asthma mark a. brown, md arizona respiratory center [email protected] tucson pediatric...
TRANSCRIPT

Asthma
Mark A. Brown, MDMark A. Brown, MDArizona Respiratory CenterArizona Respiratory [email protected]@arc.arizona.edu
Tucson Pediatric Pulmonary Tucson Pediatric Pulmonary CenterCenter

Definition
• Intermittent lower-airway obstruction Intermittent lower-airway obstruction that is reversible either spontaneously that is reversible either spontaneously or as the result of treatmentor as the result of treatment
– Inflammation and edemaInflammation and edema
– Bronchial smooth-muscle spasmBronchial smooth-muscle spasm
– Mucous pluggingMucous plugging

Definitions
• Asthma exacerbation: symptoms Asthma exacerbation: symptoms that require a change in that require a change in medication from baselinemedication from baseline
• Status asthmaticus: increasingly Status asthmaticus: increasingly severe asthma that is not severe asthma that is not responsive to drugs that are responsive to drugs that are usually effectiveusually effective

Epidemiology
• 10% of children in the US: 5 million 10% of children in the US: 5 million children under the age of 18children under the age of 18
• Prevalence is increasingPrevalence is increasing
• Asthma morbidity and mortality is Asthma morbidity and mortality is increasingincreasing
• 50% have family history of asthma, 50% have family history of asthma, rhinitis, eczematous dermatitis, or rhinitis, eczematous dermatitis, or urticariaurticaria

Onset of Symptoms in Children With Asthma
McNicol and Williams. BMJ 1973;4:7-11; Wainwright et al. Med J Aust 1997;167:218-222.
30%
20% 30%
20%
1-2 years
>3 years
<1 year
2-3 years

Natural History of Childhood Asthma
Age (Years)
Wh
eezi
ng
Pre
vale
nce
Non-atopicwheezers
Transient earlywheezers
IgE-associatedwheeze/asthma
0 3 6 11
Martinez. J Allergy Clin Immunol 1999;104:S169-S174.

Asthma Prevalence in US Children
SOURCE: US EPA (NCHS, 2006-2010).

Asthma Ambulatory Visits
Akinbami LJ, et al. Pediatrics, 2009; 123:S131-S145Akinbami LJ, et al. Pediatrics, 2009; 123:S131-S145

Childhood Asthma Deaths
Akinbami LJ, et al. Pediatrics, 2009; 123:S131-S145Akinbami LJ, et al. Pediatrics, 2009; 123:S131-S145

Arizona vs. US Asthma Age-Adjusted Mortality Rate 1991-98
0
0.5
1
1.5
2
2.5
3
1993 1994 1995 1996 1997 1998
Arizona
United States
Dea
ths/
100,
000
popu
lati
onD
eath
s/10
0,00
0 po
pula
tion

Risk Factors• Previous attack with:Previous attack with:
• Severe unexpected or rapid Severe unexpected or rapid deteriorationdeterioration
• Respiratory Failure (ICU/Intubation)Respiratory Failure (ICU/Intubation)
• Seizure or loss of consciousnessSeizure or loss of consciousness
• Recent use of oral steroids or Recent use of oral steroids or decrease in ICSdecrease in ICS
• Frequent use of short acting Frequent use of short acting -agonist-agonist

Risk Factors
• Two or more hospitalizations in Two or more hospitalizations in the last yearthe last year
• Hospitalization or ED in the last Hospitalization or ED in the last monthmonth
• 3 or more ED visits in the last 3 or more ED visits in the last yearyear

Risk Factors
• PsychosocialPsychosocial
– Denial or failure to perceive severityDenial or failure to perceive severity
– DepressionDepression
– NonadherenceNonadherence
– Dysfunctional familyDysfunctional family
– Inner-city residentInner-city resident

Busse and Lemanske. N Engl J Med. 2001;344:350-62.
Inflammation in Mild Asthma
Subject Without Asthma Patient With Mild Asthma

CXR

Chetta et al. Chest. 1997;111:852-7.
*P<.001, healthy subjects vs patients with asthma.
Airway Remodeling
P<.01
*
Severe Moderate Mild Healthy(n=6) (n=14) (n=14) (n=8)
SubepithelialLayerThickness (µm)
30
20
10
0
P<.003

Rel
ativ
e R
isk
of
Rel
ativ
e R
isk
of
Hos
pit
aliz
atio
nH
osp
ital
izat
ion
88
77
66
55
44
33
22
11
00
Prescriptions per Person-YearPrescriptions per Person-Year
NoneNone 1-21-2 2-32-3 3-53-5 5-85-8 8+8+0-10-1
ßß22-agonists-agonists
TotalTotal
Age 0-17Age 0-17
TotalTotal
Age 0-17Age 0-17
Inhaled SteroidsInhaled Steroids
Frequent Use of B2 Agonists Increased Likelihood of Asthma-related Hospitalizations
Adapted from Donahue et al. Adapted from Donahue et al. JAMA.JAMA. 1997;277:887-891. 1997;277:887-891.

B cellB cell
IgEIgE
dendriticdendriticcellcell
ICAM-1/3ICAM-1/3
IL-1IL-1
CD4CD4
antigen presentationantigen presentation
IL-12IL-12
CD8CD8
mastmastcellcell
MCP-3MCP-3
IL-5IL-5
IL-6IL-6
NCFNCFMIP-1MIP-1
LTB-4LTB-4
SCFSCF
IL-3IL-3
IL-14IL-14
tryptasetryptase
GM-CSFGM-CSF
LTC-4LTC-4
RANTESRANTES
TNF-TNF-
IL-8IL-8
eotaxineotaxin
IL-13IL-13
LTE-4LTE-4
IFN-IFN-
PGDPGD22histaminehistamine
IL-1IL-1
PAFPAF
chemokineschemokines
LTD-4LTD-4
IL-4IL-4
neuroneneurone
neurokininsneurokinins myofibroblastmyofibroblast
GM-CSFGM-CSFC-kitC-kit
IL-6IL-6Th-2Th-2
SCFSCF
GM-CSFGM-CSF
IL-13IL-13
TNF-TNF-
IL-1IL-1
IgEIgEIL-10IL-10
IL-4IL-4
IL-3IL-3
IL-5IL-5
IL-6IL-6
Th-1Th-1TNF-TNF-
IL-2IL-2
IFN-IFN-
Th-0Th-0
GM-CSFGM-CSF
IL-2IL-2
IFN-IFN-
IL-4IL-4
basophilbasophil
histaminehistaminecytokinescytokines
LTC-4LTC-4
LTD-4LTD-4
LTE-4LTE-4
IL-13IL-13
IL-4IL-4
PGSPGS
IgEIgEGM-CSFGM-CSF PAFPAF
proteaseprotease
IL-6IL-6 IL-8IL-8
neutrophilneutrophil
TNF-TNF-TGF-TGF-11
PAFPAF
LTD-4LTD-4
TXATXA
22
IL-1IL-1
IL-6IL-6
MPOMPO
O speciesO speciesBIPBIP
IL-8IL-8
LTB-4LTB-4
LTC-4LTC-4
endothelial cellendothelial cell
adhesion moleculesadhesion molecules
GM-CSFGM-CSFICAM-1ICAM-1
IL-4IL-4
L-selectinL-selectinPGSPGS
TNF-TNF-
ET-2ET-2
ET-1ET-1
IL-1IL-1
G-CSFG-CSF IL-6IL-6
fibroblastfibroblast
TGF-TGF-
PDGFPDGF
GM-CSFGM-CSFIL-1IL-1
IL-6IL-6
MIP-1MIP-1 RANTESRANTESCOLLAGEN I, II, COLLAGEN I, II,
VV
IL-8IL-8
MCP-1MCP-1
PGEPGE22
collagenasecollagenaseICAM-1ICAM-1 IL-11IL-11
SCFSCF
VCAM-1VCAM-1
eosinophileosinophil
LTC-4LTC-4
MCP-3MCP-3
IL-4IL-4
IL-6IL-6
IL-10IL-10
LTD-4LTD-4
OO22
PDGF-BPDGF-B
ECPECP
IL-5IL-5
IL-8IL-8
HB-EGFHB-EGF
TGFTGF
GM-CSFGM-CSF
TXB-2TXB-2
RANTESRANTES
TNF-TNF-
IL-3IL-3
IL-1IL-1
EDPEDP
MBPMBP
15-HETE15-HETEIL-2IL-2
PAFPAF
0 species0 species
IFN-IFN-
IL-13IL-13
MIP-1MIP-1
CR-3CR-3EDNEDN
ICAM-1ICAM-1
MCP-2MCP-2
MCP-1MCP-1
macrophagemacrophage
IL-IL-
IL-5IL-5
MCP-3MCP-3
MIP-1MIP-1
iNOSiNOS
PAFPAF
IL-10IL-10
LTB-4LTB-4
EAFEAFIL-1IL-1
TNF-TNF-
IL-6IL-6
IL-1IL-1
eotaxineotaxin
PGEPGE22
IL-12IL-12IFN-IFN-
RANTESRANTES
IL-3IL-3
GM-CSFGM-CSF
0 species0 species
IL-8IL-8proteaseprotease
epithelial cellepithelial cell
MCP-1MCP-1
IL-5IL-5IL-3IL-3
15-LD15-LD
SLPISLPI
NEPNEP
COXCOX22
iNOSiNOS
15-LT515-LT5
PGFPGF22
PGEPGE22
IGF-IIGF-I
CGRPCGRP
FGFFGFIL-16IL-16
IL-8IL-8CPLACPLA22adhesion moleculesadhesion molecules
GRO-GRO-NONO
GM-CSFGM-CSF
MCP-2MCP-2
RANTESRANTES
IL-1IL-1
TNF-TNF-
IL-6IL-6
IL-11IL-11
ET-1ET-1
VIPVIP
9/13 HODE9/13 HODE
15-HETE15-HETE
eotaxineotaxinIL-17IL-17PDGFPDGF
IL-10IL-10MIP-1MIP-1
ICAM-1ICAM-1
RANTESRANTES
smoothsmoothmuscle cellmuscle cell
cytokinescytokines
eotaxineotaxin
GM-CSFGM-CSF
IL-8IL-8
MCP-1MCP-1PGEPGE22
MCP-2MCP-2
MCP-3MCP-3
Mediator releasemodified
monocytemonocyte
IL-5IL-5
MCP-3MCP-3
MIP-1MIP-1
NONO
IL-1IL-1
TNF-TNF-
eotaxineotaxin
PGEPGE22
IFN-IFN-
RANTESRANTES
IL-3IL-3 GM-CSFGM-CSF
0 species0 species
IL-2IL-2
TXATXA22
IL-4IL-4
IL-8IL-8
cytokinescytokinesIL-6IL-6 IL-10IL-10 IL-12IL-12
LTB-4LTB-4LTC-4LTC-4 ICAM-1ICAM-1
G-CSFG-CSF
IFN-IFN-
Effects of Corticosteroids on Inflammatory Cells

ICS May Prevent Death From Asthma
Suissa et al. N Engl J Med. 2000;343:332-6.
Rate Ratio for Death From Asthma
Number of Canisters of Inhaled Corticosteroids Used in the Year Before Death From Asthma
0.0
0.5
1.0
1.5
2.0
2.5
2 4 6 8 10 12

Effects of Inhaled Corticosteroidson Inflammation
Pre- and post- 3 month treatment with budesonidePre- and post- 3 month treatment with budesonide(BUD) 600 mcg BID; E = epithelium, BM = basement membrane(BUD) 600 mcg BID; E = epithelium, BM = basement membrane
Laitinen.Laitinen. J Allergy Clin Immunol. J Allergy Clin Immunol.1992;90:32-42. 1992;90:32-42.

Budesonide Nedocromil Placebo
Childhood Asthma Management Program Research Group. N Engl J Med. 2000;343:1054-63.
No./100 Person-Year
Greater reductions in the need for emergency care
Health Resource Utilization
0
10
20
30
2.54.44.3
Hospitalizations
P=.0412
16
22
Urgent Care Visits
P<.001
P=.02

CAMP = Childhood Asthma Management Program.
Childhood Asthma Management Program Research Group. N Engl J Med. 2000;343:1054-63.
CAMP: ICS Reduced Oral Prednisone Use
First Course of Prednisone
Budesonide
Nedocromil
Placebo
0 1 2 3 4Time (y)
1.00
0.75
0.50
0.25
0.00
P<.001 budesonide vs placeboP=.32 nedocromil vs placebo
Cumulative Probability

Childhood Asthma Management Program Research Group. N Engl J Med. 2000;343:1054-63.
0
25
50
75
100
125
Prednisone Courses
No./100 Person-Year
P<.001P=.01
122
102
70
Budesonide Nedocromil Placebo
Prednisone Use

Corticosteroid Dose Response Curves for Various Outcomes
Symptoms (reduction)FEV1 (increase)Exercise (FEV1) (increase)Nitric oxide (reduction)FEF25-75% (increase)
100
80
60
40
20
0 600200 400 800Daily Dose of Budesonide (g)
% of Maximum
Barnes et al. Am J Respir Crit Care Med. 1998;157:S1-S53.
0
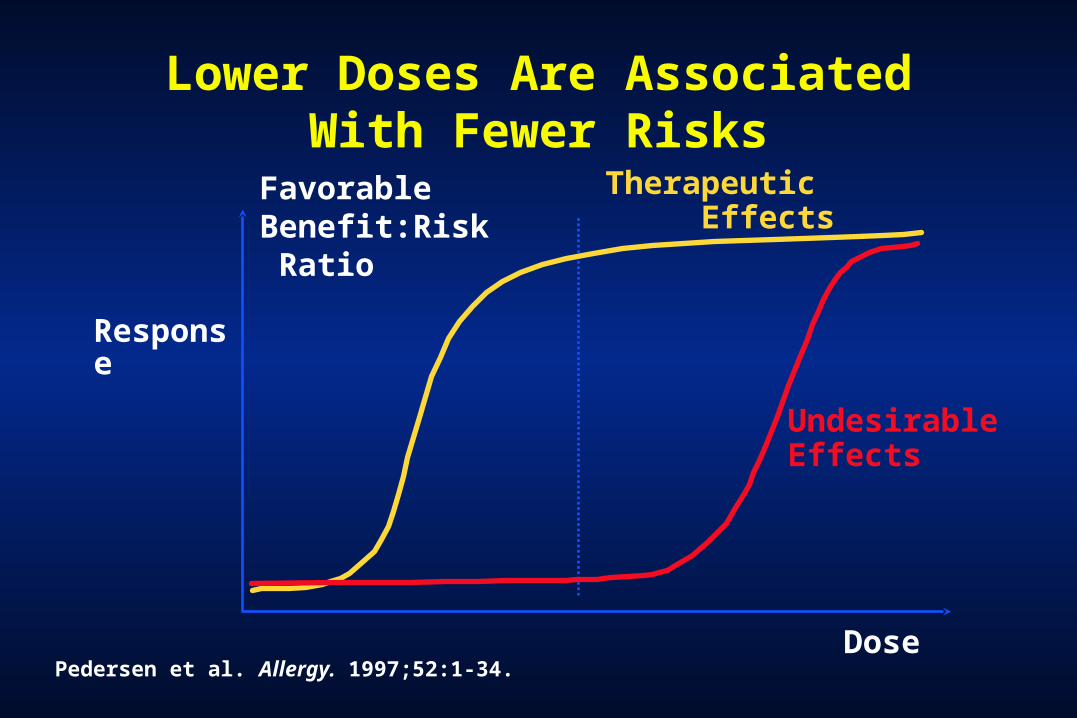
Lower Doses Are Associated With Fewer Risks
Response
Pedersen et al. Allergy. 1997;52:1-34.Dose
Therapeutic Effects
Favorable Benefit:Risk Ratio
Undesirable Effects
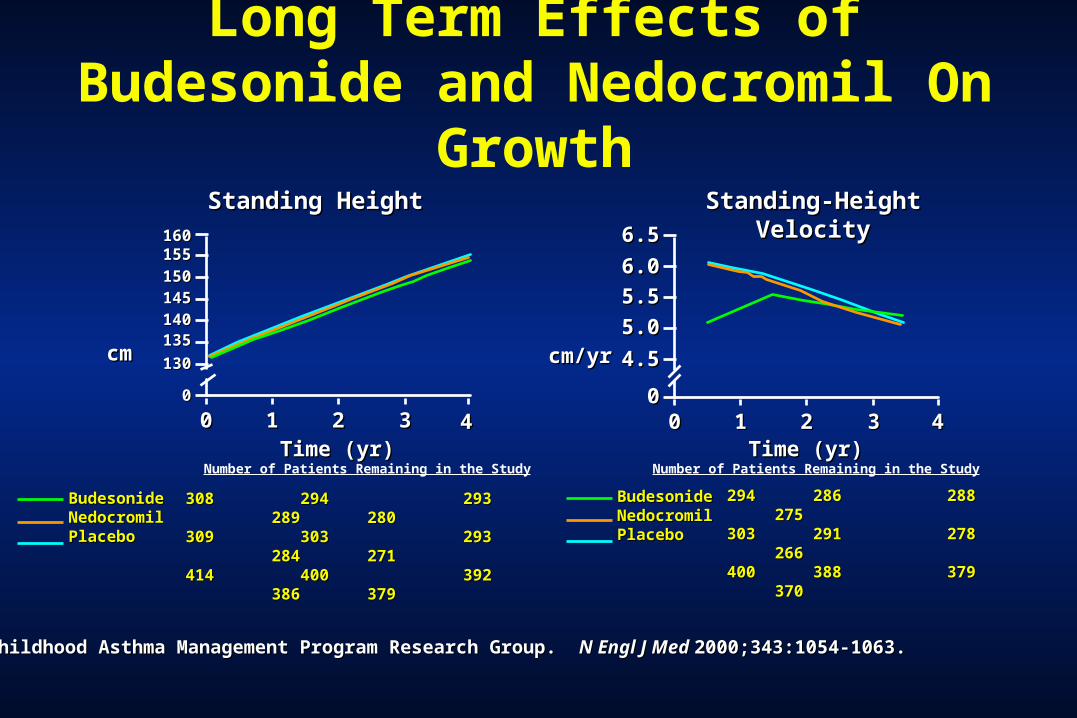
Childhood Asthma Management Program Research Group. Childhood Asthma Management Program Research Group. N Engl J Med N Engl J Med 2000;343:1054-1063.2000;343:1054-1063.
00
4.54.5
5.05.0
6.06.0
6.56.5
00 11 22 33 44Time (yr)Time (yr)
cm/yrcm/yr
Standing-Height VelocityStanding-Height Velocity
5.55.5
00
130130
135135
145145150150
00 11 22 33 44Time (yr)Time (yr)
308 294308 294 293 289 280 293 289 280309 303309 303 293 284 271 293 284 271414 400414 400 392 386 379 392 386 379
cmcm
Standing HeightStanding Height
140140
BudesonideBudesonideNedocromilNedocromilPlaceboPlacebo
155155160160
BudesonideBudesonideNedocromilNedocromilPlaceboPlacebo
Number of Patients Remaining in the Study Number of Patients Remaining in the Study
Long Term Effects of Budesonide and Nedocromil On Growth
294294 286286 288 275 288 275 303303 291291 278 266 278 266 400400 388 388 379 370 379 370

= Girls= Girls
= Boys= Boys
Agertoft L & Pedersen S. NEJM 343:1064, 2000Agertoft L & Pedersen S. NEJM 343:1064, 2000
Predicted and Measured Adult Height

Important Additional Steps
• Asthma educationAsthma education• Triggers, Adherence, Follow-upTriggers, Adherence, Follow-up
• Identify and treat comorbiditiesIdentify and treat comorbidities• Allergies, Sinus Disease, RefluxAllergies, Sinus Disease, Reflux
• Address Barriers to CareAddress Barriers to Care

Childhood Asthma
• Serious, common diseaseSerious, common disease
• InflammationInflammation
• Inhaled steroids are effectiveInhaled steroids are effective
• Environmental and social factors Environmental and social factors are very importantare very important

He who knows and knows that he knows is conceited; avoid him. He who knows not and knows not that he knows not is a fool; instruct him.He who knows and knows not that he knows is asleep; awaken him.But he who knows not and knows that he knows not is a wise man; follow him.
— Arab proverb
