assessment of fibrosis in chronic liver diseases
TRANSCRIPT

7
Journal of Digestive Diseases 2009; 10; 7–14 doi: 10.1111/j.1751-2980.2008.00356.x
Blackwell Publishing AsiaMelbourne, AustraliaCDDChinese Journal of Digestive Diseases1443-96111443-9573© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.XXXOriginal ArticleXXXXK. Zhou and LG. Lu
Assessment of fibrosis in chronic liver diseases
Kun ZHOU & Lun Gen LU
Department of Gastroenterology, Renji Hospital, Shanghai Institute of Digestive Disease, Shanghai Jiaotong University School of Medicine, Shanghai 200001, China
The assessment of liver fibrosis provides useful infor-mation not only for diagnosis but also for therapeuticdecisions. Although liver biopsy is the current goldstandard for fibrosis assessment, it has some risksand limitations, including intra-observer and inter-observer variation, sampling error and variability. Inrecent years, many studies and great interest have beendedicated to the development of non-invasive tests tosubstitute a liver biopsy for fibrosis assessment and
follow up. Advances in serological and radiologicaltests such as serum marker panels, transient elasto-graphy and their combinations can assess fibrosisaccurately and reduce the need for a liver biopsy. Butat present, all have failed to completely replace aliver biopsy because of their respective limitationsand an imperfect gold standard used in currentresearches. The searching for an ideal surrogate is stillin progress.
KEY WORDS: liver biopsy, liver fibrosis, non-invasive test, serum marker panel, transient elastography.
INTRODUCTION
Chronic liver diseases (CLD) are very common. Morethan 400 million individuals worldwide are chroni-cally infected with hepatitis B virus (HBV), and morethan 170 million are chronically infected with hepatitisC virus (HCV). Nonalcoholic fatty liver disease alsoattracts more and more attention, paralleling theincreasing prevalence of obesity, diabetes mellitus andthe metabolic syndrome, and alcoholic liver disease(ALD) is prevalent in drinkers. Advanced fibrosis andcirrhosis develop in about 20–40% of patients withCLD, some of whom finally progress to end-stage liverdisease or hepatocellular carcinoma. But the progres-sion may take years or decades. A CLD natural historyis variable and its long-term evolution differs inindividual patients.
Previously, fibrosis was thought to be an irreversibleprocess and received little attention until the 1980s,when it was discovered that hepatic stellate cells (HSC)played an important role during fibrosis. Followingchronic liver injury in CLD, HSC proliferate andactivate under inflammatory milieu, acquiring pro-inflammatory and fibrogenic properties. Activated HSCsynthesize large amounts of extracellular matrix(ECM) constituents. The accumulation of ECM distortsthe hepatic architecture by forming a fibrous scar,and the subsequent development of nodules of regen-erating hepatocytes defines cirrhosis. In the 1990s, itwas demonstrated that liver fibrosis may be reversiblewhen the cause is treated. Since, researchers have beenstimulated to develop therapies for treating hepaticfibrosis. Although successful treatments, such asantiviral therapies for HBV and HCV, seems to modifyfibrosis and prevent progression to cirrhosis andcancer, their response rates are low (especially in HCVgenotype 1 patients) and with frequent side effects andhigh costs. Thus, assessing fibrosis precisely is the maindeterminant in the management of CLD, to decidewhen to begin a treatment and assess treatmentresponse. Up to now we have developed three maintools to assess fibrosis: liver biopsies, serological and
Correspondence to: Lun Gen LU, Department of Gastroenterology, Renji Hospital, Shanghai Institute of Digestive Disease, Shanghai Jiaotong University School of Medicine, Shanghai 200001, China. Email: [email protected]© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.

8 K Zhou and LG Lu Journal of Digestive Diseases 2009; 10; 7–14
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
radiological tests. Unfortunately, they all have limi-tations and pitfalls. To discuss their advantages anddeficiencies will be helpful in scientific research andclinical practice.
INVASIVE MEASUREMENTS
Liver biopsy
The liver biopsy has been considered the gold standardfor confirming a clinical diagnosis, for assessing theseverity of necro-inflammation and fibrosis, foridentifying cofactors and comorbidities, and formonitoring the efficacy of treatment ever since the firstliver biopsy was performed by Paul Ehrlich in 1883.1
The procedure is particularly useful for diagnosing theearly stages of fibrosis and identifying patients at highrisk of progressing to fibrosis, but it has also a numberof limitations. Patient acceptance is somewhat lowbecause a biopsy is expensive, invasive and associatedwith some discomfort and complications. Pain appearsin about one-quarter of patients, and other complicationsinclude bleeding, biliary peritonitis, pneumothoraxand a mortality rate of about 0.01%.2 A sampling errorof at least 24% is reported, usually because of specimenfragmentation or inadequate length. Colloredo et al.concluded that an optimum specimen should be atleast 20 mm in length with 11 complete portal tracts.3
Even with adequate-sized biopsies, the interpretationmight be unreliable, because the distribution ofnecro-inflammation and fibrosis is not homogeneousand a liver biopsy samples only 0.00002 of the mass ofthe liver.
Several semi-quantitative scoring systems have beenproposed to describe and quantify necro-inflammation,steatosis and fibrosis in the liver, particularly forchronic viral hepatitis. These include the Knodellhistological activity index (HAI) first proposed in1981, then modified to the Scheuer system, theMETAVIR system and the Ishak modified HAI.4
However, all these scoring systems could only providequalitative descriptors to stage fibrosis, and the stagingof certain histopathological changes differ in differentsystems (Table 1). This could cause considerable intra-observer and inter-observer variation and difficulty incomparison.
Using computerized digital image analysis, the amountof fibrosis in liver biopsy specimens can be evaluatedby a quantitative score. Though this is thought to beless reliable in determining early stage fibrosis, recentadvances such as a higher resolution digital camera canimprove discrimination between the varying stages ofliver fibrosis, including mild fibrosis. It may be a more
precise method than semi-quantitative histologicalstages for monitoring fibrosis progression or regres-sion during clinical therapeutic trials.5 Consideringthe irregular shape of specimens, fractal and spectraldimension analysis can also be used to improveaccuracy.6
The detection of genes correlated with fibrosis frombiopsy samples has renewed interest in liver biopsies.Changes in liver gene expression can indicate fibrosisprogression precisely at an early stage.7 Genetic studieshave identified possible genetic polymorphisms thatinfluence the progression of liver fibrosis.8 Theidentification of panels of key genes correlating withdifferences in the progression of CLD could lead toestablishing excellent prognostic/diagnostic tools.
Hepatic venous pressure gradient (HVPG)
HVPG, as an expression of intrahepatic resistance,does not exceed 5 mmHg in the absence of significantfibrotic evolution. The measurement of HVPG is avalidated, safe and highly reproducible technique. Itmay be considered a dynamic marker of diseaseprogression in patients with HCV and an end point inantiviral therapy, irrespective of the antiviral response.9
However, the technique is invasive and expensive; itrequires technical expertise and has a low patientacceptance.
SEROLOGICAL TESTS
The limitations of liver biopsy led to the search fornon-invasive tests to assess liver fibrosis. Afdhal andNunes et al.10 suggest the following criteria for an idealmarker of liver fibrosis: it should be liver specific; it
Table 1. Scoring systems for staging fibrosis
Pathologic features Knodell Scheuer METAVIR Ishak
No fibrosis 0 0 0 0Enlargement of some
portal tracts1 1 1 1
Enlargement of most portal tracts
1 1 1 2
Periportal septa 1 2 1 2Occasional portal–
portal septa3 2 2 3
Numerous septa (portal–portal and/or portal–central)
3 3 3 4
Occasional nodules 4 4 4 5Definite cirrhosis 4 4 4 6

Journal of Digestive Diseases 2009; 10; 7–14 Assessment of fibrosis in CLDs 9
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
should not be influenced by alterations in liver, renal,or reticulo-endothelial function; it should measureone or more of the processes related to fibrosis (thestage of fibrosis, the activity of matrix deposition, orthe activity of matrix removal) and should be easy toperform.
Direct serum markers
The key step in the pathophysiology of liver fibrosis isa balance between ECM deposition and removal. Theaccumulation of ECM results from both increasedsynthesis and decreased degradation. The principalECM constituents are synthesized by activated HSC,while they are broken down by a family of enzymesknown as matrix metalloproteinases (MMP). Manystudies have been dedicated to find serum ECM markersfor fibrosis assessment: (i) collagens: N-terminalpeptide of type pro-collagen (PIIINP), type IV collagen7s domain(IV-7S); (ii) proteoglycans: hyaluronic acid;(iii) glycoproteins: laminin, human cartilage glycoprotein39; (iv) collagenases and their inhibitors: MMP, tissueinhibitor of metalloproteinases; and (v) cytokines:transforming growth factor β, platelet-derived growthfactor (PDGF), tumor necrosis factor β.
The clinical applications of such markers appearinnovative and they are useful for assessing the speedof liver fibrogenesis and estimating the response toantiviral therapies or anti-fibrotic drugs. But most ofthem are insensitive in milder fibrosis, and it must bestressed that these markers reflect fibrogenesis andfibrolysis more than fibrosis itself. In other words,there may be a highly active fibrotic process in the liver,although fibrotic tissue has not yet been developed, orthere may be heavy fibrosis in the liver but fibroticactivity is temporarily discontinued.
Serum marker panels
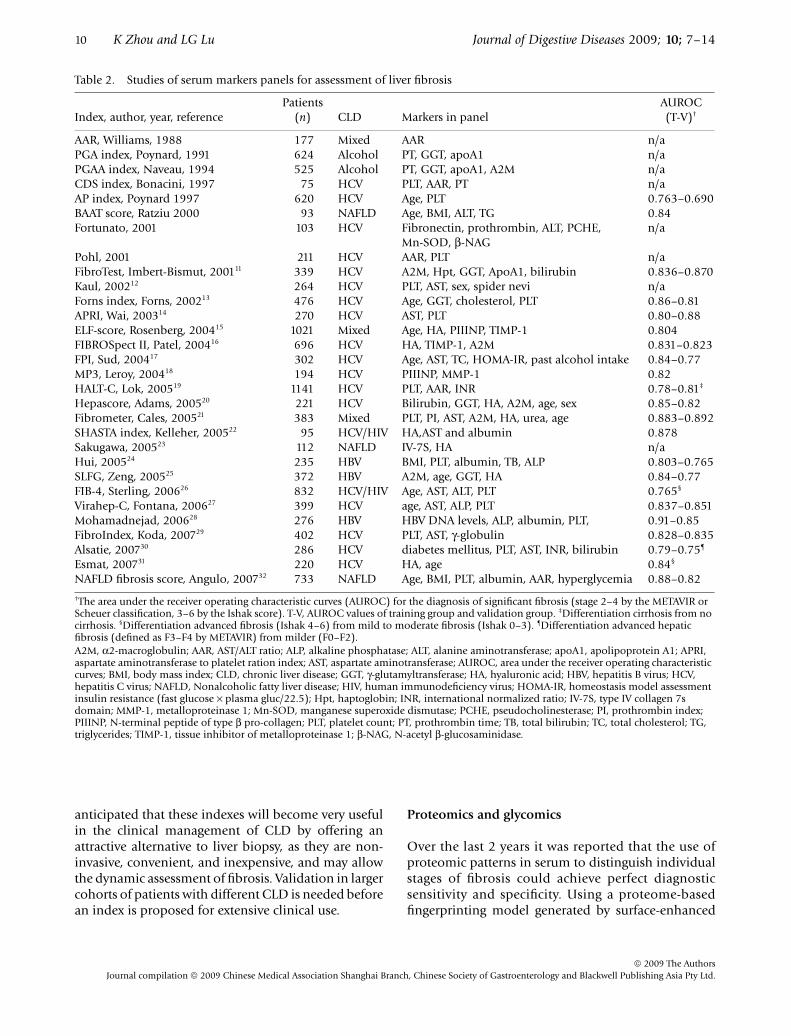
Since present direct markers cannot satisfy yet theclinical need of measuring the fibrosis, an alternativeapproach turn out to be combining a number of serummarkers to generate algorithms capable of evaluatingfibrosis. A large number of panels have been studied bygroups worldwide11–32 (Table 2).
These panels are mainly based on two kinds ofmarkers, direct and indirect. Direct markers are thosedirectly linked to the modifications in ECM metabo-lism, such as hyaluronic acid and PIIINP. Indirectmarkers include a broad range of blood tests whichhave no direct link with liver fibrosis. They reflect liverdysfunction or other phenomena caused by fibrosisrather than fibrosis per se. Generally speaking, indexes
including direct markers, such as the Fibrometer, mayperform with greater accuracy, but indexes composedby only indirect markers are effective as well, and areusually more useful because they are based on routineblood tests that are easy to be performed in a generallaboratory.
The diagnostic value of the models was assessed bycalculating the area under the receiver operatingcharacteristic curves (AUROC). Most studies reportedan AUROC > 0.80 in differentiating significant fibrosis(fibrosis spread out the portal tract with septa) fromno/mild fibrosis (no fibrosis or portal fibrosis withoutsepta). Improved performance with a higher AUROCvalue was shown in differentiating between no cirrhosisand cirrhosis. But it must be underlined that theAUROC values in Table 2 each came from differentlydesigned studies and are not suitable for making acomparison. Some well designed validation studieswere done in the last 2 years, which may give us morereliable results.33,34
There are still some limitations of these marker panelsto be considered. First, the design of every study differedin population characteristics, patient selection, significantfibrosis prevalence, blood test inclusion, biochemicalmeasurement and liver histological assessment, whichresulted in various panels with different markers andparameters. The agreement among these indexes ispoor and a validation study is needed to choose aproper panel and cut-off value for clinical use. Second,none of the studies controlled for the degree ofnecro-inflammatory activity, most of the panelsinclude markers likely to reflect or be affected byinflammation in the liver, which is much more mobilethan fibrosis stage. Third, the formulas can easily failbecause many markers included will be influenced byextrahepatic diseases or conditions such as inflamma-tion, hemolysis, cholestasis, hypercholesterolaemiaand renal failure. Finally, few of the studies includetreated patients. It is not clear whether these indexesare suitable for assessing treatment response. However,a few studies by Poynard et al. suggested that FibroTest(BioLiveScale, Angers, France) could also be used assurrogate markers of the histological impact of treatmentsin patients infected by HCV and HBV.35
These indexes, in their current form, are not able togive us the exact stage of fibrosis in most studies. Theirmain value is to reduce the need for a liver biopsy bydistinguishing significant fibrosis from no/mild fibrosis,and showing the presence of cirrhosis. It does not seemappropriate to completely replace liver biopsy withserum marker panels at the present time, but it can be
10 K Zhou and LG Lu Journal of Digestive Diseases 2009; 10; 7–14
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
anticipated that these indexes will become very usefulin the clinical management of CLD by offering anattractive alternative to liver biopsy, as they are non-invasive, convenient, and inexpensive, and may allowthe dynamic assessment of fibrosis. Validation in largercohorts of patients with different CLD is needed beforean index is proposed for extensive clinical use.
Proteomics and glycomics
Over the last 2 years it was reported that the use ofproteomic patterns in serum to distinguish individualstages of fibrosis could achieve perfect diagnosticsensitivity and specificity. Using a proteome-basedfingerprinting model generated by surface-enhanced
Table 2. Studies of serum markers panels for assessment of liver fibrosis
Index, author, year, referencePatients
(n) CLD Markers in panelAUROC (T-V)†
AAR, Williams, 1988 177 Mixed AAR n/aPGA index, Poynard, 1991 624 Alcohol PT, GGT, apoA1 n/aPGAA index, Naveau, 1994 525 Alcohol PT, GGT, apoA1, A2M n/aCDS index, Bonacini, 1997 75 HCV PLT, AAR, PT n/aAP index, Poynard 1997 620 HCV Age, PLT 0.763–0.690BAAT score, Ratziu 2000 93 NAFLD Age, BMI, ALT, TG 0.84Fortunato, 2001 103 HCV Fibronectin, prothrombin, ALT, PCHE,
Mn-SOD, β-NAGn/a
Pohl, 2001 211 HCV AAR, PLT n/aFibroTest, Imbert-Bismut, 200111 339 HCV A2M, Hpt, GGT, ApoA1, bilirubin 0.836–0.870Kaul, 200212 264 HCV PLT, AST, sex, spider nevi n/aForns index, Forns, 200213 476 HCV Age, GGT, cholesterol, PLT 0.86–0.81APRI, Wai, 200314 270 HCV AST, PLT 0.80–0.88ELF-score, Rosenberg, 200415 1021 Mixed Age, HA, PIIINP, TIMP-1 0.804FIBROSpect II, Patel, 200416 696 HCV HA, TIMP-1, A2M 0.831–0.823FPI, Sud, 200417 302 HCV Age, AST, TC, HOMA-IR, past alcohol intake 0.84–0.77MP3, Leroy, 200418 194 HCV PIIINP, MMP-1 0.82HALT-C, Lok, 200519 1141 HCV PLT, AAR, INR 0.78–0.81‡
Hepascore, Adams, 200520 221 HCV Bilirubin, GGT, HA, A2M, age, sex 0.85–0.82Fibrometer, Cales, 200521 383 Mixed PLT, PI, AST, A2M, HA, urea, age 0.883–0.892SHASTA index, Kelleher, 200522 95 HCV/HIV HA,AST and albumin 0.878Sakugawa, 200523 112 NAFLD IV-7S, HA n/aHui, 200524 235 HBV BMI, PLT, albumin, TB, ALP 0.803–0.765SLFG, Zeng, 200525 372 HBV A2M, age, GGT, HA 0.84–0.77FIB-4, Sterling, 200626 832 HCV/HIV Age, AST, ALT, PLT 0.765§
Virahep-C, Fontana, 200627 399 HCV age, AST, ALP, PLT 0.837–0.851Mohamadnejad, 200628 276 HBV HBV DNA levels, ALP, albumin, PLT, 0.91–0.85FibroIndex, Koda, 200729 402 HCV PLT, AST, γ-globulin 0.828–0.835Alsatie, 200730 286 HCV diabetes mellitus, PLT, AST, INR, bilirubin 0.79–0.75¶
Esmat, 200731 220 HCV HA, age 0.84§
NAFLD fibrosis score, Angulo, 200732 733 NAFLD Age, BMI, PLT, albumin, AAR, hyperglycemia 0.88–0.82
†The area under the receiver operating characteristic curves (AUROC) for the diagnosis of significant fibrosis (stage 2–4 by the METAVIR or Scheuer classification, 3–6 by the Ishak score). T-V, AUROC values of training group and validation group. ‡Differentiation cirrhosis from no cirrhosis. §Differentiation advanced fibrosis (Ishak 4–6) from mild to moderate fibrosis (Ishak 0–3). ¶Differentiation advanced hepatic fibrosis (defined as F3–F4 by METAVIR) from milder (F0–F2). A2M, α2-macroglobulin; AAR, AST/ALT ratio; ALP, alkaline phosphatase; ALT, alanine aminotransferase; apoA1, apolipoprotein A1; APRI, aspartate aminotransferase to platelet ration index; AST, aspartate aminotransferase; AUROC, area under the receiver operating characteristic curves; BMI, body mass index; CLD, chronic liver disease; GGT, γ-glutamyltransferase; HA, hyaluronic acid; HBV, hepatitis B virus; HCV, hepatitis C virus; NAFLD, Nonalcoholic fatty liver disease; HIV, human immunodeficiency virus; HOMA-IR, homeostasis model assessment insulin resistance (fast glucose × plasma gluc/22.5); Hpt, haptoglobin; INR, international normalized ratio; IV-7S, type IV collagen 7s domain; MMP-1, metalloproteinase 1; Mn-SOD, manganese superoxide dismutase; PCHE, pseudocholinesterase; PI, prothrombin index; PIIINP, N-terminal peptide of type β pro-collagen; PLT, platelet count; PT, prothrombin time; TB, total bilirubin; TC, total cholesterol; TG, triglycerides; TIMP-1, tissue inhibitor of metalloproteinase 1; β-NAG, N-acetyl β-glucosaminidase.

Journal of Digestive Diseases 2009; 10; 7–14 Assessment of fibrosis in CLDs 11
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
laser desorption/ionization time-of-flight (SELDI-TOF)ProteinChip (Ciphergen Biosystems, California, USA)arrays, Poon et al.36 achieved an AUROC of 0.93 inidentifying significant fibrosis. Another proteomicindex combining eight peaks established by Morra et al.37
could diagnosis advanced fibrosis with an AUROC of0.88, significantly greater than the FibroTest AUROCof 0.81. Besides, The SELDI-TOF ProteinChip technologyis useful for the early detection and prediction of HCCin patients with chronic HCV infection. Similar technolo-gies have also been used to generate profiles of serumN-glycan profile for identifying liver fibrosis.38
Further studies identifying the altered peaks in thesemodels to understand their origins may help to findnew biomarks for fibrosis, or even improve our under-standing in the mechanism of liver fibrosis.
RADIOLOGICAL TESTS
Since significant structural changes are present only inadvanced CLD, routine examinations by ultrasound(US), computed tomography and magnetic resonanceimaging (MRI) could produce specific findings, butwith very limited sensitivity. Thus, persistent effortshave been made to search for technological developments.
Perfusion examinations
MR and Doppler US techniques are being studied tofind sensitive perfusion changes in the progression offibrosis. For example, the circulatory changes willresult in a decrease of hepatic vein transit time (HVTT),which can be measured by microbubble-enhanced US.Using HVTT measurements, Lim et al. achieved 100%sensitivity and 80% specificity for diagnosis of cirrhosis,and 95% sensitivity and 86% specificity for the differen-tiation of mild hepatitis from more severe liver disease.39
Recent studies of hepatic microcirculation discoveredthat there is a progressive arterialization of the hepaticparenchyma during the progression of fibrosis,especially in the peripheral areas of the liver. The‘central–peripheral phenomenon’ belonging to thetransient hepatic arterial differences (THAD)40 can bedetected in patients with advanced fibrosis or cirrhosisby computed tomography, which is a reliable qualitativemeasurement of liver perfusion changes. However,these techniques are not strong enough to distinguishprecisely between different stages of fibrosis.
Liver stiffness measurement
Recently, an important technological advance infibrosis assessment was made by the FibroScan (Echosens,Paris, France), a new medical device based on one-dimensional transient elastography, which assesses
fibrosis through liver stiffness measurement (LSM). Aspecial probe generates an elastic shear wave propagatingthrough the liver tissue: the harder the tissue, the fasterthe shear wave propagates. Transient elastography couldaccurately predict different stages of fibrosis or cirrhosis(AUROC: 0.79 for F ≥ 2, 0.91 for F ≥ 3, and 0.97 forF = 4. by the METAVIR scoring system).41
The major advantage of transient elastography com-pared with serum markers and marker panels is that itmeasures the liver directly and there is no interferencefrom extrahepatic diseases or conditions. Furthermore,the test is standardized and completely non-invasive.Though assessing earlier fibrosis is the common short-coming of various non-invasive tests, Colletta et al.42
reported that the agreement between transient elasto-graphy and a liver biopsy was much better than a Fibro-Test in normal transaminase HCV carriers with earlystages of fibrosis.
Compared to a liver biopsy, transient elastography ispainless, and rapid: it has no risk of complications andis, therefore, very well accepted. Transient elastographymeasures a volume of liver stiffness which is 100 timesbigger than the biopsy specimen. The high reproduci-bility (the intra-observer and inter-observer agreementintra-class correlation coefficient was 0.9843) andacceptance of transient elastography makes it anattractive alternative to biopsy for individual follow-up.
There are also some physical limitations of transientelastography. The signal penetrates only 25–65 mm,making obesity (particularly the fatness of the chestwall) the most important cause of failure. But newtechnological developments may overcome thislimitation. Additional limitations include a narrowintercostal space and ascites. However, the presence ofascites generally indicates cirrhosis by itself. Steatosiscould have been expected to soften the liver because ofthe fat. Though current studies did not report thatsteatosis and necro-inflammation influence LSM,41
Fraquelli et al. found that transient elastographyreproducibility is significantly reduced in patients withsteatosis, an increased body mass index and lowerdegrees of hepatic fibrosis.43 So, larger cohorts withmore severe grades of steatosis need to be studiedbefore we make a conclusion.
The main reason that transient elastography cannottotally replace a liver biopsy is that it is only a meansto stage disease. It is unable to diagnose liver disease bydistinguishing between subtle diagnostic differences.Nor can transient elastography identify cofactors andcomorbidities or grade necro-inflammation and

12 K Zhou and LG Lu Journal of Digestive Diseases 2009; 10; 7–14
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
steatosis. But it represents a totally different approachto assessing fibrosis and therefore could be combinedwith other non-invasive modalities to better assessliver fibrosis. The combined use of transient elastographyand the FibroTest to evaluate liver fibrosis could avoida biopsy procedure in most patients with chronichepatitis C.44 Recently, Foucher et al. suggested thattransient elastography might also be useful for predictingclinical complications of end-stage liver diseases suchas esophageal varices and hepatocellular carcinomas,45
indicating the potential usefulness of transient elasto-graphy in the management of cirrhosis patients.
Real-time elastography
Real-time elastography is another ultrasound techniquedeveloped by Hitachi Medical Systems that can revealthe physical property of tissue using conventionalultrasound probes during a routine sonographyexamination. In the first study assessing real-timeelastography for the detection of liver fibrosis,46 theAUROC was 0.75 for the diagnosis of significant fibrosis.Much higher diagnostic accuracy (AUROC = 0.93) wasobtained by a mathematic combination of the elasticityscore and two routine laboratory values (platelet countand γ-glutamyltransferase), which provided a superiorway to combine serological and radiological teststogether.
Magnetic resonance elastography
Magnetic resonance elastography (MRE) is a techniqueusing a modified phase-contrast MRI sequence toimage propagating shear waves in tissue. The tech-nique has been previously applied to quantitativelyassess the viscoelastic properties of the breast, brainand muscle in humans. Several recent studies showedthat MRE is also a feasible method for assessing thestage of liver fibrosis.47 MRE has several potentialadvantages compared with ultrasound transientelastography. It can be performed in obese patients. Itcan assess larger volumes and provide full three-dimensional information about the viscoelastic parametersof tissues. With MR techniques a comprehensive exam-ination of the liver can be performed, including MRE,contrast-enhanced MRI to detect hepatocellularcarcinomas and perfusion MRI to assess liver function.However, direct comparison of the two methods is stillnot available. More studies are needed to define thesensitivity and specificity of this new technique.
Double contrast material-enhanced MRI
The conspicuity of gadolinium-enhanced lesions isincreased in the setting of a decreased signal intensity
from an uninvolved liver parenchyma following asuperparamagnetic iron oxide injection. This MRItechnique has been used to improve detection of focalhepatic lesions and hepatocellular carcinomas.Recently, Aguirre et al.48 examined 101 CLD patientswho underwent double-enhanced MR imaging todetect hyperintense reticulations, which are postulatedto represent septal fibrosis. They achieved an accuracyof greater than 90% for the diagnosis of fibrosiscompared with histopathological analysis.
Diffusion weighted magnetic resonance imaging
Diffusion weighted magnetic resonance imaging(DWMRI) has been widely used in brain imaging forthe evaluation of acute ischemic stroke. With theadvent of the echo-planar MRI technique, it becamepossible to be applied in the abdomen for the charac-terization of focal hepatic lesions. Recently, usingDWMRI to measure the apparent diffusion coefficient(ADC) of water, a parameter that is dependent on thetissue structure, has been introduced in the assessmentof liver fibrosis. The ADC value is lower in livers withheavier fibrosis because of the restriction of waterdiffusion in fibrotic tissue. Lewin et al. assessed theperformance of DWMRI in 54 patients with chronic HCVinfection with reference to several other non-invasivemethods.49 In discriminating significant fibrosis, thearea under the curve (AUC) values were 0.79 forDWMRI, 0.87 for transient elastography, 0.68 for theFibroTest, 0.81 for aspartate aminotransferase toplatelet ration index, 0.72 for the Forns index and 0.77for hyaluronate. DWMRI performed better in discrim-inating between patients staged F3–F4, when the AUCvalue increased to 0.92, the same as in transientelastography. But besides fibrosis, it seems that ADCvalues might also reflect the intensity of inflammation,necrosis and steatosis. However, DWMRI still benefitsfrom the intrinsic advantages of MRI. Several other MRtechniques have also been introduced in the area offibrosis assessment, such as ultra-short echo timeMRI50 and magnetic resonance spectroscopy,51 but theresearch data are still insufficient.
CONCLUSION
The increase of potentially effective management forCLD such as antiviral and antifibrotic therapies has ledto an urgent need for a rapid, safe and repeatable toolto assess fibrosis of CLD and to follow up progressionor regression of fibrosis during treatment. A liverbiopsy has been the gold standard for the assessmentof hepatic fibrosis, but the invasive procedure hasconsiderable limitations and fails to satisfy current

Journal of Digestive Diseases 2009; 10; 7–14 Assessment of fibrosis in CLDs 13
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
needs. Many non-invasive methods have been pro-posed with the aim of substituting for a liver biopsy.The numerous advances in serological and radiologicaltechniques and their combinations have allowedclinicians to satisfactorily identify patients withoutresorting to a liver biopsy. But each has some deficien-cies and a liver biopsy will still have an important roleto play. Applying new techniques for the detection offibrosis may potentially circumvent the pitfalls anddeficiencies of existing surrogates mentioned above.However, further studies are needed to develop orvalidate non-invasive tests that can accurately reflectthe full spectrum of hepatic fibrosis in CLD. But anincorrigible defect in our studies will be the question-able gold standard we have to use. Biopsy failure ismore common than diagnostic failure of markers.52
Mathematical modeling suggests that, assuming either80% or 90% diagnostic accuracy of a liver biopsy,non-invasive tests cannot achieve an AUROC betterthan 0.9 and are likely to perform between 0.75 and0.9, exactly where they are today. We may find a bettersurrogate for a liver biopsy, but how we can prove itwill be a challenge. A laparoscopic biopsy can decreasesampling error and increase the reliability of a his-topathological assessment. Using automated imageanalysis to assess texture features and the shaperepresentation of the fibrosis structural expansion canturn the current semiquantitative methods of liver fibrosisassessment into real quantitative methods withsignificant reduction in variability and subjectivity.53
Validating non-invasive tests against not only histologicalstage scores but also digital image analysis and clinicaloutcomes may also be a better choice.
FINANCIAL SUPPORT
This study was supported by the Prominent NationalProjects of Science & Technology (No: 2008ZX10203), theNational High Technology Research and DevelopmentProgram of China (863 Program, No: 2006AA02A411),Science and Technology Commission of ShanghaiMunicipality (No: 064119519), and Shanghai LeadingAcademic Discipline Project (No: Y0205).
REFERENCES
1 Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med 2001; 344: 495–500.
2 McGill DB, Rakela J, Zinsmeister AR, Ott BJ. A 21-year experience with major hemorrhage after percutaneous liver biopsy. Gastroenterology 1990; 99: 1396–400.
3 Colloredo G, Guido M, Sonzogni A, Leandro G. Impact of liver biopsy size on histological evaluation of chronic viral hepatitis: the smaller the sample, the milder the disease. J Hepatol 2003; 39: 239–44.
4 Brunt EM. Grading and staging the histopathological lesions
of chronic hepatitis: the Knodell histology activity index and beyond. Hepatology 2000; 31: 241–6.
5 Goodman ZD, Becker RL Jr, Pockros PJ, Afdhal NH. Progression of fibrosis in advanced chronic hepatitis C: evaluation by morphometric image analysis. Hepatology 2007; 45: 886–94.
6 Dioguardi N, Franceschini B, Aletti G, Russo C, Grizzi F. Fractal dimension rectified meter for quantification of liver fibrosis and other irregular microscopic objects. Anal Quant Cytol Histol 2003; 25: 312–20.
7 Asselah T, Bieche I, Laurendeau I et al. Liver gene expression signature of mild fibrosis in patients with chronic hepatitis C. Gastroenterology 2005; 129: 2064–75.
8 Bataller R, North KE, Brenner DA. Genetic polymorphisms and the progression of liver fibrosis: a critical appraisal. Hepatology 2003; 37: 493–503.
9 Burroughs AK, Groszmann R, Bosch J et al. Assessment of therapeutic benefit of antiviral therapy in chronic hepatitis C: is hepatic venous pressure gradient a better end point? Gut 2002; 50: 425–7.
10 Afdhal NH, Nunes D. Evaluation of liver fibrosis: a concise review. Am J Gastroenterol 2004; 99: 1160–74.
11 Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y, Poynard T. Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: a prospective study. Lancet 2001; 357: 1069–75.
12 Kaul V, Friedenberg FK, Braitman LE et al. Development and validation of a model to diagnose cirrhosis in patients with hepatitis C. Am J Gastroenterol 2002; 97: 2623–8.
13 Forns X, Ampurdanes S, Llovet JM et al. Identification of chronic hepatitis C patients without hepatic fibrosis by a simple predictive model. Hepatology 2002; 36: 986–92.
14 Wai CT, Greenson JK, Fontana RJ et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–26.
15 Rosenberg WM, Voelker M, Thiel R et al. Serum markers detect the presence of liver fibrosis: a cohort study. Gastroenterology 2004; 127: 1704–13.
16 Patel K, Gordon SC, Jacobson I et al. Evaluation of a panel of non-invasive serum markers to differentiate mild from moderate-to-advanced liver fibrosis in chronic hepatitis C patients. J Hepatol 2004; 41: 935–42.
17 Sud A, Hui JM, Farrell GC et al. Improved prediction of fibrosis in chronic hepatitis C using measures of insulin resistance in a probability index. Hepatology 2004; 39: 1239–47.
18 Leroy V, Monier F, Bottari S et al. Circulating matrix metalloproteinases 1, 2, 9 and their inhibitors TIMP-1 and TIMP-2 as serum markers of liver fibrosis in patients with chronic hepatitis C: comparison with PIIINP and hyaluronic acid. Am J Gastroenterol 2004; 99: 271–9.
19 Lok AS, Ghany MG, Goodman ZD et al. Predicting cirrhosis in patients with hepatitis C based on standard laboratory tests: results of the HALT-C cohort. Hepatology 2005; 42: 282–92.
20 Adams LA, Bulsara M, Rossi E et al. Hepascore: an accurate validated predictor of liver fibrosis in chronic hepatitis C infection. Clin Chem 2005; 51: 1867–73.
21 Cales P, Oberti F, Michalak S et al. A novel panel of blood markers to assess the degree of liver fibrosis. Hepatology 2005; 42: 1373–81.
22 Kelleher TB, Mehta SH, Bhaskar R et al. Prediction of hepatic fibrosis in HIV/HCV co-infected patients using serum fibrosis markers: the SHASTA index. J Hepatol 2005; 43: 78–84.
23 Sakugawa H, Nakayoshi T, Kobashigawa K et al. Clinical usefulness of biochemical markers of liver fibrosis in patients with nonalcoholic fatty liver disease. World J Gastroenterol 2005; 11: 255–9.
24 Hui AY, Chan HL, Wong VW et al. Identification of chronic hepatitis B patients without significant liver fibrosis by

14 K Zhou and LG Lu Journal of Digestive Diseases 2009; 10; 7–14
© 2009 The AuthorsJournal compilation © 2009 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
a simple noninvasive predictive model. Am J Gastroenterol 2005; 100: 616–23.
25 Zeng MD, Lu LG, Mao YM et al. Prediction of significant fibrosis in HBeAg-positive patients with chronic hepatitis B by a noninvasive model. Hepatology 2005; 42: 1437–45.
26 Sterling RK, Lissen E, Clumeck N et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006; 43: 1317–25.
27 Fontana RJ, Kleiner DE, Bilonick R et al. Modeling hepatic fibrosis in African American and Caucasian American patients with chronic hepatitis C virus infection. Hepatology 2006; 44: 925–35.
28 Mohamadnejad M, Montazeri G, Fazlollahi A et al. Noninvasive markers of liver fibrosis and inflammation in chronic hepatitis B-virus related liver disease. Am J Gastroenterol 2006; 101: 2537–45.
29 Koda M, Matunaga Y, Kawakami M, Kishimoto Y, Suou T, Murawaki Y. FibroIndex, a practical index for predicting significant fibrosis in patients with chronic hepatitis C. Hepatology 2007; 45: 297–306.
30 Alsatie M, Kwo PY, Gingerich JR et al. A multivariable model of clinical variables predicts advanced fibrosis in chronic hepatitis C. J Clin Gastroenterol 2007; 41: 416–21.
31 Esmat G, Metwally M, Zalata KR et al. Evaluation of serum biomarkers of fibrosis and injury in Egyptian patients with chronic hepatitis C. J Hepatol 2007; 46: 620–7.
32 Angulo P, Hui JM, Marchesini G et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007; 45: 846–54.
33 Bourliere M, Penaranda G, Renou C et al. Validation and comparison of indexes for fibrosis and cirrhosis prediction in chronic hepatitis C patients: proposal for a pragmatic approach classification without liver biopsies. J Viral Hepat 2006; 13: 659–70.
34 Leroy V, Hilleret MN, Sturm N et al. Prospective comparison of six non-invasive scores for the diagnosis of liver fibrosis in chronic hepatitis C. J Hepatol 2007; 46: 775–82.
35 Poynard T, Zoulim F, Ratziu V et al. Longitudinal assessment of histology surrogate markers (FibroTest-ActiTest) during lamivudine therapy in patients with chronic hepatitis B infection. Am J Gastroenterol 2005; 100: 1970–80.
36 Poon TC, Hui AY, Chan HL et al. Prediction of liver fibrosis and cirrhosis in chronic hepatitis B infection by serum proteomic fingerprinting: a pilot study. Clin Chem 2005; 51: 328–35.
37 Morra R, Munteanu M, Bedossa P et al. Diagnostic value of serum protein profiling by SELDI-TOF ProteinChip compared with a biochemical marker, FibroTest, for the diagnosis of advanced fibrosis in patients with chronic hepatitis C. Aliment Pharmacol Ther 2007; 26: 847–58.
38 Kam RK, Poon TC, Chan HL, Wong N, Hui AY, Sung JJ. High-throughput quantitative profiling of serum N-glycome
by MALDI-TOF mass spectrometry and N-glycomic fingerprint of liver fibrosis. Clin Chem 2007; 53: 1254–63.
39 Lim AK, Taylor-Robinson SD, Patel N et al. Hepatic vein transit times using a microbubble agent can predict disease severity non-invasively in patients with hepatitis C. Gut 2005; 54: 128–33.
40 Colagrande S, Centi N, La Villa G, Villari N. Transient hepatic attenuation differences. AJR Am J Roentgenol 2004; 183: 459–64.
41 Ziol M, Handra-Luca A, Kettaneh A et al. Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology 2005; 41: 48–54.
42 Colletta C, Smirne C, Fabris C et al. Value of two noninvasive methods to detect progression of fibrosis among HCV carriers with normal aminotransferases. Hepatology 2005; 42: 838–45.
43 Fraquelli M, Rigamonti C, Casazza G et al. Reproducibility of transient elastography in the evaluation of liver fibrosis in patients with chronic liver disease. Gut 2007; 56: 968–73.
44 Castera L, Vergniol J, Foucher J et al. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005; 128: 343–50.
45 Foucher J, Chanteloup E, Vergniol J et al. Diagnosis of cirrhosis by transient elastography (FibroScan): a prospective study. Gut 2006; 55: 403–8.
46 Friedrich-Rust M, Ong MF, Herrmann E et al. Real-time elastography for noninvasive assessment of liver fibrosis in chronic viral hepatitis. AJR Am J Roentgenol 2007; 188: 758–64.
47 Yin M, Talwalkar JA, Glaser KJ et al. Assessment of hepatic fibrosis with magnetic resonance elastography. Clin Gastroenterol Hepatol 2007; 5: 1207–13 e2.
48 Aguirre DA, Behling CA, Alpert E, Hassanein TI, Sirlin CB. Liver fibrosis: noninvasive diagnosis with double contrast material-enhanced MR imaging. Radiology 2006; 239: 425–37.
49 Lewin M, Poujol-Robert A, Boelle PY et al. Diffusion-weighted magnetic resonance imaging for the assessment of fibrosis in chronic hepatitis C. Hepatology 2007; 46: 658–65.
50 Chappell KE, Patel N, Gatehouse PD et al. Magnetic resonance imaging of the liver with ultrashort TE (UTE) pulse sequences. J Magn Reson Imaging 2003; 18: 709–13.
51 Lim AK, Patel N, Hamilton G, Hajnal JV, Goldin RD, Taylor-Robinson SD. The relationship of in vivo 31P MR spectroscopy to histology in chronic hepatitis C. Hepatology 2003; 37: 788–94.
52 Poynard T, Munteanu M, Imbert-Bismut F et al. Prospective analysis of discordant results between biochemical markers and biopsy in patients with chronic hepatitis C. Clin Chem 2004; 50: 1344–55.
53 Matalka II, Al-Jarrah OM, Manasrah TM. Quantitative assessment of liver fibrosis: a novel automated image analysis method. Liver Int 2006; 26: 1054–64.