baloch asc companion society uscap presentationhandouts.uscap.org/2016_cm24_baloc_1.pdfconcept of...
TRANSCRIPT

4/11/2016
1
The New Diagnostic Paradigms in Thyroid Surgical Pathology and
Affects on Reporting of Thyroid Fine-Needle Aspiration Specimens
Deliberations, Criticisms & DiscussionsZubair W. Baloch, MD, PhD.
Professor of Pathology & Laboratory MedicineUniversity of Pennsylvania Medical Center
Perelman School of MedicinePhiladelphia, PA, USA
ACCME/DisclosuresNo Conflicts
Questions to Myself?
4/11/2016
2
How Can I Find Relevance of My Practice of Cytopathology in a
Landscape That Won’t Stop Shifting?
Let’s Make Sense of Present &
Predict Future
In Light of Past
A Quick Look Back at 2007
The Birth of
“Bethesda System of Reporting Thyroid FNA”

4/11/2016
3
Proposals, Recommendations& Accomplishments
• Proposed Tiered Classification Scheme– Spanning the spectrum of benign to malignant diagnoses
• Inclusive of “Gray Zone” in both cytologic and surgical pathology diagnoses
– Implied risk of malignancy based on available literature review
– A thoughtful process to recommendations inclusive of everyday practice of cytopathology and thyroid nodule management (courtesy of clinical colleagues)
Thyroid FNA Bethesda Classification Scheme
The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC): Implied Risk of Malignancy and Recommended Clinical Management
Diagnostic Category Risk of Malignancy (%)
Usual Management
Non-diagnostic or Unsatisfactory Repeat FNA with ultrasound guidance
Benign 0-3% Clinical follow-up
Atypia of Undetermined Significance or Follicular Lesion of Undetermined
Significance (AUS/FLUS)
~ 5-15% Repeat FNA
Follicular Neoplasm or Suspicious for a Follicular Neoplasm (Specify if Hurthle
type or Oncocytic)
15-30% Surgical lobectomy
Suspicious for Malignancy 60-75% Near-total thyroidectomy or surgical lobectomy
Malignant 97-99% Near-total thyroidectomy
The Timing of TBSRTC TBSRTC
Growing Body of Literature Showing Inconsistencies in Surgical Pathology Diagnosis of Thyroid Cancer Among
Experts – Encapsulated Follicular Variant of PTCThe Cytology Gold Standard is not so Gold
4/11/2016
4
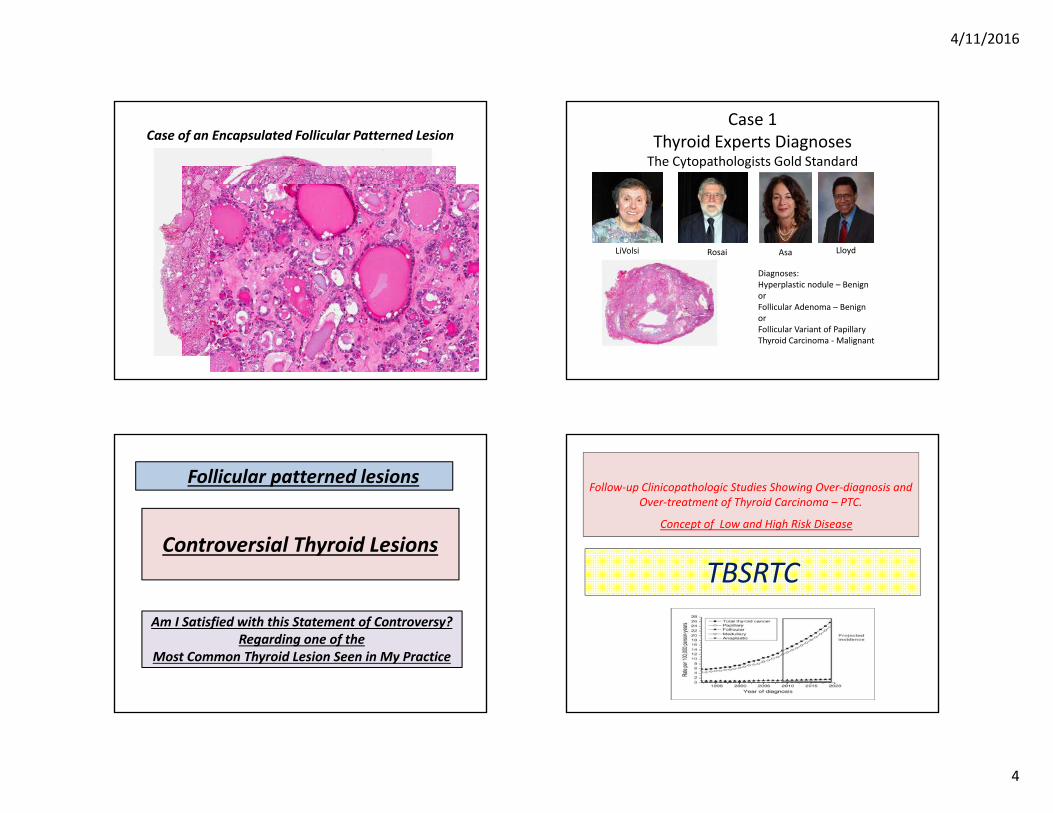
Case of an Encapsulated Follicular Patterned LesionCase 1
Thyroid Experts DiagnosesThe Cytopathologists Gold Standard
Diagnoses: Hyperplastic nodule – BenignorFollicular Adenoma – Benignor Follicular Variant of Papillary Thyroid Carcinoma ‐Malignant
LiVolsi Rosai Asa Lloyd
Controversial Thyroid Lesions
Follicular patterned lesions
Am I Satisfied with this Statement of Controversy? Regarding one of the
Most Common Thyroid Lesion Seen in My Practice
TBSRTC
Follow‐up Clinicopathologic Studies Showing Over‐diagnosis and Over‐treatment of Thyroid Carcinoma – PTC.
Concept of Low and High Risk Disease

4/11/2016
5
TBSRTC
Clinical and Radiology GuidelinesAmerican & European Thyroid Association
American College of RadiologyAmerican Society of Radiologist in Ultrasound
TBSRTCMolecular Profiling of Thyroid Tumors
+Molecular Diagnosis of Thyroid Nodules
Diagnostic Tests with High Negative and Positive Predictive Value
Mutational Analysis Gene Expression Classifier Next Gene Sequencing
TBSRTC
Growing Body of Literature Showing Inconsistencies in Surgical Pathology Diagnosis of Thyroid Cancer Among Experts – Encapsulated Follicular Variant
The Cytology Gold Standard is not so Gold
Follow‐up Clinicopathologic Studies Showing Over‐diagnosis and Over‐treatment of Thyroid Carcinoma – PTC.Concept of Low and High Risk Disease
Clinical and Radiology GuidelinesAmerican & European Thyroid Association
American College of RadiologyAmerican Society of Radiologist in Ultrasound
Molecular Profiling of Thyroid TumorsMolecular Diagnosis of Thyroid Nodules
Diagnostic Tests with high Negative and Positive Predictive Value
TBSRTC
The Aftermath
4/11/2016
6
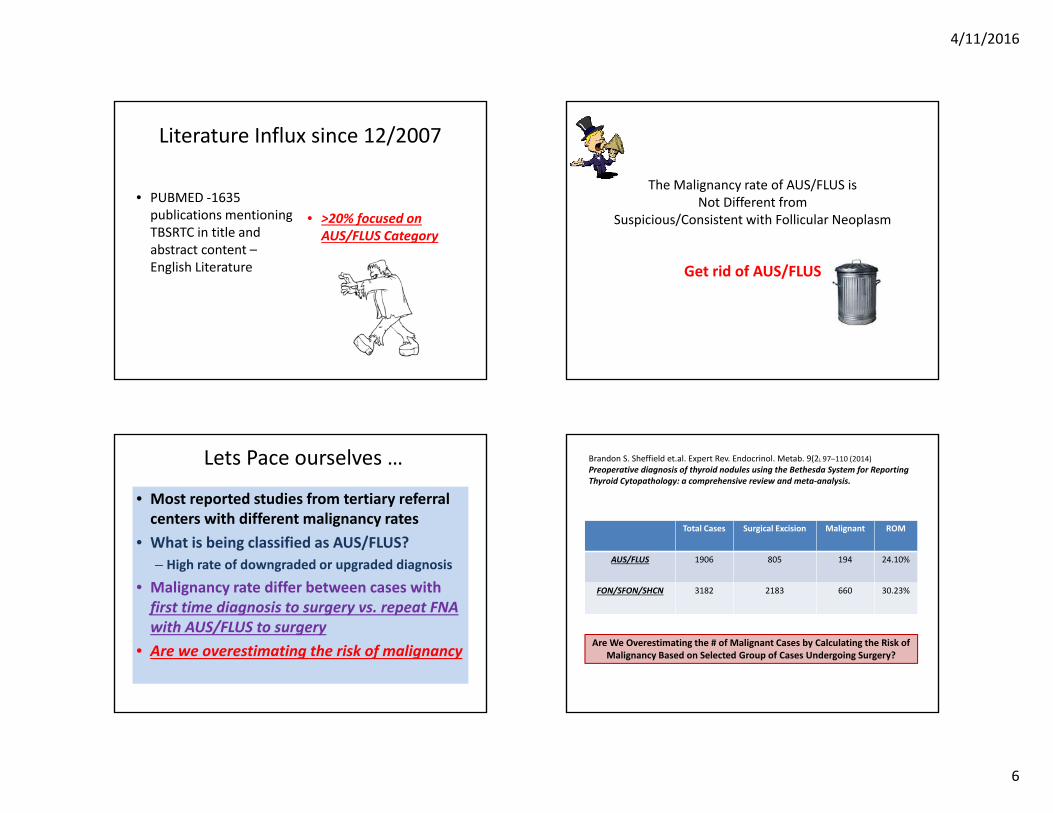
Literature Influx since 12/2007
• PUBMED ‐1635 publications mentioning TBSRTC in title and abstract content –English Literature
• >20% focused on AUS/FLUS Category
The Malignancy rate of AUS/FLUS is Not Different from
Suspicious/Consistent with Follicular Neoplasm
Get rid of AUS/FLUS
Lets Pace ourselves …
• Most reported studies from tertiary referral centers with different malignancy rates
• What is being classified as AUS/FLUS?– High rate of downgraded or upgraded diagnosis
• Malignancy rate differ between cases with first time diagnosis to surgery vs. repeat FNA with AUS/FLUS to surgery
• Are we overestimating the risk of malignancy
Brandon S. Sheffield et.al. Expert Rev. Endocrinol. Metab. 9(2), 97–110 (2014)Preoperative diagnosis of thyroid nodules using the Bethesda System for ReportingThyroid Cytopathology: a comprehensive review and meta‐analysis.
Total Cases Surgical Excision Malignant ROM
AUS/FLUS 1906 805 194 24.10%
FON/SFON/SHCN 3182 2183 660 30.23%
Are We Overestimating the # of Malignant Cases by Calculating the Risk of Malignancy Based on Selected Group of Cases Undergoing Surgery?

4/11/2016
7
Brandon S. Sheffield et.al. Expert Rev. Endocrinol. Metab. 9(2), 97–110 (2014)Preoperative diagnosis of thyroid nodules using the Bethesda System for ReportingThyroid Cytopathology: a comprehensive review and meta‐analysis.
Total Cases
Surgical Excision Malignant ROM OROM
AUS/FLUS 1906 805 194 24.10% 10%
FON/SFON/SHCN 3182 2183 660 30.23% 21%
Can we Calculate Overall Risk of Malignancy (OROM)?
There is More to How Thyroid Nodules are Managed Then Just Cytologic Diagnosis
Reality Check
Thyroid Nodule Management ParadigmsAka
Personalized Approach
Clinical Presentation+
Ultrasound+
FNA Diagnosis+
Molecular Testing
Molecular Tests
vs.Clinical Application & Practice

4/11/2016
8
Increase rate of Suspicious GEC ‐Afirma Results in Oncocytic Nodules
Suspicious nodules wsurgery
Benign Malignant
Harell et al. Endo Pract 2014 30 13 (43%)‐ 9 (69%) oncocytic lesions
17 (57%)
McIver et al. JCEM 2014 32 27 (84%)‐ 12 (44%) oncocytic lesions
5 (16%)
Brauner et al. Thyroid 2015 43* 37 (84%) 6(14%)
Lastra et al. Cancer Cytopath2014
48 26 (54%)‐ 15 (58%) oncocytic lesions
22(46%)
Total 153 103 (67%)‐73 (71%) oncocytic lesions
50 (33%)
Next‐Generation Sequencing AssayNikiforov et al. Cancer 2014,120:3627‐34
Changes in Surgical Pathology Diagnosis / Classification of “Low Risk Tumor(s)”
Concordant with How the Thyroid Cancer Staging is Perceived by our Clinical Colleagues
Application of One Management Paradigm for all Patients with Thyroid Carcinoma The Concept of Static vs. Dynamic Staging System AKA Personalized Approach
The Endocrine Society Working Group for Re‐evaluationof the Encapsulated Follicular Variant of Papillary Thyroid Carcinoma
Project Goals• Review a cohort of cases by experts in the field of endocrine pathology• Establish a consensus on diagnostic histologic criteria• Define the risk of adverse events based on long follow‐up• Recommend new terminology that reflects tumor biology and patient outcome
4/11/2016
9
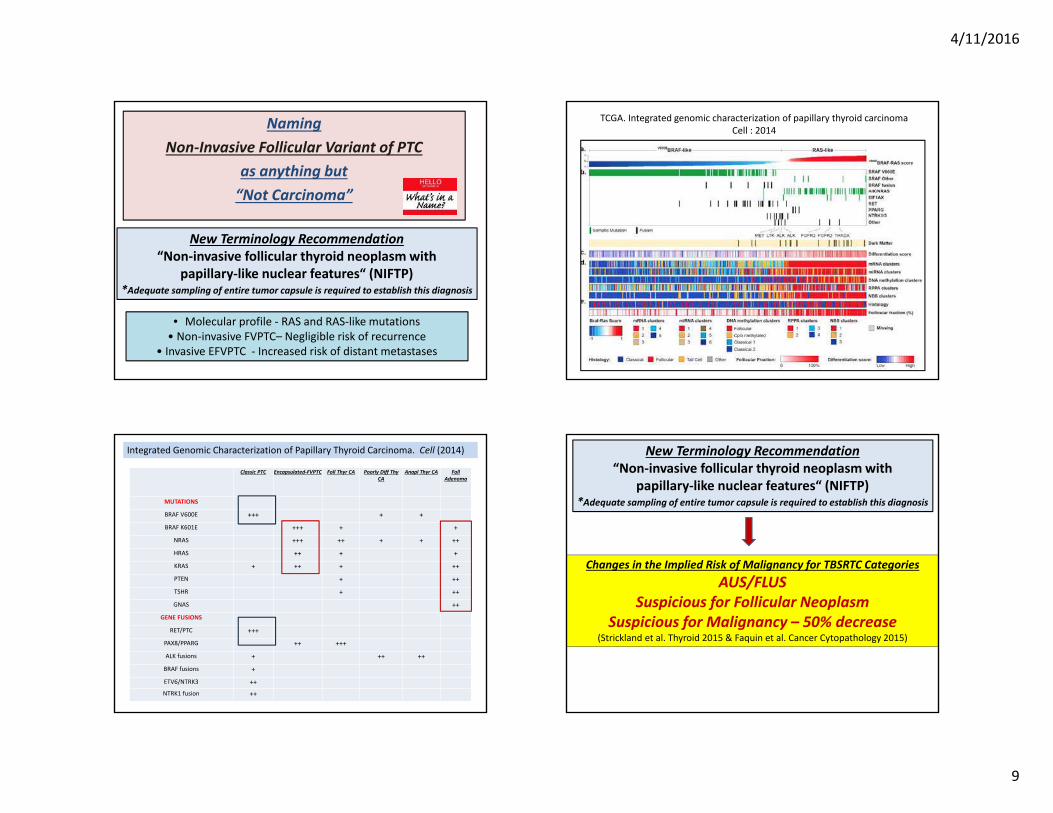
Naming Non‐Invasive Follicular Variant of PTC
as anything but“Not Carcinoma”
New Terminology Recommendation“Non‐invasive follicular thyroid neoplasm with
papillary‐like nuclear features“ (NIFTP)*Adequate sampling of entire tumor capsule is required to establish this diagnosis
• Molecular profile ‐ RAS and RAS‐like mutations• Non‐invasive FVPTC– Negligible risk of recurrence
• Invasive EFVPTC ‐ Increased risk of distant metastases
TCGA. Integrated genomic characterization of papillary thyroid carcinoma Cell : 2014
Classic PTC Encapsulated‐FVPTC Foll Thyr CA Poorly Diff Thy CA
Anapl Thyr CA FollAdenoma
MUTATIONS
BRAF V600E +++ + +
BRAF K601E +++ + +
NRAS +++ ++ + + ++
HRAS ++ + +
KRAS + ++ + ++
PTEN + ++
TSHR + ++
GNAS ++
GENE FUSIONS
RET/PTC +++
PAX8/PPARG ++ +++
ALK fusions + ++ ++
BRAF fusions +
ETV6/NTRK3 ++NTRK1 fusion ++
Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell (2014)
Changes in the Implied Risk of Malignancy for TBSRTC CategoriesAUS/FLUS
Suspicious for Follicular NeoplasmSuspicious for Malignancy – 50% decrease
(Strickland et al. Thyroid 2015 & Faquin et al. Cancer Cytopathology 2015)
New Terminology Recommendation“Non‐invasive follicular thyroid neoplasm with
papillary‐like nuclear features“ (NIFTP)*Adequate sampling of entire tumor capsule is required to establish this diagnosis

4/11/2016
10
Institutional Data Showing TBSRTC Diagnostic Categories, Surgical Follow-Up, Risk Of Malignancy With and Without Cases of Non-Invasive Follicular Variant of Papillary Thyroid Carcinoma (NI-FVPTC)
Faquin et al. Cancer Cytopathology 2015
Institution A Institution B* Institution C Institution D Institution E
TBSRTC Diagnoses
ND 37 79 51 225 14
Benign 190 1015 1112 1773 131
AUS/FLUS 115 190 480 235 8
FN/SFN 80 154 125 98 6
SM 34 38 108 31 27
Malignant 26 91 300 158 12
Surgical FU
Benign Surgical FU 103 183 393 238 32Malignant Surgical FU 69 176 428 189 15
No Surgery 310 1207 1355 2093 151
Total NI‐FVPTC 33 66 38 34 2
Risk of Malignancy for all TBSRTC Categories
ROM 40.12% 48.89% 52.13% 44.26% 31.91%OROM 14.32% 11.23% 19.67% 7.50% 7.58%
ROM excluding NI‐FVPTC Cases 20.93% 30.56% 47.50% 36.30% 27.66%OROM excluding NI‐FVPTC Cases 7.47% 7.02% 17.92% 6.15% 6.57%
% Decrease in Risk of Malignancyfor all TBSRTC CategoriesROM excluding NI‐FVPTC Cases 19.19% 18.33% 4.63% 7.96% 4.26%OROM excluding NI‐FVPTC Cases 6.85% 4.21% 1.75% 1.35% 1.01%
TBSRTC Diagnostic Categories
ND Benign AUS/FLUS FN/SFN SM Malignant
Total number of FNABs, n=6943 406 (5.8%) 4221 (60.8%) 1028 (14.8%) 463 (6.6%) 238 (3.4%) 587 (8.4%)
Surgical FU
Benign Surgical FU, n=949 52 386 273 203 31 4
Malignant Surgical FU, n=877 18 40 124 101 148 446
Total PTC, n=756
Total NI‐FVPTC, n=173 1 15 54 46 42 15
Risk of Malignancy
ROM 25.3% 9.3% 31.2% 33.2% 82.6% 99.1%
OROM 4.4% 0.9% 12.0% 21.8% 62.1% 75.9%
ROM excluding NI‐FVPTC Cases 23.9% 5.8% 17.6% 18.0% 59.2% 95.7%
**p‐value 0.19 0.04§ 0.03§ 0.03§ 0.01§ 0.1
OROM excluding NI‐FVPTC Cases 4.1% 0.5% 6.8% 11.8% 44.5% 73.4%
**p‐Value 0.18 0.05 0.02§ 0.04§ 0.02§ 0.1
% Decrease in Risk of Malignancy
ROM excluding NI‐FVPTC Cases 1.4% 3.5% 13.6% 15.1% 23.4% 3.3%
OROM excluding NI‐FVPTC Cases 0.2% 0.3% 5.2% 9.9% 17.6% 2.5%
Combined Institutional Data Showing TBSRTC Diagnostic Categories, Surgical Follow-Up, Risk Of Malignancy With and Without Cases of
Non-Invasive Follicular Variant of Papillary Thyroid Carcinoma (NI-FVPTC)
Ibrahim, La Fortuna & Wu. #404 USCAP 2016
FNA Diagnosis NIFT (46) Non‐NIFT (Invasive ‐19)
Benign 6 (13%) 0
FLUS 19 (41%) 5 (26%)
Follicular Neoplasm 6 (13%) 3 (13%)
Suspicious 8 (17%) 8 (42%)
PTC 7 (15%) 3 (16%)
Cytologic Features and Molecular Alterations in a Cohort of 39 NFVPTCs and cPTCs.
Brooke E. Howitt et al. Am J Clin Pathol 2015;144:850-857
Copyright© by the American Society for Clinical Pathology

4/11/2016
11
Where Are We Heading to?
Thyroid nodules are Common
Palpation
Ann Intern Med 1968 69:537; N Engl J Med 1993 328:553
Autopsy & US
2012450,000 FNAs estimated in USA
• The Data from future thyroid FNA studies based on changes in surgical pathology diagnoseswill be important for recommending potential changes in TBSRTC
• The Adjunct Molecular tests are here to stay• Never going to replace thyroid FNA cytology• Play a role in the current management paradigm of thyroid nodules

4/11/2016
12
What I Struggle with Everyday?
When My Roots are Basic Cytomorphology & My Practice is Facing Many Practice Changers
What I Struggle with?
• Good relationship with the clinicians– History– Results discussion– All matters
• Good relationship with radiologist and knowledge of ultrasound
• Empowering the workforce of cytopathology
How to avoid loosing thyroid FNA specimens?