assessment of medical equipment maintenance management
TRANSCRIPT

Assessment of medical equipment maintenance management: proposed checklist using Iranian experienceMorteza Arab‑Zozani1, Ali Imani2, Leila Doshmangir3, Koustuv Dalal4,5 and Rona Bahreini6*
Abstract
Background: Effective maintenance management of medical equipment is one of the major issues for quality of care, for providing cost‑effective health services and for saving scarce resources. This study aimed to develop a comprehensive checklist for assessing the medical equipment maintenance management (MEMM) in the Iranian hospitals.
Methods: This is a multi‑methods study. First, data related to factors which affect the assessment of MEMM were collected through a systematic review in PubMed, Pro‑Quest, Scopus, Embase, and web of science without any time limitation until October 2015, updated in June 2017. Then, we investigated these factors affecting using docu‑ment review and interviews with experts in the Iranian hospitals. In the end, the results of the first and second stages were combined using content analysis and the final checklist was developed in a two‑round Delphi.
Results: Using a combination of factors extracted from the systematic and qualita‑tive studies, the primary checklist was developed in the form of assessment checklists in seven dimensions. The final checklist includes 7 dimensions and 19 sub‑categories: “resources = 3,” “quality control = 3,” “information bank = 4,” “education = 1,” “service = 3,” “inspection and preventive maintenance = 2” and “design and implementation = 3.”
Conclusions: Developing an assessment checklist for MEMM provide a comprehen‑sive framework for the proper implementation of accurate assessment of medical equipment maintenance. This checklist can be used to improve the profitability of health facilities and the reliability of medical equipment. In addition, it is implicated in the decision‑making in support of selection, purchase, repair and maintenance of medical equipment, especially for capital equipment managers and medical engineers in hospitals and also for the assessment of this process.
Keywords: Hospital, Medical equipment, Medical devices, Maintenance management, Assessment
Open Access
© The Author(s) 2021. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
RESEARCH
Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49 https://doi.org/10.1186/s12938‑021‑00885‑5 BioMedical Engineering
OnLine
*Correspondence: [email protected] 6 Tabriz Health Services Management Research Center, Iranian Center of Excellence in Health Management, Student Research Committee, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, IranFull list of author information is available at the end of the article

Page 2 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
BackgroundToday’s modern hospital is highly dependent on various types of medical equipment to assist in the diagnosis, monitoring and treatment of patients. It is impractical to provide health services without them [1, 2]. Medical equipment deals with patient care including ranging from small and simple devices to complex and big devices. This ranking can be found in different types of hospitals and primary care settings [3]. According to the stud-ies conducted in Iran, about one-third of the costs of setting up and equipping the hospi-tal is allocated for purchasing medical equipment [4]. Therefore, it should be maintained in good working condition and higher safety level to prevent from injuries occurred in patients as well as in users [5].
The maintenance of medical equipment is important for reducing dispatch costs, reducing patient dissatisfaction, timely patient treatment, and reducing mortality and risks during patients care [4]. It is an integral part of the life cycle of the device. Usually, much more money is spent on maintaining equipment over than on its procurement [6]. Maintenance is defined as any action which helps hospitals to provide an adequate level of service and to protect or promote the performance of their equipment to operate regularly and efficiently. Therefore, maintenance management is a fundamental aspect of hospital management [7].
Good maintenance management to have well planned and implemented programs that hospitals can minimize breakdowns or failures of the medical device. This is par-ticularly critical in developing countries for providing good healthcare services and sav-ing scarce resources and alternatives. The equipment maintenance management of the hospital not only makes them easily accessible when needed but also increases their reli-ability and reduces their failure rate [4, 8]. Despite the importance of maintenance, there was no clear system of maintenance. The guidelines are not properly performed in many countries including Iran. In addition, there is a lack of information about the assessment and evaluation of medical equipment decisions [9].
A survey indicated that nearly 60% of the total cost of a hospital involves medical equipment [8]. Wang et al. have demonstrated that the most common cause of medical equipment downtime is poor maintenance, planning, and management [3]. One study indicates that nearly 1% of the total hospital budget is spent on maintenance costs [10]. The literatures have indicated that a 500-bed hospital spends typically around $5 mil-lion/year [6]. A study of world health organization (WHO) has shown that nearly half of medical devices in developing countries are operated incorrectly or are not maintained properly due to inappropriate management policy. On the other hand, the potential to manage and maintain medical equipment in these countries remains rather weak [11].
Medical equipment plays a significant role in the hospital system; hence, the pur-chase, maintenance and replacement of medical equipment are key factors in hospitals to implement medical care service. Thus, to assure the quality of healthcare delivery medical devices, use-safety assessment of the maintenance management in hospitals is imperative [12]. To achieve these objectives, hospitals must develop assessment check-lists which identify the performance status of medical equipment maintenance. It is essential for managers and engineers, not only to enhance hospital capability but also to predict the risks related to sudden failure. Given the lack of single and comprehensive checklists for maintenance management, the purpose of the current research is to design

Page 3 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
and develop assessment checklists for medical equipment maintenance management (MEMM).
ResultsOf 309 potentially relevant articles searched, 29 articles were included in this systematic review. Finally, 89 factors were identified that affect the medical equipment maintenance management. These factors categorized based on MOHME framework [13]. Five of the factors were found related to resources, 12 factors related to service, 4 factors related to education, 15 of these factors regarding to quality control, 19 factors related to inspec-tion, 12 factors related to information bank and 22 factors was dedicated to management [14].
The results of qualitative study were categorized into seven main themes (resources, quality control, documentation, education, service, inspection and preventive mainte-nance (IPM), designing and implementation) [15].
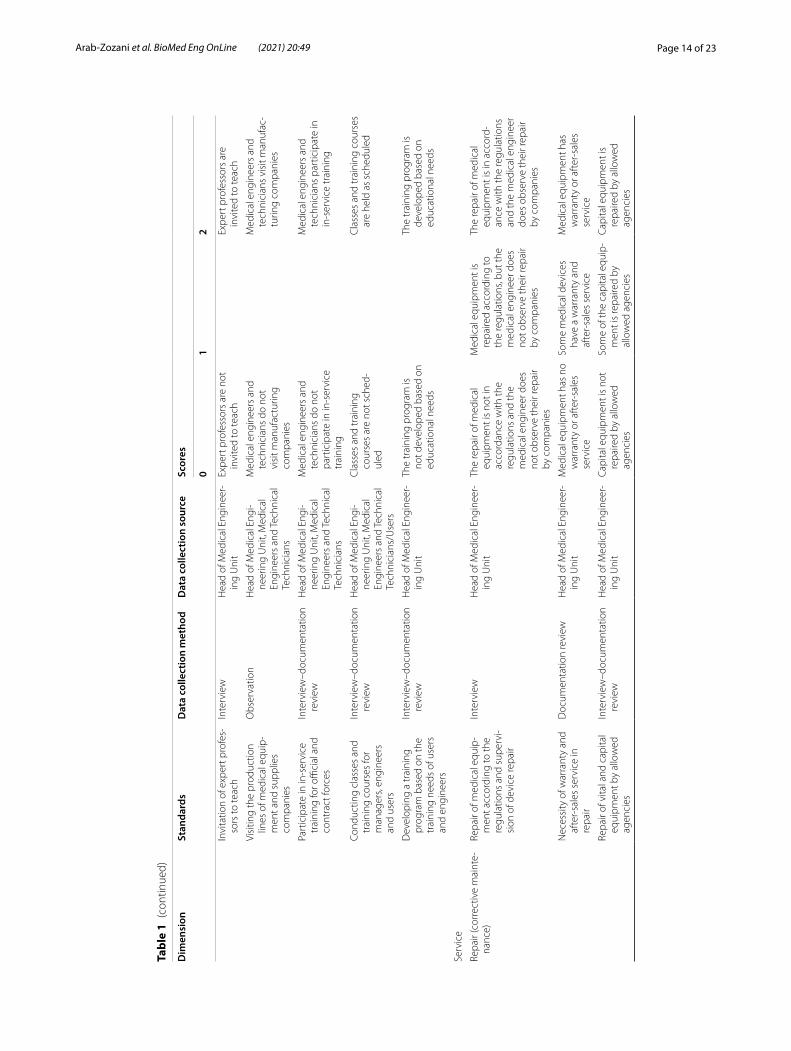
Based on the findings of the first and second steps, a medical equipment maintenance management assessment checklist was developed as follows (Table 1).
The checklists have seven dimensions, each of which includes sub-categories, such as the provision of variety of financial, human and physical resources, which means physical resources to provide a safe and secure environment equipped with the neces-sary facilities. Human resources refer to the provision and allocation of experienced and skilled manpower based on need. Financial resources also include the allocation of suf-ficient and necessary funds and budgets, which should be based on the goal and be allo-cated to priority goals according to the operational plan of the medical engineer unit.
The dimension of quality control tests in the three sub-categories of safety test, per-formance test and calibration refer to all technical tests that require special equipment and are of special importance for the health of the patient and staff. The Inspection and Preventive Maintenance Item refers to the importance and priority of PM than repairing and assessing the user and performance of personnel. In this section, there are topics such as periodic inspections, development of maintenance standards, the existence of external supervisors, and the existence of written and comprehensive guidelines.
In the field of information bank, all activities related to the process of documentation and identification of medical equipment is listed. In the training section, both techni-cal and user training for medical engineers and users are mentioned. The sub-categories of the service sector include after-sales service, repair and maintenance contracts, out-sourcing of the decommissioning process, and so on. The last dimension is design and implementation, which refers to issues such as defining the level of user access, organ-izing joint committees, establishing inter-sectorial communication, policy development, purchasing medical equipment based on needs, and so on.
The scoring method is in three categories of zero, one and two. If the item meets the criteria, score 2, in case of partial compliance, one score and in case of mismatch, no points are awarded. For some items, one score is not included. That is, only two match-ing or mismatch modes are applicable and no intermediate states. Part of the checklist is about data collection that depending on the nature of the item, the collection method involves interview, observation and documentation review. Thus, the interview will

Page 4 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
Dim
ensi
on o
f pro
pose
d m
edic
al e
quip
men
t mai
nten
ance
man
agem
ent a
sses
smen
t che
cklis
t
Sub-
cate
gori
esSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Reso
urce
s
Phys
ical
reso
urce
sPr
ovid
ing
appr
opria
te
phys
ical
spa
ceO
bser
vatio
nH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tLa
ck o
f spa
ce w
ith
adeq
uate
acc
ess
Enou
gh s
pace
but
inap
‑pr
opria
teEx
iste
nce
of a
pla
ce w
ith
adeq
uate
and
suffi
cien
t ac
cess
Prov
idin
g a
spec
ial p
lace
fo
r rep
airin
g de
vice
s in
ho
spita
ls
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Ther
e is
no
spec
ific
plac
eTh
ere
is s
peci
fic p
lace
Allo
catio
n of
mai
nten
ance
un
it in
med
ical
eng
i‑ne
erin
g un
it
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
mai
nten
ance
uni
t is
not
ass
igne
d to
the
med
ical
eng
inee
ring
unit
The
mai
nten
ance
uni
t is
assi
gned
to th
e m
edic
al
engi
neer
ing
unit
Prov
idin
g a
safe
and
he
alth
y w
ork
envi
ron‑
men
t
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
wor
k en
viro
nmen
t is
not s
afe
and
heal
thy
The
wor
k en
viro
nmen
t is
safe
and
hea
lthy
Requ
irem
ent o
f com
pute
r an
d ne
cess
ary
faci
litie
s in
med
ical
eng
inee
ring
unit
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Lack
of m
inim
um n
eces
‑sa
ry fa
cilit
ies
(tel
epho
ne
line,
fax
and
inte
rnet
)
The
nece
ssar
y fa
cilit
ies
(tel
epho
ne li
ne, f
ax a
nd
inte
rnet
) are
not
eno
ugh
Equi
pped
with
tele
phon
e lin
e, fa
x an
d in
tern
et, w
ith
the
nece
ssar
y ad
min
istr
a‑tiv
e fa
cilit
ies
Prov
idin
g lo
caliz
ed m
edi‑
cal e
quip
men
t mai
nte‑
nanc
e so
ftw
are
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
mai
nten
ance
sof
twar
e av
aila
ble
in th
e w
orld
is
not u
sed
acco
rdin
g to
th
e na
tive
cond
ition
s of
th
e co
untr
y
The
mai
nten
ance
sof
twar
e av
aila
ble
in th
e w
orld
is
used
acc
ordi
ng to
the
nativ
e co
nditi
ons
of th
e co
untr
y
The
esta
blis
hmen
t of a
m
aint
enan
ce c
ompu
ter
syst
em
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
ere
are
not e
noug
h co
nditi
ons
to s
et u
p a
com
pute
r mai
nten
ance
sy
stem
(CM
MS)
Ther
e ar
e en
ough
co
nditi
ons
to s
et u
p a
com
pute
r mai
nten
ance
sy
stem
(CM
MS)
Prov
isio
n of
som
e te
chni
‑ca
l che
cklis
ts (t
est a
nd
repa
irs c
heck
lists
)
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Lack
of c
heck
lists
nee
ded
for s
afet
y te
stin
g an
d re
pairs
Inco
mpl
ete
avai
labi
lity
of
safe
ty a
nd re
pair
test
ch
eckl
ists
Exis
tenc
e of
com
plet
e ch
eckl
ists
requ
ired
for
safe
ty te
st a
nd re
pairs

Page 5 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)Su
b-ca
tego
ries
Stan
dard
sD
ata
colle
ctio
n m
etho
dD
ata
colle
ctio
n so
urce
Scor
es
01
2
Exis
tenc
e of
a s
peci
fic
syst
em fo
r rec
ordi
ng
failu
res
Obs
erva
tion–
inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
ere
is n
o sp
ecifi
c sy
stem
fo
r rec
ordi
ng fa
ilure
sTh
ere
is s
peci
fic s
yste
m fo
r re
cord
ing
failu
res
Acc
ess
to u
p‑to
‑dat
e so
ftw
are
in th
e fie
ld o
f m
aint
enan
ce
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tIt
is n
ot p
ossi
ble
to a
cces
s up
‑to‑
date
sof
twar
e in
th
e m
aint
enan
ce a
rea
It is
pos
sibl
e to
acc
ess
up‑
to‑d
ate
soft
war
e in
the
mai
nten
ance
are
a
Hum
an re
sour
ces
Prov
idin
g a
stab
le a
nd
trai
ned
forc
e fo
r the
m
edic
al e
ngin
eerin
g un
it
Obs
erva
tion–
inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
t—m
edic
al e
ngi‑
neer
s an
d te
chni
cian
s
The
avai
labl
e m
anpo
wer
ha
s no
t bee
n fix
ed a
nd
they
hav
e no
t rec
eive
d th
e ne
cess
ary
trai
ning
The
avai
labl
e m
anpo
wer
ha
s be
en fi
xed
but h
as n
ot
rece
ived
the
nece
ssar
y tr
aini
ngO
RTh
e av
aila
ble
man
pow
er h
as
rece
ived
the
nece
ssar
y tr
aini
ng b
ut is
not
fixe
d
The
avai
labl
e m
anpo
wer
ha
s be
en fi
xed
but h
as
rece
ived
the
nece
ssar
y tr
aini
ng
Allo
catio
n of
med
ical
en
gine
erin
g fo
rce
base
d on
nee
d
Obs
erva
tion–
inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
ere
are
not e
noug
h sk
illed
man
pow
er (f
or
ever
y 10
0 ho
spita
l bed
s, at
leas
t one
eng
inee
r an
d on
e te
chni
cal
tech
nici
an)
Ther
e is
ski
lled
man
pow
er,
but n
ot e
noug
h. (F
or
ever
y 10
0 ho
spita
l bed
s, at
leas
t one
eng
inee
r an
d on
e te
chni
cal
tech
nici
an)
Ther
e is
eno
ugh
skill
ed
man
pow
er. (
For e
very
100
ho
spita
l bed
s, at
leas
t one
en
gine
er a
nd o
ne te
chni
‑ca
l tec
hnic
ian)
Fina
ncia
l res
ourc
esA
lloca
tion
fund
s to
m
edic
al e
quip
men
t m
aint
enan
ce
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e re
quire
d bu
dget
or
cred
it is
not
est
imat
ed
and
prov
ided
eac
h ye
ar
in a
ccor
danc
e w
ith th
e M
edic
al E
quip
men
t M
aint
enan
ce R
egul
a‑tio
ns
The
requ
ired
budg
et o
r cr
edit
is e
stim
ated
and
pr
ovid
ed e
ach
year
in
acco
rdan
ce w
ith th
e M
edic
al E
quip
men
t Mai
n‑te
nanc
e Re
gula
tions
Ass
igni
ng a
revo
lvin
g fu
nd
to th
e m
edic
al e
ngin
eer‑
ing
unit
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e re
volv
ing
fund
is n
ot
allo
cate
d fo
r the
med
ical
en
gine
erin
g un
it
The
revo
lvin
g fu
nd is
al
loca
ted
for t
he m
edic
al
engi
neer
ing
unit
Econ
omet
rics
and
cost
–be
nefit
cal
cula
tion
of
equi
pmen
t mai
nten
ance
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tD
ocum
ents
are
not
ava
il‑ab
leD
ocum
ents
are
inco
m‑
plet
eD
ocum
ents
are
com
plet
e

Page 6 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Qua
lity
cont
rol t
ests
Safe
ty te
stPe
rfor
m s
afet
y te
sts
Obs
erva
tion–
inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tN
one
of th
e sa
fety
test
s (e
lect
rical
, phy
sica
l–m
echa
nica
l, ra
diat
ion,
ch
emic
al, u
ser,
etc.
) are
pe
rfor
med
acc
ordi
ng to
th
e re
gula
tions
for t
he
mai
nten
ance
of m
edic
al
equi
pmen
t
Som
e sa
fety
test
s (e
lect
rical
, phy
sica
l–m
echa
nica
l, ra
diat
ion,
ch
emic
al, u
ser,
etc.
) are
pe
rfor
med
acc
ordi
ng to
th
e re
gula
tions
for t
he
mai
nten
ance
of m
edic
al
equi
pmen
t
All
safe
ty te
sts
(ele
ctric
al,
phys
ical
–mec
hani
cal,
radi
atio
n, c
hem
ical
, us
er, e
tc.)
are
perf
orm
ed
acco
rdin
g to
the
regu
la‑
tions
for m
aint
aini
ng
med
ical
equ
ipm
ent
Calib
ratio
nEn
surin
g qu
ality
con
trol
s pe
rfor
med
by
com
pa‑
nies
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tQ
ualit
y co
ntro
ls p
er‑
form
ed b
y co
mpa
nies
ar
e no
t gua
rant
eed
(no
spec
ific
oblig
atio
ns)
Qua
lity
cont
rols
per
form
ed
by c
ompa
nies
are
gu
aran
teed
(hav
e ce
rtai
n ob
ligat
ions
)
Plan
ning
and
con
duct
ing
qual
ity c
ontr
ol te
sts
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
ere
are
no s
peci
fic
prog
ram
qua
lity
cont
rol
test
s
Qua
lity
cont
rol t
ests
hav
e a
spec
ific
prog
ram
Labe
ling
of c
alib
rate
d eq
uipm
ent
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tCa
libra
ted
equi
pmen
t is
not r
egul
arly
labe
led
Calib
rate
d eq
uipm
ent i
s la
bele
d bu
t not
regu
larly
Calib
rate
d eq
uipm
ent i
s re
gula
rly la
bele
d
Perf
orm
ance
test
Perf
orm
tech
nica
l tes
tsO
bser
vatio
n–do
cum
enta
‑tio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Tech
nica
l tes
ts a
re n
ot
perf
orm
ed b
y al
low
ed
agen
cies
or s
ervi
ce
prov
ider
s
Tech
nica
l tes
ts a
re n
ot p
er‑
form
ed b
y al
low
ed a
gen‑
cies
or s
ervi
ce p
rovi
ders

Page 7 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Perf
orm
pra
ctic
al te
sts
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e re
leva
nt te
st is
not
pe
rfor
med
by
the
trai
ned
user
and
is
not a
ccor
ding
to th
e ch
eckl
ist p
rovi
ded
by
the
man
ufac
ture
r or
lega
l rep
rese
ntat
ive
and
unde
r the
sup
ervi
sion
of
the
Med
ical
Eng
inee
r‑in
g U
nit
The
rele
vant
test
is p
er‑
form
ed b
y th
e tr
aine
d us
er a
nd is
acc
ordi
ng to
th
e ch
eckl
ist p
rovi
ded
by
the
man
ufac
ture
r or l
egal
re
pres
enta
tive
and
unde
r th
e su
perv
isio
n of
the
Med
ical
Eng
inee
ring
Uni
t
Perf
orm
labo
rato
ry te
sts
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e re
leva
nt te
st is
not
pe
rfor
med
by
the
trai
ned
user
and
is
not a
ccor
ding
to th
e ch
eckl
ist p
rovi
ded
by
the
man
ufac
ture
r or
lega
l rep
rese
ntat
ive
and
unde
r the
sup
ervi
sion
of
the
Med
ical
Eng
inee
r‑in
g U
nit
The
rele
vant
test
is p
er‑
form
ed b
y th
e tr
aine
d us
er a
nd is
acc
ordi
ng to
th
e ch
eckl
ist p
rovi
ded
by
the
man
ufac
ture
r or l
egal
re
pres
enta
tive
and
unde
r th
e su
perv
isio
n of
the
Med
ical
Eng
inee
ring
Uni
t
Perf
orm
clin
ical
test
sO
bser
vatio
n–do
cum
enta
‑tio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
rele
vant
test
is n
ot
perf
orm
ed b
y th
e tr
aine
d us
er a
nd is
no
t acc
ordi
ng to
the
chec
klis
t pro
vide
d by
th
e m
anuf
actu
rer o
r le
gal r
epre
sent
ativ
e an
d un
der t
he s
uper
visi
on o
f th
e M
edic
al E
ngin
eer‑
ing
Uni
t
The
rele
vant
test
is p
er‑
form
ed b
y th
e tr
aine
d us
er a
nd is
acc
ordi
ng to
th
e ch
eckl
ist p
rovi
ded
by
the
man
ufac
ture
r or l
egal
re
pres
enta
tive
and
unde
r th
e su
perv
isio
n of
the
Med
ical
Eng
inee
ring
Uni
t

Page 8 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Insp
ectio
n an
d pr
even
tive
mai
nten
ance
(IPM
)
Man
agem
ent p
roce
sses
to
ext
end
the
life
of th
e de
vice
Perf
orm
tim
ely
and
regu
lar
prev
entiv
e m
aint
enan
ceO
bser
vatio
n–do
cum
enta
‑tio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
A p
reve
ntiv
e m
aint
enan
ce
prog
ram
is n
ot d
evel
‑op
ed a
nd im
plem
ente
d
A p
reve
ntiv
e m
aint
enan
ce
prog
ram
is d
evel
oped
bu
t it r
uns
inco
mpl
etel
y
A p
reve
ntiv
e m
aint
enan
ce
prog
ram
is d
evel
oped
an
d im
plem
ente
d
Insu
ffici
ent k
now
ledg
e in
th
e fie
ld o
f pre
vent
ive
mai
nten
ance
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
t—m
edic
al e
ngi‑
neer
s an
d te
chni
cian
s
Non
e of
the
empl
oyee
s of
th
e M
edic
al E
ngin
eer‑
ing
Uni
t hav
e su
f‑fic
ient
kno
wle
dge
and
awar
enes
s in
the
field
of
prev
entiv
e m
aint
enan
ce
Som
e em
ploy
ees
of th
e M
edic
al E
ngin
eerin
g U
nit h
ave
suffi
cien
t kn
owle
dge
and
info
r‑m
atio
n in
the
field
of
prev
entiv
e m
aint
enan
ce
All
empl
oyee
s of
the
Med
i‑ca
l Eng
inee
ring
Uni
t hav
e su
ffici
ent k
now
ledg
e an
d in
form
atio
n in
the
field
of
prev
entiv
e m
aint
enan
ce
Prev
entiv
e m
aint
enan
ce
prio
rity
over
qua
lity
cont
rol a
nd re
pair
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tPr
even
tive
mai
nten
ance
is
not
a p
riorit
y in
the
med
ical
eng
inee
ring
unit’
s ac
tion
plan
Prev
entiv
e m
aint
enan
ce is
a
prio
rity
in th
e m
edic
al
engi
neer
ing
unit’
s ac
tion
plan
Perio
dic,
inte
rnal
, cas
e,
prac
tical
insp
ectio
nEx
iste
nce
of s
ome
sub‑
rule
sIn
terv
iew
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
exis
ting
rule
s an
d re
gula
tions
rega
rdin
g m
aint
enan
ce a
re n
ot
nece
ssar
y an
d ap
prop
ri‑at
e
The
exis
ting
rule
s an
d re
gula
tions
rega
rdin
g m
aint
enan
ce a
re n
eces
‑sa
ry b
ut n
ot a
ppro
pria
te
The
exis
ting
rule
s an
d re
gula
tions
rega
rdin
g m
aint
enan
ce a
re n
eces
‑sa
ry a
nd a
ppro
pria
te
Usi
ng a
ccre
dita
tion
mea
sure
s to
ass
ess
the
mai
nten
ance
of m
edic
al
equi
pmen
t
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tFr
om a
ccre
dita
tion
mea
sure
s ar
e no
t use
d to
ass
ess
mai
nten
ance
ac
tiviti
es a
nd p
roce
sses
From
acc
redi
tatio
n m
easu
res
are
not u
sed
to a
sses
s m
aint
enan
ce
activ
ities
and
pro
cess
es

Page 9 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Exam
inat
ion
of m
edic
al
equi
pmen
t thr
ough
hu
man
sen
ses
and
spec
ializ
ed c
heck
lists
Inte
rvie
wH
ead
of th
e U
nive
rsity
M
edic
al E
quip
men
t O
ffice
or
Expe
rts
intr
oduc
ed b
y hi
m a
nd th
e he
ad o
f th
e m
edic
al e
ngin
eer‑
ing
unit
Lack
of i
nves
tigat
e an
d su
perv
isio
n of
all
oper
a‑tio
ns (r
evie
w a
nd m
oni‑
torin
g of
qua
lity
cont
rol
test
s of
med
ical
equ
ip‑
men
t, re
view
of f
acili
ties
and
anci
llary
faci
litie
s re
late
d to
equ
ipm
ent,
revi
ew o
f the
env
iron‑
men
t aro
und
med
ical
eq
uipm
ent,
asse
ssm
ent
of d
evic
e us
age
by u
ser
and
asse
ssm
ent o
f the
pe
rfor
man
ce o
f tec
hni‑
cal p
erso
nnel
)(B
y ch
eckl
ist)
Inve
stig
ate
and
supe
rvi‑
sion
of s
ome
oper
a‑tio
ns (i
nves
tigat
e an
d m
onito
ring
of q
ualit
y co
ntro
l tes
ts o
f med
ical
eq
uipm
ent,
inve
stig
ate
of fa
cilit
ies
and
anci
l‑la
ry fa
cilit
ies
rela
ted
to
equi
pmen
t, in
vest
igat
e of
the
envi
ronm
ent
arou
nd m
edic
al e
quip
‑m
ent,
asse
ssm
ent o
f de
vice
usa
ge b
y us
er
and
asse
ssm
ent o
f the
pe
rfor
man
ce o
f tec
hni‑
cal p
erso
nnel
)(B
y ch
eckl
ist)
Inve
stig
ate
and
supe
rvis
ion
of a
ll op
erat
ions
(inv
es‑
tigat
e an
d m
onito
ring
of q
ualit
y co
ntro
l tes
ts
of m
edic
al e
quip
men
t, in
vest
igat
e of
faci
litie
s an
d an
cilla
ry fa
cilit
ies
rela
ted
to e
quip
men
t, in
vest
igat
e of
the
envi
ron‑
men
t aro
und
med
ical
eq
uipm
ent,
asse
ssm
ent
of d
evic
e us
age
by u
ser
and
asse
ssm
ent o
f the
pe
rfor
man
ce o
f tec
hnic
al
pers
onne
l)(B
y ch
eckl
ist)
Det
erm
inin
g th
e tim
e pe
riod
of p
erio
dic
visi
tsIn
terv
iew
–doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Not
acc
ordi
ng to
the
actio
n pl
anA
ccor
ding
to th
e ac
tion
plan
Dev
elop
ing
plan
for p
eri‑
odic
vis
itsD
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tA
n ac
tion
plan
has
not
be
en d
evel
oped
An
actio
n pl
an h
as b
een
deve
lope
d
Exis
tenc
e of
an
exte
rnal
ob
serv
erIn
terv
iew
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit a
nd H
ospi
tal
Man
ager
The
exte
rnal
sup
ervi
sor
has
not b
een
appo
inte
d to
insp
ect a
nd o
vers
ee
the
affai
rs o
f the
med
ical
en
gine
erin
g un
it
The
exte
rnal
sup
ervi
sor
has
been
app
oint
ed to
in
spec
t and
ove
rsee
the
affai
rs o
f the
med
ical
en
gine
erin
g un
it
Dev
elop
ing
stan
dard
s in
m
aint
enan
ce c
ontr
acts
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
serv
ice,
mai
nten
ance
an
d re
pair
cont
ract
hav
e no
t a s
peci
fic fr
ame‑
wor
k. (A
ccor
ding
to
regu
latio
ns)
The
serv
ice,
mai
nten
ance
an
d re
pair
cont
ract
hav
e a
spec
ific
fram
ewor
k.
(Acc
ordi
ng to
regu
latio
ns)

Page 10 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Prep
arin
g a
list o
f ess
entia
l eq
uipm
ent
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
list o
f ess
entia
l equ
ip‑
men
t has
not
bee
n pr
epar
ed a
nd is
not
av
aila
ble
to th
e de
part
‑m
ents
A li
st o
f ess
entia
l equ
ip‑
men
t has
bee
n pr
epar
ed
but i
s no
t ava
ilabl
e to
th
e de
part
men
ts
The
list o
f ess
entia
l equ
ip‑
men
t has
bee
n pr
epar
ed
and
is a
vaila
ble
to th
e de
part
men
ts
Ensu
ring
the
exis
tenc
e of
sa
fe e
lect
ricity
(eve
ry s
ix
mon
ths,
the
hosp
ital’s
el
ectr
icity
is c
ontr
olle
d by
an
elec
tric
ian
and
the
avai
labl
e do
cum
ents
)
Obs
erva
tion
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
item
s m
entio
ned
in
the
regu
latio
ns re
gard
‑in
g el
ectr
ical
saf
ety
are
not o
bser
ved
and
perf
orm
ed
The
item
s m
entio
ned
in
the
regu
latio
ns re
late
d to
ele
ctric
al s
afet
y ar
e in
com
plet
ely
obse
rved
an
d pe
rfor
med
The
item
s m
entio
ned
in
the
regu
latio
ns re
gard
‑in
g el
ectr
ical
saf
ety
are
com
plet
ely
obse
rved
and
pe
rfor
med
Perio
dic
revi
ew o
f the
co
rrec
t ope
ratio
n of
the
devi
ce b
y th
e us
er
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e co
rrec
t ope
ratio
n of
the
devi
ce is
not
ch
ecke
d pe
riodi
cally
by
the
user
The
corr
ect o
pera
tion
of th
e de
vice
is c
heck
ed p
erio
di‑
cally
by
the
user
Lack
of u
nifo
rmity
of
asse
ssm
ent c
heck
lists
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
med
ical
eng
inee
r‑in
g un
it do
es n
ot h
ave
a sp
ecifi
c ch
eckl
ist t
o as
sess
the
mai
nten
ance
st
atus
of m
edic
al e
quip
‑m
ent
The
med
ical
eng
inee
r‑in
g un
it ha
s a
spec
ific
chec
klis
t to
asse
ss th
e m
aint
enan
ce s
tatu
s of
m
edic
al e
quip
men
t
Mor
e vi
sitin
g to
def
ectiv
e de
vice
sIn
terv
iew
–doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Def
ectiv
e de
vice
s ar
e no
t ch
ecke
d re
gula
rly b
y a
med
ical
eng
inee
r (ex
ist‑
ence
of a
ctio
n pl
an)
Def
ectiv
e de
vice
s ar
e ch
ecke
d re
gula
rly b
y a
med
ical
eng
inee
r (ex
ist‑
ence
of a
ctio
n pl
an)
Cla
rifica
tion
of re
gula
tions
an
d no
tifica
tion
inst
ruc‑
tions
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
t—m
edic
al e
ngi‑
neer
s an
d te
chni
cian
s
Non
e of
the
med
ical
en
gine
erin
g st
aff a
re
awar
e of
the
regu
latio
ns
and
inst
ruct
ions
issu
ed
by th
e D
epar
tmen
t of
Med
ical
Equ
ipm
ent/
not
all e
mpl
oyee
s kn
ow th
e ru
les
clea
rly
Som
e of
the
med
ical
en
gine
erin
g st
aff a
re
awar
e of
the
regu
latio
ns
and
inst
ruct
ions
issu
ed
by th
e D
epar
tmen
t of
Med
ical
Equ
ipm
ent/
som
e of
em
ploy
ees
know
the
rule
s cl
early
All
of th
e m
edic
al e
ngi‑
neer
ing
staff
are
aw
are
of th
e re
gula
tions
and
in
stru
ctio
ns is
sued
by
the
Dep
artm
ent o
f Med
ical
Eq
uipm
ent/
all e
mpl
oyee
s kn
ow th
e ru
les
clea
rly

Page 11 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Requ
irem
ent t
o fo
llow
or
ders
from
hig
h le
vels
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tO
rder
s is
sued
by
the
Dep
artm
ent o
f Med
ical
Eq
uipm
ent a
re n
ot
prop
erly
com
plie
d
Ord
ers
issu
ed b
y th
e D
epar
tmen
t of M
edic
al
Equi
pmen
t are
pro
perly
co
mpl
ied
Acc
ess
to th
e bo
okle
t of
the
set o
f mai
nten
ance
ru
les
and
regu
latio
ns
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tN
one
of th
e st
aff m
em‑
bers
hav
e ac
cess
to th
e bo
okle
t
Som
e of
the
staff
mem
‑be
rs h
ave
acce
ss to
the
book
let
All
of th
e st
aff m
embe
rs
have
acc
ess
to th
e bo
okle
t
Com
plet
ion
and
obse
r‑va
nce
of a
ccre
dita
tion
mea
sure
s
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e un
it do
es n
ot m
eet
any
of th
e cr
iteria
on
a re
gula
r bas
is
The
unit
mee
ts s
ome
of
the
crite
ria o
n a
regu
lar
basi
s
The
unit
mee
ts a
ny o
f the
cr
iteria
on
a re
gula
r bas
is
Impl
emen
tatio
n of
m
aint
enan
ce ru
les
and
regu
latio
ns
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e ru
les
anno
unce
d by
th
e O
ffice
of M
edic
al
Equi
pmen
t do
not r
un
regu
larly
The
rule
s an
noun
ced
by th
e O
ffice
of M
edic
al E
quip
‑m
ent r
un re
gula
rly
Exis
tenc
e of
writ
ten
and
com
preh
ensi
ve in
stru
c‑tio
ns
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Ther
e ar
e no
com
pre‑
hens
ive
guid
elin
es fo
r m
aint
aini
ng m
edic
al
equi
pmen
t
Ther
e ar
e w
ritte
n gu
ide‑
lines
for m
aint
enan
ce
med
ical
equ
ipm
ent,
but
they
are
not
com
pre‑
hens
ive
Ther
e ar
e co
mpr
ehen
sive
gu
idel
ines
for m
aint
aini
ng
med
ical
equ
ipm
ent
Info
rmat
ion
bank
Prov
idin
g m
edic
al d
evic
es
ID (i
dent
ifica
tion)
Elec
tron
ic, c
ompr
ehen
sive
an
d in
telli
gent
ele
ctro
nic
med
ical
ID
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tM
edic
al ID
are
not
re
gula
rly p
repa
red
and
upda
ted
Med
ical
equ
ipm
ent I
D h
as
been
pre
pare
d bu
t not
up
to d
ate
Med
ical
ID a
re re
gula
rly
prep
ared
and
upd
ated
Easy
acc
ess
to ID
info
rma‑
tion
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans/
Dep
art‑
men
t Em
ploy
ees
Empl
oyee
s do
not
hav
e ac
cess
to ID
info
rmat
ion
Empl
oyee
s ha
ve a
cces
s to
ID
info
rmat
ion

Page 12 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Use
of i
ndig
enou
s an
d gl
obal
evi
denc
eCo
mm
unic
ate
with
sta
nd‑
ard
scie
ntifi
c re
fere
nces
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e he
ad o
f the
med
ical
en
gine
erin
g un
it do
es
not h
ave
acce
ss to
sci
en‑
tific
stan
dard
refe
renc
es
(sci
entifi
c ar
ticle
s, sc
ien‑
tific
site
s, in
tern
atio
nal
stan
dard
s, et
c.)
The
head
of t
he m
edic
al
engi
neer
ing
unit
does
not
ha
ve a
cces
s to
sci
entifi
c st
anda
rd re
fere
nces
(s
cien
tific
artic
les,
scie
n‑tifi
c si
tes,
inte
rnat
iona
l st
anda
rds,
etc.
)
Util
izin
g th
e in
form
atio
n of
the
man
ufac
ture
r in
the
asse
ssm
ent
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
ere
is n
o ac
cess
to th
e m
anuf
actu
rer’s
info
rma‑
tion
and
it is
not
ope
r‑at
ed a
ccor
ding
ly
Ther
e is
acc
ess
to th
e m
anuf
actu
rer’s
info
rma‑
tion,
but
it is
not
ope
r‑at
ed a
ccor
ding
ly
Ther
e is
acc
ess
to th
e m
anuf
actu
rer’s
info
rma‑
tion
and
it is
ope
rate
d ac
cord
ingl
y
Cond
uctin
g st
udie
s an
d re
sear
ch in
the
field
of
med
ical
equ
ipm
ent
mai
nten
ance
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
med
ical
eng
inee
ring
unit
does
not
con
‑du
ct re
sear
ch o
n th
e m
aint
enan
ce o
f med
ical
eq
uipm
ent
The
med
ical
eng
inee
ring
unit
cond
ucts
rese
arch
on
the
mai
nten
ance
of
med
ical
equ
ipm
ent
Use
r gui
dePr
epar
ing
and
inst
allin
g qu
ick
user
labe
lsO
bser
vatio
n–do
cum
enta
‑tio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Qui
ck u
ser t
ags
are
not
prov
ided
and
inst
alle
d on
all
devi
ces
Qui
ck u
ser t
ags
are
pro‑
vide
d an
d in
stal
led
on a
ll de
vice
s
Prep
arat
ion
of m
anua
ls in
bo
th P
ersi
an a
nd E
nglis
h fo
r eac
h de
vice
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e m
anua
l of e
ach
devi
ce h
as n
ot b
een
prep
ared
and
has
not
be
en p
rovi
ded
to th
e us
er o
f the
dev
ice
The
man
ual o
f eac
h de
vice
has
bee
n pr
e‑pa
red
but h
as n
ot b
een
prov
ided
to th
e us
er o
f th
e de
vice
The
man
ual o
f eac
h de
vice
ha
s be
en p
repa
red
and
prov
ided
to th
e us
er o
f th
e de
vice
Doc
umen
tatio
nA
rchi
ve o
f exe
cutiv
e pr
oces
ses
(repa
ir, q
ualit
y co
ntro
l and
PM
doc
u‑m
enta
tion)
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tM
aint
enan
ce p
roce
dure
s ar
e no
t ful
ly d
ocu‑
men
ted
and
arch
ived
Som
e of
mai
nten
ance
pr
oced
ures
are
fully
do
cum
ente
d an
d ar
chiv
ed
Mai
nten
ance
pro
cedu
res
are
fully
doc
umen
ted
and
arch
ived
Use
of H
IS s
yste
m in
mai
n‑te
nanc
eO
bser
vatio
nH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e m
edic
al e
ngin
eerin
g un
it is
not
equ
ippe
d w
ith th
e H
IS s
yste
m
The
med
ical
eng
inee
ring
unit
is e
quip
ped
with
the
HIS
sys
tem

Page 13 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Educ
atin
g
Use
r and
tech
nica
l edu
ca‑
tion
Educ
atio
nal s
uper
viso
r pa
rtic
ipat
ion
in u
ser
trai
ning
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
t/Ed
ucat
iona
l su
perv
isor
Educ
atio
nal s
uper
viso
rs
do n
ot c
oope
rate
with
m
edic
al e
ngin
eers
in
educ
atin
g us
ers
Educ
atio
nal s
uper
viso
rs
coop
erat
e w
ith m
edic
al
engi
neer
s in
edu
catin
g us
ers
Targ
eted
trai
ning
cou
rses
Inte
rvie
wH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans/
Dep
art‑
men
t Em
ploy
ees
Trai
ning
cou
rses
are
not
pu
rpos
eful
or u
sefu
lTr
aini
ng c
ours
es a
re p
ur‑
pose
ful o
r use
ful
Acq
uain
tanc
e of
the
offici
als
of th
e m
edic
al
engi
neer
ing
unit
with
th
e m
anag
emen
t
Inte
rvie
wH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans
Non
e of
the
med
ical
en
gine
erin
g offi
cers
are
fa
mili
ar w
ith m
edic
al
equi
pmen
t mai
nten
ance
m
anag
emen
t
Som
e of
the
med
ical
en
gine
erin
g offi
cers
are
fa
mili
ar w
ith m
edic
al
equi
pmen
t mai
nte‑
nanc
e m
anag
emen
t
All
of th
e m
edic
al e
ngin
eer‑
ing
office
rs a
re fa
mili
ar
with
med
ical
equ
ipm
ent
mai
nten
ance
man
age‑
men
t
The
effec
tiven
ess
of tr
ain‑
ing
cour
ses
Inte
rvie
wH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans/
Dep
art‑
men
t Em
ploy
ees
The
trai
ning
s ar
e no
t eff
ectiv
eTh
e tr
aini
ngs
are
effec
tive
Prov
idin
g th
e po
ssib
ility
fo
r all
med
ical
eng
inee
rs
to p
artic
ipat
e in
trai
ning
w
orks
hops
Inte
rvie
wH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans
It is
not
pos
sibl
e fo
r all
engi
neer
s an
d te
chni
‑ci
ans
to p
artic
ipat
e in
tr
aini
ng w
orks
hops
It is
pos
sibl
e fo
r all
engi
‑ne
ers
and
tech
nici
ans
to p
artic
ipat
e in
trai
ning
w
orks
hops
Nur
se’ le
vel o
f edu
catio
n in
the
field
of g
ener
al
equi
pmen
t
Inte
rvie
wU
sers
Med
ical
equ
ipm
ent u
sers
ha
ve n
ot b
een
trai
ned
in
gene
ral e
quip
men
t
Med
ical
equ
ipm
ent u
sers
ha
ve n
ot b
een
trai
ned
in
gene
ral e
quip
men
t
Use
r ret
rain
ing
abou
t es
sent
ial e
quip
men
tIn
terv
iew
Use
rsU
sers
are
not
retr
aine
d ab
out e
ssen
tial e
quip
‑m
ent
Use
rs a
re re
trai
ned
abou
t es
sent
ial e
quip
men
t
Page 14 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Invi
tatio
n of
exp
ert p
rofe
s‑so
rs to
teac
hIn
terv
iew
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Expe
rt p
rofe
ssor
s ar
e no
t in
vite
d to
teac
hEx
pert
pro
fess
ors
are
invi
ted
to te
ach
Visi
ting
the
prod
uctio
n lin
es o
f med
ical
equ
ip‑
men
t and
sup
plie
s co
mpa
nies
Obs
erva
tion
Hea
d of
Med
ical
Eng
i‑ne
erin
g U
nit,
Med
ical
En
gine
ers
and
Tech
nica
l Te
chni
cian
s
Med
ical
eng
inee
rs a
nd
tech
nici
ans
do n
ot
visi
t man
ufac
turin
g co
mpa
nies
Med
ical
eng
inee
rs a
nd
tech
nici
ans
visi
t man
ufac
‑tu
ring
com
pani
es
Part
icip
ate
in in
‑ser
vice
tr
aini
ng fo
r offi
cial
and
co
ntra
ct fo
rces
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans
Med
ical
eng
inee
rs a
nd
tech
nici
ans
do n
ot
part
icip
ate
in in
‑ser
vice
tr
aini
ng
Med
ical
eng
inee
rs a
nd
tech
nici
ans
part
icip
ate
in
in‑s
ervi
ce tr
aini
ng
Cond
uctin
g cl
asse
s an
d tr
aini
ng c
ours
es fo
r m
anag
ers,
engi
neer
s an
d us
ers
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans/
Use
rs
Cla
sses
and
trai
ning
co
urse
s ar
e no
t sch
ed‑
uled
Cla
sses
and
trai
ning
cou
rses
ar
e he
ld a
s sc
hedu
led
Dev
elop
ing
a tr
aini
ng
prog
ram
bas
ed o
n th
e tr
aini
ng n
eeds
of u
sers
an
d en
gine
ers
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e tr
aini
ng p
rogr
am is
no
t dev
elop
ed b
ased
on
educ
atio
nal n
eeds
The
trai
ning
pro
gram
is
deve
lope
d ba
sed
on
educ
atio
nal n
eeds
Serv
ice
Repa
ir (c
orre
ctiv
e m
aint
e‑na
nce)
Repa
ir of
med
ical
equ
ip‑
men
t acc
ordi
ng to
the
regu
latio
ns a
nd s
uper
vi‑
sion
of d
evic
e re
pair
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e re
pair
of m
edic
al
equi
pmen
t is
not i
n ac
cord
ance
with
the
regu
latio
ns a
nd th
e m
edic
al e
ngin
eer d
oes
not o
bser
ve th
eir r
epai
r by
com
pani
es
Med
ical
equ
ipm
ent i
s re
paire
d ac
cord
ing
to
the
regu
latio
ns, b
ut th
e m
edic
al e
ngin
eer d
oes
not o
bser
ve th
eir r
epai
r by
com
pani
es
The
repa
ir of
med
ical
eq
uipm
ent i
s in
acc
ord‑
ance
with
the
regu
latio
ns
and
the
med
ical
eng
inee
r do
es o
bser
ve th
eir r
epai
r by
com
pani
es
Nec
essi
ty o
f war
rant
y an
d af
ter‑
sale
s se
rvic
e in
re
pair
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Med
ical
equ
ipm
ent h
as n
o w
arra
nty
or a
fter
‑sal
es
serv
ice
Som
e m
edic
al d
evic
es
have
a w
arra
nty
and
afte
r‑sa
les
serv
ice
Med
ical
equ
ipm
ent h
as
war
rant
y or
aft
er‑s
ales
se
rvic
e
Repa
ir of
vita
l and
cap
ital
equi
pmen
t by
allo
wed
ag
enci
es
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tCa
pita
l equ
ipm
ent i
s no
t re
paire
d by
allo
wed
ag
enci
es
Som
e of
the
capi
tal e
quip
‑m
ent i
s re
paire
d by
al
low
ed a
genc
ies
Capi
tal e
quip
men
t is
repa
ired
by a
llow
ed
agen
cies

Page 15 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Mak
e it
poss
ible
to re
pair
the
devi
ce in
side
the
hosp
ital
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tIt
is n
ot p
ossi
ble
to re
pair
som
e m
edic
al e
quip
‑m
ent i
nsid
e th
e ho
spita
l
It is
pos
sibl
e to
repa
ir so
me
med
ical
equ
ipm
ent i
nsid
e th
e ho
spita
l
Dec
omm
issi
onin
gO
bser
ving
the
deco
m‑
mis
sion
ing
proc
ess
in
mai
nten
ance
man
age‑
men
t
Obs
erva
tion–
docu
men
ta‑
tion
revi
ew–i
nter
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
deco
mm
issi
onin
g pr
oces
s is
not
follo
wed
ac
cord
ing
to th
e in
stru
c‑tio
ns a
nd n
otifi
catio
n ru
les
The
deco
mm
issi
onin
g pr
o‑ce
ss is
follo
wed
acc
ordi
ng
to th
e in
stru
ctio
ns a
nd
notifi
catio
n ru
les
Out
sour
cing
Com
mun
icat
ion
with
re
puta
ble
com
pani
esIn
terv
iew
–doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Med
ical
eng
inee
ring
unit
is n
ot a
ssoc
iate
d w
ith
repu
tabl
e co
mpa
nies
Med
ical
eng
inee
ring
unit
is
asso
ciat
ed w
ith re
puta
ble
com
pani
es
inve
stig
ate
the
per‑
form
ance
of p
rivat
e co
mpa
nies
Inte
rvie
wH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e pe
rfor
man
ce o
f pr
ivat
e co
mpa
nies
is
not m
onito
red
by th
e D
epar
tmen
t of M
edic
al
Equi
pmen
t
The
perf
orm
ance
of p
rivat
e co
mpa
nies
is m
onito
red
by th
e D
epar
tmen
t of
Med
ical
Equ
ipm
ent
The
role
of t
hird
par
ties
in
qual
ity c
ontr
olIn
terv
iew
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
Qua
lity
cont
rol i
s no
t don
e by
priv
ate
com
pani
esQ
ualit
y co
ntro
l is
done
by
priv
ate
com
pani
es
Buy
mai
nten
ance
sof
twar
e fro
m p
rivat
e co
mpa
nies
Obs
erva
tion–
docu
men
ta‑
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tM
aint
enan
ce s
oftw
are
is n
ot p
urch
ased
from
pr
ivat
e co
mpa
nies
Mai
nten
ance
sof
twar
e is
pu
rcha
sed
from
priv
ate
com
pani
es
Coop
erat
ion
and
coor
di‑
natio
n of
min
istr
ies
and
univ
ersi
ties
with
priv
ate
com
pani
es
Inte
rvie
wM
inis
try
and
univ
ersi
ty
offici
als
The
Min
istr
y an
d th
e U
ni‑
vers
ity d
o no
t coo
pera
te
with
priv
ate
com
pani
es
The
Min
istr
y an
d th
e U
nive
rsity
coo
pera
te w
ith
priv
ate
com
pani
es
Out
sour
cing
of s
ervi
ce,
mai
nten
ance
and
repa
irD
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tO
utso
urci
ng d
oes
not
have
a g
ener
al fr
ame‑
wor
k ac
cord
ing
to th
e re
gula
tions
Out
sour
cing
doe
s no
t hav
e a
gene
ral f
ram
ewor
k ac
cord
ing
to th
e re
gula
‑tio
ns

Page 16 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Des
igni
ng a
nd im
plem
enta
tion
Proc
ess
man
agem
ent
Form
atio
n of
join
t co
mm
ittee
s by
the
Dep
artm
ent o
f Med
ical
Eq
uipm
ent
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
The
com
mitt
ee’s
min
utes
ar
e no
t ava
ilabl
eTh
e m
inut
es o
f the
com
‑m
ittee
are
ava
ilabl
e, b
ut
not c
ompl
ete
The
min
utes
of t
he c
omm
it‑te
e ar
e co
mpl
ete
Defi
ne th
e le
vel o
f use
r ac
cess
to m
edic
al e
quip
‑m
ent
Inte
rvie
wH
ead
of M
edic
al E
ngi‑
neer
ing
Uni
t, M
edic
al
Engi
neer
s an
d Te
chni
cal
Tech
nici
ans/
Use
rs
The
user
acc
ess
leve
l po
licy
is n
ot d
efine
dTh
e us
er a
cces
s le
vel i
s de
fined
acc
ordi
ng to
the
rele
vant
pol
icy
Inte
r‑se
ctor
ial c
omm
uni‑
catio
n in
hos
pita
lsIn
terv
iew
–obs
erva
tion
Hea
d of
Med
ical
Eng
i‑ne
erin
g U
nit,
Med
ical
En
gine
ers
and
Tech
nica
l Te
chni
cian
s/U
sers
The
Med
ical
Eng
inee
r‑in
g U
nit d
oes
not h
ave
a sp
ecifi
c pr
otoc
ol fo
r co
mm
unic
atin
g w
ith
othe
r dep
artm
ents
and
un
its
The
Med
ical
Eng
inee
ring
Uni
t has
a s
peci
fic p
roto
‑co
l for
com
mun
icat
ing
with
oth
er d
epar
tmen
ts
and
units
Plan
ning
for m
aint
enan
ce
in th
e offi
ce o
f med
ical
eq
uipm
ent
Inte
rvie
w–d
ocum
enta
tion
revi
ewH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
tTh
e M
edic
al E
ngin
eerin
g U
nit h
as n
o pl
ans
for
any
med
ical
equ
ipm
ent
mai
nten
ance
act
iviti
es
The
Med
ical
Eng
inee
ring
Uni
t has
pla
ns fo
r som
e m
edic
al e
quip
men
t m
aint
enan
ce a
ctiv
ities
The
Med
ical
Eng
inee
r‑in
g U
nit h
as p
lans
for
all m
edic
al e
quip
men
t m
aint
enan
ce a
ctiv
ities
Dev
elop
and
defi
ne in
ter‑
nal p
olic
ies
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
No
polic
y ha
s be
en
deve
lope
d fo
r the
m
aint
enan
ce o
f med
ical
eq
uipm
ent
A p
olic
y ha
s be
en d
evel
‑op
ed to
mai
nten
ance
m
edic
al e
quip
men
t
Dev
elop
an
actio
n pl
an fo
r th
e m
edic
al e
ngin
eer‑
ing
unit
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Eng
inee
r‑in
g U
nit
An
actio
n pl
an fo
r m
aint
aini
ng m
edic
al
equi
pmen
t has
not
bee
n de
velo
ped
An
actio
n pl
an fo
r mai
ntai
n‑in
g m
edic
al e
quip
men
t ha
s be
en d
evel
oped
Man
agem
ent i
nfra
stru
c‑tu
re in
the
med
ical
eq
uipm
ent d
epar
tmen
t
Inte
rvie
wH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
t/H
ead
of M
edic
al E
ngin
eerin
g U
nit
The
Dep
artm
ent o
f Med
i‑ca
l Equ
ipm
ent d
oes
not
have
a s
tron
g in
frast
ruc‑
ture
The
Dep
artm
ent o
f Med
ical
Eq
uipm
ent h
ave
a st
rong
in
frast
ruct
ure
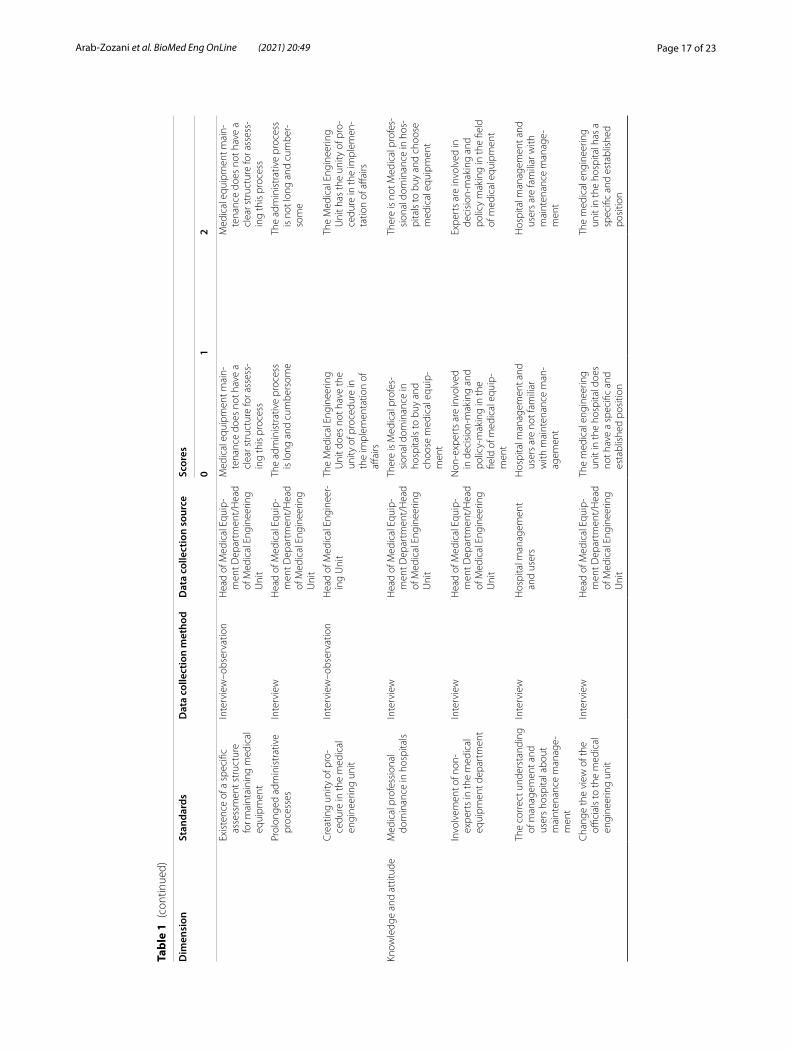
Page 17 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Exis
tenc
e of
a s
peci
fic
asse
ssm
ent s
truc
ture
fo
r mai
ntai
ning
med
ical
eq
uipm
ent
Inte
rvie
w–o
bser
vatio
nH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
t/H
ead
of M
edic
al E
ngin
eerin
g U
nit
Med
ical
equ
ipm
ent m
ain‑
tena
nce
does
not
hav
e a
clea
r str
uctu
re fo
r ass
ess‑
ing
this
pro
cess
Med
ical
equ
ipm
ent m
ain‑
tena
nce
does
not
hav
e a
clea
r str
uctu
re fo
r ass
ess‑
ing
this
pro
cess
Prol
onge
d ad
min
istr
ativ
e pr
oces
ses
Inte
rvie
wH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
t/H
ead
of M
edic
al E
ngin
eerin
g U
nit
The
adm
inis
trat
ive
proc
ess
is lo
ng a
nd c
umbe
rsom
eTh
e ad
min
istr
ativ
e pr
oces
s is
not
long
and
cum
ber‑
som
e
Cre
atin
g un
ity o
f pro
‑ce
dure
in th
e m
edic
al
engi
neer
ing
unit
Inte
rvie
w–o
bser
vatio
nH
ead
of M
edic
al E
ngin
eer‑
ing
Uni
tTh
e M
edic
al E
ngin
eerin
g U
nit d
oes
not h
ave
the
unity
of p
roce
dure
in
the
impl
emen
tatio
n of
aff
airs
The
Med
ical
Eng
inee
ring
Uni
t has
the
unity
of p
ro‑
cedu
re in
the
impl
emen
‑ta
tion
of a
ffairs
Know
ledg
e an
d at
titud
eM
edic
al p
rofe
ssio
nal
dom
inan
ce in
hos
pita
lsIn
terv
iew
Hea
d of
Med
ical
Equ
ip‑
men
t Dep
artm
ent/
Hea
d of
Med
ical
Eng
inee
ring
Uni
t
Ther
e is
Med
ical
pro
fes‑
sion
al d
omin
ance
in
hosp
itals
to b
uy a
nd
choo
se m
edic
al e
quip
‑m
ent
Ther
e is
not
Med
ical
pro
fes‑
sion
al d
omin
ance
in h
os‑
pita
ls to
buy
and
cho
ose
med
ical
equ
ipm
ent
Invo
lvem
ent o
f non
‑ex
pert
s in
the
med
ical
eq
uipm
ent d
epar
tmen
t
Inte
rvie
wH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
t/H
ead
of M
edic
al E
ngin
eerin
g U
nit
Non
‑exp
erts
are
invo
lved
in
dec
isio
n‑m
akin
g an
d po
licy‑
mak
ing
in th
e fie
ld o
f med
ical
equ
ip‑
men
t
Expe
rts
are
invo
lved
in
deci
sion
‑mak
ing
and
polic
y m
akin
g in
the
field
of
med
ical
equ
ipm
ent
The
corr
ect u
nder
stan
ding
of
man
agem
ent a
nd
user
s ho
spita
l abo
ut
mai
nten
ance
man
age‑
men
t
Inte
rvie
wH
ospi
tal m
anag
emen
t an
d us
ers
Hos
pita
l man
agem
ent a
nd
user
s ar
e no
t fam
iliar
w
ith m
aint
enan
ce m
an‑
agem
ent
Hos
pita
l man
agem
ent a
nd
user
s ar
e fa
mili
ar w
ith
mai
nten
ance
man
age‑
men
t
Cha
nge
the
view
of t
he
offici
als
to th
e m
edic
al
engi
neer
ing
unit
Inte
rvie
wH
ead
of M
edic
al E
quip
‑m
ent D
epar
tmen
t/H
ead
of M
edic
al E
ngin
eerin
g U
nit
The
med
ical
eng
inee
ring
unit
in th
e ho
spita
l doe
s no
t hav
e a
spec
ific
and
esta
blis
hed
posi
tion
The
med
ical
eng
inee
ring
unit
in th
e ho
spita
l has
a
spec
ific
and
esta
blis
hed
posi
tion

Page 18 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Tabl
e 1
(con
tinue
d)
Dim
ensi
onSt
anda
rds
Dat
a co
llect
ion
met
hod
Dat
a co
llect
ion
sour
ceSc
ores
01
2
Purc
hasi
ng m
anag
emen
tBu
y th
e de
vice
from
the
web
site
of r
eput
able
co
mpa
nies
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Equ
ip‑
men
t Dep
artm
ent/
Hea
d of
Med
ical
Eng
inee
ring
Uni
t
Med
ical
equ
ipm
ent i
s no
t pu
rcha
sed
from
repu
ta‑
ble
com
pani
es
Med
ical
equ
ipm
ent i
s pu
rcha
sed
from
repu
tabl
e co
mpa
nies
To b
uy e
quip
men
t bas
ed
on n
eed
Doc
umen
tatio
n re
view
Hea
d of
Med
ical
Equ
ip‑
men
t Dep
artm
ent/
Hea
d of
Med
ical
Eng
inee
ring
Uni
t
Med
ical
equ
ipm
ent i
s no
t pu
rcha
sed
base
d on
the
need
s of
the
area
and
th
e ta
rget
Med
ical
equ
ipm
ent i
s pu
rcha
sed
base
d on
the
need
s of
the
area
and
the
targ
et

Page 19 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
be used if we are looking for the views and attitudes of stakeholders. Dimensions that require documentation will be assessed through documentation review. The observation method is also for assessing physical items.
DiscussionIn the field of medical equipment maintenance management, there is no single and standard checklist that includes all hospitals in the country. The only available check-lists include accreditation measures that generally assess the tasks and activities of the medical engineering unit. Since the issue of maintenance management includes a wide variety of topics, and in the low- and middle-income countries, there is major weakness in this regard, so we decided to design a checklist for uniformity and accurate and com-prehensive assessment using Iranian context. The Departments of Medical Equipment of some provinces in Iran have designed a checklist natively for its affiliated hospitals, the dimension and method of which are different. For example, the maintenance man-agement evaluation checklist of Tabriz Medical Equipment Office includes 15 indica-tors (technical force, medical engineering unit, medical equipment ID, quality control tests, PM, training, medical equipment and spare parts storage, service and maintenance contract, the existence of purchase process, the existence of decommissioning process, the existence of recall system and reporting of adverse events, ensuring sound electric-ity, implementing a continuous maintenance improvement process, familiarizing with the general administration’s rules and website, management and allocating a separate budget for maintenance).
According to the medical equipment maintenance management criteria of the MOHME, some of these dimensions can be merged into one dimension and some can be separated. In addition, each of the indicators and sub-indicators can be expanded. That is, not all maintenance management issues are addressed. The scoring and classification of dimensions in this checklist does not have a specific standard and does not include all dimensions of maintenance according to the maintenance criteria of the MOHME and is generally designed.
Herrera-Galán [16] evaluated the performance of the maintenance function through management audits and their implementation in five hospitals. The aspects evaluated include equipment availability, response to a service request, monitoring and control of biomedical equipment, staff training, quality of work executed by the maintenance technicians, the workload of maintenance technicians, control of the work executed by the maintenance technicians, the effectiveness of annual maintenance planning and department performance. The results of this research show that the audit technique is a valuable checklist in the performance assessment of a hospitals. The application of the proposed method evidenced that the most critical component in the results of a man-agement audit is the human resource [16].
An effective medical equipment maintenance program consists of three main ele-ments. (1) Identifying the medical devices that need to maintenance program by the Ministry of Health. (2) Financial management, personal management, performance monitoring, operational management and performance improvement. (3) Proper imple-mentation of the maintenance program. These three elements are also considered in the

Page 20 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
designed checklists in different dimensions such as resources, designing and implemen-tation [17].
The maintenance and its management constitute a checklist that ensures the equip-ment performance. There exist four criteria in which the hospitals coincide that they should improve, even though each of them in different measure and sub-criterion. These criteria are an organization of maintenance; human resources; planning, pro-gramming and control of the maintenance and corrective maintenance. These crite-ria are among the sub-categories of maintenance management assessment checklists [18].
Amerion et al. [19] identified effective factors on the MEMM in a military hospital. Among effective factors on the MEMM, 26 components were extracted. User training components, human resources, commitment and the experience of users, the foreign exchange market, periodic visits, and trade name were the most important components which had more than 75% of the relative abundance. According to the results, factors with high importance on the management of medical equipment maintenance should be supported by the center’s directors. Attention to the use of these components can reduce maintenance costs, and therefore, increase the life of medical equipment. User training and human resources are the two main dimensions of this checklist [19].
According to the current results, documentation and service are two dimensions of MEMM. The problems of some hospitals in MEMM were introduced from the aspects of maintenance time, maintenance record, maintenance service and self-maintenance. Some measures were proposed including simplifying maintenance process through PDCA, information maintenance record, cooperating with the third-party maintainer and establishing self-maintenance team, so that precision and infor-mation medical equipment management can be realized to maximize the benefit of medical equipment management [20].
The medical equipment requires maintenance (both scheduled and unscheduled) during its useful life. The medical equipment maintenance process should be planned, implemented, monitored, and improved continually. This process requires careful supervision by healthcare administrators, many of whom may not have the technical background to understand all of the relevant factors. Maintenance management is the most important function in overall medical equipment management. In this regard, implementation of appropriate maintenance strategies requires the following types of resources: human resources, material resources, financial resources and documenta-tion. Our findings also point to the importance of these resources [21].
We need a comprehensive assessment checklist that covers all aspects of medical equipment maintenance management in hospitals. In this regard, the identification of influential factors is essential. Eighty-nine factors were identified that affect MEMM. Five of the factors were found related to resources item, 12 factors related to service, 4 factors related to education, 15 of these factors regarding quality control, 19 fac-tors related to inspection, 12 factors related to information bank and 22 factors were dedicated to management. These factors are implicated in decision-making in sup-port of selection, purchase, repair and maintenance of medical equipment, especially for capital equipment managers and medical engineers in hospitals and also for the assessment of this process. Identification and classification of influential factors can

Page 21 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
be of help for raising critical alerts about the types of equipment more prone to main-tenance problems [14].
Strengths and limitationsIn our knowledge, this study is the first comprehensive study of-its-kind addressing all of the factors affecting an effective and efficient MEMM. It offers comprehensive check-lists for assessing the status of MEMM. In addition, the present compiled checklist is the result of multi-method research in such a way that its components are determined through systematic review and obtaining the views of experts and specialists in this field. This indicates the validity and comprehensiveness of the checklists developed.
Lack of enough information concerning the concept of maintenance management, lack of specific guidelines and instructions were the most notable limitations.
ConclusionEffective maintenance management of medical devices increases the efficiency and pro-ductivity of health technology resources, which is especially important when resources are limited. This allows patients to access medical equipment that can provide an accu-rate diagnosis, effective treatment, or appropriate rehabilitation. Several factors affect the management of medical equipment maintenance, and it is important to follow each of them to improve the performance of devices and provide medical services to patients. Therefore, before designing an assessment checklist, we need to consider a specific framework for the maintenance management process to include all maintenance activi-ties. The medical equipment maintenance management assessment checklists allow for the timely identification of deficiencies and gaps in the medical equipment maintenance management process so that the necessary steps can be taken. It also can help managers and engineers to assess maintenance status and provide solutions and interventions for the decision makers and policymakers to improve its.
MethodsThe present study was a multi-methods study in four stages. In the first stage, a sys-tematic review on data related to factors which affect the assessment of MEMM was conducted. Then, a qualitative study was designed to investigate these factors from expert view and related documents. In the end, the results of the first and second stages were combined using content analysis and the final checklist was developed.
Stage 1
A systematic search of the following databases was conducted during October 2015 in the PubMed, ProQuest, Scopus, Embase, and Web of Science. The search was updated in June 2017. Our search strategy was as follow: ((“medical device*”[Title/Abstract]) OR “medical equipment”[Title/Abstract]) AND “maintenance management”[Title/Abstract])) [14]. At first, we extracted the items, then categorized the extracted items based on the Ministry of Health and Medical Education of Iran (MOHME) framework in each category [13].

Page 22 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Stage 2
In the qualitative step, semi-structured interviews and documents review were used for data collection. The collected data consisted of the perspectives of medical and biomedical engineers concerning factors influencing MEMM. Related documents were regulations of MEMM, MEMM guidelines and other related regulations or reports developed by MOHME. The content analysis approach (inductive and deduc-tive) was used to analyze the data. The extracted codes were sorted into both themes and subthemes based on comparisons between similarities and differences that were categorized into 7 main themes and 22 subthemes [15].
Stages 3
In this stage, the researchers combined the extracted data from systematic review and qualitative study using a content analysis and devised the first draft of the checklist. The primary checklist was developed in the form of assessment checklists in seven dimen-sions (providing resources, quality control tests, preventive inspection and maintenance, database, training, service, design and implementation).
Stages 4
We sent the primary draft of checklist through a Delphi to 20 experts who had sufficient scientific and information background in the field of MEMM for assessing the validity and reliability. Of them seven experts participated in this stages and send their com-ments. In the first round, experts commented on the content, dimensions, writing and appearance of the primary checklist. The research team modified the primary version based on expert’s comments and sends it again to experts. Eventually, the proposed checklist was finalized after approving the experts.AcknowledgementsThe current study is a part of MSc thesis in Healthcare Management, Rona Bahreini. The authors appreciate Tabriz Univer‑sity of Medical Sciences for its financial support.
Authors’ contributionsRB conceived of the presented idea. AI and LD were in charge of overall direction and planning. RB and MAZ drafted the manuscript. AI, LD, RB and MAZ contributed to the design and implementation of the research. All the authors discussed the results and commented on the manuscript. RB and MAZ revised the manuscript based on the reviewer’s comments. All the authors read and approved the final manuscript.
FundingThis study was funded by Tabriz University of Medical Sciences. This study is a part of MSc thesis that has been done with the ethical code TBZMED.REC.1394.570.
Availability of data and materialsThe datasets of this study are available from the corresponding authors upon reasonable request.
Declarations
Ethics approval and consent to participateThis study is a part of MSc. thesis that has been done under the support of Tabriz University of Medical Sciences with the ethical code TBZMED.REC.1394.570.
Consent for publicationAll the authors confirmed the consent for publication.
Competing interestsThe authors declare that they have no conflict of interest.

Page 23 of 23Arab‑Zozani et al. BioMed Eng OnLine (2021) 20:49
Author details1 Social Determinants of Health Research Center, Birjand University of Medical Sciences, Birjand, Iran. 2 Health Econom‑ics Department, Tabriz Health Services Management Research Center, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran. 3 Tabriz Health Services Management Research Center, Iranian Center of Excellence in Health Management, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran. 4 Department of Health Sciences (HLV), Public Health Science, Mid Sweden University, Sundsvall, Sweden. 5 Higher School of Public Health, Al Farabi Kazakh National University, Almaty, Kazakhstan. 6 Tabriz Health Ser‑vices Management Research Center, Iranian Center of Excellence in Health Management, Student Research Committee, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran.
Received: 6 October 2020 Accepted: 30 December 2020
References 1. Oshiyama NF, Silveira AC, Bassani RA, Bassani JWM. Medical equipment classification according to corrective mainte‑
nance data: a strategy based on the equipment age. Revista Brasileira de Engenharia Biomédica. 2014;30(1):64–9. 2. Taghipour S. Reliability and maintenance of medical devices: Citeseer. University of Toronto; 2011. 3. Hamdi N, Oweis R, Zraiq HA, Sammour DA. An intelligent healthcare management system: a new approach in work‑
order prioritization for medical equipment maintenance requests. J Med Syst. 2012;36(2):557–67. 4. Karimi A, Mojdeh S, Mehraban MA. The effect of six sigma program on improving medical equipment management
of operating rooms in one of the hospitals in Isfahan in 2016. Pharmacophore. 2017;8(6):e‑1173225. 5. Kihiu J, Maranga S, Mutia D. Maintenance management of medical equipment in hospitals. Indust Eng Let.
2012;2(3):9–19. 6. Jamshidi A, Rahimi SA, Ait‑kadi D, Bartolome AR. Medical devices inspection and maintenance; a literature review.
In: Institute of Industrial and Systems Engineers annual conference proceedings, vol. 3895. 2014. 7. Goszczynska M, Tyszka T, Slovlc P. Risk perception in Poland: A comparison with three other countries. J Behav Decis
Mak. 1991;4(3):179–93. 8. Patil PJ, Patil SP, Jaltade VG, Gupta SS. Departmental equipment maintenance system in Government Medical Col‑
lege. Int Arch Integr Med. 2015;2(3):79–86. 9. Alikhani P, Ganji H, Abtahi M, Vesal S, Naghdi B. Preventive maintenance of medical equipment in Alzahra Hospital,
Isfahan, Iran 2013. Int J Health Syst Disaster Manag. 2013;1(4):217. 10. Mahfoud H, El Barkany A, El Biyaali A. A hybrid decision‑making model for maintenance prioritization in health care
systems. Am J Appl Sci. 2016;13(4):439–50. 11. Abdo AM, Wahed MA, Sharawi A. Dynamic model for evaluation of medical devices maintenance in developing
countries. Int J Appl Innov Eng Manag. 2014;3(12):146–59. 12. Chen M‑F, Chu S‑L, Lee J‑K, Lin F‑H, Tsai C‑L, Kao T, et al. editors. The benefit of in‑hospital clinical engineer services
for medical devices maintenance. In: XIV Mediterranean conference on medical and biological engineering and computing. Cham: Springer; 2016. pp. 975–8.
13. Medical equipment maintenance management criteria of Ministry of Health and Medical Education (MoHME) of Iran. Available at: https:// arums. ac. ir/ imam/ fa/ page/ 7367/.
14. Bahreini R, Doshmangir L, Imani A. Affecting medical equipment maintenance management: a systematic review. J Clin Diagn Res. 2018;12(4):1–7.
15. Bahreini R, Doshmangir L, Imani A. Influential factors on medical equipment maintenance management. J Qual Maint Eng. 2019;25(1):128–43.
16. Herrera‑Galán M. Management audit applied to the maintenance department in hospital facilities//Auditoría de gestión aplicada al departamento de mantenimiento en instalaciones hospitalarias. Ingeniería Mecánica. 2017;20(3):152–9.
17. Al‑Mawali A, Pinto AD, Al‑Hinai AT. Medical equipment and healthcare technology: health vision 2050. Biomed Instrum Technol. 2018;52(6):442–50.
18. Cuzco MAV, Parra SRV, Londoño CMG, Costales JHN. Assessment of the maintenance management in hospitals of the Ecuadorian institute of social security of Zona 3 of Ecuador. Ingenius. 2019;22:59.
19. Amerion A, Alijanzadeh M, Teymourzadeh E. Effective factors on the management of medical equipment mainte‑nance in a military hospital: a qualitative study in Iran. EBNESINA. 2015;17(3):11–8.
20. Liu W, Shi B, Guilan L. Medical equipment maintenance management based on PDCA. Chin Med Equip J. 2015;36(5):138–9.
21. Wang B. Medical equipment maintenance: management and oversight. Synth Lect Biomed Eng. 2012;7(2):1–85.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.