back ache orhtopaedics
TRANSCRIPT

Low Back Pain
Low Back Pain Defined• Pain felt in your lower back may come from the spine, muscles,
nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal hernia, or a problem in the testicles or ovaries.
• A variety of symptoms may exist in the presence of back pain. There may be a tingling or burning sensation, a dull aching, or sharp pain. Weakness in the legs or feet may also exist.
• There won't necessarily be one event that actually causes low back pain. The patient may have engaged in common activities of daily living improperly -- like standing, sitting, or lifting -- for a long time. Then suddenly, one simple movement, like reaching for something in the shower or bending from your waist, leads to the feeling of pain.
EpidEmIology Low back pain (LBP)is the fifth most common
reason for all physician visits. 50 to 80 percent of adults experience LBP LBP is the leading cause of disability and lost
production in the US, with associated direct and indirect costs of $50 billion per year
Despite the widespread opinion that 75-90% of patients with LBP recover within about 6 weeks, irrespective of treatment, pain may persist in up to 72%, and disability in up to 12% of patients one year after their first episode of LBP
Etiology(Shedding light on the subject)
• Non - Spinal Causes of Low Back Pain
• Spine Related Causes of Back Pain

Non-Spinal Related CausesBladder Infection Kidney DiseaseOvarian Cancer Ovarian CystTesticular Torsion FibromyalgiaPelvic Infections AppendicitisPancreatitis Prostate Disease
Gall Bladder DiseaseAbdominal Aortic Aneurysm

Spine Related CausesArthritisFibromyalgiaKyphosisLordosisRheumatoid ArthritisAnkylosing SpondylitisArachnoiditisBone CancerChiari MalformationCompression FracturesDiscitisEpidural AbscessFacet Joint SyndromeFixed Sagittal Imbalance
OsteomyelitisOsteophytesPinched NerveRuptured DiscSpina BifidaSpinal Cord InjurySpinal TumorSpondylolisthesisSpinal StenosisSpinal Cord InjurySpinal TumorSprain or StrainSynovial CystsWedge Fractures
Low Back Pain….The Patient
HistoryPhysical ExamDiagnostic Studies
History
Location
Specific Point vs. Across Back
Superficial vs. Deep
Involve Any other region (lower extremity)
History
Quality
Dull Ache (tooth ache)
Sharp/Stabbing
Burning
Tearing/Pop
History
Quality/Severity
Intermittent
Constant
Pain Scale 1-10
History
Setting
Time of day when worst/better
After strenuous activity
HistoryAggravating/Relieving Factors
What Makes Better What Makes Worse
BEWARE OF THE PATIENT THAT SAYS NOTHING MAKES PAIN BETTER!
History
Associated Manifestations
Numbness
Tingling(pins/needles)
Burning
WeaknessIncontinence
Falls
THE EXAM
Physical Exam
General Survey
Muscle Bulk/Wasting
Posture
Alignment
Gait*Patient Should always be examined in an examination gown
Physical ExamMotor Assessment
• Motor Strength - assess to breaking• Tone• Bulk Measurements• Rapid Alternating Movements• Point-to-Point Discrimination
Physical ExamTesting Muscle Strength
•0 - No muscular contraction detected•1 - Barley detectable trace or flicker of contraction•2 - Active movement of body part with gravity eliminated•3 - Active movement against gravity•4 - Active movement against gravity with some resistance•5 - Active movement against full resistance without evidence of fatigue
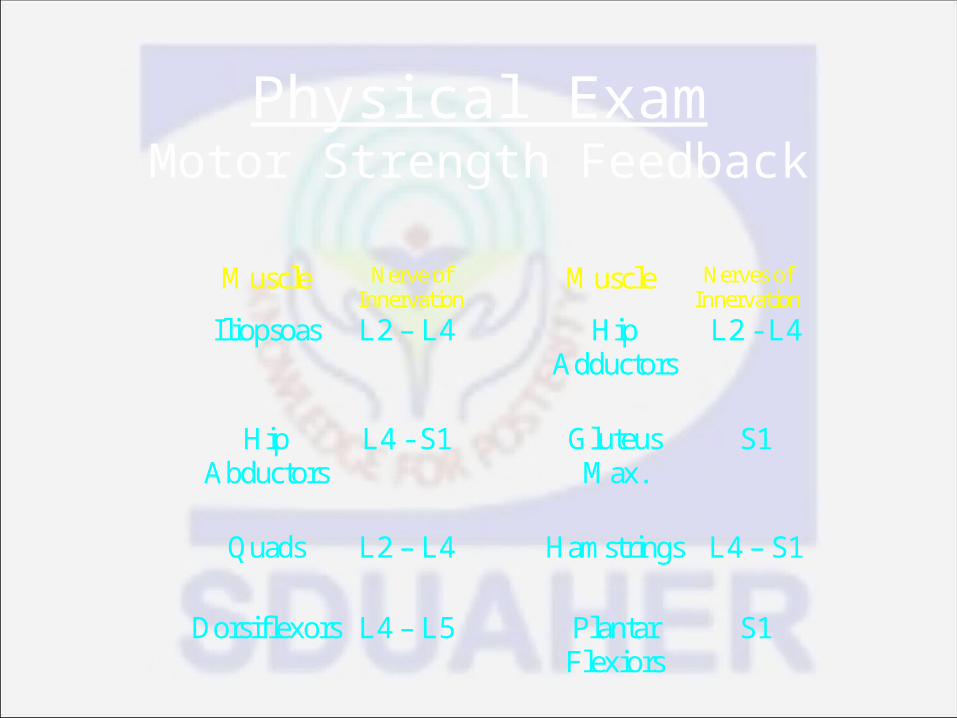
Physical ExamMotor Strength Feedback
Muscle Nerve of Innervation Muscle Nerves of
Innervation Iliopsoas L2 – L4 Hip
Adductors L2 - L4
Hip
Abductors L4 - S1 Gluteus
Max. S1
Quads L2 – L4 Hamstrings L4 – S1
Dorsiflexors L4 – L5 Plantar
Flexiors S1
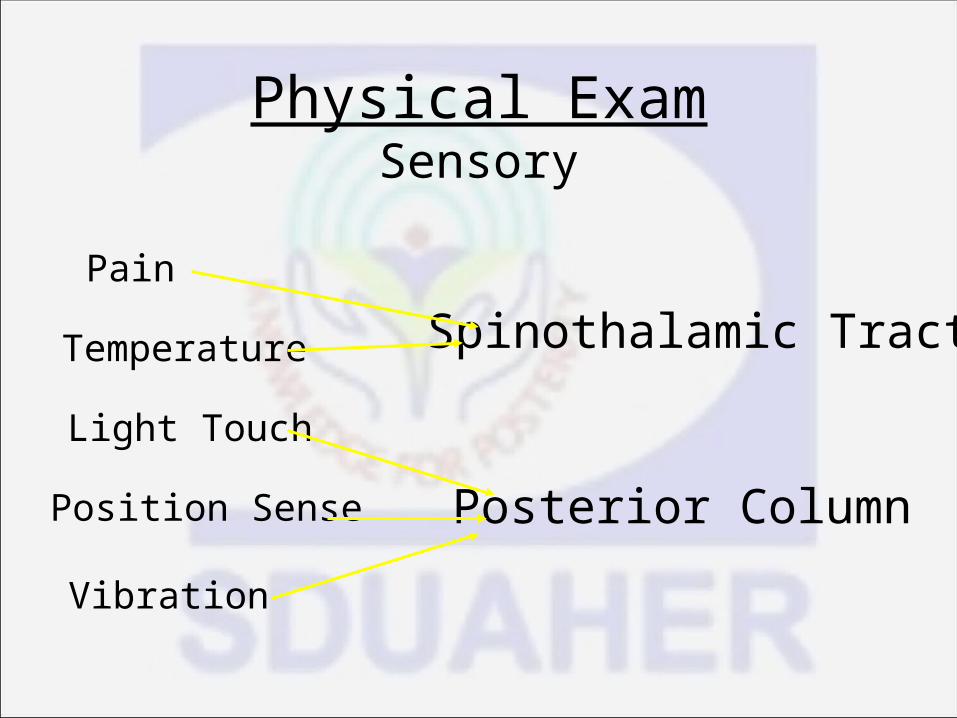
Physical ExamSensory
Pain
Light Touch
Position Sense
Vibration
Temperature Spinothalamic Tract
Posterior Column
Physical ExamReflexes
•Patellar - mediated by L2, L3, L4•Achilles - mediated by S1•Babinski - toes = upper motor neuron dysfunction•Clonus - rhythmic oscillation between dorsi & plantar flexion indicates central nervous system disease
Physical ExamReflexes
• Usually graded on a 0 to 4+ scale• 4+ Very Brisk, Hyperactive with clonus• 3+ Brisker than average, possibly, but not
indicative of disease• 2+ Average; Normal• 1+ Somewhat diminished; low normal• 0 No Response• ** There is no minus in this score system
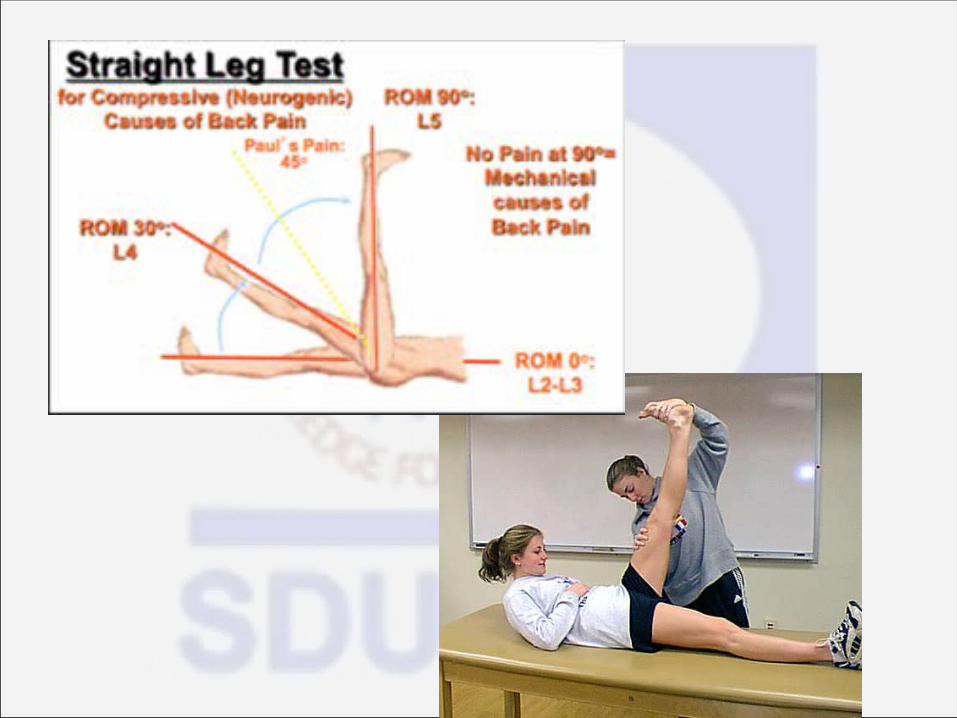
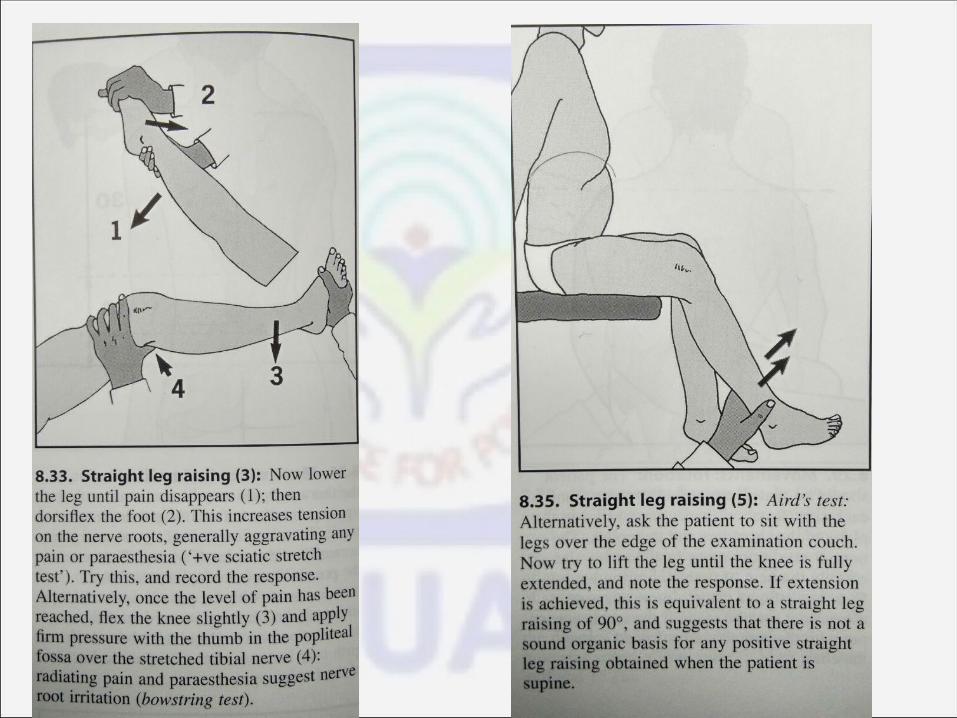
Test in lower back ache in orthopaedics.
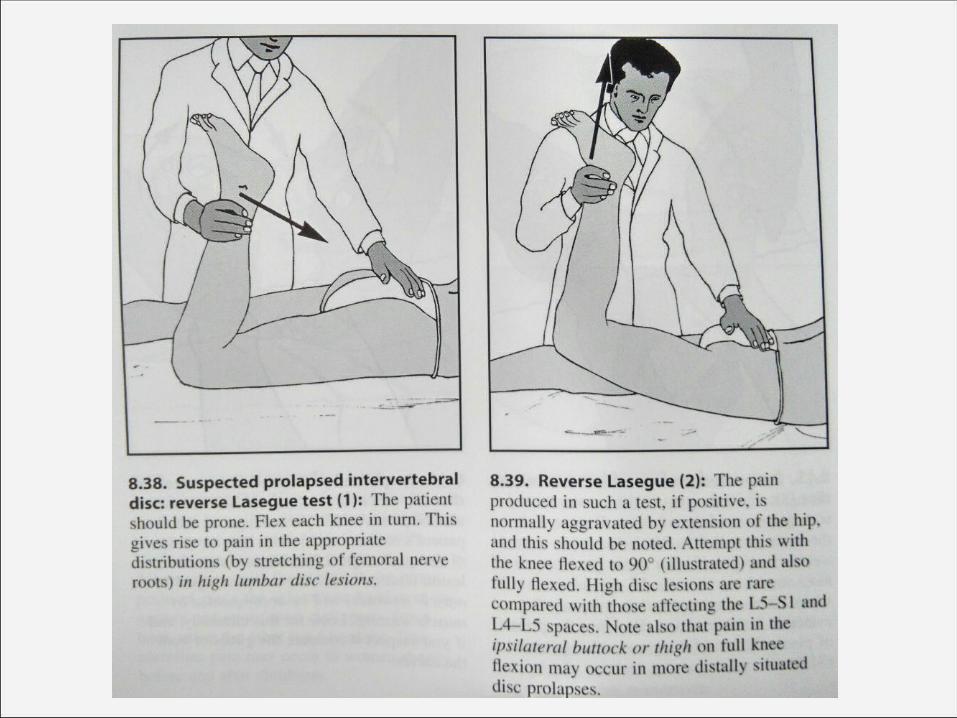
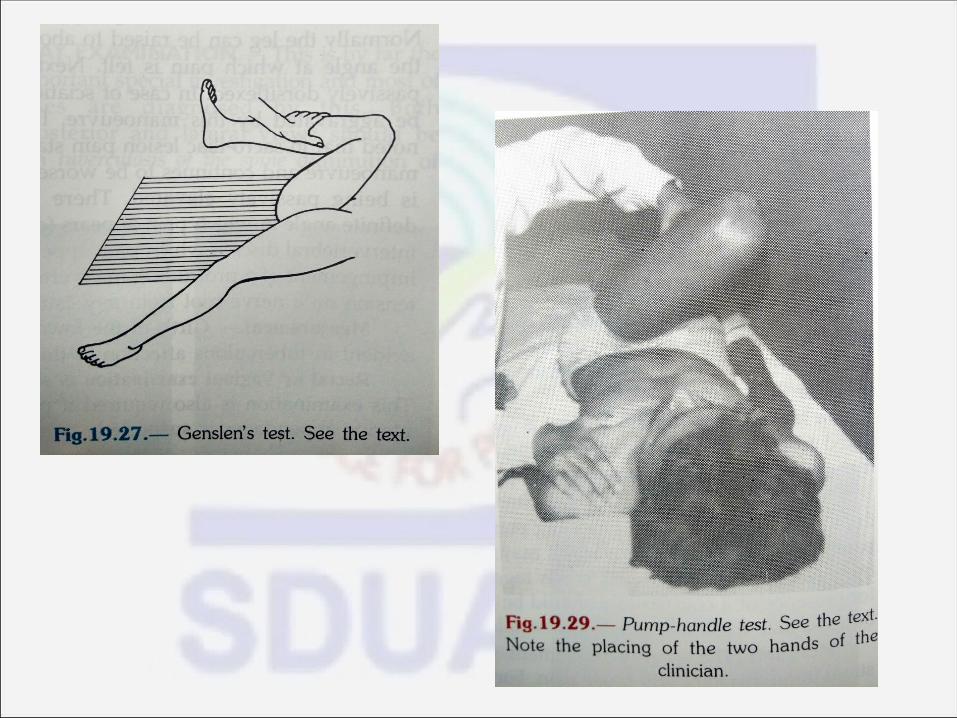
• Straight leg raising.• Lasegue and reverse lasegue• Flip test• Aird’s test• Bowstring test• Genslen’s test• Pump handle test.
Lumbosacral strain
Strains & Sprains• Muscle strains and lumbar sprains are the most
common causes of low back pain • May refer to both injuries as a category called
"musculoligamentous injuries“ .
Signs and symptoms
• Pain is limited to a local area• Pain often occurs simultaneously with an
injury• Decreased ROM from reflex contraction of the
involved muscle and the surrounding muscles• Exacerbation of pain with motion that
contracts the injured muscle
Etiology
• Muscular and ligamentous injuries• Continuous mechanical stress from poor
posture• Small tears in the annulus fibrosus
Lumbar Spinal Stenosis• The disorder can be congenital or acquired• Acquired lumbar stenosis usually is caused by
degenerative disease of the spine and is typically associated with hyperplasia, fibrosis, and cartilaginous changes in the annulus, posterior longitudinal ligament, and ligamentum flavum
• Also can be caused by Spondylolisthesis, spondylolysis, a defect in the pars interarticularis, may be related to injury, bony overgrowth such as occurs in Paget's disease, ankylosing spondylitis, rheumatoid arthritis, and diffuse idiopathic skeletal hyperostosis
Lumbar Spinal StenosisSigns & SX
•Patients present with pain that is brought on by activity and released by rest or leaning forward
•The pain involves the lower back and one or both legs, typically in a radicular distribution, and may be accompanied by numbness or weakness•Examination often reveals no abnormality, except perhaps for a depressed knee or ankle reflex. SLR is usually negative
Disc Herniation• In the lumbar spine, at least 90% of disc
herniations occur at the L5–S1 or L4–5 levels. L3–4 herniations make up only 5% of cases, with the remainder occurring at L2–3 and L1–2
• Clinically, a herniated disc at one level usually affects the nerve root that exits at the level below. For instance, a left L4–5 disc herniation usually compresses the left L5 nerve root
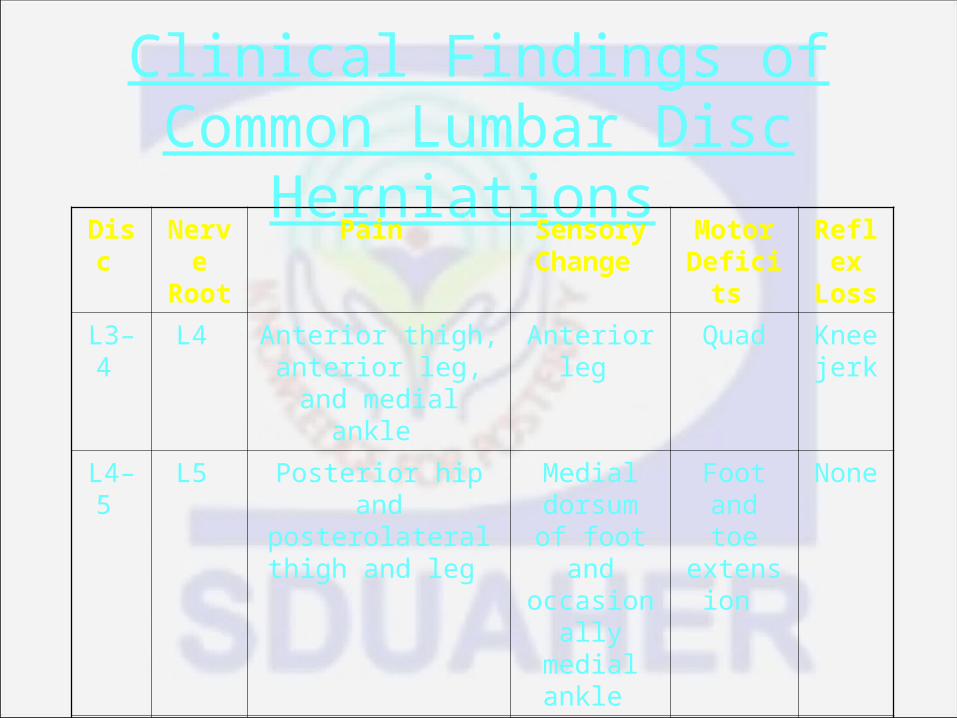
Clinical Findings of Common Lumbar Disc Herniations
Disc Nerve Root
Pain Sensory Change
Motor Deficits
Reflex Loss
L3–4 L4 Anterior thigh, anterior leg, and
medial ankle
Anterior leg Quad Knee jerk
L4–5 L5 Posterior hip and posterolateral thigh
and leg
Medial dorsum of foot and
occasionally medial ankle
Foot and toe
extension
None
L5–S1
S1 Hip, buttock, and posterior thigh and leg
Lateral foot and ankle
Plantar flexion
Ankle jerk
Disc HerniationSigns & SX
• Initial complaints are backache, and in most of those affected, there is no history of antecedent trauma
• Prior similar complaints of back pain or sciatica are common complaints
• The patient 's back pain is usually followed by severe pain that radiates into the lower extremities
• Numbness or paresthesias may occur in the same distribution as the pain, and weakness of selected muscle groups can occur
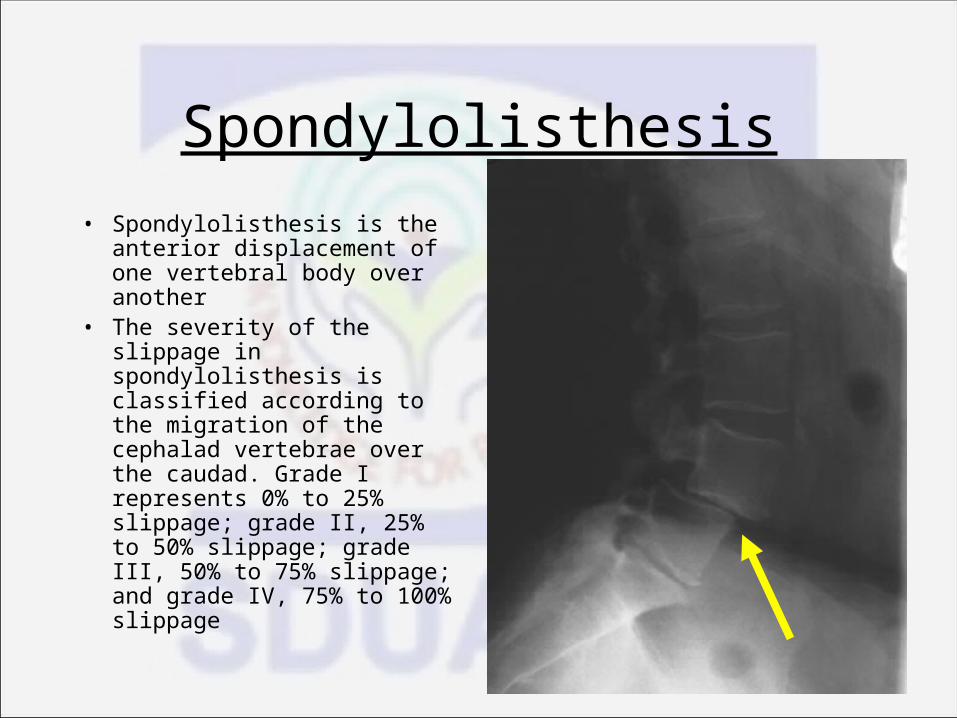
Spondylolisthesis• Spondylolisthesis is the anterior
displacement of one vertebral body over another
• The severity of the slippage in spondylolisthesis is classified according to the migration of the cephalad vertebrae over the caudad. Grade I represents 0% to 25% slippage; grade II, 25% to 50% slippage; grade III, 50% to 75% slippage; and grade IV, 75% to 100% slippage
SpondylolisthesisSigns & SX
• The patient usually complains of gradual onset of low back pain.
• Pain is characterized as deep and aching and is localized to the affected levels.
• Patients may also complain of pain in the buttock or iliac crest.
• Movement makes the pain worse, as do Valsalva maneuvers
• Radicular type symptoms exist most often due to nerve root irritation

Sacroiliac joint dysfunction
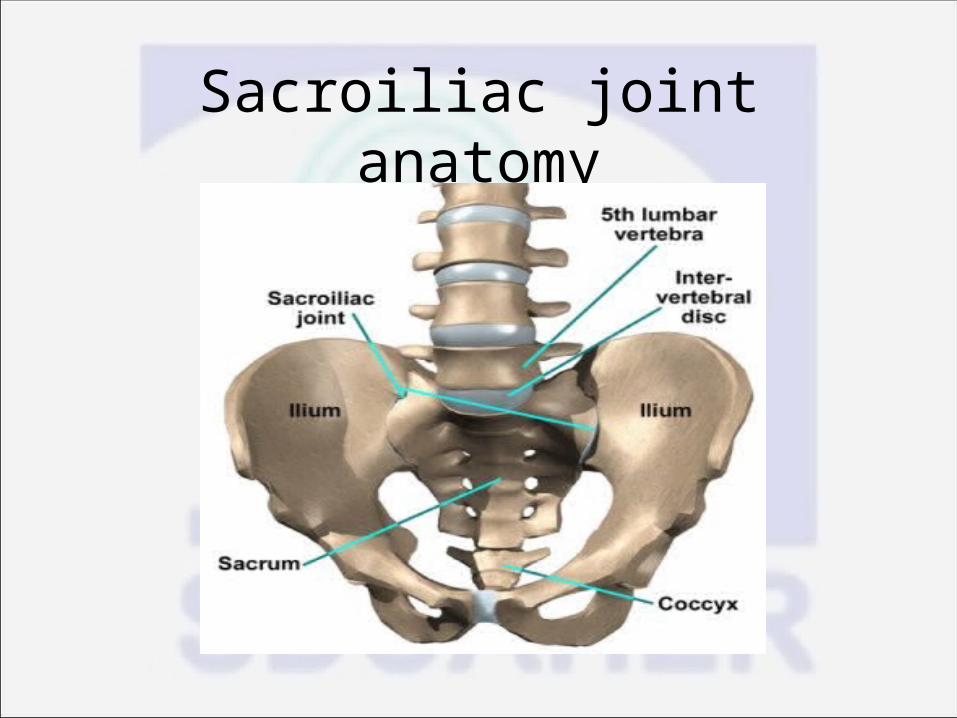
Sacroiliac joint anatomy
Anatomy The axial spine rests on the sacrum, a triangular fusion
of vertebrae arranged in a kyphotic curve and ending with attached coccyx in the upper buttocks. Iliac wings attach on either side forming a bowl with a high back and shallow front. Three joints arise from this union; the pubic symphosis in front, and the right and left SI joints in the back
It is diarthrodial joint: adjacent bones are lined by cartilage, joint cavity contains synovial fluid lined with a synovial membrane, reinforced by a fibrous capsule and ligaments, some degree of free movement.
Etiology The incidence of SI joint pain in patients with
back pain is 15 to 30 percent Sources may be intra-articular or extra-
articular sources. Examples of intra-articular sources include
infection and arthritis. Examples of extra-articular sources include
enthesopathy, fractures, and ligamentous injury.
Signs and symptoms Unilateral pain (unless both joints are affected) localized
predominantly below the L5 spinous process. Point specific tenderness over the sacral sulcus and posterior
sacroiliac spine is consistent physical finding There are several SI joint pain provocation tests that have been
developed to detect SI joint dysfunction. Some of the more commonly used tests include FABER (also
known as Patrick’s test), Gaenslen’s test, Yeoman’s test, and Pelvic rock
A combination of FABER (Flexion, Abduction and External Rotation), POSH (Posterior shear), and READ (Resisted Abduction) tests has a sensitivity of 70% to 80% and a specificity of 100%.
Lumbar zygapophyseal (Facet) arthropathy
Etiology This is pain originating from the facets joints Prevalance my be as high as 10 to 15% in individuals
with LBP With aging lumbar facet joint become weaker and their
orientation changes from coronal to saggital positioning This predisposes them to injury from rotational stress L3-4, L4-5, and L5-S1 are exposed to the most strain
during lateral bending and forward flexion. Thus they are more prone to repetitive strain,
inflammation and joint hypertrophy.
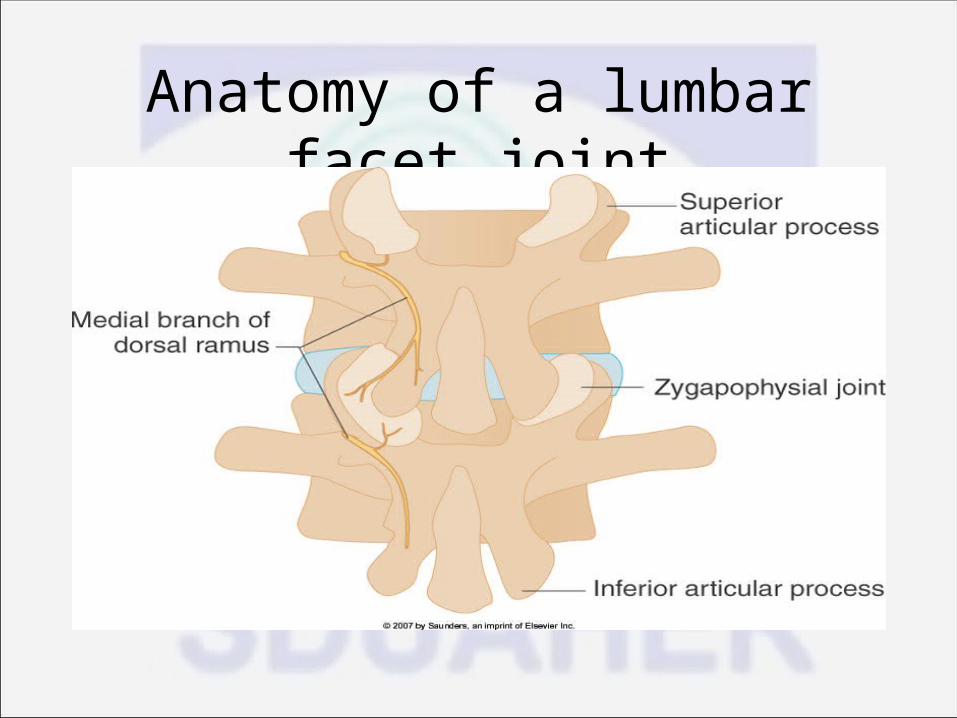
Anatomy of a lumbar facet joint
anatomy Each facet joint is formed by the superior and
inferior articular process of consecutive lumbar vertebra.
Each joint is named by the segmental number of vertebrae that form it.
Each facet joint has the typical structure of a synovial joint
The joints are innervated by the the medial branches of lumbar dorsi rami
History and physical exam There are no discrete history and physical findings
pathognomonic for lumbar facet arthropathy. Some helpful indicators on PEX: 1. Pain not relieved when rising from forward
flexion 2. Pain well relieved by recumbency 3. Pain not exacerbated by coughing 4. Pain not worsened by hyperextension Most often pain is referred to the region of the
buttocks or proximal thigh.
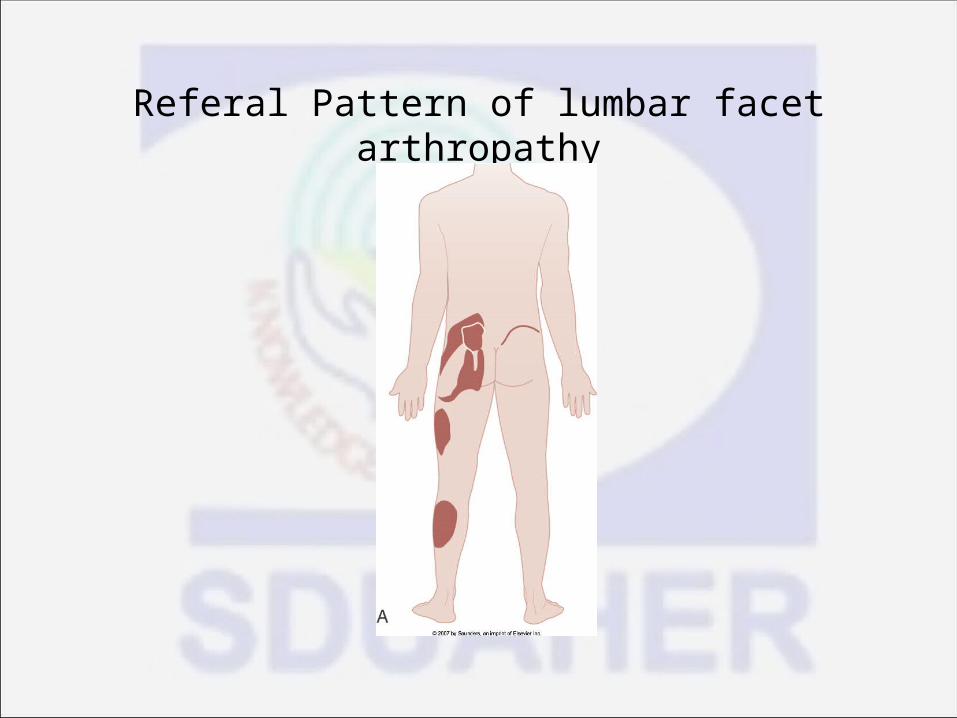
Referal Pattern of lumbar facet arthropathy
Conclusion The Evaluation of low back pain can be a
daunting task The disease possibilities are numerous Diagnostic options are often complicated and
expensive 90% of patients have a mechanical reason for
their low back pain. The remaining 10% have back pain as a
symptom of a systemic illness. The patient’s signs and symptoms often give
clues for this differentiation.
THANK YOU