ask the expert: practical advises for the use of regional ... · • upper extremity blocks – no...
TRANSCRIPT

Division of Anesthesiology, Balgrist University Hospital, Zurich
Forchstrasse 340, CH-8008 Zürich
www.balgrist.ch
Ask the Expert: Practical Advises for the Use of Regional Anesthesia
José A. Aguirre, MD, MSc
2nd SARA Annual Meeting
29th June 2013

Agenda
• General complications of regional anesthesia
• Regional anesthesia in patients at risk for compartment syndrome
• Adjuvants in peripheral regional anesthesia
• Regional anesthesia in patients with preexisting neurological diseases

• Neurological complications of pain catheters
• central catheters: 0.01% / 2 - 4.2: 100‘000Cook TM et al. BJA 2009; 102:179-90 (707‘445 central blocks)Pöpping DM et al. BJM 2008; 101:832-840 (14‘223 patients)
• peripheral catheters: 0.4 – 2%Barrington MJ et al. RAPM 200); 34:534-541 (7‘000 patients)Capdevila X et al. Anesthesiology 2005; 103:135-45 (1‘416 patients)Auroy Y et al. Anesthesiology 2002; 97:1274-80 (43‘946 patients)
• Peroneal palsy as complication of TKA: 0.3 -10%• Neurologic complications after THA: 0.08 – 7.6%
Indusuyi OB et al. JBJS Am 1996; 78:177-84Asp JP et al. Clin Orthop 1990; 261:233-7
Regional anesthesia and
complications


• Problems of ambulatory surgery
– Unplanned hospital visits due to pain and
PONV
– Readmission rate after general anesthesia:
7-27%
– Readmission rate after regional anesthesia:
4-13%
Williams BA et al. Anesthesiology 2004; 100:697-706Hadzic A et al. Anesth Analg 2005; 100:976-81
Peripheral catheters: the advantages
PONV: post anesthesia nausea and vomiting

• 18y, m, ASA 1
• Elective shoulder arthroscopy with rotator cuff repair right shoulder
• Beach chair position
• Patient wishes no pain after surgery and to sleep during the procedure
CASE
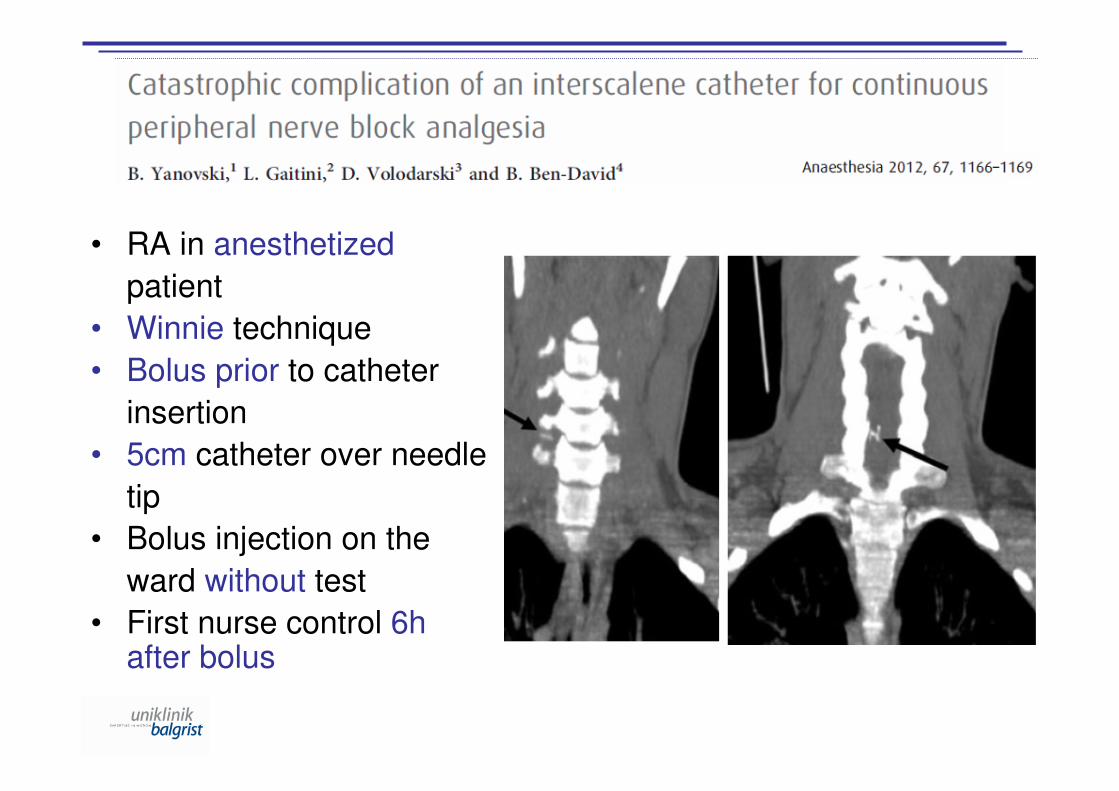
• RA in anesthetized
patient
• Winnie technique
• Bolus prior to catheter
insertion
• 5cm catheter over needle
tip
• Bolus injection on the
ward without test
• First nurse control 6h after bolus

Regional anesthesia in patients at risk of
compartment syndrome - the evidence

• 18y, m, ASA 1
• Trimalleolar fracture right ankle
• Uneventful general anesthesia and spinal anesthesia in the past for hernia repair and knee arthroscopy
• Patient wishes no pain after surgery
CASE

Compartment syndrome: Definition

Compartment syndrome: Definition
Ischemia – Reperfusion – Edema
� compartment p > capillary pressure
� arterial inflow & venous outflow
� further compartment pressure
� metabolic tissue demand > supply
� rhabdomyolysis and necrosis

Acute compartment syndrome
• 200‘000 diagnoses / year in the USA
• Majority from traumatic fractures– 40% tibial shaft fractures
– 23% soft tibial trauma
– 18% forearm fractures
• Incidence of ACS:– 4.3% after tibial shaft, 3.1% after diaphesal forearm,
0.25% after distal radial fractures
Whitesiders TE et al. J Am Acad Orthop Surg 1996; 4:209Konstantakos EK et al. Am Surg 2007; 73:1199-1209Olson SA et al. J Am Acad Orthop Surg 2005; 13:436-444Elliot KG et al. J Bone Joint Surg Br 2003; 85:625-32McQueen MM et al. J Bone Join Surg Br 2000; 82:200-203ACS: acute compartment syndrome

• Most common used
objective method in
clinical practice:
“Golden Standard”
• Difficult to use in
practice beyond 24h
Shadgan B et al. J Orthop Trauma 2008; 22:581-87Harris IA et al. J Trauma 2006; 60:1330-35
Compartment pressure

Janzing H et al. Eur J Trauma Emerg Surg 2007; 33:576-83

• Normal leg values
– Caucasians 0-15mmHg
– Nigerians 3-18mmHg (anterior comp.) /
3-14mmHg (deep comp.)
• Fasciotomy if
– Absolute pressure ≥ 30mmHg (- 45mmHg)
– DBP-CP = 10 - 20mmHg (≤ 30mmHg)
– Δ-P: MAP – CP ≤ 40mmHg
Compartment pressure
Ogunlusi JD et al. 2005; 25:200-02Mubarak SJ et al. Philadelphia: WB Saunders; 1981:113Whitesides TE et al. Clin Orthop 1975; 113:43-51Heppenstall RB et al, Clin Orthop 1988; 226:138Heppenstall B et al. Fractures in adults, 5th Ed. Lippincott W&W, 2001:332McQueen MM et al, J Bone Joint Surg Br 1996; 78:99
CP: compartment pressureDBP: diastolic blood pressureMAP: mean arterial blood pressure

Clinical symptoms
- pain (on muscle stretching)
- paresthesia, hypoesthesia
- paralysis
- pulselessness
- pallor
- reduced tenderness on palpationElliott KG et al. J Bone Joint Surg Br 2003; 85:625-32Kosir R et al. J Trauma 2007; 63:268-75Ulmer T et al. J Orthop Trauma 2002; 16:572-77
Compartment syndrome:
Assessment
Compartment syndrome and pain
Pain:
- an unreliable symptom: subjective / variable
- obviously, it does not avoid compartment
syndrome
- increasing analgesia demand precedes
neurovascular changes by 7.3h
- confounding factors: extremes of age, pain
thresholds, head injury/drugs, language barriers
- Pain not always present in ACS!Bae DS et al. J Pediatr Orthop 2001; 21:680-88
Benevides ML et al. Rev Bras Anestesiol 2006; 56:408-12Hailer NP et al. Acta Orthop 2007; 78:293-95Somayaji HS et al. J Arthroplasty 2005; 20:1081-83Nicholl JE et al. J Bone Joint Surg Br 1996; 78:812-13Badhe S et al. Injury 2009; 40:220-22

• 4 cases of compartment syndrome without any significant pain:– CS in the well leg after surgery for femoral
shaft fracture on the other side
– CS post-operatively following a tibial nailing for tibial fracture
– CS following tibial plateau fracture
– CS after closed, extraarticular multifragmentary fracture of the right prox. Tibia and fibula
CS: compartment syndrome

Compartment syndrome and pain
• Clinical signs:
• sensitivity 13-19%
• specifity 97-98%
• positive predictive value 11-15%
• negative predictive value 97-98%
Benevides ML et al. Rev Bras Anestesiol 2006; 56:408-12Hailer NP et al. Acta Orthop 2007; 78:293-95Somayaji HS et al. J Arthroplasty 2005; 20:1081-83Nicholl JE et al. J Bone Joint Surg Br 1996; 78:812-13Ulmer T. J Orthop Trauma 2002; 8:572-77Bae DS et al. J Pediatr Orthop 2001; 21:680-88
- Probability of compartment syndrome
with 1 clinical sign 25%
- Probability of compartment syndrome
with 3 clinical signs 93%

Clinical symptoms
- pain (on muscle stretching)
- paresthesia, hypoesthesia
- paralysis
- pulselessness (late sign!)
- pallor
- reduced tenderness on palpation
RA
Compartment syndrome and
regional anesthesia?
RA: regional anesthesia

General anesthesia and
compartment syndrome
• As pressure in the compartmentapproaches 10mmHg of diastolic BP, blood flow will cease
• Probably this may occur within 20mmHg of diastolic BP in injured muscle tissue
�Potential concerns wiht hypotensive
anesthesia techniques
Whitesiders TE et al. J Am Acad Orthop Surg 1996; 4:209Elliot KG et al. J Bone Joint Surg Br 2003; 85:625-32Shadgan B et al. J Orthop Trauma 2008; 22:581-87
Several cases of orthognathic surgery using hypotensive
anesthesia techniques with compartment syndrome of the lower
extremity have been described:
• Bilateral anterior ACS after short fascial plastic surgery under general anesthesia
� bilateral peroneal nerve palsiesGodeiro-Junior CO et al. Arq Neuropsiquiatr 2007; 65:826
•Two cases of othognatic surgery in general anesthesia with unilateral ACS of the
lower extremities � ankle-foot orthosisStrickland SM et al. J Oral Maxillofac Surg 2000; 58:814
• One case of ACS of the lower extremity after Le Fort osteotomy in general
anesthesia � ankle-foot orthosisBeadnell SW et al. J Oral Maxillofac Surg 1988; 46:232
ACS: acute compartment syndrome

• No randomized-controlled trial comparingoutcomes in patients at risk of ACS withregional anesthesia vs general anesthesia.
• Therefore, clincial practice is only based on casereports and retrospective case series.
• � no national or international guidelines for best practice
• Practice: regional anesthesia leads to decreasein postoperative pain and to sensory blockademasking ACS…
Compartment syndrome and
regional anesthesia
Mar GJ et al. Br J Anaesth 2009; 102:3-11ACS: acute compartment syndrome

• Central nerve blocks– have never been inplicated in delaying
diagnosis of abdominal compartmentsyndrome. Increase in perfusion pressure and decrease in intraabdominal pressure
– EDA has been implicated in ACS of lower limbs
– no report of single shot SPA or EDA implicatedin ACS
– intraoperative Δ-P only reduced in GA (DBP↓) but not during unilateral SPA
Compartment syndrome and
regional anesthesia
Hakobyan RV et al. Acta Glin Belg 2008; 63:86-92
Mar GJ et al. Br J Anaesth 2009; 102:3-11
Kakar S et al. Scott Med J 2005; 50:158-59
Gonanao C et al. Anesth Analg 2006; 102:524-29
EDA: epidural anesthesiaSPA: spinal anesthesiaACS: acute compartment syndromeGA: general anesthesia
• Upper extremity blocks
– No published case of ACS after upper limb
regional anesthesia
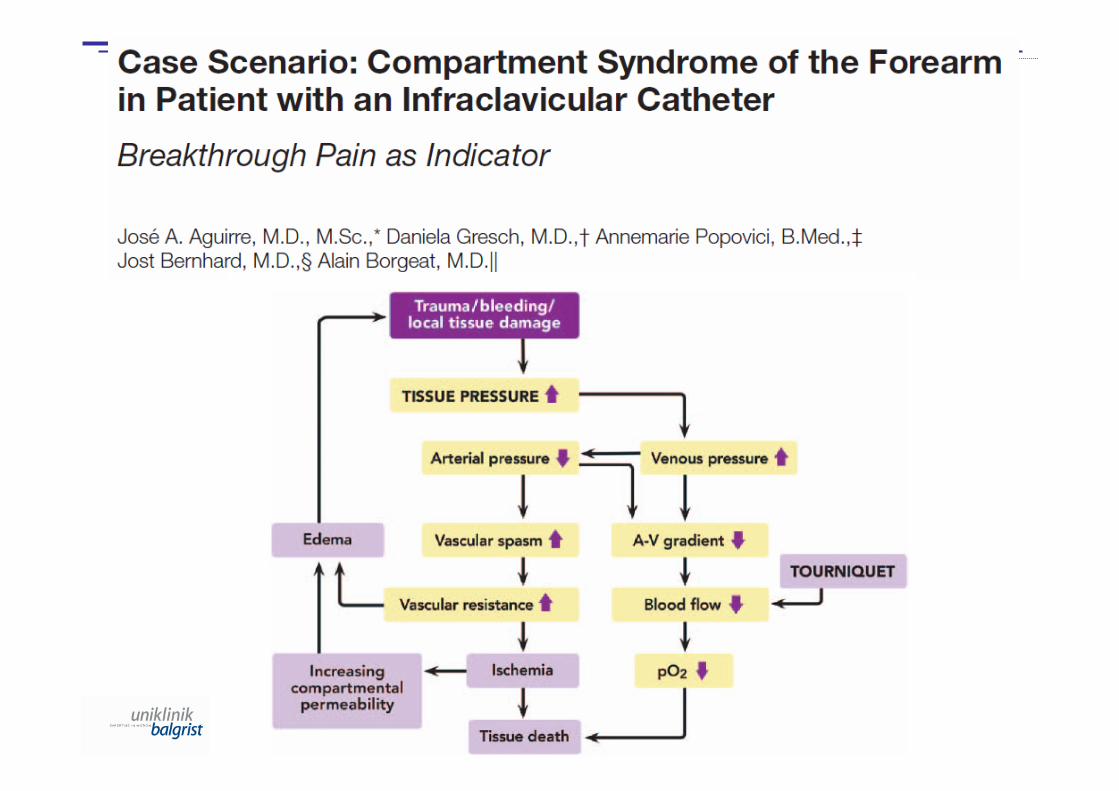
– One published case of ACS diagnose thanks to
upper limb regional anesthesia: breakthrough
pain as main indicator
Compartment syndrome and
regional anesthesia
ACS: acute compartment syndromeMar GJ et al. BJA 2009; 102:3-11Aguirre J et al. Anesthesiology 2013; 118:1198-205

• Lower extremity blocks
– One case of an ACS duirng continuous ambulant
popliteal sciatic nerve block
• Increasing pain over 2 days
• Pain relieved after splitting the patient‘s cast
• Catheter remained in place until POD4
• Four weeks after cast removal, evidence of prior full-thickess skin ulceration on the anterior aspect of the
ankle
– ACS or tight cast injury?
Compartment syndrome and
regional anesthesia
Walker BJ RAPM 2012; 37:393-7ACS: acute compartment syndrome

• Lower extremity blocks
– Three published cases of ACS after single shot
lower limb regional anesthesia
• femoral nerve block delayed ACS diagnosis after
intramedullar tibia nailing despite pain being a significant symptom
• femoral nerve block delayed ACS diagnosis afterintramedullar femoral nailing
• ankle block delayed ACS diagnosis after forefoot
arthroplasty despite pain being a significant symptom
Compartment syndrome and
regional anesthesia
Mar GJ et al. Br J Anaesth 2009; 102:3-11
Uzel AP et al. Ortho & Trauma: Surg and Res 2009; 95:309-13 ACS: acute compartment syndrome

• Lower extremity blocks
– One published case of ACS after continuous
femoral and sciatic nerve block:
• Distal femur and proximal tibia osteotomy with
external fixation of the right leg.
• General anesthesia
• Continuous femoral nerve block and continuoussciatic nerve block with 0.2% ropivacaine, 10ml/h
Compartment syndrome and
regional anesthesia
Cometa MA et al. Pain Medicine 2011; 12:823-28

Adjuvants for peripheral regional
anesthesia

• 48y, m, ASA 2
• Hallux valgus repair right foot
• Controlled arterial hypertension, increasedalcohol intake, moderate peripheralneuropathy
• No prior anesthesia
• Patient wishes no pain after surgery
CASE

Buerkle H. Best Pract Res Anaesth 2000; 14:411-18Niemi G. Best Pract Res Anaesth 2005: 19:229-45Buvanendran A et al. Best Pract Res Anaesth 2007; 21:31-49Christiansson L. Period Biol 2009; 11:161-170
Why adjuvants for LA?
• Shorten the onset time of LA action
– Only for central blocks?
• Limit the absorption of LA
– Decrease of spinal cord blood flow?
– Risk of peripheral neuropathy?
– Nausea and vomiting ?
• Improvement of block intensity/duration
– Clinical evidence?
LA: local anesthetic

Nerve
Artery
VeinNeedle
LA
97- 98%
2-3%
Systemic resorption depends on local blood flow!
Heavner JE. Curr Opin Anaesthesiol 2007; 20:336-42. ReviewCox B et al. Best Pract Res Clin Anaesthesiol 2003; 17:111-36
- 30%
Limit the absorption of local anesthetic

Improvement of block intensity:
clonidine
Analgesic benefit from the addition of clonidine to
local anesthetics? YES
Mechanisms of action?
- Centrally mediated analgesia?
- α2-mediated vasoconstriction in the periphery?
- Clear: not α2-mediated block prolongation but
inhibition of hyperpolarization-action current.
Effect more profound in C-fibers.
Buerkle H. Best Pract Res Anaesth 2000; 14:411-18Brummett CM et al. Int Anesthesiol Clin. 2011; 49: 104–16Pöpping DM et al. Anesthesiology 2009; 111:406-15McCartney CJ et al. RAPM 2007; 32:330-338Leem JW et al. RAPM 2000; 25:620-25

Side effects :
• Hypotension
• Bradycardia
• Sedation
Less side effects compared to epidural/spinal administration.
Related to the dose and to plasma levels.
Optimal dose: 150μμμμg (adults).
Improvement of block intensity:
clonidine
Buerkle H. Best Pract Res Anaesth 2000; 14:411-18Brummett CM et al. Int Anesthesiol Clin. 2011; 49: 104–16

Recommendations for the use of
adjuvants
Epinephrine: no use (as test dose??)
Clonidine: up to 150μg for adults
Dexmedetomidine: wait for better data
Buprenorphine / Tramadol: little efficacy
Dexamethasone: CAVE: dose-response-related neurotoxicity
Midazolam: CAVE: dose-response-related neurotoxicity
Brummett CM et al. Int Anesthesiol Clin. 2011; 49: 104–16
• Use the least toxic drug
– Spinal anesthesia: bupivacaine, chloroprocaine,
prilocaine.
– Peripheral: ropivacaine / bupivacaine (?), mepivacaine,
lidocaine.
• Avoid unnecessary risk with adjuvants
– NO epinephrine & lidocaine for central nerve blocks.
– NO tramadol / bicarbonate for peripheral nerve blocks.
– NO midazolam for peripheral neve blocks.
– NO adjuvants to ropivacaine. Clonidine??
Lirk P et al. RAPM 2012; 37:601-606Cuvillon P et al. BJA 2013; ahead of print
Recommendations for the use of
adjuvants

• Use perineural catheters for:
– extremely painful surgery (rotator cuff repair, total kneearthroplasty): ≥ 48h
– painful joint mobilisation (capsulotomy, synovectomy): ≥5d
– chronic pain patients and expected moderate to severepostoperative pain: ≥ 48h
– repetitive surgery (diabetic foot, wound controls): ≥ 5d
• Use perineural catheters only if:
– you and your team can manage them!!!
When to use continuous regional
anesthesia
Aguirre J et al. Anesthesiol Res Pract 2012 (online)Borgeat A, Aguirre J. Unintended Destinations of Local Anesthetics; 2012 Lippincott W&W, Philadelphia:196-204
Regional Anesthesia in the Patient
with Neurological Disease
• 28y, m, ASA 2
• Hallux valgus repair right foot
• Controlled arterial hypertension, Type 1 diabetes mellitus with implanted insulinpump, weak peripheral neuropathy
• No prior anesthesia
• Patient wishes no pain after surgery and issceptical against spinal anesthesia
CASE

The unanswered questions
• Do regional blocks worsen preexisting
neurological pathologies?
• Are LA more neurotoxic in this context?
• Does the failure rate increase?
LA: Local anestheticsBlumenthal S et al. Anesthesiology 2006; 105:1053-6Naveen E et al. Anesthesiology 2007; 107:177-178

Hebl JR et al. A&A 2006; 103:1294–1299
Double crush phenomenon
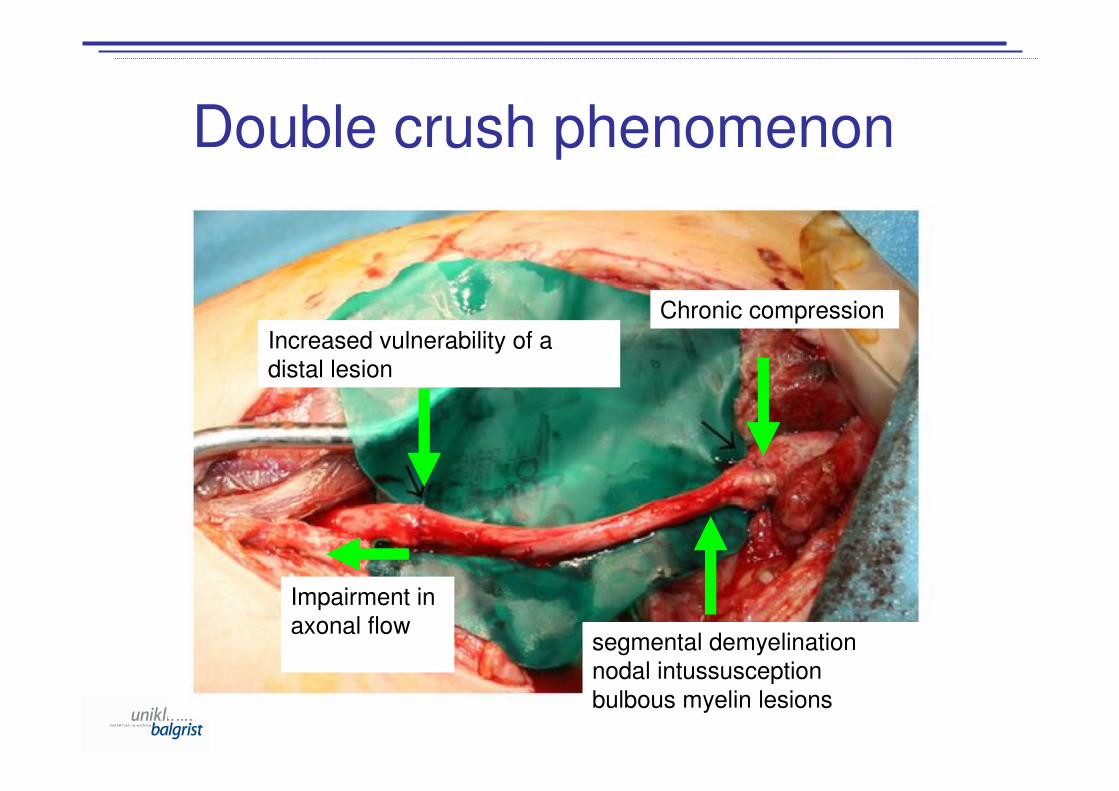
Double crush phenomenon
Chronic compression
segmental demyelination
nodal intussusception
bulbous myelin lesions
Increased vulnerability of a
distal lesion
Impairment in
axonal flow

Double crush phenomenon
Local anesthetics
Adjuvants

Double crush phenomenon


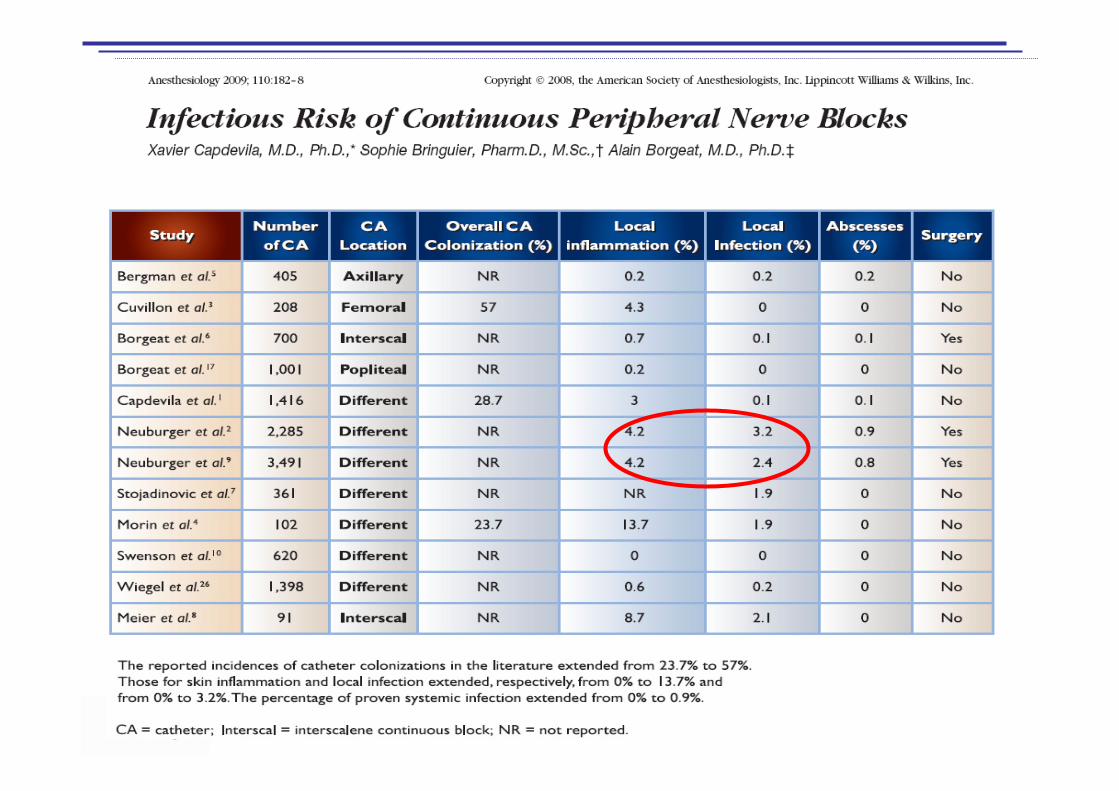
• Infectious risk of pain catheters
- local infection: 0 – 3.2%- proven systemic infection: 0 – 0.9%
Capdevila X et al. Anesthesiology 2009; 110:182-88 (12‘078 patients)
• SSI infections complicate 5% - 10% of all
surgeries increasing hospital length of stay by
48% - 310% and increase costs by 34% - 226%.
• Prevention of vasoconstriction at operation site
and increasing surgical-site tissue oxygen tension
with RA may reduce the occurrence of SSIs.
Impact on postoperative complications
Broex EC et al. J Hosp Infect 2009; 72:193-201Sessler DI et al. Anesthesiology 2010; 113:265-67Chang CC et al. Anesthesiology 2010; 113:279-84Kabon B et al. A&A 2003; 97:1812-17Buggy DJ et al. Anesthesiology 2002; 97:952-58
SSI: surgical site infectionRA: regional anesthesiaRCT: randomized controlled trial
• Neurological complications of pain catheters
• central catheters: 0.01% / 2 - 4.2: 100‘000Cook TM et al. BJA 2009; 102:179-90 (707‘445 central blocks)Pöpping DM et al. BJM 2008; 101:832-840 (14‘223 patients)
• peripheral catheters: 0.4 – 2%Barrington MJ et al. RAPM 200); 34:534-541 (7‘000 patients)Capdevila X et al. Anesthesiology 2005; 103:135-45 (1‘416 patients)Auroy Y et al. Anesthesiology 2002; 97:1274-80 (43‘946 patients)
• Peroneal palsy as complication of TKA: 0.3 -10%• Neurologic complications after THA: 0.08 – 7.6%
Indusuyi OB et al. JBJS Am 1996; 78:177-84Asp JP et al. Clin Orthop 1990; 261:233-7
Regional anesthesia and
complications
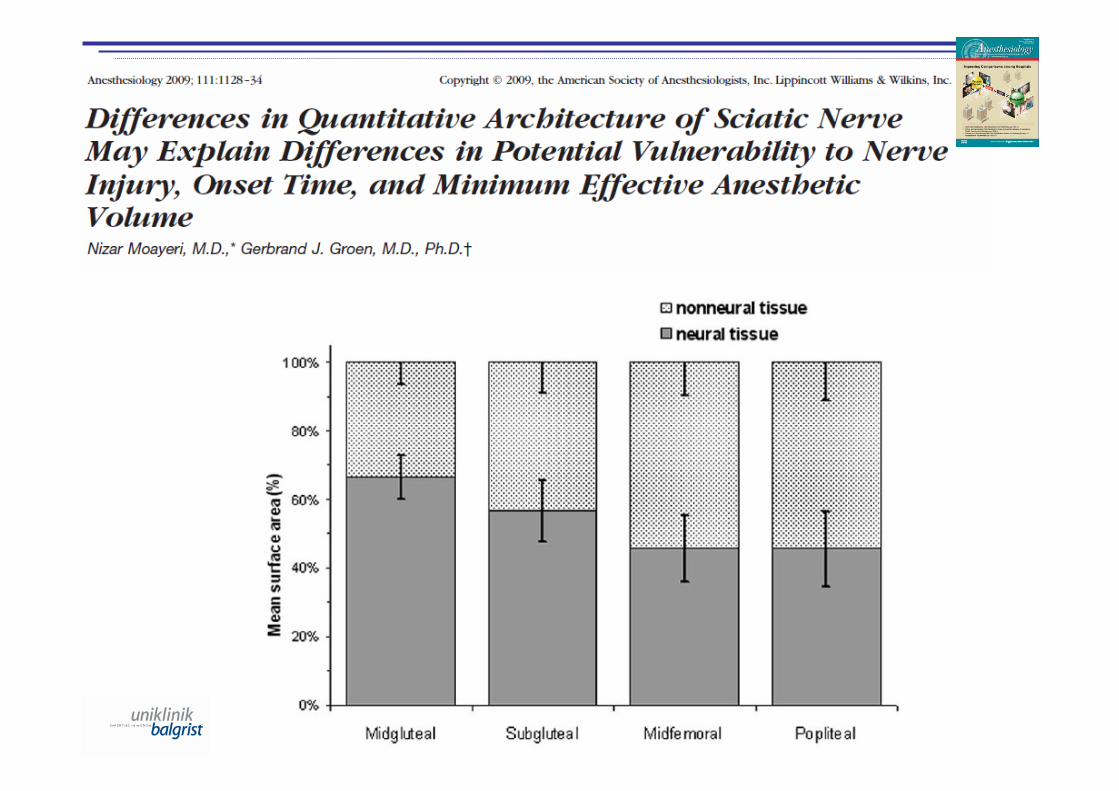
• Peripheral nerve injuries due to regional
anesthesia are often transient:
�mild paresthesias present in about 15% of
patients after peripheral nerve blocks
�most symptoms resolve within days to weeks
�99% complete resolving within 1 year
• Most neuraxial injuries are often permanent:
�15% - 80 - 100% permanent injuries
�frequency highly dependent on the type of
neural lesion Liguori GA. J Neurosurg Anesthesiol 2004; 16:84-86Borgeat A et al. A&A 2001; 95:875-80Neal JM et al. RAPM 2002; 27:402-28Auroy Y et al. Anesthesiology 2002; 97:1274-80Auroy Y et al. Anesthesiology 1997; 87:479-86Lee LA et al Anesthesiology 2004; 101:143-52
Regional anesthesia and
complications
Classification of neuromuscular
diseases
• Neuromuscular diseases (NMD)
– pre-junctional diseases (motoneurons and
peripheral nerves)
• ALS, MS, Guillan-Barré-Syndrome
– junctional diseases (synaptic transmission)
• myasthenia gravis
– post-junctional diseases (muscular)
• muscle dystrophies
• myotonies
ALS: amyothrophic lateral sclerosisMS: multiple sclerosis Papenfuss T et al. Anästh Inten Notfall Schmerz 2009: 44:766-771
Anesthetic risk factors of
neuromuscular diseases
• Cardiopulmonary comorbidities.
• Dysphagia � danger of aspirationpneumonia.
• Possible pulmonary dysfunction.
• Muscle relaxants: unpredictable durationof action.
• Volatile anesthetics: negative inotropeeffect.
Papenfuss T et al. Anästh Inten Notfall Schmerz 2009; 44:766-771Finsterer J et al. Cardiology 2000; 94:1–11Klingler W et al. Neuromuscul Disord 2005; 15:195–206Meißner S et al. Anästh Intensivmed 2009; 50:223–241
Regional anesthesia and
neuromuscular diseases
• Advantages
– avoidance of negative inotrope drugs and muscle
relaxants
– maintenance of spontaneous breathing
– hemodynamic stability
• Concerns
– double crush theory
– case reports of adverse neurological outcome
– no controlled, randomized studies
– non-binding guidelines
Upton AR et al. Lancet 1973; 2:359–362Radwan IA et al. Anesth Analg 2002; 94:319–324

• Pro RA
– Junctional and post-junctional diseases: no
damage of neurons: no absolute
contraindication for RA
– Pre-junctional diseases: Hebl et al. found a
low risk for central regional anesthesia
techniques. No absolute contraindication for
RA. Individual decision for patients with ALS,
MS, GBS etc.
Hebl JR et al. A&A 2006; 103:1294–1299Hebl JR et al. A&A 2006; 103:223–228Meissner S et al. Anästh Intensivmed 2009; 50:223–241
RA: regional anesthesiaALS: amyothrophic lateral sclerosisMS: multiple sclerosisGBS: Guillan-Barré-Syndrome
Regional anesthesia and
neuromuscular diseases
Demyelinating CNS disease:
Multiple sclerosis
• Most common demyelinating disease of the CNS. Motoneurons affected.
• Random, multiple sites of demyelination in the brain and spinal cord. Rareinvolvement of the peripheral nerve system, but described. Subtle nerve lesions wihtout real demyelination.
• Subclinical peripheral neuropathy (?)
CNS: central nervous system
Boerio D et al. Clin Neurophysiol 2007; 118:1735-8Pollocl M et al. Ann Neurol 1977; 2:41-48Vogt J et al. Ann Neurol 2009; 66:310-22Gartzen K et al. Eur J Neurol 2011; 5:789-91

Multiple sclerosis & general
anesthesia
• Autonomic dysfunction is frequent.
• Stress response may be associated
with relapse
– no difference in postoperative aggravationcompared to regional anesthesia (spinal)
• General anesthesia recommended if
– unclear disease progression
– no possible cooperation with a neurologistDrake E et al. Int J Obstet Anesth 2006; 15:115–123Bouchard P et al. Anesth Reanim 1984; 3:194–198Roissant R et al. Hrsg. Die Anästhesiologie. Heidelberg: Springer; 2004:1390–1391

• No real worsening after peripheral nerve block
– anesthetic plan influenced by case reports and personal experience
• Controversy concerning spinal and epidural
block
– effect of LA on demyelinated nerves
– systemic application of LA leads to discovery of non
diagnosed demyelinated areas
– typical symptons are aggravated temporarily
temporarily
Multiple sclerosis & regional
anesthesia
Borgeat A, Aguirre J et al. Anesthesiology 2008; 109:750-1Drake E et al. Int J Obstet Anesth 2006; 15:115–123Perlas A et al. Can J Anaesth 2005; 52:454–458Berger JM et al. Anesthesiology 1987; 66:400–402LA: local anesthetic
• Central regional anesthesia– Epidural anesthesia might be considered. Use
lowest LA dose possible. Avoid lidocaine. Ifadjuvants use clonidine / buprenorphine
– Consider spinal anesthesia only in cases of real advantage (C-section)
• Peripheral regional anesthesia– May be considered whenever possible, inform
patients about relapse possibility
Multiple sclerosis & regional
anesthesia
Confavreux C et al. N Engl J Med 1998; 339:285-291Vukusic S et al. Rev Neurol 2006; 162:299-309Dalmas AF et al. Ann Fr Anesth Reanim 2003; 22:861-64Bader AM et al. J Clin Anesth 1988; 1:21.24LA: local anesthetic

Peripheral neuropathy
• Multiple mononeuropathy: polyarteritis nodosa, SLE, sclerodermya, sarcoidosis, HIV, diabetes.
• Microorganisms (mononeuropathy): diphteria, Guillain-Barré.
• Toxic agents (polyneuropathy): sulfonamides, phenytoin, heavy metals, chemotherapy….
• Nutritional deficiency and metabolic disorders(polyneuropathy): alcoholism, perniciousanemia, diabetes…).
• Malignancy (polyneuropathy): multiple myeloma.

Diabetes: Concerns
• Oedema of the nerves may be directlyrelated to hyperglycemia.
• Microangiopathy may further lead to ischemia of the oedematous nerve and decrease blood flow and drug uptake.
• Prolonged exposure to local anesthetics.
Gebhard R et al. RAPM 2009; 34:404-07Kroin JS et al. RAPM 2010; 35:343-50
Preoperative evaluation:
• Interdisciplinary approach for cardiopulmonaldiseases– electrocardiography, X-Ray of the chest, lung
function if needed
• RA in the case of severe co-morbidities isthe first choice– epidural anesthesia for caesarean section in
patients with GBS
Baur CP et al. Anasth Intensivmed 2002; 37:77–83Meissner S et al. Anästh Intensivmed 2009; 50:223–241Alici HA et al. Int J Obstet Anesth 2005; 14: 269–270Brooks H et al. Anaesthesia 2000; 55:894–898
PNB: peripheral nerve blockRA: regional anesthesiaGBS: Guillan-Barré-Syndrome
Strategies to minimize risk in PNB
Preoperative examination:
• Exact neurological examination
– deficits must be documented
• Patients should be informed about
– technical difficulties
– possible relapses and/or progression
associated with stress, surgery and
anesthesia
Strategies to minimize risk in PNB
• Technique of RA
– No superiority of US over NS described
– Adapt stimulation setting (>0.3mA, 0.3ms, 2Hz)
• Choice / concentration of LA– All LA are neurotoxic. Neurotoxicity
comparable at equipotent doses.
– Diabtic nerves more sensitive. Reduceconcentration, longer duration
Strategies to minimize risk in PNB
RA: regional anesthesiaUS / NS: ultrasound / nerve stimulationLA: local anesthetic

• Role of adjuvants
– Epinephrine reduces blood flow in peripheral nerves � reduced wash out and prolonged LA exposure
– Clonidine may prove to be usefuladjuvants to prolong sensory block
Strategies to minimize risk in PNB
LA: local anesthetic

• Goal: to inform practioners of regional anesthesia and pain medicine regardingthe etiology, differential diagnosis, prevention, and treatment of neurologiccomplications.
• Methods: extensive review of literature byspecialists on the field.
Hebl J et al. A&A 2010; 111:1511-19

• Ultrasound and neurostimulationequivalent.
• Reduction of dose, concentration, potencyof local anesthetic and reduction(elimination) of concentration of vasoconstrictive additive are potential considerations (based on animal studies).
Hebl J et al. A&A 2010; 111:1511-19
• Patients with pre-existing peripheralneurologic disease
– theoretic increase of the risk of new or
progressive postoperative neurologic
complications. No clinical data to confirm or
refute this theory
– individual risk/benefit assessment
Hebl J et al. A&A 2010; 111:1511-19
• Patients with pre-existing central neurologic
disease
– lacking clinical evidence for increase of risk of new or
progressive postoperative neurologic complications
– individual risk/benefit assessment
• Spinal stenosis or mass lesions in spinal canal
– individual risk/benefit assessment
– high local anesthetic volume neuraxial technique(EDA) might have a higher risk of progressive mass
effect compared with low volume technique (SPA)
Hebl J et al. A&A 2010; 111:1511-19
EDA: epidural anesthesiaSPA: Spinal anesthesia
• Overall approach to patients with pre-existing neurologic deficits:– these patients might be at increased risk of new or
worsening injury regardless of the anesthetic
technique
– if regional anesthesia is chosen, modifications of the
technique (dose, volume, concentration, drugs) mightminimize the risks
– limited human data neither confirm nor refute these
modifications
Hebl J et al. A&A 2010; 111:1511-19