attrition of u.s. military enlistees with waivers for …...attrition of enlistees with hearing...
TRANSCRIPT

MILITARY MEDICINE. 172. 1:63. 2007
Attrition of U.S. Military Enlistees with Waivers for HearingDeficiency, 1995-2004
Guarantor: LTC David W. Niebiihr, MC USAContributors: LTC David W. Niebuhr, MC USA*; Yuanzhang Li, PhD*; TimothyCOL Margot R. Krauss. MC USA (Ret.)t; COL David Chandler. MC USAt; Thomas Heifer, Phbi
E. Powers, MS*
Background: Hearing deficiency is the condition for whichaccession medical waivers are most commonly granted. Theretention of individuals entering service with a waiver forhearing deficiency has not been previously studied. Meth-ods: Military retention among new enlistees with a medicalwaiver for hearing deficiency was compared with that amonga matched comparison group of fully qualified enlistees.Comparisons according to branch of service over the first 3years of service were perfonned with the Kaplan-Meier prod-uct-limit method and proportional-hazards model. Results:Army subjects had significantly lower retention rates thandid their fully qualified counterparts. In the adjusted model.Army and Navy enlistees with a waiver for hearing deficiencyhad a significantly lower likelihood of retention than didtheir matched counterparts. Discussion: The increased like-lihood of medical attrition in enlistees with a waiver forhearing loss provides no evidence to make the hearing ac-cession standard more lenient and validates a selectivehearing loss waiver policy.
Introduction
The U.S. military depends on a constant input of healthy andphysically fit individuals. Unfortunately, the prevalence of
noise-induced hearing threshold shifts is estimated to be 15.5%(95% confidence interval, 13.3-17.6%) for 12- to 19-year-oldindividuals in the United States, based on data from the ThirdNational Health and Nutrition Examination Survey.' Militaryapplicants who at least superficially meet entrance criteria un-dergo an extensive screening procedure that includes adminis-trative (background check and vocational aptitude testing),physical (height, weight, and body fat as needed), and medicalcomponents. The medical accession standards, including thosefor hearing, are contained in Department of Defense Instruction6130.4.^ Although some applicants are disqualified during themilitary entrance processing stations medicai examination,each service retains the authority to grant accession waivers fordisqualifying medical conditions, on an individual basis, Oncedisqualified individuals are granted waivers, they are qualifiedas fit for enlisted service. Over the past 10 years, hearing defi-
•Walter Reed Army Institute of Research, Division of Preventive Medicine, SilverSpring, MD 20910.
tKensjngtoii, MD 20895.ttJeparinienl of Defense Executive Agencies. Office ofthe Surgeon General. Falls
Chiin-h.VA 22041.§U.S, Army Center for Heaith Promotion and PrevenUve Medicine. Hearing Con-
servation Program, j^wrdeen Proving Ground, MD 21010-5403,The views expressed are those of the authors and should not be construed to
represent lhe positions of the Department of the Army or the Department of Defense,This manuscript was received for review In August 2005. The revised manuscripl
was accepted for pubilcallnn In July 2006.
ciency was the most common condition for which waivers weregranted, representing slightly more than 10% of all accessionmedical waivers.^
The Department of Defense Hearing Conservation Programrequires a baseline audiogram for enlistees entering service,"*The purpose of this reference audiogram is to serve as a bench-mark for comparison with periodic audiograms obtained duringthe period of service. This active surveillance process is intendedto reveal sentinel events, to allow intervention to prevent ser-vice-connected, noise-induced hearing loss.^ Service memberscan suffer noise-induced hearing loss to such an extent thattheir retainability in service is affected. When hearing loss isdiscovered, through audiometric sun'eillance or otherwise, theservice members become subject to physical evaluation, fo de-termine whether they should be medically discharged from ser-vice. As opposed to the single induction standard, each ser\'icehas its own standards for medical fitness for retention, includ-ing hearing.^'' Even if service members with hearing loss areretained on active duty, they are eligible for fultire VeteransAffairs disability payments upon separation from service. Hear-ing loss and associated sequelae are the second most prevalentcause for Veterans Affairs disability payments to veterans (M,Wells, personal communication).
The baseline audiogram may be obtained before, during, orafter basic training. If a hearing loss is suificient to precluderetention in service, then it is classified as existing before ser-vice.** On average. 74 senice members receive exist ing-before-service discharges because of hearing loss each year.'' The Navyand Marine Corps are disproportionately represented in thesedischarges, relative to the number of accessions per year perbranch of service. This is expected, however, because thesesenices uniformly perform baseline audiograms during enlisteemedical in-processing, whereas, dtiring the period of this study.only Fort Sill. Oklahoma (artillery school), obtained baselineaudiograms for enlistees in the Army.''
The purpose of this study was to compare the performance, interms of retention, of active duty individuals with waivers for ahearinjj condition with that of other enlistees. In particular.their likelihood of retention over time ("survival") was comparedwith that of a matched group of fully qualified enlistees with nomedical waivers. The study attempts to provide evidence for oragainst the hearing accession standard and selective hearingloss waiver policy.
Methods
All active duty enlistees who began service in calendar years1995 to 2004 after receiving an accession medical waiver forhearing deficiency were included as case subjects. A matchedcomparison group was selected from among all fully qualified
63 Miiitary Medicine. Voi. 172. January 2007

64 Attrition of Enlistees with Hearing Deficiency Waivers
(i.e.. no medical waiver needed) enlistees, at a 3:1 ratio (controlsubjects). The matched factors were gender, age. race, branch ofservice, montb and year of beginning active duty, and ArmedForces Qualification Test percentile score (a measure of cognitiveability). Tbese factors have heen sbown to be predictors of attri-tion;' All subjects were monitored prospectively for attrition untilDecember 31. 2004, or the completion of 4 years of service, which-ever came first. Attrition over time was first compared between thehearing waiver and fully qualified groups by using the Kaplan-Meier method. This anaiysis was performed separately accordingto service, and all-cause attrition was used as the endpoint. Aproportional-bazards model with time-dependent covariates wastben applied. In addition to tbe matched factors, tbis model con-trolled for education, marital status, and body mass index,
The time-dependent model was first used with all causes ofearly attrition as the outcome. Tbis model was then separatelycalculated by restricting attrition to that related to medical con-ditions: tbat is. only those losses that were ofTicially attributedto medical causes were treated as attrition in tbis analysis.Losses attributable to administrative or other nonmedical rea-sons were treated as censored observations at the time of loss.
Results
More tban 1.5 million active duty enlistments occurred dur-ing 1995 to 2004. Of these, >6,000 required an accession med-ical waiver because of hearing deficiency. Table I sbows tbedemographic distributions of those witb" waivers for bearingdeficiency, with the demographic distributions of all enlistees.Tbose with waivers for hearing deficiency were significantly (p <
0.01) more male, older, and more Caucasian than the generalmilitary population. Prexious studies sbowed tbese factors to bepredictors of attrition.-' Therefore, selection of a matched comparisongroup was important to nullify tbe effects of tbese factors.
The cotmts and percentages of new accessions granted awaiver for hearing deficiency were highest for tbe Army (3.674;0.65%). foUowed by the Navy (1,605: 0.39%) and the MarineCorps (584: 0,23%). There were only 78 waivers (0.03%) forbearing in tbe Air Force. A matched sample of 17,982 controlsubjects (Army, 10.986: Nax'y, 4,752: Marine Corps, 2,019: AirForce, 225) was selected from enlistees wbo did not require anyaccession medical waiver.
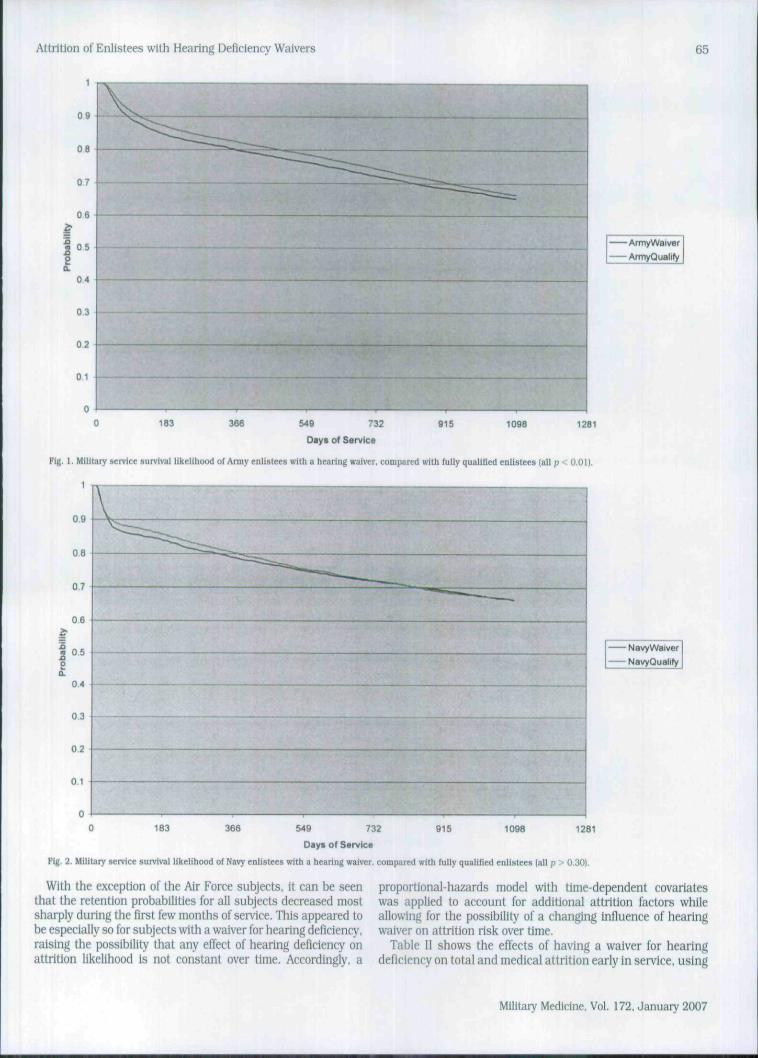
Kaplan-Meier survival curves comparing military retentionprobabilities between subject groups are shown in Figures 1to 4. It can be seen that the likelihood of staying in tbe servicevaried across the services. Army enlistees with a waiver forhearing deficiency bad a likelihood of retention that was sig-nificantly and uniformly lower than that of their matchedcounterparts (p < O.OI, using Wilcoxon, log-rank, and likeli-hood tests), Among Navy subjects, the retention probability waslower for the enlistees witii waivers tban for tbe qualified enlisteesearly in service time but tbe difference did not remain as servicetime increased; therefore, overall retention rates for tbe two subjectgroups were not significantly different.
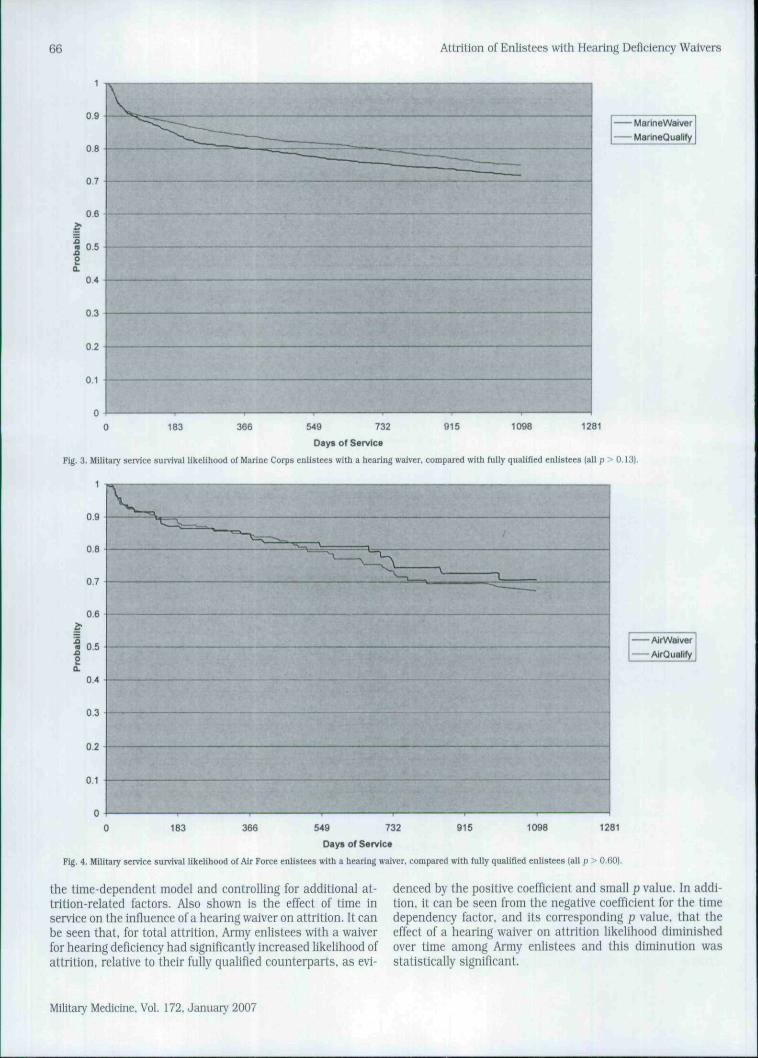
Retention probability for Marine Corps enlistees witb waiversfor hearing deficiency visually appeared lower than tbat for fullyqualified recruits, but tbe difference was not statistically signif-icant. There was almost no difference in early attrition rates fortbe Air Force subject groups, and the overall difference was notstatistically significant.
TABLE I
UEMOGi APHIC DISTRIBUTION OF ENLISTEES GiiANTED A WAiVER FOR HEARiNG DEFICIENCY VERSUS ALL ENLISTEES: 1995-2004
No. (%)"Gender|%)
FemaleMale
Age (%)17-20 years21-22 yearsS23 years
Race 1%)OtherAfrican AmericanCaucasian
BMI (%|Heavy {>30)Light (<201Overweight (25-30)Perfect 120-25!
AFQT t%)1 and 234 and 5
Army
HearingDeficiency
3.674 (0.65)
10.189.9
54.517.228.3
10.511.178.4
7.511.432.049.2
33.759.0
7.3
All
19.680.4
66.514.818.7
9.921.169.0
7.012.429.750.9
37.554.58.0
Navy
HearingDeficiency
1.605(0.39)
9.190.9
63.614.821.6
17.311.171,6
3.413.932.750.0
33.655.311.1
Ail
17.083.0
74.512.9i2.5
12.720.367.0
3.713.231.451.6
37,652.7
9.6
Marine Corps
HearingDeficiency
684 (0.23)
5.194.9
74.914.011.1
10.45.7
83.9
7.311.330.351.2
32.760.1
7.2
AU
6.993.1
83.49.76.9
12.311.875.9
5.911.828.653.8
37.954,8
7,3
Air Force
HearingDeficiency
78 (0.03)
15,484.6
62.8i6.720.5
10.37.7
82.1
1.324.426.947.4
55. i41.03.8
AU
25.075,0
74.415.010.6
9.216.774.2
0.8
14.926.757.6
47.445.3
7.3
" Counts and percentages of hearing deficiency among all enlistees entering active diiiy.BMI, body mass index (weight, in pounds, divided by height, in inches, squared and multiplied by 703): AFQT, Armed Forces Qualification Test(grouped by nationally nonned percentile groups: 1 = 93-99%. 2 = 65-92%, 3 = 50-64%, 4 = 30-49%, 5 = 1-29%).
Military Medicine, Vol. 172. Janua iy 2007
Attrition of Enlistees with Hearing Deficiency Waivers 65
0 9
08
07
06
e04
0.3 —
02
0 1
ArmyWaiver
ArmyQualify
183 366 1098 1261549 .-32
Diys of Sarvlcs
Tig. I. Military senice aurvlvHl likelihood of Anny enlistees witb a hearing waiver, compared with fully quallRed enlistees (all p < 0,01).
1
0.9
oa
0.7
0.6
I 05
0.4
0.3
02
0 1
NavyWaiver— NavyQualify
183 366 915 1098 1281549 732
Day* of Sarvlc«
Fig. 2. Militaiy service survival likelihood of Navy enlistees with a hearing waiver, compared with fully qualifled enlistees (all p > 0.30).
With the exception of the Air Force subjects, it can be seenthat the retention probabilities for all subjects decreased mostsharply during the first few months of service. This appeared tobe especially so for subjects with a waiver for hearing deficiency,raising the possibility that any effect of hearing deficiency onattrition likelihood is not constant over time. Accordingly, a
proportional-hazards model with time-dependent covariateswas applied to account for additional attrition faclors whileallowing for the possibility of a changing infiuence of hearingwaiver on attrition risk over time.
Table II shows the effects of having a waiver for hearingdeficiency on total and medical attrition early in service, using
Military Medicine, Vol. 172. January 2007
66 Attrition of Enlistees with Hearing Deficiency Waivers
MarineWaiver
MarineQualify
183 366 915 1098 1281549 732
Days of Service
Fig, 3. Military service survival likelihood of Marine Corps enlistees with a hearing waiver, compared with fully qualified enlistees (all p "• 0.13).
0.6
0.5
0.4
03
0.2
0.1
0
AirWalver
AirQuality
183 366 915 1098 1281549 732
Days of Service
Fig. 4. Military service survival likelihood of Air Force enlistees with a hearing waiver, compared with fully qualified enlistees (all p -•• 0.60).
the time-dependent model and controlling for additional at-trition-related factors. Also shown is the effect of time inservice on the influence of a hearing waiver on attrition. It canbe seen that, for total attrition. Army enlistees with a waiverfor hearing deficiency had significantly increased likelihood ofattrition, relative to their fully qualified counterparts, as evi-
denced by the positive coefficient and small p value. In addi-tion, it can be seen from the negative coefficient for the timedependency factor, and its corresponding p value, that theeffect of a hearing waiver on attrition likelihood diminishedover time among Army enlistees and this diminution wasstatistically significant.
Military Medicine, Vol. 172. January 2007

Attrition of Enlistees with Hearing Deficiency Waivers 67
TABLEC
HEARING WAIVER EFFECT OVERTIME IN SERVICE
AttritionType Service
Total Army
Navy
Marine Corps
Air Force
Medical Army
Navy
Marine Corps
Air Force
Factor
Hearing waiverTimeHearing waiverTimeHearing waiverTimeHearing waiverTimeHearing waiverTimeHearing waiverTimeHearing waiverTimeHearing waiverTime
Coefficient
0.38-0.06
0.42-0.06-0.210.07
-0.400.020.44
-0.071.14
-0,140.71
-0.131,71
-0.25
P0.010.030.020.100.490.230.720.920.020.04<.OOO10.020.090.110.350.45
Among Navy subjects, the likelihood of attrition was seen tobe greater among enlistees with a waiver for hearing deficiency,although the effect of this factor did not change significantlyover time. Finally, no statistically significant difference in attri-tion was seen between Marine Corps or Air Force enlistees andtheir matched counterparis.
When the outcome was restricted to losses attributed to med-ical reasons, it was seen that the influence of a hearing defi-ciency waiver remained significant among Army enlistees, againwith an effect diminishing over time. The likelihood of medical
reason-related attrition among Navy waiver subjects was alsosignificantly high, with the effect of hearing deficiency diminish-ing significantly over time.
Medical attrition among Marine Corps enlistees with a hear-ing deficiency waiver was borderline significantly high, with nosignificant change in this effect over time. There was no statis-tically significant diiTerence in attrition likelihood between theAir Force subject groups.
Figure 5 shows estimated all-cause attrition hazard ratiosas a function of time for subjects with hearing waivers versusfully qualified subjects according to service, and Figure 6shows analogous results for medical reason-related attrition.For all-eause attrition, the hazard ratio for hearing deficiencyover time was tiniformly higher among Navy subjects thanamong those of the other services, with Army subjects next.Although the results for the other two services appear in-verted from what would be expected, it should be kept in mindthat attrition was not significantly related to hearing waiverstatus for those two services.
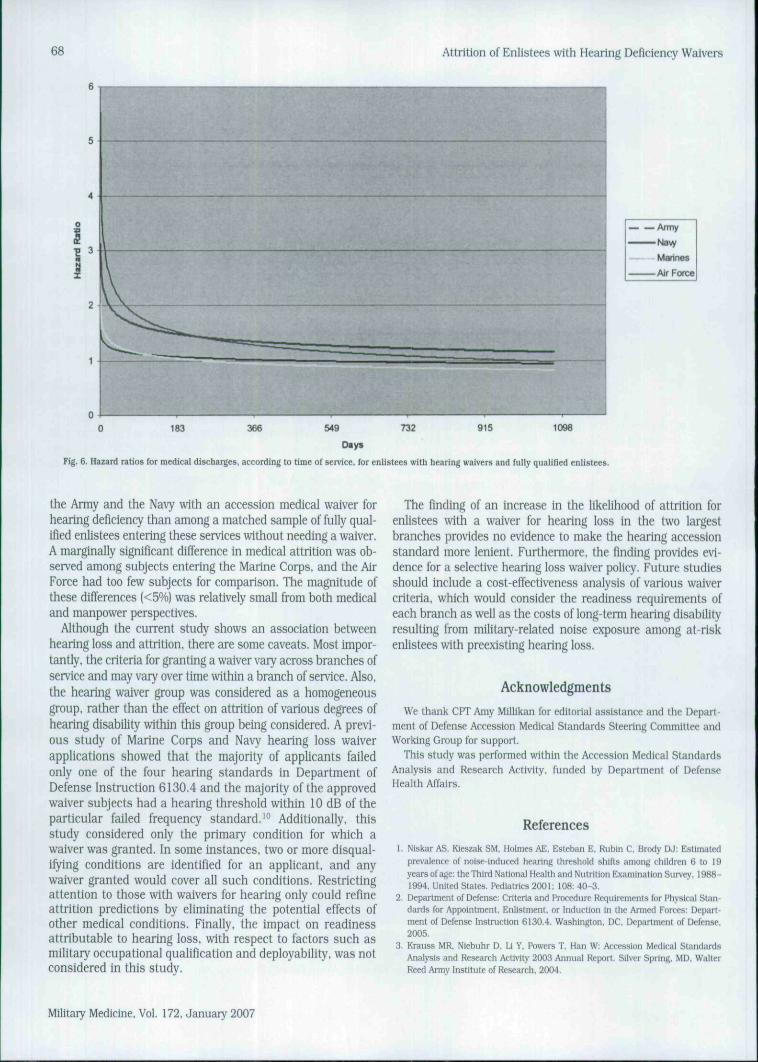
Figure 6 shows analogous results for medical reason-relatedattrition. Again it can be seen that the hazard ratio over time wasuniformly higher for the Navy subjects than for the Army subjects.The hazard ratio ctin-es for the Army and Marine Corps were quitesimilar lo one another, although, as mentioned above, the hazardratio lor the Marine Corps was only marginally significant, becauseof the smaller sample size for this service.
Discussion
The likelihood of early attrition, both all-cause and medicalreason-related, is noticeably higher among enlistees entering
Army
Marines
Air Force
163 366 915 1098549 732
D«yt
Fig. 5. Hazard ratioB for discharges, according to time of service, for enlistees with hearing waivers and fully qualified enlistees.
1281
Military Medicine, Vol. 172, January 2007
68 Attrition of Enlistees with Hearing Deficiency Waivers
Arniy
• " Na\v
Marines
Air Force
915 1098
Days
Fig. 6. Hazard ratios for medical discharges, according to time of service, for enlistees with hearing waivers and fuJly qualified enlistees.
the Ariny and the Navy with an accession medical waiver forhearing deficiency than among a matched sample of fully qual-ified enlistees entering these services without needing a waiver.A marginally significant difference in medical attrition was ob-served among subjects entering the Marine Corps, and the AirForce had too few subjects for comparison. The magnitude ofthese difi"erences [<5%) was relatively small from both medicaland manpower perspectives.
Although the current study shows an association betweenhearing loss and attrition, there are some caveats. Most impor-tantly, the criteria for granting a waiver vary across branches ofservice and may vary over time within a branch of service. Also,the hearing waiver group was considered as a homogeneousgroup, rather than the effect on attrition of various degrees ofhearing disability within this group being considered. A previ-ous study of Marine Corps and Navy hearing loss waiverapplications showed that the majority of applicants failedonly one of the four hearing standards in Department ofDefense Instruction 6130.4 and the majority ofthe approvedwaiver subjects had a hearing threshold within 10 dB of theparticular failed frequency standard,'" Additionally, thisstudy considered only the primary condition for which awaiver was granted. In some instances, two or more disqual-ifying conditions are identified for an applicant, and anywaiver granted would cover all such conditions. Restrictingattention to those with waivers for hearing only could refineattrition predictions by eliminating the potential effects ofother medical conditions. Finally, the impact on readinessattributable to hearing loss, with respect to factors such asmilitary occupational qualification and deployability. was notconsidered in this study.
The finding of an increase in the likelihood of attrition forenlistees with a waiver for hearing loss in the two largestbranches provides no evidence to make the hearing accessionstandard more lenient. Furihermore, the finding provides evi-dence for a selective hearing loss waiver policy. Future studiesshould include a cost-effectiveness analysis of various waivercriteria, which would consider the readiness requirements ofeach branch as well as the costs of long-term hearing disabilityresulting from military-related noise exposure among at-riskenlistees with preexisting hearing loss.
Ac knowledgments
We thank CPT Amy MiUlkan for editorial assistance and the Depart-ment of Defense Accession Medicai Standards Steering Committee andWorking Group for support.
This study was performed within the Accession Medical StandardsAnalysis and Research Activity, funded by Departmenl of DefenseHealth AHairs.
References
1. Nlskar AS, Kieszak SM, Holmes AE, Esteban E. Rubin C. Brody DJ: Estimatedprevalence of noise-Induced hearing threshold shifts among children 6 to 19years of age: Ihe Third National Health and Nutrition Examination Survey, 1988-1994, United States. Pediatrics 2001: 108: 40-3.
2. Department of Detense: Crilerta and Procedure Requirements for Physical Stan-dards for Appointment. Enltslment. or Induction in the i ^ i e d Forces: Depari-menl of Defense Instruction 6130.4. Washington. DC, Department of Defense,2005.
3. Krauss MR. Niebuhr D, Li Y. Powers T. Han W: Accession Medical StandardsAnalysis and Research Activity 2003 Annual Report. Silver Sprlnfl, MD, WalterReed Armv Institute of Research. 2004.
Military Medicine. Vol. 172. January 2007

Attrition of Enlistees with Hearing Deficiency Waivers
4. Department of Defense: DoD Hearing Conservation Program: Departmeni of De-fense Instruction 6055.12. Washington. DC. Department of Defense. 2004.
5. Departmcnl of lhe Army: Medical Services Standards of Medical Fitness: AmiykpS"l'>'ion 40-501. Washington. DC, Departmeni of the Amy. 2005,
6. Departmeni of the Nsvy. Bureau of Medicine iind Surgery: Manual of the MedicalDepartmeni. U.S, Navy. NAVMED p 117. Washington. DC. 2005.
7. Deparlmenl of lhe Air Force: Medical Kxaminalion and Standards: Air Forcelastniction 48-123. Washinglon. DC. Deparlmenl of the Air Force. 2001.
8. Departnient of the Army: I'ersonnel Separations: Active Duty Eniisted Adminis-
69
irailve Separations: Army Regulation 635-200. Washington, DC, Department ofthe Army, 2004.
9, Niebuhr DW. Complete JD. Heifer TM. Chandler DW: Acomparison of the miUlaiy
entrance processing station screening audiogram wilh the Defense Occupalionaland Envlroiinienlal Health Readiness System reference audiogram af Fort Sill,Oklahoma, in 2000. Mllil Med 2006: 171: 117-21.
10. Krauss MR. Niebuhr D, U Y. Powers T. Han W: Accession Medical StandardsAnalysis and Research Acllvity 2004 Annual Report. Silver Spring. MD. WallerKeed Army lnstiiute of Research. 2005.
Earn Your Challenge Coin Now!!!
AMSUS leadership believes that we need the help of cur-rent members to get the word out about the many ben-efits of an AMSUS membership. AMSUS is the only profes-sional organization representing Federal Healthcare andall medical disciplines. For every new AMSUS memberyou sponsor, we will give you an AMSUS Challenge Coin.We'll also recognize these recruiters in future issues ofthe AMSUS Newsletter. There is no better way to intro-duce new members to AMSUS than for people they al-ready know to talk about the many benefits, as well asinter-service networking opportunities that come withAMSUS membership. To receive credit for your new mem-ber, simply have them indicate your name on the "Thisapplication is sponsored by" line on their application. Oncethe application has been processed, your coin will be sentto you immediately. Supplies of the new coin are limited,so be sure to act now!!
Military Medicine. Vol. 172. January 2007
