledbySueBrockway.
InPart2ofhisproposedreformagendafortheAustralianhealthsystem,PodgeroutlinesamodelhealthsystemwiththeCommonwealthasthesinglefunder.Hedescribeshowthis system might work at four levels: national, regional,provider and patient. Immediately following this SpecialFeaturearticleisapaperbyBraithwaiteinwhichheanalysesthestrengthsandweaknessesofPodger’sproposedmodel.The purpose of inviting a comment from Braithwaite is tofacilitate discussion and debate among our readers aboutreformofhealthcaresystems.
Regulation of the Bangladesh private health care sector isthefocusofanarticlebyRahmanandBarraclough.Drawingonananalysisofdocumentsanddatafrominterviewswithkey informants, these researchers conclude that furtherreformstothelegislationanditsenforcementarerequiredto address current deficiencies and abuses of the systemandtobetterservetheinterestsofconsumers.
Michael, Robinson, Douglas and Braithwaite report theresults of a formative evaluation of the New South WalesSafety ImprovementProgramduring thefirst twoyearsofits implementation using a range of outcomes measures,including,state-wideeducationalinitiatives,policyreformsandanumberofothermeasures.Theseresearchersconcludethereisearlyevidenceofimprovement.
Continuous quality improvement is the focus of an articleby Linwood. In this Research Note the researcher reportspreliminary findings arising from the use of the AustralianBusiness Excellence Framework by the Queensland
i n t H i S i S S u E
AsiaPacificJournalofHealthManagement2006;1:2 7
Invitation to submit an article or write to the EditorThe Asia Pacific Journal of Health Management invites researchers, policy makers and managers to submit original articles that increase understanding of issues confronting health leaders in countries throughout the region and strategies being used to address these issues. Articles from the private sector will be welcomed along with those addressing public sector issues.
Readers of the Journal are also invited to express their views by writing a letter to the Editor about possible themes for future issues or about articles that have appeared in the Journal.
ACHSE is now calling for papers for the third and fourth issues of the Journal. The deadline for receipt of papers
is 31 October 2006 and 31 January 2007 respectively .

S P E c i a lF E at u r E
a Model Health System for australia – Part 2:What should a (single) commonwealth funded public health system look like?a S Podger
Editor’s note:This Special Feature titled “A Model Health System for Australia – Part 2: What should a (single) Commonwealth funded public health system look like?” is the second in a series of three to be published by the Asia Pacific Journal of Health Management. The author, Andrew Podger, is a former Secretary (Director General) of the Australian Department of Health and Ageing.
We have invited two senior health managers to comment on the reforms proposed by Podger as a way to encourage debate about systemic reform of health care systems. Jeffrey Braithwaite is the first of these managers to provide comment and his comments appear at the end of this Part 2 article. Comments from Robert Stable will appear in Issue 3 of the Journal, together with the article by Podger titled “A Model Health System for Australia – Part 3: How could this systemic change be introduced?”
abstract:This paper is the second in a three-part series about the Australian health system in which I propose Australia moves toward a (single) Commonwealth funded health system. The first of these articles described the main strengths and weaknesses of the current health system and briefly canvassed four systemic change options that could deliver more appropriate care and improve efficiency. The options, all involving a single funder or purchaser, were 1) the states (and territories) to have full responsibility for purchasing all health and aged care services; 2) the Commonwealth to take full financial responsibility for the system, as both funder and purchaser; 3) the Commonwealth and the states to pool their funds, with regional purchasers having responsibility across the full range of health and aged care services; and 4) the Scotton model, or ‘managed competition’ model, with total Commonwealth and state moneys to be available for channelling through private health insurance funds by way of ‘vouchers’ equal to each individual’s risk-rated premium which the individual
andrew PodgerAOAdjunctProfessor,AustralianNationalUniversityandGriffithUniversity;NationalPresident,InstituteofPublicAdministrationAustralia;FormerSecretary,DepartmentofHealthandAgeing;andFormerPublicServiceCommissioner.
Correspondence:[email protected]
may pass to the fund of their choice, the fund then having full responsibility as funder/purchaser of all their health and aged care services. I concluded that the only realistic systemic change option in the medium-term was Option (2), the Commonwealth having full financial responsibility, as both funder and purchaser. In this article I describe this option in detail with reference to how it might work at four levels, viz, national, regional, provider and patient.
Abbreviations:AIHW–AustralianInstituteofHealthandWelfare;CEO–ChiefExecutiveOfficer;DHA–AustralianDepartmentofHealthandAgeing;FSANZ–FoodStandardAustraliaandNewZealand;GP–GeneralPractitioner;MBS–MedicalBenefitsSchedule;NHMRC–NationalHealthandMedicalResearchCouncil;PBS–PharmaceuticalBenefitsSchedule.
Key words:patientorientedcare;allocationalefficiency;incentiveframework;singlefunder;competition;systemicreform.
introductionAsarguedintheprevious(Part1)article,Australia’shealthsystem is performing reasonably well and its futurechallenges relate in large part to its successes particularlyour increasing life expectancy beyond age 50, which isaddingtothenumbersofchronicallyillandfrailaged.Thecontinuing dire circumstances of Indigenous Australiansremainsourworsthealthproblem.
8 AsiaPacificJournalofHealthManagement2006;1:2
AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
Furthersubstantial improvementsrequiremore integratedapproaches to supporting the chronically ill and otherswith complex conditions, and greater cost effectiveness.Suchimprovementsarepotentiallyavailablefromsystemicreforms involving a move to a single funder. This couldenhance patient-oriented care by permitting greaterflexibilityacrosshealthandagedcareprograms, includinga capacity to substitute funds between programs. Greaterflexibilitycouldalsoleadtomoreinvestmentinpreventivecareandotherimprovementsinallocativeefficiency.
Such potential gains are dependent, however, on thedetailed arrangements that underpin the single fundermodelchosen.Inparticular,theyrelyuponallowingflexibilitynearthepatients,atregionalorcommunitylevel,notjustatnationalorstatelevel;andtheyrelyonsomeformofbudgetholdingcontrols.Theyalsorequirefurtherstrengtheningofprimarycarecapacitytosupportcoordinationofcare,andintegratedinformationsystems.
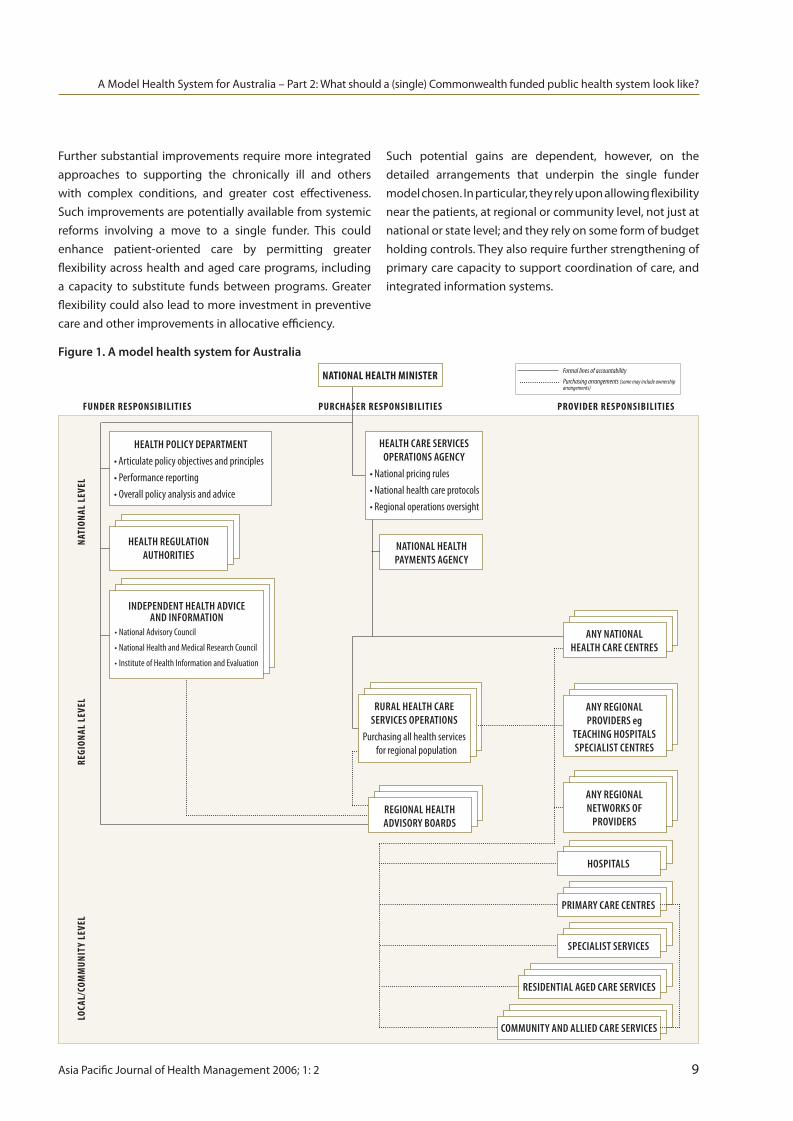
Figure 1. A model health system for Australia
LOCA
L/CO
MM
UNIT
Y LE
VEL
REGI
ONAL
LEV
ELNA
TION
AL L
EVEL
FUNDER RESPONSIBILITIES PURCHASER RESPONSIBILITIES PROVIDER RESPONSIBILITIES
HealtH Policy DePartment•Articulatepolicyobjectivesandprinciples•Performancereporting•Overallpolicyanalysisandadvice
HealtH regulation autHorities
inDePenDent HealtH aDvice anD information
•NationalAdvisoryCouncil
•NationalHealthandMedicalResearchCouncil
•InstituteofHealthInformationandEvaluation
HealtH care services oPerations agency
•Nationalpricingrules•Nationalhealthcareprotocols•Regionaloperationsoversight
rural HealtH care services oPerations
Purchasingallhealthservicesforregionalpopulation
regional HealtH aDvisory boarDs
any national HealtH care centres
any regional networks of
ProviDers
community anD allieD care services
resiDential ageD care services
sPecialist services
Primary care centres
HosPitals
NATIONAL HEALTH MINISTER
national HealtH Payments agency
any regional ProviDers eg
teacHing HosPitalssPecialist centres
Formal lines of accountabilityPurchasing arrangements (some may include ownership arrangements)
AsiaPacificJournalofHealthManagement2006;1:2 9

AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
description of the proposed modelThemodelAustralianhealthsystemthatIpropose,withtheCommonwealthasthesinglegovernmentfunder,wouldbebasedondistinguishingbetweenthefunder,purchasersandproviders.Whilepurchaser/providersplitsarenotuniversallysupported, they have considerable advantage in terms ofclearaccountabilityandthecapacityforcompetitionand/orbenchmarking amongst providers. [1] Disadvantages suchas those experienced by the Australian Capital Territory,whichhasonlyonemajorpublichospital,wouldbeavoidedbyhavinganationalapproach.Theproblemsofpurchaserswithnohealthprofessionalexpertisesettingconstraintsontheprofessionalproviderscouldbesubstantiallymitigatedby ensuring that the expertise of providers guides thepoliciesoffundersandthedecisionsofpurchasers.
Figure1 illustrates themodel Ipropose, with the columnsrepresenting the respective roles of funder, purchaser andprovider; and the sections down the page setting out theresponsibilities at the national, regional and communitylevels.
national arrangementsAtthenational level,theAustralianGovernmentasfunderwould articulate the policy objectives and the generalprinciples, set the conditions within which health careservices would be purchased and provided, and establishthe framework for reporting on performance. The policyobjectives and principles should include the requirementsofequityintermsofgeographicaccess,copayments,safetynets and acceptable queues etc, and the requirements ofvalue-for-money such as cost effectiveness, processes forlistingandpricingdrugsandhealthservices.
Economiesofscalewouldalsosupportanational(orsupra-nationalbyincludingNewZealand)approachtomostareasofhealthregulation,atleastinstandardsifnotinday-to-dayadministration. This includes regulation aimed at patientsafety and consumer protection, including licensing ofproductsandproviders(bothindividualsandorganisationssuch as hospitals and nursing homes), regulation of theprivate health insurance industry and the setting of foodstandards. In most cases where this is not currently anationalresponsibility,therearealreadymechanismsaimedat harmonising arrangements (such as Food StandardAustraliaandNewZealand[FSANZ],reciprocalprofessionalregistrationandconsistenthospitalaccreditation).[2]
National regulation has the advantage of reflecting thenational(orsupra-national)natureofmanyhealthandhealthrelated industries (eg pharmaceuticals, health insurance,hospitalnetworks,residentialagedcare,diagnosticservices,food,andthemobilityofbothprovidersandpatients).
Economiesofscalealsosuggestanationalroleindevelopinggoodpracticeprotocols,particularlyintheareasofchronicdiseasemanagementandpublichealthandensuringcosteffectivenessaswellashealtheffectiveness.[3]
Thenationaladministrativeframeworkneedstobedesignedtomeetanumberofkeyrequirements:
• politicaloversightandaccountability;
• policy-advisingcapacity,well-informedbyhealthand medicalexpertise;
• professionalintegrityinsettingandadministering regulatorystandards;and
• dedicatedeffort,appropriatemanagementandtechnical expertiseforoperations,particularlyforoversightofthe nation-widepurchasingfunction.
In my view, the scale of these responsibilities demandsthat there be a number of separate agencies performingkeyroles. At thesametime, thoseagenciesneedtoworktogether within the policy framework set by the politicalleadership.
There are many options for the national structure, but Iwouldfavoursomethingalongthefollowinglines:• apolicydepartmentresponsibledirectlytotheMinister forHealth,advisingexpertlyonthevarioushealthfunctions (egpublichealth,primaryhealthcare,acutehealthcare, agedcare),onthehealthinfrastructure(eghealthand medicalresearch,goodpracticeprotocols,workforce, information)andonbroadstrategicissues(eghealth financingandeconomics,safetyandquality,general policycoordination);
• asuiteofregulatoryauthorities,withstatutory responsibilities,butguidedbythepolicyframework establishedbytheGovernment;
• anoperationalorexecutiveagency,responsibleforthe purchasingofservicesincludingtheoversightofregional purchasingunits(seefurtherbelow),supportedbya nationalinformationandpaymentsagency;and
• astrongnationaladvisorybody,withlinkstoadvisory bodiesassociatedwitheachofthemajorregulators,and withresourcesforindependentresearchandindependent reporting.
10 AsiaPacificJournalofHealthManagement2006;1:2

This arrangement could draw very heavily on existingorganisations including respectively, the AustralianDepartmentofHealthandAgeing(DHA),existingstatutoryregulators, Medicare Australia, and the National HealthandMedicalResearchCouncil(NHMRC)andtheAustralianInstituteofHealthandWelfare(AIHW).
The framework recently adopted by the GovernmentfollowingtheUhrigReport[4]forimprovingthegovernanceof statutory authorities could be used to ensure there ispolicycoherenceacrosstherangeoforganisations.Iwouldalso strongly support all these agencies being in the oneportfolio,andtoavoidplacingsomeinaseparateindustryorhumanservicesportfoliowhichmaywishtopursueprioritiesotherthanhealth.Someoftheregulatoryfunctionscouldbe performed within the department (DHA), or within theoperational agency; and some of the policy details suchassettingnationalpricesforcertainservicesandproductscould be handled either in the department (DHA) or theoperationalagency.Thechoicesarenotclearcut,butIwouldcautionagainsthavingtoobigapolicydepartment,andnotethat the sensitivities of some regulatory functions mightbestbehandledbyseparateauthorities.UnlikeMrUhrig,[4]Iwouldprefertoseethedepartmentalsecretaryorher/hisnomineeparticipateintheadvisoryboardsforeachoftheotherportfolioagencies,andforthesecretaryandtheChiefExecutiveOfficer(CEO)oftheoperationalagencyeachtobestanding members of the other’s organisation’s executivecommittee: I do not think this would cause insuperableconflictsofinterest.
regional arrangementsThekeytoimprovingallocationalefficiencyistheincentiveframework created by regional purchasers who haveresponsibility for the health objectives for their regionalpopulation, and the flexibility to allocate funds accordingto their most cost-effective use. Their flexibility may beconstrained, nonetheless, by national policy requirementssuch as copayment limits and safety nets, and nationallynegotiatedpricesforparticularservices.Flexibilitymightalsoneedtobeconstrainedifthereisariskofpoormanagement,orofshort-termpressures(egtomeetacutecaredemands)outweighing longer-term, more cost effective priorities(egpreventivehealthinvestments). Anoptiontoconsiderregarding the latter risks is the UK concept of “earnedautonomy”,wheresustainedgoodregionalperformanceisrewardedbyincreasedflexibility.[5]
Regional purchasing arrangements need to meet thefollowingrequirements:
• closeconnectionswithprovidersandcommunity organisationstoensurethepurchasingiswell-informed andresponsivetoregionalrequirements;
• clearaccountabilitybacktothenationaloperational agency,andcompliancewithnationalpolicies;
• apopulationlargeenoughsothattheregionalpurchaser canacceptresponsibilityforthevastmajorityofhealth risks,andthattherearenottoomanypurchasersforthe nationaloperationalagencytooversight;and
• sufficientclouttonegotiatecosteffectivedealswith providersincludinghospitals,nursinghomesand specialists.
There are a number of options for these administrativearrangements,butmyownpreferencewouldbe:
• around20–30regionalpurchasers,withthepossibility ofsub-regionalarrangementstoassistcommunity responsiveness;
• eachregionalpurchasertobeunderthedirectcontrol ofthenationaloperationalauthority;
• eachtohaveastrongadvisoryboardinvolving,in particular,therelevantDivision(s)ofGeneralPractice andsomeotherregionalproviders,andsomecommunity organisations,possiblyincludingpeoplefromlocal government(someindividualnomineesselectedbythe Ministercanalsoensureaconsumervoiceandasensible balancewithoutundulypoliticisingtheboard);
• eachtohavehealthexpertiseaswellasmanagement expertise;and
• theregionalpurchasertohaveresponsibilityforpaying forallservicesprovidedtoresidentsintheregion,wherever thoseservicesareprovided(includingforexample,high levelacuteservicesinanationalcentreoutsidetheregion).
The budget arrangements should involve a “soft-capped”total budget based on the population’s risk profile, withaccesstosomespecificnationalriskpoolswheretheregioncannot be expected to manage the risk on its own.Thesemight cover, for example, the impact of Medical BenefitsSchedule (MBS)orPharmaceuticalBenefitsSchedule (PBS)safety nets, as well as some very high-cost populations orevensomehighcareepisodes.Thesoftcapwouldalsoallowbudget over-runs if necessary, where the consequenceswould be some form of performance review rather thanpenalisingtheregionalpopulation.
AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
AsiaPacificJournalofHealthManagement2006;1:2 11

AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
Theregionalbudgetwouldidentifyestimatesforcomponentparts, but with specified levels of discretion where theregionalpurchasercansubstantiateclaimsofsavingsinonecomponent that might be better employed elsewhere, orcansubstantiateclaimsofthepositiveimpactofaproposedinvestmentonbothhealthandcosts.Thedegreeofdiscretionmightbewidenedinthelightofprovenperformanceovera period of several years. Regional purchasers could beexpectedtodevelopincreasinglysophisticatedapproachesto managing the risks of sub-populations, particularly thevariouscategoriesofchronicallyill,drawingonthenationallydeveloped protocols of best-practice, cost-effective care.SubstantiallyincreasedfundingofIndigenouscommunitiescouldbeexpected,subjecttomonitoringimprovedhealthperformance.
Regional purchasers would be required to publish annualreports on performance including health outcomes,service levels and financing, preferably supplemented bybroaderinformationreportsbythenationalhealthstatisticsorganisationforallregions.
Theseregionalpurchasingarrangementscoulddrawheavilyon current state regional health authorities and state andCommonwealth regional planning arrangements (eg foragedcare).Theycouldalsodrawupon,andintimeinfluence,thestructureandroleofDivisionsofGeneralPractice.
Provider arrangementsWhile, inmost respects,providerarrangementswouldnotbe substantially changed (with most doctors and otherprofessional health providers continuing to operate asindependent private businesses, and hospitals and agedcare providers continuing to operate with a degree ofindependence as private or charitable organisations, or aspublicinstitutionswithsubstantialmanagementautonomy),someimportantchangescouldbeexpectedovertime.
The more integrated and patient-focussed approach willrequirefurtherstrengtheningofprimarycarearrangements,with GP practices becoming increasingly multi-skilled,supported by nursing staff and linked more closely withallied health professionals, as well as specialist medicalpractitioners. GP practices might effectively exerciseincreasing responsibility for the health care budget fortheirpatientswithintheframeworkdevelopedbyregionalpurchasers.Inregionalandremoteareas,andforIndigenouscommunities,primarycareservicesmaybeprovidedinmoreflexible and community-responsive ways, to address theirparticularneedsand/ortheiruniqueproblemsinattractingskilledworkers.
Regional purchasers might also consider contracting withDivisionsofGeneralPracticenotonlytoprovidesupportforGPsandforprimarycareplanning in theregions,butalsotomanagethedeliveryofsomealliedorspecialistserviceswherethelocal(private)supply isnotadequate. Regionalpurchasersmayalsofinditcosteffectivetoestablish(orre-establish or restructure) associated primary care servicessuchasmaternityandchildhealthclinics.
Hospitals providing services to public patients would befunded primarily on a case-mix basis applying nationallydevelopedpriceswitheachregionoperatingariskpoolforhandling“outlier”cases.Foraperiod,therewouldneedtobecapacitytomakethetransitiontothebenchmarkcosts,andaprocessforacceptablevariationsbecauseofgenuinelabourmarketorotherunavoidablecostdifferentials. (Iwillnot go into detail here about funding for teaching andresearch.)
Regionalpurchaserswouldbeexpectedtomovereasonablyquickly to consider options for “contracting out” or for“centres of excellence” for particular procedures andactivities to improve efficiency, and hospitals may chooseto specialise or to network as well as to improve internalefficiencies to achieve benchmark prices. As important, ofcourse,istomanagedemand(quantityofservices)inawaythatoptimisesoveralleffectiveness.ThiswillrequirehospitalstoworkmuchmorecloselywithGPsandothernon-hospitalproviderstoreducetheneedforhospitalcare,andtoexplorewith the regional purchasers where hospital outreachservices are the most cost-effective way of supportingpatients. Isuspectthiswouldleadtoreversingthedeclineinrehabilitationservices,andinvariousoutpatientservicesparticularlyinfieldssuchasdialysisandcancerremediation.
In theory, the ownership of hospitals (or residential agedcarefacilities)isnotacriticalissueunderafirmpurchaser-provider model. But the high capital costs involved inhospitalsinparticular,andtherisksoftechnology-drivencostincreases, suggest the need for a somewhat conservativeapproachtoeitherprivatisation(ortransfertothecharitablesector)ofpublichospitals,ortolettingthemremaininthehands of state governments. There is a risk of the statesnot maintaining capital investment or of not managingassets efficiently or of not integrating them with theCommonwealth’srecurrentexpenditureefforts.
12 AsiaPacificJournalofHealthManagement2006;1:2

AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
AsuitablynegotiatedtransfertotheCommonwealth,drawingon the experience in the other direction of RepatriationHospitals,couldbeafirststeptowardsestablishingregionalnetworks of hospitals responsive in an integrated way tothe requirements of the regional purchasers in terms ofdeliveringthebestcarefortheregionalpopulation.
Intime,furtheradvantageshouldbetakenofthepurchaser/provider structure under which the hospitals would bemanaged with greater independence from the purchaser,thoughpreferablyinapartnershipstyle.Themanagementof public hospitals should involve some direct interactionwith the community, and ensure good community access.It should also have the full confidence of clinical andprofessional staff. It needs to have sufficient critical massto deliver acute care services safely and efficiently; andit needs the flexibility to go with the accountability fordeliveringefficientlyandeffectively.Notwithstandingsomeinconsistency with the Uhrig approach to governance,my own preference would be to establish trusts withinthe framework of the national operations agency, withexecutive boards that include health expertise, businessacumen and some community standing. Alternatively, thehospitals could be separate agencies, each managed by aCEOappointedbythenationaloperatingorganisationandresponsible to it, with a strong advisory board. While intimeconsiderationcouldbegiventoprivatisethehospitals,there are considerable risks involved which might bestbe managed by retaining a mixture of publicly ownedand charitable hospitals, and private hospitals. Privateinstitutions may well contribute to greater efficiency andpatientresponsiveness inanenvironmentwheretherearecompetingproviders in the region,butmaypresent a riskofdepartingfromcharitableandprofessionalvalueswheretheyoperateinamonopolyposition.
Community aged care services would continue tooperate along lines similar to those operating now, butwith increased opportunity for regional purchasers tonegotiate prime contracts with organisations responsiblefornetworksofserviceprovidersdeliveringservicesinlinewithindividuals’careassessmentsandcustomer-responsiveauthorisation.Overtime,therewouldbeopportunitiesforcloserintegrationofcommunityandresidentialagedcare,andforservicesthatallowmore“ageing-in-place”,includingmore choice for the individuals concerned about the typeofaccommodationandtheservicestheyreceive(subjecttoassessmentprocedures).
Patient arrangementsTo take best advantage of this more integrated approach,individualAustralianswillneedtoparticipateinthenationalpatient information record system which, through smart-cardtechnology,wouldallowconsiderablepatientcontrolovertheinformation,whohasaccesstoitandwhocanaddtoitorvaryit.Overtime,suchasystemalsohasthepotentialto enhance patient control over their own care withoutjeopardisingprofessionalinfluenceabouteffectivenessandcost-effectiveness.
I do not believe we need to have patients register with aparticular GP, although they should be encouraged to usea particular GP regularly. The information technology (IT)systemcanalreadymeasurethedegreeof“patientloyalty”sufficientlytoallowdoctorstobepaidona(partial)capitationbasis:forexampleforhavinghighlevelsofimmunisationorcancer screening amongst their patients, or for planningandmanagingthecareofchronicallyillpatients. Sothereisnoneedtoconstrainpatientchoice,andwecancontinuetousechoiceofGPasamarketdisciplinetoaddressqualityand responsiveness (and the level of copayments) in theprimarycaresystem.
As mentioned, there is an important role for copayments,to contain demand, including demand generated bydoctors for referred services such as diagnostic services.Theequityobjectivecanbeaddressedbysetting limits tocopayments including through safety nets. The efficacyof these arrangements could be substantially improvedif government payments for services were more directlysubject to conditions over the copayments allowed,whetherthroughcontractarrangementsorthroughbroadagreements with the professions. Regional purchasersin particular could be given some flexibility to negotiate(or set through open competition) additional paymentsin exchange for specified copayment limits in regions(or localities within regions) where there is evidence ofsupplyproblemsandhenceaccessproblems.AnimportantprecedenthasalreadybeensetforthisinMedicalResonanceImaging(MRI)arrangementsinruralAustralia.
Thegrowingdemandformorechoice,particularlyregardingaged care, will require further consideration of controlmeasures including, as Professor Hogan has suggested,more emphasis on user charges in exchange for reducedemphasisonsupply-sidecontrols.[6]
AsiaPacificJournalofHealthManagement2006;1:2 13

AModelHealthSystemforAustralia–Part2:Whatshoulda(single)Commonwealthfundedpublichealthsystemlooklike?
Isuspecttherewillneedtobeamixofdemandandsupply-sidemeasures,withsomepopulationbenchmarkstoguidethoseassessingpeopleforeligibilityforassistance(asoccursnow) but with increased flexibility to meet individuals’preferencesforresidentialarrangementsandthequantumof services, subject to people paying for above-standardarrangements and services. With means tests governingaccesstogovernmentsubsidiesinthearea,thereisastrongcase for removingallexistingclawbackofadditionaluser-charges. Equity should be addressed by ensuring a goodminimum standard of care, not by penalising those whochoosetopaymoretoreceivemore.
Similar arrangements apply to other parts of the healthsystem,wherethoseadvocatingmorechoiceneedtoacceptthat any consequential escape from supply-side controls(suchasqueuingforelectivesurgery)doesneedtobeoffsetby demand-side controls including private contributionstowardsprivatehealthinsuranceandcopayments.
conclusion to part twoManyaspectsofthemodelIhavedescribedmaybedebatedbypractitionersandpublicadministrationexperts,andIamnotweddedtoeverydetail.Mypurposeistospelloutthekey design principles I believe are required to ensure therealisationofpotentialgainsfromasingle(Commonwealth)funder. Most of the changes do not in fact involve radicaldepartures from existing institutional frameworks and,asdiscussed inPartThree in thenext issueof theJournal,implementationofthemodelisfeasibleoverathreetofiveyearperiod.
acknowledgements This paper was presented as the Inaugural Lecture for thenew Menzies Centre on Health Policy at the AustralianNationalUniversityandSydneyUniversityon3March2006.ItdrawsonworkIhavedoneintheAustralianPublicServiceoverthelasttenyearswiththesupportofmanycolleagues,particularlyintheDepartmentofHealthandtheAustralianInstituteofHealthandWelfare,butalsointheDepartmentsof Prime Minister and Cabinet, Treasury and Finance. TheviewsinthepaperaremineandnotthoseoftheAustralianGovernment,andItakeresponsibilityforthecontent.
references1. Thepotentialbenefitsofpurchaser/providersplits,andofcompetition betweenprovidersunderappropriateregulatoryarrangements, havebeenatthecentreofmanyNewPublicManagementreforms overthelastdecade.Seeforexample,ProductivityCommission. Reviewofnationalcompetitionpolicyreforms.Canberra: CommonwealthofAustralia;2005.OrganisationforEconomic Co-operationandDevelopment(OECD).Towardshigh-performing healthsystems.Paris:OECD;2004.Thispublicationincludesa discussionofpurchasingapproachesindifferentcountriestoprovide incentivestoimproveefficiencyandeffectiveness.
2. ThelatestdevelopmentistheCouncilofAustralianGovernments’ (COAG)agreementtodevelopbyJuly2008anationalregistration systemforhealthprofessionalsstartingwiththenineprofessions currentlyregisteredinalljurisdictions(COAGCommunique,14July 2006).Available:http://www.coag.gov.au/meetings/140706/index. htm(Accessed19/07/06).
3. Someadvanceshavealreadybeenmadeinthisdirectionforexample throughtheNationalInstituteforClinicalStudies.TheNational HealthandMedicalResearchCouncil(NHMRC)hasalsobeenused forthispurposefromtimetotime,andtheNationalSafetyand QualityCommission.Furthereffortisneededhowever,particularly toaddresscosteffectivenessaswellashealtheffectiveness.
4. UhrigJ.Reviewofthecorporategovernanceofstatutoryauthorities andofficeholders.Canberra:AustralianDepartmentof Communications,InformationTechnologyandtheArts;2006. Available:http://wwwgov.au/cca(Accessed27/06/06).
5. SmeeC.Speakingtruthtopower:twodecadesofanalysisinthe DepartmentofHealth.OxfordUK:NuffieldTrust,Radcliffe Publishing;2005.
6. HoganWP.Reviewofpricingarrangementsinresidentialagedcare. Canberra:DepartmentofHealthandAgeing;2004.
14 AsiaPacificJournalofHealthManagement2006;1:2

a n a ly t i c a lr i P o S t E
AsiaPacificJournalofHealthManagement2006;1:2 15
response to Podger’s Model Health System for australia (Part 1 and Part 2) J Braithwaite
abstract:In this response to Podger’s proposed model health system for Australia, I take the role of analyst of his two special feature articles on ‘A model health system for Australia’, the second part of which is in this issue of Asia Pacific Journal of Health Management. My intention is not to be indifferent, but rather to meet Podger’s model head-on, and debate, albeit briefly, its merits, strengths and weaknesses – and the possibilities for success. Although my training is in psychology and management, and my professional field is organisational behaviour, I have borrowed a scalpel from a surgical colleague with which I shall try to expose Podger’s arguments, test them against their own logic and explore their feasibility.
Key words:healthpolicy,systemsreform,newmodels,logicofreform,evidence-basedpolicy
Jeffrey BraithwaitePhDDirector,CentreforClinicalGovernanceResearch,FacultyofMedicine,UniversityofNewSouthWalesAssociateProfessor,SchoolofPublicHealthandCommunityMedicine,FacultyofMedicine,UniversityofNewSouthWales
introductionThere isamajorpreoccupationamongstsomesectionsofthemediaandselectedstakeholders inthehealthsystem.I like tocall it the‘let’shaveanotherattemptat reformingthehealthsystem’game.Ithassoakedupmuchprinters’ink,andtheeffortexpendedcanbeseendiffusedthroughoutacademicandindustryjournals,majorjudicial,quasi-judicialand government inquiries and many professionally-basedor industry association-sponsored conferences.This paperresponds to Andrew Podger’s model for health reform oftheAustralianhealthsystem,thelatestinalineofproposalsgoingbackseveraldecades.
What do reformers want and what do they get?Forthemostpart,thereformers-as-game-playerswantquiteameasureofchange.Recall,eveninrelativelyrecenttimes,for example, the National Health Strategy (1990-1991);[1] the Senate Community Affairs References Committee(1999-2000); [2-4] the Productivity Commission (2004-2005); [5]andthecurrentworkofcoalitionsofbodiesandinterested individuals such as the Australian Health CareReformAlliance[6]formedbyProfessorJohnDwyerandtheHospitalReformGroup[7]ledbyProfessorKerryGoulston,tomentionsomeofmany.Reformersoftenwantonelevelor another of the health system (the Commonwealth, theStates or 20-30 health regions) to have core responsibilityforrunningmostofthehealthsystem,withtheotherlevelshavingnomajorroleorresidualfunctions.
Most proponents of change realise that regardless oftheir preferred model, the health system evolves overtime anyway, because new managerial, organisational,policy, technological, legal and clinical innovations occurboth here and internationally, and these act iteratively toinfluence institutions, services and practices. So invariablyreformersareseekingsomesortofbigbangevent,orlevelsof considered change from the status quo. Largely, theirstatedintentionsaretosecuregreatersystemefficiencyandincreasedprovidereffectivenessorimprovedpatientqualityandsafety.
Astheyplaythegame,reformerstendtothinkofthemselvesastheonesdoingtheanalysing.Essentially,withoutundulysimplifying their task, they areengaged in three activities:assessingthecurrentstateofthehealthsystem,evaluatingitsstrengthsandweaknessesandsuggestingimprovements.Others are the observers of the game or the consumersof its outputs (eg, all the academic articles and books,governmentreportsandpaperspresentedtoconferences).Theyarerelativelyinactive,andgenerallyletthenewideaspassby.Thiscouldbeasignofindifference,ortheythinkitistoohard,ortheymaybeotherwisepreoccupied,andtoobusytoworrymuchaboutreform.

Yetothersareopposedtochange,andthisoftenmanifestssuspiciouslylikevestedinterests,withthoseopposingastheoneswhostandtobenefitfromthepresentarrangementsvis à vis the proposals.There are many reasons why majorreformisstifled,includingthatitwouldtakeagreatdealinafederatednationtosecuresufficientagreementacrossninejurisdictionsandnumerousstakeholderinstitutionstomoveforward,thelackofachampionorchampionswithsufficientreforming zeal and influence, political unwillingness,conservatismandentrenchedideas.
Big bang, and lots of courageDespiteknowingallofthis,AndrewPodgerhasthrownhishatinthering,andoutlinedasetofproposalsforareformedhealthsystem.This takescourage,and Idonotmeanthatin the sense that Sir Humphrey Appleby used when hecautioned Minister and then Prime Minister Jim Hackeragainst change in the renowned BBC series Yes Ministerand Yes Prime Minister. [8,9]We need valour in these daysofnervouspublicservantsandconcernedindustrygroups.PerhapsPodgercannowmakehiscasefortheveryreasonthat he is no longer in such a prominent public sectorleadershiprole.
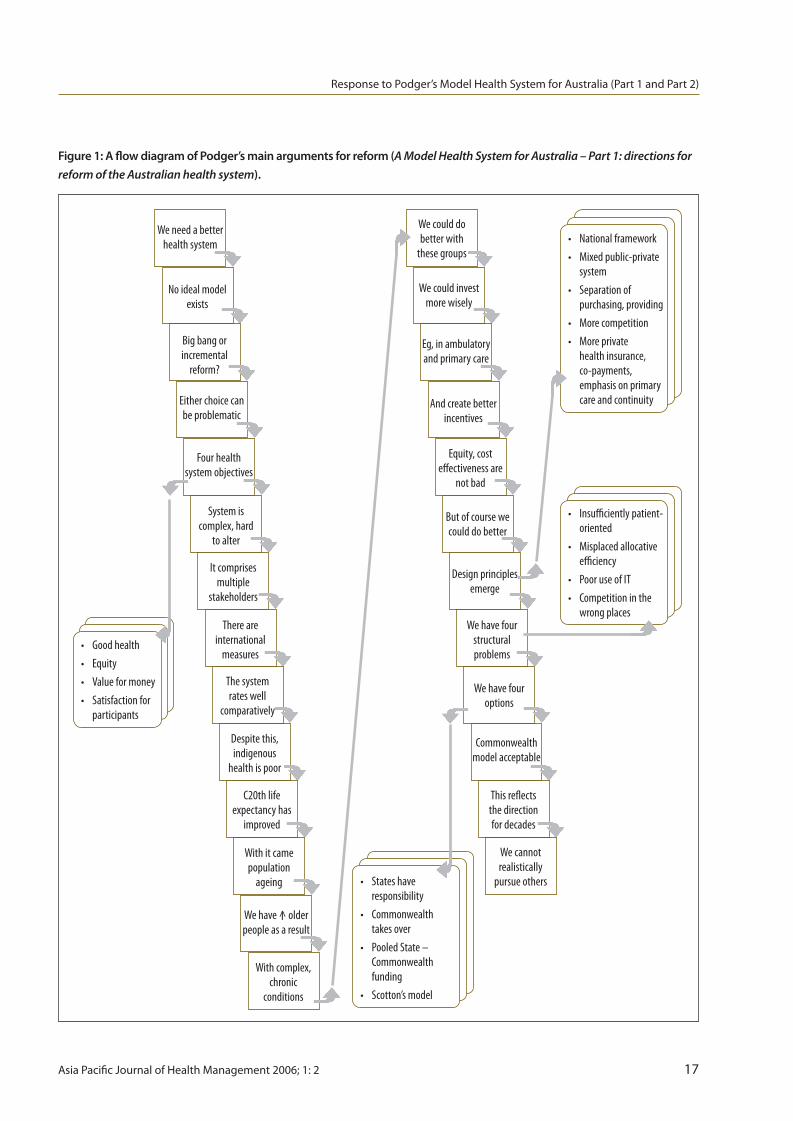
the Podger modelFigures1and2presentasummarisedversionofthemainfeaturesofthePodgermodel,whichIhavereducedtotheirmainpointsinflowchartformat.ThislaysbarewhatPodgerisproposingandthereasoningandlogicunderpinninghismodel.
There are four points to be made. Each is dealt with inturn.Theyare:theflowofandpersuasivenessofthelogic;the evidence bases for the proposals; the health systemsreformversushealthoutcomesimprovementdilemma;andstructuralversusculturalchangeasapreferredmethodofchange.
1. Flow of and persuasiveness of the logicAt first glance, Podger’s arguments look both sustainableand plausible. His ratiocination in his Part 1 article can beapproximated as follows: we need an improved healthsystem>wehavechoices>thesystemiscomplex,politicalandmulti-faceted>wecouldperformbetteralthoughweperformreasonablyinternationally>betterperformanceisneededespeciallyinindigenoushealthcare>lifeexpectancyisimproving>butthisleadstomorecomplexandchroniccareneeds>wehavestructuralproblems>weneedcertaindesignfeaturestocorrectthese>therearethefouroptions>therealisticoneisOption(b).
TheflowcontinuesinhisPart2article. Itslogicalstructureisasfollows:weneedmoreintegration,costeffectiveness,flexibility,investmentandefficiency>asinglefundermodelisneededtoachievethese>otherstructuralissuesincludeprimarycareandIT>thepreferredmodelincludesrolesoffunder, purchaser and provider > other things are neededincluding smart cards > benefits include patient-led services>themodelalsoneedsco-payments,safetynetsandmorechoiceforpatients.
There are logical weaknesses that the model needs toaddress if it is to rest on a valid platform, be fully fleshedoutandconsideredviable.Forexample,it isnotclearhowthe system design principles emerge. They appear in thePart1paperimmediatelyafterasummaryofthestructuralproblems Podger perceives in the system, but no logicalorevidentiarybasesareprovidedforhavingfeaturessuchas a national system, a mixed public-private system, co-paymentsandasinglefunder.Theseideasdonotflowfromthepreviousarguments.NoteIamnotnecessarilyarguingagainst these features. I am simply pointing out that thefoundations
onwhichtheseprinciplesrestareflimsyinlogicalterms.Tosharpentheargument,Podgerwouldneedtoshowhowallthesedesignfeaturesemergefromthepriorpointshehasmade.
There are other strengthening exercises needed in thereasoning to show how Option (b) is the only realisticalternative.These include the ways in which flexibility willbepromotedandpatientchoiceincreasedbywhatappearstobeafurthercentralisingoftheAustralianhealthsystemand itspolicy, fundingandpurchasingdecisionprocesses.This may be possible to achieve, but the arguments as tohowthiswillbeaccomplishedseemincomplete,andarenotwhollyconvincing.
Moretellingly,Podger’sfocusisreallyonthehealthsystem,nottheclient.This isaddressedbelow. Forthemoment, Iwould argue that we ought to take every opportunity tomakethepatientthestartingpoint.Toofewhealthsystemreformproponentsdothis.
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
16 AsiaPacificJournalofHealthManagement2006;1:2
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
AsiaPacificJournalofHealthManagement2006;1:2 17
Figure 1: A flow diagram of Podger’s main arguments for reform (A Model Health System for Australia – Part 1: directions for reform of the Australian health system).
Weneedabetterhealthsystem
Noidealmodelexists
Bigbangorincremental
reform?
Eitherchoicecanbeproblematic
Fourhealthsystemobjectives
Systemiscomplex,hard
toalter
Itcomprisesmultiple
stakeholders
Thereareinternational
measures
Thesystemrateswell
comparatively
Despitethis,indigenous
healthispoor
C20thlifeexpectancyhas
improved
Withitcamepopulation
ageing
Wehave^olderpeopleasaresult
Withcomplex,chronic
conditions
Wecoulddobetterwith
thesegroups
Wecouldinvestmorewisely
Eg,inambulatoryandprimarycare
Andcreatebetterincentives
Equity,costeffectivenessare
notbad
Butofcoursewecoulddobetter
Designprinciplesemerge
Wehavefourstructuralproblems
Wehavefouroptions
Thisreflectsthedirectionfordecades
Wecannotrealistically
pursueothers
Commonwealthmodelacceptable
• Nationalframework • Mixedpublic-private system • Separationof purchasing,providing • Morecompetition • Moreprivate healthinsurance, co-payments, emphasisonprimary careandcontinuity
• Insufficientlypatient- oriented • Misplacedallocative efficiency • PooruseofIT • Competitioninthe wrongplaces
• Goodhealth • Equity • Valueformoney • Satisfactionfor participants
• Stateshave responsibility • Commonwealth takesover • PooledState– Commonwealth funding • Scotton’smodel
I

2. Evidence bases for the proposalWhat do we know about the Australian health system incomparative terms? The information Podger has givenus is restricted to changes in mortality rates in the 20thcenturyandcomparativeOECDhealthexpendituredataasaproportionofGDP.Otherevidenceshowsthat,dependingonthemeasure,AustraliaperformsbetterorworsethanitsOECD counterpart health systems, that all health systemsincluding Australia’s change across time and there is nostructurallyidealmodel.Iwilldealwiththemortalitydatabelow, but obviously expenditure as a proportion of GDPmerely tells us about one particular input into the healthsystem,andsayslittleornothingaboutcomparativehealthsystem performance. Such data are even less useful inunderpinningacaseforreform.
One pointer to satisfaction levels with health systems hasbeen provided by HSCNews International’s survey of 406globalhealthcampaignersdrawnfrom38countriesin2005.[10] On an index of user-friendliness, the performance ofhealthsystemsasagroupwasratedlow;westernEuropeanhealthsystemswereratedbest,followedbyEasternEurope,AustralasiaandthePacificRim,andlastofallwerethehealthsystemsofnorthernandcentralAmerica.Thisindicatesthereis a middle-range case for reform of the Australian healthsystem,butitisnottheworstperformingonuser-friendlinesswhencomparedagainstinternationalbenchmarks.
The best source of data for our present purposes comesfromtheCommonwealthFund.[11] Ineverysurveyithasconducted in five OECD countries (Australia, Canada, NewZealand,UnitedKingdomandtheUnitedStatesofAmerica,with Germany joining the study group more recently) theCommonwealthFundfoundroomforimprovementineachhealthsystem.TheFundhasalsoconsistentlyreportedthatdifferent health systems have comparatively differentialperformance levels, with no one consistently superior orinferiorperformeroverall,withtheexceptionofthehealthsystemoftheUnitedStates,whichismorefragmentedandpoorlycoordinatedonmanymeasurescomparedwithothermembersofthereferencegroup.
Respondents to the Commonwealth Fund’s most recentsurvey[12]wereidentifiedassickerpatients(ie,thosewhohad poorer health, or serious illness, injury or disability)who, as a consequence, had considerable expertise withtheir health system (eg, through intensive medical care orhospitalisation)comparedwiththegeneralpopulation.TheAustralian sample (n=702) reported acquiring infectionswhile inhospital (7%),communicationfailures(22%),poordischargecoordination(36%)anddetectinganerrorintheir
Needamoreintegratedsystem
Needgreatercosteffectiveness
Needmoreflexibility
Flexibilityleadstomore
investment
Needasinglefundermodelto
createthis
Alsoneedstrengthenedprimarycare
AndinvestmentinIT
Roledefinitionsneeded
Patientswillbeingreatercontrol
Egoftheirowninformation
Perhapsviasmartcards
Objective:consumer-led
system
Morechoiceforpatients
Alsoneeded:safetynets,
co-payments
roles • funder: Australian Governmentvia Commonwealth Department • Purchaser 1: Ministerand supporting agencies • Purchaser 2: 20-30regional bodies • Providers: servicesegGPs, agedcareservices, community services, hospitals(much thesameas now,butmore integrated, responsiveand patient-focused)
Figure 2: A flow diagram of Podger’s main arguments for a Commonwealth funded system (A Model Health System for Australia – Part 2: What should a (single) Commonwealth funded public health system look like?).
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
18 AsiaPacificJournalofHealthManagement2006;1:2

care(19%).Havingsaidthat,nohealthsysteminthesurveywas always best or worst on the survey questions, acrossitems such as care coordination, patient safety, patient-centredcareandaccesstocare.
These data suggest, in line with other data from theCommonwealth Fund and elsewhere, that there is noideal model or superior performer across six structurallyvery different health systems. We would thus need to beconvinced of the benefits to be gained from Podger’sproposalstomovefromthecurrentstructuralarrangementstohispreferredmodel,or indeed,anyother.By institutingPodger’s proposals, even slowly over time, we would beputtingthepresenthealthsystemthroughmajordisruptionwithnoguaranteeofimprovements.Thisisnotanargumentformaintainingthestatusquo,astheCommonwealthFunddataalsosuggeststronglythatimprovementsareneededintheAustraliananditscounterparthealthsystems,butapleafor an evidence-based approach and clear understandingofthebenefitssought.Weneedtoseeaconvincingsetofargumentsforhowthenewmodelwillcreateimprovements.At thisstage in itsdevelopment,Podger’smodeldoesnotprovidethis.
3. the health systems reform versus health outcomes improvement dilemmaThisleadstotheproblemofhealthsystemstructuralreformand its relationship to thehealthof thepopulation. Doesthehealthsystemandthewayitisstructuredaffecthealthstatus? Will the model described by Podger contributeto reduced mortality, as he implies? How? In answeringPodger’smodel,Iwanttoposethepublichealthargument.What needs to be done to keep the population healthy?Every public health practitioner knows the answer to thisquestion,butsomeintheacutesector,andalargenumberofstructuralreformers,oftendonotappeartohavethoughttheanswerthrough.People’shealthinessisenabledthroughtheir access to meaningful, interesting work, reasonableincomes, education, encouragement to exercise and eatwell, intellectual stimulation, work-life balance, adequateleisuretime,cleanwaterandadecentroofovertheirheads.Reducingotherriskfactorsisalsouseful–suchasbylimitingexposure to harmful environmental factors. A populationwilldowellifsomespecificharmsarelimitedsuchasactiveand passive cigarette smoke, illicit drug-taking, excessiveuse of alcohol, and unsafe sex. Other contributors to aproductive and healthy society include an effective publictransportsystem,fruitfulrelationshipswithfamilies,friendsand workmates and a safe society, free from war and toomuchcrime.[13-16]
ThesystemPodgerseekstoreformislargelyanillnessratherthan a health system, and to a considerable extent thesedriversofpopulationhealthinessareproducedordeterminedbyothersectorsoftheeconomyoutsideofthe9.7%ofGDPthat the‘Australian health system’ consumes. Further, it isthe case that public health measures, defined broadly, aremuchmoreimportantcontributorstodeliveringimprovedmortalitythanhealthsystemservices.Inordertoachievehishealthsystemobjectives,particularlytheobjectiveof‘goodhealth’,Podgerwill thereforehavetoshowhowhismodelembracesotherindustriesandinstitutionstocreateaninter-sectoraleffort.Although it isnotobvious tosomepeople,evensomehealthprofessionals,healthisnotadeterminantsolely or even mainly of the‘health system’, but is createdby complex, multi-dimensional contributing factors whichshapeindividualandsocietalbehaviours.
4. Structural versus cultural changeThisbringsmetomyfinalpoint.Mosthealthsystemreform-ersadoptastructuralframeofreference,butonecontributionorganisational behaviour specialists have made in recentyearsistoshowthatthereareothercrucialfactorsinsystemschange. [17-19] Structural health reformers see the worldaccording to hierarchies, defined roles, responsibilities,accountabilities and fiscal performance, and in terms ofmodels, principles and frameworks.They are often heavilyinfluencedbyahomoeconomicusparadigm[20]which isindecline insomecircles. Thusthepictureof therationalperson, slavishly maximising his or her economic positionin a highly structured system, fails to account adequatelyforaltruism,valuesandthecomplexityofalternative,non-economic pursuits. This is where sociology, anthropologyandpsychologymeeteconomics.
Theboxes-on-the-chartstructuralperspectiveissocommonthat most people who hold to it do not realise there areotheralternatives. [21,22] Insociological terms, theyhavecometoseetheirviewasnormative,andtakeitforgrantedthattheirpositionisthewayeveryoneseestheworld.Thistypeofperspectiveisinrealityhighlymyopic,especiallyifitpresumesyouareatthetopofthehierarchyandyousurveytheworldfromthat lookouttower. Indeed,whenyouliveinCanberra(orWashington,orLondon)theworldprobablystartstolooklikeitdoestoRussellCroweinthemovieMaster and commander: the far side of the world.[23]Everyonebelowhas a clear job: to carry out their prescribed role, dutifullyand diligently. Design a health system from this vantagepoint,andyourstartingpositionwillalmostcertainlybetheCommonwealthDepartmentandtheMinisterandyouwill
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
AsiaPacificJournalofHealthManagement2006;1:2 19

likelyputboxesaroundthetitlesof importantpeopleandagenciesbeforeyoustipulatewhateveryoneelseshoulddoinexchangeforthemoneyyoupaythem.
Organisational behaviour over two decades has pains-takingly pointed out that the structural view of humansystemsis,inreality,amechanisticperspective.Byholdingto it, analysts of systems downplay or even precludeassessmentofcultural,politicalandbehaviouralaspectsofsystemschange.[24-27]
Usingthepoliticalframeasastartingpoint,forexample,wewouldbegintoevaluatethewaypowerandinfluenceshapethedeliveryofhealthcareandassesstheovertandcovertagendas of various stakeholder groups. We might thendevelop reform strategies to tackle these arrangements,perhaps thereby improving democratic approaches to theway patients are treated and power is displayed, enactedandusedinthehealthsystem.
In taking a cultural frame of reference we might begin toassess above-the-surface behaviours and practices whichmanifest as cultural ways of performing, and also analysesub-cultures across the health system. We would lookbelow the surface at underlying values, beliefs, attitudesand philosophies, for example exhibited in club culturesamongtheprofessions,inordertoassesshowthesemaybechanged.Wemightencouragemoreproductivebehavioursand values in providing care. The end goal following thissortofanalysismightbetoemphasiseteam-based,bottomup approaches to reform, thereby appealing to cliniciansor strengthening their skills in improving the millions ofservicenetworksthatdelivercaretopatients,asopposedto(orperhapsasacomplementto)arguingthefinepointsofwhethertheMinistershouldbethepurchaserorthefunderofhealthservices.
Inshort,Podger’smodelprivilegesstructureovercultureandpoliticsand,intheprocess,seemstounder-emphasisethetractionneededforthoroughgoingreform.Thatcomesfromtheonlypeoplewhocanmakereformwork–cliniciansandmanagersinproviderorganisations,configuredinnetworks.My own position, considered elsewhere, [28] is that wemuststartmoreprofoundlyfromtheneedsofpatientsandcliniciansratherthanwithtop-downstructure,andgroundhealth systems reforms in these types of fundamental,axiomaticprinciples.
According to organisational behaviour theory, then, thestructural view tends to gloss over the surface. Politicalandculturalanalysesoftentellyoumuchmoreaboutwhatneedstobedoneandbringtoattentioninbrutallyhonest
ways the likelihood of proposed reform measures beingsuccessful. The relevance for Podger’s proposals is that acomprehensive version of them would bring political andculturalfactorsmoreexplicitlyandfullyintohismodel.
discussionThis brief response to Podger could be seen as a critiquefromthestandpointofsomeonewho issubtlyorperhapsassertively angling for the status quo. This would notbe a true reading of my contribution. Podger’s model isimportant because it renders visible, from the position ofsomeonewhohasbeenengagedwithitatseniorlevels,andthoughtagreatdealabouttheAustralianhealthsystem,aconsidered view of its reform. There are opportunities tostrengthenthemodel’slogicalunderpinnings,itsevidencebaseandtheargumentsforitscontribution,someofwhichhavebeenraisedhere.Promotinghealthsystemreformintheabsenceofanintersectoralanalysis,andfailingtoshowhow the new model will contribute to improved healthstatusandhealthoutcomes,weakensthemodel’sviabilityandacceptability.Inshort,IarguethatthePodgercasecanbe fortified,andhaveprovidedsomepointers tohowthismaybeaccomplished.
Astructuralapproachtoreformneedstobecomplementedby adequate assessment of other system variables. Thepoliticsof themodel,andculturalandsub-cultural reformgoals, need to be assessed and understood. If Podger canincorporate such features, perhaps he might be able todevise a model that satisfies the realpolitik of oppositionor inertia, and design an implementation plan that works.If he can achieve that, he will be in a stronger position tosecuresupportforhismodel,andwill increase itschancesof success.Thus it seems that Podger’s pressing task is toconsiderwhetherandhowhismodelcanovercomesomeoftheshortfallslaidbarehere.Histhirdpaperinthisseries,ontheimplementationofhismodel,scheduledforthenextissueofAPJHM,mightprofitablyincorporatesomeofthese.
For all this, Podger’s model will still induce a level ofdiscomfortinsomecritics,andevenhostilityinothers.Themodelnotonlyprivilegesstructureovercultureandpolitics,but it also privileges certain kinds of structural change–hightomiddlelevelchange,rotatingthepowerwithinthesame old group of elites. A core question of difficulty andimportance–whatwill leadtoprofoundimprovements inthehealthofthepopulation,andfundamentallyempowerpatients – is left alone. A challenge of the radical, forexample, is never tackled: should we give resources notto providers, but to the most needy groups so they canpurchaseservicesandtherebyshapepriorities? It is surely
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
20 AsiaPacificJournalofHealthManagement2006;1:2

timeformoreblueskythinkingofthiskind.Wemightthenpromotethoroughgoing,responsive,patient-ledreform.
acknowledgementsMy appreciation goes to my colleagues Mary Westbrook,Rick Iedema and Jo Travaglia at the Centre for ClinicalGovernanceResearchatUniversityofNewSouthWalesforhelpfulcommentsonanearlierdraftof thispaper.ThanksalsotoJohannaWestbrookatUniversityofSydneyandMaryHarris,APJHM’sEditor,fortheirinsights.
competing interestsTheauthordeclaresthathehasnocompetinginterest.
references1. NationalHealthStrategy.TheAustralianhealthjigsaw:integration ofhealthcaredelivery.NationalHealthStrategyIssuesPaperNo.1. Canberra:DepartmentofHealthandAgedCare;1991.
2. SenateCommunityAffairsReferencesCommittee.Firstreport: publichospitalfundingandoptionsforreform.Canberra: CommonwealthofAustralia;2000.
3. SenateCommunityAffairsReferencesCommittee.Healingour hospitals:areportintopublichospitalfunding.Canberra: CommonwealthofAustralia;2000.
4. BraithwaiteJ,HindleD.Acutehealthsectorreform:ananalysis oftheAustralianSenate’sproposals.AustHealthRev.2001; 24(1):3-9.
5. ProductivityCommission.Australia’shealthworkforce:Research report.Canberra:CommonwealthofAustralia;2005.
6. AustralianHealthCareReformAlliance.http://www.healthreform. org.au/.Canberra:AustralianHealthCareReformAlliance,2006; (accessed:20/9/2006).
7. HospitalReformGroup.http://www.hospitalreformgroup.org/. Sydney:HospitalReformGroup,2006;(accessed20/9/2006).
8. LynnJ,JayA.ThecompleteYesMinister.London:BBCBooks;1989.
9. LynnJ,JayA.ThecompleteYesPrimeMinister.London:BBCBooks; 1989.
10. PatientView.Theviewsofhealthandsocialcampaignersworldwide. HealthandSocialCampaignersNewsInternational2005;20/21 (DoubleSummerIssue):5-28.
11. TheCommonwealthFund.http://www.cmwf.org/.NewYork: TheCommonwealthFund,2006;(accessed20/9/2006).
12. SchoenC,OsbornR,HuynhP,DotyM,ZapertK,PeughJ,etal. Takingthepulseofhealthcaresystems:experiencesofpatients withhealthproblemsinsixcountries.HealthAff.2005;24: w509-w525.
13. BeagleholeR,BonitaR.Publichealthatthecrossroads: achievementsandprospects.2nded.Cambridge:Cambridge UniversityPress;2004.
14. EvansR,BarerM,MarmorT.Whyaresomepeoplehealthyand othersnot?Thedeterminantsofhealthofpopulations.NewYork: AldinedeGruyter;1994.
15. MarmotM.Socialdeterminantsofhealth:fromobservationtopolicy. MedJofAust.2000;172(8):379-382.
16. InstituteofMedicine.Healthandbehavior:theinterplayofbiological, behavioral,andsocietalinfluences.WashingtonDC:National AcademyPress;2001.
17. BraithwaiteJ.Investinpeople,notrestructuring.BrMedJ.2005; 331:1272.
18. BraithwaiteJ,WestbrookJ,IedemaR.Restructuringasgratification. JRSocMed.2005;98(12):542-544.
19. BraithwaiteJ,WestbrookM,HindleD,IedemaR,BlackD.Does restructuringhospitalsresultingreaterefficiency?Anempiricaltest usingdiachronicdata.HealthServManageRes.2006;19(1):1-12.
20. HenrichJ,BoydR,BowlesS,CamererC,FehrE,GintisH,etal. Insearchofhomoeconomicus:behavioralexperimentsin15small- scalesocieties.AmEconRev.2001;19(2):73-78.
21. BraithwaiteJ.Analysingstructuralandculturalchangeinacute settingsusingaGiddens-Weickparadigmaticapproach.Health CareAnal.2006;14(2).Inpress.
22. BraithwaiteJ.Anempiricalassessmentofsocialstructuraland culturalchangeinclinicaldirectorates.HealthCareAnal.2006; 14(4).Inpress.
23. WeirP.Masterandcommander:thefarsideoftheworld.http:// www.imdb.com/title/tt0311113/,2003;(accessed20/9/2006).
24. BraithwaiteJ,WestbrookMT,IedemaR,MallockNA,ForsythR, ZhangK.Ataleoftwohospitals:assessingculturallandscapesand compositions.SocSci&Med.2005;60(5):1149-62.
25. HouseR,HangesP,JavidanM,DorfmanP,GuptaV,Eds.Culture, leadershipandorganisations:theGlobestudyof62societies. ThousandOaks,CA:Sage;2004.
26. AlvessonM.Understandingorganisationalculture.London:Sage; 2002.
27. MartinJ.Organisationalculture:mappingtheterrain.Thousand Oaks,CA:Sage;2002.
28. BraithwaiteJ.Axiomsforgoverninghealthsystems.BrMedJ.2005; 330:1032.
ResponsetoPodger’sModelHealthSystemforAustralia(Part1andPart2)
AsiaPacificJournalofHealthManagement2006;1:2 21

r E S E a r c Ha r t i c l E
regulation in the doldrums: reforming privatehealth care sector legislation in BangladeshMr rahman, S Barraclough
introductionForalmostaquarterofacentury,Bangladesh’sprivatehealthcaresectorhasbeenregulatedunder legislationoriginallypromulgatedundermartial lawata timewhenthissectorwas at a fledgling stage.The law has been amended onlyslightly,despitetheburgeoningofprivatehealth facilities.Problems associated with private health sector regulationand concerns about the delivery of services, quality andstandardsofcarehavebeenreportedinvariousstudies,andin the national press. [1,2,3,4,5] The growth of this sectorhasposedchallengesforthestateastheprivatesectorhasfailedtoensurethatthequalityandstandardsofhealthcaremeetthosedemandedbyconsumers.[6]
M redwanur rahmanPhD,MPhil,MSS,BSS(Hons)DepartmentofPoliticalStudiesShahjalalUniversityofScience&TechnologySylhet-3114,Bangladesh
Simon BarracloughPhD,MA,BA(Hons)SchoolofPublicHealthLaTrobeUniversityVictoria,Australia
Correspondence:[email protected]
abstractObjectives: To describe the origins of private health care sector regulation in Bangladesh and to identify both deficiencies and reforms necessary for more effective control of this growing sector, including draft legislation.
Design: The research combined documentary analysis and confidential in-depth interviews conducted in Dhaka. Informants included private health service managers, Ministry of Health officials and consumer advocates.
Setting: Unable to provide health care for the growing population, the Government of Bangladesh has welcomed private sector investment and provision, leading to the largely unregulated, rapid expansion of for-profit private clinics and hospitals. Private health sector legislation was originally promulgated under martial law in 1982 and has been poorly enforced.
Findings: A range of deficiencies in regulation were identified, including inadequate definition of services and the absence of comprehensive infrastructure requirements, leading in some cases to serious abuses. The qualifications of providers, quality of care, and excessive provision of services were not subject to regulatory scrutiny. The poorly-resourced regulatory
authorities operated in a highly centralised system, often lacking both the authority and willingness to enforce legislation. Corruption was a problem, occasionally involving the use of extortionists to intimidate government officials. The interests of consumers have not been well served due to, mismanagement and poor governance in regulating the private health sector.
Conclusions: It is imperative that regulatory reform is introduced, despite the opposition of vested medical interests and attempts to dilute its provisions. The draft law attempts comprehensive regulation but still has deficiencies. Nor does it respond to demands for a more independent and decentralised regulatory apparatus, sensitive to consumer rights and empowered to deal with corrupt practices. Further reform will therefore be necessary.
Abbreviations:BMA-BangladeshMedicalAssociation;BPMPA-BangladeshPrivateMedicalPractitionersAssociation;CMLA-ChiefMartialLawAdministrator;MOHFW-MinistryofHealthandFamilyWelfare.
Key words:Bangladesh,privatehealthsector,reform,regulation
22 AsiaPacificJournalofHealthManagement2006;1:2

In this context, the state has a responsibility to protectcitizens, and to maximise the benefits and minimise thenegative effects of the private provision of health care.The implementation of regulations is an effective way tomeetconsumerdemandsfortheprotectionoftheirrights.AccordingtofigurescitedbytheWorldBank,privatehealthexpenditure represents56%of totalhealthexpenditure inBangladesh,ofwhich93%ispaidout-of-pocket.[2,p.4]Ithasalsobeenfoundthatthedisadvantagedusetheprivatesectormorefrequentlythanthepublicsectorforoutpatientcare,despitethelatterbeingfreeofcharge.[2,p.6]
Successive governments of Bangladesh have sought toimprove the health status of the population. Governmentpolicy has been to encourage the development of theprivate health sector, which is evident in the policy andplanning documents of the Bangladesh Government.[7,8,9,10] International development assistance agencieshavealsopromotedprivatehealthcaresectorgrowthandencouraged the building of a partnership with the publicsector.[2,11,pp.42-43,46;12,p.50-56]By1997therewere6,213 private hospital beds in 158 private hospitals and29,106bedsin645publichospitals.Inaddition,thereweresome5,158privatenursinghomebeds.[2,p.3]AstheWorldBankhasnoted,morerecentdataisunavailable.[2,p.3]
The number of private hospitals and clinics is growingwithout adequate provision for quality and standards ofcare.[3,5,11,p.45-46]Therapiddevelopmentoftheprivatesectorhaschallengedthestatetoensurethatoptimalcareis provided. The implementation of regulatory activitiesis pivotal to the attainment of the Government’s missiontoensurequalityandstandards intheprivateprovisionofservices.AstheWorldBankhasobservedinarecentstudy:
. . . the form and scope of government engagement with the private sector is limited and does not seem to be in accordance with the importance of the latter. This refers not only to the lack of contractual relationships in order to harness the private sector for public policy goals, but also to the insufficient regulation of private sector providers. [2,p.6]
MethodsThis study used qualitative research methods, includingin-depth interviews undertaken in 2003. Data were drawnfrom hospitals and clinics owned by private individuals,groups, and companies, offering services on a for-profitbasis. Primary sources of data included semi-structuredconfidentialinterviewswithgovernmentofficials,including
officialsfromtheDirectorate-GeneralofHealthServicesandtheMinistryofHealthandFamilyWelfare(MOHFW),privatehospital executives, provider associations, representativesofvarioushealthrightsandadvocacygroupsandmedicalprofessionals. Official development plans were alsoconsulted as a primary source of data. Secondary sourcesincludedjournalsandpressreports.
Interviewdatawereanalysedthematicallyandtheanalyticalapproachofallsourcesofdatadrewuponthepolicyanalysismodel of Walt and Gilson [13] and stakeholder analysisconceptsofVarvasovszkyandBrugha.[14]
The Ethics Committee of the Faculty of Health Sciences,La Trobe University, Melbourne, Australia, approved theresearchproject.
FindingsBangladesh’s first-ever legislation to regulate the privatehealthsectorwasrealisedundermartiallawin1982.GeneralH.M.ErshadhadseizedpowerinMarch1982,andParliamenthad been suspended. During military rule, the power topromulgate an ordinance, normally the prerogative of thePresident, rests with the Chief Martial Law Administrator(CMLA).Howeverwhencivilianruleisrestored,theordinanceneedstobepresentedforenactmenttothefirstsessionofParliament.
Although health legislation is not normally high on theagenda of newly-installed military regimes, the Medical Practice and Private Clinics and Laboratories (Regulation) OrdinancewaspromulgatedbytheCMLAafewweeksaftertheproclamationofmartiallaw.
Not surprisingly, the legislation was not an initiative ofthe military regime: preparatory work on this ordinancehad begun prior to the military takeover. At that timephysiciansbasedtheirfeesvariouslyupontheirreputation,designation and place of practice as well as the marketdemand for their services. These disparate fees were amatter of concern. Another problem was the absence ofminimumstandardsinmanynewprivateclinics,pathologylaboratoriesanddiagnosticcentres.WhiletheGovernmentwishedtoseetheprivatehealthcaresectordevelop,italsorecognised the need for regulation to protect consumers.TheCMLAsubsequentlytookoverthisregulatoryinitiative.ThusBangladesh’sfirstprivatehealthsectorlegislationwasenactedinanauthoritarianwayusingthetechnicalsupportof the bureaucracy but without parliamentary scrutiny orpublicdebate.
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
AsiaPacificJournalofHealthManagement2006;1:2 23

the 1982 ordinance to regulate medical practice, private clinics and laboratoriesThe main features of the 1982 legislation, which is still inforce,toregulateprivateclinicsandhospitalsare:
• Licensing:Allprivateclinics,hospitalsandlaboratories mustbelicensedtoperformoperations.
• Requirements for facilities:Aclinicrequiresaspace ofatleast80squarefeetoffloorforeachin-patient bedandmustprovideanhygienicenvironment,anair- conditionedoperatingtheatre,andessentialmedicines, instrumentsandequipment.
• Staffing:Afacilityowner(s)needstoemployfull-time atleastoneregistereddoctor,twonurses,andone auxiliaryforeverytenbeds.Thisemploymentprofile mustbemaintainedatalltimes.Specialistmedical practitionersmustbeemployedforoperationsand thetreatmentofpatients.
• Charges:Alistofchargesfordifferentservicesmust bedisplayedinthepremises.Aprivatefacilitymust maintainaregisterofthenamesandaddressesofpatients andmustprovideaprintedreceipttopatientsforany payment.
• Inspection:TheDirector-General,orhisorherauthorised representative,caninspectthepremisesofaprivate facility.Ifthefacilitydoesnotfollowthelicensing conditionsorcontravenesanyprovisionofthelaw,the Director-Generalmaycancelthelicenceofthefacility, aftergivingtheowneranopportunityto‘showcause’ againstsuchcancellation.TheDirector-Generalcanalso prosecutetheownerofafacilityforcontraveningany provisionofthelaw.TheCourtmayimposeafineofup to5,000.00BangladeshiTaka(approximatelyUS$75) orimprisonmentforamaximumperiodofsixmonths, orbothontheowner(s)ofafacility.Inaddition,theCourt mayordertheconfiscationofalloranyofthemoveable propertyinthefacility.
• Appeal:Anypersonaggrievedbyanorderofthe Director-GeneralmayappealtotheGovernmentwithin 30daysofitsreceipt.ThedecisionoftheGovernment onsuchanappealisfinalandcannotbequestioned byanycourtoflaw.[15]
Problems with the 1982 ordinanceSeveral inadequacies and shortcomings in the legislationhavebecomeevidentsinceitspromulgation.
1. Inadequate definitionsThe1982legislationusesimprecisedefinitions.Forexample,a “private clinic” is merely defined as a facility in whichpatientsareadmittedorprovidedwithmedicalorsurgicaltreatment. It may be called a nursing home, hospital orclinic, despite the disparate functions of each facility.Informantsagreedthatthedefinitionsprovidedinthe1982ordinanceweretoogeneraltobeeffective.Forexample,thedefinition of“private laboratory” does not include privatebloodbanks.
Thevarietyofspecialisedfacilitiesnowoperatingnecessitatesafunctionaldefinitionofprivatehospitals,clinics,maternitycentres, nursing homes, specialised hospitals or clinics,polyclinicsandambulatoryclinics.
2. Absence of comprehensive infrastructure requirementsSeveralinformantswereconcernedthatcurrentlegislationdoesnotrequirethesubmissionofacomprehensivebuildingplanfortheestablishmentandmaintenanceofaproposedprivatehealthcarefacility.Thecurrentlawstipulatesafloor-spacerequirement,butdoesnotaddressotherinfrastructureissuesorbuildingcodes,suchasthebuildinglayout,andthenumberoftoiletsandbathrooms.Waitingrooms,outpatientareas,emergencywardsandmedicalsupportfacilities,suchas laboratories and radiology, are not mentioned; nor arekitchens, washing rooms, incinerators, hazardous wastedisposal facilities and parking areas included. Moreover,thelawdoesnotdealwithmodificationofthepremisesofafacility.
According to informants from the Ministry of Health andFamily Welfare (MOHFW), in some extreme cases, serviceproviders have established health facilities in dilapidatedpremises, in which the kitchen functioned as a pathologylaboratoryorasanX-rayroom,withoutadequateprotectionfromradiation.
Therewerealsoconcernsabouttheprovisionofemergencyfacilities. Many private hospitals lacked an emergencydepartment,whilstsomehealthserviceswhichdidhaveanemergencydepartmentwerereluctanttoadmitemergencypatientsduetoalackofspecialistmedicalstaff.Emergencypatients were often referred to public hospitals. Any newlaw should therefore make the provision of emergencydepartmentsmandatory.
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
24 AsiaPacificJournalofHealthManagement2006;1:2

3. Problems with the regulatory authority, its powers and the enforcement of the lawInformants from both the Ministry and health advocacygroups claimed that the law does not make the regulatoraccountable, nor does it create a transparent regulatorysystem.Theysawtransparencyasessentialfortheeffectiveadministrationofregulation.
The present law lacks comprehensiveness in describingthe powers and authority of the Director-General ofHealthServices.Forexample,whilethe lawstatesthattheDirector-General, or an authorised person, can inspect afacility,itdoesnotdetailwhatconstitutesaninspection,thesuspensionofalicenceor“showcause”.Noraretheprocessofdelegation,andthestatusandpowerofan“authorised”person, stipulated.Nopenaltiesarespeltout for failure toprovidenecessaryinformation.Indeed,theDirector-Generalhimselfobservedthat:
The existing law is not strong enough to prove an offence in any private clinics or hospitals. The best effort the Directorate Office can do is to bring charges against those clinics for malpractices and serve them with show cause notices. [16]
Most staff or representatives from the Directorate andMinistrysaidthatthelawwasinadequate.OneofficerintheMinistrycommented:
The law does not give enough power to the Directorate to close facilities which have failed to meet compliance requirements.
The issueofunethicalandcorruptpracticeswas raisedbysome health consumer advocates, one of whom observedthat:
The law does not regulate or monitor technology acquisition, excessive provision of services, unethical behaviour, unnecessary investigations and interventions, income tax evasion and patient referral practices.
Health rights advocates observed that the 1982 law doesnotdealwiththefitnessofindividualstoownandoperateaprivatefacility.Itdoesnotexcludedishonestpersons,loandefaulters, bankrupts or persons convicted of fraud. Norare the responsibilities of a private facility licence holderstipulated. There are no penalties for unethical practiceby providers and physicians, such as paying commissionsfor sending patients to a private facility, or fee-splitting.Accordingtoseveral informantsfromdifferentgroups,theenforcement process of the law is not articulated clearly.The lawdoesnot indicatehowtherenewalof registration
andlicencesshouldbecarriedout,orwhetheritshouldbedoneafter,orwithout,inspection.Itmakesnoprovisionfordealingwithobstructionorresistancebyowners,orothers,ofregulatoryactivities;nordoesitmakeanyprovisionsforthosewhoaidorabetanotherpersontocommitanillegaloffence. Moreover, penalties for subsequent offences arenotstated.
An additional problem identified in the literature onregulationinBangladeshisthelengthoftimetakentoissuealicence.[17,p.8]Severalparticipantscommentedthattheadministrative process is highly centralised in the capital,Dhaka City, and that registration usually takes more thansixmonths.Theprocessingofafirstlicencemaytakemorethan12months,whilerenewingalicencemaytakealmostaslong.Insomecaseslicencenegotiationsinvolvedtheuseofinducements.Someprivatesectormanagersmaintainedthat an unofficial brokerage system exists, involving thenegotiation of licences. Some claimed that local mastans(extortionists)aresometimes employed tohelp owners togainorrenewalicence.
Kawnineetal (1998)haveobservedthatthelackofclarityof regulators’ powers “…provides MOHFW inspectorswith considerable latitude for demanding a ‘rent’ fromclinic owners for approving registration”. [17, p. 9] Privatesector managers claimed that the law does not clarifymany of the issues, such as the timeframe for issuing andrenewinglicences,thedistributionpatternoffacilities,andqualifications of the owner of a facility. Even the renewalprocessisinadequatelydetailed.
Problems exist regarding the distribution of power inrelationtotheclosureofafacility.TheDirector-Generalmayservenoticetocloseafacilitybutaprovidermaynotfollowthisdirective.ThelegalpowersoftheDirector-General,thepoliceortheMOFHWarenotclearlydefinedinlegislation.Another criticism of the law is that it does not make anyprovisionforreceivinganddealingwithcomplaintsmadeby,oronbehalfof,patients.Thelawfailstomentionsanctionsforinjuryorforcausingadangertopublichealthorsafety.ThisdeficiencyhasbeenobservedinpreviousstudiesoftheprivatehealthsectorinBangladesh.Hye(2003)maintainedthatthelaw“neitherprovidesmuchattentiontoconsumerprotectionrights,nordoesitprovideanypracticablemeansofredressforharmdonetoconsumers”.[18,p.61]Ali(2000)points out that patients’“right to be admitted into healthfacilities in an emergency and their grievances are notincludedinthelegislation”.[19,p.11]
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
AsiaPacificJournalofHealthManagement2006;1:2 25

4. Staffing and quality provisionsAnotherissueofconcerntoinformantswasambiguityaboutthe qualifications of personnel. The law clearly stipulatesphysicians’ qualifications but makes no mention of thoseof allied health professionals. One health rights informantobserved:
The providers recruit non-qualified persons as technicians, pathologists, radiologists and nurses. Patients are cheated by the providers, as they allow non-experts to perform specialists’ jobs. Providers should not employ, or allow, unqualified or non-specialist persons to provide specialised medical care.
Thisproblemhasalsobeenidentifiedbyotherresearchers.As Hye (2003) observed, as a result of this legal loopholemost of the private clinics and hospitals do not employregisteredstaffnurses.[18,p.46]Thelawdoesnotspecifystaffing patterns or minimum qualifications for nurses,technicians,pharmacists,radiologists,andpathologists;nordoes it require induction programmes, in-service trainingor refreshercourses forstaff. Inaddition, the lawdoesnotaddresstheneedforspecialisednon-medicalpersonnel.
Another problem with the law is its emphasis on inputs,such as physical conditions and personnel, rather thanoutcomemeasures,intermsofqualityofcare.AnofficialintheDirectorateconcludedthat:
The law is not able to maintain quality and standards in the private sector.
Aprivatefacilitymanagerobservedthat:
Quality is a neglected issue as far as the law is concerned. There is an absence of maintaining medical records and periodic medical audit.
5. Social justice and complaints issuesConsumersandhealthcareadvocatesdemandedlegislationfor fee structures for services provided to poor patientsso that they could access necessary treatment. They alsowanted mechanisms for lodging complaints. As oneinformant put it, the new law“should clearly articulate acomplaints mechanism, consumer rights and proceduresforredress”.
6. Failure to review legislationAnotherconcernidentifiedbyallinformantswastheabsenceof any formal review process of the original legislation.Several Directorate officials observed that while changeshave occurred in medical science and technology, and inpeople’sdemandsandbehaviour,thelawhasnotkeptpacewiththesechanges.
A pertinent example of outdated legislation is that offees. ThelegislationspecifiedthattheGovernmentwouldamend the fee structure“from time to time” but this hasnothappened.Duetoinflationafeestructuresetalmostaquarterofacenturyagoisnowclearlyunrealistic.
The Government’s reluctance to reform and enforcelegislation on fees reflects the influence of the medicallobby.TheregulationoffeesbytheGovernmenthasbeenopposedbytheSecretary-GeneraloftheBangladeshMedicalAssociation(BMA)whoarguedthat,sincetheGovernmenthas endorsed market principles in the economy, it shouldnot interfere with fees for medical services. Rather, theseshouldbedeterminedbyphysiciansandtheirorganisationandshouldbeconsistentwithprevailingmarketprices.[20]The president of Bangladesh Private Medical PractitionersAssociation (BPMPA) shares this view, maintaining that inan“openmarketsystem,thereisnojustificationforhavingfixedrates”.[16]
Consumer informants (including health consumer groups)claimed that the Government’s lack of attention to feerestructuring indicated its apathy towards consumers’interests.Asoneconsumeradvocateobserved:
The Government should pay attention to consumers and determine a fee structure after consultation with various stakeholders. Providers are now charging whatever they like. It is absolutely a wrong practice.
attempts to reform the 1982 ordinance: 1996-2001TheBangladeshAwamiLeague,whichheldofficefrom1996to2001,includedrevisionofthe1982legislationinitshealthsectorreformpolicy.AdraftBillwaspreparedin2000butwasnotplacedbeforeParliament.Anewgovernment,ledbytheBangladeshNationalistPartywaselectedin2001andcontinuedtodevelopthedraftpreparedbyitspredecessor.TheGovernmentinvolvedaconsortiumofforeignaiddonoragencies,headedbytheWorldBank,inpreparinglegislationtoregulatetheprivateprovisionofservices.Thedevelopmentof this law was part of the policy agreement between theGovernmentofBangladeshandtheconsortiumtorestructurethehealthsector.[21]TheGovernmentcirculatedthedraftproposed Bill among medical stakeholders, including theBMA, the BPMPA and the Bangladesh Private Clinics andDiagnosticOwnersAssociation.TheBMAdidnotformulatea comprehensive alternative proposal but, instead soughtthedeletionofpartsoftheproposedBillconsideredharmfultoitsmembers’interestsandtheinclusionofclauseswhichwould further their interests.The BMA has a considerableinfluenceontheDirectorate’sactivitiesthroughitslinkswith
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
26 AsiaPacificJournalofHealthManagement2006;1:2

thepartyinpower.Severalpressreportshaveclaimedthatthe BMA has considerable influence upon the Ministry ofHealthandFamilyWelfare.[22,23,24]
A limited agreement was reached between the Ministryand the BMA. [25] The reworked law was subsequentlysent to the Ministry of Law, Justice and ParliamentaryAffairs for review, specifically to identify any loopholes oranycontradictionswith thecountry’sbasic laws,andthenforwardedtoCabinet.ThedraftPrivateMedicalandHealthServiceBillwasapprovedbyacabinetmeetingchairedbythePrimeMinister.[26]
However,earlyin2004itwasreportedthattheintroductionoftheproposedBilltoParliamenthadnotgoneaheadduetothedetectionofmajorflawsinafewofitsclauses.[27]
Most BMA members were reported to be against the Billand had actively lobbied for its withdrawal. In a pressinterview about the proposed law the BPMPA presidentstated:“We strongly oppose the idea of law suits againstmedical practitioners.We already have a body to monitorallegationsofmalpractice,negligenceandotherviolations.”[16]Thisassociationcontinuestobeunwillingtoaccepttheproposedlawunlesschangesordeletionstocertainclausesaremade.[16]
Intermsofthepowerofthemedical lobbyinBangladesh,it is significant that in the course of its discussions andconsultations with various stakeholders, the Governmentdidnotconsultanyconsumersorthehealthrightsadvocacygroups.
a proposed Bill to reform private health sector legislation: 2002 - 2006In 2002, in an effort to deal with the regulatory problemsassociated with the growing number of private facilities,manyofwhichwereunregisteredandnotevenincludedinofficial statistics, a new Bill was drafted. [28]The principalfeaturesofthisdraftBillinclude:
• Abroaderfocusthanwasthecasewiththeinitial1982 Ordinancewith19areasofprivatehealthcovered(the 1982lawdefinedonlyeightareas).Thenewlawalso definestherolesofnurses,privateclinics,medical assistantsandlicensees.
• Nopersonisallowedtoestablishortomaintainaprivate clinicorfacilitywithoutalicence.
• Privatefacilitieswillbeclassifiedaccordingtotheservices theyprovide.TheDirector-Generalisempoweredtomake by-lawsonequipment,personnelandcleanlinesssothat theprivatefacilitiesareobligedtomaintainminimum standards.TheDirector-Generalwilldeterminethefees tobechargedbythefacilityforprovidingdifferent services.
• Atimeframeforthegrantingandrenewalofalicence. Alicencewillbevalidforthreeyears.TheDirector-General willassessanapplicant’spremiseswithin60daysofthe submissionofalicenceapplication,andwilltakeaction accordingtotheinvestigator’sreport.
• OfficialsoftheDirectorate-GeneralofHealthServices andtheciviladministrationwithdelegatedauthority, especiallypersonnelfromtheDeputyCommissioner’s office,areempoweredtoenterandinspectanyarea ofaprivatehealthcarefacility.Theymayexamineany documentorpieceofequipmentandcantakeaway anyitemforfurtherexamination.Thepowerofthe licensingauthorityisextendedfromtemporaryclosure topermanentclosureofafacility.Ifaregulatororthe regulatoryauthoritybelievesthatafacilityisperforming anyharmfulordangerousactivity,oriftheservices providedaresubstandard,thefacilitycanbeclosed immediately.
• AsintheoriginalOrdinance,TheDirector-Generalof Healthoranauthorisedofficerhasthepowertofilea caseinthecourts;however,theproposedlawincreases thefineformedicalnegligenceormisconduct.
conclusion Legislative reform to address standards and the qualityof health care services provided by the private sector inBangladesh is years overdue. Comprehensive legislation isa vital first step for the effective regulation of the privatesector.
There are many positive features in the most recentlyproposed law. It includes some of the imperatives forreform,suchasatimeframeandproceduresfortheissuingofalicence,penaltyprovisions,thepowerofaregulatortoinvestigatepremises,provisionsforclosure,andproceduresfor the formulation of by-laws covering personnel, feesstructure,equipmentandhygiene.However,theproposedlawdisregardsmanyoftheotherrequirementsforreform,includingthedecentralisationofthelicensingprocessandconsumer demands for the inclusion of medical practiceunder the criminal or consumer protection law. Nor are
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
AsiaPacificJournalofHealthManagement2006;1:2 27

medicalpracticebyunqualifiedpersonnelandtheexcessiveprovisionofservicesfor-profitandqualityofcareincluded.Thedemandforanon-partisanandimpartialregulatorybodyis also ignored. Possible corruption of regulators, medicalnegligence and the need for a complaint mechanism arealsooverlooked.Finally,theproposedlawdoesnotaddressthe need for a detailed plan of proposed facilities to besubmittedaspartoflicensingapplications.
The Government’s failure to introduce the reformedlegislation into Parliament in a timely fashion is also aconcern.FouryearshaveelapsedsincethedraftingoftheBillin2002.Vestedmedicalinterestshavesuccessfullydelayedreform. Proponents of regulatory reform, both within thestate and in civil society, need to mobilise demands foractiononthepartoftheGovernment.TheymustensurethatthenewlegislationiseffectiveinprotectingtheinterestsoftheincreasingnumbersofBangladeshisseekinghealthcareintheprivatesector.
acknowledgementsTheauthorswishtoacknowledgetheindependentreviewersfortheirusefulsuggestionstoimprovethearticle.
competing interestsTheauthorsdeclarethattheyhavenocompetinginterests.
references 1. TheDailyStar.Privatehospital/clinicirregularities.TheDailyStar. 2003Aug22;Dhaka.TheDailyStar.Lackofproperservicesin hospitalsworriesPrimeMinister.TheDailyStar.2002April18;Dhaka.
2. TheWorldBank.Comparativeadvantagesofpublicandprivate healthcareprovidersinBangladesh.Dhaka:Bangladesh DevelopmentSeries;2005.PaperNo.4.
3. TheIndependentBangladeshPrivateMedicalpractitioners Association(BPMPA).Lawsoontoensurequalityhealthcare atprivatehospitals:PrimeMinister.TheIndependent.2002Oct28; Dhaka.
4. KhanMM.HealthsystemofBangladeshintransition-impacton cost,accessandquality.Dhaka:unpublished;1996:1-20.
5. RahmanM.Astudyonqualityofmedicalcareprovidedbyprivate clinicsofDhakaCity.[DiplomainCommunityMedicineunpublished thesis].Dhaka:UniversityofDhaka;1994.
6. AhmedY,HasanB.Healthconsumerrights:theBangladeshcontext. In:Dhaka,HealthConsumersRightsForum(unpublished);2003:1-10.
7. GovernmentofBangladesh.FirstFiveYearPlan1973-78.Dhaka: PlanningCommission,MinistryofPlanning,Governmentof Bangladesh;1973.
8. MinistryofHealthandFamilyWelfare.Nationalhealthpolicy. Dhaka:MinistryofHealthandFamilyWelfare;2000.
9. MinistryofHealthandFamilyWelfare.Healthandpopulationsector programme.Dhaka:MinistryofHealthandFamilyWelfare;1998.
10. MinistryofHealthandFamilyWelfare.Conceptualframeworkfor health,nutritionandpopulationsectorprogramme,2003.Dhaka: MinistryofHealthandFamilyWelfare;2003.Availablefrom: <www.mohfwbdgov.org/concept_toc_6.htm>Accessed:July23, 2006.
11. WorldBank.Privatesectorassessmentforhealthnutritionand populationinBangladesh.Dhaka:TheWorldBank;2003.Unpublished reportno.27005-B:1-76.
12. AsianDevelopmentBank.Policyforthehealthsector.Manila:Asian DevelopmentBank;1999.
13. WaltG,GilsonL.Reformingthehealthsectorindevelopingcountries: thecentralroleofpolicyanalysis.HealthPolicyandPlanning. 1994;9(4):353-370.
14. VarvasovszkyZ,BrughaR.Astakeholderanalysis.HealthPolicy andPlanning.2000;15(3):338-345.
15. MinistryofLawandLandReforms.TheMedicalPracticeandPrivate ClinicsandLaboratories(Regulation)Ordinance1982.Ministryof LawandLandReforms.1982.
16. TheDailyStar.Doctorsface10yearsformalpractice.TheDailyStar. 2004February13.
17. KawnineN,KillingsworthJR,GuinnessL,Hedrick-WongY,Rahman MA,HussainDN.Privatesectormedicalclinicsandhospitalsurvey. Dhaka:MinistryofHealthandFamilyWelfare,HealthEconomics Unit;1998.ResearchPaperNo.15.
18. HyeHKMA.HealthRegulationReview.Dhaka:Reportsubmitted totheWorldBank,DhakaOffice,unpublished;2003.
19. AliA.Regulatoryframeworkfortheprivatehealthcaresectors inBangladesh.Dhaka:NICAREandtheBritishCouncil;2000.
20. TheJugantor.Wrongtreatment:alawismakingwithpenalty provisions.TheJugantor,2003December29.
21. WorldBank.Donorspartiallysuspendingfundingduetostalled healthreforms.Dhaka:HealthProgramSupportOffice,TheWorld Bank;2003.
22. TheDailyStar.Politically-poweredBangladeshMedicalAssociation meddlesindoctorposting.TheDailyStar,2003November16.
23. TheDailyInqilab.BangladeshMedicalAssociationopposes governmentdecisionsonhealthandfamilyplanning.TheDaily Inqilab.2003September25.
24. TheProthemAlo.BangabundhuMedicalUniversity:partisanpolitics andlawlessness.TheProthernAlo.Dhaka;2003September12.
25. MinistryofHealthandFamilyWelfare.Noticetoinviteameeting todiscussonproposedbillonprivatemedicalandservicesBill. Dhaka:MinistryofHealthandFamilyWelfare;2002.
26. TheDailyStar.Draftofprivatemedicalserviceactapproved. TheDailyStar.2003November25;Dhaka.
27. TheNewAge.Billregulatingclinicswithdrawnduetoglitch. TheNewAge.2004January20;Dhaka.
28. MinistryofHealthandFamilyWelfare.PrivateMedicalandServices Bill(Proposed).Dhaka:MinistryofHealthandFamilyWelfare;2002.
RegulationintheDoldrums:reformingprivatehealthcaresectorlegislationinBangladesh
28 AsiaPacificJournalofHealthManagement2006;1:2
Sarah Michael1
ClinicalExcellenceCommission,NewSouthWales
Maureen robinson1
CommunioPtyLtd
Paul douglasNorthernSydneyCentralCoastAreaHealthService
Jeffrey BraithwaitePhDAssociateProfessorandDirectorCentreforClinicalGovernanceResearchinHealthFacultyofMedicine,UniversityofNewSouthWalesSydneyNSWAustralia
1.AtthetimeofthedevelopmentoftheSafetyImprovementProgram(2001-2004)SarahMichaelandMaureenRobinsonwererespectivelytheManager,SafetyImprovementandDirector,QualityandSafetyBranch,NSWHealth.
Correspondence:Email:[email protected]
r E S E a r c Ha r t i c l E
introductionThere is a growing body of international and Australianknowledge that has contributed to the introduction ofpatient safety initiatives. Borrowing from other high-riskindustrieswheresafety isparamount,Safety ImprovementPrograms (SIPs) aim to develop techniques to identifyrisks, investigate and analyse incidents and supportimprovements in practice. In principle, these techniquesallow health services to manage known risks actively anddevelopsystemstoidentifyneworemergingrisks.
Recent studies, [1-4] investigations and inquiries [5-8] intohealth care have highlighted the need for clinicians,managers, policy makers and educators to look carefullyat quality and safety. In 1995 the Quality in AustralianHealth Care Study was commissioned as part of theCommonwealth Government’s Review of ProfessionalIndemnityArrangementsforHealthCareProfessionals.
changing an incident reporting and Management Paradigm: the nSW Safety improvement ProgramS Michael, M robinson, P douglas, J Braithwaite
abstract:Objective: To conduct a formative evaluation of progress to date with safety improvement initiatives in New South Wales.
Design: Description of safety improvement initiatives. Secondary analysis of extant databases of reportable incidents, root cause analyses and categories of improvement actions to date.
Setting: The state of New South Wales, Australia.
Main outcome measures: Education initiatives, policy reforms, reportable incident data, root cause analyses categories, safety improvement activities.
Results: Over 2,500 people have been trained in the safety improvement program. Over 1,000 others have been exposed to safety improvement educational sessions.
This represents over 3.9% of the 90,000 full time equivalent staff in the New South Wales health system. Evidence shows incident reporting is increasing. Causal and contributing factors are more explicit via root cause analyses.
Conclusions:There is early evidence of systems improve-ments in New South Wales.
Abbreviations:NSW-NewSouthWales;RCA-RootCauseAnalysis; RIB - Reportable Incident Brief; SAC - SeverityAssessmentCode;SIP-SafetyImprovementProgram.
Key Words:incidentmanagement,harmreduction,adverseevents,systemsapproaches,rootcauseanalysis
AsiaPacificJournalofHealthManagement2006;1:2 29

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
This researchfocusedpublicattentiononthe incidenceofadverseevents in thehealthsystem.Thestudy foundthataround half of adverse events experienced by patientsin the health system were preventable. It showed thatinterventions, care and treatment intended to providediagnostic information or improve patient health caninadvertently cause harm and that this risk is particularlyhighintheacutehospitalenvironment.
BackgroundThispapertracesthedevelopmentofaninitiativedesignedto tackle this issue by analysing the SIP in the New SouthWaleshealthsystemsinceitsinceptionin2002.NewSouthWales is Australia’s most populous state and representsalmostathirdofAustralia’seconomy,andishometosome6.7millionresidents.Thereareover200publichospitalsandpublicnursinghomesandsome90,000fulltimeequivalentstaffemployedinthesystem.[9]Themajorityofhealthcareispubliclyfunded,andNewSouthWalesfollowsthepatternof Australian health care costs which account for around9.7%ofgrossdomesticproduct.[10]
SIP is a major initiative of NSW Health and is designed toprovide a coordinated approach to the prevention andmanagement of incidents that occur in the New SouthWaleshealthsystemthrough increasingknowledgeaboutwhyerrorsoccurandapplyingthatinformationtoenhancepatient and staff safety. Incident management is not apanaceaforqualityandsafety.Manyapproachesarerequiredforeffectiveimprovementofhealthservices.[11]Theseincludeaccreditation,theapplicationofclinicalindicators,morbidityandmortalityreview,riskmanagement,clinicalgovernanceandclinicalaudits.[12,13] Incidentmanagementisoneofthese, and is considered an important plank in improvedpatientsafety.
UntiltheintroductionofSIP,therewasnouniformstructureor process in New SouthWales at either the state or AreaHealthService leveltomanageincidents inacoordinated,standardised manner. The previous reportable incidentsystem in New South Wales did not have an embeddedmanagement process and resulted in few improvementsbeing made to the health system as a whole. At an AreaHealthServicelevel,asmallnumberofeventswassubjectto thorough investigation procedures with actions andrecommendations identifying ways to prevent similarrecurrences.
However other more frequent incidents remainedunidentified or unreported and hence uninvestigated.Exacerbatingthisissue,itwascommonforincidentsarisingin health care, as in other industries, to be blamed on theindividual.[14]Thisaffectedreportinglevelsandignoresthecontext-dependentnatureofmostincidents.[15]
TheNSWSafetyImprovementProgramattemptstoalterthisresponsepatternbyreinforcingasystemsapproachratherthananindividualapproach.Itrecognisesthatpeopledonotcometoworkintendingtodoabadjobortomakeamistake;onthecontraryitemphasisesthatcertaincircumstancesandtheworkenvironmentcancombinetoproduceunwantedoutcomes.[16]Thisleadstoanacceptancethathealthcareworkersdonotoperateinisolationandthatbothproblemsandsolutionsareofasystemsnature.[17]Wedonotknowthe extent to which deep-seated cultural characteristicscan be modified. However, SIP is an initiative designed tounderpinsuchchange.
Establishing the safety improvement programIn late 2001, NSW Health invoked a process to determinethekeycomponentsofaneffective incidentmanagementstrategy for the New South Wales health system. It was aresponsetothenationalagendaagreedbyhealthministerssubsequenttotheestablishmentoftheAustralianCouncilfor Safety and Quality in Health Care. [18] Following aliterature review, expert focus groups were conducted tocanvass attitudes and a search for effective systems wasinitiatedinterstateandinternationally.Asteeringcommitteeidentified three key components for an effective system.The first component is a culture and environment thatfacilitates identification, reporting, investigation, analysisand action associated with health care incidents. [19,20]In order to improve the systems of care provision and tobe effective, incident management requires that as manyadverseeventsornearmissesaspossibleareknownaboutandmanaged.[21,22]Thesecondisaninformationsystemthatwillsupportthischanged,incident-awareculture.Thethirdcomponent isatrainingprogramtodevelopcohortsof clinicians, managers and policy makers skilled in safetyimprovement processes and approaches. [23] Consumerswereincludedintheprograminaninnovativeapproachtosafetyeducation.
The New South Wales safety improvement initiatives arebasedonworkundertakenbytheNationalCentreforPatientSafetyintheVeteransAdministrationintheUnitedStatesofAmerica.[24-26]TheestablishmentprocessadoptedinNewSouthWalesisoutlinedinTable1.
30 AsiaPacificJournalofHealthManagement2006;1:2

Table 1: The staged establishment process of the New South Wales Safety Improvement Program, May 2003 to May 2005
• EducateandtrainthosekeypersonnelintheNewSouthWaleshealthsystemresponsibleforprogram development.
• Developresourcestosupporttheprogramstate-wide.
• Launchtheprogramtohealthcareprovidersandconsumers,withtheNSWMinisterforHealthandtheDirector oftheNationalCentreforPatientSafety.
• Pilottheprocessineighthealthservices,includingeducationandsupport.
• Amendtrainingandresourcematerialsbasedonfeedbackfromthepilotprocess.
• Provideeducationandtrainingstate-wideforallAreaHealthServicesand210hospitals.
• AppointpatientsafetymanagersineachoftheAreaHealthServices.
• Followupspecificeducationandsupportneedsfromacentralisedfaculty.
• Involvekeyclinicalgroupsinclinicalriskmanagementactivities.
ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
the implementation phaseThe implementation of SIP has involved many strategies,andresultedintheinstitutionalisationofanumberofnewconceptsandpoliciesintheNewSouthWaleshealthsystem.Theyaresummarisedasfollows:
1. Education and trainingOver 2,500 health care providers and consumers haveattendedtwoortwoandahalfdayeducationandtrainingsessions in safety improvement processes. This evidence-oriented program, [26-29] accompanied by resourcematerials,coveredthefollowing:
• Howtoidentifyhealthcareincidents;
• HowtoconductaRootCauseAnalysis(RCA)ofmajor incidents;
• HowtousetheincidentSeverityAssessmentCode(SAC);
• Howtorecogniseandminimisehumanfactorsin healthcare;and
• Howtodevelopandimplementrecommendationsand measureoutcomestoimprovehealthcaredelivery.
2. The Severity Assessment Code (SAC)TheSACisariskmatrixthatisappliedtoallnotifiedhealthcare incidents to ensure that appropriate action is taken.The incident is rated for both the severity of the outcomeandthelikelihoodthatitmightrecur.[25]Incidentsarethengivenanumericalratingfromonetofourwithonebeingthemost severe, and four the least. Stratification judgements
can be accomplished at two levels; the actual outcome,and the potential or worst case scenario for that incident.Thelatterprovidestheopportunitytomanageallincidentsand identify system vulnerabilities in order to prevent thenextseriousadverseevent,therebymaximisingthebenefitoftheSIP.TheapplicationoftheSACencourageshighriskincidentstobeacteduponimmediatelyandenableslowerrisk incidents to be aggregated into data sets for laterassessmentandmanagement.
3. The Reportable Incident Briefing System (RIBs)TheRIBsystemwasestablishedtofacilitatetheidentificationofseriousincidentsandthereportingofthesetotherelevantArea Health Service Chief Executives and NSW Health forappropriate management. A serious incident is defined asa Severity Assessment Code 1 incident and reportable totheDepartment.NationallytheAustralianCouncilforSafetyand Quality in Health care had developed a list of agreedsentinelevents.[30]However,usingtheSACrating,theRIBsystemhashighlightedadditionalseriousclinicaleventsthatwerepreviouslynotnotifiedorincludedinthenationallist.Thishasenabledfurtheranalysisofsuchincidentsandthedevelopmentofmorestate-widepoliciesforimprovement–forexamplestrategiestopreventwrongsite,wrongpatient,wrongprocedureincidents.
AsiaPacificJournalofHealthManagement2006;1:2 31

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
4. Root Cause Analysis (RCA)RootCauseAnalysiswasa relativelynewprocess formosthealthserviceswhenintroducedinthepilotphase.TheRCAprocesshassincebeenacceptedbymanycliniciansasawellstructured method for reviewing serious clinical incidentsandhascontributedtomanypreventativesolutionswhichhavebeenpromulgatedacrosstheentiresystem.
ThesystemicnatureoftheRCAprocessdemandsthatactionbetakenandaccountabilityforthatactionbeestablishedinpolicy,andheldbythechiefexecutive.
5. Centralised action and support for the NSW Safety Improvement Program Thedevelopment,implementationandsupportfortheSIPwereinstigatedbyNSWHealthandprovidedcollaborativelyby the Quality and Safety Branch in the NSW HealthDepartmentandtheformerInstituteforClinicalExcellence.Recognising the critical nature of this support, in 2004the Minister for Health expanded the role of the Institutefor Clinical Excellence and re-established it as the ClinicalExcellence Commission. The support of both agencieshas been seen as crucial for promoting uniformity inimplementation,supportforstate-widepolicydevelopment,and consistency of support for RCA teams, health servicemanagers and patient safety managers. A SIP steeringcommitteecomprisingarangeofstakeholdershasthetaskofoverseeingdevelopmentof theprogramandreviewinghowactionistaken.Abulletinalertingstafftosafetyevents,issues or risks (Safety Advocate) is published regularly byNSWHealthtoprovideevidencebased informationtothehealth system. Legislation has been enacted to providestatutoryprotectionformembersofRCAteamsandfortheworkingpapersassociatedwithRCAs.Thecausalstatementissuedbyeachteamishoweverapublicdocument.Therolesofbothagencieshavebeenclarifiedthroughthisandotherprocesses.NSWHealthisresponsibleforsafetyandqualitypolicy, implementation and outcomes, and the ClinicalExcellence Commission for ongoing support, training andassessmentofqualityandsafetyacrossthehealthsystem.
6. Human factors awarenessHumanfactorsawarenesstraininghasbeenintroducedforhealthcareproviderstoincreaselevelsofsensitivitytowardworkplaceprocesses,serioushealthcareincidentsandtheirinvestigation. This encourages a systems rather than anindividualblameapproachtoallincidents.
Ahumanfactorsperspectiverecognisesthereisacomplexsetofinter-relationshipsbetweenhumans,technologyandorganisational structures, with no perfect, fail-safe system.Ideally, recommendations about Severity AssessmentCode 1 incidents should include suggestions that aremost likely to prevent recurrence of the incident. Theseinclude forcing functions (recommendations that ensurea particular sequence will occur in specified order, suchaswhereautomatictellermachinesforceyoutotakeyourcredit card before dispensing cash).These can range fromhigh-endphysicalbarrierstotechnologicalforcing,suchasourautomatictellermachineexample,toprocessredesignrecommendations.
Errorisaprevailingfeatureofhumansystems.High-reliabilityindustries such as aviation and nuclear power generationhaverecognisedthatthe‘name,blame,shameandre-train’approach does little to prevent future errors. Instead, thesystemsapproachrecognisesanerringindividualissituatedin a complex web of inter-related, underlying social andorganisationalfactorswhichcontributetoerror.[31-33]
7. Patient Safety ManagersFundingforandappointmentofspecificallytrainedPatientSafetyManagersineachAreaHealthServiceisintegraltotheSIP.Thishashelpeddrawattentiontotheimportanceoftheprogram,providedtrainedresourcesforit,andestablishedacommitmentfromeachAreaHealthServicetotheongoingrequirementtoidentifyandtreattherisksinherentinhealthcare.
Allthiscomestogetherinanincidentmanagementprocesswhichhasbeenrefinedoverseveralyearsoftheprogram.Table2summarisesthekeystepsintheprocess.
32 AsiaPacificJournalofHealthManagement2006;1:2

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
MethodsWithin the context of this policy and systems reformwe conducted secondary analyses of available data.We examined the reportable incidents database andaggregated this information into monthly trend data forcomparative purposes. We broadly compared reportableincidents with data drawn from the previous reportingsystem,whichwasbasedonadhocreportingandtendedto be limited to corporate-type incidents and unexpecteddeaths. In addition, we analysed the main categories andnumbers of SAC 1 incidents and the causal factors of rootcauseanalysisdata.Themainactionstakeninresponsetothe safety improvement initiatives and the assessment ofSIP already undertaken by NSW Health were summarised.Statistical data were analysed using Microsoft Excel 2002versionSP3.
resultsInadditiontotheover2,500healthcarestaffandconsumersthat were trained in this education program, almost 1,000people have attended forums that have provided an
overviewoftheprogram.ParticipantshaveincludedhealthserviceBoardChairsandChiefExecutives,seniorclinicians,staff of the New South Wales Health Care ComplaintsCommission, and surveyors and staff from the AustralianCouncilonHealthcareStandards,thelargesthealthserviceaccreditationproviderinAustralia.
One way in which progress with this program can bemeasuredisbytheincreaseinthenumberofincidentsthatarenotifiedandthenactedupon.Inthefirst12monthsofreportingviatheRIBprocess,over1,600reportableincidentshave been received. Compared to the previous reportingsystem, this represents a 30% increase in the reporting ofincidents related to clinical management. Following thissteep jump, reporting has continued to rise progressively.Figure 1 shows the monthly trends in reporting of SAC1 notifications, expressed as a rate per 10,000 inpatientseparations, between May 2003 and May 2005. The datashow that an initial jump in reporting has largely beensustained.
Table 2: Key steps in the incident management process of the NSW Safety Improvement Program, May 2003 to May 2005
• Anincidentisidentifiedandreportedtoamanager.
• Themanagerusesapurpose-designedSeverityAssessmentCode(SAC)matrixtoprioritisetheincident.
• Allseriousincidents,ieSAC1and2,arereportedtotheAreaChiefExecutive.
• ASAC1incidentmustbereportedtotheNSWDepartmentofHealthwithin24hoursandaRootCauseAnalysis (RCA)orequivalentreviewoftheincidentcommencedwithin10days.
• OtherincidentsmaybereportedtotheNSWDepartmentofHealthatthediscretionoftheChiefExecutive, includingthoseattractingexternalattention.
• AreportoftheresultsoftheRCAistobeforwardedtotheNSWDepartmentofHealthwithin65days ofnotificationoftheincident.
• Analysisofincidentsandidentificationofopportunitiesforimprovementareundertakenatunit,facility, areaandstatelevels.
• ThesereportsandrecommendationsareanalysedandmanagedbytheDepartmentofHealthatthestatelevel forpossiblepolicydevelopment,andarefedbacktothesystemaslessonslearnedsoastoavoidsimilarincidents occurringinotherAreaHealthServices.
• Allincidents,includingSAC3and4,areaggregatedandreviewedregularlybytheClinicalExcellenceCommission sothatappropriateactioncanbetakentoimprovethesystemandreducetherecurrenceofcommonincidents.
Furtherinformation:http://www.health.nsw.gov.au/policies/PD/2006/PD2006_030.html
AsiaPacificJournalofHealthManagement2006;1:2 33

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
PriortoSIP,excludingreportsrelatedtosuspectedsuicides,only 5% of incident reports were about clinical care. In2004,excludingsuicides,35%ofreportsreceivedrelatedtoclinical incidents.Figure2exhibits fourmaincategoriesofSAC1incidentsreceivedfromMay2003.Theseare:clinicalmanagement,suspectedsuicide,organisational issuesandassault and security matters. Although these particularcategoriesdonotshowanincrease,overall,therearerisingreporting levels, as Figure 1 shows. Clinical managementincidents are made up of all clinical incident categories(eg falls, medication errors, wrong site surgery, and issuesrelatedtoclinicalcare).
Figure 1: Severity Assessment Code 1, reportable incident briefs per 10,000 patient admissions, New South Wales Safety Improvement Program, May 2003 to May 2005
Whilst the numbers were slightly less in the second yearfor clinical management, there was a definite reduction insome areas (eg wrong site surgery) whilst other incidentsremained stable.The suspected suicide data in 2003/2004related to suspected suicides in the community that wereknowntothementalhealthservice.Thedefinitionforthiscategorychangedin2005tobemorespecifictoincludeonlynotificationswheretherehadbeencontactwiththementalhealthservicewithinthelastsevendays.Thefluctuationsinbothcategoriesarenotstatisticallysignificantandcontinuetoremainwithincontrolin2006.
Figure 2: Main categories and number of Severity Assessment Code 1 Incidents, New South Wales Safety Improvement Program, May 2003 to May 2005
NU
MBE
R O
F RI
BS P
ER 1
0,00
0 A
DM
ISSI
ON
S
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0MAY 2003 MONTHS MAY 2005
400
350
300
250
200
150
100
50
0 Clinical Management Suspected Suicide Organisational Management Assault and Security
2003-04
2004-05
34 AsiaPacificJournalofHealthManagement2006;1:2

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
Of the total RIBs received, over 1100 (37%) are SAC 1incidents and over 40% of these have had RCAs orequivalentreviewscompleted.Analysisofthemajorcausaland contributing factors of RCAs show that these includehumanfactorsofvariouskinds,patientfactors,equipment,policy,proceduresandguidelines,andsafetymechanisms.ThemaincategoriesareshowninFigure3.
In January 2005, the NSW Minister for Health released thefirstreportonadverseeventsinNSW.[34]Thisreportfocuseson SAC 1 events and was the first of an annual reportingprogram.[35]
FollowingtheanalysisoftheRIBsandtheRCAsarangeofsystem-wideimprovementshavebeeninitiated.Thesehave
involvedthedevelopmentofnewandtherevisionofout-of-datepoliciesandprocedures,theprovisionofalertstothesystem,thepublicationofSafetyAdvocatesonspecifichighriskissues,liaisonwithmanufacturersregardingequipmentdesignandtheirimprovementandthedraftdevelopmentofstate-widereportingmechanisms.Table3providesexamplesofsomeimportantactionstakentodate.
Inadditiontotheabove, followupevaluationvisitstotheArea Health Services have been undertaken to assess theoveralluptakeoftheprogram,theissuesidentifiedandhowstaffareprogressingwithit.Thesefeedbackandevaluationprocesseshavehighlightedvariousprogramstrengthsandweaknesses(Table4).
Figure 3: Number and percentage, causal factors identified in Root Cause Analyses, of New South Wales Safety Improvement Program, May 2003 to May 2005
Table 3: Examples of safety improvement actions, NSW Safety Improvement Program, May 2003 to May 2005
• SafetyAlerts-anationalalertregardingtheuseandmanagementofPotassiumChloridewithinthehealthsystem.
• SafetyAdvocatesonmedicationandintravenoussafety,bedrailsafety,breastfeedingandthestorage ofbreastmilk,fallspreventionandtheuseofhighpressureinfusionpumps.
• Equipmentadviceincludingself-inflatingresuscitationbags,staplegunsandretainedsurgicalinstruments.
• Discussionswithmanufacturers-rapidinfusersandthedesignofvisceralretractorsusedinabdominalsurgery.
• Policydevelopment-onaccountableitems,correctpatient,correctprocedureandcorrectsite.
Policies/ProceduresGuidelines,247,22%
Equipment,53,5%
PatientFactors,87,8%
HumanFactors–WorkEnvironment/Scheduling,
160,14%
HumanFactors–Knowledge/Skills/Competence,167,15%
HumanFactors–WrittenCommunications,151,14%
HumanFactors–VerbalCommunications,132,12%
SafetyMechanisms,114,10%
AsiaPacificJournalofHealthManagement2006;1:2 35
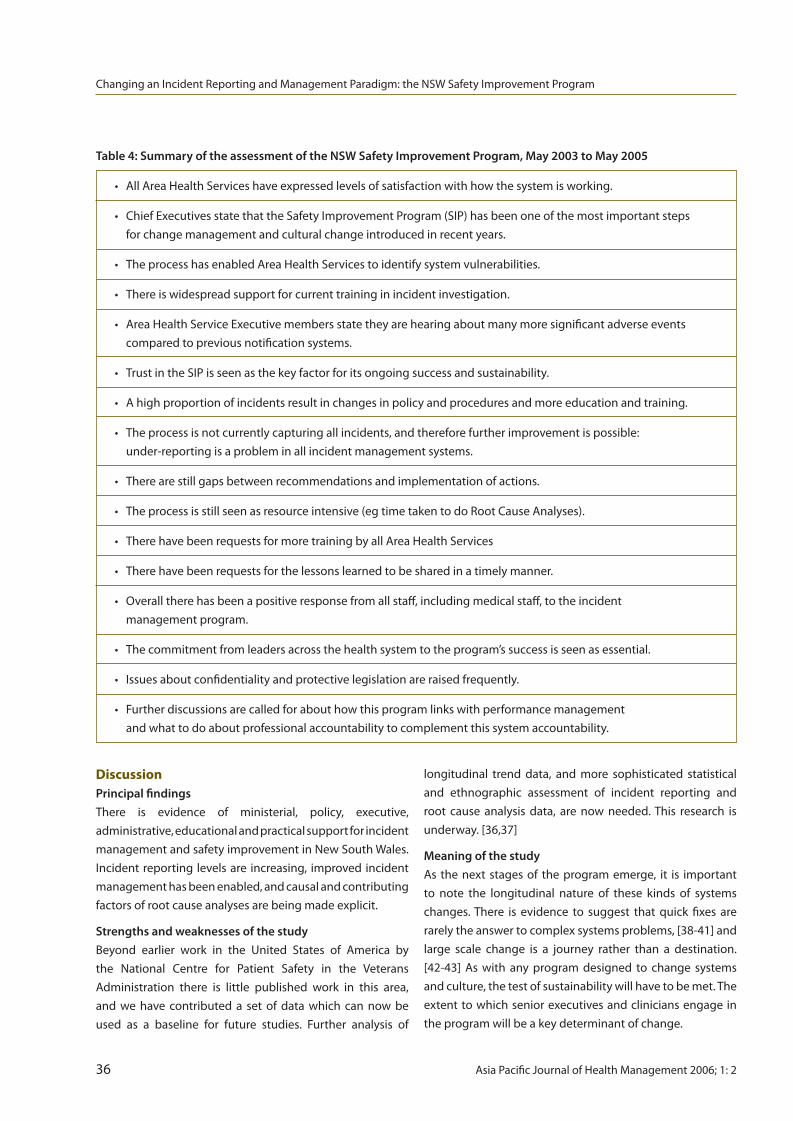
discussionPrincipal findingsThere is evidence of ministerial, policy, executive,administrative,educationalandpracticalsupportforincidentmanagementandsafetyimprovementinNewSouthWales.Incidentreportinglevelsare increasing, improvedincidentmanagementhasbeenenabled,andcausalandcontributingfactorsofrootcauseanalysesarebeingmadeexplicit.
Strengths and weaknesses of the studyBeyond earlier work in the United States of America bythe National Centre for Patient Safety in the VeteransAdministration there is little published work in this area,and we have contributed a set of data which can now beused as a baseline for future studies. Further analysis of
Table 4: Summary of the assessment of the NSW Safety Improvement Program, May 2003 to May 2005
• AllAreaHealthServiceshaveexpressedlevelsofsatisfactionwithhowthesystemisworking.
• ChiefExecutivesstatethattheSafetyImprovementProgram(SIP)hasbeenoneofthemostimportantsteps forchangemanagementandculturalchangeintroducedinrecentyears.
• TheprocesshasenabledAreaHealthServicestoidentifysystemvulnerabilities.
• Thereiswidespreadsupportforcurrenttraininginincidentinvestigation.
• AreaHealthServiceExecutivemembersstatetheyarehearingaboutmanymoresignificantadverseevents comparedtopreviousnotificationsystems.
• TrustintheSIPisseenasthekeyfactorforitsongoingsuccessandsustainability.
• Ahighproportionofincidentsresultinchangesinpolicyandproceduresandmoreeducationandtraining.
• Theprocessisnotcurrentlycapturingallincidents,andthereforefurtherimprovementispossible: under-reportingisaprobleminallincidentmanagementsystems.
• Therearestillgapsbetweenrecommendationsandimplementationofactions.
• Theprocessisstillseenasresourceintensive(egtimetakentodoRootCauseAnalyses).
• TherehavebeenrequestsformoretrainingbyallAreaHealthServices
• Therehavebeenrequestsforthelessonslearnedtobesharedinatimelymanner.
• Overalltherehasbeenapositiveresponsefromallstaff,includingmedicalstaff,totheincident managementprogram.
• Thecommitmentfromleadersacrossthehealthsystemtotheprogram’ssuccessisseenasessential.
• Issuesaboutconfidentialityandprotectivelegislationareraisedfrequently.
• Furtherdiscussionsarecalledforabouthowthisprogramlinkswithperformancemanagement andwhattodoaboutprofessionalaccountabilitytocomplementthissystemaccountability.
longitudinal trend data, and more sophisticated statisticaland ethnographic assessment of incident reporting androot cause analysis data, are now needed.This research isunderway.[36,37]
Meaning of the studyAs thenextstagesof theprogramemerge, it is importantto note the longitudinal nature of these kinds of systemschanges.There is evidence to suggest that quick fixes arerarelytheanswertocomplexsystemsproblems,[38-41]andlarge scale change is a journey rather than a destination.[42-43] As with any program designed to change systemsandculture,thetestofsustainabilitywillhavetobemet.Theextenttowhichseniorexecutivesandcliniciansengageintheprogramwillbeakeydeterminantofchange.
ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
36 AsiaPacificJournalofHealthManagement2006;1:2

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
Theearlydatasuggest that reporting levelsare increasingparticularlyinclinicallyrelatedincidents,andclearprocessesarenowavailableforsystem-wideincidentnotificationandmanagement. The program has attempted to anticipatefuturerequirementsforsustainabilityby institutinga‘trainthe trainer’ program to ensure that the expertise for RCAsandRCAtrainingisconsistentandlocallyavailable.Includingmoreclinicians,especiallydoctors,intheprogramwilllikelybeakeysuccessfactor.Theimplicationsforhealthservicesmanagersarethatreportingisnowafactoflife,andincidentreportingdataandinformationfromRCAswillincreasinglygovernmanagerialaswellasclinicalreformagendas.
Unanswered questions and future researchA determinant of future program success is the allocationofadequateresources.TheNewSouthWalesGovernmenthasmadeprovisionfor$60millionfortheNSWSafetyandClinicalQualityProgramoverthenextfiveyears.Thisisamorecomprehensiveapproachtopatientsafety involvingmanyinitiatives to strengthen accountability for safety and howsafetyissuesareled,managed,reportedandactioned.ThisbroaderprogramwillthusexpandandbuildontheplatformestablishedbyNSWSafetyImprovementProgram.Thekeyobjectivesaretoprovidesafercare,bolsterconfidenceandtrustinthehealthsystemandtodesignimprovedmodelsforthedeliveryofcare.Patientsneedtocontinuetoreceivethehighestqualityofcareknowingthatappropriatestructuresareinplacetomonitorandmanageissuesastheyarise.
Future investigators need to start to address safetyimprovementissuesinmoredetail.Furtherassessmentsofincidentreportinglevels,incidenttrenddataandRCAsandtheirconsequencesarewarranted.
conclusionTheSafetyImprovementProgramhasbeeninitiatedinNewSouthWales, and its development is encouraging. Furtherformativeevaluationofitsprogressisanticipatedovertime.
acknowledgementsTheNSWSafetyImprovementProgramwouldnothavebeenpossiblewithoutthesupportofourfriendandcolleagueDrIan O’Rourke, the inaugural Chief Executive Officer of theInstituteforClinicalExcellence[nowtheClinicalExcellenceCommission],whotragicallypassedawayon16August2004.ColleaguesthroughouttheNewSouthWaleshealthsystem,not only in NSW Health and the NSW Clinical ExcellenceCommission,butalsoinAreaHealthServicesandfacilities,supportedtheseinitiativesandourwork.Wearegratefultothemfortheirmanycontributions.
competing interestsTheauthorsdeclarethattheyhavenocompetinginterests.
references1. BakerGR,NortonPG,FlintoftV,BlaisR,BrownA,CoxJ,etal. TheCanadianadverseeventsstudy:theincidenceofadverse eventsamonghospitalpatientsinCanada.CanMedAssocJ2004; 170(11):1678-1686.
2. BrennanTA,LeapeLL,LairdNM,HebertL,LocalioAR,LawthersAG, NewhouseJP,WeilerPC,HiattHHetal.Incidenceofadverseevents andnegligenceinhospitalisedpatients.ResultsoftheHarvard MedicalPracticeStudyI.NEnglJMed1991;324(6):370-376.
3. DavisP,Lay-YeeR,BriantR,AliW,ScottA,SchugS.Adverseevents inNewZealandpublichospitals:occurrenceandimpact.NZMed J2002;115(1167):271.
4. WilsonRM,RuncimanWB,GibberdRW,HarrisonBT,NewbyL, HamiltonJD.TheQualityinAustralianHealthCarestudy.MedJAust 1995;163(9):458-471.
5. DepartmentofHealth.ReportintoPublicInquiryintoChildren’s HeartSurgeryattheBristolRoyalInfirmary1984-1995:learningfrom Bristol.TheBristolRoyalInfirmaryInquiry.London:TheStationary Office,2001.
6. DouglasN,RobinsonJ,FahyK.Inquiryintoobstetricand gynaecologicalservicesatKingEdwardMemorialHospital1990-2000. Perth:GovernmentofWesternAustralia,2001.
7. HealthandDisabilityCommissioner.SouthlandDistrictHealth Boardmentalhealthservices.Auckland:HealthandDisability Commissioner,2001.
8. SinclairCM.ReportoftheManitobapediatriccardiacsurgeryinquest. Winnipeg:ManitobaProvincialCourt,1994.
9. NSWHealthDepartment.Annualreport2003-2004.NorthSydney: NSWHealth,2004.
10. AustralianInstituteofHealthandWelfare.Australia’shealth.Canberra: AustralianInstituteofHealthandWelfare(AIHW),2004.
11. IsouardG,MessumD,BriggsD,McAlpinS,HansonS.Improving organisationalperformanceinhealthcare.In:HarrisMandAssociates. Managinghealthservices:conceptsandpractice.2nded.Sydney: MosbyElsevier;2006.
12. BlandfordJ,SmythT.Fromriskmanagementtoclinicalgovernance. In:HarrisMandAssociates.Managinghealthservices:concepts andpractice.2nded.Sydney:MosbyElsevier;2006.
13. CruickshankM,IsouardG,IrwinL,MadisonJ,ChandlerM.Managing quality.In:HarrisMandAssociates.Managinghealthservices: conceptsandpractice.2nded.Sydney:MosbyElsevier;2006.
14. CarrollJ,RudolphJ,HatekenakaS.Lessonslearnedfromnon-medical industries:rootcauseanalysisasaculturalchangeatachemical plant.QualSafHealthCare2002;11(3):266-9.
15. BattyL,Holland-ElliottK,RosenfeldD.Investigationofeyesplash andneedlestickincidentsfromanHIVpositivedonorinanintensive careunitusingrootcauseanalysis.OccupMed2003;53(2):147-50.
16.GosbeeJ.Humanfactorsengineeringandpatientsafety. QualSafHealthCare2002;11(4):352-4.
17. BoyerMM.Rootcauseanalysisinperinatalcare:healthcare professionalscreatingsaferhealthcaresystems.JPerinatNeonatal Nurs2000;15(1):24-5.18. AustralianCouncilforSafetyandQualityinHealthCare.Safetyin practice:makinghealthcaresafer.SecondreporttotheAustralian HealthMinisters’Conference.Canberra:AustralianCouncilforSafety andQualityinHealthCare,2001.
AsiaPacificJournalofHealthManagement2006;1:2 37

ChanginganIncidentReportingandManagementParadigm:theNSWSafetyImprovementProgram
19. RuncimanWB,EdmondsMJ,PradhanM.Settingprioritiesforpatient safety.QualSafHealthCare2002;11:224-249.
20. RuncimanWB.LessonsfromtheAustralianPatientSafetyFoundation: settingupanationalpatientsafetysurveillancesystem–isthisthe rightmodel?QualSafHealthCare2002;11:246-51.
21. RuncimanWB.Editorial:incidentsandaccidentsinhealthcare: it’stime!JQualClinPract1999;19:1-2.
22. RuncimanWB.LessonsfromAustralia.In:EmslieS,KnoxK, PickstoneT,editors.Improvingpatientsafety:insightsfromAmerican, AustralianandBritishhealthcare.Welwyn:ECRI;2002.
23. WestbrookM,BraithwaiteJ,TravagliaJ,LongD,JormC,IedemaR. Promotingsafety:variedreactionsofdoctors,nursesandallied healthprofessionalstoasafetyimprovementprogram.IntJHealth CareQualAssurInpress.
24. BagianJ,GosbeeJ.DevelopingacultureofpatientsafetyattheVA. AmbulOutreach2000;Spring:25-29.
25. BagianJ,GosbeeJ,DeRosierJ,StalhandskeE,EldridgeN,Williams, etal.Developinganddeployingapatientsafetyprograminalarge healthcaredeliverysystem:youcan’tfixwhatyoudon’tknowabout. JtCommJQualImprov2001;27(10):522-32.
26. BagianJ,GosbeeJ,LeeC,WilliamsL,McKnightS,MannosD. TheVeteransAffairsrootcauseanalysissysteminaction.JtComm JQualImprov2002;28(10):531-45.
27. RadtkeK.JointCommissiononHealthcareOrganisationssolutions: gettotherootofsentineleventsinvolvinginfectioncontrol.Nurs Manage2004;35(6):18-22.
28. KaplanH,FastmanB.Organisationofeventreportingdatafor sensemakingandsystemimprovement.QualSafeHealthCare 2003;12:1168.
29. GosbeeJ,AndersonT.Humanfactorsengineeringdesign demonstrationscanenlightenyourRCAteam.QualSafHealth Care2003;12:119-21.
30. AustralianCouncilforSafetyandQualityinHealthCare(ACSQHC). Patientsafety:towardsustainableimprovement.Fourthreport totheAustralianHealthMinisters’Conference.Canberra:ACSQHC, 2003.
31. BraithwaiteJ.Hunter-gathererhumannatureandhealthsystem safety:anevolutionarycleftstick?IntJQualHealthCare2005;17(6): 541-545.
32. BraithwaiteJ,TravagliaJ,MallockN,IedemaR,WestbrookM,LongD, etal.EvaluationofthepatientsafetyprograminNewSouthWales: overviewofstudies.Sydney:CentreforClinicalGovernanceResearch, UniversityofNewSouthWales,2005:38.
33. HindleD,BraithwaiteJ,IedemaR.Patientsafetyresearch:areview oftheliterature.Sydney:CentreforClinicalGovernanceResearch inHealth,UNSW,2005.
34. NSWHealth.PatientSafetyandClinicalQualityProgram.Firstreport onincidentmanagementintheNSWpublichealthsystem2003-2004. NorthSydney:NSWDepartmentofHealth,2005.
35. NSWHealth.PatientSafetyandClinicalQualityProgram.Second reportonincidentmanagementintheNSWpublichealthsystem 2004-2005.NorthSydney:NSWDepartmentofHealth,2005.
36. IedemaR,JormCM,BraithwaiteJ,TravagliaJ,LumM.Arootcause analysis:confrontingthedisjunctionbetweenformalrulesand situatedclinicalactivity.SocSciMed2006;63(5):1201-1212.
37. IedemaR,JormC,LongD,BraithwaiteJ,TravagliaJ,WestbrookMT. Turningthemedicalgazeinuponitself:rootcauseanalysisand theinvestigationofclinicalerror.SocSciMed200662(7):1605-1615.
38. HindleD,BraithwaiteJ.Softsystemsmethodology:aguidefor Australianhealthprofessionals.Sydney:CentreforClinical Governance,UNSW,2001.
39. BraithwaiteJ,HindleD,IedemaR,WestbrookJ.Introducingsoft systemsmethodologyplus(SSM+):whyweneeditandwhatitcan contribute.AustHealthRev2002;25(2):191-198.
40. KohnL,CorriganJ,DonaldonM,editors.Toerrishuman:building asaferhealthsystem.Washington,D.C.:NationalAcademyPress, 1999.
41. BraithwaiteJ.Organisationalchange,patient-focusedcare:an Australianperspective.HealthServManageRes1995;8(3):172-185.
42. Sanson-FisherRW.Diffusionofinnovationtheoryforclinicalchange. MedJAust2004;180(Suppl):S55-S56.
43. BraithwaiteJ,GoulstonK.Turningthehealthsystem90ºdownunder. Lancet2004;364(9432):397-399.
38 AsiaPacificJournalofHealthManagement2006;1:2
introductionThis research note seeks to inform readers of a study toevaluatetheeffectsoftheimplementationoftheAustralianBusiness Excellence Framework (ABEF) on organisationalperformanceinastate-wideambulanceservice.Ambulanceservices are part of the continuum of patient care yet theuse of Continuous Quality Improvement (CQI) processesin ambulance services is relatively novel. The QueenslandAmbulanceService(QAS)begantoapplybusinessprocessimprovementusingtheABEFin1997.TheABEF(Figure1)is a world class CQI model [1] which enables a structuredapproach to the re-engineering of business processes toachieveimprovedoutcomes.
abstract:Objective: This article seeks to: • raise interest in the use of quality improvement techniques in pre-hospital care;
• introduce a new continuous quality improvement (CQI) conceptual model; and
• report preliminary results of a study to evaluate the effect of a CQI intervention on patient care and organisational outcomes.
Design: The study is part of a doctoral program. The design is longitudinal with the collection of qualitative and quantitative data supported by a review of the literature and involving interviews with those involvedin the change process. It also involves the development of a CQI conceptual model for use by ambulance services.
Setting: The use of the Australian Business Excellence Framework (ABEF) by Queensland Ambulance Service (QAS) as a CQI model.
Main outcome measures: These include: • Queensland government-required key performance measures for a government agency; and
russell J linwoodASM,AFCHSEPrincipalStrategyOfficer,BusinessExcellenceDepartmentofEmergencyServicesBrisbane,Queensland,Australia.
Correspondence:[email protected]
r E S E a r c Hn o t E
the impact of a continuous Quality improvement approach on Patient care in the ambulance Environment rJ linwood
• perceptions of key informants collected over a period of time to determine the degree to which any improvements in performance measures are attributable to the use of the ABEF.
Results: As the research is still in progress, definitive results are not yet to hand. Preliminary analysis of operational performance data between 1 July 1997 and 31 December 2005 and the receipt of three Australian Business Excellence Awards by QAS suggest that use of the ABEF has had a positive effect on patient care and organisational outcomes.
Conclusions: Our preliminary findings suggest that use of a CQI model by an ambulance service has a positive effect on patient and organisational outcomes.
Abbreviations:ABEF-AustralianBusinessExcellenceFramework;CQI-ContinuousQualityImprovement;KPIs-KeyPerformanceIndicators;QAS-QueenslandAmbulanceService
Key words:Ambulance,ABEF,ContinuousQualityImprovement,PatientCare
AsiaPacificJournalofHealthManagement2006;1:2 39

leadership
customer & Market Focus
Strategy & Planning
People
Success & Sustainability
innovation,Quality & improvement
Knowledge & Information
Source:StandardsAustraliaInternationalGlobalLtd(SAIG).TheAustralianBusinessExcellenceFrameworkhandbook2004.Sydney:SAIG;2004,p.5.
Figure 1: The Australian Business Excellence Framework (ABEF)
TheImpactofaContinuousQualityImprovementApproachonPatientCareintheAmbulanceEnvironment
ThisstudyexaminestheimpactoftheapplicationofaspecificCQImethodologyontotalorganisationalperformanceinthepre-hospital(ambulance)environment.Thespecificaimsofthestudyinclude:
• todetermineifasystematicapproachtoCQIbyambulance servicescanleadtoimprovedpatientoutcomes.
• tocomparetheperformanceofanambulanceservice thatusessuchanapproachwithonethatdoesnot.
• toinformambulancemanagementinregardtothe selectionandapplicationofapossibleCQImodel.
TheliteraturerelevanttoCQIinhealthcareismostlyrelatedto hospital-based care, with clinically-focused articles oflimited application to the ambulance environment. [2,3]Mostpapersdealwithimprovementsinspecificepisodesofmedical care occurring in hospital or health care facilities,[4]andareof limitedpracticalvaluetoambulanceswhereenvironmental conditions for patient care, and especiallythe duration, are fundamentally different to an operatingtheatreornursingward.[5]
ThusthereisapaucityofliteraturepertainingtoCQIintheambulance,orpre-hospital,environment.Thisisremarkablegiventhelonghistoryofambulancecare,[6]anobservationreflectedbothlocallyandoverseas.[7,8]QAShasamissionto minimise pain or suffering through rapid, effectivetreatmentandtransportofthepatienttoaplaceofdefinitivecare.Ambulanceservicesmakeasignificantcontributiontohealth care, yet there is little discussion about CQI and itspotentialimpactonpatientoutcomes.[9]Tooffsetthis,thereisagrowingattempttoidentifyandpublishbenchmarkingdata.[10]
ThereisalsoarobustrangeofEmergencyMedicalServices(EMS) articles, predominantly from North America, whichconcentrate on clinical matters and occasionally addressCQI.[11]
Fortunately a growing body of CQI literature is evidentin other fields, notably business and manufacturing. [12]CQI is becoming increasingly applied in the health sectorand this is starting to be reflected in the literature. Thesituationimprovesinternationally,buteventhenmostdataon ambulance appear in EMS or fire journals where mostarticles are case-specific. [13,14] More advanced analysisof organisational improvements through greater use ofmeasurementisneeded.[15]
TherearefewpapersthatappeartoevaluatetheimpactofCQI programs on organisational performance outcomes.Study design can affect the degree of validity of suchresearch, especially when evaluating interventions aimedat improving the quality of care. Bizovic et al (2002)suggest possible solutions to the problems associatedwithsuchstudies.[2]TherearetwoclearapproachestotheimplementationofCQI:
• aretrospectiveapproachthatseekstofinderrorsin patientcareandthenchangepracticeinasafeand sensiblemannerusinga“learnbutlaynoblame” approach;and
• aproactiveapproachwhichseekstoimproveservices asaresultofasystematicandco-operativeapproach tocontinuousimprovement.
Pelowitz(2003)notesthatuseofcontinuousqualityimprovementasembodiedintheABEFconcentratesonthesecond,withlearningderivedfromthefirst.[16]
MethodsThestudyisanaturalexperiment,primarilyusingaqualitativeresearch methodology. It involves three sequential, inter-relatingprojects:
1. Adescriptivepolicyanalysisofthepre-1997periodand anexaminationofkeyareasofinquirypertainingtothe qualityofpatientcare.
2. Adescriptiveevaluationofwhatoccurredintheperiod 1997-2006withtheintroductionofCQI.
3. Synthesisofoutcomemeasures,processesandresults ofthefirsttwoprojectsbyexaminingthedegreetowhich useofCQIwassuccessful.
The QAS introduced the ABEF in 1997 in a large-scaleorganisationalinterventiontoachieveCQI.
40 AsiaPacificJournalofHealthManagement2006;1:2

TheImpactofaContinuousQualityImprovementApproachonPatientCareintheAmbulanceEnvironment
Since that time the QAS has collected specific data fromorganisational assessments [16] as well as extensiveperformancedata(egoutofhospitalcardiacarrestsurvivalrates,patientsatisfaction),whicharereportedpubliclyonaregularbasis.[18]Theprimarysourcesofdataforthisprojectinclude:• QuantitativedataonQASperformance(examplesofwhich appearinFigures3-7).QASperformancedatagathering hasbeenongoingforyearstoinformQASdecision-making andtomeetQueenslandandAustraliangovernmentand industrybodyreportingobligations(seeDepartmentof EmergencyServices,[18]theFederalReportonGovernment Services[19]andtheConventionofAmbulance Authorities[10]).
• Qualitativedataarisingfrominterviewswithkey organisationalstakeholderstomeasurethechange attributabletotheintroductionoftheABEF.Anexample interviewquestionis:“Pleasedescribethedegreetowhich youbelievethatpatientoutcomeshavechangedas aresultofapplyingtheABEF”.Discourseanalysiswillbe usedtoanalyseandinterpretthedataarisingfromthese interviews.
Supportingdatahasalsobeenderivedfromepisodicsurveysconducted on behalf of QAS including the QueenslandHouseholder Survey, and patient, staff and stakeholdersatisfactionsurveys.
Access to the data was provided by QAS with full supportfor the project. Interviews with key informants are nowunderway.
Queensland University of Technology Research EthicsCommitteeclearancewasgainedpriortothefieldresearch.
conceptual frameworkAn outcome of this study includes the development ofa theoretical model of the key determinants of patientoutcomes,formingtheconceptualunderpinningsofaCQIapproach for ambulance services (Figure 2).This model isanadaptationoftheABEF,andtakesontheessentialtenetsof that model, adapted to the ambulance environment.As indicated in Figure 2, inputs (eg people, competencies,leadership) lead to the generation of products, processesandservicesandtheseresultin‘outputs’,whichinthecaseofanambulanceservice,isbetterpatientoutcomes.WheretheABEFisagenericqualitymodel,thisproposedmodificationis expected to be more readily related to by ambulancepractitioners.Asanalysisofthedataunfolds,thismodelmayundergofurthermodificationbeforetheendofthestudy.
FindingsThe QAS uses a balanced scorecard approach toorganisationalperformanceevaluation.ThefollowingdatareflectsperformanceinkeyareasovertheperiodtheABEFhasbeenused(iefromOctober1997toDecember2005).
Figure3demonstratesthegrowingdemandforambulanceresponse between 2000/01 and 2004/05. The growth indemandhasmostlybeeninurgentratherthannon-urgentresponses. The rapid growth in demand has placed greatstrainonthecapacityoftheQAStomatchthisgrowthwithadditionalresources.
Source:ConceptualframeworkdevelopedbytheauthorusingconceptsderivedfromtheABEF.
ss
s
s
s
ss
leadership
People
clinical competencies
logistic Support
ProductsProcesses& Services
BetterQualityHealth
outcomes
outputs
Contin
uousQ
ual
ity
Impro
vement Data, Inform
ation
&Know
ledge
ss
s
s
inputss
s
Patient/MarketFocus
s
technical Support
Figure 2: A CQI Model for improving ambulance care and total organisational performance
Figure 3. Number of cases (urgent on the left and non -urgent on the right) responded to by QAS between 2000/01 and 2004/05 financial years
500
400
300
200
100
0
THO
USA
ND
S O
F PA
TIEN
TS
00/01 01/02 02/03 03/04 04/05
Source:DataextractedfromQueenslandDepartmentofEmergencyServicesperformancedata
AsiaPacificJournalofHealthManagement2006;1:2 41

TheImpactofaContinuousQualityImprovementApproachonPatientCareintheAmbulanceEnvironment
ResponsetimesoutlinedinFigure4indicateadropduring2001/02 and 2002/03 followed by an increase in 2004/05.Duringthistimeadditional resourcesweremadeavailableand improvements occurred in the distribution of theseresources.Figure5demonstratesthepercentageofpatientsresuscitatedandhandedovertohospitalsaliveafteroutofhospitalcardiacarrestbetween2000/01and2004/05.
Improvementinpatientsatisfactionduringthestudyperiodis reflected in the data gathered annually by QAS using astandardsurveytool(Figure6).
80
70
60
50
PERC
ENTA
GE
00/01 01/02 02/03 03/04 04/05
Figure 4. Percentage of urgent cases responded to by QAS between 2000/01 and 2004/05 financial years
Source:DataextractedfromQueenslandDepartmentofEmergencyServicesperformancedata
25
20
15
10
5
0
PERC
ENTA
GE
00/01 01/02 02/03 03/04 04/05
Figure 5. Percentage of out of hospital cardiac arrest survival rates achieved by QAS between 2000/01 and 2004/05 financial years
Source:DataextractedfromQueenslandDepartmentofEmergencyServicesperformancedata
First aid training is a major and complementary elementof the suite of QAS core services. Figure 7 refers to theproactiveoutputofcustomerstrainedinfirstaid.Outcomesofsuchactivityare impossibletomeasurecompletely,butitisknownthatpatientswhobenefitfromfirstaidpriortoarrivalofQASaremorelikelytoexperiencelowermorbidityandmortality.
100
98
96
94
92
90
88
PERC
ENTA
GE
00/01 01/02 02/03 03/04 04/05
Figure 6. Percentage of patients satisfied with QAS between 2000/01 and 2004/05 financial years
Source:DataextractedfromQueenslandDepartmentofEmergencyServicesperformancedata
80
70
60
50
40
30
20
10
0
THO
USA
ND
S
00/01 01/02 02/03 03/04 04/05
Figure 7. Number of community education certificates issued by QAS between 2000/01 and 2004/05 financial years
Source:DataextractedfromQueenslandDepartmentofEmergencyServicesperformancedata
42 AsiaPacificJournalofHealthManagement2006;1:2
discussionMy preliminary findings suggest that interventions arisingfromtheintroductionofCQIinQASthroughtheapplicationof the ABEF have resulted in improved patient outcomes.These findings are supported by the fact that, in 2005,QASreceiveda thirdAustralianBusinessExcellenceAwardsince the commencement of the program in 1997. Theaward recognised improvement in QAS organisationalperformance,includingpatientcare.
The degree to which the positive findings arising fromthe quantitative data reported in this study are directlyattributabletouseoftheABEFisnotpossibletodetermineat this stage. Qualitative evidence from key informants,togetherwithcomparisonswithsimilardatafromambulanceservices in other states will form an important part of thestudy.
ThereviewoftheCQIliteratureindicatedaconcentrationonthehospitalsectorwithveryfewarticlesdirectlyapplicableto ambulance services. Furthermore, while the body ofliterature that addresses patient care in the ambulanceenvironment is growing, most of this literature does notdirectlyaddresstheimpactofCQIintheAustraliancontext.Thisstudywillhelpfillthisgapintheliterature.
conclusionAnimportantcontributionofthisstudyisthedevelopmentandevaluationofanovelCQImodel for theQASwiththepossibilityof itbeingappliedtootherambulanceservicesandnon-hospitalhealthservices,suchasalliedhealthcareorganisations.Finaloutcomesofthisevaluationarenotdueuntil2007,sodefinitiveconclusionsmaynotyetbedrawnastotheeffectofthemodelonpatientcareandorganisationaloutcomes.Resultstodate,suggestthattheintroductionofthe ABEF in the ambulance environment makes a positivedifferencetopatientcareoutcomes.
acknowledgementsIwishtothankmydoctoralsupervisors,DrBrianOldenburg(QUT), Dr Gerry FitzGerald (QUT) and Dr Gary Day (QUT).Thanks are also extended to the Commissioner and theinspirational men and women of QAS, whose outstandingworkinspiredthisstudy.
Thisstudyisself-funded.
competing interestsTheauthordeclaresthathehasnocompetinginterests.
references1 StandardsAustraliaInternationalGlobalLtd(SAIG).TheAustralian BusinessExcellenceFrameworkhandbook2004.Sydney:SAIG; 2004;p.5.
2 BizovicKE,WearsR,LoweRA.Researchingqualityinemergency medicine.AcademyofEmergencyMedicine.2002;9(11):1116-1123.
3 Ricard-HibonA,ChollettC,SaadaS,LoridantB,MartyJ.AQuality controlprogramforacutepainmanagementinout-of-hospital criticalcaremedicine.AnnEmergMed.1999;34(6):738-743.
4 McCrackenMJ,McIlwainTF,FottlerMD.Measuringorganisational performanceinthehospitalindustry:anexploratorycomparison ofobjectiveandsubjectivemethods.HealthServManageRes. 2001;14:211-219.
5 IsouardG.Aqualitymanagementinterventiontoimproveclinical laboratoryuseinacutemyocardialinfarction.MedJAust.1999; 170(1):11-14.
6 QueenslandAmbulanceService(QAS).Tenyearreview.Brisbane: QAS;2001.
7 AmbulanceServiceofNewSouthWales(ASNSW).Bestagain–2002 –2007thefuturedirectionfortheAmbulanceServiceofNewSouth Wales.Sydney:ASNSW;2002.
8 TheAmbulanceServiceAssociation(TASA).Thefutureofambulance servicesintheUnitedKingdom–towardsperfectvision2000-2010. AMedicalCareResearchUnitMonograph.Sheffield:TASA;1999.
9 ThomsonS.Managementandsafety/qualityofservices–aresponse. HealthManager.2003;Autumn;15-17.
10 ConventionofAmbulanceAuthorities(CAA).Annualreport. Adelaide:CAA;2004.
11 CadyG,LindbergD.200–Citysurvey2000.JEMS.2001;26(2):24-33, 42-43.
12 LindsayWM,PetrickJA.Totalqualityandorganisationdevelopment. BocaRaton,FloridaStLuciePress;1994.
13MunkM.Researchmysteriesrevealed.JEMS.2000;25(9):34-38.
14 ChaseC,PerinaD.Effectsofacontinuousqualityimprovement programonhelicopterliftofftimes.Pre-hospitalEmergencyCare. 2001;5(4):384-6.
15 McCoyJ.AmbulanceServiceinVictoria.Apartnershiptoachieve qualityperformance.AustralianJournalofEmergencyCare.1996; 3(3):30-31.
16 PelowitzA.Qualityimprovement–gettingitright.HealthManager. 2003;Autumn2003:20-25.
17 QueenslandAmbulanceService(QAS).2005Organisationalself assessmentreport.(Unpublishedreport).Brisbane:QAS;2005.
18 DepartmentofEmergencyServices(DES).Annualreport2003-2004. Brisbane:DES;2004.
19SteeringCommitteefortheReviewofCommonwealth/StateService Provision.Reportongovernmentservices2003.Canberra: ProductivityCommission;2003;Vol1,p.8-42.
TheImpactofaContinuousQualityImprovementApproachonPatientCareintheAmbulanceEnvironment
AsiaPacificJournalofHealthManagement2006;1:2 43

r E S E a r c Ha r t i c l E
centralised control and devolved responsibilities: personal experiences of senior health executives on the implementation of the area health management model in new South Wales, 1990-1999Z liang, Sd Short, PF Howard, cr Brown
abstract Objective: This study explored the impact of the implementation of an Area Health Management Model (AHMM) on senior health executives in New South Wales between 1990 and 1999.
Setting: Health care reform has been a global phenom-enon and its negative effects on senior health care managers have been confirmed by empirical studies. In New South Wales, Australia, a major structural reform was the introduction of an AHMM in 1986.
Design: Qualitative methods were used to capture the personal experiences and views of senior health executives to the implementation of the AHMM. Thirteen senior executives employed by NSW Health between 1990 and 1999 were selected to participate in open-ended telephone interviews. The results were grouped into four common themes.
Results: Participants acknowledged that the AHMM had the potential to produce positive outcomes. However, they considered most of the potential benefits were not achieved due to shortcomings with the implementation process.
Zhanming liangMBBS,MScLecturerintheSchoolofPublicHealthGriffithUniversity,Queensland,Australia
Stephanie d ShortPhDProfessorandHeadoftheSchoolofPublicHealthGriffithUniversity,Queensland,Australia
Peter F HowardMBBS,MScAssociateProfessoroftheSchoolofPublicHealth,GriffithUniversity,Queensland,Australia
These shortcomings included: inadequate resources; insecurity and instability of senior management positions; control from central office; and constant and powerful political influences. The study also found that the benefits documented in NSW Health annual reports between 1990 and 1999 did not reflect the views of its senior executives.
Conclusion: During the introduction and implementation of a major health care reform in New South Wales between 1986 and 1999, barriers created by the ‘system’, centralised management processes and political influences within the Department for example, prevented the realisation of its potential benefits.
Abbreviations:AHMM-AreaHealthManagementModel;AHS-AreaHealthService;CEO-ChiefExecutiveOfficer;DG-DirectorGeneral;DOH-DepartmentofHealth;SHE-SeniorHealthExecutives.
Key words:regionalisation,areamanagementmodel,seniorhealthexecutives
claire r BrownPhDLecturerintheSchoolofPublicHealth,GriffithUniversity,Queensland,Australia
Correspondence:[email protected]
44 AsiaPacificJournalofHealthManagement2006;1:2

introduction Healthcarereformshavebeenaglobalphenomenonsincethe early 1980s. [1] Decentralisation in the provision andmanagement of health services is an example of a reformtoimprovethemanagementoftheincreasinglyexpensive,complexandfragmentedhealthsystem.[2]Decentralisationhas been developed in many states of Australia [3] andadoptedinanincreasingnumberofcountriesincludingtheUnitedKingdom,[4]NewZealand,[5,6]theNetherlands,[7]Canada,[8]ChinaandFiji.[2]
InAustralia,theintroductionoftheAreaHealthManagementModel (AHMM) is a significant structural change in thepublicly funded health care system. [9] The model wasfirstpioneeredintheearly1980sinNewSouthWales,[10]the most populous state in Australia, with an estimatedpopulationof6.77millionin2005.[11]TheNewSouthWalespublichealthsystemisthelargesthealthcareemployerinAustralia,withalmost93,000full-timeequivalentstaff.[12]
The AHMM, profoundly influenced by the British DistrictModel introduced in 1920, was further developed andrefined,basedonadecentralisedregionalstructureduringthe establishment of the Health Commission of NSW in1973. [13] The rationale was to develop a hierarchicalsystemofinstitutionsandservicesandasimpler,butmoreefficient, organisational structure to guide the allocationand reallocation of health service resources. It alsoaimed to facilitate the decentralisation of administrativeresponsibilities,bemoreresponsivetochanginglocalneeds[14,15] and to bring together all hospital and communityhealthservicesunderasingleareastructure.[2]Thecreationofthelargerareawasseenasthekeytothesuccessofthenew system, with a much larger quantum of resources,allowing area managers the scope to shift resources toachievemoreappropriateandefficientservicedelivery.[16]
In 1982, endorsed by the Health Administration Act, NSWHealthpilotedandevaluatedfourAreaHealthBoards.[17]UndertheAreaHealthServicelegislation,theseBoardswerechargedwiththefollowingobjectives:[2,p.239]
1. Responsibilityforthemaintenance,protectionand promotionofhealthofthepeopleinageographicarea byprovisionofprogramsandservices.
2. Coordinationofpublic,privateandvoluntaryhealth services.
3. Establishmentofanappropriatebalancebetween treatmentandpreventiveservices.
4. EnsuringefficiencyofhealthservicesprovidedbyArea Boards.
5. Ensuringcommunityparticipationinhealthservice planninganddecision-making.
AreviewofthepilotAreaHealthBoardswascommissionedin July 1985 to examine their impact on the efficiencyand effectiveness of services and the legal, industrial andadministrative implications of further development inNew South Wales. The review regarded‘area’ as the mostappropriate level for comprehensive high quality serviceprovision,costefficiency,co-ordinationandresponsivenessto local communities. [18] It recommended that theprovision of health services by formally constituted AreaHealthServices(AHSs)beexpandedandappliedacrosstheState.[18,19]Sincethen,theconceptofareamanagementofhealthserviceshasbeendevelopingandgaininggeneralacceptance.[4]
Althoughpositivefinancialandotherbenefitsarisingfromthe AHMM, such as improving service delivery, efficiency,effectiveness and accessibility, have been repeatedlydocumented inNSWHealthannual reportsbetween1986and1995,onlylimitedevaluationofthemodelorevaluationoftheexperiencesofmanagersresponsibleforpioneeringthe model have been documented. [3] The most relevantstudy was conducted by Ritchie and Johnson (1994)focusing on the restructuring of rural health services inNewSouthWales.[13]Thequalitativestudyconcludedthatalthoughtherestructuringhadbeensuccessfulindevolvingcontrol to a more local level during the 12 months afterimplementation,anysavingsfrommoreefficientprocesseswereunlikelytoberealisedbecauseofthe increase inthenumber of management positions. In addition, it pointedout that organisational structures in the new districtswere the result, not just of rational design, but also ofpoliticalcompromise(eg“issues…ofalignmentratherthanfunctionalareasseemedtoinfluencestructure”.[13,p.131])
To guide the successful implementation of organisationalchange, Bullock and Batten (1985) developed anintegrated, four-phase model of planned change thatinvolved exploration, planning, action and integration.[21] More recently, several studies have identified anumber of additional factors affecting the success ofimplementinglarge-scaleorganisationalchange,suchasthecharacteristicsofthesystem,itsstructureandculture,[22,23]organisationalreadiness,commitmentfromdifferentlevelsofmanagement,enoughtimeforpreparation,andsufficientmeasurementandfeedbackoftheresultsofchangetothekeystakeholders.[24,25]
CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
AsiaPacificJournalofHealthManagement2006;1:2 45

This study examines the implementation process of theAHMM and its effects on senior health executives withinNSWHealthbetween1986and1999byencapsulatingtheirpersonalexperiencesandopinions.Thisperiodwaschosenbecause implementation of the model was relatively well-established. This paper attempts to seek answers to thefollowingquestions:
1. Whatwereseniorhealthexecutives’overallexperiences withtheintroductionoftheAHMM?
2. If,intheexecutives’opinion,theimplementationofthe AHMMwasnotsuccessful,whatdidtheyconsidertobe thecontributingfactorsorshortcomings?
MethodsThestudytargetedthefollowingfourlevelsofseniorhealthexecutiveswithinNSWHealth:
• DirectorGeneral;
• DeputyDirectorGeneral;
• DOHDivisionDirector;and
• ChiefExecutiveOfficer(CEO)ofanAreaHealthService (ruralandmetropolitan).
Between 1990 and 1999, 71 senior health executivesoccupied positions across the above categories and for60 (80%) of these managers, their contact details wereavailable. Questionnaires were mailed to all managers togather information on their demographic characteristics
and employment status, and to seek their agreement toparticipate in a telephone interview. In total, 22 of the 60(37%)agreedtoparticipateandfromtheseseniorexecutives,13wererandomlyselectedforinterview.
In-depth telephone interviews were conducted in mid-2005 using open-ended questions. During the interviews,participantswereaskedtodescribefreelytheirexperiencesof the introduction and implementation of the AHMMin NSW from 1986 to 1999. At the end of the interview,they were invited to comment on the interview processand express any other concerns or issues. All interviewswere tape-recorded and transcribed. Transcriptions wereexamined for accuracy and subjected to content analysisandsortedfortheirrelevancetotheresearchquestions.Alldatawerescrutinisedforemergingpatterns.
The Griffith University Ethics Committee approved theresearchproject.
resultsStudy participantsThemajority(10/13)ofstudyparticipantswereAreaHealthServiceCEOsineitherSydneymetropolitanareaorruralNewSouthWales.The remaining three participants were eitherDirector General/Deputy Director General or Director of aDivisionwithintheNSWDepartmentofHealth(Table1).
targEt PoPulation contactaBlE PoPulation intErviEWEES
N % N % TARGET N % CONTACT POPULATION POPULATION
DirectorGeneral/DeputyDirector 17 24.0 15 88.2 3 20.0
General/DirectorofDivisionCEOMetropolitanAreaHealthService 16 22.5 16 100.0 4 25.0
CEOruralAreaHealthService 38 53.5 29 76.3 6 20.7
total 71 100.0 60 84.5 13 21.7
CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
Table 1: Study population, contactable population and study participants, by position
46 AsiaPacificJournalofHealthManagement2006;1:2

CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
Personal experiences with the aHMM Whilst 11 out of the 13 interviewees indicated that theintentionsoftheareamanagementmodelwereadmirable,several believed that the potential benefits of the reformshad not been achieved for various reasons. Moreover, themajorityof the intervieweesstressedthatthereformshadcreated barriers for senior executives to achieve the bestmanagement and service provision outcomes. Four mainthemes were generated from the interviews. A numberof quotes captured from the interviews are provided tohighlightsomeoftheviewsoftheinterviewees.
1. Potential benefits of the aHMMThe majority of the interviewees believed that the AHMMwasessentiallyaneffort todevolveoperationalaspectsofhealthcaretotheregionsandtointroduceastronglinkagebetween the community and the hospitals as well as thepublichealthservices.Theareamodelstartedto integratethe concept of a population-based focus and tried tointegratehealthservicesunderasinglemanagementtier.
One interviewee pointed out that the strength of havingan area model was to allow a more responsive and betterapproach to planning for a reasonably large population.However, a uniform approach by different areas proveddifficult.Anotherintervieweestatedthatthemodelallowedareductionofcompetitionforresourcesbetweendifferentareas, a reduction of hospital administration waste and areduction of duplication of services, which consequentlysupportedbetterclinicalservices:
The AHMM was a well regarded change by most of the senior executives; it was seen as a sensible way to go and certainly a big improvement on the dynamics of the old systems…so the structure which was really underpinned by a geographic area being as far as (possible) responsible for determining the priorities and the delivery methods and the structures for delivery (of a) full range of health care for the population was supported.
Another strength of an AHMM was more comprehensiveplanningforavarietyofservices.
2. inadequate financial resources and unachievable financial goals The majority of the interviewees pointed out that therewerenotenoughresourcestomakethesubstantialchangesrequired. The budget targets allocated were impossibleto manage even after a drastic reduction in the numberof staff within the area health structure. One interviewee
highlightedthattheAHMMwascommonlyreferredtoasa‘bankruptcymodel’bycuttingstaffnumbersheavilyinordertomeetimpossiblebudgettargets.
More than half of the interviewees claimed that seniorexecutives were expected to take the blame for theDepartment or Ministerial office when the budget orexpectationsfromthepublicwerenotbeingmet.Theytooktheblameforsomething impossibletoachievewithintheexistingfinancialarrangements:
If I got into trouble, I would be by myself. The inquiry into Campbelltown and Camden hospitals was a prime example (which affected a colleague outside the study period). When the inquiry took place, the Department tried to isolate South West Sydney AHS as much as possible and didn’t give it any support. …but I do think the shortage of resources in those hospitals in comparison to other hospitals within the State was a very big contributing factor to the problems that those two hospitals had.
Anotherintervieweestatedthattherewasscepticisminsomeparts of the health care system where financial resourceswere not provided as requested. As a result, communityhealth and hospital services were reduced and frictionbetween the practitioners within the hospital system andthosewithinthecommunityhealthserviceswascreated.
3. lack of support and insecurity in the job Interviewees claimed that while implementation of themodelbrought fear to those inseniorexecutivepositions,theDepartmentortheMinisterprovidedlittlesupportandinputduringthisperiodofconstantchange.Seniorexecutivepositions became unstable under the reform agenda andmanyexecutivesleftasaresult.Therewasaclaimthatthecareers of these people were destroyed because they leftundernegativecircumstances:
Moving from a regional structure to small district health services was a very destructive move, it created wholesale redundancies which were very lucrative. …appalling waste of public money.
There is a joke that goes around the senior executives that when the Government’s in trouble, bring on a restructure. …a real concern that every time this happens, you lose a whole lot of good people and corporate memory and knowledge; some people discount the value of corporate memory.
AsiaPacificJournalofHealthManagement2006;1:2 47

Interviewees added four other factors contributing to theunsuccessful implementation of the AHMM. They were: alackofconsultationwithseniorexecutivesbeforesettingthereformagenda;seniorexecutives’inadequateknowledgeofthereforms; insufficienttimegiventothe implementationprocess; and disenfranchisement of communities fromparticipatinginthehealthcaredebate,whichraisedbarriersbetweenthesystemandconsumers.
4. centralised control and political interference This theme was commonly mentioned by the majority oftheinterviewees.Theinitialauthoritygiventotheareaswasgradually pulled back to the central office, which causedtensionbothwithintheDepartmentandbetweenthecentralofficeandseniorexecutives.Inaddition,thedisbandmentoftheregionalofficesthatstoodbetweenNSWHealthandtheAHSs exposed senior executives to the political process atcentralleveltoagreaterextent,whichmademanagementmoredifficult.
Several interviewees pointed out that pulling away theauthority from the area level made the management ofthe health care system more centralised. The excessiveinterferencefromNSWHealthintheoperationofareahealthservicesdidnotallowtheareastomanagethemselvesandtobeaccountablefortheiroutcomes:
The AHMM is all about control really, control for the centre, that was the agenda. Getting rid of the boards and any sort of local difficulties.
One interviewee claimed that the reforms actually gavethe Minister opportunities to influence directly the healthservicesthroughthecentraloffice:
…the change to a purely corporate board and performance management and contracts didn’t necessarily advance health care delivery because it only made people responsible to the Centre, to the Department rather than trying to be innovative and engage communities and deliver good health services. ...we lost a significant amount of community support and the opportunity to actually do things because we were really required to comply with Health Department policy and to stay within those boundaries. …our health care system lost some of its good value from the reforms process.
One intervieweepointedoutthatmoreeffortscouldhavebeenputintotheintroductionandimplementationofthemodel.However, theseeffortshadnotbeenseenbecausethebarrierstothesuccesswereinfacttheexistingcentralisedmanagementprocessesandpoliticalinfluences:
The area management model was the best way to go, but things have been eroded and I personally believe there is further scope for improvement, but I don’t think governments will have the courage to do that.
Inadditionto theaboveopinions, two intervieweesmadevery explicit comments about the barriers created by theAHMM:
Too many reforms were not managed well by the Department, and there was too much centralised control and ambiguity in accountability. There were so many reforms and my experience was that each reform that happened, NSW Health got worse at handling the reforms. … at the end of the day, the patients and the staff weren’t any better off despite all the reforms.
When the AHSs (were) first formed, they actually got that fairly right, that the central administration had had responsibilities for certain things such as industrial relations, and overall policy in major planning. …the problem for an area CEO in AHSs was that there were divided responsibilities: on one hand you were responsible to the board of directors, then on the other hand, the Director General saw you as his person, so you were serving two masters and that did cause some problems.
Clearly, too much centralised control and politicalinterference were regarded as important reasons for thelimitedachievementof the fullbenefitsof theareahealthmanagementmodel.
discussionPrincipal findingsThreemainfindingsfromthepersonalexperiencesofseniorhealthexecutiveswiththeintroductionandimplementationofanareahealthmanagementmodelinNewSouthWaleshave emerged from the study. Firstly, inadequate financialandotherresourceswereprovidedfortheimplementationof changes to the system including planning, preparation,implementation andevaluation.Moresignificant were thefinancial goals set for each area without being mutuallyagreed between the central office and the Area HealthService.Thegoalswereoftenseenasunachievablebythelatter.
Secondly, the introduction of the AHMM made the seniorhealthmanager’spositionmoreunstableunderthereformagenda.Thisinevitablybroughtacertainlevelofinsecuritytothosewhowere inthesepositions,andtothosewhosepositionswereatriskofbeingmaderedundant.Moreover,insufficientsupportwasofferedtothosewhowereworking
CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
48 AsiaPacificJournalofHealthManagement2006;1:2

in the system, especially senior health managers, to assistthemwithnotonlysurvivingtheturbulentperiod,butalsoprovidingeffectiveleadershipintheimplementationofthestructuralreforms.
Thirdly, the pull back of authority initially delegated bycentralofficetoAHSexecutivesandtheincreasingexposureof senior executives to the political process createdunnecessary tensions between senior personnel in centralofficeandareahealthexecutives.Asaresult,theleadershiprole of senior executives was undermined while ongoingpolitical-level intervention created ambiguity surroundingtheaimsandscopeofthereforms.
Strengths and weaknesses of the studyThisqualitativestudywas limitedby itssmallsamplewiththe implications of selection bias. However, it enabledthe collection of the views and experiences of a group ofsenior managers who had been closely involved in theimplementation of large-scale organisational change. Thistypeof in-depthdata isnormally impossibletogainusingquantitative methods with large sample sizes. The resultsof our study provide valid insights from the sample, butit is inappropriate to generalise them to the entire seniorexecutive sector within NSW Health during the studyperiod.
The study also captured the opinions of senior executivesabout some of the successes of the introduction of theAHMM in NSW. The majority of executives believed thatthemodelwaspositiveinvariousways.Examplesincludedthe better integration of services; improved efficiency inserviceprovision,areductionintheduplicationofservicesand improvedplanning for the rangeofservicesprovidedwithin a geographical area.These benefits were similar tothe expectations of management when the AHMM wasfirst introducedandtotheoutcomesdocumentedinNSWHealthannual reports.Forexample, itwas reported in the1986 -1987AnnualReport that,“…the implementationoftheAHMMhadresultedinmuchimprovedhealthservicesfor the people of this State and a more efficient andresponsivemanagementsystemforthehealthservices,andwouldcontinuouslyimproveservicedelivery,andefficiency,effectiveness and accessibility of the NSW Public HealthSystem”.[26,p.4]
The above statement was generally supported by anevaluation conducted by Lawson and Evans in 1992. [2]It compared a well-established AHS in 1990 with a newlycreated AHS with respect to the achievement of the five
major objectives previously listed. Acknowledging thelimitationsof themethodsused, these researchersarguedthat while previous attempts at evaluation of AHSs bytraditional numerical measures had failed, the method ofcomparingbroadlysimilarAHSs,supplementedbysurveys,appearedtobeausefulapproach.[2]
However, Stoelwinder (1992), questioned the validity ofthe evaluation evidence provided to support Lawson andEvans’s (1992) conclusions, stating that methodological,epistemological, semantic and even political factors maymitigate against effective evaluation research of this kind.[3] He further explained that the major problem was thatone could not be certain that the two AHSs would havebeensimilarhaditnotbeenfortheintervention.Anyresultsarisingfromthiscomparativestudycouldbeattributedtothe differences between mature and immature sites andmaynothavebeentheresultoftheintervention.
Meaning of the studyAlthoughtheconclusionsfromourstudymaybelimitedbyitsqualitativemethods,itrepresentsanewwayofexaminingtheimplementationofanAHMMbyusingmeaningfuldatafromthosewhowereheavilyinvolvedinitsimplementation.The findings from the current study do not support thereports from NSW Health during the early stages of theimplementationoftheAHMM.FollowingBullockandBatten’s[20]Four-Phasemodelforthesuccessfulimplementationofchange,ourstudyidentifiedthatthelimitedsuccessoftheimplementationoftheNewSouthWalesAHMMmayhavebeenduetoaninadequateinvestmentoftimeandexpertiseduring the first two phases: the exploration and planningphases. This study has disclosed how the centralisedmanagementprocessesandpolitical influenceswithintheNSW Department of Health may have acted as barriers totheimplementationofitsownreforms.
Unanswered questions and future researchFurther studies are recommended to explore possiblesolutionsforminimisingthenegativeimpactofthebarrierstoimplementinglarge-scalechangeidentifiedinthisstudy.
conclusionThis study concludes that senior health executives heldpositiveviewstowardtheintentionoftheimplementationof the AHMM in New South Wales. However, the fullbenefits of the model were not achieved due to severalshortcomings during the early stages of implementation.Significant deficiencies included inadequate resources forthe implementation of change, insecurity and instability
CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
AsiaPacificJournalofHealthManagement2006;1:2 49

brought to senior health management positions, healthdepartment efforts to centralise control and on-goingpoliticalinterventions.
The significance of this study should not be understatedas this is the first study internationally that actually tapsinto the views and experiences of those who managedthe change process: senior health executives themselves.The study, therefore, makes a significant contribution tooursystematicunderstandingoftherealpoliticsofbeingaseniorhealthexecutiveduringaperiodofsignificanthealthcare reform. During the introduction and implementationofamajorhealthcarereforminNewSouthWalesbetween1986 and 1999, barriers created by the‘system’ preventedtheachievementofmanyofitspotentialbenefits.
acknowledgements WewouldliketothankalltheinformantswhoparticipatedinthestudyandtheinvaluablesupportfromtheAustralianCollegeofHealthServiceExecutives(ACHSE). Inparticular,we acknowledge and thank Mr Bill Lawrence, formerNationalDirectorofACHSEforhisguidanceintheconductofthisstudy.
competing interestsTheauthorsdeclarethattheyhavenocompetinginterests.
references 1. HigginsI.Benchmarkinginhealthcare:areviewofliterature. AustHealthRev.1997;20(4):60-69.
2. LawsonJS,EvansAR.Thesuccessfuldevelopmentofdecentralisation healthservicemanagement:anevaluationofareahealthservice inNewSouthWales.AustHealthRev.1992;15(3):237-47.
3. StoelwinderJU.HowcanIknowwhatIthinktillIseewhatIsay?’: evaluatinghealthcarestructure.AustHealthRev.1992;15(3): 248-58.
4. PalmerGR.Theregionalisationofhealthservices:objectives,models andrecentNSWexperiences.AustHealthRev.1981;4:16-21.
5. MalcolmI.Servicemanagement:aNewZealandmodelforshifting thebalancefromhospitaltocommunitycare.IntJHealthPlanning andManage.1991;6:23-35.
6. RitchieD.Managementofhealthsystemreform:aviewofchanges withinNewZealand.HealthServicesManageRes.1998;11:182-9.
7. DeBakerDH.Thedistrictconceptforprimaryhealthplanning: attemptsatimplementationintheNetherlands.HealthPolicy. 1989;13:56-64.
8. RathwellT,PersaudD.Runningtostandstill:changeand managementinCanadianhealthcare.HealthcManageForum. 2003;15(3):10-17.
9. CrichtonA.Slowlytakingcontrol?Australiangovernmentsand healthcareprovision,1788–1988.Sydney:Allen&Unwin;1990.
10. LiangZM,ShortSD,LawrenceB.HealthcarereforminNewSouth Wales1986–1999:usingtheliteraturetopredicttheimpacton seniorhealthexecutives.AustHealthRev.2005;29(3):285-91.
11. NSWDepartmentofHealth.ThehealthofthepeopleofNewSouth Wales:reportoftheChiefHealthOfficer2004.Sydney;2005.
12. NSWDepartmentofHealth.NSWDepartmentofHealthAnnual Report04/05.Sydney;2004.
13. RitchieD,JohnsonL.AReviewofruralhealthrestructuringinNew SouthWales.AustHealthRev1994.17,4:125-34.
14. NSWDepartmentofHealth.AnnualReport1994/95.Sydney;1995.
15. PalmerGR,ShortSD.Healthcareandpublicpolicy:anAustralian analysis,2nded.Melbourne:MacMillan;1994.
16. NSWDepartmentofHealth.Theareahealthserviceconference: areahealthserviceasaplanningandmanagementtoolforthe future.Sydney;1991.
17. NSWDepartmentofHealth.AnnualReport1984/85.Sydney;1985.
18. NSWDepartmentofHealth.AnnualReport1985/86.Sydney;1986.
19. NSWDepartmentofHealth.Reviewofareamanagementofhealth services.Sydney;1986.
20. KerberK,BuonoAF.Rethinkingorganisationalchange:reframing thechallengeofchangemanagement.OrganisationalDevelopment Journal.2005;23:23-39.
21. BurnesB.Managingchangeastrategicapproachtoorganisational dynamics.Edinburgh:PearsonEducationLtd;2000.
22. HeifetzM,HalleS.Leadingchange,overcomingchaos–making changesucceedinyourorganisation.HospMaterialManage Quart.1996;18(1):17-27.
23. MartinV.Leadingchangeinhealthandsocialcare.London: Routledge;2003.
24. CornellJ.Aspectsofthemanagementofchange.JManageinMedi. 1996;10(2):23-30.25. NSWDepartmentofHealth.NSWDepartmentofHealthAnnual Report86/87.Sydney;1987.
CentralisedControlandDevolvedResponsibilities:personalexperiencesofseniorhealthexecutivesontheimplementationoftheareahealthmanagementmodelinNewSouthWales,1990-1999
50 AsiaPacificJournalofHealthManagement2006;1:2
introductionTherearemanyfactorsbesidesbiologythatinfluencehealthstatus; forexample,socialandeconomic factors. [1] In thefamous Whitehall studies in England, where occupation,income, education and place of residence were similar,employeesexperienceddifferenthealthstatuseven intheoneworkplace.[2]
Recently, a national survey that included 17 of the 38Australian universities, found that 50% of university staffwere at risk of psychological illness compared with 19%in the general population. [3] Although this research maybe criticised because it was supported by funds from theNationalTertiaryEducationUnion,itwasalsosupportedby
r E S E a r c Ha r t i c l E
Health Status of Employees: defining influences on health in the tertiary education industryM J ditton
abstract Objective: The health status of employees at an Australian university was assessed in order to target subsequent workplace health interventions.
Design: A cross-sectional survey of all university employees (academic and general) was undertaken using the Short Form-36 (SF-36) in combination with a socio-demographic questionnaire. This was complemented by interviews with 40 university employees, stratified by level of employment.
Setting: The University of New England, New South Wales. A university setting was chosen because previous studies had identified that 50% of employees in the tertiary education industry in Australia were at risk of mental health problems due to stress and workplace pressure compared with 19% of the general population.
Results: A response rate of 49% was achieved (514/1047). The total study population attained significantly lower (poorer) mental health status scores than those of the Australian employed persons’ sub-group norm. Academic staff reported significantly better physical health than general staff. Grade of employment, age, domestic living arrangements, health service utilisation and smoking were factors associated with variation in health status.
Conclusions: The comparatively poor mental health status of Australian university employees combined with variation in health status based on sociodemographic measures poses a public health challenge for those concerned with maintaining and promoting the health of the tertiary education workforce. This study provides a basis for the development and evaluation of appropriate mental health promotion programs at the University of New England and raises questions for further research to explore the need for similar programs in other universities and public sector organisations.
Abbreviations:GHQ–GeneralHealthQuestionnaire;HEO–HigherEducationOfficer;NSW–NewSouthWales;SF-36–ShortForm-36self-administeredsurvey;UNE–UniversityofNewEngland.
Key words:healthstatus;universityemployees;SF-36survey;mentalhealth.
dr M J dittonMBBS,DPM,MBA,GradCertHEd,DHSMSchoolofHealth,UniversityofNewEnglandArmidale,NewSouthWales,Australia
Correspondence:Email:[email protected]
AsiaPacificJournalofHealthManagement2006;1:2 51

HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
the Australian Research Council and the Vice ChancellorsCommittee. Further, the expertise of the researchers, therigorofthemethodologyandthesoundanalysisofthedatasuggestthefindingsofthisstudywerecredible.Asaresultof their study, Winefield et al (2002) recommended thatmanagersoftheseinstitutionsshouldgivegreaterattentionto fairness of procedures, adequate compensation andincreasedjobsecurity.[3]
To investigate such findings in more detail, and tosubsequently target workplace health interventions, theauthorassessedthehealthstatusofacademicandgeneralemployeesattheUniversityofNewEngland(UNE),Armidale,NewSouthWales.Armidaleisasmall,well-resourcedinlandcitywithgoodhealthservicesandapublichospital.
MethodsData collectionA short sociodemographic questionnaire was combinedwith an internationally recognised instrument for themeasurement of health status: the self-administeredShort Form-36 (SF-36) Health Survey. [4-8] This combinedquestionnaire was sent to all UNE employees in June-July2002(n=1047:407academic;640general).
The sociodemographic questionnaire was developed toaccompany the SF-36 survey in order to define both thesamplepopulationandtoexploresociodemographicfactorsassociatedwithvariationinhealthstatus.[9]Thisinstrumentcovered age, sex, living arrangements, employmentcharacteristics, health insurance and health serviceutilisation,andlevelsofsmokingandalcoholconsumption.
TheSF-36questionnairewaschosenasameasureofhealthstatusratherthantheGeneralHealthQuestionnaire(GHQ–12) used by Winefield et al (2002) in the national surveyof university staff, [3] because the SF-36 measures bothphysical and psychological distress (mental health), ratherthan justpsychologicaldistressas in theGHQ-12. [10]TheSF-36hasbeenusedinAustraliapreviously,andpopulationnorms are available for comparison. [11] It comprises one‘self-reported health transition’ question plus 35 questionsthatmeasureeightdimensionsofhealthstatuswithfourofthedimensionsrelatedtophysicalhealthandfourtomentalhealth. [4, p. 4] Survey participants indicate how they feelabouttheirhealthstatusbymarking29(threetosixpoint)scalesandseven‘Yes’‘No’questions.
PHySical HEaltH MEntal HEaltH
Physicalfunctioning Vitality (ten questions) (four questions)
Role-physicallimitation Socialfunctioning (four questions) (two questions)
Bodilypain Role-emotionallimitation (two questions) (three questions)
Generalhealth Mentalhealth (five questions) (five questions)
The information is then summarised to provide a‘PhysicalComponent Summary’ score and a ‘Mental ComponentSummary’ score (Table 1). [4]These summary scores havebeenvalidatedfordifferentiatingpopulationswithvaryingphysicalandmentalhealth.[12,13]
Table 1: SF-36: Eight dimensions (or scales) of health status, the scores of which can be aggregated to provide summary measures of physical health and mental health
Data analysisFollowingtheSF-36scoringsystem,responsestoquestionsfor each of the eight dimensions of health status weresummarised to provide eight scores between 0 and 100.Dimensions in which health status was defined as theabsenceof incapacityhadthehighestpossiblescore(100)and, for these questions, the higher the score the betterthe health status. This scoring system applied to physicalfunctioning, role-physical, bodily pain, social functioningand role-emotional. For the remaining three dimensions(generalhealth,vitality,andmentalhealth)awiderrangeofnegativeandpositivehealthstateswasgeneratedandforthese dimensions a mid-range score (ie 50) indicated thatapersonhadreportednolimitationsordisabilities.Forthetwo summary measures (ie physical component summaryandmentalcomponentsummary),ascoreof50represented‘goodhealth’,whileascoreoflessthan50represented‘poorhealth’.[13]
With the data arising from the sociodemographicquestionnaire, informants were grouped according to age(younger than 35 years; 35–44; 45–54; or 55 and older);whether they lived in partnerships or alone; whether theywereontheacademicorgeneralstaff;andtheiremploymentgrade and length of employment. Grades of employmentforacademicstaffwere:entrylevelA(AssociateLecturer);B(Lecturer);C(SeniorLecturer);D(AssociateProfessor);andE(Professor)andSeniorExecutivepositions.
52 AsiaPacificJournalofHealthManagement2006;1:2

HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
Forgeneralstaff,gradesofemploymentweregrouped,fromentry level,HigherEducationOfficer(HEO)1and2;HEO3and4;HEO5and6;HEO7;toHEO8–10andabove.
Health insurance in addition to the Australian compulsoryMedicarelevy,[14]andthetypeofinsurance,wasestablished.Thecategorieswere:‘none’(noadditionalinsurance);‘partial’(extra basic hospital insurance); and ‘full’ (extra hospitaland ancillary insurance). The health service utilisationinformationconsistedofthenumberof1)hospitalisations;2) consultations with doctors (medical practitioners); and3) consultations with alternative therapists (ie counsellors,chiropractors,physiotherapists,herbaltherapists,osteopaths)inthepast12months.
Smoking and alcohol consumption were considered aspossibleriskbehaviours.Toidentifythegroupwhosecurrentsmokingbehaviourmaybeharminghealth,[15]informantsweregroupedaccordingtothosewhohadneversmokedorwereex-smokers;orthosewhocurrentlysmoked,regardlessoftheextent.
Dataoninformants’levelofalcoholintakewerecategorisedinto five groups: 1) do not drink at all; 2) one drinkoccasionally;3)onedrinkonceortwiceaweek;4)onedrinkmost days of the week; and 5) more than one drink everyday.InlightoftheguidelinesfromtheNationalHealthandMedical Research Council, [16] the responses were thenrecodedas:• noneorlowalcoholconsumption(1,2and3drinksperday);
• moderateconsumption(4);and
• highrisk(5).
Drinkersincategory5wereconsideredashighriskforbothshort - and long-term health problems from alcoholconsumption.
The sociodemographic data were analysed using theStatistical Package for Social Science, [17] and those fromtheSF-36accordingtotheSF-36Manualandinterpretationguide.[18]Thehealthstatusofsurveyinformantswasthencompared with SF-36 Australian population norms [11],usingStudent’s‘t’test,andFisher’s(F)testwhereappropriate.Significancewasassessedatp<0.05.Pair-wisecomparisonswere conducted to locate significant pairs in appropriatecategories. For example, a significant association betweensmoking and drinking was observed for academic staff;and no association was observed between age or genderand hospitalisation for both general and academic staff.Differences inSF-36scores for thetensub-groupsdefinedin the study population by the various sociodemographicvariablesweredetectedbymultipleregressionanalysis.[19]
TheresearchwasconductedaccordingtotheGuidelinesforHumanResearchattheUniversityofNewEngland.
results Table 2 indicates that 53% of general staff and 43% ofacademic staff responded to the survey, with an overallresponseof49%.
acadEMic gEnEral total StaFF StaFF
Questionnairesdistributed 407 640 1047
Responded 176(42.8%) 338(52.9%) 514(48.9%)
Complete data sets 176(43.2%) 334(50.6%) 500(47.8%)
Sociodemographic survey Mostoftheinformants(59%,or295employees)weremorethan45yearsold(Table3).Themeanageofacademicstaffwas48.7years (SD±8.2; range25–68);andthatofgeneralstaffwas44.6years(SD±9.4;range18–67).Atthetimeofthestudy, 131 employees (24% academic; 27% general) livedalone(Table3).
Table 2: Survey response, by academic and general staff
acadEMic StaFF gEnEral StaFF (n=176*) (n=324*)
nuMBEr % nuMBEr %
age (years)Lessthan35 6 3.4 47 14.635–44 54 30.9 96 29.745–54 65 37.1 132 40.955andover 50 28.6 48 14.8
SexMale 97 55.1 133 41.2Female 79 44.9 190 58.8
living arrangementsPartnership 133 75.6 235 72.6Livingalone 43 24.4 88 27.4
Place of birthAustralia 110 66.0 292 86.0Overseas 58 34.0 47 14.0
residence prior to employmentAustralia 126 75.0 306 90.0Overseas 42 25.0 34 10.0
*Note:asnotallquestionswerefullyanswered,subtotalsdonotallequal176foracademicsand324forgeneralstaff.
Table 3: Sociodemographic profile of academic and general staff informants
AsiaPacificJournalofHealthManagement2006;1:2 55

acadEMic StaFF gEnEral StaFF n % n %
Health insurance in addition to MedicareNone 44 25.0 122 37.8Partial 36 20.5 65 20.1Full 96 54.5 136 42.1
doctor consultations per yearNone 33 18.8 47 14.51-2 74 42.0 147 45.43-4 47 26.7 70 21.55-6 12 6.8 31 9.6≥7 10 5.7 29 9.0total doctor consultations 473 972
alternative therapy consultationsNone 126 71.6 199 61.41-2 17 9.7 42 13.03-4 7 4.0 35 10.85-6 9 5.1 19 5.8≥7 17 9.6 29 9.0total therapy consultations 325 685
Hospitalised during past yearYes 20 11.4 43 13.3No 156 88.6 297 86.7
HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
The largest group of informants (68%) were in mid-levelgradesofemployment (ie lecturerandsenior lecturerandHEO3and4andHEO5and6),9%wereinthelowestgradesof employment, while 23% were in the higher grades ofemployment(Table4).
acadEMic StaFF gEnEral StaFF (n=176*) (n=324*)
gradE oF EMPloyMEnt nuMBEr % gradE oF EMPloyMEnt nuMBEr %
AssociateLecturer 22 12.5 HEO11and2 18 5.6Lecturer 63 35.8 HEO3and4 112 34.7SeniorLecturer 51 29.0 HEO5and6 116 35.9AssociateProfessor 27 15.3 HEO7 36 11.1ProfessorandSeniorExecutive 13 7.4 HEO8-10andabove 41 12.7
duration of employment (years) duration of employment (years)1-3 36 20.5 1-3 59 18.34-10 63 35.8 4-10 88 27.311-15 30 17.0 11-15 61 18.916-20 20 11.4 16-20 39 12.221andover 27 15.3 21andover 75 23.3
*Note:Asnotallquestionswerefullyanswered,subtotalsmaynotalwaysbeequaln=176foracademicsandn=324forgeneralstaff;1.HEO:HigherEducationOfficer.
Table 4: Grade and duration of employment of academic and general staff informants
Table 5: Pattern of health service utilisation of academic and general staff in the past 12 months
In total, 50% of staff had been in employment at UNE formore than 10 years (45% of academic staff and 54% ofgeneralstaff)(Table4).
Sixty-three employees (12.6%) had been in hospital in theprevious12months(11%academic,and13%general,staff)(Table5).
54 AsiaPacificJournalofHealthManagement2006;1:2
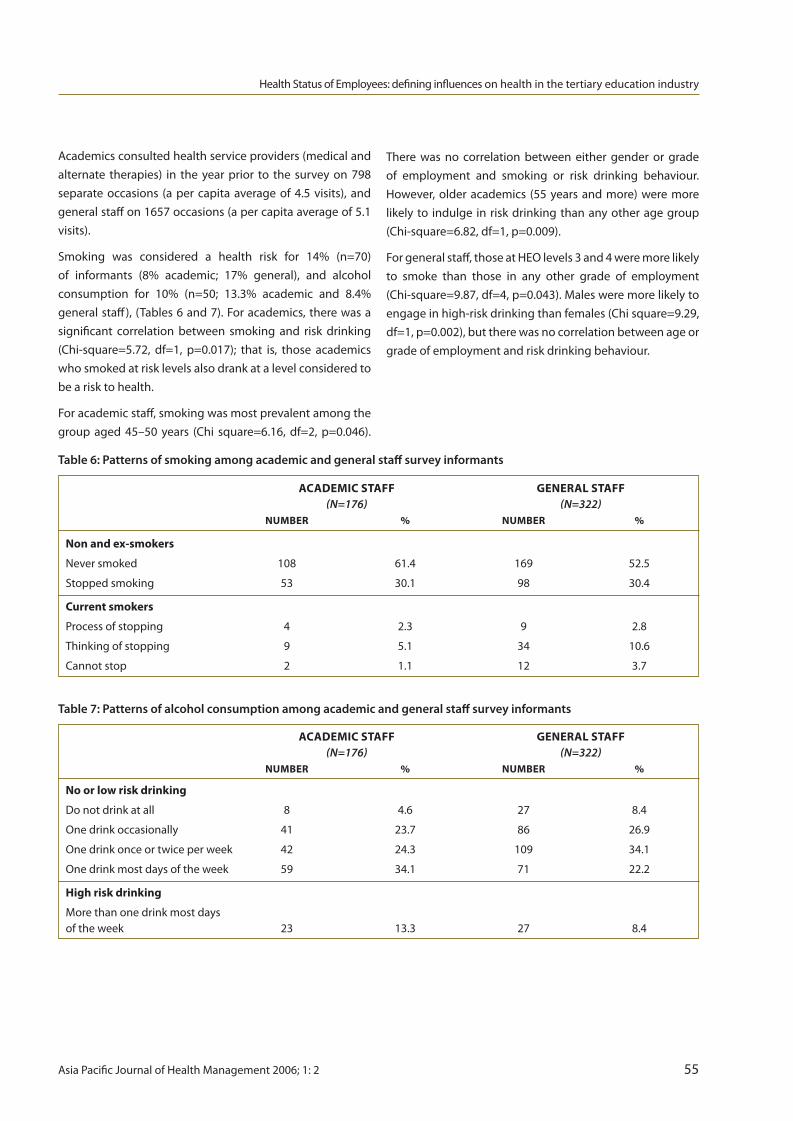
acadEMic StaFF gEnEral StaFF (n=176) (n=322) nuMBEr % nuMBEr %
no or low risk drinking
Donotdrinkatall 8 4.6 27 8.4
Onedrinkoccasionally 41 23.7 86 26.9
Onedrinkonceortwiceperweek 42 24.3 109 34.1
Onedrinkmostdaysoftheweek 59 34.1 71 22.2
High risk drinking
Morethanonedrinkmostdaysoftheweek 23 13.3 27 8.4
HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
Academicsconsultedhealthserviceproviders(medicalandalternate therapies) in the year prior to the survey on 798separate occasions (a per capita average of 4.5 visits), andgeneralstaffon1657occasions(apercapitaaverageof5.1visits).
Smoking was considered a health risk for 14% (n=70)of informants (8% academic; 17% general), and alcoholconsumption for 10% (n=50; 13.3% academic and 8.4%generalstaff), (Tables6and7).Foracademics,therewasasignificant correlation between smoking and risk drinking(Chi-square=5.72, df=1, p=0.017); that is, those academicswhosmokedatrisklevelsalsodrankatalevelconsideredtobearisktohealth.
Foracademicstaff,smokingwasmostprevalentamongthegroup aged 45–50 years (Chi square=6.16, df=2, p=0.046).
acadEMic StaFF gEnEral StaFF (n=176) (n=322) nuMBEr % nuMBEr %
non and ex-smokers
Neversmoked 108 61.4 169 52.5
Stoppedsmoking 53 30.1 98 30.4
current smokers
Processofstopping 4 2.3 9 2.8
Thinkingofstopping 9 5.1 34 10.6
Cannotstop 2 1.1 12 3.7
There was no correlation between either gender or gradeof employment and smoking or risk drinking behaviour.However,olderacademics (55yearsandmore)weremorelikelyto indulge inriskdrinkingthananyotheragegroup(Chi-square=6.82,df=1,p=0.009).
Forgeneralstaff,thoseatHEOlevels3and4weremorelikelyto smoke than those in any other grade of employment(Chi-square=9.87,df=4,p=0.043).Malesweremorelikelytoengageinhigh-riskdrinkingthanfemales(Chisquare=9.29,df=1,p=0.002),buttherewasnocorrelationbetweenageorgradeofemploymentandriskdrinkingbehaviour.
Table 6: Patterns of smoking among academic and general staff survey informants
Table 7: Patterns of alcohol consumption among academic and general staff survey informants
AsiaPacificJournalofHealthManagement2006;1:2 55

Table 8: Mean SF-36 scores for study population and Australian employed persons’1 norms
SF-36 health status survey Compared with Australian employed persons’ sub-groupnorms,[11]Table8showsthatsurveyedinformantsscoredsignificantlylower(poorerhealth)forvitality,role-emotional,andthementalhealthcomponentsummary.
Study PoPulation auStralian EMPloyEd PErSonS (n=500) (n=11,771)
SF-36 diMEnSion MEan Sd MEan Sd
Physicalfunctioning 90.1 14.7 88.8 21.6
Rolephysical 86.7 29.8 86.7 43.3
Bodilypain 79.8 20.9 80.3 32.5
Generalhealth 73.5 18.8 75.6 21.6
Vitality** 62.0 20.7 66.7 21.6
Socialfunctioning 88.1 20.6 87.9 32.5
Role-emotional** 82.9 34.0 87.2 43.3
Mentalhealth 75.6 16.9 77.2 21.6
Physical component summary 52.7 7.8 52.2 10.8
Mental component summary** 48.9 10.9 50.6 10.8
1.Australianemployedpersons’sub-groupnorms.Source:AustralianBureauofStatistics.Nationalhealthsurvey:SF-36populationnorms.Canberra:AGPS;1995.**Significanceassessedatthelevelofp<0.05.
Academicstaffscoredsignificantlyhigher (iebetterhealthstatus) than general staff on the SF-36 profile for physicalfunctioning, bodily pain and the physical componentsummary(Table9).
Table 9: SF-36 Profile of scores for study population as a whole, and for academic and general staff separately
Study PoPulation acadEMic StaFF gEnEral StaFF (n=500) (n=176) (n=323)
SF-36 diMEnSion MEan Sd MEan Sd MEan Sd
Physicalfunctioninga 90.1 14.7 93.4 9.0 88.2 16.7
Rolephysical 86.7 29.8 87.8 27.9 86.0 30.9
Bodilypainb 79.8 20.9 82.6 19.5 78.3 21.5
Generalhealth 73.5 18.8 74.2 18.4 73.1 18.9
Vitality 62.0 20.7 63.6 21.0 61.2 20.6
Socialfunctioning 88.1 20.6 89.4 19.3 86.4 21.2
Role-emotional 82.9 34.0 83.3 33.2 82.7 34.4
Mentalhealth 75.6 16.9 75.2 16.3 75.9 17.3
Physical component summaryc 52.7 7.8 54.0 6.2 52.0 8.4
Mental component summary 48.9 10.9 48.6 10.4 49.0 11.3
a,b,c–indicateasignificantdifferencebetweenacademicandgeneralstaff:a=p<0.0001;b=p<0.05;c=p<0.001.
HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
56 AsiaPacificJournalofHealthManagement2006;1:2
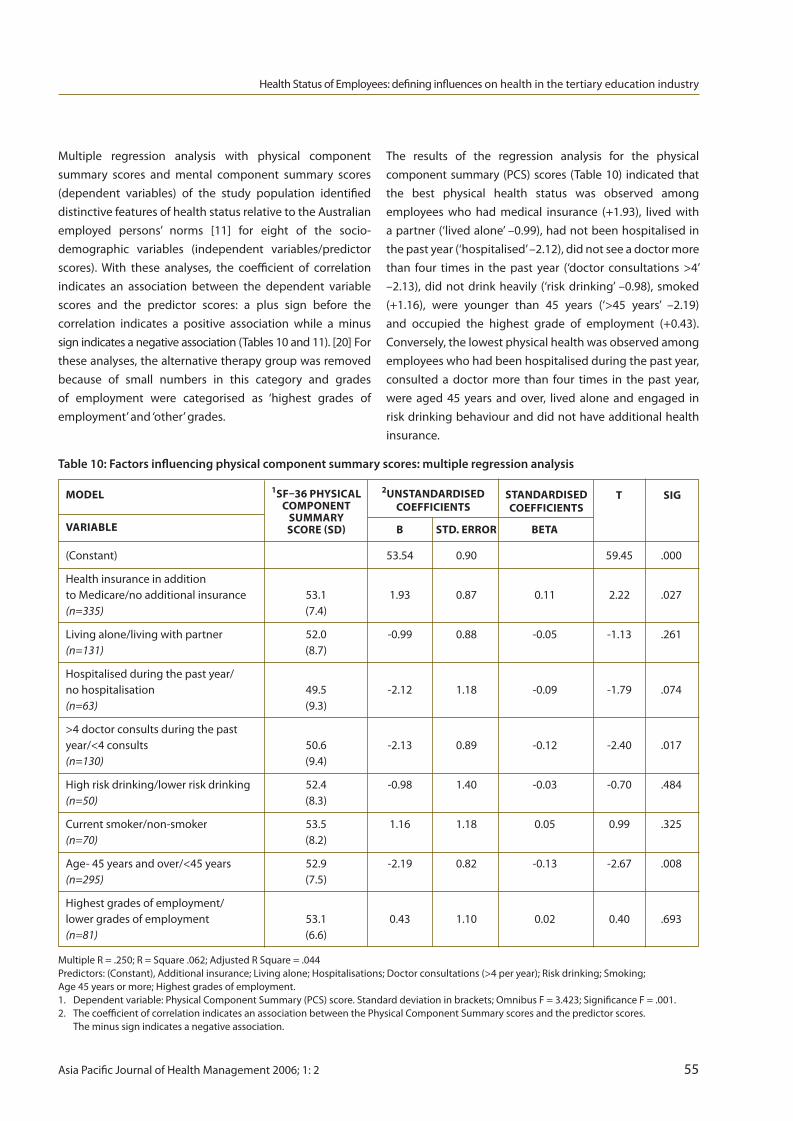
(Constant) 53.54 0.90 59.45 .000
HealthinsuranceinadditiontoMedicare/noadditionalinsurance 53.1 1.93 0.87 0.11 2.22 .027(n=335) (7.4)
Livingalone/livingwithpartner 52.0 -0.99 0.88 -0.05 -1.13 .261(n=131) (8.7)
Hospitalisedduringthepastyear/nohospitalisation 49.5 -2.12 1.18 -0.09 -1.79 .074(n=63) (9.3)
>4doctorconsultsduringthepastyear/<4consults 50.6 -2.13 0.89 -0.12 -2.40 .017(n=130) (9.4)
Highriskdrinking/lowerriskdrinking 52.4 -0.98 1.40 -0.03 -0.70 .484(n=50) (8.3)
Currentsmoker/non-smoker 53.5 1.16 1.18 0.05 0.99 .325(n=70) (8.2)
Age-45yearsandover/<45years 52.9 -2.19 0.82 -0.13 -2.67 .008(n=295) (7.5)
Highestgradesofemployment/lowergradesofemployment 53.1 0.43 1.10 0.02 0.40 .693(n=81) (6.6)
MultipleR=.250;R=Square.062;AdjustedRSquare=.044Predictors:(Constant),Additionalinsurance;Livingalone;Hospitalisations;Doctorconsultations(>4peryear);Riskdrinking;Smoking;Age45yearsormore;Highestgradesofemployment.1. Dependentvariable:PhysicalComponentSummary(PCS)score.Standarddeviationinbrackets;OmnibusF=3.423;SignificanceF=.001.2. ThecoefficientofcorrelationindicatesanassociationbetweenthePhysicalComponentSummaryscoresandthepredictorscores. Theminussignindicatesanegativeassociation.
HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
Multiple regression analysis with physical componentsummary scores and mental component summary scores(dependent variables) of the study population identifieddistinctivefeaturesofhealthstatusrelativetotheAustralianemployed persons’ norms [11] for eight of the socio-demographic variables (independent variables/predictorscores). With these analyses, the coefficient of correlationindicates an association between the dependent variablescores and the predictor scores: a plus sign before thecorrelation indicates a positive association while a minussignindicatesanegativeassociation(Tables10and11).[20]Fortheseanalyses,thealternativetherapygroupwasremovedbecause of small numbers in this category and gradesof employment were categorised as ‘highest grades ofemployment’and‘other’grades.
The results of the regression analysis for the physicalcomponentsummary (PCS)scores (Table10) indicated thatthe best physical health status was observed amongemployees who had medical insurance (+1.93), lived withapartner(‘livedalone’–0.99),hadnotbeenhospitalisedinthepastyear(‘hospitalised’–2.12),didnotseeadoctormorethan four times in the past year (‘doctor consultations >4’–2.13), did not drink heavily (‘risk drinking’ –0.98), smoked(+1.16), were younger than 45 years (‘>45 years’ –2.19)and occupied the highest grade of employment (+0.43).Conversely,thelowestphysicalhealthwasobservedamongemployeeswhohadbeenhospitalisedduringthepastyear,consulted a doctor more than four times in the past year,were aged 45 years and over, lived alone and engaged inriskdrinkingbehaviouranddidnothaveadditionalhealthinsurance.
Table 10: Factors influencing physical component summary scores: multiple regression analysis
1SF–36 PHySicalcoMPonEnt
SuMMaryScorE (Sd)
2unStandardiSEdcoEFFiciEntS
ModEl
variaBlE
StandardiSEdcoEFFiciEntS
t Sig
B Std. Error BEta
AsiaPacificJournalofHealthManagement2006;1:2 55

HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
(Constant) 47.49 1.23 38.64 .000
HealthinsuranceinadditiontoMedicare/noadditionalinsurance 49.4 0.63 1.18 0.03 0.53 .597(n=335) (7.4)
Livingalone/livingwithpartner 47.9 -1.48 1.20 -0.06 -1.24 .215(n=131) (11.5)
Hospitalisedduringthepastyear/nohospitalisation 46.1 -0.78 1.62 -0.02 -0.48 .628(n=63) (9.3)
>4doctorconsultsduringthepastyear/<4consults 45.8 -3.83 1.21 -0.16 -3.16 .002(n=130) (10.7)
Highriskdrinking/lowerriskdrinking 48.5 0.08 1.92 0.00 0.04 .966(n=50) (10.7)
Currentsmoker/non-smoker 46.6 -3.35 1.60 -0.10 -2.90 .037(n=70) (12.3)
Age-45yearsandover/<45years 50.4 4.44 1.12 0.19 3.95 .000(n=295) (10.6)
Highestgradesofemployment/lowergradesofemployment 50.0 -0.20 1.50 -0.01 -0.13 .894(n=81) (10.4)
MultipleR=.282;R=Square.080;AdjustedRSquare=.062Predictors:(Constant),Additionalinsurance;Livingalone;Hospitalisations;Doctorconsultations(>4peryear);Riskdrinking;Smoking;Age45yearsormore;Highestgradesofemployment.1. Dependentvariable:MentalComponentSummary(MCS)score.Standarddeviationinbrackets;OmnibusF=4.443;SignificanceF=.001.2. ThecoefficientofcorrelationindicatesanassociationbetweentheMentalComponentSummaryscoresandthepredictorscores. Theminussignindicatesanegativeassociation.
1SF–36 MEntalcoMPonEnt
SuMMaryScorE (Sd)
2unStandardiSEdcoEFFiciEntS
ModEl
variaBlE
StandardiSEdcoEFFiciEntS
t Sig
B Std. Error BEta
Table 11: Factors influencing mental component summary scores: multiple regression analysis
The regression analysis for mental component summary(MSC)scores(Table11)indicatedthatthebestmentalhealthstatus was found in employees who had health insurance(+0.63), lived with a partner (‘lived alone’ –1.48), had notbeenhospitalisedinthepastyear(‘hospitalised’–0.78),hadfewerthanfourmedicalconsultationsinthepastyear(‘>4doctorconsults’–3.83),engagedinriskdrinkingbehaviour(+0.08), did not smoke (‘smoked’ –3.35), were 45 years ofageormore(+4.44),andwerenotinthehighestgradesofemployment (‘higher grades of employment’ –0.20). Theworstmentalhealthwasfoundinemployeeswhovisitedamedicalpractitionermorethan four timesduringthepastyear,smoked,livedalone,werehospitalisedinthepreviousyearandwereinthehighestgradesofemployment.
discussionThis study found that UNE study participants reportedlower (poorer) mental health status than the sub-group‘norm’ for Australian employed persons. Interviews with arepresentative sample of university staff, from executive,management and employee levels, suggested that thisdifferential in mental health status was associated withsocialrelationships intheworkplacethathaddeterioratedinrecentyearsowingtohigh levelsofwork-relatedstress.[21]
Mystudyalsofoundvariationinphysicalhealthandmentalhealthstatuswithintheemployeegroupbasedontypeofwork, grade of employment, health insurance status, ageanddomesticlivingarrangements.
58 AsiaPacificJournalofHealthManagement2006;1:2

HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
For example, the academic staff at UNE reported betterphysicalhealththandidUNEgeneralstaff.Surveyparticipantsundertheageof45years,inhighergradesofemployment,those with medical insurance and those who lived with apartner reported better physical health than those olderparticipants, or those in lower grades of employment, orthosewithoutmedicalinsuranceorthosewholivedalone.Similarly, employees without health insurance and thosewho lived alone reported poorer mental health status. Ontheotherhand,thoseinthehighergradesofemploymentreportedpoorermentalhealthstatus.
Thesevariationsinmeasuresofphysicalandmentalhealthare consistent with the notion of ‘stratification’ of healthstatus as described by Comino and Howell (1999), whoclaimedthatone’spositioninsociety’seconomichierarchyis the most powerful determinant of health status, withthose people with more resources having better healthstatusthanthosewith fewerresources. [1]Stratificationofhealthstatusoccursnotonlyinsocietyatlarge,[1]butalsointheworkplace,asMarmotetal(1984)foundinBritainintheWhitehallstudies.[2]MystudylendsAustraliansupportto the phenomenon. The present study also found thatliving alone was a sociodemographic variable associatedwith poorer health status – a factor previously recognisedin the general population by the NSW Health PromotionSurvey.[1]
Employment in the tertiary education sector is usuallyassociatedwithwell-educatedemployeesgainingaregular,reasonable income and working in clean, comfortableconditions of employment – all factors associated with afavourablehealthstatus.Consideringthetheoreticalhealthadvantages of high-quality employment and constancy ofgoodincome,onewouldexpectemployeesofthetertiaryeducation industry to have a better health status thanemployeesingeneral.However,thisstudyidentifiesmentalhealth problems as particularly important for employeesin this industry, which is consistent with the findings ofWinefieldetal(2002)asindicatedintheIntroduction.[3]MystudygoesfurtherthantheWinefieldetalstudy, inthat itinvestigatesthephysical,aswellasthemental,healthstatusof university employees and explores factors associatedwithvariationinhealthstatus.
Not surprisingly, I found a significant association betweenhealth status (physical and mental) and utilisation ofhospitalandmedicalservices,withcomparativelyhighusersreportingpoorerhealth.
However, some of the findings related to health riskbehaviours (smoking and drinking) were unexpected andincludetheassociationbetween1)at-risklevelsofsmokingand better physical health scores, and 2) at-risk levels ofdrinkingandbettermentalhealthscores.Reasonsfortheseunexpected findings are not known. The influence of riskdrinkingonmentalhealthforaworkingpopulationneedsfurtherresearch.
This study supports the findings of previous researchersand offers insights into causes of mental health problemsin the tertiary education sector.The findings also suggestthateffectiveandefficienthealthpromotionprogramsarepossible. At the organisational level these programs couldincludepreventionstrategiesdesignedtoreduceworkplace‘stress’, early intervention and rehabilitation programs. Atthepersonallevel,interventionscouldbetargetedatthosewho live alone, exhibit risk-drinking behaviour, or needrehabilitationassistanceafterhospitalisation.
conclusionsVariationinhealthstatusamonguniversityemployeesbasedonsociodemographicmeasuresposesanimportantpublichealthchallengeforthoseconcernedwithmaintainingandpromotingthehealthofthisworkforce.ThisstudyprovidesabasisforthedevelopmentandevaluationofappropriatementalhealthpromotionprogramsattheUniversityofNewEnglandandraisesquestionsforfurtherresearchtoexploretheneedforsimilarprogramsinotherAustralianuniversitiesandpublicsectororganisations.
acknowledgementsThis research ispartof theauthor’s thesis‘Thehealth thatworkerswant’,passedwithcommendationsin2005tofulfillrequirementsfortheDoctorofHealthServicesManagementattheUniversityofNewEngland.DrLeighLehaneassistedwiththepreparationofthepaper.
competing interestsTheauthordeclaresthatshehasnocompetinginterests.
AsiaPacificJournalofHealthManagement2006;1:2 55

HealthStatusofEmployees:defininginfluencesonhealthinthetertiaryeducationindustry
references 1. CominoE,HowellS.SectionI:Thefacts.In:HarrisE, SainsburyP,NutbeamD,editors.Perspectivesonhealth inequity.Sydney:TheAustralianCentreforHealthPromotion; 1999.2. MarmotMG,ShipleyMJ,RoseG.Inequalitiesindeath-specific explanationsofageneralpattern?Lancet.1984;May5.1(8384): 1003-6.3. WinefieldAH,GillespieN,StoughC,DuaJ,HapuararchchiJ. OccupationalstressinAustralianuniversities:anationalsurvey 2002.Canberra:NationalTertiaryEducationUnion;2002. p.1-102.4. WareJE.TheSFCommunity–SF-36healthsurveyupdate. Availablefrom:http://www.sf-36.org/tools/SF36.shtml (Accessed24/07/06).5. PatrickDL,EricksonP.Healthstatusandhealthpolicy: qualityoflifeinhealthcareevaluationandresourceallocation. NewYork:OxfordUniversityPress;1993.6. GandekB,WareJE.IQOLAProject.JClinEpidem.1998; (NovemberSpecialIssue);p.1-324.7. HemingwayH,NicholsonA,StaffordM,RobertsR,etal. Theimpactofsocioeconomicstatusonhealthfunctioning asassessedbytheSF-36questionnaire:TheWhitehall11Study. AmJPubHealth.1997;87(2):1484-91.8. MallinsonS.Listeningtoinformants:Aqualitative assessmentoftheShort-Form36HealthStatusQuestionnaire. SocSciMed.2002;54:11-21.9. KoukouliS,VlachonikloisIG,PhilalithisA.Sociodemographic factorsandself-reportedfunctionalstatus:thesignificance ofsocialsupport.BMCHealthServicesRes.2002;2(1):20-33.10.GoldbergDP,WilliamsP.Auser’sguidetotheGeneralHealth Questionnaire.London:NFER-NELSON;1988.11.AustralianBureauofStatistics.Nationalhealthsurvey:SF-36 populationnorms.Canberra:AGPS;1995.12.McHorneyCA,WareJE,RaczekAE.TheMOS36-itemshort formhealthsurvey(SF-36):11psychometricandclinical trialsofvalidityinmeasuringphysicalandmentalhealth constructs.MedicalCare.1993;31:247-263.13.WareJE,KosinskiM.SF-36physicalandmentalhealth summaryscales:amanualforusersofversion1.Lincoln: QualityMetricIncorporated;2001.
14.RankinD,CormackM.Medicare,healthcareinsurance, compensationandliabilityissues.In:CourtneyM,BriggsD, editors.Healthcarefinancialmanagement.Sydney:Mosby Elsevier;2004.p.123-40.15.AustralianInstituteofHealthandWelfare.Nationaldrug strategyhouseholdsurvey.Canberra:AGPS;2001.16.AustralianBureauofStatistics.Statistics–Tasmania:health, healthriskfactors,alcohol,harmfuluseofalcohol. Canberra:AGPS:2002.17.SPSSInc,Statisticalpackageforsocialscience,(SPSS)® Version10.0.Chicago:SPSSInc;2000.18.WareJE,SnowKK,KosinskiM,GandekB.SF-36Health survey:manualandinterpretationguide.Lincoln:Quality MetricIncorporated;1993,2000.19.HeardL,HarrisLM.Experimental,quasi-experimentaland correlationalquantitativeresearchdesigns.In:Minichiello V.SullivanG.GreenwoodK.AxfordR.editors.Handbook forresearchmethodsinhealthsciences.Sydney:Prentice Hall;1999p.119-120.20.CookseyRW.Statisticsforbehaviouralandsocialsciences: adescriptivehandbook.Armidale:UniversityofNew England,1997p.76.21.DittonMJ.Theimportanceofsocialrelationshipsinthe workplace.Forthcoming2006.
60 AsiaPacificJournalofHealthManagement2006;1:2

introductionTheprevalenceofdiabetesisincreasinginNewZealand.Itisestimatedthattherewere147,000peoplewithdiabetesin2000andthatby2010therewillbe180,000.[1]Arangeofstakeholdersneedtobeengagedifhealthsystemsaretomeetthedemandsbeingplacedonthembydiabetes.[2]Atthesametimeahighlevelofsystemintegrationisrequired.Thisraisesquestionsabouthowstakeholdersengagewithoneanothertoproduceeffectiveintegratedmodelsofcare.
Degeling has documented differences between themajor professional sub-cultures in the health systemand the implications of these for the modernisation,clinical governance and quality agendas. [3,4] Managerspredominantly operate within a systems view and apopulationperspectiveincontrasttomedicalclinicianswhodemonstrate an individual patient ethic. Identifying theseprofessionalsubculturesastribes,Degelingclaimsthatitisthe‘destructiveantagonism’thatoftenexistsbetweenthesetribesthatcancauseattemptstointegratecaretofail.[4]
abstractObjective: To identify barriers to integrated care for diabetes services at the District Health Board/Primary Health Organisation interface, along with possible solutions to these barriers.
Design: Qualitative and interpretive using semi-structured interviews and a modified Delphi technique to collect data. A general inductive approach was used for data analysis.
Setting: Fourteen participants were recruited from one of the three Auckland, New Zealand district health boards (DHBs) and three of the primary health organisations (PHOs) located within the DHB district.
Results: The main barriers to integration identified were a lack of collaborative skills in the workforce, a lack of resources and a lack of time for stakeholders to integrate care. Study participants from each of the major professional subcultures (medicine, nursing
Hadley J Slade-JonesBHSc,MPHBusinessManager,PrimaryCareDevelopmentCountiesManukauDistrictHealthBoardSouthAuckland,NewZealand.
rod PerkinsBDS,MHA,PhD,FCHSESeniorLecturerinHealthManagementHealthSystemsGroup,SchoolofPopulationHealthTheUniversityofAuckland,Auckland,NewZealand
John WellinghamMBBS,BSc(Hons),DCH,PGDipBus,MRCP,FRNZCGPPrimaryCareAdvisorWaitemataDistrictHealthBoardTakapuna,Auckland,NewZealand
Correspondence:[email protected]
ManagEMEntPr ac ticE
integrating diabetes Services: opportunities to build cultural bridges HJ Slade-Jones, r Perkins, J Wellingham
and management) identified different barriers to integration and this divergence of views was identified as a further barrier to integration.
Conclusions: The research identified three possible solutions. The first was the creation of a work space to allow clinical staff from different sectors to build cultural bridges. The second was for funders to identify ways of being perceived by all stakeholders as adding value to the integration process and the third was the development of a funding environment supportive of integration.
Abbreviations:CEO–ChiefExecutiveOfficer;DHB–DistrictHealthBoard;IPAs–IndependentPractitionerAssociations;PHOs–PrimaryHealthorganisations.
Keywords:Diabetes,chronicillness,integration,professionalsub-cultures.
AsiaPacificJournalofHealthManagement2006;1:2 61

Independent Practitioner Associations (IPAs) began toappear in New Zealand in the early 1990s and were theprecursors to the current structures based on PrimaryHealth Organisations (PHOs). IPAs were groups of generalpractitioners that acted collectively to negotiate nationalservice contracts and budget holding arrangements. [5]ThishasledtogeneralpractitionersinNewZealandbeingrelativelymorepowerfulandactiveinthedecisionmakingprocesses of their organisations than their hospital-basedcolleagues.
Anexceptiontothissituationisspecialistphysiciansworkinginprivateclinics.Thisisbecausetheyhaveafinancialstakein the clinics they work from.They do not have the sameconstraintsonthemasdoctorsworkinginpublichospitalsandtheyarebetterplacedtobeabletoworkwithgeneralpractitioners.
With these dynamics in mind this research sought toprovideananalysisofthebarriersandpotentialsolutionstointegratedcarefordiabetesinNewZealand.Theobjectiveof this study was to identify ‘Barriers to integrated carefor diabetes services at the District Health Board/PrimaryHealth Organisation interface and possible solutions tothesebarriers’.
MethodsFourteenparticipantswererecruitedfromoneofAuckland’sthree District Health Boards (DHBs) and three PrimaryHealthOrganisations(PHOs)locatedwithintheDHBdistrict.Participants represented key stakeholders in a verticallyintegrated model of care. [8] The sampling method forthe first stage of data collection was ‘intensity’ sampling.Accordingly,researchparticipantswereidentifiedbasedonbeingdata-richintheareaofintegrationandthedeliveryofdiabetesservices.[9]TheChiefExecutiveOfficer(CEO)fromoneoftheparticipatingPHOsrecommendedsixparticipants.Criterion sampling and Opportunistic sampling were bothusedtoidentifytheeightparticipantsforthesecondroundofdatacollection.Criterionsamplingrequirestheresearchertodevelopalistofcriteriathatallresearchparticipantsmustmeetinordertobeincludedinthestudy.[10]Opportunisticsampling permits the inclusion of study participants whoarediscoveredastheresearchprogressesprovidedtheyalsomeetthepre-determinedcriteria.[10]
A modified Delphi technique was employed for thecollection of data. [6] This is a method of collecting andsynthesising opinions in response to a question to gaina consensus view. A conventional Delphi study utilises a
series of questionnaires to gather opinions from researchparticipants. The opinions from all participants are thencategorisedandre-circulatedtoeachparticipant for themto rank their agreement. This process continues until theresearcherassesses thatahighenough levelofconsensushasbeenobtained.Thismethodwaschosenas itenabledtheinquirytogetbeyondsuperficialresponsesandintothecomplexities of the participants‘attitudes, behaviours andexperiences’.[7,p.378]
Threeroundsofdatacollectiontookplace.Thefirst roundof data collection utilised semi-structured interviews withthequestionsinformedbythecurrentliteratureonbarriersandsolutionstointegratedcare.Thesecondroundofsemi-structured interviews involved a different set of researchparticipants.These interviewquestionswerebasedontheresponsesfromthefirstroundof interviews.ThethirdandfinalroundofdatacollectionhadtheparticipantsfromthesecondroundofinterviewsranktwentydistinctbarrierstointegrationintermsofimportanceonaLikertscalefromonetofive(1=veryimportantbarriertointegration,2=importantbarrier to integration, 3=neutral, 4=unimportant barrierto integration, 5=very unimportant). The list of barriersused in the third round of data collection was derivedfromparticipants’responsesduringthefirsttworoundsofinterviews.
A general inductive approach was used for data analysisof both sets of interviews. This approach calls for theresearcher to identify recurring themes appearing in theraw data before grouping similar themes into categoriesonwhichamodelortheorycanbeproposed.Thethemedcategories were determined inductively, ie they werederived from the raw data rather than from the researchobjectives. The transcripts were coded into themedcategories. Four categories emerged and each had sub-categories.Adetailedsystematicanalysiswascompletedbythe researcher that included the interpretation of phrasesandverbalinteractionstoidentifyunderlyingmeanings.Thebarriersthatparticipantsinvolvedinthethirdroundofdatacollectionrankedonafive-pointLikertscale,wereanalysedfor levels of consensus as to their relative importance byeachprofessionalsub-group(thatisthelevelofconsensusbetween, for example, general practitioners and hospitalspecialists,managersandclinicians).[11]Thiswasdonebyaggregatingtheparticipant’sresponsesandcalculatingthemedianandinter-quartileranges.
IntegratingDiabetesServices:opportunitiestobuildculturalbridges
62 AsiaPacificJournalofHealthManagement2006;1:2

resultsThe sample population included two hospital specialists,onehospitalnurse,threehospitalmanagers,threegeneralpractitioners,twocommunitybasednursesandthreePHOmanagers.
The main barriers to integration of diabetes servicesidentifiedwere:
• Anabsenceofcollaborativeskillsamongmembers oftheworkforceresponsibleforservicedeliveryacross allsectors;
• Insufficienthuman,systemsandfinancialresources insomesectors;and• Alackoftimeforstakeholderstoworktowardsan integratedmodelofcarewhilstmanagingcurrent workloads
Further, each professional group (professional subculture)identifieddifferentbarriers.
collaborationCliniciansandmanagersbothidentifiedpoorrelationshipsbetweenkeystakeholdersasamajorbarriertocollaboration.Managers perceived clinicians as poor team players whilecliniciansviewedmanagersas loyal toasystemthatoftenpromisedmuchbutfailedtodeliver.
Clinicians described relationships from an individualisticperspective,oftenintermsofwhatotherstakeholdersweredoingwrong,whatfrustratedthemandconsequentlywhatdamagedtheirrelationshipswithothers.Theywerefocussedon their own problems which resulted from the existingsystem, rather thanconsideringhowtheycouldchallengethesystemandbecatalystsforpositivechange.Incontrast,managersindicatedabroaderandmoresolution-focussedattitude to the current state of stakeholder relationships.However,theydidnotunderestimatethechallengesahead,onestating:
Historically general practice has always been disorganised. They are hard to engage with, the advent of PHOs may address this, but we are yet to see it.
Community-based and hospital-based clinicians hadcontrasting views. General practitioners viewed the needsof patients differently from specialist physicians, oneobserving:
Hospital doctors (specialists) hold onto patients when they should refer to us.
However,onespecialistconsideredtheroleofspecialistsasundervaluedbygeneralpractitioners.Hisopinionwasthatgeneralpractitionerssawspecialistsastoofarremovedfromthecoalfaceandpickingandchoosing,toacertainextent,thecaseloadstheytookon.
Patients were stated to play a key role in stakeholders’relationships.Thecontrolofthetreatmentplanandbenefitsthatfollowfromtheassociatedfundingcouldworkagainsteffective collaboration. The decision to refer or not wassometimesmadeinresponsetofinancialratherthanclinicalconsiderationsbydoctors.Whenthisoccurreditwassaidtoactasabarriertocollaboration.
Managers referred to a desire for all stakeholders to beteam players and identified the need for them to sharegoals. Clinicians also spoke about having common goalsandsuggestedeveryoneshouldbefocussedonindividualpatients. This was in contrast to managers who identifiedwithpopulationhealthgoals.
resourcingThe two funding mechanisms operating in the NewZealandpublichealthservicesectorarefee-for-serviceandcapitation.Managerswantedproviderstobepaidaccordingtothequalityoftheservicestheyprovide,onestating:
We need quality payments, payments for what actually happens. You should not get paid for the number of people you treat.
Cliniciansviewedthis issuedifferently.Theyheldthattheyneeded to spend extra time with patients with chronicillnesses to fully meet their needs.They said that this hadtheeffectofworkingagainsttheincentivescreatedbythesignificant fee-for-service funding arrangement that manyofthemworkedwith. Ratherthanmakinga linkbetweenfunding mechanisms and quality, clinicians blamed theexisting funding system for their inability to work inintegrated ways. They identified fee-for-service as notworkingtowardsmeetingtheneedsof theirchronically illpatients,onestating:
I have a busy surgery, when I do things the way I think they should be done I get half the income of a normal day.
This view was evident in statements made by all generalpractitioners,anotherobserving:
All problems come back to the amount of money (we are paid).
IntegratingDiabetesServices:opportunitiestobuildculturalbridges
AsiaPacificJournalofHealthManagement2006;1:2 63

Participants talked about money in terms of the amountoffundingthatwasavailabletothem,ratherthanfundingconstraintsoverallandtheopportunitycostofre-allocatingfunding across the sector. Notwithstanding, one saw thehospital system as having more money than it deserved,observing:
Hospitals are over funded, …have been for years and that money needs to be shifted to general practice.
Managers from both PHOs and hospitals acknowledgedthat themovementof funds fromhospitals tocommunitybasedprovidersofclinicalservicescouldbeadvantageoustointegration.Howeverincontrasttogeneralpractitioners,theysawreallocatingmoneytotheseprovidersascreatingnewsetsofproblems.Onehospitalmanagerstated:
If I say that I have a model of care that will allow the hospital to close half a ward, that has a ripple effect. It will affect the viability and funding for all the associated support services such as x-ray and labs. Their funding is woven throughout the hospital and that fabric will begin to breakdown.
timeWhile managing resource issues and managing time areinextricablylinked,theissueoftimeavailabilityintheworkinglivesofbusydoctorsandnursesisaparticularchallengetointegration and this was evident in the responses of bothclinicalgroupstoquestionsaboutit.
Clinicians and managers acknowledged the obviousimplications for time and workload management as aconsequence of integrating care. Moving to an integratedmodelofcarerequiresstakeholderstoinvestextratimeinplanningandimplementingchange.Theopportunitycostof this investment is significant for clinicians funded witha significant fee-for-service component. This group feltthattheyweretakenforgrantedintheprocess.Theywereexpected to pick up new work and adopt new practiceswithoutappropriatesupportandresources.Cliniciansfromgeneralpracticeandhospitalbasedpracticestatedthattheywereperceivedashavingtimetosparebyothers,whiletheirreality was of being overloaded, one general practitionerobserving:
The incorrect perception is that GPs have a lot of slack time to pick up extra work with no extra funding…we are perceived as having time on our hands, which is not the case.
The major issue, according to clinicians, was that they arepartofaworkforcethatistoosmalltodothenecessarywork.
Generalpractitionersbelievedthatboththegeneralpracticeandhospitalsectorsdidnothaveenoughindividualsatthefrontlineofservicedelivery,oneobserving:
We need more nurses, more receptionists…and we do not have enough experts.
Managers,incontrast,talkedaboutservicequality,notthequantityoftheavailableworkforceandofferedthefollowingsolution:
The issue is not the number of providers and staff; it is making sure that they have the capabilities and competencies to deliver services.
Further,managersdescribedintegratedmodelsofcarethatprovided the opportunity to help ensure health workersskillswereutilisedthebestwaytheycouldbe,forexampleusing nurses for clinical work rather than as receptionistsand administrators, in order to obtain the highest level ofoutput in relation to an individual’s skill sets. Managersbelieved the change agenda would positively impact onotherstakeholders’workloads.
discussionPrincipal findingsThemainfindingsofthisresearchare:
• Stakeholdersdifferfromoneanotherintheirperception ofbarrierstointegrationofdiabetesservicesinthe healthdistrictinAuckland;
• Cliniciansandmanagersareoperatingoutofdifferent paradigmswhichinfluencetheirperceptionsregarding theimportanceofintegrationandthewaytowards integratingmodelsofcare;and
• ThemajorbarrierstointegrationinNewZealandare closelylinkedtostakeholderrelationships,funding,and theworkloadsofstakeholders
Strengths and weaknesses of the studyThe New Zealand health system has a recent historyof large scale structural reform. As a result of reform,throughout the1990sclinicianshavebecome increasinglyresistant to change and mistrusting of health managers.[4] The relatively small sample size in this case study andthe fact that itwas limitedto theAucklandregion inNewZealand is a limitation. Notwithstanding this, the conflictsbetween professional subcultures that Degeling et alrefer to are evident in this research. [3, 4] In this study,clinicians observed that managers often failed to deliveronthepromisestheymade.Meanwhilemanagersbelievedclinicians were too focussed on individual patients (rather
IntegratingDiabetesServices:opportunitiestobuildculturalbridges
64 AsiaPacificJournalofHealthManagement2006;1:2

thanthepopulation)andoperatedoutsidethecontextofateam.Thesecontrastingperspectivesareasourceoftensionthatthreatensintegration.
Meaning of the studyIn order to build integrated models of care, the barriersdiscussed above need to be overcome. The solutions tosuchcomplexbarriershavenotyetbeenfoundinanyonestakeholderparadigm,andthereisnoreasontobelievethattheywillbe.Inthisresearchitappearsthatthebarriersthatexistbetweencliniciansandmanagersmaybelargerthanthe barriers between clinicians based in the communityand clinicians based in hospitals. Because of the ongoinginfluence of the IPAs on PHO structures, community-basedcliniciansaremoreeasilyabletodrivemanagementdecisions within their organisations than hospital-basedclinicians.Managementislessdominantincommunitycarethanit is inhospitalcare.An‘easywin’togainmomentumfor integration may therefore be to create additionalopportunitiesforcommunityandhospital-basedcliniciansto work more closely together on strategies to integratecare.
Interviewees said that the current environment makes itdifficultforindividualstoframeuptheirideasandopinionsand present them to others. This is particularly so forcommunity-based general practitioners. It is not alwaysclear to the individualwhotheyshoulddiscuss ideaswithandwhatifanyprocessforstagingsuchdiscussionsexistsintheirorganisation.Clearly it is importantthatstakeholdersacknowledge the different, but equally valid, perspectivesofothers.
Where the opportunity exists to create forums to enableintegration discussions to occur, early efforts could gotowards facilitating the community and hospital basedmedicalgroupsbuildingculturalbridgesandunderstanding.This would provide for a stronger starting point for moreformaldiscussionstomoveforwardwithmanagersinbothsectors.Whenclinicianshavetakenownershipoftheissuesandpossiblesolutions,theyaremorelikelytobeinapositiontocontributepositiveattitudesaboutintegration.
However, having a relevant forum for discussion will notbe sufficient as it requires more than the professionalsubculturessimplyworkingalongsideoneanother.Toturnaforumintoacatalystforintegration,itsmembersmustbewilling to collaborate, be solution focussed, and have thepotentialtomodifyfundingmodels.Thiswillrequirestrongclinicalandmanagementleadership.
The importance of strong clinical leadership as a criticalfactor in integration is a common theme in the literatureand would, for example, assist in overcoming the currentreluctance of clinicians to address the skill mix in clinics.[12,13] Whilst reinforcing this need, Bodenheimer andWagner have also identified the alignment of fundingmodelsasacriticalfactorforsuccess.[14]Thisisaparticularchallenge in health system models with funding streamsrunning in silos; and achieving this will, in turn, requirestrongandinnovativemanagementleadership.
Twopotentialopportunitiesarisefromtheseconcepts.Firstly,privatelyfunded,community-basedclinicalleadersmustbeenabledtoparticipateinthedesignanddevelopmentworkoftheforum.Funderscouldcontributetothisbyprovidingresourcestopurchasecommunitybasedcliniciantime,andtobackfilltheclinicswhichstillhavetomaintain‘businessasusual’.
Asecondopportunityisforfunderstoplayagreaterroleinfacilitating the change management processes, which willarisefromforumdecisions.Akeyissuehereisthepotentialuncertainty over the extent to which management feespaidtoPHOsshouldbeusedforthispurpose.Fundersandproviderswillneedtobeclearastohowthismoneyshouldbeusedandhowthefacilitationcanbejointlyresourced.
The amount of funding available and the mechanismsof funding service provision were also major barriers tointegrationidentifiedinthisresearch.Withoutasupportivefundingenvironmentintegrationcannotbeachieved.[15]Asuitablefundingenvironmentfor integration isonewherefunding is pooled across stakeholders rather than siloedaccordingtoindividualstakeholder’sdomains.[16]
If the resistance to devolving funding from hospitals tocommunity-basedcareistoogreat,thennewfundingbeinginvestedincommunity-basedcareshouldbeconsideredforintegrationinitiatives.Whilstnewfundstoreducethefee-for-servicecomponentthatpatientspayforexistingservicesreduces financial barriers to access services, it does notcontributetointegration.Ifqualityofcareisalsoimportant,then new money should not simply be used to subsidiseaccess, it shouldgo towards increasing integrationand, inturn,qualityofcare.
Aforumconsistingofclinicalchampionsandotherrelevantprofessional groups could work on integration goals andprocesses including mechanisms for providing pooledfunding for which all could be held responsible. It is one
IntegratingDiabetesServices:opportunitiestobuildculturalbridges
AsiaPacificJournalofHealthManagement2006;1:2 65

possiblesolutiontothecurrentlabouredandcumbersomemovement towards integrated care. This implies that anintegrated programme needs integrated governance.This research suggests that for this to be effective anunderstanding of professional sub-cultures is critical forunderstandingeachprofessionsresponsetothechallengesof integrated care and the changes those challenges maynecessitate.[4]
Unanswered questions and future researchThisresearchhaslookedatthetensionsbetweencliniciansandmanagerswhenintegratingcare.Amorein-depthstudyof the tensions between professional sub-cultures such ascommunity based clinicians, community based managers,hospital based clinicians and hospital based managerswhenintegratingcareandhowtomanagethosetensions,would provide valuable evidence to support the redesignofdecision-makingprocessesinordertojointlybuildtrulyintegratedpatientservices.
conclusionThis research has identified three action points for furtherintegratingcare.Thefirstisthecreationofappropriateworkspaces to allow clinicians from different sectors to buildculturalbridges.Thisbuildingofrelationshipsacknowledgesthatthebarriersbetweengeneralpractitionersandhospitalspecialistsmaybelessthanthebarriersbetweenmanagersandclinicians.
Thesecondopportunity isforfundersworkingtoadvanceintegration to act in ways that create value in the eyes ofgeneralpractitioners.Whenthesecliniciansseethevalueofintegratingcareasgreaterthanthecosttothempersonallytheywillmorereadilyparticipateinintegration.Atthispointmanagersmustdisplaythevisiontoaddresstheissueswithworkforcedesign.
The third opportunity is to create the supportive fundingenvironmentvitaltointegration.Ifresistancetoreallocatingfunds from hospitals to general practice is too great, thenfundersmustconsidertheallocationofnewfundstogeneralpracticeforservice-integration.
competing interestsTheauthorsdeclarethattheyhavenocompetinginterests.
references1. RedaE,DunnP,StrakerC,WorsleyD,GrossK,etal.Screeningfor diabeticretinopathyusingthemobilecamera:theWaikato experience.NZMedJ.2003;116:1180.
2. CoieraE.Theimpactofcultureontechnology:howdowecreate aclinicalcultureofinnovation?MedJAust.1999;171:508-509.
3. DegelingP,KennedyJ,HillM,CarnegieM,HoltJ.Professional sub-culturesandhospitalreform.Sydney:UniversityNewSouth WalesCentreforHospitalManagementandInformationSystems Research.1998,p.321.
4. DegelingP,MaxwellS,KennedyJ,CoyleB.Medicine,management andmodernisation:a“dansemacabre”.BMJ.2003;326:649-52.
5. MalcolmL,PowellM.Thedevelopmentofindependentpractitioner associationsandrelatedgroupsinNewZealand.NZMedJ.1996; 109:184-7.
6. JonesJ,HunterD.QualitativeResearch:consensusmethodsfor medicalandhealthservicesresearch.BMJ.1995;(311):376-380.
7. BowlingA.Researchmethodsinhealth:investigatinghealthand healthservices.Philadelphia:OpenUniversityPress;1997.p.378.
8. ShortellS,GilliesR,AndersonD,EricksonK,&MitchellJ.Remaking healthcareinAmerica:buildingorganizeddeliverysystems. SanFrancisco:Joey-BassPublishers;1996.p.165.
9. TaylorP.(1998).Programmedevelopmentandevaluation: sampling[online].Available:<http://www.uwex.edu/ces/pdande/ evaluation/evaldocs.html>[Accessed16/03/2004].
10. PattonM.Qualitativeevaluationandresearchmethods.California: SagePublications;1990.p.110-127.
11. PassmoreC,DobbieA,ParchmanM,TysingerJ.Guidelinesfor constructingasurvey.FamMed.2002;34(4):281-6.
12. WagnerE,AustinB,DavisC,HindmarshM,SchaeferJ,BonomiA. Improvingchronicillnesscare:translatingevidenceintoaction [online].HealthAff(Millwood).2001;20:64-79.Available:<http:// content.healthaffairs.org/cgi/reprint/20/6/64>[Accessed16/10/04].
13. ClarkeD,HowellJ,WellinghamJ,GribbenB.Integratinghealth care:theCountiesManukauexperience.NZMedJ.2003;116:1169.
14. BodenheimerT,WagnerE,GrumbachK.Improvingprimarycare forpatientswithchronicillness.JAMA.2002;288:1909–1914.
15. YoungsonR.Patient-centredhealthreformthroughclinical leadership[online].HealthcareandInformaticsReviewOnline. 1999;3:Available:<http://hcro.enigma.co.nz/website/index. cfm?fuseaction=articledisplay&FeatureID=72>[Accessed15/02/06].
16. AustralianDepartmentofHealthandAgeing.(2002).TheAboriginal andTorresStraightIslandercoordinatedcaretrials:national evaluationreport(Volume1).Mainreport2002,[online].Available: AustralianDepartmentofHealthandAgeingwebsite:URL<http:// www.health.gov.au/internet/wcms/publishing.nsf/content/health- oatsih-pubs-coord1.htm>[Accessed12/06/04].
IntegratingDiabetesServices:opportunitiestobuildculturalbridges
66 AsiaPacificJournalofHealthManagement2006;1:2

In this issue of the Asia Pacific Journal of Health Management, we asked Jim Birch a few questions on his career as a health manager and the challenges that such a role brings.
Jim has had a long and distinguished career in health management in South Australia. From early beginnings in clerical and administrative roles at the South Australian Health Commission and Royal Adelaide Hospital, Jim graduated with a Bachelor of Health Administration from the University of New South Wales. This was followed by Senior Executive roles at the Adelaide Children’s Hospital, Whyalla Hospital, Women’s and Children’s Hospital and the North Western Adelaide Health Service.
Jim left the health industry for some three years to take on the role of Deputy Chief Executive of the Attorney-General’s Department and Department of Justice. However the challenges of health lured him back to the Department of Human Services as Chief Executive. This was followed by his appointment as Chief Executive of the South Australian Department of Health, a role he fulfilled until recently. Jim has now taken up his own Consultancy practice.
Jim was awarded the College Gold Medal Award this year for outstanding achievement, his passion for leadership in health services management, professional development and education. He has particularly supported young managers and emerging leaders and has been a College stalwart especially in South Australia.
Jim Birch
i n P r o F i l E
AsiaPacificJournalofHealthManagement2006;1:2 67
1. What made you venture into health management?
Thiswasreallyanaccident. Istartedstudyingarchitecture
in 1974 and did not like it. I had always been interested
in health care and wanted to become a doctor. As it was
midyear when I dropped out of architecture, I needed a
jobtopaythebills,soIsoughtajobattheRoyalAdelaide
HospitalinfinancetotidemeoverandIgotit.
Early on in the job I was influenced by two senior people
whosaidthattherewastobeaboominhealthcareinthe
futureandactuallyrunningthehealthsystemwouldbea
lotoffun.Iwasencouragedtostudyhealthadministration
andas Ienjoyedthe lifearoundthehospital, Idecidedto
doso.Sothereendedamedicalcareerbeforeitstartedand
therecommencedmyhealthmanagementcareer.
2. What is the most rewarding and enjoyable aspect of your position?
Without doubt the occasion where you have been
responsibleforareformoranewservicethathasworked
wellandhasbenefitedpeople.Theabilitytohaveamajor
influenceatasystemlevelhasbeenarealbuzz.
3. What is the greatest challenge facing health managers?
Ithinkthattheabilitytoremaininnovativeandpositivein
thefaceofrelentlessdemandsuponthemfromallquarters.
That included the general public, the media, politicians,
staffandtheirownfamilies.ItisarelentlesspressurethatI
thinkisexactingatollonpeople.
4. What is the one thing you would like to see changed?
In health care I would like to see a much more serious
investmentandsupportofprimarycareandprevention.

68 AsiaPacificJournalofHealthManagement2006;1:2
JimBirch
5. What is your career highlight?
Ithinkthattherearetwoequalonesbutforentirelydifferent
reasons.ThefirstwastheGenerationalHealthReviewandits
subsequent implementation.Thesecondwasthecreation
oftheWomen’sandChildren’sHospital.
6. Who or what has been the biggest influence on your career?
Ibelievethatearlyexperiencesincommunityhealthwitha
focusuponpreventionwereveryimportant.JohnYufrom
NSW and Australian of theYear was extremely influential
because of his passion for the interests of children.There
havebeenmanygreatpeoplethatIhaveworkedwithand
allintheirownwayhavecontributed.
7. Where do you see health management heading in ten years time?
I hope that it heads towards a relentless focus on what is
bestforthebenefitofsocietyandmoreactivelychallenges
pressure groups and individuals who are self interested. I
donotbelievethat there isenoughfocusonhowwecan
improvehealthandthiswillbecomeevenmoreimportant
withageingandtheincreaseinchronicdisease.
8. What word of advice would you give to emerging health leaders?
Iwouldaskthemaquestionfirst?Whydotheywanttobein
thiscareer?Ifitissimplyajob,ormoneyorprestige,thenI
wouldadvisethemtofindanotherjob.Iftheyhavepassion
andempathyandwanttomakeadifference,thenstickwith
itastherideisworthit.
Managing Health Services: Concepts and Practice – 2nd Edition
Mary g Harris and associatesSociety for Health Administration Programs in Education Australian College of Health Service Executives
ManagingHealthServices:ConceptsandPractice2ndeditionprovidesavaluablepracticeresourceforhealthservicemanagementstudentsandmanagers.Whilenewconceptsandstrategiesofmultidisciplinaryhealthservicemanagementandleadershiphavebeenadded,thefocusremainsonprovidingcomprehensivecoverageofmanagementtopicsandissuesfacedbyhealthservicesmanagers.
Thetextisarrangedaccordingtosixmajorthemes–healthservicemanagersandthechangingorganisationalcontext;healthservicemanagementpractice–workingwithpeople;healthservicemanagementpractice–workingwithinformation;healthserviceorganisations;improvingorganisationalperformance;andcasestudiesinhealthservicemanagement.
Writtenbyover40healthservicemanagementacademicsincooperationwiththeSocietyofHealthAdministrationProgramsinEducationandtheAustralianCollegeofHealthServiceExecutives,ManagingHealthServices:ConceptsandPractice2ndeditioncontinuestomakeavaluablecontributiontohealthservicemanagementtheoryandpractice.
To order your copy of this book please contact: Elsevier australia customer Service• Phone1800263951• Fax0295178950• Email:[email protected]• Quotethefollowingcodenumberandreceive 10%discountandfreedeliverywithinAustraliaand NewZealand• CodeNumber:HPHMG1005WPubSept2005•ISBN0729537595•PB•496pp•MosbyA$79.95•NZ$94.50Mosby is an imprint of Elsevier Australia
outstanding Features:•Includesawiderrangeofshortcasestudies fromtheAsia-Pacificregion•Eachchapterincludeslearningobjectives,short casestudies,references,additionalreading& websites,conclusions,anddiscussionquestions •Increasedintegrationofpracticalissuessuch asstrategiestofacilitatemanagerand organisationallearning,workforceplanningrecruitmentandretentionstrategies,strategies toassessandmanagerisk,andstrategiesto improveorganisationalperformance. •Providesupdatesofconceptsandpractice includinggovernmentpolicychanges;advances inmedicalandinformationtechnology;changesinconsumerneedsandexpectations;advancesinhealth servicemanagement;andtheuseofresearchandevaluationtoadvancemanagementpractice.

What are the principles that should underpin a health financing system?
1Equity and access:Shouldallowequitableaccesstoallmembersof thecommunityregardlessofwheretheyliveortheirindividualmeans.
Provide quality services: Provide a level of funding thatallowsagoodqualityofservicetobedeliveredtoastandardthatmaintainsandimproveshealthoutcomes.
Cost effective service:Provideafundingmodelthatallowsfor improvedhealthoutcomesforboththeindividualandthecommunity.
Accountable: Shouldprovidetransparencyandaccount-abilitytothecommunityaroundtheresources itallocatesandtheoutcomesassociatedwiththeseresources.
Equitable:Toensurethecommunityisreassuredthatthereisanequitabledistributionofresourcesacrossallmembersofthecommunitywithoutanyinterestgroupsupportedtotheexclusionofothers.
Sustainable: Needs to ensure that the funding providedcanbemaintainedoverasustainedperiodandiscapableof responding to the changing dynamics of populationgrowthandageing,aswellasanynewhealthchallenges.This may become the basis for a long-term, population-basedresourceallocationmodel.
Workforce:Shouldensurefundingissufficienttoattractandretain a workforce to deliver the services the communityrequires.
Forward looking and flexible:Shouldensureresourcesareallocatedwithinasocialpolicyframeworkandareabletoaddressemergingneeds,ratherthanbeingsimplybasedonanhistoricalallocationmodel.
Service delivery: Support a balanced range of servicesacross the primary health and specialist hospital sector,rather than investing predominantly in one sector. Thiswould better support the range of services demanded bythecommunity.
Theoverallroleofafinancesystemisoneofsupportingtheoverallaccountabilityanddeliveryofthehealthsystem.
Mr clete MathewsBBus,FCHSE,CHEDirector Finance & Corporate Services
Drug and Alcohol Office – WesternAustralia
2Equity:Shouldassistinreducingdisparitiesinhealthaccess or outcomes, or at the very least not causefurtherdisparities.
Cost effectiveness: Should promote efficiency in servicedelivery,andfundaccesstoservicesthatdoactuallyimprovehealthoutcomes(atindividualandpopulationlevels).
Appropriateness: Should fund access to services that thepublicwillaccept.
Accountable: Should foster engagement with the publicit serves, in respect of resource allocation and serviceplanning.
Fairness:Shouldensureallpartsofthecommunityfeeltheyarefairlytreated,andthataccessisresponsivetoneed.
IneachissueoftheAPJHMweaskexperiencedhealthmanagersthroughouttheAsiaPacificRegiontoreflectonanaspectofhealthmanagementpractice.InthisissueoftheJournal,ourselectedparticipantshaveaddressedthreequestions:
1. What are the principles that should underpin a health financing system?
2. Has quality of health care improved over the past five years? If yes, what are the key drivers? If no, what are the main barriers?
3. What has been achieved from Council of Australian Government’s (COAG) health workforce reforms?
Q ’ S & a’ S
Principles that should underpin a health financing system; improvements in quality of health care over the past five years; council of australian governments (coag) health workforce reforms
AsiaPacificJournalofHealthManagement2006;1:2 69

Q’sandA’s
Forward looking: Should ensure resources are distributedwith health and social policy goals in mind, rather thansimplymaintaininghistoricallocationpatterns.
Sustainable:Shouldensurefundinglevelsandsourcescanbemaintained in the longterm, in the faceofpopulationgrowth,ageingandtheburdenofchronicdisease.
Workforce:Shouldensurefundingisatahighenoughleveltoattractandmaintainthedesiredstaffnumbersandmix.
Balanced: Should reflect the right balance between‘upstream’ (primary, community) and ‘downstream’(specialist,hospital)investment.
Integrated:Shouldensure‘wholesystem’planning,deliveryandaccountability.
Mr chris Mules BA(Hons),AFCHSE,CHEChief Planning & Funding Officer
Counties Manukau District Health Board–NewZealand
3Above all, the system must be accountable toits expectations so as to justify its existence. Themost important principle is therefore the system’s
accountability.Thebetterthesystemdoesonthisprinciple,the greater legitimacy it has. As a consequence, publicsupport for the system would be substantiated. Publicsupportcanberegardedasoneoftheprinciplestounderpinthe system, but the system itself has to firstly maintainaccountability.
Political involvement at all levels cannot be neglected asanotherimportantprinciple.Greatersupporttoensurethesystem’ssustainabilityderivedfromvariousinterestgroupscould be realised through participatory processes. Thelastbutnotleastimperativeprincipleistechnicalsupport.Knowledge becomes an essential tool for informing allpartiesinvolvedandassistingthemtomakegoodchoices.
To sum up what the principles should be, the system’saccountabilityperformancewouldbeputonthetopofthelist. The political engagement of all relevant stakeholdersandtechnicalsupportwouldcomesecondandthird.
dr Sanguan nitayarumphongMD,MPH
Secretary General of the National Health Security Office–Thailand
Has quality of health care improved over the past five years? If yes, what are the key drivers. If no, what are the main barriers?
1 Hasthequalityofhealthcareimprovedoverthepastfiveyears?Ifweexamineasliceofthisquestion,itislikelythatthequalityofacutehealthcaredelivered
toconsumersinAustraliaiscontinuouslyimprovingduetoadvancementsintechnology,techniquesandmedications.So the big picture answer is probably ‘yes’, regardingtreatmenteffectiveness.
If we narrow the question to examine the daily quality ofcaredeliveredinAustralianacutehealthcareorganisations,the real answer may well be‘we don’t know’, because wehave no agreed national quality measures. The politicalrealities of public health care at a state level dictate thatsafety,efficiencyandaccessibilityhavebeenthemainfocioverthepastfiveyears,withsomequantifiedgainsseenintheseareas. Ofcourse,eachstatetacklesimprovementinitsownuniqueway,makingitdifficulttoagree,ortobuildon,themosteffectiveapproachatanationallevel,ensuringourglacialpaceofchangeoverall.
Ifthequestionisreadas‘arewedeliveringbetterqualitycaretoeveryconsumeracrosseverydimensionofquality?’,thenthe answer is probably‘no’. We can’t say with confidencethat care is safer and more effective, appropriate, patientcentred,accessibleandefficientforeveryconsumertodaythanitwasfiveyearsago.Notonlybecausewelackstandardmeasurestoillustrateourimprovements,butbecausewedonotyethaveanational, systematicapproachtoprovidingthebestlevelofcare,ineveryqualitydimension,foreverypatient,everytime.
Wehaveabetterunderstandingin2006ofwhatweneedto do to achieve this goal, and more evolved tools andtechniqueswithwhichtoaddressit. Wehavemadesomeexcitinggainsoverthepastfiveyearsinourknowledgeofhow, and where, to tackle meaningful improvement. Butunderlying this lingers our long standing tolerance forambiguityinthewayhealthcareisdeliveredandmeasured,andourdependenceonpersonalities,ratherthansystems,to drive improvement. Whilst pursuing systematic qualityimprovementisstillperceivedasoptionalbysome,andanambivalentattitudetoqualityamongstsomeseniorhealthcare executives and clinicians remains acceptable, theanswertothisquestionwillbemoreorlessthesameinfiveyearstimeasitistoday.
dr cathy Balding AssocDipMRA,MHA,PhD,FCHSE,CHEDirector
Qualityworks–Victoria
70 AsiaPacificJournalofHealthManagement2006;1:2

2 In New Zealand we are definitely moving in theright direction.There are pockets of excellence andexamples of improved care and services, but there
aresomekeyrestraintsthataredraggingonprogress.
Financial limitations affect the degree of quality that canbeachieved.Forexample,thereisnofundingprovidedfordevelopmentandsupportofqualityandriskmanagementsystems.Shortagesofexperiencedhealthpractitionersinallareas,particularlyinnursing,causedinlargepartbylackoffundstohiresufficientstaffor topaycompetitivesalaries,depriveservicesoftheknow-howandwisdomthatisakeyfactorinqualitycare.
There is still a residual culture of blame when untowardeventsoccur,andaneedtofocusmoreonimprovingthoseareasthatarenotyetbestpractice.Apaucityofstandardisedquantitative data and mechanisms for sharing it inhibitbenchmarkingacrossservicesandmeasurementof trendsoverall.
Onthepositiveside,thereisanincreasedawarenessofandcommitmenttoimprovingqualityofcare,drivenbyseveralkeyfactors.
Theincreasing‘healthliteracy’andlitigiousnessofthepublic,andafewhighprofilesentineleventsandfailures,haveledtodemandsforbetterserviceandmoreaccountabilityfrompoliticians,healthmanagersandpractitioners.
Theinstitutionofmandatoryexternalcomplianceauditingof national Health & Disability Sector Safety Standards inhospital and residential services, and the requirement forprimaryandcommunityservicestomeetrelevantstandardsinordertogaindistricthealthboardservicecontracts,aredrivingqualityimprovementintheseareas.
Better educated health managers who understand thatquality in health care is more than just clinical safety, aredrivingqualityandriskmanagementtobecomeanintegralpartofthewayhealthcareservicesareprovided.
Ms Faye gardinerRGON,AFCHSE,CHE
Quality Auditor and Health Services Consultant–NewZealand
3 Anunequivocalyeswouldbefantasticbutwecan’tbe so dogmatic. Anecdotally, reports from the staffwouldsuggestthatithas.Anecdotallyfromthepress,
reportswouldsuggestthatithasnot.
Perhapstherealquestionshouldbe‘areweabletomeasurethequalityofhealthcare?’
Theanswertothisquestionisalsoproblematicbutwehavemadegreatstrides.
InNewSouthWales,anIncidentInformationManagementSystem (IIMS) has been introduced and, in September,released data from the first full year of reporting. Onehundredthousandstaffnowreporton-line,30,000staffhasbeentrainedtomanagethedataeffectivelyand3,000staffhasbeentrainedinRootCauseAnalysisprocedures.
The results are staggering. Across all four‘forms’ – clinical,corporate,patientstaffandvisitors,andcomplaints–therewere 125,000 reports. Eighty-eight thousand of thesereportswereontheclinicalform.TheresponseisremarkablyconsistentacrossallAreaHealthServices.
All events are coded according to a severity assessment(SAC) programme, with SAC1 being the most severe andSAC4 the least severe or near-misses not associated withharmatall.
Despite this massive system-wide reporting, the incidenceofSAC1eventshasshownnosignificant increaseoverthelastthreeyears.TheDepartmentofHealthandtheClinicalExcellenceCommissionhave jointlypublishedtworeportsonadverseeventsacrossthestatefocusingontheseSAC1events.[1,2]ThosereportsgofarbeyondthesentineleventsdefinedbytheAustralianCouncilonSafetyandQuality inHealthCare.
The annual data has demonstrated that falls remain thesingle most commonly reported adverse event followedby medication errors.The third most common problem isthemixedcategoryofclinicalmanagementwhichcoversawholerangeofclinicalanddecision-makingprocesses.
These figures suggest that an incident or adverse event,regardlessof itsseverity, is reported forapproximately7%of hospital admissions. The Quality in Australian HealthCare (QAHC) Study of 1995 [3] indicated an incidence ofapproximately16%ofadmissions.
Canwecomparethesetwostudies?Probablynot.TheQAHCStudywasathreeyearsnapshotof thesystem. Ifyou like,thefirstspeedcameratodrawourattentiontotheproblemsfacinghealthcarenotonlyinAustraliabutaroundtheworld.The IIMS data is very different. It is a voluntary reportingsystembythestaffthemselves. It isourspeedometer. Butitdoesanswerthequestion,atleastinpart,howfastarewegoingnow?Thisknowledgehastobethefirstdrivertowardsimprovementinhealthcare.
Q’sandA’s
AsiaPacificJournalofHealthManagement2006;1:2 71

None of us get up in the morning intending to do harm.Allofuswanttogohomeknowingwehavedoneanevenbetterjobthanthedaybefore.Wejustneedtoknow!
Hashealthcareimprovedinthelastfiveyears?Inshort,wedon’treallyknowbecausewehadnotbeeninthehabitofmeasuring system quality. Will it improve in the next fiveyears?Almostcertainly!–andpreciselybecausenowwearemeasuringit!
references1. NSWHealth.PatientSafetyandClinicalQualityProgram.Firstreport onincidentmanagementintheNSWpublichealthsystem2003-2004. NorthSydney:NSWDepartmentofHealth,2005.
2. NSWHealth.PatientSafetyandClinicalQualityProgram.Second reportonincidentmanagementintheNSWpublichealthsystem 2004-2005.NorthSydney:NSWDepartmentofHealth,2005.
3. WilsonRM,Runciman,WB,GibberdRW,HarrisonBT,NewbyL, HamiltonJB.TheQualityinAustralianHealthCareStudy.MedJAust 1995;163(9):458-471.
Professor clifford Hughes ao FRACS,FACS,FACCChief Executive Officer
Clinical Excellence Commission–NewSouthWales
4Anyperceptionthathealthcarestandardshavebeenimproving over recent years is difficult to sustainwithout: details on changes in health personnel
attitudes; data from quality assurance processes; clearstandards for protocols; and the collection of data onoutcomesofcare.
Intheagedcareindustry,qualityperformanceiscentraltoaccountabilityprocessesundertheAged Care Act(1997).Over99% of aged care facilities are fully accredited against thefour mandated standards and 44 outcomes.This indicatesanoverallacceptancebyindustrythatqualityperformanceisessentialtomanagementandprofessionalcareservices.
Aged care commitment to quality management reflects acultureofqualitywherevoluntarymonitoringofperform-anceindicatorsenablesstrategiestobeputinplacetoaddressimpending declines in performance. Quality PerformanceSystems (QPS Benchmarking) has been collecting andreportingclinicalandnonclinicaloutcomessincetheyear2000andprovidesagedcarefacilitiesthroughoutAustraliaand New Zealand with the opportunity to monitor andimprove their performance. For instance, performanceindicatorssuchastherateofpressureareasinthehighcaregroup have reduced from an average of 10% in 2000-2 to6%in2004-6.Similarimprovementsintherateofskintearsamonghighcareresidentsisalsodemonstrated.
Overthepastfiveyearstherehasbeenagrowthintheuseofkey performance indicators and benchmarking. More and
more managers are using key performance indicators andbenchmarking to drive their business improvements andtheireffortshavebeenenhancedbyrapidandwidespreaduptake by the aged care industry of computer basedinternetsystemsofdatacollection,reportinganddaytodaybusinessfunctions.Today,electronicsystemsandtoolsarecommonplaceand internetaccess ispredominantlybroadband.
With nationally mandated quality standards, commitmentof industry and government to shared quality goals, theembracing of technology, and sharing of informationthroughbenchmarkingmanyoftheQPSclientsareabletodemonstratesignificantandsustainedimprovementintheirdeliveryofservice.
Professor tracey Mcdonald RN,MN,PhD,MSc(Hons),BHA,DipEd,FRCNA,FCNRSL LifeCare Chair of Ageing
Australian Catholic University National
ProfessorMcDonaldcoordinatesresearchfortheQualityPerformanceSystemsAgedCareBenchmarkingProgram.
What has been achieved from Council of Australian Government’s health workforce reforms?
1Predatingthe2003AustralianHealthcareAgreement,the health workforce reform agenda saw theProductivity Commission examine issues affecting
theAustralianhealthworkforce,includingworkforcesupplyand demand, and long-term solutions to imbalances.The Productivity Commission’s process ran parallel with aCouncilofAustralianGovernments(COAG)HealthWorkingGroup examining essentially the same issues. So what aretheresultsofthesecombinedefforts?
From2007,anadditional1,000nursingplaceswillbeavailableatuniversities.Oversixhundredadditionalmedicalschoolplaceswillcomeonlineduringthenextfiveyearsandover700 additional allied and other health professional placeswill be available in 2007 as part of the Backing Australia’sFutureinitiatives.Thisisasubstantialachievement.
However, two issues become more evident from theseincreases. One is the number of applicants that ultimatelycompleteprograms.Therearecurrentlynospecificinitiativestoaddresswithdrawalrateswhich,forexampleinnursing,canresultin25%attrition.Thesecondissue,thequalityoftraining,formedpartoftheCOAGnegotiationsandresultedin states and territories guaranteeing high-quality, clinicalplacementsandinterntrainingfortheadditionalplaces.
Q’sandA’s
72 AsiaPacificJournalofHealthManagement2006;1:2

Thefundingofclinicaltrainingremainsanissueformedical,nursingandalliedhealthtraining.Onlynurseclinicaltrainingreceived additional Commonwealth funding. The othersdid not. Most notably, there remains no Commonwealthfunding for allied health professional clinical training,whichisacourserequirement.Thenursingclinicaltrainingsubsidyreceivedbyuniversitiesroseby45%to$1,000perfull time student. However, nursing load is calculated bytheCommonwealthat75%nursingand25%sciencebase,sothefundingincreasesperstudentdoesnotresultinfullfundingofclinicaltrainingforeachnewplace.
Q’sandA’s
Overall,COAGhassupportedtheProductivityCommission’sreform proposals and also its moves to create nationalaccreditation and registration bodies. COAG has settimelinesfornationalaccreditationandregistrationbodies,althoughdetailsofthestructure,governance,locationandrelationshipbetweenthesenationalbodiesarestillsubjectto negotiations. Senior officers establishing these newbodiesareduetoreporttoCOAGbytheendof2006.
Ms Margaret Banks BSc,PostgradDipPhysio,MHA,FCHSE,CHEHead Ambulatory Care
AustralianCommissiononSafetyandQualityinHealthCare
AsiaPacificJournalofHealthManagement2006;1:2 73
2007 national congress 1-3 august Sofitel Hotel – Melbourne
. . . visit the acHSE website www.achse.org.au for more information!
auStralian collEgE oF HEaltH SErvicE ExEcutivES

Book rEviEW
Beyond Patient Safety: managerial perspectives on errorreviewed by J Braithwaite
title of book:HofmanPB,PerryF,editors.Managementmistakesinhealthcare:identification,correctionandprevention.Cambridge:CambridgeUniversityPress;2005.ISBN0-521-82900-3
Agreatdealhasbeenwrittenonharmtopatients.Studies[1-4]havequantifiedthescaleoftheproblem.Dependingonthecountryandresearchdesign,adverseeventsoccurinbetween3.7%and16.6%ofalladmissions.Variousjudicialandquasi-judicialinquiries[5-7]haveteasedouttheextentoftheprobleminhumanandorganisationalterms.Overall,the patient safety literature has, to date, documented theclinicalaspectsofthesefailings,andrightlyso.
Yetwhataboutmanagementmistakes?Thisistheterritorywhereleaders,executivesandmanagerserr.Adverseeventsofthiskindcanleadtothesamedevastatingoutcomesasclinicalerrorsintermsofharmtopatients,organisationalorinstitutional damage, financial loss, political confrontationand professional compromise. Until now, no one hassystematicallyexaminedtheseissuesandwearethepoorerforit.
This book provides the beginnings of a solution, and is amust-read. The book is divided into two parts. Part onecontains six topic chapters. The scene is set by Richard JDavidson, President of the American Hospital Association.DavidsonremindsusinhisPrefaceofthetrustthatpatientsplace in health care institutions and how noble it is to bethecustodianandnurturerofthattrust.PaulBHofman,inhis opening chapter, considers a failed merger betweenhospitalsownedbyStanfordUniversityandtheUniversityof California which resulted in a loss of US$176 million(Aus$236million)overtwoandahalfyears.
He generalises from this lesson, develops a series offrameworksforunderstandingandmanagingerrorsofthiskindandprovidesasetofrecommendations.ForHoffman,learningfromothers’mistakes,stayinginformed,challengingthe status quo, valuing transparency and being open toalternativeviews,arecornerstonesofapreventivestrategy.
John Abbott Worthley discusses the context within whichmanagerial mistakes occur. He discerns eight contextualelements: legal, organisational, financial, political,professional,ethical,socialandpsychological.Inacompanionchapter, Wanda J Jones argues for the importance ofadmitting mistakes and for executive teams to be opento self-reflection and express a willingness to disclosemistakes. She discusses some of the common types ofmistake: errors in strategy formulation and execution,for example, and poor choices in resource commitments.
Changing the pace somewhat, Carol Bayley comparesmedicalwithmanagementerrors,queryingwhattheformercantellusaboutthelatterandaskingwhatlightcanmedicalerrors shed on management mistakes? She utilises JamesReason’sSwisscheesemodel,[8]andabriefculturalanalysis,toarguethatanorganisationalculture featuringtrustandtransparency,encouragedbymanagement,islikelytoproveawiseapproach.
JohnARussellandBennGreenspanlookatwaystoaddressandpreventmistakes.Theyoffercommentariesonvariousaspectsofmistakesandmakearangeofrecommendations.They suggest that there is much to be learned from casestudies and by building trust through evidence basedmanagerial decision-making. They urge executives torecognise the timing of their managerial decisions as afactorinreducingerrors.
The final chapter in Part 1, by Emily Friedman, analysesaccountability. Friedman’s plea is for the centrality ofaccountability. She wants executives to increase theiremphases on accountability, responsibility and ethicalpractices.
Parttwocontainssevenannotatedcasestudies,developedand presented by Frankie Perry. The case studies coverdisparateaspectsofmanagementmistakesincludingtruth-telling about medical errors; nursing shortages; choosing
Jeffrey BraithwaitePhDAssociateProfessorandDirectorCentreforClinicalGovernanceResearchinHealthFacultyofMedicine,UniversityofNewSouthWalesSydneyNSWAustralia
Correspondence:[email protected]
74 AsiaPacificJournalofHealthManagement2006;1:2

BeyondPatientSafety:managerialperspectivesonerror
the wrong information technology system; resourcing anewservicethatfailedtoattractpatients;secrecyaboutanunexpecteddeath;poorboardgovernancecapability;anda failedmerger.Thesecasesarewide-rangingand includevaluablecommentaries fromseniorhealthcareexecutivesacross the United States who carefully craft critical caseanalyses, paying particular attention to how these casesmightbehandledeffectively.
AsallthecasesareAmerican,RobertNichollsandAndrewWallassessthemfromaUnitedKingdomperspective.TheymakesomepracticalsuggestionsastohowthecasesmightbesolvedintheUKcontext.
In thefinalchapter,HoffmanandPerrysynthesise thekeylearningvalueofthechaptersandcases.Theyseethebookas a“call to action” for executives everywhere, not just inAmerica. According to them, executives must sponsor adifferentapproachtomanagerialerrors,lookingatthemasopportunitiesforimprovementandlearning,ratherthanasphenomenathatshouldbehiddenorignored.Theeditorsargue for the importance of clear leadership, admittingmistakes,abidingbyhighstandardsandemphasisingmorestronglythaninthepast,culturesofaccountability.
Thisbookisastrongadditionandafreshapproachtotheliterature on health care error. No one should doubt theimportanceoffindingnewwaystograpplewithmanagerialblunders,whichoftentendtogetsweptunderthecarpet.[9] Every practising manager of more than a few years’experience is likely to have witnessed or participated in,at least to some degree, damage limitation manoeuvresor thedownplayingofmanagementerrors.Thecauses forbehaviour like this in the executive suite are multifacetedand include threat of media interest, political forces(especially in publicly funded health systems), fear ofimpairing reputations, and the need to appear in controlandontopofthegame.Changingorganisationalculturestoaccepthigherlevelsofaccountabilityandtooperationaliseduties to disclose will not be easy, especially whenmanagers are so often under pressure to perform, lookgoodandappearinfallible.Forexample,mitigatingagainstany simple remedies, recent work has shown how healthcare managers’ roles, and the organisations they lead, arechallengingandcomplex,[10]busyandrelentless,[11]andhighlyambiguous. [12]Culturechange isproblematic [13]andlikelytobelongitudinal[14,15]ratherthanresolvableintheshorterterm.
ThisbooksuffersfrombeinglargelyAmericaninorientation,andhence itsapplicability tootheraudiences is limited. Itmeansthatpartsofithavetobeactivelyreconstructedbythenon-Americanreader.Despite thisshortcoming, this isa book well worth the investment. Buy it and read it witha level of discomfort, for its narratives are unsettling. Butheed well its messages, especially if you are a health carepolicymaker,executiveormanager.
competing interestsTheauthordeclaresthathehasnocompetinginterests.
references1. BakerGR,NortonPG,FlintoftV,BlaisR,BrownA,CoxJ,etal. TheCanadianadverseeventsstudy:theincidenceofadverseevents amonghospitalpatientsinCanada.CanMedAssocJ2004;170(11): 1678-1686.
2. ThomasEJ,StuddertDM,BurstinHR,OravEJ,ZeenaT,Williams EJetal.Incidenceandtypesofadverseeventsandnegligentcare inUtahandColorado.MedCare2000;38(3):261-271.
3. VincentC,NealeG,WoloshynowychM.AdverseeventsinBritish hospitals:preliminaryretrospectiverecordreview.BrMedJ2001; 322(7285):517-519.
4. WilsonRM,RuncimanWB,GibberdRW,HarrisonBT,NewbyL, HamiltonJD.ThequalityinAustralianhealthcarestudy.MedJAust 1995;163(9):458-471.
5. DepartmentofHealth.Reportintopublicinquiryintochildren’s heartsurgeryattheBristolRoyalInfirmary1984-1995:learning fromBristol.TheBristolRoyalInfirmaryInquiry.London:The StationaryOffice,2001.
6. SinclairCM.ReportoftheManitobapediatriccardiacsurgery inquest.Winnipeg:ManitobaProvincialCourt,1994.
7. WalkerB.FinalreportoftheSpecialCommissionofInquiryinto CampbelltownandCamdenhospitals.Sydney:NewSouthWales AttorneyGeneral’sDepartment,2004.
8. ReasonJT.Humanerror:modelsandmanagement.BrMedJ2000; 320:768-770.
9. HartleyR.Managementmistakesandsuccesses.8thed.NewJersey: JohnWileyandSons;2005.
10. BraithwaiteJ,FinneganT,GrahamB,DegelingP,HindleD, WestbrookM.Howimportantaresafetyandqualityforclinician- managers?Qualitativeevidencefromtriangulatedstudies.Clinical Governance2004;9(1):34-41.
11. BraithwaiteJ.Anempirically-basedmodelforclinician-managers’ behaviouralroutines.JHealthOrganManag2004;18(4-5):240-61.
12. IedemaR,DegelingP,BraithwaiteJ,WhiteL.It’saninteresting conversationI’mhearing:adoctorasmanager.OrganisationStudies 2004;25(1):15-34.
13. BraithwaiteJ,WestbrookMT,IedemaR,MallockNA,ForsythR, ZhangK.Ataleoftwohospitals:assessingculturallandscapes andcompositions.SociSciMed2005;60(5):1149-62.
14. BraithwaiteJ.Analysingstructuralandculturalchangeinacute settingsusingaGiddens-Weickparadigmaticapproach.Health CareAnal2006;14(2):forthcoming.
15. BraithwaiteJ.Anempiricalassessmentofsocialstructuraland culturalchangeinclinicaldirectorates.HealthCareAnal2006; 14(4):forthcoming.
AsiaPacificJournalofHealthManagement2006;1:2 75

ThisLibraryBulletinispartofaserviceofferedbytheHealthManagementandPlanningLibraryofACHSE.TheLibraryprovidesinformationontopicssuchashealthservicesmanagement,organisationalchange,corporateculture,humanresourcesandleadership.TheBulletinhighlightssomeofthemostuptodatearticles,books,featuresandliteratureonhealthmanagementfrombothAustraliaandinternationally.Copiesofthesearticlesareavailableatasmallcharge.Thefirstarticlecosts$10.00then$5.00foreachadditionalarticle.AllpricesareinclusiveofGST.
Toobtaincopiesofarticles,pleasecontactSueBrockway,Librarian,byphone(02)98050125orfax(02)98893099,bymailPOBox341NorthRydeNSW1670oremailto:[email protected]
l i B r a r y B u l l E t i n
agEd carECastle,NicholasGorganisational commitment and turnover of nursing Home administratorsHealth Care Management ReviewVol31(2)April-June2006pp156-165
CastleN,DegenholtzHandRosenJdeterminants of Staff Job Satisfaction of caregivers in two nursing Homes in PennsylvaniaBMC Health Services Research,20066.60http://www.biomedcentral.com/1472-6963/6/60/abstract
Cheek,Julianneandothersimproving the retirement village to residential aged care transitionAustralian Health ReviewVol30(3)August2006pp344-352
EuropeanHealthPropertyNetworkaccommodation for care of the Elderly: Single room Provision across Europe, 2006http://www.euhpn.org/docs/Accommodation_Elderly.doc
cHangE ManagEMEntOstroff,Frankchange Management in governmentHarvard Business ReviewVol84(5)May2006pp141-147(Leadersofgovernmentagenciesoperateunderhandicapslargelyunknownwithintheprivatesector.)
HEaltH carEAnderson,GerardFandothersHealth care Spending and use of information technology in oEcd countriesHealth AffairsVol25(30May/June2006pp819-831(TheUSisanoutlierinbothitshealthspendinganditsuseofhealthinformationtechnology.)
Boxall,Anne-MarieandShort,StephanieDPolitical Economy and Population Health: is australia Exceptional?Australia and New Zealand Health PolicyVol3(6)1June2006(Australiahasexperiencedconsiderablesocialandeconomicreformsoverthelast20years,withbothmajorpoliticalpartiesincreasinglyadoptingneo-liberalpolicies.Despitethesereforms,populationhealthoutcomesareamongstthebestintheworld.)http://www.anzhealthpolicy.com/content/pdf/1743-8462-3-6.pdf
Gilliard,Nicolas,Eggli,YvesandHalfon,Patriciaa Methodology to Estimate the Potential to Move inpatient Surgery to one day SurgeryBMC Health Services ResearchVol6:7819June2006http://www.biomedcentral.com/content/pdf/1472-6963-6-78.pdf
Herzlinger,ReginaEWhy innovation in Health care is so HardHarvard Business ReviewVol84(5)May2006pp58-66(Medicaltreatmenthasmadeastonishingadvancesbutthepackaginganddeliveryofhealthcareareofteninefficient,ineffectiveanduserunfriendly.)
Kernick,DavidWarning: Health Services research can damage your HealthBritish Journal of Health Care ManagementVol12(8)August2006pp246-249
76 AsiaPacificJournalofHealthManagement2006;1:2

LibraryBulletin
May,Carla rational Model for assessing and Evaluating complex interventions in Health careBMC Health Services Research, 2006 Vol6:867July2006(Understandinghownewclinicaltechniquesandtechnologiesbecomenormalisedinpracticeisimportanttoresearchers,clinicians,healthservicemanagersandpolicy-makers.)
http://www.biomedcentral.com/content/pdf/1472-6963-6-86.pdf
Mayhew,LeslieandLawrence,Davidthe costs and Service implications of Substituting intermediate care for acute Hospital careHealth Services Management ResearchVol19(2)May2006pp80-93
HEaltH FacilitiES Planning and dESignAnjali,Josephthe impact of design on infections in Health care Facilities, center for Health designFunded by the Robert Wood Johnson Foundation, July 2006 http://www.healthdesign.org/research/reports/infections.php
Carthey,JanePost-occupancy Evaluation: development of a Standardised Methodology for australian Health ProjectsThe International Journal of Construction Management Vol6(1)2006pppages63-80http://www.fbe.unsw.edu.au/chaa/downloads/Papers_Presentations/JC_IJCM_POE_Jul06.pdf
Dubbs,Danathe test of time: as Health care Evolves, so does Planetree (Patient-centred care)Health Facilities ManagementVol19(4)April2006pp29-34
Eagle,Amythe Future is now: Flexibility and Expandability drive Hospital ProjectHealth Facilities ManagementVol19(4)April2006pp14-20(TheprojectisinPhoenix,ArizonaUS)
Hendrich,AnnHospital Work Environments: implications for nursing Practice and Patient care QualityHealth care Environments Research Summit February 2006; Atlanta, Georgiahttp://hcdesign.coa.gatech.edu/paper/session2/Ann_paper.pdf
lEadErSHiPDahlen,GretchenMandBenz,BetsyArapid response teams: ten Essentials leaders need to knowHealth care ExecutiveVol21(4)July/August2006pp28-32,34
Hamm,Johnthe Five Messages leaders Must ManageHarvard Business ReviewVol84(5)May2006pp115-123(Toooftenleadersfailtoexplainwhattheymeanbytermssuchasorganisationalstructure,financialresults,timemanagement,corporateculture.Clearcommunicationisaleader’sbesttool.)
Haeuser,JamieandPreston,PaulMedical Staff collaboration: communication Strategies that get resultsHealth care ExecutiveVol21(4)July/August2006pp8-12,14(Toregaintrust,allpartiesmustbewillingtoredefinegoals,strategiesandoutcomesinwaysthataccommodatetheneedsoftheotherparty.)
Spreier,ScottW,Fontaine,MaryHandMalloy,RuthLleadership run amok: the destructive Potential of overachieversHarvard Business ReviewVol84(6)June2006pp72-82(Achievementisagoodthingbutmanagerswhoaretoostronglymotivatedbyitcandamagecompanyperformance.)
ManagEMEntEmbertson,MariKthe importance of Middle Managers in Health care organisationsJournal of Health care ManagementVol51(4)July/August2006pp223-232
Garman,AndrewMandTyler,JLarrySuccession Planning at the top: Effective Strategies in today’s EnvironmentHealth care ExecutiveVol21(4)July/August2006pp57-59
Waldman,JDeane,Smith,HowardLandHood,JacquelineNHealth care cEos and Physicians: reaching common groundJournal of Health care ManagementVol51(3)May/June2006pp171-184(PhysiciansmaybesurprisedtolearnthathealthcareCEOssharetheircorevalues,experiencesimilarfrustrationsandhaveidenticalfearsaboutthefutureofhealthcare.)
AsiaPacificJournalofHealthManagement2006;1:2 77

LibraryBulletin
MEntoringMoss,JohnRandothersMentoring for Population Health in general Practice divisionsAustralian Health ReviewVol30(1)February2006pp46-55(Implementationandevaluationofathree-waymodelofservicedevelopmentmentoring.)
QualityMcFadden,KathleenL,Stock,GregoryNandGowen,CharlesRExploring Strategies for reducing Hospital ErrorJournal of Health care ManagementVol51(2)March2006pp123-135
WorkForcE PlanningCohen,JeremyeDthe ageing nursing Workforce: How to retain Experienced nursesJournal of Health care ManagementVol51(4)July/August2006pp233-245
Seago,JeanAnnandothersthe nursing Shortage: is it really about image? Journal of Health care ManagementVol51(2)March/April2006pp96-110
Tyler,DeniseAandothersan Exploration of Job design in long-term care Facilities and its Effect on nursing Employee SatisfactionHealth Care Management ReviewVol31(2)April-June2006pp137-144
WEBSitE rEPortSAustralianGovernmentDepartmentofthePrimeMinisterandCabinetnational action Plan for Human influenza PandemicJuly2006(OutlineshowCommonwealth,state,territoryandlocalgovernmentswillworktogethertoprotectAustraliaagainstthethreatofaninfluenzapandemic.)
http://www.dpmc.gov.au/publications/pandemic/index.htm#downloads
AustraliaParliamentSenateSelectCommitteeonMentalHealtha national approach to Mental Health: From crisis to community.FinalReport,April2006http://www.aph.gov.au/senate/committee/mentalhealth_ctte/report02/index.htm
TheCommonwealthFund,committed to Safety: ten case Studies on reducing Harm to PatientsDouglasMcCarthyandDavidBlumenthal,April2006http://www.cmwf.org/usr_doc/McCarthy_safetycasestudies_923.pdf
Coulter,Angela,Engaging Patients in their Health care: How is the uk doing relative to other countries?PickerInstitute,2006(Analysisofdatafrominternationalpatientsurveyscomparesperformanceinrelationtosixindicatorsofpatientengagement.)http://www.pickereurope.org/Filestore/Downloads/Six-country-study-6-4-06-web-version.pdf
CouncilofAustralianGovernments’Meeting26July2006communiquéhttp://www.coag.gov.au/meetings/140706/index.htm#health
KingsFundCentregrow your own: creating the conditions for Sustainable Workforce developmentAugust2006http://www.kingsfund.org.uk/resources/publications/grow_your_own.html
Koh,HowardKandMcCormack,MichaelPublic Health leadership in the 21st century, center for Public leadership Working Papers 2006http://www.ksg.harvard.edu/leadership/research/publications/papers/2006/7_publichealth.pdf
NationalHealth&MedicalResearchCouncilcultural competency in Health: a guide for Policy, Partnerships and ParticipationMarch2005(GovernmentsandhealthservicesmaybebetterequippedtotackleAustralia’sfuturehealthissues,iftheyintegrateculturalissuesintotheplanninganddeliveryofhealthcareandservices,businessandcommunitygroups.)
http://www.nhmrc.gov.au/publications/_files/hp25.pdf
NSWHealthnSW: a new direction for Mental HealthJune2006http://www.health.nsw.gov.au/pubs/2006/pdf/mental_health.pdf
78 AsiaPacificJournalofHealthManagement2006;1:2

LibraryBulletin
ProductivityCommissionProductive reform in a Federal System Part B case Study one: Health reformRoundtableProceedingsVinceFitzGerald:Health reform in the Federal contextAndrewPodger:directions for Health reform in australiaStephenDuckett:discussantApril2006http://www.pc.gov.au/research/confproc/productivereform/productivereform.pdf
RobertWoodJohnsonFoundationWisdom at Work: the importance of the older and Experienced nurse in the WorkplaceJune2006http://www.rwjf.org/files/publications/other/wisdomatwork.pdf
(UK)DepartmentofHealthtacking nuisance or disturbance Behaviour on nHS PremisesAPaperforConsultation,June2006http://www.dh.gov.uk/assetRoot/04/13/59/90/04135990.pdf
NHSandSustainableDevelopmentCommissioncorporate citizenship and the nHS, 2006(HowNHSorganisationscanembracesustainabledevelopmentandtacklehealthinequalitiesthroughtheirday-to-dayactivities.)http://www.corporatecitizen.nhs.uk/
UKNHSConfederationWhy We need Fewer Beds(ThereportcitesadvancesintechnologyandnewwaysoftreatingpatientsasthereasonswhytheNHSnowneedsfewerbeds.)http://www.nhsconfed.org/docs/reputations1.pdf
USFederalFinancialInstitutionsExaminationCouncillessons learned from Hurricane katrina: Preparing your institution for a catastrophic Event, 2006(FinancialinstitutionsaffectedbyHurricaneKatrinaanditsaftermathgivetheirexperiencestohelpyourinstitutionrespondtoacatastrophicevent.)http://www.ffiec.gov/pdf/katrina_lessons.pdf
USNationalCenterforPolicyAnalysis,
Health care Spending – What the Future Will look likeJune2006http://www.ncpa.org/pub/st/st286/st286.pdf
VictorianTaskforceonViolenceinNursingFinal report, 2005http://www.health.vic.gov.au/nursing/downloads/victaskforcevio.pdf
WADepartmentofHealthanalysis of demand and utilisation of Metropolitan Emergency departments in Western australiaJune2006http://www.health.wa.gov.au/hrit/publications/docs/ED_Report_2006.pdf
WorldHealthOrganizationthe World Health report – Working together, 2006 (Containsanexpertassessmentofthecurrentcrisisintheglobalhealthworkforceandambitiousproposalstotackleitoverthenexttenyears,startingimmediately.)http://www.who.int/whr/2006/en/index.html
AsiaPacificJournalofHealthManagement2006;1:2 79

AttheinauguralmeetingoftheJournal’sEditorialAdvisoryBoardon2ndAugust2006severalimportantdecisionsweremade.These included re-defining the region for purposesof the Journal and identifying some potential themes forfutureissuesoftheJournal.
re-defining the regionIt was decided to re-define the Asia Pacific Region ascountriesofEastandNorth-EastAsia,SouthandSouth-WestAsia,South-EastAsiaandthePacific(ietoomitcountriesofNorth and Central Asia). A list of the respective countriesappearsinTable1.
ItwasalsodecidedthatfromtimetotimetheJournalshoulddraw on World Health Organisation and United Nationspublications to report comparative health performancedataforcountriesoftheregion.
uPdatE on Journal activitiES
Table 1: Asia Pacific Journal of Health Management: Countries of the Asia Pacific Region, 2006
EAST AND NORTH-EAST ASIA PACIFIC PACIFIC
ChinaDemocraticPeople’sRepublicofKoreaHongKong,ChinaJapanMacao,ChinaMongoliaRepublicofKorea
AfghanistanBangladeshBhutanIndiaIran(IslamicRepublicof )MaldivesNepalPakistanSriLankaTurkey
AmericanSamoaAustraliaCookIslandsFijiFrenchPolynesiaGuamKiribatiMarshallIslandsMicronesia(FederatedStatesof )NauruNewCaledonia
SOUTH-EAST ASIA SOUTH AND SOUTH-WEST ASIA
BruneiDarussalamCambodiaIndonesiaLaoPeople’sDemocraticRepublicMalaysiaMyanmarPhilippinesSingaporeThailandTimor-LesteVietNam
NewZealandNiueNorthernMarianaIslandsPalauPapuaNewGuineaRepublicofKoreaSamoaSolomonIslandsTongaTuvaluVanuatu
Source:ListofcountriesderivedfromUnitedNationsEconomicandSocialCommissionforAsiaandthePacific(UNESCAP).Asia-PacificinFigures2004.Table1:Totalpopulation.Bangkok:UNESCAP,StatisticsDivision;2005.Available:<http://www.unescap.org/stat/data/apif/index.asp>(Accessed5/06/06).
identifying themes for future issuesAmong suggested themes for future issues of the Journalwere:• Managementofmentalhealthservices;
• Managementofagedcareservices;
• ManagementofhealthservicesforIndigenouspopulations;
• Nationalapproachestohealthcaresystemfinancing;
• Managingandpreventingthespreadofinfectiousdiseases;
• Approachestopromotinghealthycities;
• RoleanduseofChinesemedicineandcomplementary therapies;
• Informationtechnologymanagementandsharing;
• Hospitalandhealthserviceaccreditation–definingmodels;
• Perspectivesonselectedclinicalworkforces(egnursing).
80 AsiaPacificJournalofHealthManagement2006;1:2

AsiaPacificJournalofHealthManagement2006;1:2 81
guidElinES For contriButorS
general requirementslanguage and formatManuscripts must be typed in English, on one side of thepaper,inArial11font,doublespaced,withreasonablywidemarginsusingMicrosoftWord.
AllpagesshouldbenumberedconsecutivelyatthecentrebottomofthepagestartingwiththeTitlePage,followedbytheAbstract,AbbreviationsandKeyWordsPage,thebodyofthetext,andtheReferencesPage(s).
title page and word count Thetitlepageshouldcontain:1. Title.Thisshouldbeshort(maximumof15words)but informativeandincludeinformationthatwillfacilitate electronicretrievalofthearticle.
2. Word count.Awordcountofboththeabstractandthe bodyofthemanuscriptshouldbeprovided.Thelatter shouldincludethetextonly(ie,excludetitlepage, abstract,tables,figuresandillustrations,andreferences). Forinformationaboutwordlimitssee‘TypesofManuscript –somegeneralguidelines’below.
Informationaboutauthorshipshouldnotappearonthetitlepage.Itshouldappearinthecoveringletter.
abstract, key words and abbreviations page1. Abstract–thismayvaryinlengthandformat(iestructured orunstructured)accordingtothetypeofmanuscript beingsubmitted.Forexample,foraresearchorreview articleastructuredabstractofnotmorethan300words isrequested,whileforamanagementanalysisashorter (200word)abstractisrequested.(Forfurtherdetails,see below-TypesofManuscript–somegeneralguidelines.)
2. Key words–threetosevenkeywordsshouldbeprovided thatcapturethemaintopicsofthearticle.
3. Abbreviations–theseshouldbekepttoaminimum andanyessentialabbreviationsshouldbedefined(eg PHO–PrimaryHealthOrgnaisation).
Manuscript Preparation and Submission
Main manuscriptThe structure of the body of the manuscript will varyaccordingtothetypeofmanuscript(egaresearcharticleornote would typically be expected to contain Introduction,Methods, Results and Discussion – IMRAD, while acommentary on current management practice may use aless structured approach). In all instances considerationshouldbegiventoassistingthereadertoquicklygrasptheflowandcontentofthearticle.
Forfurtherdetailsabouttheexpectedstructureofthebodyofthemanuscript,seebelow-TypesofManuscript–somegeneralguidelines.
Major and secondary headingsMajor and secondary headings should be left justified inlowercaseandinbold.
Figures, tables and illustrationsFigures,tablesandillustrationsshouldbe:
• ofhighquality;
• meetthe‘stand-alone’test;
• insertedinthepreferredlocation;
• numberedconsecutively;and
• appropriatelytitled.
copyrightFor any figures, tables, illustrations that are subject tocopyright,aletterofpermissionfromthecopyrightholderfor use of the image needs to be supplied by the authorwhensubmittingthemanuscript.
Ethical approvalAll submitted articles reporting studies involving human/oranimal subjects should indicate in the text whether theprocedurescoveredwereinaccordancewithNationalHealthand Medical Research Council ethical standards or otherappropriate institutional or national ethics committee.Whereapprovalhasbeenobtainedfromarelevantresearchethicscommittee,thenameoftheethicscommitteemustbestatedintheMethodssection.Participantanonymitymustbe preserved and any identifying information should notbe published. If, for example, an author wishes to publisha photograph, a signed statement from the participant(s)giving his/her/their approval for publication should beprovided.

Guidelinesforcontributors
82 AsiaPacificJournalofHealthManagement2006;1:2
referencesReferences should be typed on a separate page and beaccurateandcomplete.
TheVancouverstyleofreferencingisthestylerecommendedfor publication in the APJHM. References should benumberedwithinthetextsequentiallyusingArabicnumbersinsquarebrackets. [1]Thesenumbersshouldappearafterthepunctuationandcorrespondwiththenumbergiventoarespectivereferenceinyourlistofreferencesattheendofyourarticle.
Journal titles should be abbreviated according to theabbreviations used by PubMed. These can be found at:http://www.ncbi.nih.gov/entrez/query.fcgi. Once you haveaccessed this site, click on ‘Journals database’ and thenenter the full journal title to view its abbreviation (eg theabbreviationforthe‘AustralianHealthReview’is‘AustHealthRev’).Examplesofhowtolistyourreferencesareprovidedbelow:
Books and Monographs1. AustraliaInstituteofHealthandWelfare(AIHW).Australia’s health2004.Canberra:AIHW;2004.
2. NewB,LeGrandJ.RationingintheNHS.London:King’s Fund;1996.
chapters published in books3. MickanSM,BoyceRA.Organisationalchangeand adaptationinhealthcare.In:HarrisMGandAssociates. Managinghealthservices:conceptsandpractice.Sydney: Elsevier;2006.
Journal articles4. NorthN.ReformingNewZealand’shealthcaresystem. IntlJPublicAdmin.1999;22:525-558.
5. TurrellG,MathersC.Socioeconomicinequalitiesinall- causeandspecific-causemortalityinAustralia:1985-1987 and1995-1997.IntJEpidemiol.2001;30(2):231-239.
references from the World Wide Web6. PernegerTV,HudelsonPM.Writingaresearcharticle: advicetobeginners.IntJournalforQualityinHealth Care.2004;191-192.Available:<http://intqhc. oxfordjournals.org/cgi/content/full/16/3/191>(Accessed 1/03/06)
FurtherinformationabouttheVancouverreferencingstylecanbefoundathttp://www.bma.org.uk/ap.nsf/content/LIBReferenceStyles#Vancouver
types of Manuscript - some general guidelines1. analysis of management practice (eg, case study)ContentManagement practice papers are practitioner orientedwithaviewtoreportinglessonsfromcurrentmanagementpractice.
AbstractStructuredappropriatelyandincludeaim,approach,context,mainfindings,conclusions.Wordcount:200words.
Main text Structuredappropriately.Asuitablestructurewouldinclude:• Introduction(statementofproblem/issue);
• Approachtoanalysingproblem/issue;
• Managementinterventions/approachestoaddress problem/issue;
• Discussionofoutcomesincludingimplicationsfor managementpracticeandstrengthsandweaknesses ofthefindings;and
• Conclusions.
Wordcount:generalguide-2,000words.
References:maximum25.
2. research article (empirical and/or theoretical)ContentAn article reporting original quantitative or qualitativeresearchrelevanttotheadvancementofthemanagementofhealthandagedcareservicesorganisations.
Abstract Structured (Objective, Design, Setting, Main OutcomeMeasures,Results,Conclusions).
Wordcount:maximumof300words.
Main text Structured(Introduction,Methods,Results,DiscussionandConclusions).
Thediscussionsectionshouldaddresstheissueslistedbelow:• Statementofprincipalfindings;
• Strengthsandweaknessesofthestudyinrelationto otherstudies,discussingparticularlyanydifferencesin findings;
• Meaningofthestudy(egimplicationsforhealthand agedcareservicesmanagersorpolicymakers);and
• Unansweredquestionsandfutureresearch. Twoexperiencedreviewersofresearchpapers(viz, DohertyandSmith1999)proposedtheabovestructure forthediscussionsectionofresearcharticles.[2]

Wordcount:generalguide3,000words.
References:maximumof30.
NB: Authors of research articles submitted to the APJHMare advised to consult ‘Writing a research article: adviceto beginners’ by Perneger and Hudelson (2004) andavailable at: <http://intqhc.oxfordjournals.org/cgi/content/full/16/3/191>This article contains two very useful tables:1)‘Typical structure of a research paper’ and 2)‘Commonmistakesseeninmanuscriptssubmittedtothisjournal’.[3]
3. research note Content Shorterthanaresearcharticle,aresearchnotemayreporttheoutcomesofapilotstudyor thefirststagesofa largecomplex study or address a theoretical or methodologicalissueetc.Inallinstancesitisexpectedtomakeasubstantivecontributiontohealthmanagementknowledge.
AbstractStructured (Objective, Design, Setting, Main OutcomeMeasures,Results,Conclusions).
Wordcount:maximum200words.
Main textStructured(Introduction,Methods,Findings,DiscussionandConclusions).
Wordcount:generalguide2,000words.
As with a longer research article the discussion sectionshouldaddress:• Abriefstatementofprincipalfindings;
• Strengthsandweaknessesofthestudyinrelationtoother studies,discussingparticularlyanydifferencesinfindings;
• Meaningofthestudy(egimplicationsforhealthand agedcareservicesmanagersorpolicymakers);and
• Unansweredquestionsandfutureresearch.
References:maximumof25.
NB: Authors of research notes submitted to the APJHMare advised to consult ‘Writing a research article: adviceto beginners’ by Perneger and Hudelson (2004) andavailable at: <http://intqhc.oxfordjournals.org/cgi/content/full/16/3/191>This article contains two very useful tables:1)‘Typical structure of a research paper’ and 2)‘Commonmistakesseeninmanuscriptssubmittedtothisjournal’.[3]
4. review article (eg policy review, trends, meta-analysis of management research)Content A careful analysis of a management or policy issue ofcurrentinteresttomanagersofhealthandagedcareserviceorganisations.
Abstract Structuredappropriately.
Wordcount:maximumof300words.
Main textStructuredappropriatelyandincludeinformationaboutdatasources,inclusioncriteria,anddatasynthesis.
Wordcount:generalguide3,000words.
References:maximumof50
5. viewpoints, interviews, commentariesContent A practitioner oriented viewpoint/commentary about atopical and/or controversial health management issuewithaviewtoencouragingdiscussionanddebateamongreaders.
Abstract Structuredappropriately.
Wordcount:maximumof200words.
Main text Structuredappropriately.
Wordcount:generalguide2,000words.
References:maximumof20.
6. Book reviewBook reviews are organised by the Book Review editors.Pleasesendbooksforreviewto:BookReviewEditors,APJHM,ACHSE,POBox341,NORTHRYDE,NSW1670.Australia.
covering letter and declarationsThefollowingdocumentsshouldbesubmittedseparatelyfromyourmainmanuscript:
covering letterAllsubmittedmanuscriptsshouldhaveacoveringletterwiththefollowinginformation:• Author/sinformation,Name(s),Title(s),fullcontactdetails andinstitutionalaffiliation(s)ofeachauthor;
• Reasonsforchoosingtopublishyourmanuscriptinthe APJHM;
• Confirmationthatthecontentofthemanuscriptisoriginal. Thatis,ithasnotbeenpublishedelsewhereorsubmitted concurrentlytoanother/otherjournal(s).
Guidelinesforcontributors
AsiaPacificJournalofHealthManagement2006;1:2 83
declarations1. Authorship responsibility statementAuthors are asked to sign an ‘Authorship responsibilitystatement’. This document will be forwarded to thecorresponding author by ACHSE on acceptance of themanuscript for publication in the APJHM. This documentshould be completed and signed by all listed authors andthenfaxedto:TheEditor,APJHM,ACHSE(0298782272).
Criteria for authorship include substantial participationin the conception, design and execution of the work, thecontribution of methodological expertise and the analysisand interpretation of the data. All listed authors shouldapprovethefinalversionofthepaper,includingtheorderinwhichmultipleauthors’nameswillappear.[4]
2. Acknowledgements Acknowledgements should be brief (ie not more than 70words) and include funding sources and individuals whohavemadeavaluablecontributiontotheprojectbutwhodo not meet the criteria for authorship as outlined above.Theprincipalauthorisresponsibleforobtainingpermissiontoacknowledgeindividuals.
3. Conflicts of interestContributing authors to the APJHM (of all types ofmanuscripts)areresponsiblefordisclosinganyfinancialorpersonal relationships that might have biased their work.The corresponding author of an accepted manuscript isrequestedtosigna‘Conflictofinterestdisclosurestatement’.This document will be forwarded to the correspondingauthor by ACHSE on acceptance of the manuscript forpublication in the APJHM. This document should becompletedandsignedandthenfaxedto:TheEditor,APJHM,ACHSE(0298782272).
The International Committee of Medical Journal Editors(2006)maintainsthatthecredibilityofajournalanditspeerreview process may be seriously damaged unless‘conflictofinterest’ismanagedwellduringwriting,peerreviewandeditorialdecisionmaking.Thiscommitteealsostates:
‘A conflict of interest exists when an author (or author’sinstitution), reviewer, or editor has a financial or personalrelationships that inappropriately influence (bias) his orher actions (such relationships are also known as dualcommitments,competinginterests,orcompetingloyalties)....Thepotentialforconflictofinterestcanexistwhetherornotanindividualbelievesthattherelationshipaffectshisorscientificjudgment.
Financialrelationships(suchasemployment,consultancies,stock ownership, honoraria, paid expenses and testimony)are the most easily identifiable conflicts of interest andthosemostlikelytounderminethecredibilityofthejournal,authors,andscienceitself...’[4]
criteria for acceptance of ManuscriptTheAPJHMinvitesthesubmissionofresearchandconceptualmanuscripts that are consistent with the mission of theAPJHMandthatfacilitatecommunicationanddiscussionoftopical issues among practicing managers, academics andpolicymakers.
Of particular interest are research and review papers thatarerigorousindesign,andprovidenewdatatocontributeto the health manager’s understanding of an issue ormanagementproblem.Practicepapersthataimtoenhancetheconceptualand/orcoalfaceskillsofmanagerswillalsobepreferred.
Onlyoriginalcontributionsareaccepted(iethemanuscripthas not been simultaneously submitted or accepted forpublicationelsewhere).
Decisions on publishing or otherwise rest with the Editorfollowing the APJHM peer review process. The Editor issupported by an Editorial Advisory Board and an EditorialCommittee.
Peer review ProcessAll submitted research articles and notes, review articles,viewpointsandanalysisofmanagementpracticearticlesgothroughthestandardAPJHMpeerreviewprocess.
Theprocessinvolves:
1. ManuscriptreceivedandreadbyEditorAPJHM;
2. EditorwiththeassistanceoftheEditorialCommittee assignsatleasttworeviewers.Allsubmittedarticlesare blindreviewed(iethereviewprocessisindependent). ReviewersarerequestedbytheEditortoprovidequick, specificandconstructivefeedbackthatidentifiesstrengths andweaknessesofthearticle;
3. Uponreceiptofreportsfromthereviewers,theEditor providesfeedbacktotheauthor(s)indicatingthereviewers’ recommendationsastowhetheritshouldbepublished inthejournalandanysuggestedchangestoimprove itsquality.
For further informationabout thepeer reviewprocessseeGuidelinesforReviewersavailablefromtheACHSEwebsiteatwww.achse.org.au.
Guidelinesforcontributors
84 AsiaPacificJournalofHealthManagement2006;1:2

Submission ProcessAllcontributionsshouldincludeacoveringletter(seeabovefordetails)addressedtotheEditorAPJHMandbesubmittedeither:
(Preferredapproach)1) Emailsoftcopy(Microsoftwordcompatible)tojournal@ achse.org.au
Or
2) inhardcopywithanelectronicversion(MicrosoftWord compatible)enclosedandaddressedto:TheEditor, ACHSEAPJHM,POBox341,NorthRydeNSW1670;
Allsubmittedmanuscriptsareacknowledgedbyemail.
nBAll contributors are requested to comply with the aboveguidelines. Manuscripts that do not meet the APJHMguidelines for manuscript preparation (eg word limit,structureofabstractandmainbodyofthearticle)andrequireextensiveeditorialworkwillbereturnedformodification.
references 1. Hayles,J.Citingreferences:medicineanddentistry, 2003;3-4.Available:<http://www.library.qmul.ac.uk/ leaflets/june/citmed.doc>(Accessed28/02/06)
2. DohertyM,SmithR.Thecaseforstructuringthediscussion ofscientificpapers.BMJ.1999;318:1224-1225.
3. PernegerTV,HudelsonPM.Writingaresearcharticle: advicetobeginners.IntJournalforQualityinHealth Care.2004;191-192.Available:<http://intqhc. oxfordjournals.org/cgi/content/full/16/3/191> (Accessed1/03/06)
4. InternationalCommitteeofMedicalJournalEditors. Uniformrequirementsformanuscriptssubmittedto biomedicaljournals.ICMJE.2006.Available:<http:// www.icmje.org/>(Accessed28/02/06).
OtherreferencesconsultedinpreparingtheseGuidelinesEvansMG.Informationforcontributors.AcadManageJ.Available:<http://aom.pace.edu/amjnew/contributor_information.html>(Accessed28/02/06)
HealthAdministrationPress.JournalofHealthcareManagementsubmissionguidelines.Available:<http://www.ache.org/pubs/submisjo.cfm>(Accessed28/02/06)
InternationalJournalforQualityinHealthCare.Instructionstoauthors,2005.Available:<http://www.oxfordjournals.org/intqhc/for_authors/general.html>(Accessed28/02/06)
TheMedicalJournalofAustralia.Advicetoauthorssubmittingmanuscripts.Available:<http://www.mja.com.au/public/information.instruc.html>(Accessed28/02/06)
FurtherinformationabouttheAsiaPacificJournalofHealthManagementcanbeaccessedat:www.achse.org.au.
Guidelinesforcontributors
AsiaPacificJournalofHealthManagement2006;1:2 85

86 AsiaPacificJournalofHealthManagement2006;1:2

As part of the ACHSE Membership Benefit, the Management Competency for Health Professionals Assessment Package has been developed and is free to all ACHSE members and now available for sale to non-members.
The approach to competency assessment proposed by ACHSE in this package recognises that learning can come from a variety of sources, including workplace and non-workplace experiences and formal and informal learning activities.
The competency assessment instruments are designed to help you gain a better understanding of your management strengths and weaknesses so you can seek out suitable professional development strategies to address identified weaknesses and to build on your strengths.
The process of competency assessment will involve you in the following activities: • Self-assessment • Workplace assessment • Self-Review of these assessments• Development of your professional development profile and plan. Strategies to support this plan might include short courses or workshops for technical skill development, structured workplace learning experiences including coaching, and/or finding a suitable mentor with the appropriate expertise and formal courses to gain an understanding of relevant theories and concepts (eg. communication, quality improvement, economics, risk management).
The College is indebted to Dr Mary Harris MPH PhD FCHSE in developing and bringing this excellent package to fruition. Mary’s expertise and skill have been applied to assist all aspiring and practising health managers.
This is an excellent tool to use in your professional health management career. To order copies of the package on line please go to the following section on our web page www.achse.org.au/competency/index.html
Or email [email protected] or call on 02 9878 5088 or fax your orders to 02 9878 2272.
Under pUblication
These exclusive benefits are only available to you through your ACHSE membership. ContactACHSEMemberAdvantageforinformationonanyoftheabovebenefits. Phone: 1300 853 352 Email: [email protected] Web: www.member-advantage.com/achseFor every service used, Member Advantage will make a small contribution to ACHSE, which will help us support College initiatives and to further enhance our member services.
We’re improving the benefits of your membership!ACHSEisdelightedtolaunchanewrangeofmemberbenefitsandsavingsforyou.
TheCollegehasenteredintoapartnershipwithMemberAdvantagePtyLtd,anorganisationthatspecialisesinthedeliveryofhighqualitylifestyleandfinancialbenefitprogramstoprofessionalorganisations.Asamember,youcannowaccessthebenefitsofthisprogramthatinclude:
discounted Health insuranceReceive5%offthepremiumsfornewHCFproducts.
Home loan SavingsTheAffinityAMPHomeLoanpackageofferssignificantinterestratediscountsandfeewaivers,memberscouldsavethousandsandyearsofftheirmortgage.
car Hire discountsCorporatecarhirepackageincludinglowerratesthroughEuropcarallyearroundandareducedinsurancecost.
car PurchasingAcompletecarbuyingserviceincludingfleetpricesonnewcarsandwholesalepricesonsecondhandcars.
Electrical Buying Service Significantsavingsandwholesalepricesonover3000electricalproducts.
insurance CompetitiveratesandadvicethroughMemberAdvantageInsuranceServices.
Qantas club airline lounge Exclusivecorporateratesformembership.
telecommunicationsSavingsonbusinessmobile,InternetandfixedlineplansthroughOptus.
taxationProfessionaltaxreturnserviceatdiscountedmemberrates.
Management Competency for Health Professionals Assessment Package
AsiaPacificJournalofHealthManagement2006;1:2 87

2006 Participants and Presenters
88 AsiaPacificJournalofHealthManagement2006;1:2