athletes heart
TRANSCRIPT

K SRINIVAS
ATHLETE’S HEART

HISTORY
Heneschen(1890) used physical
examination to determine increased
cardiac dimensions in elite nordic skiers.
Eugene darling in the same year in
rowers of harvard university.
2/1/2015 2ATHLETE'S HEART

Paul dudely white(1900)
studied radial pulse rate
among boston marathon
competitors and was the
first to report marked
resting sinus bradycardia in
long distance runners.2/1/2015 3ATHLETE'S HEART

Earlier it was thought to be beneficial
adaptations to exercise.
But later it was postulated as a form of
overuse pathology and prolonged
participation in sport can lead to
premature cardiovascular system
collapse.
2/1/2015 4ATHLETE'S HEART

Athlete’sheart syndrome , a term often
applied to athletic patient who present
with subjective symptoms or abnormal
CVS findings.
2/1/2015 5ATHLETE'S HEART

Aerobic /endurance exercises
execises requiring primarily an increase in o2 transpot.
2/1/2015 6ATHLETE'S HEART

Resting /strength exercises
exercises primarily stressing the skeletal muscle.
2/1/2015 7ATHLETE'S HEART

PHYSIOLOGY
Physical activity acutely increases o2
demand which increases cardiac output
(Q) and arteriovenous difference (A-
V)O2.
1 lit of oxygen consumption (VO2)
produces 5-6 lit increase in Q.
2/1/2015 8ATHLETE'S HEART

The CV response to exercise has both
external and internal work rate,
External work rate is VO2 required for
exercise task and is direct determination
of Q.
Internal work rate is MO2 required for
exercise task and is direct determinant
of HR
2/1/2015 9ATHLETE'S HEART

2/1/2015ATHLETE'S HEART 10
Repetitive excercises to increase exercise capacity
Increases VO2
Increased Q(HR and SV)
Increased stroke volume

The increase in SV means that
performing the same exercise task which
requires the same VO2 can be performed
at a slower HR and a lower MO2 or
internal work rate.
2/1/2015ATHLETE'S HEART 11

The physiologic mediators of these CV
adaptations may be produced by
increased resting vagal tone and reduced
resting sympathetic tone resulting in
resting sinus bradycardia
2/1/2015ATHLETE'S HEART 12

LEFT VENTRICLE
Studies revealed LV hypertrophy and
dilation.
Pellica.et.al showed increased LV end
diastolic diameter and small percentage
had LV wall thickness more than 13mm.
2/1/2015ATHLETE'S HEART 13

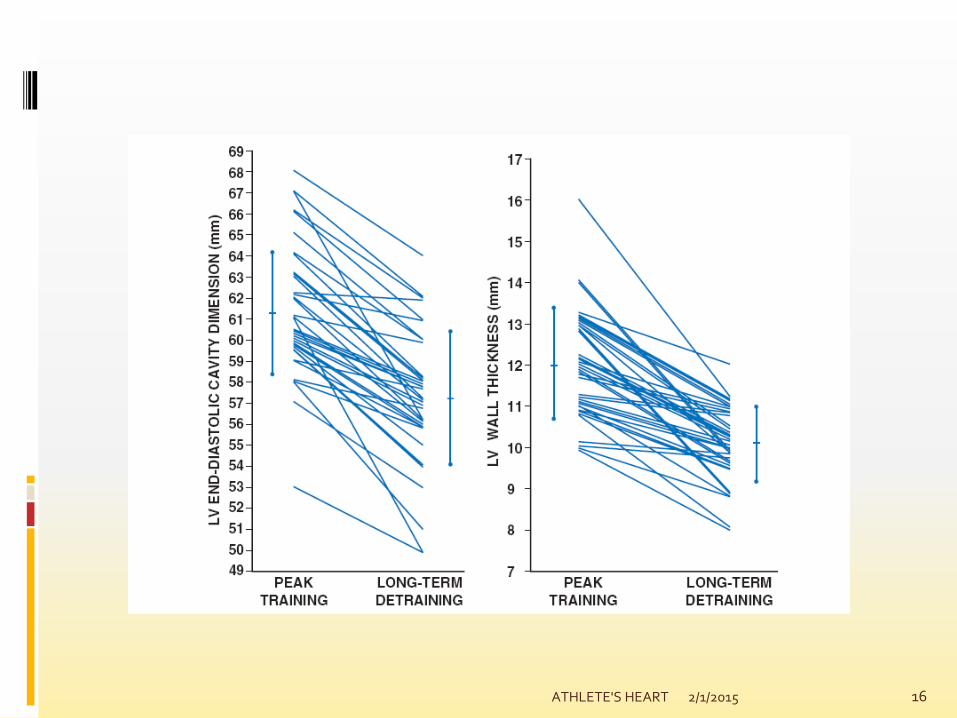
MORGANROTH HYPOTHESIS
Morganroth.et.el studies demonstrated
concentric LV hypertrophy in strength
training and eccentic LV hypertrophy in
aerobic training.
2/1/2015ATHLETE'S HEART 14

2/1/2015ATHLETE'S HEART 15
2/1/2015ATHLETE'S HEART 16

2/1/2015ATHLETE'S HEART 17

Figure 3. Impact of different clinical variables on LV end-diastolic cavity dimensions in a large
population of male and female elite athletes.
Maron B J , and Pelliccia A Circulation. 2006;114:1633-
1644
Copyright © American Heart Association, Inc. All rights reserved.2/1/2015 18ATHLETE'S HEART

On LV systolic function
demonstrated preserved LV ejection
fraction except for one study
On LV diastolic function
improved LV diastolic function is essential
mechanism in preserving stroke volume
2/1/2015ATHLETE'S HEART 19

RIGHT VENTRICLE
Cardiac remodelling is not confined to LV
Scharhag et al study demonstrated RV
enlargement parallels LV enlargement
supporting the concept of biventricular
enlargement.
2/1/2015ATHLETE'S HEART 20

AORTA
Experiences a significant hemodynamic
load during exercise.
Aerobic exercise- high volume aortic
flow with modest systemic hypertension
Strength exercises-normal volume with
profound systemic hypertension.
2/1/2015ATHLETE'S HEART 21

Babee et al studies revealed increased
aortic dimensions in strength exercise
training.
Pellica et al studies revealed incresed
aortic dimensions in aerobic training
exercises.
2/1/2015ATHLETE'S HEART 22

LEFT ATRIUM
Studies confirmed high prevalnce of left
atrial enlargement in athletes
SEX AND RACE
2/1/2015ATHLETE'S HEART 23

PATHOLOGY VS PHYSIOLOGICAL ADAPTATION
2/1/2015ATHLETE'S HEART 24

A, An electrocardiogram of a 46-year-old male triathlete who presented after long-standing
palpitations and a recent episode of syncope.
Baggish A L , and Wood M J Circulation. 2011;123:2723-
2735
Copyright © American Heart Association, Inc. All rights reserved.2/1/2015 25ATHLETE'S HEART

ARRHYTHMIAS
Brady arrhythmias such as
Sinus bradycardia
Junctional bradycardia
AV block
The reduced AV conduction velocity may take
accessory pathway such as WPW syndrome.
2/1/2015ATHLETE'S HEART 26

Increased vagal tone may be responsible
for early repolarisation and ST
abnormalities.
2/1/2015ATHLETE'S HEART 27

2/1/2015ATHLETE'S HEART 28

VALVE DISEASE IN ATHLETS
AORTIC STENOSIS
Careful evaluation of symptoms and
maximal exercise testing
Warm up dyspnea indicates clinically
important AS
2/1/2015ATHLETE'S HEART 29

AORTIC REGURGITATION
Generally tolerate AR,because of
increased HR during exercise, decreases
diastole and regurgitant.
Rarely restrict the patients with AR
unless there is ventricular deterioration.
2/1/2015ATHLETE'S HEART 30

AORTIC DISSECTION IN BAV
We do not restrict the patient unless the
patient aortic root dimensions are more
than 45 mm
Annual screening.
2/1/2015ATHLETE'S HEART 31

SYNCOPE
Majority of syncope in athlete’s is
attributed to neurocardiogenic syncope.
Manifests in the immediate post exercise
testing owing to sudden reduction in
venous return, which facilitates transient
cerebral hypoperfusion.
2/1/2015ATHLETE'S HEART 32

Syncope during exercise, there is a
possibility of malignant arrhythmias,
valvular heart disease and myocardial
ischemia.
2/1/2015ATHLETE'S HEART 33

DECREASED EXERCISE CAPACITY
Hyperthyroididm
Exercise induced asthma
Disease of the skeletal muscles
Anemia
AF
Viral illness
2/1/2015ATHLETE'S HEART 34

ELEVATED CARDIAC ENZYMES
Increase in cTnT occurs in athletes
following prolonged exertion.
Endurance athletes were documented to
have increased concentrations of CK-MB
and satellite cells in their leg muscles.
2/1/2015ATHLETE'S HEART 35

2/1/2015ATHLETE'S HEART 36

2/1/2015 37ATHLETE'S HEART

2/1/2015ATHLETE'S HEART 38