association of sporadic listeriosis with consumption of uncooked hot dogs and undercooked chicken
TRANSCRIPT

779
Public Health
ASSOCIATION OF SPORADIC LISTERIOSISWITH CONSUMPTION OF UNCOOKED HOTDOGS AND UNDERCOOKED CHICKEN
BENJAMIN SCHWARTZ1CLAIRE V. BROOME1GERI R. BROWN1
ALLEN W. HIGHTOWER2
CAROL A. CIESIELSKI1SUZANNE GAVENTA1BRUCE G. GELLIN1LAURENE MASCOLA3
AND THE LISTERIOSIS STUDY GROUP*
Meningitis and Special Pathogens Branch1 and Statistical ServicesActivity,2 Division of Bacterial Diseases, Center for Infectious
Diseases, Centers for Disease Control, Atlanta, Georgia, USA; andAcute Communicable Disease Control, Los Angeles Department of
Public Health, Los Angeles, California, USA.
Summary In 1986-87 the Centers for Disease Controlconducted an active population-based
survey of Listeria monocytogenes infections in six regions ofthe United States. Listeriosis was reported in 154 patients:one-third of cases were perinatal and the remainingtwo-thirds occurred in the elderly and immunosuppressed.28% of cases were fatal. 82 cases and 239 controls matchedfor age and underlying disease were enrolled in a study ofrisk factors for listeriosis. Cases were significantly morelikely than controls to have eaten uncooked hot dogs orundercooked chicken, with 20% of the overall risk oflisteriosis attributable to consumption of these foods. Noother risk factors were identified.
INTRODUCTION
FOOD-BORNE transmission of Listeria monocytogenesinfections has been recognised since 1981.1 Outbreaks oflisteriosis have been associated with coleslaw made fromcontaminated cabbage,1 whole and 2% milk,2 Mexican stylecheese and soft cheese in Switzerland.4 Eating shellfishmay have been linked to disease or carriage in a cluster ofcases in New Zealand,5 and consumption of raw vegetableswas linked indirectly to a cluster of cases in Boston 6Most cases of listeriosis, however, do not occur as part of a
recognised outbreak. Although individual cases have beenattributed to eating soft cheese7 and drinking raw milk,8 nocontrolled study of risk factors for sporadic listeriosis hasbeen reported.
Culture surveys of a wide range of food items have yieldedisolates of L monocytogenes from vegetables, dairy products,meat, poultry, and shellfish (refs 9-11 and personalcommunication, D. Archer, US Food and DrugAdministration). Because of the number of food productsthat may harbour L monocytogenes and the difficulty withwhich this organism is eliminated from the food chain it is
*Members of the Listeriosis Study Group: Sandra L. Sitze and MargaretSpurrier (Missouri Department of Health); Ellen Chahanovich, Gregory R.Istre, Sue Makintubee, and Jan White (Oklahoma State Department ofHealth); Robert C. McCready, David R. Cundiff, and Maureen C. Farrell(New Jersey Department of Health); Janice D. Harwell (Washington StateDepartment of Social and Health Services); Lori Chronis, Betty Grimes,Carolyn C. Hoppe, and Stephen H. Waterman (Los Angeles CountyDepartment of Health Services); Brenda K. Boner, Rose A. Kelley, Lewis B.Lelkowitz, Jr., and Jo A. Taylor (Department of Preventive Medicine,Vanderbilt University School of Medicine, Nashville, Tennessee); andWilliam F. Bibb, Arthur L. Reingold, and Robert E. Weaver (CDC).
important to establish whether sporadic listeriosis may beassociated with consumption of contaminated food andwhich types of products might be vehicles for humaninfection. In this paper, we describe a population-basedcase-control study of risk factors for sporadic listeriosis in sixregions of the United States conducted during 1986 and1987.
METHODS
Surveillance
In 1986, active surveillance for L monocytogenes and several otherbacterial pathogens was established in Missouri, New Jersey,Oklahoma, Tennessee, Washington, and Los Angeles County,California. Surveillance for listeriosis was continued to the end of
June, 1987, in all study areas except New Jersey, where surveillanceended in December, 1986. The total population in the areassurveyed was approximately 34 million, with substantial
geographic, racial, and ethnic diversity.From October to December, 1985, inclusive, doctors in the
surveillance areas were informed of the project through letters,bulletins in medical journals and newsletters, and presentations.From January, 1986, surveillance coordinators in each area
telephoned designated hospital or Health Maintenance
Organisation (HMO) contacts every 2 weeks to obtain reports of allpatients with sterile-site cultures positive for the specifiedpathogens. Information obtained for each’ case included the
patients’s age, race, sex, dates of admission and positive culture,clinical diagnosis, the site from which the organism was isolated,and the outcome of illness.To assess the sensitivity of active surveillance and to obtain
reports on cases not detected by the above mechanism, we reviewedInternational Classification of Diseases (ICD-9) dischargediagnosis codes for L monocytogenes for most hospitals in thesurveillance areas. A comparison of the number of cases thusobtained with the number reported by both ICD code andsurveillance yielded a sensitivity for surveillance of 93%.
Case-control StudyAll patients with sterile-site cultures positive for L monocytogenes
between September, 1986, and July, 1987, were eligible for thestudy. Their doctors were asked for permission to include thepatients in the study and to choose systematically from their recordsof patient visits 4 controls matched for age (± 10 years) andunderlying disease. If a case had more than one underlyingcondition, controls were matched for the illness most likely to beimmunosuppressive. For perinatal cases, the mothers were
interviewed irrespective of their own culture status, the doctorcontacted was the obstetrician, and controls (4 per patient) werematched for approximate date of conception in addition to age andillness. If a doctor was unable to provide names of controls, thehospital infection control practitioner selected matched controlsfrom recent hospital admissions.
Potential study participants were informed by telephone of thepurpose of the study and their consent was obtained. If a case orcontrol had died or could not be interviewed, an attempt was madeto obtain information from a surrogate, most often the spouse. Asecond CDC interviewer, unaware of the patient’s case or controlstatus, contacted all participants again except cases from LosAngeles (LA) county, and administered a questionnaire regardingpotential risk factors for listeriosis. Cases in LA county wereinterviewed in person by public health nurses. Patients were notenrolled if investigators were unable to contact them or an
appropriate surrogate, or were unable to identify or interviewcontrols.The interview, which lasted approximately 30 min, included
questions on demographic characteristics, underlying disease,medication, exposure to ill individuals, animals, and excavationworks, and diet history for the month preceding the date of thepositive culture (reference period). The diet history included fooditems that had been implicated in previous investigations of
780
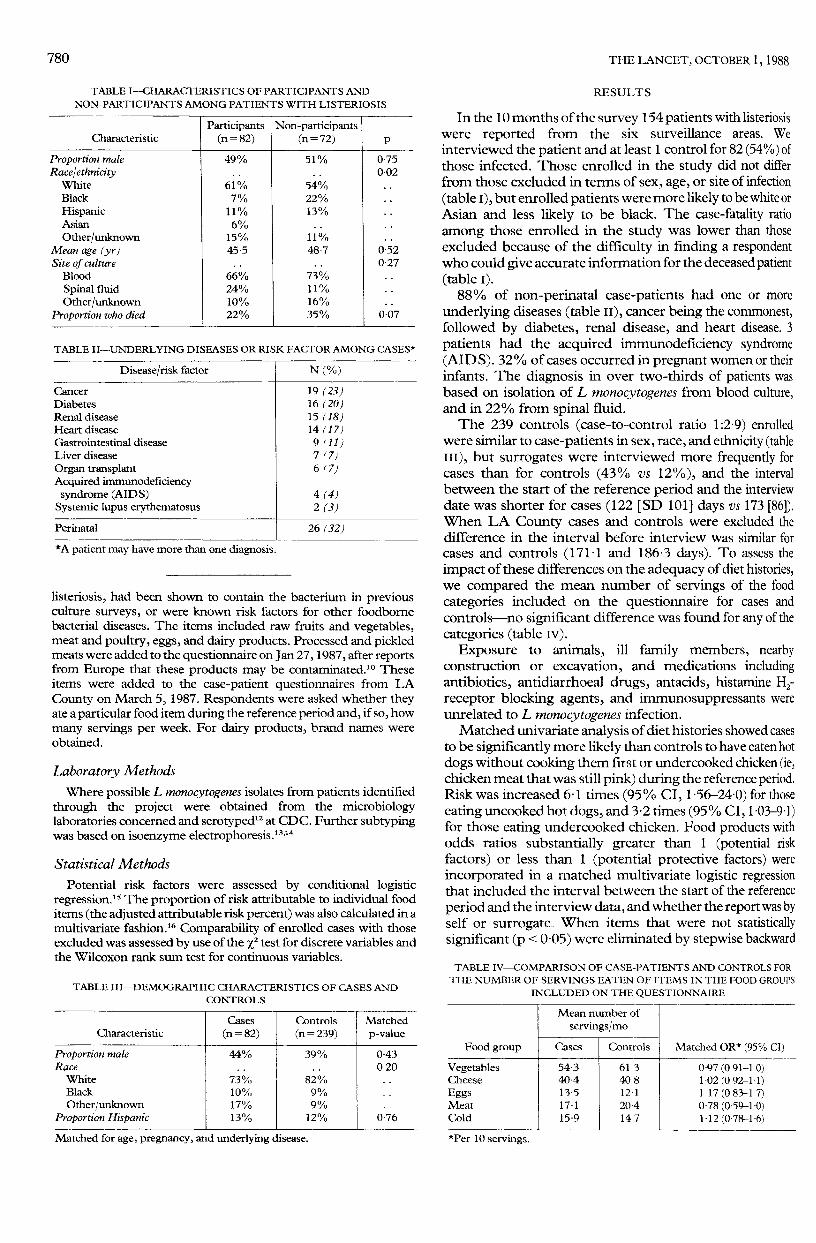
TABLE I-CHARACTERISTICS OF PARTICIPANTS AND
NON-PARTICIPANTS AMONG PATIENTS WITH LISTERIOSIS
TABLE II-UNDERLYING DISEASES OR RISK FACTOR AMONG CASES*
*A patient may have more than one diagnosis.
listeriosis, had been shown to contain the bacterium in previousculture surveys, or were known risk factors for other foodbornebacterial diseases. The items included raw fruits and vegetables,meat and poultry, eggs, and dairy products. Processed and pickledmeats were added to the questionnaire on Jan 27,1987, after reportsfrom Europe that these products may be contaminated Theseitems were added to the case-patient questionnaires from LACounty on March 5, 1987. Respondents were asked whether theyate a particular food item during the reference period and, if so, howmany servings per week. For dairy products, brand names wereobtained.
Laboratory MethodsWhere possible L monocytogenes isolates from patients identified
through the project were obtained from the microbiologylaboratories concerned and serotyped12 at CDC. Further subtypingwas based on isoenzyme electrophoresis.13.14
Statistical Methods
Potential risk factors were assessed by conditional logisticregression.1s The proportion of risk attributable to individual fooditems (the adjusted attributable risk percent) was also calculated in amultivariate fashion.16 Comparability of enrolled cases with thoseexcluded was assessed by use of the X2 test for discrete variables andthe Wilcoxon rank sum test for continuous variables.
TABLE III-DEMOGRAPHIC CHARACTERISTICS OF CASES AND
CONTROLS
Matched for age, pregnancy, and underlying disease.
.It..&..&..L..< ..........,"’.&..J..’" ’-’.L..< a , ’..F’-."’" a ’-".J.J.&.....L’ u, .1. JVU
RESULTS
In the 10 months of the survey 154 patients with listeriosiswere reported from the six surveillance areas. Weinterviewed the patient and at least 1 control for 82 (54%) ofthose infected. Those enrolled in the study did not differfrom those excluded in terms of sex, age, or site of infection
(table l), but enrolled patients were more likely to be white orAsian and less likely to be black. The case-fatality ratioamong those enrolled in the study was lower than thoseexcluded because of the difficulty in finding a respondentwho could give accurate information for the deceased patient(table I).88% of non-perinatal case-patients had one or more
underlying diseases (table 11), cancer being the commonest,followed by diabetes, renal disease, and heart disease. 3patients had the acquired immunodeficiency syndrome(AIDS). 32% of cases occurred in pregnant women or theirinfants. The diagnosis in over two-thirds of patients wasbased on isolation of L monocytogenes from blood culture,and in 22% from spinal fluid.The 239 controls (case-to-control ratio 1:2-9) enrolled
were similar to case-patients in sex, race, and ethnicity (tableill), but surrogates were interviewed more frequently forcases than for controls (43% vs 12%), and the intervalbetween the start of the reference period and the interviewdate was shorter for cases (122 [SD 101] days vs 173 [86]).When LA County cases and controls were excluded thedifference in the interval before interview was similar forcases and controls (171-1 and 186.3 days). To assess theimpact of these differences on the adequacy of diet histories,we compared the mean number of servings of the foodcategories included on the questionnaire for cases and
controls-no significant difference was found for any of thecategories (table IV).
Exposure to animals, ill family members, nearbyconstruction or excavation, and medications includingantibiotics, antidiarrhoeal drugs, antacids, histamine H2-receptor blocking agents, and immunosuppressants wereunrelated to L monocytogenes infection.Matched univariate analysis of diet histories showed cases
to be significantly more likely than controls to have eaten hotdogs without cooking them first or undercooked chicken (ie,chicken meat that was still pink) during the reference period.Risk was increased 6-1 times (95% CI, 1 -56-24-0) for thoseeating uncooked hot dogs, and 3-2 times (95% CI, 1.03-9.1)for those eating undercooked chicken. Food products withodds ratios substantially greater than 1 (potential risk
factors) or less than 1 (potential protective factors) wereincorporated in a matched multivariate logistic regressionthat included the interval between the start of the reference
period and the interview data, and whether the report was byself or surrogate. When items that were not statisticallysignificant (p < 0-05) were eliminated by stepwise backward
TABLE IV-COMPARISON OF CASE-PATIENTS AND CONTROLS FOR
THE NUMBER OF SERVINGS EATEN OF ITEMS IN THE FOOD GROUPS
INCLUDED ON THE QUESTIONNAIRE

781
TABLE V-RISK FACTORS FOR LISTERIA MONOCYTOGENESINFECTION
xCalculated by conditional logistic regression.’sVariables mcluded in the initial model (multivariate OR) and eliminated stepwise: wholemik (2-1), beef(O-48), sour cream (0-56), carrots (0 78), cole slaw (0 56), apples (0 87), raweggs (0-47).
elimination only uncooked hot dogs and undercookedchicken remained as risk factors, with odds ratios of 12 3 and20 5, respectively (table v). No foods had a significantprotective effect. The portion of risk in the study groupattributed to eating uncooked hot dogs or undercookedchicken (the multivariate adjusted attributable risk percent)was 15% and 6%. Since one case ate both foods theestimated total risk attributable to either food was 20%.
Cases who ate foods associated with an increased risk oflisteriosis did not cluster by date or geographic area, nor didthey consume more servings of these products than didcontrols. Isolates from cases who ate uncooked hot dogs orundercooked chicken included strains representing severalserotypes and isoenzyme types.Two possible listeriosis clusters were identified in the
study population. In LA County 6 of 33 cases and 4 of 101controls reported eating raw eggs (OR =6’4, 95% CI1 6-26-1). Listeriosis associated with ingestion of raw eggsoccurred between Nov 17, 1986, and March 30,1987. Of 3available isolates 2 were serotype 4b and 1 was 1/2b. Asecond potential cluster consisted of 5 infections in Hispanicpatients in LA County occurring between Feb 21,1987, andApril 24, 1987, with isolates of an identical strain (enzymetype 3). 4 of the 5 patients were enrolled in the case-controlstudy. The only common food items reported in all 4 caseswere lettuce, chicken, and whole milk. These foods were alsoeaten frequently by their matched controls, at similar rates ofconsumption.
DISCUSSION
Our controlled study has identified consumption ofcertain foods as risk factors for sporadic listeriosis. Althoughcase-reports have previously linked foods with individualcases of listeriosis, a controlled study is necessary to assessthe magnitude of the risk and the proportion of casespotentially attributable to an exposure. Since the ability ofcase-control studies to identify a risk factor is limited foreither very common or very rare exposures, or for risks thatare not large, it is important to emphasise that the lack of anassociation does not mean that a particular food is associatedwith no risk of listeriosis. Additionally, since epi-demiological associations do not establish causality it is
important to evaluate the validity and the plausibility of theassociations found in this study.
Biases that could potentially have affected our results lieprimarily in the completeness of surveillance and
representativeness of cases included in the study, and thecomparability and accuracy of diet histories of cases andcontrols. Completeness of surveillance assessed bydischarge diagnosis code review was 93%. Although nearlyhalf of the cases identified were not enrolled in the study,those excluded were similar to those enrolled except for race.Since case-control sets included in the study were highlyconcordant for race and ethnicity, dietary preferences
associated with these factors would not affect the matched
analysis or the risk estimates for individual food items.Additionally, comparability of cases and controls wasachieved by matching the two groups for age and underlyingdisease, and by using controls from the same practice toprovide an approximate match for neighbourhood andsocioeconomic status.
Although surrogates were interviewed more frequentlyfor cases than for controls, and the interval between thereference period and interview was greater for controls,neither of these factors seems to have had a significantimpact on the adequacy of diet history, measured by thesimilar frequency of consumption of the various food groupsby case-patients and controls. The reliability of
retrospective food frequency questionnaires and the
accuracy of surrogate reported data have also been
documented.17-22 Finally our multivariate results took intoaccount possible effects of surrogate reporting and intervalbetween illness and interview.
Because interviews were conducted differently in LACounty risk factors were also assessed without data from thiscounty. Their exclusion increased the width of theconfidence intervals and precluded multivariate riskestimates because of the reduction in sample size. Theunivariate odds ratios were 16.5 for consumption ofuncooked hot dogs and 27 for undercooked chicken.The impact of two other potential problems with
retrospective diet histories are more difficult to assess. Casesmight recall more clearly what they had eaten before theirillness, using their disease as a reference point, whereascontrols do not have such a reference. Such a bias is more
likely to occur for illnesses that are recognised as foodborneand cause gastrointestinal symptoms than for listeriosis,which produces symptoms not referable to the
gastrointestinal tract. Conversely, cases with a serious illnessmay be less likely to remember events that occurred beforethe illness. Although the effect of these factors on theaccuracy of diet histories cannot be quantified, they are morelikely to result in random misclassification of exposuresrather than implication of one or more specific foods. Whensuch misclassifications occur, the effect of a potentialexposure is likely to be underestimated.23,24 The possibilitythat inverviewers, knowing what foods were more likely tocontain L monocytogenes, interviewed cases and controls
differently, was minimised by blinding interviewers to caseor control status and using a structured questionnairerequiring "yes-or-no" answers. Processed meats and
poultry were not distinguished from the other productsincluded on the questionnaire, many of which were knownto be potenially culture positive.
Both uncooked hot dogs and undercooked chicken areplausible as vehicles for listeriosis. In both the United Statesand Europe processed meats are often contaminated with Lmonocytogenes.9,10,5 An investigation of an outbreak inPhiladelphia found that salami-another processed meatproduct eaten without further cooking-was a risk factor forinfection (unpublished data, B. Schwartz). If L
monocytogenes is introduced into a processing facility bycontaminated meat it is difficult to eradicate because it cansurvive on environmental surfaces and grow at refrigeratortemperatures.25.26 A survey by the American Meat Instituteof 41 meat-processing plants found Listeria sp in more thanone-third of cultures from floors and drains, and in overone-fifth of cultures from cleaning aids, wash areas, sausagepeelers, and food contact surfaces.26 Since hot dogs arecooked during processing, re-inoculation from

782
contaminated surfaces is the most likely explanation forpositive cultures of the finished product.
In culture surveys of retail poultry L monocytogenes hasbeen isolated from 15 % to 80% of specimens depending onthe sampling method .25 Undercooked chicken has beenrecognised as a risk factor for outbreaks of Salmonella andCampylobacter infections;27,28 it has also been implicatedin a population-based study of sporadic Campylobacterinfection.29 This study suggests that contaminated chickenis also a vehicle for listeriosis if cooked insufficiently to killthe organism.
Since the estimate of risk attributable to uncooked hot
dogs and undercooked chicken was only 20% of the totalrisk of listeriosis, four-fifths of the risk of sporadic infectionremains to be explained. Because of non-differentialmisclassification the risk attributed to the implicated fooditems may be underestimated and, in conjunction with thesmall sample size, may have resulted in our not identifyingother foods associated with listeriosis. Additionally, a
portion of the unattributed risk may be due to products notincluded on the questionnaire-such as shellfish. A furtherpossibility is that not all sporadic listeriosis is foodborne,although our study did not identify any non-dietary riskfactors.Our results add to a growing body of evidence that
consumption of contaminated food is a risk factor forlisteriosis. Although our findings need to be replicated, theysuggest that undercooked poultry and uncooked hot dogsneed to be added to a list of foods associated withlisteriosis-a list that already includes vegetables and dairyproducts. These results suggest that listeriosis may occurwhen a contaminated product is improperly prepared andeaten by a susceptible host. Whether systemic infectionresults directly from the exposure, or carriage is establishedwith eventual dissemination, cannot be determined by theepidemiology alone. The association of both sporadic andepidemic listeriosis with food products emphasises the needfor industry and regulatory agencies to work together toelminate L monocytogenes from food products-especiallyready-to-eat foods. Consumers, especially pregnant womenand those who are immunosuppressed, should be aware ofthe risk of listeriosis and could decrease their risk bypreparing foods properly and avoiding uncooked foodproducts that have been implicated as risk factors forlisteriosis.
Correspondence should be addressed to B. S., Meningitis and SpecialPathogens Branch, Building 1, Room 5409, Centers for Disease Control,1600 Clifton Road, NE Atlanta, Georgia 30333, USA.
REFERENCES
1. Schlech WF, Lavigne PM, Portolussi R, et al Epidemic listenosis—Evidence fortransmission by food. N Engl J Med 1983; 308: 203-06
2. Fleming DW, Cochi S, MacDonald KL, et al. Pasteurized milk as a vehicle of infectionin an outbreak of listenosis. N Engl J Med 1985; 312: 404-07.
3 Linnan MJ, Mascola L, Xiao DL, et al. Epidemic listeriosis associated with
Mexican-style cheese. N Engl J Med (in press)4. Listeriosis in Switzerland. Bull l’Office Fed Sante Publ 1988; 3: 28-29.5. Lennon D, Lewis B, Mantell C, et al. Epidemic perinatal listeriosis. Pediatr Infect Dis
1984, 3: 30-346. Ho JL, Shands KN, Friedland G, Eckind P, Fraser DW. An outbreak of type 4b
Listeria monocytogenes infection involving patients from eight Boston hospitals.Arch Intern Med 1986, 146: 520-24.
7. Bannister BA Listeria monocytogenes meningitis associated with eating soft cheese
J Infect 1987, 15: 165-688 Potel J Aethiologie der Granulomatosis Infantiseptica Wiss Z Martin Luther Univ.
Halle-Wittenberg. 1953-54, 3: 341-64.9. Skovgaard N. Listeria. food of animal origin. In: Listeriosis: Joint WHO/ROI
Consultation on Prevention and Control Vetmed-Hefte 1987, 5: 110-2110 Gilbert RJ, Pini PN Listeriosis and foodbome transmission Lancet 1988, i: 472-73.11 Gledel J Epidemiology and significance of listeriosis in France In. Listeriosis Joint
WHO ROI Consultation on Prevention and Control. Vetmed-Hefte 1987; 5: 9-20.
12 Seeliger HPR, Hohne K Serotyping of Listeria monocytogenes and related species. InBergen T, Norris JR, eds. Methods in microbiology, vol 13. London: AcademicPress, 1979: 31-49.
13. Bibb WF, Kuffner TA, Weaver RE. Typing of Listeria monocytogenes by isoenzymeanalysis Abstracts of the Annual Meeting of the American Society for
Microbiology, 1986: 393.14. Selander RK, Caugant DA, Ochman H, et al. Methods of multilocus enzyme
electrophoresis for bacterial population genetics and systematics Appl EnvironMicrobiol 1986; 51: 873-84.
15. Breslow NE, Day NE. Statistical methods in cancer research, vol 1. The analysis ofcase-control studies. Lyon: International Agency for Research on Cancer, 1980:248-81.
16. Bruzzi P, Green SB, Byar DP, Brinton LA, Schairer C. Estimating the population-attributable risk for multiple risk factors using case-control data Am J Epidemiol1985; 122: 904-14.
17 Sampson L. Food frequency questionnaires as a research instrument. Clin Nutr 1985,4: 171-78.
18. Jam M, Howe GR, Johnson KC, Miller AB. Evaluation of a diet history questionnairefor epidemiologic studies. Am J Epidemiol 1980; 111: 212-19.
19 Rohan TE, Potter JD. Retrospective assessment of dietary intake. Am J Epidemiol1984; 120: 876-87.
20. Humble CG, Samet JM, Skipper BE. Comparison of self- and surrogate-reporteddietary information. Am J Epidemiol 1984; 119: 86-98.
21. Kolonel LN, Hirohata T, Nomura AMY. Adequacy of survey data collected fromsubstitute respondents. Am J Epidemiol 1977; 106: 476-84.
22. Marshall J, Priore R, Haughey B, Rzepka T, Graham S. Spouse-subject interviewsand the reliability of diet studies. Am J Epidemiol 1980; 112: 675-83.
23. Kleinbaum DG, Kupper LL, Morgenstem H Epidemiologic Research BelmontLifetime Learning Publications, 1982: 220-38
24. Copeland KT, Checkoway H, McMichael AJ, Holbrook RH Bias due to
misclassification in the estimation of relative risk. Am J Epidemiol 1977, 105:488-95
25. World Health Organization. Report of the informal working group on foodbornelisteriosis WHO/EHE/FOS/88.5, Geneva: WHO, 1988: 1-18.
26. Amencan Meat Institute. Microbial control during production of ready-to-eat meatproducts: Controlling the incidence of Listeria monocytogenes. Washington, DCAmerican Meat Institute, 1987: 1-13.
27. Horowitz MA, Gangarosa EJ. Foodbome disease outbreaks traced to poultry, UnitedStates, 1966-74. J Milk Food Technol 1976; 12: 859-63.
28. Deming MS, Tauxe RV, Blake PA, et al. Campylobacter enteritis at a universityTransmission from eating chicken and from cats. Am J Epidemiol 1987: 126:526-34.
29. Hams NV, Weiss NS, Nolan CM. The role of poultry and meats in the etiology ofCampylobacter jejum/coli enteritis. Am J Publ Hlth 1986; 76: 407-11.
Occasional Survey
VIRUCIDAL TREATMENT OF CLOTTINGFACTOR CONCENTRATES
P. M. MANNUCCI M. COLOMBO
A. Bianchi Bonomi Haemophilia and Thrombosis Centre andInstitute of Internal Medicine, University of Milan, Italy
HEPATITIS B virus (HBV), hepatitis non-A, non-B(NANB) virus, and the human immunodeficiency virus(HIV) are important causes of morbidity and mortality inhaemophilic patients, who can become infected aftertransfusion with clotting factor concentrates made fromlarge plasma pools. Manufacturers have tried to inactivatethe viruses in concentrates by several methods (table I). Thefirst method was to expose whole plasma to ultravioletirradiation and beta-propiolactone, a denaturing agent. Thismethod can be applied to concentrates of the stable factor IXbut not to concentrates of labile factor VIII. Manufacturersthen attempted to inactivate viruses without substantial lossof factor VIII activity by heating lyophilised concentrates(dry heating) or concentrates resuspended in the organicsolvent n-heptane. Factor VIII and factor IX concentrateshave also been heated in solution (pasteurisation) and themoist bulk product has been heated with hot vapour. Allmethods based on heating use temperatures between 60°Cand 80°C for 30-72 h. Another method has been developedin which the solvent tri-n-butyl-phosphate (TNBP) and