atopic dermatitis
TRANSCRIPT

PEDIATRIC ALLERGY AND IMMUNOLOGY 08894561/99 $8.00 + .OO
ATOPIC DERMATITIS
Elizabeth Harrigan, MD, and Linda G. Rabinowitz, MD
Atopic dermatitis (AD) is a chronic condition that affects nearly 10% of all children and is often the first clinical manifestation of atopy. It is a complex multifactorial disorder that typically has its onset during the first year of life. The diagnosis is established by noting the presence of pruritus, a chronic relaps- ing course, and a personal or family history of atopy, in addition to particular morphologic features, a characteristic distribution, and associated physical find- ings (Table 1). Although the exact cause is not known, AD occurs in genetically predisposed individuals, with 80% of affected children having a personal or family history of atopy. The precise pathogenesis is unclear, but eosinophil, mast cell, and lymphocyte activation triggered by elevated production of interleukin- 4 ( IL4) by specific T-helper lymphocytes seems to be involved.
CLINICAL FEATURES
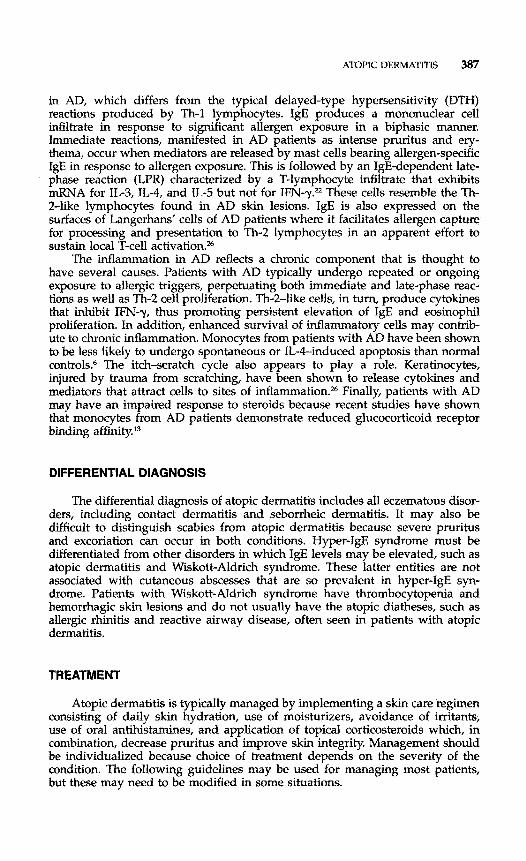
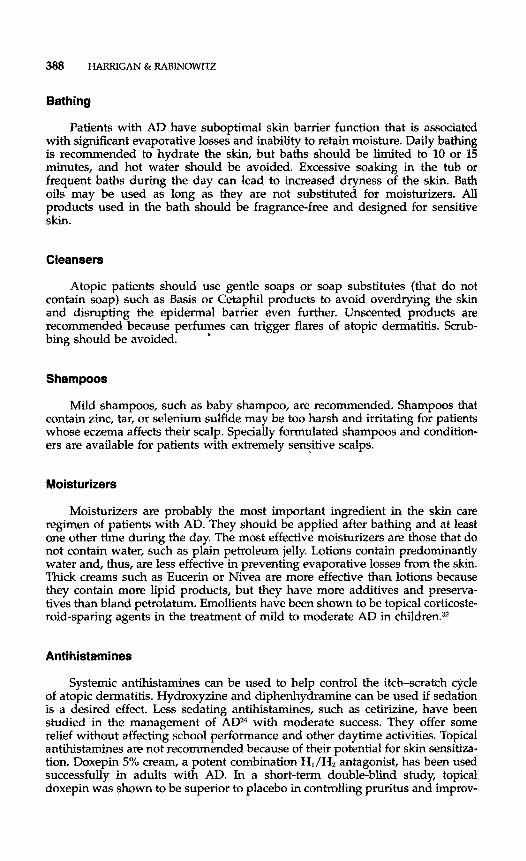
AD can develop at any age but most' often has its onset during the first 6 months of life. Approximately 50% of affected individuals will have symptoms during the first year, and the majority of patients with AD will develop allergic rhinitis or asthma later in childhood. In infants, atopic dermatitis typically involves the face, scalp, trunk, and extensor surfaces of the limbs (Fig. 1). Older children and adolescents have involvement primarily of the flexural areas, including the antecubital and popliteal fossae, wrists, and ankles (Fig. 2). Pruri- tus is the hallmark of atopic dermatitis. The primary skin lesions are papules or vesicles and are typically associated with erythema and white scale. In the acute phase, scratching leads to excoriation and subsequent oozing and crusting. Chronic skin changes include thickening, lichenification, and hypo- or hyperpig- mentation. Follicular prominence, which gives the skin a goosebump-like tex- ture, is often seen in patients with AD.
From the Department of Pediatrics (EH, LGR) (Dermatology [LGR]) and Division of Allergy and Immunology (EH), Medical College of Wisconsin, Milwaukee, Wisconsin
IMMUNOLOGY AND ALLERGY CLINICS OF NORTH AMERICA
VOLUME 19 NUh4BER 2 - MAY 1999 383

384 HARRIGAN & RABINOWlTZ
Table 1. DIAGNOSTIC CRITERIA FOR ATOPIC DERMATITIS IN CHILDREN
Major criteria Pruritus Facial and extensor involvement Chronic relapsing course Personal or family history of atopy Minor criteria Xerosis Ichthyosis, palmar hyperlinearity or keratosis pilaris Skin prick test reactivity Elevated total serum IgE Early age of onset Propensity for cutaneous infections Nipple eczema Cheilitis Dennie-Morgan fold Kera toconus Anterior subcapsular cataracts Facial pallor or erythema Pityriasis alba Intolerance to wool Food intolerance Worsening of symptoms with emotional or enviromental changes Worsening of itch with perspiration
Data from Hanifin JM, Rajka G: Diagnostic features of atopic dermatitis. Acta Dermatol 9244-47, 1980.
Figure 1. Erythema and scaling of the face, particularly the cheeks, is a common presenta- tion of atopic dermatitis in children.

ATOPIC DERMATITIS 385
figure 2. Flexural areas, such as the antecubital fossae, are typically involved during childhood.
Diagnosis and Identification of Triggers
The clinical criteria for the diagnosis of atopic dermatitis according to Hanifin and RajkaX7 are outlined in TabIe 1. No single laboratory marker exists for the diagnosis of AD. Atopic individuals typically have an elevated IgE level and eosinophilia. These findings are nonspecific and are not necessary to estab- iisfi the diagnosis of AD. One third to one half of all children with AD have a food allergy that is thought to trigger a late-phase IgE response. Sampson evaluated over 300 children with moderate to severe AD and found 63% to have food hypersensitivity confirmed by double-blind placebo-controlled food challenges.39 A recent study demonstrated that seven foods-milk, egg, peanut, soy, wheat, cod, and cashew-account for 90% of confirmed food allergy, with skin prick testing correlating in 99% of these patients? Early identification and elimination of the allergenic food can produce significant improvement in AD ~ymptoms.3~ Thus, skin-prick testing for foods is warranted in infants and young children with AD whose disease persists for several months or is unresponsive to conventional therapy.
In older children and adults, aeroallergens and contactants, rather than foods, are more common triggers of AD. Contact with irritants such as wool, feathers, fragrances and perfumes, and pet dander can trigger flares of AD and should be avoided as much as possible. The dust mite ~ e ~ u t o ~ ~ g u ~ d e s pferonyssinus is a major trigger for atopic dermatitis. Reducing the mite burden in the home environments of patients with AD has been shown to result in significant improvement in disease symptoms.B5 Because patients with AD typi- cally demonstrate elevated IgE against mite antigen, they frequently exhibit reactivity on skin-prick testing to dust mite; the significance of this is controver-

386 HARRIGAN & RABINOWITZ
sial. Studies to establish a standardized patch test technique for delayed hyper- sensitivity reaction to dust mite may be a more reliable indicator of immunologic sensitivity in AD patients.ll
For those patients who have extensive skin involvement or are dependent on oral antihistamines for symptom relief, radioallergosorbent test (RAST) may be used to identify IgE directed against specific allergens, Patients with elevated total serum IgE levels, however, can have false-positive RAST results because of nonspecific allergen bindk1g.2~
IMMUNOLOGY OF ATOPIC DERMATITIS
The immune dysregulation associated with AD occurs via several mecha- nisms. A relative imbalance between Th-2 and Th-1 lymphocyte activity exists in patients with this disorder. Patients with AD have predominant activation of Th-2 lymphocytes, resulting in relatively high levels of IL-4, IL-5, and total IgE, with underproduction of interferon gamma (IFN-y)F6 IL-4 inhibits IFN-y production and downregulates Th-1 lymphocytes.48 In addition, IL-4 serves as an IgE isotype-specific switch factor and stimulates the expression of vascular adhesion molecule1 (VCAM-l), which promotes monocyte and eosinophil mi- gration to sites of inflammation.26
IL-5 stimulates the differentiation and endothelial adhesion of eosinophils and the release of histamine from’ba~ophils.~~ The local expression of these cytokines appears to directly affect the way in which inflammation manifests in AD. A recent in situ hybridization study demonstrated IL-4 expression primarily in acute inflammatory AD lesions, whereas chronic lesions manifested IL-5 expression and infiltration of eosinophils.16
The ceIlular phenotype in AD is thought to contribute to the pathogenesis of the disease by the expression of specific cell surface markers that appear to play a role in T-cell activation. Lymphoaytic infiltrates found in acute and chronic skin lesions of AD consist primarily of CD3, CD4, and CD45RO memory T cells, which express CD25 and HLA-DR.z7,36 These cells also express cutaneous lymphocyte antigen (CLA), a skin T-cell homing receptor that can be induced by staphylococcal superantigen to enhance cutaneous inflammation and promote colonization with Staphylococcus aureus in AD.28
Increased numbers of Langerhans’ cells are found in the chronic skin lesions of patients with AD. These cells express CDlb, CD36 (not found in the Langer- hans’ cells of normal patients), and HLA-DRZ7 Keratinocytes in AD lesions have increased levels of ICAM-1, CD36, and CDla but specifically lack expression of HLA-DR (found on the keratinocytes of patients with allergic contact derma- ti ti^.)^ Eosinophils are found in increased numbers in chronic AD skin lesions. Major basic protein derived from eosinophils is found in increased amounts in AD lesions% and may contribute to tissue injury.
Patients with AD have fewer and less functional CD8+ cytotoxic T cells than healthy controls.z6 B cells from AD patients have increased expression of the low-affinity IgE receptor, CD23, which i s modulated by IL-4 production. Increased expression of CD23 has been associated with increased disease severity in patients with AD.50 Monocytes from atopic individuals also produce increased amounts of IL-10, cyclic AMP-phosphodiesterase and prostaglandin (PG) ED which inhibit IFN-y production.12, 4o IL-10 also inhibits cell-mediated immunity to bacterial pathogens, which may explain why AD patients are prone to develop secondary bacterial infections.
IgE appears to have a multifactorial role in the Th-2-mediated inflammation
ATOPIC DERMATITIS 387
in AD, which differs from the typical delayed-type hypersensitivity (DTH) reactions produced by Th-1 lymphocytes. IgE produces a mononuclear cell infiltrate in response to sigruficant allergen exposure in a biphasic manner. Immediate reactions, manifested in AD patients as intense pruritus and ery- thema, Occur when mediators are released by mast cells bearing allergen-specific IgE in response to allergen exposure. This is followed by an IgE-dependent late- phase reaction (LPR) characterized by a T-lymphocyte infiltrate that exhibits mRNA for IL-3, IL-4, and IL-5 but not for IFN-y." These cells resemble the Th- 2-like lymphocytes found in AD skin lesions. IgE is also expressed on the surfaces of Langerhans' cells of AD patients where it facilitates allergen capture for processing and presentation to Th-2 lymphocytes in an apparent effort to sustain local T-cell
The inflammation in AD reflects a chronic component that is thought to have several causes. Patients with AD typically undergo repeated or ongoing exposure to allergic triggers, perpetuating both immediate and late-phase reac- tions as well as Th-2 cell proliferation. Th-2-like cells, in turn, produce cytokines that inhibit IFN-y, thus promoting persistent elevation of IgE and eosinophil proliferation. In addition, enhanced survival of inflammatory cells may contrib- ute to chronic inflammation. Monocytes from patients with AD have been shown to be less likely to undergo spontaneous or IL-&induced apoptosis than normal controls.6 The itch-scratch cycle also appears to play a role. Keratinocytes, injured by trauma from scratching, have been shown to release cytokines and mediators that attract cells to sites of Finally, patients with AD may have an impaired response to steroids because recent studies have shown that monocytes from AD patients demonstrate reduced glucocorticoid receptor binding affinity.13
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of atopic dermatitis includes all eczematous disor- ders, including contact dermatitis and seborrheic dermatitis. It may also be difficult to distinguish scabies from atopic dermatitis because severe pruritus and excoriation can occur in both conditions. Hyper-IgE syndrome must be differentiated from other disorders in which IgE levels may be elevated, such as atopic dermatitis and Wiskott-Aldrich syndrome. These latter entities are not associated with cutaneous abscesses that are so prevalent in hyper-IgE syn- drome. Patients with Wiskott-Aldrich syndrome have thrombocytopenia and hemorrhagic skin lesions and do not usually have the atopic diatheses, such as allergic rhinitis and reactive airway disease, often seen in patients with atopic dermatitis.
TREATMENT
Atopic dermatitis is typically managed by implementing a skin care regimen consisting of daily skin hydration, use of moisturizers, avoidance of irritants, use of oral antihistamines, and application of topical corticosteroids which, in combination, decrease pruritus and improve skin integrity. Management should be individualized because choice of treatment depends on the severity of the condition. The following guidelines may be used for managing most patients, but these may need to be modified in some situations.
388 HARRIGAN 81 RABINOWITZ
Bathing
Patients with AD have suboptimal skin barrier function that is associated with significant evaporative losses and inability to retain moisture. Daily bathing is recommended to hydrate the skin, but baths should be limited to 10 or 15 minutes, and hot water should be avoided. Excessive soaking in the tub or frequent baths during the day can lead to increased dryness of the skin. Bath oils may be used as long as they are not substituted for moisturizers. All products used in the bath should be fragrance-free and designed for sensitive Skin.
Cleansers
Atopic patients should use gentle soaps or soap substitutes (that do not contain soap) such as Basis or Cetaphil products to avoid overdrying the skin and disrupting the epidermal barrier even further. Unscented products are recommended because perfumes can trigger flares of atopic dermatitis. Scrub- bing should be avoided. '
Shampoos
Mild shampoos, such as baby shampoo, are recommended. Shampoos that contain zinc, tar, or selenium sulfide may be too harsh and irritating for patients whose eczema affects their scalp. Specially formulated shampoos and condition- ers are available for patients with extremely sensitive scalps.
Moisturizers
Moisturizers are probably the most important ingredient in the skin care regimen of patients with AD. They should be applied after bathing and at least one other time during the day. The most effective moisturizers are those that do not contain water, such as plain petroleum jelly. Lotions contain predominantly water and, thus, are less effective in preventing evaporative losses from the skin. Thick creams such as Eucerin or Nivea are more effective than lotions because they contain more lipid products, but they have more additives and preserva- tives than bland petrolatum. Emollients have been shown to be topical corticoste- roid-sparing agents in the treatment of mild to moderate AD in children.32
Antihistamines
Systemic antihistamines can be used to help control the itch-scratch cycle of atopic dermatitis. Hydroxyzine and diphenhydramine can be used if sedation is a desired effect. Less sedating antihistamines, such as cetirizine, have been studied in the management of AW4 with moderate success. They offer some relief without affecting school performance and other daytime activities. Topical antihistamines are not recommended because of their potential for skin sensitiza- tion. Doxepin 5% cream, a potent combination HJH2 antagonist, has been used successfully in adults with AD. In a short-term double-blind study, topical doxepin was shown to be superior to placebo in controlliig pruritus and improv-

ATOPIC D E ~ ~ S 389
ing overall skin condition. No apparent sensitization occurred.l4 Mild sedation was a frequent side effect when doxepin was applied over a large body surface ma. The safety and efficacy of topical doxepin in children have not yet been established.
Topical Corticosteroids
Topical corticosteroids continue to be the mainstay of treatment of AD. These medications reduce the inflammation and decrease the pruritus of the disorder. Seven classes of topical corticosteroids exist, ranked according to po- tency. Table 2 summarizes the relative potency of some of the more commonly used preparations. The strength of a corticosteroid product is determined by the steroid molecule itself, in addition to its vehicle. Several products are available in multiple forms, as a lotion, gel, solution, cream, or ointment. Ointments are more potent than the comparable cream, owing to the more occlusive nature of an ointment vehicle. Class I and 11 are potent corticosteroids that should not be used for mild or moderate atopic dermatitis. If necessary, they can be used to control severe AD but should not be used on the face, groin, or intertriginous areas. Mid-~trength topical steroids can control most cases of mild to moderate AD and low potency steroids are used for mild eczema and for facial and intertriginous eczema.
Side effects from topical corticosteroids may occur with prolonged use. Local side effects include thinning and atrophy of the skin, telangiectases, striae, and possible steroid-induced rosacea. Systemic side effects, although less frequent, include potential suppression of the hypothalamic-pituitary-adrenal axis and are related to the potency of the steroid, the surface area over which it i s used, and the duration of treatment." Although one study group found no suppression in adrenal glucocorticoid function in patients with mild to moderate AD treated chronically with topical corticosteroids,35 it remains a serious concern. The risk of adrenal suppression from topical steroids is greatest in infants and young children because increased percuta.neous absorption can occur because of their greater body surface area to weight ratio.
Table 2. POTENCY OF TOPICAL CORTICOSTEROIDS
~ t r a ~ t e n ~ Temovate (clobetasol propionate) cream and ointment 0.05% Ultravate (halobetasol propionate) cream and ointment 0.05% Diprolene (betamethasone dipropionate) cream and ointment 0.05%
Halog (halcinonide) cream 0.1% Topicort (desoximetasone) ointment and cream 0.25% Diprosone (betamethasone dipropionate) ointment 0.05% Synalar (fluocinolone acetonide) ointment 0.025% Kenalog (triamcinolone acetonide) ointment 0.1% Elocon (mometasone furoate) cream 0.1% Ik-matop (prednicarbate) cream 0.1% Westcort (hydrocortisone valerate) cream 0.2% DesOwen (desonide) cream and ointment 0.05% Aclovate (aclometasone dipropionate) cream and ointment 0.05% Hydrocortisone cream and ointment 1%, 2.5%
Strong Lidex (fluocinonide) ointment 0.5%
Moderate
Mild
Verv Mild

390 HAREUGAN & RABINOWITZ
Antibiotics
Patients with AD are colonized with S. aureus that frequently causes second- ary infection of primary eczematous lesions. Studies have demonstrated s. aureus at a density of 1 X lo6 colony-forming units (CFU)/cm2 to be aggravating to AD lesions but not indicative of secondary infection. Those with a density of S. aureus greater than 1 X lo7 CFU/cmz likely are secondarily infected.' Thus, patients whose lesions are devoid of purulence, weeping, or cellulitis but are significantly excoriated warrant treatment with antibiotics. Cephalexin, dicloxa- cillin or erythromycin are generally effective for most patients. Long-term ther- apy should be avoided in order to help prevent microbial resistance to the antibiotic. Mupirocin is a broad-spectrum antibiotic used topically for the treat- ment of cutaneous infections. It is effective in reducing s. aureus colony counts and is associated with a reduction in the severity of lesions in patients with AD?' Although 10% povidone-iodine solution has been shown to reduce S. aureus colony counts on the skin lesions of patients with AD, it is irritating and has been associated with transient congenital h~othyroidism when used in pregnant and lactating patients.' Thus, its routine use in this condition is not recommended.
Systemic Cortieosteroids
Patients with severe, chronic AD may experience marked improvement with a short course of oral corticosteroids. The dose should be tapered, however, and used in conjunction with aggressive hydration, moisturizing, and topical corticosteroid application to minimize rebound flares of eczema when the oral corticosteroid is withdrawn.
P hototherapy
Ultraviolet (W) light therapy has been shown to be moderately effective in the treatment of AD, although its mechanism of action is not well understood. Short-wave W B light therapy is readily available in many dermatologists' offices. In one pediatric study, UVB light reduced the pruritus of AD and reduced the need for topical corticosteroid but did not clear lesions completely? Photochemotherapy with methoxypsoralen and W A light was used successfully in a study of adolescent patients with severe AD3; however, this modality has a fairly high incidence of side effects, including nausea, itching, hyperpigmenta- tion, premature aging and development of skin cancer.
Cyclosporine
As the immune system's role in the development of atopic dermatitis becomes better understood, immune modulators are being evaluated for their potential efficacy in the treatment of this disease. Cyclosporine inhibits T-cell immune responses and was first used as an immune suppressant in organ transplantation. The efficacy of cyclosporine in the treatment of several immune- modulated skin disorders, including psoriasis and AD, has been demonstrated. One study showed that cyclosporine decreased the number of activated T cells and IL-2 receptors and suppressed IL-5 expression by mononuclear cells in a

ATOPIC DERMATITIS 391
pediatric patient with ADT1 In another study, administration of cyclosporine to two children with AD produced an increase in IFN-y production and a reduction in IL-4 production compared with nonatopic patients.l0
Results of multiple controlled trials in adult patients with AD have demon- strated that 5 mg/kg per day of oral cyclosporine given for 2 to 8 weeks was safe and effective but was associated with a high relapse rate. Disease severity, however, declined after discontinuation of cyclosporine. Several recent pediatric studies showed that a 6-week course of 5 mg/kg per day of cyclosporine produced significant improvement in the majority of patients?, 51 Most side effects were minor (including headache and abdominal pain) but occurred with fairly high frequency. In addition, most patients had a relapse of their rash within several weeks of discontinuing treatment. An international committee on the use of cyclosporine in AD recently developed a set of guidelines for its use. Cyclosporine should not be used in patients with immunodeficiency, renal insufficiency, or compliance problems. It should not be used in conjunction with erythromycin or antifungal agents. Patients should be watched closely for the development of S. aureus or herpes simplex virus infections? Further studies are needed to establish ideal dosing and duration of therapy for the long-term use of cyclosporine in children.
Tacrolimus
Tacrolimus, or FK-506, is an immune suppressant used, like cyclosporine, to inhibit organ rejection after ~ansplantation. Recent studies have shown that 0.3% tacrolimus ointment is effective in controlling pruritus and improving skin condition in adult and pediatric AD patients, with low systemic absorption and only transient side effects.2 Tacrolimus is as effective as a class I topical cortico- steroid in reducing cutaneous inflammation. It has not been shown to cause the atrophic skin changes seen with prolonged topical corticosteroid use. Recent studies have demonstrated systemic absorption of topically applied tacrolimus; however, topical tacrolimus is significantly less bioavailable than intravenous or oral tacrolimus. Furthermore, the amoFt of tacrolimus absorbed decreases with its continued use? The most common side effect is burning at the site of application.38
Thy mopentin
Thymopentin (TP-5) is a synthetic peptide derived from the thymic hormone thymopoietin. It has been shown to increase production of IL-2 and IFN-y and suppress IL-4 producti~n.~~ Several double-blind, controlled studies indicate that TP-5 administered subcu~neously three times per week for 12 weeks can be effective in reducing severity of symptoms in AD.30 TP-5 was effective in an open trial of 16 pediatric patients with AD using a similar dosing regimen; however, relapse occurred frequently after discontinuationTO The only signhcant side effect noted was pain at the injection site. TP-5 is thought to be a safe adjunctive therapy for severe AD but is less effective than cycl0sporine.3~
Chinese Herbal Therapy
A mixture of ten Chinese herbs has been found to provide symptomatic relief for patients with AD as evidenced by several short-term double-blind,

392 HARRIGAN & RABXNOWITZ
placebwontrolled studies in adults and children." The herbs are assembled in a sachet and boiled in water for 90 minutes. Patients ingest approximately 100 mL of this tea daily until symptoms improve. The dosing interval is then gradually increased. The herbs are known to have NSAID-like properties as well as antihistamine and immunomodulatory effects. It has been postulated that Chinese herbal therapy exerts its effect by reducing expression of the low- affinity IgE receptor, CD23, on Langerhans' cells in the skin.= In one pediatric study, CHT was moderately effective in patients followed for 1 year.4I Elevated liver enzyme levels were noted in 2 of the 37 children enrolled, but these values normalized within 8 weeks of discontinuation of treatment. This herbal formula has an unpleasant odor and taste and is unacceptable to some children.
lmmunotherapy
The major role aeroallergens play in AD exacerbations suggests that desensi- tization to allergens such as D. ptemnyssinus may offer a therapeutic benefit to patients. Such attempts have been moderately successful in studies of adult patients7; however, a double-blind, placebo-controlled study of children with AD found hyposensitization with injections of mite extract to be no better than placebo in improving symptoms.15 In this report, a significant placebo effect was observed, which may have obscured actual results. Further studies are necessary to establish whether or not immunotherapy is effective in the treatment of AD in children.
Cromolyn
Cromolyn has been used with variable success in the treatment of AD. Several investigators have found topical cromolyn .ointment (disodium cromo- glycate) to be ineffective in the management of AD; however, daily topical application of 1% cromolyn nebulizer solution to AD lesions in young children has been shown to safely improve eczema, decrease pruritus, and improve sleep over a 3-week study period.= Continued application of the solution is required to prevent recurrence, and older children respond more slowly to this treatment than younger children.
Evening Primrose Oil
Evidence suggests that children with AD have abnormally low serum levels of long chain polyunsaturated fatty acids (LCPs) derived from linoleic acid. In view of this, evening primrose oil (gammaliinolenic acid or Epogam) has been touted as an effective treatment for AD. Results of a recent double-blind study, however, indicate that Epogam is not superior to placebo in improving AD symptoms in pediatric patients.18 There was significant improvement in symp- toms in both test patients as well as controls, possibly because of improved patient compliance with prestudy medication regimens that were continued throughout the study. It is also possible that global improvement in AD symp- toms was attributable to an increased understanding of the disease and close follow-up and monitoring.

ATOPIC DERMATITIS 393
Hypnotherapy
Hypnosis has been used successfully in the treatment of behavior disorders such as phobias, smoking, obesity, and anxiety. Children were previously thought to be incapable of being hypnotizable, largely because adult hypnosis techniques had been used, unsuccessfully, on them. Using age-appropriate tech- niques, such as storytelling, hypnosis has been shown to be successful in some children. In one recent study, children with severe AD, refractory to conventional therapy, experienced significant long-term improvement in their pruritus, sleep patterns, and general mood after listening to a soothing audio tape nightly for 4 to 8 weeks.@ While larger, controlled studies are necessary to determine whether hypnotherapy is truly effective in the management of AD, it appears to offer an economical treatment alternative with no side effects. In addition, it can help counteract negative psychologic effects that can be associated with this chronic and often frustrating skin disorder.
Patient Education
Education of parents and patients is the key to successful management of AD. Without a firm understanding of the rationale of therapy, parents and patients are less likely to comply with the physician’s instructions. Additionally, they may become less frustrated if they know this is a chronic condition, associated with recurrent flares and remissions. Affected individuals tend to have dry, sensitive skin throughout life, but this disorder usually improves with age.
ASSOCIATED CONDITIONS
Keratosis Pilaris
A skin condition frequently associated with atopic dermatitis is keratosis pilaris. On examination, there are numerous follicular keratotic papules that are typically distributed on the lateral cheeks and extensor aspects of the upper arms and thighs. When present on the cheeks, these papules are often misdiagnosed as acne or molluscum contagiosum. The lesions may or may not be associated with inflammation around each hair follicle. Facial lesions often disappear with age. Lesions on the upper arms frequently persist into adulthood. This condition represents a skin type, rather than a disease that needs to be cured. Treatments consist of topical medications that contain either lactic acid, retinoic acid, or urea and use of moisturizers. If inflammation is present, topical corticosteroids may be beneficial also. Patients and parents should understand that the follicular papules will usually recur when topical treatment is discontinued. The lesions are usually asymptomatic and are often treated for cosmetic reasons. If the patient does not find the problem bothersome, no treatment is necessary.
lchthyosis Vulgaris
Ichthyosis vulgaris is the most common form of ichthyosis and has an autosomal dominant inheritance pattern. Approximately one half of affected patients have concomitant AD. The cause and pathogenesis of this disorder,

394 HAlUUGAN & RABINOWITZ
characterized by fine white scales that have a “pasted on” appearance, are unknown. Sites of predilection include the extensor surfaces of the limbs and the trunk, whereas flexural areas such as the antecubital and popliteal fossae are spared. The back may be involved, as may the forehead and cheeks, but scaling in these areas diminishes with age.
Ichthyosis vulgaris is managed with emollients, such as petroleum jelly or less greasy creams. Salicylic acid, urea, lactic acid, and other alpha-hydroxy acids can also be used to improve the appearance of the skin. These medications can loosen scale and improve binding of water to the epidermis. Skin irritation, stinging, or burning are possible side effects of these preparations and may limit their use. In addition, if patients have coexisting inflammatory AD, they will probably not be able to tolerate these topical agents. As with keratosis pilaris, ichthyosis vulgaris may not need to be treated.
SUMMARY
AD is a chronic and complex immunologic disorder. Although a significant percentage of the population is affected, most patients with AD improve over time. For children with moderate to severe AD, consultation with a dermatolo- gist or allergist is advisable to help identify specific triggers and assure judicious use of medications. Guidelines established by the Joint Task Force on Practice Parameters/Work Group on Atopic Dermatitis (September 1997 issue of Annals of Asthma, Allergy and Immunology) help to standardize the approach to the management of patients with AD. As the immunological aspects of AD are better understood, treatments directed toward immune regulation, including the modulation of Th-2 cells and their associated cytokines, may expand available therapeutic options. Keratosis pilaris and ichthyosis vulgaris are often associated with AD. Recognition of these conditions is necessary to better educate patients and their parents and provide treatment when indicated.
References
1. Akiyama H, Tada J, Toi Y, et al: Changes in S t a p h y l ~ u c ~ s aweus density and lesion severity after topical application of povidone-iodine in cases of atopic dermatitis. J Dermatol Sci 1623-30,1997
2. Alaiti S, Kang S, Fiedler V, et a1 Tacrolimus (FK506) ointment for atopic dermatitis: A phase I study in adults and children. J Am Acad Dennatol38:69-76, 1998
3. Atherton DJ, Carabott F, Glover MT, et al: The role of psoralen phot~hemotherapy (PUVA) in the treatment of severe atopic eczema in adolescents. Br J Dermatol118791- 795, 1988
4. Barker JNSN, MacDonald DM Epidermal class I1 human lymphocyte antigen expres- sion in atopic dermatitis: A comparison with experimental allergic contact dermatitis. J Am Acad Dennatol 16:1175-1179, 1987
5. Berth-Jones J, Finlay A, Zaki I, et a1 Cyclosporine in severe childhood atopic dermatitis: A multicenter study. J Am Acad Dermatol34:1016-1021,1996
6. Bratton DL, Hamid Q, Boguniewicz M, et al: Granulocyte macrophage-colony stimulat- ing factor inhibition of monocyte apoptosis contributes to the chronic monocyte activa- tion in atopic dermatitis. J Clin Invest 95:211-218, 1995
7. Brehler R, Hildebrand A, Luger T: Recent developments in the treatment of atopic eczema. J Am Acad Dermatol36983-994, 1997
8. Burks AW, James JM, Hiegel A, et ak Atopic dermatitis and food hypersensitivity reactions. J Pediatr 132132-36,1998
9. Camp RDR, Reitamo S, Friedmann PS, et a1 Cyclosporin A in severe, therapy-resistant

ATOPIC DERMATITIS 395
atopic dermatitis: Report of an international workshop, April 1993. Br J Dermatol
10. Campbell DE, Kemp AS Cyclosporine restores cytokine imbalance in childhood atopic dermatitis. J Allergy Clin Immunol 99:857-859,1997
11. Castelain M, Bimbaum J, Castelain PY, et a1 Patch test reactions to mite antigens: A GERDA multicentre study. Contact Dermatitis 29246-250, 1993
12. Chan SC, Kim JW, Henderson WR, et al: Altered prostaglandin E2 regulation of cytokine production in atopic dermatitis. J Immunol 151:3345-352,1993
13. Clayton MH, Leung DYM, Surs W, et al: Altered glucocorticoid receptor binding in atopic dermatitis. J Allergy Clin Immunol96421423,1995
14. Drake LA, Fallon JD, Sober A Relief of pruritus in patients with atopic dermatitis after treatment with topical doxepin cream. J Am Acad Dermatol 3k613-616, 1994
15. Glover MT, Atherton DJ: A double-blind controlled trial of hyposensitization to Dertrzu- tup~~goides ~ ~ e r o ~ y s s ~ n ~ s in children with atopic eczema. C l i Exp Allergy 22440-446, 1992
16. Hamid Q, Boguniewicz M, Leung DYM: Differential in situ cytokine gene expression in acute versus chronic atopic dermatitis. J Clin Invest 94:870-876,1994
17. Hanifin JM, Rajka G: Diagnostic features of atopic dermatitis. Acta Dermatol 92344- 47, 1980
18. Hederos C, Berg A Epogam evening primrose oil treatment in atopic dermatitis and asthma. Arch Dis Child 753494497, 1996
19. Hiratani M, Muto K, Oshida Y, et a1 Lymphocyte responsiveness to Dermafuphagoides farinue extract in mite-sensitive patients: Effect of immunotherapy on cellular prolifera- tive response and specific immunoglobulin E antibody (RAST score). J Allergy Clin Immunol68205-211, 1981
20. Hsieh KH, Shaio MF, Liao T: Thymopentin treatment in severe atopic dermatitis- clinical and i~uno log ica l evaluations. Arch Dis Child 671095-1102,1992
21. Ishii E, Yamamoto S, Sakai R, et al: Production of interleukin-5 and the suppressive effect of cyclosporin A in childhood severe atopic dermatitis. J Pediatr 128352-155, 1996
22. Kay AM, Ying S, Vamey V, et al: Messenger RNA expression of cytokine gene cluster, interleukin 3 (IL-3)' IL-5, and granulocyte/macrophage colong-stimulating factor, in allergen-induced late-phase cutaneous reactions in atopic subjects. J Exp Med 173775- 778, 1991
23. Kimata H, Igarashi M Topical cromolyn (disodium cromoglycate) solution in the treatment of young children with atopic dermatitis. Clin Exp Allergy 20279-281,1990
24. LaRosa M, Ranno C, Musarra I, et al: Double-blind study of cetirizine in atopic eczema in children. Ann Allergy 73.117-122,1994
25. Leiferman Kh4, Ackerman SJ, Sampson HA, et a1 Dermal deposition of eosinophil granule major basic protein in atopic dermatitis: Comparison with onchocerciasis. N Eng J Med 313282-285,1985
26. Leung DYM: Atopic dermatitis: The skin as a window into the pathogenesis of chronic allergic diseases. J Allergy Clin Immunol96302-318,1995
27. Leung DYM, Bhan AK, Schneeberger EE, et a1 Characterization of the mononuclear cell infiltrate in atopic dermatitis using monoclonal antibodies. J Allergy Clin Immunol
28. Leung DYM, Gately M, Trumble A, et a1 Bacterial superantigens induce T cell expres- sion of the skin-selective homing receptor, the cutaneous lymphocyte-associated anti- gen (CLA). J Exp Med 181:747-53,1995
29. Leung DY, Hanih JM, Charlesworth EN, et al: Disease management of atopic derma- titis: A practice parameter. Ann Allergy Asthma Immunol 79:197-211,1997
30. L e q DY, Hirsch RL, Schneider I, et al: Thymopentin therapy reduces the clinical severity of atopic dermatitis. J Allergy Clin Immunol85927-933,1990
31. Lever R, Hadley K, Downey D, et al: Staphylococcal colonization in atopic dermatitis and the effect of topical muciprocin therapy. Br J Dermatol 119:189-98,1988
32. Lucky AW, Leach AD, Laskarzewski F', et al: Use of an emollient as a steroid-sparing agent in the treatment of mild to moderate atopic dermatitis in children. Pediatr Dermatol 14321-324,1997
129217-220,1993
71~4746,1983

396 HARRIGAN & RABINOWITZ
33. Nish WA, Charlesworth EN, Davis TL, et al: The effect of immunotherapy on the cutaneous late phase response to antigen. J Allergy Clin Immunol 93484493,1994
34. Pastore S, Corinti S, La Placa M, et al: Interferon-y promotes exaggerated cytokine production in keratinocytes cultured from patients with atopic dermatitis. J Allergy Clin Immunol101:538-544,1998
35. Patel L, Clayton PE, Addison GM, et a1 Adrenal function following topical steroid treatment in children with atopic dermatitis. Br J Dermatol 132950-955, 1995
36. Picker LJ, Butcher EC: Physiological and molecular mechanisms of lymphocyte hom- ing. Annu Rev Immunol 10:561-591,2992
37. Rothe MJ, Grant-Kels JM: Atopic dermatitis: An update. J Am Acad Dermatol 351- 13, 1996
38. Ruzicka T, Bieber T, Schopf E, et a1 A short-term trial of tacrolimus ointment for atopic dermatitis. N Engl J Med 337816-821,2997
39. Sampson HA: The immunopathogenic role of food hypersensitivity in atopic derma- titis. Acta Derm Venereol17634-37,1992
40. Sawai T, Ikai K, Uehara M: Elevated cyclic adenosine monophosphate phosphodiester- ase activity in peripheral blood mononuclear leucqtes from children with atopic dermatitis. Br J Dermatoll3222-24,1995
41. Sheehan MP, Atherton DJ: A controlled trial of traditional Chinese medicinal plants in widespread non-exudative atopic eczema. Br J Dermatol126179-184,1992
42. Sheehan MP, Atherton DJ: One-year follow up of children treated with Chinese medicinal herbs for atopic eczema. Br J Dermatol 130488493, 130
43. Stewart AC, Thomas SE Hypnotherapy as a treatment for atopic dermatitis in adults and children. Br J Dermatol 132778-783, 1995
44. Takigma M, Tamamor T, Horiguchi D, et a1 FceRII/CD23-pdsitive lymphocytes in atopic dermatitis. Clin Exp Immunol 1991:275-282,1991
45. Tan BB, Weald D, Strickland I, et a1 Double-blind controlled trial of effect of housedust- mite allergen avoidance on atopic dermatitis. Lancet 34715-28, 1996
46. Tay YK, More& JG, Weston WL: Experience with W B phototherapy in children. Pediatr Dermatol 13406409,1996
47. Turpeinen M Influence of age and severity of dermatitis on the percutaneous absorp- tion of hydrocortisone in children. Br J Dermatol 118517-522,1988
48. Vercelli J, Jabara HH, Lauener RP, et al: IL-4 inhibits the synthesis of IFN-y and induces the synthesis of IgE in human mixed lymphocyte cultures. J Immunol144:570-573,1990
49. Weller PF Role of eosinophils in allergy. Curr Opin Immunol4782-787, 1992 50. Xu XJ, Banejee P, Rustin MHA, et a1 Modulation by Chinese herbal therapy of
immune mechanisms in the skin of patients with atopic eczema. Br J Dermatol13654- 59,1997
51. Zaki I, Emerson R, Allen BR Treatment of severe atopic dermatitis in childhood with cyclosporin. Br J Dermatol 13521-24, 1996
Address reprint requests to Linda G. Rabinowitz, MD
Department of Pediatrics (Dermatology) Medical College of Wisconsin 9000 West Wisconsin Avenue
Milwaukee, WI 53201