associate professor of dermatology psoriasis and psa ... · pdf filekurd sk, et al. j am acad...
TRANSCRIPT

Psoriasis and PsAEpidemiology and Classification
April W. Armstrong, MD, MPHVice Chair of Clinical Research
Associate Professor of DermatologyDirector, Clinical Trials and Outcomes Research
Director, Psoriasis ProgramDepartment of Dermatology
Colorado Health Outcomes Program (COHO)University of Colorado Denver School of Medicine
Aurora, Colorado
Dafna D. Gladman MD, FRCPCProfessor of Medicine, University of Toronto
Senior Scientist, Toronto Western Research InstituteDirector, Psoriatic Arthritis Program
University Health NetworkToronto, Ontario, Canada
Philip Helliwell, MDLeeds Institute of Rheumatic and Musculoskeletal Medicine
University of LeedsChapel Allerton Hospital
Leeds, England
Content Developers
Luis R. Espinoza, MD
Professor and Chief
Section of Rheumatology
LSUHSC at New Orleans
New Orleans, Louisiana
Amit Garg, MD
Associate Professor and Founding Chair
Department of Dermatology
Hofstra NSLIJ School of Medicine
North Shore LIJ Health System
Manhasset, New York
Speakers Learning Objectives
• Describe epidemiology of psoriasis
• Examine impact of psoriasis on quality of life, work productivity, and under-treatment patterns.
• Describe epidemiology and classification of psoriatic arthritis.
• Examine factors contributing to disease progression and methods of screening for psoriatic arthritis.
Pre-Activity Question 1
How confident are you in your ability to discuss the classification of psoriatic arthritis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 2
How confident are you in your ability to discuss the epidemiology of psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident

Pre-Activity Question 3
Which of the following is NOT a disease activity-related predictor of disease progression for PsA?
1. Number of swollen joints
2. Number of tender joints
3. Initial ESR
4. Pain rating of 8 on visual analog scale
• United States– In 2010, prevalence of diagnosed
psoriasis was 3.2% in adults ≥20 yrs (NHANES)1
• ~7.5 million adults diagnosed with psoriasis
– Prevalence of undiagnosed active psoriasis2
• Conservative estimate: 0.4% (600,000 adults)
• Broad definition: 2.28% (3.6 million adults)
• Canada4
– Estimated 500,000 people affected
Prevalence of Psoriasis:North America
NHANES = National Health and Nutrition Examination Survey; NPF = National Psoriasis Foundation.1. Rachakonda TD, et al. J Am Acad Dermatol. 2013;70:512-516. 2. Kurd SK, et al. J Am Acad Dermatol. 2009;60:218-224. 3. National Psoriasis Foundation. http://www.psoriasis.org/about-psoriasis. Accessed August 29, 2014. 4. Canadian Dermatology Association. http://www.dermatology.ca/wp-content/uploads/2012/01/cdnpsoriasisguidelines.pdf. Accessed September 16, 2014.
Prevalence of Psoriasis:Europe and Russia
Parisi R, et al. J Invest Dermatol. 2013;133:377-385.
Italy 2.9%
Sweden 2.0%
Russia 0.72%
Norway 1.4%
Spain 1.43%
United Kingdom 1.48 %−1.87%
Denmark2.84%
Germany 2.0%−2.53%
Prevalence of Psoriasis: Africa and Asia
Sri Lanka<0.5%
China0.4%
Taiwan<0.5%
Africa<0.5%
Psoriasis Epidemiology
• Equal frequency in both genders
• Two peaks of occurrence
– At 20-30 years
– At 50-60 years
• 75% have onset before age 40
Impact of Psoriasis on HRQoL in Germany
• HRQoL measured by the DLQI score
• Psoriasis impacts patient HRQoL
• 34.1% of patients had very large or extremely large impairment of HRQoL (DLQI >10)
DLQI = dermatology life quality index; HRQoL = health-related quality of life.Augustin M, et al. Dermatology. 2008;216:366-372.
Overall PASI Score
Mild (≤10) Moderate (11-20) Severe (>20)
Patients 1511 / 1511 (100.0) 686 / 1341 (51.2) 395 / 1341 (29.5) 260 / 1341 (19.4)
No effect on HRQoL (0-1) 225 / 1481 (15.2) 143 / 666 (21.5) 39 / 392 (9.9) 12 / 256 (4.7)
Small effect (2-5) 427 / 1481 (28.8) 230 / 666 (34.5) 99 /392 (25.3) 38 / 256 (14.8)
Moderate effect (6-10) 324 / 1481 (21.9) 132 / 666 (19.8) 86 / 392 (21.9) 61 / 265 (23.8)
Very large effect (11-20) 385 / 1481 (26.0) 128 / 666 (19.2) 130 / 392 (33.2) 100 / 256 (39.1)
Extremely large effect (21-30) 120 / 1481 (8.1) 33 / 666 (5.0) 38 / 392 (9.7) 45 / 256 (17.6)
Impact of Psoriasis on Patients’ HRQoL measured by DLQI Scores in Relation to the Severity of Skin Lesions
Results are given as number/total with percentages in parentheses
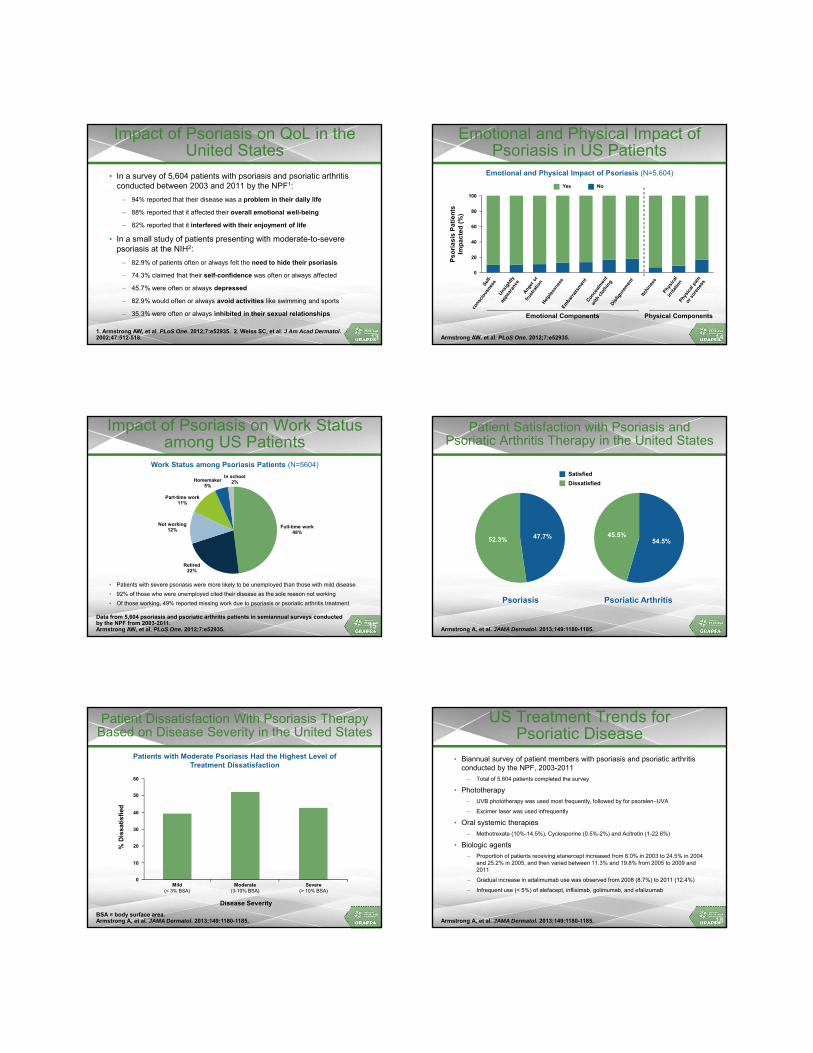
Impact of Psoriasis on QoL in the United States
• In a survey of 5,604 patients with psoriasis and psoriatic arthritis conducted between 2003 and 2011 by the NPF1:
– 94% reported that their disease was a problem in their daily life
– 88% reported that it affected their overall emotional well-being
– 82% reported that it interfered with their enjoyment of life
• In a small study of patients presenting with moderate-to-severe psoriasis at the NIH2:
– 82.9% of patients often or always felt the need to hide their psoriasis
– 74.3% claimed that their self-confidence was often or always affected
– 45.7% were often or always depressed
– 82.9% would often or always avoid activities like swimming and sports
– 35.3% were often or always inhibited in their sexual relationships
1. Armstrong AW, et al. PLoS One. 2012;7:e52935. 2. Weiss SC, et al. J Am Acad Dermatol. 2002;47:512-518. 13
Emotional and Physical Impact of Psoriasis in US Patients
Armstrong AW, et al. PLoS One. 2012;7:e52935. 14
Emotional Components Physical Components
Ps
ori
as
is P
ati
en
ts
Imp
ac
ted
(%
)
100
80
60
40
0
20
Emotional and Physical Impact of Psoriasis (N=5,604)
Yes No
Impact of Psoriasis on Work Status among US Patients
• Patients with severe psoriasis were more likely to be unemployed than those with mild disease
• 92% of those who were unemployed cited their disease as the sole reason not working
• Of those working, 49% reported missing work due to psoriasis or psoriatic arthritis treatment
15Data from 5,604 psoriasis and psoriatic arthritis patients in semiannual surveys conducted by the NPF from 2003-2011. Armstrong AW, et al. PLoS One. 2012;7:e52935.
Work Status among Psoriasis Patients (N=5604)
Full-time work48%
Retired22%
Not working12%
Part-time work11%
Homemaker5%
In school2%
Patient Satisfaction with Psoriasis and Psoriatic Arthritis Therapy in the United States
Armstrong A, et al. JAMA Dermatol. 2013;149:1180-1185.
54.5%45.5%47.7%52.3%
Psoriasis Psoriatic Arthritis
Satisfied
Dissatisfied
Patient Dissatisfaction With Psoriasis Therapy Based on Disease Severity in the United States
BSA = body surface area.Armstrong A, et al. JAMA Dermatol. 2013;149:1180-1185.
%D
iss
ati
sfi
ed
60
50
30
20
10
0
40
Disease Severity
Mild(< 3% BSA)
Severe(> 10% BSA)
Moderate(3-10% BSA)
Patients with Moderate Psoriasis Had the Highest Level ofTreatment Dissatisfaction
US Treatment Trends for Psoriatic Disease
• Biannual survey of patient members with psoriasis and psoriatic arthritis conducted by the NPF, 2003-2011
– Total of 5,604 patients completed the survey
• Phototherapy
– UVB phototherapy was used most frequently, followed by for psoralen–UVA
– Excimer laser was used infrequently
• Oral systemic therapies
– Methotrexate (10%-14.5%), Cyclosporine (0.5%-2%) and Acitretin (1-22.6%)
• Biologic agents
– Proportion of patients receiving etanercept increased from 8.0% in 2003 to 24.5% in 2004 and 25.2% in 2005, and then varied between 11.3% and 19.8% from 2005 to 2009 and 2011
– Gradual increase in adalimumab use was observed from 2008 (8.7%) to 2011 (12.4%)
– Infrequent use (< 5%) of alefacept, infliximab, golimumab, and efalizumab
Armstrong A, et al. JAMA Dermatol. 2013;149:1180-1185. 18
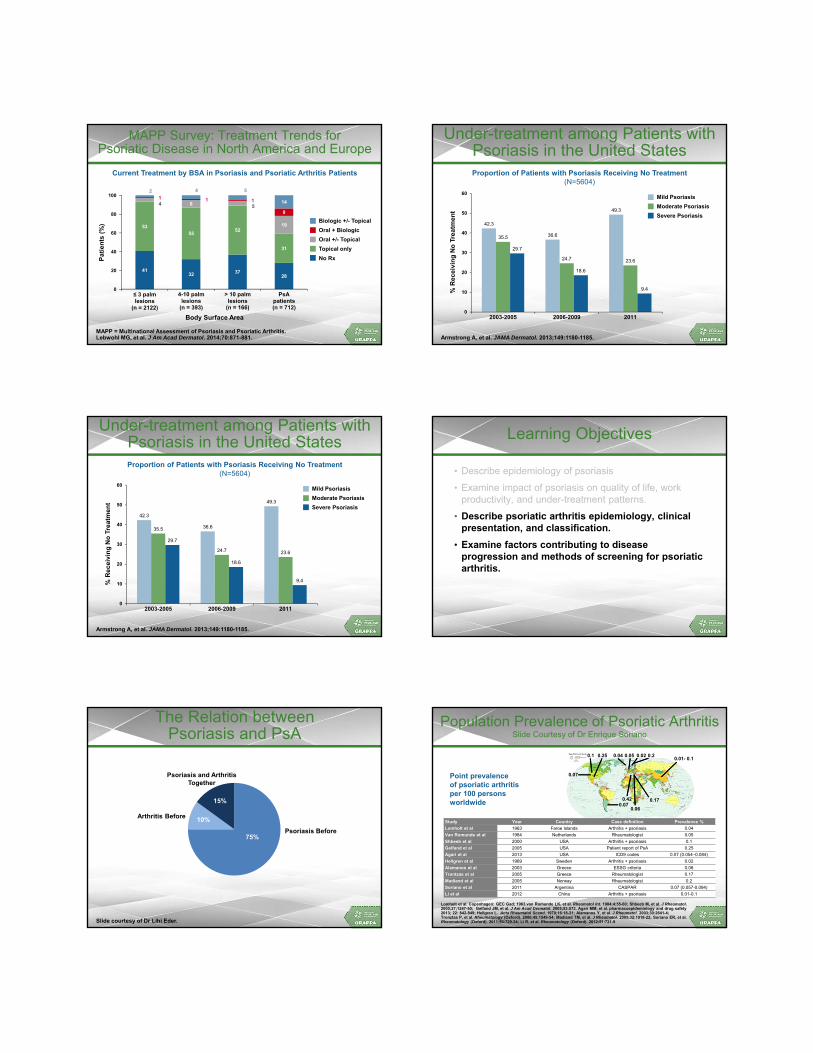
MAPP Survey: Treatment Trends for Psoriatic Disease in North America and Europe
MAPP = Multinational Assessment of Psoriasis and Psoriatic Arthritis.Lebwohl MG, et al. J Am Acad Dermatol. 2014;70:871-881.
4132 37
28
5355
52
31
4 8 5
19
1 1 1
8
2 4 5
14
≤ 3 palm lesions
(n = 2122)
4-10 palmlesions
(n = 393)
> 10 palmlesions
(n = 166)
PsApatients(n = 712)
Pa
tie
nts
(%
)
Body Surface Area
Current Treatment by BSA in Psoriasis and Psoriatic Arthritis Patients
Biologic +/- Topical
Oral + Biologic
Oral +/- Topical
Topical only
No Rx
100
80
60
40
0
20
Under-treatment among Patients with Psoriasis in the United States
Armstrong A, et al. JAMA Dermatol. 2013;149:1180-1185.
42.3
36.6
49.3
35.5
24.7 23.6
29.7
18.6
9.4
0
10
20
30
40
50
60
2003-2005 2006-2009 2011
Proportion of Patients with Psoriasis Receiving No Treatment (N=5604)
%R
ec
eiv
ing
No
Tre
atm
en
t
Mild Psoriasis
Moderate Psoriasis
Severe Psoriasis
Under-treatment among Patients with Psoriasis in the United States
Armstrong A, et al. JAMA Dermatol. 2013;149:1180-1185.
42.3
36.6
49.3
35.5
24.7 23.6
29.7
18.6
9.4
0
10
20
30
40
50
60
2003-2005 2006-2009 2011
Proportion of Patients with Psoriasis Receiving No Treatment (N=5604)
%R
ec
eiv
ing
No
Tre
atm
en
t
Mild Psoriasis
Moderate Psoriasis
Severe Psoriasis
Learning Objectives
• Describe epidemiology of psoriasis
• Examine impact of psoriasis on quality of life, work productivity, and under-treatment patterns.
• Describe psoriatic arthritis epidemiology, clinical presentation, and classification.
• Examine factors contributing to disease progression and methods of screening for psoriatic arthritis.
The Relation betweenPsoriasis and PsA
75%Psoriasis Before
Arthritis Before
Psoriasis and Arthritis Together
15%
10%
Slide courtesy of Dr Lihi Eder.
0.20.1 0.02 0.01- 0.1
0.04
0.06 0.07
0.17
0.25 0.05
0.42
0.07
Population Prevalence of Psoriatic ArthritisSlide Courtesy of Dr Enrique Soriano
Lomholt et al. Copenhagen: GEC Gad; 1963.van Romunde LK, et al. Rheumatol Int. 1984;4:55-60; Shbeeb M, et al. J Rheumatol. 2000;27;1247-50; Gelfand JM, et al. J Am Acad Dermatol. 2005;53:573. Agari MM, et al. pharmacoepidemiology and drug safety 2013; 22: 842-849; Hellgren L. Acta Rheumatol Scand. 1970;16:18-21; Alamanos Y, et al. J Rheumatol. 2003;30:2641-4; Tronztas P, et al. Rheumatology (Oxford). 2006;45:1549-54; Madland TM, et al. J Rheumatol. 2005;32:1918-22; Soriano ER, et al. Rheumatology (Oxford). 2011;50:729-34; Li R, et al. Rheumatology (Oxford). 2012;51:721-9
Study Year Country Case definition Prevalence %
Lomholt et al 1963 Faroe Islands Arthritis + psoriasis 0.04
Van Romunde et al 1984 Netherlands Rheumatologist 0.05
Shbeeb et al 2000 USA Arthritis + psoriasis 0.1
Gelfand et al 2005 USA Patient report of PsA 0.25
Agari et al 2013 USA ICD9 codes 0.07 (0.054–0.084)
Hellgren et al 1969 Sweden Arthritis + psoriasis 0.02
Alamanos et al 2003 Greece ESSG criteria 0.06
Trontzas et al 2005 Greece Rheumatologist 0.17
Madland et al 2005 Norway Rheumatologist 0.2
Soriano et al 2011 Argentina CASPAR 0.07 (0.057-0.094)
Li et al 2012 China Arthritis + psoriasis 0.01-0.1
Point prevalence of psoriatic arthritis per 100 persons worldwide

Prevalence of PsA amongPeople with Psoriasis
Author (yr) Centre No. Psoriasis Patients % PsA
Leczinsky (1948) Sweden 534 7
Vilanova (1951) Barcelona 214 25
Little (1975) Toronto 100 32
Scarpa (1984) Napoli 180 34
Stern (1985) Boston 1285 20
Zaneli (1992) Winston-Salem 459 17
Barisic-Drusko (1994) Osijek region 553 10
Salvarani (1995) Regio Emilia 205 36
Shbeeb (2000) Mayo Clinic 1056 6.25
Brockbank (2001) Toronto 126 31
Alenius (2002) Sweden 276 48
NPF (2002) US 4.4 m 23
Zachariae (2003) Denmark 5795 30
Reich (2008) Germany 1511 20.6
Haroon (2013) Dublin 100 29
Walsh (2013) Utah 189 30
Mease (2013) International 1000 30
Incidence of PsA – 2011
• 10 / 313 psoriasis patients developed PsA within 4 years of follow-up
• The annual incidence rate was 1.87 PsA cases per 100 psoriasis patients
– Assuming patients not followed did not develop PsA
• The incidence rate increased to 2.53 when only the 253 participants with at least one follow-up were included
Eder E, et al. Arthritis Care Res. 2011;63:619-22.
Exponential model shows a constanthazard rate
KM
Exp0.25
0.20
0.30
0.15
0.10
0.05
0
0 1 2 3 4
Pro
bab
ilit
y o
f D
evel
op
ing
PsA
Time from First Visit to Diagnosis of PsA (year)
23.16.6 6.1
0.1
8
3 6.3
Population Incidence of Psoriatic ArthritisSlide Courtesy of Dr Enrique Soriano
Kaipiainen-Seppänen O. Br J Rheumatol. 1996;35:1289-91; Shbeeb M, et al. J Rheumatol. 2000;27;1247-50; Hukuda S, et al. J Rheumatol. 2001;28:554-9; Soderlin MK, et al. Ann Rheum Dis. 2002;61:911-5; Alamanos y, et al. J Rheumatol. 2003;30:2641-4; Savolainen E, et al. J Rheumatol. 2003;30:2460-8; Wilson FC. Ann Rheum Dis. 2009; 36(2):361-367. Soriano ER, et al. Rheumatology (Oxford). 2011;50:729-34.
Study Year Country Case definitionAnnual Incidence cases/105
(95% confidence interval)
Kaipianinen-Seppanen et al 1996 Finland Arthritis + psoriasis 6.1 (4.6–7.6)
Shbeeb et al 2000 USA Arthritis + psoriasis 6.6 (5.0–8.2)
Hukuda et al 2001 Japan Arthritis + psoriasis 0.1
Soderlin et al 2002 Sweden Arthritis + psoriasis 8 (4–15)
Alamanos et al 2003 Greece ESSG criteria 3.0 (1.6–4.5)
Savolainen et al 2003 Finland Arthritis + psoriasis 23.1 (13.2–37.5)
Wilson et al 2009 USA CASPAR 7.2 (6–8.)
Soriano et al 2011 Argentina CASPAR 6.3 (4.2–8.3)
7.2 Annual incidence of psoriatic arthritis per 100,000 persons worldwide
Psoriatic Arthritis
• An inflammatory musculoskeletal disease associated with psoriasis
• Usually seronegative for rheumatoid factor
• Associated Features
– Spondylitis
– Enthesitis
– Dactylitis
– Iritis
– Mucous membrane ulcers
– Urethritis
– Other extra-articular features of SpA
• Classified as SpA
Psoriatic Arthritis Clinical Patterns
• Distal predominant (Distal inter-phalangeal joints of fingers and toes)
• Oligo-articular (<5 joints) often in an asymmetric distribution
• Poly-articular (≥5 joints), rheumatoid arthritis-like
• Spinal Involvement
• ‘Arthritis Mutilans’
Moll & Wright. Seminars Arthritis Rheum. 1973;32:181.
Psoriatic Arthritis
• Peripheral arthritis
• Axial arthritis
• Peripheral plus Axial
• Patterns change over time
• Early PsA
– 40% oligoarticular
– 60% polyarticular
Jones SM, et al. Br J Rheum. 1994;33:834-9. Khan M, et al. J Rheumatol. 2003;30:1022-1026. Kane D, et al. ARD. 2003;42:1460-1468.
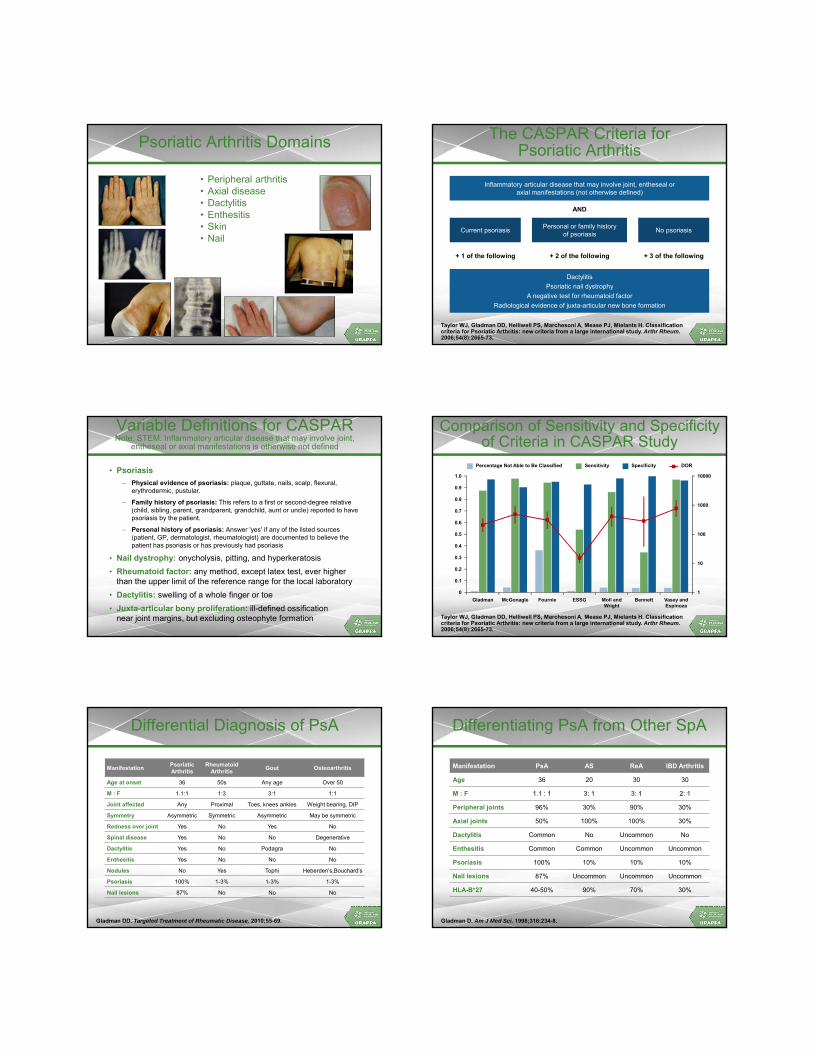
Psoriatic Arthritis Domains
• Peripheral arthritis• Axial disease• Dactylitis• Enthesitis• Skin• Nail
The CASPAR Criteria forPsoriatic Arthritis
Taylor WJ, Gladman DD, Helliwell PS, Marchesoni A, Mease PJ, Mielants H. Classification criteria for Psoriatic Arthritis: new criteria from a large international study. Arthr Rheum. 2006;54(8):2665-73.
Inflammatory articular disease that may involve joint, entheseal oraxial manifestations (not otherwise defined)
Personal or family historyof psoriasis
No psoriasisCurrent psoriasis
Dactylitis
Psoriatic nail dystrophy
A negative test for rheumatoid factor
Radiological evidence of juxta-articular new bone formation
+ 2 of the following + 3 of the following+ 1 of the following
AND
Variable Definitions for CASPAR Note: STEM: Inflammatory articular disease that may involve joint,
entheseal or axial manifestations is otherwise not defined
• Psoriasis
– Physical evidence of psoriasis: plaque, guttate, nails, scalp, flexural, erythrodermic, pustular.
– Family history of psoriasis: This refers to a first or second-degree relative (child, sibling, parent, grandparent, grandchild, aunt or uncle) reported to have psoriasis by the patient.
– Personal history of psoriasis: Answer 'yes' if any of the listed sources (patient, GP, dermatologist, rheumatologist) are documented to believe the patient has psoriasis or has previously had psoriasis
• Nail dystrophy: onycholysis, pitting, and hyperkeratosis
• Rheumatoid factor: any method, except latex test, ever higher than the upper limit of the reference range for the local laboratory
• Dactylitis: swelling of a whole finger or toe
• Juxta-articular bony proliferation: ill-defined ossification near joint margins, but excluding osteophyte formation
Comparison of Sensitivity and Specificity of Criteria in CASPAR Study
Taylor WJ, Gladman DD, Helliwell PS, Marchesoni A, Mease PJ, Mielants H. Classification criteria for Psoriatic Arthritis: new criteria from a large international study. Arthr Rheum. 2006;54(8):2665-73.
Gladman
1.0
0.9
0.6
0.4
0.3
0.2
0
0.1
0.8
0.5
10000
1000
10
1
100
McGonagle Fournie ESSG Moll andWright
Bennett Vasey andEspinoza
0.7
SensitivityPercentage Not Able to Be Classified Specificity DOR
Differential Diagnosis of PsA
ManifestationPsoriatic Arthritis
Rheumatoid Arthritis
Gout Osteoarthritis
Age at onset 36 50s Any age Over 50
M : F 1.1:1 1:3 3:1 1:1
Joint affected Any Proximal Toes, knees ankles Weight bearing, DIP
Symmetry Asymmetric Symmetric Asymmetric May be symmetric
Redness over joint Yes No Yes No
Spinal disease Yes No No Degenerative
Dactylitis Yes No Podagra No
Enthesitis Yes No No No
Nodules No Yes Tophi Heberden’s,Bouchard’s
Psoriasis 100% 1-3% 1-3% 1-3%
Nail lesions 87% No No No
Gladman DD. Targeted Treatment of Rheumatic Disease. 2010;55-69.
Differentiating PsA from Other SpA
Manifestation PsA AS ReA IBD Arthritis
Age 36 20 30 30
M : F 1.1 : 1 3: 1 3: 1 2: 1
Peripheral joints 96% 30% 90% 30%
Axial joints 50% 100% 100% 30%
Dactylitis Common No Uncommon No
Enthesitis Common Common Uncommon Uncommon
Psoriasis 100% 10% 10% 10%
Nail lesions 87% Uncommon Uncommon Uncommon
HLA-B*27 40-50% 90% 70% 30%
Gladman D. Am J Med Sci. 1998;316:234-8.

Learning Objectives
• Describe psoriasis epidemiology and clinical presentation
• Examine impact of psoriasis on quality of life, work productivity, and under-treatment patterns.
• Describe psoriatic arthritis epidemiology, clinical presentation, and classification.
• Examine factors contributing to disease progression and methods of screening for psoriatic arthritis.
PsA Is Much More Serious than Previously Recognized
• 20% with PsA develop clinical deformities and damage, resulting in functional disability
• Gladman DD, et al. Quart J Med 1987;62:127-41
• After 10 years of follow-up, 55% have ≥ 5 deformed joints
• Gladman DD. Baillière’s Clinical Rheumatology 1994;8:379-94
• 27% with early PsA had at least 1 erosion at presentation to clinic
• 47% developed erosive disease within the first 2 years
• Kane D, et al, Rheumatology, 2003; 42:1460-8
Comparing Psoriatic Arthritis to Rheumatoid Arthritis
• Established secondary care cohort
• Patients matched for age and sex and date of diagnosis
1.6
0.9
0.5
2
1.3
0.9
0.6
2
0
0.5
1
1.5
2
2.5
HAQ PainVAS/10
EQ5D x 10 SteinB
RA PsA
39
118
4
0
5
10
15
20
25
30
35
40
45
Hand Feet
RA PsA
Sokoll KB, Helliwell PS. Comparison of disability and quality of life in rheumatoid and psoriatic arthritis. J Rheumatol. 2001;28:1842–6.
Lar
sen
sco
re
Mea
n v
alu
e
HAQ and EQ5D by Psoriasis Severity
Sokoll KB, Helliwell PS. Comparison of disability and quality of life in rheumatoid and psoriatic arthritis.J Rheumatol. 2001;28:1842–6.
1.6
0.5
0.80.7
1.4
0.5
2
0.4
0
0.5
1
1.5
2
2.5
HAQ EQ5D
RA
Mild
Moderate
Severe
Me
an
va
lue
Progression of Joint Damage in PsA
Siannis F, et al. Ann Rheum Dis. 2006;65:478-481.
Clinical
Radiological0.8
0.7
1.0
0.9
0.6
0.5
0.4
0.3
0.2
0
0.1
0 5 10 15 20 25 30
Pro
po
rtio
n
Time since Clinical Entry (years)
Clinical Predictors of Progression
• Disease Activity
– Number of swollen joints
– Number of tender joints
– Initial ESR
• Damage
– Number of damaged joints
• Tenderness or swelling of a specific joint predicts subsequent damage to that joint
• Digits with dactylitis are more likely to have erosive disease than digits without dactylitis
Bond S, et al. Ann Rheum Dis. 2007;66:370-6. Cresswell L, et al. Ann Rheum Dis. 2011;70:305-8. Brockbank J, et al. Ann Rheum Dis. 2005;64:188-90.

Genetic Markers forProgression of Damage
• Progression of Clinical Damage– HLA-B27 antigen (with HLA-DR7), HLA-B*27 allele
– HLA-B39 antigen, HLA-B*39 allele
– HLA-DQw3 in the absence of HLA-DR7
– KIR2DS1
• Erosive PsA– HLA-DRB1 rheumatoid arthritis ‘shared epitope’
– IL-4 I50V
• Less Progression– HLA-DR7, HLA-DRB1*07
– HLA-B22
– HLA-C*06
Gladman DD, et al. Arthritis Rheum. 1995;38:845-50; Gladman DD, et al. J Rheumatol. 1998;25:730-3. Rahman P, et al. Arthritis Rheum. 2008;58:2207-8; Korendowych E, et al. J Rheumatol. 2003;30:96-10. Ho PY, et al. Ann Rheum Dis. 2007;66:807-11; Chandran V, et al. Hum Immunol. 2013;74:1333-8; Chandran V, et al. Rheumatology. 2014;53:233-9.
Multivariate Analysis* of Predictors ofClinical Damage: Effect of Disease Duration
VariableRelative Rate (95% CI) of
Joint Damage ProgressionP-value
Group** (PsA >2 yrs vs. PsA≤ 2 yrs) 1.62 (1.28,2.03) <.0001
Age 1.02 (1.01,1.03) <.0001
Sex 1.15 (0.93,1.42) .173
Clinical Joint Damage at 1st visit 1.03 (1.01,1.05) .0003
NSAIDS at first visit 1.04 (0.84,1.30) .690
Biologics at first visit 0.89 (0.54,1.45) .630
DMARDS at first visit 1.20 (0.95,1.51) .130
NSAIDS after first visit 1.22 (0.89,1.68) .230
Biologics after first visit 1.15 (0.90,1.46) .250
DMARDS after first visit 1.52 (1.16,1.99) .002
* Using a negative binomial model; ** 641 >2y 436 ≤ 2y.Gladman DD, et al. Ann Rheum Dis. 2011;70:2152-4.
Effect of Late Consultation
Univariate Multivariate
Variable OR P OR P
Erosions 4.58 .001 4.25 .001
Osteolysis 3.6 .01 - -
Sacroiliitis 2.28 .01 1.47 .09
Arthritis mutilans 10.6 .02 - -
Deformed joints 2.28 .002 - -
# deformed joints 1.06 .006 - -
DMARDs/TNFi failures 1.47 .007 - -
Drug free remission 0.42 .01 - -
HAQ scores 2.17 .003 2.2 .004
Haroon M, et al. Ann Rheum Dis. Online 14/02/27.
Even a 6 month delay in consultation leads to untoward outcomes
Mortality in Psoriatic Arthritis
• PsA patients are at an increased risk of death
• Overall risk is 1.62 that of Ontario Residents
– 1.65 for women
– 1.59 for men
• Causes of Death are similar to the general population
• Risk of death is related to previously active and severe disease
Ali Y, et al. A&R. 2007;56:2708-14.
Overall
Male
Female3
2
4
1
0
1982
-199
1
Sta
nd
ard
ize
d M
ort
ali
ty R
ati
o
Ten-year Rolling Periods from 1978 to 2004
1978
-198
7
1979
-198
8
1980
-198
9
1981
-199
0
1983
-199
2
1988
-199
7
1984
-199
3
1985
-199
4
1986
-199
5
1987
-199
6
1989
-199
8
1994
-200
3
1990
-199
9
1991
-200
0
1992
-200
1
1993
-200
2
1995
-200
4
Post-Activity Question 1
How confident are you in your ability to discuss the epidemiology and classification of psoriatic arthritis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 2
How confident are you in your ability to discuss the epidemiology and classification of psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident

Post-Activity Question 3
In a survey of working psoriatic patients, what percentage reported missing work (absenteeism) due to psoriasis or psoriatic arthritis treatment?
1. 12%
2. 38%
3. 49%
4. 82%
Post-Activity Question 4
Which of the following is NOT a disease activity-related predictor of disease progression?
1. Number of swollen joints
2. Number of tender joints
3. Initial ESR
4. Pain rating of 8 on visual analog scale
Questions & Answers
5/28/2015
1
Pathogenesis and Geneticsof Psoriasis and Psoriatic Arthritis
James G. Krueger, MD, PhDAssociate Professor
Medical DirectorLaboratory for Investigative Dermatology
Rockefeller UniversityNew York, New York
Christopher Ritchlin, MD, MPHProfessor of Medicine
Chief, Allergy, Immunology & Rheumatology DivisionUniversity of Rochester Medical Center
Rochester, New York
Content Developers
Paolo Romanelli, MDAssociate Professor of Medicine
Department of DermatologyUniversity of Miami
Miami, FL
Jose U. Scher, MDAssistant Professor of Medicine
Division of Rheumatology, New York University School of Medicine Director, Arthritis Clinic & Co-Director Psoriasis Arthritis Center
Director, Microbiome Center for Rheumatology and Autoimmunity NYU-Langone Hospital for Joint Diseases
New York, New York
Speakers Pre-Activity Question 1
How confident are you in describing the pathogenesis of psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 2
How confident are you in describing the pathogenesis of PsA?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 3
Genes that are highly and selectively expressed in psoriasis are induced by immune cytokines produced by “polar” T-cell subsets: Th1, Th17, and Th22.
1. True
2. False

5/28/2015
2
Psoriasis
Psoriasis Vulgaris
Unaffected Skin Psoriasis Lesion
Histopathology of Normal Appearing Background Skin and a Psoriasis Plaque (both at same magnification)
2 Defining Parts of the Psoriasis Skin Lesions: Cellular Features
• A change in epidermal growth and differentiation, along with a vascular response that creates plaques on the skin
• An underlying cellular immune response that involves myeloid dendritic cells and T-cells. Cytokines produced by these activated immune cells are key drivers of altered epidermal growth and skin structural changes.
Psoriasis Vulgaris:Clinical Pathological Correlates
• Clinical lesion is characterized by:
A. Indurated plaques
B. Scale
C. Erythema
• Histological correlates are:
A. Regular epidermal hyperplasia with elongated rete (regular acanthosis): increases epidermal thickness
B. Reduced granular layer and keratinocyte maturation with retained nuclei (parakeratosis)
C. Angiogenesis and dilation of superficial venules
Epidermal Reaction in Psoriasis
• Epidermal acanthosis results from excessive proliferation of keratinocytes.
– Demonstrated by an increase in Ki67+ nuclei (next slide) in lesional skin
• Hyperplasia triggers a wound healing differentiation program in the epidermis.
– Visualized by synthesis of keratin 16 in suprabasalkeratinocytes next slide).

5/28/2015
3
Psoriatic Plaque (Ki67 protein) Psoriatic Plaque (keratin 16)
Uninvolved Skin (Ki67 protein) Uninvolved Skin (keratin 16)Factors That May Induce Keratinocyte
Hyperplasia in Psoriasis
• Autocrine growth factors, especially EGF family (transforming growth factor-alpha, amphiregulin, and heparin-binding EGF) are all over-expressed in psoriasis
• Kertainocyte growth factor, other FGF family growth factors, and insulin-like growth factor-1 all have increased expression or activity in psoriasis lesions.
• Immune-related cytokines
– IL-1 and IL-6
– IL-10 family: IL-19, IL-20, IL-22, IL-24
Other Changes in the Epidermis
• At a molecular level, hundreds of genes in the epidermis have increased or decreased transcription in active psoriasis lesions
• Some changes reflect cell growth pathways of generalized hyperplasia
• Some changes are more specific to psoriasis—the following slide shows (red) genes with very high expression in psoriasis, but much lower expression in atopic dermatitis, another skin disease that has associated epidermal hyperplasia
S100A9(calgranulin B)
S100A7(psoriasin)
Normal LS Psoriasis
Heatmap Slide
• Genes with high expression in psoriasis lesions all have low expression in non-lesional or normal skin
• As shown by IHC at bottom for S100A7 and S100A9, the altered expression of these genes is created by over-production of corresponding proteins in epidermal keratinocytes
Key Concepts in Pathogenesis
• Genes that are highly and selectively expressed in psoriasis are induced by immune cytokines produced by “polar” T-cell subsets: Th1, Th17, and Th22
• Myeloid dendritic cells (CD11c+ DCs) regulate T-cell activation through antigen-presentation, co-stimulation, and production of cytokines such as IL-12 and IL-23 that drive activation, differentiation and survival of polar T-cell subsets

5/28/2015
4
CD3+ T-cells in Psoriasis
Uninvolved Skin Psoriasis Plaque
T-cell Subsets in Psoriasis
• Th1 (CD4+) and Tc1 (CD8+) T-cells that are defined by synthesis of interferon-gamma upon activation
• Th17 (CD4+) and Tc17 (CD8+), including conventional T-cells and gamma-delta T-cells, synthesize IL-17A and IL-17F upon activation
• Th22 (CD4+) and Tc22 (CD8+) synthesize IL-22 upon activation
Th1
Th17
Blood
Psoriasis Lesion
Th17 T-cells increased in psoriasis lesions. Th1 also increased.
Lowes, et al. J. Invest Dermatol. (2008).
“Polar” cytokines of Th1, Th22, and Th17 T-cells act on epidermal keratinocytes directly to change gene expression profiles and alter other properties of the skin that in the sum create the psoriasis phenotype at clinical, cellular, and molecular levels.
Interferon- binds to receptors that are highly expressed on epidermal keratinocytes. IFN- activates STAT1 and induces expression of many pro-inflammatory gene products
IFN-
STAT1 activation STAT1 mRNA CXCL9, 10, 11 mRNAs MHC-II mRNAs~1000 other mRNAs also regulated
Named genes strongly induced by IFN-, but not by IL-17 or IL-22
human keratinocytes
(in vitro)
What features of psoriasis may beexplained by polar T-cell cytokines
(especially IL-17 and IL-22)?
5/28/2015
5
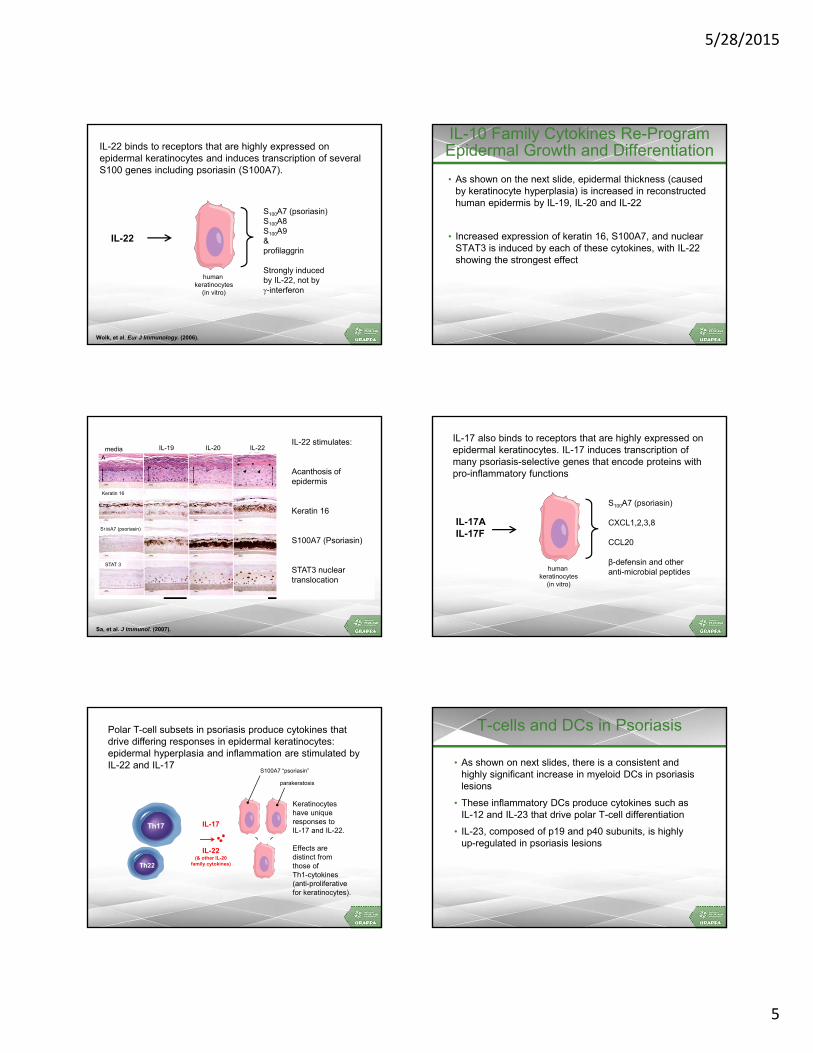
IL-22 binds to receptors that are highly expressed on epidermal keratinocytes and induces transcription of several S100 genes including psoriasin (S100A7).
Wolk, et al. Eur J Immunology. (2006).
IL-22
S100A7 (psoriasin)S100A8S100A9&profilaggrin
Strongly inducedby IL-22, not by-interferon
human keratinocytes
(in vitro)
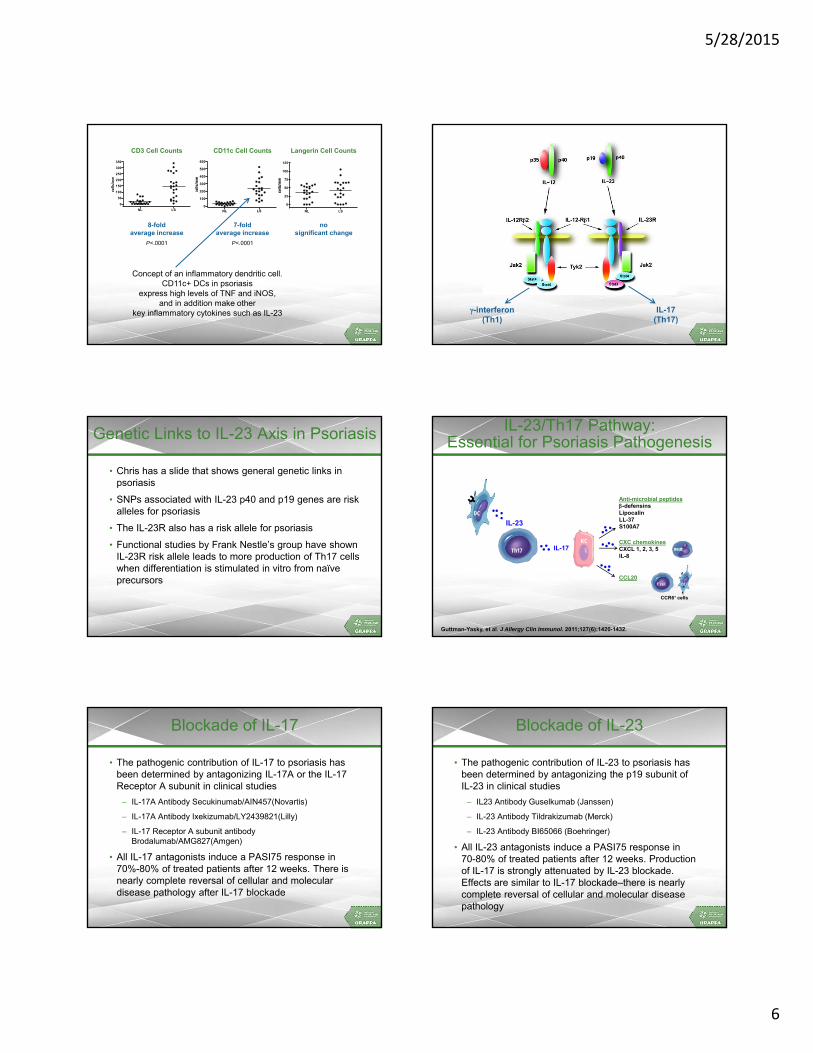
IL-10 Family Cytokines Re-Program Epidermal Growth and Differentiation
• As shown on the next slide, epidermal thickness (caused by keratinocyte hyperplasia) is increased in reconstructed human epidermis by IL-19, IL-20 and IL-22
• Increased expression of keratin 16, S100A7, and nuclear STAT3 is induced by each of these cytokines, with IL-22 showing the strongest effect
media IL-19 IL-20 IL-22 IL-24 EGF
Keratin 16
S100A7 (psoriasin)
STAT 3
Sa, et al. J Immunol. (2007).
IL-22 stimulates:
Acanthosis of epidermis
Keratin 16
S100A7 (Psoriasin)
STAT3 nuclear translocation
IL-17AIL-17F
S100A7 (psoriasin)
CXCL1,2,3,8
CCL20
β-defensin and other anti-microbial peptideshuman
keratinocytes(in vitro)
IL-17 also binds to receptors that are highly expressed on epidermal keratinocytes. IL-17 induces transcription of many psoriasis-selective genes that encode proteins with pro-inflammatory functions
Polar T-cell subsets in psoriasis produce cytokines that drive differing responses in epidermal keratinocytes: epidermal hyperplasia and inflammation are stimulated by IL-22 and IL-17
Th17
Keratinocyteshave uniqueresponses toIL-17 and IL-22.
Effects aredistinct fromthose ofTh1-cytokines(anti-proliferativefor keratinocytes).
IL-17
IL-22(& other IL-20
family cytokines)
S100A7 “psoriasin”
parakeratosis
Th22
T-cells and DCs in Psoriasis
• As shown on next slides, there is a consistent and highly significant increase in myeloid DCs in psoriasis lesions
• These inflammatory DCs produce cytokines such asIL-12 and IL-23 that drive polar T-cell differentiation
• IL-23, composed of p19 and p40 subunits, is highlyup-regulated in psoriasis lesions
5/28/2015
6
CD3 cell counts
NL LS
0
50
100
150
200
250
300
350
CD11c cell counts
NL LS0
100
200
300
400
500
600
Langerin cell counts
NL LS
0
25
50
75
100
125
8-foldaverage increase
7-foldaverage increase
P<.0001 P<.0001
nosignificant change
Concept of an inflammatory dendritic cell.CD11c+ DCs in psoriasis
express high levels of TNF and iNOS,and in addition make other
key inflammatory cytokines such as IL-23
CD3 Cell Counts CD11c Cell Counts Langerin Cell Counts
-interferon(Th1)
IL-17(Th17)
Genetic Links to IL-23 Axis in Psoriasis
• Chris has a slide that shows general genetic links in psoriasis
• SNPs associated with IL-23 p40 and p19 genes are risk alleles for psoriasis
• The IL-23R also has a risk allele for psoriasis
• Functional studies by Frank Nestle’s group have shown IL-23R risk allele leads to more production of Th17 cells when differentiation is stimulated in vitro from naïve precursors
IL-23/Th17 Pathway: Essential for Psoriasis Pathogenesis
DC
IL-23
neutTh17
KC
T cell DC
IL-17
CCL20
CCR6+ cells
CXC chemokinesCXCL 1, 2, 3, 5IL-8
Anti-microbial peptides-defensinsLipocalinLL-37S100A7
Guttman-Yasky, et al. J Allergy Clin Immunol. 2011;127(6):1420-1432.
Blockade of IL-17
• The pathogenic contribution of IL-17 to psoriasis has been determined by antagonizing IL-17A or the IL-17 Receptor A subunit in clinical studies
– IL-17A Antibody Secukinumab/AIN457(Novartis)
– IL-17A Antibody Ixekizumab/LY2439821(Lilly)
– IL-17 Receptor A subunit antibody Brodalumab/AMG827(Amgen)
• All IL-17 antagonists induce a PASI75 response in70%-80% of treated patients after 12 weeks. There isnearly complete reversal of cellular and moleculardisease pathology after IL-17 blockade
Blockade of IL-23
• The pathogenic contribution of IL-23 to psoriasis has been determined by antagonizing the p19 subunit ofIL-23 in clinical studies
– IL23 Antibody Guselkumab (Janssen)
– IL-23 Antibody Tildrakizumab (Merck)
– IL-23 Antibody BI65066 (Boehringer)
• All IL-23 antagonists induce a PASI75 response in70-80% of treated patients after 12 weeks. Productionof IL-17 is strongly attenuated by IL-23 blockade.Effects are similar to IL-17 blockade–there is nearlycomplete reversal of cellular and molecular diseasepathology

5/28/2015
7
What Is the Role of TNF in the Pathogenesis of Psoriasis?
• In vitro Normal Human Keratinocytes growthwith medium
• Treated for 24h with:
• Medium alone
• IL-17 200 ng/mL
• TNF 10 ng/mL
• IL-17 + TNF 10
• Gene sequencingby Illumina Genechip
• RT-PCR
TNF
IL-17 IL-17+TNF
Control
IL17 +TNFa
TNFaIL170
mR
NA
Exp
ress
ion
/ h
AR
P
Control
100
50
150S100A7
IL17 +TNFa
TNFaIL170
200
mR
NA
Exp
ress
ion
/ h
AR
P
Control
400
100
300
500IL8
TNF interacts with this pathway at 2 points.First, TNF induces IL-23 production in myeloid DCs.
Second, TNF and IL-17 interact synergistically and additively inkeratinocytes to increase transcription of many psoriasis-related genes
DC
neutTh17
KC
T cell DC
IL-17
CCL20
CCR6+ cells
CXC chemokinesCXCL 1, 2, 3, 5IL-8
Anti-microbial peptides-defensinsLipocalinLL-37S100A7
TNF
TNF
IL-23
Several hundred genesInduced by IL-17 + TNF:
Synergistic andAdditive Effects
Psoriasis Immunopathogenesis
CCL = chemokine (C-C motif) ligand; CXCL = chemokine (C-X-C motif) ligand; DC = dendritic cell; IFN = interferon; IL = interleukin; LL3 = human cathelicidin; STAT = signal transducer and activator of transcription; TNF = tumor necrosis factor. Adapted from Lowes MA, et al. Ann Rev Immunol. 2014;32:227-255.
Initial responseImmune
amplificationDisease phenotype: cytokine amplification of
keratinocyte hyperplasia and inflammation via KCs
Central IL-23/Th17 pathway in psoriasis
Neutrophil chemoattractionand more inflammation
IL-23 Th17
T-cell
IL-17
TNF
DC
IL-17 (synergy with TNF)
IL-12
IL-23
TNFTh17
Th1
Th22
S100A7
IP-10
IP-10
CXCL1CXCL2CXCL3CXCL8(IL-8)
STAT1 activation
IFNγHyperplasia
IL-36γIL-19
TNF
IL-22
Feed forward activation of DC recruitment and activation
CCL20LL37
IL-22IL-19IL-20IL-24
STAT 3 activation
More S100A7
K16
Keratinocyte proliferation
IL-2
Vascular and Hepatic Inflammation in Psoriasis
FDG-PET
Mehta N, et al. Archives Derm. 2011.
Psoriatic Arthritis

5/28/2015
8
Landmarks in Psoriatic Arthritis
• 1850–Jean Louis Alibert’s monograph: association between Ps and arthritis published
• 1956–First publication by Dr. Wright on PsA
• 1964–ARA recognizes PsA as separate from RA
• 1973–Landmark paper by Drs. Moll and Wright describes the five subgroups
• 1978–Dr. Gladman establishes first cohort of patients in Toronto
• 1991–Original five subgroups of Drs. Moll and Wright challenged
• 1998–Dr. McGonagle paper published in Lancet
• 2000–First paper describing beneficial effect of anti–tumor necrosis factor drugs in psoriatic arthritis
• 2003–First meeting of GRAPPA
• 2006–Publication of classification criteria for psoriatic arthritis (CASPAR)
• 2008–Publication of PsA treatment guidelines
Adapted from Ritchlin C and Helliwell P. The Rheumatologist. August 2009; Blumberg, BS, et al. Bull Rheum Dis. 1964;14:339-340.
Is PsA an Autoimmune Disease?
Rheumatoid arthritis
• Autoantibody identified
• MHC Class II (shared epitope)
• SS, vasculitis, nodules
• Type II collagen
• Homogeneous tissue response
Psoriatic arthritis
• No autoantibodies
• MHC class I
• Psoriasis, uveitis, IBD
• Over expression/deletion
of GF, cytokines, signals
• Heterogeneous tissue
response
Psoriasis and PsA
Clues to Pathogenesis:
• 40% with positive family history
• Male/Female ratio approximately 1:1
• Psoriasis usually precedes arthritis
• Association with Class I MHC alleles
– B13, B17, B27, B39 and Cw6
• Environmental triggers:
trauma (Koebner phenomena), infection (?microbiome),
stress
Genes in Psoriasis and PsA
O'Rielly and Rahman. Nature Reviews Rheumatology. 2011;7:718-732.
* Genes in which association of variants with Ps and PsAachieved GWA significance in Western cohorts
Discovery timeline of genes of which variants are implicated in the pathogenesis of Ps
Genes in Psoriasis and PsA
Pedersen, B. et. al., Ann Rheum Dis 2008
PsA MZ Twins DZ Twins Difference (95% CI), p
Moll and Wright 1/10 (10%) 1/26 (3.7%) 6.3% (‐ 11%, 34%)
CASPAR 1/9 (11%)
1/22 (4.5%) 6.6% (‐ 12%, 39%)
PsO in Twins with PsA
6/11 (55%)
6/28 (21%)
34% (‐ 2%, 60%), p<0.05
Probandwise concordance estimates on PsO and PsA
Obesity Is a Major Risk Factor for Incident Ps and PsA
Prospective examination of relationship between incident PSand BMI in 78,626 women in NH study over 14 year period.
Cohort study of 75, 395 subjects with psoriasis in the THIN database to examine the relationship between obesity and incident PsA
*Compared to BMI of 21-22.9.Setty AR, et al. Arch Int Med. 2009;167(15):167. Love TJ, et al. Ann Rheum Dis. 2012;71:1273.
BMI RR*
25-29.9 1.09 (.93-1.28)
30-34.9 1.28 (1.02-1.47)
>35 1.48 (1.20-1.81)
BMI RR*
25-29.9 1.4 (1.13-1.73)
30-34.9 1.5 (1.51-1.91)
>35 2.7 (2.12-3.4)

5/28/2015
9
The Gut-Joint Axis in SpA/PsA
Taurog J, et. al., J Exp Med 1994; Mielants, H. et al. J Rheum 1995; Orchard, TR. et. al. Gut 1998; Schatteman L, et.al., J Rheum 1995; Scarpa R., et al. J Rheum 2000
• HLA-B27 tg rats don’t develop colitis/Ps/arthritis under Germ-free conditions.
• ~2/3 of SpA patients have microscopic, subclinical gut inflammation; ~10% AS patients clinical IBD
• PsA patients have subclinical gut inflammation (16-100%)
• Is there a role for Mucosal Inflammation/Microbiome in the pathogenesis of SpA (PsA)?
The Gut Microbiome in PsA
Scher JU, Ubeda C, et. al., Arthritis Rheum 2014 (ePub)
Decreased Diversity in PsA Gut Microbiome Resembling IBD
Scher JU, Ubeda C, et. al., Arthritis Rheum 2014 (Epub); Willing BP, et al. Gastroenterology2010;139:1844-54; De Preter V, et al. Gut 2014 (Epub).
A
• IBD (and especially Crohn’s) patients have decreased diversity
• Akkermansia, Ruminoccocus and other beneficial commensals are
also absent in IBD microbiome
• Levels of protective MCFAs (hexanoate/heptanoate) are significantly
lower in IBD/Ps/PsA
Model: Microbiome in PsA EtiopathogenesisSkin
Psoriasis
Genetic predisposition (HLA-B27,Cw*6)
Environmental factors
(Stress, Infection, Skin microbiome, trauma)
~30%
Psoria c Arthri s ∆ in Skin Microbiome
∆ in Gut Microbiome (i.e., loss of Akkermansia)
~70%
Skin Psoriasis
= Skin Microbiome = Gut Microbiome
Psoriasisand
Nail Disease
Uveitis Gut
MSK
DiabetesCV
Disease
Obesity
Enthesitis
DactilitisPeripheral
Arthritis
Axial
DIP Mutilans
Psoriatic Disease and theIL-23/Th17 Pathway Sites of Joint Inflammation
RA-synovium PsA-bone, enthesis and
synovium
AS-bone,enthesis

5/28/2015
10
Synovial Histopathology of PsA
• SpA tissues (PsA, AS, USpA):
– More vascularity, neutrophil and CD 163+ macrophage infiltration
• No citrullinated proteins in polyarticular PsA
• DC163+ macrophages, PMN and lining hyperplasia correlated with swollen joint count and acute phase reactants in PsA
• Synovial histopathology of PsA (either oligo or poly) resembles other SpA subtypes more than RA
• Both groups can be differentiated from RA
Baeten D. Arthritis Care Res. 2005.
Increased Synovial RANKL and Circulating OCP in PsA
Ritchlin CT. J Clin Invest. 2003;111:824.
RANKL
Nonerosive0
Ost
eocl
asts
per
106
PB
MC
s
Erosive
750
250
1000
Control
(N=12)
0
100
Ost
eocl
asts
per
106
PB
MC
s
PsA
(N=24)
200
50
150
250
500
Increased Synovial RANKL and Circulating OCP in PsA
Ritchlin CT. J Clin Invest. 2003;111:824.
Master Cytokines in Spondyloarthritis
mRNA = messenger RNA.Miossec P, et al. Nat Rev Drug Discov. 2012;11:763-776. 58
Links Between Skin and Joint in PsA
CZP-SCT-013894-052012
Th1 and Th17cells
osteoclastprecursor
(OCPs)
TNFα/IL-17
mature osteoclast
Enthesitis
synovial lining cells type B type A
TNFα/IL-17RANKL
Bone Matrix
RANKL M-CSF
TNFα
Bone Marrow
Bonemonocyte
RANKL
Psoriatic Plaque
Skinmacrophage
T cells
lymph node
Dendriticcells
IL-12/IL-23
CD8+ IL17+ Cells Expanded in PsABut Not RA Synovial Fluid
Menon B. et al., Arthritis Rheumatol 2014; 66(5): 1272–1281.
• In RA: only CD4+ IL17+ are
elevated in SF
• In PsA: CD4+ and CD8+ IL17+
are elevated in SF
• Levels of CD8+ IL17+ correlate
with disease activity and erosions
in PsA

5/28/2015
11
Synovio-Enthesial Complex (SEC)
• In PsA, synovium and enthesisare closely related (concept of SEC)
• Stressing of SEC (danger signals due to cell injury) triggers innate immune response, which dictates clinical expression of disease
• Primary basis for pathogenesis of PsA could be biomechanical rather than autoimmune
• Spondyloarthritis could be an ‘auto-inflammatory’ disease
McGonagle D. A & R. 2007;56(8):2482-2491.
Relationship between theDIP Joint, Nail, and Enthesis
SL = Superficial lamina; DL = Deep lamina.Tan, et al. Rheumatology. 2007.
Nail plate
Extensor tendon (ET)
Distal Phalange (DP)
Nail root (NR)
F
IL-23 Induces Enthesitis and New Bone Formation
Sherlock J. Nat Med. 2012;18(7):1071
IL-23mc IL-23mc (magnified)
Alk Phos(Osteoblasts)
TRAP(Osteoclasts)
PeriostealBone
Formation
IL‐23R CD3+CD4‐CD8‐ROR‐γt+
IL-23 induce Enthesitis via activation of resident T cells…
… while IL‐22 promotes Osteoproliferation
IL-23 and Resident T-cells Promote Enthesitis and Osteoproliferation
Lories R. Nature Med. 2012;18(7):1018.
+
Three Pathways to Osteoproliferation
Lories R. Rheum Dis Clin. NA;38(2012):555.
Nuclear Membrane
Plasma Membrane
BMP
Noggin
SMAD 4
SMAD 1/5
Osteoblast Differentiation
SMAD 4
SMAD 1/5
Sfrp1
Catenin
DKK-1Sclerostin
Fz
Wnt IHH
PTCSMO
Gli
LRP5/6
Bone MorphogenicProtein signaling
WNTsignaling
Hedgehogsignaling
Mutilans Dactylitis Mutilans Normal Synovitis Dactylitis Ankylosis Mutilans
Phenotypic Diversity in PsA

5/28/2015
12
Cutaneous Nocioceptors in PsAPromote IL-23 Release
Riol-Blanco L. Nature. 2014:510:157.
Post-Activity Question 1
How confident are you in describing the pathogenesis of psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 2
How confident are you in describing the pathogenesis of PsA?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 3
Genes that are highly and selectively expressed in psoriasis are induced by immune cytokines produced by “polar” T-cell subsets: Th1, Th17, and Th22.
1. True
2. False
Questions & Answers

Psoriasis and PsA Clinical Features, Associated Conditions,
Screening, and Assessment
Amit Garg, MDAssociate Professor and Founding Chair
Department of DermatologyHofstra NSLIJ School of Medicine
North Shore LIJ Health SystemManhasset, New York
Kristina Callis Duffin, MD, MSAssociate Professor
Department of DermatologyUniversity of Utah
Salt Lake City, Utah
Laura Coates, MBChB, MRCP, PhDNIHR Clinical Lecturer in Rheumatology
Leeds Institute of Rheumatic and Musculoskeletal MedicineUniversity of Leeds and the
Leeds Musculoskeletal Biological Research UnitLeeds Teaching Hospitals NHS Trust
Leeds, England
Content Developers
Amit Garg, MDAssociate Professor and Founding Chair
Department of DermatologyHofstra NSLIJ School of Medicine
North Shore LIJ Health SystemManhasset, New York
Jose U. Scher, MDAssistant Professor of Medicine
Division of Rheumatology, New York University School of Medicine Director, Arthritis Clinic & Co-Director Psoriasis Arthritis Center
Director, Microbiome Center for Rheumatology and Autoimmunity NYU-Langone Hospital for Joint Diseases
New York, New York
Speakers Pre-Activity Question 1
How confident are you in your ability to establish a clinical framework to diagnose and screen the psoriasis patient for psoriatic arthritis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 2
PASI includes a component for patient-reported outcomes.
1. True
2. False
Pre-Activity Question 3
For what percentage of psoriasis patients do you currently perform an annual assessment for PsA?
1. 0-25%
2. 26-50%
3. 51-75%
4. 76-100%
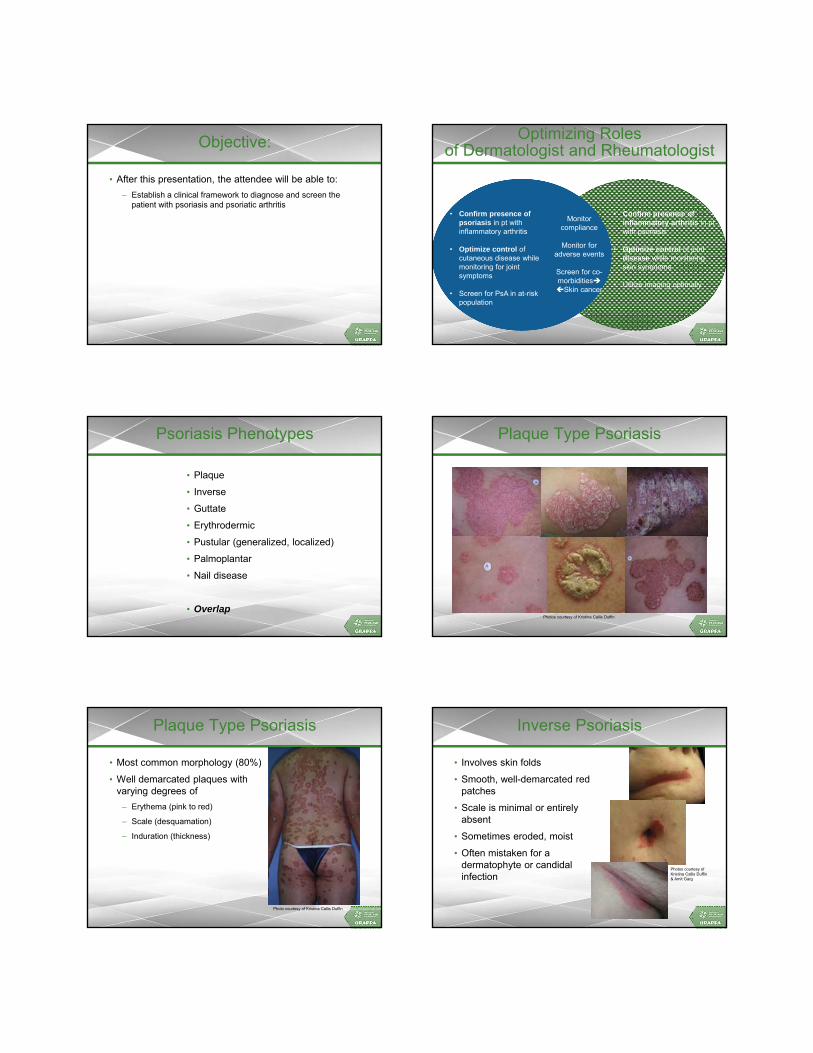
Objective:
• After this presentation, the attendee will be able to:
– Establish a clinical framework to diagnose and screen the patient with psoriasis and psoriatic arthritis
Optimizing Rolesof Dermatologist and Rheumatologist
• Confirm presence of psoriasis in pt with inflammatory arthritis
• Optimize control of cutaneous disease while monitoring for joint symptoms
• Screen for PsA in at-risk population
• Confirm presence of inflammatory arthritis in pt with psoriasis
• Optimize control of joint disease while monitoring skin symptoms
• Utilize imaging optimally
Monitor compliance
Monitor for adverse events
Screen for co-morbiditiesSkin cancer
Psoriasis Phenotypes
• Plaque
• Inverse
• Guttate
• Erythrodermic
• Pustular (generalized, localized)
• Palmoplantar
• Nail disease
• Overlap
6p4 16 17
Photos courtesy of Kristina Callis Duffin
Plaque Type Psoriasis
Photo courtesy of Kristina Callis Duffin
Photo courtesy of Kristina Callis Duffin
Photo courtesy of Kristina Callis Duffin
Plaque Type Psoriasis
• Most common morphology (80%)
• Well demarcated plaques with varying degrees of
– Erythema (pink to red)
– Scale (desquamation)
– Induration (thickness)
Inverse Psoriasis
• Involves skin folds
• Smooth, well-demarcated red patches
• Scale is minimal or entirely absent
• Sometimes eroded, moist
• Often mistaken for a dermatophyte or candidalinfection
Photos courtesy of Kristina Callis Duffin& Amit Garg

Guttate Psoriasis
• Eruptive
• Red erythematous, scaly papules and small plaques
• May follow streptococcal pharyngitis
Photo courtesy of Kristina Callis Duffin
Erythrodermic Psoriasis
• Means “red skin”
– Warm, red, scaly patches covering almost entire body surface
• Disrupted barrier function: temperature, fluids, electrolytes
• Differential diagnosis includes drug reaction, cutaneous T cell lymphoma, atopic dermatitis
Photos courtesy of Kristina Callis Duffin
Pustular Psoriasis
• Localized
– Palmo-Plantar Psoriasis
• Generalized (von Zumbusch)
– Mimics include other pustular dermatoses(pustular drug eruption/ AGEP)
Photos courtesy of Kristina Callis Duffin
Palmar Plantar Psoriasis (PPP):Pustular and non-Pustular
• Spectrum:
– Pustular: predominance of pustules
– Non-pustular: hyperkeratotic plaques
• Pustular variant: (palmoplantar pustulosis)
– Regarded as a distinct entity by some
• Not associated with HLA-Cw62
– Associated with smoking
– Treatment poses a challenge
– Associated with plaque psoriasis in ~20%
1. Farley E, Masrour S, McKey J, Menter A. Palmoplantar psoriasis: A phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am AcadDermatol. 2009;60:1024-31. 2. Asumalahti K, Ameen M, Suomela S, et al. Genetic analysis of PSORS1 distinguishes guttate psoriasis and palmoplantar pustulosis. J Invest Dermatol. 2003;120:627-32.
Photos courtesy of Kristina Callis Duffin and Amit Garg
Palmar Psoriasis
Photos courtesy of Amit Garg
Plantar Psoriasis
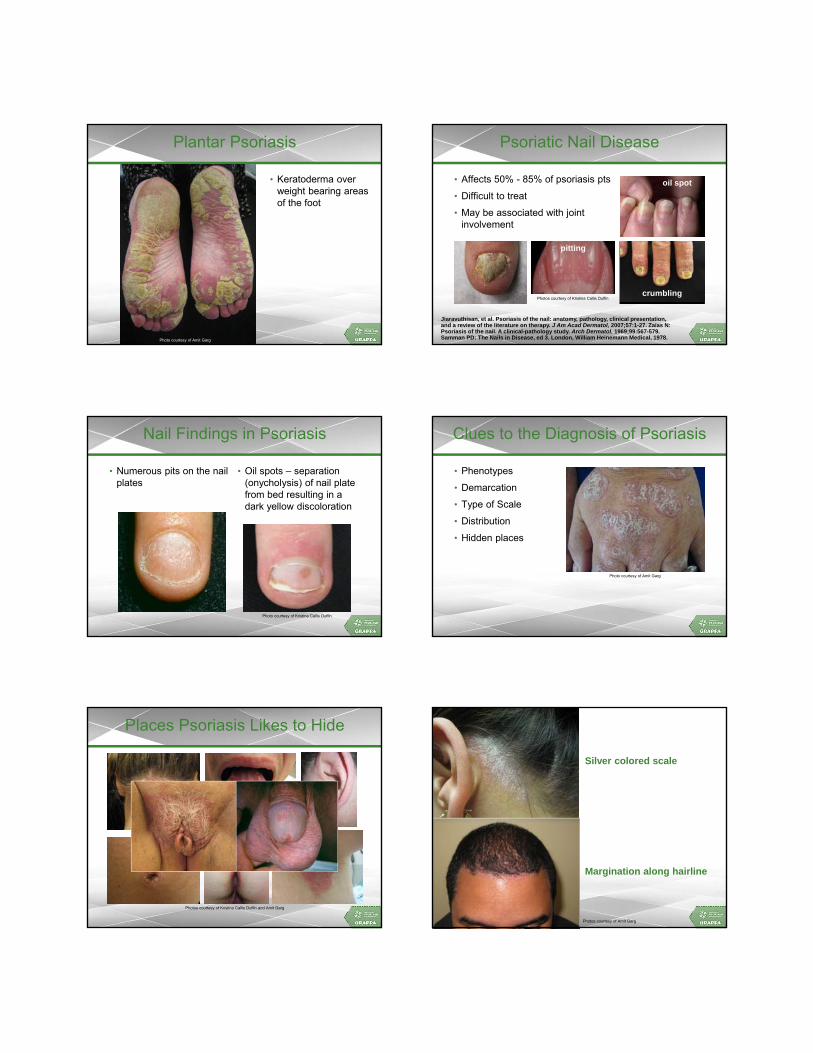
Plantar Psoriasis
• Keratoderma over weight bearing areas of the foot
Photo courtesy of Amit Garg
Psoriatic Nail Disease
• Affects 50% - 85% of psoriasis pts
• Difficult to treat
• May be associated with joint involvement
Jiaravuthisan, et al. Psoriasis of the nail: anatomy, pathology, clinical presentation,and a review of the literature on therapy. J Am Acad Dermatol, 2007;57:1-27. Zaias N: Psoriasis of the nail. A clinical-pathology study. Arch Dermatol. 1969;99:567-579.Samman PD: The Nails in Disease, ed 3. London, William Heinemann Medical, 1978.
Photos courtesy of Kristina Callis Duffin
pitting
crumbling
oil spot
Nail Findings in Psoriasis
• Numerous pits on the nail plates
• Oil spots – separation (onycholysis) of nail plate from bed resulting in a dark yellow discoloration
Photo courtesy of Kristina Callis Duffin
Clues to the Diagnosis of Psoriasis
• Phenotypes
• Demarcation
• Type of Scale
• Distribution
• Hidden places
Photo courtesy of Amit Garg
Places Psoriasis Likes to Hide
Photos courtesy of Kristina Callis Duffin and Amit Garg
Silver colored scale
Margination along hairline
Photos courtesy of Amit Garg

Is the Distinction Clear?
Dx: Psoriasis
Photo courtesy of Amit Garg
Dx: Atopic Dermatitis
Photo courtesy of Amit Garg
Dx: Dyshidosis
Photo courtesy of Amit Garg
Dx: Nummular Eczema
Photo courtesy of Amit Garg
Dx: Psoriasis
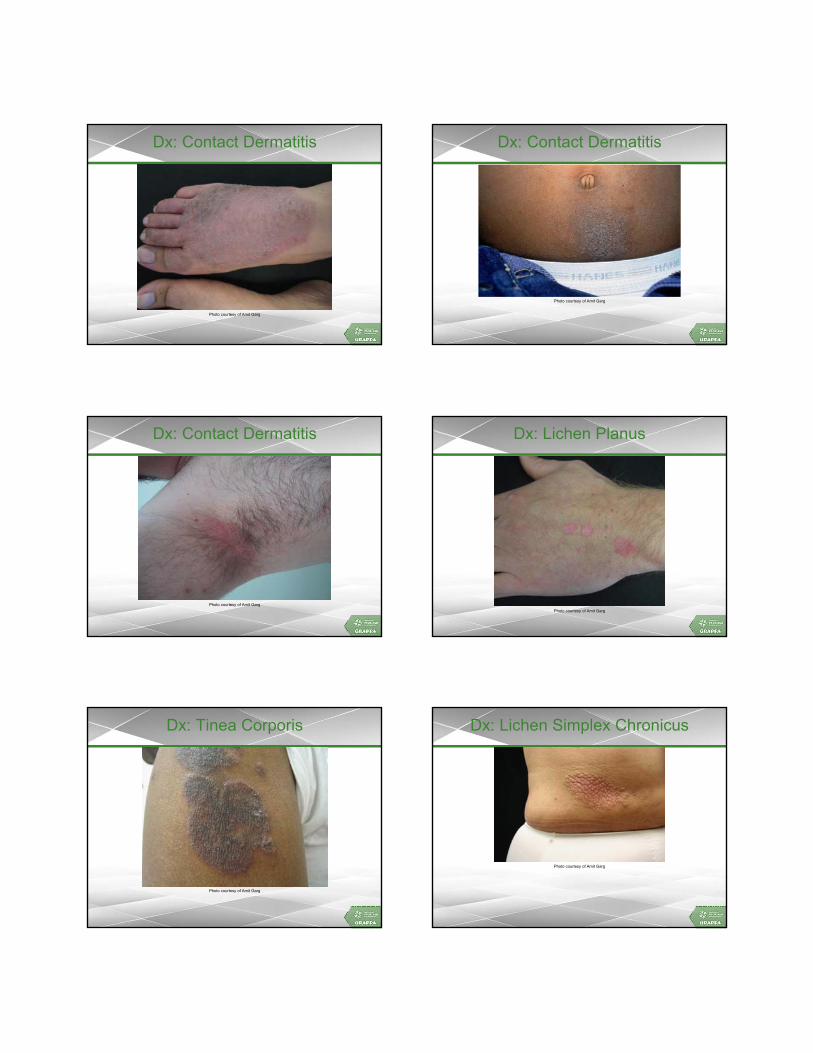
Dx: Contact Dermatitis
Photo courtesy of Amit Garg
Dx: Contact Dermatitis
Photo courtesy of Amit Garg
Dx: Contact Dermatitis
Photo courtesy of Amit Garg
Dx: Lichen Planus
Photo courtesy of Amit Garg
Dx: Tinea Corporis
Photo courtesy of Amit Garg
Dx: Lichen Simplex Chronicus
Photo courtesy of Amit Garg

Dx: Onychonycosis (white superficial)
Photo courtesy of Amit Garg
Dx: CTCL
Photo courtesy of Amit Garg
Cutaneous T-cell Lymphoma/Mycosis Fungoides
Increased risk of CTCL: biologic vs misdiagnosed?
Differential Dx
• Some conditions which may be difficult to distinguish from Psoriasis
– Seborrheic dermatitis
– Nummular eczema
– Atopic Dermatitis
– Contact dermatitis
– Hand Dermatitis
– Balanitis
– Dermatophyte or Candidal infection
– Palmoplantar keratodermas
– Cutaneous T Cell Lymphoma
– Onychodystrophy related to a number of etiologies including Dermatophyteinfection and trauma
Assessment of Psoriasis: PASI
• Most commonly utilized disease severity measure in clinical trials
• Quantify severity based on:
– Erythema, Induration, and Scale
– Body parts and surface area involved
• Separate calculation for head, trunk, upper extremities, and lower extremities
PASI Strengths
• Assesses both lesion quality and extent of involvement
• Validated instrument – Low intra-observer variability
– Moderate inter-observer variability
– Reproducible when performed by trained individuals
• Allows some historical comparison across several treatments

PASI Limitations
• Erythema, induration, and scaling are equally weighted
• Interpretation not so intuitive
– Nonlinear score
– Composite score has no clinical frame of reference
• Lacks sensitivity to change at lower ranges
• No component for patient input
Seeking Out Your Dermatology Colleague
• When diagnosis of psoriasis is not certain
• Optimization of topical therapies and regimens
• When use of oral retinoid may be appropriate
• When phototherapy may be useful
– Guttate psoriasis, or with diffuse thin plaques
– Adjunctive to systemic therapy
– Poor candidacy for systemic therapy
• When Psoriasis is flaring or unstable
• “Undifferentiated” or seronegative inflammatory disease and a rash
Diagnosis/Presentation of PsA
Features of PsA
• An inflammatory arthritis that occurs in 6%-42% of patients with psoriasis1
• Psoriasis typically precedes development of the arthritic component of PsA
– In 70% of patients with PsA, psoriasis is the first symptom to present2,3
– 20% have PsA before psoriasis2,3
– 10%-15% report simultaneous onset of skin and joint disease2,3
• Severity of psoriasis is not predictive of severity of PsA3
1. Gladman D, et al. Ann Rheum Dis. 2005; 64 (Suppl II): ii14-7. 2. Leung Y, et al. J Postgrad Med. 2007; 53: 63-71. 3. Cohen M, et al. J Rheumatol. 1999; 26: 1752-6.
Gottlieb A, et al. Journal of Dermatological Treatment. 2006;17:343–352.
70-80%
10-20%
Assessing the Psoriasis Patient
• Annual assessment for PsA to people with any type of psoriasis. Especially important within the first 10 years of onset of psoriasis.
• Use a validated tool to assess adults for psoriatic arthritis in primary care and specialist settings, such as the Psoriasis Epidemiological Screening Tool (PEST).
– PEST does not detect axial arthritis or inflammatory back pain
• As soon as psoriatic arthritis is suspected, refer to a rheumatologist for assessment and advice about planning their care.
NICE clinical guideline 153 ‘The assessment and management of psoriasis’. 2012. Available at: http://www.nice.org.uk/nicemedia/live/13938/61190/61190.pdf. Date accessed: November 2013.

Psoriatic Disease
Arthritis
Skin and nails
Enthesitis
Dactylitis
Axial Disease
Metabolic Syndrome
Inflammatory bowel
disease
Uveitis
Identifying PsA
• Dermatology
– Recognize relevant MSKL sxs among Pso pts
– CASPAR may not yet be applicable without a definition of inflammatory arthritis
• Rheumatology
– Distinguish inflammatory and non-inflammatory disease
– Identify PsA within inflammatory arthritis
– CASPAR criteria applicable to all patients
Clinical Presentation of PsA
Peripheral Arthritis
Arthritis
Present
Absent
Helliwell, et al. ARD. 2007;66:113-7.
Mease P, van der Heijde D. Int J Adv Rheumatol. 2006;4:38-48.
PsA: Radiographic Features
• Juxta-articular periostitis and ankylosis
• Joint osteolysis(pencil-in-cup)
PM3
Other Radiological Features of PsA
Tuft Resorption
Periostitis
Mease P, van der Heijde D. Int J Adv Rheumatol. 2006;4:38-48.

Slide 53
PM3 Reference I have added to this slide and next is a general review article on radiologic features of PsA and is not specific to the specific imagesadmin, 10/29/2014
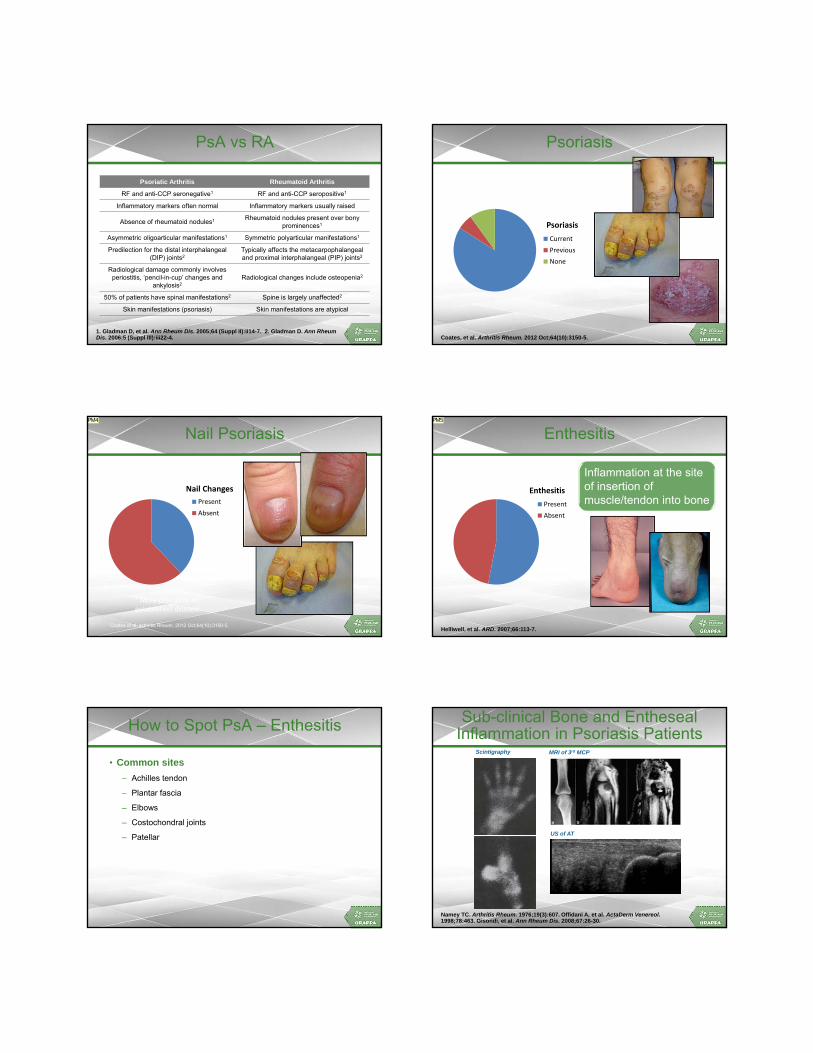
PsA vs RA
Psoriatic Arthritis Rheumatoid Arthritis
RF and anti-CCP seronegative1 RF and anti-CCP seropositive1
Inflammatory markers often normal Inflammatory markers usually raised
Absence of rheumatoid nodules1 Rheumatoid nodules present over bony prominences1
Asymmetric oligoarticular manifestations1 Symmetric polyarticular manifestations1
Predilection for the distal interphalangeal(DIP) joints2
Typically affects the metacarpophalangealand proximal interphalangeal (PIP) joints2
Radiological damage commonly involves periostitis, ‘pencil-in-cup’ changes and
ankylosis2Radiological changes include osteopenia2
50% of patients have spinal manifestations2 Spine is largely unaffected2
Skin manifestations (psoriasis) Skin manifestations are atypical
1. Gladman D, et al. Ann Rheum Dis. 2005;64 (Suppl II):ii14-7. 2. Gladman D. Ann Rheum Dis. 2006;5 (Suppl III):iii22-4.
Psoriasis
Psoriasis
Current
Previous
None
Coates, et al. Arthritis Rheum. 2012 Oct;64(10):3150-5.
Nail Psoriasis
Nail Changes
Present
Absent
Coates et al, Arthritis Rheum. 2012 Oct;64(10):3150-5.
* More prevalent in established disease
PM4
Enthesitis
Enthesitis
Present
Absent
Helliwell, et al. ARD. 2007;66:113-7.
Inflammation at the site of insertion of muscle/tendon into bone
PM5
How to Spot PsA – Enthesitis
• Common sites
– Achilles tendon
– Plantar fascia
– Elbows
– Costochondral joints
– Patellar
MRI of 3rd MCP
Namey TC. Arthritis Rheum. 1976;19(3):607. Offidani A, et al. ActaDerm Venereol. 1998;78:463. Gisondi, et al. Ann Rheum Dis. 2008;67:26-30.
T2W
US of AT
Scintigraphy
Sub-clinical Bone and EnthesealInflammation in Psoriasis Patients
Slide 57
PM4 The figure I have thought was correct was that nail changes were seen in 85% of PsA patients, yet this pie diagram suggests more like 40%. Am I interpreting this correctly and therefore I am way off in my understanding? admin, 10/29/2014
Slide 58
PM5 remove build pleaseadmin, 10/29/2014

Lower Limb Enthesopathy in Psoriasis Patients without PsA
• Ultrasound evaluation of Achilles, quadriceps, patellar entheses and plantar aponeurosis according to Glasgow Ultrasound EnthesitisScoring System (GUESS)
– 30 psoriasis patients
– 30 controls
• The mean thickness of all tendons was higher in psoriasis patients than controls
• Mean GUESS score was significantly higher with 7.9 in psoriasis patients vs. 2.9 in controls
enthesophyte
Bursitis
Gisondi, et al. Ann Rheum Dis. 2008;67:26-30.*Girolomoni, et al. JEADV. 2009;23(Suppl. 1):3-8.
“10% of patients with psoriasisprogressed to PsA over 2 yrs”*
Dactylitis
Dactylitis
Present
Absent
Helliwell, et al. ARD. 2007;66:113-7.
uniform/fusiformswelling of a digit
PM6
Spinal Involvement
Spinal pain/stiffness
Present
Absent
Helliwell, et al. ARD. 2007;66:113-7.
How to Spot PsA – Axial Disease
Inflammatory back pain
• Chronic back pain >3 months
• Onset at age <40 yrs
• Pain eased by exercise, worse at rest
• Early morning stiffness
• Waking in second half of the night
PsA in Dermatology Clinics
OA, 24
No MSK diagnosis,
28
SeverePsA,7
MildPsA,10
Other, 17
Husni. JAAD. 2007;57(4):581-7.
Referral to Rheumatology
• Arthralgia that doesn’t settle
• Inflammatory features
– Early morning stiffness
– Better with exercise
– Swollen joints
– Enthesitis
– Low back / buttock pain

Slide 62
PM6 remove build pleaseadmin, 10/29/2014

Screening Tools for PsA
• Most people have psoriasis before joint symptoms
• Is there a simple screening test for PsA?– Quick and easy
– Patient completed
– Sensitive
– Reasonably specific
• Patient-completed questionnaires– PAQ (1997) and modified PAQ (2002)
– PASE (2007)
– ToPAS (2008)
– PEST (2008)
– PASQ (2009)
PAQ = Psoriasis and Arthritis Questionnaire; PASE = Psoriatic Arthritis Screening and Evaluation. ToPAS = Toronto Psoriatic Arthritis Screen; PEST = Psoriasis Epidemiology Screening Tool. PASQ =Psoriatic Arthritis Screening Questionnaire.
PASE – Symptoms
• I feel tired for most of the day
• My joints hurt
• My back hurts
• My joints become swollen
• My joints feel ‘hot’
• Occasionally, my entire finger or toe becomes swollen, making it look like a ‘sausage’
• I have noticed that the pain in my joints moves from one joint to another, for example, my wrist will hurt for a few days, then my knee will hurt, and so on
Husni M, et al. J Am Acad Dermatol. 2007;57:581-7.
ToPAS 1 and 2
Features:
• Pictures
• Questions on
– joint symptoms
– back pain
– dactylitis
Gladman D, et al. Ann Rheum Dis. 2009;68:497-501.
PEST
• Have you ever had a swollen joint (or joints)?
• Has a doctor ever told you that you have arthritis?
• Do your finger nails or toe nails have holes or pits?
• Have you had pain in your heel?
• Have you had a finger or toe that was completely swollen and painful for no apparent reason?
Ibrahim G, et al. Clin Exp Rheumatol. 2009;27:469-74.
In the drawing below, please tick the joints that have
caused you discomfort (i.e stiff, swollen or painful joints)
CONTEST Study
• Head-to-head comparison of PASE, ToPAS and PEST
• 10 dermatology secondary care clinics in the UK
• All patients given questionnaires, in random order
• Any positive responder invited back for full rheumatological examination
Coates LC, et al. Br J Dermatol. 2013168(4):802-7.
CONTEST: Results
938 distributed
657 returned
314 positive by any tool
195 examined
47 psoriatic arthritis
Coates, et al, BJD. 2013 epub ahead of print.

CONTEST Study: Results
ToPAS PASE PEST
Sens = 76.6Spec = 29.7
Sens = 74.5Spec = 38.5
Sens = 76.6Spec = 37.2
AUC = 0.554 AUC = 0.594 AUC = 0.610
Coates LC, et al. Br J Dermatol. 2013168(4):802-7.
CONTEST Conclusions
• Sensitivity and specificity considerably lower than in original development
• NOT true sensitivity/specificity
– Sensitivity overestimated
– Specificity underestimated
• Also identified 54 patients with other arthritides
– 40 had degenerative tendinopathy or OA
Coates LC, et al. Br J Dermatol. 2013168(4):802-7.
CONTEST Results: Incidence of PsA
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1 positive 2 positive 3 positive
% of patients w
ith PsA
Number of positive screening questionnaires
Coates, et al. BJD. 2013 epub ahead of print.
Identifying PsA in Early Arthritis Clinics
• Presence of psoriasis!
• Psoriatic nail disease
• Negative immunology
• Features of SpA
• Use CASPAR features...
ROC Analysis
Criteria Score Sensitivity Specificity
Moll and Wright N/A 80 99
CASPAR 1 100 43
2 99 95
3 87 99
4 42 100
5 15 100
6 0 100
Coates, et al. Arthritis and Rheum. Oct 2012. ENB1049a Date of Preparation November 2012.
PsA Disease – Complex and Variable
Images supplied by Laura Coates, University of Leeds, UK.
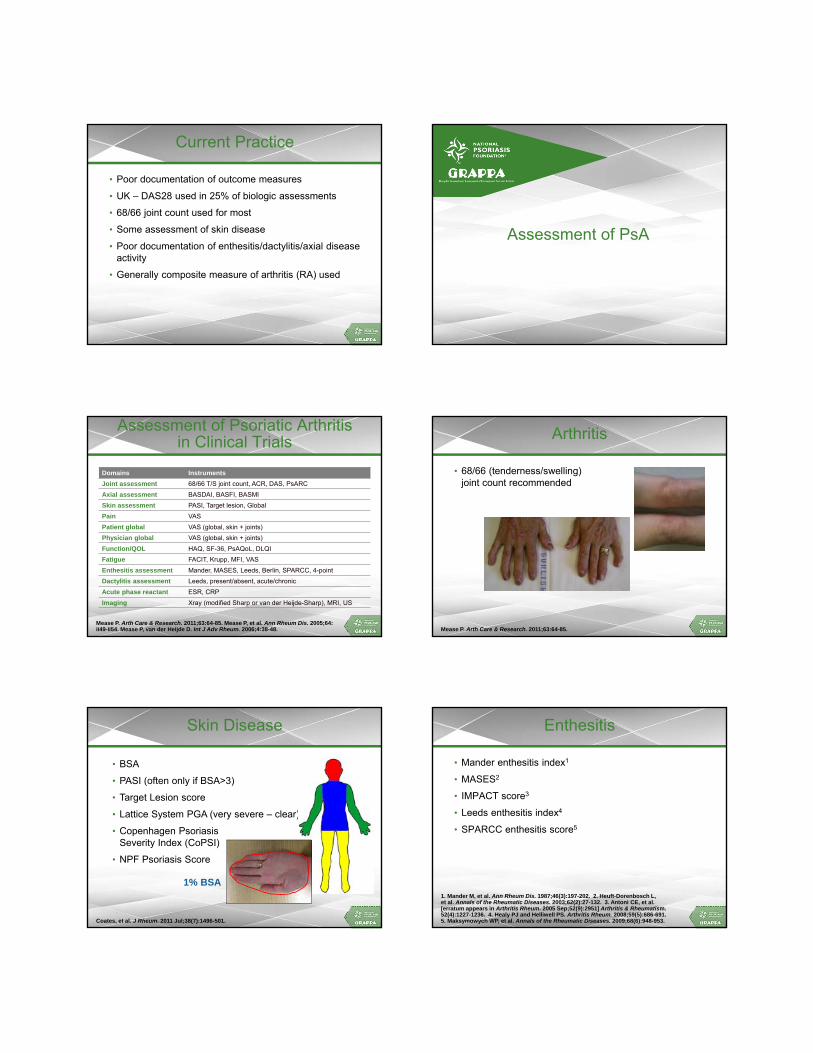
Current Practice
• Poor documentation of outcome measures
• UK – DAS28 used in 25% of biologic assessments
• 68/66 joint count used for most
• Some assessment of skin disease
• Poor documentation of enthesitis/dactylitis/axial disease activity
• Generally composite measure of arthritis (RA) used
Assessment of PsA
Assessment of Psoriatic Arthritis in Clinical Trials
Domains Instruments
Joint assessment 68/66 T/S joint count, ACR, DAS, PsARC
Axial assessment BASDAI, BASFI, BASMI
Skin assessment PASI, Target lesion, Global
Pain VAS
Patient global VAS (global, skin + joints)
Physician global VAS (global, skin + joints)
Function/QOL HAQ, SF-36, PsAQoL, DLQI
Fatigue FACIT, Krupp, MFI, VAS
Enthesitis assessment Mander, MASES, Leeds, Berlin, SPARCC, 4-point
Dactylitis assessment Leeds, present/absent, acute/chronic
Acute phase reactant ESR, CRP
Imaging Xray (modified Sharp or van der Heijde-Sharp), MRI, US
Mease P. Arth Care & Research. 2011;63:64-85. Mease P, et al. Ann Rheum Dis. 2005;64:ii49-ii54. Mease P, van der Heijde D. Int J Adv Rheum. 2006;4:38-48.
Arthritis
• 68/66 (tenderness/swelling) joint count recommended
Mease P. Arth Care & Research. 2011;63:64-85.
• BSA
• PASI (often only if BSA>3)
• Target Lesion score
• Lattice System PGA (very severe – clear)
• Copenhagen Psoriasis Severity Index (CoPSI)
• NPF Psoriasis Score
Coates, et al. J Rheum. 2011 Jul;38(7):1496-501.
Skin Disease
1% BSA
Enthesitis
• Mander enthesitis index1
• MASES2
• IMPACT score3
• Leeds enthesitis index4
• SPARCC enthesitis score5
1. Mander M, et al. Ann Rheum Dis. 1987;46(3):197-202. 2. Heuft-Dorenbosch L, et al. Annals of the Rheumatic Diseases. 2003;62(2):27-132. 3. Antoni CE, et al. [erratum appears in Arthritis Rheum. 2005 Sep;52(9):2951] Arthritis & Rheumatism. 52(4):1227-1236. 4. Healy PJ and Helliwell PS. Arthritis Rheum. 2008;59(5):686-691. 5. Maksymowych WP, et al. Annals of the Rheumatic Diseases. 2009;68(6):948-953.

Assessing Enthesitis - LEI
• Lateral epicondyle of elbow
• Medial condyle of femur
• Achilles tendon insertion
Healy PJ and Helliwell PS. Arthritis Rheum. 2008;59(5):686-691.
Assessing Enthesitis - SPARCC
• Supraspinatus
• Med/lat epicondyles
• Greater trochanter
• Patellar insertion
• Quads insertion
• Tibial tuberosity
• Achilles tendons
• Plantar fascia
Dactylitis
• Simple count (tender/swollen)1
• Count + grade 0-3 score2
• Leeds Dactylitis Instrument (LDI)3
Images supplied by Laura Coates, University of Leeds, UK
1. Kyle S, et al. Rheumatology. 2005;44:390-7. 2. Antoni CE, et al. [erratum appears in Arthritis Rheum. 2005 Sep;52(9):2951] Arthritis & Rheumatism. 52(4):1227-1236. 3. Helliwell PS, et al. Journal of Rheumatology. 2005;32(9):1745-1750.
Axial Disease
• BASDAI – doesn’t differentiate axial activity
• BASFI – doesn’t differentiate axial activity
• BASMI
• ASDAS
Image supplied by Laura C
oates, University
of Leeds, U
K
Coates, et al. J Rheum. 2011 Jul;38(7):1496-501.
IMPART: Arthritis and Dactylitis
MeasureOverall
ICC (95% CI)Rheumatologist
ICC (95% CI)Dermatologist ICC
(95% CI)
Tender joint count
0.78 (0.65, 0.89) 0.81 (0.68, 0.91) 0.73 (0.56, 0.86)
Swollenjoint count
0.24 (0.12, 0.45) 0.42 (0.23, 0.65) 0.31 (0.12, 0.57)
Dactylitis 0.29 (0.15, 0.51) 0.69 (0.52, 0.84) 0.08 (-0.07, 0.32)
PGA-PsA 0.39 (0.23, 0.60) 0.29 (0.11, 0.54) 0.50 (0.29, 0.72)
PGA = physician’s global assessment; ICC = intraclass correlation coefficients. Chandran V, et al. Arthritis Rheum. 2009;27;61:1235-1242.
PM7
Quality of Life and Function
• SF-36
• EQ5D
• DLQI
• PsAQOL
• HAQ-DI
– MID 0.35
• HAQ-S
Mease P. Arth Care & Research. 2011;63:64-85. Mease P, et al. J Rheum. 2011;38:2461-5.
Slide 89
PM7 ICC for swollen joint count for "Overall" is 0.24? Yet ICC for rheum is 0.42 and derm is 0.31 so theoretically the Overall should be in between those two numbers. Please check manuscript. admin, 10/29/2014

Composite Measures ofPsoriatic Disease
ENB1049a Date of Preparation November 2012
Composite Assessment of PsA
• Composite Measures of Arthritis
– DAS
– ACR responses
– PsARC
– DAPSA
– PsAJAI
– CDAI
– SDAI
• Composite Measures of PsA
– MDA
– CPDAI
– PASDAS
– AMDF
Mease P. Arth Care & Research. 2011;63:64-85.
A Disease State Measure
• Minimal disease activity is ideal concept
– “a state which is deemed a useful target of treatment by both physician and patient, given current treatment possibilities and limitations”
• Can act as a target for treatment
• Developed for PsA including 7 key outcome measures covering arthritis, enthesitis, skin disease, patient reported outcomes and functional ability
Wells GA, et al. J Rheumatol. 2005;32:2016-24; Coates LC, et al. Ann Rheum Dis. 2010;69(1):48-53.
MDA Criteria for PsA
• A patient is classified as in MDA when they meet 5 of 7 of the following criteria:
– tender joint count ≤1
– swollen joint count ≤1
– PASI ≤1 or BSA ≤3
– patient pain VAS ≤15
– patient global activity VAS ≤20
– HAQ ≤0.5
– tender entheseal points ≤1
Coates LC, et al. Ann Rheum Dis. 2010;69(1):48-53.
Observational Database - Toronto
• n=344
• 59% male, mean age 43 years
Coates LC, et al. Arthritis Care and Res. 2010;62(7):970-6.
Patients Achieving MDA
>1 year
<1 year
never
0
0.5
1
1.5
2
2.5
3
MDA not MDA
Progression of Joint Damage per year
Increasedamaged JC
P=.0005
Interventional Trial Cohort
• Achieving MDA in IMPACT and IMPACT2 studies
Coates LC, et al. Arthritis Care and Res. 2010;62(7):965-9.
0
5
10
15
20
25
30
35
40
45
50
55
Week 16 Week 52
Percentage of patients achieving M
DA
Infliximab
Placebo
Week 16 P<.0001
0
5
10
15
20
25
30
35
40
45
50
55
Week 24 Week 52
Percentage of patients achieving M
DA
Infliximab
Placebo
Week 24 P<.001

MDA
• Validated measure of disease state
• Doesn’t measure disease activity
• Now being reported as outcome in RCTs
• Being used in clinical trials as target
Coates LC, et al. Arthritis Care and Res. 2010;62(7):965-9 and 970-6. Coates, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101.
Composite Psoriatic Disease Activity Index (0 -15)
None (0) Mild (1) Moderate (2) Severe (3)
Peripheral Arthritis NONE≤ 4 joints; normal function (HAQ ≤0.5)
≤ 4 joints but function impaired; or > 4 joints, normal function
> 4 joints and function impaired
Skin Disease NONE PASI ≤ 10 and DLQI ≤ 10PASI ≤ 10 but DLQI >10; or PASI > 10 but DLQI ≤ 10
PASI > 10 and DLQI > 10
Enthesitis NONE≤ 3 sites; normal function (HAQ ≤0.5)
≤ 3 sites but function impaired; or >3 sites but normal function
>3 sites and function impaired
Dactylitis NONE≤ 3 digits; normal function (HAQ ≤0.5))
≤ 3 digits but function impaired; or >3 digits but normal function
>3 digits and has function impaired
Spinal Disease NONEBASDAI ≤4; normal function (ASQol ≤ 6)
BASDAI >4 but normal function; BASDAI ≤4 but function impaired
BASDAI >4 and function impaired
HAQ only counted for most severe domain involved (enthesitis/dactylitis/peripheral arthritis)
Mumtaz, A. Ann Rheum Dis. 2011;70:272-7.
GRACE Project (GRAPPA)
• Longitudinal international cohort
• High disease activity identified by increase in therapy
• 2 different methods for development
– PASDAS
• following methodology of RA DAS or ASDAS
• Logistic regression to develop weighting
– AMDF
• Each component translated to 0-1 desirability function
• Simple addition of each component
PASDAS
• 0.18 x √physician global
• + 0.159 x √patient global
• - 0.253 x √SF36-PCS
• + 0.101 x ln (SJC+1)
• + 0.048 x ln (TJC+1)
• + 0.23 x ln (LEI+1)
• + 0.37 x ln (tender dactylitis count+1)
• + 0.102 x ln (CRP+1)
Helliwell PS, et al. Ann Rheum Dis. 2013;72:986-991.
AMDF
• Sum of
– TJC
– SJC
– HAQ
– Patient VAS global
– Patient VAS joints
– Patient VAS skin
– PASI
– PsAQOL
Helliwell PS, et al. Ann Rheum Dis. 2013;72:986-991.
Optimizing Rolesof Dermatologist and Rheumatologist
Screening for PsA in at-risk population
Confirm presence of inflammatory arthritis in pt with psoriasis
Post-Activity Question 1
How confident are you in your ability to establish a clinical framework to diagnose and screen the psoriasis patient for psoriatic arthritis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 2
PASI includes a component for patient reported outcomes.
1. True
2. False
Post-Activity Question 3
For what percentage of psoriasis patients do you intend to perform an annual assessment for PsA?
1. 0-25%
2. 26-50%
3. 51-75%
4. 76-100%
Questions & Answers

5/28/2015
1
Comorbidities of Psoriasis and PsA
Joel M. Gelfand, MD, MSCEMedical Director, Clinical Studies Unit
Associate Professor of Dermatology and EpidemiologySenior Scholar, Center for Clinical Epidemiology and Biostatistics
Perelman School of MedicineUniversity of Pennsylvania
Prof. Dr. Wolf-Henning BoehnckeChair, Department of Dermatology
Geneva University HospitalGeneva, Switzerland
M. Elaine Husni, MD, MPHVice Chair of Rheumatology
Director, Arthritis and Musculoskeletal Center, Cleveland ClinicAssistant Professor, Cleveland Clinic Lerner College
of Medicine of Case Western Reserve UniversityCleveland, Ohio
Sergio Schwartzman, MDAssociate Professor of Clinical Medicine
Weill Medical College of Cornell UniversityThe Hospital for Special SurgeryNew York Presbyterian Hospital
New York, New York
Content Developers
Paolo Romanelli, MDAssociate Professor of Medicine
Department of DermatologyUniversity of Miami
Miami, FL
Speaker Pre-Activity Question 1
Psoriatic arthritis is NOT known to be an independent risk factor for which of the following:
1. Carotid artery plaques
2. Cardiovascular disease
3. Diabetes
Pre-Activity Question 2
What percentage of new psoriasis cases may be associated with obesity?
1. 20%
2. 30%
3. 76%
4. 80%
Psoriatic Arthritis and Psoriasis
• >10% of psoriasis patients seen by dermatologists had undiagnosed PsA1
• PsA generally occurs after onset of psoriasis
• PsA may be progressive and can cause permanent joint damage
• Prevalence of PsA increases with severity of skin disease but severity of PsA correlates only weekly with skin disease severity
1. Mease PJ, et al. JAAD. 2013;69:729-35. 2. Gelfand JM, et al. JAAD. 2005;53:773-7.
StrataPrevalence
95% CI2
All psoriasis 11% (9, 14)
No, little psoriasis 6% (4, 10)
1-2% BSA 14% (9, 21)
3-10% BSA 18% (10, 28)
10+% BSA 56% (34, 76)
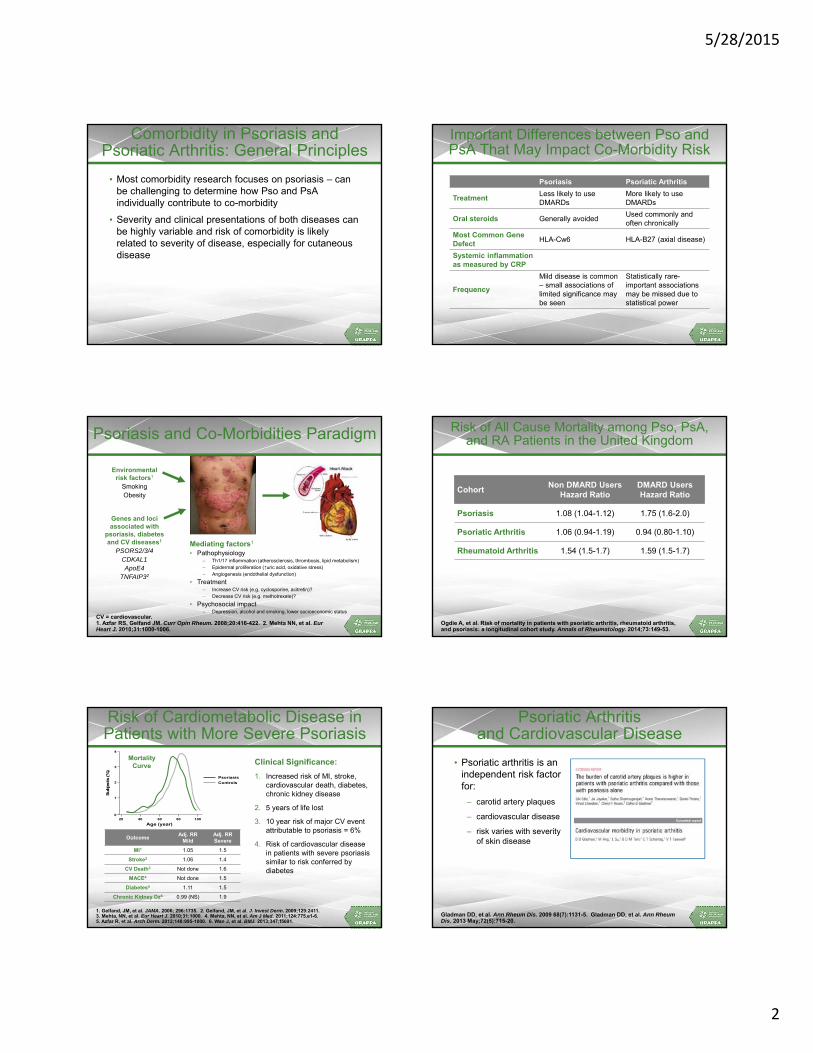
5/28/2015
2
Comorbidity in Psoriasis andPsoriatic Arthritis: General Principles
• Most comorbidity research focuses on psoriasis – can be challenging to determine how Pso and PsA individually contribute to co-morbidity
• Severity and clinical presentations of both diseases can be highly variable and risk of comorbidity is likely related to severity of disease, especially for cutaneous disease
Important Differences between Pso and PsA That May Impact Co-Morbidity Risk
Psoriasis Psoriatic Arthritis
TreatmentLess likely to use DMARDs
More likely to use DMARDs
Oral steroids Generally avoidedUsed commonly and often chronically
Most Common Gene Defect
HLA-Cw6 HLA-B27 (axial disease)
Systemic inflammation as measured by CRP
Frequency
Mild disease is common – small associations of limited significance may be seen
Statistically rare-important associations may be missed due to statistical power
CV = cardiovascular.1. Azfar RS, Gelfand JM. Curr Opin Rheum. 2008;20:416-422. 2. Mehta NN, et al. EurHeart J. 2010;31:1000-1006.
Psoriasis and Co-Morbidities Paradigm
Mediating factors1
• Pathophysiology– Th1/17 inflammation (atherosclerosis, thrombosis, lipid metabolism)– Epidermal proliferation (↑uric acid, oxidative stress)– Angiogenesis (endothelial dysfunction)
• Treatment– Increase CV risk (e.g. cyclosporine, acitretin)?– Decrease CV risk (e.g. methotrexate)?
• Psychosocial impact – Depression, alcohol and smoking, lower socioeconomic status
Genes and loci associated with
psoriasis, diabetes and CV diseases1
PSORS2/3/4CDKAL1ApoE4
TNFAIP32
Environmentalrisk factors1
SmokingObesity
Risk of All Cause Mortality among Pso, PsA,and RA Patients in the United Kingdom
CohortNon DMARD Users
Hazard RatioDMARD UsersHazard Ratio
Psoriasis 1.08 (1.04-1.12) 1.75 (1.6-2.0)
Psoriatic Arthritis 1.06 (0.94-1.19) 0.94 (0.80-1.10)
Rheumatoid Arthritis 1.54 (1.5-1.7) 1.59 (1.5-1.7)
Ogdie A, et al. Risk of mortality in patients with psoriatic arthritis, rheumatoid arthritis, and psoriasis: a longitudinal cohort study. Annals of Rheumatology. 2014;73:149-53.
Risk of Cardiometabolic Disease in Patients with More Severe Psoriasis
Clinical Significance:
1. Increased risk of MI, stroke, cardiovascular death, diabetes, chronic kidney disease
2. 5 years of life lost
3. 10 year risk of major CV event attributable to psoriasis = 6%
4. Risk of cardiovascular disease in patients with severe psoriasis similar to risk conferred by diabetes
1. Gelfand, JM, et al. JAMA. 2006; 296:1735. 2. Gelfand, JM, et al. J. Invest Derm. 2009;129:2411. 3. Mehta, NN, et al. Eur Heart J. 2010;31:1000. 4. Mehta, NN, et al. Am J Med. 2011;124:775.e1-6. 5. Azfar R, et al. Arch Derm. 2012;148:995-1000. 6. Wan J, et al. BMJ. 2013;347;f5691.
OutcomeAdj. RR
MildAdj. RR Severe
MI1 1.05 1.5
Stroke2 1.06 1.4
CV Death3 Not done 1.6
MACE4 Not done 1.5
Diabetes5 1.11 1.5
Chronic Kidney Dz6 0.99 (NS) 1.9
0
3
Subje
cts
(%
)
Age (year)
4
60
2
1
80 100 40 20
Psoriasis
Controls
Psoriasis
Controls
MortalityCurve
Psoriatic Arthritisand Cardiovascular Disease
• Psoriatic arthritis is anindependent risk factor for:
– carotid artery plaques
– cardiovascular disease
– risk varies with severity of skin disease
Gladman DD, et al. Ann Rheum Dis. 2009 68(7):1131-5. Gladman DD, et al. Ann Rheum Dis. 2013 May;72(5):715-20.

5/28/2015
3
Risk of All Cause MACE among Pso, PsA,and RA Patients in the United Kingdom
Ogdie A, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis, and rheumatoid arthritis: A population-based cohort study. Annals of Rheumatology in press.
CohortNon DMARD Users
Hazard RatioDMARD UsersHazard Ratio
Psoriasis 1.08 (1.02-1.15) 1.42 (1.17-1.73)
Psoriatic Arthritis 1.24 (1.03-1.49) 1.17 (0.95-1.46)
Rheumatoid Arthritis 1.39 (1.28-1.50) 1.58 (1.46-1.70)
Risk of CV Death among Pso, PsA,and RA Patients in the United Kingdom
Ogdie A, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis, and rheumatoid arthritis: A population-based cohort study. Annals of Rheumatology in press.
CohortNon DMARD Users
Hazard RatioDMARD UsersHazard Ratio
Psoriasis 1.09 (1.00-1.20) 1.54 (1.15-2.05)
Psoriatic Arthritis 1.07 (0.79-1.44) 0.96 (0.64-1.43)
Rheumatoid Arthritis 1.43 (1.28-1.59) 1.66 (1.48-2.05)
The ‘Psoriatic March’: A Pathogenetic Concept ofHow Severe Psoriasis May Drive CV Comorbidity
PSORIASIS OBESITY
SYSTEMIC INFLAMMATION
INSULIN RESISTANCE
ENDOTHELIAL DYSFUNCTION
ATHEROSCLEROSIS
MYOCARDIAL INFARCTION
Boehncke WH, et al. BMJ. 2010.
Does Treatment of RALower the Risk of CV Events?
• Methotrexate:
– Meta-analysis of 10 observational studies (9 RA, 1 polyarthritis, 1 psoriasis)
– RR 0.79 (0.73-0.87) cardiovascular disease
• TNF-inhibitors
– Meta-analysis of 13 observational studies in RA
– RR cardiovascular events 0.46 (0.28-0.77)
Micha R, et al. Systematic reviews and meta-analysis of methotrexate use and risk of CV disease. Am J Cardiol. 2011;108:1362-1370. Barnabe C, et al. Systematic review and meta-analysis: Anti TNF alpha therapy and cardiovascular events in rheumatoid arthritis. Arth Care and Res. 2011:63:522-529. Ljung L, et al. Treatment with TNF inhibitors and the risk of acute coronary syndromes in early RA. Arth and Rheum. 2012;64:42-52.Al-Aly Z, et al. TNF alpha blockade, cardiovascular outcomes, and survival in RA Translational Research. 2011;157:10-18.
Does Treatment of PsoriasisLower CV Events?
• VA cohort: Low-dose methotrexate is associated with lower risk of vascular disease compared to patients not receiving methotrexate (RR: 0.50, 95% CI 0.31–0.79)1
• Kaiser cohort: Lower rate of MI in TNF inhibitor vs. topical (HR: 0.50, 95% CI 0.32–0.81) and in methotrexate vs. topical (HR: 0.52, 95% CI 0.31–0.85)2
• Danish cohort: Lower rate of death, MI, stroke in patients treated with biologic (HR: 0.28, 95% CI 0.12–0.64) and methotrexate (HR: 0.50, 95% CI 0.26–0.97) compared to other therapies (cyclosporine, phototherapy, acitretin)3
• Taiwan claims data: No effect of methotrexate compared to treatment with retinoids, cyclosporine, azathioprine, mycophenolate (HR 0.97, 95% CI 0.79–1.19)4
• Meta-analysis of RCTs: TNF inhibitors and IL-12/23 inhibitors show no benefit on major CV events and IL-12/23 inhibitors possibly show harm5
• US claims data: HR 1.33 (95% CI 0.90–1.96) of methotrexate, cyclosporine, alefacept, efalizumab, adalimumab, etanercept and infliximab compared to phototherapy6
1. Prodanovich S, et al. J Am Acad Dermatol. 2005;52:262-267. 2. Wu JJ, et al. Arch Dermatol. 2012;148:1244-1250. 3. Ahlehoff O, et al. J Int Med. 2013;273:197-204. 4. Chen YJ, et al. Arthritis Rheum. 2012;64:1879-1887. 5. Ryan C, et al. JAMA. 2011;306:864-871. 6. Abuabara K, et al. Br J Dermatol. 2011;165:1066-1073.
YES
NO
Randomized Placebo Controlled Trials Evaluating Impact of Anti-Inflammatory Treatment on CV Risk
• Vascular Inflammation in Psoriasis Trial (VIP) and VIP-Ustekinumab
– Does treatment with adalimumab or phototherapy lower vascular inflammation and improve lipid metabolism in patients with moderate to severe psoriasis? (NCT01553058)
– Does treatment with ustekinumab lower vascular inflammation and improve lipid metabolism in patients with moderate to severe psoriasis (NCT02187172)
• Cardiovascular Inflammation Reduction Trial (CIRT)
– Does methotrexate lower the risk of major vascular events in patients with a history of MI and diabetes or metabolic syndrome? (NCT01594333)
• Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS)
– Does interleukin-1β (IL-1β) inhibition reduce rates of MACE among stable coronary artery disease hsCRP (2 mg/L) (NCT01327846)

5/28/2015
4
Clinical Implications: Elevated Cardiovascular Risk in Psoriatic Disease
Standard Screening Recommendations
• Hypertension
– Every 2 year if BP <120/80 mm Hg
– Every year if BP 120 to 139/80 to 89 mm Hg.
• Diabetes (Fasting plasma glucose, HbA1c, or OGTT)
– Adults ≥ 45
– Adults BMI ≥25kg/m2 who have one or more additional RFs
– Repeat every 3 years
• Cardiovascular risk assessment:
– Traditional risk factors every 4-6 years in patients 20-79
– Estimate 10 year risk in those 40 -79
US Preventative Services Task Force (HTN) 2007. American Diabetes Association Guidelines. 2014 (Diabetes Care 2014;37:S5-S13). ACC/AHA 2013 Guideline on the assessment of CV risk.
ACC = American College of Cardiology; AHA = American Heart Association; ASCVD = athereosclerotic cardiovascular disease.Goff DC, et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk.
Implementation of Risk Assessment Work Group Recommendations
Risk based on:
• Sex
• Race
• Age
• Total cholesterol
• HDL
• Systolic BP
• HTN treatment status
• Diabetes
• Current smoking status
Does the patient haveexisting clinical ASCVD?
See AHA/ACC SecondaryPrevention Guideline
Is the patient<20 y or >79 y of age?
See Pediatric Guidelinesand ACC/AHA Adult
Primary Prevention Guidelines• Blood Cholesterol
• Obesity
Assess traditional risk factorsevery 4-6 y in patients
20-79 y of age:Estimate 10-y risk in
those 40-79 y of age usingPooled Cohort Equations
Communicate risk data andrefer to ACC/AHA
Prevention Guidelines• Blood Cholesterol
• Obesity
Assess 30-y or lifetime riskin those 20-59 y of age:Communicate risk data
regardless of age and refer toAHA/ACC Lifestyle Guideline
Yes
Yes
Elevated10-y Risk(≥7.5%
No
No
Low 10-y Risk (<7.5%)
Stone NJ, et al. 2013 ACC/AHA Guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults.
Major Recommendations for Statin Therapy for ASCVD Prevention
Statin Benefit Groups
1. Clinical ASCVD
2. LDL-C>190 mg/dl
3. Age 40-75 with DM and LDL-C 70-=189 mg/dl without ASCVD
4. Age 40-75 with LDL-C 70-189 mg/dL and have 10 year ASCVD ≥ 7.5%
Definitions of High- andModerate-Intensity
Statin Therapy
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention.
In individuals not receiving cholesterol-lowering drug therapy, recalculate estimated10-y ASCVD risk every 4-6 y in individuals aged 40-75 y without clinical ASCVD
or diabetes and with LDL-C 70-189 mg/dL.
ASCVD Prevention Benefit of Statin Therapy may be less clear in other groupsIn selected individuals, consider additional factors influencing ASCVD risk and
potential ACSVD risk benefits and adverse effects, drug-drug interactions,and patient preferences for statin treatment.
Estimate 10-y ASCVD riskwith Pooled Cohort Equations
≥7.5% Estimated10-y ASCVD Riskand age 40-75 y
ClinicalASCVD
LDL-C≥190 mg/dL
DiabetesType 1 or 2Age 40-75 y
No
Yes
No
No
No
Age ≤75 y High-Intensity Statin(Moderate-intensity statin if not
candidate for high-intensity statin)
Age >75 y OR if not candidatefor High-Intensity Statin
Moderate-intensity Statin
High-Intensity Statin(Moderate-intensity statin if not
candidate for high intensity statin)
Moderate-Intensity Statin
Estimated 10-y ASCVD risk ≥7.5%High-Intensity Statin
Moderate-to-High Intensity Statin
Yes
Yes
Yes
Adults age >21 y anda candidate for statin therapy
Yes
HighDaily dose
lowers LDL-Cby approx.
≥50%
ModerateDaily dose
lowers LDL-Cby approx.
30% to <50%
Risk of Diabetes among Patients with Incident PsA, Psoriasis, and RA in the United Kingdom
Dubreuil M, et al. The Independent Impact of Psoriatic Arthritis, Psoriasis, and Rheumatoid Arthritis on Diabetes Incidence: A UK Population-Based Cohort Study. Rheumatology In press.
Cohort N Patients Hazard Ratio
Adjusted forAge and Sex
FullyAdjusted
Psoriasis 4196 1.72 1.33
Psoriatic Arthritis 59,281 1.39 1.21
Rheumatoid Arthritis 11,158 1.12 0.94
Metabolic Syndrome Components Increase with Affected BSA
Langan SM, Seminara NM, Shin DB, Troxel A, Kimmel SE, Mehta NN, Margolis DJ, and Gelfand JM. Prevalence of metabolic syndrome in patients with psoriasis: A population based study in the United Kingdom. Journal of Investigative Dermatology. 2012 Mar;132:556-62.
1
1.1
1.2
1.3
1.4
1.5
1.6
1.7
Trigs Glucose Obesity
Od
ds
Ra
tio
<3% BSA
3-10% BSA
10+% BSA
Obesity and Psoriasis
• Obesity may be a risk factor for psoriasis and possibly for psoriatic arthritis
• 30% of new psoriasis cases are attributable to obesity
• Psoriasis associated with metabolic syndrome in both children and adults
Naldi, et al. JID. 2005;125:61-67. Setty, et al. Arch Int Medicine. 2007;167:1670-75. Love JT, et al. Arch Derm. 2010:doi:10.1001/archdermatol.2010.370. Koebnick C, et al. J of Pediatrics. 2011.03.006. Soltani-Arabshahi R. Arch Derm. 2010;146:721-6.

5/28/2015
5
Impact of BMI onPsoriasis Treatment Effectiveness
Takeshita, et al. SID. 2014. Clark & Lebwohl. JAAD. 2008;58:443-6.
0
10
20
30
40
50
60
70
80
Adalimumab Etanercept Methotrexate
Cle
ar
or A
lmos
t Cle
ar P
reva
lenc
e (%
)
Under or Normal Weight (BMI ˂ 25)
Overweight (25 ≤ BMI ˂ 30)
Obese (BMI ≥ 30)
P for trend = 0.002
P for trend = 0.01
Obesity Is a Negative Predictor of Achieving and Maintaining MDA
HR for not achieving MDA In PsA
• 1st-Degree Obesity (BMI <30 kg/m2) 3.98 (95% CI 1.96–8.06,P<.001)
• 2nd-Degree Obesity (BMI 30–35 kg/m2)5.40 (95% CI 3.09–9.43, P<.001)
Di Minno, et al. Arthritis Care & Research. 2013;65(1):141-147.
Normal Weight(n=135)
10
100
11st Degree Obesity
(n=100)2nd Degree Obesity
(n=35)
Ris
k (
HR
) o
fN
ot
Ac
hie
vin
g M
DA
Obesity, Diabetes, Metabolic Syndromeand Psoriasis: Clinical Implications
• Recommend maintenance of normal body weight in those at greatest risk of developing psoriasis (e.g. + FH)
• Screening for diabetes and lipid disorders in patients with psoriasis, particularly when severe
– Fasting plasma glucose ≥ 126 mg/dl or HbA1c ≥ 6.5% or random glucose > 200 mg/dl in symptomatic patients
– Pre-diabetes fasting glucose 100-125 mg/dl, HbA1c5.7%-6.4%.
Inzucchi SE. Diagnosis of Diabetes. NEJM. 2012;367:542-550.
Obesity, Diabetes, Metabolic Syndromeand Psoriasis: Clinical Implications
• Altered risk/benefit profile of treatment– Decrease efficacy of non-weight based treatments
– Methotrexate: more aggressive monitoring with liver biopsies
*Methotrexate toxicity is associated with a history of total lifetime alcohol intake before methotrexate therapy. The exact amount of alcohol that confers risk is unknown and differs among persons.Kalb RE, et al. JAAD. 2009;60:824-37.
Risk Factors for Hepatic Toxicity from Methotrexate
• History of or current alcohol consumption*
• Persistent abnormal liver chemistry studies
• History of liver disease, including chronic hepatitis B or C
• Family history of inheritable liver disease
• Diabetes mellitus
• Obesity
• History of significant exposure to hepatotoxic drugs or chemicals
• Lack of folate supplementation
• Hyperlipidemia
Monitoring for Hepatotoxicity in High-Risk Patients
• Consider the use of a different systemic agent
• Consider delayed baseline liver biopsy (after 2 to 6 months of therapy to establish medication efficacy and tolerability)
• Repeat liver biopsies after approximately 1.0 to 1.5 g of therapy
Smoking and Psoriatic Disease
• Smoking may be a risk factor for psoriasis1
– Rationale – Nicotine activates dendritic cells, T cells, and Th-1 cytokines
• Heavy smoking associated with more severe psoriasis2
• Among psoriasis patients smoking may be associated with a decreased risk of PsA3
• Smoking associated with worse PsA symptoms and poorer response to TNF inhibitors4
1. Naldi, et al. JID. 2005; 125:61-67. 2. Fortes, et al. Arch Derm. 2005;141:1580-84. 3. Eder L, et al. Ann Rheum Dis. 2012;71:219-24. 4. Hojgaard P, et al. Ann Rheum Dis. doi:10.1136/annrheumdis-2014-205389.
Alcohol and Psoriasis
• Excess alcohol intake associated with:
– Psoriasis, particularly in males
– More severe psoriasis
– Treatment noncompliance
Kurd, et al. Expert Rev Clin Immunol. 2007;3:171-185.
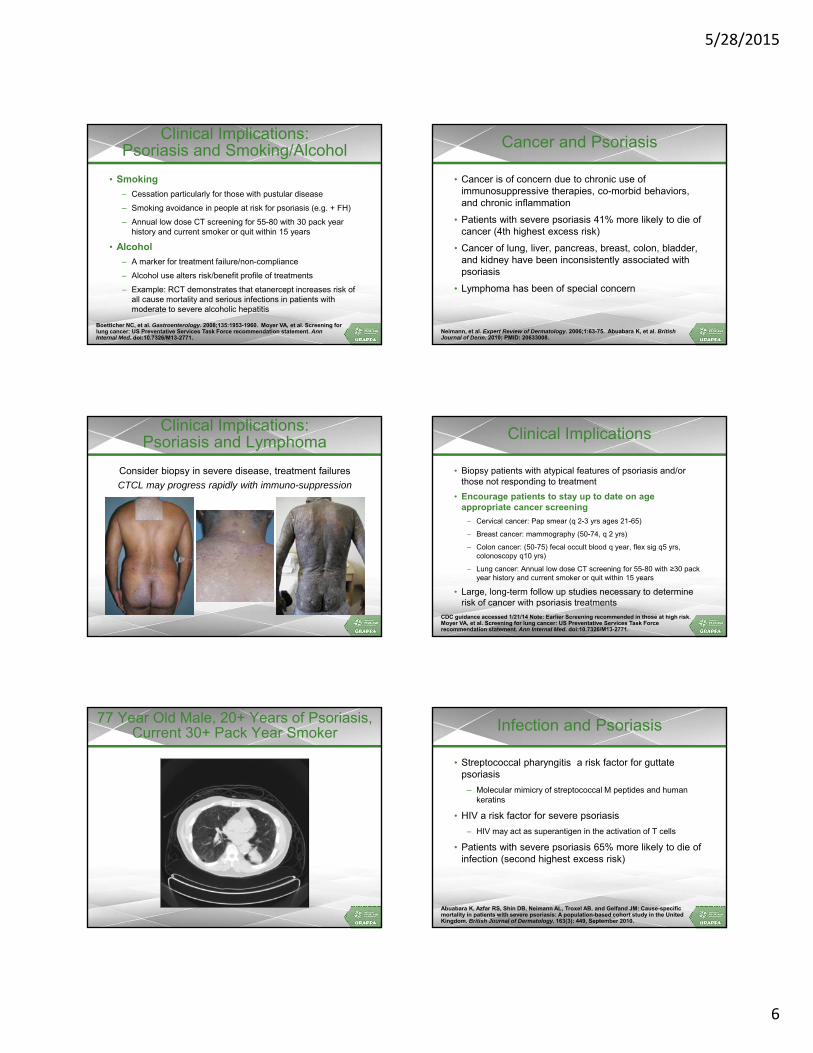
5/28/2015
6
Clinical Implications:Psoriasis and Smoking/Alcohol
• Smoking
– Cessation particularly for those with pustular disease
– Smoking avoidance in people at risk for psoriasis (e.g. + FH)
– Annual low dose CT screening for 55-80 with 30 pack year history and current smoker or quit within 15 years
• Alcohol
– A marker for treatment failure/non-compliance
– Alcohol use alters risk/benefit profile of treatments
– Example: RCT demonstrates that etanercept increases risk of all cause mortality and serious infections in patients with moderate to severe alcoholic hepatitis
Boetticher NC, et al. Gastroenterology. 2008;135:1953-1960. Moyer VA, et al. Screening for lung cancer: US Preventative Services Task Force recommendation statement. Ann Internal Med. doi:10.7326/M13-2771.
Cancer and Psoriasis
• Cancer is of concern due to chronic use of immunosuppressive therapies, co-morbid behaviors, and chronic inflammation
• Patients with severe psoriasis 41% more likely to die of cancer (4th highest excess risk)
• Cancer of lung, liver, pancreas, breast, colon, bladder, and kidney have been inconsistently associated with psoriasis
• Lymphoma has been of special concern
Neimann, et al. Expert Review of Dermatology. 2006;1:63-75. Abuabara K, et al. British Journal of Derm. 2010; PMID: 20633008.
Clinical Implications: Psoriasis and Lymphoma
Consider biopsy in severe disease, treatment failures
CTCL may progress rapidly with immuno-suppression
Clinical Implications
• Biopsy patients with atypical features of psoriasis and/or those not responding to treatment
• Encourage patients to stay up to date on age appropriate cancer screening
– Cervical cancer: Pap smear (q 2-3 yrs ages 21-65)
– Breast cancer: mammography (50-74, q 2 yrs)
– Colon cancer: (50-75) fecal occult blood q year, flex sig q5 yrs, colonoscopy q10 yrs)
– Lung cancer: Annual low dose CT screening for 55-80 with ≥30 pack year history and current smoker or quit within 15 years
• Large, long-term follow up studies necessary to determine risk of cancer with psoriasis treatments
CDC guidance accessed 1/21/14 Note: Earlier Screening recommended in those at high risk.Moyer VA, et al. Screening for lung cancer: US Preventative Services Task Forcerecommendation statement. Ann Internal Med. doi:10.7326/M13-2771.
77 Year Old Male, 20+ Years of Psoriasis, Current 30+ Pack Year Smoker Infection and Psoriasis
• Streptococcal pharyngitis a risk factor for guttatepsoriasis
– Molecular mimicry of streptococcal M peptides and human keratins
• HIV a risk factor for severe psoriasis
– HIV may act as superantigen in the activation of T cells
• Patients with severe psoriasis 65% more likely to die of infection (second highest excess risk)
Abuabara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, and Gelfand JM: Cause-specific mortality in patients with severe psoriasis: A population-based cohort study in the United Kingdom. British Journal of Dermatology. 163(3): 449, September 2010.

5/28/2015
7
Clinical Implications: Psoriasis and Infection
• Screen for Streptococcal infection with guttate flares
• Screen for HIV in severe psoriasis
• Vaccination for
– influenza (annually)
– pneumonia (PCV13 and PPSV23)
– zoster (age ≥60)
• Live vaccine – not recommended while on immune suppression
– hepatitis B
– HPV (ages 9-26)
Wine-Lee L, et al. JAAD. 2013; 69(6):1003. http://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf
Psoriasis and Mood Disorders:Clinical Outcomes Data
OutcomeHazardRatio
Extra Cases associated with Psoriasis per Year in UK
Depression 1.4 10,400
Anxiety 1.3 7,100
Suicidality 1.44 350
Kurd SK, Troxel AB, Crits-Christoph P, and Gelfand JM. Arch Dermatol. 2010:146:891-5.
Psoriasis and Mood Disorders:Clinical Implication
• Ask about depression and anxiety symptoms and monitor impact of treatment on psychiatric symptoms
• Refer for treatment as appropriate
• Some data to suggest that cognitive-behavioral therapies and meditation may modestly enhance response to psoriasis treatments
Kabat-Zinn J, et al. Psychosomatic Medicine. 1998 60:625-632. Zachariae R, et al. J Am Acad Dermatol. 1996;34:1008-15.
Emerging Co-Morbidities
• Sleep apnea
• Nonalcoholic steatohepatitis (NASH)
• Chronic obstructive pulmonary disease (COPD)
• Adverse infectious disease outcomes• Chronic and end stage renal disease
• Peptic ulcer disease
• Osteoporosis
Callis Duffin K, et al. JAAD. 2009;60:604-8. Wakkee, et al. JAAD. 2011;65:1135-44. Van der Voort ET, et al. JAAD. 2014;70:517-24. Yeung H, et al. JAMA Derm. 2013;149:1173-9. Yang YW, et al. Br J Derm. 2011;165:1037-43. Reddy SA, et al. J Rheumatol. 2010;37:1-7.
Conclusion
• Evolving literature identifying:
– Environmental Risk Factors for psoriasis
– Diseases which may occur as a consequence of chronic psoriasis
• More research needed to determine how psoriatic treatment increases or decreases the risk of metabolic, cardiovascular, psoriatic arthritis, and cancer outcomes
• Important implications for the management of psoriatic disease
John D. Reveille, MDProfessor of Medicine
University of Texas Medical School at HoustonHouston, Texas
Speaker

5/28/2015
8
IBD
Extra Dermal andExtra-Articular Manifestations
Immune Mechanisms Shared between IBD and SpA
• Genetic susceptibility
• Aberant recognition of self
• Autoantibodies against specific antigens shared by the colon and other extra-colonic tissues
• Increased intestinal permeability
• Microbiome
• Infection
Articular involvement in IBD Prevalence: 16-33%
GI tract involvement in SpAPrevalence: 70%Long-term: 7-12% SpA will develop overt IBD
Lymphocyte recirculationMigration pathway altered by adhesion molecules and chemokines
Intestinal lymphocytes traffic to joints
Activated intestinal lymphocytes in IBD patients adhere to inflamed synovial tissues via adhesion molecules like VAP-1
NOD2/CARD 15/IBD1 mutationsLink to CD and SpA bowel inflammation and isolated sacroiliitis
HLA-B2750-78% of IBD patients with AS are HLA-B27+
*J Crohns and Colitis. 2010:4:257.
Pathophysiology: Gut-Joint Axis in Inflammatory Bowel Disease*
Hypopyon Uveitis
WBC layer in lower anterior chamber

5/28/2015
9
Ciliary Flush Classification
• Anatomy
• Time Course
• Etiology
Classification – Etiology
• Autoimmune
• Infectious
• Misc.
Etiology
Systemic Illness
Over 50 different disease states
Idiopathic
Autoimmune
Etiology – Autoimmune
• HLA-B27 associated uveitis
– Ankylosing spondylitis
– Reactive Arthritis
– Psoriatic arthropathy
– Inflammatory bowel disease
• Sarcoidosis
• Behcet’s disease
• Juvenile Idiopathic Arthritis
Prevalence of Uveitis in Spondyloarthropathies
1. Literature review 957 articles identified, 126 used
2. Acute in 88.7%
3. Unilateral in 87.3%
Zeboulon, et al. Ann Rheum Dis. 2008;67:955-959.
Prevalence of Uveitis % (SD)
All SpA 32.7 (0.5)
AS 33.2 (0.8)
PsA 25.1 (2.3)
IBD associated Arthritis 36.9 (4.4)
Reactive Arthritis 25.6 (3.8)
Undifferentiated SpA 13.2 (2.9)

5/28/2015
10
Psoriatic Autoimmune Ophthalmic Involvement
Psoriatic Disease Psoriasis 6 PsA 15
Additional Systemic Illnesses Sarcoid 3 RA 3
7
3 3
2
1
0 0
3
Pattern of Musculoskeletal Involvement
Number of Patients
6
3
5
4
2
1 1
Ocular Manifestations
Number of Patients
Schwartzman, et al. ACR. 2014.
Ocular Manifestations
• 30% of patients had only skin disease.
• Although it appears that anterior uveitis is the most common autoimmune ocular manifestation in this cohort it is frequently chronic, differentiating this ocular manifestation from the pattern in Ankylosing Spondylitis.
• 29% of patients had an overlap of two underlying systemic autoimmune diseases.
• The most common pattern of PsA in patients with autoimmune ophthalmic disease is the oligoarticular form.
Post-Activity Question 1
Psoriatic arthritis is NOT known to be an independent risk factor for which of the following:
1. Carotid artery plaques
2. Cardiovascular disease
3. Diabetes
Post-Activity Question 2
What percentage of new psoriasis cases may be associated with obesity?
1. 20%
2. 30%
3. 76%
4. 80%
Questions & Answers
5/28/2015
1
Management of Psoriasis and PsA:Biologics and Non-Biologics
Content Developers
Amit Garg, MDAssociate Professor and Founding ChairDepartment of DermatologyHofstra NSLIJ School of MedicineNorth Shore LIJ Health SystemManhasset, New York
Philip Mease, MDDirector, Rheumatology ResearchSwedish Medical CenterClinical ProfessorUniversity of Washington School of MedicineSeattle, Washington
Prof Oliver FitzGerald, MD, FRCP(UK), FRCPIConsultant Rheumatologist and Newman Clinical Research Professor St. Vincent's University Hospital and Conway Institute for Biomolecular ScienceUniversity College Dublin, Ireland
Alice Bendix Gottlieb, MD, PhDChair and Dermatologist in ChiefHarvey B Ansell Professor of DermatologyTufts Medical Center and Tufts University School of MedicineBoston, Massachusetts
Arthur Kavanaugh, MDProfessor of MedicineUniversity of California, San Diego San Diego, California
Speakers
Luis R. Espinoza, MDProfessor and Chief
Section of RheumatologyLSUHSC at New OrleansNew Orleans, Louisiana
Amit Garg, MDAssociate Professor and Founding Chair
Department of DermatologyHofstra NSLIJ School of Medicine
North Shore LIJ Health SystemManhasset, New York
Pre-Activity Question 1
MTX has been shown to result in a significantly greater improvement in ACR20 response compared to placebo.
1. True
2. False
Pre-Activity Question 2
How confident are you in describing the mechanism of action of PDE4 Inhibitors?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 3
How confident are you in describing the mechanism of action of JAK inhibitors?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
5/28/2015
2
Non-Biologic Therapies for Psoriasis
• Keratolytics– Salicylic Acid, Urea
• Corticosteroids
• Vit D Analogs– Calipotriene
• Calcineurin inhibitors– Tacrolimus
• Topical Retinoids– Tazarotene
• Tars– Goeckerman Technique
– Ingram Technique
• Anthralins– Dihydroxyanthralin
• UV Light– UVA +/- psoralen, UVB, narrow
band UVB
• 311nm laser device
• Methotrexate
• Cyclosporine
• Acitretin
• Emerging Therapies
Topical Treatments for Psoriasis
Topical Therapies
• Most commonly prescribed form of treatment
• Frequently used in combination with other topicals and with systemic therapies
• Several options
– Over the counter (OTC)
– Prescription
• Typically applied once or twice a day, each
• Vehicle matters
– effect, side effect
– creams, ointments, lotions, solutions, foams, gels, shampoos, and baths
Keratolytics
• Help to debride scale and allow other medications to penetrate better.
• Urea 20%-80% cream and gel
• Sal Acid: 3-5% in cold cream or hydrophilic ointments
– Rare: salicylate toxicity with tinnitus, confusion, refractory hypoglycemia, esp in Pts with diabetes or renal disease.
Corticosteroids
• Suprapotent (Class I) Corticosteroids for body and extremities
• Low potency for body folds and face
• Pick one in each class and remember it!
– Class 1: clobetasol, halobetasol
– Class 6: desonide, hydrocortisone
• Consideration of vehicle
• Rotational or alternating therapy to minimize AEs
Vitamin D Analog
• Calcipotriene 0.005% or Calcitriol
– Vitamin D3 analog that regulates KC differentiation
– Available as cream, ointment or solution
– Ointment form works best
– Should be applied 2x/day to be effective
– May be irritating to unaffected skin
– Often used in combination/rotation with a topical steroid
• Also comes branded in combination with betamethasone dipropionate

5/28/2015
3
Calcineurin inhibitors
• Tacrolimus 0.03%, 0.1% ointment; Pimecrolimus 1% cream
– Inhibits T-cell activation by inhibiting the synthesis and release of cytokines (IL-2) from T-cells.
– Ointment vehicle works best
– Better on thin skin areas (ie face, groin)
– Should be applied 2x/day to be effective
– May cause local irritation
– May be in rotation with a topical steroid
Retinoids
• Tazarotene 0.05%, 0.1% cream and gel
– Vitamin A derivative that binds retinoic acid receptors (RAR β and RAR γ)
– Modulates KC differentiation and proliferation, and suppresses inflammation
– Local irritation is treatment limiting
Phototherapy
Phototherapy
• Light unit directing ultraviolet light in specific wavelengths to affected areas
• Proposed mechanisms:
– Alterations in cytokine expression with suppression of Th1/Th17 inflammatory axis
– Apoptosis of several cell types in the skin
• Activated T cells in epidermis and dermis, Keratinocytes, and to a lesser degree Langerhans cells
– Suppression of Langerhans cell function
• Present day utilization: nbUVB >>> PUVA
Wong, et al. J Cutan Med Surg. 2013 Jan-Feb; 17(1): 6-12.
Phototherapy
• Narrow Band Ultraviolet B (NBUVB)
– Most efficacious for thin plaque psoriasis and especially guttate psoriasis
– Monotherapy or in combination with topical or systemic treatments
– Administered 2-3 times week. Patients may clear in 25-30 treatments.
– Requires maintenance treatments to retain efficacy
– Less carcinogenic than broad band UVB and UVA
– Copay and Time Lost are barriers
Laser Device Therapy
• 311 nm device
– Hand-held lasers emits a focused wavelength of light
– Best for treating individual plaques and small areas
– May not be widely available
– Well tolerated with low risk

5/28/2015
4
Non-Biologic Systemic Medications
for Psoriasis
Methotrexate
• Exact MOA of MTX for inflammatory disease is complex.
• MTX transported into variety of cells
• Intracellular glutamation
• MTXGlun inhibition of key enzymes in the folate pathway
• Inhibition and accumulation of AICAR and ATIC nucleotides increased adenosine into circulation.
• Extracellular adenosine increased cAMP
• cAMP inhibits production of pro-inflammatory cytokines (TNF-α, IFN-γand IL-1β)
Montesinos, et al. Adenosine A2A or A3 receptors are required for inhibition of inflammation by methotrexate and its analogue MX-68. Arthritis Rheum. 2003, 48:240-247.Ochaion, et al. Methotrexate enhances the anti-inflammatory effect of CF101 via up-regulation of the A3 adenosine receptor expression. Arthritis Res Ther. 2006,8:R169.
Methotrexate
• Dose: 10-25 mg weekly + folic acid 1mg daily
• PASI 75 achieved in 35-42%
• AEs: GI upset, oral ulcers, hair shedding, fatigue >>> marrow suppression, hepatic fibrosis, pulmonary fibrosis
• Pregnancy category: X
Barker, et al. Efficacy and safety of infliximab vs methotrexate in patients with moderate-to-severe plaque psoriasis: results of an open-label, active-controlled, randomized trial (RESTORE1). Br J Dermatol. 2011;165(5):1109-17.Saurat, et al. Efficacy and safety results from the randomized controlled comparative study of adalimumab vs methotrexate vsplacebo in patients with psoriasis (CHAMPION). Br J Dermatol. 2008;158:558-566.
Menter, et al. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol 2009;61:451-85.
Liver Biopsy?
Cyclosporine
• CSA 5 mg/kg/day yielded PAS75 response in 50 to 97% of patients
• CSA 2.5 mg/kg/day yielded PASI 75 response in 28 to 85%.
• Remission could be maintained at CSA dose of at least 3mg/kg/day More than 50% of patients treated with CSA may have an increase in serum creatinin value >30% of baseline if treatment is prolonged for 2 years.
• CSA 2.5 mg/kg/day effective in 89% of patients with palmoplantarpustulosis.
• CSA 3 to 5 mg/kg/day yielded a significant improvement in >50% of patients with erythrodermic psoriasis
Maza, et al. JEADV. 2011, 25 (Suppl. 2), 19-27.
Acitretin
• Dose: 10-50mg daily
• Oral retinoid that slows KC proliferation and stimulates differentiation
• Interferes with intracellular metabolism of natural retinoids. Competes with retinoic acid for CRABP binding and activates retinoic acid nuclear receptors
• Teratogen. Not given to women of child bearing age.
• Etretinate formed when acitretin used with ethanol.
– Detected in 100% patients with an average weekly consumption of >200g ethanol (15 pints of beer)
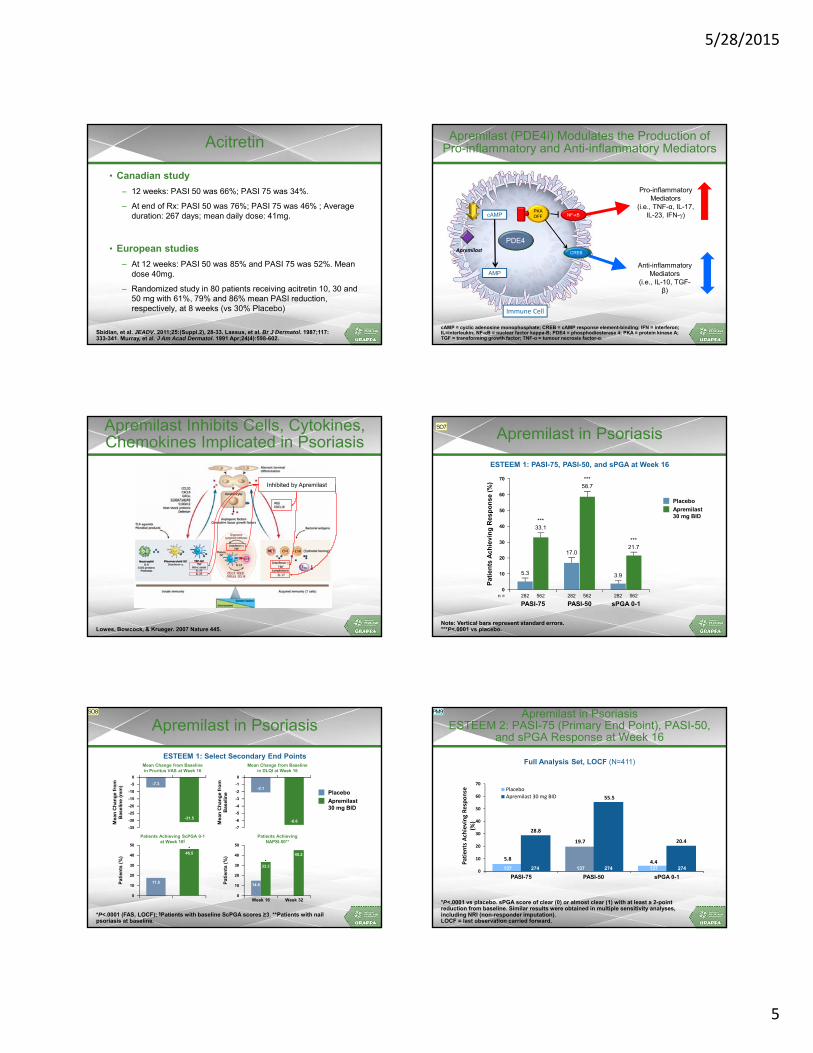
5/28/2015
5
Acitretin
• Canadian study
– 12 weeks: PASI 50 was 66%; PASI 75 was 34%.
– At end of Rx: PASI 50 was 76%; PASI 75 was 46% ; Average duration: 267 days; mean daily dose: 41mg.
• European studies
– At 12 weeks: PASI 50 was 85% and PASI 75 was 52%. Mean dose 40mg.
– Randomized study in 80 patients receiving acitretin 10, 30 and 50 mg with 61%, 79% and 86% mean PASI reduction, respectively, at 8 weeks (vs 30% Placebo)
Sbidian, et al. JEADV. 2011;25:(Suppl.2), 28-33. Lassus, et al. Br J Dermatol. 1987;117:333-341. Murray, et al. J Am Acad Dermatol. 1991 Apr;24(4):598-602.
Anti-inflammatoryMediators
(i.e., IL-10, TGF-β)
Pro-inflammatoryMediators
(i.e., TNF-α, IL-17, IL-23, IFN-)
Immune Cell
cAMP
PDE4
AMP
Apremilast CREB
NF-κBPKAONPKAOFF
CREB
Apremilast (PDE4i) Modulates the Production of Pro-inflammatory and Anti-inflammatory Mediators
cAMP = cyclic adenosine monophosphate; CREB = cAMP response element-binding; IFN = interferon; IL=interleukin; NF-B = nuclear factor kappa-B; PDE4 = phosphodiesterase 4; PKA = protein kinase A; TGF = transforming growth factor; TNF-α = tumour necrosis factor-α.
Lowes, Bowcock, & Krueger. 2007 Nature 445.
Apremilast Inhibits Cells, Cytokines, Chemokines Implicated in Psoriasis
Inhibited by Apremilast
Apremilast in Psoriasis
Note: Vertical bars represent standard errors.***P<.0001 vs placebo.
ESTEEM 1: PASI-75, PASI-50, and sPGA at Week 16
70
50
40
30
20
10
0
PASI-75 PASI-50 sPGA 0-1
Pa
tie
nts
Ac
hie
vin
g R
es
po
ns
e (
%)
Apremilast30 mg BID
Placebo60
5.3
17.0
3.9
***33.1
***21.7
***58.7
282 282 282562 562562n =
SO7
Apremilast in Psoriasis
*P<.0001 (FAS, LOCF); §Patients with baseline ScPGA scores ≥3. **Patients with nail psoriasis at baseline.
ESTEEM 1: Select Secondary End PointsMean Change from Baselinein Pruritus VAS at Week 16
Apremilast30 mg BID
Placebo
0
20
Pat
ien
ts (
%) 40
10
30
50
Patients Achieving ScPGA 0-1at Week 16§
*46.5
17.5
Mean Change from Baselinein DLQI at Week 16
Week 320
20
Pat
ien
ts (
%)
Week 16
40
10
30
50
Patients AchievingNAPSI-50**
45.2
14.9
-4
-6
-35
-15
Mea
n C
han
ge
fro
mB
asel
ine
(mm
) -5
-25
-10
0
-31.5
-7.3
-7
-3
Mea
n C
han
ge
fro
mB
asel
ine
-1
-5
-2
0
-6.6
-2.1
-20
-30
*33.3
14.9
SO8 Apremilast in PsoriasisESTEEM 2: PASI-75 (Primary End Point), PASI-50,
and sPGA Response at Week 16
*P<.0001 vs placebo. sPGA score of clear (0) or almost clear (1) with at least a 2-point reduction from baseline. Similar results were obtained in multiple sensitivity analyses, including NRI (non-responder imputation). LOCF = last observation carried forward.
5.8
19.7
4.4
28.8
55.5
20.4
0
10
20
30
40
50
60
70
Patients Achieving Response
(%)
PlaceboApremilast 30 mg BID
*
*
PASI-75 PASI-50
137 274 137 274
*
137 274
sPGA 0-1
Full Analysis Set, LOCF (N=411)
PM9
Slide 28
SO7 put at the top Apremilast in Psoriasis and then the current title in smaller font below that. Reference would need to be found.Stacey Ohana, 10/30/2014
Slide 29
SO8 needs Apremilast in Psoriasis at the top then current title as a subtitle in smaller fontStacey Ohana, 10/30/2014
Slide 30
PM9 This is a slide provided by Alice. Will need a reference which perhaps can be found in pubmed if published - otherwise would be an abstract ref that Alice will need to supplyadmin, 10/26/2014
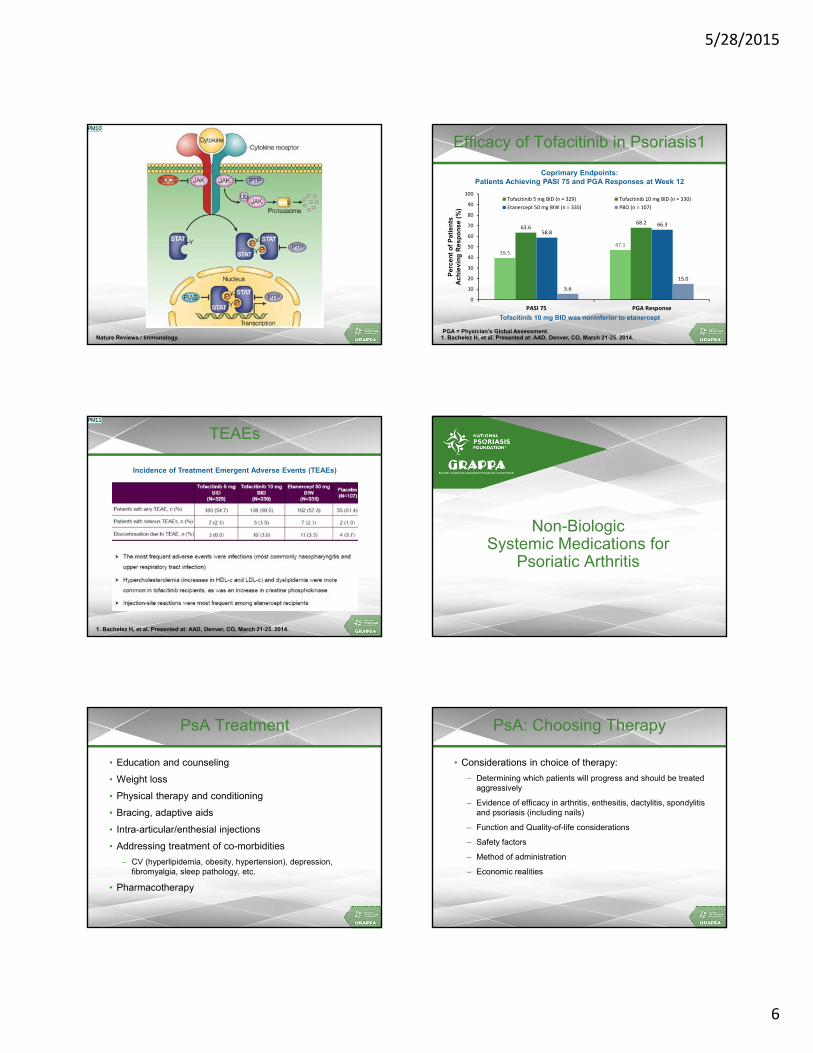
5/28/2015
6
Nature Reviews / Immunology.
PM10
Efficacy of Tofacitinib in Psoriasis1
39.5
47.1
63.668.2
58.8
66.3
5.6
15.0
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PGA Response
Tofacitinib 5 mg BID (n = 329) Tofacitinib 10 mg BID (n = 330)
Etanercept 50 mg BIW (n = 335) PBO (n = 107)
Pe
rce
nt
of
Pa
tie
nts
A
ch
iev
ing
Re
sp
on
se
(%
)
PGA = Physician’s Global Assessment.1. Bachelez H, et al. Presented at: AAD, Denver, CO, March 21-25. 2014.
Tofacitinib 10 mg BID was noninferior to etanercept
Coprimary Endpoints: Patients Achieving PASI 75 and PGA Responses at Week 12
1. Bachelez H, et al. Presented at: AAD, Denver, CO, March 21-25. 2014.
TEAEs
Incidence of Treatment Emergent Adverse Events (TEAEs)
PM11
Non-BiologicSystemic Medications for
Psoriatic Arthritis
PsA Treatment
• Education and counseling
• Weight loss
• Physical therapy and conditioning
• Bracing, adaptive aids
• Intra-articular/enthesial injections
• Addressing treatment of co-morbidities
– CV (hyperlipidemia, obesity, hypertension), depression, fibromyalgia, sleep pathology, etc.
• Pharmacotherapy
PsA: Choosing Therapy
• Considerations in choice of therapy:
– Determining which patients will progress and should be treated aggressively
– Evidence of efficacy in arthritis, enthesitis, dactylitis, spondylitis and psoriasis (including nails)
– Function and Quality-of-life considerations
– Safety factors
– Method of administration
– Economic realities

Slide 31
PM10 This was a slide provided by Alice. I do not know the specific referenceadmin, 10/26/2014
Slide 33
PM11 This is a slide provided by Alice summarizing the safety issues of the tofa in pso trial (see previous slide which I provided on efficacy). This will need an overall title indicating it is about tofa in pso and bringingthe ref over from the previous slideadmin, 10/26/2014

5/28/2015
7
GRAPPA: Treatment Guidelinesfor PsA on the Basis of Severity
Mild
Moderateto severe
Peripheral arthritis
Skin and nail disease
Axial disease Dactylitis Enthesitis
NSAID
IA STEROIDS
DMARDsBIOLOGICS(ANTI-TNF)
TOPICALS
PUVA/UVB
DMARD
DMARDsBIOLOGICS
NSAID
PHYSIO
ANALGESIA
BIOLOGICS)
BIOLOGICS)
BIOLOGICS
NSAID
INJECTION
NSAIDS
PHYSIO
STEROIDS
Reassess response to therapy and toxicity if patient fails to demonstrate an acceptable clinical improvement over an appropriate period
DMARDsBIOLOGICS
Kavanaugh A, Ritchlin C. J Rheum. 33;1417-1456.
EULAR PsA Management Recomendations: Use of Synthetic DMARDs in PsA
• Patients with active PsA and a potentially poor prognosis should be started on DMARDs
– According to the EULAR guidelines for management of PsA, methotrexate (MTX) is the first choice synthetic DMARD for PsA
– Synthetic DMARDs do not appear to be effective for the treatment of enthesitis and axial disease
– None of the synthetic DMARDs have demonstrated efficacy for limiting structural damage in PsA
Gossec L, et al. Ann Rheum Dis. 2012;71:4-12.
Steroid Injections
• Sacroiliac and peri-sacroiliac steroid injections appear beneficial in small randomized trials.
• Steroid injection of inflamed peripheral joints may be beneficial
Traditional PsA Therapy
• Nonsteroidal anti-inflammatory drugs
• Corticosteroids
• DMARDs
– Sulfasalazine
– Methotrexate
– Leflunomide
– Cyclosporine
– Antimalarials
Mease P. Ann Rheum Dis. 2011;70(1):i77-i84. Gladman DD. Rheum Dis Clin North Am. 1998.
DMARDs in PsA
DrugN RCTs /
N PatientsN OtherStudies
Main Results
Methotrexate 3 / 93 7Joints and skin: Modest efficacyXrays, enthesitis, dactylitis: no data
Sulfasalazine 7 / 666 2Joints:Modest efficacySkin no efficacyXrays, enthesitis, dactylitis: no data
Leflunomide 1 / 190 3Joints and skin: Modest efficacyXrays, enthesitis, dactylitis: no data
Cyclosporine 3 / 206 6
Short term effficacy on joints (modest) and skin – long-termtoxicityXrays, enthesitis, dactyliits no data
Ash Z, et al. Ann Rheum Dis. 2012;71:319-26. Mease P. Ann Rheum Dis. 2011;70(1):i77-i84. Kingsley GH, et al. Rheumatology. 2012 51(8):1368-77.
Effectiveness of MTX in PsA in a Randomized, Placebo-Controlled Trial (MIPA)
• No evidence of a significant effect of MTX on PsARC, ACR20, DAS28, joint counts, ESR, CRP, pain and HAQ scores after 6 months treatment
• The only significant benefits of MTX treatment of PsA were in physician and patient global assessments (P=.03 and P<.001, respectively) and skin scores (P=.02)
Global Index after 6 Mo OR (95% CI) P-value
PsARC 1.77 (0.9, 3.23) .06
ACR20 2.00 (0.66, 6.22) .23
DAS28 1.70 (0.90, 2.17) .10
DBRCT, 221 pts, Active oligo- or polyarthritis, 6 Months

5/28/2015
8
86.3
72.5
49
66.7
39.6
18.8
0
20
40
60
80
100
ACR20 ACR50 ACR70
IFX+MTX MTX P=0.021
Pa
tie
nts
(%
)
P=.0009
P=.0018
ACR responses at week 16 in patients with PsA treated with infliximab (IFX) plus MTX (n=57) or MTX alone (n=58) in an open-label trial. All
patients were MTX naïve and were not taking DMARDs prior to treatment.
Baranauskaite A, et al. Ann Rheum Dis. 2012;71:541-548.
ACR20 ACR70ACR50
86.3
49
72.566.7
18.8
39.6
P=.0009
Effectiveness of MTX in PsA inOpen-Label RESPOND Trial
MTX
IFX+MTX
Emerging Non-Biologic Therapies in Psoriasis and PsA
Apremilast (PDE4 inhibitor)
Tofacitinib (JAK inhibitor)
Intracellular Signaling Pathways
2
2
2
2
3 4 5
6
AC = adenylyl cyclase; BTK = Bruton's tyrosine kinase; cAMP = cyclic adenosine monophosphate; ERK = extracellular signal-related kinases; IKK = inhibitor of kappa B kinase; JAK = Janus kinase; JNK = c-Jun N-terminal kinase; MAPK = mitogen-activated protein kinase; NFκB = nuclear factor kappa B; PDE = phosphodiesterase; PI3K = phosphoinositide 3-kinase; PK = protein kinase; STAT = signal transducer and activator of transcription; Syk = spleen tyrosine kinase.1. O’Sullivan L, et al. Molec Immunol. 2007;44:2497-2506. 2. Mavers M, et al. Curr Rheum Rep. 2009;11:378-85. 3. Rommel C, et al. Nat Rev Immunol. 2007;7:191-201. 4. Tasken K, et al. Physiol Rev. 2004;84:137-67. 5. Baier G, et al. Curr Opin Cell Biol. 2009;21:262-7. 6. Ruderman E, et al. Arthritis Res Ther.2011;13:125.
PALACE 1: Apremilast in PsA
• Apremilast is an oral phosphodiesterase 4 (PDE4) inhibitor
• RDBPC trial stratified for DMARD use, N=489, 1:1:1 randomization
• Major adverse events diarrhea and nausea, resolve over time
Kavanaugh A et al, Ann Rheum Dis. 2014 Jun;73(6):1020-6. doi: 10.1136/annrheumdis-2013-205056. Epub 2014 Mar 4
*
ACR20 ACR70
45
% A
ch
iev
ing
Re
sp
on
se §
ACR50
Week 16 Week 24
ACR20
Apremilast 30mg BID Apremilast 20mg BIDPlacebo
*P<0.05; §P<0.0001
§
ACR20 Response over 52 Weeks: PALACE 1, 2, 3Apremilast 30 mg BID
52
Kavanaugh A, et al. EULAR 2013 [oral presentation]. Cutolo M. SIR 2013 [oral presentation]. Cutolo M. ACR 2013 [oral presentation]. Edwards CJ, et al. ACR 2013 [poster 311].
0
10
20
30
40
50
60
70
PALACE 1
PALACE 2
PALACE 3
Study Week16 24 40 52
55.0
63.0
52.6
Patients Receiving Apremilast from BaselineData as Observed
Pa
tie
nts
Ac
hie
vin
g a
nA
CR
20
Re
sp
on
se
(%
)
PALACE 1 (Responders/n) 64/150 73/145 80/140 71/130
PALACE 2 (Responders/n) 52/145 60/138 61/121 61/116
PALACE 3 (Responders/n) 69/154 63/145 82/131 80/127
Apremilast Effects onEnthesitis and Dactylitis
*P=.02 vs placebo; †P=.01 vs placebo.Gladman DD, et al. ACR. 2013, San Diego, #816
Data Pooled from PALACE 1–3 Week 24
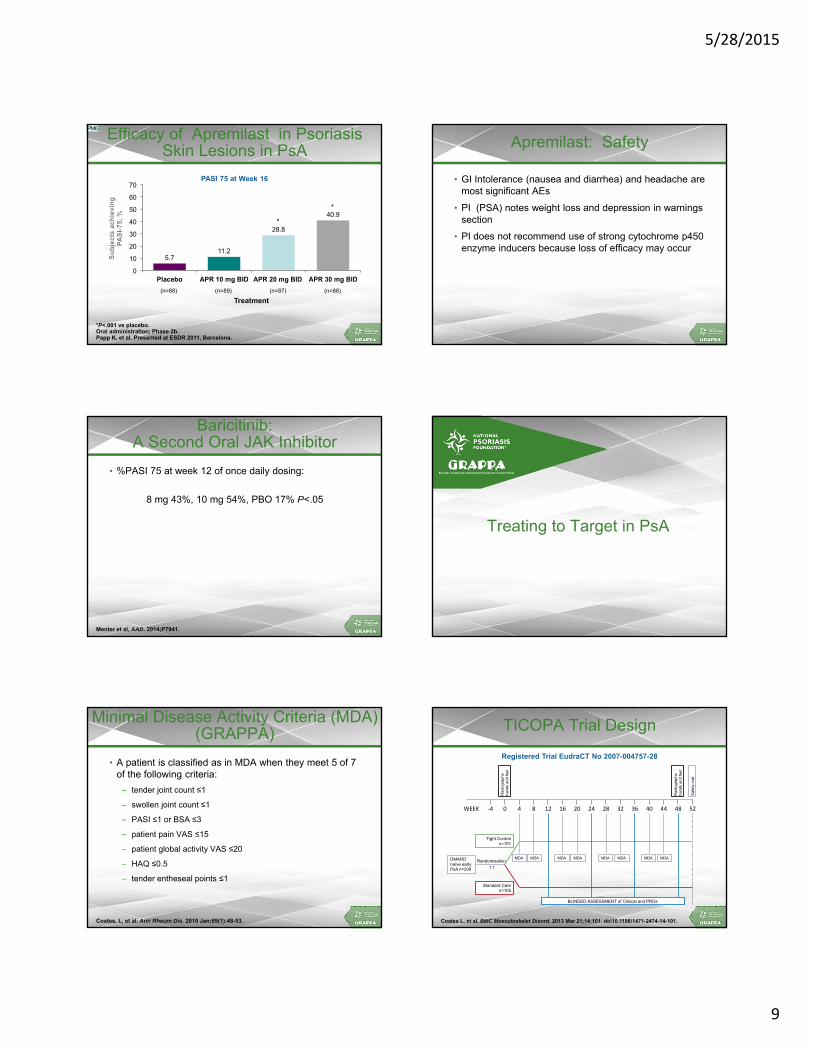
5/28/2015
9
Efficacy of Apremilast in Psoriasis Skin Lesions in PsA
5.7 11.2
28.8
40.9
0
10
20
30
40
50
60
70
Placebo APR 10 mg BID APR 20 mg BID APR 30 mg BID
Su
bje
cts
ach
ievi
ng
P
AS
I-75
, %
Treatment
PASI 75 at Week 16
(n=88) (n=89) (n=87) (n=88)
*
*
*P<.001 vs placebo.Oral administration; Phase 2b.Papp K, et al. Presented at ESDR 2011, Barcelona.
PM6
Apremilast: Safety
• GI Intolerance (nausea and diarrhea) and headache are most significant AEs
• PI (PSA) notes weight loss and depression in warnings section
• PI does not recommend use of strong cytochrome p450 enzyme inducers because loss of efficacy may occur
Baricitinib:A Second Oral JAK Inhibitor
• %PASI 75 at week 12 of once daily dosing:
8 mg 43%, 10 mg 54%, PBO 17% P<.05
Menter et al, AAD. 2014;P7941.
Treating to Target in PsA
Minimal Disease Activity Criteria (MDA) (GRAPPA)
• A patient is classified as in MDA when they meet 5 of 7 of the following criteria:
– tender joint count ≤1
– swollen joint count ≤1
– PASI ≤1 or BSA ≤3
– patient pain VAS ≤15
– patient global activity VAS ≤20
– HAQ ≤0.5
– tender entheseal points ≤1
Coates, L, et al. Ann Rheum Dis. 2010 Jan;69(1):48-53.
Registered Trial EudraCT No 2007-004757-28
TICOPA Trial Design
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
WEEK ‐4 0 4 8 12 16 20 24 28 32 36 40 44 48 52
DMARD naïve early PsA n=206
Tight Control n=101
Standard Care n=105
BLINDED ASSESSMENT of Clinical and PROs
MDA MDA MDA MDA MDA MDA MDA MDA
Rad
iog
raph
s h
and
s an
d fe
et
Sa
fety
vis
it
Randomisation
1:1
Rad
iog
raph
s h
and
s an
d fe
et

Slide 54
PM6 Check for publication of psoriasis studyadmin, 10/12/2014

5/28/2015
10
Continue
MDA
MTX and SSZEscalating to 1g bd at 4-8 wks, then to 40mg/kg/day max
Not MDA
MDA
1st line anti-TNF therapy for 12 weeks
Not MDA (≥3T/S Jts)
Not MDA(≥3T/S Jts)
MDA
Continue
MDA
2nd line anti-TNF therapy for 12 weeks.
Not MDA
TICOPA (n=206)
MTXStart at 15mg/wk escalating to 25mg/wk at 6 weeks
INTENSIVE MANAGEMENT GROUP STANDARD THERAPY GROUP
Standard therapy as per treating physician
Not MDA(<3T/S Jts)
ORMTX and CyAIncreasing by 1mg/kg/day every 4 weeks
MTX and LEFInitially 10mg/day increasing to 20mg/day at 4 weeks
OR
Not MDA(<3T/S Jts)
MTX and CyAIncreasing by 1mg/kg/day every 4 weeks
MTX and LEFInitially 10mg/day increasing to 20mg/day at 4 weeks
MDA
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
Primary Outcome – Complete Case Analysis
p=.02
p=.0004
p=.002
N=172 N=170 N=172
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
PASI Outcomes
N=156
Outcome Measure
ORLower95% CI
Upper95% CI
P value
PASI75 2.92 1.51 5.65 .0015
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
Prescribed Therapy at 48 Weeks
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
Serious Adverse Events
Tight Control Standard Care
Deaths 0 0
SAE 25 8
SAE related to drug 8 2
Blood/lymph systemCardiacGIHepatobiliaryImmune systemInfection/infestationInjury/poisoningMSK and CTDNeoplasmsNervous systemRenal/urinaryReproductive/breastRespiratory and thoracic
1152131401114
0020010212000
Coates L, et al. BMC Musculoskelet Disord. 2013 Mar 21;14:101. doi10.1186/1471-2474-14-101.
Conclusions
• Treatment recommendations
– Establishing diagnosis is critical
– Determine severity of clinical domains involved and assess impact on function and QoL
– Sensitivity to patient’s concerns about safety and therapy choices
• Management team
– Patient
– Physical, occupational therapy
– Dermatology
– Rheumatology
– Counseling
– Surgery
5/28/2015
11
Post-Activity Question 1
MTX has been shown to result in a significantly greater improvement in ACR20 response compared to placebo.
1. True
2. False
Post-Activity Question 2
How confident are you in describing the mechanism of action of PDE4 Inhibitors?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 3
How confident are you in describing the mechanism of action of JAK inhibitors?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Management ofPsoriasis and PsABiologics
Pre-Activity Question 1
How confident are you in using biologic therapy to achieve remission or low disease activity psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Pre-Activity Question 2
How confident are you in using biologic therapy to achieve remission or low disease activity in PsA?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident

5/28/2015
12
Pre-Activity Question 3
For patients who do not achieve adequate efficacy, I most often:
1. Switch in class
2. Switch to a different MOA
3. Give the current therapy more time
4. Add-on another therapy
Psoriatic Arthritis
PsA Treatment: GRAPPA Evidence Review
NSAIDs x xIntra-articular steroids xTopicals xPhysiotherapy xPsoralen UVA/UVB xDMARDS (MTX, CsA, SSZ, Lef) x xBiologics (anti-TNF antagonists) x x x x x
Axial Disease*
PeripheralArthritis
Skin and Nail Disease
Dactylitis Enthesitis
*Based on data from ankylosing spondylitis trials (used as surrogate for PsA spondylitis).Kavanaugh A, Ritchlin C (eds). J Rheum. 33;1417-1456.
Baseline Characteristics of Patients in Active Treatment Arms of anti-TNF Phase 2-3 Trials in PsA
ADAADEPTN=151
IFXIMPACTIII
N=100
ETNPhase IIIN=101
ETNPRESTAN=752
USTKNB (phase II)
N=146GLM
N=405
Age 49 47 45 47 49 47
PsA, yrs 9.6 8.0 9.2 7.0 5.5 7.5
Weight 86 86 86 82.9
SJC, N 14 14 16 12.5 8.5 13.2
TJC, N 25 25 20 19.2 17.8 22.8
HAQ, N 1.0 1.1 1.1 0.8
CRP (mg/dl) 1.4 2.1 2.2 0.55 1.3
Previous DMARDS 1.5 1.7
Enthesitis% 39 38 46 77
Dactylitis,% 41 43 37 46
Mease P. Ann Rheum Dis. 2011;70:77-84.
*12 weeks; **14 weeks; +16 weeks; X24 weeks.Mease, et al. Lancet. 2000;356:385-90; Antoni, et al, A8R. 2005; 52:1227; Mease, et al. A&R. 2004;50:2264-72; Antoni et al. ARD. 2005; 64:1150; Mease, et al A&R. 2004; 50:2264; Mease, et al, ARD. 2005; 52:3279; Kavanaugh, et al. Arthritis Rheum. 2007; Mease, et al. Ann Rheum Dis. 2014 Jan;73(1):48-55.
Anti-TNF Therapies in PsA:ACR and PASI Responses
Trial n ACR20 % ACR50 % ACR70 % PASI75 %
Rx P Rx P Rx P Rx P
Adalimumab 2/3x 315 58 14 36 4 20 1 59 1
Certolizumab 3+ 409 58 24 36 11 25 3 62 15
Etanercept 2* 60 74 14 48 5 13 0 26* 0*
Etanercept 3* 205 59 15 38 4 11 0 23 3
GolimumabX 405 52 8 32 3.5 18 0.9 61 1
Infliximab 2+ 100 69 8 49 9 29 0 68 0
Infliximab 3** 200 58 11 36 3 15 1 60 1
Anti-TNFs in PsA: Other Outcomes
• Enthesitis
– ~60-75% improvement
– Assessment methods: 4-point, MASES, Leeds, SPARCC
• Dactylitis
– ~60% improvement
– Assessment methods: Count, score, Leeds dactylometer
• Function
– Significant improvement achieved as assessed by HAQ
• QOL
– Significant improvements in SF-36, PsAQOL, DLQI, EQ-5D
• Fatigue - Significant improvement observed
Mease P. Ann Rheum Dis. 2011;70:77-84. Mease P. Arth Care & Research. 2011:63;64-85.

5/28/2015
13
Current RA Therapies – Use in PsA?
• IL-1 Inhibitors, e.g. Anakinra (Kineret) – not effective
• Co-stimulatory blockade: Alefacept (Amevive) (LFA3-CD2), Abatacept (CTLA4Ig) (B7-CD28)
• B cell ablators and modulators (minimally effective)
Mease P. Ann Rheum Dis. 2011;70:77-84. Curr Opin Rheumatol. 2013 May;25(3):287-96.
Abatacept in PsA ACR Responses at Day 169
0
20
40
60
80
30/10 10 3 Placebo
AC
R r
esponse
s (%
)
Abatacept (mg/kg)
ACR20 ACR50 ACR70
Error bars represent 95% CI; *P=.022; †P=.006; ‡P=.121 vs placebo.Mease P, et al. Arth Rheum. 63:939-48.
*
†
‡
Abatacept: Effect of Prior Anti-TNF Therapyon ACR20 Response at Day 169
0
20
40
60
80
30/10 10 3 Placebo
AC
R20
res
po
nse
(%
)
Abatacept (mg/kg)
No prior anti-TNF Prior anti-TNF
n=21 n=22 n=27 n=13 n=29 n=16 n=30 n=12
Error bars represent 95% CI.Mease P, et al. Arth Rheum. 63:939-48.
Abatacept: PASI 50 Response
Mease P, et al. Arth Rheum. 2011;63:939-48.
PASI 50 response: ≥50% improvement in PASI score in patients with ≥3% BL body surface area affected with psoriasis
Emerging Biologic Therapies for PsA
• IL12-23i
– Ustekinumab highly effective in psoriasis, modest in PsA
– Briakinumab – discontinued because of CV safety concerns
• IL-17i
– Importance of IL23R and TH17 cell in PsA
– Outstanding efficacy in psoriasis, data in PsA emerging
• IL-6 and IL-6Ri
– IL-6 richly expressed in psoriasis plaques and PsA synovium
– Background concern about potential for LFT/lipid increase
– May be used as monotherapy without background MTX
– Plus/minus effectiveness of tociliumab in PsA case reports
– Data from Phase 2 trial of clazakizumab in PsA pending
Mease P. Ann Rheum Dis. 2011;70 (Suppl 1) 77-84. Mease P. Curr Opin Rheumatol. 2013 May;25(3):287-96.
T Cell Differentiation Pathways

5/28/2015
14
Zaba LC, Cardinale I, Gilleaudeau P, et al. Amelioration of epidermal hyperplasia by TNF inhibition is associated with reduced Th17 responses. J Exp Med.
Effect of anti-TNF Therapy (Etanercept) on Cytokine Expression in Psoriasis Lesions
Ustekinumab (IL12/23) in Psoriatic Arthritis: ACR20/50/70 Responders at Week 24
*
PrimaryEndpoint
Dosing schedule: weeks 0, 4 and q12 weeks, thereafter.*P<.001.McInnes I, et al. Lancet. 2013 Aug 31;382(9894):780-9.
*
* *
* *
PSUMMIT I and PSUMMIT IIComparisons of Efficacy Results at Week 24 (Anti TNF Naïve)
22.8
8.7
2.4
11
42.4
24.9
12.2
57.2
49.5
27.9
14.2
62.4
0
20
40
60
80
ACR20 ACR50 ACR70 PASI75
Percent of Patients
PBO (n=206) UST 45 mg (n= 205)
UST 90 mg (n= 204)
PSUMMIT I PSUMMIT II
90
28.6
7.14.8
10
53.5
20.9
9.3
58.355.3
31.9
12.8
62.5
0
20
40
60
80
ACR20 ACR50 ACR70 PASI75
Percent of Patients
PBO (n=42) UST 45 mg (n=43)
UST 90 mg (n=49)
Ritchlin C, et al. Ann Rheum Dis. 2014 Jun;73(6):990-9.
PSUMMIT II Efficacy Results at Week 24 in Anti TNF Experienced Patients
14.5
6.51.6 2.0
36.7
15.0
5.0
45.5
34.5
15.5
5.2
48.8
0
20
40
60
80
100
ACR20 ACR50 ACR70 PASI75
Percent of Patients
PBO (n=62) UST 45 mg (n=60) UST 90 mg (n=58)
91
***
*
*P<.02Ritchlin C, et al. Ann Rheum Dis. 2014 Jun;73(6):990-9.
PSUMMIT II Safety Summary Through Week 24
92
PBO(n=104)
EEPBO 45 mg(n=31)
UST45 mg(n=83)
EE 45 mg
90 mg(n=20)
UST 45 mg Comb.(n=103)
UST90 mg
(n=104)
Avg. duration of f/u, wks 19.41 8.15 23.76 24.06 23.81 23.30
Avg. no. of injections 5.26 NR 2.55 NR NR 2.59
Total no. of injections 1637 NR 342 NR NR 321
Avg. exposure, no. of administrations
2.88 1.97 2.92 2.95 2.92 2.89
Patients with ≥1 AEs66
(63.5%)13
(41.9%)59
(71.1%)14
(70.0%)73
(70.9%)72
(69.2%)
Patients with ≥1 infection30
(28.8%)4
(12.9%)37
(44.6%)6
(30%)43
(41.7%)37
(35.6%)
Patients with ≥1 SAEs5
(4.8%)1 (3.2%) 0 0 0
2 (1.9%)
Patients with ≥1 serious infection
1(1.0%)
0 0 0 0 0
Total no. of pts with ISRs 5 (1.6%) NR 2 (1.5%) NR NR 4 (3.2%)
Injections with ISRs 6 (0.4%) NR 2 (0.6%) NR NR 5 (1.6%)
Patients with ≥1 malignancy 0 0 0 0 0 0
Patients with MACE events 0 0 0 0 0 0
*Values are n (%) unless otherwise stated.Ritchlin C, et al. Ann Rheum Dis. 2014 Jun;73(6):990-9.
Brodalumab in PsA: ACR 20 and 50 Responsesthrough 52 Weeks: Observed Analysis
SE = Standard Error.Mease P, et al. New England J Med. 2014;370:2295-306.
Brodalumab 280 mg Q2W (n = 56)PBO (n = 55) Brodalumab 140 mg Q2W (n = 57)
2716 33
Week52
Week12
Week24
4715 33
384 20
= indicates time point at which all subjects began receiving 280 mg Q2W brodalumab
ACR 50
Perc
enta
ge (9
5% C
I) of
Su
bjec
ts A
chie
ving
AC
R 5
0
Week
100
0
20
30
40
50
60
90
80
70
10
242 4 8 12 16 52
280 mg Q2W
PBO
140 mg Q2W
4550 55 53 51 50 45
4654 53 51 52 50 42
4956 56 53 53 51 45
Number of Subjects
ACR 20
Perc
enta
ge (9
5% C
I) of
Su
bjec
ts A
chie
ving
AC
R 2
0
Week
5019 44
Week52
Week12
Week24
7140 51
5644 64
100
0
20
30
40
50
60
90
80
70
10
242 4 8 12 16 52
280 mg Q2W
PBO
140 mg Q2W
4550 55 53 50 49 45
4654 52 51 52 49 42
4756 56 51 53 51 45
Number of Subjects

5/28/2015
15
Brodalumab in PsA: Mean Change in DAS28to 52 Weeks: Observed Analysis
Mease P, et al. New England J Med. 2014;370:2295-306.
Brodalumab 280 mg Q2W (n = 56)PBO (n = 55) Brodalumab 140 mg Q2W (n = 57)
= indicates time point at which all subjects began receiving 280 mg Q2W brodalumab
Mean (SE) Chan
ge in
DAS28
Response
0.0
-2.5
-1.5
-1.0
-0.5
Week
-1.70
-1.40
-2.13-2.0
Number of Subjects
522 12 16 244 8
140 mg Q2W
280 mg Q2W
PBO4151 49 4554 51
4551 49 4353 52
4051 48 4652 5155
50
51 -5
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
Brodalumab in PsA: Mean Change from Baseline inDactylitis and Enthesitis through Week 52:
Observed Analysis
Mease P, et al. New England J Med. 2014;370:2295-306.
EnthesitisDactylitis
Brodalumab 280 mg/brodalumab 280 mgBrodalumab 280 mg Q2W
PBO/brodalumab 280 mgPBO
Brodalumab 140 mg/brodalumab 280 mgBrodalumab 140 mg Q2W
Me
an
(S
E)
Sc
ore
Ch
an
ge
fr
om
Ba
se
lin
e
Week 52Week 12Week 52Week 12
3.13.1 3.02435 342844 39
Baseline score: 4.04.1 4.6n = 2128 292536 38
FUTURE 1: Study DesignRandomized, Multicenter, Double-blind, Placebo-controlled
Phase 3 Study
Randomization was stratified according to whether subjects were anti–TNF-naïve or had previous intolerance or inadequate response to anti-TNF therapy. BL, baseline; i.v., intravenous; q4wk, every 4 weeks; s.c., subcutaneous; SJC, swollen joint count; R, randomized; TNF, tumor necrosis factor; TJC, tender joint count; wk, week.
Loading
Secukinumab10 mg/kg i.v.
Secukinumab 10 mg/kg i.v.
Week BL 2 4
R1:1:1
Placebo i.v. Placebo s.c.
Secukinumab 150 mg s.c. Wk 16 then q4wk
Secukinumab 75 mg s.c. Wk 16 then q4wk
NON-RESPONDERS (<20% reduction in TJC and/or SJC)
R1:1
Placebo s.c.Secukinumab 150 mg s.c. Wk 24 then q4wk
Secukinumab 75 mg s.c. Wk 24 then q4wk
RESPONDERS (≥20% reduction in TJC and/or SJC)
R1:1
Escape treatment
Treatment
8 12 16 20 24
Secukinumab 75 mg s.c.Wk 8 then q4wk
Secukinumab 150 mg s.c.Wk 8 then q4wk
52
Primaryendpoint
q4w
Mease P ACR 2014
Secukinumab (IL-17Ai): FUTURE 1ACR20 Responses Through Week 52
*P < 0.0001 vs. placebo (P-values at Week 24 adjusted for multiplicity of testing).Missing values were imputed as nonresponse (nonresponder imputation) up to Week 24. Observed data from Week 28–52.
80
0
60
40
20
04 24 40 528 12 16 20 28 32 36 44 481 2
69.5%
*
*
* *
**
* *
** * * *
66.9%50.5%
50.0%
17.3%
Primary endpoint
**
*
Per
cent
age
of R
espo
nder
s
Weeks
N = 202 202 202 202 202 202 202 188 183 181 181 178 179 174N = 202 202 202 202 202 202 202 179 183 175 174 165 169 172N = 202 202 202 202 202 202 202 -- -- -- -- -- -- --
Secukinumab 10/mg/kg i.v. 75 mg s.c.Secukinumab 10/mg/kg i.v. 150 mg s.c. Placebo
Mease P ACR 2014
ACR50 Responses Through Week 52
*P < 0.0001, †P < 0.001; §P < 0.01; ‡P < 0.05 vs. placebo (P-values at Week 24 adjusted for multiplicity of testing)
Missing values were imputed as nonresponse (nonresponder imputation) up to Week 24. Observed data from Week 28–52.
60
0
50
40
20
04 24 40 528 12 16 20 28 32 36 44 481 2
30
10
**
**
**
*
*
30.7%
34.7%
7.4%
**
*
†
‡
§
50.0%
38.4%
Weeks
Per
cent
age
of R
espo
nder
s
Secukinumab 10/mg/kg i.v. 75 mg s.c.Secukinumab 10/mg/kg i.v. 150 mg s.c. Placebo
N = 202 202 202 202 202 202 202 188 183 181 181 178 179 174N = 202 202 202 202 202 202 202 179 183 175 174 165 169 172N = 202 202 202 202 202 202 202 -- -- -- -- -- -- --
Mease P ACR 2014
ACR70 Responses Through Week 52
*P < 0.0001, †P < 0.001; §P < 0.01; ‡P < 0.05 vs. placeboMissing values were imputed as nonresponse (nonresponder imputation) up to Week 24. Observed data from Week 28–52.
60
0
50
40
20
04 24 40 528 12 16 20 28 32 36 44 481 2
30
10
28.2%
25.6%*
*
*
16.8%
18.8%
2.0%
*
*
§
§†
‡§ §
†
Weeks
Per
cent
age
of R
espo
nder
s
N = 202 202 202 202 202 202 202 188 183 181 181 178 179 174N = 202 202 202 202 202 202 202 179 183 175 174 165 169 172N = 202 202 202 202 202 202 202 -- -- -- -- -- -- --
Secukinumab 10/mg/kg i.v. 75 mg s.c.Secukinumab 10/mg/kg i.v. 150 mg s.c. Placebo
Mease P ACR 2014

5/28/2015
16
39.0
22.0
10.2
38.3
16.711.7
16.9
5.10.0
54.5
39.9
22.4
55.6
36.6
19.017.5
8.42.8
ACR 20/50/70 Responses in Anti–TNF-Naïve and
Anti–TNF-IR Subjects at Week 24
*P < 0.0001, §P < 0.01; ‡P < 0.05 vs. placebo. Missing values were imputed as nonresponse (nonresponder imputation).
Statistical analysis of ACR70 response in the anti–TNF-IR subjects not performed due to lack of responders in the placebo arm.
Anti–TNF-Naïve Anti–TNF-IR
Secukinumab 10 mg/kg i.v 150 mg s.c. Secukinumab 10 mg/kg i.v. 75 mg s.c. Placebo
70
ACR20
Per
cent
age
of R
espo
nder
s 60
50
40
20
0
70
Per
cent
age
of R
espo
nder
s 60
50
40
20
0ACR50 ACR70 ACR20 ACR50 ACR70
30
10
30
10
* *
* *
**
143 142 143 143 142 143 143 142 143 59 60 59 59 60 59 59 60
§
‡
§
‡
Responses were sustained through Week 52 in both subgroups of subjects
Mease P. ACR 2014
48.1
56.7
15.5
46.0 48.8
12.8
Resolution of Dactylitis and Enthesitisat
Weeks 24 and 52
*P < 0.0001 vs. placebo.
Resolution of dactylitis and enthesitis amongst those subjects with these symptoms at baseline (dactylitis: n = 104 [150 mg], 104 [75 mg] and 116 [placebo]; enthesitis: n = 126 [150 mg], 129 [75 mg] and 117 [placebo]).Missing values were imputed as nonresponse (nonresponder imputation) at Week 24. Observed data presented at Week 52.
Secukinumab 10 mg/kg i.v 150 mg s.c. Secukinumab 10 mg/kg i.v. 75 mg s.c. Placebo
100
Per
cent
age
of S
ubje
cts 80
60
20
0
100
Per
cent
age
of S
ubje
cts 80
60
20
0Week 24 Week 24
40 40
Week 52 Week 52
82.6 79.487.7 89.7
**
* *
Resolution of Dactylitis Resolution of Enthesitis
Mease P. ACR 2014
PASI 75 Responses Through Week 52
*P < 0.0001, †P < 0.001, ‡P < 0.05 vs. placebo (P-values at Week 24 adjusted for multiplicity of testing).
Analysis performed in subjects with psoriasis ≥ 3% body surface area that were randomized. Missing values were imputed as nonresponse (nonresponder imputation) up to Week 24. Observed data from Week 32–52.
*
*
64.8%
61.1%
8.3%
*
Per
cent
age
of R
espo
nder
s
Weeks
100
0
60
40
20
04 24 40 528 12 16 20 28 32 36 44 481 2
80
*
*
**
†
‡
*
**
83.8%
71.7%
†
Secukinumab 10/mg/kg i.v. 75 mg s.c.Secukinumab 10/mg/kg i.v. 150 mg s.c. Placebo
N = 108 108 108 108 108 108 108 104 99 99
N = 108 108 108 108 108 108 108 101 100 99N = 109 109 109 109 109 109 109 -- -- --
Mease P ACR 2014
Mean Change From Baseline in HAQ-DI
Through Week 52
*P < 0.0001; †P < 0.001 vs. placeboP-values at Week 24 adjusted. for multiplicity of testing. Means are from mixed-effect model repeated measures shown up to Week 24. Observed data from Week 28–52.
1. Mease P. Arthritis Care Res
2011;63(Suppl 11):S64–85
MCID1 = –0.35
0
0
–0.2
–0.64 24 40 528 12 16 20 28 32 36 44 481 2
–0.4
Mea
n C
hang
e F
rom
Bas
elin
e
*
**
**
†
***
*
Weeks
†
*
**
* *
Secukinumab 10/mg/kg i.v. 75 mg s.c.Secukinumab 10/mg/kg i.v. 150 mg s.c. Placebo
N = 202 202 202 202 202 202 202 187 183 178 181 178 179 174N = 202 202 202 202 202 202 202 179 184 169 174 163 165 172N = 202 202 202 202 202 202 202 -- -- -- -- -- -- --
Mease P ACR 2014
0.13
0.02
0.08
0.57
0.5
0.6
Mean Change from Baseline in mTSSat Week 24
‡P < 0.05 vs. placeboP-values for pooled secukinumab group adjusted for multiplicity of testing.
Secukinumab 10/mg/kg i.v. 75 mg s.c. (n = 202)
Placebo (n = 202)
Secukinumab 10/mg/kg i.v. 150 mg s.c. (n = 202)
Secukinumab pooled doses (n = 404)
mTSS
0.4
0.3
0.2
0Mea
n C
hang
e F
rom
Bas
elin
e in
mT
SS
0.1
‡‡
‡
Mease P ACR 2014
Adverse Events of Special Interest Through Entire Safety Reporting Period
Candida infections
• Oral candidiasis in 8 (1.3%) subjects (4 with 75 mg; 4 with 150 mg); 1 (0.2%) case of esophageal candidiasis
• All cases of candidiasis were considered mild or moderate and responded to oral therapy; subjects continued in study
Neutropenia
• Grade 3 in 3 (0.5%) subjects (1 with 75 mg, 2 with 150 mg); no subject discontinued treatment. No Grade 4 cases were reported
Treatment-emergent anti-secukinumab antibodies
• Treatment-emergent anti-secukinumab antibodies detected in 1 (0.2%) subject; no loss of efficacyGrade 3 neutropenia: ˂ 1.0‒0.5 x 109 neutrophils/L; Grade 4: ˂ 0.5 x 109 neutrophils/L; MACE, major adverse cardiac event.
Variable
Any secukinumab150 mg s.c.
(n = 295)
Any secukinumab75 mg s.c.(n = 292)
Placebo (n = 202)
Exposure to treatment, mean days 439.4 437.6 128.5
AEs, exposure-adjusted incidence rate (number of cases per 100 patient-years)
Malignant or unspecified tumors 0.3 0.9 1.4
MACE 0.3 1.4 0.0
Mease P ACR 2014

5/28/2015
17
Secukinumab 150 mg s.c. Wk 8 and q4wk,
FUTURE 2: Study DesignRandomized, Multicenter, Double-blind, Placebo-controlled Phase 3 Study
MaintenanceLoading
1 2 8 12 16 20 Wk 523 4Week 0
Secukinumab 75 mg s.c.Wk 8 and q4wk
Secukinumab 75 mg s.c.Wks 0,1,2,3,4,
Secukinumab 150 mg s.c. Wks 0,1,2,3,4
Secukinumab 300 mg s.c.Wk 8 and q4wk
Secukinumab 300 mg s.c.Wks 0,1,2,3,4,
Placebo s.c.Wks 0,1,2,3,4,
24
Placebo s.c.Wks 8, 12
Placebo s.c. Wks 16, 20
Secukinumab 300 mg s.c. Wk 24 and q4wk
Secukinumab 150 mg s.c.Wk 24 and q4wk
RESPONDERS
Secukinumab 300 mg s.c.Wk 16 and q4wk
Secukinumab 150 mg s.c. Wk 16 and q4wk
NON-RESPONDERS (<20% reduction in TJC and/or SJC)
R1:1
R1:1
R1:1:1:1
Primaryendpoint
Randomization stratified by prior anti-TNF therapy (being anti‒TNF-naïve or anti‒TNF-IR). Only benefitting subjects continue after Week 52 q4wk, every 4 weeks; R, randomization; s.c., subcutaneous; SJC, swollen joint count; TJC, tender joint count; wk, week
McInnes I ACR 2014
Secukinumab FUTURE 2:Proportion of Patients Achieving ACR20 Responses
0
20
40
60
0 4 8 12 16 20 24
‡
***
*
†
†
Per
cen
tag
e o
f R
esp
on
der
s
Week
Secukinumab 75 mg (n = 99)Secukinumab 150 mg (n = 100) Placebo (n = 98)Secukinumab 300 mg (n = 100)
*P < 0.0001; †P < 0.001; §P < 0.01; ‡P < 0.05 vs. placebo (P-values at Week 24 adjusted for multiplicity). Missing values imputed as nonresponse (nonresponder imputation).
**
‡‡
‡ ‡
**
51.0%
54.0%
29.3%
15.3%
1 2 3
McInnes I. ACR 2014
58.2
38.8
22.4
63.5
44.4
27.0
36.9
24.6
6.2
15.9
6.31.6
0
10
20
30
40
50
60
70
80
‡
‡
‡
ACR20 ACR50 ACR70
Secukinumab 75 mg(n = 65)
Placebo(n = 63)
Secukinumab 150 mg(n = 63)
Secukinumab 300 mg(n = 67)
Per
cen
tag
e o
f R
esp
on
der
s
‡
‡
‡
‡
‡
ACR Responses at Week 24 in Anti‒TNF-naive Subjects
‡P < 0.05 vs. placebo
Missing values were imputed as nonresponse (nonresponder imputation).
McInnes P ACR 2014
45.5
27.3
15.2
29.7
18.9
10.8
14.7
5.9 5.9
14.3
8.6
00
10
20
30
40
50
60
‡P < 0.05 vs. placebo
Missing values were imputed as nonresponse (nonresponder imputation).
‡
‡
Secukinumab 75 mg(n = 34)
Placebo(n = 35)
Secukinumab 150 mg(n = 37)
Secukinumab 300 mg(n = 33)
Per
cen
tag
e o
f R
esp
on
der
s
ACR20 ACR50 ACR70
ACR Responses at Week 24 in Anti‒TNF-IR Subjects
McInnes I ACR 2014
Biologic Therapy: Safety Issues
• Infection
• TB/Opportunistic infections
• Neoplasm/lymphoma/skin cancer
• Autoimmune/lupus/MS/psoriasis
• CHF
• Administration reactions
• Vaccination issues
Special Issues
• Durability of biologic therapy effectiveness
– Immunogenecity
– Tolerability and safety
• Cost
• Patient acceptability
• Biosimilars

5/28/2015
18
Psoriasis
Choosing a Biologic Therapy for Psoriasis
Yes and failed NSAIDS
MTX, TNF BLOCKER, MTX+TNF BLOCKEREtanercept*,† Infliximab*†, Adalimumab*†,Golimumab*, Ustekinumab*,†
Certolizumab*
No
Contraindicationsto TNF blockade
No
Ustekinumab†
Etanercept*†, Infliximab*†, Adalimumab*†, Golimumab*, Ustekinumab†,* Certolizumab *
Yes
*FDA approved for the treatment of psoriatic arthritis. †FDA approved for the treatment of plaque psoriasis.
Does Patient have PsA?
Comparing Efficacy of Biologics in Psoriasis
% Patients Achieving Response
PASI 50 PASI 75 PASI 90
Supportive care 13.1 (9.6, 17.1) 4.3 (2.9, 6.2) 0.7 (0.4, 1.1)
Infliximab (5 mg/kg) 92.8 (90.1, 95.2) 80.8 (75.7, 85.8) 55.3 (48.2, 62.9)
Ustekinumab (45 mg) 88.8 (85.2, 91.9) 73.5 (67.5, 78.9) 45.5 (38.7, 52.4)
Ustekinumab (90 mg) 85.0 (80.2, 89.1) 67.2 (60.1, 73.8) 38.4 (31.3, 45.8)
Adalimumab (40 mg EOW) 84.8 (79.2, 88.7) 66.9 (58.7, 73.1) 38.1 (30.0, 45.0)
Etanercept (50 mg BiW) 74.4 (69.6, 79.3) 52.5 (46.9, 58.7) 24.9 (20.5, 30.1)
Etanercept (25mg BiW) 61.6 (55.4, 68.0) 38.3 (32.3, 45.0) 15.0 (11.4, 19.3)
Signorovitch et al. Br J Dermatol. 2014 Oct 7. [Epub ahead of print].
NOT in head to head trials, Meta analysis
Etanercept Efficacy: Psoriasis
Mea
n Im
pro
vem
ent
inP
AS
I S
core
(%
)P
atie
nts
wit
h P
GA
of
Cle
ar o
r A
lmo
st C
lear
(%
)
Leonardi CL, et al. N Engl J Med. 2003;349:2014-2022.
Adalimumab Efficacy in ThreePhase III Clinical Trials: PASI 75
British Journal of Dermatology, Vol 168 (2). pages 374-380, 13 Dec 201.2Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a phase III, multicentre, double-blind trial. The Lancet. Volume 366, Issue 9494, 2005, 1367-1374.
PASI 50 PASI 75 PASI 90
Per Protocol Intention to Treat
Dose: 5mg / kg IV
Infliximab Efficacy: Psoriasis
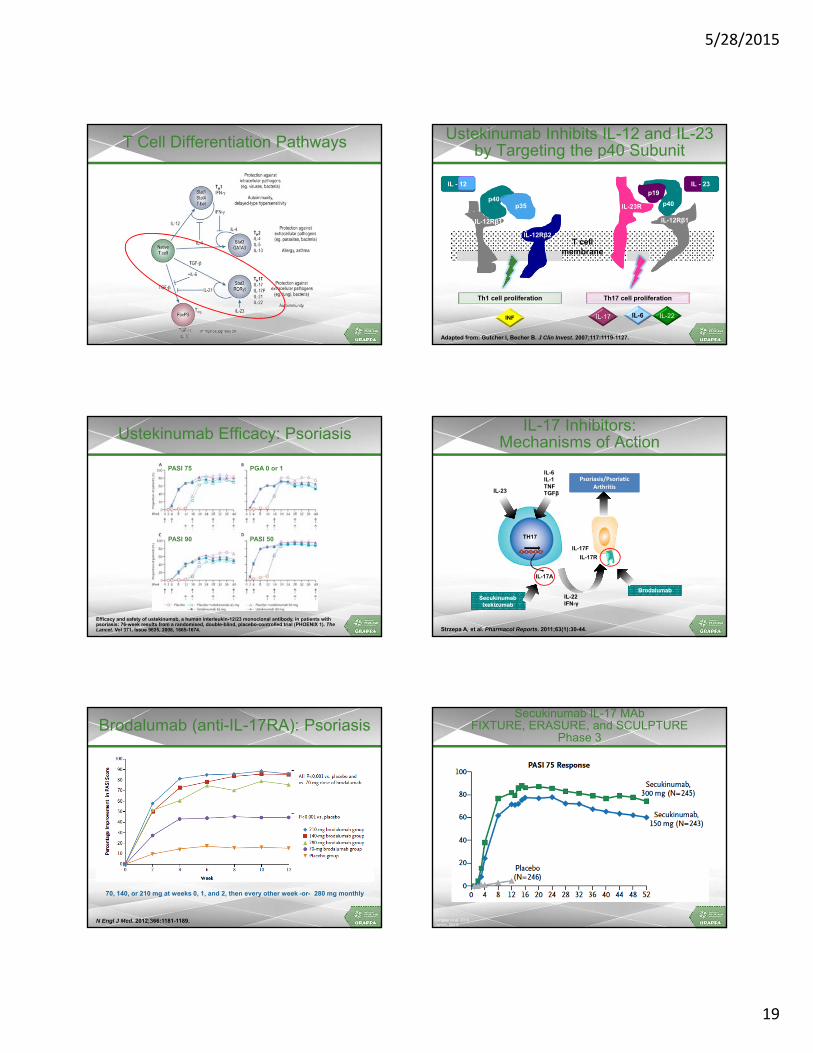
5/28/2015
19
T Cell Differentiation Pathways
T cellmembrane
IL - 23
IL-17INF
p40p35 p40
IL-12Rβ2
IL-12Rβ1
IL-23R
IL-6 IL-22
Th1 cell proliferation Th17 cell proliferation
p19
IL-12Rβ1
Ustekinumab Inhibits IL-12 and IL-23 by Targeting the p40 Subunit
Adapted from: Gutcher I, Becher B. J Clin Invest. 2007;117:1119-1127.
IL - 12
Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). The Lancet. Vol 371, Issue 9625, 2008, 1665-1674.
PASI 75
PASI 90 PASI 50
PGA 0 or 1
Ustekinumab Efficacy: Psoriasis IL-17 Inhibitors: Mechanisms of Action
Strzepa A, et al. Pharmacol Reports. 2011;63(1):30-44.
SecukinumabIxekizumab
SecukinumabIxekizumab
BrodalumabBrodalumab
Psoriasis/Psoriatic Arthritis
Psoriasis/Psoriatic Arthritis
IL-6IL-1TNFTGFβIL-23
TH17
IL-17A
IL-17R
IL-22IFN-γ
IL-17F
Brodalumab (anti-IL-17RA): Psoriasis
N Engl J Med. 2012;366:1181-1189.
70, 140, or 210 mg at weeks 0, 1, and 2, then every other week -or- 280 mg monthly
Secukinumab IL-17 MAbFIXTURE, ERASURE, and SCULPTURE
Phase 3
Langley et al, 2014.Jancin, 2013.

5/28/2015
20
Ixekizumab (anti-IL17A): Psoriasis
N Engl J Med. 2012 Mar 29;366(13):1190-9.
Dosed weeks 0, 2, 4, 8, and 12. Primary endpoint PASI 75 at week 12
Cytokine Targets in Psoriasis Therapy
Dis Model Mech. 2012 Jul;5(4):423-33.
p19 antibodies
Conclusions
• Biologic therapy has revolutionized the treatment of psoriasis and PsA
• Achievement of remission or low disease activity is now achievable
• For patients who don’t achieve adequate efficacy, lose efficacy, or cannot tolerate med, switching in class or different MOA can occur
• Safety is an issue and close monitoring is necessary
Post-Activity Question 1
How confident are you in using biologic therapy to achieve remission or low disease activity psoriasis?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 2
How confident are you in using biologic therapy to achieve remission or low disease activity in PsA?
1. Very confident
2. Confident
3. Somewhat confident
4. Not confident
Post-Activity Question 3
For patients who do not achieve adequate efficacy, I plan to:
1. Switch in class
2. Switch to a different MOA
3. Give the current therapy more time
4. Add-on another therapy

5/28/2015
21
Questions & Answers