assessment & treatment of spastic muscle overactivity · assessment & treatment of spastic...
TRANSCRIPT
Assessment & Treatment of
Spastic Muscle Overactivity
Cori Ponter, PT, MPT, NCS
Gerard Francisco, MD
TPTA SED Meeting
March 29, 2012
2
Objectives
Participants will be able to:
Identify types of muscle overactivity and their clinical
presentations
Discuss the pathophysiology and origins of spastic
muscle overactivity
Identify and differentiate various assessment tools
used in assessing muscle overactivity
Discuss various treatment options for spastic
muscle overactivity, including medical management
and therapeutic management
3
What is “Spasticity?”
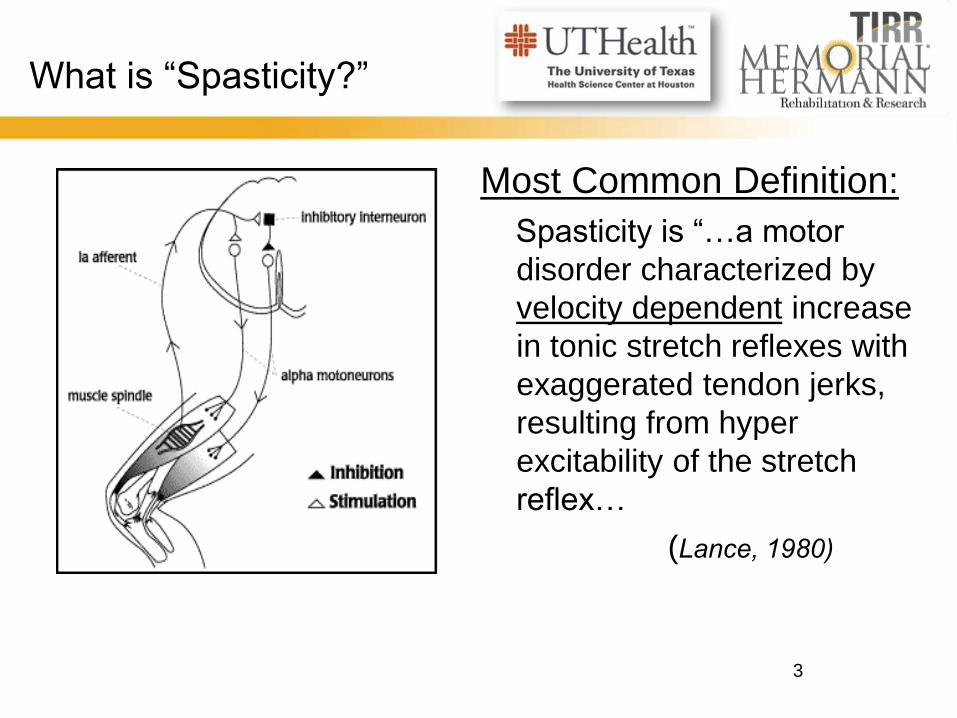
Most Common Definition:
Spasticity is “…a motor
disorder characterized by
velocity dependent increase
in tonic stretch reflexes with
exaggerated tendon jerks,
resulting from hyper
excitability of the stretch
reflex…
(Lance, 1980)
4
What is “Spasticity?”
Clinically:
Most “talked about,” but other types of overactivity are
usually grouped together as “spasticity.”
Just one type of muscle overactivity that occurs with
CNS lesions.
By itself, may not cause a high level of
disability
Triggered by stretch and velocity
5
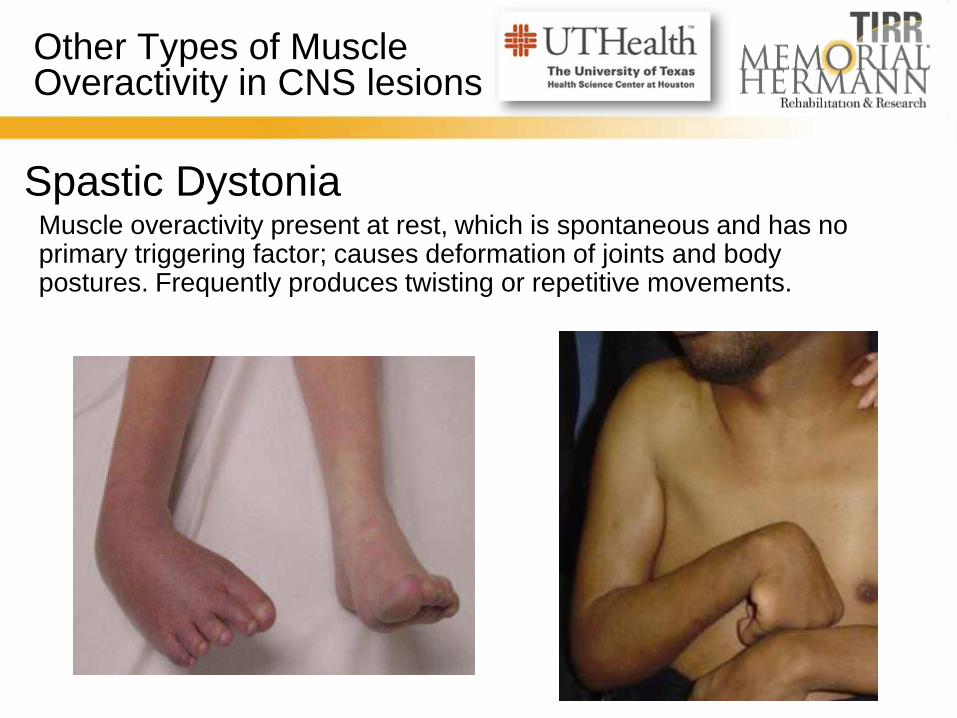
Other Types of Muscle Overactivity in CNS lesions
Muscle overactivity present at rest, which is spontaneous and has no primary triggering factor; causes deformation of joints and body postures. Frequently produces twisting or repetitive movements.
Spastic Dystonia
6
Other Types of Muscle Overactivity in CNS lesions
Hypertonic Rigidity Similar resistance is felt with PROM regardless of the
speed or direction of movement
Spastic Co-Contraction Unwanted activity of antagonistic muscle group during
voluntary agonistic movements (ex: activation of triceps
during voluntary elbow flexion).
7
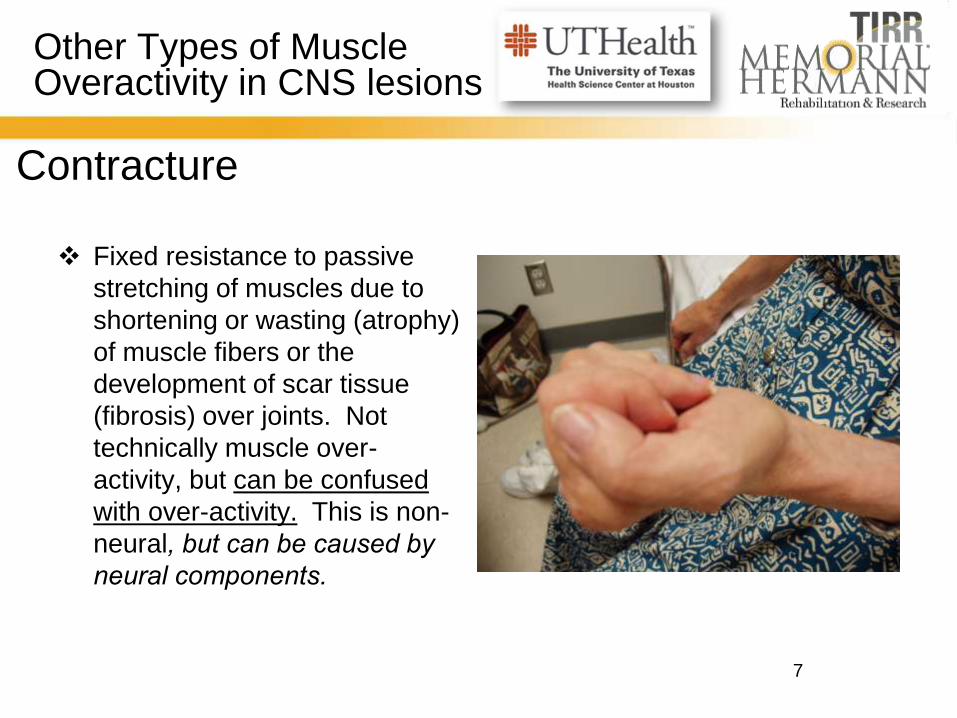
Other Types of Muscle Overactivity in CNS lesions
Contracture
Fixed resistance to passive
stretching of muscles due to
shortening or wasting (atrophy)
of muscle fibers or the
development of scar tissue
(fibrosis) over joints. Not
technically muscle over-
activity, but can be confused
with over-activity. This is non-
neural, but can be caused by
neural components.
8
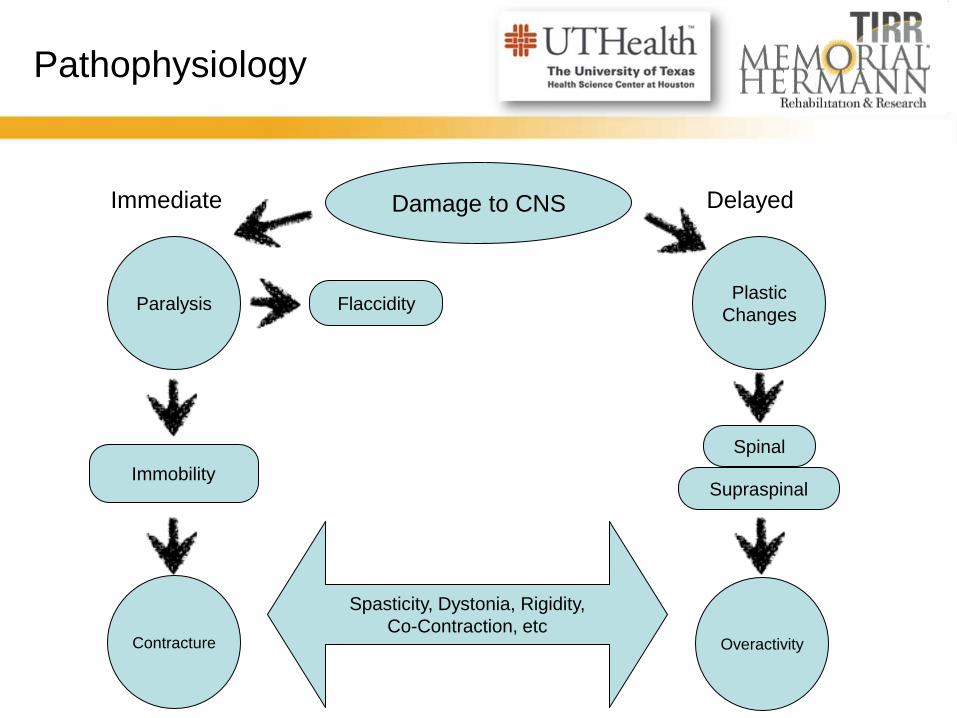
Pathophysiology
8
Damage to CNS
Paralysis
Contracture
Immobility
Flaccidity Plastic
Changes
Spinal
Overactivity
Supraspinal
Spasticity, Dystonia, Rigidity,
Co-Contraction, etc
Immediate Delayed
9
Pathophysiology of Spasticity & Other Muscle Overactivity
Immediate paralysis, leading to immobility
Active and passive tissue changes:
Type I fibers (slow/tonic) change to Type II (fast twitch/fatigable)
Muscle extensibility decreases due to a decrease in the # of
sarcomeres and connective tissue accumulation in extrafusal
fibers
These tissue changes lead to increases in stretch transmission
to muscle spindle
Plastic changes within the CNS
Rerouting at spinal level
Recruitment of new motor pathways
10
How Does Spasticity Develop?
Possible mechanisms of spasticity
Increased neuronal excitability
Enhanced excitatory synaptic
input
Segmental afferents
Regional excitatory
interneurons
Descending pathways, i.e.,
lateral vestibulospinal tract
Reduced inhibitory synaptic
input
Renshaw cell recurrent
inhibition
Ia inhibitory interneurons
Ib afferent fibers
Change in intrinsic electrical
properties of the neuron
Change in passive membrane
electrical properties
Change in voltage sensitive
membrane conductance
Enhanced stretch-evoked
synaptic excitation of neurons
γ efferent hyperactivity
Excitatory interneurons more
sensitive to muscle afferent
11
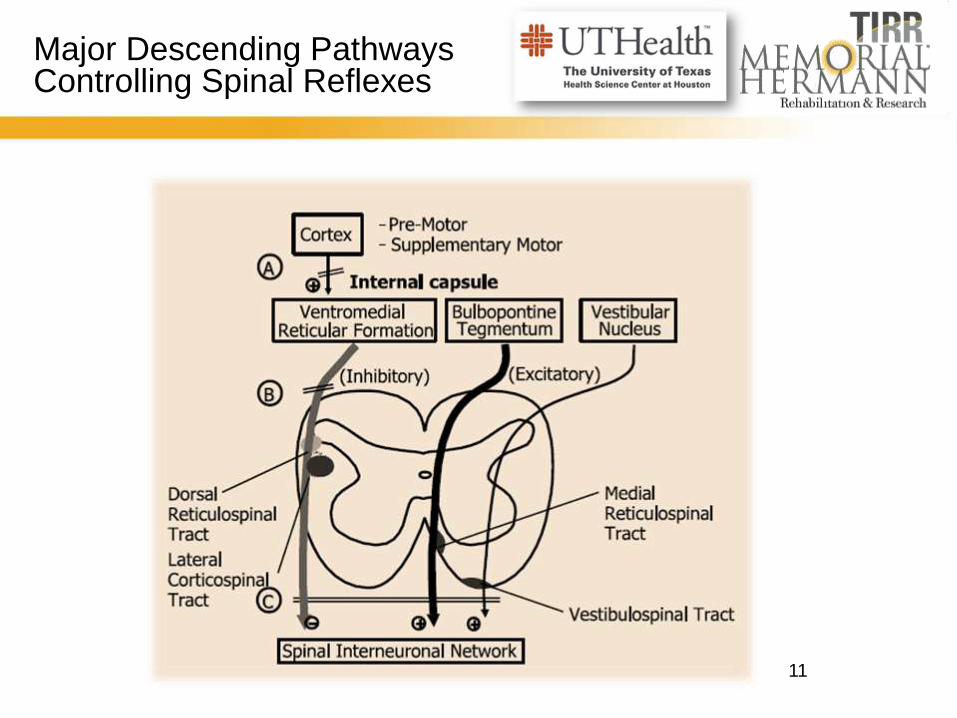
Major Descending Pathways Controlling Spinal Reflexes
12
Origins of Muscle Overactivity
Spinal - SCI, MS
Inhibitory message is sent but cannot be
received due to disruption of spinal cord
Cerebral -
BI, CVA, CP, MS
Lack of inhibition messages
being sent
13
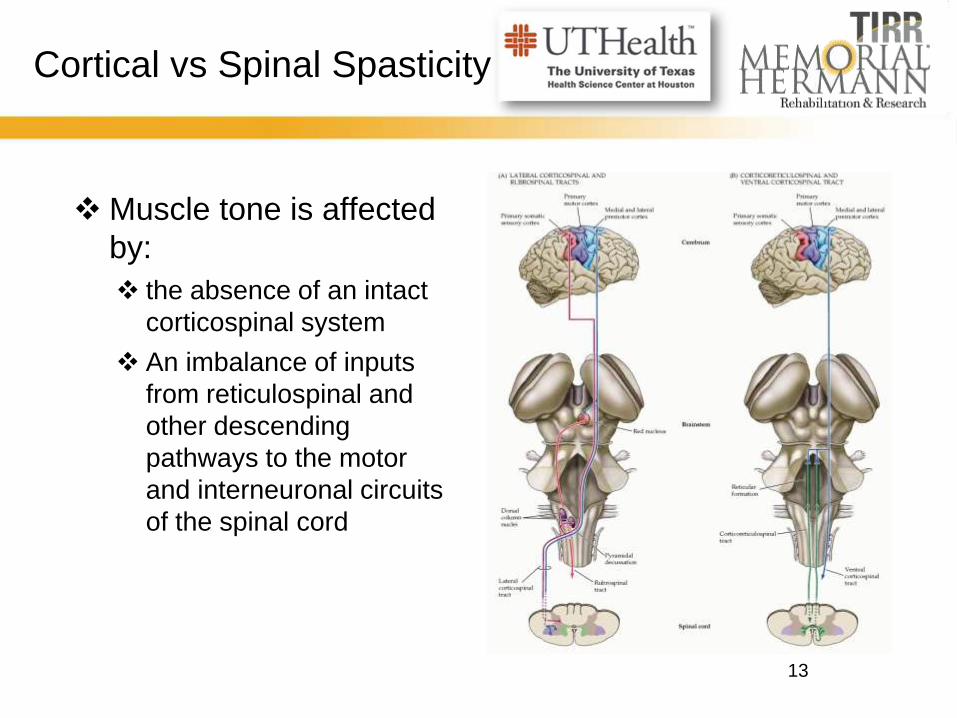
Cortical vs Spinal Spasticity
Muscle tone is affected
by:
the absence of an intact
corticospinal system
An imbalance of inputs
from reticulospinal and
other descending
pathways to the motor
and interneuronal circuits
of the spinal cord
14
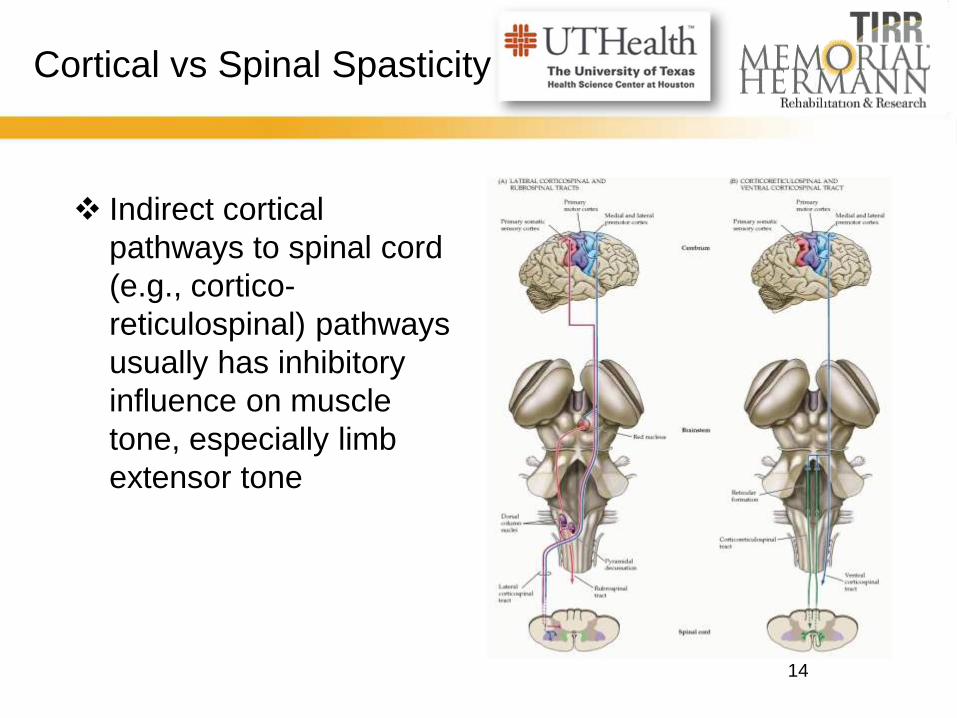
Cortical vs Spinal Spasticity
Indirect cortical
pathways to spinal cord
(e.g., cortico-
reticulospinal) pathways
usually has inhibitory
influence on muscle
tone, especially limb
extensor tone
15
Cortical vs Spinal Spasticity
Loss of descending tonic or phasic excitatory and
inhibitory inputs to the spinal motor apparatus
Alterations in the segmental balance of excitatory and
inhibitory control
Denervation supersensitivity
Neuronal sprouting
16
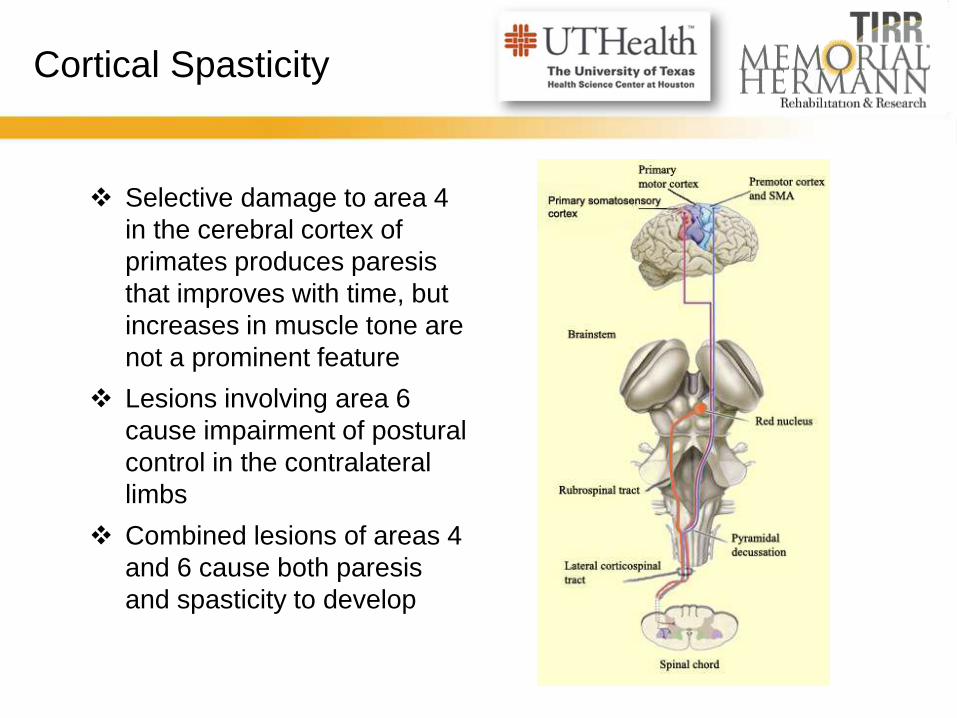
Cortical Spasticity
Selective damage to area 4
in the cerebral cortex of
primates produces paresis
that improves with time, but
increases in muscle tone are
not a prominent feature
Lesions involving area 6
cause impairment of postural
control in the contralateral
limbs
Combined lesions of areas 4
and 6 cause both paresis
and spasticity to develop
17
Spinal Changes
During the development of spasticity, the spinal cord
undergoes neurophysiologic changes in the excitability
of motor neurons, interneuronal connections, and local
reflex pathways
The excitability of alpha motor neurons is increased, as
is suggested by enhanced H-M ratios and F-wave
amplitudes
Judged by recordings from Ia spindle afferents, muscle
spindle sensitivity is not increased in human spasticity
18
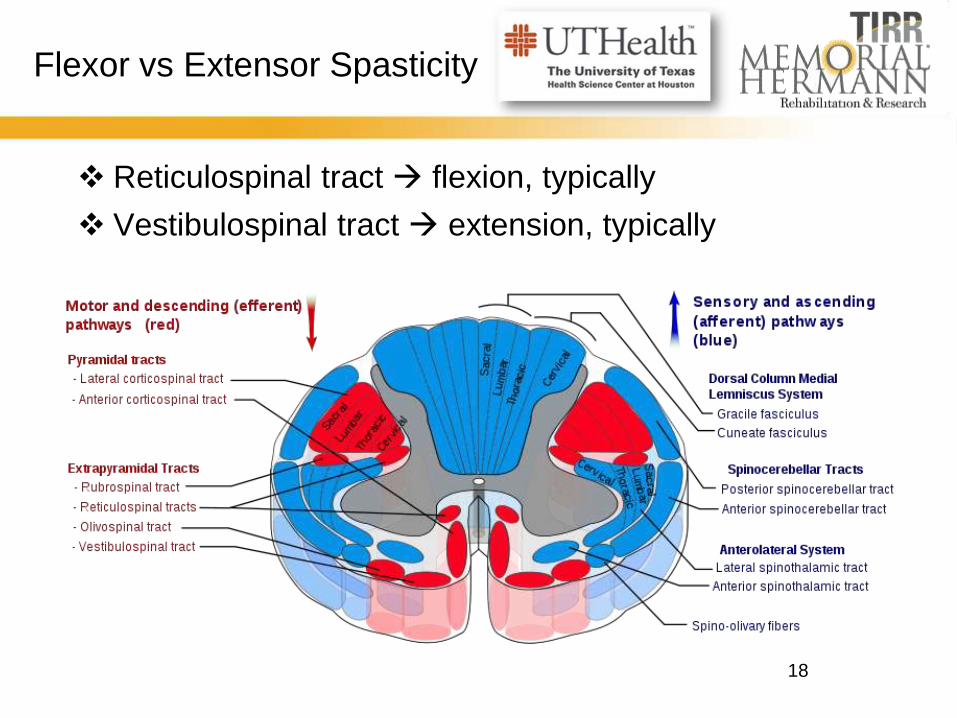
Flexor vs Extensor Spasticity
Reticulospinal tract flexion, typically
Vestibulospinal tract extension, typically
19
Pathophysiology of Spasticity
Imbalance between excitatory and inhibitory impulses
to the alpha motor neuron in the spinal cord
Due to a loss of descending inhibitory input to the
alpha motor neuron due to injury to the cortical spinal
tracts
Descending
Inhibition Sensory
Excitation
20
Treatment Options
20
Botulinum
Toxins
Physical
Modalities
and Therapy
Intrathecal
therapies
Phenol
and
Alcohol
injections
Surgery
Oral
Drugs
21
Considerations for Management Choices
✦When considering management choices for Cerebral
Origin muscle overactivity, we need to be aware of the
effect of the medications on the brain’s recovery process
✦Many oral anti-spasticity medications have the side
effect of making people sleepy, slowing cognitive
processes, and may ultimately slow the recovery of
function
✦ The challenge is to
manage abnormal tone
without interfering with
brain healing/recovery
22
Best Practices Spasticity Management
EFFECTIVE APPROACH
An integrated and
multidisciplinary program
of physical and medical
interventions
A clear individualized
patient management
strategy
WHEN AND HOW TO TREAT
Significance, i.e. disabling
Distribution of spasticity
Chronicity, severity, and
cause
Concomitant conditions
Cost
It’s never too late to treat
spasticity
23
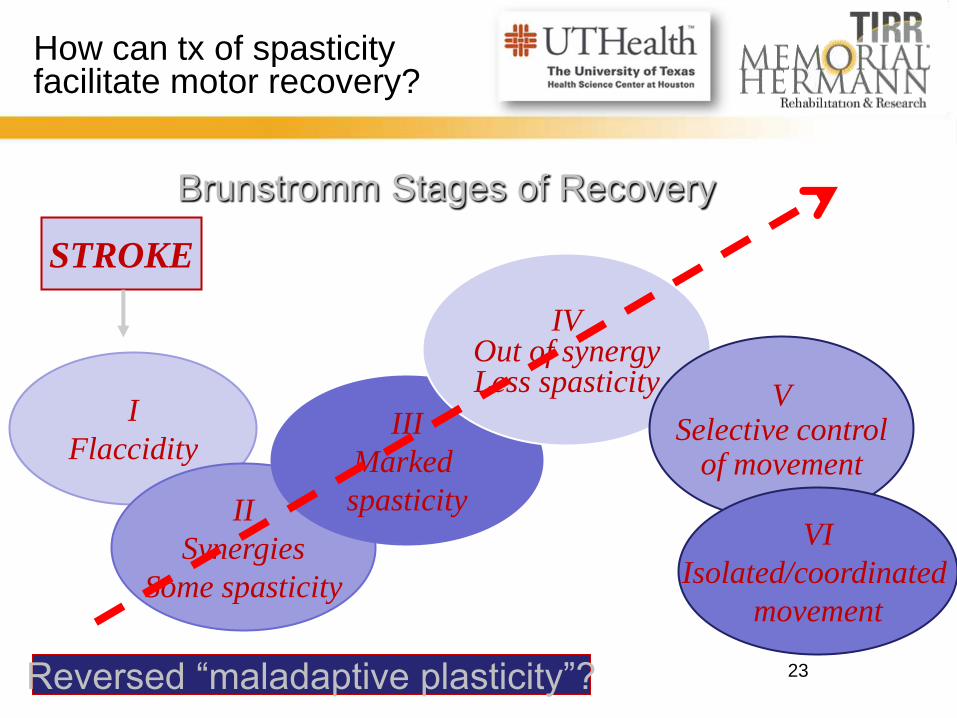
How can tx of spasticity facilitate motor recovery?
23
Brunstromm Stages of Recovery
STROKE
I
Flaccidity
II
Synergies
Some spasticity
III
Marked
spasticity
IV Out of synergy Less spasticity V
Selective control of movement
VI
Isolated/coordinated
movement
Reversed “maladaptive plasticity”?
24
Goal-Setting
PRIMARY EFFECTS
• Focus • Tone reduction
• Spasm reduction
• Locus • Central
• Peripheral
SECONDARY
EFFECTS
• Symptom Relief
• Correct Deficit • Exercise
• Compensation
• Restitution
25
Goal-Setting
Spasticity is not the reason for treatment.
Instead, it is the impact of spasticity on a
person’s well-being
Significance, not severity, of
spasticity should dictate need for
treatment
26
Management Starts with Goal-Setting
TECHNICAL
Decrease hypertonia
(Ashworth)
Decrease spasm
frequency and severity
Increase range of motion
FUNCTIONAL
“PASSIVE”
Facilitating wearing of
splints
Decreasing pain
associated with abnormal
posture and spasms
Improve nursing care
“ACTIVE”
Increase performance
OTHERS
Improve body image
27
Spasticity Management Interdisciplinary Approach
Pharmacologic
Functional Re-training
Physical Intervention
28
Spasticity Management
Assessment Goal-Setting Choice of Treatment
29
Management Options - Therapy
✦Therapeutic
Interventions: ✦Weight bearing
✦Serial Casting/Splinting
✦Locomotor Training
✦Positioning
✦E-stim
✦Strengthening
Medical Management should always be
supplemented by therapeutic management for
optimal improvement!
30
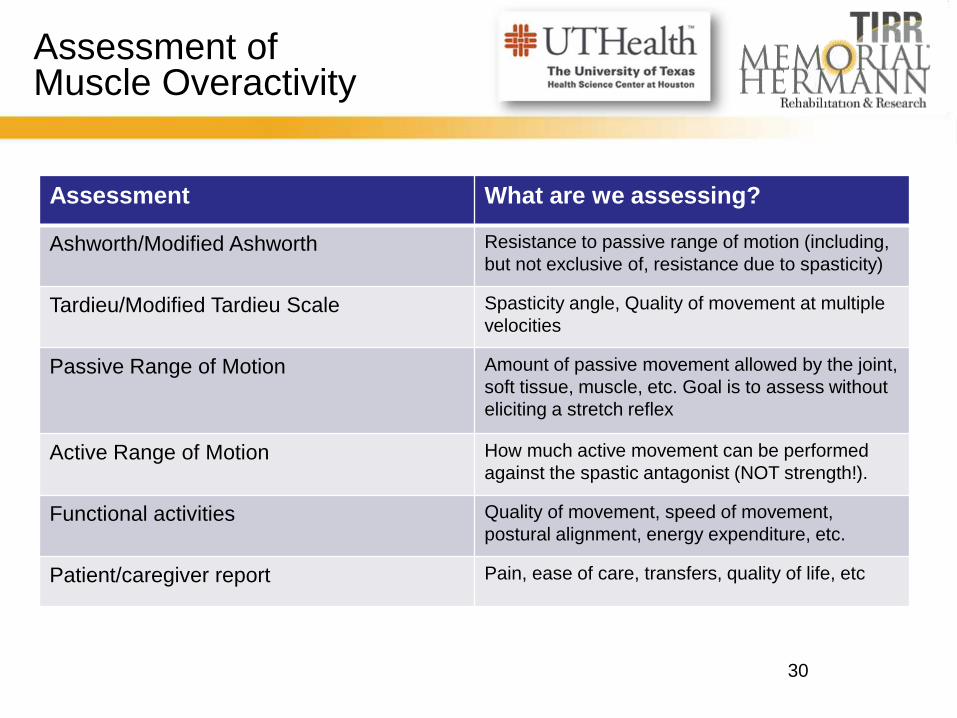
Assessment of Muscle Overactivity
Assessment What are we assessing?
Ashworth/Modified Ashworth Resistance to passive range of motion (including,
but not exclusive of, resistance due to spasticity)
Tardieu/Modified Tardieu Scale Spasticity angle, Quality of movement at multiple
velocities
Passive Range of Motion Amount of passive movement allowed by the joint,
soft tissue, muscle, etc. Goal is to assess without
eliciting a stretch reflex
Active Range of Motion How much active movement can be performed
against the spastic antagonist (NOT strength!).
Functional activities Quality of movement, speed of movement,
postural alignment, energy expenditure, etc.
Patient/caregiver report Pain, ease of care, transfers, quality of life, etc
31
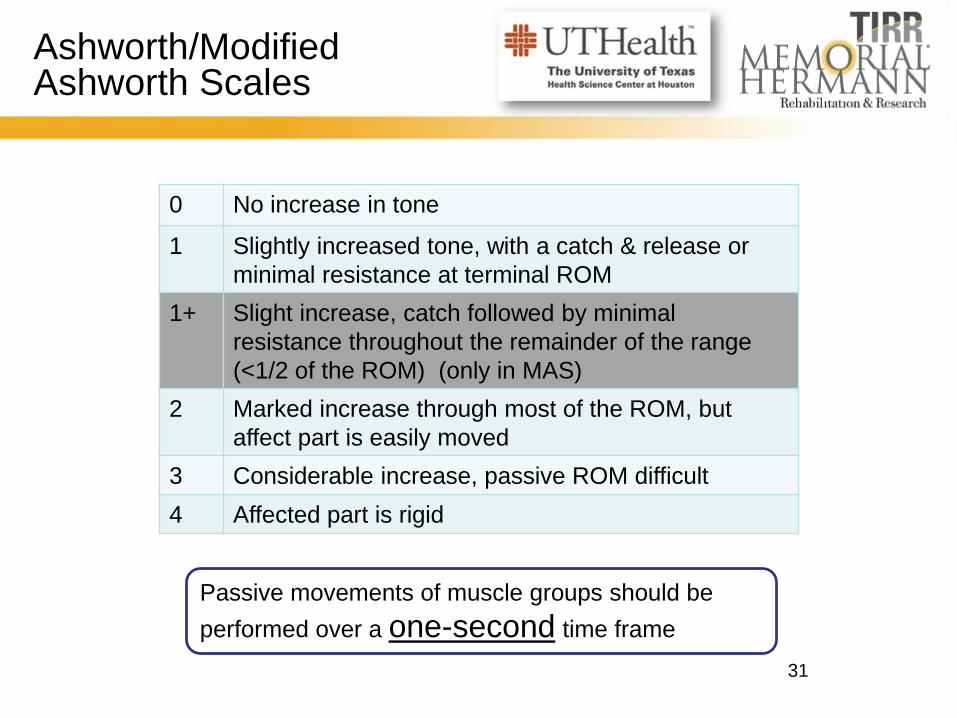
Ashworth/Modified Ashworth Scales
0 No increase in tone
1 Slightly increased tone, with a catch & release or
minimal resistance at terminal ROM
1+ Slight increase, catch followed by minimal
resistance throughout the remainder of the range
(<1/2 of the ROM) (only in MAS)
2 Marked increase through most of the ROM, but
affect part is easily moved
3 Considerable increase, passive ROM difficult
4 Affected part is rigid
Passive movements of muscle groups should be
performed over a one-second time frame
32
Ashworth/Modified Ashworth Scales
33
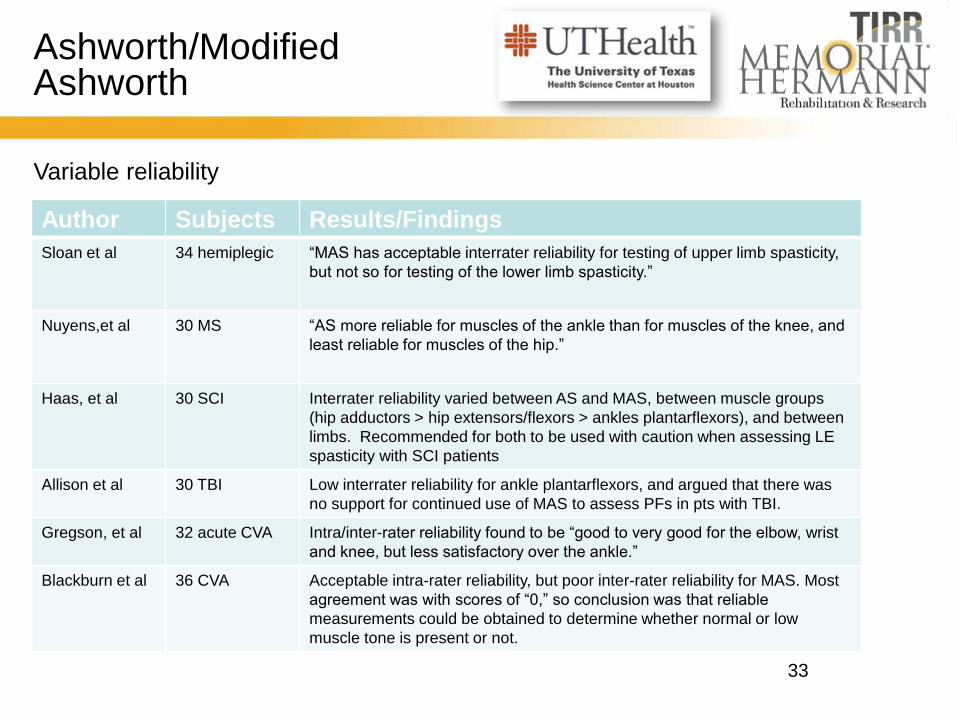
Ashworth/Modified Ashworth
Variable reliability
Author Subjects Results/Findings
Sloan et al
34 hemiplegic “MAS has acceptable interrater reliability for testing of upper limb spasticity,
but not so for testing of the lower limb spasticity.”
Nuyens,et al 30 MS “AS more reliable for muscles of the ankle than for muscles of the knee, and
least reliable for muscles of the hip.”
Haas, et al 30 SCI Interrater reliability varied between AS and MAS, between muscle groups
(hip adductors > hip extensors/flexors > ankles plantarflexors), and between
limbs. Recommended for both to be used with caution when assessing LE
spasticity with SCI patients
Allison et al 30 TBI Low interrater reliability for ankle plantarflexors, and argued that there was
no support for continued use of MAS to assess PFs in pts with TBI.
Gregson, et al 32 acute CVA Intra/inter-rater reliability found to be “good to very good for the elbow, wrist
and knee, but less satisfactory over the ankle.”
Blackburn et al 36 CVA Acceptable intra-rater reliability, but poor inter-rater reliability for MAS. Most
agreement was with scores of “0,” so conclusion was that reliable
measurements could be obtained to determine whether normal or low
muscle tone is present or not.
34
“The results...are clear and tell us the Ashworth Scale has insufficient
validity and reliability to be used as a measure of spasticity. However, we
are left with the problem of how to measure spasticity in a valid and
reliable way. The quest for this holy grail is ongoing.”
- Katharina S Sunnerhagen
So what else can we use??
35
Modified Tardieu Scale
Developed by Tardieu as a way to assess the velocity component of
spasticity in 1950s, modified by Boyd and Graham
Measures spasticity using two parameters
The spasticity angle
The spasticity grade
May be more useful to clinicians in
assessing functional implications of
spasticity, as well as effects of treatment
36
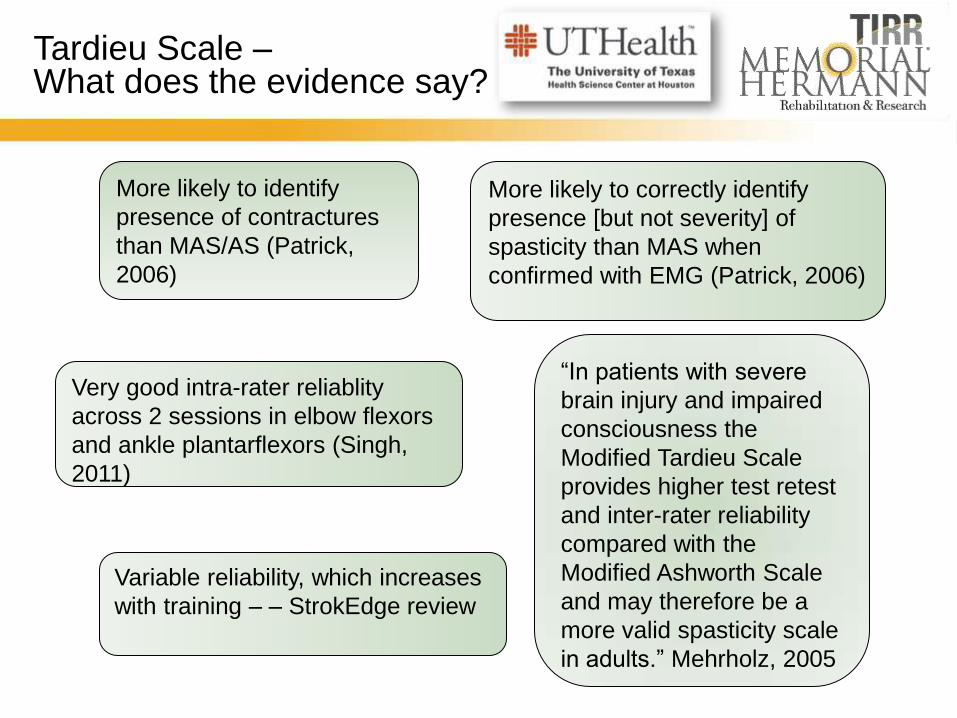
Tardieu Scale – What does the evidence say?
More likely to identify
presence of contractures
than MAS/AS (Patrick,
2006)
More likely to correctly identify
presence [but not severity] of
spasticity than MAS when
confirmed with EMG (Patrick, 2006)
Very good intra-rater reliablity
across 2 sessions in elbow flexors
and ankle plantarflexors (Singh,
2011)
“In patients with severe
brain injury and impaired
consciousness the
Modified Tardieu Scale
provides higher test retest
and inter-rater reliability
compared with the
Modified Ashworth Scale
and may therefore be a
more valid spasticity scale
in adults.” Mehrholz, 2005
Variable reliability, which increases
with training – – StrokEdge review
37
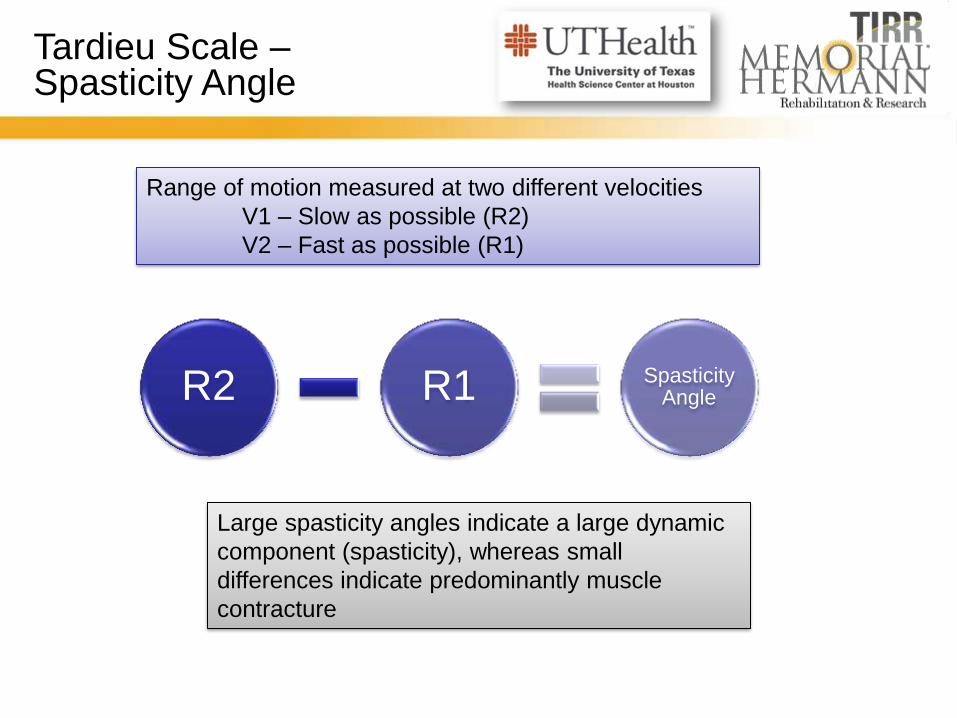
Tardieu Scale – Spasticity Angle
Range of motion measured at two different velocities
V1 – Slow as possible (R2)
V2 – Fast as possible (R1)
R2 R1 Spasticity Angle
Large spasticity angles indicate a large dynamic
component (spasticity), whereas small
differences indicate predominantly muscle
contracture
38
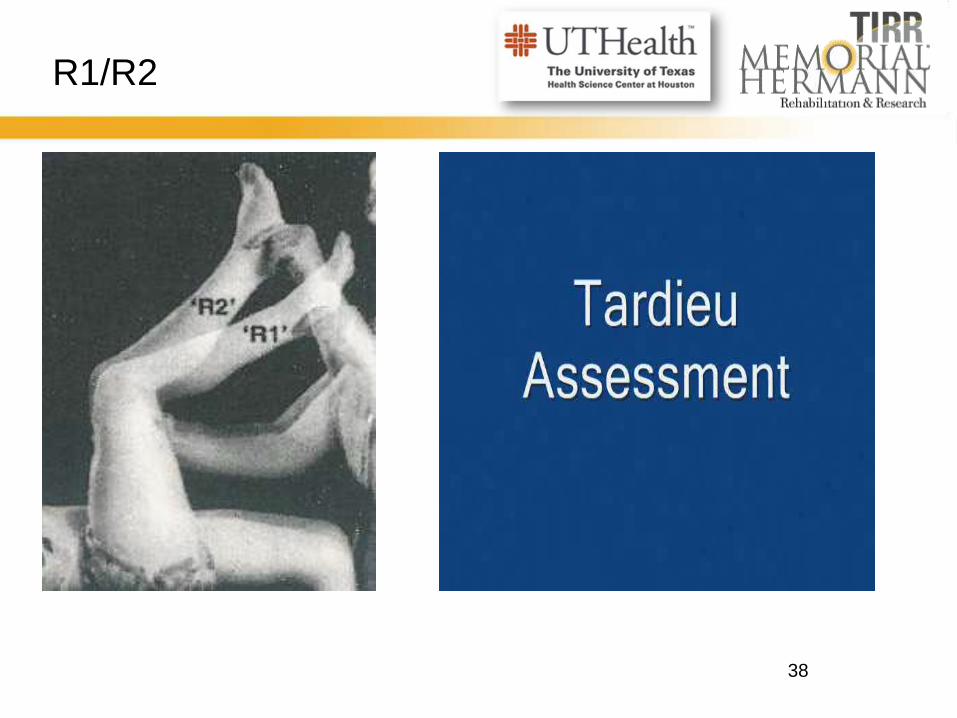
R1/R2
R2 R1
39
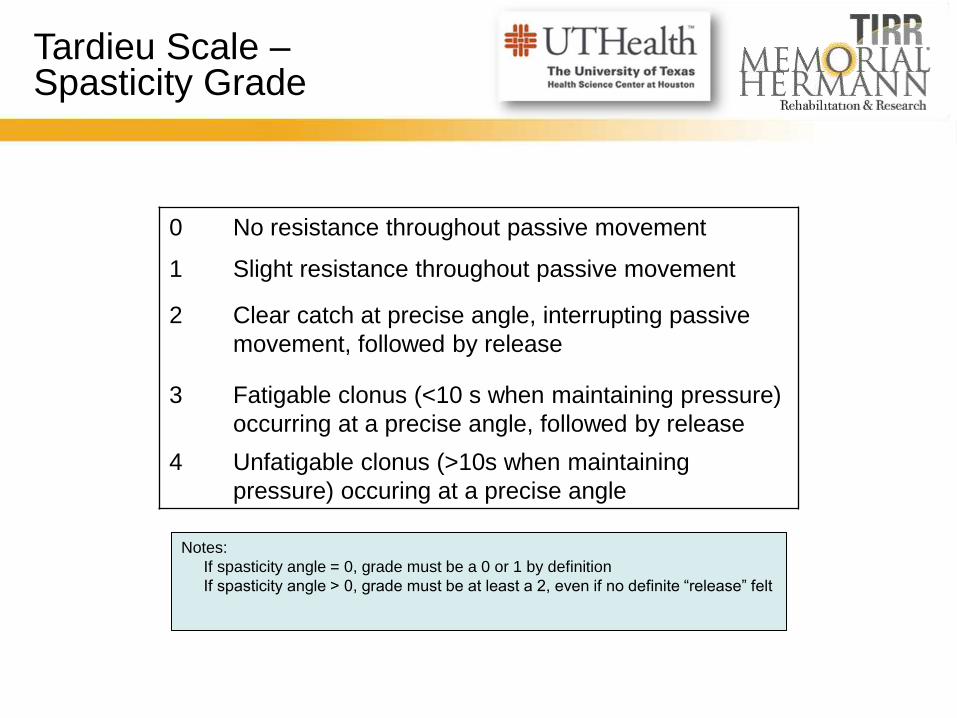
Tardieu Scale – Spasticity Grade
0 No resistance throughout passive movement
1 Slight resistance throughout passive movement
2 Clear catch at precise angle, interrupting passive
movement, followed by release
3 Fatigable clonus (<10 s when maintaining pressure)
occurring at a precise angle, followed by release
4 Unfatigable clonus (>10s when maintaining
pressure) occuring at a precise angle
Notes:
If spasticity angle = 0, grade must be a 0 or 1 by definition
If spasticity angle > 0, grade must be at least a 2, even if no definite “release” felt
40
Active Range of Motion
Objective measure of how much the agonist can move against
the overactive antagonist
Example – To assess overactive biceps, we could measure the
degrees of active extension that a patient can achieve.
NOT looking at the strength of the extensors, but rather how
much the overactivity of the flexors can be overcome
Following treatment, would want to reassess to see if the
patient can achieve more active movement,
May be a more functional measurement than passive
measurements
41
Functional Evaluation
Ask Questions! How is this impacting their lives? Severity ≠ Significance
What are their goals of treatment?
Observe! Watch them walk, transfer, propel w/c, eat, dress, etc
How are they positioned?
Video, video, video!!
Be Objective when you can! Use measures such as 10MWT, Gaitrite
asssessment, Modified Frenchay Arm Test, Disability
Assessment Scale
42
Other Assessments
Penn Spasm Frequency Scale
Timed repeated contractions
Barry Albright Dystonia Scale
43
Summary
Clinicians often focus on the direct effects of spasticity;
however, it is the indirect/disabling effects of spasticity
that most impact patients’ daily life
Effective rehabilitation consists of appropriate
assessment, and an individualized, interdisciplinary
approach that may incorporate both pharmacologic and
nonpharmacologic treatments
Spasticity and other chronic stroke complications should
be assessed and managed on a continual basis to
sustain functional gains
44
References
• www.wemove.org
• Lance JW, Feldman RG, Young RR, Koeller C. Spasticity: disorder of motor control. Chicago, IL:
Year Book Medical; 1980.
• Gracies JM. Pathophysiology of spastic paresis. I: Paresis and soft tissue changes. Muscle Nerve
2005;31:535-51.
• Gracies JM. Pathophysiology of spastic paresis. II: Emergence of muscle overactivity. Muscle
Nerve 2005;31:552-71
• Barnes MP. An overview of the clinical management of spasticity. In: Barnes MP, Johnson GR,
editors. Upper motor neurone syndrome and spasticity. Clinical management and
neurophysiology. Cambridge: Cambridge University Press; 2001. pp 1 – 11
• Patrick E, Ada L. The Tardieu Scale differentiates contracture from spasticity whereas the
Ashworth Scale is confounded by it. Clinical Rehabilitation. 2006;20(2):173–181.
• Gracies JM, Burke K, Clegg NJ, Browne R, Rushing C, Fehlings D et al. Reliability of the Tardieu
Scale for assessing spasticity in children with cerebral palsy. Arch Phys Med Rehabil
2010;91:421-8.
• Pandyan AD, Johnson GR, Price CI, Curless RH, Barnes MP, Rodgers H. A review of the
properties and limitations of the Ashworth and modified Ashworth Scales as measures of
spasticity. Clin Rehab 1999;13(5):373 – 383.
• Haugh AB, Pandyan AD, and Johnson GR. A systematic review of the Tardieu Scale for the
measurement of spasticity. Disability and Rehabilitation 2006; 28(15): 899-907
45
References
• Sloan RL, Sinclair E, Thompson J, Taylor S, Pentland B. Inter-rater reliability of the modified
Ashworth Scale for spasticity in hemiplegic patients. Int J Rehabil Res 1992; 15: 158–61.
• Allison SC, Abraham LD, Petersen CL. Reliability of the modified Ashworth Scale in the
assessment of plantar flexor muscle spasticity in patients with traumatic brain injury. Int J Rehabil
Res 1996; 19:67–78.
• Hass BM, Bergstrom E, Jamous A, Bennie A. The inter-rater reliability of the original and of the
modified Ashworth Scale for the assessment of spasticity in patients with spinal cord injury.
Spinal Cord 1996; 34: 560–64.
• Nuyens G, De Weerdt W, Ketelaer P et al. Interrater reliability of the Ashworth Scale in multiple
sclerosis. Clin Rehabil 1994; 8: 286–92.
• Blackburn M, van Vliet P, Mockett SP: Reliability of measurements obtained with the Modified
Ashworth Scale in the lower extremities of people with stroke. Phys Ther 2002;82:25–34.
• Gregson JM, Leathley M, Moore AP, et al: Reliability of the Tone Assessment Scale and the
Modified Ashworth Scale as clinical tools for assessing poststroke spasticity. Arch Phys Med
Rehabil 1999;80:1013–1016.
• Fleuren JFM, Voerman GE, Erren-Wolters CV, et al. Stop using the Ashworth Scale for the
assessment of spasticity. J Neurol Neurosurg Psychiatry 2010;81:46–53.
• Platz T, Eickhof C, Nuyens G, Vuadens P. Clinical scales for the assessment of spasticity,
associated phenomena, and function: a systematic review of the literature. Disabil Rehabil
2005;27(1-2):7-18.

46
References
• Biering-Sørensen F, Nielsen JB, Klinge K. Spasticity-assessment: a review. Spinal Cord 2006;
44:708-722
• American Physical Therapy Association, Neurology Section. StokEdge Documents.
http://www.neuropt.org/files/StrokeEDGE_Taskforce_Summary_Document.pdf
• Sunnerhagen, K. Stop Using the Ashworth scale for the assessment of spastisity [letter]. J Neurol
Neurosurg Psychiatry 2010. 81:2
• Singh P, Joshua A, Ganeshan S, Suresh S. Intra-rater reliability of the modified Tardieu scale to
quantify spasticity in elbow flexors and ankle planta flexors in adult stroke subjects. Annals of
Indian Academy of Neurology 2011. 14(1): 23-36
• Adams M, Hicks A. Comparison of the effects of body-weight-supported treadmill training and tilt-
table standing on spasticity in individuals with chronic spinal cord injury. J Spinal Cord Med. 2011;
34(5): 488-94
• Francisco G, Boake C. Improvement in Walking Speed in Poststroke Spastic Hemiplegia After
Intrathecal Baclofen Therapy: A premliinary Study. Arch Phys Med Rehabil . 2003; 84: 1194-99
• Park E, Rha D, Yoo J, Kim S, Chang W, Song S. Short-term Effects of Combined Serial Casting
and Botulinum Toxin Injextion for Spasitc Equinus in Ambulatory Children with Cerbral Palsy.
Yonsei Medical Journal. 2010; 51(4): 579-584
• Yaser E, Tok F, Balaban B, Yilmaz B, Alaca R. The efficacy of serial casting after botulinum toxin
type A injection in improving equinovarus deformity in patients with chronic stroke. Brain Injury.
2010. 24(5): 736-739
47
References
• Verplancke D, Snape S, Salisbury C, Jones P, Ward A. A randomized controlled trial of
botulinum toxin on lower limb spasticity following acute acquired severe brain injury. Clinical
Rehabilitation. 2005. 19(2): 117-125
• Schuhfried O, Crevenna R, Fialka-Moser V, Paternostro-Sluga T. Non-Invasive Neuromuscular
Electrical Stimulation in Patients with Central Nervous System Lesions: An Educational Review.
Journal of Rehabilitation Medicine. 2011. 44(2); 99-105
• Pak S, Patten C. Strengthening to Promote Functional Recovery Poststroke: An Evidence-Based
Review. Top Stroke Rehabil 2008. 15(3):177-199
• Bohannon R, Larkin P, Smith M, Horton M. Relationship Between Satic Muscle Strength Deficits
and Spasticity in Stroke Patients with Hemiparesis. Physical Therapy 1987. 67:1068-1071
48
Additional Resources
• Chou R, Peterson K, Helfand M. Comparative efficacy and safety of skeletal muscle relaxants for
spasticity and musculoskeletal conditions: a systematic review. J Pain Symptom Manage
2004;28:140-175.
• Cutter NC, Scott DD, Johnson JC, Whiteneck G. Gabapentin effect on spasticity in multiple
sclerosis: a placebo-controlled, randomized trial. Arch Phys Med Rehabil 2000;81:164-169.
• Dario A, Tomei G. A benefit-risk assessment of baclofen in severe spinal spasticity. Drug Saf
2004;27:799-818.
• Elovic EP, Simone LK, Zafonte R. Outcome assessment for spasticity management in the patient
with traumatic brain injury: the state of the art. J Head Trauma Rehabil 2004;19:155-177.
• Elovic E, Zafonte RD: Spasticity management in traumatic brain injury. Phys Med Rehabil State
Art Rev 2001; 15: 327-348.
• Esquenazi A, Mayer NH. Instrumented assessment of muscle overactivity and spasticity with
dynamic polyelectromyographic and motion analysis for treatment planning. Am J Phys Med
Rehabil 2004;83:S19-S29.
• Francis HP, Wade DT, Turner-Stokes L, Kingswell RS, Dott CS, Coxon EA. Does reducing
spasticity translate into functional benefit? An exploratory meta-analysis. J Neurol Neurosurg
Psychiatry 2004;75:1547-1551.
• Gooch JL, Patton CP. Combining botulinum toxin and phenol to manage spasticity in children.
Arch Phys Med Rehabil 2004;85:1121-1124.
49
• Good DC. Measurement of spasticity. In: Gelber DA, Jeffrey DR, eds. Clinical Evaluation and
Management of Spasticity. Totowa, NJ: Humana Press; 2002:27-44
• Heythaler, Jay, ed: Spastic Hypertonia. Physical Medicine and Rehabilitation Clinics of North
America; Vol. 12, Number 4: November 2001.
• Ivanhoe CB, Reistetter TA. Spasticity: the misunderstood part of the upper motor neuron
syndrome. Am J Phys Med Rehabil 2004;83:S3-S9.
• Ivanhoe C, Francisco, G, McGuire J, Subramanian T, Grissom S. Intrathecal Baclofen
Management of Poststroke Spastic Hypertonia: Implications for Function and Quality of Life. Arch
Phys Med Rehabil 2006; 87: 1509-1515
• Keenan MAE, McDaid PJ. Orthopedic interventions for the management of limb deformities in
upper motoneuron syndromes. In: Gelber DA, Jeffrey DR, eds. Clinical Evaluation and
Management of Spasticity. Totowa, NJ: Humana Press; 2002:197-255.
• Kogler GF. Orthotic management. In: Gelber DA, Jeffrey DR, eds. Clinical Evaluation and
Management of Spasticity. Totowa, NJ: Humana Press; 2002:67-91.
• Leathley MJ, Gregson JM, Moore AP, Smith TL, Sharma AK, Watkins CL. Predicting spasticity
after stroke in those surviving to 12 months. Clin Rehabil 2004;18:438-443
• Meythaler JM, Clayton W, Davis LK, Guin-Renfroe S, Brunner RC. Orally delivered baclofen to
control spastic hypertonia in acquired brain injury. J Head Trauma Rehabil 19:101-8, 2004.
• Pierson SH. Physical and occupational approaches. In: Gelber DA, Jeffrey DR, eds. Clinical
Evaluation and Management of Spasticity. Totowa, NJ: Humana Press; 2002:47-66.
Additional Resources
50
• Rizzo MA, Hadjimichael OC, Preiningerova J, Vollmer TL. Prevalence and treatment of spasticity
reported by multiple sclerosis patients. Mult Scler 2004;10:589-595.
• Satkunam LE. Rehabilitation medicine: 3. Management of adult spasticity. CMAJ 2003;169:1173-
1179.
• Tilton AH. Approach to the rehabilitation of spasticity and neuromuscular disorders in children.
Neurol Clin 2003;21:853-881.
• Zackowski KM, Dromerick AW, Sahrmann SA, Thach WT, Bastian AJ. How do strength,
sensation, spasticity and joint individuation relate to the reaching deficits of people with chronic
hemiparesis? Brain 2004;127:1035-1046.
• Zafonte R, Elovic EP, Lombard L. Acute care management of post-TBI spasticity. J Head Trauma
Rehabil 2004;19:89-100.
• Zahavi A, Geertzen JH, Middel B, Staal M, Rietman JS. Long term effect (more than five years) of
intrathecal baclofen on impairment, disability, and quality of life in patients with severe spasticity
of spinal origin. J Neurol Neurosurg Psychiatry 2004;75:1553-1557.
Additional Resources
