balance problems in the geriatric patient · balance problems in the geriatric patient dennis e....
TRANSCRIPT
TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
1 | P a g e
Grand Rounds
Balance Problems in the Geriatric Patient Dennis E. Enix, DC, MBA1*; Joseph H. Flaherty, MD2; Kasey Sudkamp, PT, DPT3; Jessica Schulz, OT, MOTR/L4 Address:
1Assistant Professor, Logan College of Chiropractic, Research Division, Chesterfield, MO, USA;
2Associate
Professor of Medicine, Department of Internal Medicine & Division of Geriatrics, Saint Louis University School of Medicine, St. Louis, MO, USA;
3Logan College of Chiropractic, Chesterfield, MO, USA;
4 SSM Rehabilitation Hospital,
St. Louis, MO, USAR Email: Dennis E. Enix, DC, MBA
* Corresponding Author
Topics in Integrative Health Care 2011, Vol. 2(1) ID: 2.1002 Published on March 30, 2011 | Link to Document on the Web
Abstract
Balance problems and falls are common among the elderly and are a leading cause of institutionalization
in this group. Low back pain (LBP) is the most frequently reported musculoskeletal condition in the
elderly and is a leading comorbid factor directly linked to the incidence of falls. Balance disorders in the
geriatric population are often a multifactorial condition. While there is not a single solution to postural
control problems, there is evidence that the most effective treatment strategies for balance disorders
consist of a multimodal approach including a re-evaluation of medications, manual therapy, exercise,
and behavioral modification programs. This case report describes an interdisciplinary approach to the
diagnosis and management of an 85 year old woman with balance problems.
Introduction
Balance problems and falls are common among the elderly and are a leading cause of institutionalization
in this group that result in over five million patient outpatient visits per year. It is estimated that
between 28% and 35% of individuals over age 65 fall each year, with a fifth of those requiring medical
attention.1 The number of fallers increases to over 40% for those 75 and older.1 A history of falling is
also a robust predictor of morbidity among the elderly.2,3
Low back pain (LBP) is the most frequently reported musculoskeletal condition in the elderly, with a

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
2 | P a g e
prevalence ranging from 19.7% in people over the age of 65, to as high as 40 % for individuals over
75.1,2,4 LBP is a leading comorbid factor directly linked to the incidence of falls in the elderly and is
sharply on the rise; LBP prevalence has increased in the last fourteen years from 3.9% to 10.2%.4,5 LBP in
the elderly can involve a wide range of possible diagnoses and co-morbidities, including a high incidence
of malignant or visceral causes and therefore necessitate a close review of systems in addition to the
usual musculoskeletal examination.5,6
Balance disorders in the geriatric population are often a multifactorial condition. Weakness in the core
stabilizing muscles, altered muscle activation patterns, loss of proprioception, and an inability to control
normal postural sway can all result in decreased balance in the elderly.7,8 A decrease in physiological
reserves as we age, limits the ability to react quickly to perturbations. While there is not a single
solution to postural control problems, there is evidence that the most effective treatment strategies for
balance disorders consist of a multimodal approach including a re-evaluation of medications, manual
therapy, exercise, and behavioral modification programs.7,9 This case report describes an
interdisciplinary approach to the diagnosis and management of an 85 year old woman with balance
problems.
History
An 85 year old Caucasian woman with a history of balance problems presented to an outpatient clinic
for evaluation and treatment. This patient’s previous medical history included chronic obstructive
pulmonary disease (COPD), asthma, hypertension, osteoarthritis, and osteoporosis. Her past surgical
history included a total hip arthroplasty (THA) to repair a fractured right femur as the result of a fall in
2004. She also had an open reduction internal fixation of a fracture of her right humerus as a result of a
fall in 2006. She wears an orthotic in her right shoe to accommodate a post-surgical leg length
discrepancy and complains of right foot and leg pain when walking long distances. She has had periodic
transient episodes of mild low back pain which she reports as worse in the morning. Her current
medications include Spiriva (PRN), Trazodone (50 mg qd), Loratadine (10 mg qd), Benzonatate (100mg
qd), Benicar/HCTZ (40/25 mg qd), and Aleve (220 mg PRN).
She lives in an independent living center and is ambulatory with a cane. She voiced concerns about her
steadiness and reported a significant fear of falling again. She denies smoking or alcohol use and reports
a sedentary lifestyle. She drives, but limits her trips to grocery shopping and medical appointments.
She was treated by a physical therapist for 4 weeks following her THA in 2004.
Physical Examination and Diagnostic Test Results
This patient’s vital signs were the following: BP 134/64, pulse 72 bpm, weight 134 lbs, height 66”,
Temperature 97.6° F. Her Achilles tendon reflexes were 1+ bilaterally; patellar reflexes were 1+ on the

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
3 | P a g e
right and 2+ on the left. Dermatomes and myotomes were intact. There was no evidence of
neurological involvement, ataxia, or vestibular problems. There was a 2.0 cm actual leg length
discrepancy on the right. There were bilateral hamstring and piriformis adaptive shortening. Manual
muscle testing revealed 3+/5 in the gluteus medius, 4+/5 in the quadriceps; 4/5 in the iliopsoas, tibialis
anterior, adductors and gluteus maximus muscles bilaterally. Previous MRI’s showed moderate diffuse
degenerative disc disease in the lumbar spine.
Several balance tests were performed with the following results: Tinetti Performance Oriented Mobility
Assessment 16/24 (high fall risk), Berg balance test 37/56 (medium fall risk), and the Timed up and Go
Test required 17.23 seconds (below normal functional independence and high fall risk).
Two computerized balance tests were performed on the NeuroCom Balance Master device including the
Limits of Stability Test (LOS) and the Clinical Test for Sensory Integration of Balance (CTSIB). On the
Limits of Stability Test (LOS), the patient scored below the age adjusted norms for endpoint and max
excursions in the forward, left, and right directions along with exhibiting decreased reaction times and
directional control. In the CTSIB test, the patient scored below the age adjusted norms on the firm
surface with her eyes closed and on the foam surface with both eyes open and eyes closed.
The patient also completed several standardized subjective reports including the following: Tampa Scale
for Kinesiophobia 38/68, Visual analogue scale 2/10, Falls Efficacy Scale 60/100 (moderate fear of
falling), and Oswestry Low Back Pain Questionnaire 28/50. The SF-36 health questionnaire scored a
31.1/100 and 52.8/100 on physical and mental health categories respectively. This demonstrated a
below average functional health personal assessment while the mental portion was within the normal
score set.
Diagnosis
1. Balance deficits
2. Gait abnormality
3. Diffuse degenerative disc disease in the lumbar spine.
Treatment
As discussed earlier, balance problems are often a multifactorial in nature, lacking a single underlying
pathology. Many studies have shown the merit to a team approach when treating individuals with
balance problems.10 An ideal plan of care for this patient should address as many of the contributing
factors as possible. Therefore, treatment options for this patient are discussed from the standpoint of a
chiropractor, a medical physician, a physical therapist and an occupational therapist.
TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
4 | P a g e
Discussant 1
Dennis Enix, DC, MBA is an Assistant Professor at the Logan College of Chiropractic Division of
Research, and the Principal Investigator on a multidisciplinary research collaboration with the VA
Geriatric Research Education and Clinical Center and the Saint Louis University Center Division of
Geriatrics. The three year HRSA funded study examines balance problems and low back pain in the
geriatric population.
This patient’s risk for falls appears to be multifactorial. Her risk for falls is influenced by her overall
posture, decreased flexibility, muscular strength, proprioception and certain medications and is further
complicated by periodic bouts of low back pain. Her high kinesiophobia scores and reported fear of
falling indicate not only a fear of movement and falling but also represent an increased psychological
risk factor for future falls. Sarcopenia and a loss of flexibility and proprioception predispose an
individual to an increased risk of falls and loss of independence. The general health status of this patient
and loss of physiological reserves significantly limits her ability to react quickly in response to small
perturbations. The ability to maintain normal balance is not only a function of the visual, vestibular, and
somatosensory systems but also requires proper sensory-motor integration. Balance testing indicates
that in addition to over or under estimating distances, this patient’s increased postural sway and
decreased reaction time puts her at further risk of falling.
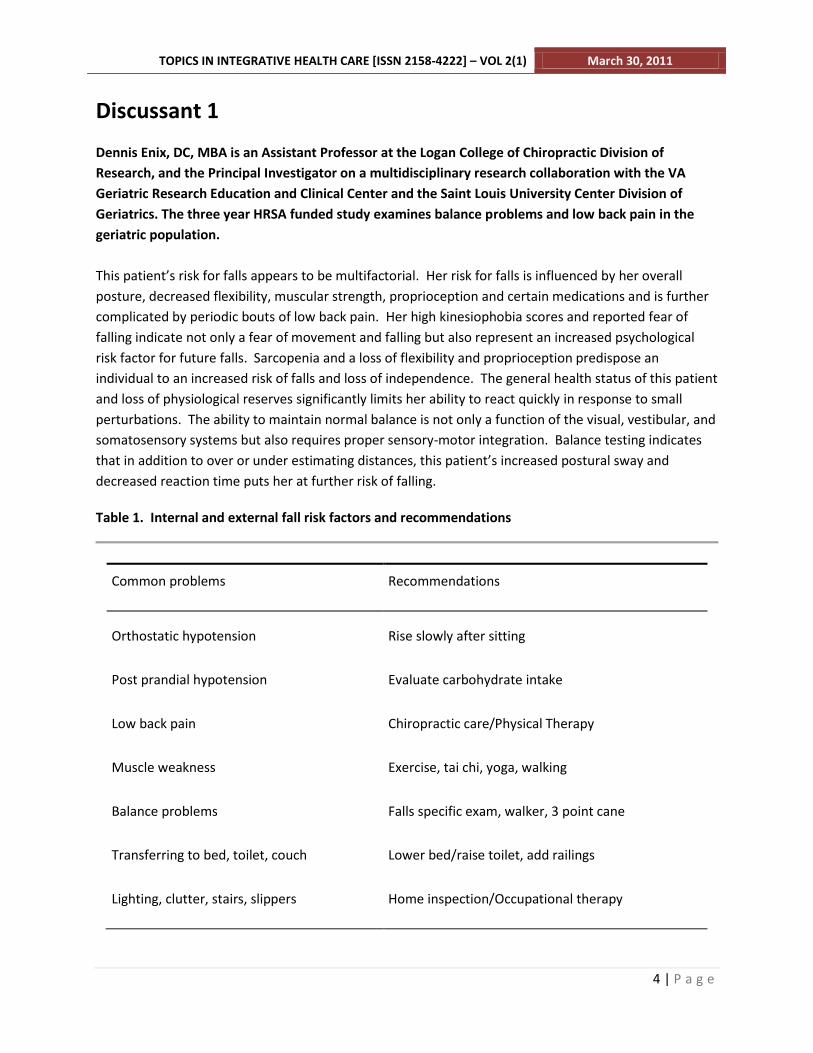
Table 1. Internal and external fall risk factors and recommendations
Common problems Recommendations
Orthostatic hypotension Rise slowly after sitting
Post prandial hypotension Evaluate carbohydrate intake
Low back pain Chiropractic care/Physical Therapy
Muscle weakness Exercise, tai chi, yoga, walking
Balance problems Falls specific exam, walker, 3 point cane
Transferring to bed, toilet, couch Lower bed/raise toilet, add railings
Lighting, clutter, stairs, slippers Home inspection/Occupational therapy

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
5 | P a g e
Common problems Recommendations
Medication increased fall risk Review medications, like psychotropics
Fear of falls/loss of independence Medic-Alert Pendant/bracelet
When working as part of a multispecialty group, it is important to coordinate a plan of care with the
other members of the health care team. Recognizing the strengths within areas of specialization, a
treatment plan tailored to a patient’s specific need increases outcomes (Table 1). From the perspective
of a chiropractor, I would focus on the patient’s complaints of low back pain as it relates to her postural
control problems. People with LBP have a 2-fold greater odds of falling than people without LBP.11 The
pathology of LBP and the related disequilibrium is often multifactorial, including inhibition of core
stabilizing muscles, altered muscle activation patterns, and loss of proprioception resulting in an inability
to control normal postural sway.8,12 This patient’s previous diagnosis of lumbar disc disease and
complaints of intermittent low back pain, loss of flexibility and proprioception make her a good
candidate for manipulative therapy.
In addition to increasing this patients muscle mass, we want to help restore her flexibility, which
includes not only stretching but also joint manipulation and mobilization. The goal of manual therapy
will be to increase the range of motion and joint flexibility while decreasing the patients low back pain
and nociception. Sixty percent of our balance comes from the somatosensory system. Manipulation has
been shown to create both biomechanical and neurological changes. Along with decreases in pain and
the production of substance P, manipulation has been shown to increase ranges of motion, change
functional muscle activation patterns and increase postural control in patients with LBP.13,14
Given her past surgical history of THA to repair a fractured right femur and humerus, and the resultant
post-surgical leg length discrepancy, examination of the pelvis may reveal asymmetries that would
respond well to manual therapy. Along with asymmetrical positioning of the pelvis, altered muscle firing
patterns from LBP respond well to manipulation. Manipulation of the feet and ankles in elderly adults
has also been shown to partially compensate for postural control changes by stabilizing postural sway.15
When appropriately screened for treatment with a clinical prediction rule, the benefit of manipulative
therapy increases to a 92% chance of successful outcome. The minimum number of treatments per
week needed to show a benefit at 4 weeks is 1.9.16 The cost effectiveness of chiropractic manipulation
for LBP is equivalent to standard medical and other forms of therapy including hospital outpatient
services.17 While an effective treatment and competitive from the standpoint of a cost model,
chiropractic care remains an underutilized therapy among this age cohort. There is strong evidence that
a multifactorial program of therapy is an effective treatment for LBP in older adults.17 With this

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
6 | P a g e
patient’s complex past medical history and current clinical presentation, coordination of her care within
a multispecialty group ensures not only more accurate diagnosis but better outcomes.
References:
1. Blake AJ, Morgan K, Bendall MJ, Dalloso H, Ebrahim S, Arie T, et al. Falls by elderly people at home:
prevalence and associated factors. Age Ageing 1988;17:365-72.
2. Prudham D, Evans Grimley J. Factors associated with falls in the elderly: a community study. Age
Ageing 1981;10:141-6.
3. Rao SS, Prevention of falls in older patients. Am Fam Physician 2005;72: 81-8, 93-4.
4. Jacobs JJ, Andersson GBJ, Bell JE, Weinstein SL, Dormans JP, Gnatz SM, Lane N, Puzas EJ, St. Clair WE.
United States Bone & Joint Decade: The Burden of Musculoskeletal Diseases in the United States.
Rosemont, IL: American Academy of Orthopaedic Surgeons. 2008. ISBN 978-0-89203-533-5
5. Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, Castel LD, Kalsbeek WD,
Carey TS. The rising prevalence of chronic low back pain. Arch Intern Med 2009;169(3):251-258.
6. Bressler A, Hartley B. The prevalence of low back pain in the elderly: a systematic review of the
literature. Spine 1999;24:1813-1819.
7. Barnett A, Smith B, Lord S, Williams M, Baumand A: Community-based group exercise improves
balance and reduces falls in at-risk older people: a randomized controlled trial. Age Ageing 2003;32:
407–414.
8. Sterling M, Jull G, Wright A. The effect of musculoskeletal pain on motor activity and control. J Pain
2001;2(3):135-45.
9. Chang JT, Morton SC, Rubenstein LZ, Mojica WA, Maglione M, Suttorp M Interventions for the
prevention of falls in older adults: systematic review and meta-anaylsis of randomized clinical trials. BMJ
2004;328 680- 688.
10. Dagenais S, Mayer J, Mooney V. Evidence-informed management of chronic low back pain with
lumbar extensor strengthening exercises. Spine J 2008;8:96-113.
11. Hicks GE, Gaines JM, Shardell M, Simonsick EM. Associations of back and leg pain with health status
and functional capacity of older adults: findings from the retirement community back pain study.
Arthritis Rheum 2008;59(9):1306-13.
12. Brumagne S, Cordo P, Lysens R, et al. The role of paraspinal muscle spindles in lumbosacral position
sense in individuals with and without low back pain. Spine 2000; 25:989–994.
13. Anderson R, Meeker W, Wirick B, Mootz R, Kirk D, Adams A. A meta-analysis of clinical trials of spinal
manipulation. J Manipulative Physiol Ther 1992;15:181-94.
14. Sung PS, Kang YM, Pickar JG. Effect of spinal manipulation duration on low threshold
mechanoreceptors in lumbar paraspinal muscles. Spine 2004;30(1):115-22.
15. Vaillant J, Vuillerme N, Janvy A, Louis F, Braujou R, Juvin R, Nougier V. Effect of manipulation of the
feet and ankles on postural 1 control in elderly adults. Brain Res Bull 2008, 31;75(1):18-22.
16. Childs J D, Fritz J M, Flynn T W, Irrgang J, Johnson K, Majkowski G R, Delitto A. A clinical prediction
rule to identify patients with low back pain most likely to benefit from spinal manipulation: A validation
study. Ann Intern Med 2004;141:920-928.
17. Meade TW, Dyer S, Browne W, Frank AO. Randomized comparison of chiropractic and hospital
TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
7 | P a g e
outpatient management for low back pain: results from extended follow up. BMJ 1995;311(7001):349-
51.
Discussant 2
Joseph Flaherty, MD is a Professor of Medicine at Saint Louis University School of Medicine and the
VA Geriatric Research Education and Clinical Center.
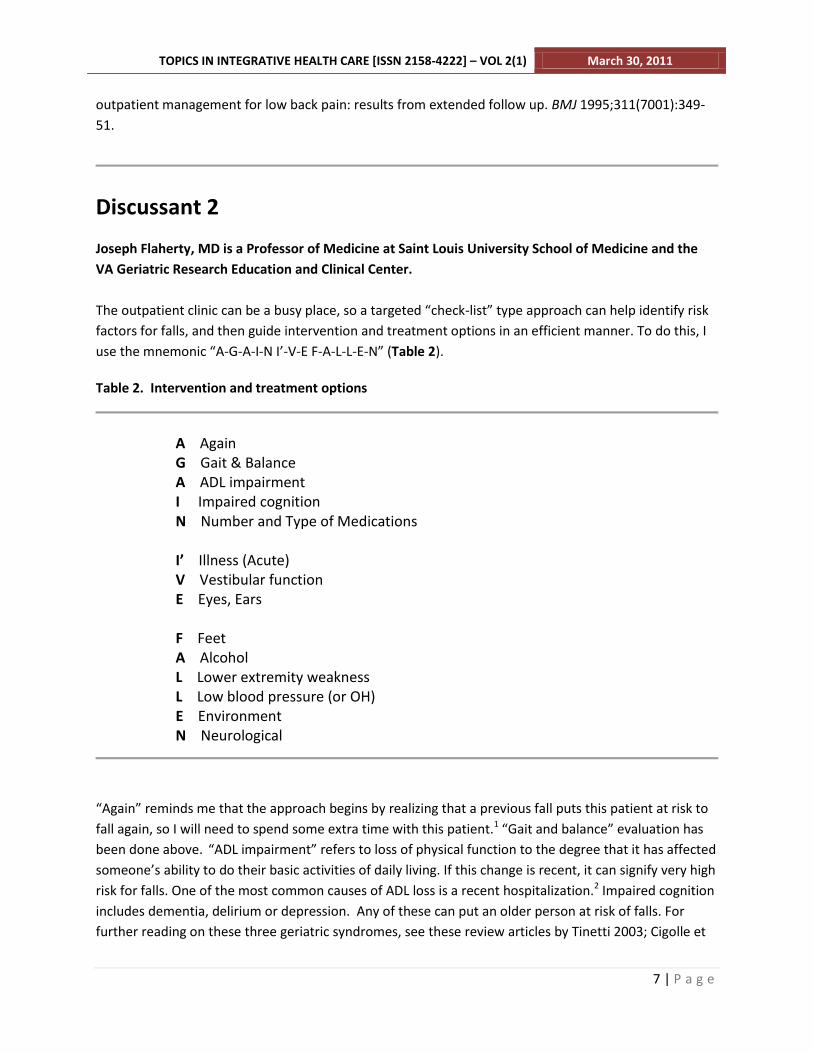
The outpatient clinic can be a busy place, so a targeted “check-list” type approach can help identify risk
factors for falls, and then guide intervention and treatment options in an efficient manner. To do this, I
use the mnemonic “A-G-A-I-N I’-V-E F-A-L-L-E-N” (Table 2).
Table 2. Intervention and treatment options
A Again G Gait & Balance A ADL impairment I Impaired cognition N Number and Type of Medications I’ Illness (Acute) V Vestibular function E Eyes, Ears F Feet A Alcohol L Lower extremity weakness L Low blood pressure (or OH) E Environment N Neurological
“Again” reminds me that the approach begins by realizing that a previous fall puts this patient at risk to
fall again, so I will need to spend some extra time with this patient.1 “Gait and balance” evaluation has
been done above. “ADL impairment” refers to loss of physical function to the degree that it has affected
someone’s ability to do their basic activities of daily living. If this change is recent, it can signify very high
risk for falls. One of the most common causes of ADL loss is a recent hospitalization.2 Impaired cognition
includes dementia, delirium or depression. Any of these can put an older person at risk of falls. For
further reading on these three geriatric syndromes, see these review articles by Tinetti 2003; Cigolle et

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
8 | P a g e
al. 2007 and Harlein et al. 2009.3,4,5 The number and type of drugs are some of the most important risk
factors for falls. Taking >4 drugs is a risk factor by itself.6 Certain types of drugs will also increase risk. In
a meta-analysis of 40 observational studies comparing fallers to non-fallers, the following psychotropic
medications had increased odds ratio [(OR) (95% confidence interval)]: any psychotropic use [1.73 (1.52-
1.97)], neuroleptics [1.66 (1.38-2.00)], sedative/hypnotics [1.54 (1.40-1.70)], any antidepressant [1.66
(1.4-1.95)], benzodiazepines [1.48(1.23-1.77)].7
“Illness” indicates that acute as well as subtle illness can contribute to risk for falls. For example,
someone with a mild anemia might continue to drop their blood count over time so slowly that the first
symptom might be weakness and a fall.3 The fall might be what brings them to the emergency room.
Vestibular function changes with age. There may be an age-related decline in balance due to
accumulation of minute calciferous granules within the stratoconic membrane, which could lead to
vestibular dysfunction.3 Impaired vision, more so than impaired hearing, contribute to risk of falls. In
addition, bifocals increase risk for falls. Cerumen is not only a common cause of hearing impairment,
but if impacted, it can affect balance.3
Foot problems that can affect balance include calluses, bunions, poorly fitting shoes and thick or long
toenails. Alcohol can affect balance. Lower extremity weakness is one of the strongest predictors of falls,
increasing risk anywhere from 2 to 8 times compared to people without weakness. It is important to test
for lower extremity weakness in a dynamic way by doing the “5 sit to stand” with arms crossed.3,8,9 Low
blood pressure can occur if someone is dehydrated or just overtreated with antihypertensive
medications. “OH” stands for orthostatic hypotension. This is a drop in systolic blood pressure of 20
mmHg or diastolic of 10 mmHg when going from a sitting to standing position. Environmental causes
such as throw rugs in the home, or pets, should be queried about. Lastly, neurological problems as risk
factors should be considered, such as peripheral neuropathy.
As these apply to our patient, we already know she has a gait and balance problem, so physical therapy
evaluation is in order. She has no obvious ADL impairment, but if it takes her longer to do her ADLs than
usual, an occupational therapist might be beneficial. We should screen our patient for dementia with a
tool like the Saint Louis University Mental Status Exam, which is better than the traditional mini-mental
status exam at picking up mild cognitive impairments.10 Depression can be screened for in just a few
minutes using something like the Geriatric Depression Scale.11 Although treatment with antidepressants
carries some risk for falls, depression is associated with several other negative outcomes in addition to
falls, so it should be treated. Delirium typically occurs in hospitalized patients, and to a lesser extent,
nursing homes, so this may not apply to our patient unless she gets hospitalized. On review of her meds,
the goal would be to get her to 4 or fewer. We should investigate the need for trazodone and
loratadine, and consider stopping them if possible. We’ll address the Benicar/HCTZ below.
It does not seem that she has an acute or subtle illness, but keeping a relatively high index of suspicion
would be prudent. We should check her vision, and look in her ears. Most importantly, we could have
her do 5 “sit to stands” with her arms crossed. If she cannot do this, referring her to PT for leg
strengthening exercises would be indicated. Her blood pressure might be considered on the low side for

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
9 | P a g e
her age, and we should definitely check her blood pressure not just sitting, but standing. If OH is
present, I would either stop or at least cut back her Benicar/HCTZ. Lastly, if she had fallen at home, I
would consider ordering a home care evaluation (by an OT) to examine her environmental risks for falls.
References
1. Blake AJ, Morgan K, Bendall MJ, Dalloso H, Ebrahim S, Arie T. Falls by elderly people at home:
prevalence and associated factors. Age Ageing 1988; 17:365-72.
2. Sager M A, Franke T, Inouye S K, Landefeld C S, Morgan T M, Rudberg M A, Siebens H, Winograd C H.
Functional outcomes of acute medical illness and hospitalization in older persons. Arch Intern Med
1996; 156(6):645-652.
3. Tinetti M E, Speechley M, Ginter S F. Risk factors for falls among elderly persons living in the
community. N Engl J Med 1988; 319:1701-1707.
4. Cigolle C T, Langa K M, Kabeto M U, Tian Z, Blaum C S. Geriatric conditions and disability: the health
and retirement study. Ann Intern Med 2007;147:156-164.
5. Harlein J, Dassen T, Halfens R J G, Heinze C. Fall risk factors in older people with dementia or
cognitive impairment: a systematic review. J Adv Nursing 2009 65:5, 922–33.
6. Tinetti M E. Preventing falls in elderly persons. N Engl J Med 2003; 348:42-49 1:2.
7. Leipzig R M, Cumming R G, Tinetti M E. Drugs and falls in older people: a systematic review and meta-
analysis: I. Psychotropic drugs. J Am Geriatr Soc 1999,47:30-39
8. Robbins A S, Rubenstein L Z, Josephson K R, Schulman B L, Osterweil D, Fine G. Predictors of falls
among elderly people: results of two population based studies. Arch Intern Med 1989 149(7):1628-33.
9. Tinetti M E, Williams T F, Mayewski R. Fall risk index for elderly patients based on number of chronic
disabilities. Am J Med 1986;80(3):429-34.
10. Tariq S H, Tumosa N, Chibnall J T, Perry M H, Morley J E. Comparison of the Saint Louis University
Mental Status Examination and the Mini-Mental State Examination for detecting dementia and mild
neurocognitive disorder: a pilot study. Am J Ger Psych 2006;14:11, 900-10.
11. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, Leirer VO. Development and validation of a
geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982-1983;17(1):37-49.
Discussant 3
Kasey Sudkamp, PT, DPT is a Physical Therapist involved with the HRSA funded geriatric balance and
low back pain study.
As a physical therapist, treatment of balance disorders, especially in the geriatric population, is an
important aspect of my profession. The elderly represent more than one third of all hospital injury
admissions, and more than 80% of these injuries are caused by unintentional falls.1 These falls are the
leading cause of nonfatal injuries requiring medical attention in the United States.2
TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
10 | P a g e
As we age, changes in the body’s systems affect our mobility and balance. The dynamic equilibrium
model shows that both sensory and motor components determine our ability to maintain balance3. The
sensory portion of the balance system is composed of 3 areas: vestibular, visual, and
somatosensory/proprioception.3 The motor portion of the equilibrium consists of our bodies’ ability to
act on the sensory information provided using muscle contractile patterns and synergies. While balance
disorders are often multifactorial in nature, the goal in management is to minimize physical disability
and improve functional performance.
In order to develop a patient-specific treatment plan, a thorough evaluation of the neuromuscular and
musculoskeletal systems is needed. Limitations imposed by range of motion deficits, muscle weakness,
poor muscle endurance, and pain affect the ability to maintain dynamic equilibrium. Based on the
subjective and objective measures listed in the patient history, I would focus on the muscle strength
deficits, the adaptive shortening of one and specifically two joint muscles, the pain complaints, and her
overall lack of postural control and motor coordination. The optimal initial treatment frequency is 2-3
times per week for 4-6 weeks.
Ankle, hip, and stepping strategies are our body’s way to manage the amount of sway during specific
activities. If range of motion and strength is reduced in the leg and trunk joints, then the ability to
correctly activate and use these strategies is decreased. I would choose light resistive exercises involving
Theraband and gravitational pull to strengthen the hip, knee, and ankle musculature with specific focus
on the gluteus medius and the tibialis anterior. The exercises chosen should strengthen throughout the
entire available range of motion as well as use concentric and eccentric contractions. Static as well as
dynamic stretching of the rectus femoris, piriformis, and hamstrings will also be performed during the
treatment regimen.
To improve the coordination and efficiency of translating the patient’s sensory signals into motor
control actions, a controlled instability environment is extremely helpful4. It requires putting the patient
in a safe environment while at the same time challenging her base of support limits. This can be done in
a variety of ways including stance activities on different supportive surfaces and varying the use of her
upper extremities to assist her stability during standing exercises. Single leg stance work also fits into
this category. Based on her NeuroCom CTSIB scores, the patient relies heavily on her vision and
proprioception to maintain balance. Thus, having her perform standing activities with her eyes closed
along with using unstable surface platforms (foam), will encourage activation of the vestibular system
and reinforce her movement compensation strategies.
The patient’s low back pain complaints appear consistent with osteoarthritis and her diagnosis of
degenerative disc disease. A lumbar stabilization exercise program can address both her pain and
improve her postural control, which are important components in the balance algorithm. Any sudden
increase in pain might require ultrasound, trigger point release, mobilization, and activity adjustment.
Finally, education is an important key when treating balance deficits in the elderly. Most falls happen in
the home5 so instruction on the necessity to reduce tripping hazards such as clutter, poor lighting,

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
11 | P a g e
electric cords or throw rugs is important. The patient should also be made aware of other factors that
put her at increased risk for falling such as performing activities that force her outside of a comfort level
of stability i.e. carrying heavy objects, changing a light bulb, climbing a ladder. This patient’s current
assistive device for gait is a single point cane, and while that may give her a small increase in base of
support, a two or four wheeled walker can provide even more gait steadiness until she feels some
improvement. A simple yet effective home exercise program is also imperative for rehabilitation
success. In order for the patient to maintain any advances she made during her physical therapy
sessions, she will need to have been instructed on a daily exercise program that is easily followed.
References
1. Greenwald BD, Burnett DM, Miller MA. Congenital and acquired brain njury. 1. brain Injury:
epidemiology and pathophysiology. Arch Phys Med Rehabil 2003;84(Suppl 1):S3-S7
2. Adams PF, Dey AN, Vickerie JL. (2007). Summary health statistics for the U.S. population: National
Health Interview Survey, 2005. Vital and Health Statistics 2007;Series 10(233):1–104.
3. Nashner LM: Sensory, neuromuscular and biomechanical contributions to human balance. Proc Forum
Amer Phys Ther Assoc. Nashville: Amer Phys Ther Assoc, 1989:5-12.
4. Wulf G, Landers M, Lewthwaite R, Tollner T. External focus instructions reduce postural instability in
individuals with Parkinson disease. Phys Ther 2009;89:162–168.
5. Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults:
systematic review and meta-analysis of randomized clinical trials. BMJ 2004; 328:680.
Discussant 4
Jessica Schulz, MOTR/L is an Occupational Therapist at the SSM Rehabilitation Hospital in St. Louis,
MO.
The goal of an Occupational Therapist (OT) treating balance disorders is to address one’s physical,
cognitive, psychosocial, and sensory aspects of their life in order to enhance independence, well being,
and quality of life.2 Older adults and elderly make up a high percentage of people OTs evaluate and
treat on a daily basis. Falls are the leading cause of injury and accidental death in adults over the age of
65.1 A fall can cause a dramatic change to an older adult’s life; reducing mobility, strength, and
functional endurance.4
Treatment of balance disorders is an important aspect of working with older adults. Evaluation of person
and home are significant in order to best treat the older adult. An OT would evaluate one’s Activities of
Daily Living, such as whether they stand up or sit while putting on pants, as well as their Instrumental
Activities of Daily Living, such as cooking while standing up at the stove, to assess their strengths and
weaknesses.4

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
12 | P a g e
Assessment and modification of the home environment by an OT can significantly reduce the number of
falls in older adults.3,5 Assessment and modification of one’s home is an important step in implementing
a safe foundation.4
There are many ways to adapt one’s environment to help protect people with balance disorders from
falls. Bathrooms have a tendency to be wet and slippery, therefore increasing the risk of falls.
Appropriate rugs that will safeguard the patient from slips and trips are the first and most efficient step;
they should be advised to discard throw rugs and get flat, non-slip rugs.1 Grab bars, shower chairs, hand
held shower heads, and raised toilet seats are durable medical equipment that will safeguard many
people from unnecessary falls. In the kitchen, safety improvements include storing food in easy-to-reach
places and setting up cooking tasks sitting down. In hallways, create clear pathways free from thick
carpeting or rugs and install handrails if necessary. In the bedroom, create clear pathways as well as
assess the bed’s height to ensure safety getting into and out of bed. Bedside commodes next to one’s
bed at night are a way to decrease the risk of falls in case of urgency in the middle of the night.1
OT treatments for balance disorders and fall prevention include increasing postural stability/strength,
upper extremity strength/endurance, proprioceptive awareness, and safe functional mobility.3
Functional standing tasks during an Instrumental Activity of Daily Living, such as emptying the
dishwasher, can promote dynamic standing strength and proprioceptive awareness as well as increase
strength and endurance in postural muscles. This task also allows the OT to assess when the patient is
fatiguing and educate him or her on energy conservation/safety techniques. Activities of Daily Living
that require dynamic standing balance, such as lower body dressing and bathing tasks, are also
functional ways to increase balance and safety as well as independence.3
The use of adaptive equipment has been associated with promoting safety and independence in an
older adult.4 A reacher is a piece of adaptive equipment that allows one to clasp onto pants and pull
them up to the thighs, allowing for safer dressing. The reacher is also used as adaptive equipment while
walking with a wheeled-walker. A reacher is hung conveniently on the wheeled walker in order to safely
pick up dropped items from the floor.
Finally, it is very important to educate the patient and family/caregivers on fall prevention techniques
and home modification suggestions. A study completed by Wyman, et al., revealed that home
modification education and individual counseling led to significant safety changes in older women at risk
for falling.6 Educating patients on proper medication schedules is also very important.3,4 If not taken
correctly, dizziness and loss of balance may occur. An OT can educate older adults on their medications
and help them use a weekly medication organizer, if needed. It is important that the patient
understands the value of following home safety techniques and the simple home exercise plan in order
to maximize the benefits of the OT sessions.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 2(1) March 30, 2011
13 | P a g e
References:
1. American Occupational Therapy Association. American Occupational Therapy Association, Inc Page.
http://www.aota.org/Consumers/consumers/Adults/Falls/35156.aspx. Updated March 16, 2007.
Accessed March 9, 2011.
2. American Occupational Therapy Association. Policy 5.3.1: Definition of occupational therapy practice
for State Regulation. Amer J Occupational Ther 2004;58:694-695.
3. Di Monaco M, Vallero F, De Toma E, De Lauson L, Tappero R, Cavanna A. A single home visit by an
Occuaptional Therapist reduces the risk of falling after hip fracture in eldery women: A quasi-
randomized controlled trail. J Rehabil Med 2008;40(6):446-50.
4. Leland N, Porell F, Murphy S. Does fall history influence residential adjustments? The Gerontologist
2010; 51:190-200.
5. Pighills A, Torgerson D, Sheldon T, Drummond A, Bland J. Environmental assessment and modification
to prevent falls in older adults. J Amer Geriatr Soc 2007.
6. Wyman J, Croghan C, Nachreiner N, Gross C, Stock H, Talley K, Monigold M. Effectiveness of
education and individualized counseling in reducing environmental hazards in the homes of community-
dwelling older women. J Amer Geriatr Soc 2007; 55: 1548-1556.
Conclusion
Older adults represent the fastest growing population segment, but research into age-related conditions
such as LBP has failed to keep pace with this growth5. Progress is dependent on a number of factors
including treatment regimen, frequency of care, patient motivation, catastrophizing behavior, as well as
the number of comorbidities present. Geriatric studies are under-represented in the back pain
literature and there is a need to improve epidemiologic reporting of LBP in the elderly6.