autonomic modulation as a paradigm for cardiovascular
TRANSCRIPT
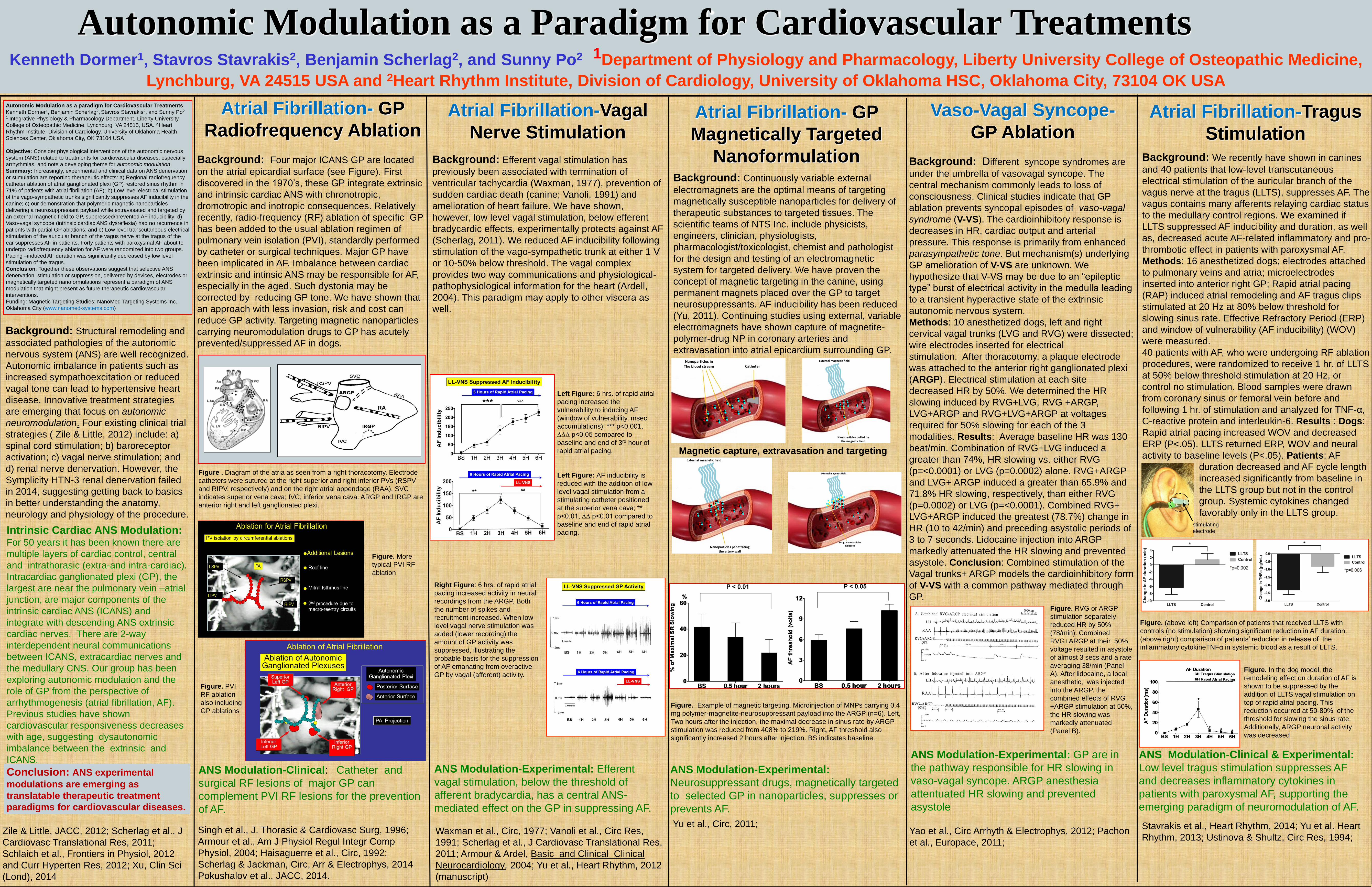
Autonomic Modulation as a Paradigm for Cardiovascular Treatments Kenneth Dormer1, Stavros Stavrakis2, Benjamin Scherlag2, and Sunny Po2 1Department of Physiology and Pharmacology, Liberty University College of Osteopathic Medicine,
Lynchburg, VA 24515 USA and 2Heart Rhythm Institute, Division of Cardiology, University of Oklahoma HSC, Oklahoma City, 73104 OK USA
Atrial Fibrillation- GP
Radiofrequency AblationAtrial Fibrillation-Vagal
Nerve StimulationAtrial Fibrillation- GP
Magnetically Targeted
Nanoformulation
Abstract:
Background: Structural remodeling and
associated pathologies of the autonomic
nervous system (ANS) are well recognized.
Autonomic imbalance in patients such as
increased sympathoexcitation or reduced
vagal tone can lead to hypertensive heart
disease. Innovative treatment strategies
are emerging that focus on autonomic
neuromodulation. Four existing clinical trial
strategies ( Zile & Little, 2012) include: a)
spinal cord stimulation; b) baroreceptor
activation; c) vagal nerve stimulation; and
d) renal nerve denervation. However, the
Symplicity HTN-3 renal denervation failed
in 2014, suggesting getting back to basics
in better understanding the anatomy,
neurology and physiology of the procedure.
Intrinsic Cardiac ANS Modulation: For 50 years it has been known there are
multiple layers of cardiac control, central
and intrathorasic (extra-and intra-cardiac).
Intracardiac ganglionated plexi (GP), the
largest are near the pulmonary vein –atrial
junction, are major components of the
intrinsic cardiac ANS (ICANS) and
integrate with descending ANS extrinsic
cardiac nerves. There are 2-way
interdependent neural communications
between ICANS, extracardiac nerves and
the medullary CNS. Our group has been
exploring autonomic modulation and the
role of GP from the perspective of
arrhythmogenesis (atrial fibrillation, AF).
Previous studies have shown
cardiovascular responsiveness decreases
with age, suggesting dysautonomic
imbalance between the extrinsic and
ICANS.
Atrial Fibrillation-Tragus
Stimulation
Background: Continuously variable external
electromagnets are the optimal means of targeting
magnetically susceptible nanoparticles for delivery of
therapeutic substances to targeted tissues. The
scientific teams of NTS Inc. include physicists,
engineers, clinician, physiologists,
pharmacologist/toxicologist, chemist and pathologist
for the design and testing of an electromagnetic
system for targeted delivery. We have proven the
concept of magnetic targeting in the canine, using
permanent magnets placed over the GP to target
neurosuppressants. AF inducibility has been reduced
(Yu, 2011). Continuing studies using external, variable
electromagnets have shown capture of magnetite-
polymer-drug NP in coronary arteries and
extravasation into atrial epicardium surrounding GP.
Background: Four major ICANS GP are located
on the atrial epicardial surface (see Figure). First
discovered in the 1970’s, these GP integrate extrinsic
and intrinsic cardiac ANS with chronotropic,
dromotropic and inotropic consequences. Relatively
recently, radio-frequency (RF) ablation of specific GP
has been added to the usual ablation regimen of
pulmonary vein isolation (PVI), standardly performed
by catheter or surgical techniques. Major GP have
been implicated in AF. Imbalance between cardiac
extrinsic and intinsic ANS may be responsible for AF,
especially in the aged. Such dystonia may be
corrected by reducing GP tone. We have shown that
an approach with less invasion, risk and cost can
reduce GP activity. Targeting magnetic nanoparticles
carrying neuromodulation drugs to GP has acutely
prevented/suppressed AF in dogs.
Vaso-Vagal Syncope-
GP Ablation
Autonomic Modulation as a paradigm for Cardiovascular Treatments
Kenneth Dormer1, Benjamin Scherlag2, Stavros Stavrakis2, and Sunny Po2
1 Integrative Physiology & Pharmacology Department, Liberty University
College of Osteopathic Medicine, Lynchburg, VA 24515, USA. 2 Heart
Rhythm Institute, Division of Cardiology, University of Oklahoma Health
Sciences Center, Oklahoma City, OK 73104 USA
Objective: Consider physiological interventions of the autonomic nervous
system (ANS) related to treatments for cardiovascular diseases, especially
arrhythmias, and note a developing theme for autonomic modulation.
Summary: Increasingly, experimental and clinical data on ANS denervation
or stimulation are reporting therapeutic effects: a) Regional radiofrequency
catheter ablation of atrial ganglionated plexi (GP) restored sinus rhythm in
71% of patients with atrial fibrillation (AF); b) Low level electrical stimulation
of the vago-sympathetic trunks significantly suppresses AF inducibility in the
canine; c) our demonstration that polymeric magnetic nanoparticles
delivering a neurosuppressant payload while extravasated and targeted by
an external magnetic field to GP, suppressed/prevented AF inducibility; d)
Vaso-vagal syncope (intrinsic cardiac ANS dysreflexia) had no recurrence in
patients with partial GP ablations; and e) Low level transcutaneous electrical
stimulation of the auricular branch of the vagus nerve at the tragus of the
ear suppresses AF in patients. Forty patients with paroxysmal AF about to
undergo radiofrequency ablation for AF were randomized into two groups.
Pacing –induced AF duration was significantly decreased by low level
stimulation of the tragus.
Conclusion: Together these observations suggest that selective ANS
denervation, stimulation or suppression, delivered by devices, electrodes or
magnetically targeted nanoformulations represent a paradigm of ANS
modulation that might present as future therapeutic cardiovascular
interventions.
Funding: Magnetic Targeting Studies: NanoMed Targeting Systems Inc.,
Oklahoma City (www.nanomed-systems.com)
ANS Modulation-Clinical: Catheter and
surgical RF lesions of major GP can
complement PVI RF lesions for the prevention
of AF.
Background: Efferent vagal stimulation has
previously been associated with termination of
ventricular tachycardia (Waxman, 1977), prevention of
sudden cardiac death (canine; Vanoli, 1991) and
amelioration of heart failure. We have shown,
however, low level vagal stimulation, below efferent
bradycardic effects, experimentally protects against AF
(Scherlag, 2011). We reduced AF inducibility following
stimulation of the vago-sympathetic trunk at either 1 V
or 10-50% below threshold. The vagal complex
provides two way communications and physiological-
pathophysiological information for the heart (Ardell,
2004). This paradigm may apply to other viscera as
well.
Waxman et al., Circ, 1977; Vanoli et al., Circ Res,
1991; Scherlag et al., J Cardiovasc Translational Res,
2011; Armour & Ardel, Basic and Clinical Clinical
Neurocardiology, 2004; Yu et al., Heart Rhythm, 2012
(manuscript)
ANS Modulation-Experimental: Efferent
vagal stimulation, below the threshold of
afferent bradycardia, has a central ANS-
mediated effect on the GP in suppressing AF.
ANS Modulation-Experimental:
Neurosuppressant drugs, magnetically targeted
to selected GP in nanoparticles, suppresses or
prevents AF.
ANS Modulation-Experimental: GP are in
the pathway responsible for HR slowing in
vaso-vagal syncope. ARGP anesthesia
attentuated HR slowing and prevented
asystole
ANS Modulation-Clinical & Experimental:
Low level tragus stimulation suppresses AF
and decreases inflammatory cytokines in
patients with paroxysmal AF, supporting the
emerging paradigm of neuromodulation of AF.
Background: We recently have shown in canines
and 40 patients that low-level transcutaneous
electrical stimulation of the auricular branch of the
vagus nerve at the tragus (LLTS), suppresses AF. The
vagus contains many afferents relaying cardiac status
to the medullary control regions. We examined if
LLTS suppressed AF inducibility and duration, as well
as, decreased acute AF-related inflammatory and pro-
thrombotic effect in patients with paroxysmal AF.
Methods: 16 anesthetized dogs; electrodes attached
to pulmonary veins and atria; microelectrodes
inserted into anterior right GP; Rapid atrial pacing
(RAP) induced atrial remodeling and AF tragus clips
stimulated at 20 Hz at 80% below threshold for
slowing sinus rate. Effective Refractory Period (ERP)
and window of vulnerability (AF inducibility) (WOV)
were measured.
40 patients with AF, who were undergoing RF ablation
procedures, were randomized to receive 1 hr. of LLTS
at 50% below threshold stimulation at 20 Hz, or
control no stimulation. Blood samples were drawn
from coronary sinus or femoral vein before and
following 1 hr. of stimulation and analyzed for TNF-α,
C-reactive protein and interleukin-6. Results : Dogs:
Rapid atrial pacing increased WOV and decreased
ERP (P<.05). LLTS returned ERP, WOV and neural
activity to baseline levels (P<.05). Patients: AF
duration decreased and AF cycle length
increased significantly from baseline in
the LLTS group but not in the control
group. Systemic cytokines changed
favorably only in the LLTS group.
Zile & Little, JACC, 2012; Scherlag et al., J
Cardiovasc Translational Res, 2011;
Schlaich et al., Frontiers in Physiol, 2012
and Curr Hyperten Res, 2012; Xu, Clin Sci
(Lond), 2014
Conclusion: ANS experimental
modulations are emerging as
translatable therapeutic treatment
paradigms for cardiovascular diseases.
Stavrakis et al., Heart Rhythm, 2014; Yu et al. Heart
Rhythm, 2013; Ustinova & Shultz, Circ Res, 1994;
Yu et al., Circ, 2011; Singh et al., J. Thorasic & Cardiovasc Surg, 1996;
Armour et al., Am J Physiol Regul Integr Comp
Physiol, 2004; Haisaguerre et al., Circ, 1992;
Scherlag & Jackman, Circ, Arr & Electrophys, 2014
Pokushalov et al., JACC, 2014.
Background: Different syncope syndromes are
under the umbrella of vasovagal syncope. The
central mechanism commonly leads to loss of
consciousness. Clinical studies indicate that GP
ablation prevents syncopal episodes of vaso-vagal
syndrome (V-VS). The cardioinhibitory response is
decreases in HR, cardiac output and arterial
pressure. This response is primarily from enhanced
parasympathetic tone. But mechanism(s) underlying
GP amelioration of V-VS are unknown. We
hypothesize that V-VS may be due to an “epileptic
type” burst of electrical activity in the medulla leading
to a transient hyperactive state of the extrinsic
autonomic nervous system.
Methods: 10 anesthetized dogs, left and right
cervical vagal trunks (LVG and RVG) were dissected;
wire electrodes inserted for electrical
stimulation. After thoracotomy, a plaque electrode
was attached to the anterior right ganglionated plexi
(ARGP). Electrical stimulation at each site
decreased HR by 50%. We determined the HR
slowing induced by RVG+LVG, RVG +ARGP,
LVG+ARGP and RVG+LVG+ARGP at voltages
required for 50% slowing for each of the 3
modalities. Results: Average baseline HR was 130
beat/min. Combination of RVG+LVG induced a
greater than 74%, HR slowing vs. either RVG
(p=<0.0001) or LVG (p=0.0002) alone. RVG+ARGP
and LVG+ ARGP induced a greater than 65.9% and
71.8% HR slowing, respectively, than either RVG
(p=0.0002) or LVG (p=<0.0001). Combined RVG+
LVG+ARGP induced the greatest (78.7%) change in
HR (10 to 42/min) and preceding asystolic periods of
3 to 7 seconds. Lidocaine injection into ARGP
markedly attenuated the HR slowing and prevented
asystole. Conclusion: Combined stimulation of the
Vagal trunks+ ARGP models the cardioinhibitory form
of V-VS with a common pathway mediated through
GP.
Magnetic capture, extravasation and targeting
Figure . Diagram of the atria as seen from a right thoracotomy. Electrode
catheters were sutured at the right superior and right inferior PVs (RSPV
and RIPV, respectively) and on the right atrial appendage (RAA). SVC
indicates superior vena cava; IVC, inferior vena cava. ARGP and IRGP are
anterior right and left ganglionated plexi.
Figure. Example of magnetic targeting. Microinjection of MNPs carrying 0.4
mg polymer-magnetite-neurosuppressant payload into the ARGP (n=6). Left,
Two hours after the injection, the maximal decrease in sinus rate by ARGP
stimulation was reduced from 408% to 219%. Right, AF threshold also
significantly increased 2 hours after injection. BS indicates baseline.
Yao et al., Circ Arrhyth & Electrophys, 2012; Pachon
et al., Europace, 2011;
Left Figure: 6 hrs. of rapid atrial
pacing increased the
vulnerability to inducing AF
(window of vulnerability, msec
accumulations); *** p<0.001,
∆∆∆ p<0.05 compared to
baseline and end of 3rd hour of
rapid atrial pacing.
Left Figure: AF inducibility is
reduced with the addition of low
level vagal stimulation from a
stimulating catheter positioned
at the superior vena cava; **
p<0.01, ∆∆ p<0.01 compared to
baseline and end of rapid atrial
pacing.
Right Figure: 6 hrs. of rapid atrial
pacing increased activity in neural
recordings from the ARGP. Both
the number of spikes and
recruitment increased. When low
level vagal nerve stimulation was
added (lower recording) the
amount of GP activity was
suppressed, illustrating the
probable basis for the suppression
of AF emanating from overactive
GP by vagal (afferent) activity.
Figure. RVG or ARGP
stimulation separately
reduced HR by 50%
(78/min). Combined
RVG+ARGP at their 50%
voltage resulted in asystole
of almost 3 secs and a rate
averaging 38/min (Panel
A). After lidocaine, a local
anesthetic, was injected
into the ARGP. the
combined effects of RVG
+ARGP stimulation at 50%,
the HR slowing was
markedly attenuated
(Panel B).
Figure. More
typical PVI RF
ablation
Figure. PVI
RF ablation
also including
GP ablations
Figure. In the dog model, the
remodeling effect on duration of AF is
shown to be suppressed by the
addition of LLTS vagal stimulation on
top of rapid atrial pacing. This
reduction occurred at 50-80% of the
threshold for slowing the sinus rate.
Additionally, ARGP neuronal activity
was decreased
Figure. (above left) Comparison of patients that received LLTS with
controls (no stimulation) showing significant reduction in AF duration.
(above right) comparison of patients’ reduction in release of the
inflammatory cytokineTNFα in systemic blood as a result of LLTS.
stimulating
electrode