assessing social skill challenges in kids: autism, anxiety ... · mutism? odd? adhd? psychosis?...
TRANSCRIPT
Renée Marchant, Psy.D.Pediatric [email protected]
Assessing Social Skill Challenges in Kids: Autism,
Anxiety, Trauma?

Participants will learn:
1. Common pitfalls in mis-diagnosis of social-emotional issues
2. Key components of an ASD-focused neuropsychological evaluation
3. Usefulness of projective/performance-based testing4. Case study: ASD vs. psychiatric disorders
Eddie is a 9 year old boy in the 4th grade. His teacher notices that Eddie isn’t completing his homework, forgets his backpack most days, and is behind in math. He sits alone at lunch and doesn’t have any friends. He’s obsessed with magic. He “shuts down” when classwork gets hard. His eye contact is poor. He doesn’t talk much. He sometimes wears the same shirt a few days in a row.
Is this Autism?
Is this something else?
Is this both?

Social Skill Issues & Emotional Issues
one of the most challenging aspects of children’s functioning to assess
COMPLEX TRAUMA?
SOCIAL ANXIETY?
OCD?
LEARNING DISORDER?
DEPRESSION?
PROGRESSIVE HEARING LOSS?
TIC DISORDER?
ATTACHMENT DISORDER?
INTELLECTUAL DISABILITY?
LANGUAGE DISORDER?
SELECTIVE MUTISM?
ODD?
ADHD?
PSYCHOSIS?
ADJUSTMENT DISORDER?
EATING DISORDER?
PTSD?
GLOBAL DEVELOPMENTAL DELAY?
AUTISM?
ENURESIS?
Caution:
Easier to rule-in ASD…harder to rule-out ASD
Benefits & Challenges of Screening Tools
● Captures/quantifies behavior and social-emotional challenges as a screening tool
● Early diagnosis is best● Can initiate E.I. or a
comprehensive neuropsychological evaluation
● Vulnerable to rater biases● More “false positives”● Does not capture
thinking/cognition skills & other parts of functioning
● Weak discriminant validity…
Could be ASD OR could be anxiety….
SRS: Social Responsiveness ScaleWould rather be alone than with others
Can’t get his mind off something once he starts thinking about it
Avoids eye contact, or has unusual eye contact
ASD? Anxiety?
Or something else?
“Whole Picture” Neuropsychological Evaluation
Key components of an ASD-focused neuropsychological evaluation
Accurately diagnosing ASD is challenging!
No biological tests for ASD exist
Variable behaviors across different children with ASD
Variable behaviors within the same child with ASD across different contexts and across time/development
Symptom overlap between ASD and other disorders
Standards for a comprehensive ASD evaluation
1. Assessment of multiple areas of functioning (including adaptive skills)
2. Appreciation that variation in ability & performance is common
3. The use of a developmental perspective when assessing behavior and synthesizing results
DSM 5: Autism Spectrum Disorder
persistent deficits in social communication and social interaction across multiple contexts...,
...restricted, repetitive patterns of behavior, interests, or activities....”
“ONSET DURING THE EARLY DEVELOPMENTAL PERIOD”
Evaluating ASD: Core Domains
Detailed History
Observations of the child
Parent/Caregiver Interview
Contact with other professionals (teachers, therapist)
Cognition, Communication/language, “Gold Standard” measures of ASD, Social-Emotional skills, and Applied Life Skills
HistoryBirth History
Early Developmental History
Medical History
Family and Psychosocial History
Onset of Symptoms
Educational/Testing/Service History

Behavioral Observations
Transition to the testing office & hygiene/attire
Language & Social Communication
Motor Skills
Unusual Behaviors
Attention & Self-Regulation
Play
Cognition and Learning
Determine verbal and non-verbal strengths and weaknesses (IQ)
Executive Functioning
Memory Skills
Visual-motor skills
Academic Functioning
Communication & Language
● Expressive and receptive vocabulary● Grammar & Syntax● Pragmatics:
○ Non-Literal Language, Meaning from Context, Inferences, Social Rules/Conversation Skills
DSM 5: Autism Spectrum Disorder
persistent deficits in social communication and social interaction across multiple contexts...,
...restricted, repetitive patterns of behavior, interests, or activities....”
“ONSET DURING THE EARLY DEVELOPMENTAL PERIOD”
“Gold Standard” Measures for ASDADOS-2: semi-structured, standardized measure of communication, social interaction, play, and restricted and receptive behaviors
CARS-2: 15 item rating scale of key areas related to autism
Must incorporate: Parent interview, direct observation, school data
ADOS-2
● Ages 12 months to adulthood● Modules 1 to 4 based on level of language● Requires special training to administer, score,
interpret● Not sufficient for a diagnosis without other data● Creates a “Social world” rather than a “test”


ADOS-2 examples
Make-Believe Play
Joint Interaction Play
Cartoons
Response to Name & Social Smile
Demonstration Task
Telling a Story from a Book
Emotions
Description of a Picture
Break
Friends, Relationships, Marriage
Anticipation of a Social Routine
Joint Attention
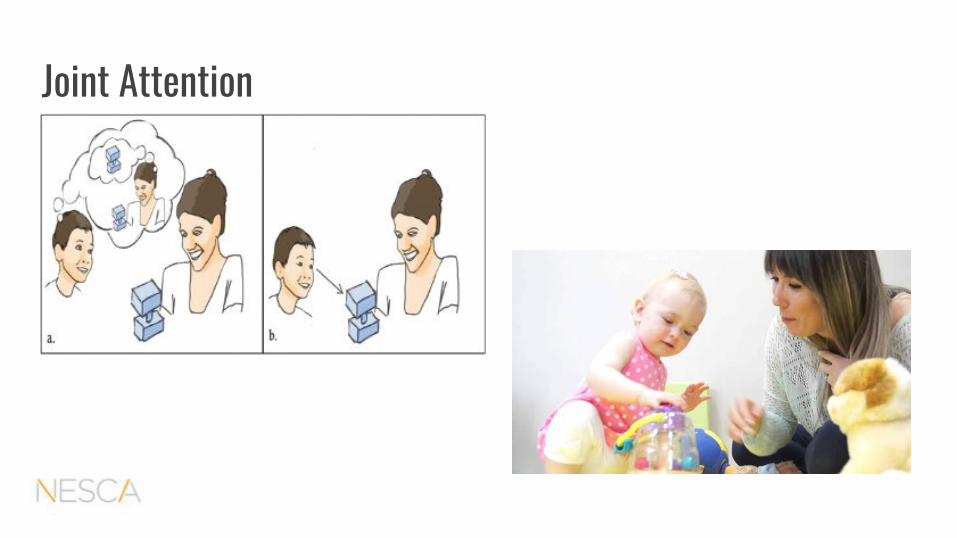
Joint Attention

Gestures
Adaptive Functioning: Applied Life Skills (VABS-3 & ABAS-3) ● Measurement of Adaptive
Functioning is critical to service access and delineation of severity in ASD and ID
● What an individual does in real life not what they’re capable of
● Practical skills● Social skills● Conceptual skills● Motor Skills● Maladaptive Behaviors

Social-Emotional Functioning
● Parent and Teacher Rating scales/questionnaires (CBCL/ASEBA, BASC-3)
● Self-report questionnaires of thoughts, emotions, and behavior○ Symptom inventories (BDI-2, RCMAS-2)○ Developing Personality Traits (MMPI-A, PAI-A, MACI)
● Projective/Performance-Based Measures

Projective Tests
Rorschach Inkblot Test
Story-telling Tasks (TAT, CAT, ROBERTS-2)
Sentence Completion Test
Patterns of Thinking, Feeling, Doing
Thinking Style & Reality Testing
Mood
Self-Esteem
Interpersonal Relationships
Projective Testing Referrals● Thinking problems (clarify
psychosis)● Mood presentation● Anxiety presentation● Coping Style● Trauma/attachment issues● Developing personality traits● Evaluate Risk● Capacity for Insight● Emotional StrengthsT
The Dark Mirror (1947)
Projective Testing: Caution for ReferralsChildren with:
visual acuity, processing & organization of visual info.
receptive & expressive language problems
high/low IQ
ASD
Learning disabilities
●
·
Projective Testing: Caution for Referrals
Projective testing should be integrated with other testing data
● Cognition: language and visual skills● Learning● Behavior, Attention & Self-regulation
Otherwise, there is an increased risk for mis-diagnosis of psychotic symptoms

Case Study
Eddie is a 9 year old boy in the 4th grade. His teacher notices that Eddie isn’t completing his homework, forgets his backpack most days, and is behind in math. He sits alone at lunch and doesn’t have any friends. He’s obsessed with magic. He “shuts down” when classwork gets hard. His eye contact is poor. He doesn’t talk much. He sometimes wears the same shirt a few days in a row.
Eddie
Hospitalized for “acute psychosis”
Aggression & threats
Legal custody of grandmother
Bio father moved to a new state
Witness to DV
Age 3: neurologist diagnosed “ASD”
No IEP or previous testing
Dx: depression with psychotic features
Started on risperdal
ASD “not appropriate”
Social
No “unusual” behaviors
Misses his father/mad at his grandma
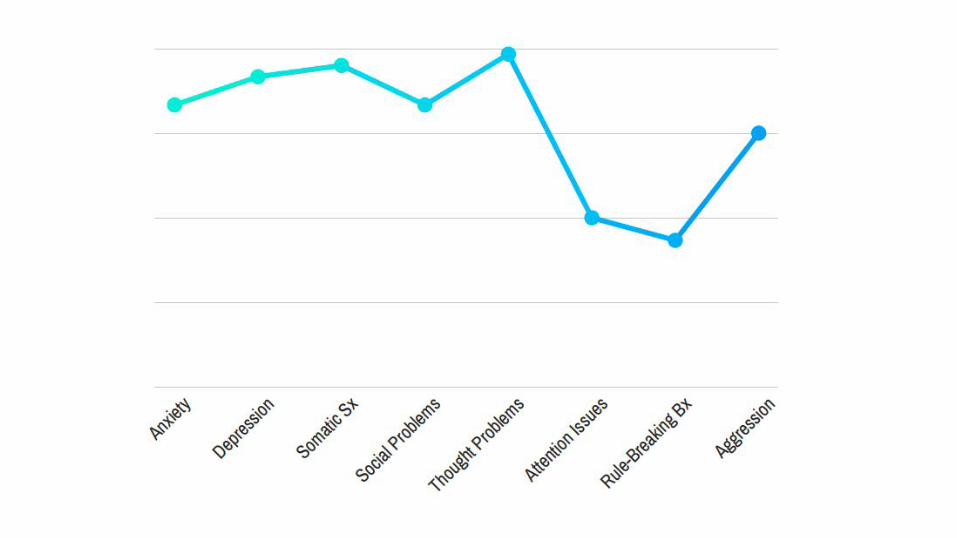
CBCL: Thought Problems
Can’t get his mind off of certain thoughts
Deliberately harms self or attempts suicide
Nervous movements or twitching
Picks nose, skin, other parts of body
Repeats certain acts over and over
Sleeps less than most kids
Strange Behavior (lays on the floor, makes weird noises)
Strange ideas (hates convenience store clerk because “he doesn’t let me take candy”)
Trauma?...Psychosis?...ASD?
Eddie was referred for Neuropsychological Testing...
Evaluating ASD: Core Domains
Detailed History
Observations of the child
Parent Interview
Contact with other professionals (teachers, therapist)
Cognition, Communication/language, “Gold Standard” measures of ASD, Social-Emotional skills, and Applied Life Skills

Neuropsych Testing Highlights
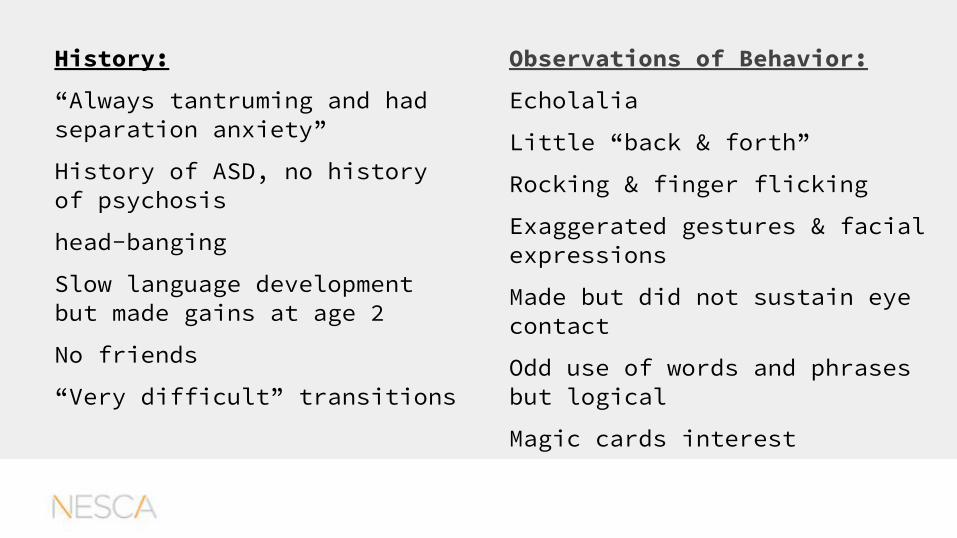
History:
“Always tantruming and had separation anxiety”
History of ASD, no history of psychosis
head-banging
Slow language development but made gains at age 2
No friends
“Very difficult” transitions
Observations of Behavior:
Echolalia
Little “back & forth”
Rocking & finger flicking
Exaggerated gestures & facial expressions
Made but did not sustain eye contact
Odd use of words and phrases but logical
Magic cards interest
Cognition: average verbal and non-verbal skills, poor memory of social stories, poor organization and planning, couldn’t “switch gears”
Academic: impaired word problems, slower reading speed
Communication/language: average concrete skills, impaired pragmatic & nonliteral language
ADOS-2: Consistent with ASD diagnosis
Social-Emotional: anxious & depressed; “Unique” thinking rather than inaccurate/bizarre
Life Skills: below expectations for his age
Diagnoses:
Autism Spectrum Disorder
Unspecified Anxiety Disorder
Unspecified Depressive Disorder
Attachment Disruptions/Complex Trauma
Caution: Psychosis or Social Communication Deficits?
● Changing topics of conversation to a new unrelated topic without preparing the listener for a topic change
● Incorrect/inappropriate reasoning ● Social withdrawal, poor eye contact & flat affect● When stressed, ASD can “look” like paranoia

ASD vs. PsychosisConcrete, immature thinking
Social deficits more long-standing
repetitive, concrete or odd language
Scripts
Repetitive “rigid” behaviors
Skills go up & down over time
complex/bizarre thinking
Social deficits may increase over time
Disjointed & more bizarre language
Hallucinations
Strange,often not rigid behaviors
Skills decline over time

Take Home Points
It’s never just about test scoresASD diagnosis is about functioning with peers in the world
Scores on CARS, ADOS-2 don’t “diagnose” ASD but are meant to be incorporated in a thorough, comprehensive evaluation
No single psychometric test is sufficient or appropriate, by itself, for assessing ASD
You need collateral information about “real life” skills and detailed, thorough history
Evaluating ASD: Core Domains
Detailed History
Observations of the child
Parent Interview
Contact with other professionals (teachers, therapist)
Cognition, Communication/language, “Gold Standard” measures of ASD, Social-Emotional skills, and Applied Life Skills
What do we do with kids who have complex social-emotional challenges?1. Be cautious with evaluations that have not assessed
various domains of functioning (e.g. brief “one-test” evaluations)
2. Refer the child for a “whole picture” neuropsychological evaluation
3. Projective testing should be integrated with other testing data and isn’t for everyone

Why do we care?Social
&
Emotional Issues
Treatment is different for ASD vs.
other diagnoses
Treatment can build skills, emotional safety, and/or problem-solving
Early, accurate diagnosis
matters
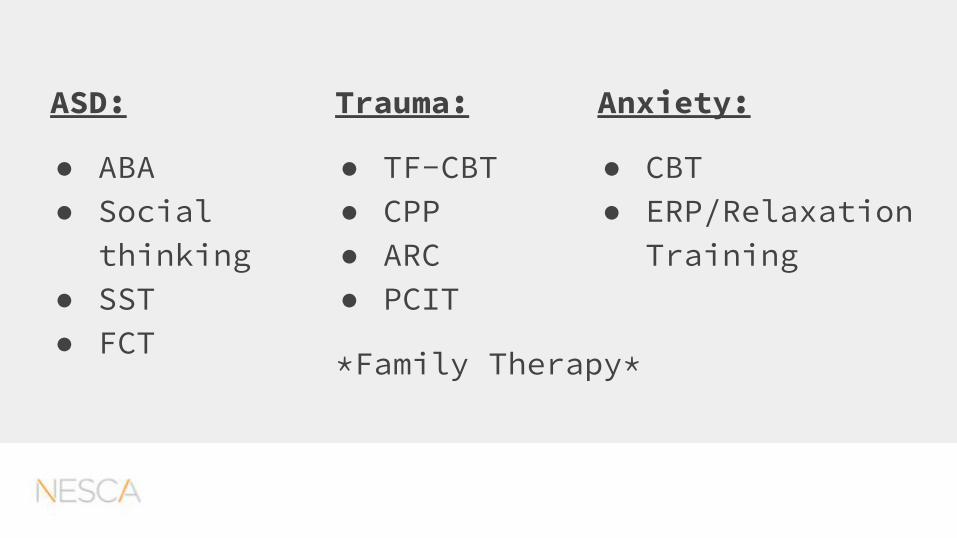
ASD:
● ABA● Social
thinking● SST● FCT
Trauma:
● TF-CBT● CPP● ARC● PCIT
*Family Therapy*
Anxiety:
● CBT● ERP/Relaxation
Training

Treatment Outside of PsychoTherapy
Speech and Language Therapy
Occupational Therapy
Physical Therapy
Academic Tutoring
Executive Functioning Coaching and Tutoring
Camps & Extra-curriculars
ASD Treatment:
Anxiety and Trauma Treatment:
ADHD Treatment: