australian physiotherapy per spee tives onqua11 ty - … · australian physiotherapy jennifer...
TRANSCRIPT
AUSTRAlIAN PHYSIOTHERAPY
Jennifer RobertsJillian Freeman
PER SPEe TIVES ONQ UA11 TY
Hydrotherapy managementof low baekpain: a qualityimprovementprojeet
An audit of 81 patients referred to hydrotherapyfor low back pain was carried out over 12months. The audit recorded response tohydrotherapy in terms of area of pain; intensityof pain; range of motion and ability to performactivities of daily living; treatment frequencyand duration; and hydrotherapy programcontent.Results showed a highly significant beneficialresponse {t
IB7}=9.2, p<0.DD1}. Changes tathe
hydrotherapy service resulting from the studyinclude improved documentation; standardisedassessment; re-worked hydrotherapy program;and regular assessment of patients withinplanned time-frames.[Roberts JM and FreemanJ: Hydrotherapymanagement of low back pain: A qualityimprovement project. Australian Journal ofPhysiotherapy 41: 205-208]
Key words: Backache;Hydrotherapy; lumbosacralRegion; Quality Assurance,Health Care
JM Roberts HAppSc, MAPA is SeniorPhysiotherapist, Hydrotherapy, at the WodenValley.Hospital, Canberra.
J Freeman DipPhty, MAPA is OutpatientsSupervisor at the Woden Valley Hospital,Canberra.
Correspondence: JM Roberts, PhysiotherapyDepartment, Woden Valley Hospital, PO Box11, Woden, ACT 2606.
xercise therapies for treatment oflow back pain have beenextensively researched, but with
few studies showing randomisedcontrolled trials (Koes et al 1991). Of16 studies reviewed by Koes et al(1991), only six showed a positivebenefit from exercise.
It is not possible to extrapolate fromresults ofland based exercise tohydrotherapy programs. Theproperties ofwater (buoyancy, fluidityand heat) will all have an effect on theexercising body (Skinner et al 1983).Muscle tone will be reduced, as willpain, and a more finely gradedprogression.of exercises is possible(Skinner et al 1983).
The biomechanical forces on thelumbar.spine may also be different inwater. Bogduk etal(1992) andNachemson and Elfstrom (1970) citevery high lumbar compression loadsduring conventional exercises. As yet,no published biomechanical analysis ofexercises in water is available andtherefore it is·not possible todetermine whether these undesirableloads are reduced in a hydrotherapyprogram.
In 1988, Landridge and Phillipsdescribed a management plan for backpain sufferers involving grouphydrotherapy exercises. The patientswith a history of chronic low back painreported reduction in pain levels andimproved quality of life onquestionnaire.
Smit and Harrison (1991) observedreduction in pain levels and improvedspinal mobility in their pilot study of
20 subjects with lumbar spondylosisattending hydrotherapy. They alsopublished a description of thehydrotherapy exercises which wereperformed by the subjects, which isvaluable information for otherclinicians.
Since these two studies suggestpositive outcomes for patients with lowback pain, an audit was proposed toevaluate outcomes for patientsattending the hydrotherapy service atWoden Valley Hospital in Canberra.At a group discussion,physiotherapystaffvoiced a perception that a highproportion of patients were failing torespond to hydrotherapy. However, nodata had been collected. There was noexercise protocol in use, and noguidelines to determine the effectivelength for a course of hydrotherapyhad been developed.
A retrospective audit was performedon the records of 107 patients who hadreceived hydrotherapy for low backpain over the previous 18 months. Theaudit sought to record diagnoses ofpatients, outcomes of treatment andthe duration of the course oftreatment. The major problem withthis audit was that many of the patientshad not been reassessed followinghydrotherapy and the outcomes werenot documented.
Physiotherapy staff decided toimplement standard procedures fordocumentation and regular assessmentand reassessment ofpatients duringtheir course of treatment. With theseprocedures in place, a concurrent audit-
PERSPECTIVES ON QUAliTY AUSTRAliAN PHYSIOTHERAPY
"":"":":":::""""""1
:.••.•••:••••••••••••••.;.; ;..:.» : >.>.>: •••••••• ' .
1::2 :2.............••.•:'.
,::: ."'''::4: 11 0
,}F ,0:............:...:.. ,: ...:......:..... """"1........,
: ....... "::"1
0 0
22 4••• :., ••• '., •••• :.,.'.::., •• >..... :,., •••• :,>.' ••
.......... '.":.
.................
ability to perform activities of dailyliving. One point was awarded for eachfactor which improved, one pointsubtracted for each factor whichworsened, and no points awarded for afactor which remained the same. For apatient to be described as better, ascore of two points or more wasrequired. For a patient to be noted asthe same, a score of one or zero wasrequired4 For a patient to be listed asworse, a negative score was required.
Statistical analysis
Scores of response to hydrotherapywere analysed using a two tailed,unpaired t test4 Analysis of the exerciseprotocols which the patient hadfollowed was precluded by theclinicians' freedom to tailor exercise
i,Better":·:::: ,',:-Same
···········:···,········:······17 ...... 2::: ..
7>.·... ·<.·.· ... ..,........... 140 ()
..,.............:.
..:>
......... '" ."'."
68
••.•••••>•• ' ···:··:'·'··'·'··':::B,etter,.:••• :: ••:.:<:',.::.:','Same"::}-::.':.:::,;:::',WO:fS~::':: •• :': •••• ::>::.: ••:: .......:•••...
: : •••• >.: •••» S~ot¢: >',://,/~cr)re>:<?,:.:</ S~~re,n , ' ":.,:.'].,'.; 4~::i:3:~:::,2'::::',: ••.:":,:.<:::':>::::::'l:'~::,'O,j>:,:::,:,;±:l::~:r~~::;,\.E,~·~:,:}+J:I.:::.:':":~:::::,:·.·.
:.:<:.,' : •••.•:•.••••• :.> .
:·'··><......... >::13 "':"·:,:'''':::''''·:::::'::13
'..... '..... '.,..... '..
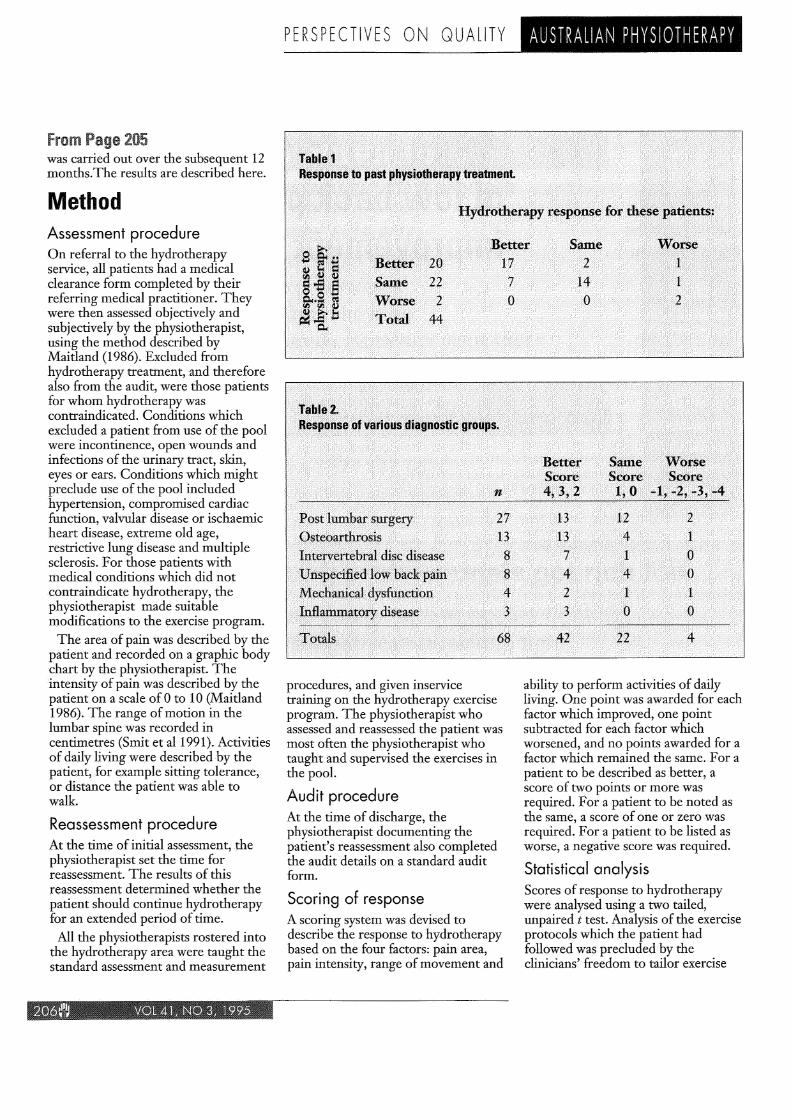
,"JalJ'le:':2:i, "':I!~I:~.~e",o~ VariOU$::'dUjg'Q~'~i~:::9r.~~~~,.
:'.,".
',(;)~~,~,()~Wrosi~, ", ,Inte~~~~ebtil>als¢:::aisease
",':i~p::~J(ji,~:¢a:·Jl~~d::~ilf~R' :p1tiri',M~clia.vilcar',q¥sf1Iii¢t:io~mfl~ll1:~tQ~Yf-a.ise$e
,,1fl~ta~$,',
procedures, and given inservicetraining on the hydrotherapy exerciseprogram. The physiotherapist whoassessed and reassessed the patient wasmost often the physiotherapist whotaught and supervised the exercises inthe pooL
Audit procedure
At the time of discharge, thephysiotherapist documenting thepatient's reassessment also completedthe audit details on a standard auditform4
Scoring of response
A scoring system was devised todescribe the response to hydrotherapybased on the four factors: pain area,pain intensity, range of movement and
1,)'·?TatJl~L1,,' ',', ' , '1::::::::('j:,~:~p:e.9t;.~.J~::past ..p:~Y$iotberapy treatment..:.'
I.·>:: ... ··;..... ·: •• ::: ... •••• "'"
from Page 205was carried out over the subsequent 12months.The results are described here4
Assessment procedure
On referral to the hydrotherapyservice, all patients had a medicalclearance form completed by theirreferring medical practitioner4 Theywere then assessed objectively andsubjectively by the physiotherapist,using the method described byMaitland (1986)4 Excluded fromhydrotherapy treatment, and thereforealso from the audit, were those patientsfor whom hydrotherapy wascontraindicated. Conditions whichexcluded a patient from use of the poolwere incontinence, open wounds andinfections of the urinary tract, skin,eyes or ears. Conditions which mightpreclude use of the pool includedhypertension, compromised cardiacfunction, valvular disease or ischaemicheart disease, extreme old age,restrictive lung disease and multiplesclerosis4 For those patients withmedical conditions which did notcontraindicate hydrotherapy, thephysiotherapist made suitablemodifications to the exercise program.
The area of pain was described by thepatient and recorded on a graphic bodychart by the physiotherapist4 Theintensity of pain was described by thepatient on a scale of 0 to 10 (Maitland1986). The range of motion in thelumbar spine was recorded incentimetres (Smit et a11991)4 Activitiesof daily living were described by thepatient, for example sitting tolerance,or distance the patient was able towalk4
Reassessment procedure
At the time of initial assessment, thephysiotherapist set the time forreassessment4 The results of thisreassessment determined whether thepatient should continue hydrotherapyfor an extended period of time4
All the physiotherapists rostered intothe hydrotherapy area were taught thestandard assessment and measurement
Method
AUSTRAliAN PHYSIOTHERAPY
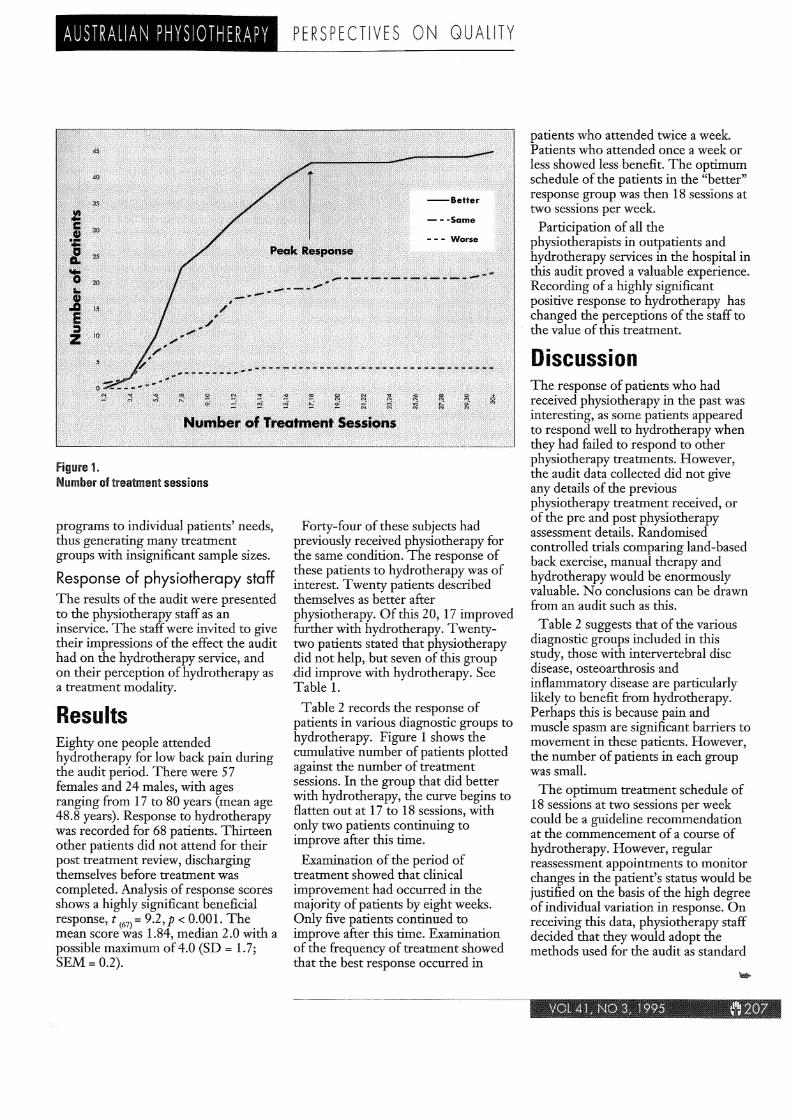
Figure 1.Number of treatment sessions
programs to individual patients' needs,thus generating many treatmentgroups with insignificant sample sizes.
Response of physiotherapy staffThe results of the audit were presentedto the physiotherapy staff as aninsemce. The staff were invited to givetheir impressions of the effect the audithad on the hydrotherapy service, andon their perception of hydrotherapy asa treatment modality.
ResultsEighty one people attendedhydrotherapy for low back pain duringthe audit period. There were 57females and 24 males, with agesranging from 17 to 80 years (mean age48.8 years). Response to hydrotherapywas recorded for 68 patients. Thirteenother patients did not attend for theirpost treatment review, dischargingthemselves before treatment wascompleted. Analysis of response scoresshows a highly significant beneficialresponse, t (67) =9.2, P< 0.001. Themean score was 1.84, median 2.0 with apossible maximum of4.0 (SD = 1.7;SEM= 0.2).
PERSPECTIVES ON QUAliTY
Forty-four of these subjects hadpreviously received physiotherapy forthe same condition. The response ofthese patients to hydrotherapy was ofinterest. Twenty patients describedthemselves as better afterphysiotherapy. Of this 20, 17 improvedfurther with hydrotherapy. Twentytwo patients stated that physiotherapydid not help, but seven of this group~id improve with hydrotherapy. SeeTable 1.
Table 2 records the response ofpatients in various diagnostic groups tohydrotherapy. Figure 1 shows thecumulative number of patients plottedagainst the number of treatmentsessions. In the group that did betterwith hydrotherapy, the curve begins toflatten out at 17 to 18 sessions, withonly two patients continuing toimprove after this time.
Examination of the period oftreatment showed that clinicalimprovement had occurred in themajority of patients by eight weeks.Only five patients continued toimprove after this time. Examinationof the frequency of treatment showedthat the best response occurred in
patients who attended twice a week.Patients who attended once a week orless showed less benefit. The optimumschedule of the patients in the "better"response group was then 18 sessions attwo sessions per week.
Participation of all thephysiotherapists in outpatients andhydrotherapy services in the hospital inthis audit proved a valuable experience.Recording of a highly significantpositive response to hydrotherapy haschanged the perceptions of the staff tothe value of this treatment.
DiscussionThe response of patients who hadreceived physiotherapy in the past wasinteresting, as some patients appearedto respond well to hydrotherapy whenthey had failed to respond to otherphysiotherapy treatments. However,the audit data collected did not giveany details of the previousphysiotherapy treatment received, orof the pre and post physiotherapyassessment details. Randomisedcontrolled trials comparing land-basedback exercise, manual therapy andhydrotherapy would be enormouslyvaluable. No conclusions can be drawnfrom an audit such as this.
Table 2 suggests that of the variousdiagnostic groups included in thisstudy, those with intervertebral discdisease, osteoarthrosis andinflammatory disease are particularlylikely to benefit from hydrotherapy.Perhaps this is because pain andmuscle spasm are significant barriers tomovement in these patients. However,the number of patients in each groupwas small.
The optimum treatment schedule of18 sessions at two sessions per weekcould be a guideline recommendationat the commencement of a course ofhydrotherapy. However, reguJarreassessment appointments to monitorchanges in the patient's status would bejustified on the basis of the high degreeof individual variation in response. Onreceiving this data, physiotherapy staffdecided that they would adopt themethods used for the audit as standard

from Page 207practice for the service, includingstandardised assessment proceduresand scheduling regular reassessmentappoinnnents in order to monitorresponse.
A hydrotherapy back class has alsocommenced as a result of this project.A patient, once assessed, beginsindividual hydrotherapy sessions. Oncestable in response to the exercises, inthat they are nat aggravating the lowback pain, the patient then progressesto the group class.
ConclusionThis quality assurance project hadmany positive outcomes for thehospital's hydrotherapy service. Itsupported the premise thathydrotherapy has beneficial effects fora variety of patients with lumbar regionpain, including some for whom
PER SPEe TI VES ON QUAll TY
physiotherapy had nat been successful.The data demonstrated the mosteffective treatment schedule andreinforced the advantages of regularreassessments during this time.
An audit was found to be °a usefulmethod to examine practice in thehydrotherapy service within thelimitationsofa busy public hospitaldepartment. It is planned that a followup audit be performed to review theeffects of the changes to practice in theservice in terms of patient outcomesand service efficiency.
References
BogdukN, Pearcy MJ and Hadfield G (1992): Thean~t?mya.nd biomechanicsofthepsoas major.Clzntcal BlOmechanics 7: 109-,119.
Koes BW,BouterLM, BeckermanH Van DerHeijdenG]MG and KnipschildPG (199J):P~ysiotherapy exercises and back pain: AblInded. review. British Medical Journal302: 1572-6.
AUSTRAliAN PHYSIOTHERAPY
Langridge JC and Phillips D .(1988): Grouphydrotherapy exercises for chronic back painsufferers - introduction and monitoring.Physiotherapy 74: 269-273.
MaitlandGD (1986): Vertebral Manipulation (5thed.) London: Butterworth, pp. 43-102.
Nachemson A and Elfstrom G (1970): Intravitaldynamic.pressure measurements in lumbardiscs. A study of common movements,manoeuvres and exercises. ScandinavianJournalofRebabilitation Medicine Supplement1: 1-40.
PriceDD, McGrath PA, Rafii A and BuckinghamB (1983): Th~ vaHdationofvisual analoguescales as ratio measures for chronic andexperimental pain. Pain J7: 45-56.
Skinner ET and Thompson AM (1983): Duffield'sExercise in Water (3rd ed.) London: BalliereTindall, pp. 56-62.
Smit TE and ~arrison R (1991): Hydrotherapyandchr~nlc lower back pain: A pilot study.AustralIan Journal of Physiotherapy36: 229-233.
Zusman M (1986): The absolute visual analoguescale (Ay-AS) asa measure of pain intensity.Australtan Journal of Physiotherapy32: 244-246.