augusto b. federici - islhislh.org/presentation_upload/presentation_uploads/11_35_1400... ·...
TRANSCRIPT

International Society Laboratory Hematology Milan, 12-14 May 2016
Current and Emerging Approaches for Assessingvon Willebrand disease (VWD) in 2016
Augusto B. FEDERICI
Hematology and Transfusion Medicine Luigi Sacco University Hospital, University of Milan

Employment NONE
Research support NONE
Scientific advisory board BAXALTA, CSL-BEHRING, GRIFOLS, KEDRION-LFB, OCTAPHARMA, WERFEN-IL
Consultancy NONE
Speakers bureau BAXALTA, CSL-BEHRING, GRIFOLS, KEDRION-LFB, OCTAPHARMA, WERFEN-IL
Major stockholder NONE
Patents NONE
Honoraria BAXALTA, CSL-BEHRING, GRIFOLS, KEDRION-LFB, OCTAPHARMA, WERFEN-IL
Travel support NONE
Other NONE
DisclosuresA.B. Federici

February 1926E.A. von
WILLEBRAND
1959Nilsson IM et al,
Acta Med Scand; 164:263-
78
1971Zimmerman
TS et al, JCI; 50:244-
54
History of VWD

VWD is the most common inherited bleedingdisorder and is due to quantitative (VWD3 &VWD1) and/or qualitative (VWD2A, VWD2B,VWD2M, VWD2N) defects of VWF: in severe formsof VWD3, VWD1 & VWD2N FVIII is also reduced
Despite the complex and heterogeneous nature ofthe VWF defects, nowadays all VWD types can bemanaged efficiently in most patients.
VWD: Clinical and Lab DiagnosisBackground 2016 (1)

CPlatelet plug formation
BDamaged vessel wall
torque
initialplatelettethering
plateletactivationand adhesion
plateletrolling
activatedaIIbb3
extracellularmatrix
collagenfibrils
A Intact vessel wall
matrixVWF
endothelialcell
platelet
plasmaVWF
GpIba
NonactivatedaIIbb3
How Does VWF Work

• Correct VWD diagnosis and classification cannotbe always available in several Centers to providethe best therapeutic approach.
• Differently from HA easily classified (severe,moderate, mild) by baseline FVIII levels, clinicalseverity of different VWD forms is not welldefined within types so far.
VWD: Clinical and Lab DiagnosisBackground 2016 (2)
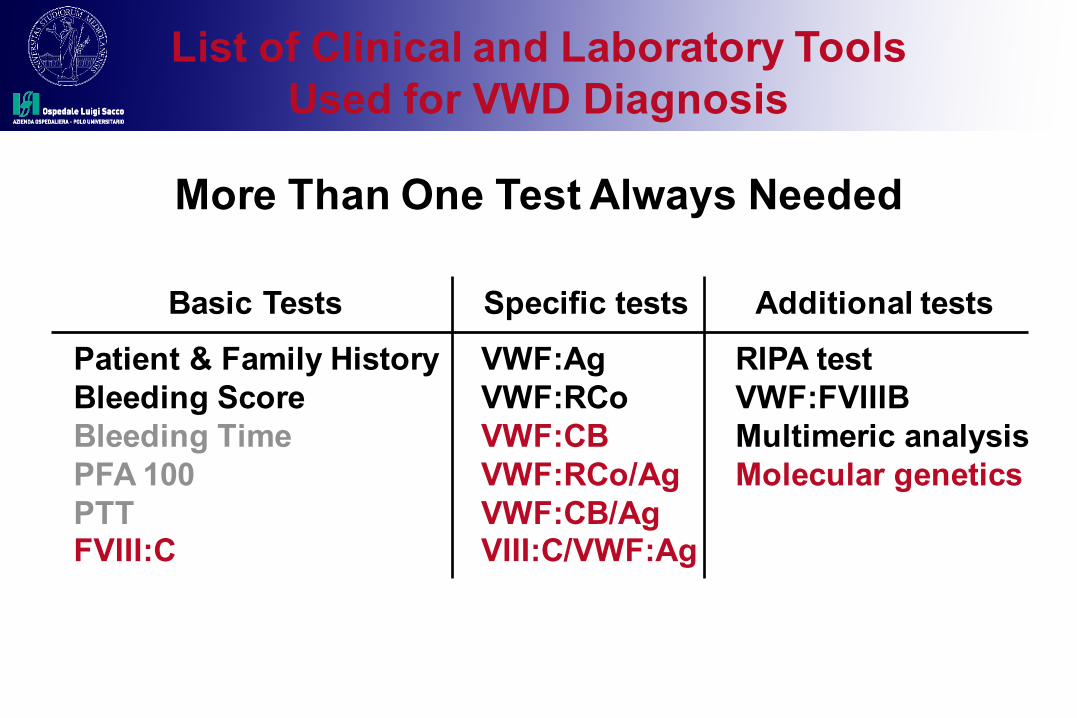
List of Clinical and Laboratory ToolsUsed for VWD Diagnosis
Basic Tests Patient & Family HistoryBleeding ScoreBleeding TimePFA 100PTTFVIII:C
Specific tests VWF:AgVWF:RCoVWF:CBVWF:RCo/AgVWF:CB/AgVIII:C/VWF:Ag
Additional tests RIPA testVWF:FVIIIBMultimeric analysisMolecular genetics
More Than One Test Always Needed
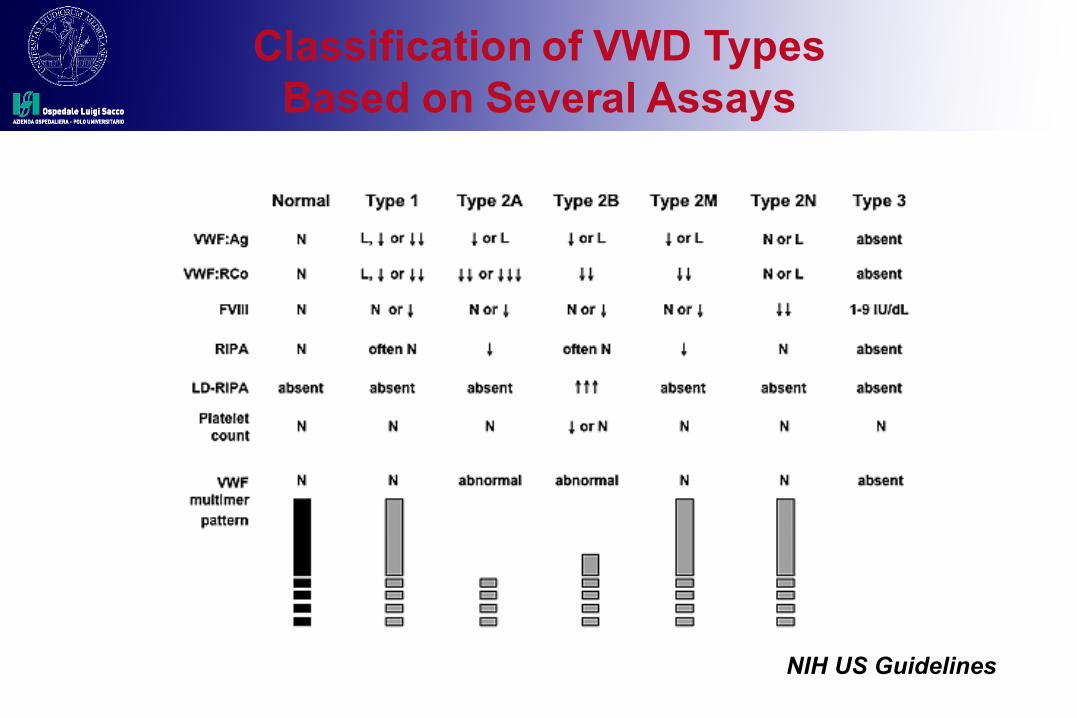
Classification of VWD TypesBased on Several Assays
NIH US Guidelines

Heterogeneity of VWD PatientsBased on Cohort Studies
VWF:RCo <10 U/dL+ FVIII:C < 20 U/dL
VWF:RCo 10-30 U/dL+ FVIII:C 20-40 U/dL
VWF:RCo 30-50 U/dL+ FVIII:C 40-70 U/dL
VWD Severe Forms:VWD1, VWD2A, VWD3
VWD Moderate FormsVWD1, VWD2B, VWD2M, VWD2N
Bleeders: VWD1 Mild FormsNon bleeders:
Low Levels of VWF
Diagnosed VWD: the tip of the iceberg?
Federici AB et al, Blood 2014; 123: 4037-44.
Heterogeneous VWD Cohort:Italian Registries (RENAWI)
Bleeders versus Non Bleeders

Criteria for Correct Diagnosis(Bleeding History, Low VWF Activity, Inheritance)
Tosetto et al JTH 2006
PlateletGPIba
A1
C C C CA2
SubEndothelium Collagen I and III
Collagen VIHeparinSulphatide
VWF:RCo
VWF:CBA3
ADAMTS 13
W
W
WI:1
III:3 W
I
II
III

Clinical and Lab Diagnosis of VWDOutlines
• Definitions and classification of VWD• Clinical parameters for VWD• First-level laboratory tests• Second-level laboratory tests• Additional and automatic assays • Severe or mild VWD types: outcomes

VWF:RCo(Platelet Aggregometric Method)
Normal Fixed Platelets + Patient Plasma Dilutions + Ristocetin [1 mg/mL]
Multimeric Pattern (2A & 2B)Mutations in the A1 Domain (2M)
Parameters That Influence the VWF:RCo
VWF:Ag

Normal VWD 2A VWD 2B
1 min. 1 min.1 min.
Transmission
Ristocetinmg/ml
VWF:RIPA(Ristocetin Induced Platelets Agglutination)
Platelet Rich Plasma from Patients + RISTOCETIN [0.2-2.0 mg/ml]Ruggeri ZM et al, JCI 1978

VWF Multimeric Analyses(Kindly Provided by U. Budde)

VWF:FVIIIB(Binding Assay - ELISA)
0
750
1500
VWF Immobilized
Bou
ndFV
III:C
Homozygous R854Q
Heterozygous R854Q
Normal
0 750 1500

VWF Pro-PeptideUsefulness of this assay
The assay for VWF pro-peptide measures incirculation the amount of protein cleaved fromPRE-PRO-VWF synthesized in Endothelial Cells
Increased VWF:pp/VWF:Ag ratio identifies thosepatients with shortened VWF survival
Shortened VWF survival can also be observedduring the infusion trial with DDAVP

Ruggeri et al, Blood 1982 Federici AB et al, Blood 2004; 103: 2032-2038
DDAVP Challenge Test: An important assessment at diagnosis

Clinical and Lab Diagnosis of VWDOutlines
• Definitions and classification of VWD• Clinical parameters for VWD• First-level laboratory tests• Second-level laboratory tests• Additional and automatic assays • Severe or mild VWD types: outcomes

VWF:CB(Collagen Binding Activity)
• Evaluates VWF capability to bind to collagen- Mimics VWF interaction with sub-endothelial collagen
matrix at site of vascular injury
• Dependent on VWF multimeric size- Collagen binds more readily with HMWM- Studies show VWF:CB can serve as a surrogate measure
for presence of HMWM
• When tested with VWF:Ag and VWF:RCo can improve differentiation between VWD types 1, 2A, 2B and 2M
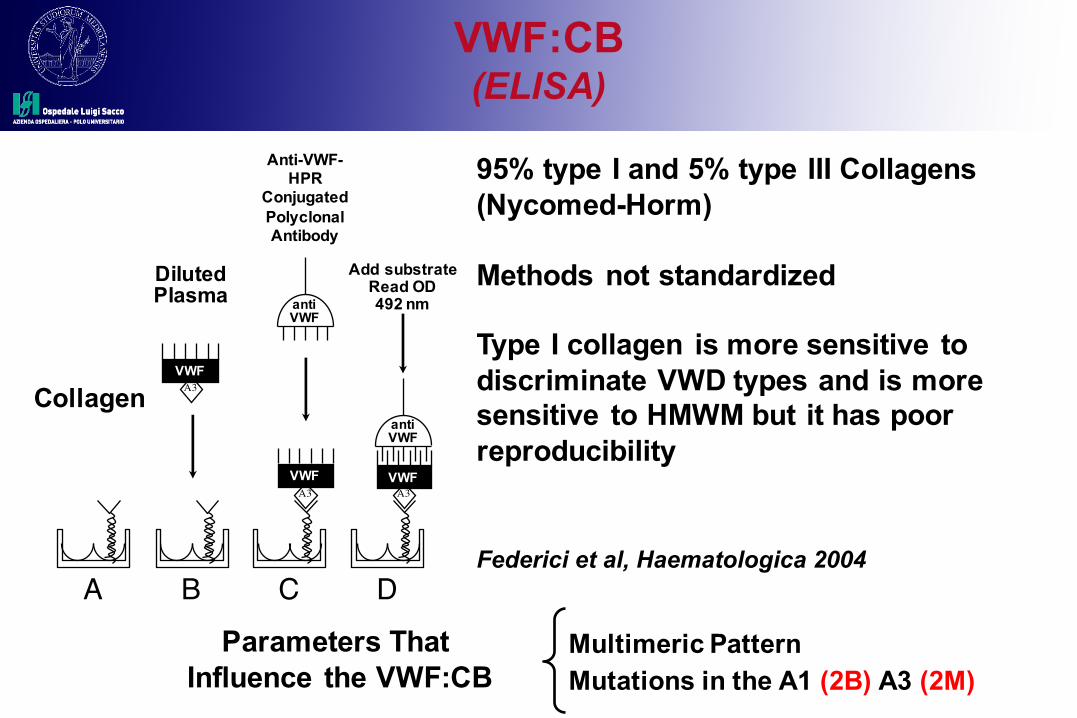
VWF:CB(ELISA)
B C D
Add substrateRead OD492 nm
DilutedPlasma
A
Collagen
Anti-VWF-HPR
ConjugatedPolyclonal Antibody
A3VWF
A3VWF
antiVWF
A3VWF
antiVWF
95% type I and 5% type III Collagens (Nycomed-Horm)
Methods not standardized
Type I collagen is more sensitive to discriminate VWD types and is more sensitive to HMWM but it has poor reproducibility
Federici et al, Haematologica 2004
Multimeric PatternMutations in the A1 (2B) A3 (2M)
Parameters That Influence the VWF:CB

Platelet Dependent-VWF Activity(Nomenclature and Methodology)
Bodó et al on behalf of ISTH-SSC-SC on VWF JTH 2014

VWF:RCo(Recent Automated Methods)
Immunoturbidimetric ChemiluminescenceHemosIL VWF:RCo Assay HemosIL AcuStar VWF:RCo Assay
Reaction MechanismLatex particles coated with arecombinant fragment of plateletgp1b, through a monoclonalantibody, which binds VWF in thepresence of ristocetin resulting inagglutination.
Reaction MechanismLatex particles coated with arecombinant fragment of plateletgp1b, through a monoclonalantibody, which binds VWF in thepresence of ristocetin resulting inagglutination.

Gain-of-Function Mutant GPIb-Binding (VWF:GPIbM) Assays
Bodó et al on behalf of ISTH-SSC-SC on VWF JTH 2014
*NotavailableforsaleintheUS.

Flow chart for VWD DiagnosisUsed in Italian Registry

Clinical and Lab Diagnosis of VWDOutlines
• Definitions and classification of VWD• Clinical parameters for VWD• First-level laboratory tests• Second-level laboratory tests• Additional and automatic assays • Severe or mild VWD types: outcomes

Aims of the RENAWI-2
To evaluate the incidence, types and severity of spontaneous bleeding episodes requiring DDAVP and/or VWF concentrates in a large cohort of VWD patients
To characterize bleeding phenotype in different VWD types and to predict clinical outcome in these patients.

Bleeding Phenotype in VWDEvidence-Based Methods
Federici AB et al, Blood 2014; 123: 4037-4044
Restricted Cubic Spline Curve Cox’s Proportional Hazard Model

Bleeding Phenotype in VWD typesType of Bleeding Symptoms
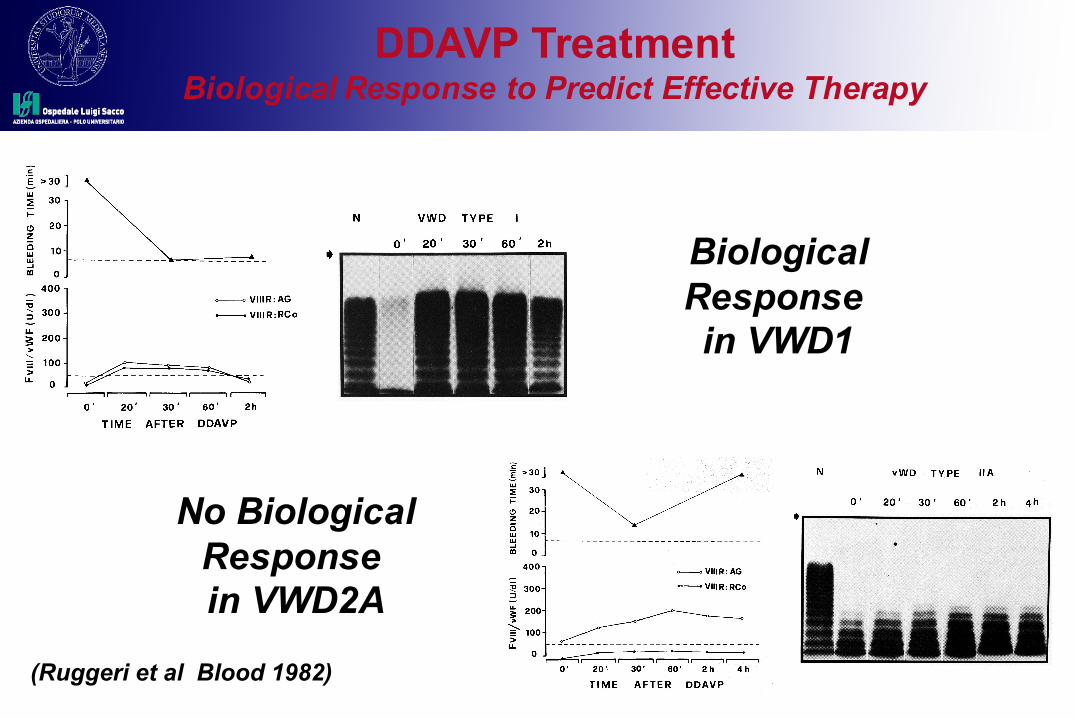
BiologicalResponse in VWD1
No BiologicalResponse in VWD2A
(Ruggeri et al Blood 1982)
DDAVP TreatmentBiological Response to Predict Effective Therapy

Clinical Use of DDAVP According to Clinical Phenotype (BS) of VWD
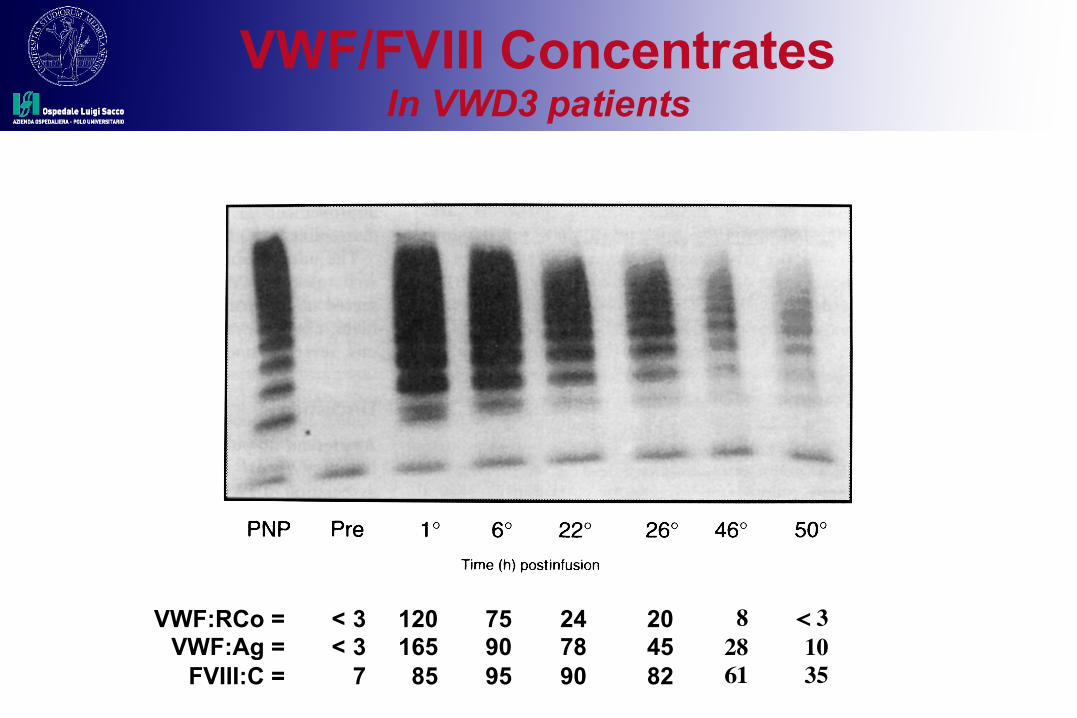
VWF/FVIII ConcentratesIn VWD3 patients
< 31035
82861
204582
247890
759095
12016585
< 3< 3
7
VWF:RCo =VWF:Ag =
FVIII:C =

Clinical Use of VWF/FVIII Concentrates According to Clinical Phenotype (BS) of VWD

Conclusions of RENAWI-2
The bleeding score (BS) correlates with VWF levels in VWD and helps to predict clinical
outcomes in adult patients with VWD.

Clinical and Lab Diagnosis of VWD Current Perspectives in 2016
• BS and of specific tests for VWF activities should be always used together in Adults to identify VWD patients with bleeding phenotype
• More specific and automatic lab tests should be available in most laboratory world-wide for a rapidVWD diagnosis of bleeding individuals
VWD: Clinical and Lab DiagnosisACKNOWLEDGEMENTS
AB BONOMI Hemophilia Thrombosis Center (Milan):P. BUCCIARELLI, P.M. MANNUCCI, F. PEYVANDI
R. BADER, L. BARONCIANI, M.T. CANCIANI and VWD LAB
Italian Association of Hemophilia Centers (AICE):G. CASTAMAN, M.G. MAZZUCCONI, M. MORFINI,
A. ROCINO, F. RODEGHIERO, M. SCHIAVONI