assessment of coronary reserve by transoesophageal doppler
TRANSCRIPT
European Heart Journal (1997) 18, 514-523
Assessment of coronary reserve bytransoesophageal Doppler echocardiography
Direct comparison between different modalities of dipyridamole andadenosine administration
M. Kozakova, C. Palombo, L. Pratali, G. Bigalli, M. Marzilli, A. Distante andA. L'Abbate
Institute of Clinical Physiology, C.N.R. Pisa, Italy
Background This study was undertaken to compare thecoronary vasodilator response to different applicationmodalities of intravenous vasodilators, in order to identifythe optimal pharmacological protocol for the evaluation ofcoronary reserve by means of transoesophageal Dopplerechocardiography.
Methods Blood flow velocity in the left anterior descend-ing artery, coronary vascular resistance and left maincoronary artery cross-sectional area were assessed bytransoesophageal echo-Doppler during an i.v. adenosinebolus (5 mg), a 5-min adenosine infusion (infusionrate 140 ug . kg~ ' . min~ '), and low (0-56 mg . kg~ ' .4min~1), and high-dose (0-84 mg . kg~ ' . 9 min~ ') di-pyridamole infusions in 10 healthy normals (Group 1) andin 20 patients (Group 2) with either coronary microvasculardisease (11 patients) or coronary artery disease (ninepatients).
Results In both groups, the highest flow velocity and thelowest coronary vascular resistance were observed duringthe adenosine infusion. Flow velocity values and indices ofcoronary vasodilator capacity observed after the adenosinebolus and the high-dose dipyridamole infusion were very
close to those obtained during the adenosine infusion,especially in Group 1. Coronary flow velocity was lowerand coronary vascular resistance higher after low-dosedipyridamole, significantly in Group 2. The maximal flowresponse to the adenosine bolus was observed within a fewseconds after the injection, and was very short. The peakresponse to the adenosine infusion was observed 57 ± 27 safter its start. The coronary flow velocity response todipyridamole was dose dependent and differed betweenGroups 1 and 2.
Conclusion In combination with transoesophagealDoppler echocardiography, a short-lasting adenosine infu-sion at a rate of 140 ug . kg ~ ' . min ~ ' seems to be prefer-able to an adenosine bolus and dipyridamole infusion. Theeffect of the bolus is too short for an accurate measurementof coronary flow velocity, while the dipyridamole infusion,especially at a low dose, induces a submaximal vasodilatorresponse.(Eur Heart J 1997; 18: 514-523)
Key Words: Transoesophageal echocardiography,coronary reserve, adenosine, dipyridamole.
Introduction
The main techniques used in clinical cardiology for theassessment of coronary vasodilator capacity are atpresent intracoronary Doppler and positron emissiontomography. In the last few years, several authorshave demonstrated the possibility of monitoring thecoronary flow velocity response to vasoactive agents in
Revision submitted 26 September 1996, and accepted 2 October1996.
Correspondence: Carlo Palombo, MD, Institute of ClinicalPhysiology, C.N.R., Via Savi 8, 56126 Pisa. Italy.
the proximal left anterior descending artery by means oftransoesophageal Doppler echocardiography11""1.
Transoesophageal Doppler echocardiography,thanks to its limited invasiveness, allows serial assess-ment of coronary flow velocity reserve in the samepatient and in subjects in whom an invasive procedure isnot justified'71. Coronary flow velocity by transoesopha-geal Doppler echocardiography can be adequately moni-tored in the proximal part of the left anterior descendingartery, being the ultrasound beam optically aligned withthe direction of flow at this level only. Due to such alimitation, this method may be useful in patients withdiffuse microvascular disease15"71, or in selected subsets
OI95-668X/97/030514+10 S18.00/0 1997 The European Society of Cardiology
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
Assessment of coronary reserve 515
of patients with coronary artery disease'8 U). In theformer, impairment of vasodilator capacity may involvethe entire coronary bed, so that measurements of cor-onary reserve in the left anterior descending arteryterritory may be representative of the overall left ven-tricle. In patients with coronary artery disease, thefunctional significance of intermediate stenosis of theleft anterior descending artery'"1 as well as the late resultof angioplasty may be evaluated'8"101.
The aim of the present study was to identify theoptimal pharmacological protocol for the evaluation ofcoronary reserve by means of transoesophageal Dopplerechocardiography in the spectrum of patients suitablefor this approach. The majority of studies published sofar used low-dose dipyridamole as the vasodilator'4'9'101;recently adenosine was proposed as a superior agent'"1.However, a direct comparison between the two agents asregards coronary vasodilator response, systemic haemo-dynamic effects and side effects has not been made.
Methods
Study population
Thirty subjects were investigated, including 10 healthyvolunteers (Group 1) and 20 patients (Group 2). In thehealthy volunteers (mean age 44 ±22 years) the presenceof significant coronary artery disease was excludedthrough a comprehensive non-invasive investigation(clinical history, basal electrocardiogram and echo-cardiogram, exercise stress test and dipyridamole-atropine echocardiographic test).
Patients (Group 2: 13 men and seven women,mean age 57 ±13 years) were selected from thosereferred to our Institute for diagnostic coronary angio-graphy. Out of these, 11 had angiographically normalcoronary arteries, while nine had coronary stenosis.Among patients with angiographically normal coronaryarteries seven were hypertensives with left ventricu-lar hypertrophy (left ventricular mass index 158 ±29 g . m ~2), and four had non-obstructive hypertrophiccardiomyopathy (left ventricular mass index 182 ±33 g . m ~ ) . Among patients with coronary artery dis-ease, all had intermediate left anterior descending arterystenosis (50-75%) and four also had 50-75% stenosis ofeither the right coronary artery or the circumflex artery.Exclusion criteria were acute myocardial infarction,unstable angina, congestive heart failure, atrioventricu-lar block of any degree, previous coronary bypasssurgery or percutaneous transluminal coronary angio-plasty, obstructive pulmonary disease, or treatment withdipyridamole or theophylline preparations.
None of the volunteers was under drug therapyat the time of the study; in patients, calcium antagonistsand nitrates were discontinued at least 72 h before thestudy, and all other medications at least one weekbefore. All subjects were requested to abstain fromxanthine-containing food and drinks for at least 24 hbefore the study.
The study had been approved by the internalethical committee; all the subjects studied were informedabout the procedure and provided consent in accordancewith the declaration of Helsinki.
Study protocol
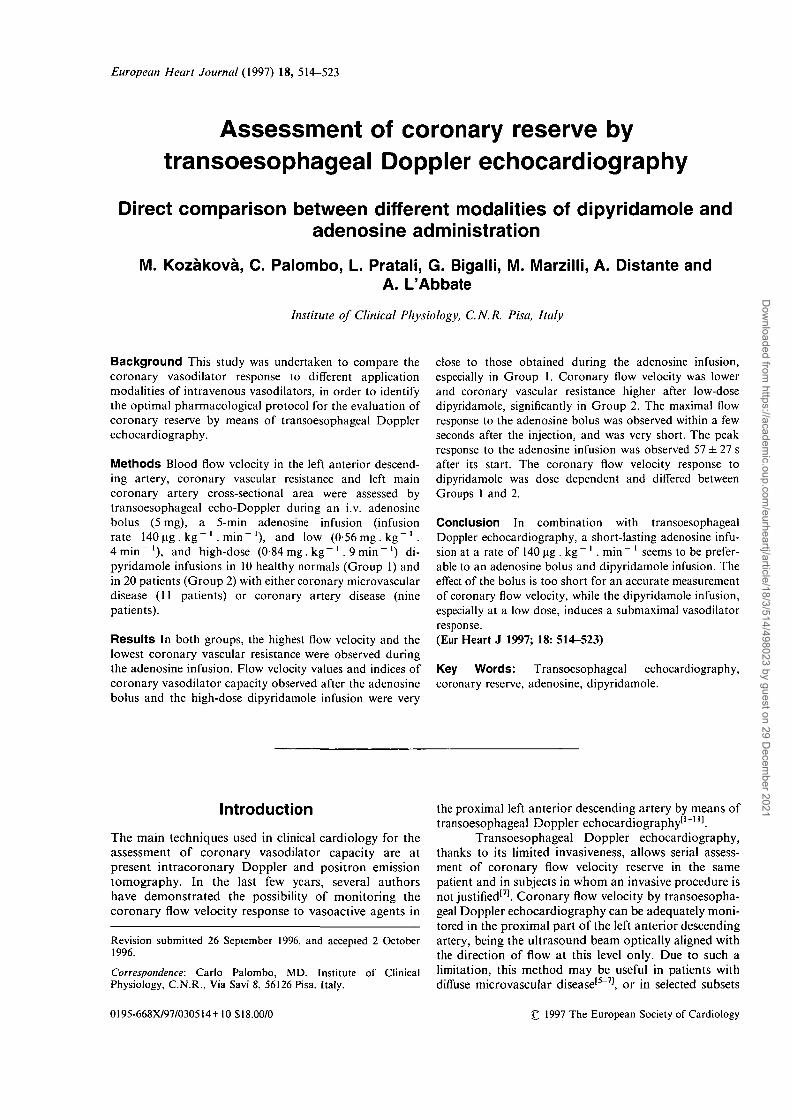
After topical anaesthesia of the oropharynx and awakesedation by i.v. diazepam (5 to 10 mg), the trans-oesophageal omniplane probe (SONOS 1500; Hewlett-Packard Co.; Andover, Mass, U.S.A.) was introducedinto the upper oesophagus. The proximal part of the leftanterior descending artery was visualized, and bloodflow detected by colour and spectral Doppler (Fig. 1).The angle between the ultrasound beam and thedirection of the artery was adjusted as close to zero aspossible and never exceeded 30°.
After each subject had rested for at least 2 min,the first basal recording of the spectral Doppler signalwas performed. The 2-D image, showing the position ofthe Doppler sample volume in the left anterior descend-ing artery, was stored in the cine-loop memory and wasrepeatedly retrieved during the study to ensure that thecoronary flow velocity was always measured at the samelevel. 'Zoomed' 2-D images of the left main coronaryartery were obtained to measure the luminal diameter ofthe epicardial vessel.
Adenosine (solution of crystalline adenosine,Sigma Chemical Co., Milan, Italy, in sterile pyrogen freevials provided by Laboratori Baldacci, Pisa, Italy)and dipyridamole (Persantine, Boehringer Ingelheim,Germany) were sequentially administered through anindwelling 18 G cannula in the left antecubital vein. Thepharmacological protocol was started with a 5 mg bolusinjection of adenosine. Flow velocity in the left anteriordescending artery was continuously recorded in ordernot to miss the short-lasting peak flow response. Twominutes after the adenosine bolus, a 5 min infusion ofadenosine was started (140 ug . kg" ' . min" '). TheDoppler signal was continuously recorded during theinfusion, and the flow velocity and left main diameterwere measured at the time of peak response.
After the adenosine infusion, sufficient time wasallowed to let the coronary flow velocity return to itsbasal value; a second basal recording was made offlow velocity and left main artery diameter. Followingthis, the first dose of dipyridamole (0-56 mg . kg" ') wasinjected in 4 min (low-dose dipyridamole); measure-ments of flow velocities in the left anterior descendingartery were provided midway (2 min) and at the end ofthe dose, while the left main artery diameter wasmeasured only at the end of the dose. After a 3-mininterval, flow velocity measurements were repeatedand a further dose (0-28 mg. kg"1) of dipyridamolewas injected over 2 min. After this overall dose(0-84 mg . kg" ' . 9 min~', i.e. high-dose dipyridamole)coronary flow velocity was monitored for a further4 min and the highest flow response was measuredtogether with the left main artery diameter. At the end of
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
516 M. Kozakova et al.
Figure 1 The coronary blood flow velocity profile from the proximal partof the left anterior descending artery has a biphasic pattern, with a smallersystolic and larger diastolic component.
the study, or at the onset of myocardial ischaemia,aminophylline at a dose of 80-240 mg was injected in allsubjects.
Throughout the study, the three-lead ECG wasmonitored continuously and the 12-lead ECG was re-corded every 2 min. Blood pressure was continuouslyassessed by a Finapres monitor (Ohmeda, Englewood,CO) in the arm contralateral to that receiving the druginfusion.
Coronary blood flow velocity measurement
The coronary blood flow velocity profile from the proxi-mal part of the left anterior descending artery showed atypical biphasic pattern (Fig. 1). For the purpose of thisstudy, the average of the instantaneous spectral peakvelocities during one cardiac cycle was measured atdifferent steps of the study (Fig. 2), rather than atmaximal diastolic velocity, as it better corresponds tovolume flow rate1'2131. The average peak velocity wasobtained by manually tracing the circumference of thebiphasic velocity spectrum and by automatic measure-ment of instantaneous velocities at multiple small timeintervals.
Flow velocity was assessed by pulsed Doppler,and when its value exceeded the Doppler limit duringmaximal vasodilation, continuous wave Doppler wasused. Coronary flow velocity measurements wereprovided off-line from videotapes by one observer. Tenrandomly selected studies were analysed twice by thesame observer (M.K.) at a 2-month interval, as well asby a second observer (C.P.) to assess intra- and inter-individual variability. Final values of flow velocityrepresent an average of five cardiac cycles.
Assessment of coronary vasodilator response
The coronary vasodilator response to both adenosineand dipyridamole was expressed as coronary reserve andcoronary vascular resistance. Coronary reserve wasestimated as a ratio of average peak velocity after eachvasodilator stimulus and the corresponding basalaverage peak velocity. Coronary vascular resistance wascalculated as the ratio of simultaneously measured meanblood pressure and average peak velocity at differentsteps of the study.
Evaluation of coronary artery calibre
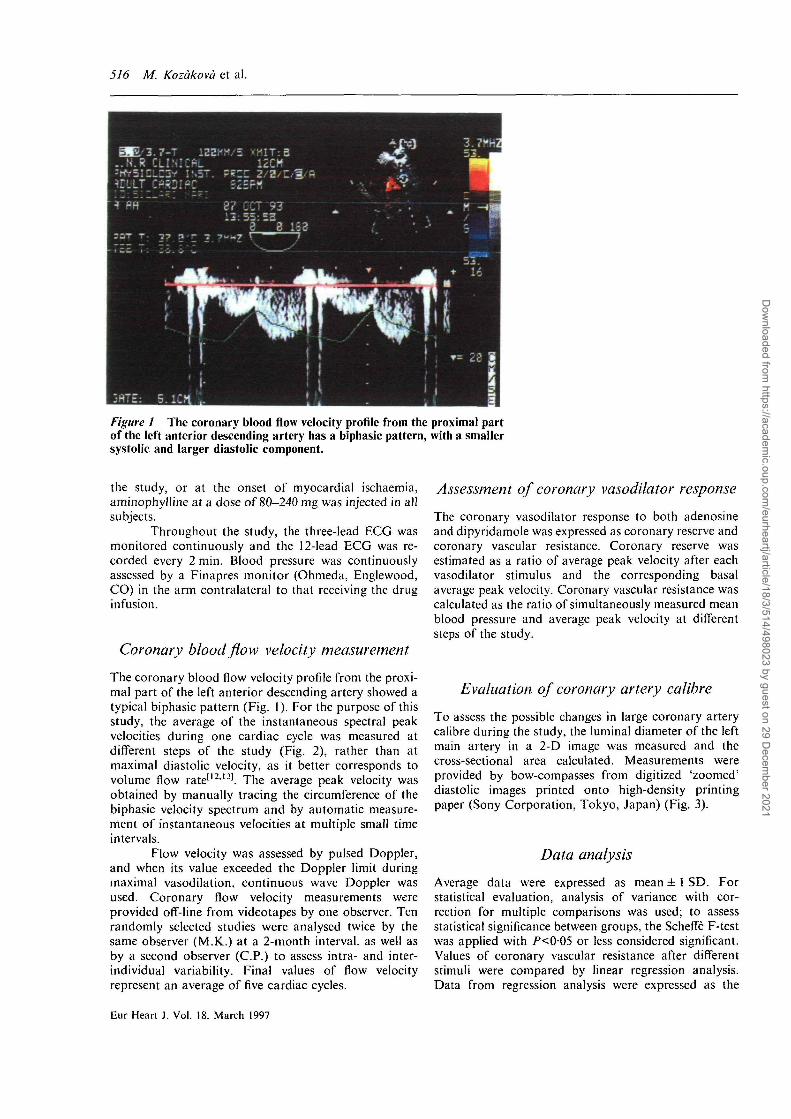
To assess the possible changes in large coronary arterycalibre during the study, the luminal diameter of the leftmain artery in a 2-D image was measured and thecross-sectional area calculated. Measurements wereprovided by bow-compasses from digitized 'zoomed'diastolic images printed onto high-density printingpaper (Sony Corporation, Tokyo, Japan) (Fig. 3).
Data analysis
Average data were expressed as mean ± 1 SD. Forstatistical evaluation, analysis of variance with cor-rection for multiple comparisons was used; to assessstatistical significance between groups, the Scheffe F-testwas applied with /><005 or less considered significant.Values of coronary vascular resistance after differentstimuli were compared by linear regression analysis.Data from regression analysis were expressed as the
Eur Heart J. Vol. 18. March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
Assessment of coronary reserve 517
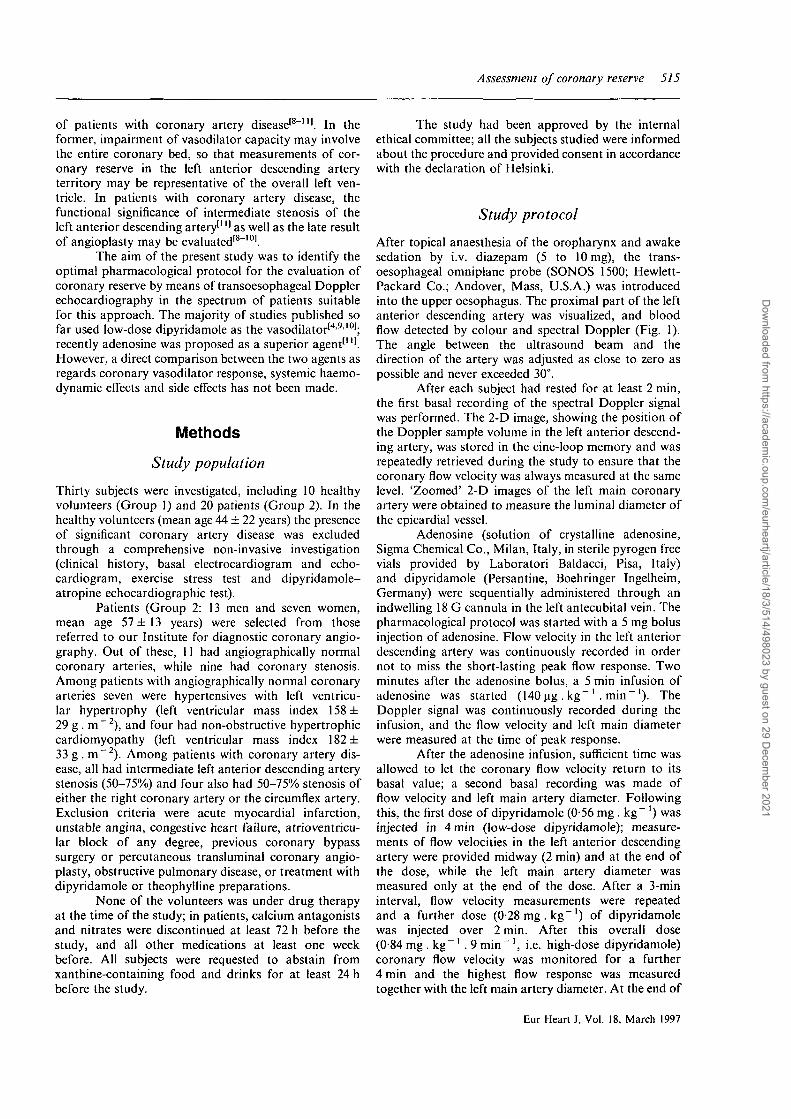
Basal 1 Ado bolus Ado infusion
APV = 42.5 cm.s"1
MBP = 120 mmHgHR = 86 beats.min
APV = 113 cm.sMBP = 122 mmHgHR = 88 beats.min"1
APV = 130 cm.s"1
MBP = 110 mmHgHR = 95 beats.min
Basal 2 Dip low Dip high
APV = 41.5 cm.s"1
MBP = 108 mmHgHR = 81 beats.min
APV = 106 cm.s"1
MBP = 108 mmHgHR = 85 beats.min"1
APV = 114 cm.s"1
MBP = 102 mmHgHR = 106 beats.min
Figure 2 Spectral Doppler signal of the flow in the left anterior descending artery during thefirst basal measurement, during the adenosine bolus, the adenosine infusion and during thesecond basal measurement of low-dose and high-dose dipyridamole. Due to differences invelocity scale in the various images, a black arrow was introduced to indicate a 100 cm . s ~ 'value. APV = time average of the spectral peak velocity; MBP=mean blood pressure; HR = heartrate.
correlation coefficient (r), slope, and the significance ofthe relationship. The agreement between two readingsperformed by two observers was evaluated, estimatingthe consistent bias between the two readings, as recom-mended by Bland and Altman for the comparison oftwo methods of clinical measurement'141. Statisticalanalysis was performed using commercially availablesoftware (StatView SE +Graphics, Abacus ConceptsInc., Berkeley, CA, U.S.A.).
Results
Variability of coronary flow velocitymeasurements
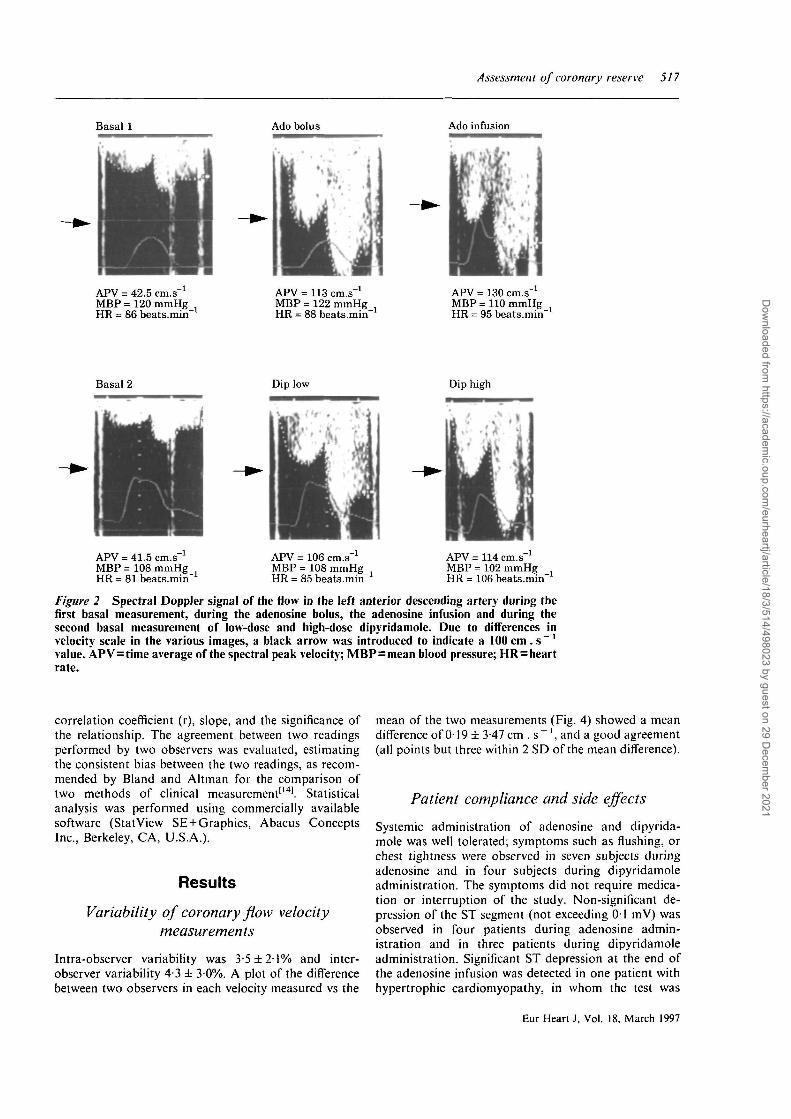
Intra-observer variability was 3-5 ± 2 1 % and inter-observer variability 4-3 ± 30%. A plot of the differencebetween two observers in each velocity measured vs the
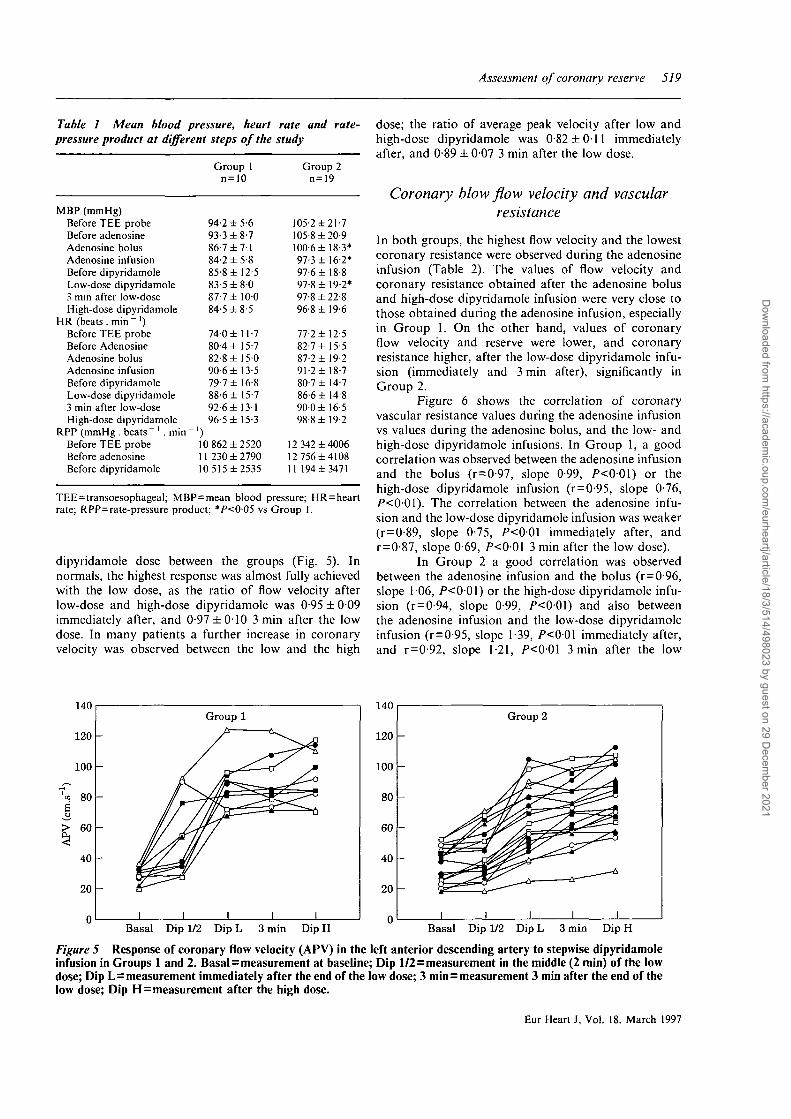
mean of the two measurements (Fig. 4) showed a meandifference of 019 ± 3-47 cm . s~ ', and a good agreement(all points but three within 2 SD of the mean difference).
Patient compliance and side effects
Systemic administration of adenosine and dipyrida-mole was well tolerated; symptoms such as flushing, orchest tightness were observed in seven subjects duringadenosine and in four subjects during dipyridamoleadministration. The symptoms did not require medica-tion or interruption of the study. Non-significant de-pression of the ST segment (not exceeding 01 mV) wasobserved in four patients during adenosine admin-istration and in three patients during dipyridamoleadministration. Significant ST depression at the end ofthe adenosine infusion was detected in one patient withhypertrophic cardiomyopathy, in whom the test was
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
5J8 M. Kozakova et al.
Figure 3 'Zoomed' diastolic 2-D image of the left main coronary artery,from which the luminal diameter of the vessel was measured.
interrupted and the dipyridamole infusion not per-formed. Thus, only 19 patients were considered forfinal evaluation.
Systemic haemodynamic responses
Data on mean arterial blood pressure and heart rate inthe two groups is reported in Table 1. In Group 2, meanblood pressure was higher at almost every step of thestudy, as compared to Group 1. Adenosine bolus, aswell as adenosine infusion mildly decreased mean bloodpressure as compared to the basal values ( — 4-8 ± 109and — 7-6 ± 11-1%, respectively). Mean blood pressure
20
15
10
5
0
-5
-2
-10
-15
-
-
-
. 1
o n
° o ^
, 1
o
<$>
. 1
n
i i
o rO
1
0
(
0
1
oo
I
I
1 I
20 40 60 80 100 120 140Mean (cm.s l)
Figure 4 Inter-individual variability of coronary flowvelocity determination: plot of the difference between thetwo observers' values vs the mean of the measured values.Good agreement is seen with a zero bias (mean difference0-19 ±3-47 cm . s - l ) . Lines represent boundaries of± 2 S D .
before the dipyridamole infusion was slightly lower thanthat before the adenosine injection ( — 7-3 ± 102%),and the dipyridamole infusion did not further de-crease blood pressure. In relation to basal values, theheart rate slightly increased during the adenosinebolus (+3-7 ±9-5 beats . min~ ') and adenosine in-fusion (+9-0 ± 101 beats . min~ ') as well as duringthe dipyridamole infusion ( + 6-9 ± 9-3 beats. min~'immediately after the low-dose infusion, +10-3±101 beats . min~' 3 min after the low-dose infusion,and +17-7 ± 14-4 beats . min ~ ' after the high-doseinfusion).
In both groups, the rate-pressure product duringthe first basal flow measurement was comparable to thatpreceding the introduction of the transoesophagealprobe and slightly, although not significantly, higherthan that found during the second basal flow measure-ment (Table 1).
Time-course of the hyperaemic response toadenosine and dipyridamole
The response to the 5 mg adenosine bolus was short,lasting about five cardiac cycles, and was observedwithin 8 ± 4 s after the end of the injection. The averagetime from the onset of the adenosine infusion to peakflow velocity was 57 ± 27 s; flow returned to baselinewithin 3 min of the interruption of the infusion in allsubjects. No differences in the time response of flowvelocity to adenosine were observed between the twogroups.
The coronary flow velocity response to di-pyridamole was dose-dependent. There was a differencein the dependence of coronary flow velocity on the
Eur Heart J. Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
Assessment of coronary reserve 519
Table 1 Mean blood pressure, heart rate and rate-pressure product at different steps of the study
MBP (mmHg)Before TEE probeBefore adenosineAdenosine bolusAdenosine infusionBefore dipyridamoleLow-dose dipyridamole3 min after low-doseHigh-dose dipyridamole
HR (beats . min ~ ')Before TEE probeBefore AdenosineAdenosine bolusAdenosine infusionBefore dipyridamoleLow-dose dipyridamole3 min after low-doseHigh-dose dipyridamole
RPP (mmHg . beats" ' . min"Before TEE probeBefore adenosineBefore dipyridamole
Group 1n=10
94-2 ± 5-693-3 ±8-786-7 ± 7184-2 ± 5-885-8 ± 12-583-5 ± 8 087-7 ± 10084-5 ±8-5
74-0 ± 11-780-4 ± 15-782-8 ± 15090-6 ± 13-579-7 ± 16-888-6 ±15-792-6± 13196-5 ± 15-3
')10 862 ±252011 230 ± 279010 515 ±2535
Group 2n=19
105-2 ±21-7105-8 ±20-9100-6 ± 18-3*97-3 ± 16-2*97-6 ± 18-897-8 ±19-2*97-8 ±22-896-8 ±19-6
77-2 ±12-582-7 ± 15 587-2 ± 19-291-2 ± 18-780-7 ± 14-786-6 ±14-8900 ± 16-598-8 ±19-2
12 342 ±400612 756±410811 194 ±3471
TEE = transoesophageal; MBP = mean blood pressure; HR = heartrate; RPP = rate-pressure product; *P<005 vs Group 1.
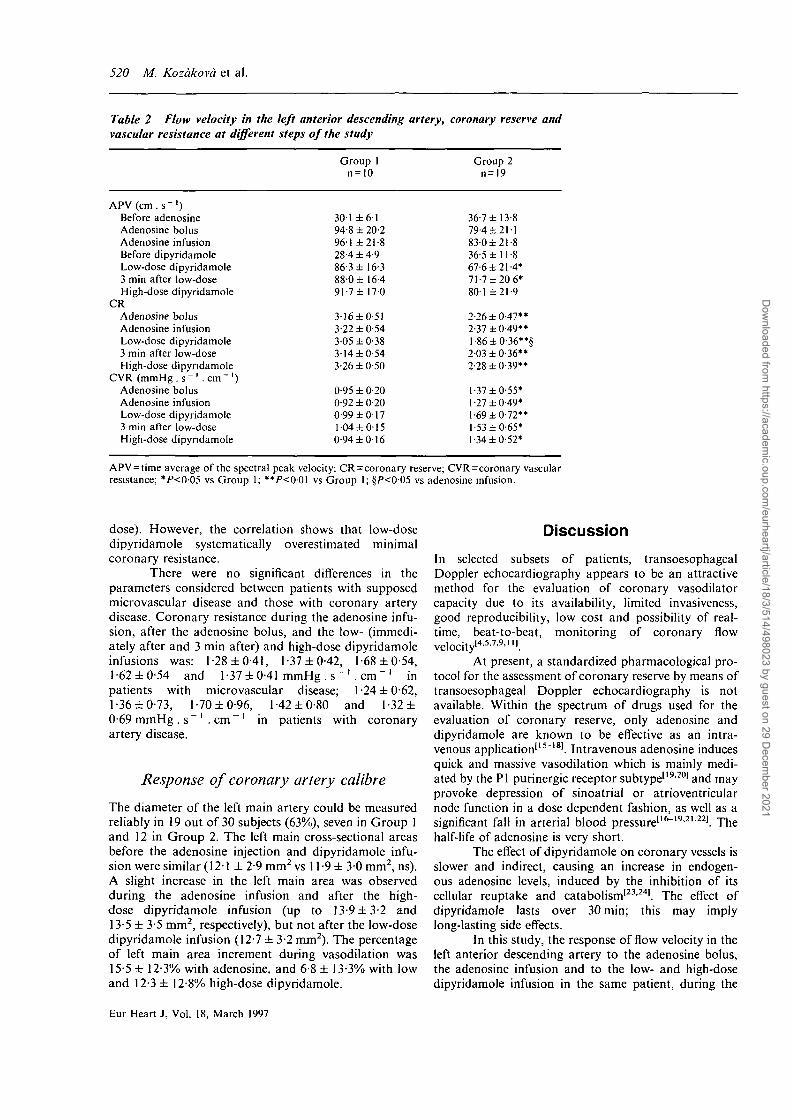
dipyridamole dose between the groups (Fig. 5). Innormals, the highest response was almost fully achievedwith the low dose, as the ratio of flow velocity afterlow-dose and high-dose dipyridamole was 095 ± 009immediately after, and 0-97 ±0-10 3 min after the lowdose. In many patients a further increase in coronaryvelocity was observed between the low and the high
dose; the ratio of average peak velocity after low andhigh-dose dipyridamole was 0-82 ±011 immediatelyafter, and 0-89±007 3 min after the low dose.
Coronary blow flow velocity and vascularresistance
In both groups, the highest flow velocity and the lowestcoronary resistance were observed during the adenosineinfusion (Table 2). The values of flow velocity andcoronary resistance obtained after the adenosine bolusand high-dose dipyridamole infusion were very close tothose obtained during the adenosine infusion, especiallyin Group 1. On the other hand, values of coronaryflow velocity and reserve were lower, and coronaryresistance higher, after the low-dose dipyridamole infu-sion (immediately and 3 min after), significantly inGroup 2.
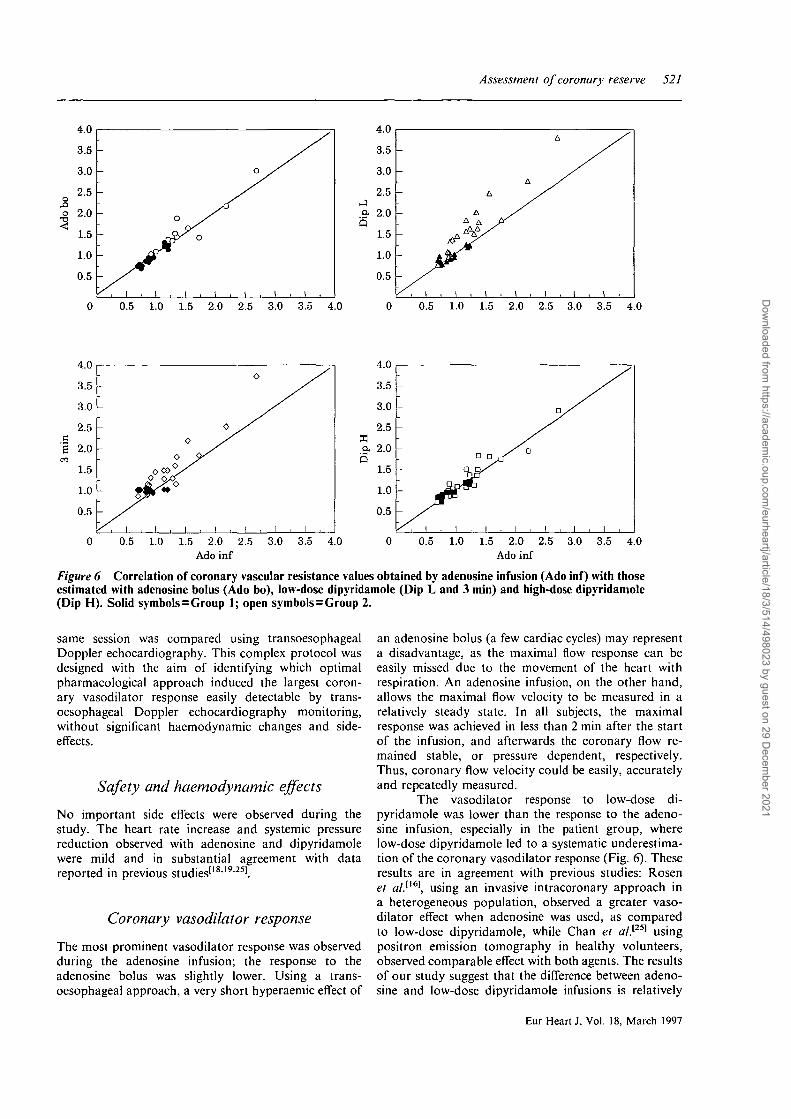
Figure 6 shows the correlation of coronaryvascular resistance values during the adenosine infusionvs values during the adenosine bolus, and the low- andhigh-dose dipyridamole infusions. In Group 1, a goodcorrelation was observed between the adenosine infusionand the bolus (r=0-97, slope 0-99, P<001) or thehigh-dose dipyridamole infusion (r = 0-95, slope 0-76,P<001). The correlation between the adenosine infu-sion and the low-dose dipyridamole infusion was weaker(r = 0-89, slope 0-75, P<00l immediately after, andr=0-87, slope 0-69, P<001 3 min after the low dose).
In Group 2 a good correlation was observedbetween the adenosine infusion and the bolus (r=0-96,slope 106, P<0-01) or the high-dose dipyridamole infu-sion (r=0-94, slope 0-99, P<001) and also betweenthe adenosine infusion and the low-dose dipyridamoleinfusion (r=0-95, slope 1-39, P<001 immediately after,and r=0-92, slope 1 -21, /><001 3 min after the low
Basal Dip 1/2 Dip L 3 min Dip H Basal Dip 1/2 Dip L 3 min Dip H
Figure 5 Response of coronary flow velocity (APV) in the left anterior descending artery to stepwise dipyridamoieinfusion in Groups 1 and 2. Basal=measurement at baseline; Dip 1/2=measurement in the middle (2 min) of the lowdose; Dip L=measurement immediately after the end of the low dose; 3 min = measurement 3 min after the end of thelow dose; Dip H=measurement after the high dose.
Eur Heart J, Vol. 18. March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
520 M. Kozakova et al.
Table 2 Flow velocity in the left anterior descending artery, coronary reserve andvascular resistance at different steps of the study
APV(cm.s" ')Before adenosineAdenosine bolusAdenosine infusionBefore dipyridamoleLow-dose dipyridamole3 min after low-doseHigh-dose dipyridamole
CRAdenosine bolusAdenosine infusionLow-dose dipyridamole3 min after low-doseHigh-dose dipyridamole
CVR (mmHg.s"1 .cm"1)Adenosine bolusAdenosine infusionLow-dose dipyridamole3 min after low-doseHigh-dose dipyridamole
APV = time average of the spectral peak velocity; CR = coronary reserve; CVR=coronary vascularresistance; */><005 vs Group 1; **P<001 vs Group 1; §/"<005 vs adenosine infusion.
Group 1n=10
301 ± 6 194-8 ± 20-2961 ±21-828-4 ±4-986-3 ±16-3880 ± 16-491-7 ± 1 7 0
3-16 ±0-513-22 ±0-543-05 ±0-383-14 ±0-543-26 ±0-50
0-95 ± 0-200-92 ± 0-200-99 ±0-171 04 ±0-150-94 ± 0 1 6
Group 2n=19
36-7 ± 13-879-4 ±21-183-0± 21-836-5 ±11-867-6 ±21-4*71-7 ±20 6*801 ±21-9
2-26 ±0-47**2-37 ±0-49**l-86±0-36**§2-03 ±0-36**2-28 ±0-39**
1-37 ±0-55*1-27 ±0-49*1-69 ±0-72**1-53 ±0-65*1-34 ±0-52*
dose). However, the correlation shows that low-dosedipyridamole systematically overestimated minimalcoronary resistance.
There were no significant differences in theparameters considered between patients with supposedmicrovascular disease and those with coronary arterydisease. Coronary resistance during the adenosine infu-sion, after the adenosine bolus, and the low- (immedi-ately after and 3 min after) and high-dose dipyridamoleinfusions was: 1-28 ±0-41, 1-37 ±0-42, 1-68 ±0-54,1-62 ± 0 5 4 and 1-37 ± 0-41 mmHg . s~ ' . cm" ' inpatients with microvascular disease; 1-24 ±0-62,1-36 ±0-73, 1-70 ±0-96, 1-42 ±0-80 and 1-32 ±0-69 mmHg . s~ ' . cm ~ ' in patients with coronaryartery disease.
Response of coronary artery calibre
The diameter of the left main artery could be measuredreliably in 19 out of 30 subjects (63%), seven in Group 1and 12 in Group 2. The left main cross-sectional areasbefore the adenosine injection and dipyridamole infu-sion were similar (121 ±2-9 mm2 vs 11 -9 ± 30 mm2, ns).A slight increase in the left main area was observedduring the adenosine infusion and after the high-dose dipyridamole infusion (up to 13-9 ± 3-2 and13-5 ± 3-5 mm2, respectively), but not after the low-dosedipyridamole infusion (12-7 ± 3-2 mm2). The percentageof left main area increment during vasodilation was15-5 ± 12-3% with adenosine, and 68 ± 13-3% with lowand 12-3 ± 12-8% high-dose dipyridamole.
Discussion
In selected subsets of patients, transoesophagealDoppler echocardiography appears to be an attractivemethod for the evaluation of coronary vasodilatorcapacity due to its availability, limited invasiveness,good reproducibility, low cost and possibility of real-time, beat-to-beat, monitoring of coronary flowvelocity'4-5-7'9-1".
At present, a standardized pharmacological pro-tocol for the assessment of coronary reserve by means oftransoesophageal Doppler echocardiography is notavailable. Within the spectrum of drugs used for theevaluation of coronary reserve, only adenosine anddipyridamole are known to be effective as an intra-venous application'15"181. Intravenous adenosine inducesquick and massive vasodilation which is mainly medi-ated by the PI purinergic receptor subtype'19201 and mayprovoke depression of sinoatrial or atrioventricularnode function in a dose dependent fashion, as well as asignificant fall in arterial blood pressure1'6"19-2122'. Thehalf-life of adenosine is very short.
The effect of dipyridamole on coronary vessels isslower and indirect, causing an increase in endogen-ous adenosine levels, induced by the inhibition of itscellular reuptake and catabolism'23'24'. The effect ofdipyridamole lasts over 30 min; this may implylong-lasting side effects.
In this study, the response of flow velocity in theleft anterior descending artery to the adenosine bolus,the adenosine infusion and to the low- and high-dosedipyridamole infusion in the same patient, during the
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
Assessment of coronary reserve 521
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0Ado inf
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0Ado inf
Figure 6 Correlation of coronary vascular resistance values obtained by adenosine infusion (Ado inf) with thoseestimated with adenosine bolus (Ado bo), low-dose dipyridamole (Dip L and 3 min) and high-dose dipyridamole(Dip H). Solid symbols = Group 1; open symbols=Group 2.
same session was compared using transoesophagealDoppler echocardiography. This complex protocol wasdesigned with the aim of identifying which optimalpharmacological approach induced the largest coron-ary vasodilator response easily detectable by trans-oesophageal Doppler echocardiography monitoring,without significant haemodynamic changes and side-effects.
Safety and haemodynamic effects
No important side effects were observed during thestudy. The heart rate increase and systemic pressurereduction observed with adenosine and dipyridamolewere mild and in substantial agreement with datareported in previous studies'18'19'251.
Coronary vasodilator response
The most prominent vasodilator response was observedduring the adenosine infusion; the response to theadenosine bolus was slightly lower. Using a trans-oesophageal approach, a very short hyperaemic effect of
an adenosine bolus (a few cardiac cycles) may representa disadvantage, as the maximal flow response can beeasily missed due to the movement of the heart withrespiration. An adenosine infusion, on the other hand,allows the maximal flow velocity to be measured in arelatively steady state. In all subjects, the maximalresponse was achieved in less than 2 min after the startof the infusion, and afterwards the coronary flow re-mained stable, or pressure dependent, respectively.Thus, coronary flow velocity could be easily, accuratelyand repeatedly measured.
The vasodilator response to low-dose di-pyridamole was lower than the response to the adeno-sine infusion, especially in the patient group, wherelow-dose dipyridamole led to a systematic underestima-tion of the coronary vasodilator response (Fig. 6). Theseresults are in agreement with previous studies: Rosenel al.ll6\ using an invasive intracoronary approach ina heterogeneous population, observed a greater vaso-dilator effect when adenosine was used, as comparedto low-dose dipyridamole, while Chan el a/.[25] usingpositron emission tomography in healthy volunteers,observed comparable effect with both agents. The resultsof our study suggest that the difference between adeno-sine and low-dose dipyridamole infusions is relatively
Eur Heart J. Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
522 M. Kozakova et al.
small in normals but significant in patients with micro-vascular disease or coronary artery disease. The bluntedresponse to low-dose dipyridamole in the patient groupis also evident from the time-course of coronary flowvelocity during the dipyridamole infusion (Fig. 5). Whilein normals the highest velocity was almost achieved withthe low dose, in the majority of patients a furtherincrease in coronary velocity and a decrease in coronaryvascular resistance were observed between the low andhigh dose.
It is not within the aim of this clinical study toestablish the pathophysiological mechanism responsiblefor the blunted response to low-dose dipyridamole inour patients. Whatever the underlying mechanism, thesubmaximal response to low-dose dipyridamole has animportant practical impact as the majority of studiesassessing coronary reserve in a non-invasive way bypositron emission tomography or transoesophagealDoppler echocardiography used low-dose dipyridamoleas a vasodilator stimulus'1-4'9'10-25-261.
To our knowledge, this it the first study compar-ing the coronary vasodilator response to adenosineinfusion with that of high-dose dipyridamole. In termsof coronary resistance, high-dose dipyridamole alsoslightly underestimated the coronary vasodilatorcapacity.
Response of large coronary artery diameter
To assess the coronary flow response to differentpharmacological agents with transoesophageal Dopplerechocardiography, a constant vessel diameter isassumed, so that changes in coronary flow can beconsidered proportional to changes in flow velocity.However, the administration of dipyridamole, adenosineand papaverine was shown to mildly dilate epicardialvessels through flow-mediated dilation'27"291. In ourstudy, a mild increase in coronary cross-sectional areawas observed both with adenosine and dipyridamole (16or 12%). This finding decreases the accuracy of coronaryvasodilator capacity estimation based on the evaluationof the flow velocity response.
The left main artery was chosen because itafforded better two-dimensional image visualizationthan the left anterior descending artery, assuming thatthe two arterial segments respond similarly to vasoactiveagents and flow increase.
Study limitations
The introduction of a transoesophageal probe mayincrease arterial blood pressure and heart rate, leadingto an increase in resting myocardial oxygen demand andbasal coronary flow, thus affecting the value of coronaryreserve'301. For this reason an interval of at least 2 minbetween the introduction of the probe and the first basalmeasurement of flow velocity was adopted in this study.At the time of the first basal flow recording, the valueof the rate-pressure product was equivalent to thatmeasured before the introduction of the probe.
Adenosine and dipyridamole were administeredfollowing a uniform administration sequence: theo-retically, some concern might be raised that the results inthe latter part of the sequence, when dipyridamole wasadministered, could have been influenced by the effectsof the earlier part of the sequence (i.e. adenosine);however, randomization of the order in which thevasodilator agents were administered was not poss-ible due to the long half-life of intravenousdipyridamole'16-24'251. Moreover, the basal conditionsbefore adenosine and dipyridamole were comparable, asdiscussed before.
Clinical significance
In combination with transoesophageal Doppler echo-cardiography, short-lasting (3-5 min) adenosine infu-sions at the rate of 140 ug . kg" ' . min"' appear to bethe most convenient for a quick and easy assessmentof coronary vasodilator capacity. Using an adenosinebolus, the maximal vasodilator effect can easily bemissed, due to a very short effect of the drug.
Adenosine is preferable to dipyridamole; di-pyridamole requires a much longer investigation time,and — especially in a low dose (0-56 mg . kg" ' .4 min ~ ') — it induces a submaximal response mainly inpatients with coronary abnormality. Thus, low-dosedipyridamole may underestimate the maximal coronaryvasodilator capacity, and its long-term effect implies thepossibility of persistent side-effects.
The changes in the diameter of the epi-cardial vessels observed after both adenosine and thedipyridamole infusion result in a mild underestima-tion of coronary flow response when calculated fromcoronary flow velocities only.
We are grateful to Dr Edward Farrants for the revision of themanuscript for English language use.
This study was partially supported by a Grant of the NationalResearch Council (C.N.R.) Targeted Project 'FATMA', Rome,Italy.
References
[1] Radvan J, Marwick TH, Williams MJ, Camici PD. Evaluationof the extent and timing of the coronary hyperemic responseto dipyridamole: a study with transesophageal echocardiogra-phy and positron emission tomography with oxygen 15 water.J Am Soc Echocardiogra 1995; 8: 864-73.
[2] Yamagashi M, Miyatake K., Beppu S et al. Assessment ofcoronary blood flow by transesophageal two-dimensionalechocardiography. Am J Cardiol 1988; 62: 641-5.
[3] Kozakova M. Palombo C, Zanchi M, Distante A, L'AbbateA. Increased sensitivity of flow detection in left coronaryartery by transesophageal echocardiography after intravenousadministration of transpulmonary stable echocontrast agent.J Am Soc Echocardiogr 1994; 7: 327-36.
[4] Iliceto S, Marangelli V, Memmola C, Rizzon P. Trans-esophageal Doppler echocardiography evaluation of coronaryblood flow velocity in baseline conditions and duringdipyridamole-induced coronary vasodilation. Circulation1991; 83: 61-9.
Eur Heart J. Vol. 18. March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021
Assessment of coronary reserve 523
[5] Palombo C, Kozakova M, Vassalle C, Distante A, L'AbbateA. Coronary pressure-flow diagrams during maximal vaso-dilation as assessed by transesophageal Doppler of left cor-onary artery: A new tool for evaluation of absolute coronaryflow reserve (Abstr). J Am Coll Cardiol 1994; 115A.
[6] Kozakova M, Palombo C, Pittella G, Distante A. Trans-esophageal echocardiography in myocardial ischemia- areview. Echocardiography 1995; 12: 479-94.
[7] Kozakova M, Palombo C, Galetta F el al. Coronary vaso-dilator capacity in physiologic and hypertensive left ventricu-lar hypertrophy: a study by transesophageal echo (Abstr). EurHeart J 1995; 16 (Abstr Suppl): 7.
[8] Isaaz K, Bruntz JF, Ethovenot G, Courtalon T, Weber JL,Aliot E. Transesophageal Doppler coronary flow patternsbefore and after coronary angioplasty (Abstr). Eur Heart J1993; 14 (Abstr Suppl): 2453.
[9] Hutchison SJ, Marwah OS, Posley KM, Kawanishi DT,Chandraratna PAN. Coronary flow velocity reserve aftersuccessful balloon angioplasty and directional atherectomy.Echocardiography 1995; 12: 591-603.
[10] Muro T, Yoshida K, Toyama H. Transesophageal Dopplerechocardiographic evaluation of coronary flow reserve beforeand after PTCA (Abstr). Circulation 1992; 86 (Suppl I): 1-726.
[11] Redberg RF, Sobol Y, Chou TM el al. Adenosine-inducedcoronary vasodilation during transesophageal Dopplerechocardiography. Rapid and safe measurement of coronaryflow reserve ratio can predict significant left anterior descend-ing coronary stenosis. Circulation 1995; 92: 190-6
[12] Richards KL, Cannon SR. Physiologic basis for the evalu-ation of valvular function. In: Marcus ML, Schelbert HR,Skorton DJ, Wolf GL, eds. Cardiac Imaging. Philadelphia,London, Toronto, Montreal, Sydney, Tokyo: WB SaundersCompany; 1991: 57-9.
[13] Doucette JW, Corl PD, Payne HM el al. Validation of aDoppler guide wire for intravascular measurement of cor-onary artery flow velocity. Circulation 1992; 85: 1899-911.
[14] Bland MJ, Altman DG. Statistical method for assessingagreement between two methods of clinical assessment. Lancet1986; 8: 307-9.
[15] Kern MJ, Deligonul U, Tatineni S, Serota H, Aguirre F,Hilton TC. Intravenous adenosine: Continuous infusion andlow dose bolus administration for determination of coronaryvasodilator reserve in patients with and without coronaryartery disease. J Am Coll Cardiol 1991; 18: 718-29.
[16] Rosen JD, Quillen JE, Lopez AG, Stenberg RG, Talman CL,Winniford MD. Comparison of coronary vasodilation withintravenous dipyridamole and adenosine. J Am Coll Cardiol1991; 18: 485-91.
[17] Christensen CW, Rosen LB. Gal RA. Haseeb M, Lassar TA.Port SC. Coronary vasodilator reserve. Comparison of theeffect of papaverine and adenosine on coronary flow, ventricu-lar function and myocardial metabolism. Circulation 1991; 83:294-303.
[18] Marzilli M, Klassen G, Marraccini P, Trivella MG, Camici P,L'Abbate A. Effects of exogenous adenosine on human cor-onary circulation. In: Inoue M, Hori M, Imadi S, Berne RM,eds. Regulation of coronary blood flow. Tokyo: SpringerVerlag, 1991: 179-91.
[19] Wilson RF, Wyche K, Christensen BV, Zimmer S, LaxsonDD. Effects of adenosine on human coronary arterial circula-tion. Circulation 1990; 82: 1595-1606.
[20] Hori M, Kitakaze M. Adenosine, the heart and coronarycirculation. Hypertension 1991; 18: 565-74.
[21] Abreu A, Hahmarian JJ, Nishimura S, Bryce TM. Verani MS.Tolerance and safety of pharmacologic coronary vasodilationwith adenosine in association with thallium-201 scintigraphyin patients with suspected coronary artery disease. J Am CollCardiol 1991; 18: 730-5.
[22] Cerqueira MD, Verani MS, Schwaiger M, Heo Y, IskandrianAS. Safety profile of adenosine stress perfusion imaging:results from the adenosine multicenter trial registry. J Am CollCardiol 1994; 23: 384-9.
[23] Fitzgerald GA. Dipyridamole. N Engl J Med 1987; 316:1247-56.
[24] Knabb RM, Gidday JM, Ely SW, Rubio R, Berne RM,Effects of dipyridamole on myocardial adenosine and activehyperemia. Am J Physiol 1984; 247: H804-10.
[25] Chan SY, Brunken RC, Czernin J et al. Comparison ofmaximal myocardial blood flow during adenosine infusionwith that of intravenous dipyridamole in normal men. J AmColl Cardiol 1992; 20: 979-85.
[26] Rosen SD, Uren NG, Kaski JC, Tousoulis D, Davies GJ,Camici PG. Coronary vasodilator reserve, pain perceptionand sex in patients with syndrome X. Circulation 1994; 90:50-60.
[27] Hintze TH, Vatner SF. Dipyridamole dilates large coronaryarteries in conscious dogs. Circulation 1983; 68: 1321-7.
[28] Drexler H, Zeiher AM, Wollschlager H, Meinertzer T, Just H,Bonzel T. Flow-dependent coronary artery dilation inhumans. Circulation 1989; 80: 466-74.
[29] Kuo L, Davis MJ, Chilian WH. Endothelium-dependentflow-induced dilation of isolated coronary arterioles. Am JPhysiol 1990; 259: HI063-70.
[30] Rossen JD, Winniford MD. Effect of increases in heart rateand arterial pressure on coronary flow reserve in humans.J Am Coll Cardiol 1993; 21: 343-8.
Eur Heart J, Vol. 18. March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/514/498023 by guest on 29 D
ecember 2021