atlanta plumbers and steamfitters health and welfare fund
TRANSCRIPT

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: Active Plan Participants
From: Board of Trustees
Date: November 15, 2020
RE: Important Announcement regarding Dependent Coverage
IMPORTANT ANNOUNCEMENT ABOUT YOUR HEALTHCARE BENEFITS
The Board of Trustees of the Atlanta Plumbers & Steamfitters Health and
Welfare Fund (“the Fund”) has established a special committee to work on
improving participants’ experience with using their benefits. The committee
has met numerous times over the course of the 2020 plan year and will
continue to meet to evaluate and simplify plan rules and requirements, with
the objective of providing participants with a more convenient experience.
Dependent Coverage Contribution Requirements
The Trustees recognize that the initial process that was established for
collecting dependent coverage contributions has, at times, led to
dissatisfaction from plan participants. The Trustees are pleased to announce
revised dependent coverage contribution guidelines that have been
established to address this challenge.
What’s Changing
Initial Dependent Coverage: When a participant completes the
enrollment process to add new dependents, such as a new spouse or new
dependent child, eligible dependents will be enrolled in the plan without
requiring that dependent coverage contributions be received in advance.
How does this help? Previously, participants had to remit their dependent
coverage contributions before their dependents could be covered, which
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Jarrett Wade
UA Local Union 72
Mr. Alan Tomberlin
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Andy Sumpter
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical Services
Mr. John McKenney
McKenney’s Inc.
Mr. James K. Estabrook
Lindabury, McCormick,
Estabrook & Cooper, P.C.
Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
sometimes led to delays in getting new dependents covered. This new process will eliminate these
delays.
Continuing Dependent Coverage: If a participant has an interruption in their dependent coverage
contributions, dependent coverage will not be immediately lost.
How does this help? Previously, if the full amount due for each month was not received, dependent
coverage was dropped until the participant self-paid the contributions owed. This happened for a
variety of reasons, including participants being out of work, participants taking vacation time,
deduction errors at participants’ employers, etc.
Under the new requirements, participants will still owe the same amount for the coverage; however,
participants will have until December 15th each year to pay any shortages due that have accumulated
throughout the year. This new process will eliminate the interruptions in dependent coverage due
to missed contributions.
NEBA will continue to provide periodic self-pay statements for dependent contributions owed and
the Trustees encourage participants to pay shortages due as soon as possible to avoid accumulating
a large self-pay amount due at the end of the year.
Dependent Coverage Contribution Reconciliation for Participants with Dependents
Each year, NEBA will review each participant’s dependent contribution history for the 12-month period
beginning November 1 of the prior year through October 31 of the current year, to determine if there are
any shortages due. One month of dependent contributions will be owed for each month of dependent
coverage that was provided during the current year.
Following this review, NEBA will notify each participant that has a dependent contribution shortage with
a statement of amounts due. Participants must submit payment for amounts due no later than
December 15th. Dependent coverage will terminate on December 31st for Participants who do not remit
the amounts due by December 15th. Dependent coverage that has been terminated due to non-payment
may only be reinstated under the limited circumstances outlined on the next page.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Conditions for Re-Enrolling Dependent Children or Spouse After Lapse in Coverage Due to Non-Payment
A participant may re-enroll a Dependent child or spouse after a lapse in coverage due to non-payment of
dependent contributions, provided that the Dependent child or Dependent spouse otherwise meets the
remaining Plan eligibility requirements as of the enrollment date, and the following conditions are met:
The participant remits payment in full for all outstanding dependent coverage contributions; and,
the participant becomes newly eligible for benefits after a lapse in coverage, pursuant to the
reinstatement of eligibility rules; or
the Dependent child or Dependent spouse would otherwise be eligible to enroll during a
subsequent open enrollment period; or
the Dependent child or Dependent spouse becomes eligible for a special enrollment right pursuant
to the Health Insurance and Portability Act.
Enclosed with this memorandum is a Summary of Material Modifications (SMM) which describes these
changes in detail. The SMM should be kept with your Summary Plan Description (SPD). As always, please
feel free to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc.
(“NEBA”) at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – January 1, 2021
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta
Plumbers and Steamfitters Health and Welfare Fund (the “Fund”). This SMM modifies the language found
in your Summary Plan Description (SPD). All statements made in this document are subject to the terms
and conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan
Document, the Plan Document will govern. Copies of the SPD and Plan Document are available for review
at any time during normal working hours at NEBA’s offices.
Dependent Eligibility
The eligibility rules of the Fund have been revised to reflect the following requirements for dependents.
Dependent Child
A Dependent child of an Employee who becomes eligible for benefits shall become eligible for
benefits for each month beginning as of the date upon which the Employee first becomes eligible for
benefits and enrolls the Dependent child, if any required contribution is made to the Trust on behalf of
the Dependent child for each such month; provided, that if any such required contribution is not paid for
any applicable month or months, coverage for the Dependent child shall continue during the month or
months for which the required contribution has not been paid.
The total amount of any unpaid monthly contributions for a Plan Year shall be due and payable on
or before the December 15 of the year in which the monthly contributions are due. In the event that
unpaid monthly contributions are not paid by the applicable December 15, the Dependent child will not
be eligible to receive coverage under the Plan for any subsequent Plan Year during which the monthly
contributions remain unpaid, and shall not again become eligible to enroll in the Plan until the date upon
which the past due contributions are paid in full and either: (A) the Employee again becomes eligible for
benefits after a lapse in coverage, pursuant to the reinstatement of eligibility rules; (B) the Dependent
child would otherwise be eligible to enroll during a subsequent open enrollment period; or (C) the
Dependent child becomes eligible for a special enrollment right pursuant to the Health Insurance and
Portability Act; provided, that the Dependent child otherwise meets the remaining Plan eligibility
requirements as of the enrollment date.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Dependent Spouse
A Dependent spouse of an Employee, except for an Employee classified as a “residential
employee,” who becomes eligible for benefits shall become initially eligible for benefits beginning as of
the first day of the third month following a period of twelve (12)-consecutive months or less during which
such Employee has worked at least twelve hundred (1,200) hours; provided, that Employer contributions
are properly paid to the Fund on behalf of the Employee or, as applicable, reciprocal contributions are
received by the Fund for each such month; provided, further, that the Covered Employee enrolls the
Dependent spouse and pays to the Trust the required contribution on behalf of the Dependent spouse for
each such month.
If any required contribution is not paid by the Covered Employee for any applicable month or
months, coverage for the Dependent spouse shall continue during the month or months for which the
required contribution has not been paid. The total amount of any unpaid monthly contributions for a Plan
Year shall be due and payable on or before the December 15 of the year in which the monthly
contributions are due. In the event that unpaid monthly contributions are not paid by the applicable
December 15, the Dependent spouse will not be eligible to receive coverage under the Plan for any
subsequent Plan Year during which the monthly contributions remain unpaid, and shall not again become
eligible to enroll in the Plan until the date upon which the past due contributions are paid in full and either:
(A) the Employee again becomes eligible for benefits after a lapse in coverage, pursuant to the
reinstatement of eligibility rules; (B) the Dependent spouse would otherwise be eligible to enroll during a
subsequent open enrollment period; or (C) the Dependent spouse becomes eligible for a special
enrollment right pursuant to the Health Insurance and Portability Act; provided, that the Dependent
spouse otherwise meets the remaining Plan eligibility requirements as of the enrollment date. Spouses
of Employees classified as ‘residential employees’ are not eligible to participate in the Plan.”
This Summary of Material Modifications should be kept with your Summary Plan
Description.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: All Plan Participants
From: Board of Trustees
Date: April 2020
RE: Health & Welfare Benefits
IMPORTANT ANNOUNCEMENTS ABOUT YOUR HEALTH
AND WELFARE BENEFITS
The Board of Trustees of the Atlanta Plumbers and Steamfitters Health and
Welfare Fund (“Fund”) wishes to extend their best wishes for the wellbeing of
you and your families during this unprecedented time. In accordance with the
Families First Coronavirus Response Act (“FFCRA”), a package of provisions
aimed at providing emergency relief and support during the 2020 novel
coronavirus/COVID-19 pandemic, the Board has approved certain changes to
your benefit plan.
The following services will be covered without any cost sharing charges (e.g. no
deductible, co-payment, or co-insurance) for the Fund’s eligible participants and
dependents:
1. Diagnostic tests to detect the coronavirus that are approved or authorized
by the FDA, including the administration of such tests; and
2. Items and services furnished to individuals during provider office visits
(whether in-person or via telehealth), urgent care visits, and emergency
room visits that result in an order for, or the administration of, a test as
described above, but only to the extent such items or services relate to the
furnishing or administration of the test or the evaluation of whether the
individual needs the test.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Jarrett Wade
UA Local Union 72
Mr. Alan Tomberlin
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Andy Sumpter
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. James K. Estabrook
Lindabury, McCormick,
Estabrook & Cooper, P.C.

Atlanta Plumbers and Steamfitters
Health & Welfare Benefits Page 2
This provision applies to tests, items and services provided on or after March 18, 2020 through the end of
the federal government’s declared emergency period related to COVID-19.
Medically necessary treatment of COVID-19 remains covered under the normal rules of the Plan (including
cost sharing and other requirements).
Dependent Coverage Contributions
If you are not currently working and were previously making dependent coverage contributions via payroll
deductions, there are several options available to you. You may self pay for the contributions owed via credit
card, debit card, check or money order. If you are on the “Out of Work” list at Local 72 or are furloughed,
you may withdraw hours from your hour bank to use as payment instead.
If You Are on The Local 72 Out of Work List or Furloughed
• You may submit an hour bank withdrawal form via NEBA’s website,
https://www.nebainc.com/send-secure-file/ (preferred). A copy of the form is enclosed.
• You may submit an hour bank withdrawal form via U.S. Mail to the following address. A copy of the
form is enclosed.
Atlanta Plumbers & Steamfitters H & W Fund
2010 N.W. 150th Avenue, Suite 100
Pembroke Pines, FL 33028
(Postal service delays may occur)
• You may remit payment by credit or debit card via NEBA’s website,
https://os.nebainc.com/atldependent (preferred).
• You may remit payment via check or money order via U.S. Mail to the address listed above. (Postal
service delays may occur)
If You Are Not Working, Not on The Local 72 Out of Work List, and Not Furloughed
• You may remit payment by credit or debit card via NEBA’s website,
https://os.nebainc.com/atldependent (preferred).
• You may remit payment via check or money order via U.S. Mail to the address listed above.
(Postal service delays may occur)

Atlanta Plumbers and Steamfitters
Health & Welfare Benefits Page 3
Instructions for Remitting Credit or Debit Card Payments:
1. Visit https://os.nebainc.com/atldependent.
2. Complete the checkout process.
A. Complete all requested information
in the fillable form.
B. If you are unsure how much you
owe, or what coverage period you
must pay for, please contact NEBA
at:
or
1-888-365-0072
C. Click Continue to complete
checkout.
D. Enter your credit or debit card
details.
E. Enter your email address to get an
email confirmation.
F. Check the “I’m not a robot” box.
G. Click the “Pay With Your Credit
Card” box to complete the
transaction.

Atlanta Plumbers and Steamfitters
Health & Welfare Benefits Page 4
Instructions for Using the Secure Upload Feature of NEBA’s Website:
1. Visit https://www.nebainc.com/send-secure-file/.
A. Complete the requested information in the fillable form.
B. Choose the Atlanta Office from the department drop down list.
C. Click the “Choose File” button to select the file you wish to send. This will allow you to
select a saved file on your computer, or open your device camera if you are using a
smartphone or other mobile device with a camera.
D. Click the “Submit” button.

Atlanta Plumbers and Steamfitters
Health & Welfare Benefits Page 5
As always, please feel free to call the Plan’s Third Party Administrator, National Employee Benefits
Administrators, Inc. (“NEBA”) with any questions.
NEBA can be reached at:
National Employee Benefits Administrators, Inc.
374 Maynard Terrace SE, Suite 072
Atlanta, GA 30316
Toll Free 888.365.0072 | Fax 404.464.7905

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
To: All Plan Participants
From: Board of Trustees
Date: April 2019
RE: Dental and Vision Benefits
IMPORTANT ANNOUNCEMENT ABOUT YOUR HEALTHCARE
BENEFITS
This document is a “Summary of Material Modifications” (SMM) which
describes changes to the Atlanta Plumbers and Steamfitters Health and Welfare
Fund (the “Fund”). This SMM modifies the language found in your Summary
Plan Description (SPD). All statements made in this document are subject to the
terms and conditions of the Plan Document. If there is a discrepancy between
the SPD or this SMM and the Plan Document, the Plan Document will govern.
The Board of Trustees of the Atlanta Plumbers and Steamfitters Health and
Welfare Fund is pleased to announce that effective June 1, 2019, dental and
vision benefits will be reinstated for all eligible plan participants. All enrolled
participants and dependents will be automatically enrolled in the new dental
and vision programs, so no action is required.
Dental care benefits will be insured by Delta Dental. Vision care benefits will
be insured by Group Vision Service (GVS). Enclosed are benefit summaries for
both plans. Dental and vision ID cards will be mailed to your home in late May.
Following are some highlights regarding your new benefits: Dental Benefits*
(Delta Dental)
Waiting Periods None
Deductible $50 per person each calendar year * waived for Diagnostic & Preventative
Maximums $1,000 per person each calendar year
Diagnostic & Preventative Benefits Exams, cleanings and x-rays covered at 100%
Basic Services , Endodontics, Periodontics, Oral Surgery
Covered at 75%
Major Services & Prosthodontics Covered at 50%
* See benefit summary for full details
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Jarrett Wade
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. James K. Estabrook
Lindabury, McCormick,
Estabrook & Cooper, P.C.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
Benefit Highlights, continued…
Vision Benefits* (Group Vision Service)
Vision Examination- In Network Once Every 12 Months/ $5.00 copay *Includes Dilation as indicated
Eyeglass Lenses- In Network Once Every 12 Months/ No copay
Frames – In Network Once Every 12 Months/ Covered at 100% up to a $150.00 retail value
Contact Lenses – Elective Once Every 12 Months/ Covered at 100% up to $150.00 Allowance
Contact Lenses – Medically Necessary Once Every 12 Months/ Covered at 100% up to $250.00
* See benefit summary for full details
As always, please feel free to call the Plan’s Third Party Administrator, National Employee Benefits
Administrators, Inc. (“NEBA”) with any questions. NEBA can be reached at:
National Employee Benefits Administrators, Inc.
374 Maynard Terrace SE, Suite 072 | Atlanta, GA 30316
Toll Free 888.365.0072 | Fax 404.464.7905
This Summary of Material Modifications should be kept with your Summary Plan
Description.

Copyright © 2018 Delta Dental. All rights reserved. HL_PPO #112725A (rev. 4/18)
1 In Texas, Delta Dental Insurance Company provides a dental provider organization (DPO) plan.
2 You can still visit any licensed dentist, but your out-of-pocket costs may be higher if you choose a non-PPO dentist. Network dentists are paid contracted fees.
3 You are responsible for any applicable deductibles, coinsurance, amounts over annual or lifetime maximums and charges for non-covered services. Out-of-network dentists may bill the difference between their usual fee and Delta Dental’s maximum contract allowance.
4 Applies only to procedures covered under your plan. If you began treatment prior to your effective date of coverage, you or your prior carrier is responsible for any costs. Group- and state-specific exceptions may apply. If you are currently undergoing active orthodontic treatment, you may be eligible to continue treatment under Delta Dental PPO. Review your Evidence of Coverage, Summary Plan Description or Group Dental Service Contract for specific details about your plan.
LEGAL NOTICES: Access federal and state legal notices related to your plan at deltadentalins.com/about/legal/index-enrollee.html.
Save with PPOVisit a dentist in the PPO1 network to maximize your savings.2 These dentists have agreed to reduced fees, and you won’t get charged more than your expected share of the bill.3 Find a PPO dentist at deltadentalins.com.
Set up an online accountGet information about your plan anytime, anywhere by signing up for an online account at deltadentalins.com. This free service, available once your coverage kicks in, lets you check benefits and eligibility information, find a network dentist and more.
Check in without an ID cardYou don’t need a Delta Dental ID card when you visit the dentist. Just provide your name, birth date and enrollee ID or social security number. If your family members are covered under your
plan, they will need your information. Prefer to take a paper or electronic ID card with you? Simply log in to your account, where you can view or print your card with the click of a button.
Coordinate dual coverage If you’re covered under two plans, ask your dental office to include information about both plans with your claim, and we’ll handle the rest.
Understand transition of careDid you start on a dental treatment plan before your PPO coverage kicked in? Generally, multi-stage procedures are only covered under your current plan if treatment began after your plan’s effective date of coverage.4 You can find this date by logging in to your online account.
Newly covered?Visit deltadentalins.com/welcome.
Save with a PPO dentist
PPO NON–PPO
Keep Smiling Delta Dental PPOTM

Eligibility Primary enrollee, spouse and eligible dependent children to the end of the month dependent turns age 26
Deductibles $50 per person each calendar year Deductibles waived for Diagnostic & Preventive (D & P)? Yes
Maximums $1,000 per person each calendar year D & P counts toward maximum? Yes
Waiting Period(s) Basic Benefits None
Major Benefits None
Prosthodontics None
* Limitations or waiting periods may apply for some benefits; some services may be excluded from your plan.Reimbursement is based on Delta Dental maximum contract allowances and not necessarily each dentist’ssubmitted fees.
** Reimbursement is based on PPO contracted fees for PPO dentists, Premier contracted fees for Premier dentists and program allowance for non-Delta Dental dentists.
Delta Dental Insurance Company 1130 Sanctuary Parkway, Suite 600 Alpharetta, GA 30009
Customer Service 800-521-2651
Claims Address P.O. Box 1809 Alpharetta, GA 30023-1809
deltadentalins.com This benefit information is not intended or designed to replace or serve as the plan’s Evidence of Coverage or Summary Plan Description. If you have specific questions regarding the benefits, limitations or exclusions for your plan, please consult your company’s benefits representative.
HLT_DDIC_PPO_2COL_(Rev. 4/11/2019)
Plan Benefit Highlights for: Atlanta Plumbers & Steamfitters Local 72 Group No: 20000 Effective Date: 6/1/2019
Benefits and Covered Services*
Delta Dental PPO dentists**
Non-Delta Dental PPO dentists**
Diagnostic & Preventive Services (D & P) Exams, cleanings and x-rays
100 % 100 %
Basic Services Fillings, sealants and denture repair/relining/rebase
75 % 75 %
Endodontics (root canals) Covered Under Basic Services 75 % 75 %
Periodontics (gum treatment) Covered Under Basic Services 75 % 75 %
Oral Surgery Covered Under Basic Services 75 % 75 %
Major Services Crowns, inlays, onlays and cast restorations
50 % 50 %
Prosthodontics Bridges and dentures 50 % 50 %

This plan provides coverage for a vision examination, eyeglass lenses or contact lenses and frame and a hearing exam with allowances for hearing aids. Vision benefits are available from an extensive national network of participating providers powered by Eye Med Vision Care. You can easily find a conveniently located provider near you. You have a choice of independent optometrists and ophthalmologists, as well as retail locations such as Lens Crafters, Sears Optical, Target Optical and JC Penney Optical and most Pearle Vision Centers. Members will receive additional savings from Network Providers for lens upgrades and additional pair purchases.
NETWORK PROVIDERS - By using a network provider, you minimize your out-of-pocket costs and receive the benefit of our paperless claims processing. Network Providers verify your eligibility and obtain all the necessary information to validate your level of coverage. You simply pay your copayment and any remaining balance for non-covered services or materials at the time of your appointment. In addition, Network Providers offer you discount pricing which is significantly below retail. You receive substantial savings of 15%-40% or more on most additional pair purchases, conventional contact lenses, lens treatments, specialized lenses and various accessory items. Out of Network Benefits** – If you choose to go to a non-network provider, you must pay the provider his or her full charges at the time of service. Members will be responsible for submitting a claim for reimbursement for the amount indicated in the member reimbursement schedule.
Benefits from a Network Provider* Member
Copay Out-of-Network
Benefit Schedule **
Vision Examination – includes dilation as indicated Once Every 12 Months* $ 5.00 Vision Examination
Up to $32.00
Eyeglass Lenses - single vision, bifocal, or trifocal in standard/basic plastic w/Standard Scratch Resistance and Polycarbonate Lenses for dependent children under 19
Once Every 12 Months* $ 0.00
Lenses
• Single Vision
• Bifocal
• Trifocal
• Standard Scratch
• Polys Child
Up to $30.00 Up to $45.00 Up to $75.00 Up to $12.00 Up to $32.00
Frame – covered in full up to a $ 150.00 retail value. Members receive 20% off balance for selection costing more than the plan allowance. Glasses available through glasses.com
Once Every 12 Months* N/A Frame Up to $66.00
Contact Lenses - in lieu of spectacle lenses (does not include fitting and follow-up)
• Elective – Disposable or Conventional, covered in full up to $ 150.00 Allowance. Conventional lenses: members receive 15% discount off balance over plan allowance.
Contacts available through contactsdirect.com
• Medically Necessary – Covered in full up to $ 250.00
Once Every 12 Months* N/A
Elective Contact Lenses (in lieu of spectacle lenses) Medically Necessary Contact Lenses
Up to $120.00 Up to $200.00
* Benefits are available 12 months from last date of service *In-network services and materials may be subject to a copayment at the time of service. **Out-of-Network amounts are maximum reimbursable amounts paid to members after the claim is filed. Co-pays don’t apply to the out of network reimbursement
Additional Savings Program
Lens Options Member
Pricing Other Options/Services Member Pricing
877-606-3742
Please contact EPIC to utilize the hearing aid discount
plan
Tint (solid & gradient) $15.00 Other Lens Add-Ons and
Services 20% off Retail
UV Coating $15.00 Complete Pair Purchases *** 40% off Retail
Standard Scratch Resistance* Covered Conventional Contact Lenses 15% off Retail
Standard Polycarbonate Adult
$40.00
Standard Contact Lens Fitting
& Follow-up
$40.00
Standard Polycarbonate
Children* Covered
Premium Contact Lens Fitting
& Follow-up 10% discount
Standard Anti-Reflective $45.00 EPIC Hearing Savings Plan Fixed fee schedule
on hearing aids
*Covered by plan benefit. ** Standard/Premium Progressive lenses are not covered benefits – however when upgrading in conjunction with your funded benefit the bifocal lens amount will be applied. Members are responsible for the lens copayment and any additional charges. (bifocal co-pay + $65 + 80% of retail less $120 *** Discount applies on complete pair purchase once funded benefit is used.
Standard Progressive Lens** $65.00 Photo chromatic Lenses 20% discount
Premium Progressive Lenses** 20% off Retail
Retinal Imaging $39.00

Vision Limitations & Exclusions
Fees charged by a provider for services other than a covered benefit must be paid in full by the insured to the provider. Such fees or materials are not covered under the policy. Benefit allowances provide no
remaining balance for future use within the same benefit frequency. No benefits will be paid for services or materials connected with/or charges arising from
• Orthoptic or vision training, subnormal vision aids and any associated supplemental testing; Aniseiikonic lenses; medical and/or surgical treatment of the eye, eyes or supporting structures
• Any corrective eyewear, required by a policyholder as a condition of employment, safety eyewear, services provided as a result of any Worker’s Compensation law, or similar legislation or required by any governmental agency or program whether federal, state or subdivision thereof
• Plano (non-prescription) lenses; non-prescription sunglasses
• Two pair of glasses in lieu of bifocal
• Services or materials provided by another group benefit plan providing vision care
• Services rendered after the date an insured ceases to be covered under the policy, except when vision materials ordered before coverage ended are delivered and the services rendered to the insured are within 31 days from the date of such order
• Lost or broken lenses, frames, glasses or contact lenses will not be replaced except in the next benefit frequency when vision materials would next become available.
• Certain frame brands in which the manufacturer imposes a no-discount policy
• Covered benefits may not be used in conjunction with coupons or other provider discount offers
• If an Insured and the Insured Spouse are both Insured by the plan, one Insured party may request to be a Dependent spouse of the other. A Dependent child may not be covered by more than one Insured.
Visit the GVS web site to “Locate a Provider” or “View your Benefits” and learn more about
our Additional Savings Program
Web Site – www.gvsmd.com - click “Members” to locate a provider or view your benefits Customer Service and IVR – at 866-265-4626 Call customer service to ask about your benefits or to locate a provider.
Access 7Days
a Week
Call Center Hours
7:30 a.m. to 11:00 p.m. EST-Monday – Saturday 11:00 a.m. to 8:00 p.m. EST - Sunday
Locating a Provider
Network Providers 1. Find network provider at www.gvsmd.com click on “Providers”. 2. Schedule an exam with the provider of your choice. When scheduling your appointment inform the provider that you are a
GVS/EyeMed member and provide your name and date of birth (DOB). The provider will verify your eligibility and plan benefits prior to your appointment.
3. If you have already made an appointment show your ID card at the time of service or provide your name and DOB for quick verification of eligibility and plan coverage.
4. Members will be responsible to pay the provider at the time of service for any applicable copayment /costs that exceed the plan coverage.
Out-of-Network Providers 1. Visit non-network provider 2. Members are required to pay the entire amount for exam and eyewear at the time of service. 3. Members must obtain an OON claim form from the GVS website at www.gvsmd.com. (click “Members”). 4. Members must submit OON claim form and provider receipt to the Claims Address indicated on the form. 5. Member will be reimbursed based on OON benefits indicated in their benefit summary.
Personalized Member Website Access For Members to Access their Benefits: You must first register on the GVS website – www.gvsmd.com
1. Under the MEMBER tab select VIEW YOUR BENEFITS 2. Welcome to the GVS Member - Click here to Login/Register 3. Select Register for an account 4. When you enter the Member Site to Register for an Account - USE the LAST FOUR DIGITS of your social security number and pick
your own user ID. 5. Site will send an Email confirmation and password selection

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – January 1, 2019
This document is a “Summary of Material Modifications” (SMM) which
describes changes to the Atlanta Plumbers and Steamfitters Health and
Welfare Fund (the “Fund”). This SMM modifies the language found in your
Summary Plan Description (SPD). All statements made in this document are
subject to the terms and conditions of the Plan Document. If there is a
discrepancy between the SPD or this SMM and the Plan Document, the Plan
Document will govern. Copies of the SPD and Plan Document are available for
review at any time during normal working hours at the Plan’s office.
Effective January 1, 2019, the weekly benefit available through the
Fund’s Loss of Time Benefit is $300 per week for any period in which
you are temporarily Totally Disabled. This weekly benefit will continue
to be subject to Federal FICA tax withholdings. See the chart below for
additional details about the Short Term Disability Benefit.
Benefit Description Benefit Available
Total Benefit Duration Available 36 weeks
Total Monetary Benefit Available $300 per week
If you have any questions, please contact National Employee Benefits
Administrators, Inc. at (888) 365-0072.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Jarrett Wade
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. James K. Estabrook
Lindabury, McCormick,
Estabrook & Cooper P.C.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
To: All Plan Participants Except Helpers, Tradesmen and Pipe Tradesmen
From: Board of Trustees
Date: January 29, 2018
RE: Benefit Changes
As a member of Plumbers, Pipefitters, & HVACR Technicians Local 72 (“Local
72”) you receive health care benefits through the Atlanta Plumbers and
Steamfitters Health and Welfare Fund (“the Fund”). The Fund is run by a group
of people called the Board of Trustees; the Trustees include Local 72
representatives and representatives from employers that employ Local 72
members (“Contributing Employers”).
Over the last two years, the Board of Trustees has issued a number of
communications indicating that changes are necessary in order to bring the
Fund’s expenses in line with income. The Trustees have been working diligently
towards achieving a balanced budget for the Fund in order to protect its long
term financial health and provide you with the best benefits available using the
monies paid into the Fund.
Last year, changes were made to increase income to the Fund in a balanced
way, without placing all of the burden of change on one group or entity. Local
72, Contributing Employers and Participants all came together to be part of the
solution. Participants began contributing towards dependent coverage;
Contributing Employers increased the Health & Welfare Fund contribution by
$1.39 per hour; Local 72 reallocated contributions from the Pipe Fund and the
Joint Apprenticeship and Training Trust Fund; the Mechanical Contractors
Association reallocated contributions from the MIC Management Fund.
Increasing income to the Fund is half of the equation in establishing a balanced
budget. This year, the Trustees must focus on plan design changes that are
necessary to reduce plan expenses and bring them in line with income. The
following pages describe the benefit changes which will be effective April 1,
2018. Please carefully review this notice and contact NEBA with any questions.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Jarrett Wade
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. James K. Estabrook
Lindabury, McCormick,
Estabrook & Cooper, P.C.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
Summary of Material Modifications – April 1, 2018
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta
Plumbers and Steamfitters Health and Welfare Fund (the “Fund”). This SMM modifies the language found in
your Summary Plan Description (SPD). All statements made in this document are subject to the terms and
conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan
Document, the Plan Document will govern. As always, please feel free to call the Plan’s Third Party
Administrator, National Employee Benefits Administrators, Inc. (“NEBA”) at (888) 365-0072 with any
questions. Copies of the SPD and Plan Document are available for review at any time during normal working
hours at NEBA’s offices.
Benefit Changes Applicable to the Non-Residential Plan effective April 1, 2018:
Out of Pocket Maximum
The Out of Pocket Maximum will be adjusted annually to match the Federal
limit set by the U.S. Department of Health and Human Services. Medical and
Prescription Drug benefits fall under one combined Out of Pocket maximum.
$7,350 per covered individual
$14,700 per family
Deductible
Medical and Rx benefits fall under one combined deductible.
$1,200 per covered individual
$3,600 per family
Physician Office Visit to Treat Illness or Injury
Also applies to office visits to Urgent Care centers and Convenience Care
centers. Does not apply to chiropractors.
$50 copay for Office Evaluation
LiveHealth Online
LiveHealth Online is a 24/7 service that connects members with board-
certified doctors through a two-way, live video chat from their smartphone,
tablet or computer with a webcam. Members can get medical advice, a
diagnosis and even a prescription.
$0 Copay
No Cost to You
Medical Benefits Coinsurance 30%
Prescription Drug Benefits Coinsurance
See OptumRx Formulary to determine which category your prescription drug
falls under.
15% for Generic drugs
35% for Preferred drugs
50% for Non-Preferred drugs
Emergency Room $500 Specific Deductible per
Visit
*Also subject to Plan Deductible

PLAN CHANGES
WHAT DO THEY MEAN?
What is an Out of Pocket maximum? The Out of Pocket maximum is a
financial protection for you that is built in to your plan. This is the maximum amount
you will have to pay in deductibles, copays and coinsurance for your covered in-network claims.
Once you have met this maximum, the plan will pay 100% of your covered in-network claims.
You earn credit towards meeting your Out of Pocket maximum each time you incur covered expenses
with your in-network healthcare providers. For example, if you receive services at a hospital and incur a
$100 charge towards your deductible, when your claim is processed, the plan will credit you with meeting
$100 towards your Out of Pocket maximum. Medical and Prescription drug expenses count towards your
Out of Pocket maximum.
What will my deductible be? You must pay all the costs up to the deductible amount
before the plan begins to pay for covered services you use. Your deductible is waived for
some services. Your deductible counts towards your Out of Pocket Maximum and applies to both
medical and prescription drug benefits.
What will I pay for a primary care or specialist doctor’s office visit
to treat an injury or illness? A set office visit copay allows you to plan
and budget for doctors’ visits. Instead of paying a percentage of an unknown
charge, you will know exactly how much you have to pay with an office visit copay benefit.
(Labs and other services performed during the office visit are subject to your deductible and coinsurance).
Continued…
Effective April 1, 2018, your copay for visiting an in-network primary care doctor or
specialist to treat an illness or injury will be $50. Your deductible will not apply to
doctors’ visits. *Not applicable to chiropractors.
Effective April 1, 2018, your Out of Pocket maximum will be $7,350 per covered
Individual or $14,700 per Family.
Effective April 1, 2018, your deductible will be $1,200 per covered individual, or
$3,600 per family. Your deductible does not apply to wellness visits or physicians’
office evaluation charges ( other than a chiropractor).

PLAN CHANGES
WHAT DO THEY MEAN?
What will I pay for other medical services? After you meet your deductible, the
plan covers a percentage of your claims and you cover the remaining percentage, called
your coinsurance. Your coinsurance counts towards your Out of Pocket Maximum.
What will I pay for prescription drugs? After you have met your deductible, the
plan covers a percentage of your prescription drug claims and you cover the remaining
percentage, called your coinsurance. Your coinsurance level depends on the
classification of your prescription drug as either Generic, Preferred or Non-Preferred.
See your Optum Rx Formulary to determine your drug’s classification. Your deductible and coinsurance
count towards your Out of Pocket Maximum.
What if I have an Emergency? The Board of Trustees wants you to
receive the most appropriate care for your situation. Sometimes that means
going to a hospital Emergency Room; however, consider this: the average hospital
Emergency Room claim is about ten times costlier than an Urgent Care center claim.
Effective April 1, 2018, your additional deductible for visiting a hospital Emergency
Room will be $500. You can save money by using an Urgent Care Center, Retail
Health Clinic, or LiveHealth Online.
Effective April 1, 2018, your coinsurance percentage will be 30% for services subject
to coinsurance.
Effective April 1, 2018, your coinsurance for prescription drugs will depend on what
type of medication you are receiving.
Generic Medication…………………..15% Coinsurance
Preferred Medication…………………35% Coinsurance
Non-Preferred Medication…………50% Coinsurance

PLAN CHANGES
WHAT DO THEY MEAN?
The wait times are usually much shorter than at an ER and you can avoid the $500 specific deductible that applies to each ER visit.

31709GAMENBGA Rev. 07/14
LiveHealth Online® Easy, fast doctor visits. All from the comfort of your own computer or mobile device.
Talk to a doctor today, tonight, anytime — 365 days a year. Just enroll at livehealthonline.com or on the free mobile app.

*As legally permitted in certain states.
LiveHealth Online is the trade name of Health Management Corporation, a separate company providing telehealth services on behalf of Blue Cross and Blue Shield of Georgia.
Blue Cross and Blue Shield of Georgia, Inc. is an independent licensee of the Blue Cross and Blue Shield Association. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association.
Now you can get the health care you need without all the hassleHave a health question? Under the weather? With LiveHealth Online, you don’t have to schedule an appointment, drive to the doctor’s offi ce, and then wait for your appointment. In fact, you don’t even have to leave your home or offi ce. Doctors can answer questions, make a diagnosis, and even prescribe basic medications when needed.*
With LiveHealth Online, you get:
Immediate doctor visits through live video.
Your choice of U.S. board-certifi ed doctors.
Help at a cost of only $49 per visit, subject to deductible and coinsurance.
Private, secure and convenient online visits.
What are the qualifi cations of the doctors you consult via LiveHealth Online?
U.S. board-certifi ed.
Average 15 years practicing medicine.
Mostly primary care physicians.
Specially trained for online visits.
When can you use LiveHealth Online?
As always, you should call 911 with any emergency. Otherwise, you can use LiveHealth Online whenever you have a health concern and don’t want to wait. Doctors are available 24 hours a day, seven days a week, 365 days a year. Some of the most common uses include:
Cold and fl u symptoms such as a cough, fever and headaches
Allergies
Sinus infections
Family health questions
Start a conversation now.
Just enroll for free at livehealthonline.com or on the app, and you’re ready to see a doctor.
play.google.com/store
apple.com
Download the app now!
Available at no cost toeligible Participants of
the Atlanta Plumbers &Steamfitters Healthand Welfare Fundeffective April 1,
2018!

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: All Plan Participants
From: Board of Trustees
Date: April 25, 2017
RE: Important Announcement regarding Dependent Coverage
As a member of Plumbers, Pipefitters, & HVACR Technicians Local 72 (“Local
72”) you receive health care benefits through the Atlanta Plumbers and
Steamfitters Health and Welfare Fund (“the Fund”). The Fund is run by a group
of people called the Board of Trustees; the Trustees include Local 72
representatives and representatives from employers that employ Local 72
members (“Contributing Employers”).
On an ongoing basis, the Board of Trustees monitors the financial status of the
Fund; their focus is to provide you with the best benefits available using the
monies paid into the Fund. Over the last year and a half, the Board of Trustees
has issued a number of communications indicating that changes are necessary
in order to bring the Fund’s expenses in line with income. The Trustees have
been working diligently towards achieving a balanced budget for the Fund in
order to protect its long term financial health.
The Trustees have considered and continue to consider many different ways
to increase income and reduce expenses in a balanced way, without placing all
of the burden of change on one group or entity. The Trustees believe that this
problem is one that can only be solved together, with participation and
compromise from all parties. Local 72, Contributing Employers and Participants
must all be part of the solution.
The following pages describe how the Fund’s eligibility rules are changing with
respect to dependent coverage. In order to maintain coverage for
dependents, your action will be required. Please carefully review this
memorandum and Summary of Material Modifications (SMM) and contact
NEBA with any questions.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Terry Sinyard
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. Grant Willis
Willis Mechanical, Inc.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
These important steps are being taken with the sole focus of preserving the financial integrity of the Fund
so that valuable benefits can continue to be provided to you now and in the future.
Active Employees and Non-Bargaining Unit Employees
• Spousal coverage will continue to be available to non-bargaining unit employees and bargaining unit
employees working in a classification under the Collective Bargaining Agreement (CBA) which
requires Health and Welfare Fund contributions at a rate that is at least equal to the Journeyman
Health and Welfare contribution rate. Coverage for dependent children will continue to be available
to non-bargaining unit employees and bargaining unit employees working in all classifications.
Please refer to your Collective Bargaining Agreement for specific contribution rates.
• As of the date of this memo, CBA classifications with a Health and Welfare contribution rate at least
equal to the Journeyman Health and Welfare contribution rate include:
• 1st - 5th year Apprentice
• Mechanical Equipment Serviceman
• Journeyman
• Foreman, Crew Foreman, & General Foreman
• Provisional Journeyman
• Tradesman (Not Including Pipe Tradesman)
• Spousal coverage is no longer available to employees working in a CBA classification which requires
Health and Welfare Fund contributions at a rate that is less than the Journeyman Health and Welfare
contribution rate. This coverage was eliminated effective April 1, 2017 and notice was provided in a
memo dated January 31, 2017. As of April 1, 2017, these classifications include Helper, Pipe Tradesman
and Residential. Please refer to your Collective Bargaining Agreement for specific contribution rates.
• Eligible employees working in a classification that permits spousal coverage must determine
whether or not they wish to elect spousal coverage. Employees should consider all coverage options
available for their spouse, such as coverage through his/her employer or the Healthcare Marketplace.
Loss of coverage under the Atlanta Plumbers and Steamfitters Health and Welfare Fund may trigger
special enrollment rights for spouses who have lost coverage, which would allow them to enroll in
another group health plan or in a plan available through the Healthcare Marketplace at
Healthcare.gov.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
• Each employee who elects to cover his/her spouse as a dependent must make a weekly contribution
of $25, effective the first payroll period in June 2017. First Year Apprentices are exempt from this
contribution requirement. Contribution payments will be collected by Contributing Employers via
payroll deductions. Contribution rates are set by the Board of Trustees and may be modified
periodically.
• Each employee who elects to cover his/her dependent child(ren) must make a contribution for
coverage. First Year Apprentices are exempt from this contribution requirement.
• The contribution requirements for dependent child(ren) coverage vary. First Year Apprentices are
exempt from this contribution requirement.
o The dependent child(ren) contribution rate for employees working in a classification under the
Collective Bargaining Agreement (CBA) which requires Health and Welfare Fund contributions
at a rate that is at least equal to the Journeyman Health and Welfare contribution rate has
been set at $5 per week, effective the first payroll period in June 2017. This rate is for all
dependent children covered by the employee; it is not a per-child rate. Contribution
payments will be collected by Contributing Employers via payroll deductions.
o The dependent child(ren) contribution rate for employees working in a classification under the
Collective Bargaining Agreement (CBA) which requires Health and Welfare Fund contributions
at a rate that is less than the Journeyman Health and Welfare contribution has been set at $250
per month, per child. This contribution requirement was effective April 1, 2017 and notice was
provided in a memo dated January 31, 2017. As of April 1, 2017, these classifications include
Helper, Pipe Tradesman and Residential. Contribution payments must be self-paid by
employees.
• Employees who are out of work may elect to pay their dependent coverage contributions by
withdrawing hours from their bank. One hour will be worth the value of the then-current hourly
Journeyman Health & Welfare contribution rate. For example, based on the current rate of $5.51,
4.54 hours may be withdrawn in order to pay a $25.00 contribution. ($25.00 / $5.51 = 4.54 hours).
Employees will be required to complete a request form in order to do this. Employees may elect to self-
pay the contribution instead.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
• Each year, during an “Open Enrollment” period, employees must decide whether or not to cover
their dependent spouses and/or children for the upcoming year. Enrollment elections may be made
using a paper form or online through the Member Portal website; details will be provided in a separate
Open Enrollment notice.
• Employees may not change their dependent coverage election during the year, outside of the Open
Enrollment period, unless a Qualifying Event has occurred. Qualifying Events include life changes
such as marriage, divorce and birth of a child.
• The first Open Enrollment will be conducted from May 1st – May 20th for coverage effective
September 1, 2017. During this Open Enrollment period, employees will be given the opportunity to
elect dependent spouse and/or dependent child(ren) coverage effective September 1, 2017.
• An in-person Open Enrollment meeting will be held at the Local 72 Union Hall from 8:00 a.m. – 5:00
p.m. on May 2, 2017. Further announcements will be made regarding in-person meetings to be
scheduled at large employer sites.
• Subsequent Open Enrollments will be conducted each September for coverage changes effective the
following January. During each annual Open Enrollment, employees may enroll new dependents, drop
existing dependents or elect not to carry dependent coverage.
• Employees who do not elect coverage during Open Enrollment will lose coverage for their
dependent spouse and/or child(ren) effective August 31, 2017. Dependents may be re-enrolled
during the next Open Enrollment period for coverage effective January 1, 2018.
• Spouses and dependent children who lose coverage will be provided with a certificate of coverage
showing the date coverage was lost. Spouses and dependent children may need this certificate in
order to enroll in another plan.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Early Retirees Who Retire on or After March 1, 2018
• Early retirees are those retirees who elect retiree coverage prior to age 65.
• Each early retiree who retires on or after March 1, 2018, who elects to cover his/her spouse as a
dependent, must make a monthly contribution of $108.34, in addition to the regular retiree
contribution. Contribution rates are set by the Board of Trustees and may be modified periodically.
• Each early retiree who retires on or after March 1, 2018, who elects to cover his/her dependent
child(ren), must make a monthly contribution of $21.67, in addition to the regular retiree
contribution. Contribution rates are set by the Board of Trustees and may be modified periodically.
Enclosed with this memorandum is a Summary of Material Modifications (SMM) which describes these
changes in detail. The SMM should be kept with your Summary Plan Description (SPD). Also enclosed is
an Open Enrollment notice which provides details regarding how you may elect spousal and dependent
child(ren) coverage. As always, please feel free to call the Plan’s Third Party Administrator, National
Employee Benefits Administrators, Inc. (“NEBA”) at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – June 1, 2017
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta
Plumbers and Steamfitters Health and Welfare Fund (the “Fund”). This SMM modifies the language found
in your Summary Plan Description (SPD). All statements made in this document are subject to the terms
and conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan
Document, the Plan Document will govern. Copies of the SPD and Plan Document are available for review
at any time during normal working hours at NEBA’s offices.
Active Employees and Non-Bargaining Unit Employees
Eligibility Changes – Dependent Coverage
• Effective for coverage September 1, 2017 and after, non-bargaining unit employees and bargaining
unit employees working under Collective Bargaining Agreement (CBA) classifications that permit
spousal coverage must make an election to cover their spouse as a dependent. As of the date of this
memo, the classifications include:
• 1st - 5th year Apprentice
• Mechanical Equipment Serviceman
• Journeyman
• Foreman, Crew Foreman, & General Foreman
• Provisional Journeyman
• Tradesman (Not Including Pipe Tradesman)
• Each employee who elects to provide coverage to a dependent spouse under the Fund must make a
weekly contribution of $25. First year Apprentices are exempt from this contribution requirement.
Weekly spousal coverage contributions will be collected via payroll deductions.
• Effective for coverage September 1, 2017 and after, non-bargaining unit employees and bargaining
unit employees working in a classification under the Collective Bargaining Agreement (CBA) which
requires Health and Welfare Fund contributions at a rate that is at least equal to the Journeyman
Health and Welfare contribution rate must make an election to cover their dependent child(ren) under
the Fund and make a weekly contribution of $5, regardless of the number of dependent children

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
covered. First year Apprentices are exempt from this contribution requirement. Weekly dependent
child(ren) coverage contributions will be collected via payroll deductions.
• Employees who are out of work may elect to pay their dependent spouse and/or dependent child(ren)
coverage contributions by withdrawing hours from their bank. One hour will be worth the value of
the then-current hourly Journeyman Health and Welfare contribution rate.
Early Retirees Who Retire on or After March 1, 2018
Eligibility Changes – Dependent Coverage
• Early retirees are those retirees who elect retiree coverage prior to age 65.
• Each early retiree who retires on or after March 1, 2018, who elects to cover his/her spouse as a
dependent, must make a monthly contribution of $108.34, in addition to the regular retiree
contribution.
• Each early retiree who retires on or after March 1, 2018, who elects to cover his/her dependent
child(ren), must make a monthly contribution of $21.67, in addition to the regular retiree contribution.
As always, please feel free to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc. (“NEBA”) at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365.0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: Pipe Tradesmen, Helper and Residential Plan Participants of the
Atlanta Plumbers and Steamfitters Health and Welfare Fund
From: Board of Trustees
Date: January 31, 2017
RE: Important Announcement regarding Plan Changes
As a member of Plumbers, Pipefitters, & HVACR Technicians Local 72 (“Local
72”), you receive health care benefits through the Atlanta Plumbers and
Steamfitters Health and Welfare Fund (the “Fund”). The Fund is run by a group
of people called the Board of Trustees; the Trustees include Local 72
representatives and representatives from employers that employ Local 72
members.
On an ongoing basis, the Board of Trustees monitors the financial status of the
Fund; their focus is to provide you with the best benefits available using the
monies paid into the Fund by your employers. Sometimes it is necessary for
them to modify, reduce or eliminate benefits in order to protect the long term
financial health of the Fund, which is also in the best interest of participants.
When the Trustees are faced with these difficult decisions, they carefully
consider their options and aim to protect the benefits which they believe are
most important to participants. The Trustees have determined, with the
assistance of their professional advisors, that changes are necessary.
First, the current Pipe Tradesmen, Helper and Residential Plan benefits
program is costing far more in claims expenses than it is receiving in
employer contributions; therefore, effective April 1, 2017, the existing
benefits have been modified so that expected expenses more closely
match expected contributions. Enclosed with this notice is an updated
Summary of Benefits and Coverage (SBC) which describes your new
benefits.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Terry Sinyard
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. Grant Willis
Willis Mechanical, Inc.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365.0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Second, the current contributions for the Pipe Tradesmen, Helper and Residential Plan do not
support providing coverage for dependents at no additional cost to employees; therefore,
effective April 1, 2017, coverage will be provided at no cost for employees only.
Effective April 1, 2017, coverage for dependent children may be elected at a cost, which must be
self-paid by the Participant.
Effective April 1, 2017, dependent spouses will no longer be covered under the Pipe Tradesmen,
Helper and Residential Plan.
Please know that these important steps were taken with the sole focus of preserving the financial
integrity of the Fund so that good benefits can continue to be provided to you now and in the future.
Enclosed with this memorandum is a Summary of Material Modifications (SMM) which describes these
changes in detail. The SMM should be kept with your Summary Plan Description (SPD). As always, please
feel free to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc.
(“NEBA”), at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365.0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – April 1, 2017
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta
Plumbers and Steamfitters Health and Welfare Fund (the “Fund”). This SMM modifies the language found
in your Summary Plan Description (SPD). All statements made in this document are subject to the terms
and conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan
Document, the Plan Document will govern. Copies of the SPD and Plan Document are available for review
at any time during normal working hours at the Plan’s office.
Benefit Changes effective April 1, 2017
The Pipe Tradesmen, Helper and Residential Plan benefits have been modified in accordance with the
enclosed Summary of Benefits and Coverage (SBC).
Eligibility Changes effective April 1, 2017
The Pipe Tradesmen, Helper and Residential Plan no longer includes coverage for dependent spouses.
The Pipe Tradesmen, Helper and Residential Plan no longer affords coverage to dependent children at
no cost. Participants may elect to cover Dependent children at a cost of $250 per month, per child.
Please contact NEBA at 1-888-365-0072 if you wish to elect coverage for dependent children.
Your dependent coverage contribution check must be payable to the Atlanta Plumbers and Steamfitters
Health and Welfare Fund and must be received by NEBA no later than the 15th day of the month prior to
the coverage month, as shown in the examples below.
Coverage Month Dependent Child Contribution Due Date April March 15th May April 15th June May 15th July June 15th
August July 15th September August 15th
etc.…
As always, please feel free to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc. (“NEBA”) at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – January 1, 2017
This document is a “Summary of Material Modifications” (SMM) which
describes changes to the Atlanta Plumbers and Steamfitters Health and
Welfare Fund (the “Fund”). This SMM modifies the language found in your
Summary Plan Description (SPD). All statements made in this document are
subject to the terms and conditions of the Plan Document. If there is a
discrepancy between the SPD or this SMM and the Plan Document, the Plan
Document will govern. Copies of the SPD and Plan Document are available for
review at any time during normal working hours at the Plan’s office.
Effective January 1, 2017, charges for the purchase and fitting of
hearing aids at Costco Wholesale stores and retail locations will be
covered according to the hearing aid limitations outlined in the
Schedule of Benefits. Although Costco Wholesale stores do not
participate in the Anthem/Blue Cross Blue Shield provider networks,
hearing aid services incurred in a Costco Hearing Center will be
considered a covered expense subject to the in-network Hearing Aid
benefit.
If you have any questions, please contact National Employee Benefits
Administrators, Inc. at (888) 365-0072.
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Terry Sinyard
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. Ken Harbour
Cleveland Mechanical
Services
Mr. John McKenney
McKenney’s Inc.
Mr. Grant Willis
Willis Mechanical, Inc.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: Participants in the Atlanta Plumbers and Steamfitters
Health and Welfare Fund
From: Board of Trustees
Date: May 20, 2016
RE: Important Announcement regarding Plan Changes
As a member of Plumbers, Pipefitters, & HVACR Technicians Local 72 (“Local
72”) you receive health care benefits through the Atlanta Plumbers and
Steamfitters Health and Welfare Fund (“the Fund”). The Fund is run by a group
of people called the Board of Trustees; the Trustees include Local 72
representatives and representatives from employers that employ Local 72
members.
On an ongoing basis, the Board of Trustees monitors the financial status of the
Fund; their focus is to provide you with the best benefits available using the
monies paid into the Fund by your employers. Sometimes it is necessary for
them to modify, reduce or eliminate benefits in order to protect the long term
financial health of the Fund, which is also in the best interest of participants.
When the Trustees are faced with these difficult decisions, they carefully
consider their options and aim to protect the benefits which they believe are
most important to participants. The Trustees have determined, with the
assistance of their professional advisors, that changes are necessary.
First, the current dental and vision programs are no longer affordable
for the Fund to continue to provide at this time; therefore, effective
June 1, 2016, the existing dental and vision benefit plans are being
suspended. It is the intent of the Trustees to reinstate the benefits
after stabilizing the financial status of the Fund.
The decision to suspend these benefits was not made lightly; it is important to
the Trustees that the Fund be in a position to offer dental and vision coverage
in the future and they will continue to monitor the finances and look for an
Board of Trustees
Union Trustees
Mr. Jeff Housworth
Co-Chairman
UA Local Union 72
Mr. Terry Newsome, Jr.
UA Local Union 72
Mr. Steve Newsome
UA Local Union 72
Mr. Terry Sinyard
UA Local Union 72
Mr. Greg Stephens
UA Local Union 72
Employer Trustees
Mr. Jon Sterling
Co-Chairman
Maxair Mechanical, Inc.
Mr. Gary Fowler
Mechanical Contractors
Association of Georgia
Mr. John Helms
W.B. Wallis & Company
Mr. John McKenney
McKenney’s Inc.
Mr. Grant Willis
Willis Mechanical, Inc.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
affordable way to offer these benefits when the suspension is lifted. Dental and vision claims incurred
on or before May 31, 2016 will continue be processed in accordance with the plan of benefits in effect
at the time the claims were incurred.
Second, an increase in the Emergency Room deductible is necessary to more accurately reflect the
cost of receiving benefits in an Emergency Room setting. Effective June 1, 2016, the Emergency
Room deductible has increased to $250 per visit.
These benefit changes are reflected in the new Summary of Benefits and Coverage (SBC) that was recently
sent to your home, in April 2016.
Third, the Trustees have determined that they can obtain better discounts on healthcare services
by changing Preferred Provider Networks.
Effective September 1, 2016, Anthem Blue Cross Blue Shield of Georgia will replace Cigna as the Preferred
Provider Organization. Blue Cross Blue Shield of Georgia is the largest insurer in Georgia. They have over
16,000 physicians, over 130 hospitals and an excellent reputation. They were able to provide a significant
improvement in discount levels over the current Cigna provider network. Please expect some additional
communications in the coming months which more fully explain the transition from Cigna to Blue Cross
Blue Shield of Georgia.
Fourth, the Trustees have determined that the current method of delivering healthcare benefits
to retired participants does not take full advantage of subsidies and discounts that Medicare
affords plans that cover Medicare-eligible retirees. As a result, the Trustees have decided to
change the way benefits are delivered to Medicare-eligible retirees.
Effective September 1, 2016, the Board of Trustees is pleased to announce that they have established a
stand alone retiree plan for retired participants of the Atlanta Plumbers and Steamfitters Health and
Welfare Fund.
Effective September 1, 2016, coverage will be provided to Medicare-eligible retirees and their Medicare-
eligible dependents under the new plan, the Atlanta Plumbers and Steamfitters Retiree Health and
Welfare Fund (“the Retiree Fund”).

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Non-Medicare-eligible retirees and dependents will continue to be provided coverage under the active
plan at this time.
Medicare-eligible retirees and their Medicare-eligible spouses covered under the Retiree Fund will receive
a Health Reimbursement Arrangement (HRA) account to help them pay for new coverage through a
private Medicare exchange. The exchange provides individuals with a choice of benefit plans at a defined
cost. The Trustees have carefully evaluated the numerous plan options available via the exchange to
determine the HRA funding level that will enable all Medicare-eligible retirees and their Medicare-eligible
spouses to obtain coverage similar to their current coverage, with the potential for some participants to
reduce their costs. The Trustees have set the funding level of the HRA account at $200 per month per
covered Medicare-eligible retiree and $200 per month per Medicare-eligible spouse of a covered retiree.
The Trustees understand that this method of delivering benefits is very different than what has been done
in the past, so they have selected RightOpt, a private health insurance exchange, to help Medicare-eligible
retirees and spouses navigate their available plan options and enroll in the plans that best meet their
needs. RightOpt has representatives, called Enrollment Advocates, who will work one on one with each
individual to be sure that they understand all of the options available to them and walk them through the
process of enrolling. There is no cost to use RightOpt’s services. RightOpt will send you more information
and their Enrollment Advocates will reach out to you to explain next steps.
Since your current group coverage will end on September 1, 2016, you will enroll in new coverage through
RightOpt from July 1 through August 19. This will ensure your new coverage is in place and you do not
have a gap in coverage.
Please know that these important steps were taken with the sole focus of preserving the financial
integrity of the Fund so that good benefits can continue to be provided to you and your families now
and in the future.
Enclosed with this memorandum is a Summary of Material Modifications (SMM) which describes these
changes. The SMM should be kept with your Summary Plan Description (SPD). As always, please feel free
to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc. (“NEBA”) at
(888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Summary of Material Modifications – June 1, 2016
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta
Plumbers and Steamfitters Health and Welfare Fund (the “Fund”). This SMM modifies the language found
in your Summary Plan Description (SPD). All statements made in this document are subject to the terms
and conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan
Document, the Plan Document will govern. Copies of the SPD and Plan Document are available for review
at any time during normal working hours at the Plan’s office.
Effective June 1, 2016, the self-insured dental and vision plans have been temporarily suspended.
Effective June 1, 2016, the Emergency Room Deductible has increased to $250.
Effective September 1, 2016, Anthem Blue Cross Blue Shield of Georgia will replace Cigna as the
Preferred Provider Organization.
Effective September 1, 2016, retired Medicare-eligible participants of the Atlanta Plumbers and
Steamfitters Health and Welfare Fund and their Medicare-eligible dependents will no longer be
provided coverage through the Fund; retired Medicare-eligible Participants and their Medicare-
eligible dependents will be provided coverage under a new stand alone retiree plan through the
Atlanta Plumbers and Steamfitters Retiree Health and Welfare Fund (“Retiree Fund”).

Atlanta Plumbers and Steamfitters
Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
To: Participants in the Atlanta Plumbers and Steamfitters Health and Welfare Fund
From: Board of Trustees
Date: March 31, 2016
RE: Eligibility Changes
The purpose of this Notice is to inform you that the Trustees of the Health and Welfare Fund have changed
some of the rules governing how eligibility is determined based on work performed on and after May 1,
2016.
Eligibility which is based on work performed before May 1, 2016 will be determined in accordance with
the rules in effect at that time.
The enclosed document sets forth the new rules in detail. Here are the highlights:
Changes applicable to new Participants and Participants that have been ineligible for 6 or more
consecutive months:
Employees who lose coverage for a period of six (6) consecutive months or more must meet the
initial eligibility requirements in order to be reinstated. Previously, Employees who lost coverage
had to meet the continuing eligibility requirements to be reinstated.
There are two levels of coverage for initial eligibility with different minimum hour requirements.
The first level includes eligibility for the Employee and his or her dependent children; the second
level includes eligibility for the Employee, dependent children and spouse. Previously, there was
one level of coverage which included the Employee, dependent children and spouse.
The number of hours required for initial eligibility for the Employee and his or her dependent
children has increased to 800 hours within a twelve (12) consecutive month period. The number
of hours required for initial eligibility for the Employee, dependent children and spouse has
increased to 1,200 hours within a twelve (12) consecutive month period. Previously, the number
of hours required for initial eligibility was 390 hours in a three (3) consecutive month period.

Page 2
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E., Suite 72 Atlanta, GA 30316
3715 Northside Parkway, Suite 2-495 Atlanta, GA 30327
Changes applicable to Apprentices attending school:
Apprentices attending school must meet the same continuing eligibility requirements as all other
classifications. Previously, Apprentices attending school had a reduced minimum hour requirement for
continuing eligibility.
Changes applicable to the Residential Job Classification:
The Contribution (Work) Months and Benefit Months will be the same for all classifications.
Previously, the Residential classification had a shorter administrative lag between the Contribution
(Work) Month and the Benefit Month.
Please review the enclosed notice for further details regarding the changes. As always, please feel
free to call the Plan’s Third Party Administrator, National Employee Benefits Administrators, Inc.
(“NEBA”) at (888) 365-0072 with any questions.

Atlanta Plumbers and Steamfitters Health and Welfare Fund
c/o National Employee Benefits Administrators, Inc. 1 (888) 365-0072
ADMINISTRATIVE MANAGER:
National Employee Benefits Administrators, Inc. 1.888.365-0072 (Toll Free) • 954.266.6322 • 954.266.2079 (Fax)
www.nebainc.com
2010 N.W. 150th Ave, Suite 100 Pembroke Pines, FL 33028
374 Maynard Terrace, S.E. Suite 72
Atlanta, GA 30316
3715 Northside Parkway Suite 2-495
Atlanta, GA 30327
Summary of Material Modifications – May 1, 2016
This document is a “Summary of Material Modifications” (SMM) which describes changes to the Atlanta Plumbers and Steamfitters Health and Welfare Fund (the “Plan”). This SMM modifies the language found in your Summary Plan Description (SPD). All statements made in this document are subject to the terms and conditions of the Plan Document. If there is a discrepancy between the SPD or this SMM and the Plan Document, the Plan Document will govern. Copies of the SPD and Plan Document are available for review at any time during normal working hours at the Plan’s office. The Board of Trustees has approved the following changes to the Rules of Eligibility effective for work performed on or after May 1, 2016, unless otherwise noted herein.
Changes to the Rules of Eligibility Transition Rule Employees who have earned coverage for future periods based on work performed prior to May 1, 2016 will remain eligible for coverage in accordance with the eligibility rules in effect prior to May 1, 2016. Please refer to your Summary Plan Description (SPD) for a full description of these rules. Eligibility Rules Effective for Work Performed on and after May 1, 2016 Initial Eligibility | All Classifications Initial eligibility for coverage for the Employee and his or her eligible dependent children begins on the first day of the Benefit Month that corresponds to the first Contribution (Work) Month in which contributions for at least 800 hours have been made on behalf of a bargaining unit Employee within a period of twelve (12) consecutive months or less. Initial eligibility for coverage for the Employee’s eligible spouse begins on the first day of the Benefit Month that corresponds to the first Contribution (Work) Month in which contributions for at least 1,200 hours have been made on behalf of a bargaining unit Employee within a period of twelve (12) consecutive months or less. Bargaining unit Employees who have been ineligible for benefits for a period of six (6) or more consecutive calendar months are treated in the same manner as bargaining unit Employees who have not been previously eligible for benefits.

Page 2
Continuing Eligibility |All Classifications Once a bargaining unit Employee satisfies the Initial Eligibility requirements, eligibility for coverage shall continue thereafter for each subsequent Benefit Month for which at least 130 hours of contributions are made on behalf of the bargaining unit Employee, withdrawn from the bargaining unit Employee’s Hour Bank or self-paid by the bargaining unit Employee for the corresponding Contribution (Work) Month. This Continuing Eligibility Rule shall apply to Apprentices attending school, effective for work performed on and after May 1, 2016. Contribution (Work) Months and the corresponding Benefit Months shall be as follows. Contribution (Work) Months and Benefit Months | All Classifications All bargaining unit Employees who satisfy the minimum hour requirement during a Contribution (Work) Month will be eligible for benefits during the Benefit Month that corresponds to the Contribution (Work) Month during which the hour requirement was satisfied. The Contribution (Work) Months and Benefit Months are as follows:
Contribution (Work) Month Benefit Month
October
November
December
January
February
March
April
May
June
July
August
September
January
February
March
April
May
June
July
August
September
October
November
December
Reinstatement of Eligibility A bargaining unit Employee whose eligibility for benefits has been terminated will have his or her eligibility reinstated on the first day of the Benefit Month that corresponds to the Contribution (Work) Month during which at least 130 hours of contributions are made on the Employee’s behalf. Bargaining unit Employees who have been ineligible for benefits for a period of six (6) or more consecutive months are treated in the same manner as bargaining unit Employees who have not been previously eligible for benefits, and may earn eligibility in accordance with the Initial Eligibility Rules described herein. If you have any questions, please contact National Employee Benefits Administrators, Inc. at 1 (888) 365-0072.

Atlanta Plumbers & Steamfitters Health and Welfare Fund c/o National Employee Benefits Administrators, Inc.
2010 N.W. 150th Avenue, Suite 100 | Pembroke Pines, FL 33028 1 (888) 365-0072 | Fax (954) 266-2079
Date: January 1, 2016 To: All Eligible Participants From: Board of Trustees Re: 2016 Forms
Happy New Year! In preparation for the year ahead, NEBA has designed a number of forms for your use in 2016. Enclosed are the following documents: Annual Claim Form - This form provides NEBA with updated information about you and your enrolled
dependents. You must file this form on an annual basis. If NEBA has not received your annual claim form
and a claim is submitted for you or your enrolled dependents, the claim will be denied and a request for the
form will be sent to you. You will have a limited period of time to return the form in order to have your
claims reprocessed. Please refer to your Summary Plan Description for details regarding claims filing
deadlines. File the claim form at the beginning of each year to promote more efficient processing of your
claims.
PHI Authorization Form – This form enables you and/or your enrolled dependents to authorize NEBA staff
to speak with other individuals about your Protected Health Information (PHI), including eligibility and
claims. This form is only required if you wish to authorize this.
Accident/Injury Details Form – This form may be requested from you if NEBA receives a claim with a
diagnosis that could be related to an accident or an injury. This form helps NEBA staff determine if your
claim should be covered by the Atlanta Plumbers & Steamfitters Health and Welfare Fund and if additional
information is needed. If you have an accident, or suffer an injury, you should submit this form to NEBA.
There are several ways to return the forms to NEBA.
Visit https://www.nebainc.com/SendFile.aspx and use the Secure File Upload. If you visit the site on your mobile device you can use your device camera to upload photos of the documents. Photos must be clear enough to read and you must include a photo of all pages of the form(s).
Visit https://luxsci.com/perl/public/securesend.pl and register to use the Secure Send Encrypted Email Portal. The portal allows you to create a free email account only for use in sending emails to NEBA in an encrypted fashion.
Mail them to NEBA at 2010 N.W. 150th Avenue, Suite 100 | Pembroke Pines, FL 33028.
Fax them to NEBA at (954) 266-2079.
If you have any questions, please call NEBA at 1-888-365-0072.

ATLANTA PLUMBERS & STEAMFITTERS LOCAL 72
FRINGE BENEFIT FUNDS
DO YOU HAVE UNFILED PRESCRIPTION DRUG
CLAIMS?
FILE THEM BY 12/23/15 TO AVOID ANY DELAY IN
REIMBURSEMENT
Send claims to Southern Benefit Administrators, Inc. (SBAI) through 12/23/15.
After 12/23/15, send claims to NEBA at 2010 N.W. 150th
Avenue, Ste. 100 Pembroke Pines, FL 33028
NEW ADMINISTRATIVE MANAGER IN 2016
NEBA, Inc. to replace Southern Benefit Administrators, Inc.
If you have unfiled prescription
drug claims, please file them with
SBAI before December 23, 2015.
SBAI will continue to process
prescription claims they receive
through December 31, 2015.
After January 1, 2016, there will
be a short period of time where
processing times will be longer
than usual while NEBA loads
historical data from SBAI into their
systems.
Once this is complete, normal
processing times will resume.
REMINDER: The Board of Trustees of
the Atlanta Plumbers & Steamfitters
Local 72 Fringe Benefit Funds has
selected National Employee Benefits
Administrators (NEBA) to serve as
Administrative Manager to the
Fringe Benefit Funds effective
January 1, 2016. NEBA will replace
Southern Benefit Administrators,
Inc. (SBAI). NEBA can be reached at:
1-888-365-0072 weekdays from 8:00 a.m. – 5:00 p.m. EST.
NEBA will also have a representative
at Local Union 72 to serve you
beginning in early February.
ATLANTA PLUMBERS & STEAMFITTERS LOCAL 72
FRINGE BENEFIT FUNDS
IMPORTANT ANNOUNCEMENT – NEW ADMINISTRATIVE MANAGER EFFECTIVE 1/1/2016
IMPORTANT ANNOUNCEMENT – NEW ADMINISTRATIVE MANAGER EFFECTIVE 1/1/2016
DO YOU HAVE UNFILED PRESCRIPTION DRUG
CLAIMS?
FILE THEM BY 12/23/15 TO AVOID ANY DELAY IN
REIMBURSEMENT
Send claims to Southern Benefit Administrators, Inc. (SBAI) through 12/23/15.
After 12/23/15, send claims to NEBA at 2010 N.W. 150th
Avenue, Ste. 100 Pembroke Pines, FL 33028
NEW ADMINISTRATIVE MANAGER IN 2016
NEBA, Inc. to replace Southern Benefit Administrators, Inc.
REMINDER: The Board of Trustees of
the Atlanta Plumbers & Steamfitters
Local 72 Fringe Benefit Funds has
selected National Employee Benefits
Administrators (NEBA) to serve as
Administrative Manager to the
Fringe Benefit Funds effective
January 1, 2016. NEBA will replace
Southern Benefit Administrators,
Inc. (SBAI). NEBA can be reached at:
1-888-365-0072 weekdays from 8:00
a.m. – 5:00 p.m. EST.
NEBA will also have a representative
at Local Union 72 to serve you beginning in early February.
If you have unfiled prescription
drug claims, please file them with
SBAI before December 23, 2015.
SBAI will continue to process
prescription claims they receive
through December 31, 2015.
After January 1, 2016, there will
be a short period of time where
processing times will be longer
than usual while NEBA loads
historical data from SBAI into their
systems.
Once this is complete, normal
processing times will resume.
December 15, 2015
ATTENTION RETIREES: NEW ADMINISTRATIVE MANAGER IN 2016 NEBA, Inc. to replace Southern Benefit Administrators, Inc. (SBAI)
The Board of Trustees of the Atlanta Plumbers &
Steamfitters Local 72 Fringe Benefit Funds is pleased to
announce that they have selected a new Administrative
Manager to serve the Fringe Benefit Funds effective
January 1, 2016.
ROLE OF THE ADMINISTRATIVE MANAGER
Effective January 1, 2016,
NEBA will take over all of
the day-to-day administra-
tive tasks. This includes
many important tasks such
as issuing retirement
benefit payments. NEBA’s friendly, know-
ledgeable staff will be
available toll free at:
1-888-365-0072
Weekdays from 8:00 a.m.
to 5:00 p.m. EST. You may also visit their
Atlanta or Florida offices in
person.
IMPORTANT ANNOUNCEMENT – NEW ADMINISTRATIVE MANAGER EFFECTIVE JANUARY 1, 2016
WHO IS NEBA?
NEBA stands for “National
Employee Benefits
Administrators, Inc.”
NEBA is a Third Party
Administrator (TPA) that
specializes in
administering benefit
plans that cover
employees working for
Contributing Employers
under Collective
Bargaining Agreements
(CBAs) with various
Unions across the United
States.
NEBA has been in
business for over twenty
(20) years and employs
approximately eighty (80)
Union members covered
under a Collective
Bargaining Agreement
with the United Food and
Commercial Workers Local
Union 1625.
NEBA’s staff looks forward
to being of service to you
and your family beginning
January 1, 2016!
EFFECTIVE
JANUARY 1, 2016,
NATIONAL
EMPLOYEE
BENEFITS
ADMINISTRATORS,
INC. (NEBA) WILL
REPLACE
SOUTHERN
BENEFIT
ADMINISTRATORS
AS THE
ADMINISTRATIVE
MANAGER FOR THE
FRINGE BENEFIT
FUNDS
ATLANTA PLUMBERS & STEAMFITTERS LOCAL 72 FRINGE BENEFIT FUNDS

WHO WILL ISSUE MY PENSION CHECKS?
Southern Benefit Administrators
will issue your January 2016 pension payment.
NEBA will issue your pension payment for February 2016 and after based on the information Southern Benefit Administrators has on file for you.
WHO WILL ISSUE MY 2015 TAX FORM?
NEBA will issue your 1099R for 2015.
DO I NEED TO DO ANYTHING?
Tell NEBA if you have moved or had a change in your bank account where your check is direct deposited.
WHO CAN I CALL IF I HAVE QUESTIONS?
Call NEBA at 1-888-365-0072.
NEBA OFFICE LOCATIONS
Atlanta, GA
3715 Northside Parkway
Suite 2-495
Atlanta, GA 30327
and
Beginning in early February…
Local Union 72
374 Maynard Terrace, S.E.
Atlanta, GA 30316
Jacksonville, FL
8657 Baypine Road
Building 5 – Suite 200
Jacksonville, FL 32256
West Palm Beach, FL
1920 N. Florida Mango Rd.
West Palm Beach, FL 33409
Pembroke Pines, FL
2010 N.W. 150th Avenue
Suite 100
Pembroke Pines, FL 33028

IMPORTANT ANNOUNCEMENT FROM
THE BOARD OF TRUSTEES OF THE
ATLANTA PLUMBERS & STEAMFITTERS
LOCAL 72 FRINGE BENEFIT FUNDS
NEW ADMINISTRATIVE MANAGER
EFFECTIVE JANUARY 1, 2016
Atlanta Plumbers & Steamfitters
Local 72 Fringe Benefit Funds
c/o NEBA, Inc.
2010 N.W. 150th Avenue, Suite 100
Pembroke Pines, FL 33028

November 15, 2015
ATTENTION PARTICIPANTS: NEW ADMINISTRATIVE MANAGER IN 2016
NEBA, Inc. to replace Southern Benefit Administrators, Inc. (SBAI)
The Board of Trustees of the Atlanta
Plumbers & Steamfitters Local 72
Fringe Benefit Funds is pleased to
announce that they have selected a
new Administrative Manager to serve
the Fringe Benefit Funds effective
January 1, 2016. Look for further
communications regarding this
transition, which will be sent during
the month of December.
ROLE OF THE ADMINISTRATIVE MANAGER NEBA to take over all of the functions currently handled by SBAI
Effective January 1, 2016, NEBA will
take over all of the day to day
administrative
functions. This
includes many
important tasks
such as:
collecting fringe
benefit
contributions
from
Contributing
Employers,
determining
eligibility for
health care
benefits,
processing
health care
claims, determining eligibility for
retirement benefits, calculating
retirement benefits, issuing retirement
benefit payments, etc.
NEBA will work closely with the Board
of Trustees and their professional
advisors to deliver excellent
administration services to you.
NEBA has offices to serve you in
Atlanta, as well as three Florida offices
located in
Pembroke Pines,
Jacksonville, and
West Palm Beach.
Their friendly,
knowledgeable
staff will be
available Monday
through Friday
from 8:00 a.m. to
5:00 p.m. Eastern
Standard Time via
telephone. You
may also visit
their offices in
person.
In order to
provide you with convenient access to
information regarding your benefits,
NEBA will also be making available a
mobile-ready website which you can
access via the internet on your tablet,
computer, or smart phone. This will be
available once NEBA completes the
conversion of data from SBAI in the
summer of 2016.
IMPORTANT ANNOUNCEMENT – NEW ADMINISTRATIVE MANAGER EFFECTIVE JANUARY 1, 2016
WHO IS NEBA?
NEBA stands for “National
Employee Benefits
Administrators, Inc.”
NEBA is a Third Party
Administrator (TPA) that
specializes in
administering benefit
plans that cover
employees working for
Contributing Employers
under Collective
Bargaining Agreements
(CBAs) with various
Unions across the United
States.
NEBA has been in
business for over twenty
(20) years and employs
approximately eighty (80)
Union members covered
under a Collective
Bargaining Agreement
with the United Food and
Commercial Workers Local
Union 1625.
NEBA’s staff looks forward
to being of service to you
and your family beginning
January 1, 2016!
EFFECTIVE
JANUARY 1, 2016,
NATIONAL EMPLOYEE
BENEFITS
ADMINISTRATORS, INC.
(NEBA) WILL REPLACE
SOUTHERN BENEFIT
ADMINISTRATORS, INC.
AS THE ADMINISTRATIVE
MANAGER FOR THE
FRINGE BENEFIT FUNDS
ATLANTA PLUMBERS & STEAMFITTERS LOCAL 72 FRINGE BENEFIT FUNDS

IMPORTANT ANNOUNCEMENT FROM
THE BOARD OF TRUSTEES OF THE
ATLANTA PLUMBERS & STEAMFITTERS
LOCAL 72 FRINGE BENEFIT FUNDS
NEW ADMINISTRATIVE MANAGER
EFFECTIVE JANUARY 1, 2016
Atlanta Plumbers & Steamfitters
Local 72 Fringe Benefit Funds
c/o NEBA, Inc.
2010 N.W. 150th Avenue, Suite 100
Pembroke Pines, FL 33028
[Type the recipient name]
[Type the recipient address]

ATLANTA PLUMBERS &
STEAMFITTERS LOCAL NO. 72 HEALTH & WELFARE FUND
NOVEMBER 5, 2014
BENEFIT IMPROVEMENTS ANNOUNCED EFFECTIVE JANUARY I, 20 IS
Dear Participant:
Our primary duty as Trustees of the Atlanta Plumbers and Steamfitters Local No. 72 Health and Welfare Fund is to provide the best schedule of health care benefits possible to you and your eligible dependents while doing our part to help contain the cost of those benefits. This means that we must contiimally examine the adequacy of the Plan's reserves and ensure that the Plan's income and reserves are sufficient to pay for those benefits over time. Of course, federal law which regulates these benefits is evolving on almm~t a daily basis, requiring that the benefits we attempt to provide to your family are in compliance with federal mandates.
We are very pleased to announce that in recognition of all of these responsibllities, we recently approved two -enhancements which will not only broaden the coverage available to you and your family, but which will enable the Fund to maintain compliance with federal law, including the· Affordable Care. Act. Those. changes are as follows:
ATLANTA PLUMBERS & STEAMFIITERS LOCAL NO. 72 HEALTH & WELFARE FUND
Administered by: Southern Benefit Administrators, Incorporated 3835 Presidential Parkway, Suite·123 Atlanta, Georgia 30340 Phone: (770) 455-3802, Fax: (770) 455-6845 Toll-Free: (800) 382~926.
New Annual Out-Of-Pocket Maximum Added for the Purchase of Specialty Drugs As is provided for under the Schedule of Benefits available to you and your family, each covered person is subject to an annual out-of-pocket maximum of $3,000, including any covered charges not paid due to application of the Plan's $300 calendar year deductible. Further, no more than two covered persons in each family are required to satisfy the out-of-pocket maximum during a calendar year. What this means, very simply, is that no covered person is responsible for any covered medical expenses incurred during the course of the calendar year which exceeds $3,000, and no family is responsible for more than $6,000 during the calendar year.
There is currently one exception to the manner in which the annual out-of-pocket maximum is applied. Costs incurred for the purchase of specialty drugs are covered by the Plan at 80%. Unlike the expenses incurred for other covered medical charges, however, the 20% maximum for which the covered person is responsible has no limit. In other words, the covered person's 20% share of specialty drug costs cannot be applied toward the individual's out-of-pocket maximum nor is it limited to any particular dollar amount.
We are very pleased to announce, however, that effective with specialty drug charges incurred on and after January 1, 2015, an annual out-of-pocket maximum is being implemented for specialty drug costs. The new maximum is $3,600 per calendar year, which is the Fund's Plan Year. Thus, for a covered person who does not use specialty drugs, the only cost sharmg which will be applied will be the annual $300 major medical deductible and the Plan's 20% copayment percentage, but only up to the existing $3,000 annual out-of-pocket maximum. For individuals who require the use of specialty drugs, your $3,000 annual out-of-pocket maximum for all covered medical ex-

PAGE 2
penses, which includes the $300 annual deductible, plus an additional $3,600 only for specialty drug charges must be satisfied each calendar year.
This Plan improvement can have the effect of dramatically reducing a covered person's share of costs for the purchase of specialty drugs because effective with those purchased on and after January 1, 2015 you will never be required to pay out of your pocket more than $6,600 in tota~ medical expenses. For those who must use specialty drugs, this can mean a savings of several thousands of dollars per year. As we explained in a prior announcement, specialty drugs are generally those that are identified as costing more than $500 per month, typically require special handling, and in many cases are available only as injectable or infusion drugs.
Annual Vision Care Benefit Maximum Eliminated for Eligible Dependent Children Under 19 Years of Age Currently, each covered person eligible for benefits under the Plan is entitled to reimbursement for up to $200 in vision care costs per calendar year. In a previous change, we also agreed that any unused portion of the maximum: could be carried over for one additional calendar year so that up to $400 in covered charges for vision care could be paid during that year.
· Because eligible dependent children sometimes have special needs and in an effort to ensure compliance with. the Affordable Care Act, we have eliminated the annual benefit maximum as.it applies to eligible dependent children under 19 years of age. However, any covered vision charges incurred by an eligible dependent child under 19 years of age above the existing $200 calendar year maximum, or up to $400 in a two consecutive year period, will be covered by the Plan's major medical benefit and· be subject to the annual deductible and the applicable copayment percentage .. Please note that all other exclusions and limitations applicable to vision care will reinain in effect. While we believe this action will be in the best interest of all eligible dependent children under the age of 19 years, we want to encourage you to continue to incur charges for vision care only as required. The Plan establishes certain usual, customary and reasonable standards which will be applied to ensure that charges paid by the Fund for this coverage will be reasonable.
We hope you are pleased with our continuing efforts to maximize•the benefits. available to you and your family. Should you have any questions concerning these changes or regarding your Plan of Benefits in general, please do not h~sitate to contact the Fund Office.
ATlANTA PLUMBERS & STEAHfllTERS LOCAL NO. 12 HEALTH & WELFARE FUND
Best regards,
BOARD OF TRUSTEES
Union Trustees: Mr. JeffHousworth, Co-Chairman Mr. John Home Mr. Charlie Key Mr. Steve Newsome Mr. Greg Stephens
Management Trustees: Mr. Jon Sterling, Co-Chairman Mr. Gary P. Fowler Mr. John Helms Mr. John McKenney Mr. Grant Willis
JTB/mhb 72hl014

ATLANTA PLUMBERS &
STEAMFITTERS LOCAL NO. 72
HEALTH & WELFARE F.UND
NOVEMBER 5, 2014
BENEFIT IMPROVEMENT ANNOUNCED EFFECTIVE JANUARY I, 20 IS
Dear Participant:
Our primary duty as Trustees .of the Atlanta Plumbers and Steamfitters Local No. 72 Health and Welfare Fund is to provide the best schedule of. health care benefits possible to you and. your eligible dependents while doing our part to help contain the cost ofthose benefits. This means that we must continually examine the adequacy of the Plan's reserVesand.ensure.thatthe Pl~n's income and
· reserves are sufficient to pay for tho~e benefits overtime. Of col1rse, (ederallaw which regul~tes these benefits is evolving. on almost a daily basis~ requiring that the benefits we attemptto provide to your family are in conipli~
· ancewith federalmand~tes, · ·
We are very pleased to announce thatin recognition of all of these responsibilities, we. recently approved a benefit ellhancement.·which will·not only broaden the coverage available to you and your family~ but which will ena- · blethe Fund to maintain eompliance with federal law, induding the Affordable Care Act. ·
ATLANTA PLUMBERs & S~AMFlitlmS LOCAL NO. 72 HEALTH & WELFARE :FUND
Administered .by: Southern Benefit Administrators; Incorporated. · 3~B5 Presidential' Parkway, Suite 123 •. ·Atlanta; Georgia 30340 Phone: (770) 455:.3802; Fax: (770) 455-6845 Tolt:.Free: (800) 382:.6926
. " ....... ,___ .-.:·. ;.->
New Annual Out-Of-Pocket Maximum Added for the Purchase of Specialty Drugs · · . As is provided for under the Schedule of Benefits available to you and your~amily, each covered person is sub;. . ject to an annual out-of-pocket m~imum ()f $3,0?0, .including any covered charges not patd due to apphcatton of the Plan's $3'00 calendar year deductible. Further, no more than two covered p~rsons in each· family are required to satisfy the out-of~pocket maximum during a calem:lar year. What this means, very' simply; is that no . covered person is :responsible for any cov~ted mediCal .expenses incurred during the course of 'the cal~ndar year which exceeds $3 000 and no family. is responsible for
. ' , :· ·,.... . ... more thal1 $6,000 during the calendary~ar.
There is currently one exception to the t;n'afiner in which the annual out-of-pocket maximum is applied. Costs. in.curred for the purchase of specialty <irugs are.covered by the Plan at 80%. Unlike the. expenses incurred for other
· covered medical charges, however,· the 20% maximum for which the covered person: is responsible has llo limit; In other words, the covered person's 20% sijare of spe-. cialty drug costs cannot be appliedtow~d the individual's out-of ... pocket maximum nor i~ it lin:iited to any par-ticular dollar amount. · ,
We are very pleased to announce, howt}ver,.that effeetive with specialty drug charges incurred on and after January 1, 2015, an annual out-of-pocket maximum is being implemented for specialty drug costs. The new maximum is $3,600 per calendar year, which is the Ftind~s Plan Year. ·
• Thus; for a covered person who does 'not use specialty drugs, the. only cost sharing which Will be applied will be the annual $300 major medical deductible and the Plan's 20% copayment percentage, but only up to the existing .· $3,000 annual out~of-pocket maximum. For .individuals ·
· who require the use of specialty drugs, your $3,000 annu. al out-of-pocket maximum for all covered medical' ex-

PAGE 1
penses, which includes the $300 annual deductible, plus an additional $3,600 only for specialty . drug charges. must be satisfied each calendar year. . '
This Plan improvement can. have the effect of dramatically reducing a·covered person's share of costs for the purchase. of specialty drugs because effective with those. purchased on and after Januaryl, 2015 you.will never be required to pay out of your pocket more than $6,600 in total medical expenses. Forthose who must use specialty drugs, this can mean a savings of several thousands of dollars per year. As we explained in a prior announcement, specialty drugs are generally those that are identi-:-. tied as costing more than $500 per month, typically require special handling, ·and ill many cases are .available only as injectable or infuSion drugs.
·. We hope you are pleased with our continuing efforts to inaximize the· benefits available to you· and. your· family. ·Should you have any questi()ns concerning this change or regarding your Plan of Benefits in general, please do not hesitate to· contaCt the. Fund Office. .
Bes.t regards,
BOARD OF TRUSTEES
. Union Trustees: ... Mr~JeffHousworth, Co-Chairman Mr. JoOO: Home . . . . .
Mr. Charlie Key · Mr. Steve Newsome Mr .. Greg Stephens
Management Trustees: Mr. Jon.Sterling, cO-chairman · Mr. GaryP~ Fowler · Mr. John HeliD.s · · ·Mr~ John McKenney
Mr. Grant Willis
ITB/rrihb 72hll 0514Helpers
ATLANTA PLUMBERS & STEAMFITTERS LOCAL NO. 12 HEALTH & WELFARE FUND
ATLANTA PLUMBERS & STEAMFITTERS
HEALTH & WELFARE FUND OCTOBER 28, 2013
IMPORTANT PLAN DESIGN CHANGES ANNOUNCED - EFFECTIVE JANUARY I, 2014
Dear Participant:
The purpose of this notice is to announce to you a number of improvements to the benefits provided to you and your eligible family members under the Atlanta Plumbers and Steamfitters Health and Welfare Fund. The changes announced herein become effective with covered charges incurred on and after January 1, 2014. We encourage you to carefully read this notice in its entirety and then place it with your permanent records for future reference.
CALENDAR YEAR BENEFIT MAXIMUMS ELIMINATED
The following calendar year benefit payment maximums per individual are being removed from the plan effective with covered charges incurred on and after January 1, 2014:
$250,000 - all covered charges combined ($150,000 for Residential Employees) ($50,000 for Helpers)
$10,000- outpatient prescription drugs $500 - oxygen/oxygen refills $400 - new onset diabetes education
ATLANTA PLUMBERS & STEAMFIITERS HEALTH & WELFARE FUND
Administered by: Southern Benefit Administrators, Incorporated 3835 Presidential Parkway, Suite 123 Atlanta, Georgia 30340 Phone: (770) 455-3802, Fax: (770) 455-6845 Toll-Free: (800) 382-6926
Again, all of the calendar year benefit payment maximums mentioned above are being removed from the plan . effective with covered charges incurred on and after January 1, 2014.
PRE-EXISTING CONDITIONS LIMITATION ELIMINATED '
Currently, the fund has a pre-existing conditions limita- . tion which applies to all Covered Family Members, with the exception of dependent children under the age of 19. Effective with covered charges incurred on and after January 1, 2014, the pre-existing conditions limitation is being removed from the plan in its entirety.
Please feeLfree to contact the fund office with any questions you may have regarding the changes anriounced in this notice.
Best regards,
BOARD OF TRUSTEES
Union Trustees: Mr. JeffHousworth, Co-Chairman Mr. John Home Mr. Charlie Key Mr. Steve Newsome Mr. Greg Stephens
Management Trustees: Mr. Jon Sterling, Co-Chairman Mr. Gary P. Fowler Mr. John Helms Mr. David M. McKenney Mr. Grant Willis
JDB/bkr 72hl013

ATLANTA PLUMBERS & STEAMFITTERS
HEALTH & WELFARE FUND i
! MARCH 22, 2013
IL _____________ IM_Po_~_AN_r~cH_AN_G_Es_AN_N_ou_Nc_Eo __________ ~ll Dear Participant:
In a notice dated November 27, 2012 we announced a number of important plan design changes which were enacted with an effective date of January l, 2013. The purpose of this notice is to. inform you that we have decided to fine-tune two of those changes in an effort to make them work better· for you.
First, as you may recall, we announced an overall revision to the manner in which coverage is provided under the plan for prescription drug charges. Among the changes announced was a requirement that covered drugs must be pw:chased using the InformedRx discount card in order for the charges to be eligible for reimbursement under the plan. We. have learned, however, that in a number of instances, you are able to purchase some drugs at certain locations on a less expensive basis without using the drug card. Therefore, effective immediately, rather than reimbursing for drugs only if they are purchased using the discount card, coverage will also be provided under the plan for covered drugs purchased without the drug card, if those drugs can be purchased on a less costly basis without the card.
We aiso informed you in the November 27 notice that the plan's calendar year vision care payment maximum was being reduced from $400 to $200 per covered family member. effective with covered charges incurred on and
ATLANTA PLUMBERS & STEAMFIITERS HEALTH & WELFARE FUND
·Administered by: Southern Benefit Administrators, Incorporated 3835 Presidential Parkway, Suite 123 Atlanta, Georgia 30340 Phone: (770) 455-3802, Fax: (770) 4554i845 Toll-Free: (800) 382-6926
after January 1, 2013. At our most recent meeting we /' decided to fine-tune that change to allow unused portions
1
of the $200 maximum to be carried forward to the next calendar year, subject to a maximum accumulation of $400 per person. This change is effective retroactively to January 1, 2013, and we have instructed the fund office to first look back to 2012 for any possible carry overs, but only up to $200. For example, if you incurred $180 in covered vision charges during 2012, you will be allowed
1
to carry forward a total of $20 to 2013, resulting in a ! maximum of$220. However, ifyou incurred$210 duri?g \ 2012 no charges will be carried forward to 2013. Agam, · each year going forward, unused portions of the $200 maximum will be carried forward to the next calendar year, but you will not be allowed to accumulate a vision care maximum in excess of $400. In other Words, any unused portion of any carryover amount will not be carried forward to the next year.
Please do not hesitate to contact the fund office with any questions you may have regarding the changes announced in this notice.
Best regards,
·BOARD OF TRUSTEES
Union Trustees: Mr. Richard L. Oliver, Co-Chairman Mr. Jeff Housworth Mr. Ben Jacobs Mr. Steve Newsome
Management Trustees: Mr. Jon Sterling, Co-Chairman Mr. Gary P. Fowler Mr. John Helms Mr. David M. McKenney Mr. Grant Willis
72h313

".\·}
ATLANTA PLUMBERS & STEAMFITTERS
HEALTH & WELFARE FUND NOVEMBER 27. 2012
IMPORTANT PLAN DESIGN CHANGES ANNOUNCED - EFFECTIVE JANUARY I, 2013
Dear Participant:
One of our primary duties as trustees of the Atlanta Plumbers and Steamfitters Health and Welfare Fund is to provide the best and broadest,plan of benefits possible from· the resources· which are available to us. To make sure we accomplish this goal, we employ the services of professional advisors to help us determine whether the benefits are being properly funded. We also meet on a regular basis to monitor the ongoing fmancial experience oftheplan.
As you are no doubt aware, the lengthy economic recession and downturn in employment has caused hardships throughout this country. Nowhere is this more evident
. than in the construction trades industry. For your information, employment among plan participants has dropped precipitously ·over the course of the past two years and, during just the most recent two year period, the fund's assets have fallen by approximately ($5,800,000), with ($4,672,000) of the. loss occurring during just the latest year. Moreover, we expect the fund to continue to suffer losses on a regular basis going forward absent corrective action.on our part.
Therefore we have ·decided to .implement_ a number of plan design changes which· will hopefully stem the tide ofthe ongoing losses and allow the fund to at least break even from a financial standpoint during the upcoming
ATLANTA PLUMBERs & STEAMFITTERS HEALTH 8t WELFARE FUND
Administered by: Southern Benefit Administrators, Incorporated 3835 Presidential Parkway, Suite 123 Atlanta, Georgia 3034-0 • Phone: (770) 4-55-3802, Fax: (770) 4-55-684-5 Toll-Free: (800) 382-6926
calendar year. These changes also give us the opportunity to focus more ori preventive benefits by significantly improving and expanding the wellness benefits the plan has been providing for many years. All of the changes, as described below, will become effective with covered charges incurred on and after January 1, 2013. We encourage you to carefully read this notice in its entirety and then place it with your permanent records for future reference.
COVERAGE FOR IN-NETWORK PREVENTIVE CARE CHARGES EXPANDED - TO BE COVERED AT I 00%
WITH NO COST SHARING
. Effective with covered charges ·incurred on aild after January 1, 2013, an array of in-network preventive care services will be covered under the plan at 100% with no cost sharing ·requirements. You may visit www.healthcare.gov/news/factsheets/20 1 0/07/preventive -services-list.html for an up to date list of these innetwork preventive services which will be covered by. the plan. Included are services such as·s~reening for Type 2
· diabetes for adults with high blood pressure, PSA tests for men, mammography screenings every one to two years for women over 40 years ofage, and cervical cancer screening for women. Those·areonly a few examples of the many new preventive serv-ices·.whlch will be cov"" ered by the plan beginning on January 1, 201:>. Many of the new covered services apply to all covered adults, while some are gender specific, with an array of services for women only, and some for children only. Again, you should visit the website mentioned above for a compre- . hensive list of these new covered services~
FUTURE COVERAGE RESTRICTED TO IN-NETWORK PROVIDERS ONLY AT NEW BENEFIT PERCENTAGE
"Since September 1, 2006 Cigna.HealthCare has served as the Fund's Preferred Provider .. Organization (PPO). Under our arrangement with Cigna, Cigna is responsible for maintaining a broad network . of health care providers

PAGE 2 .. . ..
·who offer diseounts in return for referrals o{patients. ·. Cigna has negotiated these discounts which they ~cu~
. late before Southern Benefit processes your da.inis. Over· ; · the last six years we have worked diligently with Cigna to expand their network 'in our area so that. it will beSt · match the needs of all of the Fwid's participants. ·
As ;a result, effective with all claims incurred by a Cov.- · ered Person on and after January 1, 2013 a charge will be · covered by the Fund only if it is. incurred with a· Cigna . PPO provider, with certain very limited exceptions. You· are therefore strongly encouraged to. make sure a. provider participates in Cigna's network. before incurring <;harges .. with that provider. Your provider should be able t9 tell ·
•· ~
ATlANTA PWMBERS & STEAMFIJTERS HEALTH & WElfARE. FUND
At tlte present time, the plan's payment perce11tage in:" creases to 100% for covered charges incuired With a. PPO ptoyider once the total of covered PPO charges not paid by the fund, including covered charges not paid due ·to .aPPli~on ofthe.calendar year de<fuctible, equal or ex. ceoo $2,000 per covered family meniber/$4,000 per fami-
ly in any calendar year. Effective January 1, 2013, the out -of;..pocketmaximum is being increased to $3,0()0/$6,000
··per calendar year. .
COVERAGE FOR PRESCRIPTION DRUGS REVISED
you if they participate in Cigna's network. Ifthey.ar.e not .. Effective with all prescription drugs purchased by a Cov.,. sure, you can contact Cigna at www.cigna.cofu/SA-PPO~< '· ered Per5on on and after January 1, 20 13; the following or 1 .:.800-768-4695for this information. ·•· benefit percentages and rules will apply: . ·
• Reimbursement will be made by the fund oilly if the .· Iri. ·a further eff~rt to .help.control costs.that are,grmvmg: ·drug is· purchased using the Infotrned.Rx disoount. card every day, the Fund's major medical benefit perce11~ge: previously issued to· you (if you no loriger have this
· is· being reduced from 85% to 80%. Again, for a elm~ to . card, please contact the Fund office for a replacement); · · be payable;· it inlls.t ~. ipcurred with aCignaPPQ provi4- •· · . • Generic 'drugs will continue to be reiml>ur$ed at 100% ·. er and the ainoup.t tllat will: be· payable :will be. $0~ of and will not be subject to the major medical deductible;. qigna' s llegotiated,price with the provid,er, . · · · · · •. Brand drugs will be reimbursed at the following per~
··•· · . · · · · · · · ·· ·. .· · . ·. centages after, the major. medicid. deductible has been . R~@izmg that circum$tances sometimes· arise that can satisfied• and the· Plan's out-:Qf.;;pocket :iliaxinium ·will
···i>i~;Verit the: use of an· in"-netwoik .pmvider, ·we< have ap- ,·· . 11ever:·beapplied'to them:·
• ci~~,~~.:st~n:v.;~~7erii'f~ic:r·. : =~~!t~::;:;~nOt - • Charges for tr~~dment incun:ed :with ~ . out-Of~ , . • AIL·sp~ialty medications, iadudfug allhlfusion anq1> .
· net.Wqrk, providet.Whell it is M~fPliJ;J.ed tblit ·lli:~~ is .. , ··Injectable dtugs, will be paid a8 brand drUgs with the . · . no..· w-net'W()rk proy~der. q1u~ljfiep. tQ a~Miis~C?f: tpaJi: ;, . exception of insulin. purchased on a generic baSis. . treatineritwithin40 111ile~.oftb.~·patienf s;zip'~e; · · .· ·•; .·
• .... Initial.d:iarges for Life·Thr~i.eriing Elll~rgencies ~ ;,;, Jt:is important to remember that these new niles will be that'teJllllS defmed in tbe PJa,fi; 3}.td:: . . . . . . .. . . . ·.· ... : ". , strictly applied in all situations -whether the· dnig is ad-·
• AwolJ!lts charge.d for.anesthesiology,.radjology:; pa:"··· ·•· ministered by a phyl)ician or self·a<iJ.llinistered and that . tlJ.o}ogy artd re~~t~d.labseJ,yi9eS Wh~n IDCtlq~,ID . . 100% of fue brand drugs will never· be J#id under the .
.. ~oiin~ii<Jn with tr~tmentad.nimistered by.pai-tjcipat-: .· . . Plan'~ o11t~f~pdeketin~iriuuri~ . . . .. . . . .·. ·. ·. irig Clgna primary care pliysictaJ1S;:specialty ~~si~ . ; .; ' .--~·· ~ ...... _. ~· --~-....... ~ ..... ~~~ ..... -i-.---.---.. • cians, surgeons, hose1tats and o*er facilities. :· .. · cALENDAR YEAR MAXIMUM F<l'R DENTAl BENEFITS
..• · .. REDUCEQ . When these exceptions are applied;J~O% of the reasona'7 '· ble'and CU$tO~ary chargefor tflat s~f\rice .will ~. pliid~ . ·.. ,· ....
. · ... At present the plan's. dental care benefit niaxhnum per
CALENDAR YEAR OUT-Of•POCKET MAXIMUM · .. :.\individual, excluding prevent~ve>~.rvices, is $t,ooo per · ··· · : caleh9ar year. Effective with·¢dy~f:~'charges incurred on
1, .. ,:. INCREASED-·. ·.;,:,. ;,,,,,:1
• · andafterJan~t.2o13,th~ii~~j::taaryearmaximumis ~-_.;.;;..;..;.;,.;...;..;,;;.;;;..,..;;.;:......,;---:.....,;....;;...;..;;,;....,.;......---;.;;;.;,;......._.....;...;;;iioi; ... F being reauced tO $500. ' .?. · ... :. < ..
The pl~'s c~iehoar y6ar otrt-of~poeket fririxiin\lttfi~ b&-:; iiig increased from .• $2~000 per covered ·family member/· $4~000: per·. family of. covered individuals< to $3,000/: .
. $6~00~ effective. ~ith covered charges irtcurred on Jllld . . ~er January 1, 2013, · · · · · , . · .·. ·
CALENDAR YEAR PAyMENT MAXIMU~·.FORVISI08 .. ·. BENEFITS REDUCED:
. . ~.
. .·, ''<.The;plan's calendar year vision care payment maximu:m
:Y:····· . ::;~

PAGE 3
is also being reduced from $400 per covered family member to $200 per covered family member effective with covered charges incurred on and after. January 1, 2013.
CHANGES THAT APPLY TO SCHEDULE OF BENEFITS FOR RESIDENTIAL EMPLOYEES
A number of the changes announced above do not apply to the schedule of benefits in effect for residential employees because of differences which already exist between the plan's regular schedule of benefits and the schedule of benefits for residential employees. Those changes which do apply are: the increase in the calendar year out-of-pocket maximum from $2,000/$4,000 to $3,000/$6,000; the elimination of non-PPO coverage from the plan with the three exceptions, and a proportional decrease in the major medical payment percentage for charges incurred with a Cigna PPO provider. Fot the residential schedule, . the major medical payment percentage is being reduced from 80% to 75%. Additionally, no coverage will be provided for prescription drugs unless they are purchased using the discount drug card from a participating lnformedRx pharmacy. Also, prescription drug charges will not be credited toward the out-of-pocket maximum and the payment percentage ·for prescription drugs will never increase to 100% .
. We hope you understand the need for the very difficult decisions addressed in this notice which. are required to preserve the plan and, more importantly, the benefits available to you and your family. Please do not hesitate to contact the fund office with ·any questions you may have regarding any of the changes announced herein.
Best regards,
BOARD OF TRUSTEES
Union Trustees: Mr. Richard L. Oliver, Co-Chairman Mr. Bruce A. Earnest Mr~ JeffHousworth Mr. Ben Jacobs
Management Trustees: Mr. Jon Sterling, Co-Chairman Mr. Gary P. Fowler Mr. John Helms Mr. David M. McKenney Mr. Grant Willis
72h1112
ATlANTA PWHBERS & STEAHF11TERS HEAI,TH & WELFARE FUND
FUND OFFICE ADDRESS AND PHONE NUMBERS
Atlanta Plumbers and Steamfitters Health and Welfare Fund3835 Presidential Parkway, Suite 123
Atlanta, Georgia 30340Phone: (770) 455-3802
Toll-Free: (800) 382-6926
PREFERRED PROVIDER ORGANIZATION
The Fund participates in the CIGNA HealthCare preferred provider organization(PPO). As explained in this booklet, services obtained from a participating pro-vider are subject to substantial discounts. A participating provider is any doctor orhospital or other provider that is a member of the PPO.
The plan provides greater coverage for covered expenses when a PPO provider isutilized. A listing of PPO providers is automatically furnished to all participants ina separate booklet. If you have not received one, contact the Fund office and adirectory will be furnished free of charge. To determine whether your doctor orhospital is a member of the PPO, you may call CIGNA at:
Toll-Free: (800) 768-4695
Or you may search for participating providers on the internet at:
www.cigna.com/SA-PPO2
MAIL ORDER DRUG COVERAGE/PHARMACY DISCOUNT PROGRAM
Coverage for prescription drugs is provided under the Comprehensive MajorMedical Expense Benefit as outlined in the Schedule of Benefits. The Fund hasentered into an arrangement with InformedRx to secure discounts on prescriptiondrugs. When you have a prescription filled at a participating pharmacy, the cost ofthe prescription is discounted to both you and the Fund. Additionally, InformedRxoffers a mail order drug program for maintenance drugs.
You should have received a drug discount card which is to be presented to yourpharmacy when you have a prescription filled. If you have not received one, pleasecontact the Fund office. For information, or to locate a pharmacy, you may callInformedRx at:
Toll-Free: (800) 880-1188
Or you may contact them on the internet at:
www.informedrx.com

BLANK
ATLANTA PLUMBERS AND STEAMFITTERSHEALTH AND WELFARE FUND
Dear Plan Participant:
We are pleased to provide you with this updated summary of the health and welfarebenefits available to you and your covered family members. This booklet has beenrevised and updated to bring it into compliance with recent important federallegislation, including the Affordable Care Act, commonly referred to as “healthcare reform,” and the Mental Health Parity and Addiction Equity Act.
In accordance with provisions of the Affordable Care Act, the schedules of benefitshave been totally restated. Among the more important benefit changes are theelimination of the $1 million overall lifetime cap on benefits, the extension ofcoverage for dependent children up to age 26, and exempting children under age19 from the pre-existing condition exclusion. In addition to removing the overalllifetime maximum, individual lifetime maximums on the following types of serviceshave been eliminated as well:
• Organ transplants,• Convalescent hospital room and board benefits,• Hearing and audiometry testing,• Durable medical equipment,• Treatment of sleep apnea, and• Treatment of temporomandibular joint dysfunctions (TMJ).
In order to comply with the Mental Health Parity and Addiction Equity Act, benefitshave been revised to assure that claims related to mental and nervous disordersand substance abuse are paid the same as for any other illness.
In addition to describing the benefits available to you and your dependents, thisbooklet contains a detailed explanation of the rules of eligibility. It also includesmany other important sections, including information regarding claims filing dead-lines, your right to appeal denied claims and a statement of your additional rightsunder the provisions of the Employee Retirement Income Security Act.
Please read this booklet carefully. Along with your Fund ID card and your PPOdirectory it will help you access important health coverage for you and your fam-ily members. If you do not have a current Fund ID card or PPO directory, pleasecontact the Fund office and these items will be provided to you free of charge.

If you should have absolutely any questions regarding the contents of this bookletor concerning the operation of your Plan, please feel free to contact the Fund officeat the address and telephone numbers listed in this booklet.
Best regards,
Your Board of Trustees

INDEX
Board of Trustees – Plan Administrator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Schedules of Benefits:
Schedule of Benefits for Non-Residential Employees and Retirees . . . . . 3Schedule of Benefits for Residential Employees . . . . . . . . . . . . . . . . . . . 8
Claim Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Definitions:
Accidental Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Average Semi-Private Room Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Convalescent Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Covered Employment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Covered Family Member . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Custodial Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Disabled/Disability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Eligible Dependent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Eligible Employee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Emergency Room . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Hospice Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Intensive Care and Coronary Care Accommodations . . . . . . . . . . . . . . . . 19Life-Threatening Emergency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Medically Necessary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Non-Occupational Disease or Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Other Hospital Services and Supplies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Out-of-Area Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Physician . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Reasonable and Customary Charges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Retiree . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Room and Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Surgical Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Rules of Eligibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Eligibility for Non-Bargaining Employees . . . . . . . . . . . . . . . . . . . . . . . . 31
Notice Regarding Continuation (COBRA) Coverage . . . . . . . . . . . . . . . . . . . 33Employee and Retiree Death Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Dependent Death Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Employee Accidental Death and Dismemberment Benefit . . . . . . . . . . . . . . . 40Employee Loss of Time Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Physical Examination Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45

Comprehensive Major Medical Expense Benefit . . . . . . . . . . . . . . . . . . . . . . . 46Pre-Existing Conditions Limitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Vision Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Dental Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61Appeal Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Coordination of Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70Subrogation and Reimbursement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76Information You Should Know. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78Rights of Plan Participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87Information Required by ERISA:
Name of Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90Type of Plan. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90Name and Address of Plan Administrator . . . . . . . . . . . . . . . . . . . . . . . . . 90Type of Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91Collective Bargaining Agreements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91Plan Sponsors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91Source of Contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92Funding Medium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92Circumstances that May Result in Loss of Eligibility or Benefits . . . . . . 92Agent for Service of Legal Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93Plan Identification Numbers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93Fiscal Year . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93

ATLANTA PLUMBERS AND STEAMFITTERSHEALTH AND WELFARE FUND
This Plan is Administered by:THE BOARD OF TRUSTEES
Contract Administration Services Are Provided By:
SOUTHERN BENEFIT ADMINISTRATORS, INCORPORATED3835 Presidential Parkway, Suite 123
Atlanta, Georgia 30340
Phone: (770) 455-3802Toll-Free: (800) 382-6926
Fax: (770) 455-6845
The Trustees of the Fund are:
UNION TRUSTEES:
MR. GEORGE S. HEADPlumbers & Steamfitters Local Union No. 72P.O. Box 17806Atlanta, Georgia 30316
MR. BRUCE A. EARNESTPlumbers & Steamfitters Local Union No. 721900 Clark AvenueAlbany, Georgia 31705
MR. BEN JACOBS20 Spring CourtNewborn, Georgia 30056
(1)
EMPLOYER TRUSTEES:
MR. GARY P. FOWLERMechanical Contractors Association of Georgia4500 Hugh Howell Road, Suite 250Tucker, Georgia 30084-4709
MR. JOHN HELMSW.B. Wallis & CompanyP.O. Box 847Scottdale, Georgia 30079
MR. DAVID M. McKENNEY5026 Green Pine DriveSandy Springs, Georgia 30342

UNION TRUSTEES:
MR. CHARLIE KEY299 Tony TrailMableton, Georgia 30126
MR. TERRY SINYARDPlumbers & Steamfitters Local Union No. 72P.O. Box 17806Atlanta, Georgia 30316
(2)
EMPLOYER TRUSTEES:
MR. JON STERLINGMaxair, Incorporated1621 Sands PlaceMarietta, Georgia 30067
MR. GRANT WILLISWillis Mechanical, Incorporated3230-R Peachtree Corners CircleNorcross, Georgia 30010
The Fund Consultant is:
SOUTHERN BENEFIT ADMINISTRATORS, INCORPORATEDP.O. Box 1449
Goodlettsville, Tennessee 37070-1449
The Fund Attorney is:
CHARLES ELRODPARKER, HUDSON, RAINER & DOBBS, LLP
1500 Marquis Two Tower285 Peachtree Center Avenue, N.E.
Atlanta, Georgia 30303
The Fund Auditor is:
DENNIS G. JENKINS, C.P.A.1690 Stone Village Lane
Suite 501Kennesaw, Georgia 30152

SCHEDULES OF BENEFITS
Following are the Schedules of Benefits. In addition to the various maximums,restrictions and limitations listed as a part of the Schedules of Benefits, there areother restrictive Plan provisions outlined in this booklet. Please review this book-let very carefully before incurring expenses which you anticipate will be paid bythe Fund.
SCHEDULE OF BENEFITS FOR NON-RESIDENTIALEMPLOYEES AND RETIREES
PARTICIPANT CLASSIFICATIONS
CLASS I – Active Employees and Non-Bargaining EmployeesCLASS II – HelpersCLASS III – Retirees with MedicareCLASS IV – Retirees without MedicareCLASS V – Employees of Local 72
BENEFITS
CLASSES I, IV AND V
DEATH BENEFIT
Employee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $10,000Dependent Spouse or Child . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ 2,000
CLASS III
RETIREE DEATH BENEFIT
Retiree Under Age 65 (Disabled Retiree) . . . . . . . . . . . . . . . . . . . . . . . . . $10,000Retiree Age 65 or Older . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ 5,000
(3)

CLASSES I, IV AND V
EMPLOYEE ACCIDENTAL DEATH AND DISMEMBERMENT BENEFIT
Full Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $10,000
CLASS I
EMPLOYEE LOSS OF TIME BENEFIT
To receive this benefit, you must be disabled and under the regular care of a medicaldoctor (M.D.)
Weekly Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $285
Benefit Duration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36 Weeks
Payment Begins: If Due to Accidental Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . First Day If Due to Illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Eighth Day*
*Unless Hospital confined within such eight day period, in which case benefitsbegin on the first day of Hospital confinement. Benefits will also be paid for thefirst seven days of a disability due to an illness if the disability continues longerthan 21 days.
CLASSES I, IV AND V
PHYSICAL EXAMINATION
Maximum Benefit per Individual per Calendar Year:For Eligible Employees and Spouses . . . . . . . . . . . . . . . . . . . . . . . . . $800For Dependent Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200
(4)

(5)
FOR ALL CLASSES(Except As Noted)
COMPREHENSIVE MAJOR MEDICAL EXPENSE BENEFIT(Non-Occupational)
Calendar Year Deductible: For a routine colonoscopy performed on an Eligible Employee or spouse age 50 or older when rendered by a participating PPO provider . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . None For the Purchase of Generic Equivalent Prescription Drugs . . . . . . . . . None For all other Covered Charges: Per Person . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $300 Per Family . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $900
Hospital Emergency Room Deductible: Per Visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100
Payment Percentage: Prescription Drugs– Generic equivalent prescription drugs . . . . . . . . . . . . . . . . . . . . . . 100% Brand name prescription drugs when a generic equivalent is not available or when a generic equivalent is not medically appropriate as documented by the Covered Family Member’s attending Physician . . . . . . . . . . . . . . . . . . . . . . . . . 90%* All other name brand prescription drugs . . . . . . . . . . . . . . . . . . . . 75%* For treatment by or under the supervision of a chiropractor (subject to the maximum payments and minimum age limit outlined in this Schedule) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100% For the purchase and fitting of replacement prosthetic devices or parts, when furnished to an Eligible Employee, Retiree or spouse . . . . . . 75% For a routine colonoscopy performed on an Eligible Employee or spouse age 50 or older when rendered by a participating PPO provider . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100% For all other Covered Charges— For treatment rendered by a PPO provider, for Out-of-Area Treatment, and for treatment of a Life-Threatening Emergency 85%* For All Other Treatment Rendered By a Non-PPO Provider . . . . . . 75%

*The payment percentage will be increased to 100% for these types of CoveredCharges once the total of such types of Covered Charges incurred but not paid bythe Fund, including any Covered Charges not paid due to application of the calen-dar year deductible, equal or exceed $2,000 per Covered Family Member or $4,000per family of covered individuals in any calendar year. The payment percentagewill not be increased when other group health care coverage is available and thePlan coordinates benefits with the other coverage.
NOTE: Charges incurred for non-PPO anesthesiology, radiology, pathology or re-lated laboratory services during the course of a confinement in a participating PPOHospital, or in connection with services provided by a participating PPO Physi-cian, will be paid as though incurred with a PPO provider.
Maximum Calendar Year Payment Per Individual: For education in connection with the diagnosis of new onset diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $400 For the purchase of oxygen or oxygen refills . . . . . . . . . . . . . . . . . . . . . $500 For all Covered Charges incurred for the purchase of outpatient prescription drugs, other than drugs administered as chemotherapy treatment, or in connection with chemotherapy treatment . . . . . . . . . . . . . . . . . . . $10,000 For All Covered Charges combined— For Helpers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50,000 For All Others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $250,000
Other Limits: Hospital Room and Board limit . . . . . . . . . . . . . . . . . Semi-private room rate Treatment by or under the supervision of a chiropractor (chiropractic coverage is not provided to Eligible Dependent children under seven years of age )– Maximum payment per visit (payable at 100%): Initial office visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50 Each subsequent visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $25 Maximum number of visits . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 per day
3 per week45 per calendar year
For the Purchase and Fitting of Hearing Aids– Maximum payment per hearing aid . . . . . . . . . . . . . . . . . . . . . . . . $1,000 Maximum Frequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . One per Ear
Every Five Years
(6)

(7)
For a routine colonoscopy performed on an Eligible Employee or spouse age 50 or older when rendered by a participating PPO provider– Maximum Frequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . Once Every
Five Years
CLASSES I, III, IV AND V
VISION BENEFITS
Maximum Payment per Covered Family Member per Calendar Year . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $400
CLASSES I, IV AND V*
DENTAL BENEFITS
Maximum per Individual per Calendar Year (Excludes Preventive Services) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $1,000
Deductible per Individual per Calendar Year for Basic, Complex, or Restorative Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50
Payment Percentage: Preventive Services – Type A (Not subject to deductible or calendar year maximum) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100% Basic Restorative Services – Type B . . . . . . . . . . . . . . . . . . . . . . . . . . . 75% Complex or Major Restorative Services – Type C . . . . . . . . . . . . . . . . . 50% Orthodontic Care – Type D (For Eligible Dependent children under age 19 only) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100%
Orthodontic Lifetime Benefit for Eligible Dependent children under age 19 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $250
NOTE: Pre-certification with the Fund office is recommended for expenses over$150.
*Dental Benefits are also provided to the spouses of Class III Retirees until thedate on which those spouses become eligible for Medicare benefits.

SCHEDULE OF BENEFITS FOR RESIDENTIAL EMPLOYEES
EMPLOYEE DEATH BENEFIT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $5,000
EMPLOYEE ACCIDENTAL DEATH ANDDISMEMBERMENT BENEFIT
Full Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $5,000
EMPLOYEE LOSS OF TIME BENEFIT
To receive this benefit, you must be disabled and under the regular care of a medi-cal doctor (M.D.).
Weekly Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100Benefit Duration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 WeeksPayments Begin: If Due to Accidental Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . First Day If Due to Illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Eighth Day*
*Unless Hospital confined within such eight day period, in which case benefitsbegin on the first day of Hospital confinement.
COMPREHENSIVE MAJOR MEDICAL EXPENSE BENEFIT(Non-Occupational)
Calendar Year Deductible: For all Covered Charges: Per Person . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200 Per Family . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $600
Hospital Emergency Room Deductible: Per Visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100
Payment Percentage: For the purchase of generic equivalent prescription drugs . . . . . . . . . . . 80% For the purchase of name brand prescription drugs . . . . . . . . . . . . . . . . 70%
(8)
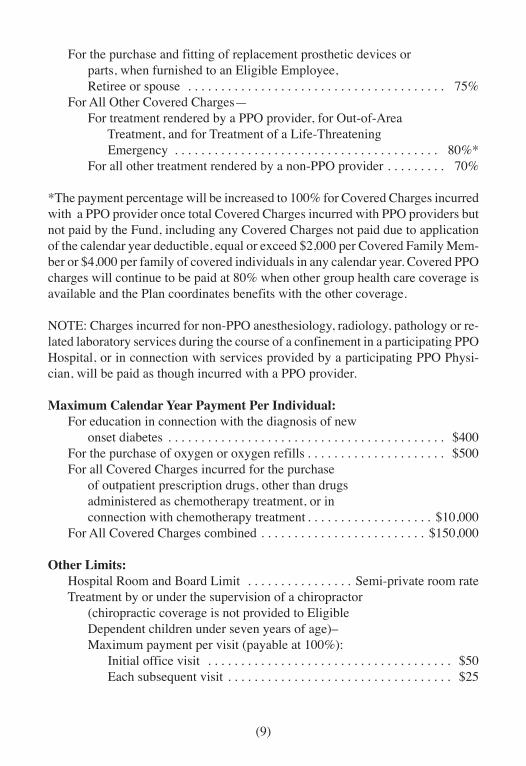
For the purchase and fitting of replacement prosthetic devices or parts, when furnished to an Eligible Employee, Retiree or spouse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75% For All Other Covered Charges— For treatment rendered by a PPO provider, for Out-of-Area Treatment, and for Treatment of a Life-Threatening Emergency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80%* For all other treatment rendered by a non-PPO provider . . . . . . . . . 70%
*The payment percentage will be increased to 100% for Covered Charges incurredwith a PPO provider once total Covered Charges incurred with PPO providers butnot paid by the Fund, including any Covered Charges not paid due to applicationof the calendar year deductible, equal or exceed $2,000 per Covered Family Mem-ber or $4,000 per family of covered individuals in any calendar year. Covered PPOcharges will continue to be paid at 80% when other group health care coverage isavailable and the Plan coordinates benefits with the other coverage.
NOTE: Charges incurred for non-PPO anesthesiology, radiology, pathology or re-lated laboratory services during the course of a confinement in a participating PPOHospital, or in connection with services provided by a participating PPO Physi-cian, will be paid as though incurred with a PPO provider.
Maximum Calendar Year Payment Per Individual: For education in connection with the diagnosis of new onset diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $400 For the purchase of oxygen or oxygen refills . . . . . . . . . . . . . . . . . . . . . $500 For all Covered Charges incurred for the purchase of outpatient prescription drugs, other than drugs administered as chemotherapy treatment, or in connection with chemotherapy treatment . . . . . . . . . . . . . . . . . . . $10,000 For All Covered Charges combined . . . . . . . . . . . . . . . . . . . . . . . . . $150,000
Other Limits: Hospital Room and Board Limit . . . . . . . . . . . . . . . . Semi-private room rate Treatment by or under the supervision of a chiropractor (chiropractic coverage is not provided to Eligible Dependent children under seven years of age)– Maximum payment per visit (payable at 100%): Initial office visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50 Each subsequent visit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $25
(9)

Maximum number of visits . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 per day3 per week
45 per calendar year For the Purchase and Fitting of Hearing Aids— Maximum payment per hearing aid . . . . . . . . . . . . . . . . . . . . . . . . $1,000 Maximum Frequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . One per Ear
per FiveYear Period
(10)

CLAIM PROCEDURES
HOW TO FILE YOUR CLAIMS
When you have a claim, please follow the instructions outlined below.
1. Time Limit for Filing a Claim — All claims must be submitted within 180days after the end of the calendar year in which they are incurred.
2. When you receive services from a doctor, hospital or other health care pro-vider, you must furnish to that provider the information needed to file a claim.This information is found on your Fund ID card. The provider should thenfile the necessary bills and related information with the Fund’s PPO.
3. Claims for non-medical benefits must be filed by you (or your beneficiary incase of your death) directly with the Fund office. Forms for these types ofclaims are available at the Fund office.
4. If a claim is filed without sufficient information or documentation regardingthe claim, you will be notified within 30 days after the Fund receives theclaim. To the extent possible, missing information will be requested fromyour health care provider. However, on some occasions, it may be necessaryto request some information directly from you.
Remember, it is your responsibility to provide your doctor, hospital and any othermedical service providers with information about your coverage under the planand about their responsibility to file claims with the Fund.
PAYMENT OF CLAIMS BY FUND OFFICE
Once the information required to make a determination as to whether a claim ispayable has been received, a decision will be made promptly by the Fund officestaff and you will be notified regarding any benefit payments. However, in noevent will the decision regarding payment be made more than 30 days after theclaim has been fully and properly filed.
If the Fund office determines that additional information is required from you or inyour behalf, you will be given 45 days in which to provide any missing informa-tion necessary to process the claim.
(11)

PRE-APPROVAL OF A CLAIM
This Fund has no pre-certification or pre-approval requirements for treatment.However, certain treatments and procedures are not covered under the Fund, andyou may wish to contact the Fund office prior to receiving treatment in order toassure that the treatment will be covered. The following rules apply to pre-approval of treatment:
1. Approval of Medically Necessary Treatment — As explained in this booklet,a charge must be Medically Necessary to be covered by the plan. If there isany doubt about whether your expected treatment will be considered MedicallyNecessary under the plan, you may contact the Fund office for an advancedecision. As explained in this booklet, you may appeal any adverse decisionmade by the Fund office regarding Medical Necessity.
2. Compliance With Plan Provisions, Exclusions and Limitations — In an effortto help control the cost of providing benefits under the plan, and in order tolimit coverage to benefits for treatment of a medical nature, various planprovisions, exclusions and limitations have been included in the plan. Theseare very specific and they are described in this booklet. However, questionssometimes arise as to whether a particular provision, exclusion or limitationapplies to a specific condition or treatment.
If there is any question as to whether your anticipated treatment will be coveredunder the plan, you should contact the Fund office in advance. Onceappropriate information is received, the Fund office staff will let you knowwhether your expected treatment will be covered under the plan. If you receivean adverse decision, you may of course appeal that decision as explained inthis booklet.
THE PLAN’S RESPONSIBILITIES TO RESPOND TO YOUR REQUESTSFOR PRE-APPROVAL
As explained in the preceding section, even though the plan does not have any pre-certification or pre-approval requirements, you may want to request pre-approvalof treatment to ensure that it will be covered under the plan. The Fund office staffwill respond to all such requests in a timely manner, as follows:
1. Urgent Care Claims — If proposed treatment is determined to be urgent in
(12)

nature, as defined below, a decision on your request for pre-approval will bemade and communicated to you within 72 hours of receipt of your request. Ifit is determined that additional information is necessary to make a decisionon your claim, you will be notified of such as soon as possible but in noinstance more than 24 hours after receipt of the request. You will then begiven not less than 48 hours to provide the required information.
An Urgent Care Claim is a claim which, if treated as a claim for non-urgentcare:
(a) Could seriously jeopardize the life or health of the claimant or the abilityof the claimant to regain maximum function, or
(b) In the opinion of a Physician with knowledge of the claimant’s medicalcondition, would subject the claimant to severe pain that cannot beadequately managed without the care or treatment that is the subject ofthe claim.
2. Non-Urgent Care Claims — If proposed treatment is determined to be of anon-urgent nature, a decision on your request for pre-approval will be madeand communicated to you within 15 days of receipt of your request. If it isdetermined that additional information is necessary to make a decision onyour claim, the plan may require up to an additional 15 days to make a deci-sion on your request. If such an extension is required, you will be notifiedwithin 15 days of receipt of your request regarding the extension and a deci-sion will be made as soon as possible. If the extension is required because itis necessary for you to provide additional information, you will be given atleast 45 days to provide the requested information.
These procedures for processing requests for pre-approval of both urgent and non-urgent care claims have been adopted solely as guidelines and to assure compli-ance with applicable federal law. It will continue to be the practice of the Trustees,as the plan administrator, along with the Fund office staff, to timely process allrequests for pre-approval and to respond to all such requests immediately wherepossible, but always within the time periods prescribed above.
(13)

DEFINITIONS
In order to properly explain each of the benefits to which you and your family maybe entitled, it has been necessary to use certain specific terms in this booklet todescribe these benefits. The definitions of many of those terms are as follows:
ACCIDENTAL INJURY
“Accidental Injury” means an injury sustained by a Covered Family Member that:
1. Results from and is caused by a sudden and violent event;
2. Is caused by an external force or object; and
3. Occurs unexpectedly and by chance, and is not due to any fault or miscon-duct on the part of the injured person.
The term “Accidental Injury” does not include any injury that is the result of aself-destructive act or intentionally self-inflicted injury, illness or condition, un-less the self-destructive act or intentionally self-inflicted injury, illness or condi-tion is the result of the Covered Family Member’s medical condition, includingboth physical and mental health conditions.
The term “Accidental Injury” also does not include any injury sustained by a Cov-ered Family Member involving any act for which the individual is convicted, orpleads guilty or nolo contendere to, driving while intoxicated or driving under theinfluence of alcohol or illegal drugs by a court of competent jurisdiction.
AVERAGE SEMI-PRIVATE ROOM RATE
“Average Semi-Private Room Rate” means:
1. The standard charge made by a Hospital for semi-private room and boardaccommodations, or the average of such charges where a Hospital has morethan one established level of such charges; or
2. 80% of the lowest charge made by a Hospital for single bed room and boardaccommodations when the Hospital does not provide semi-private room andboard accommodations.
(14)

CONVALESCENT HOSPITAL
“Convalescent Hospital” means an institution which:
1. Primarily provides skilled nursing under the supervision of a Physician orregistered nurse;
2. Has available, on duty or call, at all times a Physician who is a staff memberof a Hospital;
3. Has a registered nurse on duty 24 hours a day;
4. Maintains daily medical records for each patient;
5. Complies with all licensing and other legal requirements; and
6. Is not, except incidentally, a place for Custodial Care, for the aged, for drugaddicts, for alcoholics, for the care of the mentally ill or persons with nervousdisorders, for the care of senile or mentally deficient persons, a hotel, or asimilar institution.
COVERED EMPLOYMENT
“Covered Employment” means hours worked for an employer for which theemployer is obligated to make contributions to the Fund under a collectivebargaining agreement or other written agreement. Covered Employment also meanshours worked for the Union, the JATC or the North Georgia Building Trades forwhich contributions are made to the Fund.
COVERED FAMILY MEMBER
“Covered Family Member” means any Eligible Employee or Retiree who iscovered under this Fund and the Eligible Dependents of an Eligible Employee orRetiree.
CUSTODIAL CARE
“Custodial Care” means care which:
1. Is provided mainly to maintain an individual;
(15)

2. Is designed in order to help the individual meet his activities of daily living;or
3. Is not provided mainly as a type of therapy in the treatment of a sickness orinjury.
“Custodial Care” includes but is not limited to the following:
1. Help in walking, bathing, dressing or feeding;
2. Preparing special diets; and
3. Supervising the administration of medications that do not require constantattention of trained medical personnel.
DISABLED/DISABILITY
See pages 43 and 58.
ELIGIBLE DEPENDENT
“Eligible Dependent” means the following:
1. The spouse of an Eligible Employee or Retiree. A spouse will cease to be anEligible Dependent on the date the Eligible Employee or Retiree and his orher spouse are divorced or legally separated.
2. The following child or children of an Eligible Employee or Retiree:
(a) Any child who has not yet attained age 26; and
(b) Any unmarried child who is incapable of self-sustaining employmentbecause of mental or physical handicap and who is chiefly dependent onthe Eligible Employee or Retiree for support and maintenance, regard-less of age, provided (i) the incapacity commenced prior to age 26, (ii)the Eligible Employee or Retiree was eligible for benefits at the time theincapacity commenced, or the child is the natural child of the EligibleEmployee or Retiree, is over age 26 and was incapacitated at the timethe Eligible Employee or Retiree became eligible for benefits under the
(16)

Plan, and (iii) the incapacity was not caused by or in connection withalcohol or drug abuse or addiction. A child will only be considered inca-pacitated if proof of the incapacity is submitted to the Fund office within31 days of the date his coverage would otherwise terminate, and subse-quently, as may be required by the Trustees. Proof of the EligibleDependent’s incapacity will not be required more frequently than annu-ally after the two-year period following the child’s attaining age 26.
As used in this section, “child” means only an Eligible Employee’s or Retiree’snatural children, step-children and adopted children as well as any childrenplaced with the Eligible Employee or Retiree for adoption, but where theadoption has not become final. Being placed for adoption means that theEligible Employee or Retiree has assumed, and retains, a legal obligation fortotal or partial support of the child in anticipation of adoption of the child.The child’s placement with the Eligible Employee or Retiree terminates upontermination of the legal obligation. Upon an adoption becoming final, thechild may continue to meet the definition of Eligible Dependent in accor-dance with (a) or (b) above.
No child who has other employer-sponsored coverage available in his or hisspouse’s name will be considered an “Eligible Dependent.”
For the purposes of benefits payable as a result of pregnancy, “Eligible Depen-dent” means the Eligible Employee’s or Retiree’s spouse only.
ELIGIBLE EMPLOYEE
“Eligible Employee” means any employee who meets the Rules of Eligibility asoutlined in this booklet.
EMERGENCY ROOM
“Emergency Room” means a facility which is established for the emergencytreatment of accidents and life-threatening illnesses and which is attached to or onthe premises of a licensed Hospital. Additionally, the facility must be open andmust provide Physician services 24 hours a day, and must have available suchservices so as not to require referral to other similar facilities. “Emergency Room”also includes a free-standing or walk-in clinic that is not attached to a Hospital, butonly to the extent of emergency treatment for accidents and life-threatening illnesses.
(17)
HOSPICE CARE
“Hospice Care” means a coordinated program of home and in-patient care for thespecial physical, psychological and social needs of terminally ill persons and theirfamilies. A terminally ill person is one who has been diagnosed by a Physician ashaving a life expectancy of six months or less. A hospice is a facility, or part ofone, which:
1. Provides in-patient care;
2. Is licensed as such and operating within the scope of the license;
3. Maintains medical records on each patient and provides an ongoing qualityassurance program;
4. Has full-time supervision by at least one Physician; and
5. Provides 24-hour nursing services by registered nurses.
HOSPITAL
“Hospital” means an institution that is licensed as a hospital (if licensing is re-quired by law where the institution is located) and which meets all of the followingrequirements:
1. It is engaged primarily in providing medical care and treatment of sick andinjured persons on an in-patient basis at the patient’s expense and maintainsdiagnostic and therapeutic facilities for medical diagnosis and treatment ofsuch persons by or under the supervision of a staff of duly qualified Physi-cians;
2. It continuously provides twenty-four (24) hour a day nursing services by orunder the supervision of registered graduate nurses;
3. It has an operating room where surgical procedures are performed (unlessthe institution is a duly licensed psychiatric hospital);
4. It maintains daily medical records for each patient; and
(18)

5. It is not, other than incidentally, a clinic, convalescent home, institution fordrug addicts or alcoholics, a place of rest, a place for the aged, or a nursinghome.
In addition, for the purposes of benefits paid under this Plan for Mental or NervousDisorders, the term Hospital will include an institution which is accredited by astate licensing agency for the treatment of Mental or Nervous Disorders and whichhas accommodations for resident bed patients, facilities for the treatment of Men-tal or Nervous Disorders, a resident psychiatrist always on duty or call, and as aregular practice charges the patient for the expense of confinement.
INTENSIVE CARE AND CORONARY CARE ACCOMMODATIONS
“Intensive Care and Coronary Care Accommodations” means an accommodationwhich is exclusively reserved for critically and seriously ill patients requiring con-stant audio-visual observation as prescribed by the Physician attending the Cov-ered Family Member and which provides room and board, specialized registerednursing care and other nursing care, and special equipment or supplies immedi-ately available on a stand-by basis and segregated from the rest of the Hospitalfacilities.
LIFE-THREATENING EMERGENCY
“Life-Threatening Emergency” means a medical condition that manifests itselfsuddenly by symptoms of sufficient severity, including severe pain, that withoutimmediate medical attention could reasonably be expected, by a prudent lay per-son who possesses an average knowledge of health and medicine, to result in:
1. Serious jeopardy to the mental or physical health of the individual;
2. Danger of serious impairment of the individual’s body functions;
3. Serious dysfunction of any of the individual’s bodily organs; or
4. In the case of a pregnant woman, serious jeopardy to the health of the fetus.
MEDICALLY NECESSARY
“Medically Necessary” means that a service or supply which the patient receivesis required to identify or treat an illness or Accidental Injury or other covered
(19)

condition which a Physician has diagnosed or reasonably suspects. To be Medi-cally Necessary the service or supply must:
1. Be consistent with the diagnosis and treatment of the patient’s condition;
2. Be in accordance with standards of good medical practice;
3. Not be for the convenience of the patient or his Physician; and
4. Be performed in the least costly setting required by the patient’s medicalcondition.
NON-OCCUPATIONAL DISEASE OR INJURY
“Non-Occupational Disease or Injury” means a disease or Accidental Injury thatdoes not arise out of (or in the course of) any work for pay or profit, nor in any wayresults from such work for pay or profit. However, if proof is furnished to theTrustees that an individual covered under a workers’ compensation law (or otherlaw of similar purpose) is not covered for a particular disease under such law, thatdisease will be considered “non-occupational” regardless of its cause.
In the event an employee claims that a disease or injury is work connected and theemployer disputes this contention, the Trustees agree to be bound by the finaldecision of any court or commission which determines the issue. In the event alegal determination is not sought in such case, the Trustees may decide whetherthe illness or accident is occupational or non-occupational. In the event paymentsare made under this plan for a condition later determined to be occupational andcompensable under any workers’ compensation or similar law, the employee re-ceiving the payments is obligated to make restitution (pay back) to the Trustees ofthe amount of benefits received from any settlement or judgement obtained.
OTHER HOSPITAL SERVICES AND SUPPLIES
“Other Hospital Services and Supplies” means the actual charges made by aHospital, in its own behalf, for services and supplies rendered to the individual,and required for treatment of that person, other than charges for Room and Board,the professional services of any Physician, and any private duty or special nursingservices (including intensive nursing care by whatever name called), regardless ofwhether such services are rendered under the direction of the Hospital or otherwise.
(20)

OUT-OF-AREA TREATMENT
“Out-of-Area Treatment” means treatment rendered by a non-PPO provider to aCovered Family Member whose residence is at least 35 miles from the nearestPPO provider capable of providing the required treatment.
PHYSICIAN
“Physician” means a doctor of medicine (M.D.), a doctor of osteopathy (D.O.), achiropractor (D.C.M.), a dentist (D.D.S.), a psychologist (Ph.D), or an optometrist(O.D.) practicing within the scope of his license and who is licensed to practice assuch in the state in which treatment is rendered.
REASONABLE AND CUSTOMARY CHARGES
“Reasonable and Customary Charges” means the prevailing fee or fees most fre-quently charged by the providers of a like service or supply with similar trainingand experience for the performance of a comparable service, or a service of com-parable gravity, severity and magnitude, in the locality where the service was per-formed.
RETIREE
“Retiree” means a former Eligible Employee who meets the requirements for Re-tiree eligibility as outlined in this booklet.
ROOM AND BOARD
“Room and Board” means all charges for room and board, general duty nursing,and any other charges by whatever name such charges are called, which are madeby a Hospital as a condition of occupancy of the class of accommodations occupied,but not including charges for professional services of Physicians.
SURGICAL PROCEDURE
“Surgical Procedure” means any procedure included in one of the followingcategories that is performed by a Physician, other than a resident Physician orintern of a Hospital, and also customary post-operative care for a period not toexceed two weeks following the surgery:
(21)
1. The incision, excision, or electrocauterization of any organ or part of thebody;
2. The manipulative reduction of a fracture or dislocation;
3. The suturing of a wound; or
4. The removal by endoscopic means of a stone or other foreign object from thelarynx, bronchus, trachea, esophagus, stomach, urinary bladder, urethra, colonor ureter or the diagnostic examination by endoscopic means of these organs.
“Surgical Procedure” does not include any alternative medical treatment, whetheror not such alternative treatment is in place of or accomplishes the same result asthe performance of the corresponding surgical operation or procedure.
(22)

RULES OF ELIGIBILITY
An employee working for a contributing employer or employers within the juris-diction of the Fund will be eligible to receive benefits and will become an EligibleEmployee after meeting the requirements outlined below.
INITIAL ELIGIBILITY
1. FOR EMPLOYEES OF EMPLOYERS CURRENTLY PARTICIPATING:
An employee and his Eligible Dependents will become initially eligible forbenefits on the first day of the third month following a period of three con-secutive months or less during which the employee has worked at least 390hours for which Employer contributions are paid to the Fund or for which areciprocal contribution is received by the Fund. This requirement is reducedto 300 hours for apprentices who are attending school as a part of the appren-ticeship program. Eligibility will be continued for the remainder of the monthin which eligibility is gained. Continuing eligibility will then be based onother applicable sections of these Rules of Eligibility.
2. FOR EMPLOYEES OF A NEW SIGNATORY EMPLOYER:
For those employees employed by an employer located within the jurisdic-tion of the Union at the time that employer first becomes signatory to a writ-ten agreement requiring contributions to the Fund, the following initial eligi-bility requirement will apply in place of that outlined in 1. above, but onlyfor the period of employment immediately following and continuous withthe employer’s initial participation. This requirement will apply only to full-time employees who have been continuously employed by the employer fora minimum period of six consecutive months as of the date of the agreement,and to whom group health benefits have been continuously provided by theemployer during that period. The requirement outlined in 1. above will applyto all other employees of the employer.
The employer will be required to begin making contributions as requiredunder the written agreement for the month in which the agreement is effec-tive (the first month of participation). The initial contribution must be madefor the prior month, based on hours worked by the employees during theprior month. For example, if the written agreement requiring contributions
(23)

to the Fund is effective on January 1, the first contribution will be due inJanuary for hours worked in December. All later contributions will be madeas required in the written agreement.
If an employee described above continues in such employment, he will be-come initially eligible for benefits on the first day of the second month ofparticipation. For example, if contributions are first made in the month ofJanuary for work performed in December, the employee will become ini-tially eligible on February 1. Eligibility will then be continued for the re-mainder of the month in which eligibility has been gained, provided the em-ployee continues in employment for which employer contributions are re-quired. Continuing eligibility will be based on other applicable sections ofthese Rules of Eligibility. However, if such an employer later ceases partici-pation in the Fund, the eligibility of all employees described under this pro-vision will terminate as of the date the employer’s obligation to make contri-butions to the Fund ceases. No further eligibility will be granted under anysection of these Rules of Eligibility.
CONTINUING ELIGIBILITY
Once an employee and his Eligible Dependents become eligible for the benefitsprovided under this Fund, they will remain eligible during each successive BenefitMonth provided the employee has worked a minimum of 130 hours during thecorresponding Contribution Month for which employer contributions are paid tothe Fund or for which a reciprocal contribution is received by the Fund. The monthlyeligibility requirement for apprentices who are attending school as a part of theapprenticeship program is 100 hours.
Contributions months and the corresponding benefit months are as follows:
Contribution Months Benefit Months
Hours Worked In: Earn Eligibility For:
October . . . . . . . . . . . . . . . . . . . . . . . . . . . . . JanuaryNovember . . . . . . . . . . . . . . . . . . . . . . . . . . . FebruaryDecember . . . . . . . . . . . . . . . . . . . . . . . . . . . . MarchJanuary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . AprilFebruary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . May
(24)

March . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . JuneApril . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . JulyMay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . AugustJune . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . SeptemberJuly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . OctoberAugust . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . NovemberSeptember . . . . . . . . . . . . . . . . . . . . . . . . . . . December
HOUR BANK
Once an employee has satisfied the requirements for Initial Eligibility, any hoursfor which employer contributions are received during a Contribution Month inexcess of 130 (100 for apprentices attending school) will be credited to theemployee’s hour bank. However, no more than 780 hours may be accumulated inthe employee’s hour bank at any time (600 hours for apprentices attending school).
If for any reason an employee works an insufficient number of hours during aContribution Month, the number of hours necessary to continue eligibility will bewithdrawn from the employee’s hour bank, if such hours are available.
SELF-CONTRIBUTIONS FOR ACTIVE ELIGIBLE EMPLOYEES
If, after becoming initially eligible for benefits under the Fund, an Eligible Em-ployee is in danger of losing his eligibility because he has failed to work the re-quired 130 hours (100 for apprentices attending school), and if the hours accumu-lated in the Eligible Employee’s hour bank are not sufficient to continue his eligi-bility, the Eligible Employee will be entitled to make self-contributions to con-tinue his eligibility in effect. Self-payments will be in an amount equal to the dif-ference between the hours actually worked for the Contribution Month specifiedand 130 hours (100 hours for apprentices while in school), multiplied by the thencurrent employer contribution rate.
Self-contributions will be limited to six consecutive Benefit Months, except thatthose employees working under a reciprocal agreement requiring contributions tothis Fund in their behalf will be entitled to make unlimited additional consecutiveself-contributions for each Contribution Month in which contributions are trans-ferred to this Fund for at least one hour worked. All self-contributions must bereceived by the Fund office no later than the date established by the Trustees fromtime to time.
(25)
TERMINATION OF EMPLOYEE ELIGIBILITY
In the event an Eligible Employee’s hours worked plus his accumulated hour bankhours are insufficient to continue his coverage under the Fund, and if he does notmake the appropriate self-contribution, or is not entitled to do so, his eligibilitywill terminate as of the last day of the last Benefit Month for which he is eligible,and any hours remaining in his accumulated hour bank will be immediately forfeited.
Additionally, should an employee enter employment within the geographicaljurisdiction of the United Association of Plumbers and Pipefitters of the UnitedStates and Canada, AFL-CIO, in the same industry, trade or craft as that coveredby the collective bargaining agreement in effect between the employers and theunion for an employer who is not required to make contributions to the Fund forsuch employment, or should he continue in such employment after his employerceases to be obligated to make such contributions, his eligibility will terminate asof the last day of the month in which he commences such employment. Upontermination of eligibility under this paragraph, any hours accumulated in theemployee’s hour bank will be immediately forfeited and the employee will not beentitled to continue his eligibility under the SELF-CONTRIBUTIONS FORACTIVE ELIGIBLE EMPLOYEES provisions.
REINSTATEMENT OF ELIGIBILITY
Once an employee has gained eligibility under the Fund and later lost his eligibility,he will once again become eligible for benefits upon satisfying the requirementsfor CONTINUING ELIGIBILITY.
DISABILITY CREDIT
For each seven day period during which an Eligible Employee is entitled to a Lossof Time Benefit under this Plan, or is entitled to workers’ compensation benefits,the Eligible Employee’s hour bank will be credited with an amount determined bythe Trustees from time to time as if the employee had worked in employment forwhich contributions were due the Fund during such period.
DUAL COVERAGE UNDER THE PLAN
If both a husband and wife are covered under the plan as Eligible Employees and/or Retirees, Eligible Dependent children of such husband and wife will be eligible
(26)

for coverage under both parents, subject to the COORDINATION OF BENEFITSprovisions outlined in this booklet. Likewise, if a husband and wife are both cov-ered under the Plan as Eligible Employees, such individuals will be covered asEligible Dependent spouses of one another, subject to the COORDINATION OFBENEFITS provisions. In no event will benefits provided under the Plan exceed100% of covered charges.
SERVICE IN THE ARMED FORCES
An Eligible Employee who is inducted or enlists or is otherwise called to activeduty in the Uniformed Services of the United States of America will be entitled tocredit or the right to make self-contributions for continued coverage as set forthbelow.
1. For active uniformed service of 31 days or less – The Eligible Employee willbe credited with 8 hours per day for each day (Monday-Friday) of activeuniformed service provided the Eligible Employee reports to work no laterthan the first regularly scheduled working period one week after terminationof active duty.
2. For active uniformed service of more than 31 days – All benefits for an Eli-gible Employee and his Eligible Dependents will be terminated on the datehe enters uniformed service for a period of service in excess of 31 days,except as follows:
(a) The Eligible Employee may choose to continue coverage through theuse of any current hours worked, as calculated for CONTINUING ELI-GIBILITY, or through the use of hour bank hours.
The Eligible Employee may elect to use this accumulated eligibility tocontinue coverage under the Fund, or may elect to defer the use of hiseligibility until his reemployment as described on the following page, ormay elect to use a portion of his hours and defer usage of the remainder.Failure to affirmatively elect continued coverage will result in an auto-matic deferral of the use of accumulated eligibility.
(b) Upon termination of coverage as otherwise outlined in this section, andfollowing any extension of coverage under paragraph (a) above, an Eli-gible Employee may elect to continue coverage for the period of active
(27)

uniformed service, not to exceed 24 months, by making self-contribu-tions in the amount and under the terms set forth in this booklet formaking self-contributions for continued coverage (COBRA coverage).In order to be entitled to make self-contributions, the Eligible Employeemust notify the Fund office in writing within 60 days of his entry intoactive uniformed service.
Former Eligible Employees who are discharged from active uniformed service of60 months or less will be reinstated for benefits provided the individual submits anapplication for reemployment or seeks reemployment through a participating localunion within 14 days (if the active uniformed service is for 31 to 181 days) or 90days (if the active uniformed service is more than 181 days) after discharge. Thetime for reemployment application will be extended in the event of injury orhospitalization as further provided in the Uniformed Services Employment andReemployment Rights Act of 1994.
If an Eligible Employee has chosen to use his accumulated eligibility credits asoutlined above and, as a result, has insufficient eligibility accumulated to his creditto continue his coverage under the Fund upon his reemployment, the EligibleEmployee will be required to make monthly payments to the Fund in order toregain and continue his coverage. Monthly payments will be required until suchtime as the employee has worked sufficient hours to satisfy the requirements forCONTINUING ELIGIBILITY.
The term active uniformed services includes active duty with the Armed Forces,the Army National Guard and the Air National Guard (when engaged in activeduty training, inactive duty training or full time National Guard duty), thecommissioned corps of the Public Health Service and any other category of personsdesignated by the President of the United States in the time of war or emergency.
TERMINATION OF DEPENDENT ELIGIBILITY
An Eligible Dependent’s eligibility for benefits under the Plan will terminate onthe earliest of the following:
1. On the date the Eligible Dependent ceases to be an Eligible Dependent;
2. Except as provided under ELIGIBILITY FOR RETIREES AND THEIRSPOUSES on the following page, the date on which the Eligible Employee’sor Retiree’s coverage under the Plan terminates;
(28)

3. The date on which the Eligible Dependent enters the United States ArmedForces on full time active duty, except as outlined above;
4. The date on which the Plan is terminated;
5. In the event of the death of the Eligible Employee or Retiree, the later of thelast day of the Benefit Month in which the Eligible Employee or Retiree diesor the last day of any Benefit Month for which the Eligible Employee orRetiree would have been eligible based on hours worked prior to the death ofthe Eligible Employee or Retiree, including hour bank hours; or
6. The date on which the Plan is amended so as to terminate the benefits of theEligible Dependent.
SUSPENSION OF HOUR BANK HOURS FOR EMPLOYEES ENTERINGNON-COVERED EMPLOYMENT
If an Eligible Employee enters employment with a contributing employer in workthat is not Covered Employment, the use of his accumulated hour bank hours to-ward continuing eligibility will be suspended. The accumulated hours will onceagain become available on the date on which the employee returns to CoveredEmployment, but only if he does so within the twelve consecutive month periodimmediately following the date he entered non-Covered Employment. If the formerEligible Employee fails to return to Covered Employment within the allotted time,his suspended hour bank hours will be permanently forfeited.
ELIGIBILITY FOR PREGNANCY BENEFITS
Subject to the other provisions outlined in this booklet, an Eligible Employee,Retiree or Eligible Dependent spouse will be eligible for benefits arising out ofpregnancy if, at the time expenses are incurred, such person is either eligible forbenefits or has ceased to be eligible because of disability due to pregnancy whichprevents the individual from engaging in her regular or customary occupation.Eligible Dependents who are not spouses of Eligible Employees or Retirees willnot be eligible for benefits arising out of pregnancy.
ELIGIBILITY FOR RETIREES AND THEIR SPOUSES
1. Retiree Eligibility. An Eligible Employee who retires from employment maycontinue coverage under the Fund, subject to the following:
(29)

(a) The Eligible Employee must have been a member in good standing ofLocal 72 for a period of at least 36 consecutive months leading up to andcontinuous with his or her retirement date;
(b) The retirement date for the Eligible Employee will be the effective dateof benefits under either the Atlanta Plumbers and Steamfitters PensionFund or the Plumbers and Pipefitters National Pension Fund;
(c) The Eligible Employee must be eligible for benefits under this Fund onthe date of his retirement;
(d) The Eligible Employee must elect at the actual time of his or her retire-ment to continue eligibility under the Fund either under these provisionsor under the provisions for COBRA Continuation Coverage. Election ofone of these options will automatically constitute a waiver of the otheroption;
(e) The Eligible Employee must have satisfied any one of the followingrequirements:
(1) The Eligible Employee must have been continuously eligible underthis Fund for a minimum period of 36 consecutive months leadingup to and continuous with his or her retirement date; or
(2) The Eligible Employee must have been available for work as certi-fied by Local 72 for a minimum period of 36 consecutive monthsleading up to and continuous with his or her retirement date; or
(3) The Eligible Employee must have worked for a contributing em-ployer in a capacity that did not require contributions to this Fundfor a minimum period of 36 consecutive months leading up to andcontinuous with his or her retirement date; or
(4) The Eligible Employee must have satisfied a combination of any ofthe provisions outlined in (1), (2) and (3) above to make up the 36month requirement;
(f) The Retiree must remit all payments for coverage on a timely basis inthe amount and manner established by the Trustees; and
(30)

(g) The Retiree must maintain membership in good standing with Local 72.
2. Benefits for Medicare-Eligible Retirees/Dependents. This Plan will not du-plicate the payment of any benefits by Medicare to a Retiree or his EligibleDependents. The medical benefits payable by the Fund for Retirees and theirEligible Dependents are limited to only those Covered Charges which arenot payable under Medicare.
3. Dependent Spouses of Retirees. The Eligible Dependent spouse of a Retireewill mean only the spouse, if any, to whom the Retiree is legally married onthe date on which he first qualifies under the Fund as a “Retiree.” Spousesacquired at a later date, including those acquired during a period of reem-ployment, are excluded from coverage under this provision.
ELIGIBILITY FOR NON-BARGAINING (OPTIONAL) EMPLOYEES
An employer who is obligated through a collective bargaining agreement or otherwritten agreement to make contributions to this Fund on behalf of employees cov-ered by that agreement may elect to also make contributions on employees whoseemployment is not covered by that agreement. These other, non-bargaining em-ployees are referred to as Optional Employees. The employer may make applica-tion to the Fund office to make contributions for the purpose of maintaining eligi-bility for those Optional Employees under the Fund. Participation of OptionalEmployees is subject to the approval of the Trustees.
The employer will be required to make a monthly contribution to the Fund onbehalf of each and every Optional Employee regularly employed by the employeron a full-time basis. Eligibility for each Optional Employee will begin on the firstday of the month for which a contribution is first made in his behalf. Eligibilitywill terminate on the last day of the last month for which a contribution is made forthe employee. No hour bank will be established for Optional Employees, nor willthey be allowed to make self-contributions to continue their coverage, whether asan active or retired employee, except as explained under the Continuation Cover-age “COBRA” provisions as outlined in this booklet. Additionally, no disabilitycredit will be granted for time off due to disability.
Except as outlined in this subsection, all other provisions of these Rules of Eligi-bility will apply to Optional Employees.
(31)

CHANGE IN BENEFITS FOR RESIDENTIAL EMPLOYEES
An Eligible Employee who changes from residential work to non-residential workwill become eligible for the Schedule of Benefits for Non-Residential Employeesand Retirees effective with the Benefit Month for which he has satisfied the eligi-bility requirement as a non-residential employee.
CHANGE IN ELIGIBILITY RULES
The Trustees may, in their discretion, change or amend these Eligibility Rules atany time.
(32)

AN IMPORTANT NOTICE ABOUT YOURCONTINUATION COVERAGE RIGHTS UNDER COBRA
This notice is furnished to you as a covered participant under the Atlanta Plumbersand Steamfitters Health and Welfare Fund (the Plan). This notice contains impor-tant information about your rights to COBRA continuation coverage, which is atemporary extension of coverage under the Plan. The right to COBRA continua-tion coverage was created by a federal law, the Consolidated Omnibus BudgetReconciliation Act of 1985 (COBRA). COBRA continuation coverage can be-come available to you and to other members of your family who are covered underthe Plan when you would otherwise lose your group health coverage. This noticegenerally explains COBRA continuation coverage, when it may become avail-able to you and your family, and what you need to do to protect the right toreceive it. The Plan administrator is the Board of Trustees of the Fund. The re-sponsibility for administering COBRA continuation coverage has been delegatedto the Fund office staff at:
Atlanta Plumbers and SteamfittersHealth and Welfare Fund
3835 Presidential Parkway, Suite 123Atlanta, Georgia 30340Phone: (770) 455-3802
Toll-Free: (800) 382-6926
COBRA CONTINUATION COVERAGE
COBRA continuation coverage is a continuation of Plan coverage when coveragewould otherwise end because of a life event known as a “qualifying event.” Spe-cific qualifying events are listed later in this notice. COBRA continuation cover-age must be offered to each person who is a “qualified beneficiary.” A qualifiedbeneficiary is someone who will lose coverage under the Plan because of a quali-fying event. Depending on the type of qualifying event, employees, spouses ofemployees, and dependent children of employees may be qualified beneficiaries.Under the Plan, qualified beneficiaries who elect COBRA continuation coveragemust pay for COBRA continuation coverage.
If you are an employee, you will become a qualified beneficiary if you lose yourcoverage under the Plan because either one of the following qualifying eventshappens:
(33)

1. Your hours of employment are reduced; or
2. Your employment ends for any reason other than your gross misconduct.
If you are the spouse of an employee, you will become a qualified beneficiary ifyou lose your coverage under the Plan because any of the following qualifyingevents happens:
1. Your spouse dies;
2. Your spouse’s hours of employment are reduced;
3. Your spouse’s employment ends for any reason other than his or her grossmisconduct; or
4. You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverageunder the Plan because any of the following qualifying events happens:
1. The parent-employee dies;
2. The parent-employee’s hours of employment are reduced;
3. The parent-employee’s employment ends for any reason other than his or hergross misconduct; or
4. The child stops being eligible for coverage under the plan as an “EligibleDependent.”
The Plan will offer COBRA continuation coverage to qualified beneficiaries onlyafter the Fund office has been notified that a qualifying event has occurred. Whenthe qualifying event is the end of employment or reduction of hours of employ-ment, your employer will notify the Fund office automatically. In the event of thedeath of an employee, your employer is required to notify the Fund office. How-ever, it may be in the best interest of qualified beneficiaries to contact the Fundoffice as well so that notification of death can be made as timely as possible. Youremployer must notify the Fund office within 30 days of any of these events.
(34)

For the other qualifying events (divorce or legal separation of the employee andspouse or a dependent child’s losing eligibility for coverage as a dependent child),you must notify the Fund office in writing within 60 days after the qualifyingevent occurs. You must send this notice to the Fund office at the address listed inthis section. In the event of divorce or separation, you must also furnish a copy ofthe divorce decree or separation papers. In the event of a child ceasing to qualify asan Eligible Dependent, you must furnish a copy of the dependent’s birth certificateor other proof of date of birth.
Once the Fund office receives notice that a qualifying event has occurred, COBRAcontinuation coverage will be offered to each of the qualified beneficiaries. Foreach qualified beneficiary who elects COBRA continuation coverage, COBRAcontinuation coverage will begin on the date that Plan coverage would otherwisehave been lost.
COBRA continuation coverage is a temporary continuation of coverage. When thequalifying event is your death, your divorce or legal separation, or a dependentchild losing eligibility as an Eligible Dependent, COBRA continuation coveragelasts for up to 36 months.
When the qualifying event is the end of employment or reduction of your hours ofemployment, COBRA continuation coverage lasts for up to 18 months. There arethree ways in which this 18 month period of COBRA continuation coverage canbe extended:
Disability Extension of 18-Month Period of Continuation Coverage
If you or anyone in your family covered under the Plan is determined by theSocial Security Administration to be disabled at any time during the first 60days of COBRA continuation coverage and you notify the Fund office in atimely fashion, you and your entire family can receive up to an additional 11months of COBRA continuation coverage, for a total maximum of 29 months.You must make sure that the Fund office is notified of the Social SecurityAdministration’s determination within 60 days of the date of the determina-tion and before the end of the 18-month period of COBRA continuation cov-erage. You must send this notice and proof of determination of disability tothe Fund office at the address listed on page 33.
(35)

Maximum Period of 24 Months for Service in the Armed Forces
As described on pages 27 and 28, if you enter active duty in the UniformedServices of the United States of America for a period of more than 31 days,the maximum period of COBRA coverage which you may elect is 24 months,provided you notify the Fund office in writing within 60 days of your entryinto active uniformed service.
Second Qualifying Event Extension of 18-Month Period of Continua-tion Coverage
If your family experiences another qualifying event while receiving COBRAcontinuation coverage, your spouse and dependent children can get addi-tional months of COBRA continuation coverage, up to a combined maxi-mum of 36 months. This extension is available to your spouse and dependentchildren if you die or get divorced or separated. The extension is also avail-able to your dependent child when that child stops being eligible under thePlan as an Eligible Dependent child. In all of these cases, you must makesure that the Fund office is notified of the second qualifying event within60 days of the second qualifying event. This notice must be sent to theFund office along with proof of divorce or separation or date of birth ofyour dependent child.
PROCEDURE FOR OBTAINING CONTINUATION COVERAGE
Once the Fund office knows that an event which qualifies you or a dependent forcontinuation coverage has occurred, the Fund office will send an election notice toyour last known address or to the address of your dependent, as applicable. Youwill have sixty days after the date on the election notice in which you or yourdependent must notify the Fund office of an election to continue coverage. If youor your dependent do not elect coverage within the sixty day time period, the rightto continue group health coverage will end. A period of forty-five days will beallowed from the date of an election of continued coverage in which to make anyretroactive payment due under this provision. Each employee, or each covereddependent if electing separately, will be required to make monthly payments in anamount and manner which will be determined by the Trustees in accordance withapplicable law. The monthly amount of each payment will be established no moreoften than once a year.
(36)

TYPE OF COVERAGE EXTENDED
The benefits provided under COBRA will be the same as those provided to allother employees in your Class.
CANCELLATION OF COBRA COVERAGE
Continued coverage will be cancelled by the Fund upon the occurrence of any ofthe following events:
1. You do not make the required monthly payment by the due date, includingthe allowable 30 day grace period;
2. The Plan terminates;
3. You become covered under any other group health care plan, unless the otherplan contains an exclusion or limitation with respect to any pre-existing con-ditions (coverage under this provision will then continue until such time asthe waiting period under the other plan is satisfied, subject to the maximumperiod of coverage under this Plan); or
4. You become covered by Medicare.
IF YOU HAVE QUESTIONS
If you have questions about your COBRA continuation coverage, you should con-tact the Fund office or you may contact the nearest Regional or District Office ofthe U.S. Department of Labor’s Employee Benefits Security Administration(EBSA). Addresses and phone numbers of Regional and District Offices are avail-able through EBSA’s website at www.dol.gov/ebsa.
KEEP YOUR PLAN INFORMED OF ADDRESS CHANGES
In order to protect your family’s rights, you should keep the Fund office in-formed of any changes in the addresses of family members. You should alsokeep a copy, for your records, of any notices you send to the Fund office.
(37)

EMPLOYEE AND RETIREE DEATH BENEFIT
(Class I, Class III, Class IV, Class V and Residential Employees Only)
On receipt of proof of the death of an Eligible Employee or Retiree covered underthis benefit, the Fund will pay the amount of Death Benefit specified in the Sched-ules of Benefits, subject to the provisions outlined below.
BENEFICIARY
Each covered Eligible Employee and Retiree may designate a beneficiary in writ-ing to the Fund office. If, on the death of the Eligible Employee or Retiree, there isno surviving designated beneficiary for all or any part of the benefit payable, thebenefit will be paid to the Eligible Employee’s or Retiree’s surviving spouse. If nospouse survives the Eligible Employee or Retiree, then the benefit will be paid tothe Eligible Employee’s or Retiree’s estate. Any payment so made will, to theextent of such payment, release the Trustees from all liability.
The Eligible Employee or Retiree may change the designated beneficiary fromtime to time by filing a written notice of change with the Fund office. The changeof beneficiary will be effective as of the date the Eligible Employee or Retireesigns the notice of change, whether or not the Eligible Employee or Retiree isliving on the date the notice is received, but without prejudice to the Trustees onaccount of any payment made before the notice of change has been received.
If more than one beneficiary is designated and the Eligible Employee or Retireehas failed to specify each beneficiary’s respective interest, the beneficiaries willshare equally. If any designated beneficiary predeceases the Eligible Employee orRetiree, the interest of that beneficiary will terminate, and his share will be pay-able equally to the remaining beneficiaries.
ASSIGNMENT
The benefits provided hereunder are not assignable.
(38)

DEPENDENT DEATH BENEFIT
(Non-Residential Class I, Class IV and Class V Only)
If an Eligible Employee’s or Retiree’s Dependent (see definition below) dies whilecovered under this benefit, the Fund will pay the amount of the Dependent DeathBenefit specified in the Schedule of Benefits to the Eligible Employee or Retireeonly.
DEFINITION OF DEPENDENT
For purposes of this benefit, Dependent will include only the following:
1. The Eligible Employee’s or Retiree’s spouse, as long as the employee andspouse are not divorced or legally separated; and
2. The Eligible Employee’s or Retiree’s Eligible Dependent children over 10days of age but under 26 years of age and not otherwise covered under theFund as an Eligible Employee.
ASSIGNMENT
The benefits provided hereunder are not assignable.
TERMINATION OF BENEFIT
The Dependent Death Benefit terminates on the earlier of:
1. The date a Dependent ceases to satisfy the definition of “Dependent” as out-lined above; or
2. The exact time of the Eligible Employee’s or Retiree’s death.
(39)

EMPLOYEE ACCIDENTAL DEATH AND DISMEMBERMENT BENEFIT
(Class I, Class IV, Class V and Residential Employees Only)
An Accidental Death and Dismemberment Benefit will become payable if:
1. A Covered Eligible Employee or Retiree has sustained any of the losses listedin the following Table of Losses as a direct result of Accidental Injury; and
2. The loss occurred independently of all other causes, as evidenced by a vis-ible contusion or wound on the exterior of the body (except in the case ofdrowning or internal injuries revealed by an autopsy); and
3. The date of occurrence of the injury was not more than 90 days prior to thedate the loss was sustained.
In such an event, the Fund will pay to the Eligible Employee or Retiree or hisdesignated beneficiary or other person, if there is no designated beneficiary, theamount specified below, and in the Schedules of Benefits. The term “Full Benefit”means the maximum amount payable as a benefit on account of accidental deathor dismemberment of an Eligible Employee or Retiree.
LOSS BENEFIT
Life . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Full Benefit
Both hands, Both Feet or Both Eyes . . . . . . . Full Benefit
One Hand and One Foot, One Hand and One Eye, or One Foot and One Eye . . . . . . Full Benefit
One Hand, One Foot, or One Eye . . . . . . . . . . One Half of the Full Benefit
With respect to hands or feet, “loss” means dismemberment by severance at orabove the wrist or ankle joint. With respect to eyes, “loss” means the entire andirrecoverable loss of sight. No more than the Full Benefit will be paid for all lossessustained by the Eligible Employee or Retiree as the result of any one accident.
(40)

EXCLUSIONS
No benefit will be payable for any loss which results directly or indirectly, whollyor partly, from:
1. Self-destruction or attempted self-destruction or intentionally self-inflictedinjury, while sane or insane;
2. Insurrection or war, or any act attributable thereto;
3. Participation in a riot;
4. Committing an assault or felony;
5. Operating or riding in or descending from any kind of aircraft if the EligibleEmployee or Retiree is a pilot, officer or member of the crew of such aircraftor is giving or receiving any kind of training or instruction or has any dutiesaboard such aircraft or requiring descent therefrom;
6. Disease of the body or mental infirmity, or as a result of medical or surgicaltreatment or diagnosis therefor;
7. Ptomaines or bacterial infection (except pyogenic infection occurring simul-taneously with and in consequence of a visible accidental cut or wound);
8. Taking of poison, whether voluntary or involuntary; or
9. Asphyxiation from inhaling gas, whether voluntary or involuntary, whichdoes not arise out of or in the course of employment.
EXAMINATION
The Fund has the right and opportunity to examine any individual whose injury isthe basis of a claim when and as often as it may reasonably require while a claim ispending, and also the right and opportunity to make an autopsy in case of death,where it is not forbidden by law.
BENEFICIARY
Benefits for loss of life, if any, and all other benefits which remain unpaid at the
(41)

death of the Eligible Employee or Retiree, are payable to the beneficiary on thesame basis as under the Employee Death Benefit. All other benefits are payable tothe Eligible Employee or Retiree or his personal representative or guardian orexecutor.
ASSIGNMENT
The benefits provided hereunder are not assignable.
(42)

EMPLOYEE LOSS OF TIME BENEFIT
(Class I and Residential Employees Only)
On receipt of proof from a licensed Doctor of Medicine (M.D.) that an EligibleEmployee has become Disabled, as defined below, due to a Non-OccupationalDisease or Injury, the Fund will pay to the Eligible Employee the Loss of TimeBenefit shown in the Schedules of Benefits. Loss of Time Benefits will be payablefor the portion of the period of disability beginning on the day shown in the Sched-ules of Benefits, up to the maximum period of benefits shown in the Schedules ofBenefits for each separate disability.
Successive periods of disability due to the same or related causes are consideredone period of disability unless they are separated by the Eligible Employee’s re-turn to full-time active employment with a participating employer for all of theregular working days in a two consecutive week period. Successive periods ofdisability due to entirely unrelated causes are considered one period of disabilityunless separated by the Eligible Employee’s return to full-time active employmentwith a participating employer for at least one full day.
Benefits are compared and paid on a weekly basis. Payments for partial weeks ofdisability are paid at the daily rate of one-seventh of the weekly benefit.
DEFINITION OF DISABILITY
An Eligible Employee will be considered Disabled under this provision only if heis prevented, solely because of a Non-Occupational Disease or Injury, from engag-ing in his regular or customary occupation, provided that he will not be deemed tobe Disabled during any period in which he is engaged in any other occupation forcompensation or profit. Disability will also include pregnancy if a female EligibleEmployee is prevented by such condition from engaging in her regular or custom-ary occupation.
EXCLUSIONS
No benefit will be paid under this provision for:
1. Any period of disability during which the Eligible Employee is not under thecare of a Doctor of Medicine (M.D.);
(43)

2. Any disability resulting from injuries sustained while doing any act of orpertaining to any occupation or employment for remuneration or profit, orfrom sickness for which benefits are payable in accordance with the provi-sions of any workers’ compensation or similar law;
3. Any disability not certified by the Eligible Employee’s Physician and em-ployer;
4. Any disability certified by a chiropractor;
5. Any disability for a period when the Eligible Employee was actively at workin Covered Employment;
6. Any disability for a period when the Eligible Employee was on the out-of-work list with the union; or
7. Any disability commencing prior to the employee becoming eligible for ben-efits under the Plan.
TAX ON BENEFITS
Loss of Time Benefits may be required to be included as part of your gross incomefor federal income tax purposes unless you are totally and permanently disabledand are retired on disability. You should contact a competent tax advisor to deter-mine whether you are subject to this tax.
Additionally, federal law requires that the Fund withhold FICA taxes from Loss ofTime Benefits. This tax is automatically deducted from such payments and depos-ited in accordance with applicable federal laws and regulations. The Fund itselfwill pay that portion of the FICA tax normally paid by an employer.
(44)

PHYSICAL EXAMINATION BENEFIT
(Non-Residential Class I, Class IV, and Class V Only)
On receipt of proof that a Covered Family Member has received a physicalexamination from a Physician, the Fund will pay the amount actually charged forthe examination, not to exceed the maximum amount shown in the Schedule ofBenefits. This Physical Examination Benefit covers routine check-ups andexaminations, and, for Eligible Dependent children, routine immunizations andother well child charges. This benefit will not apply when such charges are otherwisecovered under the Plan due to an illness or injury.
(45)

COMPREHENSIVE MAJOR MEDICAL EXPENSE BENEFIT
(All Classes Except as Noted)
Comprehensive Major Medical Expense Benefits become payable if a CoveredFamily Member incurs Covered Charges which are in excess of the deductibleamount.
The deductible amounts, Covered Charges, payment percentages and maximumamounts are described on the following pages and shown in the Schedules ofBenefits.
The deductibles, payment percentages and maximums are applied separately foreach Covered Family Member unless otherwise specified. The deductible andcharges in excess of the amount paid by the Plan are the responsibility of the EligibleEmployee or Retiree.
USE OF PREFERRED PROVIDER ORGANIZATION (PPO)
The Fund uses the services of the CIGNA HealthCare preferred providerorganization to help provide quality health care at affordable prices to planparticipants. A preferred provider organization (PPO) is a network of health careproviders including doctors, hospitals and other facilities which provide servicesat discounted or fixed rates.
By securing your health care services from a participating CIGNA provider, youreduce not only the cost of providing coverage under the Fund, but also the amountof your portion of any bill payable for such medical services. You may of coursechoose to receive services from a non-participating provider, but in that case, PPOdiscounts do not apply, and your benefits will be paid at a lower level.
A directory of participating providers has been furnished to plan participants. Ifyou would like to verify that a particular doctor or hospital is still participating inthe PPO, please contact your PPO at the telephone number listed on the insidefront cover. If you need a PPO directory, contact the Fund office and one will beprovided free of charge.
CALENDAR YEAR DEDUCTIBLE AMOUNT
The Calendar Year Deductible amount is the amount to be paid in cash for services
(46)

or supplies for treatment of an illness or injury or other covered condition. Theamount of the deductible which must be met during a calendar year by each CoveredFamily Member, and by each family, is specified in the Schedules of Benefits.Only Covered Charges as outlined in this section may be used to meet the deductible.
If an individual is suffering from a condition for which Covered Charges are incurredin two or more calendar years, the deductible must be met for each calendar year.Any expenses applied during October, November or December of a calendar yearto that year’s deductible will also be applied in the same amount to the deductibleof the next calendar year.
PAYMENT PERCENTAGE
Once the applicable deductible has been satisfied by a Covered Family Member,the Plan will pay the percentages specified in the Schedules of Benefits of theCovered Charges incurred by that person during the remainder of the calendaryear. The amounts remaining after the appropriate deductible has been satisfiedwill have the payment percentages applied to them.
MAXIMUM OUT-OF-POCKET EXPENSE
As indicated in the Schedules of Benefits, many Covered Charges are subject to amaximum out-of-pocket expense. For such Covered Charges, the paymentpercentage will be increased to 100% once the total Covered Charges not paid bythe Fund, including any charges not paid due to the application of the calendaryear deductible, equal or exceed the amount indicated in the Schedules of Benefits.
COVERED CHARGES
Covered Charges will include only the Reasonable and Customary Charges whicha Covered Family Member actually incurs for medical care, services and suppliesreceived or furnished by or upon the recommendation and approval of a Physicianwho is attending the Covered Family Member for the Medically Necessary treatmentof a disease or Accidental Injury or other covered condition, and provided suchcharges are not otherwise excluded or limited as outlined in this booklet and arenot for Custodial Care.
For Retirees eligible for Medicare, Covered Charges are limited to those chargesapproved by Medicare, except for prescription drugs which are covered at theactual reasonable cost.
(47)

(48)
A Covered Charge will be considered incurred on the date on which the particularservice, treatment or supply giving rise to the expense is rendered or obtained. Inthe absence of proof to the contrary, when a single charge is made for a series ofservices, treatments or supplies, each service, treatment or supply will be deemedto bear a pro-rata share of the charge. Charges incurred for and during a Hospitalconfinement will be considered incurred on the date of admission to the Hospital.
Covered Charges are limited to the following:
1. Charges for Hospital Room and Board incurred as an inpatient subject to thefollowing:
(a) The maximum Covered Charge for confinement in a semi-private roomor in an Intensive Care or Coronary Care Accommodation will be theactual charge, and
(b) The maximum covered charge for confinement in a private room will bethe Average Semi-Private Room Rate.
2. Charges incurred as an inpatient for Other Hospital Services and Supplies.
3. Charges actually made by a professional anesthetist or by a Physician foranesthetics, oxygen, and their administration.
4. Charges actually made by a Physician as fees for diagnosis, treatment or theperformance of a Surgical Procedure.
5. Charges actually made for x-ray, radiotherapy (including the use of x-ray,radium, cobalt, or other radioactive substances), or diagnostic laboratoryexaminations.
6. Charges incurred on an outpatient basis for Other Hospital Services andSupplies for emergency sickness treatment, emergency accident treatmentwithin 48 hours of an Accidental Injury, and medical care and treatmentreceived on the day of and in connection with a Surgical Procedure.
7. Convalescent Hospital room benefits up to the daily Room and Board limit.Benefits are payable only if confined to a Hospital as a registered inpatientfor at least three consecutive days and then confined to a Convalescent

(49)
Hospital within fourteen days after discharge from the Hospital for the sameor related injury or disease that caused the Hospital confinement.
8. Charges made for speech therapy, physical therapy, occupational therapy,cardiac rehabilitation therapy and any other type of therapy provided by anindividual licensed or certified to deliver such services which is recommendedby an attending Physician, provided that such therapy is certified as beingMedically Necessary by the case management/medical managementconsultant retained by the Trustees for such purpose.
9. Charges for Hospice Care, subject to review.
10. Pre-admission tests or exams.
11. Charges for repair of Accidental Injuries to natural teeth arising from anoutside force, including replacement and treatment of a fractured jaw andrelated x-rays.
12. Local ambulance charges for emergency transportation to the nearest Hospital.
13. Private duty nursing care by a licensed nurse (R.N. or L.P.N.). Payment willbe made for only that portion of the nurse’s services that require the specialknowledge and skill of a trained professional nurse, and then only upon receiptof a Physician’s written documentation of such need and a listing of the specialcare services to be provided. Nursing care is not covered for routine patientcare that is provided by a registered nurse or which is provided by a non-professional individual on a maintenance of care basis.
14. Radiation therapy treatment.
15. Casts, splints, surgical dressings and trusses.
16. The rental cost – up to the purchase price – of durable medical equipment.This will include coverage for the cost of a wheelchair, along with any specialfeatures and accessories, required in the permanent care or maintenance of aCovered Family Member, when certified as Medically Necessary by theattending Physician.
17. Blood transfusions – including the cost of whole blood or plasma not donatedor replaced.

(50)
18. Prosthetic devices required due to a loss or injury, subject to the following:
(a) Coverage is limited to one such device in any twelve consecutive monthperiod when required by an Eligible Dependent child;
(b) With regard to Eligible Employees, Retirees and Eligible Dependentspouses, coverage will be provided for the purchase and fitting of theinitial device the same as any other Covered Charge. Thereafter, limitedcoverage will be provided for the purchase and fitting of replacementdevices or parts contingent on the Eligible Employee or Retiree provid-ing proof of payment of the Covered Family Member’s portion of thetotal charge made for the device or part.
19. Charges made by an ambulatory surgical center when a Surgical Procedureis performed.
20. Drugs or medicines which by law need to be prescribed by a Physician, subjectto the annual maximum listed in the Schedules of Benefits. Birth controlpills, other contraceptives or any kind of contraceptive devices, regardless ofthe purpose for which they are prescribed, are not covered. Drugs not approvedby the Federal Food and Drug Administration, dietary supplements, vitamins,and food extracts are also not covered.
21. Charges for home health care by a home health care agency, subject to review.
22. Charges for chiropractic services and treatment rendered by a licensedchiropractor, subject to the limitations outlined in the Schedules of Benefits.This benefit is provided only for those services where a chiropractor is actingwithin the scope of his license, and only when services are rendered to aCovered Family Member seven years of age or older. Maintenance care isnot considered a Covered Charge.
23. Charges for hearing and audiometry testing as well as for the purchase andfitting of hearing aids, subject to the limitations listed in the Schedules ofBenefits.
24. Benefits for pregnancy and pregnancy-related conditions of EligibleEmployees/Retirees and Eligible Dependent spouses, payable in the samemanner and subject to the same limitations and conditions as any other

(51)
disability (injury or sickness) under the Plan. Charges for any abortion otherthan a non-elective abortion are not Covered Charges.
25. Charges incurred due to complications of pregnancy (for female EligibleDependent children). If, while covered under the Plan, a female EligibleDependent child incurs expenses due to a complication of pregnancy,Comprehensive Major Medical Expense Benefits only will be payable in thesame manner and subject to the same limitations and conditions as any othersickness.
Complications of pregnancy means: (a) conditions requiring Hospitalconfinement (when the pregnancy is not terminated), the diagnoses of whichare distinct from pregnancy but are adversely affected by pregnancy or arecaused by pregnancy, such as acute nephritis, nephrosis, cardiacdecompensation, missed abortion, preeclampsia, intra-uterine fetal growthretardation, and similar medical and surgical conditions of comparableseverity, and (b) ectopic pregnancy which is terminated.
26. Charges incurred for the purchase of oxygen or oxygen refills subject to theannual maximum listed in the Schedules of Benefits (exclusive of theequipment required to administer the oxygen, as covered under item 16).
27. Charges made by a Hospital or a Physician for routine care of an EligibleDependent newborn during the Hospital confinement immediately followingbirth, including circumcision of a newborn male infant.
28. Charges made for a cardiac rehabilitation and exercise program accompaniedby cardiac monitoring for the purpose of modifying coronary risk factorsand promoting recovery, when ordered by an attending Physician andperformed by an individual duly licensed or certified to render the service,up to a maximum treatment period of twelve weeks.
29. Charges made for the following services and supplies when rendered inconnection with reconstructive breast surgery following a mastectomy:
(a) Reconstruction of the breast on which the mastectomy was performed,
(b) Surgery and reconstruction of the other breast to produce symmetricalappearance, and

(52)
(c) Coverage for prostheses and physical complications of all stages ofmastectomy including lymphedemas,
in a manner determined in consultation with the attending physician andpatient.
30. Charges incurred in connection with a reduction mammoplasty when there ismedical documentation of intractable pain, not amenable to other forms oftreatment, and which is the result of excessively large, pendulous breasts.This procedure will be covered only if all of the following criteria are met,and are documented in writing by a Physician:
(a) The pain must have been present at least one year,
(b) The suprasternal notch to nipple measurement must be at least 21 centi-meters, and
(c) The amount of breast tissue removed must be at least 450 grams perside.
35. Charges incurred for the education of a Covered Family Member in connec-tion with a diagnosis of new onset diabetes, subject to the annual maximumlisted in the Schedules of Benefits.
36. Charges incurred for services rendered by a podiatrist (D.P.M.), but onlywhen the Covered Family Member has been referred to the podiatrist by aDoctor of Medicine (M.D.).
37. Charges incurred for gastroenterostomy, gastric stapling, jejunoileal bypassand other surgical procedures of a like nature, provided the surgery is certi-fied as Medically Necessary by the medical case manager retained by theTrustees for that purpose.
38. Charges made for, or in connection with, pain management, provided suchservices are certified as being Medically Necessary by the medical case man-ager retained by the Trustees for that purpose.
39. For Non-Residential Eligible Employees and spouses only, charges made fora routine colonoscopy performed on an Eligible Employee or his or her

(53)
Eligible Dependent spouse, provided the individual is age 50 or older andthe services are rendered by a participating PPO provider, and subject to thelimitation outlined in the Schedule of Benefits.
LIMITATIONS AND EXCLUSIONS
No benefits will be payable for or in connection with any charges:
1. For dental work or treatment, except (i) charges in connection with the re-moval of impacted teeth, and (ii) charges in connection with and as a resultof injuries to natural teeth, including the initial replacement of natural teeth,sustained in an accident, to the extent the dental work or treatment is re-ceived promptly after such accident. No charge for the initial replacement ofnatural teeth in excess of $50 multiplied by the number of natural teeth re-placed as a direct cause of such accident will be included as a Covered Charge.
2. For blood and plasma for which the Hospital or other supplier makes a re-fund or allowance to or on behalf of the Covered Family Member, either as aresult of the operation of a group blood bank, private donor or otherwise.
3. For medical care, services or supplies received or furnished in connectionwith, or as a result of, any cosmetic surgery, except (i) charges in connectionwith and as a result of the necessary repair of disfigurement caused by bodilyinjuries sustained in an accident, provided such cosmetic surgery is receivedpromptly after such accident, (ii) charges in connection with and as a resultof an abnormal congenital condition, and (iii) charges specifically listed un-der the Covered Charges.
4. For hearing aids or the fitting of hearing aids except as specifically outlinedunder Covered Charge 23.
5. For medical care, services or supplies received or furnished in connectionwith, or as a result of, any injury or sickness resulting from, or caused, di-rectly or indirectly, wholly or partly, by (a) war or any act of war, whetherdeclared or undeclared, (b) service in any military, naval or air force of anycountry while such country is engaged in war, whether declared or unde-clared, (c) police duty as a member of any military, naval or air force organi-zation, (d) insurrection, (e) participation in a riot, or (f) any atomic explosionor other release of nuclear energy (except when being used solely for medi-

(54)
cal treatment of a Non-Occupational Injury or Sickness) whether in peace orin war and whether intended or accidental.
6. For medical care, services or supplies received in, or furnished by, a Hospi-tal, institution or other facility owned or operated by the United States (otherthan a Veterans Administration hospital), or any agency or instrumentalitythereof unless otherwise required by law.
7. Charges which would not have been made in the absence of this coverage orwhich the Eligible Employee, Retiree or Eligible Dependent is not legallyobligated to pay.
8. For any medical care, services or supplies received or furnished in connectionwith, or as a result of, (a) any bodily injury which arises out of, or in thecourse of, any employment or occupation for compensation or profit, or (b)any sickness for which benefits are payable under any workers’ compensationlaw, occupational disease law, or any other legislation of similar purpose.
9. For medical care, services or supplies received or furnished in connectionwith, or as a result of, any injury or sickness resulting from participation in,or in consequence of having participated in, the commission of an assault ora felony except in cases of domestic violence.
10. For any medical care, services or supplies not recommended and approvedby the Physician who is attending the Covered Family Member.
11. For any medical care, services or supplies received or furnished while theindividual is not eligible for benefits.
12. For a disability not directly caused by Non-Occupational Disease or Injury.
13. For treatment of infertility, artificial insemination or in vitro fertilization,microsurgical resectioning and reanastomosis of tubes, reversal of vasecto-mies and vasoplasty.
14. For any surgical or laser procedure intended to correct or improve impairedvision resulting solely from presbyopia/myopia, hyperopia, astigmatism orother refractive error except when the individual’s vision cannot be correctedto at least 20/70 in the better eye by normal corrective glasses and the indi-vidual cannot, for medical reasons, wear contact lenses.

(55)
15. In the case of an Eligible Dependent who is employed:
(a) For expenses due to an accident on the job whether or not such accidentis covered by workers’ compensation or similar legislation, or
(b) For expenses due to an illness which is covered by workers’ compensa-tion or similar legislation.
16. To the extent that benefits are payable with respect to:
(a) An Eligible Employee, Retiree or Eligible Dependent under workers’compensation or similar legislation,
(b) An Eligible Employee, Retiree, or Eligible Dependent under any insur-ance contract, plan or fund for which an employer, directly or indirectly,has paid part or all of the cost, or
(c) Visits or treatment of an Eligible Dependent if such individual is en-titled to benefits as an Eligible Employee or Retiree.
17. Resulting from an act of war occurring while the individual is covered.
18. For treatment in a charitable hospital which does not bill patients for servicesrendered.
19. Resulting from occupational injury, disease or sickness.
20. Which are duplicate charges incurred by a person covered under the Planand by any other group insurance or government sponsored medical program.
21. Incurred in connection with confinement to any institution or part thereofused principally as a rest facility, a facility for the aged, chronically ill, drugaddicts or alcoholics, or as a facility providing primarily custodial, educa-tional or rehabilitative care.
22. Except as specifically provided, for routine physical examinations or anyother routine care.
23. For maternity benefits for Eligible Dependent children, except for complica-tions arising as specifically outlined under Covered Charge 25.

(56)
24. For eye care charges: any charge for or in connection with (a) exams to de-termine the need for (or changes of) eyeglasses or lenses of any type, (b)eyeglasses or lenses of any type except initial replacements for loss of thenatural lens, (c) eye surgery such as radial keratotomy, where the primarypurpose is to correct myopia (nearsightedness), hyperopia (farsightedness)or astigmatism (blurring), except as provided in item 14 of this section.
25. For unnecessary services or supplies: charges for services or supplies, in-cluding tests and check up exams, that are not Medically Necessary for medicalcare of a diagnosed sickness or Accidental Injury (except as specifically pro-vided).
26. Related to any abortion other than an abortion performed because the mother’slife would be endangered if the fetus were carried to term.
27. For weight control programs.
28. In connection with sex transformation or sexual dysfunctions.
29. In connection with smoking cessation.
30. For reversal of sterilizations.
31. For or in connection with infertility treatments or procedures.
32. To the extent that they are in excess of the Reasonable and Customary Chargesfor the applicable services or supplies.
33. Which the patient is not required to pay.
34. Incurred for treatment by, or under the supervision of, a chiropractor (D.C.M.)when rendered to an individual under the age of seven years.
35. Which are incurred due to an injury that does not meet the definition of Ac-cidental Injury as it appears in this booklet.
PRE-EXISTING CONDITIONS LIMITATION
1. No benefits will be paid for any charge incurred by a Covered Family Mem-ber for or in connection with a medical condition, regardless of the cause of

(57)
the condition, for which medical advice, diagnosis, care or treatment wasrecommended or received during the look-back period. As used in this sec-tion, “look-back period” means the ninety-day period ending on the later ofthe following dates:
(a) For an Eligible Employee or Eligible Dependent, the first day of thecalendar month in which the employee commenced a period of employ-ment upon which initial eligibility or regained eligibility was grantedunder the Plan; or
(b) For an Eligible Dependent who was not a dependent of the employee onthe date outlined under (a) above, the date on which the Eligible Depen-dent became a dependent of the employee.
A “medical condition,” as used in this section, means any condition, whetherphysical or mental, including, but not limited to, any condition resulting fromillness, injury (whether or not accidental), or congenital malformation, ex-clusive of genetic information.
2. This exclusion for such medical condition will end at the end of a twelvemonth period beginning on the later of (i) the first day of the calendar monthmentioned in 1(a) above, or (ii) the date outlined in 1(b) above.
3. EXCEPTIONS
(a) Credit for days of “creditable coverage,” as defined in Section 2590.701-2of the Employee Retirement Income Security Act, as amended, will beapplied to reduce the waiting period described above.
(b) No pre-existing condition exclusion will apply to any Eligible Depen-dent child under the age of 19.
(c) Pregnancy will not be considered a pre-existing condition.
4. YOUR RIGHT TO CREDITABLE COVERAGE
Federal law requires that you be given credit for “creditable coverage” towardthe waiting period described under (2) above. “Creditable Coverage” isprevious coverage for health benefits or health insurance. In order to qualify

(58)
as “creditable coverage,” your previous coverage must not have terminatedmore than sixty-three days prior to the day on which you commencedemployment for a contributing employer or, for a dependent you acquireafter your date of employment, sixty-three days prior to the date on whichthat person becomes your dependent.
In order to receive credit for “creditable coverage” you can request a certificatefrom your prior plan or insurance carrier certifying your previous coverage.If you would like, the Fund office will be glad to assist you in requesting acertificate of your previous coverage from your former plan or insurancecarrier. You may contact the Fund office for a more complete description ofthe effect any “creditable coverage” may have on reducing your waiting periodunder this pre-existing condition exclusion.
EXTENSION OF COMPREHENSIVE MAJOR MEDICAL EXPENSEBENEFIT
In the event coverage under the Plan is terminated for an Eligible Employee orEligible Dependent, and on that date such individual is Disabled, as defined in thefollowing paragraph, and under a Physician’s care, such person’s ComprehensiveMajor Medical Expense Benefit will be extended. During the period of extendedbenefits, coverage will apply only to the Disabled Eligible Employee or EligibleDependent, and only for covered charges incurred as a result of the disability forwhich benefits are extended.
As used in this section, Disabled means, with respect to an Eligible Employee, thathe is prevented, solely because of a Non-Occupational Disease or Injury, fromengaging in his regular or customary occupation. An Eligible Employee will notbe deemed to be Disabled during any period in which he is engaged in any otheroccupation for compensation or profit. With respect to an Eligible Dependent,Disabled means that the individual is prevented solely because of disease orAccidental Injury from engaging in substantially all of the normal activities of aperson of like age and sex in good health.
Benefits extended under this provision will terminate on the earliest of:
1. The date on which the Eligible Employee’s or Eligible Dependent’s disabilityterminates,

(59)
2. The last day of the third month following the month in which the benefitswould have otherwise terminated, or
3. The date the Eligible Employee or Eligible Dependent becomes eligible underany other group health plan providing benefits similar to those continuedunder this provision.

(60)
VISION BENEFITS
(Non-Residential Class I, Class III, Class IV and Class V Only)
If a Covered Family Member incurs expenses as a result of a vision examinationmade by a licensed optometrist or ophthalmologist, or for the purchase of lenses orframes, including contact lenses, or for laser-assisted in situ keratomileusis (lasik)surgery or a similar procedure designed to improve vision when performed by amedical doctor (M.D.), he will be entitled to coverage for such expenses subject tothe limitations outlined below and the maximum amount per calendar year out-lined in the Schedule of Benefits.
EXCLUSIONS
Covered charges do not include any charges for:
1. Any lenses which do not require a prescription; or
2. Any service performed or supplies provided in connection with special pro-cedures such as orthoptics or visual training.

(61)
DENTAL BENEFITS
(Non-Residential Class I, Class IV and Class V Only)
This benefit provides for the coverage of the dental services described below whenrendered to a Covered Family Member by a dentist as a result of a Non-OccupationalDisease or Injury, for care and treatment of any disease or defect, or for preventivedental care. Charges covered under this provision are subject to the maximumdental benefit listed in the Schedule of Benefits.
The deductible listed in the Schedule of Benefits is applied separately to eachCovered Family Member. If two or more Covered Family Members in the samefamily are injured in one accident, only one deductible will be applied in eachcalendar year to all of the covered dental charges incurred as a result of that accident.
The following classes of dental services are covered:
• Type A – Preventive Services . . . . . . . . . . . . . . . . . . . . . . . . . . . Paid at 100%
These charges are not subject to the deductible or calendar yearmaximum. Diagnostic and preventive care, including sterilization fees,are covered up to two visits in each calendar year and one full set ofmouth x-rays in any consecutive thirty-six month period.
• Type B – Basic Restorative Services . . . . . . . . . . . . . . . . . . . . . . . Paid at 75%
These charges are subject to the deductible and maximum payment.Restorative (fillings), oral surgery, endodontics and periodonticprocedures are covered.
• Type C – Complex or Major Restorative Services . . . . . . . . . . . . . Paid at 50%
These charges are subject to the deductible and maximum paymentamount. Charges are covered for porcelain crowns, gold crowns, goldinlays, dentures and implants.
• Type D – Orthodontic Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Paid at 100%
Subject to the maximum lifetime benefit listed in the Schedule ofBenefits, payment will be made for orthodontic services rendered toEligible Dependent children only, and only prior to attainment of agenineteen.

(62)
EXCLUSIONS:
No benefit will be paid under this provision for:
1. Treatment or supplies furnished on account of a dental defect which arisesout of, or in the course of, any occupation for wage or profit.
2. Any loss sustained as a result of a declared or undeclared war, or any actthereof, or of military or naval service for any country.
3. Dental procedures performed in a hospital or facility owned by the UnitedStates Government or any agency thereof, unless required by law.
4. Any expense for dental procedures or supplies to the extent that payment isreceived from any other group policy or prepayment plan (individual poli-cies are not affected by this limitation).
5. Orthodontia, except as specifically outlined in this section.
6. Any treatment which is performed for cosmetic purposes.
7. Treatment by other than a legally qualified dentist, except charges for cleaningsperformed by a licensed dental hygienist under the supervision and directionof a dentist.
8. In connection with dentures, bridgework, crowns or prosthetic devices for:
(a) expenses for prosthetic devices started prior to the effective date ofcoverage,
(b) expenses for replacement made less than five years after an immedi-ately preceding placement or replacement,
(c) expenses for extension bridges or prosthetic devices previously paid forby the Fund except for expenses incurred for new extended areas, or
(d) loss or theft.
9. Expenses incurred which are for procedures not completed within a 90-dayperiod after the initial commencement of work for which the claim is made.

(63)
NOTE: These benefits are also provided to the spouses of Class III Retirees untilthe date on which such a spouse becomes eligible for Medicare benefits.

(64)
APPEAL PROCEDURES
A Person whose claim for benefits has been denied under the terms of the plan isentitled to certain rights, including the right to receive a full explanation of thedenial and an opportunity to appeal the denial. The following procedures havebeen adopted by the Board of Trustees explaining those rights:
NOTICE OF ADVERSE BENEFIT DETERMINATION (Notice of Denial)
Upon determination that a claim submitted by or on behalf of a Covered FamilyMember is not covered under the plan, the Eligible Employee or Retiree will benotified in writing within the time frame set forth in this booklet regarding theadverse benefit determination. This notice will set forth, in a manner calculated tobe understood by the claimant, all of the following information:
1. The specific reason or reasons for the adverse determination;
2. Reference to the specific plan provisions on which the determination is based;
3. A description of any additional material or information necessary for theclaimant to perfect the claim and an explanation of why such material orinformation is necessary;
4. A description of the Plan’s review procedures and the time limits applicableto such procedures, including a statement of the claimant’s right to bring acivil action under section 502(a) of the Employee Retirement Income Secu-rity Act of 1974, as amended, following an adverse benefit determination onreview;
5. If an internal rule, guideline, practice or procedure was relied upon in mak-ing the adverse determination, a statement that a copy of such rule, guide-line, practice or procedure will be provided free of charge to the claimantupon request;
6. If the adverse benefit determination is based on medical necessity orexperimental treatment or similar exclusion or limit, an explanation that theclaimant will be provided free of charge upon request an explanation of thescientific or clinical judgment applied to the terms of the plan with respect tothe claimant’s medical circumstances used in making the determination; and

(65)
7. If the claim involves urgent care, a description of the expedited review processapplicable to such claims. If an adverse benefit determination involves anurgent claim, the contents of this notice may be provided orally to the claimant.However, in such instances, this written notification will be furnished to theclaimant not later than three days after the oral notification.
CLAIMANT’S RIGHT TO APPEAL AN ADVERSE BENEFITDETERMINATION
A claimant whose claim for benefits has been denied under the terms of the planand to whom a notice of adverse benefit determination has been issued in accor-dance with the preceding section will have the right to appeal the adverse benefitdetermination and will be entitled to a full and fair review of the decision by theBoard of Trustees, or by a committee appointed by them. The procedures by whichthe claimant may appeal the adverse benefit determination and receive a full andfair review of the claim are as described below. The procedures will:
1. Provide claimants at least 180 days following receipt of a notification of anadverse benefit determination in which to appeal the determination;
2. Provide for an independent review by the Board of Trustees, or their com-mittee. The review will not be conducted by the individual who made theadverse benefit determination that is the subject of the appeal, nor by thesubordinate of such individual;
3. Provide that, in deciding an appeal of any adverse benefit determination thatis based in whole or in part on a medical judgment, including determinationswith regard to whether a particular treatment, drug, or other item is experi-mental, investigational, or not medically necessary or appropriate, the Trust-ees or their committee shall consult with a health care professional who hasappropriate training and experience in the field of medicine involved in themedical judgment;
4. Provide for the identification of medical or vocational experts whose advicewas obtained on behalf of the plan in connection with a claimant’s adversebenefit determination, without regard to whether the advice was relied uponin making the benefit determination;
5. Provide that the health care professional engaged for purposes of this appeal

(66)
is neither an individual who was consulted in connection with the adversebenefit determination that is the subject of the appeal, nor the subordinate ofany such individual; and
6. Provide, in the case of a claim involving urgent care, for an expedited reviewprocess under which —
(a) a request for an expedited appeal of an adverse benefit determinationmay be submitted orally or in writing by the claimant, and
(b) all necessary information, including the Plan’s benefit determination onreview, will be transmitted between the plan and the claimant by tele-phone, facsimile or other available similarly expeditious method.
NOTICE OF TRUSTEES’ DECISION
The Board of Trustees, or their committee, will review all appeals in accordancewith the following and will notify the claimant as indicated:
1. Urgent Care Claims — When the appeal of a claim involving urgent care, asthat term is defined on page 13 of this booklet, is received as provided by thePlan, a decision on the appeal will be made and will be communicated inwriting (and otherwise as appropriate) within 72 hours of receipt of theclaimant’s request for review of an adverse benefit determination. Appealsof adverse benefit determinations involving urgent care will be addressedpromptly by the Trustees, or by their committee, taking into account the urgentnature of the claim, but in no instance will the decision be made later than 72hours after receipt of the claimant’s request.
2. Non-Urgent Care Claims — Appeals of adverse benefit determinationsreceived from claimants which are of a non-urgent care nature shall bereviewed by the Trustees, or their committee, in accordance with the followingguidelines, and notification of the decision shall be communicated in writingto the claimant within the time period prescribed.
(a) Pre-Service Claims — If the appeal involves a request for review of anadverse benefit determination for medical services which have not yetbeen provided, the Trustees or their committee will make a decision onthe appeal and the decision will be communicated in writing to the

(67)
claimant not later than 30 days after receipt of the claimant’s request forreview.
(b) Post-Service Claims — If the claimant’s request for review of an adversebenefit determination involves a claim for medical services which havealready been provided, a decision on the claimant’s appeal will be madeby the Trustees or their committee and communicated in writing to theparticipant within five days of the decision. The appeal will be reviewedat the meeting of the Trustees or the committee which immediatelyfollows the Plan’s receipt of a request for review, unless the request forreview is filed within 30 days preceding the date of such meeting. Insuch case, a benefit determination will be made no later than the date ofthe second meeting following the plan’s receipt of the request for review,but in no instance more than 120 days following receipt of the appeal.
3. Notwithstanding the statements set forth above, notice of every appealsdetermination will be given to the claimant within 5 days of the determination.
ACCESS TO PLAN DOCUMENTS
At any time during the course of these appeal proceedings a claimant will be grantedaccess to, and copies of, documents, records and other information relied upon bythe Trustees or the committee in making their decision, as requested by the claimant.
NOTIFICATION OF DECISION ON APPEAL
Each claimant whose adverse benefit determination has been appealed to theTrustees will receive notification in writing, within the time period outlined above,of the Trustees’ or the committee’s decision. Such notification will set forth, in amanner calculated to be understood by the claimant:
1. The specific reason or reasons for the adverse determination;
2. Reference to the specific plan provisions on which the benefit determinationis based;
3. A statement that the claimant is entitled to receive, upon request and free ofcharge, reasonable access to, and copies of, all documents, records and otherinformation relevant to the claimant’s claim for benefits;

BLANK
4. A statement describing any additional voluntary appeal procedures offeredby the plan and the claimant’s right to obtain information about suchprocedures, should the Board of Trustees adopt such procedures, and astatement of the claimant’s right to bring an action under section 502(a) ofthe Employee Retirement Income Security Act of 1974, as amended; and
5. The following information where applicable —
(a) If an internal rule, guideline, practice or procedure was relied upon inmaking the adverse determination, a statement that such rule, guideline,practice or procedure was relied upon in making the adverse determina-tion and that a copy of the rule, guideline, practice or procedure will beprovided free of charge to the claimant upon request;
(b) If the adverse benefit determination is based on a medical necessity orexperimental treatment or similar exclusion or limit, a statement that anexplanation of the scientific or clinical judgment for the determination,applying the terms of the plan to the claimant’s medical circumstances,will be provided free of charge to the claimant upon request; and
(c) A statement that you and your plan may have other voluntary alternativedispute resolution options, such as mediation. One way to find out whatmay be available is to contact your local U.S. Department of Labor Officeand your State Insurance Regulatory Agency. While the Plan does notcurrently offer voluntary alternative dispute resolution options to theprocedures set forth above, you may contact the Local U.S. Departmentof Labor Office and your State Insurance Regulatory Agency to determinewhat options might be available to the Plan.
COMPLIANCE WITH APPEAL PROCEDURES
1. You may, at your own expense, have legal representation at any stage ofthese Appeal Procedures.
2. Every effort will be made by the Trustees to interpret plan provisions in aconsistent and equitable manner, and you will be given maximum opportu-nity to present your viewpoints regarding any claim for benefits.
(68)

BLANK
3. Every participant and beneficiary will be required to exhaust each and everystep of these Appeal Procedures before he proceeds to litigation, and anyattempt to circumvent these Appeal Procedures in any manner will be resistedby the Trustees.
(69)

BLANK
COORDINATION OF BENEFITS
The objective of this Coordination of Benefits provision is to limit thereimbursement from this Plan and any other plan providing benefits to 100% ofAllowable Expenses. Payments made by the Fund cannot be more than what wouldnormally be paid if this provision did not exist.
Benefits are coordinated with other group plans including the following coverages:
1. Group, blanket, or franchise insurance coverage;
2. Hospital or medical service organizations, group practice and other pre-payment coverage;
3. Any coverage under any labor-management plans, union welfare plans,employer organization plans or employee benefit organization plans; and
4. Any coverage provided under government programs or any coverage requiredor provided by any statute.
ALLOWABLE EXPENSES
Benefits are paid under this Coordination of Benefits provision for AllowableExpenses. In addition to expenses covered under this Plan, Allowable Expensesinclude any necessary, reasonable and customary expense that is covered underanother plan. This does not imply that this Fund would normally pay benefits forsuch expenses. It means that when expenses are calculated to determine theCoordination of Benefits payments, any charge that is covered under another planbut is not covered under this Plan, will, for this purpose only, be considered anAllowable Expense.
CLAIM DETERMINATION PERIOD
The Coordination of Benefits provision is administered on a calendar year basis.This calendar year basis for administration of the Coordination of Benefits provisionis sometimes referred to as the Claim Determination Period. Any benefit savingsresulting from this Coordination of Benefits provision in any calendar year will beheld in a benefit account for that individual for that calendar year. Monies will bereleased from the benefit credit during that calendar year, if necessary, to givereimbursement of 100% of Allowable Expenses.
(70)

BENEFIT DETERMINATION
1. General. When there is a claim under this Plan and another plan, this Plan isa secondary plan which has its benefits determined after those of the otherplan, unless:
(a) the other plan has rules coordinating its benefits with those of this Plan;and
(b) both those rules and this Plan’s rules, in paragraph 2. below, require thatthis Plan’s benefits be determined before those of the other plan.
2. Rules. The Plan determines its order of benefits using the first of the follow-ing rules which applies:
(a) Non-Dependent/Dependent. The benefits of the plan which covers theperson as an employee, member or subscriber (that is, other than as adependent) are determined before those of the plan which covers theperson as a dependent, except under the circumstances outlined in thefollowing sentence. If the person is also a Medicare beneficiary and,under applicable Federal regulations, Medicare is secondary to the plancovering the person as a dependent and primary to the plan covering theperson as other than a dependent (for example as a retired employee),then the benefits of the plan covering the person as a dependent aredetermined before those of the plan covering that person as other than adependent.
(b) Dependent Child/Parent Not Separated or Divorced. Except as stated insubparagraph (3) below, when this Plan and another plan cover the samechild as a dependent of different persons:
(1) the benefits of the plan of the parent whose birthday falls earlier ina year are determined before those of the plan of the parent whosebirthday falls later in that year; but
(2) if both parents have the same birthday, the benefits of the plan whichcovered the parent longer are determined before those of the planwhich covered the other parent for a shorter period of time.
(71)

(3) However, if the other plan does not have the rule described in (1)immediately above, but instead has a rule based upon the gender ofthe parent, and if, as a result, the plans do not agree on the order ofbenefits, the rule in the other plan will determine the order of ben-efits.
(c) Dependent Child/Separated or Divorced Parents. If two or more planscover a person as a dependent child of divorced or separated parents,benefits for the child are determined in this order:
(1) first, the plan of the parent with custody of the child; and
(2) then, the plan of the spouse of the parent with custody of the child;and
(3) finally, the plan of the parent not having custody of the child.
However, if the specific terms of a court decree state that one of theparents is responsible for the health care expenses of the child, and theindividual obligated to pay or provide the benefits of the plan of thatparent has actual knowledge of those terms, the benefits of that plan aredetermined first. This paragraph does not apply with respect to any ben-efits which are actually paid or provided before the individual has thatactual knowledge.
When the group health plan with which this plan is being coordinateddoes not contain the rules described in this sub-paragraph (c), the plancovering the dependent as a dependent of a male shall be the primaryplan and the plan covering the dependent as a dependent of a femaleshall be the secondary plan.
(d) Joint Custody. If the terms of a court decree state that the parents shallshare joint custody, without stating that one of the parents is responsiblefor the health care expenses of the child, the plans covering the childshall follow the Order of Benefit Determination Rules outlined under(b) above.
(e) Active/Inactive Employee. The benefits of a plan which covers a personas an employee who is neither laid off nor retired (or as that employee’s
(72)

dependent) are determined before those of a plan which covers that per-son as a laid off or retired employee (or as that employee’s dependent).If the other plan does not have this rule, and if, as a result, the plans donot agree on the order of benefits, this section (e) is ignored.
(f) Continuation Coverage. If a person whose coverage is provided under aright of continuation under Federal or State Law also is covered underanother group health plan, the following will be the order of benefitdetermination;
(1) First, the benefits of the plan covering the person as an employee,member or subscriber (or as that person’s dependent);
(2) Second, the benefits under the continuation coverage.
If the other plan does not have the rule described above, and if as a resultthe plans do not agree on the order of benefits, this rule is ignored.
(g) Longer/Shorter Length of Coverage. If none of the above rules deter-mines the order of benefits, the benefits of the plan which covered anemployee, member or subscriber longer are determined before those ofthe plan which covered that person for the shorter time.
RIGHT TO RECEIVE AND RELEASE NECESSARY INFORMATION
For the purpose of determining the applicability of and implementing the terms ofthis provision of this Plan or any provision of similar purpose of any other plan,this Plan may, without the consent of or notice to any other person, release to orobtain from any insurance company or other organization or person, anyinformation, with respect to any person, which the Fund deems to be necessary forsuch purposes. Any person claiming benefits under this Plan will be required tofurnish to the Fund such information as may be necessary to implement thisprovision.
RIGHT OF RECOVERY
Whenever payments have been made in error by the Fund in excess of CoveredCharges, the Fund shall have the right to recover such payments, to the extent ofany excess payment, from among one or more of the following, as the Fund shalldetermine:
(73)

1. The Eligible Employee or Retiree,
2. The payee, if other than the Eligible Employee or Retiree,
3. Any insurance company or other organization furnishing coverage to theCovered Family Member, or
4. Any further claims made to this Fund by the Covered Family Member.
GENERAL
Under the Coordination of Benefits Provision, it is necessary that claim be madefor any benefits the individual may be entitled to from any source. Whether or notclaim is made to these other sources, the Coordination of Benefits Provision willbe fully operable as if claim were made.
COORDINATION WITH MEDICARE
Regardless of any other provisions to the contrary, this Fund’s benefits will be paidprimary to those of Medicare in behalf of any Eligible Employee, or the EligibleDependent of any Eligible Employee, unless:
1. The Eligible Employee or Eligible Dependent, has elected, in accordancewith procedures established by the Trustees under appropriate federal law, tohave Medicare as his or her primary coverage, or
2. The Eligible Employee or Eligible Dependent is entitled to Medicare benefitsas a result of end stage renal disease, in which case benefits are coordinatedas outlined below. During the period outlined below, this Plan’s benefits willbe determined before any benefits payable by Medicare in behalf of anyCovered Family Member who is entitled to Medicare benefits due to endstage renal disease. This period of primary coverage for the Plan will beginon the earliest of the following and will end 30 months afterward:
(a) The month in which the Covered Family Member began a regular courseof renal dialysis,
(b) The month in which the Covered Family Member received a kidneytransplant,
(74)

(75)
(c) The month in which the Covered Family Member was admitted to aHospital in anticipation of a kidney transplant that was performed withinthe next two months, or
(d) The second month before the month in which the kidney transplant wasperformed, if performed more than two months after admission.
COORDINATION OF DUAL COVERAGE BY HUSBAND AND WIFE
If a husband and wife are both eligible for benefits under the Plan as EligibleEmployees, benefits for such husband and wife and their Eligible Dependentchildren shall be coordinated and shall be paid on the basis of paying the maximumamount available based upon the eligibility of both husband and wife, provided,however, that in no event shall the total benefits paid for any Covered FamilyMember exceed the total amount of expenses incurred on behalf of such individual.

SUBROGATION AND REIMBURSEMENT
In the event that an Eligible Employee or Eligible Dependent (collectively referredto as a “Covered Family Member”) receives any benefits (the “Benefits”) underthis Plan arising out of any loss, injury, or illness (the “Injury”) for which theCovered Family Member has asserted or may assert any claim or right to recoveryagainst a third party or parties or his or her or their insurer(s), except against anyinsurer on any policy of insurance issued to and in the name of such CoveredFamily Member, then any payment or payments by the Fund for such benefitsshall be made on the condition and with the agreement and understanding that theFund shall be reimbursed by the Covered Family Member to the extent of, but notexceeding, the amount or amounts received by the Covered Family Member (the“Recovery”) from such third party or parties or his or her or their insurer(s) (the“Responsible Party”), whether by way of settlement or in satisfaction of anyjudgment(s) or otherwise.
The Covered Family Member shall reimburse the Fund, starting with the first dollarthat the Covered Family Member receives from the Responsible Party, no matterwhether the Recovery is designated as actual or punitive damages, costs or expenses,medical expenses, pain and suffering, lost wages, workers’ compensation, disabilitypayments, loss of consortium, loss of work payments, emotional distress, orotherwise, and the Covered Family Member shall continue to reimburse the Funduntil all Benefits related to the Injury are reimbursed or the full amount of theRecovery is paid to the Fund, whichever occurs first.
The Fund has the right to first recovery and the “make whole” doctrine is notapplicable to the Fund’s subrogation and reimbursement rights. The Fund has theright of first reimbursement for all Benefits paid related to the Injury, such firstreimbursement to be paid out of any Recovery the Covered Family Member isable to obtain, even if the Covered Family Member has not been fully compensatedfor the Injury.
The Fund does not recognize the “common-fund doctrine,” the “Fund Doctrine,”the “Attorneys’ Fund Doctrine,” or any other legal theory compelling the Fund toreduce the amount it is owed hereunder in order to pay any portion of a CoveredFamily Member’s attorney’s fees and costs. Rather, if it becomes necessary for theCovered Family Member to retain an attorney in order to obtain a Recovery or torecover Benefits paid by the Fund relating to the Injury, the amount to be reimbursedto the Fund may, at the sole discretion of the Fund, be reduced by the Fund’s prorata share of those attorneys’ fees and expenses.
(76)

(77)
If the Trustees retain an attorney to recover any amounts that are owed under thisprovision, then the Covered Family Member shall be liable for, in addition to allamounts outlined in the previous paragraphs, all costs of collection of the Fund,including the Fund’s reasonable attorneys’ fees and expenses. As a means ofcollecting the amount owed under this provision, the Fund may, in addition to anyother means allowed by law, set off future Benefits to the Covered Family Memberor lessen the reduction allowed by the Fund for the Covered Family Member’sattorneys’ fees and expenses incurred in obtaining the Recovery. However, thisprovision shall not limit the Fund’s right to collect its attorneys’ fees and expensesand shall be cumulative with all other rights the Fund may have to collect itsattorneys’ fees and expenses.
As security for all amounts due to the Fund under this provision, the Fund shall besubrogated to all of the claims, demands, actions, and rights of recovery of theCovered Family Member against the Responsible Party or his, her, or their insurer(s)to the extent of any and all Benefits paid under this Plan. The Covered FamilyMember shall execute and deliver any instruments and documents requested bythe Trustees and shall do whatever else the Trustees shall deem necessary to protectthe Fund’s rights. The Covered Family Member shall take no action to prejudicethe Fund’s rights to such reimbursements and subrogation. The Trustees maywithhold any Benefits to which the Covered Family Member is entitled under thisPlan until the Covered Family Member executes and delivers any such instrumentsand documents as may be requested by the Trustees.
Prior to the payment of Benefits under this Plan to a Covered Family Member orassignee of a Covered Family Member for injuries, expenses, or losses for which athird party is or may be liable in whole or part, the Covered Family Member orassignee or both may be required to execute a written subrogation andreimbursement agreement in form and substance satisfactory to the Plan.

INFORMATION YOU SHOULD KNOW
THIS BOOKLET IS ONLY A SUMMARY
Although this booklet contains a great deal of information about your Plan, it isnot the purpose of this booklet to cover every detail or every situation that mightarise under your Plan.
However, there is a complete set of rules and regulations which governs theoperation and administration of this Plan. These rules and regulations are set forthin a legal document referred to as the Plan document.
So that you have all the details readily available, a copy of the Plan document willbe made available for your examination at the Fund office or a copy of it will bereproduced for you at your request for a reasonable charge.
The rules and regulations set forth in the Plan document are final and binding.Nothing in this booklet is meant to interpret or extend or change in any way theprovisions expressed in the Plan document itself. If there is any difference betweenthe Plan document and the summary in this booklet, the Plan document will control.
THE TRUSTEES INTERPRET THE PLAN
Any interpretation of the Plan’s provisions rests with the Board of Trustees.However, the Board of Trustees has authorized the administrative manager and theFund office staff to handle routine requests from participants regarding eligibilityrules, benefits and claims procedures. But, if there are questions involvinginterpretation of any Plan provisions, the administrative manager will secure fromthe Board of Trustees a final determination for you. No person other than a Trusteeor a member of the Fund office staff, acting with the consent of the full Board ofTrustees, may provide interpretations of Plan provisions.
THE PLAN MAY BE CHANGED
The Trustees are endowed with the authority to change the Plan, subject to anycollective bargaining agreement that applies to it.
Although the Trustees expect to maintain and to improve benefits, this can only bedone within the limits of available financial resources. The Trustees have an
(78)

obligation to make whatever Plan changes are necessary to assure the financialstability of this Plan.
The Trustees also may change the Plan in any way to protect its tax exempt statusunder Internal Revenue Service rules. From time to time, these rules may changeand the Trustees may have to alter certain Plan provisions in order to preserve thetax exempt status of your Plan.
YOUR PLAN IS TAX EXEMPT
The Internal Revenue Code provides that your employers’ contributions to theTrust are not taxable to you nor are most of the benefits paid on your behalf taxableas personal income. Also, investment earnings on Plan assets are excluded as taxableincome of the Trust since they are specifically set aside for the purpose of providingbenefits to participants.
Obviously, such tax exemption works to the benefit of both employer and employee.In effect, it means that money which otherwise might be payable as taxes can beused to purchase benefits and to cover administrative expenses.
The Trustees are well aware of these advantages and will take whatever steps arenecessary to keep your Plan “qualified” as a tax exempt trust under Internal RevenueService rules.
PAYMENT AND ASSIGNMENT OF BENEFITS
Benefits which are payable under this Plan and which have not been assigned to aprovider of covered services will be paid to you, whether the claim is made onbehalf of yourself or one of your dependents, unless benefits are being providedunder a Qualified Medical Child Support Order, as that term is defined in theOmnibus Budget Reconciliation Act of 1993. In such case, benefits otherwisepayable to you will generally be paid to the custodial parent or legal guardian ofthe dependent child on behalf of whom the benefits are provided.
You may assign benefits which are payable to you under this Plan, but only to amedical service provider. If benefits are provided under a Qualified Medical ChildSupport Order, benefits may also be assigned by the custodial parent or legalguardian of the dependent child on whose behalf the benefits are provided. Benefitassignments made in accordance with any state Medicaid law will also be honoredby the Plan.
(79)

QUALIFIED MEDICAL CHILD SUPPORT ORDERS
As explained under the previous heading, the Fund will honor the provisions of aQualified Medical Child Support Order. The Fund office has established proce-dures for determining whether such an order meets all of the legal requirements. Acopy of these procedures will be furnished to you, without charge, upon writtenrequest filed with the Fund office.
MEDICAL EXAMINATION
Although you will not be required to undergo a physical examination to attaineligibility or to remain eligible for benefits under this Plan, the Trustees may requirea medical examination of you or any one of your dependents in determining coveragefor a claim under the Plan. They may also require an autopsy in the event of death,where it is not forbidden by law.
NOTICE AND PROOF OF CLAIMS
1. A written notice of the injury or of the illness for which a Covered FamilyMember is making claim must be given to the Trustees as soon as possible,and all forms, bills and information necessary to pay the claim must be pro-vided within 180 days of the end of the calendar year in which the claim wasincurred.
2. If the individual does not furnish notice and data within the time provided bythe Plan, such lack of notice will not jeopardize the claim if it is shown thatit was not reasonably possible to furnish such notice when required and suchnotice was furnished as soon as it was reasonably possible.
INCURRED DATE
A claim will be considered to be incurred on the date on which the services orsupplies are rendered or obtained. For inpatient Hospital claims this means that theincurred date for any particular charge is the date of admission. For benefits pay-able due to death or dismemberment, the claim will be considered to be incurredon the date of the death or dismemberment. Claims for Loss of Time Benefits willbe considered to be incurred on each day for which those benefits are payable.
(80)

PAYMENT OF BENEFITS
1. Except in the case of Death Benefits and Accidental Death Benefits, benefitsare payable to the Eligible Employee whether the claim is on the EligibleEmployee or on one of the employee’s Eligible Dependents. If benefits areassigned, however, benefits will be paid to the assignee instead of directly tothe Eligible Employee. Benefits are payable when the required forms havebeen submitted to the Plan.
2. If an individual, in the Trustees’ opinion, is not capable of giving a validreceipt for payments due and no guardian has been appointed for such per-son, the Trustees may make payment to the individual or individuals who, intheir opinion, has assumed the care and principal support of the individual. Ifthe individual should die before all amounts that are due have been paid, theTrustees may, at their option, make payment to the executor or administratorof the estate of the individual or to his surviving spouse, parent, child orchildren or to any individual who, in the Trustees’ opinion, is entitled to thebenefits.
3. Any payments that are made by the Trustees in accordance with these provi-sions shall fully discharge the liability of the Trustees to the extent of thepayments.
NO CONVERSION PRIVILEGE
These benefits cannot be converted to individual coverage.
CONSTRUCTION BY TRUSTEES
The Trustees have full authority and discretion to construe the provisions of thisPlan and any construction placed upon the Plan by the Trustees shall be final andbinding upon all parties.
TERMINATION OF FUND
The information regarding the conditions under which the Fund may be termi-nated, and disposition of the assets of the Fund on termination, are furnished inaccordance with Federal Laws and Regulations.
(81)

The Fund will be terminated upon the termination of the Trust Agreement estab-lishing the Fund. The Trust Agreement will terminate upon the occurrence of ei-ther of the following events:
1. In the event the Union and the contributing employers agree in writing toterminate the Trust; or
2. In the event the Trustees decide to terminate the Trust when there is no longera written agreement requiring employers to contribute to the Fund.
In the event the Trust is terminated, any remaining funds available, after meetingall outstanding obligations, will be used in such a manner as will, in the opinion ofthe Trustees, best effectuate the purposes of the Trust including, but not limited to,the purchase of insurance benefits or the transfer of such remaining funds to an-other health and welfare trust. In no event shall any of the funds revert to or berecovered by any employee (except as benefits payable under the Fund), employeror union.
STATEMENT OF RIGHTS UNDER THE NEWBORNS’ AND MOTHERS’HEALTH PROTECTION ACT
Under federal law, group health plans and health insurance issuers offering grouphealth insurance coverage generally may not restrict benefits for any hospital lengthof stay in connection with childbirth for the mother or newborn child to less than48 hours following a vaginal delivery, or less than 96 hours following a deliveryby cesarean section. However, the plan or issuer may pay for a shorter stay if theattending provider (for example, your physician, nurse midwife, or physicianassistant), after consultation with the mother, discharges the mother or newbornearlier.
Also, under federal law, plans and issuers may not set the level of benefits or out-of-pocket costs so that any later portion of the 48-hour (or 96-hour) stay is treatedin a manner less favorable to the mother or newborn than any earlier portion of thestay.
In addition, a plan or issuer may not, under federal law, require that a physician orother health care provider obtain authorization for prescribing a length of stay ofup to 48 hours (or 96 hours).
(82)

IMPORTANT NOTICE REGARDING THE WOMEN’S HEALTH ANDCANCER RIGHTS ACT
Under federal law, group health plans and insurance issuers offering group healthinsurance coverage that includes medical and surgical benefits with respect to amastectomy shall include medical and surgical benefits for breast reconstructivesurgery as part of a mastectomy procedure. Breast reconstructive surgery in con-nection with a mastectomy shall at a minimum provide for: (1) reconstruction ofthe breast on which the mastectomy has been performed; (2) surgery and recon-struction of the other breast to produce a symmetrical appearance; and (3) prosthe-ses and physical complications for all stages of mastectomy, includinglymphedemas; in a manner determined in consultation with the attending physi-cian and the patient. As part of the Plan’s Schedules of Benefits, such benefits aresubject to the Plan’s appropriate cost control provisions such as deductibles andcopayments.
NOTICE TO ACTIVE PARTICIPANTS AND THEIR SPOUSES WHO AREELIGIBLE FOR MEDICARE
This notice is required by federal law. It is addressed to active participants onlyand does not apply to Retirees. It concerns your health care benefits once youreach age 65 if you or your spouse are eligible for Medicare and are also eligiblefor coverage under this Fund. In accordance with that law, coverage under thisFund is made available to all active participants age 65 or older and their spousesunder the same conditions as coverage is made available to active eligibleparticipants and spouses of eligible participants under age 65. In addition, federalstatutes currently provide that any persons age 65 or older are entitled to selectMedicare for their primary health insurance coverage in place of any group healthplan offered by their employer. We would therefore urge you, if you are an activeeligible participant under the Plan and eligible for Medicare benefits, to read thefollowing:
If you are eligible for coverage under the Plan, federal law requires that the Planpay first up to the maximum amounts provided for under the Plan and then Medicarecoverage be applied up to the maximum limits provided under Medicare. Thisapplies to active participants age 65 or older as well as the dependent spouses age65 or older of active participants.
Federal law does permit an active participant who is age 65 or older, or the dependentspouse age 65 or older of an active participant, to reject the group health care plan
(83)

as the primary payer of his or her benefits and to elect Medicare as the primarypayer of benefits. Although such an election will reduce the Plan’s expenses, itwill generally not work to the advantage of a participant or his spouse. In fact, ifMedicare is elected as the primary payer, a participant or spouse is likely to incurhigher out-of-pocket medical expenses than would be the case if the Plan is theprimary payer of benefits. The reason for this is that if you or your spouse electMedicare as the primary payer, the Plan is not permitted under federal law to provideany supplemental coverage for hospital or surgical expenses. The Plan is permitted,however, to provide and will continue to provide death benefits, accidental deathand dismemberment benefits, loss of time benefits, prescription drug coverageand vision and dental benefits, as applicable, even if you or your spouse selectMedicare as the primary payer.
Also, if Medicare is elected as the primary payer, the Plan is not permitted to payany of the deductibles or co-insurance required for Medicare services. If for somereason, you or your spouse would rather have Medicare as the primary payer, youeach have the right to indicate this preference in writing to the Fund office. Suchelection can be made upon becoming eligible for Medicare, or at any time thereafter.If you do not make a written election, this Fund will continue to be your primaryprovider of health coverage.
In making this decision, we urge you and your spouse to carefully compare thebenefits provided under this Plan, as outlined in this booklet, and the benefitsavailable under Medicare. A description of Medicare benefits can be obtained fromyour local Social Security office or the Fund office will provide you with adescription of those benefits upon your request. Since the Plan’s benefits are usuallymore generous than Medicare benefits, it generally will not be advantageous foryou or your spouse to elect Medicare as the primary payer of benefits. Remember,if you select Medicare as the primary payer, the Plan may not supplement Medicarecoverage in any way and you will be totally responsible for any medical expensesnot covered by Medicare.
As you probably know, Part A Medicare coverage is provided at no charge to allindividuals who are age 65 and older. However, in order to be entitled to Part AMedicare, it is necessary that you enroll for such coverage. It is therefore extremelyimportant that you enroll for Medicare at least three months before your 65thbirthday, even if you intend to continue working beyond age 65. If you have alreadyreached your 65th birthday and have not applied for Medicare, we would encourageyou to determine the date the next Medicare enrollment period begins and makearrangements to apply at that time.
(84)

These provisions do not apply to Retirees.
Please contact the Fund office for assistance and information regarding this notice.
PROTECTED HEALTH INFORMATION
The Health Insurance Portability and Accountability Act of 1996 (HIPAA)established a comprehensive set of rules for handling and disclosing confidentialhealth information (called protected health information or “PHI”). PHI is anyinformation relating to your health, the provision of health care to you, payment ofyour health claims and your eligibility for health claims.
The Atlanta Plumbers and Steamfitters Health and Welfare Fund is bound by HIPAAto protect your PHI, and that of your dependents, by treating all such informationas confidential. While such treatment will generally prove beneficial to you, itmay sometimes inconvenience you when calling or corresponding with the Fundoffice to check on or discuss the health claims of other family members. Federallaw will not allow us to divulge PHI on other adult family members, such as yourhusband or wife, without their written permission. Generally, parents will haveaccess to the PHI of their minor children.
Authorization forms are available in the Fund office that are designed to allow youor your spouse to designate another individual or individuals, such as each other,to have access to your PHI. The information required for this authorization is veryspecific, and no forms other than the one furnished by the Fund office will behonored.
Remember, the Fund office is bound by federal law to restrict access to your PHI.If you want to allow such access by another person, you must complete an approvedauthorization form.
NOTICE REGARDING THE AFFORDABLE CARE ACT (HEALTH CAREREFORM)
This group health plan believes that it is a “grandfathered health plan” under thePatient Protection and Affordable Care Act (the Affordable Care Act). As permittedby the Affordable Care Act, a grandfathered health plan can preserve certain basichealth coverage that was already in effect when that law was enacted. Being agrandfathered health plan means that your plan may not include certain consumer
(85)

protections of the Affordable Care Act that apply to other plans, for example, therequirement for the provision of preventive health services without any cost sharing.However, grandfathered health plans must comply with certain other consumerprotections in the Affordable Care Act, for example, the elimination of lifetimelimits on benefits.
Questions regarding which protections apply and which protections do not applyto a grandfathered health plan and what might cause a plan to change fromgrandfathered health plan status can be directed to the plan administrator at theaddress and telephone numbers listed on the inside front cover of this booklet. Youmay also contact the Employee Benefits Security Administration, U.S. Departmentof Labor at 1-866-444-3272 or www.dol.gov/ebsa/healthreform. This website hasa table summarizing which protections do and do not apply to grandfathered healthplans.
(86)

RIGHTS OF PLAN PARTICIPANTS
As a participant in this Fund, you are entitled to certain rights and protectionsunder the Employee Retirement Income Security Act of 1974 (ERISA). ERISAprovides that all Plan participants shall be entitled to:
RECEIVE INFORMATION ABOUT YOUR PLAN AND BENEFITS
Examine, without charge, at the Plan administrator’s office and at other specifiedlocations, such as worksites and union halls, all documents governing the Plan,including collective bargaining agreements, and a copy of the latest annual report(Form 5500 Series) filed by the Plan with the U.S. Department of Labor andavailable at the Public Disclosure Room of the Employee Benefits SecurityAdministration.
Obtain, upon written request to the Plan Administrator, copies of documentsgoverning the operation of the Plan, including collective bargaining agreements,and copies of the latest annual report (Form 5500 Series) and updated summaryplan description. The administrator may make a reasonable charge for the copies.
Receive a summary of the Plan’s annual financial report. The Plan Administratoris required by law to furnish each participant with a copy of this summary annualreport.
CONTINUE GROUP HEALTH PLAN COVERAGE
Continue health care coverage for yourself, spouse or dependent if there is a lossof coverage under the plan as a result of a qualifying event. You or your dependentsmay have to pay for such coverage. Review this summary plan description and thedocuments governing the plan for the rules governing your COBRA continuationcoverage rights.
Reduction or elimination of exclusionary periods of coverage for preexistingconditions under your group health plan, if you have creditable coverage fromanother plan. You should be provided a certificate of creditable coverage, free ofcharge, from your group health plan or health insurance issuer when you losecoverage under the plan, when you become entitled to elect COBRA continuationcoverage, when your COBRA continuation coverage ceases, if you request it beforelosing coverage, or if you request it up to 24 months after losing coverage. Without
(87)

evidence of creditable coverage, you may be subject to a preexisting conditionexclusion for 12 months (18 months for late enrollees) after your enrollment datein your coverage.
PRUDENT ACTIONS BY PLAN FIDUCIARIES
In addition to creating rights for plan participants, ERISA imposes duties upon thepeople who are responsible for the operation of the employee benefit plan. Thepeople who operate your plan, called “fiduciaries” of the plan, have a duty to do soprudently and in the interest of you and other plan participants and beneficiaries.No one, including your employer, your union or any other person, may fire you orotherwise discriminate against you in any way to prevent you from obtaining awelfare benefit or exercising your rights under ERISA.
ENFORCE YOUR RIGHTS
If your claim for a welfare benefit is denied or ignored, in whole or in part, you havea right to know why this was done, to obtain copies of documents relating to thedecision without charge, and to appeal any denial, all within certain time schedules.
Under ERISA, there are steps you can take to enforce the above rights. For instance,if you request a copy of Plan documents or the latest annual report from the Planand do not receive them within 30 days, you may file suit in a Federal court. Insuch a case, the court may require the Plan Administrator to provide the materialsand pay you up to $110 a day until you receive the materials, unless the materialswere not sent because of reasons beyond the control of the administrator. If youhave a claim for benefits which is denied or ignored, in whole or in part, you mayfile suit in a state or Federal court. In addition, if you disagree with the Plan’sdecision or lack thereof concerning the qualified status of a domestic relationsorder or a medical child support order, you may file suit in a Federal court. If itshould happen that Plan fiduciaries misuse the plan’s money, or if you arediscriminated against for asserting your rights, you may seek assistance from theU.S. Department of Labor, or you may file suit in a Federal court. The court willdecide who should pay court costs and legal fees. If you are successful, the courtmay order the person you have sued to pay these costs and fees. If you lose, thecourt may order you to pay these costs and fees, for example, if it finds your claimis frivolous.
(88)

ASSISTANCE WITH YOUR QUESTIONS
If you have any questions about your Plan, you should contact the PlanAdministrator. If you have any questions about this statement or about your rightsunder ERISA, or if you need assistance in obtaining documents from the PlanAdministrator, you should contact the nearest office of the Employee BenefitsSecurity Administration, U.S. Department of Labor, listed in your telephonedirectory or the Division of Technical Assistance and Inquiries, Employee BenefitsSecurity Administration, U.S. Department of Labor, 200 Constitution Avenue N.W.,Washington, D.C. 20210. You may also obtain certain publications about yourrights and responsibilities under ERISA by calling the publications hotline of theEmployee Benefits Security Administration.
(89)

INFORMATION OF INTEREST AS REQUIRED BY THEEMPLOYEE RETIREMENT INCOME SECURITY ACT (ERISA)
You most likely have heard about ERISA. ERISA stands for the EmployeeRetirement Income Security Act which was signed into law in 1974.
This federal law establishes certain minimum standards for the operation ofemployee benefit plans including the Atlanta Plumbers and Steamfitters Healthand Welfare Fund. The Trustees of your Plan, in consultation with their professionaladvisors, have reviewed these standards carefully and have taken whatever stepsare necessary to assure full compliance with ERISA.
ERISA requires that plan participants and beneficiaries be provided with certaininformation about their benefits, how they may qualify for benefits, and theprocedure to follow when filing a claim for benefits. This information is presentedto you in this booklet.
ERISA also requires that participants and beneficiaries be furnished with certaininformation about the operation of the Plan and about their rights under the Plan.This information follows:
NAME OF THIS PLAN
The legal and common name of this Plan is the Atlanta Plumbers and SteamfittersHealth and Welfare Fund.
TYPE OF PLAN
This plan provides death, accidental death and dismemberment, loss of time,comprehensive major medical, dental and vision benefits.
For specific coverage see the Schedules of Benefits outlined in this booklet.
NAME AND ADDRESS OF THE PLAN ADMINISTRATOR AS DEFINEDBY ERISA
Your Health Plan is maintained and administered by a Board of Trustees on whichlabor and management are equally represented.
(90)

There are five labor Trustee and five management Trustee positions on the Board.A list of all of the Trustees as of the date this booklet was prepared is contained inthe front of this booklet.
This Board has the primary responsibility for decisions regarding eligibility rules,types of benefits, administrative policies, management of Plan assets andinterpretation of Plan provisions.
Any communication with the Board of Trustees should be addressed to the Fundoffice at:
Board of TrusteesAtlanta Plumbers and Steamfitters Health and Welfare Fund
3835 Presidential Parkway, Suite 123Atlanta, Georgia 30340
TYPE OF ADMINISTRATION
Although the Trustees are legally designated as the Plan Administrator, they havedelegated the performance of the day-to-day administrative duties to a professionaladministrative manager, Southern Benefit Administrators, Incorporated.
The Fund office staff maintains the eligibility records, accounts for employercontributions, processes claims, informs participants of Plan changes and performsother routine administrative functions in accordance with Trustee decisions.
COLLECTIVE BARGAINING AGREEMENTS
This Plan is maintained pursuant to one or more collective bargaining agreements.Copies of any or all of these agreements will be made available to you for yourinspection and a copy of any or all of these agreements may be examined at thePlan office during normal business hours or at your local union office during normalbusiness hours. Further, should you so request, a copy of the agreements will bemade available at your place of employment within 10 days of your request if youwill advise your employer of your desire to examine the agreements. If you requesta copy of the agreements, a reasonable charge for them will be made by theadministrator, the amount of which will be stated to you before you order.
PLAN SPONSORS
The Board of Trustees is the Plan sponsor. The Board of Trustees consists of an
(91)

equal number of employer and union representatives, selected by the employersand the unions that have entered into collective bargaining agreements that relateto the Fund. The names and addresses of the current members of the Board ofTrustees are listed on pages 1 and 2 of this booklet. If you wish to contact theBoard of Trustees, you may use the address and telephone number below:
Board of TrusteesAtlanta Plumbers and Steamfitters Health and Welfare Fund
3835 Presidential Parkway, Suite 123Atlanta, Georgia 30340
Phone: (770) 455-3802, Toll-Free: (800) 382-6926
Participants and beneficiaries may receive from the Fund office, upon writtenrequest, information as to whether a particular employer or union has entered intoa collective bargaining agreement that relates to the Fund and thus is a sponsor ofthe Fund and, if the particular employer or union is a sponsor, the employer’s orunion’s address.
SOURCE OF CONTRIBUTIONS
The primary source of financing for the benefits provided under this Plan is employercontributions. The rate of contribution is spelled out in the collective bargainingagreements negotiated by the unions with participating employers.
No money is ever deducted from your paycheck to pay for Plan benefits. However,under the terms of this Plan, a participant may make self-contributions in order toretain his eligibility if he does not work sufficient hours.
A portion of the Plan assets are invested and this produces additional Fund income.
FUNDING MEDIUM FOR THE ACCUMULATION OF PLAN ASSETS
All contributions and investment earnings are accumulated in a trust fund. Benefitsare provided directly from the trust fund. Some plan assets are invested.
CIRCUMSTANCES THAT MAY RESULT IN LOSS OF ELIGIBILITY ORBENEFITS
Throughout this booklet those circumstances that might lead to a loss of your
(92)

eligibility and a description of the limitations, exclusions or restrictions applicableto specific benefits are explained to you.
Please familiarize yourself with this information, especially as it relates to therequirements which must be met in order to maintain your eligibility or make upthe difference by timely self-payments. If at any time you are uncertain about howspecific circumstances might affect your eligibility or benefit coverage, pleasecontact the Fund office and, if possible, do so before the circumstances arise.
AGENT FOR SERVICE OF LEGAL PROCESS
Every effort will be made by the Trustees of this Plan to resolve any disagreementswith participants promptly and equitably. It is recognized, however, that on occasion,some participants may feel that it is necessary for them to take legal action. Beadvised that the following has been designated as agent for service of legal process:
Mr. Charles ElrodParker, Hudson, Rainer & Dobbs, LLP
1500 Marquis Two Tower285 Peachtree Center Avenue, N.E.
Atlanta, Georgia 30303
Or legal papers may be served on the Board of Trustees collectively or individuallyas well as the Fund office manager.
PLAN IDENTIFICATION NUMBERS
When filing various reports with the Department of Labor and the Internal RevenueService, certain numbers are used to properly identify the Atlanta Plumbers andSteamfitters Health and Welfare Fund including:
Employer Identification Number (EIN) assigned by the Internal Revenue Service . . . . . . . . . . . . . . . . . 58-0625978Plan Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 501
FISCAL YEAR
The accounting records of this Plan are kept on the basis of a fiscal year whichends on December 31.
(93)

This Booklet
Designed By
SOUTHERN BENEFIT
ADMINISTRATORS, INCORPORATED