award presentation - disc prolapse and genetics
TRANSCRIPT

This presentation won the
In annual conference of
Neurosurgical society of India.
At Indore, 2015.

Association of COL1A1 sp1 gene polymorphism with Disc prolapse from a subset of Indian population: a case control study
Shailendra D Anjankar

• Author– Dr. Shailendra D. Anjankar
• Guides – Dr. Subodh Raju, Dr. M.A. Jaleel, Dr. Dilnavaz B., Dr. Q. Hasan
Department of Neurosurgery
& Department of Genetics and Molecular Medicine,
Kamineni Hospitals, LB Nagar, Hyderabad, Telangana State, India.
Introduction
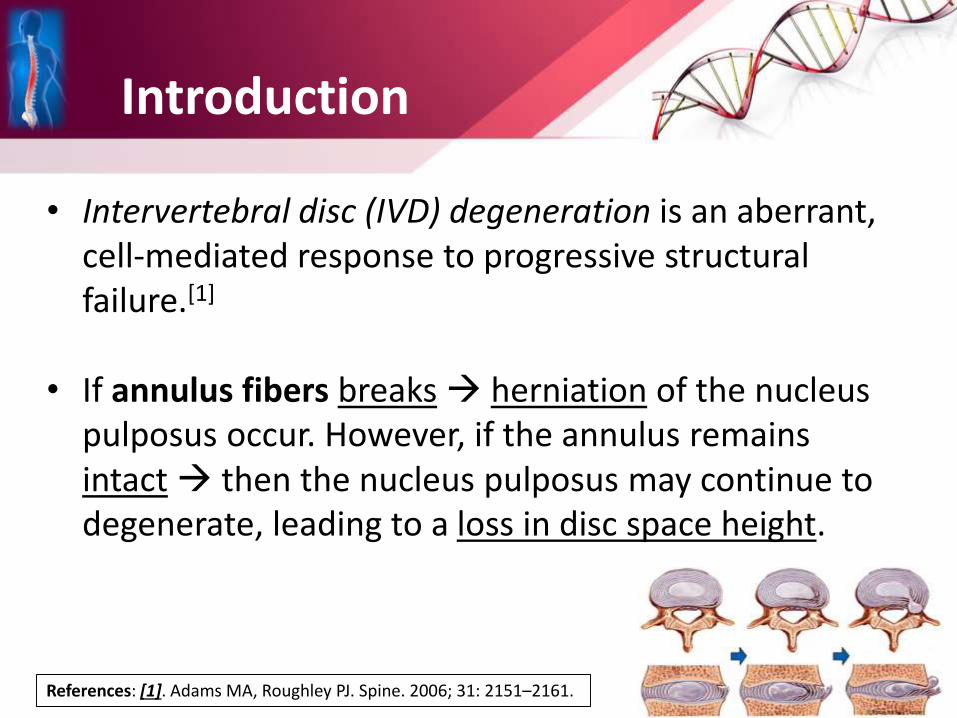
• Intervertebral disc (IVD) degeneration is an aberrant, cell-mediated response to progressive structural failure.[1]
• If annulus fibers breaks herniation of the nucleus pulposus occur. However, if the annulus remains intact then the nucleus pulposus may continue to degenerate, leading to a loss in disc space height.
References: [1]. Adams MA, Roughley PJ. Spine. 2006; 31: 2151–2161.

• Rajashekaran et al showed that the initiatingfactor for disc degeneration is the damage to the endplate. [2]
• Scanning Electron Microscopy has also demonstrated structural failure of annulus fibrosus, delamination and matrix cracking resulting in radial tears in annulus in degenerated discs. [3]
References: [2.] Rajasekaran S et al. Eur Spine J. 2008; 17:626–643. [3.] Iatridis JC, ap Gwynn I. J Biomech. 2004; 37:1165-75.

• Research question:
Type I Collagen – is major component of Annulus fibrosus.
Is the defective development of this collagen responsible for early disc prolapse.?

Etiology of DDD (Degenerative Disc Disease)
• Etiology of disc degeneration is multifactorial in nature.
• Many researchers unanimously agree that genetic factors are largely responsible for it.[2]
• Disc degeneration is regulated by –environmental factors, multiple genes, gene-gene interactions and gene-environment interactions.[3]
References: [4.] Ala-Kokko L. Ann Med. 2002; 34: 42-7. [5.] Solovieva S et al. Spine. 2002; 27: 2691-6
Genetics and Collagen 1
• Type I collagen consists of two alpha-1 and one alpha-2 chains, which are encoded by the COL1A1 and COL1A2 genes, respectively.
• COL1A1 gene is located at the 17q21.3-q22 and is 18 kb (kilo bases) in size and is composed of 52 exons.
• In Sp1 polymorphism the guanine (G) is substituted by thymidine (T) in the fourth Sp1 binding site in intron 1 of COL1A1, more specifically – in the promoter +1245 base pair from the transcription start site.

Diagrammatic representation of COL1A1 gene locus on chromosome 17, and functional polymorphism at the Sp1 site from guanine (G) to thymidine (T).

Materials and Methods
• Study type Case control study
• Sample size 100 (50 + 50)
50 disc prolapse cases and 50 healthy volunteers
• Study period From Nov 2009 to Nov 2012.
• Department of Neurosurgery & Genetics
• After obtaining Institutional Ethics Committee clearance.

Inclusion criteria of cases :
(i) age group 18–60 years,
(ii) occupation not involving rigorous activities,
(iii) Pain score of > 3 score of VAS,
(iv) failed conservative management for a period of at least 3 months,
(v) MRI sequences with evidence of disc prolapse / extrusion / sequestration.

Exclusion criteria of cases:
(i) Age > 60 years,
(ii) occupations like manual laborers lifting heavy weights or persons dealing with vibratory tools,
(iii) body mass index (BMI) more than 30
(iv) smokers.
Criteria for Controls (N=50)Age-matched volunteers, Without any history of neck or back pain Without surgical history for disc prolapse

Disc prolapse due to tear in annulus (A) pictorial representation, (B) MRI T2 Axial and (C) MRI T2 Sagittal images showing disc prolapse.

BLOOD SAMPLE2 ml of EDTA sample
after CONSENT
DNA Isolation
Processed for PCR • RFLP• AGE
Gel Picture
Methodology and DNA Isolation


Ethidium bromide stained 2% Agarose gel picture showing bands corresponding to GG, GT and TT
genotypes.
Statistical analysis
• Chi square test (χ2) and Odds ratio
• MedCalc version 12.6.1.0 software (windows XP/7/8).
• Two tailed P-values less than 0.05 were considered significant.

Results
Demography Characteristics
Cases (n=50) Controls (n=50) P value
Mean age (mean ± SD)
41.7 ± 11.9 43.6 ± 6.7 0.3276
BMI (mean ± SD) 25.67 ± 1.64 25.22 ± 1.36 0.1385
Gender – number of males (% ) 38 (76%) 16 (32%) <0.0001
Positive family history (%)
3 (6 %) 0 (0 %) 0.1882
Demography of the cases and controls
The mean age and BMI in both the groups were similar, but males were significantly more in DDD patient than the control group.

COL1A1 gene polymorphism in cases with intervertebral disc disease and healthy volunteers.
Homozygous – GG, heterozygous GT and homozygous TT genotypes were seen in 38(76%), 10 (20%) and 2(4%) cases respectively, controls had similar percentage of the genotypes as well.

• G allele and T allele (abnormal variant gene) as compared in cases and control group shows no significant difference (p=0.6744).
Alleles Cases Controls
G 86 88
T 14 12
Total 100 100
Table showing frequency of alleles in cases and controls

Genotype
Cases Controls
Expected Observed
Hardy Weinberg
equilibrium
Expected Observed
Hardy Weinberg
Equilibrium
Common homozygotes
GG36.98 38 73.96% 38.72 39 77.44%
Heterozygotes GT
12.04 10 24.08% 10.56 10 21.12%
Rare homozygotes
TT0.98 2 1.96% 0.72 1 1.44%
χ2 = 1.44 (p value = 0.2309)
This polymorphism follows the Hardy-Weinberg Equilibrium in the study population.

Genotypes groups compared
odds ratio95% confidence
intervalp value
TT+GT vs. GG(Dominant model)
1.1196from 0.3175 to
1.8124p=0.5341
TT vs. GT+GG (Recessive model)
2.0417from 0.1792 to
23.2672p=0.5653
GT vs. GG+TT (Co-dominant model)
1.0000from 0.3753 to
2.6645p=1
T allele vs. G allele 1.5315from 0.3753 to
6.2502p= 0.5525
The genotypes matched for dominant, co-dominant and recessive models, statistically significant difference was not observed.
Table showing association of gene polymorphism

There was no significant difference in the frequency of different genotypes at cervical or lumbar region (P=0.5525).
The heterozygous GT genotype was present more in lumbar disc degeneration patients as compared with cervical level (χ2 = 0.0009), but have no significant difference when compared with controls.
Graph showing percentages of different genotypes in cases with disc degeneration at lumbar and cervical region
0
10
20
30
40
50
60
70
80
GG GT TT
Cervical
Lumbar

GG genotype
GT genotype
TT genotype
G allele T allele
Cervical (n=8)
6(75%)
1(12.5%)
1(12.5%)
13/16 (81.25%)
3/16 (18.75%)
Lumbar (n=42)
32(76.19%)
9*(21.42%)
1(2.38%)
73/ 84 (86.75%)
11/84 (13.09%)
Controls(n=50)
39(78%)
10(20%)
1(2%)
88/100(88%)
12/100(12%)
Frequency of genotypes and alleles in cases with disc degeneration at cervical and lumbar region
(* χ2 for GT genotype at Lumbar vs Cervical level, p=0.0009; and Lumbar level vs. controls, p= 0.8981)

Summarizing the results -
1. The mean age and body mass index in cases and controls were similar.
2. Homozygous – GG, heterozygous GT and homozygous TT genotypes were seen in 38(76%), 10 (20%) and 2(4%) casesrespectively, controls had similar percentage of the genotypes as well.
3. The alleles in cases and control group showed no significant difference (p=0.6744) and followed the Hardy-Weinberg Equilibrium in the study population.

Discussion
• Intervertebral disc degeneration is a complex, multifactorial disorder where both environmental and genetic factors play a role.
• Genome Wide Association studies and Candidate Gene Polymorphisms analysis have shown that more than 20 genes may be involved in the etiology of DDD. [6]
• The GT polymorphism in a regulatory region of COL1A1 described for first time by Grant et al [7] .
References: [6]. Mayer JE et al.Spine. 2013; 13: 299-317. [7]. Grant SF et al. Nat Genet. 1996; 14: 203–205.

Authors(year)
Sample sizePopulation Disease Association
Cases Controls
Grant et al [7]
(1996) 299 British Osteoporosis Positive
Pluijm et al [8]
(2004) 966 Dutch
Osteoporosis, Lumbar disc degeneration
Positive
Tilkeridis et al[9]
(2005) 24 12 Greek
Lumbar disc degeneration
Positive
Bei et al [10]
(2008) 24 66 Greek
Lumbar disc degeneration
Positive
(present study) (2015)
50 50 IndianLumbar and Cervical disc degeneration
Negative
Studies till date, showing association of COL1A1 genes with diseases
Reference : [8] Pluijm SMF et al. Ann Rheum Dis. 2004; 63: 71–77. [9] Tilkeridis C et al. J Med Genet. 2005; 42: e44. [10] Bei T, Hormones (Athens). 2008; 7: 251–254.

• 99 polymorphism in 29 selected candidate genes were evaluated by Videman et al and COL1A1, COL9A1 and COL11A2 were shown to be associated with disc signal intensity [11]
• In a recent studies from America by Mayer et al [6] and India by Rathod et al [12] found that Collagen type IX gene polymorphism was associated with disc degeneration.
References: [11] Videman T et al.Arthritis & Rheumatism. 2009; 60: 470–481. [12] Rathod TN et al.Indian J Orthop. 2012; 46: 420 – 426. [6]. Mayer JE et al.Spine. 2013; 13: 299-317.

I Genes Encoding for Matrix components
Collagen
a. Collagen Type I
a. Collagen Type IX
Aggrecan
Cartilage intermediate layer protein (CLIP)
II
Gene encoding for Cytokines
Interleukin -1
Interleukin -6
IIIGenes encoding for proteinases
Matrix Metalloproteinase – 3
IV Genes encoding for Vitamin D receptor
VGenes encoding for Miscellaneous Proteins
Caveolin-1, Asporin, HAPLN1..
Literature review of – Gene polymorphism associated with DDD

• Present study is the first study which evaluated COL1A1 ‘rs1800012’ polymorphism in Indian population.
• And first study in the literature to evaluate disc degeneration of cervical along with lumbar disc with COL1A1 Sp1 gene polymorphism.
• The results of the present study indicate that sp1 COL1A1 is not responsible for DDD in Indian population. May be other collagen gene is involved.
• Disc degeneration is multifactorial and anticipated to be a result of multiple genes involvement and gene – gene interaction.

Conclusion
• Intervertebral disc degeneration is a complex disease and several genes are associated with its etiology.
• The present preliminary study has looked at ‘rs1800012’ Sp1 COL1A1 gene, which showed that, it is in Hardy Weinberg equilibrium in the subset of Indian population studied. But it was not found to be associated with DDD (degenerative disc disease).

Limitations
1. Most of the patient included in the study were from south India it is possible that patients from other parts of India may show an association similar to that observed in Dutch and Greek populations.
2. Secondly, it is impossible to predict that the age related healthy individuals who served as controls will never have disc degeneration and herniation at later date.
3. Thirdly, population studied for the gene is small.

Future prospects
• There is a need to study this polymorphism in a larger population to have confirmatory result.
• As well as to evaluate other probable candidate genes like – vitamin D receptor, aggrecan, Type IX collagen, asporin, MMP3, IL1, and IL6, etc.
• Such genetic studies are crucial for understanding the molecular mechanism of the intervertebral disc degeneration in different populations.

AcknowledgementThankful to my Guides- Dr. Subodh Raju, Dr. M. A. Jaleel, Dr. Dilnavaz BTo our Dean DNB and HOD Genetics- Dr. Q. HassanTo Managing Director - Dr. Shashidhar Kamineni Sir and KHL, LB Nagar staff.
To my colleagues –Dr. S. Ramesh. Dr. Harikishor Reddy, Dr. Swapnil, Dr. Dnyandeepand junior consultants-Dr. Renuka Sharma, Dr. Srinivas B.
To Genetic and Neurosurgery department staffPatients and controls – most importantly.
To my wife – Dr. Sumedha Anjankar and my parents Dr. Deepak and Vidhya Anjankar