aug 26 2015 webinar combined presentation slides...
TRANSCRIPT

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 1
2015 Pharmacy Education Series
August 26, 2015System Elements of a Medication Error Reduction Program:y g
What Every Pharmacist Needs to Know
Featured Speakers:
Allen Vaida, PharmD, FASHP Gerard Kalbfell, RN, BSN, MSHAExecutive Vice President Director, Patient SafetyInstitute for Safe Medication Practices Community Health Systems
1
Submission of an online evaluation is the only way to obtain CE credit for this
Online Evaluation, Self-Assessmentand CE Credit
y ywebinar
Go to www.ProCE.com/CHSRx Webinar attendees will also receive an email with a direct link to the web page Print your CE statement of completion online
– Credit for live or enduring only
Deadline: September 25, 2015 CPE Monitor (applicable to pharmacists & pharmacy technicians)
– CE information automatically uploaded to NABP/CPE Monitor within 1 to 2 weeks of the completion of the self‐assessment and evaluation
2
completion of the self assessment and evaluation
CE Broker ‐ this CE activity is approved for State of Florida Medication Safety CE credit. Pharmacists and pharmacy technicians licensed in the State of Florida must provide their license number to [email protected] for completed CE credit to be posted to CE Broker.
Event Code
Code will be provided at the end of today’s activity

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 2
How to Ask a Question
Locate menu bar on your computer desktop Click No!
Click orange arrow button
Menu box will open
Type question into question box
Click Send
Do not close menu box
– This will disconnect you from the Webcast
Please submit questions throughout presentation
Enter question
Click Send
3
Accessing PDF Handout
Click the hyperlink that is located directly above the No!located directly above the question box
Do not close menu box
– This will disconnect you
from the Webcast
Close other applications Clickhyperlinkhyperlink
4

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 3
August 26, 2015System Elements of a Medication Error Reduction Program:
What Every Pharmacist Needs to Know
Featured Speakers:
Allen Vaida, PharmD, FASHP Gerard Kalbfell, RN, BSN, MSHAExecutive Vice President Director, Patient SafetyInstitute for Safe Medication Practices Community Health Systems
5
It is the policy of ProCE, Inc. to ensure balance, independence, objectivity and scientific rigor in all of its continuing education activities. Faculty must disclose to participants the existence of any significant financial interest or any other relationship with the manufacturer of any commercial product(s) discussed in an educational presentation. Mr. Kalbfell has no relevant commercial and/or financial relationships to disclose. Dr. Vaida has no relevant commercial and/or financial relationships to disclose.
Please note: The opinions expressed in this activity should not be construed as those of the CME/CE provider. The information and views are those of the faculty through clinical practice and knowledge of the professional literature. Portions of this activity may include unlabeled indications. Use of drugs and devices outside of labeling should be considered experimental and participants are advised to consult prescribing information and professional literature.
Institute for Safe Medication Practices Community Health Systems
CE Activity Information & Accreditation
ProCE, Inc. (Pharmacist and Pharmacy Technician CE)
– 2.0 contact hours
F di
This CE activity is approved for State of Florida Medication Safety CE credit.
6
Funding:This activity is self‐funded through CHSPSC.

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 4
System Elements of Medication Safety: What Every Pharmacist y y
Needs to Know
CHS Medication Safety Webinar
August 26, 20152 4 ET 1 3 CT2 pm – 4 pm ET; 1 pm – 3 pm CT
Presented by: Allen Vaida, Pharm.D., FASHP
Executive Vice President
7
Disclosure
Allen Vaida declares no conflicts of interest, real or apparent and no financial interests in any companyapparent, and no financial interests in any company,
product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and
honoraria.
8

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 5
Objectives
• Identify where errors are likely to occur in the medication use processmedication use process
• Explain system‐based causes of error and how to avoid patient harm
• Recognize the difference between prospective and retrospective risk identification
Li fi k f i i l i di i• List five key safety principles to use in medication error prevention
9
Finding Errors: Risk Identification
10

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 6
Risk Identification
Risk identification in healthcare…..
• Detection of a potential or actual problem associated with patient care
• Recognizing variations in process or expected outcomes which may or may not involve patient harmharm
• Error repor ng alone ≠ Risk iden fica on
11
Risk is Everywhere
Ri k i i h l b d• Risk is not inherently bad
• Healthcare can be “safe” but not “risk‐free”
• Which risks are worth taking?
12

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 7
Identification Methodology
• Prospective/Proactive
– Condition or state of beingCondition or state of being
– Hazardous condition or behavior
– FMEA, What if?
• Retrospective
– May or may not have reached the patient
– May or may not have resulted in harm
– Incident reports, RCA
13
Sources for Internal Capture
• Voluntary error reporting programs
Ad D R ti ti• Adverse Drug Reaction reporting
• Observation methods
• Chart review (e‐codes, ICD, triggers)
• Technology data (ADCs, Rx system, CPOE, Bar Coding, Smart pumps,..
Ph i t i t ti• Pharmacist interventions
• Surveillance Systems
14
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 8
Ask Yourself
• Can we see weak signals of failure and make sense of them? (failure in the system)(f y )
• Churchill’s protocol: (nature of mindfulness)– Why didn’t I know?
– Why didn’t my advisor’s know?
– Why wasn’t I told?
– Why didn’t I ask?
Managing the Unexpected: Resilient Performance in an Age of Uncertainty: By Karl E. Weick, Kathleen M. Sutcliffe
15
The Tip of the Iceberg
Event reports
Hidden items
16

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 9
Incidents Detected by Three Methods
Olsen, S. et al. Qual Saf Health Care 2007;16:40‐44
17
Voluntary Reporting Programs
• Capture unexpected occurrences
– Adverse events near misses errors hazardousAdverse events, near misses, errors, hazardous conditions
• Can provide for timely investigation of event
• Provide raw data for identification of risk
• Engage frontline staff
( f )• Report dangerous conditions (potential for error)
• Indicator of culture in an organization
18
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 10
Enhance Voluntary Reporting
• Make it a goal
E h i ti f h d diti d• Emphasize reporting of hazardous conditions and close calls/near misses
– Easier to talk about events that did not lead to an error or reach a patient
• Give feedback – safety rounds – staff meetings
19
Question
Does your organization have a ‘good catch’ program’ that promotes reporting of risks that may not havethat promotes reporting of risks that may not have caused errors (hazardous conditions)?
a. Yes
b. No
20

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 11
“You Can See a Lot Just by Looking ”You Can See a Lot Just by Looking.
Yogi Berra USA Baseball player and coach
21
Specific Risk Identification Methods
22

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 12
Sources of Information
• Variety of sources
F t li t ff– Front line staff
– Patients (rounds, satisfaction, advocate)
– Medical records (retrospective)
– Information systems (order entry data)
– Device reports (automated dispensing cabinets p ( p g[ADCs], smart pumps, barcode point‐of‐care information) (retrospective)
– External sources (prospective)
23
Other Sources of Information
• Rapid response team reports (retrospective)
F d di ti i ( ti )• Focused medication reviews (prospective)
• FMEAs (prospective)
• RCAs (retrospective)
• Self Assessments (prospective)
• Safety or executive walk‐arounds (prospective)y (p p )
• Safety briefings/staff meetings (prospective)
FMEA: failure mode and effects analysisRCA: root cause analysis
24

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 13
Concurrent Risk Assessment
• Pharmacy interventions
N i i t ti• Nursing interventions
• Triggers and markers (also could be retrospective)
• Active surveillance
• Clinical decision support
25
Self Assessments
26

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 14
Self Assessments
27
Failure Mode and Effects Analysis (FMEA)
• A proactive process to identify potential errors and determine possible effects
• Team‐based, systematic, proactive approach
• Identify the ways that a process or design
– Can fail
– Why it might fail
– What will happen if it fails
– How it can be made safer
• Veterans Affairs National Center for Patient Safety
28

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 15
Consider the Process Flow
• Who purchases?
Wh t d?
• Who administers it?
H / h it ?• Where stored?
• Who prescribes?
• How is it ordered?
• Where is it used?
• How does it arrive?
• How/who monitors?
• Who adjusts therapy?
• How is administration documented?
• How is it reordered?
• What COULD happen?
29
30

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 16
31
32

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 17
33
Available External Information
• Safety newsletters and articles – ISMP, TJC, FDA, d ti t t tivendor reporting program, state reporting program
advisories…
• National alerts
• Journal Articles
• Media – what your administrator and board are following
34

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 18
External Reports
35
Triggers
• An easily identifiable, focused item representing an opportunity (or clue) that may lead to an adverseopportunity (or clue) that may lead to an adverse event
• Medications, laboratory tests, patient conditions
• Something went wrong
• Effective method for measuring harm
36

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 19
Pharmacist Interventions
• During order entry or verification
D dj t t d l ti– Dose adjustments, drug selection recommendations
• Customized screening alerts
– Patient information, lab information, drug database warnings
• Active surveillance triggers
37
Observation
• AU MEDS www.medaccuracy.com
B k t l A b U i it– Barker, et.al. Auburn University
• Requires a direct observer
• Compared observation of what was administered to original order
• 2002 study found almost 1 in 5 (19%) of the doses were in error
– 7% were rated potentially harmful
38

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 20
Observation
• Take this further than medication d i i t tiadministration
– Processes (verbal orders, compounding, programming infusion pumps, workflow)
– Storage conditions
– Communication dynamics
39
Technology Data
• Information systems– Alerts
d– Overrides– Missing patient information
• Barcode point of care systems– Wrong medications, wrong patient, wrong time
• Automated Dispensing Cabinets– Overrides
• Infusion pumps– Hard maximum limit triggers– Soft low and maximum limit triggers
40

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 21
Question
How many of you have a software surveillance system in place to help identify interventions and directin place to help identify interventions and direct resources to patients who require it the most?
a. Yes
b. No
41
System thinking: How to analyze events
42

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 22
Systems Thinking
• A system is a group of interacting, i t l t d d i t d d t tinterrelated, and interdependent components that form a complex and unified whole
• A way of understanding the relationship among a system’s parts, rather than the parts themselves
43
To Err is Human
• No one is immune
• Human error is not a behavioral choice• Human error is not a behavioral choice
• Least manageable link in error
• Manage causes and consequences of errors through system design
44

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 23
Experience is the name everyone gives to their mistakes.Oscar Wilde‐‐‐Oscar Wilde
Anyone who has never made a mistake has never tried anything new.‐‐‐Einstein
45
‐‐‐Einstein
We All Drift
• Drifting = at‐risk behaviors
i• Primary reasons
‐ Desire to accomplish more
‐ Fading perceptions of risk
‐ Unknowingly create unjustifiable risk
‐ Convince one’s self they are in a safe place
• Example
‐ Driving an automobile
46

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 24
Drift
• Behavioral choices that increases risk where risk is not recognized, or is mistakenly believed to be
f djustified
• Driven by perception of consequences
‐ Immediate and certain consequences are strong
‐ Delayed and uncertain consequences are weak
• System‐based causes; culture tolerant of riskSystem‐based causes; culture tolerant of risk
‐ “It’s never happened here” syndrome
47
Everyday Risk ‐ ‘Choices’ ‐ Drift
• Wearing seat belts in cars
U i bil h hil d i i• Using a mobile phone while driving
• Texting while driving
• Driving over the speed limit
• Right turn on red without stopping
48

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 25
Everyday Risk at Work ‐ ‘Choices’ ‐ Drift
• Perform time‐outs
• Correct double‐check when needed or required
• Labeling of all syringes and bowls
• Read back or repeat back of verbal/telephone orders
• Reuse of single dose vials
• Using bar code scanning systems
• Responding to computer alerts p g p
• Take the MAR (paper or electronic) directly to bedside
49
50
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 26
Latent (System) Failures
• Incomplete information about a patient
• Unclear communication of a drug order• Unclear communication of a drug order
• Lack of computer warnings (interactions, allergies, dosages, etc.)
• Ambiguous drug references
• Drug storage (look alike/sound alike medications, hazardous chemicals)hazardous chemicals)
• Unclear policies/procedures
• Failed checking processes
51
Limitations on Human Performance
• Limited ability to multi‐task
I t ti d di t ti• Interruptions and distractions
• Fatigue and psychological factors
• Environnemental factors (light, noise, temperature)
• Human Factors
– Confirmation bias
– Dependence on heuristics during times of stress
– Normalization of deviance
52
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 27
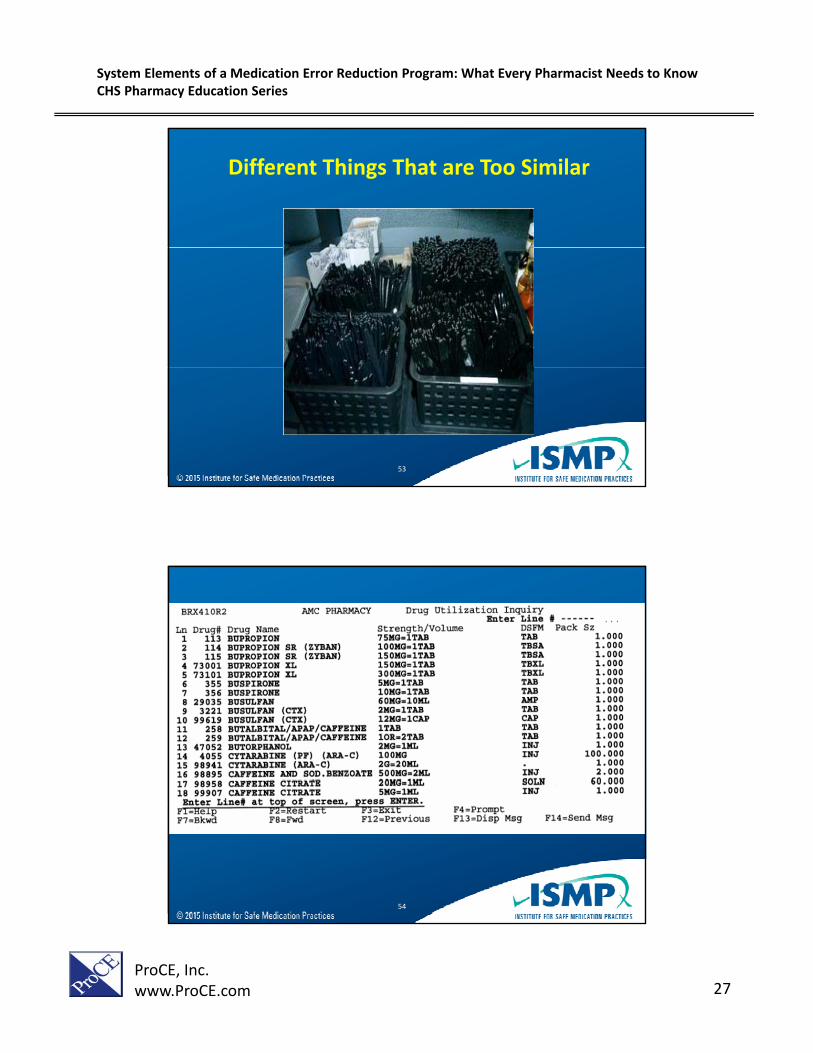
Different Things That are Too Similar
53
54

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 28
Systems of Medication Use™
1. Patient information
2. Drug information
6. Device acquisition, use, and monitoring
3. Communication of drug information
4. Labeling, packaging, and nomenclature
5. Drug storage, stock, t d di ti d
7. Environmental factors
8. Staff competency and education
9. Patient education
10.Quality, culture, and risk t istandardization, and
distributionmanagement issues
55
Error Reduction Strategies
56

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 29
Primary Principles for Error Reduction
• Reduce or eliminate the possibility of error
M k i ibl• Make errors visible
• Minimize the consequence of errors
• Report and analyze internal errors
• Report errors externally and use external information
57
Error Reduction Strategies
Strategy– Fail‐safes and constraints
Forcing functions
Power (Leverage)
Car won’t start if alcohol is detected– Forcing functions
– Automation and computerization
– Standardization
– Redundancies
– Reminders and checklists
– High (“Blunt end”)
– Medium
alcohol is detected on breath
Reminder signs and
checkpoints
Rule/Law: It’s illegal
– Rules and policies
– Education and information
– Suggestions to “be more vigilant”
– Low (“Sharp end”)
/ gto drive over the allowable alcohol
limit
58

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 30
59
Use Constraints to Limit Access
• Reduce access to dangerous items
P hibit h b h i t– Prohibit pharmacy access by non‐pharmacists
– Limit number of choices/concentrations
• Move problem products out of reach
– Potassium chloride
– Neuromuscular blockers
60

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 31
Forcing Functions
• Ensures that parts from different systems are not interchangeableinterchangeable
• Forces proper methods of use
• Makes errors immediately visible
– Preprinted order forms or computer options that “force” selection (Limited Medications, Available d )
61
dosages)
– Oral syringe should not be able to fit onto an intravenous line
Simplify: Reduce the number of options
62

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 32
Available Heparin Concentrations
• 10 units/mL
• 100 units/mL
• 5,000 units/mL– 1 mL vial• 100 units/mL
– 1 mL vial
– 10 mL vial
• 1,000 units/mL
– 1 mL vial
– 2 mL vial
– 10 mL vial• 10,000 units/mL
– 1 mL vial– 4 mL vial– 5 mL vial– 10 mL vial
63
– 10 mL vial
– 30 mL vial
• 20,000 units/mL– 1 mL vial– 5 mL vial
Simplify: Reduce the number of options
64

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 33
Externalize: Transfer error‐prone tasks
• Use commercially‐available productsavailable products
• Outsource low volume solutions
• Prepare chemotherapy in a centralized location with specialized staffwith specialized staff
65
Redundancy: Multiple pathways
• No single failure can cause an eventcause an event
• Second pathway prevents failure
66

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 34
Redundancy: Double checks
• Can be an important safety strategy
T k t ti• Takes extra time
• Some believe may lead to more mistakes as staff may rely upon the checker to catch the mistake
• Work best when independent
– No cues from the person who carried out the work
67
Redundancy: Double checks
• Identify a high rate of errors
• Study of prescriptions awaiting pick upStudy of prescriptions awaiting pick up
– 5,700 prescriptions
– 240 filled in error (2.1% considered potentially harmful)
• Studies where artificial errors were introduced
– 93‐97% were identified by an independent double– 93‐97% were identified by an independent double check
• Hard to find your own mistakes (confirmation bias)
68

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 35
Situational Awareness: Enhance understanding to reduce drifting into
unsafe behaviors
Si l ti• Simulation
– Clinical scenarios
– Real‐life conditions
– Initial and ongoing training
– Used in pharmacy schoolUsed in pharmacy school education
– Available in many hospitals
69
Positive Performance Shaping: Improve human performance
• Environment
T t
• Workload
Shift l th– Temperature
– Lighting
– Noise
– Distractions
– Shift length
– Importance of breaks
– Multi‐tasking
– Mixed messages
– Rewarding risky g ybehavior
70

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 36
Checklists/Reminders: Assist with remembering
• Reminders
Order sets (e g
• Check lists
IV Compounder set– Order sets (e.g., management of hypoglycemia)
– Auxiliary labeling (e.g., “FOR INTRAVENOUS USE ONLY FATAL IF
– IV Compounder set up
– Adding a new drug to a database
– Complex validation processes (e.g.,
ONLY – FATAL IF GIVEN BY OTHER ROUTES”)
chemotherapy preparation)
71
Summing UpError Reduction Strategies
• Error prevention strategies are not mutually exclusive
Th f t t d i t l ti t l b• The fastest and easiest solution may not always be the best… and may introduce new sources of error
• People cannot be expected to compensate for work systems
72

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 37
Conclusion
• Risk identification must go beyond just voluntary error reportingerror reporting
• It is best to utilize both prospective and retrospective methods
• The best safety plan will combine different levels of risk reduction strategies
E d b f i i l• Empowered to use a number of principles to prevent medication errors
73
ISMP National Medication Errors Reporting Program and Vaccine Errors
Reporting Program
ISMP is a federally certified patient safety organization (ISMP is a federally certified patient safety organization (PSO)PSO)ISMP is a federally certified patient safety organization (ISMP is a federally certified patient safety organization (PSO)PSO)
74

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 38
CHS PSO, LLC
Presented By:
Gerard P. Kalbfell, Director, Patient Safety, CHS PSO
75
ALL INFORMATION CONTAINED IN THIS PRESENTATION IS PROTECTED UNDER THE CHS PSO, LLCThe information contained in this presentation was developed and provided through CHS PSO, LLC, Patient Safety Organization for the conduct of patient safety activities. As a result, the content of this information is confidential patient safety work product. It is protected from disclosure pursuant to the provisions of the Patient Safety and Quality Improvement Act (42 CFR, Part 3) and other state and federal laws. Unauthorized disclosure or duplication is prohibited. As a recipient of this information, you federal laws. Unauthori ed disclosure or duplication is prohibited. As a recipient of this information, youacknowledge and agree to the following:
• any and all such information gained through my experience or association with CHS PSO, LLC is strictly confidential;
• CHS PSO, LLC and its participating members shall own all right, title and interest in and to the patient safety work product or related PSO documentation; and
• not to release, relay, transcribe, photocopy, retain or in any manner disseminate said information, either orally or in writing, to any person or organization without the express consent of CHS PSO, LLC legal counsel.
CHS PSO LLC Confidential patient safety work product document Protected from disclosure pursuantCHS PSO, LLC. Confidential patient safety work product document. Protected from disclosure pursuant to the Patient Safety and Quality Improvement Act (42 CFR Part 3) and other state/federal
laws. Unauthorized disclosure or duplication is prohibited.
76

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 39
SAFETY FIRST – LIVE THE SAFETY MESSAGE
TO KEEP SAFETY TOP OF MIND IN THINKING AND– TO KEEP SAFETY TOP‐OF‐MIND IN THINKING AND
DECISION MAKINGSAFETY AS A CORE VALUE!
77
Objectives• Demonstrate an understanding of the Patient
Safety and Quality Improvement Act of 2005, andthe Final Rule Promulgating the Act, effectiveJanuary 19, 2009
• Demonstrate an understanding of the PatientSafety Evaluation System
• Identify Three Ways Humans Perform• Identify Individual and System Failures• Demonstrate Components of Cause AnalysisDemonstrate Components of Cause Analysis• Identify Leading Causes of Action Failure
78
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 40
What is a PSO?• Patient Safety & Quality Improvement Act
– Congress passed in 2005
d d h– To encourage provider‐driven initiatives to improve the safety & quality of patient care
– Established a framework by which providers may conduct a wide range of patient safety activities through participation in a Patient Safety Organization (PSO)
79
What is a PSO?• PSOs:
– An entity or a component of another organization (private or public) that has a mission and primary activity of improving patient safety and the quality of healthcare deliverypatient safety and the quality of healthcare delivery.
– Afford both privilege and confidentiality protection, which creates a secure environment where providers can collect, aggregate, and analyze data to improve quality.
• Subject to exceptions, such as criminal proceedings
– Approved and listed by AHRQ http://www.pso.ahrq.gov/listing/psolist.htmp // p q g / g/p
80

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 41
What is a PSO?• A PSO serves as a resource that collects, analyzes, and aggregates “patient safety work product” (e.g., RCAs, event reports) to develop i i h i h d l i f iinsights into the underlying causes of patient safety events.PSWP = “Any data, reports, records, memoranda, analysis (such as RCA), or written or oral statements (or copies of any of this material)”
• Types of PSOs:• Types of PSOs:– Component‐affiliated
– Commercial
– Association‐based
81
Purpose
• CHS PSO is a component PSO– Shared staff and resources – PSWP must remain separate from the rest of the parent organization.
• AHRQ approved & officially listed CHS PSO, LLC effective 1/11/12 as a component PSO of CHS/Community Health Systems, Inc.
• Each CHS affiliated hospital is a member of the PSO id d b t d ti i ti tas evidenced by executed participation agreements
82

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 42
Patient Safety Activities• The PSO carries out the following patient safety activities:
_ Efforts to improve patient safety and the quality of healthcare delivery.
– Collection and analysis of patient safety work product (PSWP).– Development and dissemination of information regarding patientDevelopment and dissemination of information regarding patient
safety, such as recommendations, protocols or information regarding best practices.
– Utilization of PSWP for the purposes of encouraging a culture of safety as well as providing feedback and assistance to effectively minimize patient risk.
– Maintenance of procedures to preserve confidentiality with respect to PSWP.
– Provision of appropriate security measures with respect to PSWP.– Utilization of qualified staff– Utilization of qualified staff.– Activities related to the operation of a patient safety evaluation
system (PSES) and to the provision of feedback to participants in a PSES.
83
What is a PSES?• Definition:
– “Patient safety evaluation system means the collection, management, or analysis of information for reporting to or by a PSO.”or by a PSO.
42 CFR Part 3, PSQIA, Final Rule §3.20; 73 Fed. Reg. 70798.
• It is the mechanism through which information can be collected, maintained, analyzed, and communicated.
– “Protected space or system that is separate, distinct and resides alongside but does not replace other information collection activities . . .”
• Typically exists at the hospital or single provider level, but can exist within a parent organization as well as with providers.
84

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 43
What is a PSES?
• Think of the PSES as a “protected space” or
an information sharing “structure”:an information sharing structure :
PSES*PSWP‐ data aggregation‐ causation analysis‐ ideas for prevention and improvement
To: Providers/Reporters• Safety Alerts• Best Practices• Training & Education• Safety Improvement
Plans
From: Providers/ Reporters• Events• Raw DataRaw Data• Medical Records
85
EVENT REPORTING SYSTEM (ERS)SYSTEM (ERS)
ERS = the patient safety p yevaluation system for CHS PSO affiliated providers
86

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 44
Events that should be reported include:Medication Variances
Adverse Drug Reactions
Falls
Surgical/Invasive/Tests or Procedures
Equipment
Perinatal
Miscellaneous and Pressure Ulcers
B h i lBehavioral
Complaints and Grievances
Needlestick and Sharp Injuries
87
Reporting – What Should be Reported?
• Patient Complaints and Grievances – complaints about wait times, scheduling, facilities, safety/quality of care, communication, behavior, parking
• Adverse Drug Reaction: no error has occurred and patient has had a reaction to a medication
Below are some examples of what should be reported, this may not be all inclusive, when in doubt ASK ; It is okay not to know, it is not okay not to find out.
medication
• Lab Specimens‐ orders written or entered for wrong patient or test; delays in reporting ; mislabeled specimens, delay in physician review of results, delay in contacting patient with results
• Medication Errors – wrong: dose/ medication/ person/ route ; Wrong Prescription: dose/ medication/ person/ route/ pharmacy ; medication prescribed or administered with known patient allergy
• Falls – any patient or visitor falls
• Patient Injury – from equipment ; from casting, bandaging or splinting ; injection site; lab draw
• Procedural issues – any complications ; any injury ; wrong: patient/ procedure/ implant/ site, includes events discovered as a result of hospital care.
• Diagnostic Imaging – delay in patient notification of results, wrong person/wrong site (Left vs Right) / procedure performed incorrectly (head vs abdomen) or (supine vs lateral),
88

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 45
Privilege• PSWP is privileged
• “Notwithstanding any other provision of Federal, State, Local, or Tribal Law” PSWP is not subject to:– Civil Subpoena or Order– Civil Subpoena or Order
– Discovery in administrative proceedings
– State/Federal FOIA requests
• Cannot be admitted as evidence in federal or state civil or criminal proceeding, administrative rule‐making or adjudicatory proceeding or in any professional disciplinary proceeding
• Limited purpose release does not constitute a waiver• Limited purpose release does not constitute a waiver
• Protection might reach back to July 29, 2005 in certain circumstances
• PSA preempts conflicting state law
89
Patient Safety Work Product Privilege
• Not subject to subpoena, civil discovery, j p , y,State/Federal FOIA requests
• PSWP privileged if:– Assembled or developed by the member provider for the purpose of reporting and is reported to the PSO
– Developed for the purpose of conducting patient safety activitiesact t es
– Analysis of PSWP either by the member provider or PSO for promoting patient safety
90

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 46
Confidentiality• PSWP is confidential and shall not be disclosed unless the disclosure meets the
requirements for disclosure:– in a criminal proceeding;
– to permit equitable relief for reporters;
th i d b id tifi d id– authorized by identified providers;
* for patient safety activities;
• between a provider and PSO;
• to a contractor of a PSO;
• among affiliated providers; or
• to another PSO or provider.
– of nonidentifiable PSWP;
– for research;
– to the Food and Drug Administration (“FDA”) and entities required to report to the FDA;
l l d b d– voluntarily to an accrediting body;
– for business operations; and
– to law enforcement.
• PSWP disclosed per the exceptions above, or disclosed impermissibly, shall continue to be privileged and confidential.
91
PSOs in the Real World
• Handling requests/demands for production of PSWPPSWP
• Third‐party requests for production of documents & subpoenas– Generally PSWP not subject to discovery
92

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 47
PSOs in the Real World
• Regulatory Oversight Agencies– e.g., CMS Surveyors– Both a privilege and disclosure problem– PSO workforce may field questions regarding CMS & AHRQ access to information
– Both are aware of this dynamic and “discussions” are ongoing
• Release of PSWP– Operational reasons? PR/marketing?– PR/marketing?
– Medical staff reasons?– Participating providers should consult with CHS PSO regarding dissemination of PSWP
93
PSO Involvement…..
• Medication Management Committee
• Medication Safety Committee
• Patient Safety Committee
• QSE Committee – Physician Office Practices
• And on and on and on….
94

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 48
Comprehensive Risk Assessment
• Every January, your facility Risk or Quality Di t ill d t it i kDirector will conduct an onsite risk assessment
• Review the items on the Risk Assessment and be prepared to demonstrate procedures, policies and practicesp , p p
• Best practices, policies for corrective actions are posted on the intranet
95
ComprehensiveRisk Assessment Program
• Where do the questions come from?
K t f f t t– Known root causes of safety events
– Risk reduction strategies or alerts from nationally recognized associations (e.g. ISMP Alerts, AAFP)
– Standardized best practices
– Regulations and industry standards (e.g. OSHA)
– History of Liability Claims and Serious Safety Events
– Advisory review risk assessments annually and concurrently (e.g. Risk, Lab, IC, Facilities, RM, Pharmacy, Imaging, Quality, Clinical Services)
• Recommend revision or additions to risk assessment
96

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 49
Why Events Occur
Ways the brain functions that allows human errors
How system flaws contribute to human error
How both system flaws and h bi thuman errors combine to cause patient injury
© Adapted for CHS PSO, LLC by Healthcare Performance Improvement LLC; ALL RIGHTS RESERVED97
Knowledge BasedP f Rule Based
Three Ways Humans Perform
Skill Based
Performance(Figuring-It-Out Mode)
Rule BasedPerformance
(If-Then-Response Mode)
Skill BasedPerformance
(Auto Pilot Mode)
© Adapted for CHS PSO, LLC by Healthcare Performance Improvement LLC; ALL RIGHTS RESERVED
98

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 50
Skill Based Rule Based Knowledge Based
Activity
Type
Familiar, routine acts that can be carried out smoothly in an automatic fashion
Problem solving in a known situation according to set of stored “rules,” or learned
Problem solving in new, unfamiliar situation for which the individual knows no rules – requires a plan of action to
Human Error ClassificationBased on the Skill/Rule/Knowledge classification of Jens Rasmussen and the Generic Error Modeling System of James Reason
in an automatic fashionprinciples
requires a plan of action to be formulated
Error
Types
Slips
Lapses
Fumbles
Wrong rule
Misapplication of a rule
Non-compliance with rule
Formulation of incorrect response
Error
PreventionSelf checking – stop and
Educate if wrong rule
Think a second time if misapplication
Non compliance red ce Stop and find an expertPrevention
Themesthink before acting Non-compliance – reduce
burden, increase risk awareness, improve coaching culture
Stop and find an expert
Error
Probability1:1000 1:100 3:10 to 6:10
© 2007 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
99
Human Error Types Best Practice Error Prevention Tools
Skill‐Based Errors • Self Checking with S.T.A.R.• Team Member Checking/Coaching & ARCC
Rule‐Based Errors • Team Member Checking/Coaching & ARCC• Read/Repeat Backs with Clarifying Questions• SBAR/Hand‐offs• STOP and Resolve – Validate and Verify• Document Legibly and Accurately
Knowledge‐Based Errors • Team Member Checking/Coaching & ARCC• Read/Repeat Backs with Clarifying Questions• SBAR• STOP and Resolve – Validate and Verify• Document Legibly and Accurately
100

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 51
Individual Human Error Diagnostic Chart
1) Failures Modes of people
2) 20 Failure Modes in Five Categories:Categories:• Competency
• Consciousness (Inattention to Detail)
• Communication
• Critical Thinking
• Compliance
3) Internal Factors affecting Human Performance
Describes the “how” of the mistakes that were made.101
System Failures Diagnostic Chart
1) Failure Modes of systems, programs and processes)
2) 26 Failure Modes in Five2) 26 Failure Modes in Five Categories: Structure
Culture
Process
Policy & ProtocolPolicy & Protocol
Technology & Environment
3) External factors to human performance
Describes the “why” of the mistakes that were made102
System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 52
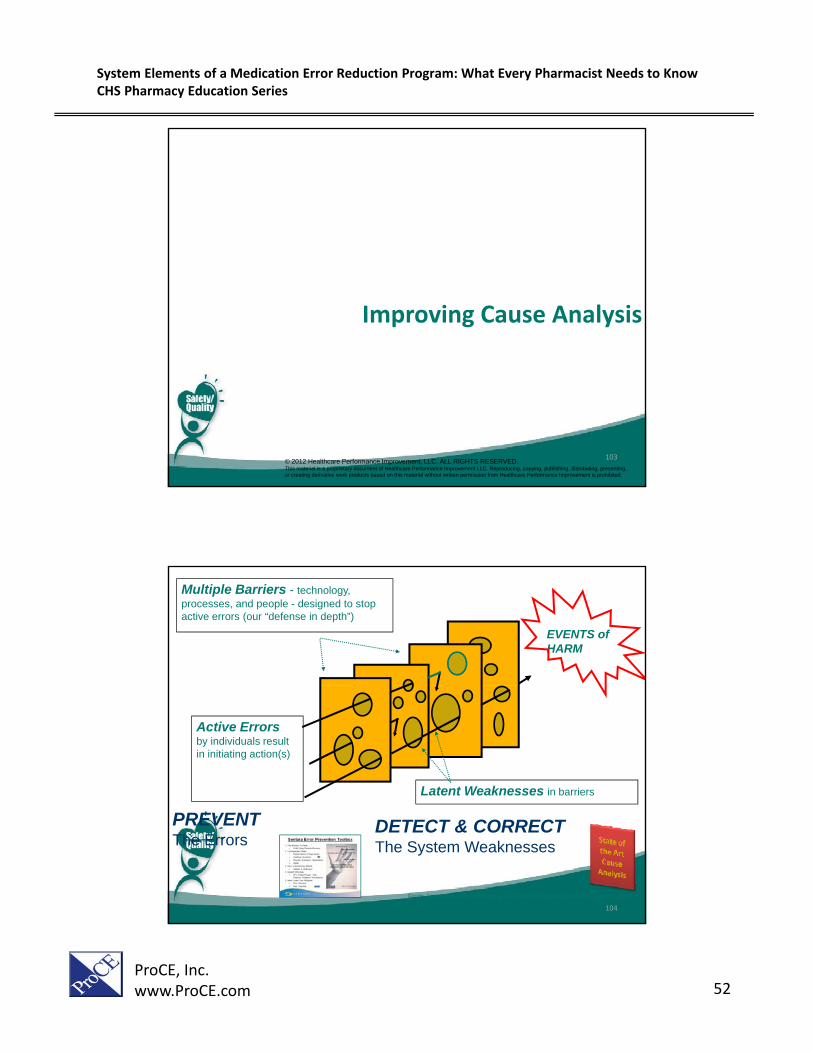
Improving Cause Analysis
© 2012 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.This material is a proprietary document of Healthcare Performance Improvement LLC. Reproducing, copying, publishing, distributing, presenting, or creating derivative work products based on this material without written permission from Healthcare Performance Improvement is prohibited.
103
EVENTS ofHARM
Multiple Barriers - technology, processes, and people - designed to stop active errors (our “defense in depth”)
Active Errorsby individuals result in initiating action(s)
Latent Weaknesses in barriers
From James Reason, Managing the Risks of Organizational Accidents, 1997
PREVENTThe Errors
DETECT & CORRECTThe System Weaknesses
104

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 53
The HPI Approach to Cause AnalysisThree Components:
R t A t CRootCauseAnalysis
ApparentCauseAnalysis
CommonCauseAnalysis
A structured problem‐solving technique that
A limited investigation of an event that is performed
A method to periodically examine the commonsolving technique that
results in one or more corrective actions to prevent recurrence of an event.
an event that is performed instead of RCA for less‐significant (e.g. Precursor or Near‐Miss) events.
examine the common characteristics and causes of many previous events (Serious, Precursor, or Near‐Miss).
105
RCA Methods
SingleInappropriate Acts
Work EnvironmentIssues
No Work EnvironmentIssues
Barrier Analysis
Direct Derivation
MRI? CT?X-ray?
Single Event
MultipleInappropriate Acts
Inappropriate ActsObscure
Issues
Events & CausalFactors Analysis
Change Analysis
E t R l t d i
Stream AnalysisCausal FactorsKnown
Multiple Events
Events Related inNature (any # cases)
Events Different inNature (>25 cases)
Common Cause Analysis
Some Causal FactorsKnown
Density Chart Analysis
106

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 54
RCA Analyst TeamIndividuals who carry out detail work of RCA process.
Can be under the guidance of a team leader / coordinator (who has experience in performing root
cause investigations)
Team Leader / Coordinator Responsibilities
RCA Team Sponsor
RCA Analyst Team Leader / Coordinator Responsibilities• Coordinates investigation efforts• Facilitates the RCA process• Maintains RCA investigation documents • Provides status reports to the RCA Project Sponsor
regarding investigation and any problems
RCA Analysts • Individuals of diverse backgrounds and experiences
Leader / Coordinator
Stakeholders & Subject Matter
RCA Analysts
• Include at least 1 subject matter expert if not part of overall project team
• Keep group as small as possible, yet sized appropriately for the scope of the investigationPeople Involved
in the Event
Experts
107
RCA Executive SponsorA senior leader who “owns” the quality of the
overall RCA outcomes ‐ to assure correct root cause and corrective actions to prevent recurrence.
RCA Team Sponsor
RCA Analyst Responsibilities
• Acts to stabilize the situation
• Charters the RCA Team
• Meets with RCA Team to discuss and agree on investigation scope and objectives
• Establishes priority and allocates resources
• Communicates investigation status
RCA Analyst Leader/Coordinator
Stakeholders & Subject Matter
RCA Analysts
• Ultimately responsible for the root solution and implementation of corrective actions
• Addresses any issues team has with finalizing project
• Provides reports to hospital committees and other reporting groups
People Involvedin the Event
Subject Matter Experts
108

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 55
Team Charter• A clear, careful, and specific problem
statement created by team sponsor for RCA Team members
• Charter should indicate:• Charter should indicate:
– Members of the team
– Subject experts to be involved
– Leadership to be involved
– Timeframe for project to be completed
– Expectations regarding updates on project statusproject status
– Other related issues from previous events to incorporate into analysis
109
RCA Three Meeting ModelOperations Owns – Quality/Risk/Safety Facilitates
Facts Meeting• Review Charter
RCA Executive Sponsor, Operational Leader & Subject Matter Experts
• Stabilize RecommendationCauses Meeting
Investigate Determine failure E t bli h t
• Review Charter• Confirm scope of
investigation• Identify & coordinate
interviews & data gathering
RCA Analyst Team
• Stabilize situation
• Control evidence
Analysts meet as
Meeting• Consensus on root
causes • Finalize Corrective
Action plan
• Agree on facts & proximate causes
• Build consensus for possible root causes
goccurrence to determine sequence of events and potential causes
scenario including individual and system failures for each inappropriate act
Establish root causes and conceptualize corrective actions
Analysts meet as often as necessary to complete work
110

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 56
BESTPRACTICE
Rapid Response to Potential Safety Event
•24 to 48 hours post discovery•15-30 minute meeting•Update on known facts•Immediate risk mitigationg•Assignment of resources/plan for next steps
Benefits:•Everyone on the same page
•Insures that patient/family/staff needs are p yaddressed (as well as other immediate risk
mitigation issues)•Establishes facts (not rumors)
•Sets the tone for action and ownership
111
A “Bad Thing” has happened…
Roles and Responsibilities
Leader, physicians, and staff in department or
Risk and/or Quality Management
Executive Owner
A “Bad Thing” is presumed to be a Serious Safety Event until proven otherwise.
staff in department or area where event
occurred
Management
• Stabilize the situation; provide treatment, care, or assistance to the patient, family, and staff
• Notify Risk
• Assist department leader with stabilization and immediate risk mitigation
• Select/notify executive
• Assist department leader if needed
• Call/conduct Code E meeting
Notify Risk Management
• Notify next level leader
Select/notify executive owner and prep for Code E meeting
112

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 57
Events & Causal Factors Charting
Root CauseIdentification of system
failures
PrimaryEvent Line
Consequence
Causal Factors(Failure Mechanisms)
Inappropriate Act
Descriptor
Identification of individual failures
Descriptor
113
Opportunity for structured communication:Post-event there may be the opportunity to issue a Safety Alert if there is a specific, immediate tactical opportunity to prevent possible re-occurrence. (Using SBAR to format the alert is a great best practice.)
114

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 58
Human Error ‐ Proven Corrective Actions
Skill‐Based Errors• Reduce time pressure• Simplify tasks• Red ce distractions • Reduce distractions• Alert mental state• Awareness aids• Experience
Rule-Based Errors Validation and verification (V&V)
Knowledge-Based Errors Problem-solving skills Work specialization
Validation and verification (V&V) Work specialization Training on fundamentals
Training on work processes Training on fundamentals Improve communication
115
Effectiveness of Error Prevention Strategies
1. Design process for minimum error – “mistake‐proof” it.
2 Control errors with active safety devices
Most Effective
2. Control errors with active safety devices.
3. Provide warning devices for manual action.
4. Use procedures for reduction of error and control.
5. Use administrative controls for reduction of error.
6. Rely on knowledge and skill of staff.
Least Effective
116

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 59
Leading Causes of Action Failure Hidden non‐commitment
(there seems to be agreement, but managers later back out)
Soft cost – benefit analysis
We have met the enemy
and he is us Soft cost benefit analysis(the best root solution is always the cost effective solution)
Resistance from constituency groups(Involve early in the process and rely on tactful diplomacy)
Poor implementation accountability(Corrective Action Plan should have responsible parties
and he is us…
(Corrective Action Plan should have responsible parties by name and date)
From Maximize Patient Safety with Advanced Root Cause Analysis; Corbett, Clapper, & Johnson; 2004.
117
Resources and Contact InformationFor more information on Patient Safety Organizations:
http://www.pso.ahrq.gov/index.html• Terrie Van Buren, Sr. Director, Patient Safety Officer:
– Terrie [email protected]_ @– (615)465‐7518
• Gerard Kalbfell, Director Patient Safety– [email protected]– (615)465‐7323
• Giselle Krieger, Director Patient Safety– [email protected]– (615)465‐2724
D Sh h d K Vi P id t Q lit d Cli i l T f ti• Dr. Shaheed Koury, Vice President Quality and Clinical Transformation– [email protected]
– (615)428‐6695
118

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 60
Thank you for all you do toThank you for all you do to keep our patients and staff
safe!119
U d t C tU d t C t PhPhUpdate on Current Update on Current Pharmacy Pharmacy Initiatives and StrategiesInitiatives and Strategies
121
Robert Fink, Pharm.D., M.B.A., FASHP, FACHE, BCNSP, BCPS
Chief Pharmacy Executive
Community Health Systems

System Elements of a Medication Error Reduction Program: What Every Pharmacist Needs to KnowCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 61
122