attainment of globally acceptable cure rate through … · · 2015-03-05acceptable cure rate...
TRANSCRIPT

ATTAINMENT OF GLOBALLY ATTAINMENT OF GLOBALLY ACCEPTABLE CURE RATE ACCEPTABLE CURE RATE THROUGH QUALITY DOTS THROUGH QUALITY DOTS
SERVICES IN SELECTED AREAS OF SERVICES IN SELECTED AREAS OF THE NATIONAL CAPITAL REGIONTHE NATIONAL CAPITAL REGION
(2006(2006--2009)2009)
Amelia C. Medina, MD, MPHHead, Infectious Disease Prevention and
Control ClusterCenter for Health Development-Metro Manila

The Philippines ......
Total Population : 84,241,341 Total Population : 84,241,341 (2005)(2005)
Land area : 300,000 Land area : 300,000 sq. kms.sq. kms.
RegionsRegions : 17: 17ProvincesProvinces : 79: 79CitiesCities : 115: 115Municipalities : 1,495Municipalities : 1,495

National Capital Region (Metro Manila)
Population : 10,485,356(2005)
Land Area : 636 sq. kms.Urban Poor Pop. : 39.9%Pop. Density : 16,486/sq.km.Annual Growth Rate : 1.06%Literacy Rate : 94%Cities : 14Municipalities : 3Barangays : 1,697

TB and NTP…..The Philippines is 9th among the 22 HBCs3rd in the Western Pacific Region 6th leading cause of morbidity and 5th leading cause of mortalityRegion wide implementation of DOTS in 2000DOTS reporting centers
433 health centers4 CHD-MM retained hospitals18 PPMD Units
29 QA Centers14 TB Diagnostic Committees128 Microscopy Centers
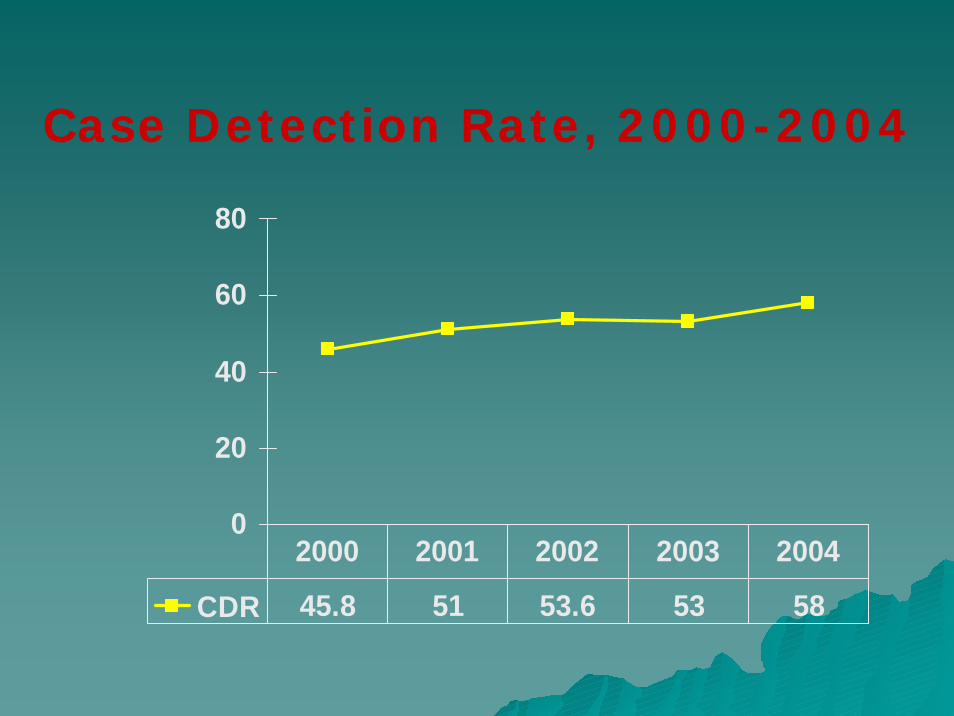
Case Detection Rate, 2000-2004
0
20
40
60
80
CDR 45.8 51 53.6 53 58
2000 2001 2002 2003 2004

Treatment Outcome 2003,New Smear (+) Cases
1.6%7.6%6.7%
1.2%
75%
7.6%
Cured Completed FailureTrans-out Defaulter Died

Cure Rate by City / Municipality, 2003
0.0
20.0
40.0
60.0
80.0
100.0
Cure Rate 67.7 84.4 62.4 66.5 87.6 94.7 87.4 75.1 78.3 68.8 56.6 63.9 82.4 75.0 77.8 74.6 76.8 75.0
Malabon
Navotas
Valenzuel
Marikina
Pasig
Pateros
Taguig
Makati
Mandaluy
San Juan
Las Piñas
Muntinlup
Parañaque
Manila
Quezon
Caloocan
Pasay
CHD-MM

Cure Rate vs. Completion Rate, 2000-2003
0%
20%
40%60%
80%
100%
Completion Rate 11.6% 3.3% 9% 7.6%Cure Rate 69% 78% 73.3% 75%
2000 2001 2002 2003

Stakeholders AnalysisBeneficiaries Implementing
AgenciesDecision Makers
Partner Agencies
Funding Agencies
Potential Opponents
TB casesHealth WorkersCommunityCity Health OfficesHealth CentersMicroscopy CentersLocal Government Units
City Health OfficesHealth CentersPPMD UnitsCHD-MM Retained HospitalsSelected DOH HospitalsNGOsMass MediaFaith-based OrganizationsLocal Coalitions
Local Govern-mentUnitsCenter for Health Dev’t-Metro ManilaInfectious Disease Office-DOH
JICALEAD for Health Project-MSHWHOTDFI-GFATMPhilCATPhilTIPS-USAIDCATiMM
Local Government UnitsCHD-MMIDO-DOHGFATMLEAD for Health Project-MSHJICA
Private Practition-ersPrivate ClinicsPrivate HospitalsGovern-ment Hospitals

PROBLEM ANALYSISPoor socioeconomic condition
Increase morbidity and mortality from TB
Low Cure Rate
Health workers do notImplement NTP
Policies and guidelines
Poor adherenceto treatment among
TB cases
Monitoring patient responseTo treatment is not
Strictly followed
Weak monitoring andEvaluation of the
program
Poor case holdingmanagement
Lack of commitment andLow morale of Health workers
Health workers lackKnowledge on NTP
Defaulter mechanismNot implemented
Referral system notIn place
Low salaries andbenefits
Untrained newly hiredpersonnel
Insufficient budget fortraining
Lack of vehicle and Transportation allowance
For defaulter tracing
Inadequate health educationProvided to patients
Lack of IEC materials andcollaterals
Insufficient number of Staff to conductHealth education
Limited budget for healthPromotion activities
Undermanned healthcenters
Non-filling up of vacancies Exodus of health workers
Low salaries and compensation

Low Cure Rate
Health workers Do not implementThe NTP policiesAnd guidelines
Poor adherenceTo treatment
Among TB cases
Monitoring patientResponse to
Treatment is notStrictly followed
Weak Monitoring
And Evaluation Of the
program
Poor qualityOf laboratory
services
TB patient unableTo collectSputum
specimen
Lack of trainedStaff to conduct
Monitoring &Evaluation
Lack of budgetFor program
reviews
No vehicle/transportation
allowanceFor monitoring
purposes
No standardizedMonitoring tool
At all levels
Multiprogram/MultifunctionSupervisors &coordinators
Lack of Knowledge on
NTP monitoring
No specific training On monitoring Supervision &
Evaluation
Lack of healthbudget
Inadequate Number of Microscopy
Centers
Insufficient Number of Med. Techs
Lack of super-Vision to the
patient
PROBLEM ANALYSIS

OBJECTIVE ANALYSISOBJECTIVE ANALYSIS Improved socioeconomic condition
Decrease morbidity and mortality from TB
High Cure Rate
Strict implementation ofNTP Policies and
Guidelines by health workers
Good adherenceto treatment among
TB cases
Monitoring patient responseTo treatment is Strictly Followed as scheduled
Effective and Regular monitoring andEvaluation conducted
Excellent case holdingmanagement
Committed and highlymotivated
Health workers
Health workers are Knowledgeable on NTP
Defaulter tracingmechanism
Is implemented
FunctionalReferral system
High salaries andbenefits
Trained newly hiredpersonnel
Sufficient budget fortraining
Vehicle and Transportation allowance
For defaulter tracingprovided
Adequate health educationIs provided to patients
Adequate IEC materials and
collaterals
Sufficient number oftrained
Staff to conductHealth education
Provision of budget forhealth
Promotion activitiesWell staffed health
centers
Vacancies filled up Health workers stick withTheir jobs
High salaries and compensationCAPABILITY BUILDING
APPROACH
Health Education Approach

High Cure Rate
Strict ImplementationOf NTP policiesAnd guidelines
Good adherenceTo treatment
Among TB cases
MonitoringPatient comp-Liance to treat
Ment is strictly followed
Effective andRegular
Monitoring andEvaluation conducted
Quality Laboratory
services
TB patientsCollect sputumFor follow-upexamination
Adequate no.Of trained
Staff toConduct
monitoring
Regular Conduct of
Programreview
Vehicle/Transportation
Allowanceprovided
Existence ofA standard
Monitoring toolAt all levels
NTP Monitoring is A priority of
Coordinators & supervisors
Adequate Knowledge on
NTPmonitoring
Training on Monitoring,Supervision& Evaluationconducted
Allocation ofSpecific budget For monitoring
purposes
Adequate Number of Microscopy
centers
SufficientNumber ofMed. Techs
ImprovedPatient
supervision
OBJECTIVE ANALYSIS
Quality Assurance Approach
Monitoring andEvaluation Approach
QUALITY SERVICE
APPROACH
QUALITY SERVICE
APPROACH

PROJECT NAME : ATTAINMENT OF GLOBALLY ACCEPTABLE CURE RATE THROUGH QUALITY DOTS SERVICES IN SELECTED AREAS OF THE NATIONAL CAPITAL REGION
TARGET GROUPS : Health Workers
TARGET AREAS : Cities of Valenzuela, Marikina, Muntinlupa and Las Pinas
DURATION :Three (3) Years Three (3) Years
SCHEDULE :July, 2006 July, 2006 –– July, 2009July, 2009

NarrativeSummary
Objectively Verifiable Indicators
Means of Verification
ImportantAssumptions
Overall Goal:
Decrease morbidityand mortality from TB
TB morbidityand mortality is reduced by 10% at the end of the project.
Health Indices
Field Health Services Information System
The change in administration will not affect project imple-mentation
Comprehensive Unified Policy (CUP) on TB is strictly followed by other GOs, NGOs, POs, etc.

Narrative Summary
Objectively Verifiable Indicators
Means of Verification
ImportantAssumptions
Project Purpose:
To achieved a cure rate of 85% or more.
Increased cure rate by 30% in 2009
Cohort Analysis
Private Initiated PPMD Units continuously network and coordinate with their public counterparts

Outputs:
1. Health workers complied and strictly implemented the NTP policies and guidelines on case holding management.
1.1 By the end of the project, all health workers are trained and accurately and effectively implement the NTP policies and guidelines on case holding mechanism.
1.2 Policies and procedures for detecting defaulters and getting them back to treatment are implemented and monitored for effectiveness in 100% of DOTS centers by 2009
1.3 By 2009, 80% of the DOTS Centers developed and implemented policies and procedures ensuring an effective referral system
1.4 Defaulter and transfer out rates is less than 3% by 2009
Baseline and Endline Survey Results
NTP Records and Reports
Written policy/protocols on defaulter tracing
Cohort Analysis
Referral/Transfer Forms
Return Slip from Receiving Units
NTP Register
Cohort Analysis
Trained health workers will remain working with the health offices.
Budget will be provided by both the Department of Health and local government units as planned.

Outputs:
2. 2. Laboratory networks with Quality Assurance System established.
3.1 3.1 All sputum follow-up examinations are performed on scheduled dates during the course of treatment.
3.2 External Quality Assessment conducted every quarter by qualified controllers by the end of 2007.
3.3 All microscopy and quality assurance centers have functional microscopes and adequate laboratory supplies.
NTP Register
Feedback Sheets
Follow up Sheets
Annual Slide Reading Quality Check and Smear Preparation Quality Check
Inventory Reports
Stock Cards
Patients do not have the difficulty of collecting sputum specimen towards the end of treatment
Controllers will not be assigned to other sections of the public health laboratory
Trained medical technologists stick on with their jobs

Outputs:
3. 3. Effective and comprehensive monitoring and evaluation is regularly conducted.
3.13.1Quarterly Quarterly monitoring and supervision conducted.
3.2 DOTS centers with improved recording and reporting system increased by 95% at the end of the project.
3.3 Standard monitoring tool developed and used at all levels.
Interview of health workers
Written reports and recommendations made during supervisory visits.
NTP records and reports
Filled-up monitoring tools
Other funding agencies like Global Fund, JICA and MSH will not require specific monitoring tool for their projects.

Outputs:
4. DOTS Centers are certified and accredited
90% of DOTS centers are certified and accredited by 2009.
List ofCertified and AccreditedDOTS Centers from NCC-PPMD
Certification Standards are sustained by the certified and accredited facilities.

ACTIVITIES:
1.1 Training Needs Assessment1.2 Capability Building1.3 Development and maintenance
of a database on human resource development
1.4 Workshop on policy formulation1.5 Formulate and implement a
DOTS Centers networking and referral system.

ACTIVITIES….2.1 Setting-up of quality assurance
centers2.2 Training of Controllers on External
Quality Assessment2.3 Training of untrained Medical
Technologists on Basic NTP Microscopy2.4 Training of laboratory technicians on
sputum smearing and staining procedures
2.5 Inventory and provision of microscopes and laboratory supplies
2.6 Provision of recording and reporting forms.

ACTIVITIES….3.1 Development of a monitoring tool3.2 Development of a Monitoring and
Evaluation training syllabus 3.3 Training of coordinators and supervisors
on NTP monitoring and evaluation3.4 Supervised field practicum on M&E3.5 Quarterly monitoring and supervision3.6 Quarterly program implementation review3.7 Year-end evaluation and consultative
planning workshops

ACTIVITIES….4. DOTS Centers certification and
accreditation4.1 Organize and train TA teams for
DOTS certification4.2 Actual provision of technical
assistance on DOTS Certification and Accreditation4.3 Conduct assessment and
certification of DOTS Centers4.4 Coordinate with PhilHealth for
accreditation4.5 Quality check of certified and
accredited DOTS Center for sustainability

ACTIVITIES….
5. Support activities5.1 Operational research on
patient’s delay5.2 Pilot study of a surveillance
system for NTP

INPUTS:Manpower:NTP City Medical Coordinator Statistician NTP City Nurse Coordinator PhysiciansController NursesHEPO MidwivesSupervisors – at least 3/city Medical TechnologistsSentrong Sigla Coordinator Laboratory TechniciansAssessors and Certifiers BHWsTA Team for DOTS Certification and Accreditation
VehiclesTransportation Allowances Equipment and Laboratory SuppliesGlass slides & glass slide boxes AFB Staining KitsSputum cups Transport BoxesImmersion oil Disinfectants Reporting and Recording Forms AlcoholMicroscopes
FacilitiesDOTS CentersQA Centers
Project Cost : Php 8,000,000

PRECONDITIONS:
1. The city government and the city health offices will have a full support to the project
2. Clear budget allocation from the national and local government

THANK YOU!THANK YOU!
THANK YOU!