aspiration complications following nasogastric ... peg-els aspiration during nasogastric ... peg-els...
TRANSCRIPT
INTRODUCTION
P olyethylene Glycol-Electrolyte Lavage Solution(PEG-ELS), “Golytely,” has been availablesince the early 1980s. Davis et al, developed it as
a safer alternative for traditional bowel cleansing
using balanced electrolyte solution. It provides rapidcleansing of the bowel with only minimal transmu-cosal movement of water or sodium (1). PolyethyleneGlycol (PEG) is a linear polymer made up of repeatingtwo-carbon length hydrocarbons joined by oxygen toform an ether linkage. This structure produces ahydrophobic and hydrophilic portion of the polymer.The hydrophilic oxygen molecules allow for bondingto surrounding water molecules. PEG 3350 is the mostcommon form used in gastric lavage solutions. It isone of the larger PEG molecules made up of 68–84units. Its large size keeps it from being absorbed by the
PRACTICAL GASTROENTEROLOGY • NOVEMBER 200226
Aspiration Complications FollowingNasogastric Administration of Polyethylene Glycol (PEG) Solution
A CASE TO REMEMBER
Peter Lutz, MD, PGY-2, and Ronald Mason, MD,Assistant Professors of Medicine, Discipline of Gas-troenterology, University of Alabama School of Medi-cine, Montgomery Internal Medicine Residency Pro-gram, Montgomery AL.
Peter Lutz Ronald Mason
Polyethylene Glycol-Electrolyte Lavage Solution (PEG-ELS), “Golytely,” has been avail-able since the early 1980s. It was developed as a safer alternative for traditional bowelcleansing solutions. We present a case of Acute Respiratory Distress Syndrome secondaryto PEG-ELS aspiration during nasogastric administration and contrast it to other suchre p o rted cases. There are several possible mechanisms through which PEG-ELS mayinduce ARDS, including its high osmotic effect, structural similarities to lung surfactant,as well as direct alveolar membrane damage. In patients requiring administration ofPEG-ELS via nasogastric tube, we suggest placing the patient in full aspiration pre c a u-tions, reducing the rate of infusion, or use of another bowel cleansing solution.
intestinal mucosa. It is used in gastric lavage solutionsbecause its lack of absorption and highly osmoticstructure helps to retain fluid in the gut (2). Since itsintroduction, PEG-ELS has become one of the mostcommon methods of preparations for colonoscopy,barium enemas, and colon surgery. It is generally welltolerated with the most common adverse effects beingdisagreeable taste, minimal nausea and abdominalbloating. Rare cases have been reported of hypother-mia, obstruction-perforation, lavage-induced pill, mal-absorption, electrolyte-metabolic abnormalities, andcardiac arrhythmias (3). Among the side eff e c t sreported, there have been only five cases of PEG-ELSaspiration during bowel preparation for a colonoscopyand its effects. We present another such case in whichthe aspiration is believed to have caused Acute Respi-ratory Distress Syndrome (ARDS).
CASE REPORTA 65-year-old woman with a past medical history ofdeep vein thrombosis on Coumadin treatment, COPD,and congestive heart failure presentedto the emergency department withbright rectal bleeding occurring 24hours prior to the presentation. Sheadmitted to intermittent use ofNSAIDs. She denied any hematemesis,melena, or abdominal pain. On admis-sion her vital signs were: pulse 93, res-pirations 20, blood pressure 121/48,and temperature of 97.1°F. Gastriclavage did not show any evidence ofblood. Initial laboratory data showed ahemoglobin of 6.3 and hematocrit of19.9 and a PT of 34.4 and INR of 7.59.Her abdomen was soft and nontenderwith hyperactive bowel sounds. Herstool was grossly bloody.
The patient received packed redblood cells to correct her anemia andfresh frozen plasma for her coagulopa-t h y. An EGD was performed and did notreveal a source of bleeding. The patientcontinued to have hematochezia withdecreasing hematocrit. A colonoscopy
was scheduled for the next day. Bowel prep was under-taken with PEG-ELS. A PEG-ELS composed of Poly-ethylene Glycol 31.3 mmol/L, sodium 65 mmol/L, chlo-ride 53 mmol/L, bicarbonate 17 mmol/L, and potassium5 mmol/L in 4 L of water was infused via nasogastrictube at the recommended rate of approximately 20-30cc/minute (4). Approximately 1 hour after beginning thebowel prep, the patient began to have respiratory diff i-culty and chest pain. She quickly progressed to acuterespiratory failure requiring intubation and mechanicalventilation. Post intubation greater then 500cc of clearfluid was suctioned from the patient’s lungs. This fluidwas felt to be the PEG-ELS that was being given at thetime of the event.
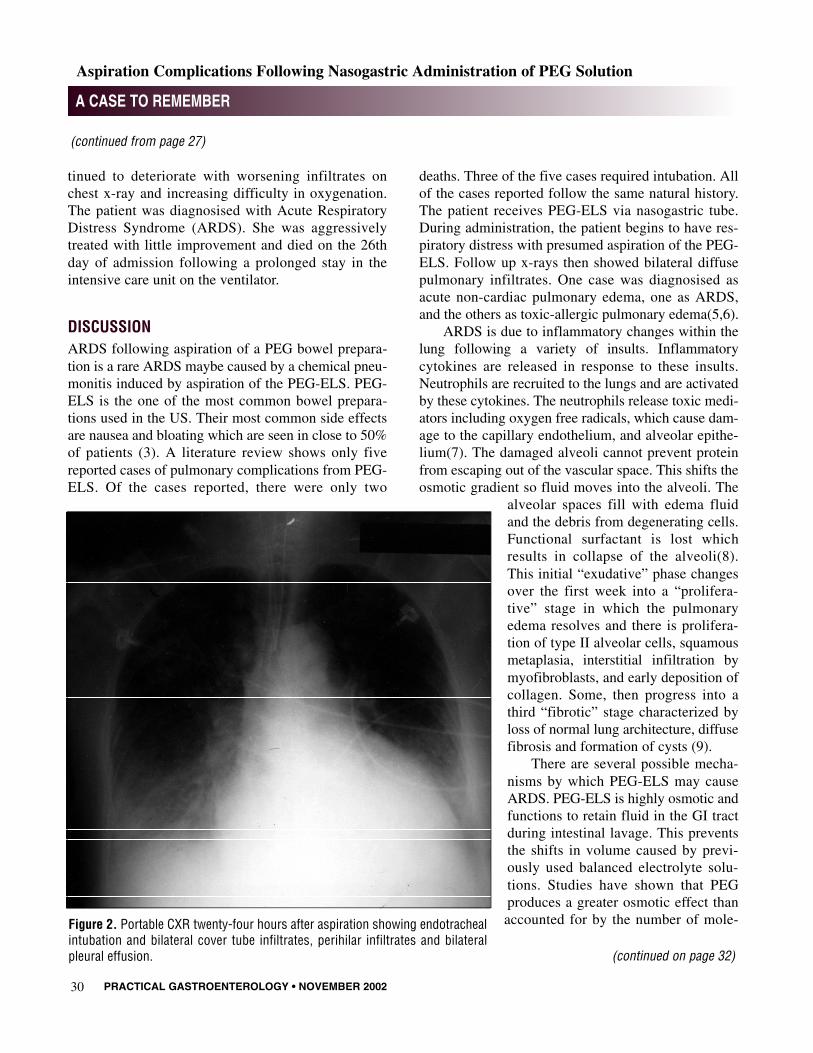
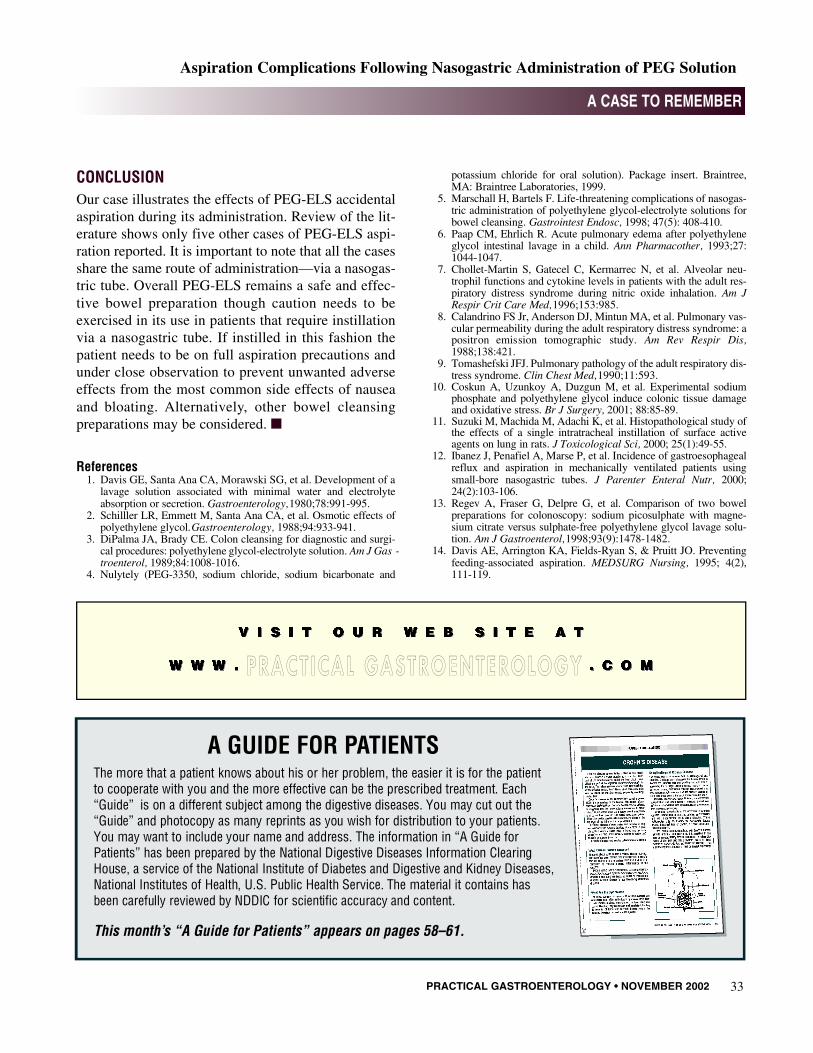
Chest x-rays preformed several hours prior to intu-bation compared with the morning post intubationshowed increasing diffuse bilateral pulmonary infil-trates (Figure 1 and Figure 2). Myocardial infarctionwas ruled out and diuresis failed to improve her respi-ratory failure. Over the next few days, the patient con-
PRACTICAL GASTROENTEROLOGY • NOVEMBER 2002 27
A CASE TO REMEMBER
Aspiration Complications Following Nasogastric Administration of PEG Solution
Figure 1. Portable CXR prior to aspiration showing mild cardiomegaly and asmall left pleural effusion.
(continued on page 30)
PRACTICAL GASTROENTEROLOGY • NOVEMBER 200230
A CASE TO REMEMBER
Aspiration Complications Following Nasogastric Administration of PEG Solution
tinued to deteriorate with worsening infiltrates onchest x-ray and increasing difficulty in oxygenation.The patient was diagnosised with Acute RespiratoryDistress Syndrome (ARDS). She was aggressivelytreated with little improvement and died on the 26thday of admission following a prolonged stay in theintensive care unit on the ventilator.
DISCUSSIONARDS following aspiration of a PEG bowel prepara-tion is a rare ARDS maybe caused by a chemical pneu-monitis induced by aspiration of the PEG-ELS. PEG-ELS is the one of the most common bowel prepara-tions used in the US. Their most common side effectsare nausea and bloating which are seen in close to 50%of patients (3). A literature review shows only fivereported cases of pulmonary complications from PEG-ELS. Of the cases reported, there were only two
deaths. Three of the five cases required intubation. Allof the cases reported follow the same natural history.The patient receives PEG-ELS via nasogastric tube.During administration, the patient begins to have res-piratory distress with presumed aspiration of the PEG-ELS. Follow up x-rays then showed bilateral diffusepulmonary infiltrates. One case was diagnosised asacute non-cardiac pulmonary edema, one as ARDS,and the others as toxic-allergic pulmonary edema(5,6).
ARDS is due to inflammatory changes within thelung following a variety of insults. Inflammatorycytokines are released in response to these insults.Neutrophils are recruited to the lungs and are activatedby these cytokines. The neutrophils release toxic medi-ators including oxygen free radicals, which cause dam-age to the capillary endothelium, and alveolar epithe-lium(7). The damaged alveoli cannot prevent proteinfrom escaping out of the vascular space. This shifts theosmotic gradient so fluid moves into the alveoli. The
alveolar spaces fill with edema fluidand the debris from degenerating cells.Functional surfactant is lost whichresults in collapse of the alveoli(8).This initial “exudative” phase changesover the first week into a “prolifera-tive” stage in which the pulmonaryedema resolves and there is prolifera-tion of type II alveolar cells, squamousmetaplasia, interstitial infiltration bymyofibroblasts, and early deposition ofcollagen. Some, then progress into athird “fibrotic” stage characterized byloss of normal lung architecture, diffusefibrosis and formation of cysts (9).
There are several possible mecha-nisms by which PEG-ELS may causeARDS. PEG-ELS is highly osmotic andfunctions to retain fluid in the GI tractduring intestinal lavage. This preventsthe shifts in volume caused by previ-ously used balanced electrolyte solu-tions. Studies have shown that PEGproduces a greater osmotic effect thanaccounted for by the number of mole-
(continued on page 32)
(continued from page 27)
Figure 2. Portable CXR twenty-four hours after aspiration showing endotrachealintubation and bilateral cover tube infiltrates, perihilar infiltrates and bilateralpleural effusion.

PRACTICAL GASTROENTEROLOGY • NOVEMBER 200232
A CASE TO REMEMBER
Aspiration Complications Following Nasogastric Administration of PEG Solution
cules in solution. PEG 3350 is a large molecule capa-ble of ordering a relatively large region of water. Thisgives it a very high osmotic effect(2). Once introducedin the lung, this high osmotic potential may act to shiftthe osmotic gradient so that a large amount of fluid ismoved out of the pulmonary vasculature and into thealveolar space causing pulmonary edema (6).
PEG-ELS may also interrupt the function of lungsurfactant. During aspiration, the filling of the alveoliwith fluid would interrupt the surfactant’s functionsimilar to edema fluid. PEG also shares similar chem-ical properties to artificial surfactants used in the pre-vention of neonatal respiratory distress syndrome.Many of the artificial surfactants are classified as poly-ethylene glycols. The PEG could interrupt the normalinteraction of natural surfactant and the alveolar mem-brane on a molecular level leading to more extensivecollapse of the alveoli than by fluid interruption alone.
The PEG may also damage the alveolar membranedirectly. Coskun et al, (10) has shown that PEG solu-tion can cause both histological and oxidative stress tothe mucosal membrane of rat colons. After instillationof a PEG solution, loss of superficial mucosa andepithelial denudation was noted histologically in themucosal cells. Testing also indicated oxidative stresson the cells as demonstrated by elevated levels of mal-onyldialdehyde. Malonyldialdehyde is a chemicalindicator of increased oxidant activity. It is likely thatsimilar damage and oxidative stress could be seen inalveolar tissue, perhaps more because there are lessprotective mechanisms in the lung compared to the GItract against direct contact with chemical agents.
In a study by Suzuki M et al, polyoxyethylene 9lauryl ether (Laureth-9) was instilled intratracheallydirectly in the lung. Laureth-9 is another member ofthe PEG family and is similar in general structure toPEG 3350 used in intestinal lavage solutions. The firstday after instillation, edema, hemorrhage, and inflam-matory cell infiltration due to epithelial degenerationand desquamation was noted on histological sections.In later days, hyperplasia of epithelium and sporadicfibrosis was noted as part of the wound healing processof the lung (11). These changes are similar to thoseseen in ARDS.
Based on the chemical properties discussed above,PEG-ELS aspirated directly into the lungs is the most
likely cause of the ARDS in our patient and similarARDS-like pictures are seen in the other reportedcases. The common feature in all the cases of pul-monary complications with PEG-ELS use has beenadministration via a nasogastric tube. PEG-ELS hasbeen shown to be a safe and effective form of bowelpreparation for procedures. The most common sideeffects are nausea and abdominal bloating (3). Mostpatients requiring administration via nasogastric tubesare likely have other comorbidities. The most commonbeing decreased mental status, impaired respiratory orcardiac status, and elevated age. These comorbiditieswould reduce the patient’s ability to tolerate or warnstaff when nausea or bloating occurs. The nasogastrictube also increases their risk of aspiration further byviolating the seal at the esophageal gastric junction(12). In these patients when bowel prep is necessary,consideration may be given to using sodium picosul-phate plus magnesium citrate. Regev A et al (13),showed that sodium picosulphate plus magnesium cit-rate is better tolerated with statistically lower inci-dence of nausea and vomiting than PEG-ELS. If PEG-ELS is used, we would then suggest infusing the solu-tion at half or less than the manufacturer’s suggestedrate and over a longer period of time. The packageinsert for the PEG-ELS use does suggest reducing therate of infusion if bloating or nausea occur (4). Wewould suggest a rate of ~10–15 cc per minute or less.The patient should also be placed on full aspirationprecautions including close monitoring of the patientby nursing, checking residual stomach contents afterone hour, and positioning the patient at 30–45 degreesof head elevation (14). Even the use of prokineticagents such as metaclopromide may be contemplated.
No clinical trials or research has been done toassess the proper treatment of PEG-ELS solution aspi-ration. Should aspiration occur, the most commontherapy noted among the surviving patients wasaggressive suction of the aspirate and/or broncho-alve-olar lavage. This may help by reducing the time thePEG-ELS remains in contact with lung tissue. Other-wise, only maximal supportive and symptomatic carecan be recommended. Consideration may be given toproviding antibiotic coverage for aspiration pneumo-nia should such signs or symptoms suggesting bacter-ial infection develop.
(continued from page 30)
CONCLUSION Our case illustrates the effects of PEG-ELS accidentalaspiration during its administration. Review of the lit-erature shows only five other cases of PEG-ELS aspi-ration reported. It is important to note that all the casesshare the same route of administration—via a nasogas-tric tube. Overall PEG-ELS remains a safe and effec-tive bowel preparation though caution needs to beexercised in its use in patients that require instillationvia a nasogastric tube. If instilled in this fashion thepatient needs to be on full aspiration precautions andunder close observation to prevent unwanted adverseeffects from the most common side effects of nauseaand bloating. Alternatively, other bowel cleansingpreparations may be considered. ■
References1. Davis GE, Santa Ana CA, Morawski SG, et al. Development of a
lavage solution associated with minimal water and electrolyteabsorption or secretion. Gastroenterology, 1 9 8 0 ; 7 8 : 9 9 1 - 9 9 5 .
2 . Schilller LR, Emmett M, Santa Ana CA, et al. Osmotic effects ofpolyethylene glycol. G a s t r o e n t e r o l o g y , 1 9 8 8 ; 9 4 : 9 3 3 - 9 4 1 .
3 . DiPalma JA, Brady CE. Colon cleansing for diagnostic and surgi-cal procedures: polyethylene glycol-electrolyte solution. Am J Gas -t r o e n t e r o l , 1 9 8 9 ; 8 4 : 1 0 0 8 - 1 0 1 6 .
4 . Nulytely (PEG-3350, sodium chloride, sodium bicarbonate and
potassium chloride for oral solution). Package insert. Braintree,MA: Braintree Laboratories, 1999.
5 . Marschall H, Bartels F. Life-threatening complications of nasogas-tric administration of polyethylene glycol-electrolyte solutions forbowel cleansing. Gastrointest Endosc, 1998; 47(5): 408-410.
6 . Paap CM, Ehrlich R. Acute pulmonary edema after polyethyleneglycol intestinal lavage in a child. Ann Pharmacother, 1 9 9 3 ; 2 7 :1 0 4 4 - 1 0 4 7 .
7 . Chollet-Martin S, Gatecel C, Kermarrec N, et al. Alveolar neu-trophil functions and cytokine levels in patients with the adult res-piratory distress syndrome during nitric oxide inhalation. Am JRespir Crit Care Med, 1 9 9 6 ; 1 5 3 : 9 8 5 .
8 . Calandrino FS Jr, Anderson DJ, Mintun MA, et al. Pulmonary vas-cular permeability during the adult respiratory distress syndrome: apositron emission tomographic study. Am Rev Respir Dis,1 9 8 8 ; 1 3 8 : 4 2 1 .
9 . Tomashefski JFJ. Pulmonary pathology of the adult respiratory dis-tress syndrome. Clin Chest Med, 1 9 9 0 ; 1 1 : 5 9 3 .
1 0 . Coskun A, Uzunkoy A, Duzgun M, et al. Experimental sodiumphosphate and polyethylene glycol induce colonic tissue damageand oxidative stress. Br J Surgery, 2001; 88:85-89.
1 1 . Suzuki M, Machida M, Adachi K, et al. Histopathological study ofthe effects of a single intratracheal instillation of surface activeagents on lung in rats. J Toxicological Sci, 2000; 25(1):49-55.
1 2 . Ibanez J, Penafiel A, Marse P, et al. Incidence of gastroesophagealreflux and aspiration in mechanically ventilated patients usingsmall-bore nasogastric tubes. J Parenter Enteral Nutr, 2 0 0 0 ;2 4 ( 2 ) : 1 0 3 - 1 0 6 .
1 3 . Regev A, Fraser G, Delpre G, et al. Comparison of two bowelpreparations for colonoscopy: sodium picosulphate with magne-sium citrate versus sulphate-free polyethylene glycol lavage solu-t i o n . Am J Gastroenterol, 1 9 9 8 ; 9 3 ( 9 ) : 1 4 7 8 - 1 4 8 2 .
1 4 . Davis AE, Arrington KA, Fields-Ryan S, & Pruitt JO. Preventingfeeding-associated aspiration. MEDSURG Nursing, 1995; 4(2),1 1 1 - 1 1 9 .
PRACTICAL GASTROENTEROLOGY • NOVEMBER 2002 33
A CASE TO REMEMBER
Aspiration Complications Following Nasogastric Administration of PEG Solution
A GUIDE FOR PATIENTSThe more that a patient knows about his or her problem, the easier it is for the patient to cooperate with you and the more effective can be the prescribed treatment. Each“ G u i d e ” is on a different subject among the digestive diseases. You may cut out the“Guide” and photocopy as many reprints as you wish for distribution to your patients.You may want to include your name and address. The information in “A Guide forPatients” has been prepared by the National Digestive Diseases Information ClearingHouse, a service of the National Institute of Diabetes and Digestive and Kidney Diseases,National Institutes of Health, U.S. Public Health Service. The material it contains has been carefully reviewed by NDDIC for scientific accuracy and content.
This month’s “A Guide for Patients” appears on pages 58–61.
PRA CT I CA L GA ST RO ENT EROLO GY