aum sri sai ram pranams at the lotus feet of our b eloved bhagavan
Post on 21-Dec-2015
213 views
TRANSCRIPT

Aum Sri Sai Ram
Pranams at the Lotus Feet ofPranams at the Lotus Feet ofOur Our BBeloved Bhagavaneloved Bhagavan
Grama Seva is
Rama Seva
GRAMA SEVA
• Villages have been the life line of our Country protecting our Ancient and Noble Culture, Heritage, Traditions and Values.
• More than 75% of our population lives in Villages. • Even after 60 years of Independence our villages are still
crippled with several problems like Illiteracy, Illness, Ignorance, Social Evils, Poverty, Unemployment, Scarce Drinking Water, Shelter, Roads and other amenities.
• Its our collective responsibility to address these problems and work for betterment of our villages.
• Bhagavan has been continuously guiding and directing us to focus our service activities towards this objective of Improving life in Villages.
Bhagavan’s Upadesh on Grama Seva
•Bhagavan in all His mercy has given us Divine Guidelines on the ‘how’ of Grama Seva.
•Over the years He has indicated many aspects to be carefully followed while doing Grama Seva.
In His Ugadi message of 2007, Swami highlighted the importance of the FAMILY as the Basic Unit of Society, whether in the Village, Town or City.He instructed us to concentrate on the FAMILY in our Grama Seva Activity.
Swami’s Focus
Goals of Grama Seva
• Villages during Grama Seva should be viewed from both the Micro level and the Macro level.
• The activities undertaken should be on a Sustained Basis.
• Service Activities should be planned for Comprehensive Integrated Development.
Villages in India
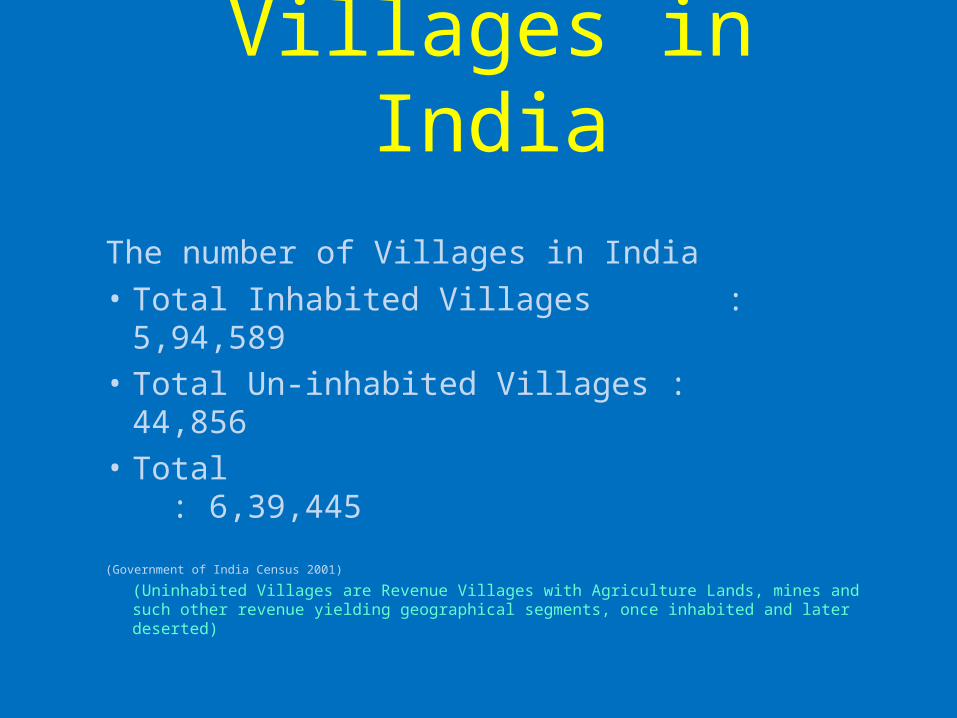
The number of Villages in India
• Total Inhabited Villages : 5,94,589
• Total Un-inhabited Villages : 44,856
• Total : 6,39,445
(Government of India Census 2001)
(Uninhabited Villages are Revenue Villages with Agriculture Lands, mines and such other revenue yielding geographical segments, once inhabited and later deserted)
Population Distribution in Villages
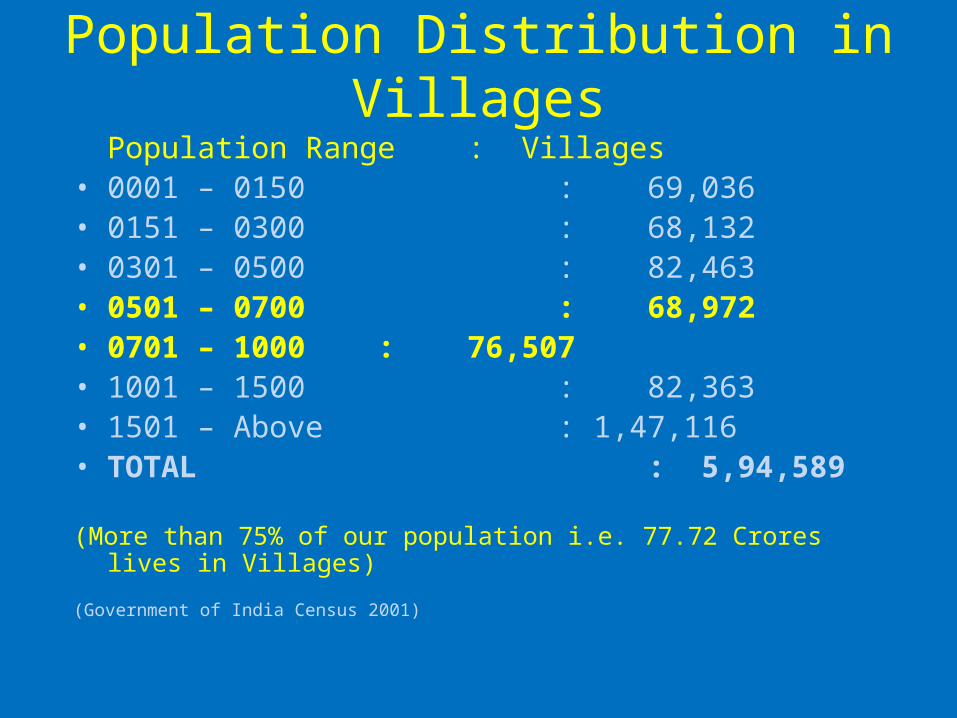
Population Range : Villages• 0001 – 0150 : 69,036• 0151 – 0300 : 68,132• 0301 – 0500 : 82,463• 0501 – 0700 : 68,972• 0701 – 1000 : 76,507• 1001 – 1500 : 82,363• 1501 – Above : 1,47,116• TOTAL : 5,94,589
(More than 75% of our population i.e. 77.72 Crores lives in Villages)
(Government of India Census 2001)
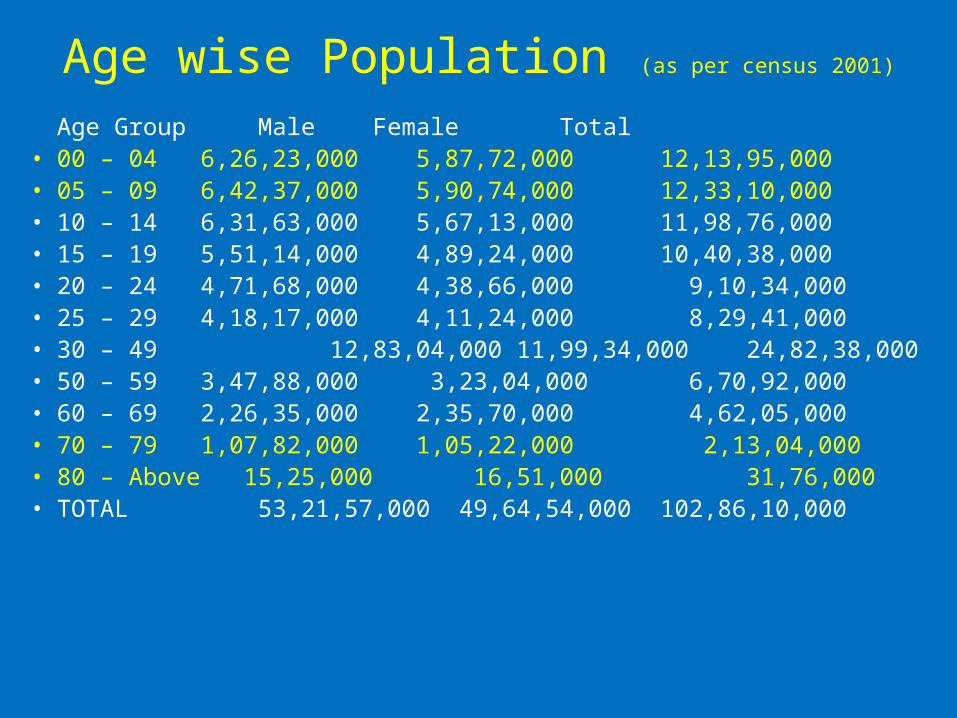
Age wise Population (as per census 2001) Age Group Male Female Total
• 00 – 04 6,26,23,000 5,87,72,000 12,13,95,000• 05 – 09 6,42,37,000 5,90,74,000 12,33,10,000• 10 – 14 6,31,63,000 5,67,13,000 11,98,76,000• 15 – 19 5,51,14,000 4,89,24,000 10,40,38,000• 20 – 24 4,71,68,000 4,38,66,000 9,10,34,000• 25 – 29 4,18,17,000 4,11,24,000 8,29,41,000• 30 – 49 12,83,04,000 11,99,34,000 24,82,38,000• 50 – 59 3,47,88,000 3,23,04,000 6,70,92,000• 60 – 69 2,26,35,000 2,35,70,000 4,62,05,000• 70 – 79 1,07,82,000 1,05,22,000 2,13,04,000• 80 – Above 15,25,000 16,51,000 31,76,000• TOTAL 53,21,57,000 49,64,54,000
102,86,10,000
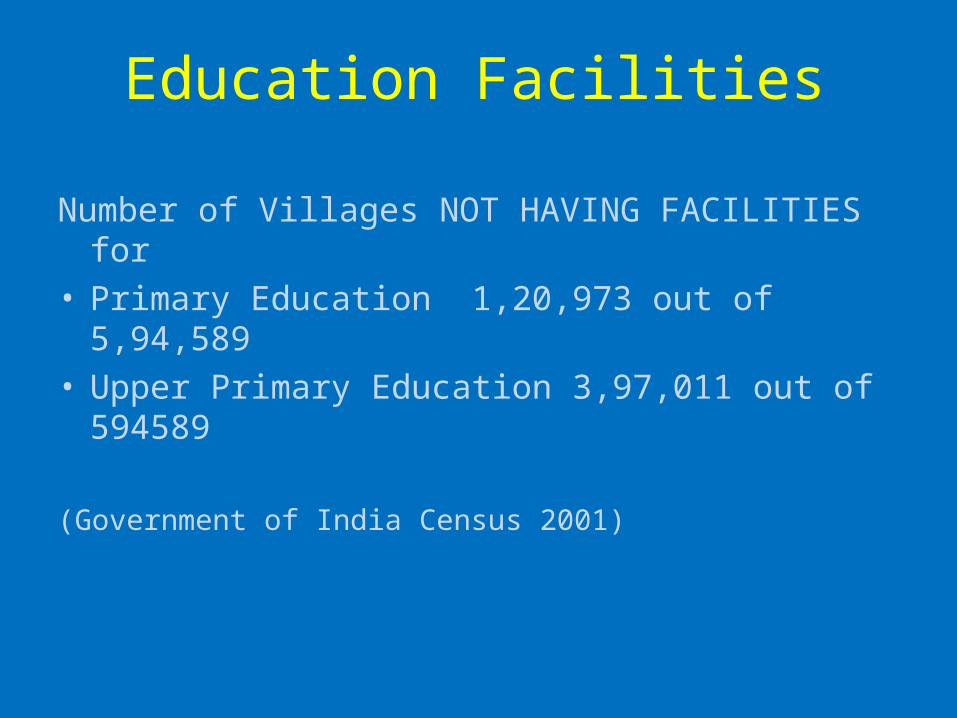
Education Facilities
Number of Villages NOT HAVING FACILITIES for• Primary Education 1,20,973 out of 5,94,589• Upper Primary Education 3,97,011 out of
594589
(Government of India Census 2001)
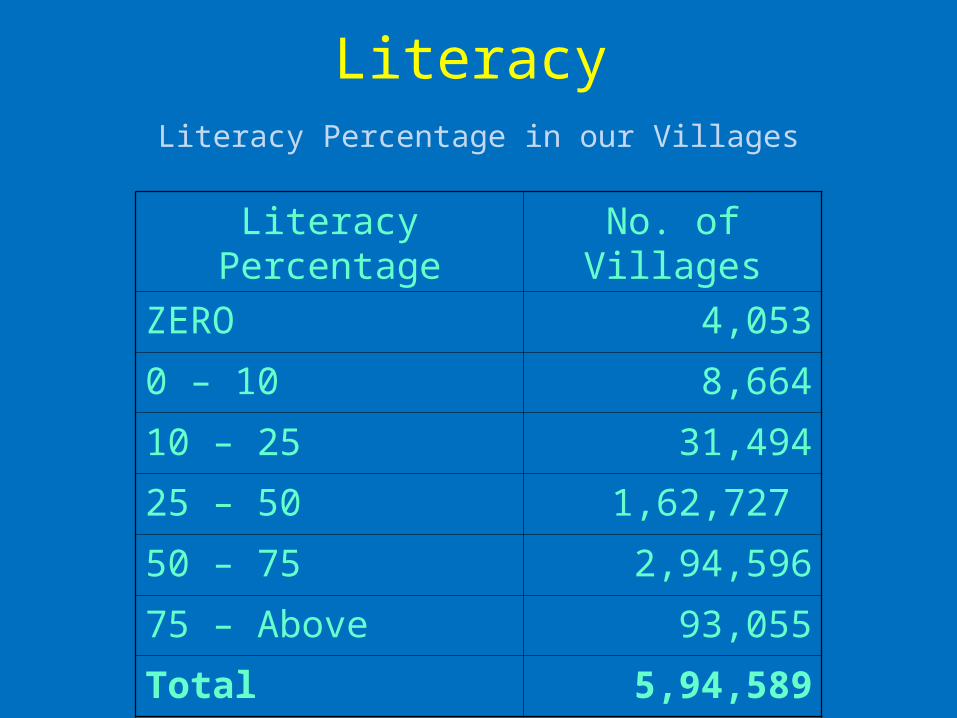
LiteracyLiteracy Percentage in our Villages
Literacy Percentage No. of Villages
ZERO 4,053
0 – 10 8,664
10 – 25 31,494
25 – 50 1,62,727
50 – 75 2,94,596
75 – Above 93,055
Total 5,94,589
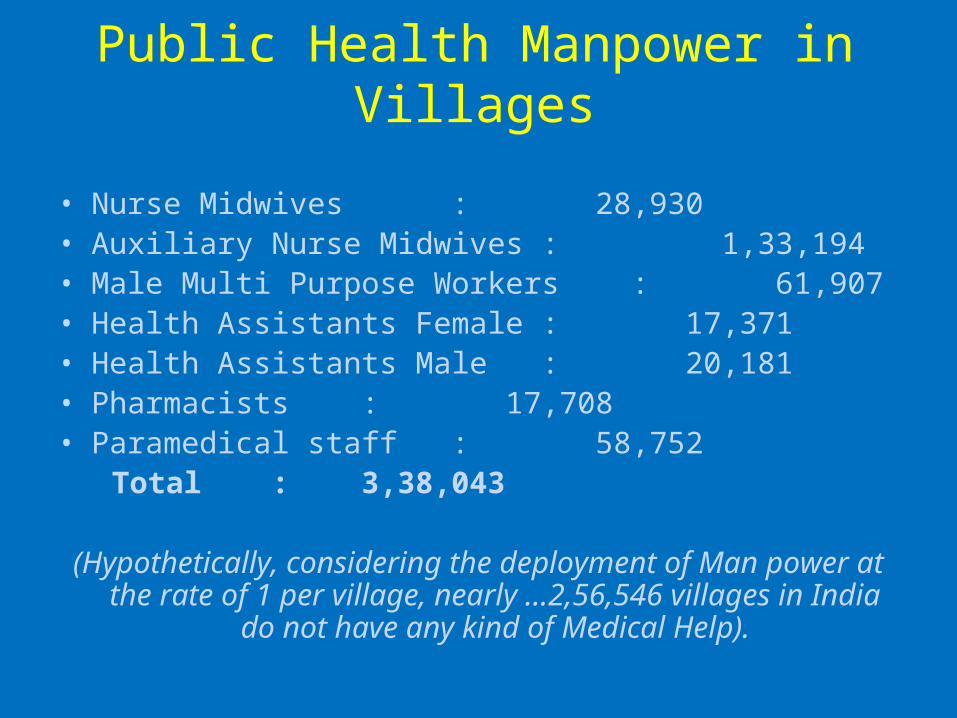
Public Health Manpower in Villages
• Nurse Midwives : 28,930 • Auxiliary Nurse Midwives : 1,33,194• Male Multi Purpose Workers : 61,907• Health Assistants Female : 17,371• Health Assistants Male : 20,181• Pharmacists : 17,708• Paramedical staff : 58,752 Total : 3,38,043
(Hypothetically, considering the deployment of Man power at the rate of 1 per village, nearly …2,56,546 villages in
India do not have any kind of Medical Help).

Public Health Infrastructure in Villages
• Sub Health Centres : 1,46,026• Public Health Centres : 23,236• Community Health Centres : 3,346
Shortage declared by the Ministry Of Health is SHCs :19,209 PHCs : 4,337 CHCs : 3206
Per every 4500 -5000 population there should be One SHC, per 30,000 population One PHC and One CHC in a centrally located and easily accessible Town per population of 1,20,000.
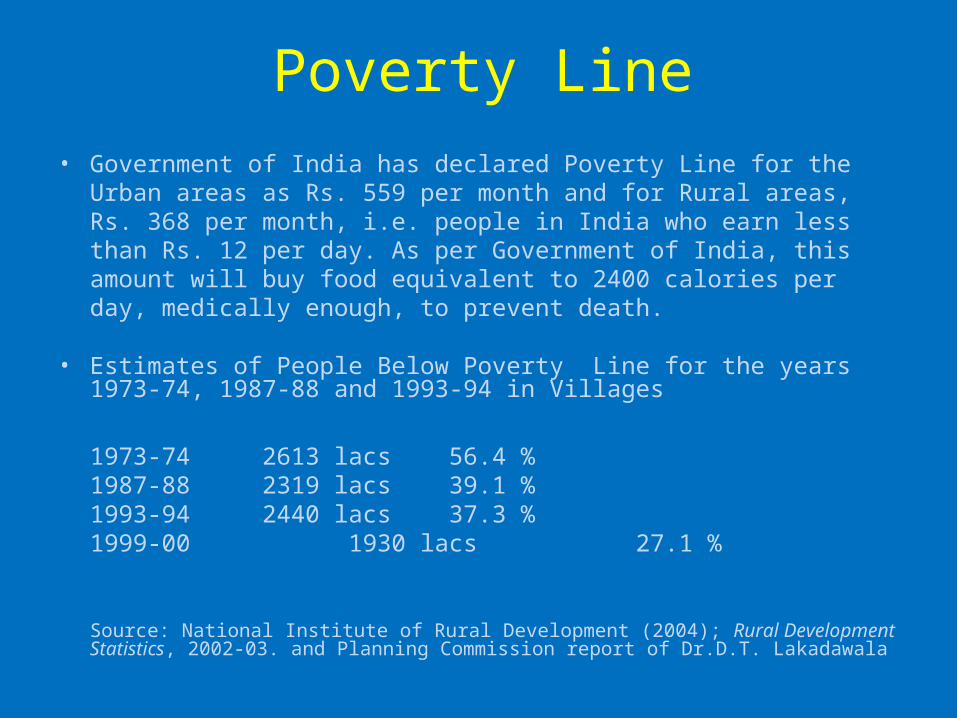
Poverty Line• Government of India has declared Poverty Line for the Urban areas
as Rs. 559 per month and for Rural areas, Rs. 368 per month, i.e. people in India who earn less than Rs. 12 per day. As per Government of India, this amount will buy food equivalent to 2400 calories per day, medically enough, to prevent death.
• Estimates of People Below Poverty Line for the years 1973-74, 1987-88 and 1993-94 in Villages
1973-74 2613 lacs 56.4 %1987-88 2319 lacs 39.1 %1993-94 2440 lacs 37.3 %1999-00 1930 lacs 27.1 %
Source: National Institute of Rural Development (2004); Rural Development Statistics, 2002-03. and Planning Commission report of Dr.D.T. Lakadawala
Drinking Water
• About 44 million are estimated to be affected by problems related to water quality with excess of Fluoride, Iron, Nitrate, Arsenic, Heavy Metals and Salinity.(Shiva et al, 2002: 3)
• 32% of Villages do not have Drinking Water at all

Percentage of Households with the Principal Source of Drinking Water and the Sanitation Facility in Major States in India: 1998
Sl.No
State Drinking water source No Latrine
Used
Rural Urban Rural Urban
TapTubewell/Handpump
Tap
Tubewell/Handpump
1Andhra Pradesh 26.2 46.9
75.1 12.8 88.5 30.8
2 Assam 7.3 49.542.2 38.4 24.7 2
3 Bihar 0.7 70.335.3 43.1 89.4 45.3
4 Gujarat 46.6 31.791.1 7.3 79.9 21.1
5 Haryana 31.1 49.980.5 19.4 84.5 32.9
6 Karnataka 26.6 53.980.9 11.2 88.9 30
7 Kerala 10.6 1.440.2 3.5 23.1 5.1
8Madhya Pradesh 5 52.2
76.1 13.1 94.5 45.2
9 Maharashtra 41.1 24.4 92 5.3 85.8 15.8
10 Orissa 2.9 53.238.7 32.3 96.1 35.8
11 Punjab 14.8 82.764.4 35.5 67.9 14.8
12 Rajasthan 19.2 36.285.4 10.4 87 25.5
13 Tamil Nadu 50 31.1 74 18.7 88.5 32.5
14 Uttar Pradesh 8.8 63.543.2 53.2 90.6 28.2
15 West Bengal 4.1 75.6 56 38.2 76.1 15.2
India 18.7 50.170.1 21.3 82.5 25.5
Note: These 15 major states account for about 90% of the population of India as per 2001 census. For the interstate analyses, these 15 major states are considered by most of the scholars. There are a total of 35 states and Union Territories in India. Source: NSSO (1999: 40, A-27 to A-39)
Village Infrastructure
• Census showed that there was a shortage of 137 lacs Houses and there were 103 lacs unserviceable kutcha houses, It means nearly 12 crores of population in villages have Shelter problem.
• Fifty-three per cent of Indian villages are still without any Roads.
• 82% of rural population do not use Latrines.• Nearly 50% of rural house holds do not have
Electricity.
* Source: Government of India, Press Information Bureau release no. 37
Problem ComplexIlliteracy IllnessMalnutrition PovertyUnemployment Migration to TownsPoor Sanitation Poor HygieneSafe Drinking Water Conventional Farming
MethodsLack of Medical Facilities Poor InfrastructurePoor Living Standards Natural CalamitiesSocial Evils Poor RoadsLack of Communication FacilitiesLoss of Ancient Culture, Heritage and ValuesLack of Alternative Earning / Additional Source of Incomeand Such other…
Bhagawan Baba has inspired the Sai Organisation and Sai Youth
to mitigate these problems

SRI SATHYA SAIVILLAGE INTEGRATED
PROGRAMME
Bhagavan Baba said that Our Grama Seva activity should be
focused on the Holistic Development of the Family and thereby of the Village, District and the State.
This will be called the Village Integrated
Programme

GRAMA SEVA AT PRESENT
VILLAGE
HOUSEHOUSE HOUSE
Partial Focus
Grama Seva at Present
• A Village is selected for rendering Seva after conducting a survey and interacting with the Panchayat President and other elders. The activities consist of Medical Camps, Veterinary Camps, Temple cleaning, Bhajan Centres, Balvikas etc.
• We also provide some village specific utility services like Bore Well, Overhead Tank, Roads, Sanitation etc.

Points of Emphasis in Grama Sevaat Present
• Focus is on the total Village - Medical Camps, Veterinary Camps, Bhajan Mandali, Balvikas etc. are done on this basis.
• Focus is not on the Family, its problems, needs (material and psychological) etc.
• No records of the family members are kept on a continuous basis.
• In many cases the activity is a one-shot affair and not on a sustained basis.
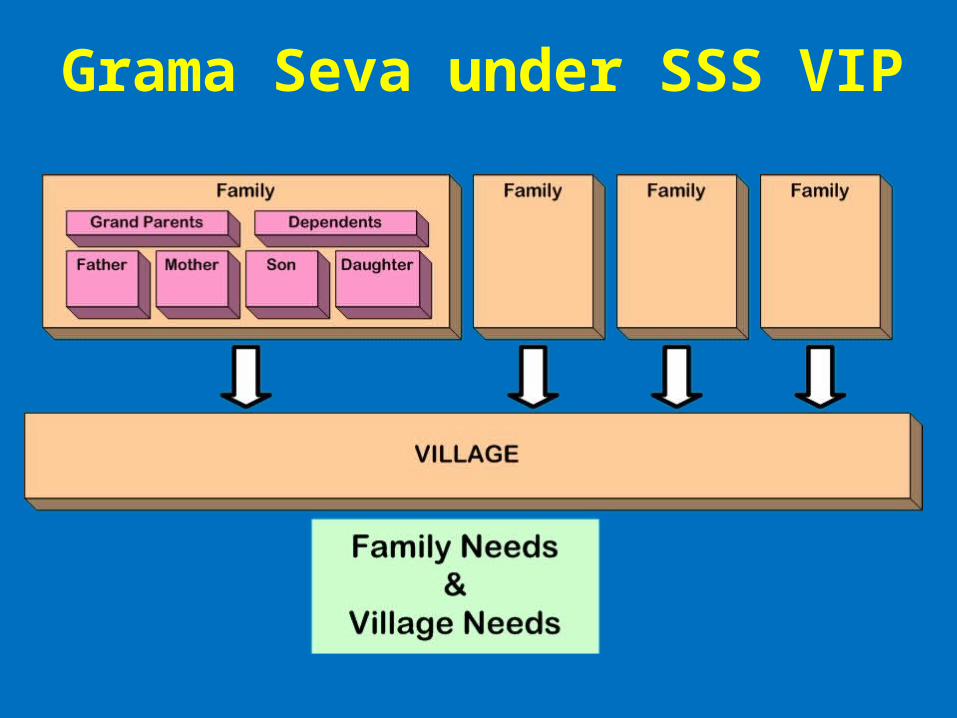
Grama Seva under SSS VIP

Grama Seva under SSS VIP
Bhagavan wants us to start from the Individual Family, each of its members and from there spread to the Village.
Bhagavan wants us to carefully think how we can serve every Family in a Holistic manner.
Our Seva should be primarily based on selfless Love and Shramadan to give them self-confidence and hope.
Our main focus is not on material support involving financial outlays.
Core issues to be tackled by SSS VIP
• Re-Structuring our Grama Seva Model.• Shift of Focus to Family.• Comprehensive Orientation on Village.• Need Identification and Prioritisation.• Integration of Services.• Resources Planning.• Manpower Sourcing and Training.• Activity Plan.• PERT (Progress Evaluation Review Technique)
where ever it is possible.
Approach
• Comprehensive Professional Survey.• Data Compilation and Computerisation.• Need Identification at Family and Village levels. • Priority Categorisation of Families.• Need Classification.• Planning Tailor-made Service Activities.• Resource Planning of 4 Ms (Man, Money
Material and Machines & Tools). • Scheduling, Phasing and Fixing Time Frame for
Activities. • Monitoring. • Progress Evaluation Review Technique (PERT).
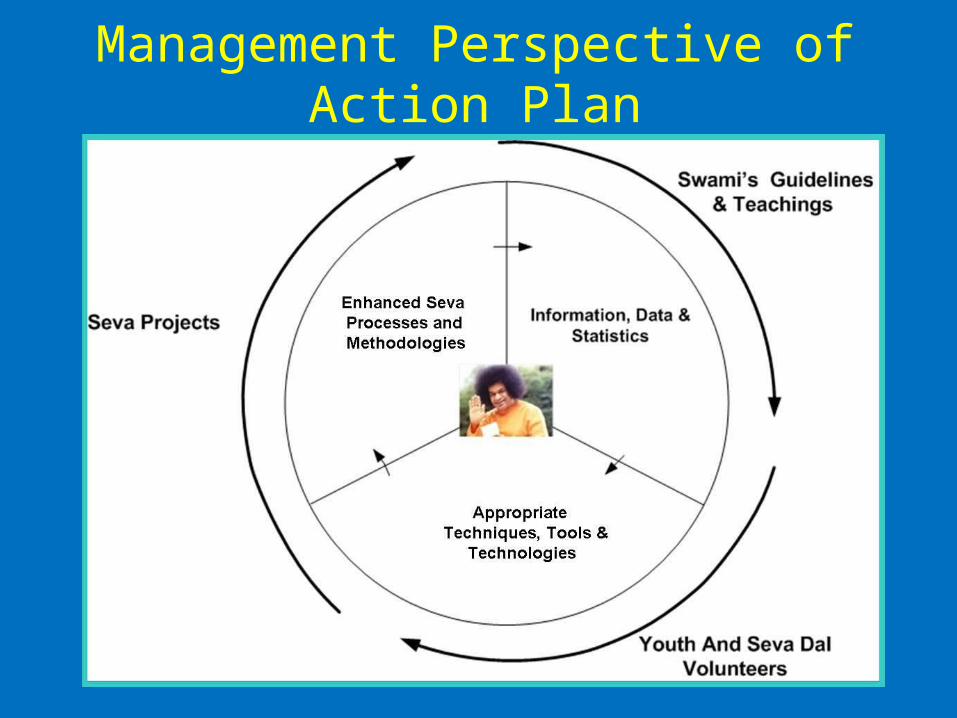
Management Perspective of Action Plan
FocusEducational Care Medical Care Social Care
At Family Level: Providing relief from illiteracy, illness and hunger by both proactive and reactive measures, inculcating Values and bring about family transformation through Love.
At Village Level: Providing community development activities, generation of employment, better income, better living conditions, better infrastructure and village transformation by inculcating values through Love and Service.

ACTION PLAN• Selection of the village• Primary Survey of village• Individual Data collection• Need Identification• Need Classification• Need Categorisation• Need Prioritisation• Activity Planning• 4 M’s Planning• Scheduling• Implementation• Monitoring• PERT
Selection of the Village• Houses: 100 to 150 Nos• Population : 500 to 1000 • Majority of the Families Below Poverty Line• Poor Hygiene and Sanitation• Children with lower Education, Education Dropouts and Child Labour• Presence of Social Evils – Alcohol, Smoking etc.• Poor Drinking Water Facility• Poor Medical Facility• Poor Transportation • Lack of Communication Facilities• Untrained and Unemployed Youth• Should be easily accessible from the main Samithi or Unit• Non- adoption of the village by any other Organisations• Village not covered by any Government Schemes

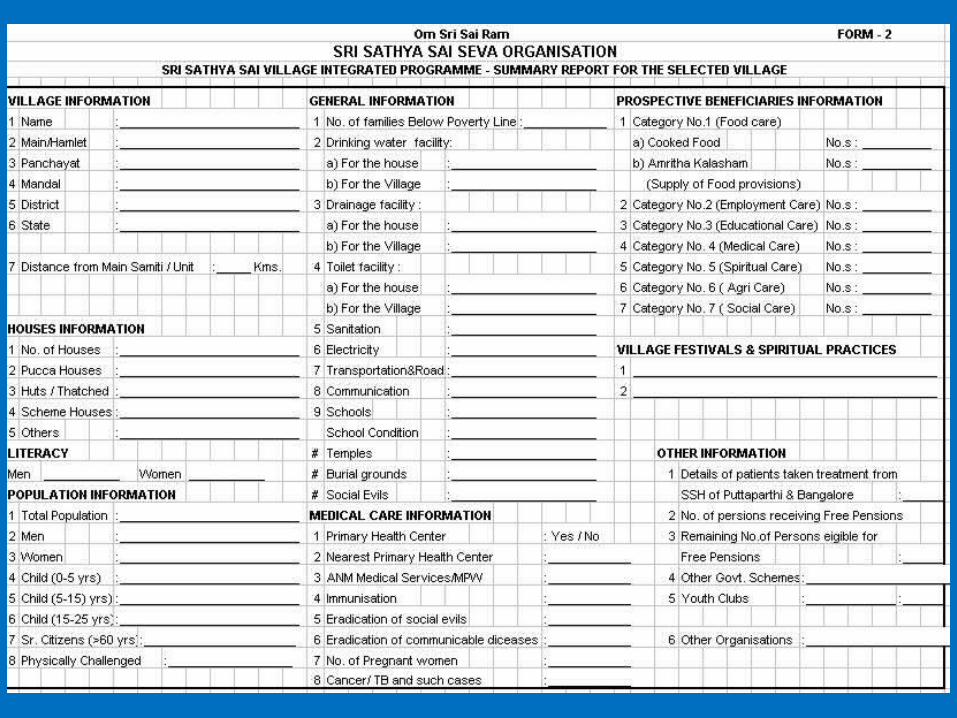
PRIMARY SURVEY• Collect the Village information from competent government office to Identify Suitable Village.• Data may be collected on number of Houses, Population, Gender Census, Academic, Health, Economy, Revenue, Agriculture, Other Sources of Revenue, Socio-Economic conditions, Religions, Faiths, Communities and Infrastructure Facilities. • Visit the village and confirm the data collected. • A Village Group may be constituted including women and youth to support and ensure participation of entire village in service activities.• Data may be collected on the Government Welfare Schemes and the Beneficiaries.• Data may be Computerised.
INDIVIDUAL DATA COLLECTION
• Data may be collected about each member in the
Family and about family as a whole.• Family’s Income, Education, Health, Wealth, Vocation,
Skills and other relevant information like the Benefits
from the Government Schemes may be collected,
verified and computerised.
Once the SSS V.I.P commenced, stay with them for 2-3
days to build confidence about our work and know about
their lifestyles, living standards, social responsibilities etc
very closely

Needs
• Needs will be Identified, Classified,
Categorised and Prioritised.
• Needs may be enlisted based on individual focus areas of Educational
Care, Medical Care and Social Care.
• Needs may be assessed on their worthiness with cost benefit ratio on both short term and long term basis.
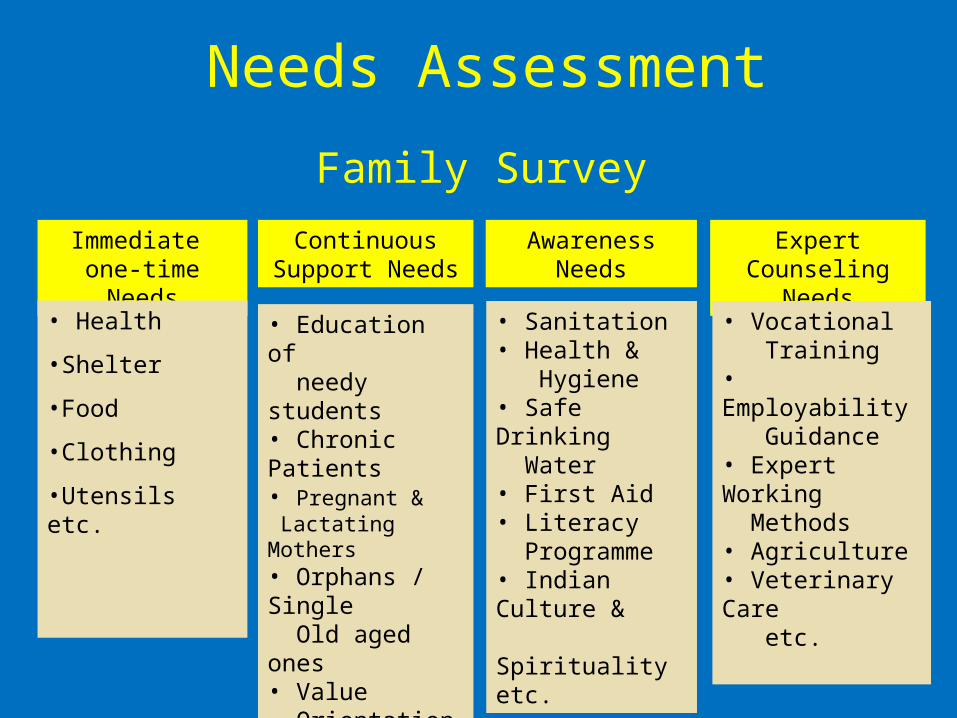
Needs Assessment
Family Survey
Immediate one-time Needs
Continuous Support Needs
Awareness Needs
Expert Counseling Needs
• Health
•Shelter
•Food
•Clothing
•Utensils etc.
• Education of needy students• Chronic Patients• Pregnant & Lactating Mothers• Orphans / Single Old aged ones • Value Orientation etc.
• Sanitation• Health & Hygiene• Safe Drinking Water• First Aid• Literacy Programme• Indian Culture & Spirituality etc.
• Vocational Training• Employability Guidance• Expert Working Methods• Agriculture• Veterinary Care etc.

Need Categorisation
• Category-1 Individual Care
• Category-2 Employment Care
• Category-3 Educational Care
• Category-4 Medical Care
• Category-5 Spiritual Care
• Category-6 Agri Care
• Category-7 Social Care
Family - Child Care
Age Group 0-10 years• Ensure Immunisation• Check for Malnutrition• Hygiene• Periodical Dental and Ophthalmic check-up• Induction into Balvikas • Conducting Competitions• Inculcating Values and Exposure to Indianness,
Tradition, Culture and Heritage• Academic Supplementation• Needs like Note books, crayons, bags etc
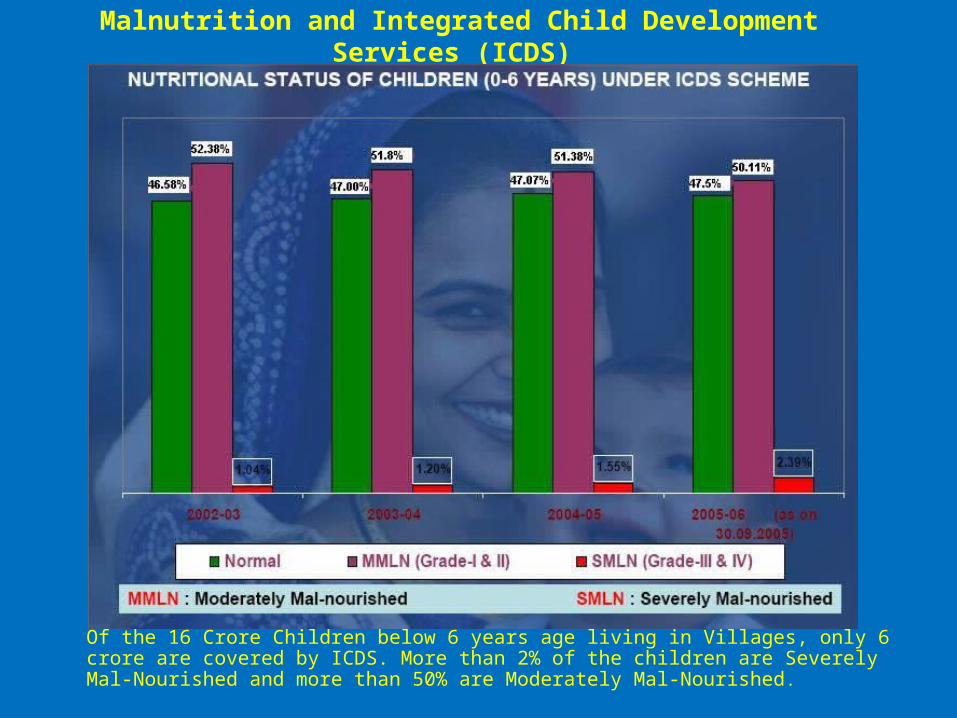
Malnutrition and Integrated Child Development Services (ICDS)
Of the 16 Crore Children below 6 years age living in Villages, only 6 crore are covered by ICDS. More than 2% of the children are Severely Mal-Nourished and more than 50% are Moderately Mal-Nourished.
Family - Child Care
Between 10 years and 15 years • Periodical Health Check-up• Identification of Malnutrition and Supplementation• Balvikas – Motivation• Promoting against Child-Labour• Motivating for Schooling, Eco Protection &
Cleanliness• Academic Support• Conducting Competitions in Essay, Elocution etc..• Skills, Talents Identification and encouragement• Encouraging Sports, Games and Arts• Promoting Values of Unity, Togetherness

Family – Youth Care• Academic Support• Counseling for Bad Habits and Social Evils• Motivating for Service• Training for Self Empowerment• Self Help Groups for Career Guidance and Development• Training in Skills and Trades, Tailoring, Embroidery,
Handicrafts etc..• Vocational Training / Higher Studies• Support to Meritorious Students• Training in First – Aid and Disaster Management• Values Inculcation and retaining Culture and Heritage• Encouraging to learn Village Folk Art Forms like Chekka
Bhajan, Kolatam etc.• Conducting Competitions in Village Sports
Family – Women Care
• Hygiene, Sanitation• Training in Child care• Literacy• Values Inculcation – Family Concepts• Alternative Revenue Creation and training• Training in Tailoring, Embroidery etc• Economic Empowerment - growing Cattle, Poultry,
Vegetables etc..• Creating Positive Diversion into Traditional Arts,
Heritage Games, Folk and Fine Arts• Inducting into Bhajans and SSS Spirituality

Bhagavan’s Compassion
for needy Mahilas

Family – Men Care
• Educating on Modern Techniques of Agriculture for Better Income
• Alternative – Supplementary – Supportive Revenue generation
• Literacy• Exposure to Various Skills• Supplementing and Supporting activity for Self -
Employment• Training in First – Aid and Disaster Management• Values Inculcation• Motivation for Service• Encouraging to learn Village Folk Art Forms like Chekka
Bhajan, Kolatam etc.• Conducting Competitions in Village Sports

Family - Critical Care
Focused Survey may be conducted on
• Neonates• Pregnant Women• Physically Challenged• Old Citizen
• Minimum needs for healthy and better living may be planned on continuous and sustainable basis

Bhagavan’s compassion for Physically Challenged
Bhagavan in Neonatal care
Special CareSpecial care may be taken for Sick, Handicapped and very Old.
•Cooked Food Distribution (daily) and other necessary items.
•Food Material Distribution Annapurna Amrutha KalasamRice -10 kgs + Dall -1 kg + Oil - 1kg + other provisions like bathing and detergent soaps 1 each (every month) + Fuel (firewood or coal) for cooking.
•Providing Attendant facility if necessary and if possible.
Annapurna Amrutha Kalasam

Village – Educational Care• Literacy Activity• Knowledge Transfer• Skills Training, Computers and IT training• Alternative Revenue Generation• Bringing Village back into Spiritual Path• Exposure to Indian Culture, Heritage, Tradition and Values
by Audio - Visual gadgets, Role-Plays, Mono Actions, Drama, Street Plays and such other innovative methods
• Technical Interaction Sessions with Agriculture, Horticulture, Veterinary Specialists
• Training in First-Aid, Nursing and Midwifery• Educating on Community and Preventive Medicine• Educating on the ill effects of Social Evils of Alcoholism etc• Yuva Vikas
Village – Medical Care• Medical Census and Computerised Records• Focus on Malnutrition• Contagious Diseases • Terminal Illnesses like Cancer, AIDS, HIV etc• Skin, Teeth, Eyes Periodical Check-ups• Pregnant Women, Neonates, Geriatrics, Physically
Challenged – Special Focus• Periodical need based Multi-Specialty Screening
and Medical camps• Creating Awareness on Hygiene, Sanitation,
Preventive Medicine and Community Health through audio-visuals and other means.
• Mobile Hospital

Bhagavan in Medical Care

Bhagavan in Care of Hygiene
andSanitation
Village – Social Care
• Creating Awareness on their village needs and Community Development and participation through Seva.
• Schemes for Inadequacy of food, Illness, Illiteracy and Infrastructure and motivating the villagers participation.
• Additional / Supportive / Supplementary Revenue generation.
• Technical Support to Self Employment Trades.• Encouraging Gramothsavas, Traditional Fairs, Community
Festivals, Sports, Games and Art Forms.• Promoting National Spirit, Cooperation, Unity of Castes,
Faiths and Religions.• Training in Disaster Management and Natural Calamities.• Starting Sri Sathya Sai Bhajana Mandali.

Village Agri Care
• Training farmers in latest Cultivation Techniques
• Preparation of Vermi Compost and Organic Manures
from Agri, Veterinary and Domestic Waste.• Providing Agricultural Tools • Milk production (providing cattle)• Veterinary Medical Camps• Awareness about the duplicate Seeds, Fertilizers
and Government Schemes• Review camps and continuous monitoring• Motivating for a Co-operative Farming and Marketing
Bhagavan in Veterinary Care
Village Spiritual Care
• Village Rituals• Culture and Heritage• Performing Pooja • Veda Chanting• Balvikas classes • Study Circles• Providing Spiritual Literature, audio and video • Spiritual Discourses• Pallaki Seva, Samoohika Vrathams etc.• Conducting Upanayanams • Free Marriages for deserving poor girls• Practicing Ceiling on Desires

Bhagavan in Spiritual Care

Village - Infrastructure
• Gober gas, Solar Energy and Renewable energy Systems.
• Water Harvesting and Drip Irrigation.• Cooperative Poultry farming, Cattle farming etc.• Safe Drinking Water : De-Mineralisation, De-
Flouridisation, De-Salination (DM,DF, DS plants).• Environment Protection – Tree Plantation of
Flowering and Fruit Bearing Plants.• Sanitation, Community Latrines, Healthier
Surroundings, Drainage etc.• Internal Roads and Approach Roads.• Rural Industries – Cottage Industries etc.
4 M’s Planning
Manpower: Integrate the services of expertise and experience of SSSSO members of all age groups, multiple skills and varied interests. Skill and expertise may be outsourced if need be. The selected personnel may be briefed and trained appropriately. Group-III Balvikas students may be inducted into SSSVIP as project work during vacation guided by Balvikas Coordinator.
Money, Material and Machine: Mobilise, pool up and procure through internal sources as per the needs.
Timeframe• SSSVIP for the selected village may be
planned for minimum of 2 years and maximum of 3 years.
• Plan the Activities with a Timeframe to accomplish the set objectives.
• Activities may be phased out on priority.• Schedule, Implement and Monitor the
planned activities periodically.• PERT – Progress may be Evaluated by
Review Technique and suitable measures may be taken with Contingency plans to complete the task.

Our TargetOur Target Build a Better
Tomorrow with our Constant, Consistent and Continuous Efforts Today with Love.

UNITY PURITY
DIVINITY
Let us Work Together withLet us Work Together with




JAI SAI RAM