association of camp nurses
TRANSCRIPT

. . .w
ork
ing
for
hea
lth
ier
cam
p c
om
mu
nit
ies
by
sup
port
ing
th
e p
ract
ice
of
cam
p n
urs
ing.
In This Issue…
Association of Camp Nurseswww.campnurse.org
September 2012 volume 22, number 3
– My View – Immunizations: Challenge and Opportunity
I am frequently asked about immunizations. Parents want to know if camps “really need those dates.” Camp nurses want to know what to do when a camper’s health form simply states “up-to-date” across the immunization grid. Camp directors want to know what to do about international campers and staff. Everyone asks what immunizations “really make a difference at camp,” and various regulating bodies are interested in knowing just what they should be requiring. I recently engaged ACN’s Board in a brief email conversation about this topic. The Association will eventually develop a statement that lays out ACN’s recommendation but, before getting too far down that path, I want to open this conversation with ACN members. This means that I may be a bit provocative in my writing, but I’m doing so in the interests of getting at the nuggets surrounding this topic. I want to lay out some thoughts and ideas about which I’d like your feedback. ACN has a history of discussing controversial topics and considering various perspectives in order to arrive at common ground. Let’s see where this discussion takes us. Many voices seem to agree that having the date/year for each person’s tetanus immunization makes sense. Given the exposure to cuts, scratches and camp life enjoyed by campers and staff, this immunization is protective in a camp setting. Do you agree? In addition, some States direct that camps licensed by that State collect immunization information. If a State so directs, then the camp had best comply. ACA Standards, specifically HW.5D, direct that the camper health history includes “a statement from the custodial parent/guardian attesting that all immunizations required for school are up to date and including the actual date (month/year) of last tetanus shot” (American Camp Association, 2012, pg. 77). The “date (month/year) of last tetanus shot” (American Camp Association, 2012, pg 94) is all that the Standards direct be on staff health history forms. Given this, some camps may decide to pare down the information collected about immunizations, especially if State regulations associated with the camp license are silent about immunizations. Even with this, however, camps will have to make a determination about what school district is referenced – the one in which the camp is located or the one from which the individual comes. Interesting. When it comes to immunizations, I believe that a camp’s administrative team has to consider more than what is directed by regulation and/or Standards. The risk profile of both camper and staff populations makes a difference; the potential for exposure to communicable diseases related to the robustness of the camp’s control strategies makes a difference; and the camp’s capacity to cope with an outbreak makes a difference. In addition, the re-emergence of illnesses like pertussis (whooping cough) – related to waning protection of the childhood immunization process – and chicken pox (in spite of being immunized) seems to warrant consideration by camp leaders. While most of us recognize the need for knowing each person’s tetanus status, perhaps – assuming that pertussis will continue to be a threat – there’s need to know the status of that immunization next summer and/ or recommend that parents update their child’s pertussis immunization given the exposure potential at camp. That being said, I do not mean to imply that a camp experience is threatening to health. Rather, such a comment recognizes that camp, like school, puts people in close contact with others.
Linda Erceg, RN, MS, PHN
My View: Immunizations: Challenge and Opportunity ........... 1Partnering with Camp M.I.T.I.O.G: A Win-Win Experience for Both Students and Campers ............................................ 3
Super Sleuth .......................................................................... 6
Understanding Menorrhagia: Camp Nurses can Help ........... 7
Wounds at Camp: Could it be MRSA? .................................11Why Campers and Staff Seek Care from Health Center Staff ......................................................................... 13
It Happened This Summer: 2012 Camp Nurses Share Their Experiences................................................................ 16
Perspectives Worth Sharing: Children with Sensory Impairment: Camps for “Athletes” of Experiential Learning ..................... 19
New Products, New Ideas ................................................... 21
ACN’s 2013 Camp Nurse Symposium ................................ 22
Association News ................................................................ 23

2
Volume 22, No. 3
2
CompassPoint is an official publication of the Association of Camp Nurses (ACN), a not-for-profit nursing organization. CompassPoint is published four times a year and is intended as an informational resource only. Neither ACN nor its staff can be held liable for the practical application of any ideas found herein. Readers are invited to submit items for publication to Susan Baird, Editor, via email at [email protected]. Contents may not be reproduced without prior written consent. Member dues and subscription fees are $50 annually. CompassPoint is indexed in CINAHL.
ACN Board
President & Board Chair .............Vernon-John “VJ” Gibbins, RN, BScN, MS [email protected] 617-697-2616 Founder’s Chair .................................................Jeanne Otto, RN, MS, MEd 617-661-0917 Education Chair ................................Tracey Gaslin, RN, PhD, CRNI, CPNP [email protected] 502-744-6803 Research Chair, Executive Committee ...................Ellen Buckner, RN, DNS [email protected] 205-934-6799 Executive Committee ...........................................................Jill Ashcraft, RN [email protected] 503-784-9497 Member-Linkage Co-Chair .............................Cheryl Bernknopf, RN, BScN [email protected] 905-771-6577
Member at Large ........................................................ Lisa South, RN, DSN [email protected] 662-552-5352 Finance Chair .................................................................William (Bill) Jones [email protected] 952-922-2545
Member-Linkage Co-Chair ..........................................Edward (Ed) Schirick [email protected] 845-794-3113 Executive Director ............................................Linda Ebner Erceg, RN, MS [email protected] 218-586-2633
ACN Member Leaders
CompassPoint Editor..........................................Susan Baird, RN, MPH, MA [email protected] 508-888-3249 American Camp Association (ACA) Liaison ..........Linda Ebner Erceg, RN, MS [email protected] 218-586-2633 CompassPoint Editorial Board .................................. Kathleen Bochsler, RN
Barbara Hill, RN, MSN, CNE, CMSRN Mary Marugg, RN Jane McEldowney, BS, RN, NCSN Doris Nerderman, RN, BSN Ellen Reynolds, RN, MSN, CPNP
Education Committee…..….… Lisa Cranwell-Bruce, RN, MS, FNP-C, APRN Bonnie Huston, RN, BSN, CEN Carol Jelfo, RN, MS Michelle McKinney, RN, BSN Professionalization Committee...................................Myra Pravda, RN, MSN Linda E. Erceg, RN, MS
Research Committee.........................................Cheryl Bernknopf, RN, BScN Nancy Krahl, RN, MSN, MA Ellen Reynolds, RN, MSN, CPNP Lisa South, RN, PhD
Association of Camp Nurses (ACN)
8630 Thorsonveien NE – Bemidji, MN 56601Phone: 218-586-2633 Fax: 218-586-8770
www.campnurse.org Email: [email protected]
Immunizations continued from page 1As with all close encounters of the human kind, the potential for an ill person to pass their illness along to the next person certainly exists. Those of us who have coped with an outbreak at camp – think of pertussis or chicken pox – know the effort needed to work through that experience. It impacts the Health Center, food service, activities, laundry, sanitation and camp personnel. But such an outbreak can also impact camp parents and/or the community in which the camp is located. The necessary people need to be informed. I think we’ve now progressed enough to state that there’s an expectation that the camp will inform parents about outbreaks in a timely manner. The reasons for doing so are varied but two reasons should not be minimized: (a) there may be an immune-comprised person at camp who is unknown to the camp and (b) campers/staff who go home may inadvertently expose susceptible individuals (e.g., aging grandparents, very young children, health compromised sibling). Getting this information to the right people – especially when there’s an immunization that can be given to limit the illness’s spread – is critical. Since some people are not immunized – again, for various reasons – a camp cannot depend on “herd immunity” as a protective factor. That being said, I’ve noticed a slight unfreezing among the “I do not immunize my child” population. When I engage these parents and explain my concern about tetanus, pertussis and flu, some parents are changing their minds and get these immunizations for their camper. Granted, it hasn’t been a lot of people but enough have responded that it makes me wonder. Perhaps camps need to do a better job of describing why we want immunized campers. And camp administrators should be clear about what they expect of parents should their child come down with a communicable illness while at camp.
Interesting how this discussion about immunizations bleeds easily into communicable disease control at camp. Our campers and staff decide on a camp experience for reasons that generally do not include getting ill. Perhaps we, as camp professionals, need to be more explicit about our stance regarding immunizations and partner that stance with education so people understand why we’re concerned. In so doing, I can understand how an immunization decision for a day camp might vary from that made by a resident camp or a camp serving a special population. The risk potential varies. We need to keep each camp’s risk profile in mind as we discuss the immunization policy for a given camp. Finally, when making this policy decision, also consider how the immunization policy gets enforced. Opening day is not the time for a camp nurse to make a big deal about someone’s immunization status. That has to get front-loaded and, probably, handled by the camp administrator with responsibility for policy enforcement. So back to my initial question: what do you think about immunizations? What criteria should be considered as camps revised various health forms for 2013? I’d like to know, so shoot me an email ([email protected]).
References American Camp Association (2012). Accreditation process guide.
Monterey, CA: American Camp Association.
Linda Erceg, RN, MSN, PHN is Assistant Director for Health and Risk Management at Concordia Language Villages of Bemidji, MN, and the Executive Director of the Association of Camp Nurses.
September 2012
3
Volume 19, No. 2
Partnering with Camp M.I.T.I.O.G: A Win-Win Experience for Both Students and Campers
Nancy Krahl, RN, MSN, MA
With Katie Cook, Lindsey Davis, and Jenny Stromsted
Abstract: A camp nursing elective course offered to St. Luke’s College of Health Sciences’ students includes an on-site component at Camp M.I.T.I.O.G. at Lake Doniphan Conference and Retreat Center. The campers have spina bifida and students prepare for their on-site experience by learning camp nursing fundamentals, meeting with camp leaders, touring the site, and developing health promotion presentations for campers. During their stay at camp students perform a variety of camp nurse tasks including health screening, medication administration, and carrying out treatments specific to spina bifida management. Students experience camp life along with the campers yielding further insights into the patient population.
“When I first came to camp I didn’t really know what to expect. I waited all summer in anticipation and worked through logistical concepts in class, but I really didn’t know what life would be like at Lake Doniphan Conference and Retreat Center in late July. In class it was emphasized that the M.I.T.I.O.G experience was more exciting than Christmas for many of the campers that attend. I didn’t really process this fact until I was sitting with a camper during an enema. The camper said to me, ‘Sometimes I really wish that I could be normal...but have spina bifida once a year so that I could still come to camp. It’s the best week of my life!’ Hearing this statement really left an impact. In that moment I realized that this week was more than just about fulfilling a college credit, it was about helping to make these camper experiences the best that they could possibly be.” stated Katie Cook, a senior nursing student at Saint Luke’s College of Health Sciences in Kansas City, Missouri. Many students have expressed similar thoughts since this two credit hour elective course was first offered in 1992. One of the most gratifying experiences I have had as a nurse educator began in 1991 when our diploma nursing school closed and we began developing courses for our College curriculum. When it was decided we needed more elective offerings for the students, I reflected on what I might be able to contribute. Because of my previous experiences as a camp nurse, I thought immediately – why not have an elective in Camp Nursing? I knew exactly which camp would be the best for meeting student learning outcomes, where they would be warmly received and get the most “hands on” experience possible. Camp M.I.T.I.O.G. (Made in the Image of God), is an ACA accredited special medical needs residential camp designed for children ages 7 through 16 who have spina bifida. Camp M.I.T.I.O.G is held each summer at Lake Doniphan Conference and Retreat Center, Excelsior Springs, Missouri. I had been a volunteer camp nurse there in the past and was well acquainted with the camp’s program and health objectives and had developed a collegial relationship with the camp director and the nursing staff. I felt that it would be a good “fit” for our students. Once the curriculum committee approved this elective, the College gained approval for the clinical site by the Missouri State Board of Nursing and completed a contract between the
College and Camp M.I.T.I.O.G. Little did I realize what I was getting myself in to when I made my proposal to the Curriculum Committee that April day in 1991! However, 21 years later, I don’t regret for one second that I took that leap of faith and pioneered one of the few camp nursing courses in the United States.
The Student Experience Prior to Camp Our students, under direct faculty supervision, have been doing their camp practicum portion of the camp nursing elective at this “labor intensive” camp every summer since 1992. This ongoing partnership between Camp M.I.T.I.O.G. and Saint Luke’s College of Health Sciences allows our students to benefit from this unique experience. Many of the students who have taken this elective would agree with me that it is a labor of love. Prior to participation in the camp clinical experience, students complete a one credit hour prerequisite didactic portion, “N 331 Caring for Clients at Camp.” During these two weeks of class they:
• Learn the “basics of camp nursing” content through lectures, class discussion, viewing DVD’s, reviewing journal articles, and discussing the assigned readings from their textbook by Erceg, L. and Pravda, M. (2009) The Basics of Camp Nursing. American Camping Association. Martinsville, IN.
• Take a walking tour of Doniphan Conference and Retreat Center camp grounds and facilities and conclude with interviewing the camp nurse at the Health Center.
Kelly Delong and Lindsey Davis stressing
importance of fiber in diet.

4
Volume 22, No. 3
4
• Dialogue with guest speakers, Carol Hafeman, RN, MA, ET and Edie Roderick, RN, CPNP from Children’s Mercy Hospital, Kansas City, Missouri. Carol has been Camp M.I.T.I.O.G.’s Camp Health Coordinator for the past 25 years. Edie has been serving as our Advanced Practice RN for the past eight years. They are both experts in caring for children with spina bifida and provide the students with an excellent overview of the needs of this vulnerable camp population.
• Present their health promotion teaching project to faculty and classmates
• Take a final exam and conclude with an exam review.
The Student Experience at Camp While at camp the students are involved in a variety of nursing and camp activities. Since it is a residential camp, the students and I stay overnight and we do not leave the camp grounds. We arrive on Friday evening, prior to the campers’ registration on Saturday, to set up the Health Center, do the initial screening on counselors and staff, clean and stock equipment and place bath chairs and supplies in all of the camper bathrooms. As campers and parents arrive on
Last night, I returned from Camp M.I.T.I.O.G., back to cell phone service, spacious showers, and the ability to sleep in until the sun is actually well up in the sky. Despite this return to my fairly comfortable everyday existence, I believe there is a bit of me that remained at camp with the special children, counselors and nurses with whom I spent the past few days. When I signed up for the camp nursing class at Saint Luke’s, I was expecting an experience where I would administer medications at meals and then sit in a nursing station and put band-aids on cuts and ice on turned ankles. I feared it would be unbearably hot and that I would come away from Lake Doniphan with skin that was sunburned and riddled with bug bites, despite my best efforts with sunscreen and bug spray. However, what I actually lived for three plus days was much, much different in a completely positive way. M.I.T.I.O.G. gave me my first opportunity with pediatric nursing. While I did treat cuts and bruises and turned ankles, I also learned a lot about how very different children are from adults. Every day I spent at camp was filled with small inspirations and moments of joy. I danced with, taught, sang with, swam with, and laughed with those amazing children. The resilience of these children was touching and really surprised me. I was shocked to see just how highly functioning some of the children were despite the seriousness of their conditions. I am still having a hard time wrapping my mind around how open the kids were, both with their conversation and their bodies. There was no embarrassment during treatment – catheters, enemas, whatever the moment called for. One of my fondest memories of camp was observing the interactions between a young camper and his counselor. Their relationship was truly touching – it was obvious
that the camper looked up to his counselor with love and hero-like worship. The way the counselor interacted with the camper was at the same time like a best friend, teacher, father and care-giver. I was truly astounded – not just with this pair, but with many others – how attached two people could become to one another in just a few short days. I think I understand why counselors and staff return to camp year after year, despite the grueling work and vast responsibilities with which they are presented. The only things that I did not like at camp were seemingly superficial. It was hot and miserable at times, and the showers were small, the beds uncomfortable, and the time allowed for sleep too short. But it was easy to overcome these negatives with the overwhelming positives that presented. I am so pleased that Saint Luke’s offers this program. I was able to both refine and better my skills as a nurse and grow as a human being. Being immersed in the camp life was difficult and exhausting at times, but I ended up with an experience that I will never forget. There should be more programs like this one offered to student nurses as they allow you to experience nursing away from the hospital – a huge culture shock in itself – but also to work closely with varying personalities, practice and improve valuable nursing skills, and to realize there is so much more to nursing than just treating an ailment. Camp M.I.T.I.O.G and this class wildly surpassed my expectations. Being able to not just treat the kids when they were hurt or needed assistance but also being able to interact, teach skills and have fun together on a daily basis brought me a lot of joy. I am so happy I was able to learn so much while having such a great time.
Saturday afternoon, the students assist with the camper health screening check-in and begin the laborious task of organizing the campers’ medication (MARS) and treatment plans. During camp, with faculty and nursing staff supervision, the students provide first aid for the camp community, set up medications for 56 campers for 24 hour periods of time, administer medications at breakfast, lunch, dinner and at bedtime following the evening campfire. Each student is assigned with an RN to assist with treatments throughout the day and evening. Additionally, the students teach a health promotion class each morning following the flag raising and the “Good Morning M.I.T.I.O.G” session. While their counselors are dismissed to attend a daily counselor meeting and have a bit of “respite” from their campers, the students divide the campers into three different age groups: 7-10 years, 11-14 years, and 15-16 years of age for a 30 minute teaching session. Two students per group engage the campers at the appropriate developmental level in creative learning activities on such health related topics as: Latex Allergies, High Fiber Diet, Protecting and Caring for Your Skin, and Prevention of Infections. However, the students use more
Camp M.I.T.I.O.G. ReflectionJenny Stromsted

September 2012
5
I have always had a special place in my heart for the children at camp M.I.T.I.O.G., having been a counselor there for three years. However, going as a student nurse this year has absolutely given me a new idea of what camp M.I.T.I.O.G. stands for. As a counselor, I was one-on-one with a single camper all week long. The only way I was able to have interaction with other campers was if my camper wanted to talk to or associate with them. However, as a nurse, it was wonderful to be able to get to know all the different campers and to assist any camper that needed our help during the week. I loved getting to know the campers’ names, their specific needs and the day-to-day tasks they were able to perform. However, there were quite a few things that surprised me about the campers at M.I.T.I.O.G. I found I still have so many things to learn about spina bifida and the children affected. I never knew how many medications the campers could be on for their condition. In the past, I had very healthy and independent older campers who did not require a large amount of medication. However, spending hours and hours filling medications for the campers made me realize how individual the effects of this condition are in this population. I also never realized the varying abilities of the campers with spina bifida, both physically and intellectually. I now know that location of the lesion in the spinal cord affects the degree of physical limitation. I noticed quite a range of mental abilities as well but was not able to figure out why. Another element of camp that was surprising was how many people came to the health center, both campers and counselors. Their requests ranged from trash bags to candy to catheters and from pain medication to athlete’s foot treatment. There were so many aspects about camp that I enjoyed as a student nurse. I absolutely loved getting to know all of
the campers -- their names and their individual personalities and to truly be able to enjoy their company. Another aspect I liked was the teamwork among all of the nurses. It was obvious that all of the nurses wanted to help one another. Their tag team approach worked very well and it was nice to enjoy their company throughout the day as well. I also enjoyed being able to participate in all the camp activities. The nursing students were stationed at different activities happening on camp grounds and it was relaxing to be able to enjoy all of the various classes such as recreation, fishing and swimming. I acquired various skills I know that I will need throughout my nursing career. I learned several procedures such as how to master straight catheterization, catheterization through a Mitroffanoff, and enemas rectally and via a M.A.C.E. I learned a lot about oral medication administration of agents commonly used in this population and how to communicate effectively with pediatric patients. These were all tasks I had never done before and I am so happy I had this opportunity. Above all things, Camp M.I.T.I.O.G. inspired me this week. I never realized how truly happy the campers are. They try so hard and give everything they have to enjoy the life they have, making the best of what they have and going with it. They don’t let their physical limitations hold them back. They are also very much aware of how to take care of themselves. They taught me more about catheters, enemas, M.A.C.E.’s and medications than I ever knew a child could comprehend. However, it is a part of their day-to-day life and I think that is what inspired me most. They go through so many challenges on a daily basis just to complete their activities of daily living, and yet they are still so happy. Most of all, I think I was inspired to come back to camp M.I.T.I.O.G. again, as a nurse. After being a student nurse there, my love for the camp has only deepened.
“catchy” titles such as: Duck, Duck, Poop; Happy Pee; and Spina Bifida Bingo! Prior to implementing the classes, students write at least three learner objectives and prepare a content outline that includes a list of the materials needed and the references they used. We debrief immediately following the classes to determine what went well and what could be improved. The campers have responded enthusiastically to these classes year after year.
Camper Issues the Students Address Many of the campers arrive at camp with varying degrees of pressure ulcers. Our goal is not only to prevent pressure sores at camp but to send those campers who arrive at camp with sores home more healed than when they came. Therefore, all students get hands on experience assisting with wound care. Nearly all campers are on a bowel management program. Therefore, all students have the opportunity to assist the campers with their daily bowel management program by administering daily enemas rectally or through a M.A.C.E. (Malone Antegrade Continence Enema). Almost all campers are on a routine catheterization program as well. The students perform straight catheterizations on campers who aren’t able to “self cath” and assist campers catheterized via a Mitrofanoff (a urinary catheterizable stoma). Several students usually have the opportunity to do “cabin inspections” and report the results at the morning Flag Raising ceremony. In addition, students are rotated with the campers
Camp M.I.T.I.O.G. Reflection PaperLindsey Davis
Campers enjoy the creative learning
sessions that help them assume more responsibility in their
daily routines.

6
Volume 22, No. 3
throughout the day at the various camp activities such as the swimming pool, recreation center, crafts, and fishing to ensure that campers are reapplying sunscreen, hydrating, and not becoming heat exhausted. As much as time permits, the students dance with the campers at the “big” Monday night dance, cheer during the camper talent show on Wednesday evening and sing along with campers and counselors at the evening campfires.
Benefits of the Student Experience Students are able to participate in the concluding camp activities, closing ceremony, and campers’ departure. This provides an opportunity to meet parents and share significant information with them about their child’s health and/or camp experiences. The students assist the nurses in doing inventory and in “breaking down” the Health Center and storage of the Health Center’s supplies and equipment for next year’s camp. Students have excellent nurse role-models at camp. They are able to take advantage of the many opportunities to administer medications, perform procedures, teach individuals and groups and to observe the various roles the professional nurse implements within a healthy camp community of campers with spina bifida. They are able to see firsthand the enormous preparation and attention to detail it takes by everyone to have a safe, successful camp experience. An additional benefit of having students at camp is the fact that
many of our graduates return as RN’s to help manage the health care while some help with other special needs camps which is great too! It is a fantastic experience for our students and many have remarked that it has been a “life changing” event for them.
My Experience I love teaching and I love teaching this course in particular. While preparing this article I happened to read some excerpts from students’ journals written many years ago and I realized that students are still saying the same things today about their experiences at Camp M.I.T.I.O.G. as they did back then. Perhaps Katie Cook, who took the camp elective this summer, said it best: “Camp M.I.T.I.O.G. is probably one of the best things I’ve done with my life so far. I’ve never met any other group of patients that have so greatly altered the way I look at my practice and life in general.”
Nancy Krahl, RN, MSN, MA is an Associate Professor at Saint Luke’s College of Health Sciences, Kansas City, Missouri. She has been involved in camp nursing for 40 plus years and is also a member of ACN’s Research Committee. Katie Cook, Lindsey Davis and Jenny Stromsted are senior nursing students at Saint Luke’s College of Health Sciences who participated in the Camp Nursing Elective this summer.
Super Sleuth Janice Springer, RN, PHN, MA
On Monday, John, the counselor comes into the camp health center saying the itching on his back is getting to be too much. You see this picture.
A
Later that week, Andrew comes in complaining that he was up all night itching on his back, would you take a look, and you see this picture.
B
What is going on??? Are they the same? Are they different? If so, how different? The answer is on page 11.
Super Sleuth Janice Springer, RN, PHN, MA
The answer is on page 10.
It has been over 90°F for a week. The last night of camp is a big soccer game between campers and staff. About midnight, one of the counselors wakes you up to come over to the cabin where 10-year-old Ardie is moaning in his bunk. When you arrive, you see Ardie lying on his left side, holding onto his calf, groaning and saying, “I can’t move my leg!” What does he have? Why? What can you do about it?
Ouch!After the dance on Saturday night, Alan hobbles into the Health Center and says he cannot get his toe to go back down and that it hurts. The great toe is pointed to the sky and he cannot get it to stay down. What does he have? Is it the same concern as Ardie?
September 2012
7
Understanding Menorrhagia: Camp Nurses can Help
Diana Mathis, RN, BS
Abstract: Menorrhagia is a major public health problem in women and can pose management difficulties in the camp setting for both campers and staff members. Understanding the causes, diagnosis, and treatment approaches will aid the camp nurse in helping those affected adjust and enjoy camp life despite the challenges posed. The nurse can provide assistance in managing supplies, hygiene, activities, dress and diet.
Statistically, 20% of your female counselors and campers will be menstruating at any given time. Many will spend much of their summer somewhat preoccupied by menstrual bleeding, worrying about changing pads, fearful of embarrassing overflow and not able to fully enjoy camp activities. Heavy menstrual bleeding can make it difficult to work, play or to even get out of bed. Menorrhagia is a major public health problem in women. According to a report by the World Health Organization, at least 5–10% of women of reproductive age will seek medical attention for menorrhagia in their lifetime (Shaw & Shaw, 2011).
What is normal? In 2006, the American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics issued a committee consensus report which stated that normal menstruation begins at 11–14 years of age, the normal cycle interval is 21–45 days, and the normal length of menstrual flow is 7 days resulting in an estimated blood loss between 25-80 ml. (ACOG, 2001).
What is menorrhagia? “Heavy period” is still a very subjective term. Periods vary greatly from one woman to another in duration of bleeding, span of time between periods and in the amount of blood lost. Based on guidelines determined by ACOG, menorrhagia is defined as menstrual bleeding lasting for more than seven days or menstrual bleeding resulting in the loss of more than 80 ml. per cycle (ACOG, 2000). Menorrhagia is a common clinical problem, reported by 10-15% of women of reproductive age (Vessey et al., 1992). Menorrhagia, heavy menstrual bleeding which occurs on a regular cycle, is different than metrorrhagia which is bleeding occurring on an irregular cycle. Both present multiple problems for women although menorrhagia is more common and is actually the most common type of abnormal uterine bleeding. Bleeding problems in women are often unrecognized or misdiagnosed. Many women are not aware that their symptoms are abnormal and do not seek medical care. Unfortunately, there are many women who do recognize their bleeding as abnormal and seek medical care but often do not receive appropriate treatment due to lack of awareness in the medical community.
Causes of Menorrhagia It is often difficult to determine the cause of menorrhagia. In approximately 50% of cases, the etiology of heavy menstrual bleeding remains unknown even after investigation (Warner et al., 2001). It is generally recognized, however, that there are numerous causes of heavy menstrual bleeding. The diagnosis of menorrhagia can only be made after ruling out other gynecologic disorders, medical conditions or medications which may be causing heavy bleeding. Signs and symptoms of menorrhagia may include:
• Passing clots larger than the size of a quarter with menstrual flow.
• Soaking through more than one pad or tampon every 1-2 hours for several consecutive hours.
• Bleeding which requires doubling up on pads or using both a pad and a tampon to contain menstrual flow.
• Bleeding which requires getting up during the night to change pad or tampon.
• Activities of daily living are being impacted by bleeding.• Exhibiting symptoms of anemia such as weakness, fatigue
or shortness of breath. Possible causes of heavy menstrual bleeding generally fall into one of four categories:1. Uterine-related causes:
• Endometrial hyperplasia: A benign condition in which there is excessive proliferation of cells of the endometrium.
• Non cancerous growths or tumors of the uterus; uterine fibroids, polyps.
• Malformations of uterus.• Pregnancy complications: Complications such as miscarriage
or ectopic pregnancy can cause abnormal bleeding.• IUD: Heavy menstrual bleeding is a common side effect of
the IUD. If menorrhagia is excessive, the device may need to be removed.
• Adenomyosis: a condition in which the glands from the lining of the uterus become imbedded in the muscular wall.
• Malignancies of the uterus or cervix.• Pelvic inflammatory disease
2. Hormone-related causes: In a normal cycle, the balance between estrogen and progesterone regulates the build up of the lining of the endometrium which is shed during menstruation. An imbalance in these hormones may lead to excess build up of the endometrium which is eventually shed during menstruation.

8
Volume 22, No. 3
8
Anovulation is a common cause of menorrhagia. If ovulation does not occur properly, progesterone is not produced. During adolescence and menopause, menstrual cycles are often anovulatory, meaning no egg is released. This leads to irregular shedding of the endometrium and may cause increased and prolonged bleeding with menstruation. Girls are especially prone to anovulatory cycles in the first year and a half after their initial menstrual period. 3. Other illnesses or disorders:
• Thyroid, liver or kidney disease or endocrine disorders• Bleeding disorders and menorrhagia: It is estimated that
0.8-1.3% of the general population in the United States have some form of von Willebrand’s disease (VWD) (Rodeghiero, Castaman, and Dkini, 1987), a disorder which results from a deficiency or defect in the body’s ability to produce von Willebrand factor, a protein that is necessary for proper blood clotting. VWD is the most common bleeding disorder affecting women.
Although VWD affects both men and women equally, women have more opportunity to exhibit symptoms because of menstruation or childbirth. In addition to VWD, platelet function disorders may also be responsible for bleeding symptoms in women.
Menorrhagia is the most common bleeding symptom reported by women with bleeding disorders. In a survey conducted by the United States Centers for Disease Control and Prevention (CDC), 84% of women with von Willebrands disease reported menorrhagia (Kirtava et al., 2004). Women with VWD are five times more likely to experience menorrhagia than women in the general population (Sramek et al., 1995)
• Undiagnosed Bleeding Disorder: Very often, menorrhagia is the presenting symptom of an undiagnosed bleeding disorder. The prevalence of undiagnosed bleeding disorders among women with menorrhagia is high, with estimates ranging anywhere from 5–20% (Edlund et al., 1996). Many affected
women are unaware of their bleeding disorder and simply believe that they just “have heavy periods.” This condition is often undiagnosed when women seek medical attention for heavy menstrual bleeding due in part to the subjectiveness of symptoms
4. Medications:• Many medications including steroids, chemotherapy
agents, anti inflammatory drugs, anticoagulants and aspirin can cause an increase in menstrual bleeding.
• When not used as prescribed, oral contraceptives and other hormone preparations can cause heavy menstrual bleeding.
. Impact and Complications The morbidity of menorrhagia is profound. Menorrhagia can interfere with professional or academic activities which may have economic consequences. Heavy bleeding can disrupt leisure, social and physical activities. Having to change pads during the night can also lead to sleep disruption. Heavy bleeding can lead to mood changes and feelings of self-consciousness.Shanker, Chi, and Kadir (2008) reviewed studies examining quality of life and menstrual flow and found that more than 50% of women who described their menstrual bleeding as excessive felt forced to refrain from social activities during their periods. (10). –Author--I had some trouble with the underlined Disruption in actives of daily living may be due to distress caused by excessive bleeding in addition to menstrual volume alone. Menorrhagia is often accompanied by severe menstrual cramping, or dysmenorrhea, which may be severe enough to require prescription pain relievers. The uterus is very vascular and can lose a great deal of blood in a very short time Excessive blood loss may deplete iron stores enough to cause anemia. Anemia occurs in about two thirds of women with menorrhagia. Even mild anemia can cause weakness and fatigue. Severe anemia can have serious medical consequences and may lead to disruptions in the cardiovascular and respiratory systems. Symptoms of severe anemia include shortness of breath, chest pain, difficulty concentrating, dizziness, headache, or rapid heart rate.
Treatment of Menorrhagia Heavy menstrual bleeding may be a sign of an undiagnosed medical or gynecological condition. A full evaluation to try to determine the etiology of bleeding is important prior to beginning treatment. The underlying cause of bleeding will determine the best plan of care. Many effective treatments are available which offer relief to women suffering from heavy menstrual bleeding. Drug Therapy:
• Iron supplements are used to replace lost iron stores which may lead to anemia.
• NSAIDS are a first line therapy for menorrhagia. Studies have shown that NSAIDs reduce the amount of menstrual bleeding by as much as 30-40% (Livshits and Seidman, 2010). NSAIDs or other pain relievers
Table 1. Clinical evaluation of Mennorrhagia
An evaluation of menorrhagia may include:
Clinical history: A thorough clinical history will include the amount and duration of bleeding, the last menstrual periods, the age of menarche, and detailed family history. Pregnancy should be excluded.
Physical examination: This which should include a pelvic exam. Blood tests: to determine if there is any anemia or medical conditions such as thyroid abnormalities which may be causing symptoms.
Pap test Diagnostic imagining: This may include pelvic or transvaginal ultrasoundhysteroscopyEndometrial biopsy Laparoscopy Dilation and curettage (D&C)

September 2012
9
may also help reduce pain and menstrual cramping. NSAIDS should be used cautiously as they can increase bleeding.
Hormonal therapy:
• Hormonal therapy including oral contraceptives such as estrogen and progesterone combinations or progesterone alone may be used to correct hormonal imbalances. Combined hormonal contraceptives reduce menstrual blood loss by thinning the endometrium or by entirely suppressing menstruation. An added benefit of hormonal supplements is that they may also increase factor VIII and VWF levels.
• Combined hormonal contraceptive methods currently available include the combined oral contraceptive pill, transdermal contraceptive patches, and vaginal rings. The levonorgestrel intrauterine system (LNG-IUS, Mirena®) is an effective medical treatment for menorrhagia and has been shown to be useful in reducing menstrual blood loss. The Mirena is an IUD which has been impregnated with and releases progestin.
• Antifibrinolytic medications (tranexamic acid and aminocaproic acid) will help secure blood clot and delay clot breakdown by inhibition of plasmin which is an enzyme that helps dissolve blood clots.
Surgical Treatment:
• Dilation and curettage (D & C): D&C is a procedure which involves dilating the cervix and scraping the lining of the uterus to remove the top layer of uterine lining. This procedure may need to be repeated over time.
• Hysteroscopy: A hysteroscopy is a surgical procedure in which a scope is inserted into the cervix though the vagina to remove fibroids, polyps, correct abnormalities of the uterus or to remove uterine lining.
• Endometrial ablation: Endometrial ablation is a procedure in which the first few millimetres of thickness in the endometrium are destroyed by laser or heat. Some women will stop having menstrual periods altogether after an ablation, others may continue to menstruate but the menstrual flow will be lighter than before. Although the procedure does not remove the uterus, it will prevent women from becoming pregnant in the future.
• Hysterectomy. A hysterectomy is a major surgical procedure that involves removal of the entire uterus. After having this procedure, a woman can no longer become pregnant and will stop having periods.
• Laparoscopy: A laparoscopy is a procedure which is done through two small incisions in the abdomen. A laparoscopy is done to remove excess tissue that has formed on the outside of the uterus which commonly causes menstrual pain and bleeding.
Menorrhagia in the Camp Setting Menorrhagia away from home is problematic and is especially difficult at camp where even basic hygiene can be challenging. These difficulties are amplified when dealing with heavy menstrual bleeding. Education is extremely important. Many girls – campers and counselors – may be in the early, possibly anoovulatiory, stages of menses. Bleeding may be heavy or may occur irregularly out of cycle. Discussing the possibility of menses occurring during camp with both campers and counselors is essential. It is much easier to deal with menstruation at camp when you are prepared for it. General Management: Keep ample supply of pads, tampons and extra underwear readily available and make sure girls know where they are stored. Zip lock bags should be available for storage of clean pads or tampons and will keep them dry canoeing, boating, etc. Zip lock bags are also useful for disposal of used pads and tampons to keep animals at bay, especially when wilderness camping. Keep in mind that girls may need to use the bathroom during the night or may need to use the restroom urgently. Discuss this with counselors and make sure plans are made to accommodate this. Consider the location of activities, cabins and tents in proximity to restrooms. Evaluate your dress code policy or uniforms. Most women prefer not to wear tight clothing while having their periods. Darker bottoms and long T shirts may help avoid embarrassment. Provide opportunities for bathing or showering daily, even if this just means a sink bath or washing in the lake. Disposable wet naps will help in between. Privacy is important.Activities and Camp Life: While swimming is perfectly okay, some girls may prefer to avoid this. Dark swimsuit bottoms will help to hide any bleeding while in the water if tampons are not used or if there is overflow. Lake swimming is certainly less risky than swimming in a crystal clear pool as any bleeding will be less visible. Decide how your camp will deal with these requests and have a policy in place. These decisions are much harder to make last minute and often lead to unnecessary camp drama. Provide opportunities for rest periods. Girls with menorrhagia may experience fatigue, anemia or sleep disruption and may require additional rest periods. Again, discuss how your camp will deal with this before camp begins and have a policy in place. Offer a diet rich in iron to help body replace lost iron stores. Most “camp” foods are not especially high in iron Sources of food highest in iron include red meat, fish, poultry, egg yolks, dairy, dark leafy green vegetables (spinach, collards), beans, lentils, chick peas and soybeans, liver, or iron fortified foods. There are many tasty snack foods which are surprisingly high in iron – dried fruit, prunes, raisins figs, and roasted sunflower, sesame, pumpkin or squash seeds are all iron rich foods. Also, CHOCOLATE! An average dark chocolate bar will provide about 7% of recommended daily iron in an average 1.5 ounce bar.
Summary As we all know, camp can be a life-changing experience. It is very likely that one of your campers or counselors will be affected by heavy menstrual bleeding. With a little preparation, menorrhagia does not need to make camp an unpleasant experience.

10
Volume 22, No. 3
10
References
Shaw J. A., Shaw H.A. (2011). Menorrhagia. Medscape, 2011 http://www.emedicine.com/MED/topic1449.htm.
ACOG Committee on Practice Bulletins: Gynecology, American College of Obstetricians and Gynecologists (2001). ACOG practice bulletin: management of anovulatory bleeding. Int J Gynaecol Obstet , 72, 263–71.
ACOG (2000). Management of anovulatory bleeding, American College of Obstetricians and Gynecologists: Washington, DC. 1-12.
Edlund M, Blomback, B., von Schoultz, et al. (1996). On the value of menorrhagia as a predictor for coagulation disorders. Am J Hematol, 53(4):234–238.
Kirtava, A., Crudder, S., Dilley, A., et al. ((2004). Trends in clinical management of women with von Willebrand disease: a survey of 75 women enrolled in haemophilia treatment centres in the United States. Haemophilia, 10(2):158–161.
Livshits, A. and Seidman, D.S. (2010). The Role of Nonsteroidal Anti-inflammatory Drugs in Gynecology. Pharmaceuticals 2010(3):2082-2089.
Rodeghiero, F., Castaman, G., Dini, E. (1987). Epidemiological investigation of the prevalence of von Willebrand’s disease. Blood, 69(2): 454-9.
Shankar M, Chi C, Kadir RA. (2008). Review of quality of life: menorrhagia in women with or without inherited bleeding disorders. Haemophilia, 14:15-20
Sramek, A., Eikenboom, J.C., Briet, E., Vandenbroucke, J.P., Rosendaal, F. R (1995). Usefulness of patient interview in bleeding disorders. Arch Intern Med 1995; 155(13): 1409-15
Vessey, M.P., Villard-Mackintosh, L., McPherson, K., Coulter, A. &Yeates, D. (1992). The epidemiology of hysterectomy: findings in a large cohort study. British Journal of Obstetrics and Gynaecology, 99: 402–407.
Warner, P., Critchley, H.O., Lumsden, M.A., Campbell-Brown, M., Douglas, A., Murray, G. (2001). Referral for menstrual problems: cross sectional survey of symptoms, reasons for referral, and management. Br Med J, 323: 24–8.
Diana Mathis, RN, BS, is a nurse coordinator in the Hemophilia and Coagulation Disorders program at the University of Michigan. In the summer she is also health director for Camp Bold Eagle, a residential camp sponsored by the Hemophilia Foundation of Michigan for children with bleeding disorders serving campers from all over the Midwest.
Super Sleuth Answer – Ouch!Both Ardie and Alan have a muscle spasm, or Charley horse. Common causes for muscle spasms are heat, rigorous physical activity, dehydration, stress, muscle fatigue and/or shoes that do not fit well. Another contributing factor to muscle cramps can be vitamin deficiency, such as calcium, potassium, Vitamin D or magnesium. But in the summertime, in the heat, too much soccer on a hot day or poorly fitting shoes will be your best first guess.
Exam tips: A spasm tends to be a sudden onset of severe pain and you may find a firm area in the muscle that is tender. Remember, before massaging a calf look at the limb check for redness, streaks, swelling, deformity, assessing distal circulation, motion and sensation. If you suspect a blood clot or fracture proceed accordingly.
What to do? The routine things you do for prevention come first such as staying hydrated, cooling down, and making sure there are good breaks during vigorous physical events or scheduling them at cooler times of day. Stretching exercises before physical activity may help. Well-fitting shoes are better than tight ones.
Once you have the camper in front of you moaning, there are a couple things to try. Holding the calf muscle or toe in spasm and helping the camper relax all over will help the muscle in
spasm also relax. Setting the foot in warm water can help the toe spasm diminish. Sometimes massage can help the muscle relax. Sometimes the spasm comes so quickly and violently that there is an ache in the muscle after the spasm has passed. Warm packs can sooth this ache. Some sources suggest an ice pack. Let the camper be your guide for what feels best.
Most spasms of this nature are short term and self-correcting. If your camper has cramps like this “all the time” they may need to see their primary care provider when they get home.
Reference
Muscle Cramps from http://www.webmd.com/sleep-disorders/tc/nighttime-
leg-cramps-topic-overview.
Toe Cramps from http://www.buzzle.com/articles/toe-cramps-cause.
Wilderness First Aid: Emergency Care for Remote Locations (2008) 3rd Ed.
Jones and Bartlett: Sudbury, MA. (p121).
Janice Springer, RN, PHN, MA, DNP(c)American Red CrossDisaster Health Services Advisor, Minnesota

September 2012
11
Wounds at Camp: Could it be MRSA?Doris Nerderman, RN, BSN
Abstract: Wounds are a fairly common experience in the camp setting and infections can occur. In assessing infected wounds, the camp nurse needs to have a degree of suspicion for Community Acquired MRSA because camp activities and the community living setting are those commonly associated with the transmission of this infection. Infections can present in a variety of forms and with a variety of symptoms. Careful assessment and treatment initiation are important as is incorporating infection prevention into all aspects of camp life.
For many years MRSA was associated with a hospital acquired infection that only debilitated people seemed susceptible to. Today, Community Acquired or CA-MRSA is an all too common problem in otherwise healthy people. Of these healthy people, it is frequently the young athlete who develops MRSA. Transmission of MRSA skin infections is through close skin to skin contact with another person or contact with a fomite or surface contaminated with MRSA. Most often involvement includes a young athlete because of the close contact with others during games and afterward in the locker room where shower facilities are shared and contact with personal items of others is more apt to occur. Does this have a familiar ring? Camp settings, like sports facilities, can be a highly susceptible risk for the presence of MRSA and its spread. Campers develop scrapes and/or cuts while playing, then come in contact with others during activities and sharing common spaces such as cabin interiors, dining areas, bathrooms and showers.
Consider the following scenarios: Camp nurses never know what situation is going to present each time someone arrives at the Health Center. I wasn’t expecting these recent issues. Joe, age 14, arrives at the Health Center complaining of a “pimple like” area above his right knee. He initially noticed it yesterday afternoon but it is more painful today. He also has a scabbed area on his right knee that he tells you he sustained during a soccer camp that he attended the previous week. Upon examination, a two inch area around a pimple-like lesion is red, swollen, warm and tender to touch. Joe also states that he has a headache and had experienced chills during the night. Joe’s temperature is 101.2°F. In this case, Joe had an open area to his skin. The staph germs that commonly live on the skin and don’t usually cause any harm can be dangerous when open skin occurs. Jim, age 18, arrives at the Health Center complaining of aches, chills and headache. His temperature is 102°F. He has been feeling bad since this morning and also complains of pain in his thigh. Upon exam it is noted that Jim has an approximately six inch circular area on top of right thigh that is reddened, warm, tender to touch and swollen. There are no open areas and he is not aware of any injury to his leg.
There was no real identifier for the second case, but this is not unusual. Again, any open area – no matter how small – can allow staph germs into the body. Infections can present in a variety of forms regardless of the causative agent. These forms include:
• Cellulitis• Impetigo• Folliculitis• Furunculosis• Carbuncle• Abscess
• Presentation may initially be diagnosed as a spider bite.A helpful resource for learning more about the appearance of these forms can be found at http://www.cdc.gov/mrsa. The pictures at this site can be especially helpful and there are also some good educational materials.
Assessment Regardless of whether a skin issue is MRSA or not, thorough skin assessment is vital.Look at the skin:
• Note the color of the area. Is it normal skin color or reddened? • Touch the skin. Is the area warm and/or tender to the touch? • Assess for local swelling. If it is swollen, it is a good idea to
mark the area to assess any increase or decrease with each subsequent assessment.
• Consider general skin integrity. Are there other areas of concern?
• Inspect for any drainage or pustule presence if draining. Note color and consistency of drainage.
Ask the camper questions:• How long has it been there?• Is the camper aware of any injury or bite to the skin?• Is there any history of previous skin issues
Check for fever and other symptoms, such as achiness or joint pains that could indicate systemic infection.
Care Approaches If the area is not significantly swollen and there is no specific recent issue, simply monitoring may be the appropriate approach but it is wise to mark the area to facilitate swelling assessment. Applying warm soaks may draw the infection out and will soothe the area. If the area is open, it may be advisable to apply antibiotic ointment,

12
Volume 22, No. 3
12 12
cover the open area and monitor closely. If camper has a fever as my campers did, this indicates a need for more prompt and aggressive diagnosis and treatment. If there is an open wound or pustule, a culture should be taken before antibiotic treatment is initiated. If there is no open area, definitive diagnosis for MRSA cannot be made but the physician may elect to treat as MRSA based on the assessment of the site and the camper. Providers may choose to treat with IV antibiotics and the patient may need to return to the hospital or treatment setting for additional dosages. If this is the case, the person will be returning to camp with a heparin lock in place and need to be instructed on proper care of the catheter and any activity limitations. Alternatively, the affected person may be given oral antibiotics and/or a combination of both IV and PO medications. The camp nurse needs to be sure medications are taken as directed and that the prescribed course is completed. Teaching includes instructing campers taking these medications to eat yogurt or provide with acidophilus tablets to prevent yeast overrun. Table 1 highlights antibiotics commonly used for MRSA infections.
It is also very important to communicate health issues with parents and keep them updated accordingly. Together, along with the health care provider, a determination can be made as to whether the child should remain at camp, have a shortened stay or go home for a few days and return when feeling better. Whatever the plan of care, parents should remain informed on the status of the child.
Prevention: Opportunities for Health Teaching Preventing MRSA and other infections at camp is an important Health Center challenge. Camp nurses can be very creative in finding ways to incorporate prevention messages into orientation and day-to-day activities. They may seem like such simple messages but are essential in preventing the occurrence and/or spread MRSA (or any other bacteria). And, the messages bear repeating throughout the season. These basic messages include:
Table 1.
Antimicrobial Adult Dose2** Pediatric Dose2**
Trimethoprim-sulfamethoxazole (TMP/SMX) DS
Minocycline or Doxycycline
Clindamycin1
1-2 double strength tablets 8-12 hours3
00 mg PO 12 hours4
300-450 mg PO 8-12 hours
Base dose on TMP: 8-12 mg TMP (& 40-60 mg SMX) per kg/day in 2 doses; not to exceed adult dose
Not recommended for children younger than 9 years of age. For children 9 years or older: 4 mg/kg/day in 2 divided doses, not to exceed 200 mg/day.
10-30 mg/kg/day in 3-4 divided doses; not to exceed adult dose
NOTE: Outpatient use of quinolones or macrolides. Fluoroquinolones (e.g., ciprofloxacin, levofloxacin, moxifloxacin, gatifloxacin) and macrolides (e.g., erythromycin, clarithromycin, azithromycin) are NOT recommended for treatment of MRSA because of ready development of resistance. If fluoroquinolones are being considered, consult with an infectious disease specialist before use. Source: CDC
Interim Guidelines for Empiric Oral Antimicrobial Treatment of Outpatients with Suspected MRSA Skin and Soft Tissue Infections (SSTI)
• Eat right.• Get plenty of sleep. • Practice good hygiene and use hand sanitizers when soap
and water not available.• Don’t share towels and be careful not to hang towels on top
of others.• Do not share personal items.• Keep cuts, abrasions clean; instruct campers to keep
wounds clean and reinforce this teaching repeatedly. During staff training discuss the importance of keeping open areas clean and signs and symptoms the staff should look for. Having staff “tuned in” to preventive measures can be very helpful in keeping campers healthy. Staff members are more likely than the nurse to be the first to see a skin issue if they are educated about what to look for. Also, reiterate to your staff to seek the nurse’s assistance in dealing with skin issues to promote early intervention and surveillance. Appropriate messages for staff education include:
• Wipe off equipment before and after using it. From the scenario at the beginning of this article, note that Jim had been spending time in the weight room and may have picked up MRSA from contaminated equipment.
• Disinfect surfaces with disinfectant products available at retail and grocery stores. Some antibacterial wipes are easy to use and effective against many bacteria. Whether you use the wipes or spray, check the label for a list of germs the product can destroy. Labels that indicate effectiveness against Staphylococcus Aurous should be effective against MRSA. Read the label carefully for proper use and handling as well.
• You can make your own effective bleach solution. Mix 1 tablespoon of bleach into 1 quart of water. Be aware that you must make a fresh solution each time you plan to clean because the bleach
evaporates reducing the strength of the solution. Fortunately, recent research has shown CA-MRSA is on the decrease but it is still very important to be alert to the potential for MRSA to occur in a communal living situation such as a camp setting. Certainly, every wound you see will not develop into MRSA, but it is certainly good practice to consider the possibility.
Resourceshttp://cdc.gov/mrsa/.
Doris Nerderman, RN, BSN just completed her 27th year of camp nursing experience at Camp Belknap, NH. During the rest of the year she teaches LPNs in Ohio. She is a CompassPoint Editorial Board member.
September 2012
13
Abstract: Using a three-week convenience sample based on logged entries from three residential camp Health Centers, this descriptive study rank ordered the reasons campers and staff sought healthcare to (a) inform prospective nurses about anticipated injuries and illnesses; (b) determine if medical protocols were sufficient; (c) determine if Health Center supplies were adequate; and (d) use the data as a lagging indicator about the camps’ risk management initiatives. Headache (109 entries) was the most frequent reason for seeking care followed by wounds (94), general aches/strains (89), and respiratory problems related to the common cold (75); additional data is presented in table form. Need for improved protocols was determined for trouble sleeping and wounds from leeches, and a post-summer audit of individual health documentation was suggested to gain deeper understanding of several interest points.
Why Campers and Staff Seek Care from Health Center Staff
Linda Ebner Erceg, RN, MS, PHN, and Rachel J. Brodin
As we become more effective in managing camp health services, the need to know why campers and staff seek healthcare continually rises to the surface. This descriptive study was initiated to answer that question. Knowing why people seek healthcare contributes to preparing the camp nurse to handle anticipated needs and helps assure that medical protocols cover anticipated injuries and illnesses. The knowledge also informs decisions about what supplies are needed in the Health Center and provides a lagging indicator for assessing the effectiveness of risk management strategies. A second tier reason for doing this study was to demonstrate a basic research process that others may want to replicate in order to be more informed about their camp’s injury-illness experience.
What Does Literature Say? In 1998 Rauckhorst and Aroian published a now classic descriptive study that examined the relationship between camper age, developmental level, gender and use of camp health services. Using the Health Center’s log book, the researchers utilized a convenience sample and determined that the most frequent reason for seeking healthcare was associated with injury (30.6% of logged Health Center visits). The next most common reason was associated with communicable illnesses (20.6%), most frequently upper respiratory infections (e.g., the common cold). This was followed by “discomfort-related problems (554 or 16.1%), which included symptoms such as knee pain, headache, and (in the girls’ camp) dysmenorrhea” (pg. 203). Allergies held the fourth spot (12%) followed by other events that were less than 10% of the total reasons. Interestingly, the Rauckhorst and Aroian study remarked that psychosocial problems ranked lowest in frequency (0.3%) “perhaps . . . because counselors dealt more with these children in loco parentis on a daily basis. . . and the children may have viewed the camp nurse as someone from whom they could seek assistance with physical rather than psychosocial/emotional problems” (pg. 203). The next article that addressed the topic appeared in 2006 (Yard, Scanlin, Erceg, Powell, Wilkins, Knox and Comstock). Also a descriptive study using a convenience sample with data coming from 25 contributing camps (day and resident), this study
reported that cuts/scrapes were the most common injury diagnosis (33.3%) followed by fracture (14.6%), and then sprains/strains (10.4%). The gastrointestinal system ranked highest (43.1%) in the illness category followed by headache (29.4%) and throat (17.6%) problems. Reported communicable illnesses comprised 11.8% of cases and related to illness among others at camp. Readers should note that this study’s illness data did not focus on diagnosis but rather on body system involved. The American Camp Association’s five year Healthly Camp Study (2011), an epidemiologic study of camp injuries and illnesses, included an overview of reasons why campers and staff sought healthcare. In assessing that data, note that this study’s injury-illness experiences were included only if the injury or illness met the study’s case definition (the injury or illness had to pull resident campers and staff away from their camp routine for at least four hours; that case criteria changed to one hour for day campers and staff). Consequently, not all reasons for seeking healthcare were reported. With that caveat in mind, the study reported that campers and staff experienced the following injuries in rank order: sprains (most common reason), wounds, bruises/contusions, blows to the head, fractures, and dislocations. All other injuries were less than 2% of reported categories. The same study reported that illness associated with the upper respiratory track consistently represented just over 20% of reported illness in each year of the study. Illnesses associated with the gastro-intestinal tract ranked a close second and all other illness categories were consistently less than 5% of reported totals. This last 5% included allergic reactions, heat-related illnesses, asthma flares, genital-urinary conditions and illness associated with ticks (American Camp Association, 2011)
Research Process and Results Keeping in mind that the purpose of this project was to examine why campers and staff sought healthcare (descriptive), the researchers accessed a convenience sample of campers and staff from three residential camps. Each camp was under the same administrative umbrella, thus increasing the likelihood that protocols were the same and limiting the impact of confounding variables. Campers were 8-18 years old; staff ranged from 18-50 plus years with the majority of staff in their second decade of life. The sample group was generally a healthy population; people with chronic health

14
Volume 22, No. 3
14 14
concerns – asthma, diabetes, allergies and so forth – were capable self-managers with stabile care plans upon arrival. While staff remained at camp, the campers represented one-, two- and four-week groups during the three-week data collection period. During the three weeks that data were collected, there was a minimum of 327 total people at the camps; at most, there were 392. These campers and staff accumulated 5,593.5 days of camp participation (the sum of the number of people at camp multiplied by the number of days each person was at camp during the data collection period). The total number of logged visits to the camp Health Centers during the three week period (21 days) was 1,019. That averages to 48.52 people seen per day (daily average for the three health centers combined) and represents about 15% (14.98%) of the population seeking healthcare on any given day. Three weeks of logged entries were retrospectively examined and the reason for seeking healthcare was sorted into categories. That sorting is summarized in Table 1. A discrete entry was made for each logged Health Center visit and grouped under injury, illness or psychosocial categories. To limit the potential that a logged entry might be sorted differently, the same researcher sorted the data but discussed uncertainties with the fellow researcher. In addition, the team made decisions about reasons for seeking care that did not fit cleanly into an injury or illness category. For example, dysmenorrhea isn’t really an illness but it isn’t an injury either. In addition, rashes could be related to illness, the result of an incident (e.g., getting poison ivy from contact with the plant), or of undetermined etiology. In situations like this, the researchers put priority on capturing the reason for seeking healthcare and, consequently, took liberty with assigning the category (e.g., dysmenorrhea to illness; rashes/poison ivy to injury). Of significant note was the observation that the logged reason for seeking healthcare did not, necessarily, remain the reason once nursing assessment was completed. In other words, why the individual sought care might vary from what was really needed. For example, a client’s “rash” was assessed and care provided based on etiology. Poison ivy was handled differently from heat rash, contact dermatitis, impetigo, rash associated with a reaction to an antibiotic, and so forth. What made the client seek care was “rash” so that category was used in this data set. Knowing the reason why people sought healthcare was then compared to the camp’s written protocols to determine if the nursing staff had adequate care guidance. Protocols were found for all listed reasons except for leeches, blisters, trouble sleeping, depression and anxiety. Anecdotal reports from the nursing team indicated that nurses utilized the camp’s wilderness first aid text when caring for leech wounds and blisters, and drew on their general nursing assessment skills to handle complaints of sleeplessness, depression and/or anxiety. Anecdotal report also indicated that Health Center staff “made do” with what supplies were on hand when caring for client injuries and illnesses. While some supplies or protocols were available specifically for some needs – for example, giving acetaminophen for headache, cleaning and bandaging a wound, referring people to a physician when otitis was suspected – a few reasons for seeking care weren’t adequately supported. When asked, the Health Center staff requested protocols for assessing and addressing sleeplessness, and deeper
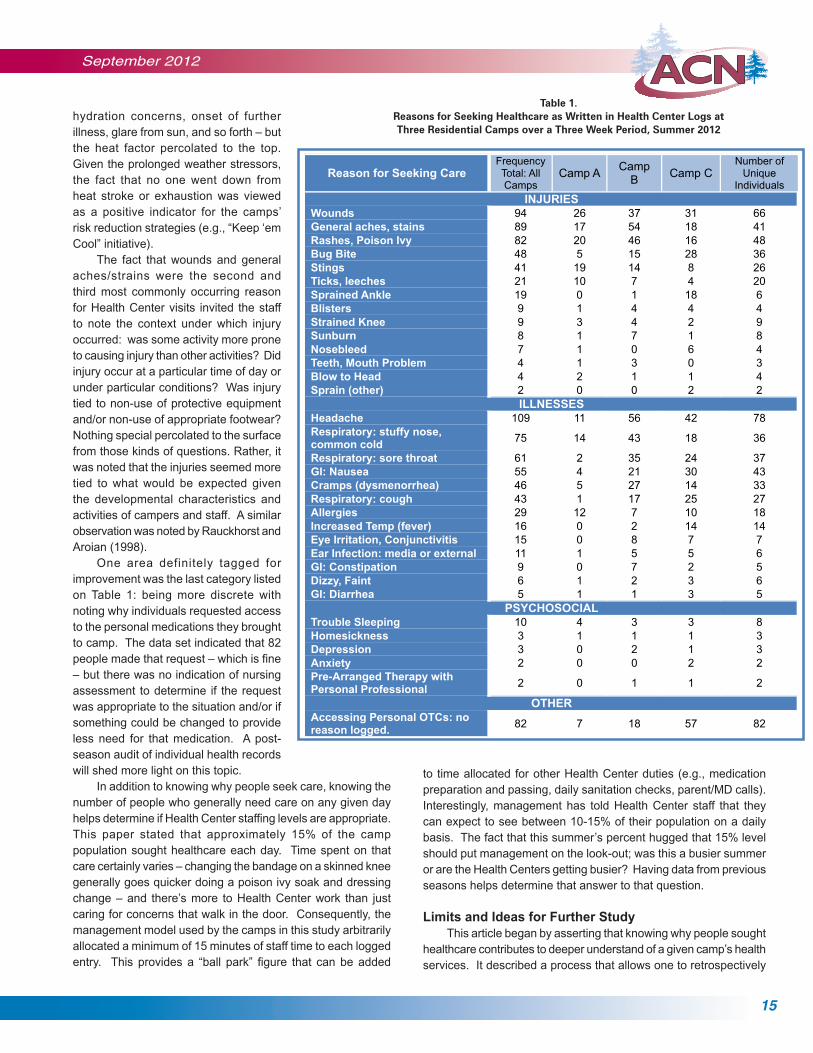
information about assessing and caring for blows to the head. The study also noted the impact of the final column in Table 1: “Number of Unique Individuals.” Given a specific category (wounds, general aches/strains, rashes/poison ivy, etc.), this column counted the number of different people who presented with that injury, illness or psychosocial need. For example, there were a total of 94 wounds events that caused people to seek healthcare but those wound events were reported by 66 unique individuals. Some people returned more than once for wounds. Noting such data has implications for identifying individuals who may be predisposed to certain ailments, workers who may need retraining (e.g., to have fewer cuts), communicability of some illnesses, and provide a lagging indicator for therapies that may not be effective (e.g., does the person return because what was done the first time didn’t resolve the problem). Observations such as these, however, must be balanced with the rationale for return visits. Certain problems – like having poison ivy – typically require return visits as the problem moves toward resolution. In other words, some return would be expected in some situations.
Discussion What started as a simple study – why do people seek healthcare? -- resulted in specific ideas for improving the camp’s health services. First, a deeper knowledge about both the load of people seeking healthcare on a daily basis was obtained as well as a deeper understanding about why that care was sought. Assuming that pooled data from three camps would provide the “critical mass” needed to extrapolate information, the data in Table 1 clearly helps prospective camp nurses understand the reasons why campers and staff typically seek care. Knowing this allows the nurse to assess his/her own knowledge base; it is adequate for working in this Health Center? If not, can knowledge gaps be addressed prior to camp and/or by accessing resources while at camp? One can also look at the data for individual camps and see some interesting differences. For example, Camp A demonstrated a lower frequency than the other camps in several categories. Why is that? Might Camp A be doing something protective that could be applied to other camps? This observation would not have been noticed had the data not been reviewed. Doing so provides opportunity for deeper investigation to more fully understand what is or isn’t happening at Camp A. The frequency with which a health problem triggers a visit to the Health Center provides other information. In this data set, “headache” was the most common reason for seeking care (109 entries) followed by wounds (94 entries), general aches/strains (89) and rashes/poison ivy (82). Given the number of headaches, it was beneficial to audit individual health records to determine the reason. In doing so, the most common reason for headache was related to the many days of high heat/humidity that hit the camps’ northern Minnesota location. Health Center staff referred to it as “heat stress,” the cluster of symptoms that humans experience when under assault from consistently hot, humid conditions. Yes, there were other reasons too –
September 2012
15
Volume 19, No. 2
hydration concerns, onset of further illness, glare from sun, and so forth – but the heat factor percolated to the top. Given the prolonged weather stressors, the fact that no one went down from heat stroke or exhaustion was viewed as a positive indicator for the camps’ risk reduction strategies (e.g., “Keep ‘em Cool” initiative). The fact that wounds and general aches/strains were the second and third most commonly occurring reason for Health Center visits invited the staff to note the context under which injury occurred: was some activity more prone to causing injury than other activities? Did injury occur at a particular time of day or under particular conditions? Was injury tied to non-use of protective equipment and/or non-use of appropriate footwear? Nothing special percolated to the surface from those kinds of questions. Rather, it was noted that the injuries seemed more tied to what would be expected given the developmental characteristics and activities of campers and staff. A similar observation was noted by Rauckhorst and Aroian (1998). One area definitely tagged for improvement was the last category listed on Table 1: being more discrete with noting why individuals requested access to the personal medications they brought to camp. The data set indicated that 82 people made that request – which is fine – but there was no indication of nursing assessment to determine if the request was appropriate to the situation and/or if something could be changed to provide less need for that medication. A post-season audit of individual health records will shed more light on this topic. In addition to knowing why people seek care, knowing the number of people who generally need care on any given day helps determine if Health Center staffing levels are appropriate. This paper stated that approximately 15% of the camp population sought healthcare each day. Time spent on that care certainly varies – changing the bandage on a skinned knee generally goes quicker doing a poison ivy soak and dressing change – and there’s more to Health Center work than just caring for concerns that walk in the door. Consequently, the management model used by the camps in this study arbitrarily allocated a minimum of 15 minutes of staff time to each logged entry. This provides a “ball park” figure that can be added
Table 1.
Reasons for Seeking Healthcare as Written in Health Center Logs
at Three Residential Camps over a Three Week Period, Summer 2012
Reason for Seeking CareFrequency Total: All Camps
Camp ACamp
BCamp C
Number of Unique
Individuals
INJURIES
Wounds 94 26 37 31 66
General aches, stains 89 17 54 18 41
Rashes, Poison Ivy 82 20 46 16 48
Bug Bite 48 5 15 28 36
Stings 41 19 14 8 26
Ticks, leeches 21 10 7 4 20
Sprained Ankle 19 0 1 18 6
Blisters 9 1 4 4 4
Strained Knee 9 3 4 2 9
Sunburn 8 1 7 1 8
Nosebleed 7 1 0 6 4
Teeth, Mouth Problem 4 1 3 0 3
Blow to Head 4 2 1 1 4
Sprain (other) 2 0 0 2 2
ILLNESSES
Headache 109 11 56 42 78
Respiratory: stuffy nose, common cold
75 14 43 18 36
Respiratory: sore throat 61 2 35 24 37
GI: Nausea 55 4 21 30 43
Cramps (dysmenorrhea) 46 5 27 14 33
Respiratory: cough 43 1 17 25 27
Allergies 29 12 7 10 18
Increased Temp (fever) 16 0 2 14 14
Eye Irritation, Conjunctivitis 15 0 8 7 7
Ear Infection: media or external 11 1 5 5 6
GI: Constipation 9 0 7 2 5
Dizzy, Faint 6 1 2 3 6
GI: Diarrhea 5 1 1 3 5
PSYCHOSOCIAL
Trouble Sleeping 10 4 3 3 8
Homesickness 3 1 1 1 3
Depression 3 0 2 1 3
Anxiety 2 0 0 2 2
Pre-Arranged Therapy with Personal Professional
2 0 1 1 2
OTHER
Accessing Personal OTCs: no reason logged.
82 7 18 57 82
Table 1. Reasons for Seeking Healthcare as Written in Health Center Logs at Three Residential Camps over a Three Week Period, Summer 2012
to time allocated for other Health Center duties (e.g., medication preparation and passing, daily sanitation checks, parent/MD calls). Interestingly, management has told Health Center staff that they can expect to see between 10-15% of their population on a daily basis. The fact that this summer’s percent hugged that 15% level should put management on the look-out; was this a busier summer or are the Health Centers getting busier? Having data from previous seasons helps determine that answer to that question.
Limits and Ideas for Further Study This article began by asserting that knowing why people sought healthcare contributes to deeper understand of a given camp’s health services. It described a process that allows one to retrospectively
16
Volume 22, No. 3
It Happened This Summer2012 Camp Nurses Share Their Experiences
use logged information to (a) inform prospective nurses about injuries and illnesses they can anticipate caring for, (b) determine if protocols cover needs, (c) determine if Health Center supplies are adequate, and (d) provides a lagging indicator about the camp’s risk management program. The study was merely descriptive and quite narrow in scope; looking at causation would require a much more robust design. The study reflects the experience of three resident camps that shared a common administrative umbrella; this limits its generalizability to other programs. Questions were posed in the body of the article that require deeper exploration, thus giving rise to the need for continued research. This is especially true regarding a documentation audit to determine if what was suggested by logged information was, indeed, supported by nursing assessment and interventions. Nonetheless, studies like this provide management with much needed indicators about program effectiveness and modifications. How much better to go into the autumn having some idea how one might improve, especially in the area of injury and illness experience! Our campers and staff deserve that.
References American Camp Association (2011). The healthy camp study impact report.
Martinsville, IN: American Camp Association.
Rauckhorst, L. and Aroian, J.F. (1998). Children’s use of summer camp health facilities: A longitudinal study. Journal of Pediatric Nursing, 13 (4), 200-209.
Yard, E.E., Scanlon, M.M., Erceg, L.E., Powell, G.M., Wilkins, J.R., Knox, C.L., and Comstock, R. D. (2006). Illness and injury among children attending summer camp in the United States, 2005. Pediatrics,118 (5), pg. 1342-1349).
Linda Erceg, RN, MSN, PHN is Assistant Director for Health and Risk Management at Concordia Language Villages of Bemidji, MN, and the Executive Director of the Association of Camp Nurses. Rachel J. Brodin worked as a Health Center Assistant this past summer at Concordia Language Villages, Bemidji, MN, where her duties included helping Linda Erceg with management of the Language Villages’ health services.
It’s Always Something I was at camp for seven days and had an event almost every day – the first time ever for anything out of the ordinary! It rained for most of the week. Camp kept going but everyone stayed wet, had blisters from wearing their Chacos or water shoes constantly, and had colds and runny noses. The counselor from England was on the soccer fields playing soccer in the rain – mostly mud sliding. The rain caused the ants to come out and they were floating in the rain water along with fresh cut grass. The counselor appeared in my doorway and he was quickly becoming covered with hives. He had raised whelps and red splotches everywhere. I never quite figured out if he reacted to ant bites or to a hay/grass allergy. He was given Benadryl and observed closely. Eventually the hives faded and he was able to return to work within about three hours, after sleeping off the Benadryl. I insisted that he not go back to the soccer field and suggested he be tested for allergies when he returned home. Lisa South, RN, DSN Maben, MS
Bats are Still Around! Last year I wrote an article (CompassPoint 21:4, 7-11) about how one copes with presumptive exposure to rabies when a bat is flying in a cabin in which people (campers and staff) are sleeping. As I emerge from this summer, I wanted to let you all know that we caught six bats that managed to meet the definition for presumptive exposure to rabies for our program. All six bats were submitted for testing and all came back negative. While we breathed a sigh of relief over that news, an interesting piece of information was that those captures were due to the valiant efforts of our bat catchers. Some captures really took effort! For example, one team could not catch the bat on the night of the exposure so they moved all the kids to other sleeping areas and kept an all-night vigil. They caught the bat at 5:17 am the next morning– and yes, we did a celebratory dance. Another team also couldn’t find their bat and they ended up doing a thorough search of the cabin the next morning. And I mean thorough; they stripped beds, moved everything away from walls, shined flashlights into cracks, poked a wire into various holes, and eventually found the bat under a rug on the floor. My take-away from this was that persistent rechecking for a bat typically pays off. Yes, the initial capture may not be successful but rechecking–even over several hours–is a good idea. We also continue working with a professional exterminating team to reduce the load of bats in our sleeping areas. We have 12 sites and over 100 designated sleeping areas, so the quest is substantial. We’ve seen a decrease in the number of bats that meet the testing criteria so we’re making headway.
Linda Erceg, RN, MS, PHN Concordia Language VillagesBemidji, MN
Improving Healthcare Outcomes The majority of our campers come to one of our five Atlanta area Girl Scout camps for a six day session. We review their health histories before camp, but the parents supply medications on opening day. My goal this summer was to be proactive, and I initiated two checks to improve our health care outcomes:1. We checked and double-checked the expiration date on all Epi Pens and also asked parents when it was last used (“never” was the usual answer) and even had the camper read the directions for use. At one camp we found three expired pens on one check-in day.2. For campers who carried a rescue inhaler for PRN use, we again

September 2012
17
Camp Was Where We Landed “It was the best of times, it was the worst of times.” Dickens had it right. It was the best of times—my husband Terry and I had just bicycled 2700 miles over seven weeks from Oregon and the Pacific Ocean to Bemidji, Minnesota, and had arrived at Concordia Language Villages to see our son, who was working at the Norwegian camp. Wonderful reunion with Erik! It was the worst of times—six miles from camp, my husband was struck by a car which broke his arm in two places, and that was the end of our cross country bike trip. But camp was where we landed, and it was a good place to begin the healing process from a broken arm and a broken dream of 32 years. I had worked there as a camp nurse several years ago, and I felt right at home. Linda Erceg’s house is on the camp property, and I was able to visit with her twice, and borrow her accordion, too. (If you ever need an accordion, Linda has one!)
Camp is many things and I learned that it can also be the perfect place to start moving through the grieving process when one’s long anticipated bike trip comes to an abrupt and painful end. Terry and I were surrounded by our son, supportive staff and
campers, and we could interact with camp activities or be alone as our physical and mental anguish fluctuated. The camp dean invited us to stay as long as we wanted, and we felt warmly welcomed. Two days after the bike accident, we did an all-camp tire dipping ceremony at the lake. Terry and I had started our bike trip by dipping our rear bike tires in the Pacific Ocean, and with Erik’s help with Terry’s bike, we dipped our front tires in the lake at camp, signifying an end to the first part of our cross country trip. Terry and I talked about our trip and the dean read a beautiful and inspiring certificate she had created for us. It was a very camp-y thing to do and it felt just right. This was my first summer in 15 years of not being a camp nurse. Last summer I was at a camp in the Swiss Alps (CompassPoint 21:3), and I will return there next year. Before our bike trip began, I knew that being at the Norwegian camp would give me my camp fix (albeit very short!) for this summer, but I didn’t know that it would come to play such an important role in my emotional health. We all know how healing camp can be, and it certainly did its part in beginning that process for Terry and me. We couldn’t have picked a better place for us to be for an abrupt ending of our bike trip than to have been at Skogfjorden. Camp—a healing place for us and for many, for sure.
Mari Rudd, RNPortland, OR
checked for expiration, last use and whether the camper know how to use it correctly. For campers who only carried a rescue inhaler (did not use maintenance allergy or asthma medications), the nurse or health assistant checked with them daily to ask if they had needed to use their rescue inhaler and documented this data on the Medication Administration Record System (MARS). I initiated the daily check in to be able to intervene early for a camper who may have been experiencing difficulty with the hot weather and/or poor air quality days. In addition to these checks, I initiated other actions related to air quality. I asked the nurses to check in with campers and staff at high risk for respiratory problems. I kept the camp zip codes for the five camps in my weather alert system on my Ipad. For days that were high alert respiratory days, I quickly texted the health assistant/nurse/camp director or e-mailed them alerting them to the air quality warning. I asked them to check in with campers and staff who were high alert for respiratory problems. One camp was close to the city and had a couple of “code red” days. We had discussed ahead of time having alternative indoor activities for those who were high risk and requested the rangers avoid any maintenance activities which would stir up grasses, leaves and dust on those high alert days. There appeared to be ready acceptance of these measures and we believe it added to the safety and quality of care at our camps. Lisa Cranwell-Bruce, MS, RN, FNPC, APRN
Girl Scouts of Greater AtlantaAtlanta, GA
Surprise Diagnosis We had a 19 year old counselor this summer who came to the nurse complaining of swollen ankles. Swollen they were - she had pitting edema in both ankles. Elevation, cool packs, and a good history was taken. She also complained of unexplained fatigue and generally not feeling her best. An existing diagnosis of hypothyroidism indicated the need for a routine blood draw. In view of her unusual symptoms, additional blood work was decided upon. She ended up in the ICU that night with a blood glucose level of 863! What seemed most amazing is that she didn’t have more symptoms! She had probably been living with high glucose for some period of time and her body had slowly adapted. She now has a new diagnosis of Type 1 diabetes and is beginning appropriate care and monitoring. She was able to return to camp and complete her last few weeks as a counselor. Boy – you just don’t know what each day will bring! Mary Marugg, RN Sonlight Christian Camp Pagosa Springs, Co

18
Volume 22, No. 3
Our New Health Center So it was finally here, our new infirmary…oh, I mean Health Center. We had waited years, literally, for this summer season. Our director had worked tirelessly to secure funding, develop the plans, supervise construction and design our beautiful new digs for our 1200+ campers that come every summer. It was beautiful and a far cry from our last infirmary that had faithfully served our camp for the past 30 years. There were no leaks in the ceiling or oozing from the floor (we never figured out exactly what that was), no strange smell, no supplies stocked under camper beds, no arranging and rearranging equipment just to make it work. We wouldn’t have to turn on window air conditioners, set out mouse traps or act as traffic cops just to shuffle our kids around in our small space during sick call. No, our new digs were spectacular: four beautiful treatment rooms with new equipment, a gigantic medication room, a private office for phone calls….the list goes on and on. And it was big, really big. We had plenty of storage space, enough camper rooms so we wouldn’t have to cohabit sick campers with “not so sick” campers, and a huge porch and front area so that the kids weren’t on top of each other. We even had lap tops so we could begin electronic charting. We had moved into the big time. So why, on my first night as I was lying there in my new room with lovely new furniture, was I feeling melancholy, wistful even? Did I actually miss the smell, the cramped feeling, the hours of cleaning it took just to start the year? Was that possible? Camp for me is all about the traditions. The first ride into camp past the lake, meals in the dining hall, song sessions, and color war….as a camper and as a staff member, I don’t like too much change in my camp routine. I missed it, my old home. I missed the plaques on the wall that had been made by the nursing staff throughout the years but that didn’t really match with our new decorations. I missed our one big desk and the old chairs that we sat around many nights and laughed about some incident that happened that day; I missed the murals on the walls painted by one group or another through the years; I missed the whirl of the window air conditioner and the hand crank to raise the med window. Our new health center was clean, antiseptic; it was like a doctor’s office. It didn’t feel campy at all. I sighed, rolled over on my new pillow top mattress and rested to ready myself for the first day of camp. Our first camper in the new Health Center arrived quickly – a first year camper who was stung by a bee as she stepped off the bus. She was given an ice pack, medicaine and a hug and sent on her way. They came quickly after that. There were lots of accolades for our new place, some also sad about the loss of our old friend, the infirmary. It took no time, however, before the campers were coming in as usual
– bug bites, scrapes and bruises, headaches, sore throats. I sat at the long front desk and listened to the tale of how he fell off his mountain scooter, gave a nebulizer in our new fancy room dedicated to respiratory problems, and soaked a toe that had been damaged by the benches in the dining hall in the new foot soaking room. A week later as we all sat around one night and laughed about the camper that always forgot his meds, the staff member with the curious shaped sunburn from his sandals and the mom who wouldn’t stop calling about her son, I realized that our Health Center was still our infirmary. It wasn’t the location or building that made it campy; it was the campers, staff, the doctors and nurses. Camp is more than activities and schedules. Camp is a community, a feeling, a connection that can’t be changed by a new building. Our new Health Center was great—everything we had hoped for. However, it didn’t change the nature of who we are or how we care for our camp family. Jodie Rodriguez, RN, MS, CPNP, AE-C
Camp Barney MedintzCleveland, GA
Who Let the Cats Loose in July?!? Our camps are located in a part of the US that experienced many, many days of very hot weather and high humidity during July. Our northern Minnesota location wasn’t protective whatsoever. Getting and keeping people cooled down got tricky. While no one experienced classic heat reactions (way to use those cooling strategies!), stress related to being hot was evident. Tempers flared more quickly, appetites were off, sleep wasn’t as restful, and get-up-and-go got-up-and-went for everyone. I suspect many readers can relate. The fact that camp continued, albeit a bit slower, was great and the fact that no one went down because of heat exhaustion/stroke was even better. But July also brought:
• A case of pertussis;• A case of chicken pox;• A wind storm that knocked out electricity and several trees;• A flooded metro area so parents couldn’t pick up their camper nor could some in-coming campers get to us;• A couple of nurses who resigned;• More deer ticks than ever before;• Interesting skin breakdown (rashes?) related to prolonged heat and humidity.
Things were percolating so quickly it made me wonder what happened. Perhaps one simply has a wild season every so often, yes? I’m more than ready to put the cats back into their bag but I’m also thankful for what we learned as we coped with these challenges. And I was glad I had a team of other camp leaders to work with as well as a solid communication record with our parents.
Linda Erceg, RN, MS, PHN Concordia Language VillagesBemidji, MN

September 2012
19
– Perspectives Worth Sharing –Children with Sensory Impairment:
Camps for “Athletes” of Experiential LearningEllen B. Buckner, DNS, RN, CNE, Traci C. Morrow MSN, APRN-BC, FNP, and Kim C. Norris, MSN, RN
Research Perspectives The 2011 ACN Award for Best Individual Research Study in a camp setting went to researchers Donna Goodwin, Lauren Lieberman, Keith Johnson and Jennifer Leo whose qualitative research identified themes reflecting the social meaning of the camp experiences for campers with visual impairment. In their work entitled, “Connecting through summer camp: Youth with visual impairments find a sense of community,” the authors engaged campers in focus groups and one-to-one conversations about their experiences of camp. Three major themes were connected, reaching out, and resisting/acquiescing. The researchers chose the phenomenological method for their stated reason of eliciting “the kind of listening, seeing and responding, necessary to understand the reality of the young people.” The setting was a sports camp and campers were called “athletes” with identified moderate to total blindness. Athletes participated in adaptive physical activity during a one-week camp. Open ended questions elicited responses to: “What is it like to be with others who have visual impairment?” and “What did you learn about yourself and others at camp?” Some limitation in responses occurred due to fatigue in campers. Data were recorded and transcribed with analysis reflecting consensus of researchers and data checking in the subsequent year with available participants. Results indicated three major themes essential to overcoming social stigma and the physical void of home life.Connected: Campers stated they shared an emotional connection as they bonded with others who shared their impairment. Older athletes supported younger athletes, in whom they saw their own journey. They reported a sense of belonging to a community.
Abstract: The perspectives of camp researchers, director and nurse are blended in this description of camps for youth with sensory impairment. Award-winning qualitative research by Goodwin, Lieberman, Johnson & Leo, Adapted Physical Activity Quarterly, 28, 40-55, revealed themes of connected, reaching out and resisting/acquiescing. Examples of adaptive activities, in camps for children with visual and hearing impairment, show mechanisms of inclusion and overcoming social isolation. Stories of meaning emerge from director, from camper and from camp nurse which show the profound effects such experiences create in lives. Camper “athletes” were encouraged to stretch beyond social isolation in both physical and personal domains.
Finally campers reported that the camp environment “leveled the playing field” where no one would make fun of them or discriminate against them.Reaching out: The camp environment was viewed as a “landscape that made reaching out to explore one’s thoughts, imaginations, and physical limitations possible (p.47).” Campers stated experiences fulfilled the “need to be the author of my own identity.” Campers recognized the effects would be transferred to other contexts, revealing a depth of experience of transformation. Reciprocal relationships were formed between younger and older camper athletes, with support and interdependence as a result. Campers could perform beyond their own expectation, which unlocked new avenues of accomplishment.Resisting/Acquiescing: Athletes and coaches interacted in complex
ways. Coaches were instrumental in success and provided for safety; however, in some cases they were limiting and overprotective. In summary, athletes were able to exceed previous levels of participation and skills, discard stereotypes, seek their potential, and set new self-defined standards. The campers’ experience in the specialty camp provided a sense of community.
Strategies for Campers with Sensory Impairment So what mechanisms in camps facilitate this experience of acceptance and development of social meaning? The school hosts annual week-long summer camps for students who are ages 6 -16 years, blind or visually impaired and deaf or hearing impaired. The campers reside in the state of Alabama and can interact with other children who are blind or have vision loss. These may be their first experience with others with visual or hearing limitations. Discussions were held with Charlotte Lowry, MEd, Principal, Alabama School for the Blind, which hosts the summer camps as outreach for public school children with sensory impairment. Activities are held on site including connecting with the school-based resources such as a stuffed polar bear for tactile experiences, a fragrance garden, water activities and special equestrian or hippo therapy. The campers are there to test their personal limits and experience first-hand the school’s offerings.
The only thing worse than being blind is having sight but no vision.
~ Helen Keller

20
Volume 22, No. 3
The history of the camp spans 28 years when the school decided to offer visual or hearing impaired public school students the opportunity to have some of the experiences provided to Alabama school for the Blind’s students. A three-week summer program was started with activities of daily living (home economics),
orientation and mobility, art, music, drama, fun classes in science, computer and a full recreation program. Later the camp was shortened to one week to prevent campers from becoming too exhausted because they were not used to so many activities. The staff is comprised of teachers and teacher aides. Sometimes the most significant experiences are the most basic. Lowry described, “When we had the first camp, I was the home economics teacher. I had a totally blind boy who had never peeled a banana, and another student who had never felt uncooked bacon. This shows you how sheltered some students are and how limited their independent living skills.” Traci Morrow MSN, APRN-BC, FNP, Director of Nursing for Alabama Institute for Deaf and Blind (AIDB), described the types of adaptive experiences offered. These include football which uses a drumbeat to cue for play for the hearing impaired. Goalball uses a ball with a bell inside. Children with low vision cue with whistles. Children with deafness picked up beginning sign language. Seasoned “signers” could “talk” with others for extensive peer communication. Track activities were shared by both groups with coaches serving as guides or team members paired with opposing limitations to develop interdependence. Teamwork was an intentional emphasis of the camp and campers learned to work together to achieve the greatest distance for their run, throw, or roll. In some experiences, all campers were blindfolded to equalize teams, in other games, Easter eggs “beeped” to be found. A wide variety of activities complemented the natural and resource environment of the school and outdoors. Both Lowry and Morrow related camper’s descriptions of having the experience of “feeling normal” or “feeling accepted” sometimes for the first time in their lives. They bonded to each other and to the animals
who shared their world. A beloved dog, Daisy, allowed camp staff to brush her teeth, teaching campers the importance of brushing their own. In another example, staff recounted adolescents whose experience was so powerful they talked parents into letting them return for the school year. One said it was the first time he had felt he fit in. Another young girl who said in the regular class, “I don’t have a name…can’t sign…and have no voice” was encouraged through these adaptive experiences to reach her full potential.
Meaningful experiences for Nurse and Camper Morrow described an early experience with a camper who was totally blind. As part of a physical assessment, Nurse Traci was using her physical assessment tools. The camper wanted to touch the stethoscope. She wanted to hold the otoscope and “look in” Nurse Traci’s ears, too. Finally the child said, “I want to hear my heart” at which point the nurse placed the earpieces in her ears and placed the stethoscope on her chest. She listened. “What are you listening to?” asked Ms. Morrow, “It sounds like a miracle” the camper replied. “That’s why I am a nurse today,” stated Nurse Traci. In another meaningful moment, Nurse Traci described what vision is really about. One night, a camper with two prosthetic eyes was riding piggyback on Nurse Traci’s back, “Stop and look!” the camper called out. “What?” Nurse Traci asked. The camper said, “Look at the all the stars in the sky – aren’t they beautiful?” Perspectives of researchers, directors and nurses are made rich by the experiences of campers. Where are the stars in your world?
Resources Alabama Institute for the Deaf and Blind, www.aidb.org.
American Foundation for the Blind, www.afb.org.
International Council for Education of People with Visual Impairments, www.icevi.org.
Lighthouse International, www.lighthouse.org.
Lions Club International, www.lionsclub.org.
National Federation of the Blind, www.nfb.org.
Ellen Buckner and Kim Norris are faculty members at the College of Nursing, University of South Alabama. Ellen Buchner, DSN, RN, CNE is a member of the ACN Board of Directors and serves as ACN Research Chair in addition to her faculty responsibilities. Kim Norris, MSN, RN, is an instructor and coordinates nursing student experiences and nursing in summer camps at Camp Grace for campers with diabetes, rheumatoid arthritis, cerebral palsy, autism and cancer. Traci Morrow, MSN, APRN-BC, FNP has worked as Director of Nursing at the Alabama Institute for Deaf and Blind since 2003. She is responsible for the medical care of students ages 3-21 at the Alabama School for the Deaf, Alabama School for the Blind and The Helen Keller School of Alabama.
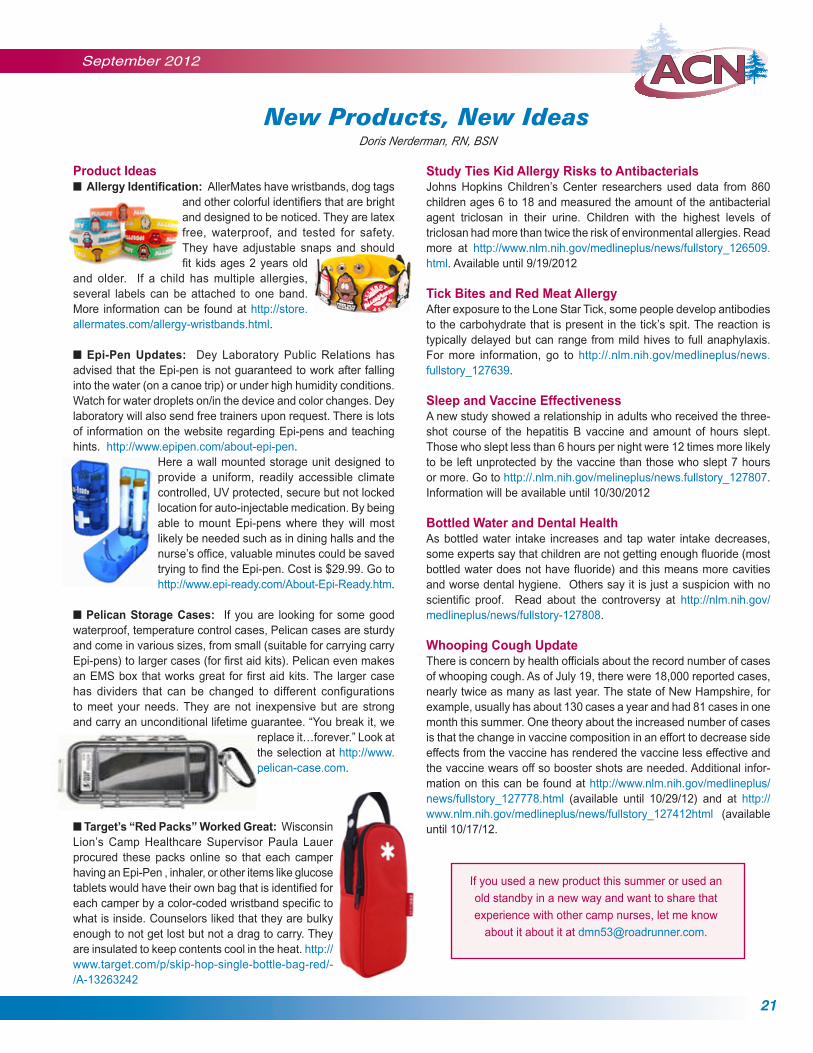
September 2012
21
Product Ideasn Allergy Identification: AllerMates have wristbands, dog tags
and other colorful identifiers that are bright and designed to be noticed. They are latex free, waterproof, and tested for safety. They have adjustable snaps and should fit kids ages 2 years old
and older. If a child has multiple allergies, several labels can be attached to one band. More information can be found at http://store.allermates.com/allergy-wristbands.html. n Epi-Pen Updates: Dey Laboratory Public Relations has advised that the Epi-pen is not guaranteed to work after falling into the water (on a canoe trip) or under high humidity conditions. Watch for water droplets on/in the device and color changes. Dey laboratory will also send free trainers upon request. There is lots of information on the website regarding Epi-pens and teaching hints. http://www.epipen.com/about-epi-pen.
Here a wall mounted storage unit designed to provide a uniform, readily accessible climate controlled, UV protected, secure but not locked location for auto-injectable medication. By being able to mount Epi-pens where they will most likely be needed such as in dining halls and the nurse’s office, valuable minutes could be saved trying to find the Epi-pen. Cost is $29.99. Go to http://www.epi-ready.com/About-Epi-Ready.htm.
n Pelican Storage Cases: If you are looking for some good waterproof, temperature control cases, Pelican cases are sturdy and come in various sizes, from small (suitable for carrying carry Epi-pens) to larger cases (for first aid kits). Pelican even makes an EMS box that works great for first aid kits. The larger case has dividers that can be changed to different configurations to meet your needs. They are not inexpensive but are strong and carry an unconditional lifetime guarantee. “You break it, we
replace it…forever.” Look at the selection at http://www.pelican-case.com.
New Products, New Ideas Doris Nerderman, RN, BSN
If you used a new product this summer or used an
old standby in a new way and want to share that
experience with other camp nurses, let me know
about it about it at [email protected].
Study Ties Kid Allergy Risks to AntibacterialsJohns Hopkins Children’s Center researchers used data from 860 children ages 6 to 18 and measured the amount of the antibacterial agent triclosan in their urine. Children with the highest levels of triclosan had more than twice the risk of environmental allergies. Read more at http://www.nlm.nih.gov/medlineplus/news/fullstory_126509.html. Available until 9/19/2012
Tick Bites and Red Meat Allergy After exposure to the Lone Star Tick, some people develop antibodies to the carbohydrate that is present in the tick’s spit. The reaction is typically delayed but can range from mild hives to full anaphylaxis. For more information, go to http://.nlm.nih.gov/medlineplus/news.fullstory_127639.
Sleep and Vaccine EffectivenessA new study showed a relationship in adults who received the three-shot course of the hepatitis B vaccine and amount of hours slept. Those who slept less than 6 hours per night were 12 times more likely to be left unprotected by the vaccine than those who slept 7 hours or more. Go to http://.nlm.nih.gov/melineplus/news.fullstory_127807. Information will be available until 10/30/2012
Bottled Water and Dental Health As bottled water intake increases and tap water intake decreases, some experts say that children are not getting enough fluoride (most bottled water does not have fluoride) and this means more cavities and worse dental hygiene. Others say it is just a suspicion with no scientific proof. Read about the controversy at http://nlm.nih.gov/medlineplus/news/fullstory-127808.
Whooping Cough UpdateThere is concern by health officials about the record number of cases of whooping cough. As of July 19, there were 18,000 reported cases, nearly twice as many as last year. The state of New Hampshire, for example, usually has about 130 cases a year and had 81 cases in one month this summer. One theory about the increased number of cases is that the change in vaccine composition in an effort to decrease side effects from the vaccine has rendered the vaccine less effective and the vaccine wears off so booster shots are needed. Additional infor-mation on this can be found at http://www.nlm.nih.gov/medlineplus/news/fullstory_127778.html (available until 10/29/12) and at http://www.nlm.nih.gov/medlineplus/news/fullstory_127412html (available until 10/17/12.n Target’s “Red Packs” Worked Great: Wisconsin
Lion’s Camp Healthcare Supervisor Paula Lauer procured these packs online so that each camper having an Epi-Pen , inhaler, or other items like glucose tablets would have their own bag that is identified for each camper by a color-coded wristband specific to what is inside. Counselors liked that they are bulky enough to not get lost but not a drag to carry. They are insulated to keep contents cool in the heat. http://www.target.com/p/skip-hop-single-bottle-bag-red/-/A-13263242
22
Volume 22, No. 3
ACN’s 2013 Camp Nurse Symposium
At the Hyatt Regency in Dallas, TX12-13 February
ACN’s Annual Meeting will be held Monday night, 11 February.Make travel plans so you arrive for the Annual Meeting too!
“Deep in the Camp Nursing Heart of Texas”
• Conference fees held steady for the third straight year! The Symposium is a great deal!
o Full Registration (Tuesday and Wednesday) is $250 for members and $350 for non-members. This includes contact hours, breaks, and Tuesday’s Camp Nurse Lunch.
o Registration for Tuesday only is $175 for members and $275 for non-members.
o ACN members attend Monday evening’s Annual Meeting at no charge.
• ACN is co-located with ACA’s national conference. This means that ACN members will enjoy Wednesday with other camp professionals.
• Google “Hyatt Regency Dallas at Reunion” to see where we’ll be and what hotel amenities are available.
Want to revitalize and update your camp nursing practice?
ACN’s Camp Nurse Symposium provides cutting edge sessions thatexplore aspects of camp health and nursing practice. Network with othercamp nurses, meet camp nurse leaders, shop at the Camp Nurse Store,
leave with an expanded knowledge base and so much more!Plan NOW to be in Dallas next February!
This activity has been submitted to WNA CEAP forapproval to award contact hours. Wisconsin Nurses
Association is accredited as an approver of continuingnursing education by the American Nurses
Credentialing Center’s Commission on Accreditation.
Want to Know More?Plans are in development but moving along quickly.
Additional information will be posted online atwww.ACN.org as it is ready.
Go there for the most up-to-date information!
“Deep in the Camp Nursing Heart of Texas” is Looking for Presenters More Alive than Dead and Willing to Lead our Posse of Knowledge Seekers
Hello Potential Symposium Speakers:
How about presenting at the next ACN Camp Nurse Symposium? Now is the time to consider this wonderful opportunity. Following ACN’s Annual Meeting on Monday evening, 11 February, the Symposium will be held in Dallas, TX, 12-13 February 2013.
Tuesday is our “just for camp nurses” day while Wednesday brings a partnership with the American Camping Association with joint educational sessions for nurses and other camp professionals.
As you consider presenting at the Symposium, please note the following:
1. Speakers are expected to register for the Symposium but pay $50 less than other participants.
All other costs associated with participation in the event are the expense of each individual.
2. ACN provides one year of membership following successful completion of your presentation at
the Symposium. You must be a current member of ACN to receive this benefit.
3. Speakers are encouraged to bring copies of his/her presen-tation (handouts) for distribution to Symposium participants.
If you are interested, please email the information below to [email protected]. In the subject heading of the email, please type “ACN Potential Speaker”.
Presentation Proposals for the Symposium
“Deep in the Camp Nursing Heart of Texas” is Looking for Presenters More Alive than Dead and Willing to Lead our Posse of Knowledge
Seekers Hello Potential Symposium Speakers: How about presenting at the next ACN Camp Nurse Symposium? Now is the time to consider this wonderful opportunity. Following ACN’s Annual Meeting on Monday evening, 11 February, the Symposium will be held in Dallas, TX, 12-13 February 2013. Tuesday is our “just for camp nurses” day while Wednesday brings a partnership with the American Camping Association with joint educational sessions for nurses and other camp professionals. As you consider presenting at the Symposium, please note the following:
1. Speakers are expected to register for the Symposium but pay $50 less than other participants. All other costs associated with participation in the event are the expense of each individual.
2. ACN provides one year of membership following successful completion of your presentation at the Symposium. You must be a current member of ACN to receive this benefit.
3. Speakers are encouraged to bring copies of his/her presentation (handouts) for distribution to Symposium participants.
If you are interested, please email the information below to [email protected]. In the subject heading of the email, please type “ACN Potential Speaker”.
Name Phone Number Second Phone Number Email address Topic Interested in Presenting
Once I receive this initial information, you will receive a speaker packet from me via email. ACN’s Education Committee, the group responsible for planning Symposium content, asks that you complete and return the speaker packet by October 15, 2012. Additional instructions are in the speaker packet. Incomplete or late speaker packets may not be considered for presentation at the Symposium. Thank you for your commitment to camp nursing. Through events such as the Symposium, we continue to raise awareness of the vital role camp nurses play in the pediatric healthcare of our nation as well as increase the body of knowledge that undergirds our profession. I look forward to hearing from you! Sincerely, Tracey Gaslin RN, PhD, CRNI, CPNP Chair, Education Committee Association of Camp Nurses
• Name
• Phone Number
• Second Phone Number
• Email address
• Topic Interested in Presenting
Once I receive this initial information, you will receive a speaker packet from me via email. ACN’s Education Committee, the group responsible for planning Symposium content, asks that you complete and return the speaker packet by October 15, 2012. Additional instructions are in the speaker packet. Incomplete or late speaker packets may not be considered for presentation at the Symposium.
Thank you for your commitment to camp nursing. Through events such as the Symposium, we continue to raise awareness of the vital role camp nurses play in the pediatric healthcare of our nation as well as increase the body of knowledge that undergirds our profession. I look forward to hearing from you!
Sincerely,Tracey Gaslin RN, PhD, CRNI, CPNPChair, Education CommitteeAssociation of Camp Nurses

September 2012
23
v Board Election Complete; Board Advance Scheduled for October It’s official – ACN’s new Board takes office on 1 January 2013. The in-coming Board includes current members Cheryl Bernknopf, Tracey Gaslin, and Lisa South. They will be joined by these newly elected people: Lisa Cranwell-Bruce, Paula Lauer, Tom Meyer, Mary Rogers and Jeana Wilcox. Both the current and in-coming Board will meet during the Board Advance, an event scheduled for 12-14 October in Minneapolis, MN. The Advance kicks-off at noon on the 12th when in-coming Board members go through an orientation to their role with current president VJ Gibbins and Linda Erceg, Executive Director. By supper, the current Board joins the new Board to launch the Board Advance, a strategic planning session that, given ACN’s history as well as current opportunities, plans the future. On Sunday morning, the new Board will also elect ACN’s next president and make Board assignments to various committees. ACN members can rely on December’s CompassPoint to carry a summary article about the Advance and the plan for ACN’s next three to five years. Many thanks to the member who returned their ballots; your support means a lot!
v CompassPoint’s Feature Editors are Shaking Things Up! CompassPoint readers have enjoyed Mary Marugg’s timely and common sense content in her feature, Keeper of the Kits, for several years. Originally developed to address concerns about first aid products and practices at camp, Mary expanded those horizons over time to keep readers current on many facets of camp health and safety. Each column reflects her experience providing practical ideas for both novice and experienced camp nurses. And now, sadly but understandably, Mary has decided that it is time to pass this responsibility on to someone else. Mary’s contributions are deeply appreciated and, happily, she will continue as a member of CompassPoint’s Editorial Board. CP’s Editorial Board members were asked if there was an “heir apparent” within the group to take on Mary’s feature and Doris Nerderman answered the call. Doris is a camp nurse with twenty-seven years experience and she certainly knows well the challenges and trends within Health Centers. After many years of responsibility for the New Products, New Ideas feature, she is eager for the change. Doris will probably change the feature’s name but the focus will remain current and practical approaches to practice issues that arise in the Health Center. Look for Doris’s first new feature in the December issue. Who will take on the responsibility for New Products, New Ideas? A new feature editor is being sought to continue this valued feature. This volunteer editor will prepare four columns a year or two editors can share this feature. This column is best done by an “information seeker” who likes perusing the internet and tapping into a variety of information sources. Doris is very willing to help the new editor identify helpful sources to get started. The person(s) who take on this feature will also join CompassPoint’s Editorial Board. Contact Editor Susan Baird for further information at [email protected] or 508-888-3249.
v CompassPoint Readies Manuscript Peer Review Process CompassPoint is moving toward being a peer-reviewed publication thanks to the valued work of the Peer Review Process Task Force and the recruitment of members to serve as peer reviewers. Peer review is a “Good Housekeeping Seal of Approval” type of process used by
Association Newsnumerous publications in all fields. Regardless of the process, it really means that other people have reviewed the manuscript prior to its publication for timeliness, accuracy, etc. and have given their opinion on whether or not to publish the paper. Peer Review status has been a long-term goal of CompassPoint and is probably of most interest to our members and readers who are associated with academia as faculty are strongly encouraged to publish and to do so in peer-reviewed publications. This is also true of some clinical settings, often those closely attached with academic institutions. It is hoped that being peer reviewed may encourage authorship. Members of the Peer Review Process Task Force have worked to develop the structure, process, and forms to facilitate peer review. Member volunteers on this Task Force are: Susan B. Baird, RN, MPH, MA, Chair; Ellen Buckner, RN, DNS, Lisa Cranwell-Bruce, MS RN, FNPC, APRN; Tracy Gaslin, RN, PhD, CRNI, CPNP; Doris Nerderman, RN, BSN; Lisa South, RN, DSN; and Jeana Wilcox, PhD, RN, CNS CNE. This group brings a lot of experience with the Peer Review Process to the tasks at hand and is to be congratulated on its achievements. When its tasks are completed, the information will be available on line at ACN’s website and sent to prospective authors on request. Reviewers are now being sought to facilitate implementation of the peer review process. ACN members interested in volunteering to review authored papers are encouraged to respond to the “Call for Reviewers” on page 24 of this issue. This is a great way to be involved in your Association and share your expertise.
v Association Assessment Coming Your Way – Soon! This is Your Opportunity to Influence ACN’s Future Every three years or so, ACN conducts an organizational assessment. One portion of the assessment is informed (completed) by members and another is contributed by stakeholders, those individuals with an interest in ACN’s mission. Information from both groups contributes to the Board’s strategic planning process. ACN will use email to provide members with electronic, online access to this year’s assessment tool. The information will arrive in late August to the email address each member has on file with ACN’s office and be followed by periodic reminders so everyone has opportunity to contribute by the end of September. Be looking for this – and if you’ve changed your email address, get the update to ACN’s office NOW ([email protected]). Thank you!
v CompassPoint Seeks Editorial Board Members Are you interested in becoming more active in ACN? Do you enjoy receiving CompassPoint and want to have a more active voice in its continuing development? Perhaps becoming an Editorial Board member is in your future! We are seeking a few new members to join the team that helps provide oversight. Volunteers assist the editor in setting policies, providing direction, and generating ideas as well as identifying potential topics and authors. A few take responsibility for regular features and each member is encouraged to write occasional content. Experience in camp nursing is needed but previous publishing experience is not. If interested in learning more about this role, contact Editor Susan Baird at [email protected] or 508-888-3249.

24
Volume 22, No. 3
Association of Camp Nurses8630 Thorsonveien NEBemidji, Minnesota 56601
PRSRT1ST CLASS MAIL
U.S. POSTAGE PAIDBEMIDJI, MN
PERMIT NO. 19
ACN’s CompassPointSeeks Peer Reviewers
A Peer Review Process is being implemented to facilitate publication decisions. The Peer Review Team will be comprised of members volunteering for a two-year renewable term. Reviewers will read draft manuscripts submitted for publication consideration and make recommendations about manuscript acceptance. The team will collectively need expertise in all aspects of camp nursing so we are interested in the variety of experience that individual members can contribute. And, we want all levels of academic preparation represented.
This activity is a great way to be involved in ACN from home when a larger committee commitment may not be workable. Serving as a reviewer for a national publication is a great “resume builder” and it’s fun to see a variety of topics and writing styles! It is anticipated each reviewer will be asked to review 2-6 manuscripts a year depending on the reviewer’s areas of interest and expertise. A two-week turnaround time will be requested and all communication will be via e-mail. A blind-review process will be used in which reviewers do not know the author’s identity and authors do not know the reviewer’s identity.
Previous review experience is not needed. Volunteers new to the review process will be given assistance in getting started. Camp nursing experience is the best preparation for this process.
Interested?Contact CompassPoint Editor Susan Baird at [email protected] or 508-888-3249.
AnnouncingACN’s Annual Meeting
Monday Evening, 11 February 2013.ACN’s 2013 Camp Nurse Symposium
Tuesday - Wednesday12-13 February 2013
Both events will take place at the Hyatt Regency Dallas at Reunion, Dallas, TX.
Mark your calendars now! See the pre-conference information
in this issue of CompassPoint.
FREE ACA Membership for You JOIN NOW!
www.ACAcamps.org/membership/free
Coupon is good for one-year free membership. Coupon is good only for individuals who are not existing or previous ACA members. Coupon must be redeemed by the individual signing up online at www.ACAcamps.org/memebrship/free and using this coupon code ACN-2012 at checkout. Coupons allows individual to join in whatever membership category best fits. Individual must provide a unique e-mail address when signing up (as opposed to the camp’s email). Membership is not transferrable to another person once individual signs up. Once each individual signs up and com-pletes the basic membership form online, he or she will receive another coupon for a free e-Institute course. This offer is valid through October 2012.