asian development bank · asian development bank pcr: png 29634 program completion report on the...
TRANSCRIPT

ASIAN DEVELOPMENT BANK PCR: PNG 29634
PROGRAM COMPLETION REPORT
ON THE
HEALTH SECTOR DEVELOPMENT PROGRAM Loans 1516-PNG and 1517-PNG(SF)
AND THE
HEALTH SECTOR INVESTMENT COMPONENT
Loan 1518-PNG(SF)
IN
PAPUA NEW GUINEA
October 2004
CURRENCY EQUIVALENTS
Currency Unit – kina (K)
At Appraisal At Project Completion (14 February 1997) (13 February 2004)
K1.00 = $0.73 $0.314000 $1.00 = K1.37 K3.184713
ABBREVIATIONS
ADB – Asian Development Bank AusAid – Australian Agency for International Development BME – benefit monitoring and evaluation CAHS – College of Allied Health Sciences DNPRD – Department of National Planning and Rural Development DOF – Department of Finance DOT – Department of Treasury HMIS – health management information system HRD – human resources development HSDP – health sector development program NDOH – National Department of Health NHP – national health plan PCC – program coordination committee PCR – program completion report PHA – provincial health adviser PHO – provincial health office PIU – project implementation unit PNG – Papua New Guinea SDR – special drawing rights SOE – statement of expenditure SWAP – Sector-wide approach TA – technical assistance
NOTES
(i) The fiscal year (FY) of the Government ends on 31 December. FY before a calendar year denotes the year in which the fiscal year ends, e.g., FY 2004 ends on 31 December 2004.
(ii) In this report, “$” refers to US dollars.
CONTENTS
Page
BASIC DATA ii
MAP vii
I. PROGRAM DESCRIPTION 1
II. EVALUATION OF DESIGN AND IMPLEMENTATION 1 A. Relevance of Design and Formulation 1 B. Program Outputs 2 C. Program Costs 7 D. Disbursements 8 E. Program Schedule 8 F. Implementation Arrangements 9 G. Conditions and Covenants 10 H. Related Technical Assistance 10 I. Consultant Recruitment and Procurement 10 J. Performance of Consultants, Contractors, and Suppliers 11 K. Performance of the Borrower and the Executing Agency 11 L. Performance of the Asian Development Bank 12
III. EVALUATION OF PERFORMANCE 12 A. Relevance 12 B. Efficacy in Achievement of Purpose 13 C. Efficiency in Achievement of Outputs and Purpose 15 D. Preliminary Assessment of Sustainability 15 E. Environmental, Sociocultural, and Other Impacts 16
IV. OVERALL ASSESSMENT AND RECOMMENDATIONS 16 A. Overall Assessment 16 B. Lessons Learned 16 C. Recommendations 17
APPENDIXES 1. Implementation and Compliance with Program Measures 19 2. Schedule of Actual Expenditures from the Asian Development Bank’s and Borrower’s Funds 25 3. Project Implementation Schedule 26 4. Status of Compliance with Loan Covenants 27

ii
BASIC DATA
A. Loan Identification 1. Country 2. Loan Numbers
3. Program Title Project Title
4. Borrower 5. Executing Agency 6. Amount of Loan
7. Program and Project Completion Report Number
Papua New Guinea 1516, 1517(SF), and 1518(SF) Health Sector Development Program Health Sector Investment Component Papua New Guinea Department of Finance Policy-based loans: SDR3,511,000 and $45,000,000 Investment Project: SDR7,022,000 PCR: PNG 860
B. Loan Data 1. Appraisal – Date Started – Date Completed 2. Loan Negotiations – Date Started – Date Completed 3. Date of Board Approval 4. Date of Loan Agreement 5. Date of Loan Effectiveness – In Loan Agreement – Actual
6. Closing Date 1518(SF) a
– In Loan Agreement – Actual – Number of Extensions 1516 and 1517(SF) b
– In Loan Agreement – Actual
7. Terms of Loan
1517(SF) and 1518(SF) – Interest Rate – Maturity (number of years) – Grace Period (number of years) 1516
– Interest rate – Maturity (number of years) – Grace Period (number of years)
15 July 1996 2 August 1996 28 January 1997 31 January 1997 20 March 1997 26 September 1997 26 December 1997 23 October 1997 31 December 2001 13 February 2004 Three 30 June 2000 8 December 1999 1% service charge per annum 35 years 10 in accordance with the Asian Development Bank’s currency specific lending rate; commitment charge rate of 0.75% per annum 25 5
a Loan 1518-PNG(SF): Health Sector Investment Component. b Loan 1516-PNG/1517-PNG(SF): Health Sector Development Program.

iii
9. Disbursements a. Dates 1518(SF)
Initial Disbursement 23 December 1997
Final Disbursement 13 February 2004
Time Interval 74 months
1516 5 December 1997 6 December 1998 12 months 1517(SF) 8 December 1997 6 December 1998 12 months 1518(SF)
Effective Date 23 October 1997
Original Closing Date 31 December 2001
Time Interval 50 months
1516 and 1517(SF) 23 October 1997 30 June 2000
32 months
SF = special fund
b. Amount ($) Cat. No.
Project
Component
Original
Allocation
Last Revised
Allocation
Net Amount
Available
Amount
Disbursed
Amount
Canceled Loan 1518(SF) 1 Civil Works 5,905,982 5,905,982 4,748,592 4,748,592 1,157,390 2 Equipment 486,014 486,014 255,560 255,560 230,454 3 PIU 43,569 43,569 28,079 28,079 15,490 4 Training/Fellowship 704,931 704,931 578,634 578,634 126,296 5 Consultancy Services 825,516 825,516 792,416 792,416 33,101 6 Operations Maintenance 69,155 69,155 62,416 62,416 6,739 7 Service Charges 47,204 47,204 47,205 47,205 8 Unallocated 1,714,834 1,714,834 0 0 1,714,834 Total 9,797,205 9,797,205 6,512,903 6,512,903 3,284,303a Loan 1516
01
45,000,000
45,000,000
45,000,000
45,000,000
0 Loan 1517(SF)
01
4,793,590
4,793,590
4,793,590
4,793,590
0 Cat. = category, No. = number, PIU = project implementation unit, SF = special fund
a This cancelled amount was taken from the Loan Financial Information System (LFIS) (ALR 985).
10. Local Costsa (Financed [Asian Development Bank portion only]) - Amount ($) 953,003.92 - Percent of Local Costs 41.43% - Percent of Total Cost 9.53% a Applies only to Loan 1518-PNG(SF): Health Sector Investment Program and does not apply to Loans 1516-
PNG/1517-PNG(SF): Health Sector Investment Component.

iv
C. Project Data
1. Project Cost ($’000) Cost Appraisal Estimate Actual
Loan 1518(SF) a Foreign Exchange Cost 7,700 5,560 Local Currency Cost 5,300 4,105
Total 13,000 9,665 Loan 1516 b Foreign Exchange Cost 45,000 45,000
Total 45,000 45,000 Loan 1517(SF) a Foreign Exchange Cost
4,794
4,794
Total 4,794 4,794 SF = special fund a Loan 1518-PNG(SF): Health Sector Investment Component. b Loan 1516-PNG/1517-PNG(SF): Health Sector Development Program
2. Financing Plan ($’000)
Cost Appraisal Estimate Actual Implementation Costs (Loan 1518[SF])a Borrower-Financed 3,000 3,152 ADB-Financed 10,000 6,513 Other External Financing
Total 13,000 9,665 IDC Costs Borrower-Financed ADB-Financed 0.200 0.047 Other External Financing
Total 0.200 0.047
Implementation Costs (Loan 1516 and 1517[SF]) b
Borrower-Financed
ADB-Financed 0 0
Other External Financing 49,794 49,794
Total 49,794 49,794 ADB = Asian Development Bank, IDC = interest during construction, SF = special fund a Loan 1518-PNG(SF): Health Sector Investment Component. b Loan 1516-PNG/1517-PNG(SF): Health Sector Development Program
v
3. Cost Breakdown by Project Component (Loan 1518[SF]) ($'000)
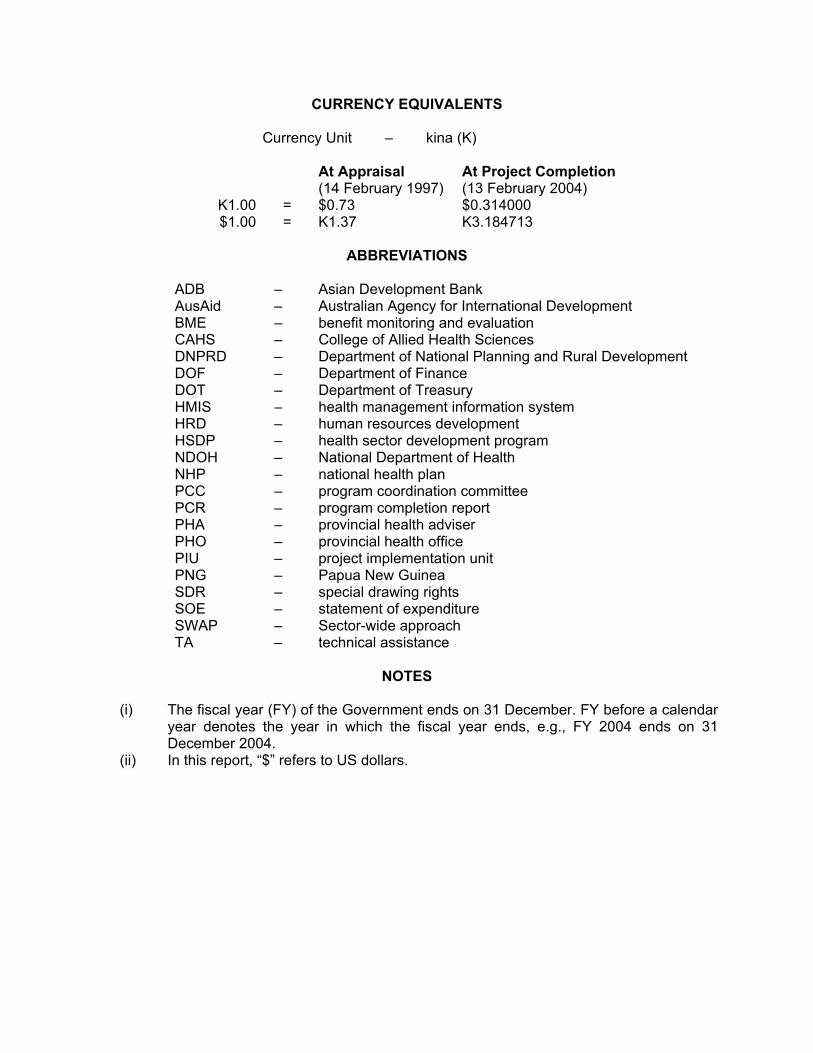
Component Appraisal Estimate Actual Civil Works 3,820 6,755 Equipment 1,135 298 PIU 353 67 Training and Fellowship 2,796 961 Consulting Services 2,640 1,474 Operations and Maintenance 400 63 Service Charges 200 47 Unallocated 1,656
Total 13,000 9,665 PIU = project implementation unit, SF = special fund. 4. Project Schedule (Loan 1518[SF])
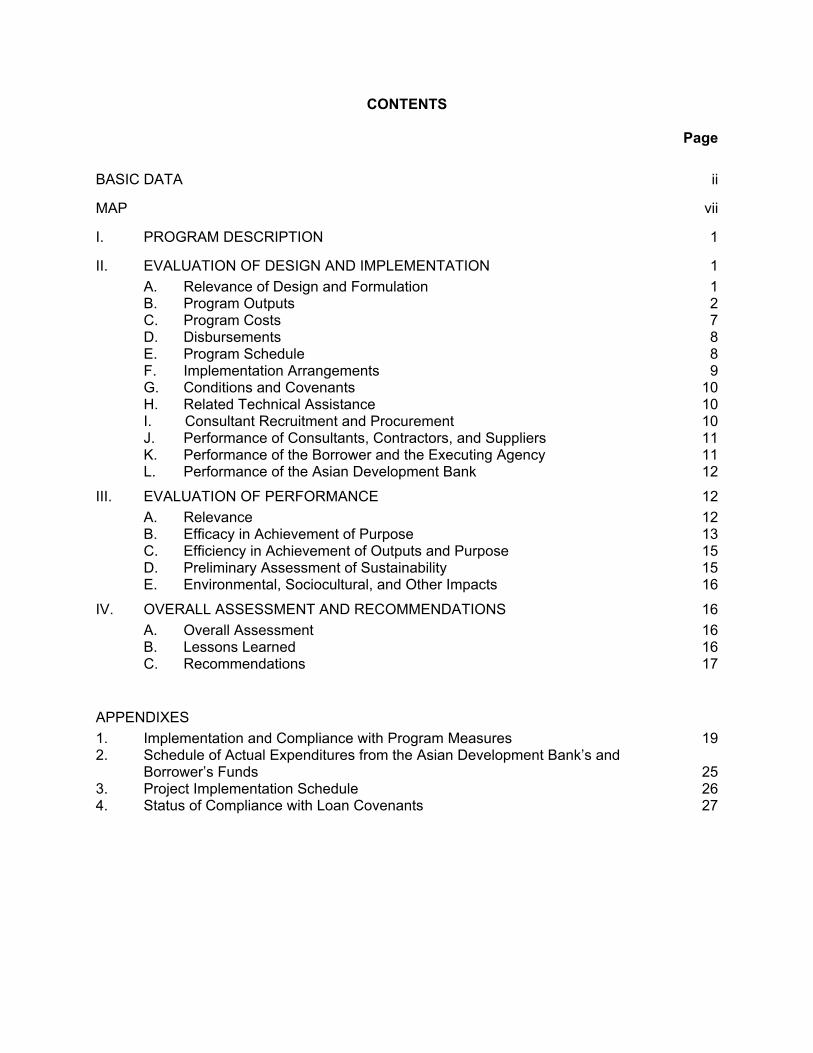
Item Appraisal Estimate Actual Date of Contract with Consultants Structon Architects – CW Project Managers Duncan Wells – M&R System Analyst Richard Cibulskis – M&R BME Adviser Patricia Urbiztondo – M&R Programmer/Analyst James MacPherson – HRM Curriculum Specialist Nayareh Kaviani – Curriculum Specialist Wydoncha Limited
17 April 1998
1 May 20001 October 19972 January 2002
1 June 19971 January 2002
15 April 2002
17 April 1998
1 May 20001 October 2001
1 March 20021 October 199715 March 2002
15 April 2002
Completion of Engineering Designs CAHS – Madang Media Print Shop – Gordons Laloki In-Service Training College
August 1998August 1998
January 1999
September 1998September 1998 31 August 1999
Civil Works Contract Date of Award CAHS – Madang Media Print Shop-Gordons Laloki In-Service Training College
January 1999January 1999January 1999
January 1999January 1999
22 November 2001 Completion of Work CAHS –Madang Media Print Shop-Gordons Laloki In-Service Training College
30 September 2000
31 March 200031 December 2001
31 June 2002
31 August 200230 September 2003
Equipment and Supplies Dates First Procurement 2 January 1998 19 January 1998 Last Procurement 31 December 2001 30 September 2003 Completion of Equipment Installation 31 December 2001 31 January 2004Start of Operations 31 December 2001 1 July 2004 Completion of Tests and Commissioning 31 December 2001 31 January 2004 Beginning of Start-Up 1 January 2002 1 July 2004Other Milestones Note: This schedule is not applicable for the program loan component loans: 1516-PNG/1517-PNG(SF): Health Sector Development Program.
vi
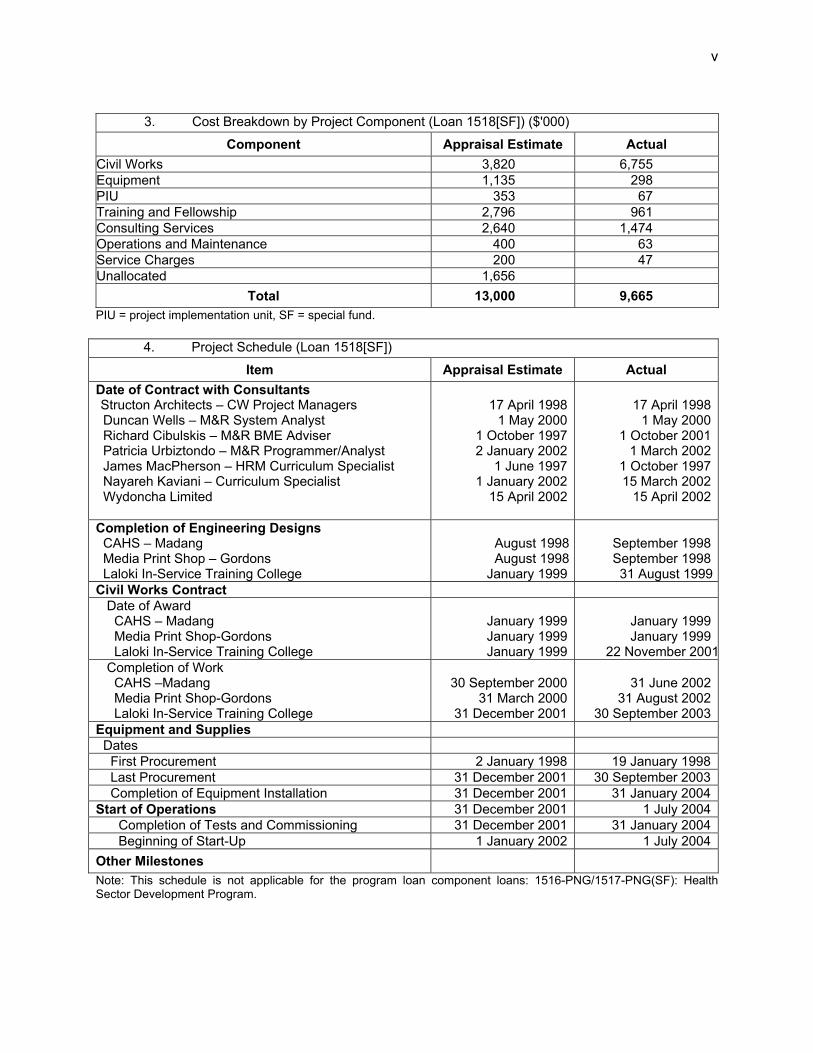
5. Project Performance Report Ratings
Ratings
Implementation Period Development Objectives
Implementation Progress
Loan 1518(SF) a From 1 January 2002 to 31 December 2002 Satisfactory Partly Satisfactory From 1 January 2003 to 31 December 2003 Satisfactory Satisfactory From 1 January 2004 to 29 February 2004 Satisfactory Satisfactory Loan 1516 and 1517(SF) b From 23 October 1997 to 8 December 1999 Satisfactory Satisfactory
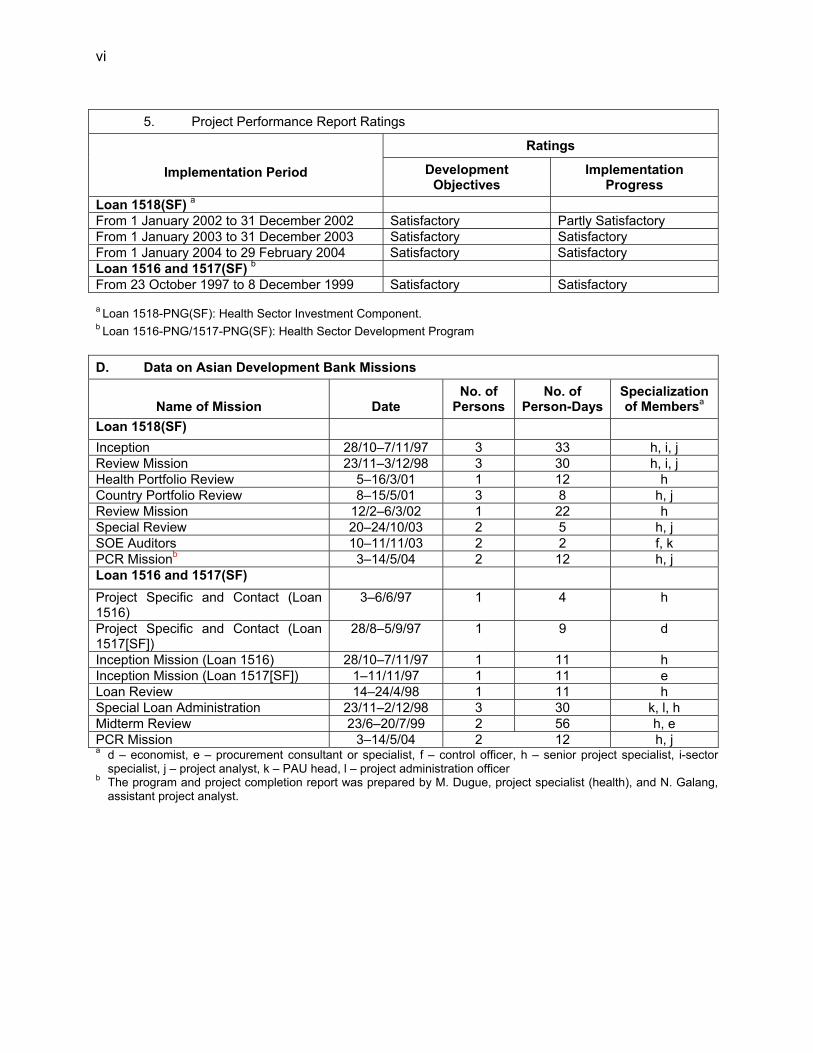
a Loan 1518-PNG(SF): Health Sector Investment Component. b Loan 1516-PNG/1517-PNG(SF): Health Sector Development Program D. Data on Asian Development Bank Missions
Name of Mission
Date
No. of Persons
No. of Person-Days
Specialization of Membersa
Loan 1518(SF) Inception 28/10–7/11/97 3 33 h, i, j Review Mission 23/11–3/12/98 3 30 h, i, j Health Portfolio Review 5–16/3/01 1 12 h Country Portfolio Review 8–15/5/01 3 8 h, j Review Mission 12/2–6/3/02 1 22 h Special Review 20–24/10/03 2 5 h, j SOE Auditors 10–11/11/03 2 2 f, k PCR Missionb 3–14/5/04 2 12 h, j Loan 1516 and 1517(SF) Project Specific and Contact (Loan 1516)
3–6/6/97 1 4 h
Project Specific and Contact (Loan 1517[SF])
28/8–5/9/97 1 9 d
Inception Mission (Loan 1516) 28/10–7/11/97 1 11 h Inception Mission (Loan 1517[SF]) 1–11/11/97 1 11 e Loan Review 14–24/4/98 1 11 h Special Loan Administration 23/11–2/12/98 3 30 k, l, h Midterm Review 23/6–20/7/99 2 56 h, e PCR Mission 3–14/5/04 2 12 h, j a d – economist, e – procurement consultant or specialist, f – control officer, h – senior project specialist, i-sector
specialist, j – project analyst, k – PAU head, l – project administration officer b The program and project completion report was prepared by M. Dugue, project specialist (health), and N. Galang,
assistant project analyst.

I. PROGRAM DESCRIPTION
A. Health Sector Development Program
1. Despite many efforts, the public health system was unable in the middle 1990s to attain previous rates of improvement in health outcomes and treat most common diseases, particularly among the rural poor and women and children. At that time, the public health system was trying to cope with the situation without changing its management approach. 2. The reforms supported by the Health Sector Development Program (HSDP) envisaged major changes in the health management system, which included (i) greater participation of users and local governments; (ii) increased autonomy of key institutions, such as hospitals; (iii) more drugs and medical supplies available at the primary health care facilities level; (iv) better financial management of the health sector, including cost sharing arrangements with users; and (v) enhanced participation of the private sector, nongovernment organizations, and religious groups. 3. Policy-based loans were designed to support the implementation of the Government’s national health plan (NHP) 1996–2000, and they reflected the reform process embodied in the recently passed Organic Law on Provincial Governments and Local Level Governments (1995), adjusting and completing the process of decentralization that began after independence. Implementation of the HSDP coincided with the progressive implementation of the National Health Administration Act (1997), which began in 1998. B. Health Sector Investment Component
4. The objectives of the investment component were to (i) establish a competency-based personnel training system in the health sector and (ii) strengthen the health management information system. The component consisted of two parts. Part A focused on human resources development (HRD). Part B focused on the health management information system (HMIS). Part A comprised three activities focusing on (i) developing an in-service training system, which included the building of an in-service training complex; (ii) strengthening performance standards and evaluation; and (iii) strengthening institutional capacity within the National Department of Health (NDOH) in human resources planning and management. Part B was aimed at assisting the Government in integrating and improving existing public health care and epidemiology databases and providing new modules on health-related personnel, drugs, and monitoring and evaluation.
II. EVALUATION OF DESIGN AND IMPLEMENTATION
A. Relevance of Design and Formulation
5. A major cause of the deterioration of health services in Papua New Guinea (PNG) was the macroeconomic crisis of 1994–1995. Imbalances in PNG’s fiscal performance in the early 1990s resulted in a precipitous halt of government spending on goods and services in 1994, and this was followed by an economic rescue effort in 1995–1996 by the International Monetary Fund and the World Bank, assisted by Australia and Japan. The economic recovery package provided a government policy to redirect spending to the social sector (in health and education). These events established a framework conducive to a health sector program loan as part of the overall rescue effort.
2
6. Assistance to the health sector in PNG had focused in the 1980s and early 1990s on improving access to rural health services by investing mainly in infrastructure (aid posts, health centers, and staff housing). Evaluations confirmed the improved physical accessibility to health facilities of many remote parts of the country and showed that extending facilities did not solve the problems of closure or limited operation of facilities resulting from a shortage of staff members, insufficient drugs, malfunctioning equipment, and poor maintenance of buildings. 7. The HSDP was designed to support the implementation of long-term reforms, focusing on the whole sector, with a major emphasis on performance of rural health service delivery. The HSDP was prepared and implemented at a time when a new law on decentralization of all government services and activities was passed. This new law transferred the responsibility of rural health service to local governments, limiting the role and responsibility of the National Department of Health (NDOH) to supporting policy, setting technical and quality standards, and monitoring and evaluation. Launched without sufficient preparation for its implementation, the law proved extremely disruptive to the health system, breaking down the vertical integration that is essential to ensuring a strong link between policy development and implementation. 8. In this difficult context, the HSDP’s design and formulation was and remains adequate and relevant. The investment component was an appropriate and timely response in view of the priority given to HRD in the health sector. B. Program Outputs
1. Policy Reform Program
a. Shifting Emphasis from Urban to Rural Areas
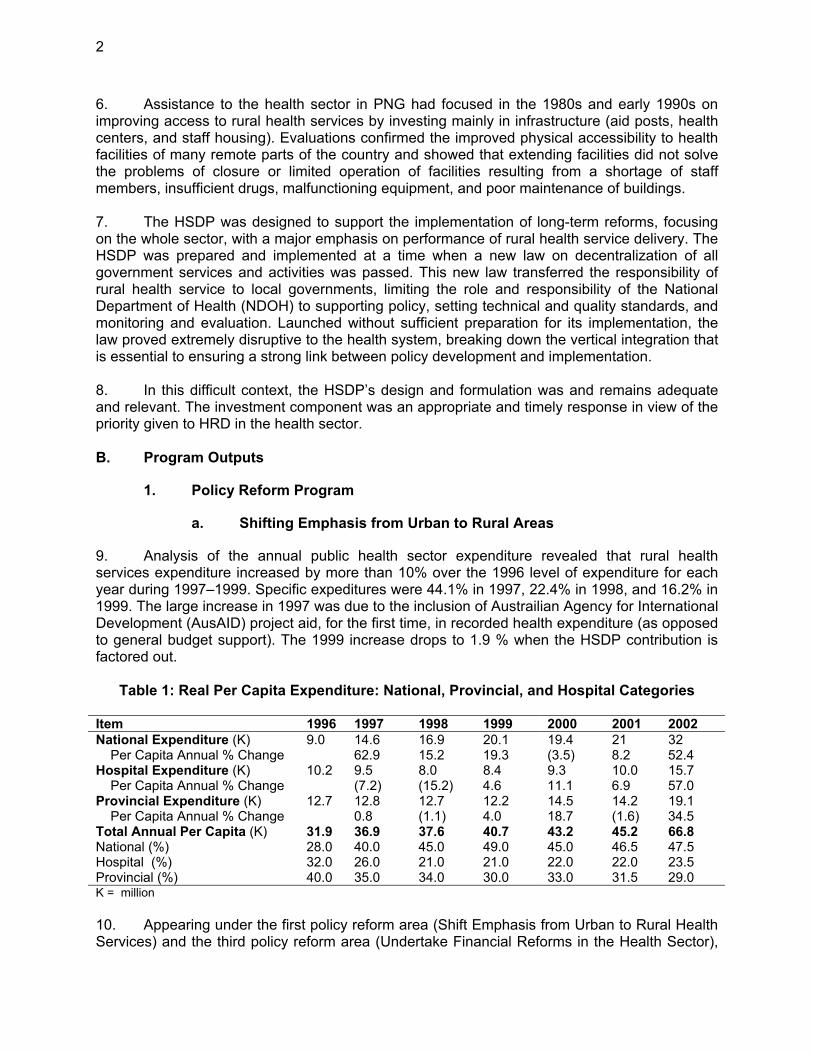
9. Analysis of the annual public health sector expenditure revealed that rural health services expenditure increased by more than 10% over the 1996 level of expenditure for each year during 1997–1999. Specific expeditures were 44.1% in 1997, 22.4% in 1998, and 16.2% in 1999. The large increase in 1997 was due to the inclusion of Austrailian Agency for International Development (AusAID) project aid, for the first time, in recorded health expenditure (as opposed to general budget support). The 1999 increase drops to 1.9 % when the HSDP contribution is factored out.
Table 1: Real Per Capita Expenditure: National, Provincial, and Hospital Categories
Item 1996 1997 1998 1999 2000 2001 2002 National Expenditure (K) 9.0 14.6 16.9 20.1 19.4 21 32 Per Capita Annual % Change 62.9 15.2 19.3 (3.5) 8.2 52.4 Hospital Expenditure (K) 10.2 9.5 8.0 8.4 9.3 10.0 15.7 Per Capita Annual % Change (7.2) (15.2) 4.6 11.1 6.9 57.0 Provincial Expenditure (K) 12.7 12.8 12.7 12.2 14.5 14.2 19.1 Per Capita Annual % Change 0.8 (1.1) 4.0 18.7 (1.6) 34.5 Total Annual Per Capita (K) 31.9 36.9 37.6 40.7 43.2 45.2 66.8 National (%) 28.0 40.0 45.0 49.0 45.0 46.5 47.5 Hospital (%) 32.0 26.0 21.0 21.0 22.0 22.0 23.5 Provincial (%) 40.0 35.0 34.0 30.0 33.0 31.5 29.0 K = million 10. Appearing under the first policy reform area (Shift Emphasis from Urban to Rural Health Services) and the third policy reform area (Undertake Financial Reforms in the Health Sector),
3
benchmarks for the release of the second tranche were exceeded in both cases. The first benchmark was to increase the value of drug supplies to health centers and aid posts to K3.00 per capita in the area served. In 1998, the value was K4.29 per capita. In 1999, the value was K6.00 per capita. The second benchmark was to increase the allocation for drugs and medical supplies to 25.0% of NDOH’s budgetary allocation for 1998. In 1998, the allocation of drugs and supplies as a percentage of total NDOH expenditure was 28.0%. In 1999, the allocation increased to 31.8%. 11. In terms of the contribution made by the HSDP to the total expenditure on drugs and medical supplies, in 1998 the contribution was 34.7%, and in 1999 the contribution was 26.6%. More importantly, the nature of the contribution resolved the persistent problem of inadequate drug supplies reaching aid posts, the lowest level of the public health system. A standard aid post medicine kit was designed with three rounds of drug supplies shipped annually. The kits were delivered directly to provincial health offices (PHOs), bypassing NDOH’s area medical store network. PHOs used HSDP-supplied trucks and funds to distribute the kits to all functioning aid posts. Because the kits are assembled in the country, health promotion materials from various sources (National HIV/AIDS Council, NDOH, and World Health Organization) were frequently added to the kits for broad rural dissemination. 12. The aid post medicine kit system was widely viewed by NDOH and other central agencies and provincial governments as a successful initiative. Responsibility for procurement and distribution rested entirely with NDOH, PHOs, and rural health facilities. The aid post medicine kit system can easily be maintained as a permanent feature in NDOH’s provision of medicines nationwide.
b. Shifting Orientation from Curative to Preventive Health Service
13. Improving Disease Control Mechanisms. The HSDP supported improvement in water supply, including supply to schools, focusing essentially on reticulation and wells, as rain catchments proved in 1997 to be inefficient in case of drought. This is important, particularly in the highlands, where the incidence of typhoid is high. The HSDP’s funds also supported the provision of bed nets and insect repellant spray for malaria control.
14. Health Information and Education Campaigns. Health promotion remains underfunded, at less than 1% of total health expenditure, although some health promotion campaigns are funded under family health and diseases control, and some provinces used HSDP funds to pay for the broadcasting of a health education program on radio or including health education information in newspapers. More efforts are now being targeted at HIV/AIDS education campaigns.
c. Undertaking Financial reforms
15. Stable Funding. An increase in health sector financing during the period covered by the HSDP resulted mainly from an increase in development agency financing and only marginally from the Government’s budget (0.75% per year, on average, in real terms). While provinces agreed in 2000 to increase their financial commitment to health to 15% of their budget, none have yet reached this objective. However, the 2004 budget has seen the first substantial improvement, with all provinces committing more than 6% of their resources to health. 16. Financial Planning. The recent decentralization of responsibilities in the health sector led to a multiplication of the budgeting authority to the district (89 districts), province (20
4
provinces), and DOH levels, with each of these levels having a different budget structure in 1997. Gaining a clear picture of health sector funding is therefore difficult. Establishing a standard budget form under the HSDP greatly improved the process, but comparing the before and after HSDP scenarios is unreliable. 17. Strengthening Financial Management of the Health Sector. Improving financial management at national and, especially, provincial levels was an important change brought about by Asian Development Bank (ADB) support, mainly through an efficient HSDP secretariat and the development of tools, guidelines, and procedures for accounting, expenditures, monitoring, reporting, training, and supervision of performance related to HSDP funds. A simple budget structure was developed under the Strengthening Financial Management of the Health Sector project.1 The issues debated, which the program coordination committee (PCC) influenced, included official recognition by the Department of Finance’s Budgets Division of the standard program categories, establishing a uniform budget structure in health for all three levels of government. PCC also served as an important forum to discuss annual appropriations in health, both at the national and provincial levels. The weak budgetary support to health services in many provinces was a recurring theme, as was the unstable appropriation of HSDP funding from year to year. 18. User Fees. Hospitals were enabled to collect and retain user fees by the Public Hospital and Dental Charges Act, which was passed in 1995. However, by the end of 1997, the National Executive Council decided that fees should be reduced by 50%, in response to the difficulties encountered by the population following the drought. The collection of fees by rural health facilities was never put in place, due to a lack of consensus on the adequacy of this measure.
d. Enhance Efficiency of Health Delivery System
19. While the fourth policy reform area (Enhance the Efficiency of Health Service Delivery) has as its principal benchmark the establishment of national and provincial health boards, the underlying objective was to improve the management of the delivery of public health services. The management structures and processes developed and implemented under the HSDP served as an overall management strengthening process that extended beyond the HSDP policy matrix. The success of these processes is to a great extent based on the ownership developed through the wide consultation and participation in their establishment and the investment in capacity building in provinces through regular supervision and the performance review process. 20. Many PHOs and their respective provincial governments responded well to the continuous process of management strengthening. The process served to highlight principal governance issues, creating a more transparent environment in which these issues received greater attention and often became the subject of local discussion and remedial action. All provinces received the same oversight, while their particular problems and recognized weakness were given individual attention. The decentralized management of HSDP funds at the provincial level was effective. Provincial health advisers (PHAs) were allowed by the HSDP to act as managers of health services in their provinces, under the supervision of the HSDP secretariat. 21. However, while rural health is primarily a provincial function, as per the New Organic Law on decentralization, provinces increased only marginally their health-related spending, until 1 TA No. 2772-PNG, approved on 20 March 1997.
5
2002. The channel to fund rural church health services was recentralized (from the provincial to the national level) during this period, to ensure a steady and sufficient flow of resources. 22. Annual agreements are passed between NDOH and each provincial government. The annual activity plan and performance monitoring framework contain the priority strategies, activities, and performance measures for the health sector in each province. A joint review of performance against requirements is conducted annually. As a result of this process, provincial budget allocation for health substantially increased in 2004, for the first time since decentralization. 23. Hospital Management. Provincial health boards were established in all but two provinces (North Solomons and Southern Highlands2). Most boards, however, are not functioning. An interesting innovation was brought about by Western Highlands Province, where the hospital board took over from the provincial health board. At a time when NDOH is trying to unify the health system after the disruption introduced by the New Organic Law (NOL), this move is regarded as promising.
24. Human Resources Management. The human resources branch was established in NDOH as stated in the HSDP’s policy letter. In 1997, NDOH developed a brief policy on in-service training, with four main objectives: (i) develop in-service training programs, (ii) institutionalize in-service training for rural health workers, (iii) build provincial and district capacity, and (iv) develop a framework for in-service training coordination. The policy aimed to achieve these objectives through (i) establishing an information system, (ii) identifying in-services training needs, (iii) identifying and training trainers, (iv) developing training materials, (v) supporting district in-service training programs, and (vi) establishing two regional in-service training centers.
25. However, in the absence of authority and leadership and political will, this area remains the weakest in PNG’s health sector, while still absorbing a disproportionate share of resources. Despite a high level of expenditure on wages, salaries, and benefits, the health system remains largely understaffed. As a result of the scarcity of qualified health workers and the difficulty in retaining them in remote areas, a steady reduction occurred in the number of health workers deployed at aid posts since 1995, which caused the closure of about 25% of the facilities at this level. Some of the issues are discussed under the investment component (para. 30), as human resources was its main focus.
26. Greater Involvement of Nongovernment Organizations and Churches and the Private Sector. An official partnership agreement was passed in 2003 between church health services and NDOH, and the recentralization of church health services funding by NDOH ensured a better flow of financial resources. 27. Development of Health Facilities Maintenance. With the assistance of AusAID, maintenance teams were established and trained and workshops installed in provincial hospitals. Their duties include maintaining equipment for health centers.
2. Health Sector Investment Component
28. The component was implemented between March 1998 and December 2003. The following section describes its outputs under the three principal parts. 2 North Solomons suffered a decade of civil unrest, and tribal fights affected Southern Highlands for several years.
6
a. Health Personnel Training
29. Most of the component’s parts and their supportive activities changed substantially when the civil works were reprogrammed in about the second year of the undertaking. Instead of just renovation and minor new construction for in-service facilities in Madang and Port Moresby, major new construction projects were recommended, which resulted in the construction of the new Laloki facility (national in-service training center) and the Gordons media unit. All physical works were completed in October 2003. The College of Allied Health Services (CAHS) Madang construction renovation was completed in December 2002. Refurbishment and renovation of the media print shop in Gordons was completed in August 2002. 30. The human resources activity for consulting services for human resources development was abandoned because the human resources management branch made no progress in defining its plans and expectations and did not recruit most of the consultants identified in the component’s design. Most were reprogrammed to other consulting services, as needed by NDOH, particularly to improve the HMIS. Similarly, most of the in-service training provisions for noninstitution-based learning were not done for lack of programs from the human resources management branch and hospitals. 31. Very little progress occurred in health personnel training, as emphasized by a review of in-service training undertaken in 2003. This review uncovered the the following:
(i) The human resources branch had little capacity to plan and coordinate in-service training. Responsibility for in-service training was located with the training and curriculum section of the human resources branch, and activities of this section were not properly linked with staff development and workforce planning processes. Consequently, in-service training was planned outside of workforce needs, and skills deficits were identified through staff appraisals.
(ii) The human resources branch started establishing a database of people employed in the health sector, with the support of the investment project for the new payroll system. Progress, however, was slow, and only 13 provinces were covered.
(iii) The system’s inadequate records of training and lack of a central database made determining the extent and coverage of the courses undertaken impossible.
(iv) The system had a tendency to wait for resources and not plan for alternative or creative solutions.
(v) The system had no database of training materials or processes for monitoring training material development.
(vi) The system did not evaluate or have means to assess the impact of in-service training.
b. Health Management Information System
32. Assistance to the HMIS included (i) reviewing the NHP 1996–2000 and establishing the baseline for the NHP 2001–2010; (ii) developing a set of 19 core indicators for the NHP 2001–2010, which constituted the backbone of the performance monitoring framework of the health system; and (iii) developing a health workforce database, which unfortunately was not completed due to the lack of commitment of the human resources branch. Assistance was also provided in specialized areas, such as database management and epidemiology. The progress made depended largely on the level of skills of monitoring and research branch staff members.

7
Therefore, a substantial portion of unused funds for training were reallocated for additional training of monitoring and research branch and provincial staff members. 33. The national health information system was further developed and implemented nationwide under ADB’s loan. Five instruments were developed and are now in use:
(i) information system (information on health center activities and disease statistics), (ii) national inventory of health facilities (health center staffing and equipment), (iii) aid post update list (aid post status and staffing), (iv) provincial workbook (PHO resources and activities), and (v) hospital workbook (hospital resources and activities).
34. The system is generally perceived as performing well, and the reliable data produced notably supported the elaboration of the last two NHPs. The sytem produces health and service indicator data on a monthly basis at provincial and national levels, and it produces most of the information for monitoring sector performance, using the 19 core indicators of NHPs. A burden of disease study was carried out in PNG, largely based on the data produced by the HMIS. Considerable progress was noted in strengthening analysis and use of data at the provincial level as well as building capacity of the monitoring and research branch to enhance analytical skills for annual reporting. C. Program Costs
1. Health Sector Development Program
35. ADB provided a loan of $45.00 million from its ordinary capital resources and a loan of $5.00 million (SDR3.51) from its Special Funds resources. The policy loans were released in equal tranches. The counterpart funds thus generated were to be used by the Government to implement health sector reforms in rural areas.
2. Health Sector Investment Component
36. At appraisal, the total cost of the investment component was estimated at $13.00 million, including physical and price contingencies and interest charges during construction. Of the total cost, $7.70 million (59%) comprised the foreign exchange cost, and $5.30 million (41%) comprised the local currency cost. ADB provided a loan of $10.00 million (SDR7.02 million) to finance the entire foreign exchange cost and 43% of the local cost. The Government committed to financing the balance of the local currency costs of $3.00 million. 37. The overall actual cost of ADB’s component was roughly $6.51 million. The net amount disbursed by ADB was also roughly $6.51 million (about $5.55 million in foreign currency cost, including service charge during construction [85.37%], and about $0.95 million in local currency cost [14.63%]). Details of appraisal and actual costs are provided in Appendix 2. The Government’s overall share in the ADB-financed component was about $3.15 million

8
D. Disbursements
1. Health Sector Development Program
38. The first tranche of the program loan was disbursed between December 1997 and February 1998. For loan 1516,3 $4.50 million was disbursed on 5 December 1997, $5.82 million was disbursed on 29 December 1997, $9.49 million was disbursed on 8 January 1998, and $2.68 million was disbursed on 4 February 1998. For loan 1517(SF),4 $0.50 million was disbursed on 8 December 1997 and $1.88 million was disbursed on 29 December 1997. 39. The second tranche of $22.50 million (loan 1516) and $2.41 million (loan 1517[SF]) was released on 6 December 1999.
2. Health Sector Investment Component
40. No disbursement projections were made at appraisal for the investment component. An imprest account was provided to facilitate component implementation through the timely release of funds. The initial advance to this facility was $1.00 million. Due to the overall slow implementation of the component, actual disbursements were below yearly disbursement projections, which also resulted in the cancellation of the unused loan balance of $3.28 million (SDR2.21) at final loan closing on 13 February 2004. E. Program Schedule
1. Health Sector Development Program
41. The loans were approved on 20 March 1997 and became effective on 23 October 1997. The Government complied with all conditions, but a shortage of Asian Development Fund money did not allow earlier effectivity. The funds for the program loans were to be released in two tranches. The first tranche release was further delayed due to constraints on Asian Development Fund availability and was completed by the end of February 1998. Full provisions for the program were not specifically included in the original 1997 appropriation, and this resulted in start-up delays. In addition, the Department of Treasury (DOT) did not deposit the counterpart funds in the appropriate trust account until 22 April 1998. As a result, the original closing date of the program loans was November 1998, but the loans actually closed on 8 December 1999. Appropriation in the Government of Papua New Guinea (GoPNG) budget was insufficient to implement the program within the expected time frame, and the unpredictable release of warrants to NDOH resulted in further delays.
2. Health Sector Investment Component
42. The investment component was envisaged at appraisal to be implemented over a period of 4 years, with completion in March 2001. Substantial delays in the implementation of the component were attributed to the major change in scope approved on 11 April 1999, allowing the Government’s request to reprogram the capital works components by shifting the location of the in-service training complex from Madang and Gordon to Laloki. Poor performance of the project implementation unit and the consultant recruited as civil works manager resulted in additional delays. The loan closing date was extended three times. The first was from the
3 Loan 1516-PNG: Health Sector Development Program. 4 Loan 1517-PNG(SF): Health Sector Development Program

9
original closing date of 31 December 2001 to 31 December 2002. A second extension was approved from 31 December 2002 to 30 June 2003, which was necessary due to slow construction progress. A third extension was approved from 30 June 2003 to 30 September 2003. F. Implementation Arrangements
1. Health Sector Development Program
43. Inevitably for an innovative program, the implementation process was not smooth, particularly as the program started under crisis conditions. Considerable confusion was apparent at the beginning regarding the nature of the funding. The difficulty arose from the use of counterpart funds, which, in contrast to the case of a traditional program loan, were not available for budgetary support but were instead to be used for the agreed specific program. This also raised considerable debate and caused difficulties with DOT after the release of the second tranche. The full amount of the second tranche was removed from the HSDP account in the Bank of Papua New Guinea, which is PNG’s central bank, and credited to the PNG public account (general revenue), in breach of the Loan Agreement’s stipulation regarding counterpart funds, which stated that the funds were to remain in the HSDP-ADB trust account until such time as they were made available to the Implementing Agency for use in the implementation of the HSDP (in practice, implementation of the NHP). Once an agreement was reached regarding the funds being appropriated in the annual budget cycle, the HSDP became one of the largest, and frequently one of the first, targets for budget reduction measures. Both the continual need for overall budgetary discipline and the frequent changes of the Department of Finance’s (DOF’s) top management ensured that at each budget cycle a protracted and intense battle to defend appropriation under the HSDP was inevitable. 44. PCC, established by DOF to ensure timely and efficient coordination in the implementation of the HSDP, had a supervisory role. PCC’s chairperson was the secretary for finance and the head of the Executing Agency. However, the secretary for health most often chaired PCC meetings, in the absence of the secretary for finance. Yet, DOF representation was good and usually included its Budgets Division, Public Accounts Division, and Information Technology Division. The Department of National Planning and Monitoring (now called the Department of National Planning and Rural Development [DNPRD]), which is closely associated with DOF, was also usually well represented. Meeting three times a year, on average, PCC brought together senior NDOH staff members, PHAs, Churches Medical Council and nongovernment organization representatives, and other public health stakeholders in a unique forum with key DNPRD and DOF representatives and, on occasion, representatives of the Department of Personnel Management, Department of Provincial Affairs and Local Level Governments, and the National Monitoring Authority. 45. Under the steady leadership of the secretary for health, issues of importance in the context of the HSDP and health services delivery overall were discussed openly and constructively. Indeed, PCC meetings offered a rare opportunity for DOT and DNPRD managers, among others, to hear directly from key representatives in the health sector. An important function of PCC was to provide a forum for PHAs to report to PCC’s extensive membership PHA successes and difficulties. Changes in NDOH, with the appointment of a new secretary, and the transformations brought about by the participation of development partners in the trust account mechanism led to PCC’s interruption in 2000, which was finally revived as part of the sectorwide approach preparation process in 2002.
10
46. Overall, the implementation arrangements put in place for the policy-based loans proved to be very successful in monitoring the progress on reforms and involved for the first time a broad range of stakeholders.
2. Health Sector Investment Component
47. NDOH’s project implementation unit (PIU) was responsible for the day-to-day implementation of the investment component’s activities. The PIU was headed by a full-time project coordinator who reported to the secretary of NDOH and was responsible for (i) implementing PCC policy decisions and guidelines; (ii) planning project implementation and record keeping of project activities; (iii) recruiting consultants; (iv) procuring goods; (v) conducting civil works; and (vi) monitoring project implementation and preparing progress reports. Issues with the PIU are detailed in paras 55 and 56. G. Conditions and Covenants
1. Health Sector Development Program
48. The first tranche of the policy-based loans was disbursed at effectivity, the Government having already taken the necessary actions. As stated in the Loan Agreement, the release of the second tranche was subject to the fulfillment by the Government of eight specific conditions, four of which were fully met at midterm review, three were almost met, and one was not met. ADB's Board endorsed the waiver of this condition when approving the release of the second tranche. This last condition, related to the privatization of drugs and medical supplies to nodal centers in provincial hospitals is yet to be complied with.
2. Health Sector Investment Component
49. Of the total 18 covenants, 8 were fully complied with while the remaining 10 were partly complied with. Main difficulties were with a lack of (i) adequate record keeping and accounting practices by PIU, (ii) adequate supervision in PIU and poor management of contracting, and (iii) counterpart funds availability. H. Related Technical Assistance
50. The comprehensive approach adopted under the HSDP included the provision of associated technical assistance to strengthen the health financing system and devise ways in which funding could be better linked with the health status of the population. The technical assistance had a crucial role in program implementation. Implementation started in August 1997. It supported the operationalization of the imprest and trust accounts to disburse health funds. It also served as a major link between DOF and NDOH, through the support provided to the HSDP secretariat. 51. The technical assistance provided essential inputs for the Government in meeting program conditions and was central to building the capacity of NDOH to move toward a sectorwide approach in health. I. Consultant Recruitment and Procurement
52. Health Sector Investment Component. Procurement was done in accordance with ADB’s Guidelines on Procurement. Likewise, all consultants were recruited in accordance with

11
ADB’s Guidelines on the Use of Consultants. Major administrative delays occurred in recruiting most consultants, and this had a negative impact on implementation of the investment component. For instance, no engagement of consultants resulted from the recruitment drive initiated during December 2000. Of the four positions advertised, two positions (HRD programmer and applied epidemiologist) were deferred for further review of requirements. Database manager position candidates were all rejected, and only the national health information system programmer position was filled. J. Performance of Consultants, Contractors, and Suppliers
53. Health Sector Investment Component. Two consultants were recruited to assist the human resources branch in reviewing the curriculum for health officers and nurses, and they performed satisfactorily. The consultants recruited for the HMIS were (i) one monitoring and evaluation specialist, (ii) one computer programmer analyst, (iii) one management information specialist and system analyst in the monitoring and research branch, and (iv) one database manager. The experts consisted of individual consultants, and all successfully completed their assignments. 54. In the civil works part of the investment component, reporting from the civil works project manager (a consulting firm) made following up the progress difficult. Despite strong recommendations from ADB’s missions, the Executing Agency decided to continue working with this consultant, who performed badly. Design flaws and multiple delays plagued the implementation of the investment component. K. Performance of the Borrower and the Executing Agency
1. Health Sector Development Program 55. Serious difficulties occurred with DOF and DOT, which did not make available the entire amount generated by the second tranche to NDOH, and low appropriation and slow release of funds plagued implementation. The Executing Agency’s performance was rated unsatisfactory.
2. Health Sector Investment Component 56. PIU’s project management and coordination capacity became extremely weak, as already identified in the project completion reports of two other projects.5 While this did not bear consequences for the policy-based loans, this impacted negatively on the investment component. Recording and filing systems were inadequate. The Executing Agency was slow in identifying and recruiting consultants, and this resulted in major delays and/or cancellation of components. The project coordinator left NDOH 18 months before implementation was finished. This resulted in further disruption, inadequate supervision, and improper reporting. 57. ADB’s special review missions in 2003 noted that the records and files of PIU were in disarray. Recordings in the ledgers were not up-to-date, and some contract variations were approved twice for the same amount and scope of work. Loose and inaccurate recording of transactions and reporting mechanisms were identified. The accounting function systematically underperformed, and delays and errors systematically occurred in compiling and auditing component accounts. Relevant findings indicated that adequate measures and supervision did
5 ADB. Project Completion Report on the Third Rural Health Service. Manila. ADB. 2002. Project Completion Report on Population and Family Planning. Manila.
12
not exist from the Executing Agency’s side in ensuring timely completion of the component. Finally, lack of counterpart funds resulted in delays and cancellation of component activities. Apart from the review missions, wherein discussions with the Executing Agency and project management unit emphasized the need to improve their recording system and project administration, ADB’s PNG Resident Mission was always readily available for advice and support on matters relating to ADB policy and administration. However, inadequate supervision within PIU, due to the long absence of the project coordinator, adversely affected the component’s smooth implementation. Although a temporary replacement existed, the level of experience and supervision was not comparable with that of the incumbent project coordinator. In view of this, the Executing Agency’s performance was rated unsatisfactory. L. Performance of the Asian Development Bank
1. Health Sector Development Program 58. ADB was very supportive of the Government’s efforts to move toward a sectorwide approach and responsive to the Government’s request for more technical assistance in this area (The affected technical assistance was extended, and a new technical assistance undertaking was processed).6 Numerous missions were fielded, and ADB’s performance was rated satisfactory.
2. Health Sector Investment Component
59. Frequent review missions were undertaken during HSDP implementation. No disagreements with NDOH occurred during component implementation. The Government appreciated ADB’s timely responses to requests. ADB’s PNG Resident Mission was always readily available for advice and support on matters relating to ADB policy and administration. ADB fielded several special review missions to assist PIU in accounting. Overall, ADB supervision was adequate. Extensions of loan closing dates and needed reallocations were processed in a timely manner and to the satisfaction of the Borrower. ADB’s performance was therefore rated satisfactory.
III. EVALUATION OF PERFORMANCE
A. Relevance
60. The fundamentally new approach of the present loan was innovative for PNG and ADB. This was the first quasi sectorwide approach to health sector development, and it allowed NDOH to use the funds for essential priorities at its own discretion, within the general framework of the NHP 1995–2000 and the NHP 2001–2010 and the objectives stipulated in the Loan Agreement. This flexibility allowed NDOH to use funds for essential priorities (such as drugs), coping with unforeseen crises to keep the health system operational (lack of government resources at the beginning of the financial year) and support financing of rural health service priorities directly through the provincial health authorities. For the provincial health authorities, access to additional funds for maintaining and improving service delivery was essential, especially in a context of reduced provincial budget allocations to health.
6 TA 3660-PNG: Health Sector Policy, approved on 30 May 2001, for $0.220 million and $0.242 million in 21 May
2002.
13
61. Excellent aid coordination was achieved, largely through close professional contact between staff members of key aid agencies, and sustained, despite some differences in approach. This collaboration was given practical expression in the endorsement by the Government’s highest authority of the Sector Wide Approach (SWAp) for health. 62. The reform process initiated under the HSDP introduced a framework that established a working relationship between NDOH and the provinces, in line with the Organic Law on Provincial Governments and Local Level Governments, and to which other departments and government agencies were also party. Management innovations were instituted, creating an environment of greater transparency and accountability. Issues related to performance began receiving greater attention, and public service officials were becoming increasingly responsive to governance issues. This is of fundamental importance in a country where public spending on health hardly translates into a larger supply of effective health supply, due to major inefficiency, poor accountability, and lack of transparency in public service provision. The program and project loans were considered highly relevant to the Government’s health sector development strategy and to ADB’s lending strategy for PNG. B. Efficacy in Achievement of Purpose
1. Health System Performance
63. Despite a coherent framework for health sector activity, as evidenced by the NHPs, the performance of the health sector deteriorated over recent years. While resources available to the health sector were substantially increased, performance dropped, as measured by the 19 core indicators. Most alarming was the deterioration in output indicators that measure what the health sector achieved.
Table 2: Overall Sector Performance as Measured by the 19 Core Indicators (%)
Indicator 1996–2001 1999–2000 2000–2001 Input 42.0 6.0 5.0 Process 6.7 6.3 (1.0) Output 0.5 (4.8) (1.8) Process and Output 3.1 (1.8) (1.6)
Source: Annual Health Sector Review 2002 64. These overall figures mask significant interprovincial differences. Provincial performance to some extent mirrors the level of poverty and also health expenditure in each province, highlighting an inadequate poverty focus in government expenditure for health. 65. Numerous factors, both internal and external to the health sector, contributed to the weak performance of the health sector over recent years. The principal factors are examined in the following paragraphs. 66. External Factors. Increased decentralization resulted in a disruption of the vertical integration of the health system. This broke the links between the different levels of care, reducing the ability of higher levels to call poorly performing lower levels to account. The management culture of PNG’s public sector was not performance-based, with few rewards available for officials who perform well and few sanctions available to deal with those who perform poorly. Financial management systems are weak, with little accountability and evidence
14
of misuse of public resources. Budgeted funds were not always available to enable implementation of sector activity plans. Many provincial authorities did not prioritized health services through budget support. Provincial governors all agreed to allocate 15% of provincial revenue to health. None have yet done so. Peripheral health services were damaged by disproportionate retrenchment of key health staff members, which occurred when savings were required. The macroeconomic position of PNG deteriorated over recent years, and projections would suggest that this will continue in the immediate future.
67. Factors Internal to the Health Sector. Health policy is generally sound, but policy implementation was weak or nonexistent, reflecting the lack of vertical integration in the health sector and management weaknesses. Supportive supervision, a basic management tool for achieving and maintaining performance, is weak at all levels of the health system. Focus was on developing high-quality studies and policy papers and guidelines, and significant effort was invested in planning rather than service delivery.
2. Reforms and Innovation
a. Financial Management Performance Requirements
68. Of paramount importance to the success of the HSDP was the introduction of measures that established minimum management performance levels (essentially strict adherence to the procurement and financial management rules) in the provinces as a prerequisite to qualifying for continued HSDP funding. This was possible because HSDP funding was appropriated at the level of NDOH. As such, NDOH was under no obligation to provide funds to a given province, although clearly the objectives of the NHP can be met only through the active support of provinces, which in turn implement their annual health activity plans. To qualify for continued HSDP funding, systematic supervisory reviews determined that provinces must comply with minimum requirements set in a procedure manual that was used to train all provincial staff members. 69. The initial release of funds to a PHO was contingent on the successful completion of training. The next release of funds depended on the outcome of the review on the use of the initial advance of funds. The required review took place in the province and was conducted by the HSDP secretariat, under the field visit heading, to better address the difficulties encountered. Each field visit or review would be recorded in a standard format covering issues and recommendations. Usually only a page or two in length, the field visit report would be shared within a week of the review with the PHA and senior management in NDOH.
b. Performance Audits
70. A series of further innovations were introduced in 2000. An independent audit firm was contracted to conduct performance audits on the use of HSDP funds by PHOs. The audits reviewed PHO conduct of business against HSDP procedures and expenditure statements and supporting documentation. Assets procured under the HSDP were physically verified, and a determination made as to whether value for money was obtained and if the assets were used for their declared and intended purpose. Four provincial performance audits were conducted in 2000, eight were conducted in 2001, and seven were conducted in 2002.
15
71. This process was subsequently extended to the national level. A performance audit7 covering financial management and procurement8 was carried out over a 2-month period, and the findings were presented by the accounting firm to NDOH’s senior executive management in 2001. The report established that controls over procurement and expenditure within NDOH were ineffective and not conducive to efficient operation. In particular, NDOH had an inadequate managerial control framework, inadequate operational procedures, and inadequate controls that did not ensure compliance with the Public Finance and Management Act. Furthermore, NDOH’s management was not able or willing to take appropriate action in the event of a suspected breach of statutory requirements or ethical business practice. Subsequent senior executive management meetings were held to review the performance audit findings, which resulted in a decision to proceed with the implementation of the recommended corrective measures. Importantly, senior executive management recognized that NDOH could not undertake the proposed reforms alone. The consulting branch of the accounting firm, which conducted the performance audit, was contracted by NDOH to assist in the implementation of the reform measures. 72. Perhaps one of the greatest constraints to progress in the reform process is the inability or unwillingness of senior management to exercise personnel management options in relation to nonperformance or breach of ethical business practices. NDOH’s ineffectiveness in this area of management responsibility is entrenched and supported by nonresponsive central government agencies, in particular DOF and the Department of Personnel Management. Public service reforms addressing personnel management issues will have to reach across all government agencies and all levels of government if they are to have a permanent impact on public service culture. In view of the foregoing, the HSDP was rated less efficacious. C. Efficiency in Achievement of Outputs and Purpose
73. No economic and financial analysis was done during project preparation. Assessing the efficiency of the investment is therefore not feasible. The Executing Agency’s project management efficiency and ADB’s support and supervision are discussed in paras. 55–59. This was rated less efficient. D. Preliminary Assessment of Sustainability
74. Substantial progress was made in the areas of (i) sector planning and prioritization and (ii) management and supervision, particularly at the provincial level. This progress led development partners and the Government to agree on a progressive move of assistance to PNG’s health sector, from project-type modality toward a sectorwide approach under the leadership of NDOH. Sustainability of this approach will depend on (i) steady leadership from NDOH, (ii) continued central agency support and commitment during this process, and (iii) continuous high levels of development partner coordination and commitment to the SWAp. 75. The reform process should be expected to take hold within NDOH over the medium term and perhaps longer depending on the pace of reform processes undertaken in other government departments and central agencies. Many of the weaknesses identified within NDOH are present to varying degrees in all government agencies. Progress in NDOH will have to be matched with progress in other agencies, to ensure sustainable public service reform.
7 Department of Health. 2001. Procurement and Expenditure Review. 8 The review covered recurrent expenditure by NDOH.

16
76. The sustainability of the investment component will depend, as a last resort, upon the availability of resources and the institutional capacity within the Government and NDOH to operate and manage the facilities built (mainly the Laloki national in-service training center in Port Moresby and the college in Madang). Human resources management was the sector where the least progress was made over the past 10 years, and a whole Government approach is necessary, given the decentralized nature of the health system in PNG and the authority of the Department of Personnel Management in this matter. Overall, sustainability was rated likely. E. Environmental, Sociocultural, and Other Impacts
77. The HSDP had no adverse environmental and sociocultural impacts. One of the major problems encountered with HSDP policy-based loans was that they were used as substitutions for a part of the funds normally allocated to the health sector by the provinces, instead of allowing extra funding to help implement the reform of the health sector. However, the HSDP clearly prevented many rural health services from completely collapsing at a time of fiscal stringency, which protected the rural poor against a further degradation of services. Therefore, institutional development and other impacts were considered moderate.
IV. OVERALL ASSESSMENT AND RECOMMENDATIONS
A. Overall Assessment
78. The HSDP was rated partly successful, based on the following considerations9:
(i) The HSDP’s objectives remained highly relevant long after appraisal. Organizational reforms are key to any progress in health outcomes in PNG.
(ii) The HSDP played a key role in preventing rural health services from further deteriorating during periods of severe budget cuts, particularly at the provincial level.
(iii) The HSDP allowed the Government and development partners to test the elements of a sectorwide approach in PNG, thus setting the foundation for a major transformation of the way assistance to the health sector is envisaged. It has, in particular, allowed the Government to take a position of leadership in managing assistance to the sector.
(iv) The health management system was further improved. However, many reforms envisaged were not implemented, primarily for lack of political will and commitment, which resulted in serious underfunding of the system and a further worsening of health outcomes. No progress was made in human resources management.
B. Lessons Learned
79. The choice of a quick-disbursing approach, with release of two large tranches was not adequate for the kind of reforms and support envisaged in the HSDP. This approach resulted in major difficulties between DOT and NDOH, with the latter not releasing funds as scheduled. The approach also did not allow ADB’s close monitoring of the progress made during the program’s entire life, as any leverage disappeared after the release of the second tranche.
9 This PCR is part of a sample of PCRs independently reviewed by the Operations Evaluation Department. The
review has validated the methodology used and the rating given per PAI No. 6.07 para. 12.
17
80. Capacity building through the use of consultants varied largely depending on the area. The major problem was the availability of local counterparts and the continuity of their presence during the job. Too often they were transferred to other sectors after being trained. While this modality was very effective with the HMIS, due to the stability and leadership within the monitoring and research branch, the transfer of the senior finance officer trained in the HSDP secretariat to another sector puts at risk the capacity built in this area by the attached technical assistance. 81. The reform process underway in NDOH, with the assistance of an international accounting firm, also needs to be sustained. The progress to date is substantial, but a change in public service culture will require continued assistance and the progressive and active involvement of the relevant government support agencies, including the Auditor General’s Office, DOF, Department of Intergovernment Relations, Department of Personnel Management, and others. A public service culture change cannot occur in a sustainable manner in one government department alone. 82. The HSDP established early on a policy of producing and disseminating information on as broad a basis as possible. The attention given to transparency and resolving issues raised through the monitoring process also served to underscore the importance of the monitoring and information process. The useful application of information in the management process is acquired through practice. Only when managers have acquired this skill is the costly exercise of producing information justified. 83. Alternate staffing arrangements should be introduced in PIUs, in cases when the project manager or project coordinators go on long leave, to ensure smooth project implementation. Alternates should have hands-on experience in administering projects, specifically those funded by ADB. C. Recommendations
1. Program Related
84. Future Monitoring. The performance monitoring framework of the health sector, which was developed under the HSDP, should continue to be used and refined to measure the impact of the reforms on health outcomes. NDOH is preparing (i) the business plan for Laloki college and (ii) a national in-service training policy. These should be approved by the end of 2004. Monitoring the 2005 budget appropriation for the operation of the college will also be important. 85. Additional Assistance. The Government requested further ADB assistance in the health sector, through ADB’s participation in the SWAp. Project preparatory technical assitance was provided, and further discussions are scheduled to refine the form of assistance ADB would provide. The SWAp is being considered as a program loan rather than a project loan. 86. Timing of the Program Performance Audit Report. The report can be prepared by 2005, when additional data on achievement of outcomes is available, notably progress in provincial budgeting and a business plan for the Laloki in-service training center. In view of the nature of the program and the overlap of interventions between the HSDP and AusAID’s program of assistance (which contributed financially, along with New Zealand's International and Aid Agency, to the trust account), the postevaluation should consider whether a more useful exercise might be a joint evaluation, with the Government, AusAID, and New Zealand's International Aid and Development Agency.

18
2. General
87. In laying the foundation to develop the SWAp in the health sector, the HSDP undertook initiatives in key support areas. These initatives contributed to the success of the overall program. Continued attention to these important support functions should remain an essential feature to the developing SWAp and health sector improvement program. Some of these areas are covered in the following paragraphs. 88. The program of external audits contributed much to broadening public sector recognition of the fact that governance issues are at the heart of poor performance levels in the health sector. This process, and the debate it fuels, should be maintained and supported. 89. Supervision and support by the HSDP secretariat of PHOs and PHAs was very beneficial, in most cases. However, a need exists to take this process further down the public health infrastructure pyramid, to the district and health facilities. Indeed, experience revealed that the basic principles upon which functioning organizations and management are grounded are frequently lacking. These principles and their practical applications are best taught in an on-the-job, hands-on environment. NDOH, which has a vested interest in improving performance at the decentralized level, should itself devote greater human resources and time to this function.

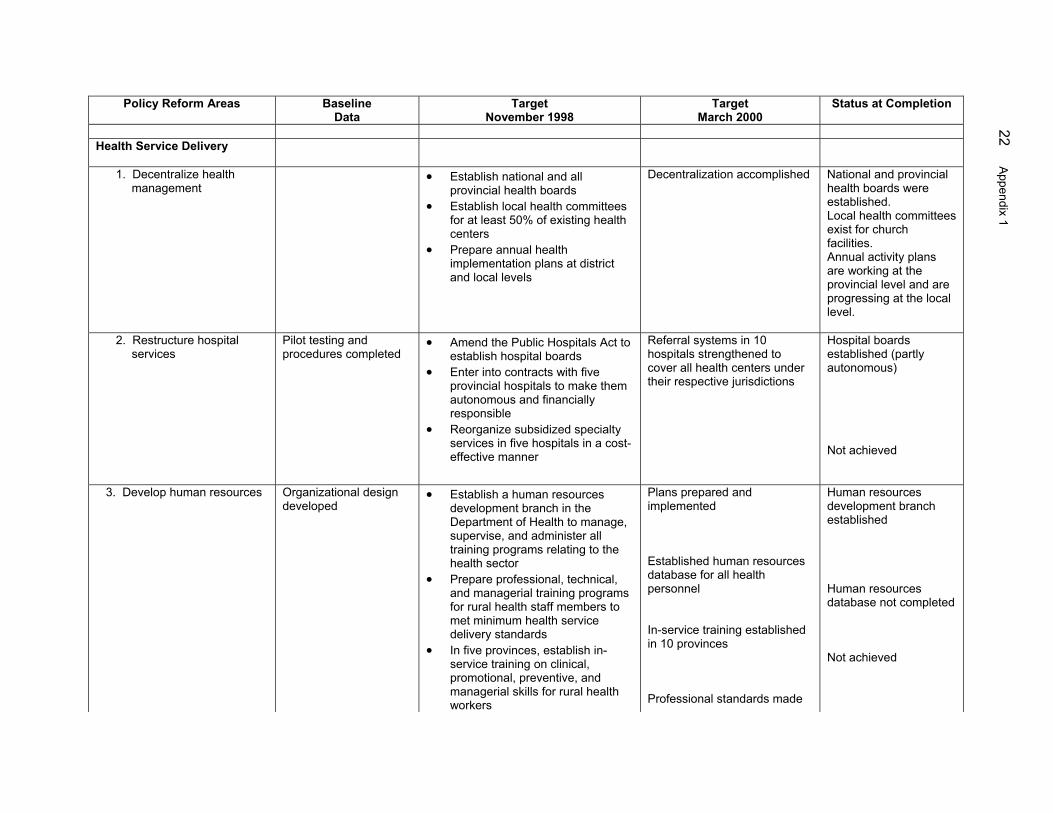
IMPLEMENTATION AND COMPLIANCE WITH PROGRAM MEASURES
(Health Sector Development Program)
Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
A. Shift Emphasis from Urban to Rural Health Services
1. Enhance resources to rural areas
1995 level of expenditure
• Increase financial allocations for rural health centers and aid posts by not less than 10% over the 1996 level of expenditure every year in 1997, 1998, and 1999
Restoring and maintaining overall government health expenditure to the level of 1993
Partly accomplished. Health expenditure for rural areas was restored to previous levels only when development partners’ assistance is included.
Only ad hoc training is provided
• Improve effectiveness of rural facilities through increased on-site training of 5 person-days per year for health center staff members
Ten person-days per year on-site training for each health center staff member in rural areas
Not complied with.
Ad hoc visits are made according to expediency
• At lease two clinical supervisory visits per year by hospital medical staff members to rural health centers
Four clinical supervisory visits per year to each rural health center
Not complied with. Only 33% of health facilities had a medical officer visit in 2002, and 41% had a provincial visit.
2. Promote community participation in rural health services
• Promote community participation in health delivery decisions and implementation by providing written instructions and guidelines for community health committees at each health center.
Not complied with. Community health committees are active in most church facilities, not government facilities.
B. Shift Orientation from Curative to Promotional and Preventive Health Services
1. Improve epidemiological analysis for strengthening
Data available for selected districts only
Prepare health survey scores for 89 districts
Health survey scores for 89 districts prepared
Complied with. HMIS follows up, gathers, and analyzes data on all
Appendix 1 19

Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
promotional and preventive health services
districts.
2. Improve family health services.
Antenatal visits 68.0% Supervised delivery 30.0% Family Planning acceptors 6.7% Measles 35% Triple antigen 59% Refrigerators 86% Access to safe water 12%
Increase maternal and child health patrols, to achieve the following targets: Antenatal visits 74.0% Supervised delivery 45.0% Family planning acceptors 7.9% Increased immunization to achieve the following targets: Measles 57% Triple antigen 65% Increase provision of refrigerators to 94% of health centers. Access to safe water 20%
Antenatal visits 80% Supervised delivery 50% Family planning acceptors 9% Measles 70% Triple antigen 70% Refrigerators 99% Access to safe water 30%
Data 2002: Antenatal visits 57.0% Supervised delivery 38.0% Family planning acceptors 6.2% Measles 53% Triple antigen 61% Refrigerators 89% Access to safe water 24%
3. Improve disease control
Tuberculosis treatment completion rate 65%
Improve contract screening and treatment completion rate for tuberculosis patients up to 74%
Tuberculosis treatment completion rate 80%
Tuberculosis treatment completion rate 67%
4. Improve health Distribution of standard treatment Health center coverage Data not available
20 Appendix 1

Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
information and education campaign
protocols and health education materials to health centers 30% Provide 60 minutes of weekly radio programming to improve knowledge of nutrition and other relevant health subjects
50% Not achieved
Radio network coverage 60%
Establish radio communications network and provide training for medical use and maintenance to 78% of health centers
Radio communication coverage 90%
Not achieved
Promote healthy behavior with campaigns, information, and education against smoking and sexually transmitted diseases and HIV/ AIDS prevention, through posters located in 30% of health centers
Partly achieved. Efforts underway toward prevention of HIV/AIDS over the 1996 level of expenditure AIDS
C. Undertake Financial Reforms in the Health Sector
1. Assure steady and stable allocation of financial resources
Health expenditures as percentage of government expenditures: 7.7% in 1994
Increase government health expenditure to 8% of total government health expenditures
Health expenditures as percentage of Government expenditures: 10%
Achieved
2. Share the burden of public health expenditures with users
Revenue collections $4 of hospital costs
Continue increase of revenue collection from hospital users to 8% of total hospital operating costs
Revenue collections 10% of hospital costs
Revenue collection less than 10%. User fees are raised but are poorly managed.
3. Allocate greater amounts of resources for goods and services
Drugs and medical supplies budget K15.4 million
Increase allocation for drugs and medical supplies to 25% of the Department of Health's budgetary allocation for 1998
Allocations for drugs and supplies to reach 30% of the Department of Health’s budget
Drugs and medical supplies are 32% of the Department of Health’s budget when development partners’ contributions are included.
D. Enhance the Efficiency of
Appendix 1 21
Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
Health Service Delivery 1. Decentralize health
management • Establish national and all
provincial health boards • Establish local health committees
for at least 50% of existing health centers
• Prepare annual health implementation plans at district and local levels
Decentralization accomplished National and provincial health boards were established. Local health committees exist for church facilities. Annual activity plans are working at the provincial level and are progressing at the local level.
2. Restructure hospital services
Pilot testing and procedures completed
• Amend the Public Hospitals Act to establish hospital boards
• Enter into contracts with five provincial hospitals to make them autonomous and financially responsible
• Reorganize subsidized specialty services in five hospitals in a cost-effective manner
Referral systems in 10 hospitals strengthened to cover all health centers under their respective jurisdictions
Hospital boards established (partly autonomous) Not achieved
3. Develop human resources Organizational design developed
• Establish a human resources development branch in the Department of Health to manage, supervise, and administer all training programs relating to the health sector
• Prepare professional, technical, and managerial training programs for rural health staff members to met minimum health service delivery standards
• In five provinces, establish in-service training on clinical, promotional, preventive, and managerial skills for rural health workers
Plans prepared and implemented Established human resources database for all health personnel In-service training established in 10 provinces Professional standards made
Human resources development branch established Human resources database not completed Not achieved
22 Appendix 1

Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
• Upgrade preservice and in-service
training for 30% of nursing officers by updating curricula, training teachers, and providing print and audiovisual materials
• Prepare and enforce operational and professional standards, assign supervisory responsibilities for enforcement of standards, and implement standards through quarterly supervisory visits
• Improve quality of training imparted by community health worker schools
operational and implemented
Not achieved Curriculum revised, but not yet fully implemented
4. Improve management of drugs and medical supplies
Preparation started • Privatize distribution of drugs and medical supplies to nodal centers in provincial hospitals
• Invite private drug and pharmaceutical companies to establish outlets in all hospitals
• Conduct staff member training (30 training days) in procurement procedures, contract packaging and bidding, and maintenance of cold chains for vaccines
Drug distribution privatized Not complied with
5. Increase involvement of nongovernment organizations and churches and the private sector
• Adopt guidelines for better integration of nongovernment organization and church health services with public health services
• Provinces to formalize relationships with nongovernment organization- and church-operated health services by establishing coordinating committees and rationalizing allocation of financial, medicinal, and personnel resources.
Standards of service published Achieved Partnership agreement between Government and churches health services signed Review/audit of churches health services done
Appendix 1 23

Policy Reform Areas Baseline Data
Target November 1998
Target March 2000
Status at Completion
• Monitor the standards of
nongovernment organization- and church-operated health services
• Promote private sector health services by establishing standards of services and incentives
• Promote involvement of private sector in health insurance schemes
No health insurance established
6. Enhance the health management information system and support medical research
7. Develop health facilities
maintenance programs
Basic information system established No systematic procedures in place
• Develop a national and uniform computerized monitoring and evaluation system based on standard health indicators
• Establish a national health management information system that includes a reporting system for service delivery, disease surveillance, and personnel information system
• Improve the link between research efforts and national health priorities by instituting research grants in priority areas
• Issue guidelines for maintenance
of health facilities and equipment through local boards and committees
• Create a fund for providing matching grants for maintenance
Improved links established, grants allocated to priority areas. Maintenance programs developed, guidelines produced, training in progress
Performance Monitoring Framework established, with comprehensive coverage of all the districts on service delivery and disease surveillance Medium-Term Expenditure Framework for health prioritizes funding on the basis of the burden of disease measured Maintenance of technical equipment done by trained provincial hospitals teams
• Establish standards and procedures for maintaining equipment and facilities by developing manuals and guidelines in local languages and providing staff member training
24 Appendix 1

All amounts in US dollars
Component Appraisal Actual (all local)Total Foreign Local Total Foreign Local
Part I - Health Personnel Trainingcompetency-based in-service training system/upgrading training facilities (CAHS/Media Print/Laloki)management training and job supervisionHRD Capacity Building - trainings
(a) Civil Works 3,030,000.00 2,600,000.00 430,000.00 4,748,592.00 4,748,592.00 - 790,000.00 2,006,804.04 (b) Equipment 910,000.00 800,000.00 110,000.00 255,560.00 185,333.00 70,227.00 225,000.00 39,168.16 (c) PIU 105,000.00 52,500.00 52,500.00 14,039.50 384.00 13,655.50 71,500.00 19,841.07 (d) Training/Fellowship 1,485,000.00 550,000.00 935,000.00 356,840.00 106,344.36 250,495.64 876,000.00 245,277.67 (e) Consultancy Services 1,205,000.00 1,147,500.00 57,500.00 95,152.00 48,667.08 46,484.92 115,000.00 567,700.93 (f) Operations/Maintenance 100,000.00 100,000.00 31,208.00 - 31,208.00 100,000.00 149.44 (g) Service Charges 100,000.00 100,000.00 - 23,603.00 23,603.00 -
Subtotal (A) 6,935,000.00 5,250,000.00 1,685,000.00 5,524,994.50 5,112,923.44 412,071.06 2,177,500.00 2,878,941.31 Part II - Health Management Information System (HMIS)integrating all available health databases at national and provincial levels into an inter-linked health management information system
(a) Civil Works - - - - - (b) Equipment - - - - - 2,970.59 (c) PIU 105,000.00 52,500.00 52,500.00 14,039.50 384.00 13,655.50 71,500.00 19,692.64 (d) Training/Fellowship 435,000.00 380,000.00 55,000.00 221,793.94 66,096.64 155,697.30 137,014.35 (e) Consultancy Services 1,205,000.00 1,147,500.00 57,500.00 697,264.00 356,891.94 340,372.06 115,000.00 113,713.14 (f) Operations/Maintenance 100,000.00 100,000.00 31,208.00 - 31,208.00 100,000.00 149.43 (g) Service Charges 100,000.00 100,000.00 0.00 23,603.00 23,603.00 -
Subtotal (B) 1,945,000.00 1,680,000.00 265,000.00 987,908.44 446,975.58 540,932.86 286,500.00 273,540.15 Physical Escalation 610,000.00 470,000.00 140,000.00 - 240,000.00 Price Escalation 510,000.00 300,000.00 210,000.00 296,000.00
Grand Totals 10,000,000.00 7,700,000.00 2,300,000.00 6,512,902.94 5,559,899.02 953,003.92 3,000,000.00 3,152,481.46
Notes :1. Actual amount disbursed data for ADB financing were taken from the ADB LFIS mainframe system queries.2. Data for GoPNG were provided by the project accountant of the PIU/EA.Source : Asian Development Bank's RRP and EA's ledgers.
Appraisal Actual
Loan 1518-PNG(SF) : Health Sector Investment Project
GoPNGADB
Schedule of Actual Expenditures from ADB and Borrower's Funds
Appendix 2 25
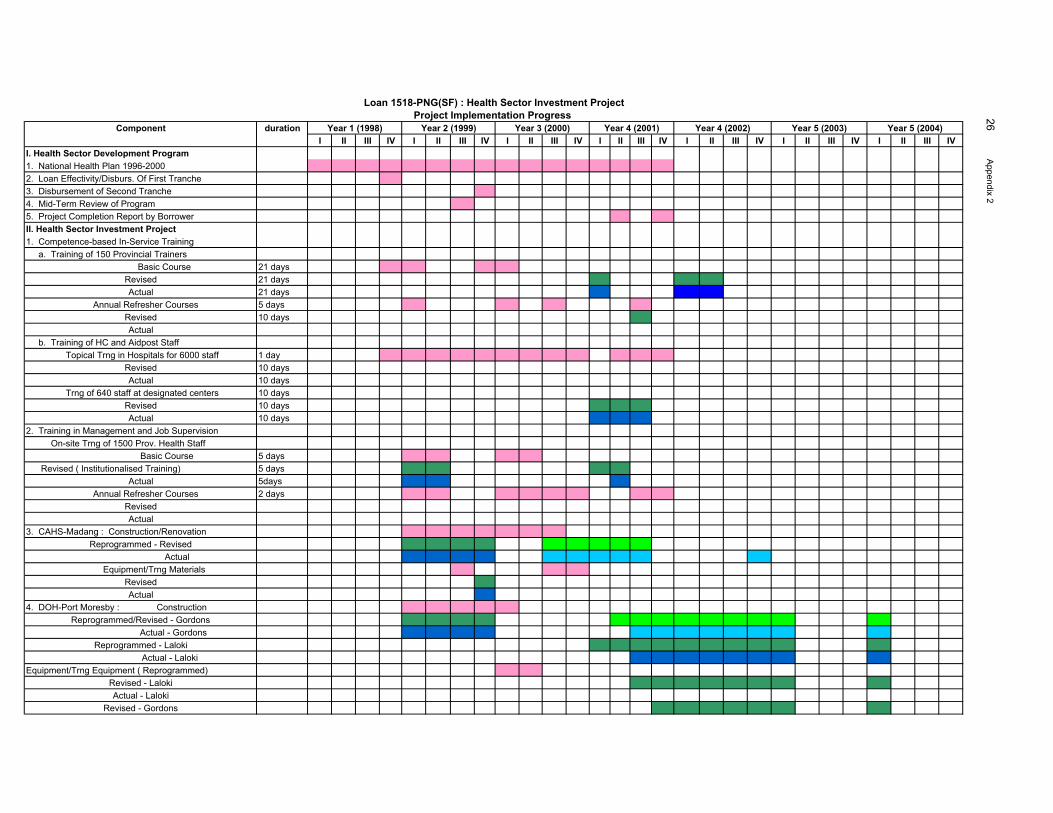
Component durationI II III IV I II III IV I II III IV I II III IV I II III IV I II III IV I II III IV
I. Health Sector Development Program1. National Health Plan 1996-20002. Loan Effectivity/Disburs. Of First Tranche3. Disbursement of Second Tranche4. Mid-Term Review of Program5. Project Completion Report by BorrowerII. Health Sector Investment Project1. Competence-based In-Service Training a. Training of 150 Provincial Trainers Basic Course 21 days
Revised 21 daysActual 21 days
Annual Refresher Courses 5 daysRevised 10 daysActual
b. Training of HC and Aidpost Staff Topical Trng in Hospitals for 6000 staff 1 day
Revised 10 daysActual 10 days
Trng of 640 staff at designated centers 10 daysRevised 10 daysActual 10 days
2. Training in Management and Job Supervision On-site Trng of 1500 Prov. Health Staff Basic Course 5 days Revised ( Institutionalised Training) 5 days
Actual 5days Annual Refresher Courses 2 days
RevisedActual
3. CAHS-Madang : Construction/RenovationReprogrammed - Revised Actual
Equipment/Trng MaterialsRevisedActual
4. DOH-Port Moresby : ConstructionReprogrammed/Revised - Gordons Actual - Gordons
Reprogrammed - Laloki Actual - Laloki
Equipment/Trng Equipment ( Reprogrammed)Revised - LalokiActual - Laloki
Revised - Gordons
Loan 1518-PNG(SF) : Health Sector Investment ProjectProject Implementation Progress
Year 4 (2002) Year 5 (2003) Year 5 (2004)Year 1 (1998) Year 2 (1999) Year 3 (2000) Year 4 (2001)
26 Appendix 2
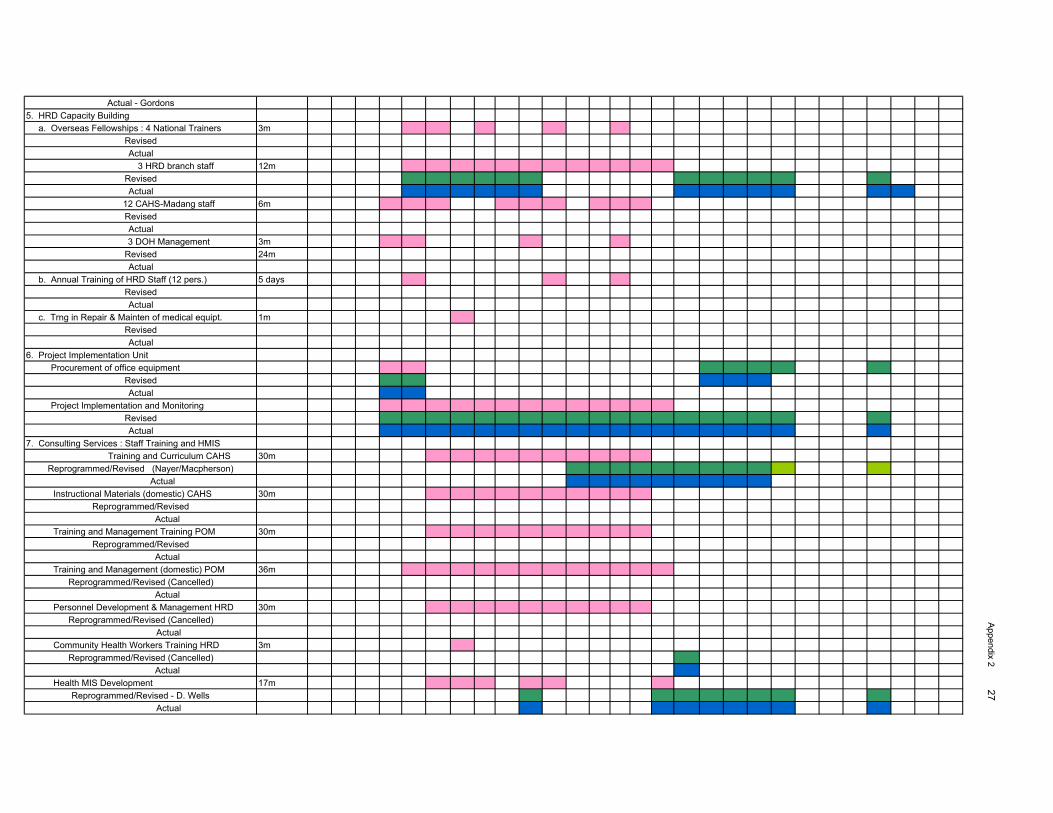
Actual - Gordons5. HRD Capacity Building a. Overseas Fellowships : 4 National Trainers 3m
RevisedActual
3 HRD branch staff 12mRevisedActual
12 CAHS-Madang staff 6mRevisedActual
3 DOH Management 3mRevised 24mActual
b. Annual Training of HRD Staff (12 pers.) 5 daysRevisedActual
c. Trng in Repair & Mainten of medical equipt. 1mRevisedActual
6. Project Implementation Unit Procurement of office equipment
RevisedActual
Project Implementation and MonitoringRevisedActual
7. Consulting Services : Staff Training and HMIS Training and Curriculum CAHS 30m
Reprogrammed/Revised (Nayer/Macpherson) Actual
Instructional Materials (domestic) CAHS 30mReprogrammed/Revised
Actual Training and Management Training POM 30m
Reprogrammed/Revised Actual
Training and Management (domestic) POM 36mReprogrammed/Revised (Cancelled)
Actual Personnel Development & Management HRD 30m
Reprogrammed/Revised (Cancelled) Actual
Community Health Workers Training HRD 3mReprogrammed/Revised (Cancelled)
Actual Health MIS Development 17m
Reprogrammed/Revised - D. Wells Actual
Appendix 2 27
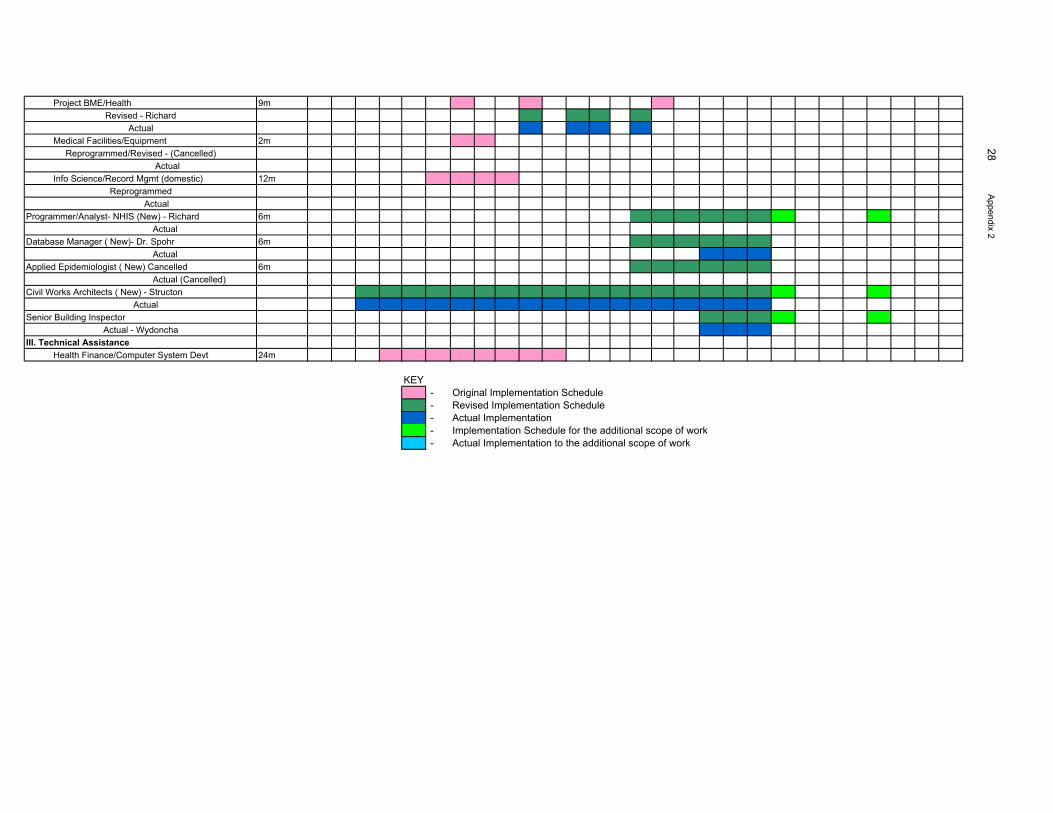
Project BME/Health 9mRevised - Richard
Actual Medical Facilities/Equipment 2m
Reprogrammed/Revised - (Cancelled) Actual
Info Science/Record Mgmt (domestic) 12mReprogrammed Actual
Programmer/Analyst- NHIS (New) - Richard 6m ActualDatabase Manager ( New)- Dr. Spohr 6m ActualApplied Epidemiologist ( New) Cancelled 6m Actual (Cancelled)Civil Works Architects ( New) - Structon
ActualSenior Building Inspector
Actual - WydonchaIII. Technical Assistance Health Finance/Computer System Devt 24m
KEY - Original Implementation Schedule - Revised Implementation Schedule - Actual Implementation - Implementation Schedule for the additional scope of work - Actual Implementation to the additional scope of work
28 Appendix 2
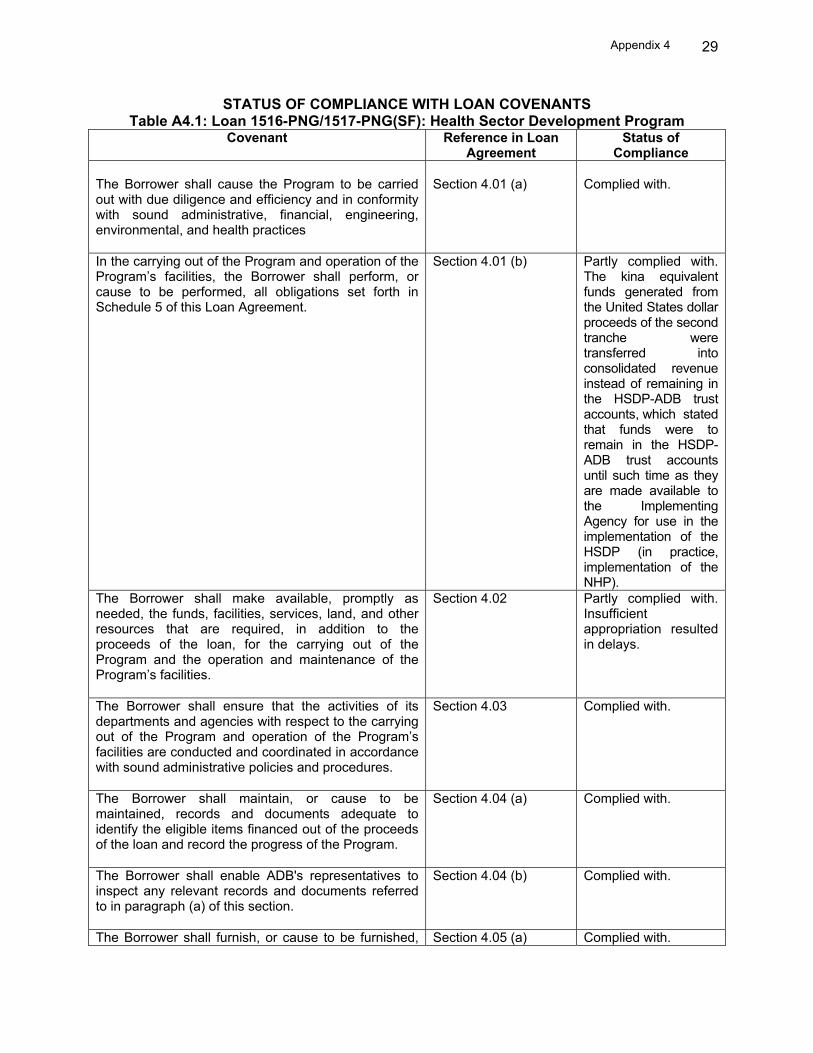
Appendix 4 29
STATUS OF COMPLIANCE WITH LOAN COVENANTS Table A4.1: Loan 1516-PNG/1517-PNG(SF): Health Sector Development Program
Covenant Reference in Loan Agreement
Status of Compliance
The Borrower shall cause the Program to be carried out with due diligence and efficiency and in conformity with sound administrative, financial, engineering, environmental, and health practices
Section 4.01 (a) Complied with.
In the carrying out of the Program and operation of the Program’s facilities, the Borrower shall perform, or cause to be performed, all obligations set forth in Schedule 5 of this Loan Agreement.
Section 4.01 (b) Partly complied with. The kina equivalent funds generated from the United States dollar proceeds of the second tranche were transferred into consolidated revenue instead of remaining in the HSDP-ADB trust accounts, which stated that funds were to remain in the HSDP-ADB trust accounts until such time as they are made available to the Implementing Agency for use in the implementation of the HSDP (in practice, implementation of the NHP).
The Borrower shall make available, promptly as needed, the funds, facilities, services, land, and other resources that are required, in addition to the proceeds of the loan, for the carrying out of the Program and the operation and maintenance of the Program’s facilities.
Section 4.02 Partly complied with. Insufficient appropriation resulted in delays.
The Borrower shall ensure that the activities of its departments and agencies with respect to the carrying out of the Program and operation of the Program’s facilities are conducted and coordinated in accordance with sound administrative policies and procedures.
Section 4.03 Complied with.
The Borrower shall maintain, or cause to be maintained, records and documents adequate to identify the eligible items financed out of the proceeds of the loan and record the progress of the Program.
Section 4.04 (a) Complied with.
The Borrower shall enable ADB's representatives to inspect any relevant records and documents referred to in paragraph (a) of this section.
Section 4.04 (b) Complied with.
The Borrower shall furnish, or cause to be furnished, Section 4.05 (a) Complied with.

Appendix 4 30
Covenant Reference in Loan Agreement
Status of Compliance
to ADB all such reports and information as ADB shall reasonably request concerning (i) the loan, and the expenditure of the proceeds and maintenance of the service thereof; (ii) the goods financed out of the proceeds of the loan; (ii) the counterpart funds and the use thereof; (iv) the implementation of the Program, including the accomplishment of the targets and carrying out of the actions set out in the policy letter; (v) the financial and economic conditions in the territory of the Borrower and the international balance-of-payments position of the Borrower; and (vi) the remaining matters, if any, relating to the purposes of the loan. Without limiting the generality of the foregoing, the Borrower shall furnish, or cause to be furnished, to ADB quarterly reports on the carrying out of the Program and the accomplishment of the targets and carrying out of the actions set out in the policy letter. Such reports shall be submitted in such form and in such detail and within such a period as ADB shall reasonably request, and they shall indicate, among other things, progress made and problems encountered during the quarter under review, steps taken or proposed to be taken to remedy these problems, and proposed programs of activities and expected progress during the following quarter.
Section 4.05 (b) Complied with.
Promptly after the closing date for withdrawals from the loan account, but in any event not later than 3 months thereafter or at such a later date as may be agreed for this purpose between the Borrower and ADB, the Borrower shall prepare and furnish to ADB a report, in such form and in such detail as ADB shall reasonably request, on the execution of the Program, including the cost, performance by the Borrower of its obligation under this Loan Agreement, and accomplishment of the purposes of the loan.
Section 4.05 (c) Complied with.
The mutual intention of the Borrower and ADB is that no other external debt owed a creditor other than ADB shall have any priority over the loan by way of a lien on the assets of the Borrower. To that end, the Borrower undertakes (i) that, except as ADB may otherwise agree, if any lien shall be created on any assets of the Borrower as security for any external debt, such lien will ipso facto equally and ratably secure the payment of the principal of and service charge and any other charge on the loan; and (ii) that the Borrower, in creating or permitting the creation of any such lien, will make express provision to that effect.
Section 4.06 (a) Complied with.
The provisions of paragraph (a) of this section shall Section 4.06 (b) Complied with.

Appendix 4 31
Covenant Reference in Loan Agreement
Status of Compliance
not apply to (i) any lien created on property, at the time of purchase thereof, solely as security for payment of the purchase price of such property or (ii) any lien arising in the ordinary course of banking transactions and securing a debt maturing not more than 1 year after its date. The term "assets of the Borrower" as used in paragraph (a) of this section includes assets of the Borrower and assets of any entity owned or controlled by or operating for the account or benefit of the Borrower, including assets of Bank of Papua New Guinea and other institutions performing the functions of a central bank for the Borrower.
Section 4.06 (c) Complied with.
Regarding the implementation of the policy letter, the Borrower shall carry out, or cause to be carried out, the policies and actions set out in the policy letter, which include the schedule of policy reforms attached thereto, unless otherwise agreed with ADB.
Schedule 5, para. 1
Partially complied with. Some achievements were made and some groundwork was established. This will be a continuing effort of the health sector and government in regard to overall implementation of public sector reforms.
Regarding policy dialogue, the Borrower shall keep ADB informed of and the Borrower and ADB shall from time to time exchange views on the progress made in carrying out the policies and actions set out in the policy letter and in the health policy and national health plan. The Borrower shall keep ADN informed of policy discussions concerning the health sector undertaken with other international and bilateral aid agencies, as ADB may reasonably request, and shall provide ADB with an opportunity to comment on any resulting proposals. The Borrower shall continue policy dialogue with ADB on problems and constraints encountered during implementation of the Program and on desirable changes to overcome or mitigate such problems and constraints. Regarding the use of counterpart funds, the Borrower shall ensure that the counterpart funds are used to support implementation of the health reforms detailed in the national health plan under the Program for rural health services. Withdrawals from the special account shall be in support of priority programs and projects implemented by NDOH that are satisfactory to ADB for
Schedule 5, para.2 Schedule 5, para. 3 Schedule 5, para. 4 Schedule 5, para. B.9
Complied with. Complied with. Complied with. Partly complied with. Some funds were used to support indirect expenditures that were not program priorities but essential to health service

Appendix 4 32
Covenant Reference in Loan Agreement
Status of Compliance
this purpose, in amounts to be agreed with ADB. Regarding fees for health services, the Borrower shall ensure, or cause to be ensured, that the health boards in consultation with NDOH shall: (i) develop an assessment mechanism to determine the adequacy of health service fees; (ii) introduce cost recovery measures within NDOH-recommended limits that ensure free access to health services for the poor and vulnerable groups; and (iii) ensure that visits for immunization programs, family planning services, safe motherhood, nutrition and community school health programs are exempted from payment of such user fees. Regarding user fee revenues, the Borrower shall ensure, or cause to be ensured, that (i) DOF and NDOH develop systems for accounting and control of the user fees to be collected by hospitals, health centers, and aid posts and (ii) hospital, health center, and aid post accounting and control systems referred to under (a) have been developed in order to fund maintenance programs for health facilities and equipment. Regarding health legislation, the Borrower shall prepare and finalize, to the satisfaction of ADB, the following: (i) a draft national health (administration) bill and (ii) a draft drugs registration bill. The Borrower shall also finalize and adopt, to the satisfaction of ADB, the National Drugs Policy.
Schedule 5, para. 17 Schedule 5, para. 18 Schedule 5, para. 20
provision (e.g., settling outstanding utility bills for NDOH and hospitals). Partly complied with. These are ongoing reform processes that will take time to achieve. Partly complied with. These are ongoing reform processes that will take time to achieve. Partly complied with. These are ongoing reform processes that will take time to achieve.
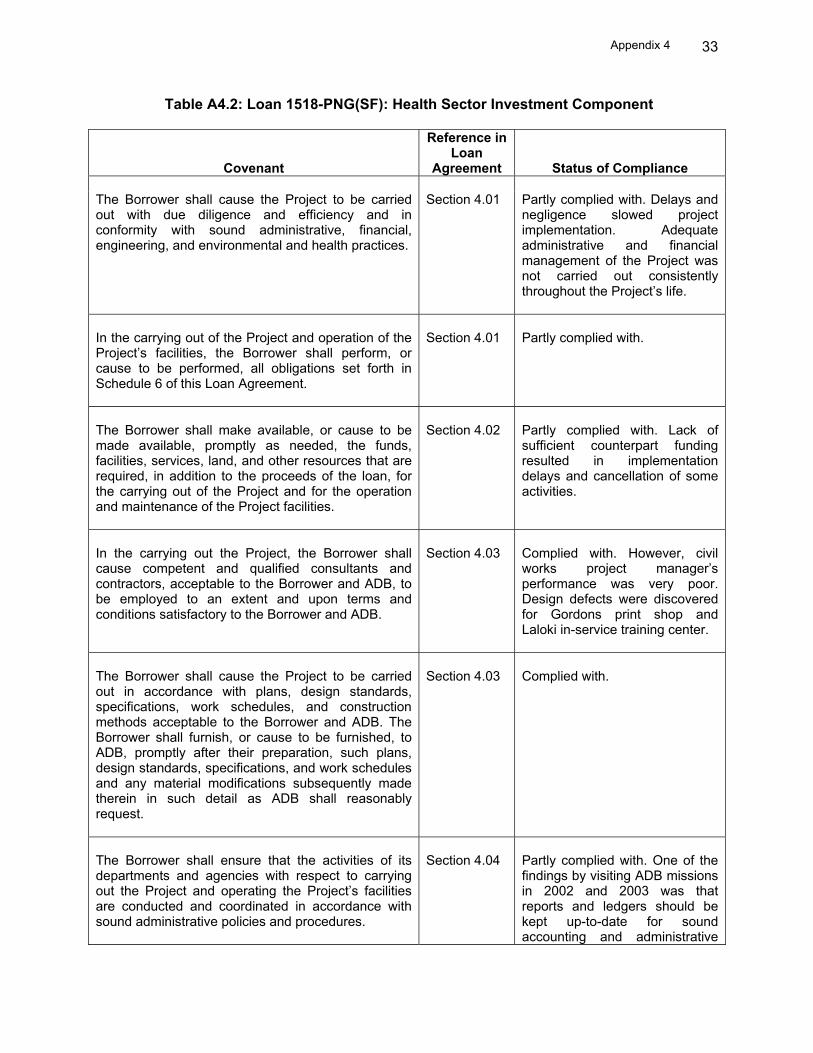
Appendix 4 33
Table A4.2: Loan 1518-PNG(SF): Health Sector Investment Component
Covenant
Reference in Loan
Agreement
Status of Compliance The Borrower shall cause the Project to be carried out with due diligence and efficiency and in conformity with sound administrative, financial, engineering, and environmental and health practices.
Section 4.01 Partly complied with. Delays and negligence slowed project implementation. Adequate administrative and financial management of the Project was not carried out consistently throughout the Project’s life.
In the carrying out of the Project and operation of the Project’s facilities, the Borrower shall perform, or cause to be performed, all obligations set forth in Schedule 6 of this Loan Agreement.
Section 4.01
Partly complied with.
The Borrower shall make available, or cause to be made available, promptly as needed, the funds, facilities, services, land, and other resources that are required, in addition to the proceeds of the loan, for the carrying out of the Project and for the operation and maintenance of the Project facilities.
Section 4.02
Partly complied with. Lack of sufficient counterpart funding resulted in implementation delays and cancellation of some activities.
In the carrying out the Project, the Borrower shall cause competent and qualified consultants and contractors, acceptable to the Borrower and ADB, to be employed to an extent and upon terms and conditions satisfactory to the Borrower and ADB.
Section 4.03
Complied with. However, civil works project manager’s performance was very poor. Design defects were discovered for Gordons print shop and Laloki in-service training center.
The Borrower shall cause the Project to be carried out in accordance with plans, design standards, specifications, work schedules, and construction methods acceptable to the Borrower and ADB. The Borrower shall furnish, or cause to be furnished, to ADB, promptly after their preparation, such plans, design standards, specifications, and work schedules and any material modifications subsequently made therein in such detail as ADB shall reasonably request.
Section 4.03
Complied with.
The Borrower shall ensure that the activities of its departments and agencies with respect to carrying out the Project and operating the Project’s facilities are conducted and coordinated in accordance with sound administrative policies and procedures.
Section 4.04
Partly complied with. One of the findings by visiting ADB missions in 2002 and 2003 was that reports and ledgers should be kept up-to-date for sound accounting and administrative

Appendix 4 34
Covenant
Reference in Loan
Agreement
Status of Compliance management of the Project. However, minimal improvement was noted by ADB.
The Borrower shall make arrangements satisfactory to ADB for insurance of the Project’s facilities to such extent and against such risks and in such amounts as shall be consistent with sound practice.
Section 4.05
Complied with.
Without limiting the generality of the foregoing, the Borrower undertakes to insure, or cause to be insured, the goods to be imported for the Project and to be financed out of the proceeds of the loan against hazards incident to the acquisition, transportation, and delivery thereof and of the place of use or installation, and for such insurance any indemnity shall be payable in a currency freely unable to replace or repair such goods.
Section 4.05
Partly complied with. GoPNG self-insures its assets. Goods procured overseas are CIF.
The Borrower shall maintain, or cause to be maintained, records and accounts adequate to identify the goods and services and other items of expenditure financed out of the proceeds of the loan to disclose the use thereof in the Project; record the progress of the Project (including the cost thereof); and reflect, in accordance with consistently maintained sound accounting principles, the operations and financial condition of the agencies of the Borrower responsible for carrying out the Project and operation of the Project’s facilities or part thereof.
Section 4.06
Partly complied with. Records were not up-to-date, recordings of financial transactions were not properly done, reporting mechanisms were not adequate, and reports were not provided on time. Audited financial statements were provided very late, despite several follow-up attempts.
The Borrower shall (i) cause NDOH to establish and maintain separate accounts for the Project and have such accounts and statements audited annually, in accordance with appropriate auditing standards consistently approved by independent auditors, whose qualifications, experience, and terms of reference are acceptable to ADB; (ii) furnish to ADB as soon as available, but in any event not later than 12 months after the end of each related fiscal year, certified copies of such audited accounts and financial statements and the report of the auditors relating thereto, including the auditors’ opinion on the use of loan proceeds and compliance with the covenants of this Loan Agreement, all in the English language; and (iii) furnish to ADB such other information concerning such account and financial statements and the audit thereof as ADB shall from time to time reasonably request.
Section 4.06
Partly complied with. Records were not up-to-date, recordings of financial transactions were not properly done, reporting mechanisms were not adequate, and reports were not provided on time. Audited financial statements were provided very late, despite several follow-up attempts.

Appendix 4 35
Covenant
Reference in Loan
Agreement
Status of Compliance The Borrower shall enable ADB, upon ADB’s request, to discuss the Borrower’s financial statements for the Project and its financial affairs related to the Project, from time to time, with the Borrower’s auditors and ensure that a representative of such auditors shall participate in any such discussions requested by ADB, provided that any such discussion shall be conducted only in the presence of an authorized officer of the Borrower, unless the Borrower shall otherwise agree.
Section 4.06
Complied with.
The Borrower shall furnish, or cause to be furnished, to ADB all such reports and information as ADB shall reasonably request concerning (i) the loan and the expenditure of the proceeds and maintenance of the service thereof; (ii) the goods and services and other items of expenditure financed out of the proceeds of the loan; (iii) the Project; (iv) the administrative, operations, and financial condition of the agencies of the Borrower responsible for carrying out the Project operation of the Project’s facilities or any part thereof; (v) the financial and economic conditions in the territory of the Borrower and the international balance-of-payments position of the Borrower; and (vi) the other matters, if any, relating to the purposes of the loan.
Section 4.07
Partly complied with. The project implementation unit and the Executing Agency have not been diligently updating their financial records, and the reporting feedback system is poor, which is very evident whenever visiting ADB missions come for reviews and the unit and agency are slow to provide the required data and information. With concientious administrative work, all reporting mechanisms should be easily extracted from computers and retrieved.
Without limiting the generality of the foregoing, the Borrower shall cause NDOH to furnish to ADB quarterly reports on the carrying out of the Project and on the operation and management of the Project’s facilities. Such reports shall be submitted in such form and in such detail and within such a period as ADB shall reasonably request and shall indicate, among other things, progress made and problems encountered during the quarter under review, steps taken or proposed to be taken to remedy these problems and the proposed program of activities, and expected progress during the following quarter.
Section 4.07
Partly complied with. Quarterly reports were not regularly sent to ADB. The project implementation unit office itself do not have copies filed and ready for visiting missions to use. Filing is in disarray.
Promptly after physical completion of the Project, but in any event not later than 3 months thereafter, or such later date as may be agreed for this purpose between the Borrower and ADB, the Borrower shall furnish to ADB a report, in such form and in such detail as ADB shall reasonably request, on the execution and initial operation of the Project, including cost, performance by the Borrower, obligations under this Loan Agreement, and
Section 4.07
A very incomplete draft PCR was provided to ADB’s PCR Mission. The PCR format was provided to the project implementation unit and the Executing Agency in 2003, and this is already the third time the Executing Agency encountered ADB requirements for PCR preparation. However,
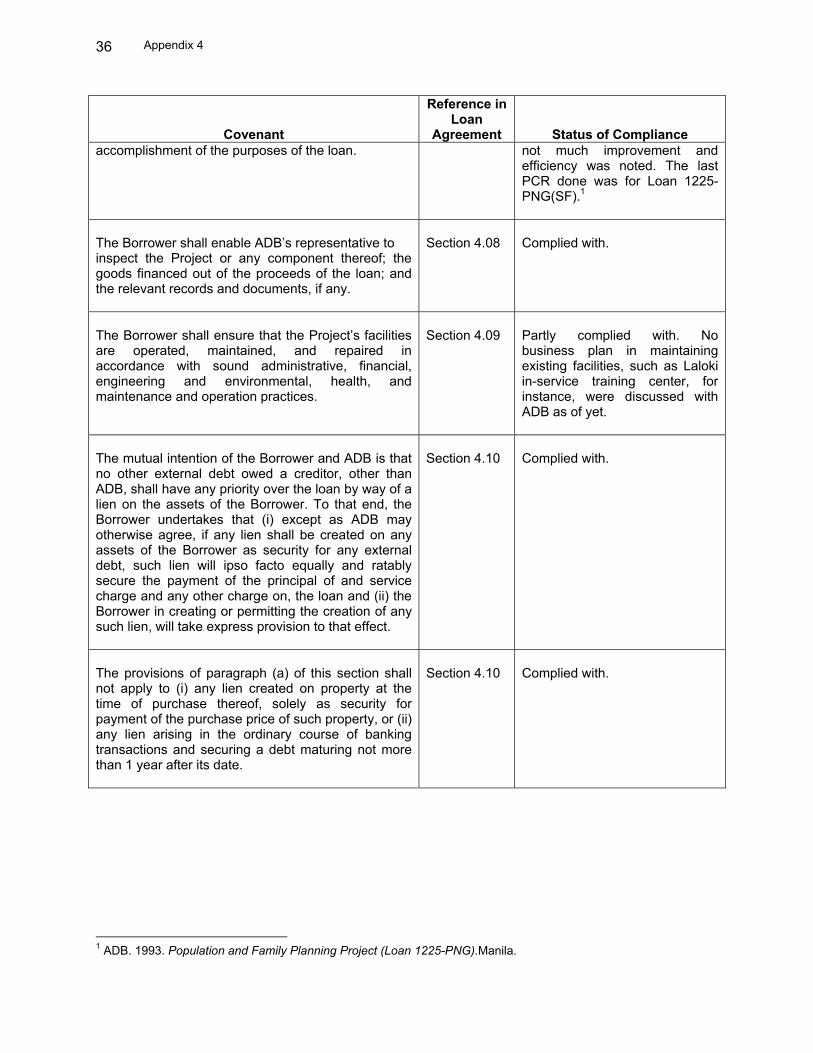
Appendix 4 36
Covenant
Reference in Loan
Agreement
Status of Compliance accomplishment of the purposes of the loan.
not much improvement and efficiency was noted. The last PCR done was for Loan 1225-PNG(SF).1
The Borrower shall enable ADB’s representative to inspect the Project or any component thereof; the goods financed out of the proceeds of the loan; and the relevant records and documents, if any.
Section 4.08
Complied with.
The Borrower shall ensure that the Project’s facilities are operated, maintained, and repaired in accordance with sound administrative, financial, engineering and environmental, health, and maintenance and operation practices.
Section 4.09
Partly complied with. No business plan in maintaining existing facilities, such as Laloki in-service training center, for instance, were discussed with ADB as of yet.
The mutual intention of the Borrower and ADB is that no other external debt owed a creditor, other than ADB, shall have any priority over the loan by way of a lien on the assets of the Borrower. To that end, the Borrower undertakes that (i) except as ADB may otherwise agree, if any lien shall be created on any assets of the Borrower as security for any external debt, such lien will ipso facto equally and ratably secure the payment of the principal of and service charge and any other charge on, the loan and (ii) the Borrower in creating or permitting the creation of any such lien, will take express provision to that effect.
Section 4.10
Complied with.
The provisions of paragraph (a) of this section shall not apply to (i) any lien created on property at the time of purchase thereof, solely as security for payment of the purchase price of such property, or (ii) any lien arising in the ordinary course of banking transactions and securing a debt maturing not more than 1 year after its date.
Section 4.10
Complied with.
1 ADB. 1993. Population and Family Planning Project (Loan 1225-PNG).Manila.