basic life support training for...
TRANSCRIPT
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BASIC LIFE SUPPORT TRAINING FOR
NURSES:
EVALUATING AN ALTERNATIVE
CD-BASED APPROACH
Submitted by
KAREN MARDEGAN
Diploma of Applied Science (Nursing)
Bachelor of Nursing (Honours)
Graduate Diploma of Critical Care Nursing
Master of Nursing Science
A thesis submitted in total fulfilment
of the requirements for the degree of
Doctor of Public Health
School of Public Health
Faculty of Health Sciences
La Trobe University
Bundoora, Victoria 3086
Australia
NOVEMBER, 2011
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table of Contents
Acknowledgements .................................................................................. XIII
Summary .................................................................................................... XV
Statement of Authorship ....................................................................... XVII
Chapter 1 Basic Life Support: Practice, Performance and Training ...... 1
Introduction .................................................................................................................................................. 1
Outline of Thesis. ........................................................................................................................... 2
Resuscitation Practice .................................................................................................................................. 3
Basic life support procedure. ........................................................................................................ 4
Specific skills within the BLS procedure. ....................................................................................... 5
Changes to the BLS procedure. ...................................................................................................... 6
The performance of BLS. .............................................................................................................. 8
Instructional Technology ........................................................................................................................... 14
Training design and delivery. ..................................................................................................... 15
Principles of training design and delivery. ................................................................................... 15
Training delivery methods. ........................................................................................................... 17
Trainee characteristics. ................................................................................................................. 18
Basic Life Support Training and Assessment .......................................................................................... 19
Regulation of BLS training programs. ....................................................................................... 19
Traditional BLS training approaches. ....................................................................................... 20
BLS assessment. ............................................................................................................................ 21
Chapter 2 Basic Life Support Training: Review of the Effectiveness of
Training Methods ....................................................................................... 24
Evaluation of Traditional Training Programs ......................................................................................... 24
Alternatives to the Traditional Approach to BLS Training ................................................................... 31
Basic life support training using Videotape. .............................................................................. 31
Founding studies in BLS Video. ................................................................................................... 32
Subsequent BLS Video studies. .................................................................................................... 36
Conclusions from BLS Video studies. .......................................................................................... 41
Digital Video Disc BLS training programs. ............................................................................... 43
CD basic life support training programs. .................................................................................. 50
Basic life support training available through the Internet. ...................................................... 56
Internet BLS training programs. .................................................................................................. 57
BLS animations. ............................................................................................................................ 65
Contents III | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Virtual world BLS training. .......................................................................................................... 65
Conclusions from BLS Internet studies. ...................................................................................... 66
BLS Training Design, Delivery and Outcomes ........................................................................................ 68
BLS training design and delivery. .............................................................................................. 68
Basic life support training outcomes. ......................................................................................... 70
Summary of BLS skill, knowledge and current modes of training.......................................... 73
Chapter 3 Method ....................................................................................... 76
Aims ............................................................................................................................................................. 76
Primary aim. ................................................................................................................................ 76
Secondary aims. ........................................................................................................................... 76
Hypothesis. ................................................................................................................................... 76
Research Design .......................................................................................................................................... 76
Setting. .......................................................................................................................................... 79
Sampling frame. ........................................................................................................................... 79
Participants ................................................................................................................................................. 79
Recruitment of organisations. ..................................................................................................... 79
Recruitment of participants. ....................................................................................................... 80
Participant assignment. ............................................................................................................... 80
Participant characteristics. ......................................................................................................... 80
Procedure .................................................................................................................................................... 82
Training procedures. ................................................................................................................... 82
The BLS CD training program. .................................................................................................... 82
The basic life support CD. ............................................................................................................ 83
Traditional BLS program. ............................................................................................................ 85
CD and Traditional BLS program content and length. ............................................................... 85
Post Test procedures. ................................................................................................................... 86
Measures ..................................................................................................................................................... 88
Questionnaire. .............................................................................................................................. 88
Demographic and computer literacy sections of the questionnaire. ........................................... 89
BLS experience and knowledge sections of the questionnaire. ................................................... 90
BLS experience questions. ............................................................................................................ 90
BLS knowledge questions. ............................................................................................................ 90
Internal consistency of the questionnaire. ................................................................................... 90
BLS assessment form. .................................................................................................................. 91

Contents IV | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Laerdal Skill Reporter™
Resusci Anne®. ................................................................................... 93
Program evaluation forms. ......................................................................................................... 93
Questions common to both program evaluation forms. ............................................................... 94
Additional questions...................................................................................................................... 94
Internal consistency of the program evaluation tools. ................................................................. 95
Data Analysis .............................................................................................................................................. 95
Sample size calculation and power analysis............................................................................... 95
Questionnaire. .............................................................................................................................. 96
Age group. ..................................................................................................................................... 96
Gender and previous BLS training. ............................................................................................. 96
Overall computer literacy. ............................................................................................................ 96
Participants’ self-rating of BLS skill post training. ..................................................................... 97
BLS Knowledge. ............................................................................................................................ 97
Overall BLS knowledge. ............................................................................................................... 97
BLS knowledge of each question. ................................................................................................. 97
Retention of BLS knowledge. ....................................................................................................... 98
BLS skills assessment form. ........................................................................................................ 98
Overall BLS skill competence. ...................................................................................................... 98
BLS skill categories and specific BLS skills. ............................................................................... 99
Retention of BLS skill level and competence. .............................................................................. 99
Laerdal Skill Reporter™
Resusci Anne® Printout. .................................................................... 99
Program evaluation forms. ....................................................................................................... 100
Ethical Considerations ............................................................................................................................. 100
Trialing of Materials ................................................................................................................................ 101
Design of pilot study. ................................................................................................................. 103
Pilot study results. ...................................................................................................................... 103
Measures. .................................................................................................................................... 103
BLS competence. ......................................................................................................................... 104
Implications of the pilot study. ................................................................................................. 104
Chapter 4 Results ...................................................................................... 105
The Effectiveness of the BLS Training for Novice and Practising Nurses .......................................... 105
Evaluation of BLS Skill for the Two Training Methods ....................................................................... 107
Overall BLS skill competence. .................................................................................................. 107
Overall BLS skill competence at Post Test 1. ............................................................................. 107
Contents V | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Overall BLS skill competence at Post Test 2. ............................................................................. 108
Evaluation of competence in BLS skill categories and specific BLS skills. ........................... 109
Competence in BLS skill categories at Post Test 1. ................................................................... 109
Competence in BLS skill categories at Post Test 2. ................................................................... 110
Specific BLS Skills Competence at Post Test 1 and Post Test 2. ............................................... 112
Retention of BLS skill level and BLS skill competence. ......................................................... 113
Retention of BLS skill level. ....................................................................................................... 113
Retention of BLS skill competence. ............................................................................................ 114
Participants’ rating of their BLS skill post training. .............................................................. 115
BLS skill summary..................................................................................................................... 116
Evaluation of BLS Knowledge for the Two Training Methods ............................................................ 117
Overall BLS knowledge. ............................................................................................................ 117
Overall BLS knowledge at Post Test 1. ...................................................................................... 117
Overall BLS knowledge at Post Test 2. ...................................................................................... 118
Specific BLS knowledge questions at Post Test 1 and Post Test 2. ........................................ 119
Retention of BLS knowledge for the two training methods. .................................................. 119
BLS knowledge summary. ........................................................................................................ 120
Participants’ Program Evaluation for the Two Training Methods ..................................................... 121
Overall participant rating of the BLS training programs. ..................................................... 121
Participant rating of program components and specific questions. ...................................... 122
Participant rating of program components. ............................................................................... 122
Participant rating of specific program evaluation questions. .................................................... 124
Participants’ program evaluation summary. ............................................................................. 124
Summary of Results ................................................................................................................................. 125
Chapter 5 Discussion and Conclusions ................................................... 126
Comparison with Existing Research on BLS Training ......................................................................... 126
Specific BLS skills. ..................................................................................................................... 128
Participants’ evaluation of the training programs. ................................................................. 128
Methodological Issues .............................................................................................................................. 129
Research design. ......................................................................................................................... 129
Selection of effect size. ................................................................................................................ 129
Study participants. ..................................................................................................................... 130
Testing regimens. ....................................................................................................................... 131
Post Test attendance. ................................................................................................................. 132

Contents VI | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS training programs. ............................................................................................................ 132
The BLS CD training program. .................................................................................................. 132
Traditional BLS program. .......................................................................................................... 133
Training program access. ........................................................................................................... 133
Measures. .................................................................................................................................... 134
Questionnaire and program evaluation. .................................................................................... 134
BLS assessment form. ................................................................................................................. 134
BLS assessor reliability. .............................................................................................................. 136
Automated manikin. .................................................................................................................... 136
Implications for Practice .......................................................................................................................... 138
BLS training. .............................................................................................................................. 139
A suggested future approach to BLS training............................................................................ 139
The potential of CD BLS programs. ........................................................................................... 140
Frequent practice. ....................................................................................................................... 141
Recommendations for Further Research ............................................................................................... 141
A systematic approach. .............................................................................................................. 142
CD training methods. .................................................................................................................. 143
DVD-manikin systems and Internet programs. ......................................................................... 143
Future directions. ....................................................................................................................... 144
The mechanisms behind sub-optimal BLS performance. .......................................................... 144
Psychological factors on BLS performance. .............................................................................. 144
Potential expansion of BLS training. ......................................................................................... 145
Conclusion ................................................................................................................................................. 145
References .................................................................................................. 147
Contents VII | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
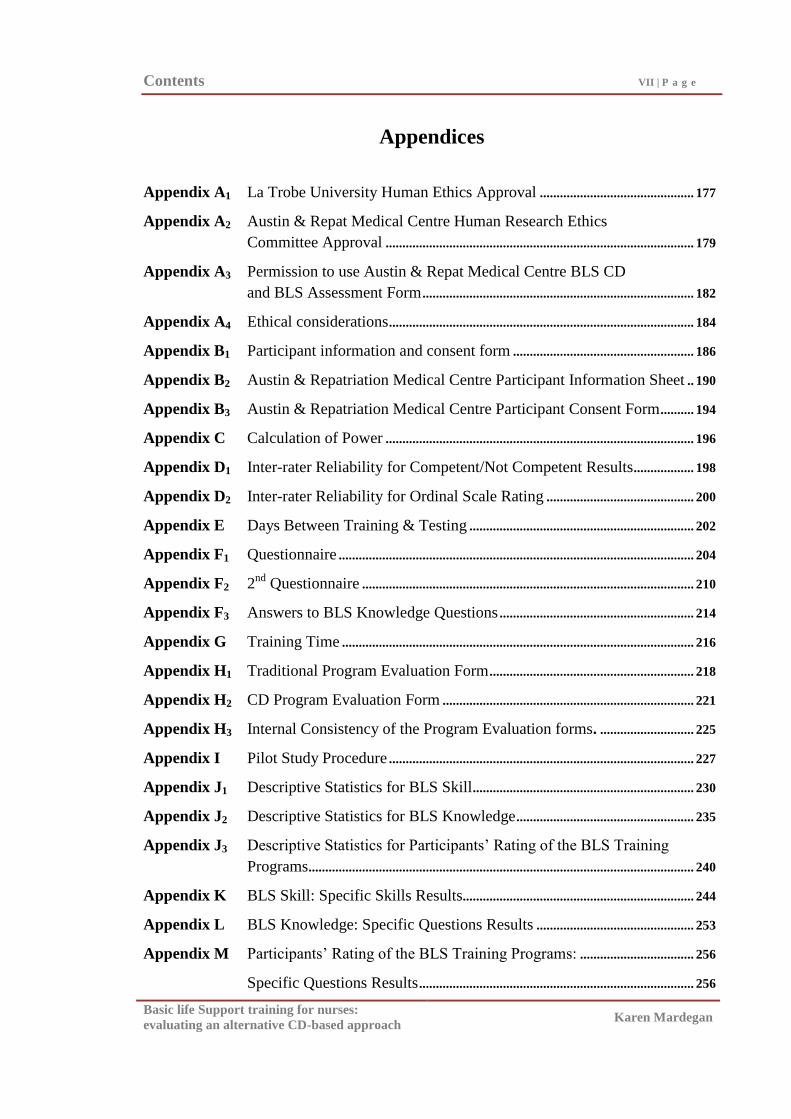
Appendices
Appendix A1 La Trobe University Human Ethics Approval .............................................. 177
Appendix A2 Austin & Repat Medical Centre Human Research Ethics
Committee Approval ............................................................................................ 179
Appendix A3 Permission to use Austin & Repat Medical Centre BLS CD
and BLS Assessment Form ................................................................................. 182
Appendix A4 Ethical considerations ........................................................................................... 184
Appendix B1 Participant information and consent form ...................................................... 186
Appendix B2 Austin & Repatriation Medical Centre Participant Information Sheet .. 190
Appendix B3 Austin & Repatriation Medical Centre Participant Consent Form .......... 194
Appendix C Calculation of Power ............................................................................................ 196
Appendix D1 Inter-rater Reliability for Competent/Not Competent Results .................. 198
Appendix D2 Inter-rater Reliability for Ordinal Scale Rating ............................................ 200
Appendix E Days Between Training & Testing ................................................................... 202
Appendix F1 Questionnaire .......................................................................................................... 204
Appendix F2 2nd
Questionnaire ................................................................................................... 210
Appendix F3 Answers to BLS Knowledge Questions .......................................................... 214
Appendix G Training Time ......................................................................................................... 216
Appendix H1 Traditional Program Evaluation Form ............................................................. 218
Appendix H2 CD Program Evaluation Form ........................................................................... 221
Appendix H3 Internal Consistency of the Program Evaluation forms. ............................ 225
Appendix I Pilot Study Procedure ........................................................................................... 227
Appendix J1 Descriptive Statistics for BLS Skill .................................................................. 230
Appendix J2 Descriptive Statistics for BLS Knowledge ..................................................... 235
Appendix J3 Descriptive Statistics for Participants‘ Rating of the BLS Training
Programs ................................................................................................................... 240
Appendix K BLS Skill: Specific Skills Results..................................................................... 244
Appendix L BLS Knowledge: Specific Questions Results ............................................... 253
Appendix M Participants‘ Rating of the BLS Training Programs: .................................. 256
Specific Questions Results .................................................................................. 256
Contents VIII | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
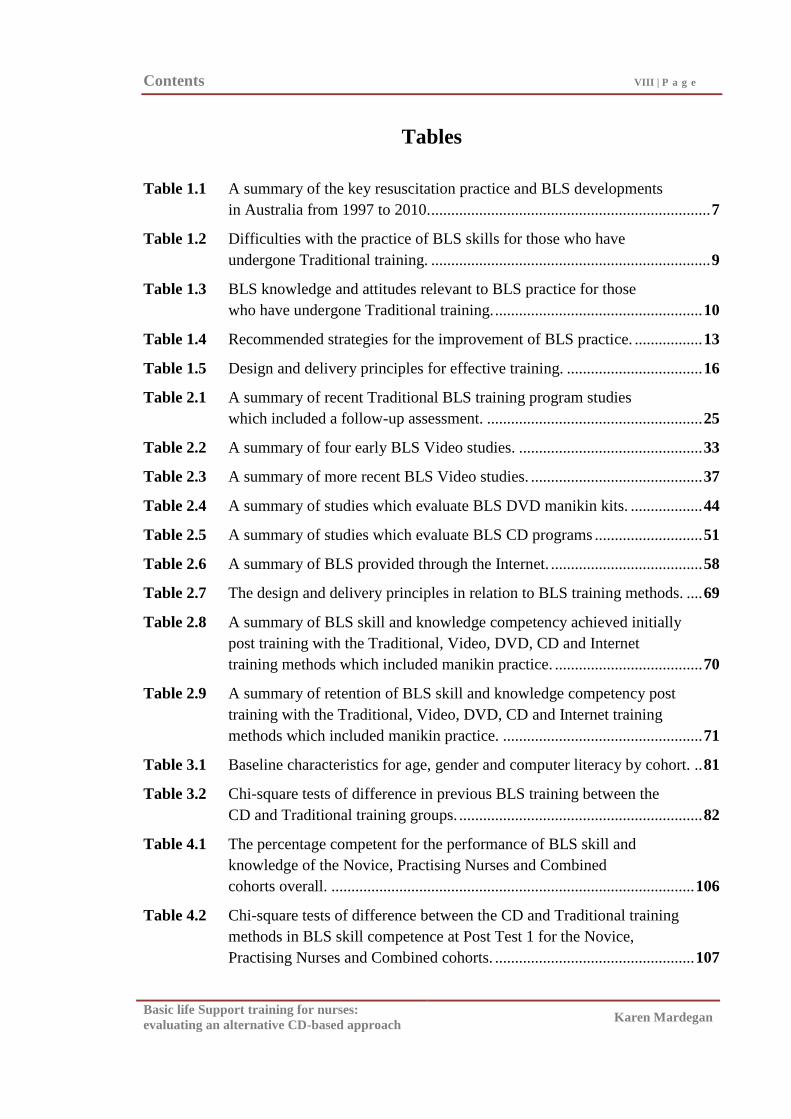
Tables
Table 1.1 A summary of the key resuscitation practice and BLS developments
in Australia from 1997 to 2010. ...................................................................... 7
Table 1.2 Difficulties with the practice of BLS skills for those who have
undergone Traditional training. ...................................................................... 9
Table 1.3 BLS knowledge and attitudes relevant to BLS practice for those
who have undergone Traditional training. .................................................... 10
Table 1.4 Recommended strategies for the improvement of BLS practice. ................. 13
Table 1.5 Design and delivery principles for effective training. .................................. 16
Table 2.1 A summary of recent Traditional BLS training program studies
which included a follow-up assessment. ...................................................... 25
Table 2.2 A summary of four early BLS Video studies. .............................................. 33
Table 2.3 A summary of more recent BLS Video studies. ........................................... 37
Table 2.4 A summary of studies which evaluate BLS DVD manikin kits. .................. 44
Table 2.5 A summary of studies which evaluate BLS CD programs ........................... 51
Table 2.6 A summary of BLS provided through the Internet. ...................................... 58
Table 2.7 The design and delivery principles in relation to BLS training methods. .... 69
Table 2.8 A summary of BLS skill and knowledge competency achieved initially
post training with the Traditional, Video, DVD, CD and Internet
training methods which included manikin practice. ..................................... 70
Table 2.9 A summary of retention of BLS skill and knowledge competency post
training with the Traditional, Video, DVD, CD and Internet training
methods which included manikin practice. .................................................. 71
Table 3.1 Baseline characteristics for age, gender and computer literacy by cohort. .. 81
Table 3.2 Chi-square tests of difference in previous BLS training between the
CD and Traditional training groups. ............................................................. 82
Table 4.1 The percentage competent for the performance of BLS skill and
knowledge of the Novice, Practising Nurses and Combined
cohorts overall. ........................................................................................... 106
Table 4.2 Chi-square tests of difference between the CD and Traditional training
methods in BLS skill competence at Post Test 1 for the Novice,
Practising Nurses and Combined cohorts. .................................................. 107
Contents IX | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
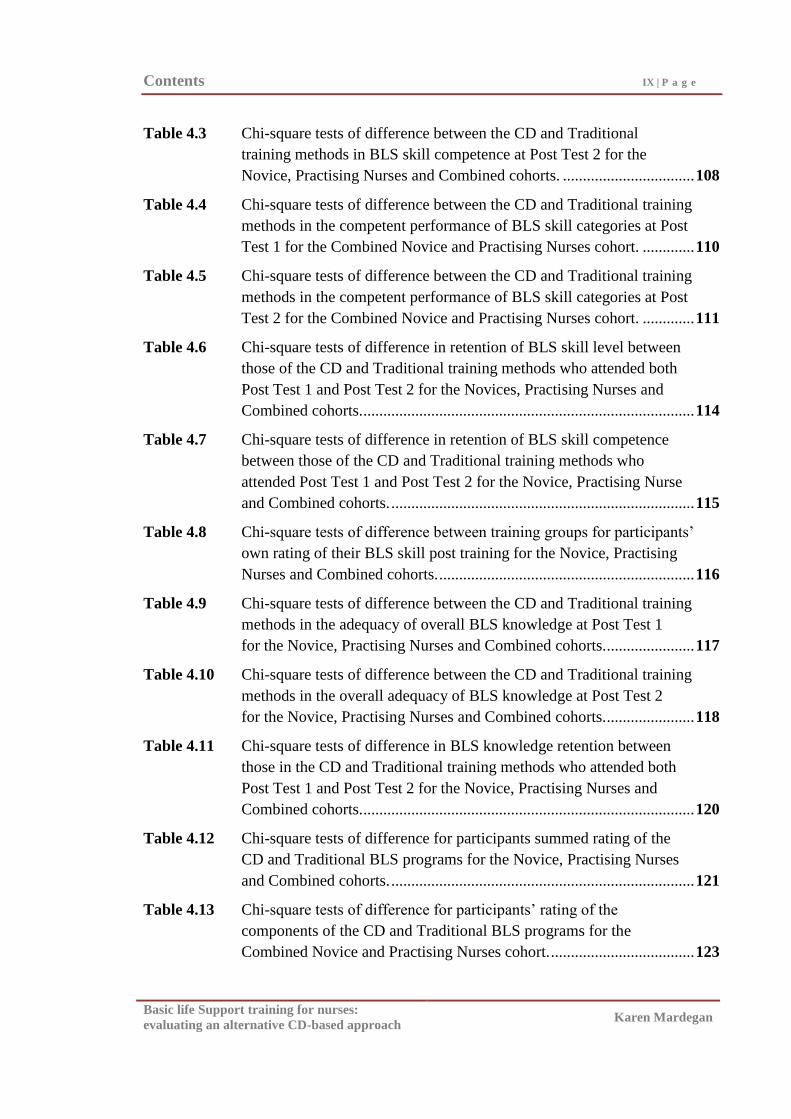
Table 4.3 Chi-square tests of difference between the CD and Traditional
training methods in BLS skill competence at Post Test 2 for the
Novice, Practising Nurses and Combined cohorts. ................................. 108
Table 4.4 Chi-square tests of difference between the CD and Traditional training
methods in the competent performance of BLS skill categories at Post
Test 1 for the Combined Novice and Practising Nurses cohort. ............. 110
Table 4.5 Chi-square tests of difference between the CD and Traditional training
methods in the competent performance of BLS skill categories at Post
Test 2 for the Combined Novice and Practising Nurses cohort. ............. 111
Table 4.6 Chi-square tests of difference in retention of BLS skill level between
those of the CD and Traditional training methods who attended both
Post Test 1 and Post Test 2 for the Novices, Practising Nurses and
Combined cohorts. ................................................................................... 114
Table 4.7 Chi-square tests of difference in retention of BLS skill competence
between those of the CD and Traditional training methods who
attended Post Test 1 and Post Test 2 for the Novice, Practising Nurse
and Combined cohorts. ............................................................................ 115
Table 4.8 Chi-square tests of difference between training groups for participants‘
own rating of their BLS skill post training for the Novice, Practising
Nurses and Combined cohorts. ................................................................ 116
Table 4.9 Chi-square tests of difference between the CD and Traditional training
methods in the adequacy of overall BLS knowledge at Post Test 1
for the Novice, Practising Nurses and Combined cohorts. ...................... 117
Table 4.10 Chi-square tests of difference between the CD and Traditional training
methods in the overall adequacy of BLS knowledge at Post Test 2
for the Novice, Practising Nurses and Combined cohorts. ...................... 118
Table 4.11 Chi-square tests of difference in BLS knowledge retention between
those in the CD and Traditional training methods who attended both
Post Test 1 and Post Test 2 for the Novice, Practising Nurses and
Combined cohorts. ................................................................................... 120
Table 4.12 Chi-square tests of difference for participants summed rating of the
CD and Traditional BLS programs for the Novice, Practising Nurses
and Combined cohorts. ............................................................................ 121
Table 4.13 Chi-square tests of difference for participants‘ rating of the
components of the CD and Traditional BLS programs for the
Combined Novice and Practising Nurses cohort. .................................... 123
Contents X | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
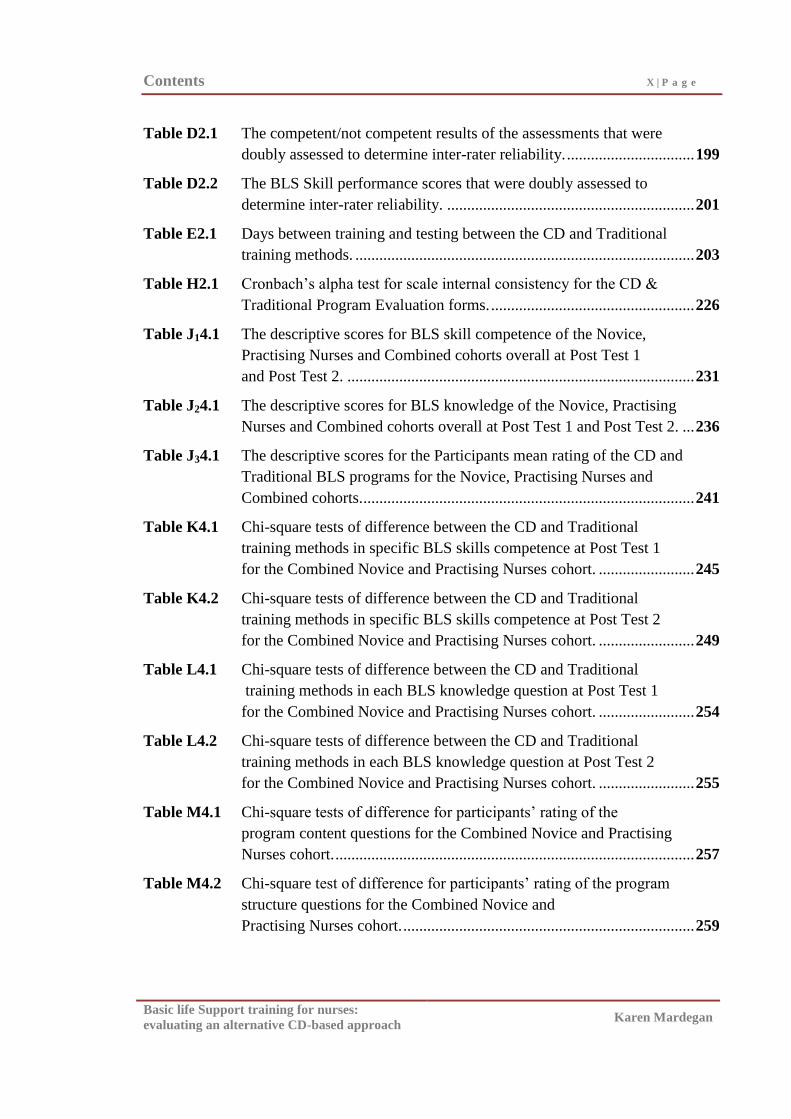
Table D2.1 The competent/not competent results of the assessments that were
doubly assessed to determine inter-rater reliability. ................................ 199
Table D2.2 The BLS Skill performance scores that were doubly assessed to
determine inter-rater reliability. .............................................................. 201
Table E2.1 Days between training and testing between the CD and Traditional
training methods. ..................................................................................... 203
Table H2.1 Cronbach‘s alpha test for scale internal consistency for the CD &
Traditional Program Evaluation forms. ................................................... 226
Table J14.1 The descriptive scores for BLS skill competence of the Novice,
Practising Nurses and Combined cohorts overall at Post Test 1
and Post Test 2. ....................................................................................... 231
Table J24.1 The descriptive scores for BLS knowledge of the Novice, Practising
Nurses and Combined cohorts overall at Post Test 1 and Post Test 2. ... 236
Table J34.1 The descriptive scores for the Participants mean rating of the CD and
Traditional BLS programs for the Novice, Practising Nurses and
Combined cohorts. ................................................................................... 241
Table K4.1 Chi-square tests of difference between the CD and Traditional
training methods in specific BLS skills competence at Post Test 1
for the Combined Novice and Practising Nurses cohort. ........................ 245
Table K4.2 Chi-square tests of difference between the CD and Traditional
training methods in specific BLS skills competence at Post Test 2
for the Combined Novice and Practising Nurses cohort. ........................ 249
Table L4.1 Chi-square tests of difference between the CD and Traditional
training methods in each BLS knowledge question at Post Test 1
for the Combined Novice and Practising Nurses cohort. ........................ 254
Table L4.2 Chi-square tests of difference between the CD and Traditional
training methods in each BLS knowledge question at Post Test 2
for the Combined Novice and Practising Nurses cohort. ........................ 255
Table M4.1 Chi-square tests of difference for participants‘ rating of the
program content questions for the Combined Novice and Practising
Nurses cohort. .......................................................................................... 257
Table M4.2 Chi-square test of difference for participants‘ rating of the program
structure questions for the Combined Novice and
Practising Nurses cohort. ......................................................................... 259

Contents XI | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table M4.3 Chi-square tests of difference for participants‘ rating of the
program assessment questions for the Combined Novice and
Practising Nurses cohort. ......................................................................... 260
Table M4.4 Chi-square tests of difference for participants‘ rating of the
program quality & satisfaction questions for the Combined Novice
and Practising Nurses cohort. .................................................................. 260
Contents XII | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Figures Figure 3.1 Study Design ............................................................................................. 78
Figure 3.2 Nurses – Basic Life Support assessment form .......................................... 92
Figure 3.3 Pilot Study Design ................................................................................... 102
Figure C2.1 Sample size calculation and power analysis ............................................ 197
Figure J14.1 Histogram of BLS skill scores for the Novice cohort at
Post Test 1 and Post Test 2 ...................................................................... 232
Figure J14.2 Histogram of BLS skill scores for the Practising Nurses cohort at
Post Test 1 and Post Test 2 ...................................................................... 233
Figure J14.3 Histogram of BLS skill scores for the Combined Novice and
Practising Nurses cohort at Post Test 1 and Post Test 2 ......................... 234
Figure J24.1 Histogram of BLS knowledge scores for the Novice cohort at
Post Test 1 and Post Test 2. ..................................................................... 237
Figure J24.2 Histogram of BLS knowledge scores for the Practising Nurses
cohort at Post Test 1 and Post Test 2. ...................................................... 238
Figure J24.3 Histogram of BLS knowledge scores for the Combined Novice
and Practising Nurses cohort at Post Test 1 and Post Test 2. .................. 239
Figure J34.1 Histogram of Participants‘ Program Evaluation scores for the
Novice cohort, Practising Nurses cohort and Combined cohort. ............ 242
Acknowledgements XIII | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Acknowledgements
I wish to acknowledge and express my sincere appreciation to the following
individuals for their assistance in the completion of this project.
To Professor Margot Schofield and Professor Gregory Murphy for
their guidance, support and encouragement throughout the project.
To Dr Jane Pierson for her assistance in the early phases of the project.
To the La Trobe University School of Nursing and the co-ordinator of
the Nursing Therapies & Practices – The Older Person subject –Anne
Pitcher for endorsing my project and assisting with co-ordinating
access to the students.
To Austin Health, the Director of Ambulatory & Nursing Services –
Mark Petty, and the Manager of the Clinical Nursing Education
Department - Dr Joanne Wilkinson for supporting the project and for
the use of the Austin Health BLS CD, assessment and questionnaire
tools.
To the Graduate Nurse Year Program Co-ordinator – Sue Thorpe for
supporting the student‘s participation in the project and assisting with
co-ordinating access to the students.
To Jenny Corbin Senior Librarian and the La Trobe University Library
document delivery team for their expert advice and assistance with
searching and obtaining documents which are relevant to this project.
To La Trobe University School of Public Health and Faculty of Health
Sciences for Post Graduate Support Grants of $1,637.30 for CPR
equipment and research assistants.
Acknowledgements XIV | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
To the six expert BLS assessors Karen Herbert, Renee Chmielewski,
Margaret Holley, Sue Thorpe, Christina Seales, and Melissa
Schrober for their assistance with the BLS assessments.
To Laerdal Australia – Bill Thalmeier (Victorian State Manager) &
Daniel Beelitz (Simulation Specialist) for the loan of the Laerdal Skill
Reporter™
Resusci Anne® manikins used in the project.
To the 306 participants who volunteered to take part in this study with
no promise of reward except knowing that they contributed to
Resuscitation Education.
To Professor Ian Baldwin, Dr Maria Murphy, Jacqueline Howard,
Kathryn Stephenson and Nicolle Judd for their assistance with
preparing the thesis for submission.
To Douglas MacPherson, Olive MacPherson, Eva Elleman and
Gary Mardegan for their assistance and encouragement throughout the
project.
To my husband Gary and daughters Danielle, Emily and Gabrielle for
their unfaltering support, encouragement and endless patience and love.
Lastly, to my late mother and father, Hedi and Lou Mardegan for
always believing in me and encouraging me to strive higher.
Your generosity is most appreciated!
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Summary
Basic Life Support (BLS) or Cardiopulmonary Resuscitation (CPR) is a life saving
skill. However, studies have reported limitations in BLS training outcomes for both
health professional and lay populations, including poor retention of BLS skill and
knowledge post training, and the resource and time intensive nature of Traditional
training approaches. This study aimed to evaluate the effectiveness of a CD-based BLS
training program with a Traditional BLS training program.
Method:
The study compared the two training programs using a quasi-experimental post-test
with follow-up design. The sample comprised two cohorts: Novice second-year
undergraduate Nursing students (n=187) and Practising Nurses (n=107) in their first year
of hospital employment. The two training programs were a CD-based BLS training
program which included unsupervised manikin practice, and a Traditional BLS training
program involving lecture, demonstration, and supervised practice. Participants‘ BLS
skill and knowledge were assessed at one week and at two months post training.
Participants‘ self-rating of skill and evaluation of the training program was also obtained
at the one week post test.
Findings:
No statistically significant differences were found between the CD and Traditional
BLS training methods in BLS skill competence and knowledge of Novice and Practising
Nurses at one week and at two months post training. However, there was a decrement in
skill between one week and two months post-training and an overall low level of
competence even for the Practising Nurses. Program evaluation findings demonstrated
participants' preference for the Traditional BLS training program.

Summary XVI | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Conclusion:
A CD-based BLS program has been shown to be as good as a more resource
intensive Traditional BLS training program. However, competence is less than optimal
for both training methods suggesting a need for renewed efforts to develop and evaluate
BLS training programs which can achieve high rates of competence with acceptable
retention over time.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Statement of Authorship
―Except where reference is made in the text of the thesis, this
thesis contains no material published elsewhere or extracted in
whole or in part from a thesis submitted for the award of any
other degree or diploma.
No other person's work has been used without due
acknowledgment in the main text of the thesis.
This thesis has not been submitted for the award of any degree
or diploma in any other tertiary institution."
This thesis was supervised by Professor Margot Schofield and
Professor Gregory Murphy.
All research procedures reported in the thesis were approved by
the Ethics Committees of La Trobe University and participating
organisations.
Signed
Karen Mardegan
Dated: 11 / 11 / 2011
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Chapter 1
Basic Life Support:
Practice, Performance and Training
Introduction
The Basic Life Support (BLS) procedure is a life-saving skill and the fundamental
therapy in resuscitation practice (Australian Resuscitation Council & New Zealand
Resuscitation Council [ARC & NZRC], 2010d; Hazinski et al., 2010; Sayre et al., 2010).
It is thus a required skill for the majority of health professionals (particularly nurses,
doctors, and paramedics) and encouraged in the lay population (ARC & NZRC, 2010a).
Studies have reported variable initial training outcomes and poor retention of BLS skill in
both health professional (Kallestedt et al., 2010; Madden, 2006) and lay populations
(Brennan & Braslow, 1998; Woollard et al., 2004). The limitations to current training
practices, and the large number of health professionals and lay people needing training
and regular updates have led to recommendations for re-evaluation of BLS training
methods, and innovative approaches to the training, updating and practising of BLS skills
(Australian Resuscitation Council [ARC], 2007b; International Liaison Committee on
Resuscitation [ILCOR], 2005; Mancini et al., 2010; ARC & NZRC, 2010a).
The development of Video (and its modern equivalent Digital Video Disc [DVD])
BLS training programs and kits, which incorporate independent manikin practice have
been advocated as an appropriate alternative to the Traditional BLS programs which
involve lecture, demonstration and supervised practice (Mancini et al., 2010). However,
variable skill acquisition and retention of BLS skill remain a significant problem
(Braslow et al., 1997; Einspruch, Lynch, Aufderheide, Nichol, & Becker, 2007; Roppolo
et al., 2007a). There is therefore a need to continue to evaluate innovative BLS training
approaches to more adequately address BLS skill and retention issues.
BLS Compact Disc (CD) computer based programs remain relatively unevaluated
(Fabius, Grissom, & Fuentes, 1994; Monsieurs et. al., 2004; Moule & Gilchrist, 2001;
Moule, 2002; Reder, Cummings, & Quan, 2006). However CD programs, in particular,
Chapter 1 — BLS: Practice, Performance and Training 2 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
which incorporate independent manikin practice could provide a valuable addition to
available BLS training approaches and potentially improve on the encouraging
demonstrated benefits of BLS Video and DVD manikin kits (Cason, Kardong-Edgren,
Cazzell, Behan, & Mancini, 2009; Christenson et al., 2007; Chung, Siu, Po, Lam, &
Wong, 2010; Isbye, Rasmussen, Lippert, Rudolph, & Ringsted, 2006; Mancini,
Cazzell, Kardong-Edgren, & Cason, 2009; Roppolo et al., 2007a; Todd et al., 1998). It is
therefore the intention of this doctoral thesis to evaluate the effectiveness of a CD-based
BLS training program that incorporates unsupervised manikin practice with a Traditional
BLS training program among Novice and Practising Nurses.
Outline of Thesis.
Chapter One of this thesis, Basic Life Support: Practice, Performance and Training,
outlines resuscitation practice, Basic Life Support (BLS) and how the BLS procedure has
changed over time. It analyses the performance of BLS by health professionals and lay
people. Chapter one also describes training design and delivery and the various
technologies used to provide training. It discusses the regulation of BLS training
programs and how these programs are traditionally delivered and assessed.
Chapter Two, Basic Life Support Training: Review of the effectiveness of training
methods, critically reviews previous studies that evaluate the design, delivery and
outcomes of traditional and alternative methods of BLS training. The results of these
studies are analysed with regard to the acquisition and retention of BLS skill and
knowledge. The lack of published studies which compare Traditional BLS training
approaches with BLS CD-based programs incorporating unsupervised manikin practice is
established. The chapter also examines the potential BLS skill and knowledge outcomes
with these modes of training.
Chapter Three, Method, explains the aim and design of this doctoral thesis. It
details the research method employed and the tools used to assess the results of this study.
This chapter also describes the pilot study undertaken to review the design and method of
this thesis.
Chapter Four, Results, presents the results of this study and analyses the
effectiveness of the two modes of delivery of BLS training taking into account the initial
results at one week after training and the retention of skill and knowledge demonstrated at
Chapter 1 — BLS: Practice, Performance and Training 3 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
two months post training. There is also presentation of the participants‘ self-rating of
skill and evaluation of the two different training methods.
Chapter Five, Discussion and Conclusion, compares the results of this study with
existing research on BLS training and discusses the results of the study and the
conclusions that can be drawn from these results. The chapter also states the implications
for practice as a result of this study and makes recommendations for further research that
could be undertaken to contribute to the body of knowledge related to the training of
Basic Life Support.
Resuscitation Practice
The International Liaison Committee on Resuscitation (ILCOR) is the world authority on
resuscitation (Hazinski et al., 2010). This body releases recommendations in relation to
resuscitation practice every five years (Hazinski et al., 2010; ILCOR, 2000a, 2000b,
2005a, Sayre et al., 2010). Some of the particular recommendations of ILCOR for
improving BLS practice are presented in Table 1.4. Resuscitation councils around the
world, including the Australian Resuscitation Council (ARC), produce practice guidelines
that conform to these ILCOR recommendations. In 2010, Australia and New Zealand
Resuscitation Councils collaborated to produce joint guidelines for resuscitation practice
for the two countries (ARC & NZRC, 2010e).
Resuscitation practice entails both BLS and advanced life support (ALS), (Hazinski
et al., 2010; ARC, 2007b; ARC & NZRC, 2010c, 2010d). BLS is defined as ―emergency
treatment of a victim of cardiac or respiratory arrest‖ (Harris, Nagy, & Vardaxis, 2006, p.
187), and a ―basic emergency procedure for life support …consisting of assessment of the
victim,‖ and then, if required to sustain life, the performance of ―artificial respiration and
manual external cardiac massage‖ (Harris et al., 2006, p. 303). Its role is to therefore
maintain cerebral and myocardial perfusion until definitive treatment can be given
(Devlin, 1999; ILCOR, 2000a).
ALS, also referred to as advanced cardiac life support (ACLS), involves a ―higher
level of emergency medical care … in which BLS efforts are augmented by the
establishment of an intravenous fluid line, defibrillation, drug administration, control of
cardiac arrhythmias, endotracheal intubation and the use of ventilation equipment‖
(Harris et al., 2006 p.48-49).
Chapter 1 — BLS: Practice, Performance and Training 4 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Recently an intermediate form of life support training, referred to as immediate life
support (ILS), has been introduced as an alternative for health professionals (ARC &
Resuscitation Council (United Kingdom [UK]), 2007; Resuscitation Council (UK), 2006).
It involves BLS, simple airway management, and manual and automated defibrillation,
enabling health professionals to more effectively manage patients in cardiac arrest until
the arrival of a cardiac arrest team (ARC & RC (UK), 2007; RC (UK), 2006). All nurses,
doctors and paramedics are expected to be able to competently perform BLS (ARC &
NZRC, 2010a). Those with specialised training also have either ILS or ALS skills (ARC,
2007b; ARC & NZRC, 2010c, 2010d).
Basic life support procedure.
The BLS procedure (ARC, 1997) which was current in Australia at the time that this
project commenced comprised the following stages: 1. Danger (D): checking for danger,
to the rescuer and/or to the victim; 2. Response (R): checking for response (level of
consciousness) in the victim; 3. Airway (A): ensuring the victim‘s airway is open and
clear; 4. Breathing (B): checking the victim for signs of breathing, and if it is absent,
commencing artificial respiration (ventilation) by way of mouth-to-mouth resuscitation or
by way of apparatus-assisted ventilation; 5. Circulation (C): checking for a pulse; and if
it is absent, performing cardiopulmonary resuscitation.
Cardiopulmonary resuscitation (CPR) is the term commonly used to refer to only
the ventilation and chest compression (Betz, Callaway, Hostler, & Rittenberger, 2008;
Bolle, Scholl, & Gilbert, 2009; Choa, Park, Yoon, Kim, & Yoo, 2006) components of the
BLS procedure. However, in some instances, the term CPR is also used in the literature
to denote the full BLS procedure (Choa et al., 2009; Creutzfeldt, Hedman, Medin, Wallin,
& Fellander-Tsai, 2008; Hopstock, 2008; Lorem, Steen, & Wik, 2010). Therefore, to
ensure clarity, the term BLS will be used in this project to refer to the full procedure, and
the term CPR will be used only to refer to ventilation and chest compressions.
It is also noteworthy that in Australia and New Zealand, the BLS procedure
flowchart commences with a check for danger (ARC, 2002, 2006c; ARC & NZRC,
2010b; Australian Resuscitation Council), whereas the checking for danger is advised in
BLS guidelines for the United States of America (US), UK and the rest of Europe, but the
BLS procedure flowchart begins with checking for responsiveness in the victim
Chapter 1 — BLS: Practice, Performance and Training 5 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
(American heart association; European Resuscitation Council; Hazinski et al., 2010;
ILCOR; Resuscitation Council (UK); Sayre et al., 2010).
Specific skills within the BLS procedure.
Each of the stages (i.e. DRABC) of the BLS procedure described above entails one
or more BLS skill steps. For the BLS procedure used for the project, these BLS steps
were as bolded in what follows, and these steps and associated processes correspond to
the procedure that was demonstrated, practised and assessed for all of the study‘s training
groups.
According to the ARC (1997) guideline for BLS, the danger stage entails checking
for any factors posing a danger to the rescuer(s), prior to approaching the victim, and
then for any factors posing a danger to the victim. If danger is identified, it needs to be
addressed prior to proceeding further. The response stage entails checking for a response
from the victim by shaking them and shouting at them. If no response is elicited, the
rescuer(s) calls for help from ambulance paramedics, and from other by-standers and, if
possible, notes the time. The rescuer should not leave the victim unless this is
unavoidable. The airway stage entails checking the victim’s airway for any form of
obstruction (the tongue or foreign matter) and opening the victim’s airway by
performing a jaw thrust manoeuvre. If an obstruction is found, the victim should be
rolled onto his or her side, and the obstruction cleared with a finger sweep.
The breathing stage entails laying the victim on his or her back, then checking the
victim for breathing by looking for rise and fall of the chest, listening for breath sounds,
and feeling for breath escaping from the mouth and nose. If there is no signs of breathing,
the rescuer(s) needs to ensure that the airway is still open and clear, then commences
ventilation, by delivering two breaths via the mouth, or by using ventilation
apparatus. The circulation stage entails checking for a pulse, for no longer than 10
seconds. If no pulse is present, the rescuer(s) proceeds by commencing CPR, at a ratio
of 2 ventilations to 15 chest compressions for a solo person, and 1 ventilation to 5
compressions for two person CPR. The rescuer(s) needs to stop CPR and check the
victim for the presence of breathing and a pulse at least every two minutes (ARC, 1997;
Gee, 1993; Handley, 1997; Quinn & Ord, 1996a, 1996b).
Chapter 1 — BLS: Practice, Performance and Training 6 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Changes to the BLS procedure.
A number of changes to the BLS procedure have been recommended by ILCOR in
their five-yearly reviews of resuscitation literature (ILCOR, 2000b, 2005c; Hazinski et al.,
2010; Morley et al., 2010; Sayre et al., 2010), and subsequently incorporated into the
Australian resuscitation guidelines (ARC, 2002, 2006a, 2006c; ARC & NZRC, 2010e,
2010f) since the data collection of this study was completed. These changes are described
next.
In 2002, the ARC guidelines‘ recommended approach to assessing a victim‘s
response (conscious state) was changed from ‗shake and shout’ to ‗talk and tap’. The
finger sweep to remove an airway obstruction was no longer recommended; placing the
victim on his or her side, thereby allowing gravity to remove the obstruction, or using
suction where available, was now advocated. The ventilation/compression ratios for CPR
was changed from 1 ventilation/5 compressions for two operators and 2 ventilations/15
compressions for one operator, to 2 ventilations/15 compressions for both one and two
operators, which aimed at simplifying the process. The introduction of defibrillation into
the BLS procedure was also recommended at this time (ARC, 2002; ILCOR, 2000a,
2000b). Defibrillation is performed, when needed, to restore the heart‘s normal rhythm
and it can be performed manually by staff with specialised training using a defibrillator or
by the use of a semi-automatic device by those who are untrained in BLS, as well as by
those who have basic or specialised BLS training (ARC, 2004b, 2006c; ILCOR 2005d).
In November 2005, the ARC recommended further simplifying the BLS procedure
by introducing the concept of checking for signs of life (i.e. consciousness, breathing and
movement). Furthermore, the pulse check was removed, the ventilation/compression
ratio was changed to 2 ventilations/30 compressions, and defibrillation was added to the
BLS sequence, changing the procedure in Australia in 2006 from DRABC to DRABCD
(ARC, 2006).
In October 2010, ILCOR remarked on the need for improving the flow of the BLS
procedure and the importance of high quality CPR (Hazinski et al., 2010; Mancini et al.,
2010; Sayre et al., 2010). The additional stage of sending (S) for help was added to the
sequence after the response stage, and if the person was unconscious, and either not
breathing or not breathing normally (occasional gasps), then 30 compressions are to be
Chapter 1 — BLS: Practice, Performance and Training 7 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
given followed by the previously prescribed 2 ventilations/30 compressions ratio.
Furthermore, although performing both ventilations and compressions continues to be
recommended, where the rescuer is unwilling or unable to provide conventional CPR,
compression-only CPR has been advised (ARC & NZRC, 2010b; Hazinski et al., 2010;
Mancini et al., 2010; Sayre et al., 2010). These latest recommendations changed the
procedure in Australia in 2010 from DRABCD to DRSABCD (ARC & NZRC, 2010b).
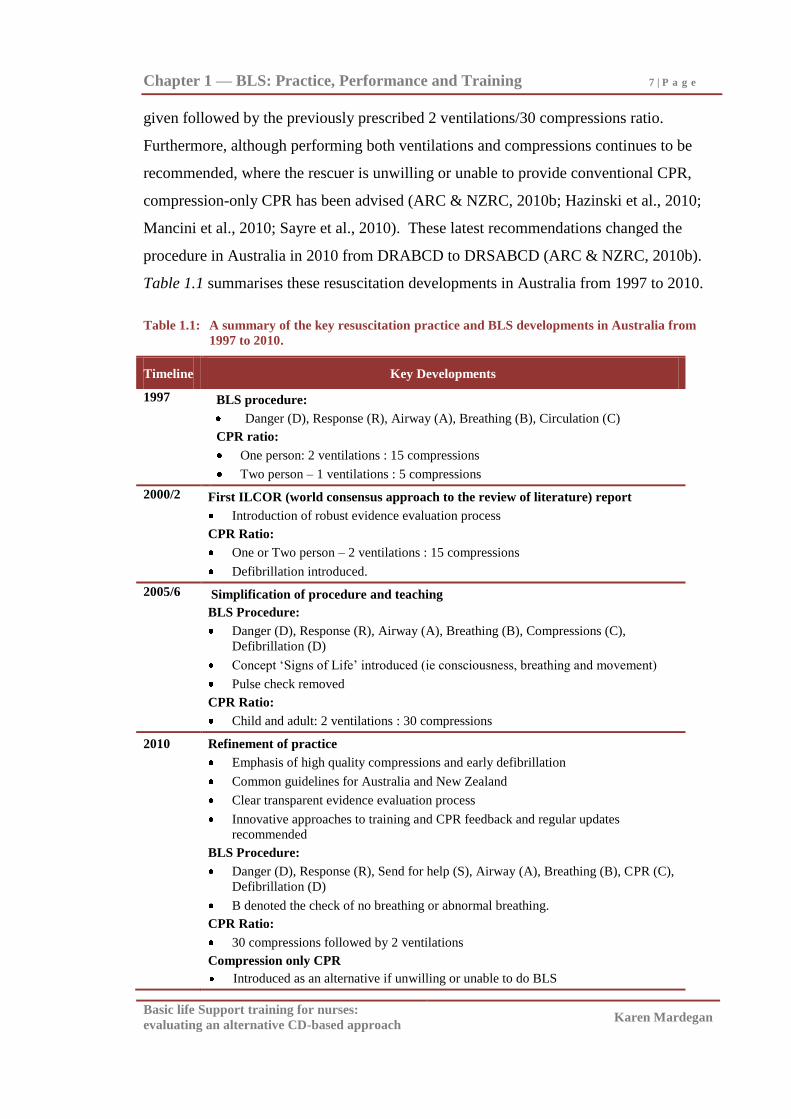
Table 1.1 summarises these resuscitation developments in Australia from 1997 to 2010.
Table 1.1: A summary of the key resuscitation practice and BLS developments in Australia from
1997 to 2010.
Timeline Key Developments
1997
BLS procedure:
Danger (D), Response (R), Airway (A), Breathing (B), Circulation (C)
CPR ratio:
One person: 2 ventilations : 15 compressions
Two person – 1 ventilations : 5 compressions
2000/2
First ILCOR (world consensus approach to the review of literature) report
Introduction of robust evidence evaluation process
CPR Ratio:
One or Two person – 2 ventilations : 15 compressions
Defibrillation introduced.
2005/6
Simplification of procedure and teaching
BLS Procedure:
Danger (D), Response (R), Airway (A), Breathing (B), Compressions (C),
Defibrillation (D)
Concept ‗Signs of Life‘ introduced (ie consciousness, breathing and movement)
Pulse check removed
CPR Ratio:
Child and adult: 2 ventilations : 30 compressions
2010 Refinement of practice
Emphasis of high quality compressions and early defibrillation
Common guidelines for Australia and New Zealand
Clear transparent evidence evaluation process
Innovative approaches to training and CPR feedback and regular updates
recommended
BLS Procedure:
Danger (D), Response (R), Send for help (S), Airway (A), Breathing (B), CPR (C),
Defibrillation (D)
B denoted the check of no breathing or abnormal breathing.
CPR Ratio:
30 compressions followed by 2 ventilations
Compression only CPR
Introduced as an alternative if unwilling or unable to do BLS
Chapter 1 — BLS: Practice, Performance and Training 8 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
While BLS is a fundamental therapy, many questions remain to be answered about
the circumstances and survival following cardiac arrest which are fundamental to the
continued evolution of the BLS procedure (Cummins & Hazinski, 2000; Handley,
Monsieurs, & Bossaert, 2001; ILCOR, 2000a, 2000b). Clinical research in this area is
challenging, not least because of the ethical issues encountered. However a continued
emphasis on rigorous investigation, promoted through the ongoing development of
international guidelines, is essential to ensuring continued improvement of the life
support provided to victims of respiratory and/or cardiac arrest (Gabbott et al., 2005). It is
therefore envisaged that the BLS procedure will continue to evolve over time based on a
philosophy of evidence-based best practice (Smith, 2005).
The performance of BLS.
Nurses, doctors, and paramedics, who are at the frontline of resuscitation practice
and health-care are expected to be proficient in performing BLS. However, difficulties in
the performance of BLS amongst health professionals, students of the health professions,
and lay people, and the poor retention of these skills and knowledge over time, have been
reported by many researchers. More recent studies which have evaluated the performance
of BLS have been listed in Table 1.2 and Table 1.3.
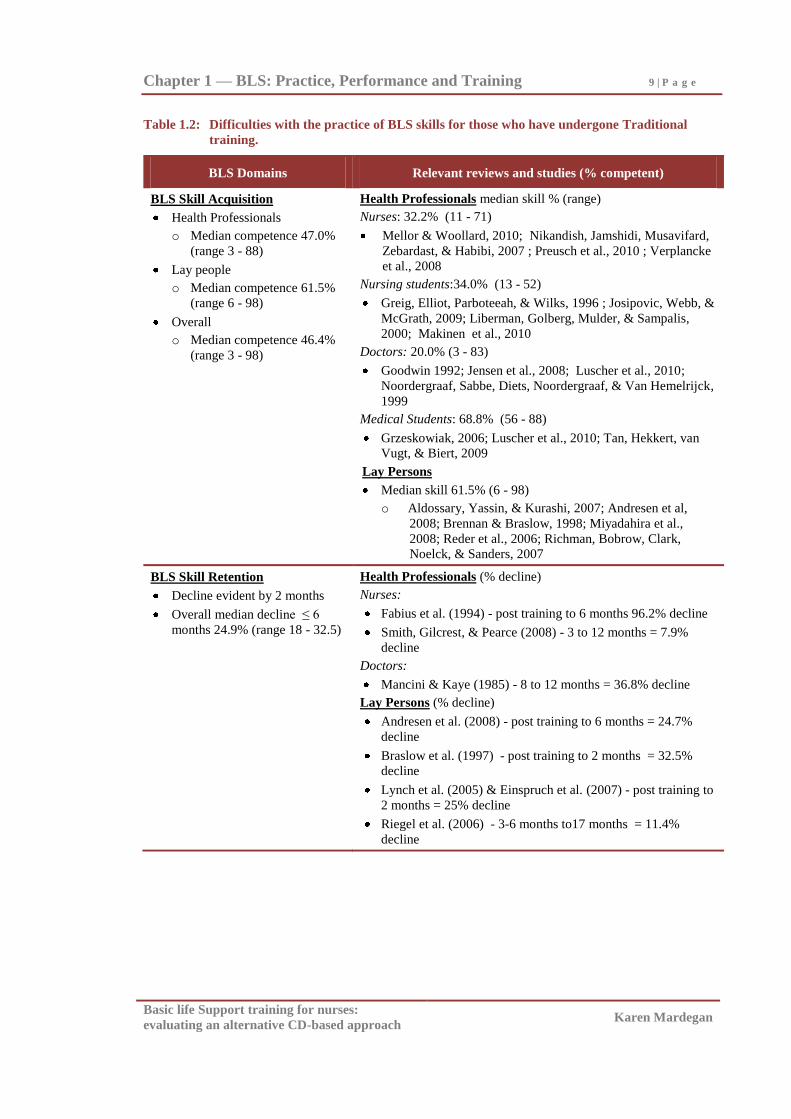
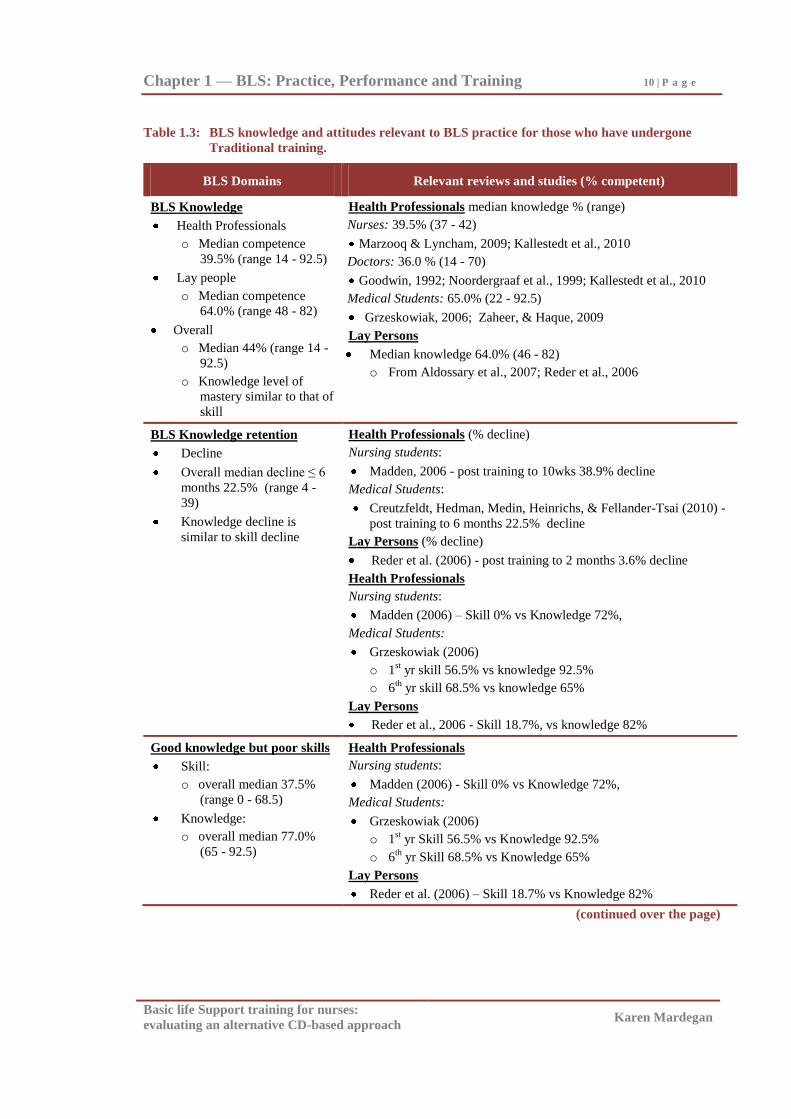
It is reasonable to expect that a higher standard of competence should be achieved
by health professionals compared with lay people, however the studies in Table 1.2
illustrate that student and practising health professionals in nursing and medicine often do
not demonstrate a higher overall level of BLS competence than do members of the lay
public (% competent: health professional = median 47.0% [range 3-88] vs lay public =
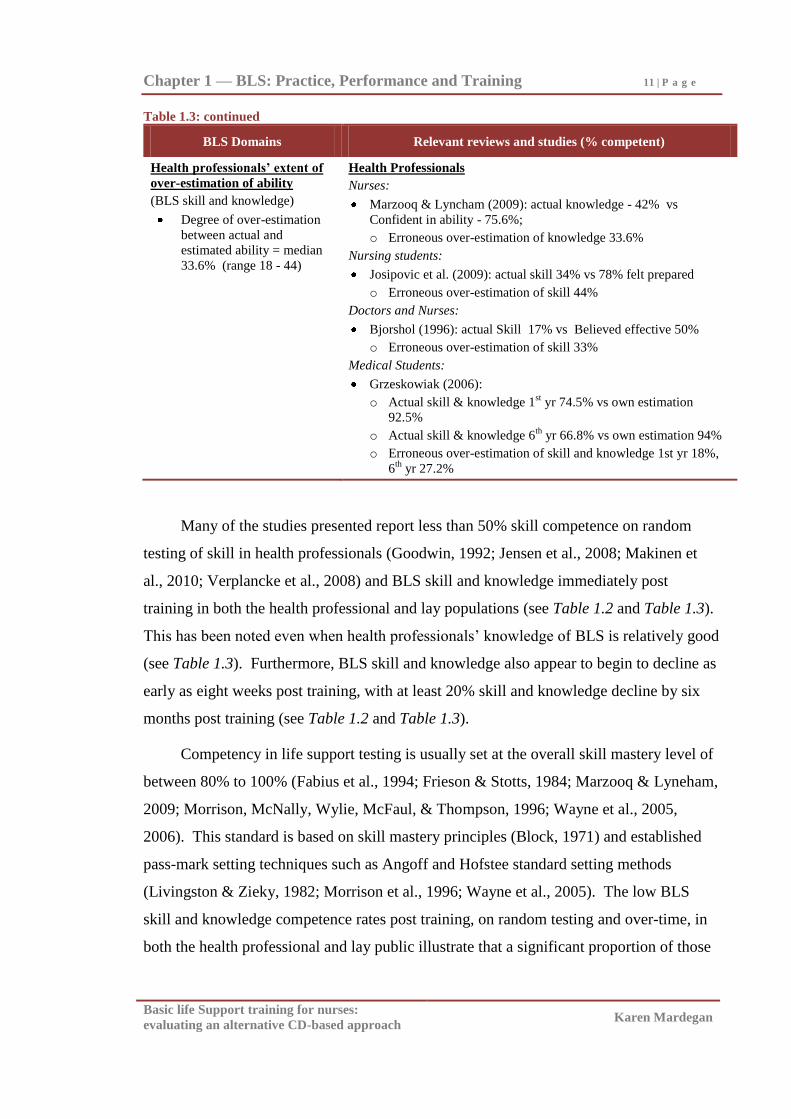
median 61.5% [range 6-98]), and practising health professionals have been noted to over-
estimate their ability (median erroneous over-estimation 33.6% (range 18-44, [see Table
1.3]).
Chapter 1 — BLS: Practice, Performance and Training 9 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 1.2: Difficulties with the practice of BLS skills for those who have undergone Traditional
training.
BLS Domains Relevant reviews and studies (% competent)
BLS Skill Acquisition
Health Professionals
o Median competence 47.0%
(range 3 - 88)
Lay people
o Median competence 61.5%
(range 6 - 98)
Overall
o Median competence 46.4%
(range 3 - 98)
Health Professionals median skill % (range)
Nurses: 32.2% (11 - 71)
Mellor & Woollard, 2010; Nikandish, Jamshidi, Musavifard,
Zebardast, & Habibi, 2007 ; Preusch et al., 2010 ; Verplancke
et al., 2008
Nursing students:34.0% (13 - 52)
Greig, Elliot, Parboteeah, & Wilks, 1996 ; Josipovic, Webb, &
McGrath, 2009; Liberman, Golberg, Mulder, & Sampalis,
2000; Makinen et al., 2010
Doctors: 20.0% (3 - 83)
Goodwin 1992; Jensen et al., 2008; Luscher et al., 2010;
Noordergraaf, Sabbe, Diets, Noordergraaf, & Van Hemelrijck,
1999
Medical Students: 68.8% (56 - 88)
Grzeskowiak, 2006; Luscher et al., 2010; Tan, Hekkert, van
Vugt, & Biert, 2009
Lay Persons
Median skill 61.5% (6 - 98)
o Aldossary, Yassin, & Kurashi, 2007; Andresen et al,
2008; Brennan & Braslow, 1998; Miyadahira et al.,
2008; Reder et al., 2006; Richman, Bobrow, Clark,
Noelck, & Sanders, 2007
BLS Skill Retention
Decline evident by 2 months
Overall median decline ≤ 6
months 24.9% (range 18 - 32.5)
Health Professionals (% decline)
Nurses:
Fabius et al. (1994) - post training to 6 months 96.2% decline
Smith, Gilcrest, & Pearce (2008) - 3 to 12 months = 7.9%
decline
Doctors:
Mancini & Kaye (1985) - 8 to 12 months = 36.8% decline
Lay Persons (% decline)
Andresen et al. (2008) - post training to 6 months = 24.7%
decline
Braslow et al. (1997) - post training to 2 months = 32.5%
decline
Lynch et al. (2005) & Einspruch et al. (2007) - post training to
2 months = 25% decline
Riegel et al. (2006) - 3-6 months to17 months = 11.4%
decline
Chapter 1 — BLS: Practice, Performance and Training 10 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 1.3: BLS knowledge and attitudes relevant to BLS practice for those who have undergone
Traditional training.
BLS Domains Relevant reviews and studies (% competent)
BLS Knowledge
Health Professionals
o Median competence
39.5% (range 14 - 92.5)
Lay people
o Median competence
64.0% (range 48 - 82)
Overall
o Median 44% (range 14 -
92.5)
o Knowledge level of
mastery similar to that of
skill
Health Professionals median knowledge % (range)
Nurses: 39.5% (37 - 42)
Marzooq & Lyncham, 2009; Kallestedt et al., 2010
Doctors: 36.0 % (14 - 70)
Goodwin, 1992; Noordergraaf et al., 1999; Kallestedt et al., 2010
Medical Students: 65.0% (22 - 92.5)
Grzeskowiak, 2006; Zaheer, & Haque, 2009
Lay Persons
Median knowledge 64.0% (46 - 82)
o From Aldossary et al., 2007; Reder et al., 2006
BLS Knowledge retention
Decline
Overall median decline ≤ 6
months 22.5% (range 4 -
39)
Knowledge decline is
similar to skill decline
Health Professionals (% decline)
Nursing students:
Madden, 2006 - post training to 10wks 38.9% decline
Medical Students:
Creutzfeldt, Hedman, Medin, Heinrichs, & Fellander-Tsai (2010) -
post training to 6 months 22.5% decline
Lay Persons (% decline)
Reder et al. (2006) - post training to 2 months 3.6% decline
Health Professionals
Nursing students:
Madden (2006) – Skill 0% vs Knowledge 72%,
Medical Students:
Grzeskowiak (2006)
o 1st yr skill 56.5% vs knowledge 92.5%
o 6th
yr skill 68.5% vs knowledge 65%
Lay Persons
Reder et al., 2006 - Skill 18.7%, vs knowledge 82%
Good knowledge but poor skills
Skill:
o overall median 37.5%
(range 0 - 68.5)
Knowledge:
o overall median 77.0%
(65 - 92.5)
Health Professionals
Nursing students:
Madden (2006) - Skill 0% vs Knowledge 72%,
Medical Students:
Grzeskowiak (2006)
o 1st yr Skill 56.5% vs Knowledge 92.5%
o 6th
yr Skill 68.5% vs Knowledge 65%
Lay Persons
Reder et al. (2006) – Skill 18.7% vs Knowledge 82%
(continued over the page)
Chapter 1 — BLS: Practice, Performance and Training 11 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 1.3: continued
BLS Domains Relevant reviews and studies (% competent)
Health professionals’ extent of
over-estimation of ability
(BLS skill and knowledge)
Degree of over-estimation
between actual and
estimated ability = median
33.6% (range 18 - 44)
Health Professionals
Nurses:
Marzooq & Lyncham (2009): actual knowledge - 42% vs
Confident in ability - 75.6%;
o Erroneous over-estimation of knowledge 33.6%
Nursing students:
Josipovic et al. (2009): actual skill 34% vs 78% felt prepared
o Erroneous over-estimation of skill 44%
Doctors and Nurses:
Bjorshol (1996): actual Skill 17% vs Believed effective 50%
o Erroneous over-estimation of skill 33%
Medical Students:
Grzeskowiak (2006):
o Actual skill & knowledge 1st yr 74.5% vs own estimation
92.5%
o Actual skill & knowledge 6th
yr 66.8% vs own estimation 94%
o Erroneous over-estimation of skill and knowledge 1st yr 18%,
6th
yr 27.2%
Many of the studies presented report less than 50% skill competence on random
testing of skill in health professionals (Goodwin, 1992; Jensen et al., 2008; Makinen et
al., 2010; Verplancke et al., 2008) and BLS skill and knowledge immediately post
training in both the health professional and lay populations (see Table 1.2 and Table 1.3).
This has been noted even when health professionals‘ knowledge of BLS is relatively good
(see Table 1.3). Furthermore, BLS skill and knowledge also appear to begin to decline as
early as eight weeks post training, with at least 20% skill and knowledge decline by six
months post training (see Table 1.2 and Table 1.3).
Competency in life support testing is usually set at the overall skill mastery level of
between 80% to 100% (Fabius et al., 1994; Frieson & Stotts, 1984; Marzooq & Lyneham,
2009; Morrison, McNally, Wylie, McFaul, & Thompson, 1996; Wayne et al., 2005,
2006). This standard is based on skill mastery principles (Block, 1971) and established
pass-mark setting techniques such as Angoff and Hofstee standard setting methods
(Livingston & Zieky, 1982; Morrison et al., 1996; Wayne et al., 2005). The low BLS
skill and knowledge competence rates post training, on random testing and over-time, in
both the health professional and lay public illustrate that a significant proportion of those
Chapter 1 — BLS: Practice, Performance and Training 12 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
who have received BLS training have not achieved nor maintained skill mastery. These
results indicate low BLS training program effectiveness (see Table 1.2 and Table 1.3).
A number of explanations have been given for the reported difficulty in
performance and retention of BLS skills. While BLS is a set of technical skills, with an
easily defined area of skill, and prescribed competencies (Braun, 2002; Clark et al., 2000;
Lewis, 1997; Moule, Gilbert, & Chalk, 2001), the actual performance of these
psychomotor skills, is considered to be technically complex (Cooper & Cooper, 2008;
Miyadahira, 2001; Salmoni, Schmidt, & Walter, 1984; Wilson, 1994). In addition,
psychological factors such as self-confidence in one‘s own ability, the expected level of
involvement in, and prior experience of, cardiac arrests (which are low-frequency, high-
stress events), have been shown to influence the motivation of health professionals toward
BLS training and performance (Dwyer & Williams, 2002; Lynch & Einspruch, 2010;
Marteau, Johnston, Wynne, & Evans, 1989). Nurses have also reported feeling
marginalised once the arrest team arrives, resulting in them often not being given an
opportunity to put into practice their BLS skills at actual events (Covell, 2006; Dwyer &
Williams 2002; Hamasu et al., 2009; Ranse & Arbon, 2008). Consequently, studies have
reported difficulties in actually performing BLS in accordance with the guidelines
provided by ILCOR, both by health professionals (Higdon et al., 2006; Kirves et al.,
2007; Kobayashi et al., 2008), and members of the general public (Donnelly, Assar, &
Lester, 2000; Rea, Stickney, Doherty, & Lank, 2010).
These widely-reported problems of poor BLS skills amongst health professionals,
students of the health professions, and lay people, and the poor retention of those skills
over time, which have been listed in Table 1.2 and Table 1.3, have led to many authors
recommending a re-evaluation of both the way in which BLS is performed, and the way
in which it is taught (ARC, 2006, 2007a; Chamberlain & Hazinski, 2003; Cummins &
Hazinski, 1999; ILCOR, 2005b, 2005c, 2005e; McClelland, 2007; Richman et al., 2007;
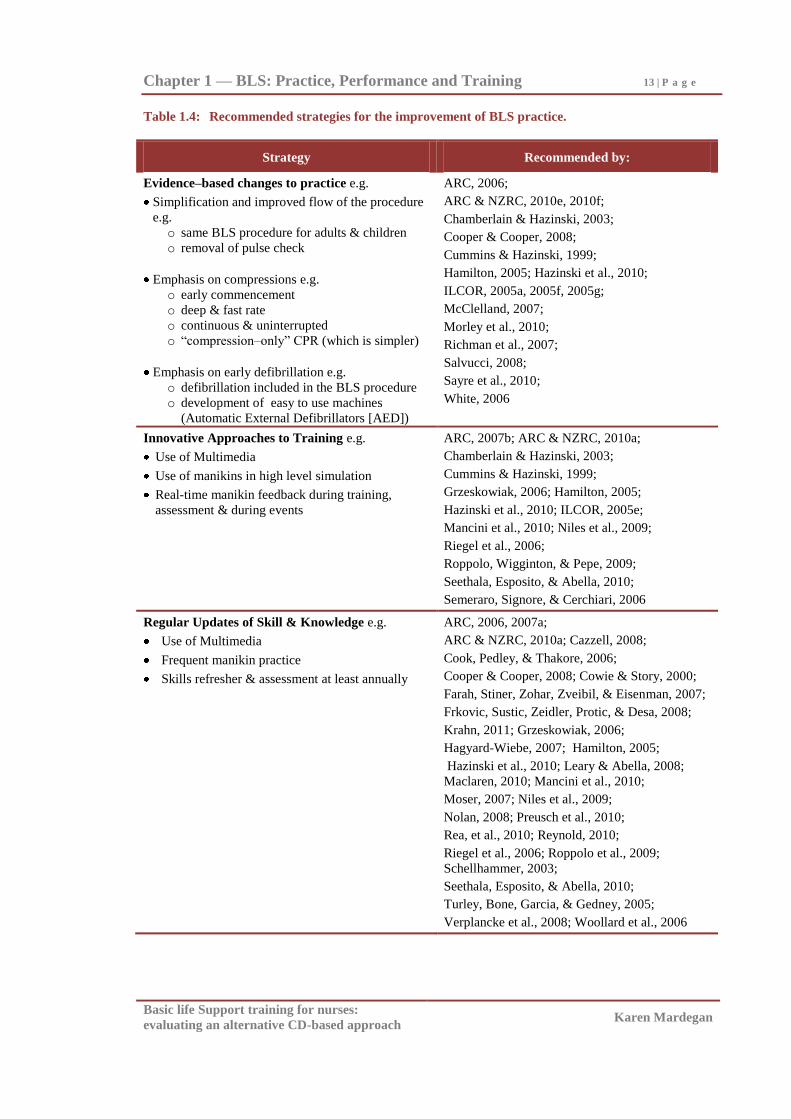
Salvucci, 2008; White, 2006). A range of strategies have been suggested for addressing
BLS skill and retention issues. These include: evidence-based changes to practice which
have led to simplification of the procedure, and an emphasis on compressions and early
defibrillation; the use of innovative approaches to BLS training; and regular updates for
those already trained in BLS (see Table 1.4).
Chapter 1 — BLS: Practice, Performance and Training 13 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 1.4: Recommended strategies for the improvement of BLS practice.
Strategy Recommended by:
Evidence–based changes to practice e.g.
Simplification and improved flow of the procedure
e.g.
o same BLS procedure for adults & children
o removal of pulse check
Emphasis on compressions e.g.
o early commencement
o deep & fast rate
o continuous & uninterrupted
o ―compression–only‖ CPR (which is simpler)
Emphasis on early defibrillation e.g.
o defibrillation included in the BLS procedure
o development of easy to use machines
(Automatic External Defibrillators [AED])
ARC, 2006;
ARC & NZRC, 2010e, 2010f;
Chamberlain & Hazinski, 2003;
Cooper & Cooper, 2008;
Cummins & Hazinski, 1999;
Hamilton, 2005; Hazinski et al., 2010;
ILCOR, 2005a, 2005f, 2005g;
McClelland, 2007;
Morley et al., 2010;
Richman et al., 2007;
Salvucci, 2008;
Sayre et al., 2010;
White, 2006
Innovative Approaches to Training e.g.
Use of Multimedia
Use of manikins in high level simulation
Real-time manikin feedback during training,
assessment & during events
ARC, 2007b; ARC & NZRC, 2010a;
Chamberlain & Hazinski, 2003;
Cummins & Hazinski, 1999;
Grzeskowiak, 2006; Hamilton, 2005;
Hazinski et al., 2010; ILCOR, 2005e;
Mancini et al., 2010; Niles et al., 2009;
Riegel et al., 2006;
Roppolo, Wigginton, & Pepe, 2009;
Seethala, Esposito, & Abella, 2010;
Semeraro, Signore, & Cerchiari, 2006
Regular Updates of Skill & Knowledge e.g.
Use of Multimedia
Frequent manikin practice
Skills refresher & assessment at least annually
ARC, 2006, 2007a;
ARC & NZRC, 2010a; Cazzell, 2008;
Cook, Pedley, & Thakore, 2006;
Cooper & Cooper, 2008; Cowie & Story, 2000;
Farah, Stiner, Zohar, Zveibil, & Eisenman, 2007;
Frkovic, Sustic, Zeidler, Protic, & Desa, 2008;
Krahn, 2011; Grzeskowiak, 2006;
Hagyard-Wiebe, 2007; Hamilton, 2005;
Hazinski et al., 2010; Leary & Abella, 2008;
Maclaren, 2010; Mancini et al., 2010;
Moser, 2007; Niles et al., 2009;
Nolan, 2008; Preusch et al., 2010;
Rea, et al., 2010; Reynold, 2010;
Riegel et al., 2006; Roppolo et al., 2009;
Schellhammer, 2003;
Seethala, Esposito, & Abella, 2010;
Turley, Bone, Garcia, & Gedney, 2005;
Verplancke et al., 2008; Woollard et al., 2006
Chapter 1 — BLS: Practice, Performance and Training 14 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
As poor BLS skill acquisition and retention impacts on the quality of BLS during
actual resuscitations (Dine et al., 2008), the effectiveness of various formats for training
of BLS skills and the required frequency of refresher training and assessment is therefore
of importance. Furthermore, despite these recommendations summarised in Table 1.4,
poor BLS skills demonstrated by health professionals continues to be regularly reported
(Bohn & Gude, 2008; Kakora-Shiner, 2009; Makinen et al., 2007a; Marzooq & Lyncham,
2009; McClelland, 2007; Mellor & Woodard, 2010; Nikandish et al., 2007; Spader,
2008). Yet BLS is a life-saving procedure. So it is of importance that health
professionals and the lay public perform BLS correctly and efficiently. There is therefore
an ongoing need for remediation of the reported deficits, re-evaluation of the BLS skill
for both health professionals and the lay public, and continued development and
evaluation of alternative innovative approaches to training.
Instructional Technology
When attempting to develop skill in trainees, trainers are generally guided by
recommendations from applied psychology research into learning and performance
(Aguinis & Kraiger, 2009). Much of the adult learning research comes from studies of
employees attempting to learn work-related skills (Aguinis & Kraiger, 2009). In the last
four decades there have been seven reviews in the Annual Review of Psychology on
training and development (Aguinis & Kraiger, 2009; Campbell, 1971; Goldstein, 1980;
Latham, 1988; Salas & Cannon-Bowers, 2001; Tannenbaum & Yuki, 1992; Wexley,
1984). Training is defined as ―the systematic approach to affecting individuals‘
knowledge, skills and attitudes in order to improve individual, team and organisational
effectiveness‖ (Aguinis & Kraiger, 2009, p. 452). The reviews examine the need for
training, training design and delivery, training evaluation and transfer of training, and the
influence of training states (i.e. motivation, prior experience, prior training, and self
efficiency) on the outcome of training (Aguinis & Kraiger, 2009).
The life-saving nature of the BLS procedure and skill deficit, outlined earlier,
clearly establishes the need for BLS training, and suggests the need for the review of
particularly BLS training design and delivery methods. Therefore each of these training
Chapter 1 — BLS: Practice, Performance and Training 15 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
and development factors identified in the applied psychology literature are briefly
reviewed below in relation to training design and delivery.
Training design and delivery.
The training design and delivery aspect of these reviews are particularly relevant to
evaluation of BLS skill performance and training. It has been suggested in these reviews
(Aguinis & Kraiger, 2009; Campbell, 1971; Goldstein, 1980; Latham, 1988; Salas &
Cannon-Bowers, 2001; Tannenbaum & Yuki, 1992; Wexley, 1984) that the design of
training should take into account the principles of training, the learning objectives, trainee
characteristics, current knowledge about learning processes and practical considerations
such as constraints and costs in relation to benefits (Arthur, Bennett, Edens & Bell, 2003;
Tannenbaum & Yukl, 1992).
Principles of training design and delivery.
Training design and delivery is considered within these reviews and generally in the
literature, to be most effective when the training method adheres to four basic principles:
Relevant information; Demonstration; Practice; and Feedback (Salas & Cannon-Bowers,
2001). These are summarised in Table 1.5.
The principle of relevance in the reviews pertains to the presented information
being factual, up-to date and covering all aspects of the training, as well as the content
needing to be relevant to the learner. The principle of demonstration includes illustration
of the knowledge, skills and attitudes needed. The opportunity to practise the skill
during, and on an ongoing basis after training, as well as feedback during and after
practice are considered to be essential elements of training design and delivery because it
is thought to particularly assist in the transfer of learning (Aguinis & Kraiger, 2009;
Campbell, 1971; Goldstein, 1980; Latham, 1988; Salas & Cannon-Bowers, 2001;
Tannenbaum & Yuki, 1992; Wexley, 1984).
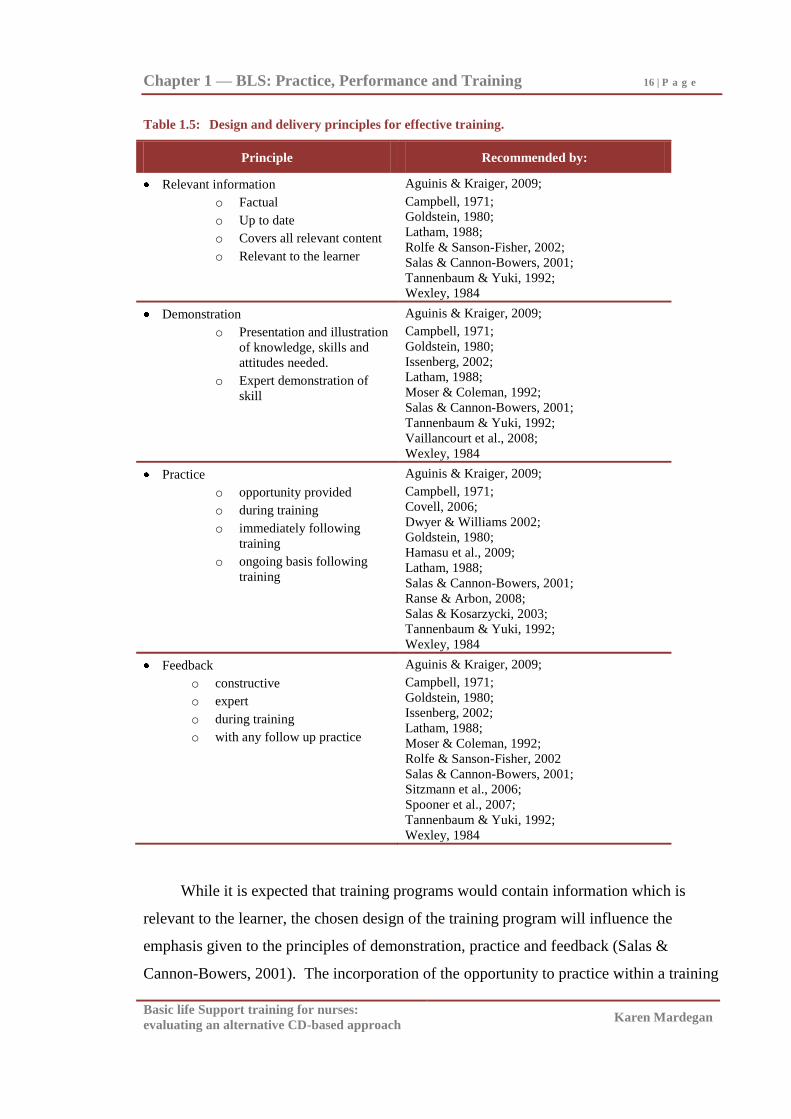
Chapter 1 — BLS: Practice, Performance and Training 16 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 1.5: Design and delivery principles for effective training.
Principle Recommended by:
Relevant information
o Factual
o Up to date
o Covers all relevant content
o Relevant to the learner
Aguinis & Kraiger, 2009;
Campbell, 1971;
Goldstein, 1980;
Latham, 1988;
Rolfe & Sanson-Fisher, 2002;
Salas & Cannon-Bowers, 2001;
Tannenbaum & Yuki, 1992;
Wexley, 1984
Demonstration
o Presentation and illustration
of knowledge, skills and
attitudes needed.
o Expert demonstration of
skill
Aguinis & Kraiger, 2009;
Campbell, 1971;
Goldstein, 1980;
Issenberg, 2002;
Latham, 1988;
Moser & Coleman, 1992;
Salas & Cannon-Bowers, 2001;
Tannenbaum & Yuki, 1992;
Vaillancourt et al., 2008;
Wexley, 1984
Practice
o opportunity provided
o during training
o immediately following
training
o ongoing basis following
training
Aguinis & Kraiger, 2009;
Campbell, 1971;
Covell, 2006;
Dwyer & Williams 2002;
Goldstein, 1980;
Hamasu et al., 2009;
Latham, 1988;
Salas & Cannon-Bowers, 2001;
Ranse & Arbon, 2008;
Salas & Kosarzycki, 2003;
Tannenbaum & Yuki, 1992;
Wexley, 1984
Feedback
o constructive
o expert
o during training
o with any follow up practice
Aguinis & Kraiger, 2009;
Campbell, 1971;
Goldstein, 1980;
Issenberg, 2002;
Latham, 1988;
Moser & Coleman, 1992;
Rolfe & Sanson-Fisher, 2002
Salas & Cannon-Bowers, 2001;
Sitzmann et al., 2006;
Spooner et al., 2007;
Tannenbaum & Yuki, 1992;
Wexley, 1984
While it is expected that training programs would contain information which is
relevant to the learner, the chosen design of the training program will influence the
emphasis given to the principles of demonstration, practice and feedback (Salas &
Cannon-Bowers, 2001). The incorporation of the opportunity to practice within a training
Chapter 1 — BLS: Practice, Performance and Training 17 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
program is considered necessary for skill acquisition. However, not all practice was
considered equal (Salas & Kosarzycki, 2003). Although repeated practice is
recommended throughout training (Tannenbaum & Yakl, 1992), recent reviews of
research are beginning to suggest that to be effective, practice may involve a complex
process, not just task repetition (Salas & Cannon-Bowers, 2001; Salas & Kosarzycki,
2003). Effective practice has been determined to involve restating or applying the
principles covered in training rather than just recalling them. It also needs to involve the
opportunity to adapt the learned behaviour/skill to varying situations rather than just
imitating it repeatedly in the same situation (Salas & Kosarzycki, 2003; Tannenbaum &
Yakl, 1992).
Significant decay in skill acquisition was also regularly reported in these reviews,
especially when delays between training and implementation occurred (Salas & Cannon-
Bowers, 2001). Therefore the need for immediate and ongoing opportunity to apply the
training and practise the skill within the post-training environment was also seen as being
crucial to knowledge and skill transfer, and long-term retention (Aguinis & Kraiger,
2009; Salas & Cannon-Bowers, 2001; Salas & Kosarzycki, 2003; Tannenbaum & Yuki,
1992).
Feedback both during and after practice has also been identified in the reviews as an
essential ingredient for effective training (Salas & Kosarzycki, 2003; Sitzmann, Kraiger,
Stewart & Wisher, 2006). The benefit of feedback also appears to be enhanced if it is
specific to the individual (Salas & Kosarzycki, 2003; Sitzmann et al., 2006). The reviews
suggest that all available sources of feedback should be used and it should be accurate,
credible, timely and constructive (Tannenbaum & Yakl, 1992). Feedback should be
immediate and trainees should be given specific feedback on what was done correctly,
what mistakes were made, and be directed to appropriate alternatives (Salas &
Kosarzycki, 2003; Tannenbaum & Yakl, 1922).
Training delivery methods.
Within the reviews it appears that researchers are seeking cost-effective, content-
valid, easy to use, engaging and technology-based methods for the delivery of training
(Salas & Cannon-Bowers, 2001). Training is reported to continue to rely heavily on
classroom techniques, however training methods which have received the most attention
Chapter 1 — BLS: Practice, Performance and Training 18 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
in the reviews are those involving technologies such as video conferencing, video,
computer-aided instruction, equipment simulators, simulations, games, online internet
training delivery options (Aguinis & Kraiger, 2009; Goldstein, 1980; Latham, 1988; Salas
& Cannon-Bowers, 2001; Tannenbaum & Yakl, 1992). These methods reduce the need
for human instructors. The suggested benefits of these methods are: more opportunities
for self-pacing, active involvement and expert tutoring for each trainee (Tannenbaum &
Yakl, 1992). Advancements in these training methods continue at a rapid pace. The
linking of several of these training methods within the one program has also been thought
to enhance the benefits of these methods (Goldstein, 1980; Latham, 1988; Salas &
Cannon-Bowers, 2001; Tannenbaum & Yakl, 1992).
In conjunction with the review of training delivery technologies, some attention in
these reviews has also been given to team training (Salas & Cannon-Bowers, 2001;
Tannenbaum & Yakl, 1992). Knowledge transfer and the development of effective
communication, co-ordination, compensatory behaviour, mutual performance, exchange
of feedback, peer support and adaption to varying situational demands have been
suggested benefits for employing team training methods (Aguinis & Kraiger, 2009; Salas
& Cannon-Bowers, 2001; Tannenbaum & Yakl, 1992).
Trainee characteristics.
Another prominent feature in the reviews was the emphasis placed on the influence
of trainee characteristics on skill acquisition and retention (Aguinis & Kraiger, 2009;
Latham, 1988; Salas & Cannon-Bowers, 2001; Tannenbaum & Yukl, 1992). Self
efficacy, a person‘s self confidence or belief in their ability to perform a specific task, and
motivation are seen as predictors of training success as they are believed to lead to better
learning and performance (Goldstein, 1980; Latham, 1988; Salas & Cannon-Bowers,
2001; Tannenbaum & Yakl, 1992). General intelligence (cognitive ability) is seen to
promote self efficacy and performance (Salas & Cannon-Bowers, 2001). Furthermore, if
the training is mandatory versus voluntary, it is also thought to enhance motivation to
learn (Salas & Cannon- Bowers, 2001; Tannenbaum & Yakl, 1992). Not surprisingly,
higher trainee motivation has been associated with greater learning and more positive
reactions to the training (Aguinis & Kraiger, 2009; Latham, 1988; Tannenbaum & Yakl,
1992). In addition, it has also been suggested that trainees‘ previous experiences (both
Chapter 1 — BLS: Practice, Performance and Training 19 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
positive and negative), expectations of the training, and prior training also affect learning
and retention (Latham, 1988; Salas & Cannon- Bowers, 2001).
In conclusion, these reviews of training design and delivery would suggest that a
training program which addresses the training and delivery principles of relevance,
demonstration, practice and feedback, along with attitudinal concepts within the design of
the skills training program would most likely be the most effective form of training. It is
noteworthy that the recommended strategies for the improvement of BLS performance
(presented in Table 1.4) and the noted relevance of trainee characteristics within the BLS
literature are congruent with this applied psychology literature.
Basic Life Support Training and Assessment
Modern Basic Life Support techniques were first standardised in the 1960s (Dent &
Gillard, 1993). Since then, more than 40 years of training of firstly health professionals,
and more recently, the lay population, has occurred (Brennan & Braslow, 1998;
Whitcomb & Blackman, 2007).
Regulation of BLS training programs.
The design of BLS training courses and regulation of BLS training, are governed by
each country‘s (or union‘s) respective resuscitation council. The key organisations that
are represented on each resuscitation council are country (or union) specific, but examples
of organisations that are usually represented are: the Red Cross, National Heart
Foundations and associations, medical and nursing professional bodies, national first aid
organisations, safety councils, surf-life-saving associations, and ambulance organisations.
These organisations, along with health facilities, educational institutions, health
professional associations, and private organisations, are the key players in the design and
regulation of BLS courses, while also being the main providers, worldwide, of BLS
training. The BLS courses provided by these organisations are designed to comply with
the standards of ILCOR and the relevant resuscitation council.
In Australia, all providers of resuscitation training programs are required to follow
ARC guidelines, which themselves were developed and revised to comply with the
standards of ILCOR (Australian Critical Care Nurses & ARC, 2008; ARC, 2006, 2007a,
2007b; ARC & NZRC, 2010 a, b, f, g). Using these guidelines, the Australian
Chapter 1 — BLS: Practice, Performance and Training 20 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Community Services and Health Industry Skills Council sets requirements and monitors
registered community providers of programs (Registered Training Authorities - RTOs).
The release, in 2007, of the Health Training HLT07 Package, is a progressive step aimed
at prescribing the course content of community programs providing first aid and BLS
training (Community Services & Health Industry Skills Council). Key providers of these
community programs in Australia are: the Australian Red Cross, St John Ambulance, Surf
Life Saving Australia, along with many private providers (for example A & A Training,
EmergCare, and Premium Health). In the Australian health and tertiary education sectors,
BLS initial training and reaccreditation (refresher) programs are predominately provided
to health staff and students by their education departments, in accordance with the ARC
guidelines.
Traditional BLS training approaches.
The format for the majority of BLS training programs, for both health professionals
and lay people, around the world, is predominately a Traditional instructor-led program
which contains a presentation, the demonstration of the BLS steps using a manikin, and
trainees‘ supervised practice of the BLS procedure on manikins, with feedback on
performance provided by the instructor (Australian Red Cross; St John Ambulance
Australia; Surf-Life Saving Australia; Kallestedt et al., 2010; Stromsoe et al., 2010). In
some courses, the Traditional program has evolved to include a
presentation/demonstration that is supplemented by instruction provided by Videotape or
DVD, followed by instructor-supervised manikin practice (American Heart Association;
Cason et al., 2009; Christenson et al., 2007; Mancini et al., 2009; Roppolo et al., 2007;
Swigger, 2001). The manikins typically used are essentially a replica of the human head
and upper torso, therefore allowing ventilation of the lungs, and chest compressions, to be
simulated. Manikins have evolved to include models that also incorporate ventilation and
compression performance feedback devices (Bohn et al., 2011; Spooner et al., 2007;
Sutton et al., 2007; Van Berkom, Noordergraaf, Scheffer, & Noordergraaf, 2008; Van
Berkom & Noordergraaf, 2008; Wik, Thowsen, & Steen, 2001).
The content of a Traditional program often extends beyond BLS to incorporate
general first aid and recognition and management of respiratory and cardiac conditions.
For example, the US AHA Heartsaver course teaches adult rescuer BLS, management of
Chapter 1 — BLS: Practice, Performance and Training 21 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
airway obstruction, as well as recognition and prevention of heart disease (American
Heart Association). Furthermore, in Traditional programs, all steps in the BLS procedure
are firstly outlined and then the techniques of artificial ventilation and cardiac
compression are explained, demonstrated, and then practised.
Training programs using the Traditional approach usually range from three to six
hours in length, depending on the country (Braslow et al., 1997; Brennan & Braslow,
1998; Kallestedt et al., 2010; Madden, 2006; Todd et al., 1998, 1999; Woollard et al.,
2004). Instructor to trainee ratios vary, but usually do not exceed one instructor to eight
trainees, and trainees often share a manikin and therefore have limited practice time
(Todd et al., 1999). Aside from concerns about the potential for limited manikin practice
with the design of Traditional BLS training, the design has incorporated the four
principles of training design and delivery ‗relevant information, demonstration, practice
and feedback‘ (Salas & Cannon-Bowers, 2001), and as such should therefore be an
effective form of training.
BLS assessment.
BLS knowledge, when specifically assessed, is usually tested with a short- answer
and/or a multiple-choice examination, and this is often in the context of a broader first aid
program (Cason et al., 2008; Creutzfeldt, Hedman, Medin, Stengard, & Fellander-Tsai,
2009; Creutzfeldt, Hedman, Medin, Heinrichs, & Fellander-Tsai, 2010; Moule, Albarran,
Bessant, Brownfield, & Pollock, 2008a). Performance of BLS skill is most commonly
assessed by a certified instructor and participants are expected to perform according to a
set skills checklist (Khan, Shafquat, & Kundi, 2010; Makinen, Niemi-Murola, Makela, &
Castren, 2007b; Van der Heide, Toledo-Eppinga, Van der Heide, & Van der Lee, 2006).
In more recent years, this instructor assessment has often been paralleled by an
instrumented (automated) manikin, which produces a recording of CPR performance
(Lynch, Einspruch, Nichol, & Aufderheide, 2008; Makinen et al., 2007b; Van Berkom &
Noordergraaf, 2008). One such model is the Skill Reporter™
Resusci Anne® Manikin,
which was produced by Laerdal and used in this thesis (Laerdal, 2002; Todd et al., 1999).
This device is a standard Laerdal manikin – a rubber replica of the human head and upper
torso, which is instrumented with electronic sensors that compute and generate a digital
record of ventilation and chest compression characteristics, which can be printed out and
interpreted. It is calibrated to comply with the criteria of the relevant resuscitation
Chapter 1 — BLS: Practice, Performance and Training 22 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
council. The manikin provides feedback on CPR performance when used for practice,
and provides an independent analysis of CPR performance when used during assessment
(Laerdal, 2002; Todd et al., 1999).
A small number of studies have relied on manikin assessment of CPR skills alone
(Choa et al., 2006, 2008; Fabius et al., 1994; Kardong-Edgren, Oermann, Odom-Maryon,
& Ha, 2010; Thoren, Axelsson, & Herlitz, 2007). The limitations of these studies are
essentially that they are only assessing the CPR component of BLS not the full BLS
procedure and as such skill reliability has not been fully established. Furthermore, good
correlation between the two forms of assessment of CPR skills has not always been found
when assessments of CPR performance by instructors (utilising a checklist) have been
paralleled by, and compared with, the print-outs produced by an instrumented manikin
(Jensen et al, 2008; Kaye & Mancini, 1998; Lynch et. al., 2008; Makinen et al., 2007b;
Ringsted et al., 2007; Van Berkom & Noordergraaf, 2008). Consequently dual
assessment of BLS performance is advocated by many researchers (Jensen et al, 2008;
Makinen et al., 2007b; Ringsted et al., 2007; Van Berkom & Noordergraaf, 2008).
Owing to the documented high degree of BLS skill decay (Braslow et al., 1997;
Einspruch et al., 2007; Mancini & Kaye, 1985; Reder et al., 2006; Roppolo et al., 2007;
Smith et al., 2008), regular formal re-training and re-assessment (called reaccreditation)
in BLS is a requirement for health professionals. The literature suggests that revision is
needed every three to six months (see for example Anthonypillai, 1992; ARC, 2007a;
Baessler, 2000; Broomfield, 1996; Davies & Gould, 2000; Farah et al., 2007; Garvey,
1999; ILCOR, 2005; O‘Steen, Kee, & Minick, 1996; West, 2000; Woollard et al., 2006).
Consideration of the logistics of reaccrediting large numbers of both health professionals
and lay people (Taylor, 2008) has led to the recommendation in the Australian guidelines
of frequent practice and at least 12 monthly reaccreditation (ARC, 2007a; ARC & NZRC,
2010a; Hazinski et al., 2010; ILCOR, 2005; Mancini et al., 2010).
Time-efficient and cost-effective alternatives for BLS re-training are required if
regular reaccreditation is to be achieved for all health professionals and the lay public.
The emergence of analogue Videotape and digital media, including the CD, DVD and
Internet, has allowed the development of innovative and flexible delivery tools for
education and training. The use of digital media to deliver BLS training, could be an
Chapter 1 — BLS: Practice, Performance and Training 23 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
effective answer to the 2005 and 2010 ILCOR recommendations for innovative
approaches to BLS training and may have the potential to improve the standard of BLS
skills in health professionals and the lay public in a more efficient manner. It could also
be of value in overcoming some of the logistical difficulties with the provision of frequent
practice and re-training.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Chapter 2
Basic Life Support Training:
Review of the Effectiveness of Training Methods
In order to address BLS performance and training delivery concerns, future
directions for BLS training needs to be derived from the evaluation of Traditional and
alternative BLS training methods. The research selected in this chapter appraises BLS
skill and/or knowledge following training via Traditional and the alternative Video, DVD,
CD and Internet BLS training methods. It was obtained via medline, cinhl, embase and
current content database searches using the key terms: Basic Life Support, Cardiac life
support, Cardiopulmonary Resuscitation, Cardiorespiratory resuscitation, mouth to mouth
resuscitation, education, training, instruction, skill, CD, Video, DVD, Multimedia,
Internet, Web, Computer, re-accreditation, recertification, reassessment and abbreviations
and combinations of these terms. The databases were searched from 1960 to present.
The presented literature is from 1990 to October 2011. A review of this BLS training
method literature and how this research informs BLS training and practice follows.
Evaluation of Traditional Training Programs
Since the inception of BLS training, numerous studies have evaluated health
professionals‘ and/or lay people‘s BLS skills, therefore indirectly assessing the
effectiveness of Traditional BLS training. Some examples of this research have been
presented in chapter one (see Table 1.2). Nine recent studies which have evaluated BLS
skill and knowledge post Traditional BLS training have been outlined in Table 2.1. These
include four involving training of health professionals and five with various lay
populations.
These nine studies comprised one randomised controlled trial (Andresen, Arntz,
Grafling, Hoffman, Hofmann, &Kraemer, 2008), seven prospective studies and five that
included a pre-test, three of which were in health professionals and two in lay people. No
comparison group was included in the design of seven out of the nine studies.
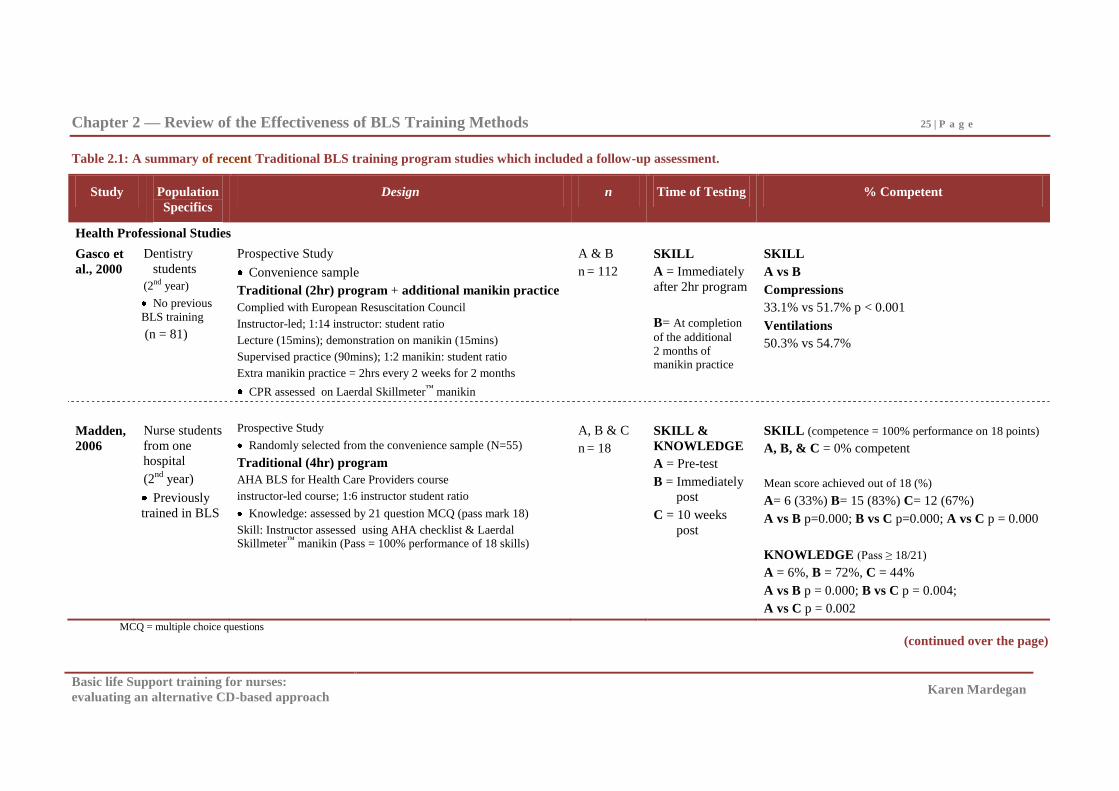
Chapter 2 — Review of the Effectiveness of BLS Training Methods 25 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.1: A summary of recent Traditional BLS training program studies which included a follow-up assessment.
Study Population
Specifics
Design n Time of Testing % Competent
Health Professional Studies
Gasco et
al., 2000
Dentistry
students
(2nd year)
No previous
BLS training
(n = 81)
Prospective Study
Convenience sample
Traditional (2hr) program + additional manikin practice
Complied with European Resuscitation Council
Instructor-led; 1:14 instructor: student ratio
Lecture (15mins); demonstration on manikin (15mins)
Supervised practice (90mins); 1:2 manikin: student ratio
Extra manikin practice = 2hrs every 2 weeks for 2 months
CPR assessed on Laerdal Skillmeter™ manikin
A & B
n = 112
SKILL
A = Immediately
after 2hr program
B= At completion
of the additional
2 months of manikin practice
SKILL
A vs B
Compressions
33.1% vs 51.7% p < 0.001
Ventilations
50.3% vs 54.7%
Madden,
2006
Nurse students
from one
hospital
(2nd
year)
Previously
trained in BLS
Prospective Study
Randomly selected from the convenience sample (N=55)
Traditional (4hr) program
AHA BLS for Health Care Providers course
instructor-led course; 1:6 instructor student ratio
Knowledge: assessed by 21 question MCQ (pass mark 18)
Skill: Instructor assessed using AHA checklist & Laerdal Skillmeter™ manikin (Pass = 100% performance of 18 skills)
A, B & C
n = 18
SKILL &
KNOWLEDGE
A = Pre-test
B = Immediately
post
C = 10 weeks
post
SKILL (competence = 100% performance on 18 points)
A, B, & C = 0% competent
Mean score achieved out of 18 (%)
A= 6 (33%) B= 15 (83%) C= 12 (67%)
A vs B p=0.000; B vs C p=0.000; A vs C p = 0.000
KNOWLEDGE (Pass ≥ 18/21)
A = 6%, B = 72%, C = 44%
A vs B p = 0.000; B vs C p = 0.004;
A vs C p = 0.002
MCQ = multiple choice questions
(continued over the page)
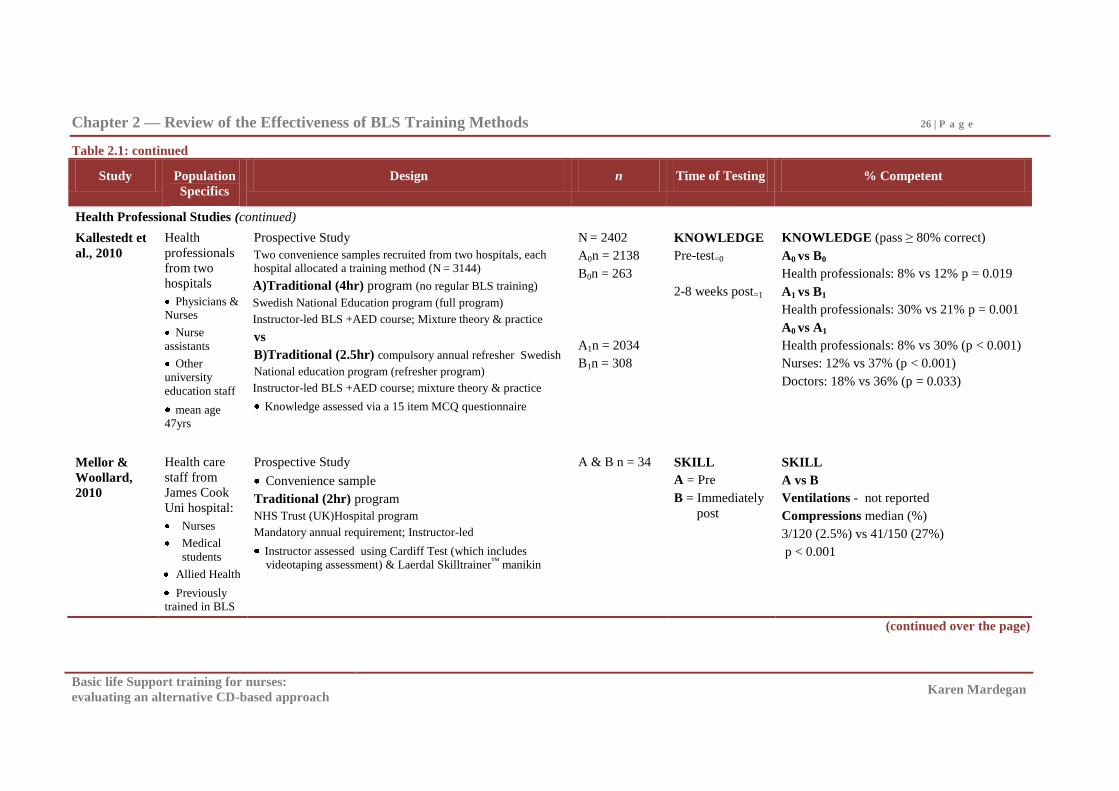
Chapter 2 — Review of the Effectiveness of BLS Training Methods 26 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.1: continued
Study Population
Specifics
Design n Time of Testing % Competent
Health Professional Studies (continued)
Kallestedt et
al., 2010
Health
professionals
from two
hospitals
Physicians & Nurses
Nurse
assistants
Other
university
education staff
mean age 47yrs
Prospective Study
Two convenience samples recruited from two hospitals, each hospital allocated a training method (N = 3144)
A)Traditional (4hr) program (no regular BLS training)
Swedish National Education program (full program)
Instructor-led BLS +AED course; Mixture theory & practice
vs
B)Traditional (2.5hr) compulsory annual refresher Swedish
National education program (refresher program)
Instructor-led BLS +AED course; mixture theory & practice
Knowledge assessed via a 15 item MCQ questionnaire
N = 2402
A0n = 2138
B0n = 263
A1n = 2034
B1n = 308
KNOWLEDGE
Pre-test=0
2-8 weeks post=1
KNOWLEDGE (pass ≥ 80% correct)
A0 vs B0
Health professionals: 8% vs 12% p = 0.019
A1 vs B1
Health professionals: 30% vs 21% p = 0.001
A0 vs A1
Health professionals: 8% vs 30% (p < 0.001)
Nurses: 12% vs 37% (p < 0.001)
Doctors: 18% vs 36% (p = 0.033)
Mellor &
Woollard,
2010
Health care
staff from
James Cook
Uni hospital:
Nurses
Medical
students
Allied Health
Previously trained in BLS
Prospective Study
Convenience sample
Traditional (2hr) program
NHS Trust (UK)Hospital program
Mandatory annual requirement; Instructor-led
Instructor assessed using Cardiff Test (which includes videotaping assessment) & Laerdal Skilltrainer™ manikin
A & B n = 34
SKILL
A = Pre
B = Immediately
post
SKILL
A vs B
Ventilations - not reported
Compressions median (%)
3/120 (2.5%) vs 41/150 (27%)
p < 0.001
(continued over the page)
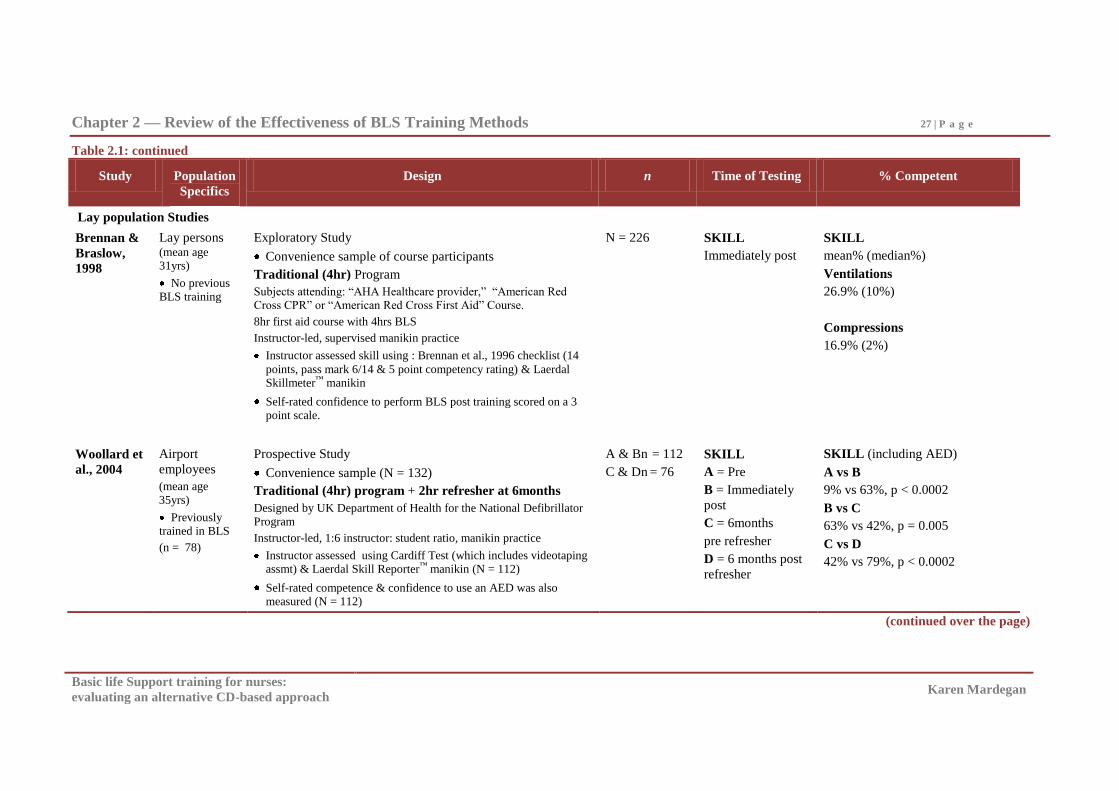
Chapter 2 — Review of the Effectiveness of BLS Training Methods 27 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.1: continued
Study Population
Specifics
Design n Time of Testing % Competent
Lay population Studies
Brennan &
Braslow,
1998
Lay persons (mean age 31yrs)
No previous BLS training
Exploratory Study
Convenience sample of course participants
Traditional (4hr) Program
Subjects attending: ―AHA Healthcare provider,‖ ―American Red Cross CPR‖ or ―American Red Cross First Aid‖ Course.
8hr first aid course with 4hrs BLS
Instructor-led, supervised manikin practice
Instructor assessed skill using : Brennan et al., 1996 checklist (14
points, pass mark 6/14 & 5 point competency rating) & Laerdal Skillmeter™ manikin
Self-rated confidence to perform BLS post training scored on a 3 point scale.
N = 226 SKILL
Immediately post
SKILL
mean% (median%)
Ventilations
26.9% (10%)
Compressions
16.9% (2%)
Woollard et
al., 2004
Airport
employees
(mean age
35yrs)
Previously trained in BLS
(n = 78)
Prospective Study
Convenience sample (N = 132)
Traditional (4hr) program + 2hr refresher at 6months
Designed by UK Department of Health for the National Defibrillator Program
Instructor-led, 1:6 instructor: student ratio, manikin practice
Instructor assessed using Cardiff Test (which includes videotaping assmt) & Laerdal Skill Reporter™ manikin (N = 112)
Self-rated competence & confidence to use an AED was also measured (N = 112)
A & Bn = 112
C & Dn = 76
SKILL
A = Pre
B = Immediately
post
C = 6months
pre refresher
D = 6 months post
refresher
SKILL (including AED)
A vs B
9% vs 63%, p < 0.0002
B vs C
63% vs 42%, p = 0.005
C vs D
42% vs 79%, p < 0.0002
(continued over the page)
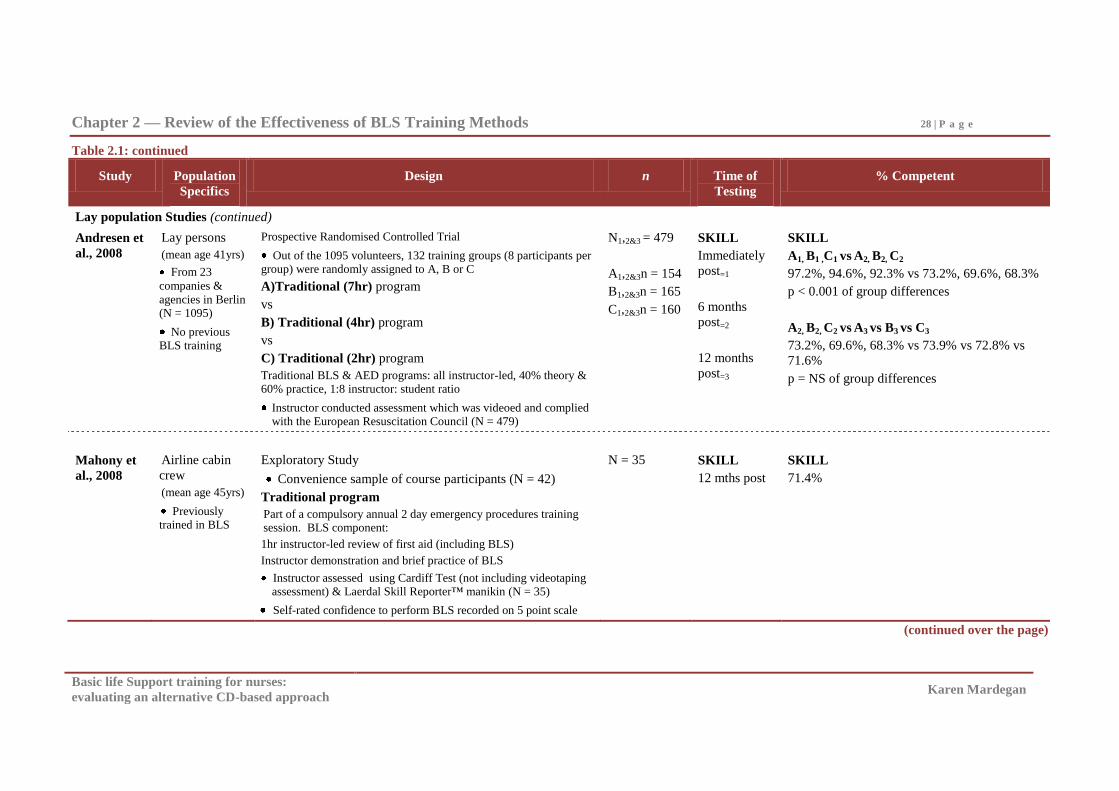
Chapter 2 — Review of the Effectiveness of BLS Training Methods 28 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.1: continued
Study Population
Specifics
Design n Time of
Testing
% Competent
Lay population Studies (continued)
Andresen et
al., 2008
Lay persons
(mean age 41yrs)
From 23
companies &
agencies in Berlin (N = 1095)
No previous BLS training
Prospective Randomised Controlled Trial
Out of the 1095 volunteers, 132 training groups (8 participants per group) were randomly assigned to A, B or C
A)Traditional (7hr) program
vs
B) Traditional (4hr) program
vs
C) Traditional (2hr) program
Traditional BLS & AED programs: all instructor-led, 40% theory & 60% practice, 1:8 instructor: student ratio
Instructor conducted assessment which was videoed and complied with the European Resuscitation Council (N = 479)
N1,2&3 = 479
A1,2&3n = 154
B1,2&3n = 165
C1,2&3n = 160
SKILL
Immediately
post=1
6 months
post=2
12 months
post=3
SKILL
A1, B1 ,C1 vs A2, B2, C2
97.2%, 94.6%, 92.3% vs 73.2%, 69.6%, 68.3%
p < 0.001 of group differences
A2, B2, C2 vs A3 vs B3 vs C3
73.2%, 69.6%, 68.3% vs 73.9% vs 72.8% vs
71.6%
p = NS of group differences
Mahony et
al., 2008
Airline cabin
crew
(mean age 45yrs)
Previously trained in BLS
Exploratory Study
Convenience sample of course participants (N = 42)
Traditional program
Part of a compulsory annual 2 day emergency procedures training session. BLS component:
1hr instructor-led review of first aid (including BLS)
Instructor demonstration and brief practice of BLS
Instructor assessed using Cardiff Test (not including videotaping assessment) & Laerdal Skill Reporter™ manikin (N = 35)
Self-rated confidence to perform BLS recorded on 5 point scale
N = 35
SKILL
12 mths post
SKILL
71.4%
(continued over the page)
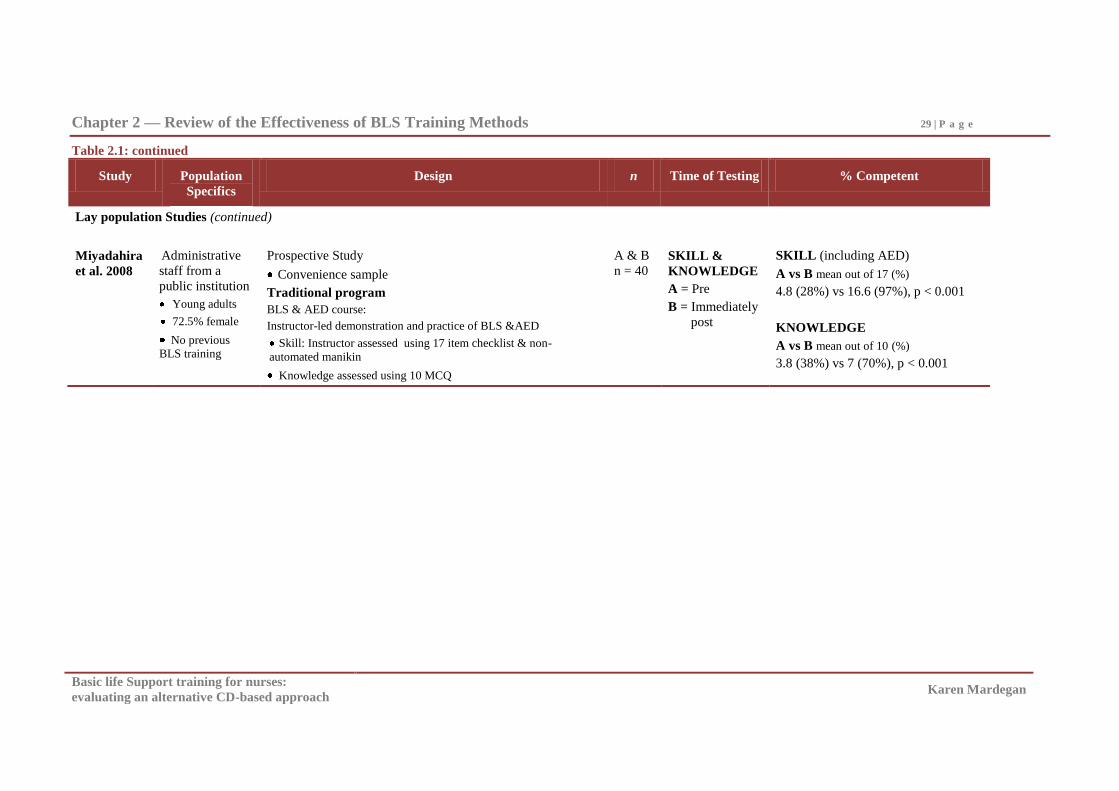
Chapter 2 — Review of the Effectiveness of BLS Training Methods 29 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.1: continued
Study Population
Specifics
Design n Time of Testing % Competent
Lay population Studies (continued)
Miyadahira
et al. 2008
Administrative
staff from a
public institution
Young adults
72.5% female
No previous BLS training
Prospective Study
Convenience sample
Traditional program
BLS & AED course:
Instructor-led demonstration and practice of BLS &AED
Skill: Instructor assessed using 17 item checklist & non-
automated manikin
Knowledge assessed using 10 MCQ
A & B
n = 40
SKILL &
KNOWLEDGE
A = Pre
B = Immediately
post
SKILL (including AED)
A vs B mean out of 17 (%)
4.8 (28%) vs 16.6 (97%), p < 0.001
KNOWLEDGE
A vs B mean out of 10 (%)
3.8 (38%) vs 7 (70%), p < 0.001
Chapter 2 — Review of the Effectiveness of BLS Training Methods 30 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Sample sizes ranged from 3144 in the Kallestedt et al., (2010) BLS knowledge study to
four BLS skill studies with samples sizes between 112 – 479 (Andresen et al., 2008;
Brennan & Braslow 1998; Gasco, Avellanel, & Sanchez 2000; Woollard et al., 2004), and
four where the sample sizes were 18 - 40 participants (Madden, 2006; Mahony, Griffiths,
Larsen, & Powell, 2008; Mellor &Woollard, 2010; Miyadahira, Quilici, Martins, Araujo,
& Pelliciotti, 2008).
From these Traditional approaches (presented in Table 2.1), BLS skill competence
immediately post training was found to be between zero and 33% in health professionals
with (Madden, 2006; Mellor & Woollard, 2010) and without (Gasco, Avellanel, &
Sanchez 2000) previous training. BLS skill competence immediately post training in lay
populations appears to be more variable than in health professional groups with two
studies reporting competence immediately post training ranged from 17% to 63%
(Brennan & Braslow 1998; Woollard et al., 2004), and two where competence was 92%
to 97% (Andresen et al., 2008; Miyadahira et al., 2008).
The two health professional (Gasco et al., 2000; Madden, 2006) and three lay
(Andresen et al., 2008; Mahony et al., 2008; Woollard et al., 2004) studies in Table 2.1,
that examined retention of BLS skill, suggest that BLS skill deteriorates by at least 20%
by two to six months post Traditional training. The data, however, suggest that a
refresher practice two to six months after training could assist in the maintenance of skill
in both the health professional and lay populations (Gasco et al., 2000; Wollard et al.,
2004).
Of the three studies in Table 2.1 which examined BLS knowledge, it appears that
knowledge immediately post training is around 70% for both health professionals
(Madden, 2006) and lay people (Miyadahira et al., 2008), but as seen with skill, BLS
knowledge declines to 21 - 44% of health professionals maintaining knowledge
competence by eight to ten weeks post training (Madden, 2006; Kallestedt et al., 2010).
The wide range of mastery levels demonstrated post training and the noted
deterioration of skill and knowledge competency over time suggest that Traditional BLS
programs have limits to their effectiveness in training health professionals and lay people
in BLS (Hagmann, 2007; Hamilton, 2005). This is consistent with the overview of BLS
skill and knowledge presented in Table 1.2 and Table 1.3. It is, however surprising,
Chapter 2 — Review of the Effectiveness of BLS Training Methods 31 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
considering that the Traditional training method incorporates all four training design and
delivery principles (Salas & Cannon-Bowers, 2001). This reduced effectiveness with
Traditional training methods could be attributed partially to the potential variation in the
content and delivery of the program by the various human instructors, the limited amount
of opportunity to practise when manikins are shared, (typical in Traditional programs),
and the variability in the provision of feedback to trainees. How skill and knowledge are
rated, be it an overall score or designated items deemed mandatory (Kallestedt et al.,
2010), can also potentially influence the determination of competence.
It is assumed that program content is designed, delivered and assessed by experts.
The concerns with this training method are therefore most likely attributed to the reduced
opportunity to practise with feedback, during and on an ongoing basis following the
training (Gasco et al., 2000; Wollard et al., 2004). Exploration of training methods which
incorporate more practice time and allow for ongoing practice with feedback at a time
convenient to the user, such as Multimedia methods, warrant consideration in view of the
suboptimal outcomes and potential benefits of additional practise suggested in this review
of Traditional training methods.
Alternatives to the Traditional Approach to BLS Training
Alternatives to the Traditional presentation/demonstration/supervised manikin
practice approach to BLS skills training include: BLS training programs delivered
through Videotape, DVD, and CD training packages (most of which are now also able to
be accessed via the Internet). A review of the effectiveness of these BLS training
alternatives is presented below.
Basic life support training using Videotape.
Videotapes were initially used in BLS training in attempts to accommodate the
large number of health professionals and lay people who needed to be trained in BLS
(Hekelman, Phillips, & Bierer, 1990; Schluger, Hayes, Turino, Fischman, & Fox, 1987).
It was hoped that BLS training presented in this format would be equally as effective or
more effective than Traditional training methods, would reach larger audiences, and thus
reduce training times (Batcheller et al., 2000; Braslow et al.,1997; Todd et al., 1998,
1999).
Chapter 2 — Review of the Effectiveness of BLS Training Methods 32 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Founding studies in BLS Video.
Evaluation of BLS Videos began around the 1980s (Plank & Steinke, 1989;
Schluger et al., 1987). However, it was not until the publication of the Braslow et al.
(1997), Todd et al. (1998, 1999), and Batcheller et al. (2000) BLS Video studies, that the
merits of Video as a possible alternative to Traditional BLS training were seriously
contemplated. These four founding studies, three evaluating lay populations and one
involving medical students have been summarised in Table 2.2.
These early Video studies (Braslow et al., 1997; Todd et al., 1998, 1999; Batcheller
et al., 2000) compared the BLS performance of a Traditionally-trained group who
attended the four hour American Heart Association (AHA) Heartsaver course with that of
a group who trained using a 34 minute self-instructional Videotape and unsupervised
manikin practice program developed by the Braslow team in 1997.
They (Braslow et al., 1997; Todd et al., 1998, 1999; Batcheller et al., 2000), did not
include a pre-test, but the Todd (et al., 1998, 1999) and Batcheller (et al., 2000) teams
randomised participants to Video and Traditional BLS training groups, and used sample
sizes ranging from 89 (Todd et al., 1998) to 202 (Batcheller et al., 2000) following the
larger initial study conducted by Braslow et al. (1997) in lay participants which evaluated
a convenience sample of 643 people. Post test intervals varied from immediately post
training (Braslow et al., 1997; Batcheller et al., 2000) to 106 days post training (Todd et
al., 1998). In each case, the value of the Braslow et al. (1997) Videotape Self Instruction
(VSI) method for BLS training for both student health professionals and the general
community was demonstrated. Competence for those trained by the VSI method was
81% at 106 days post training for medical students (Todd et al., 1998) and ranged from
63-80% immediately post training for lay people (Batcheller et. al., 2000; Braslow et al.,
1997). By comparison, skill competence in those completing the Traditional program
was 57% in medical students at 106 days post training (Todd et al., 1998) and ranged
from six to 45% immediately post training in lay samples (Batcheller et. al., 2000;
Braslow et al., 1997). The significantly higher pass rates for those trained using the VSI
method compared with the Traditional method suggests that the VSI method is better than
Traditional methods.
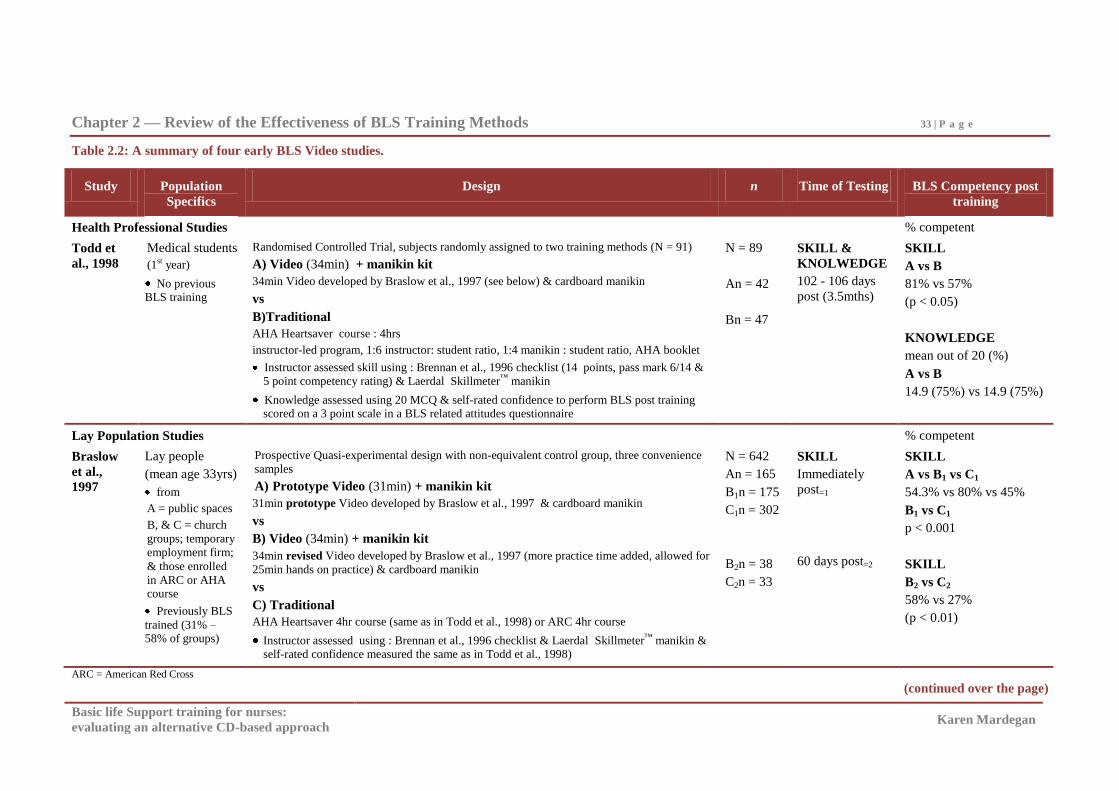
Chapter 2 — Review of the Effectiveness of BLS Training Methods 33 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.2: A summary of four early BLS Video studies.
ARC = American Red Cross
(continued over the page)
Study Population
Specifics
Design n Time of Testing BLS Competency post
training
Health Professional Studies % competent
Todd et
al., 1998
Medical students
(1st year)
No previous BLS training
Randomised Controlled Trial, subjects randomly assigned to two training methods (N = 91)
A) Video (34min) + manikin kit
34min Video developed by Braslow et al., 1997 (see below) & cardboard manikin
vs
B)Traditional
AHA Heartsaver course : 4hrs
instructor-led program, 1:6 instructor: student ratio, 1:4 manikin : student ratio, AHA booklet
Instructor assessed skill using : Brennan et al., 1996 checklist (14 points, pass mark 6/14 &
5 point competency rating) & Laerdal Skillmeter™ manikin
Knowledge assessed using 20 MCQ & self-rated confidence to perform BLS post training scored on a 3 point scale in a BLS related attitudes questionnaire
N = 89
An = 42
Bn = 47
SKILL &
KNOLWEDGE
102 - 106 days
post (3.5mths)
SKILL
A vs B
81% vs 57%
(p < 0.05)
KNOWLEDGE
mean out of 20 (%)
A vs B
14.9 (75%) vs 14.9 (75%)
Lay Population Studies % competent
Braslow
et al.,
1997
Lay people
(mean age 33yrs)
from
A = public spaces
B, & C = church
groups; temporary
employment firm;
& those enrolled
in ARC or AHA course
Previously BLS
trained (31% – 58% of groups)
Prospective Quasi-experimental design with non-equivalent control group, three convenience
samples
A) Prototype Video (31min) + manikin kit
31min prototype Video developed by Braslow et al., 1997 & cardboard manikin
vs
B) Video (34min) + manikin kit
34min revised Video developed by Braslow et al., 1997 (more practice time added, allowed for
25min hands on practice) & cardboard manikin
vs
C) Traditional
AHA Heartsaver 4hr course (same as in Todd et al., 1998) or ARC 4hr course
Instructor assessed using : Brennan et al., 1996 checklist & Laerdal Skillmeter™ manikin & self-rated confidence measured the same as in Todd et al., 1998)
N = 642
An = 165
B1n = 175
C1n = 302
B2n = 38
C2n = 33
SKILL
Immediately
post=1
60 days post=2
SKILL
A vs B1 vs C1
54.3% vs 80% vs 45%
B1 vs C1
p < 0.001
SKILL
B2 vs C2
58% vs 27%
(p < 0.01)
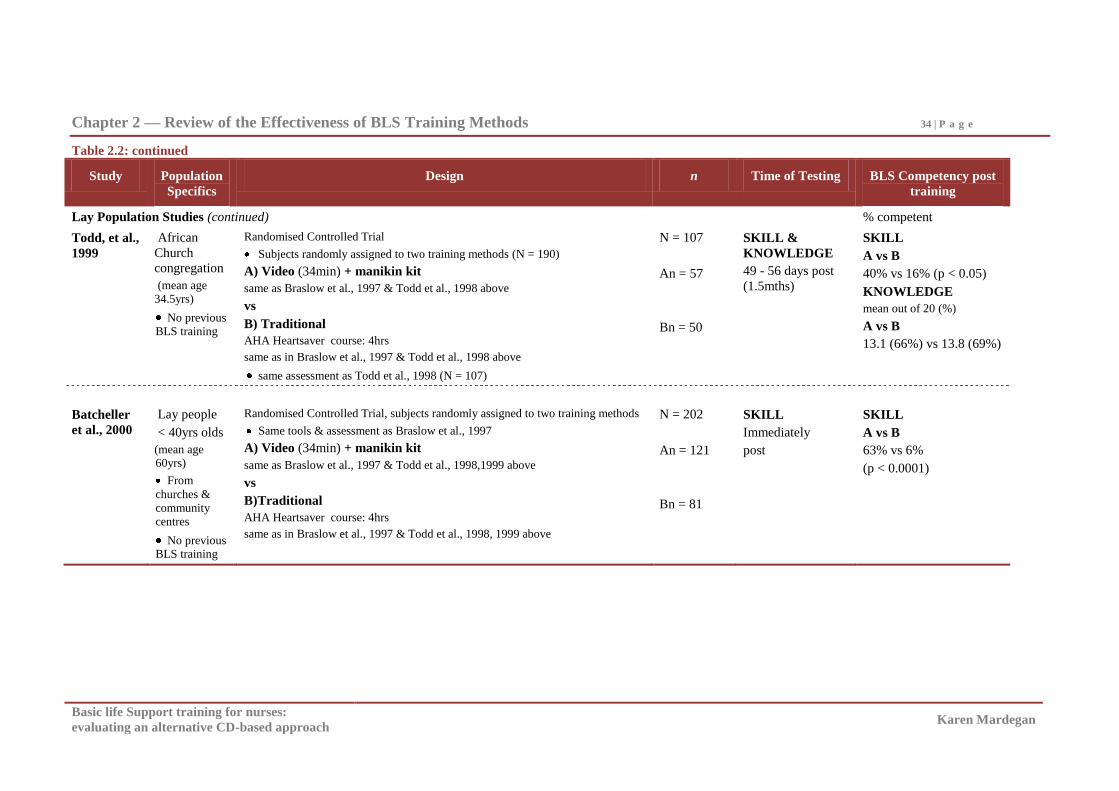
Chapter 2 — Review of the Effectiveness of BLS Training Methods 34 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.2: continued
Study Population
Specifics
Design n Time of Testing BLS Competency post
training
Lay Population Studies (continued) % competent
Todd, et al.,
1999
African
Church
congregation
(mean age 34.5yrs)
No previous BLS training
Randomised Controlled Trial
Subjects randomly assigned to two training methods (N = 190)
A) Video (34min) + manikin kit
same as Braslow et al., 1997 & Todd et al., 1998 above
vs
B) Traditional
AHA Heartsaver course: 4hrs
same as in Braslow et al., 1997 & Todd et al., 1998 above
same assessment as Todd et al., 1998 (N = 107)
N = 107
An = 57
Bn = 50
SKILL &
KNOWLEDGE
49 - 56 days post
(1.5mths)
SKILL
A vs B
40% vs 16% (p < 0.05)
KNOWLEDGE
mean out of 20 (%)
A vs B
13.1 (66%) vs 13.8 (69%)
Batcheller
et al., 2000
Lay people
< 40yrs olds
(mean age 60yrs)
From
churches &
community centres
No previous BLS training
Randomised Controlled Trial, subjects randomly assigned to two training methods
Same tools & assessment as Braslow et al., 1997
A) Video (34min) + manikin kit
same as Braslow et al., 1997 & Todd et al., 1998,1999 above
vs
B)Traditional
AHA Heartsaver course: 4hrs
same as in Braslow et al., 1997 & Todd et al., 1998, 1999 above
N = 202
An = 121
Bn = 81
SKILL
Immediately
post
SKILL
A vs B
63% vs 6%
(p < 0.0001)
Chapter 2 — Review of the Effectiveness of BLS Training Methods 35 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
However, there was a large BLS skill attrition rate (20%) in lay people by 60 days
post training in the Braslow et al. (1997) study, and competency was 40% in the Video
group and 16% in the Traditional group at 56 days post training in the Todd et al. (1999)
study suggesting poor skill retention for lay people with both the Video and Traditional
methods. Furthermore, validity of the findings of these studies is brought into question
because of a number of methodological limitations: potential bias of the assessment
checklist, questionable determination of competency levels, and the validity of assessing
participants directly following training.
The assessment checklist used in these studies was created by the developers of the
Video (Brennan et al., 1996), which raises the possibility that the assessment was better
suited to the VSI group than to the Traditional group who were trained via the AHA
Heartsaver program (Batcheller et al., 2000; Todd et al., 1998, 1999). Why it was
deemed necessary to develop and validate a new checklist, rather than using the AHA
assessment checklist (possibly altered and then validated) is unclear, but doing so would
have reduced this potential for bias.
Additionally, participants were required to competently perform only six out of a
possible 14 skills (43%) correctly to be deemed competent in these studies. The actual
BLS skill level (competence) and therefore the effectiveness of both the Traditional and
Video training methods in these studies are questionable when skill competence has been
set at such a low rate.
Furthermore, participants in the Braslow et al. (1997) and Batcheller et al. (2000)
studies, along with a number of studies presented later in the review, were assessed
immediately after training, which raises the issue of whether immediate recall or
consolidated knowledge and skill mastery is being assessed. Assessing participants
initially at least one week post training in these studies would have provided a clearer
determination of the level of initial skill acquisition. Therefore, the potential bias toward
the VSI group afforded by the nature of the checklist, the low (6/14) definition of
competence and the timing of assessment need to be taken into account when drawing
conclusions from these studies which show significantly higher BLS skill competence
with this VSI method compared to Traditional instructor-led programs.

Chapter 2 — Review of the Effectiveness of BLS Training Methods 36 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Subsequent BLS Video studies.
Numerous research efforts have followed the founding BLS Video studies discussed
above. Six subsequent BLS Video studies, five in lay populations and one in medical
students have been summarised in Table 2.3 below.
These subsequent Video studies also did not include a pre-test, but the five studies
in lay populations were Randomised Controlled Trials (RCT). Two were substudies of a
multi-centred trial and had very large sample sizes of between 2,700 - 6,100 participants
(Christenson et al., 2007; Riegel et al., 2006). The remaining RCT studies had smaller
sample sizes of between 133 - 336 participants (Bobrow et al., 2011; Einspruch et al.,
2007; Lynch et al., 2005).
The Lynch et al. (2005) and Einspruch et al. (2006) studies compared a
commercially prepared AHA 22 minute Video plus manikin kit (based on the VSI
Braslow et al. 1997 studies in Table 2.2) with the Traditional instructor conducted AHA
Heartsaver course, (which at this time did not include a BLS skill Video). In the Lynch et
al. (2005) study, 60% of participants trained using the Video manikin kit compared with
40% from the Traditional program were deemed competent immediately post completion
of the training and this was statistically significant. Furthermore, skill decline in both the
Video and Traditional methods was noted over time in the two month follow-up
(Einspruch et al., 2007). This is consistent with the earlier Video manikin (VSI) studies
in the lay population presented in Table 2.2. The higher number of competent medical
students post training in the self-directed ―pre-reading, Video and independent manikin
practice‖ design evaluated in the Done and Parr (2002) study is consistent with the high
competency rates seen in the Todd et al. (1999) study in medical students.
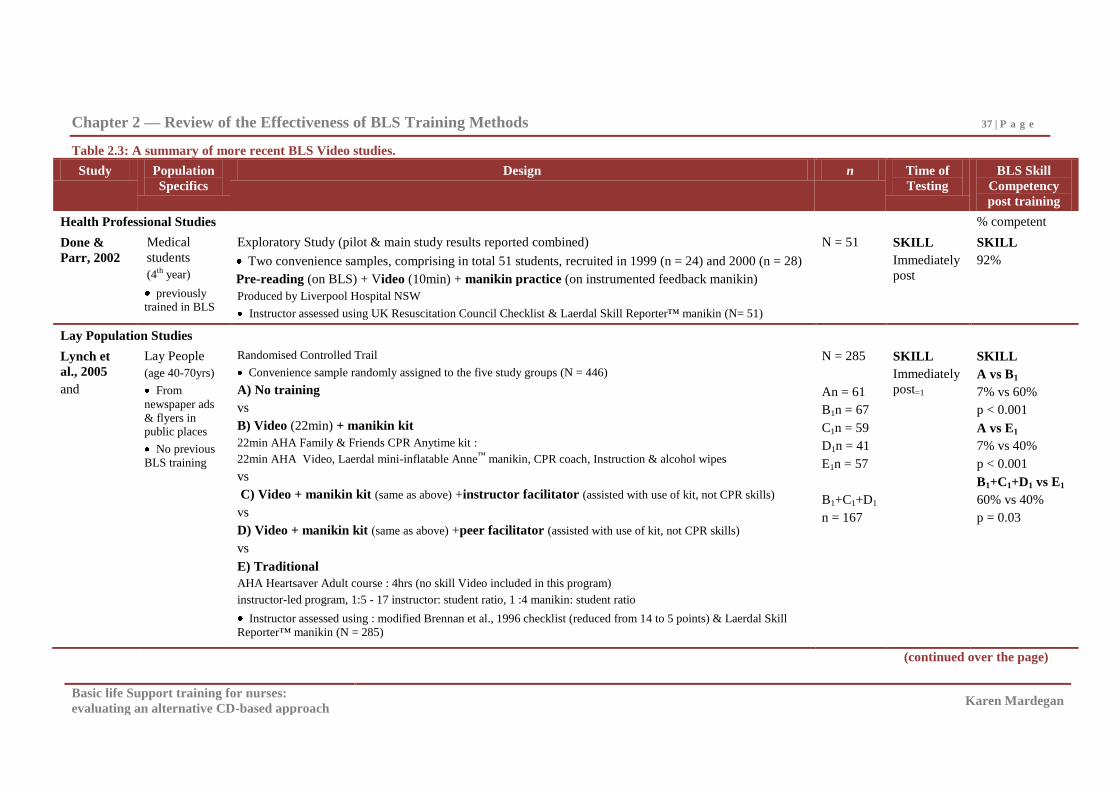
Chapter 2 — Review of the Effectiveness of BLS Training Methods 37 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.3: A summary of more recent BLS Video studies.
Study Population
Specifics
Design n Time of
Testing
BLS Skill
Competency
post training
Health Professional Studies % competent
Done &
Parr, 2002
Medical
students
(4th year)
previously trained in BLS
Exploratory Study (pilot & main study results reported combined)
Two convenience samples, comprising in total 51 students, recruited in 1999 (n = 24) and 2000 (n = 28)
Pre-reading (on BLS) + Video (10min) + manikin practice (on instrumented feedback manikin)
Produced by Liverpool Hospital NSW
Instructor assessed using UK Resuscitation Council Checklist & Laerdal Skill Reporter™ manikin (N= 51)
N = 51
SKILL
Immediately
post
SKILL
92%
Lay Population Studies
Lynch et
al., 2005
and
Lay People
(age 40-70yrs)
From
newspaper ads
& flyers in public places
No previous
BLS training
Randomised Controlled Trail
Convenience sample randomly assigned to the five study groups (N = 446)
A) No training
vs
B) Video (22min) + manikin kit
22min AHA Family & Friends CPR Anytime kit :
22min AHA Video, Laerdal mini-inflatable Anne™ manikin, CPR coach, Instruction & alcohol wipes
vs
C) Video + manikin kit (same as above) +instructor facilitator (assisted with use of kit, not CPR skills)
vs
D) Video + manikin kit (same as above) +peer facilitator (assisted with use of kit, not CPR skills)
vs
E) Traditional
AHA Heartsaver Adult course : 4hrs (no skill Video included in this program)
instructor-led program, 1:5 - 17 instructor: student ratio, 1 :4 manikin: student ratio
Instructor assessed using : modified Brennan et al., 1996 checklist (reduced from 14 to 5 points) & Laerdal Skill
Reporter™ manikin (N = 285)
N = 285
An = 61
B1n = 67
C1n = 59
D1n = 41
E1n = 57
B1+C1+D1
n = 167
SKILL
Immediately
post=1
SKILL
A vs B1
7% vs 60%
p < 0.001
A vs E1
7% vs 40%
p < 0.001
B1+C1+D1 vs E1
60% vs 40%
p = 0.03
(continued over the page)
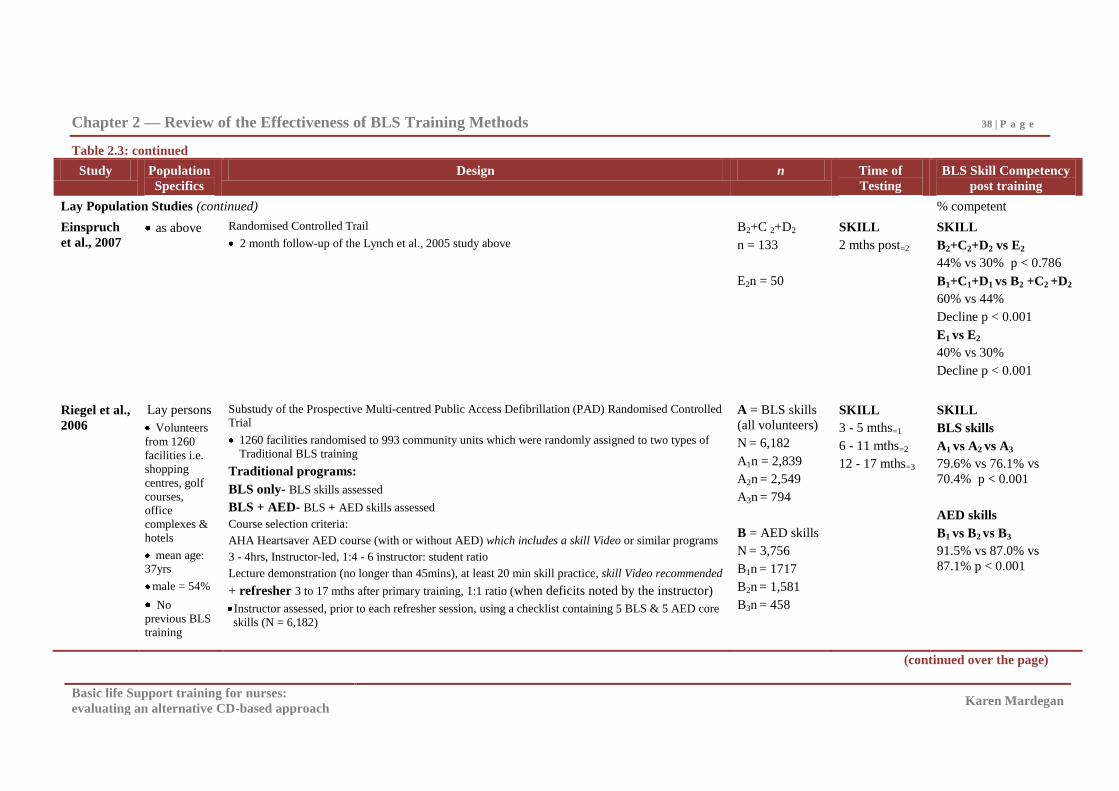
Chapter 2 — Review of the Effectiveness of BLS Training Methods 38 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.3: continued
Study Population
Specifics
Design n Time of
Testing
BLS Skill Competency
post training
Lay Population Studies (continued) % competent
Einspruch
et al., 2007 as above Randomised Controlled Trail
2 month follow-up of the Lynch et al., 2005 study above
B2+C 2+D2
n = 133
E2n = 50
SKILL
2 mths post=2
SKILL
B2+C2+D2 vs E2
44% vs 30% p < 0.786
B1+C1+D1 vs B2 +C2 +D2
60% vs 44%
Decline p < 0.001
E1 vs E2
40% vs 30%
Decline p < 0.001
Riegel et al.,
2006
Lay persons
Volunteers
from 1260
facilities i.e.
shopping
centres, golf
courses,
office
complexes &
hotels
mean age: 37yrs
male = 54%
No
previous BLS
training
Substudy of the Prospective Multi-centred Public Access Defibrillation (PAD) Randomised Controlled Trial
1260 facilities randomised to 993 community units which were randomly assigned to two types of
Traditional BLS training
Traditional programs:
BLS only- BLS skills assessed
BLS + AED- BLS + AED skills assessed
Course selection criteria:
AHA Heartsaver AED course (with or without AED) which includes a skill Video or similar programs
3 - 4hrs, Instructor-led, 1:4 - 6 instructor: student ratio
Lecture demonstration (no longer than 45mins), at least 20 min skill practice, skill Video recommended
+ refresher 3 to 17 mths after primary training, 1:1 ratio (when deficits noted by the instructor)
Instructor assessed, prior to each refresher session, using a checklist containing 5 BLS & 5 AED core
skills (N = 6,182)
A = BLS skills
(all volunteers)
N = 6,182
A1n = 2,839
A2n = 2,549
A3n = 794
B = AED skills
N = 3,756
B1n = 1717
B2n = 1,581
B3n = 458
SKILL
3 - 5 mths=1
6 - 11 mths=2
12 - 17 mths=3
SKILL
BLS skills
A1 vs A2 vs A3
79.6% vs 76.1% vs
70.4% p < 0.001
AED skills
B1 vs B2 vs B3
91.5% vs 87.0% vs
87.1% p < 0.001
(continued over the page)
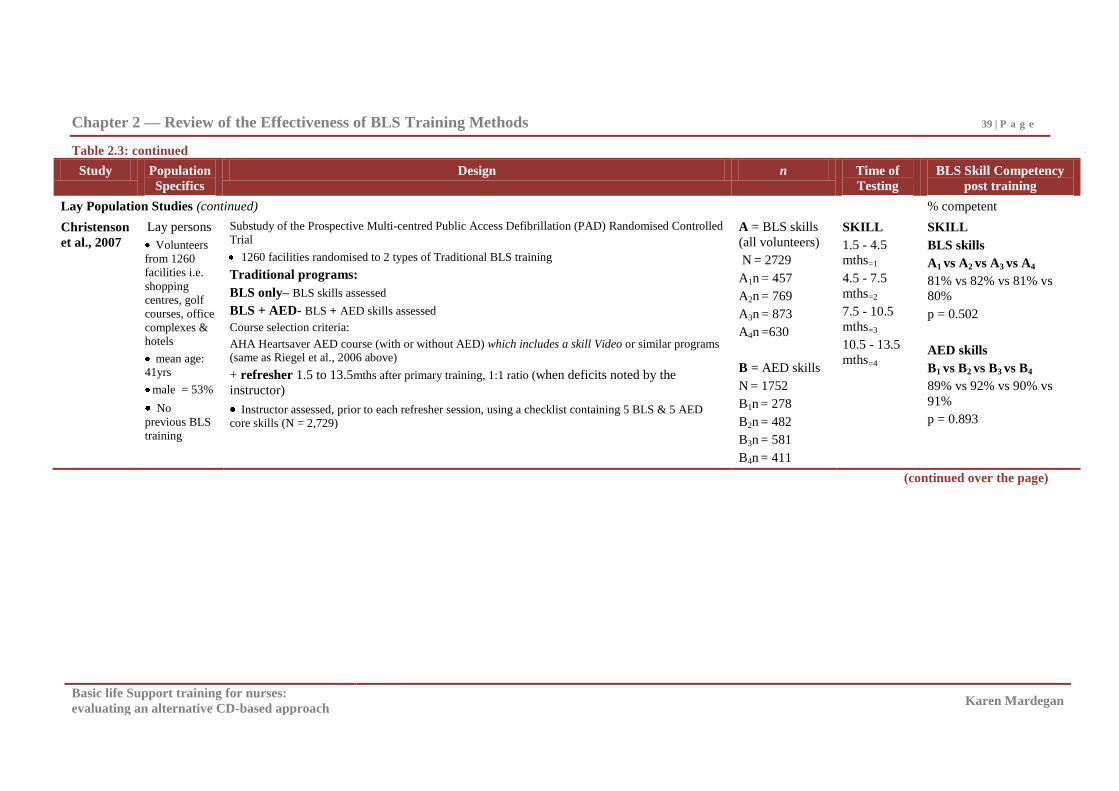
Chapter 2 — Review of the Effectiveness of BLS Training Methods 39 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.3: continued
Study Population
Specifics
Design n Time of
Testing
BLS Skill Competency
post training
Lay Population Studies (continued) % competent
Christenson
et al., 2007
Lay persons
Volunteers
from 1260
facilities i.e.
shopping
centres, golf
courses, office
complexes &
hotels
mean age: 41yrs
male = 53%
No
previous BLS
training
Substudy of the Prospective Multi-centred Public Access Defibrillation (PAD) Randomised Controlled
Trial
1260 facilities randomised to 2 types of Traditional BLS training
Traditional programs:
BLS only– BLS skills assessed
BLS + AED- BLS + AED skills assessed
Course selection criteria:
AHA Heartsaver AED course (with or without AED) which includes a skill Video or similar programs (same as Riegel et al., 2006 above)
+ refresher 1.5 to 13.5mths after primary training, 1:1 ratio (when deficits noted by the
instructor)
Instructor assessed, prior to each refresher session, using a checklist containing 5 BLS & 5 AED core skills (N = 2,729)
A = BLS skills
(all volunteers)
N = 2729
A1n = 457
A2n = 769
A3n = 873
A4n =630
B = AED skills
N = 1752
B1n = 278
B2n = 482
B3n = 581
B4n = 411
SKILL
1.5 - 4.5
mths=1
4.5 - 7.5
mths=2
7.5 - 10.5
mths=3
10.5 - 13.5
mths=4
SKILL
BLS skills
A1 vs A2 vs A3 vs A4
81% vs 82% vs 81% vs
80%
p = 0.502
AED skills
B1 vs B2 vs B3 vs B4
89% vs 92% vs 90% vs
91%
p = 0.893
(continued over the page)
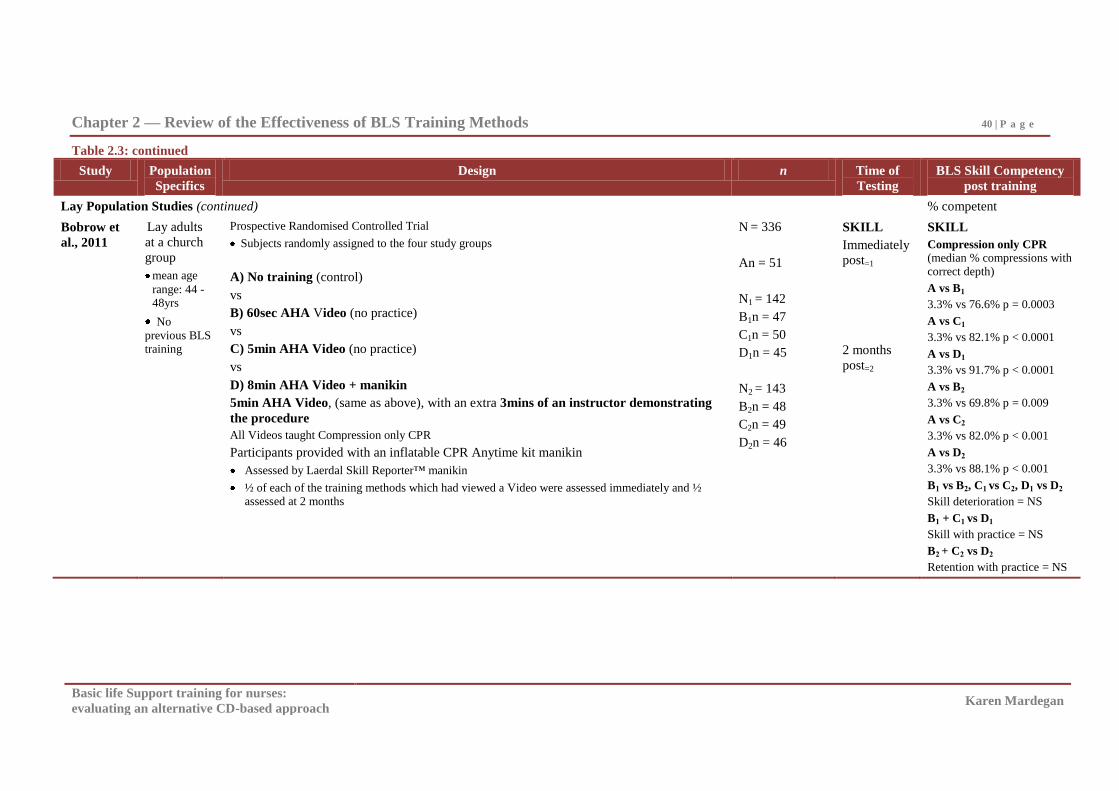
Chapter 2 — Review of the Effectiveness of BLS Training Methods 40 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.3: continued
Study Population
Specifics
Design n Time of
Testing
BLS Skill Competency
post training
Lay Population Studies (continued) % competent
Bobrow et
al., 2011
Lay adults
at a church
group
mean age
range: 44 - 48yrs
No
previous BLS training
Prospective Randomised Controlled Trial
Subjects randomly assigned to the four study groups
A) No training (control)
vs
B) 60sec AHA Video (no practice)
vs
C) 5min AHA Video (no practice)
vs
D) 8min AHA Video + manikin
5min AHA Video, (same as above), with an extra 3mins of an instructor demonstrating
the procedure
All Videos taught Compression only CPR
Participants provided with an inflatable CPR Anytime kit manikin
Assessed by Laerdal Skill Reporter™ manikin
½ of each of the training methods which had viewed a Video were assessed immediately and ½ assessed at 2 months
N = 336
An = 51
N1 = 142
B1n = 47
C1n = 50
D1n = 45
N2 = 143
B2n = 48
C2n = 49
D2n = 46
SKILL
Immediately
post=1
2 months
post=2
SKILL
Compression only CPR
(median % compressions with correct depth)
A vs B1
3.3% vs 76.6% p = 0.0003
A vs C1
3.3% vs 82.1% p < 0.0001
A vs D1
3.3% vs 91.7% p < 0.0001
A vs B2
3.3% vs 69.8% p = 0.009
A vs C2
3.3% vs 82.0% p < 0.001
A vs D2
3.3% vs 88.1% p < 0.001
B1 vs B2, C1 vs C2, D1 vs D2
Skill deterioration = NS
B1 + C1 vs D1
Skill with practice = NS
B2 + C2 vs D2
Retention with practice = NS
Chapter 2 — Review of the Effectiveness of BLS Training Methods 41 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The Christenson et al. (2007) and Riegel et al. (2006) studies where the Traditional
program is supplemented by a BLS Video appear to produce a higher number of
competent participants post training than the Video manikin kit studies in lay people
(Einspruch et al., 2007; Lynch et al., 2005). The skill decline noted in the Video manikin
kit studies (Einspruch et al., 2006 and Table 2.2), and Traditional programs (see Table
2.1), is also not apparent when a Video supplements the Traditional program (Riegel et
al., 2006). There does however appear to be around 10% improvement in skill
competence when an additional 6 month refresher is provided (Christenson et al., 2007),
which is consistent with comparative literature (Woodard et al., 2004). Studies which
compare Video manikin kits with Traditional instructor-led programs that include skill
Videos are therefore of interest to determine the relative value of these two video designs
(Video manikin kit and Traditional programs with a skill Video).
The recent Bobrow et al. (2011) RCT, where very brief 60 second and five minute
AHA Videos (with and without an additional three minutes of manikin practice) was
compared to no training, is also of interest. BLS skill competence in this study was high
and ranged from 70 – 92% immediately and two months post training in all those who
viewed the Videos. There was also no significant difference in the competence of those
who viewed the Video which included three minutes of manikin practice. These findings
appear to question the role of practice, which has been emphasised as essential in training
design and delivery and resuscitation reviews (ARC & NZRC, 2010a; Hazinski et al.,
2010; Mancini et al., 2010; Salas & Cannon-Bowers, 2001; Salas & Kosarzycki, 2003;
Tannenbaum & Yakl, 1992).
Conclusions from BLS Video studies.
The investigation into Videotape as a medium for BLS training has been relatively
extensive. The significantly higher skill competence for those trained using the Video
manikin method, than for those trained by the Traditional method, suggests that this self-
directed method may in fact be superior to Traditional instructor-led methods, while at the
same time being a quicker and cheaper alternative. BLS Videos also appear to improve
skill competence and retention when used within Traditional instructor-led programs
(Christenson et al., 2007; Riegel et al., 2006).
Chapter 2 — Review of the Effectiveness of BLS Training Methods 42 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
For training to be deemed fully effective, it needs to produce high levels of initial
competence that is maintained over time. Therefore, the skill decline by two to six months
post training for lay people with both the Video manikin kits and Traditional instructor-
led programs (Einspruch et al., 2007 and Table 2.2) is of concern and suggests that the
Video manikin method has some limitations.
The role and necessity for practice is also suggested in the Bobrow et al. (2011)
study to be not as influential on BLS training outcomes as previously thought. This
finding brings into question the role of practice in BLS training, and the possibility that
the four principles of training delivery may not necessarily be of equal importance.
It is also of particular interest that the Video manikin method has incorporated only
the three training and delivery principles of ‗relevant information, demonstration and
practice.‘ Feedback is not possible with the basic manikins supplied with this program
design. Yet, the Video manikin appears to be more effective than the Traditional method
which includes instructor feedback. This could possibly be explained by the standardised
program content and extensive opportunity to practise on a manikin during and after the
Video training. However, the logical question that follows on from these findings is the
potential improvement possible if feedback was able to be included into the Video
manikin design. Studies which compare Video alone with Video manikin kits and
Traditional instructor-led programs that include skill Videos are therefore of continued
interest to assist our understanding of the role of practice and feedback with BLS Video
programs.
The BLS Video studies presented (in Table 2.2 and Table 2.3) have concentrated on
evaluating BLS skill immediately post training and retention of BLS skill among novice
lay people with only two studies in medical students (Done & Parr, 2002; Todd et al.,
1998). Two studies have investigated BLS knowledge (Todd et al., 1998; Todd et al.,
1999) and three studies have also evaluated BLS related attitudes which include skill
confidence post training (Batcheller et al., 2000; Braslow et al., 1997; Todd et al., 1998,
1999). No significant difference between the Video and Traditional training methods in
BLS knowledge and skill confidence was reported. Studies which evaluate the
effectiveness of BLS Video training in practising health professionals and rating of BLS
Video training programs from the participants‘ perspective have not been found. Studies
Chapter 2 — Review of the Effectiveness of BLS Training Methods 43 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
which clarify the role of practice and feedback in BLS training outcomes and further
investigate retention of BLS skill are also still needed to complete the appraisal of this
method.
Digital Video Disc BLS training programs.
The DVD is relatively new technology, developed as the contemporary form of
analogue videotape technology. Research examining BLS training programs on DVD has
begun to emerge in the literature since 2005. As in the early Videotape literature, BLS
DVDs were initially described in product reviews and pilot studies (Anonymous, 2005;
Thoren et al., 2007). The BLS DVD studies which followed these early reviews continue
the exploration into the BLS Video manikin kit design developed by Braslow et al.
(1997), using DVD technology. The eight studies that have evaluated DVD manikin kits
(two in health professionals and six in various lay populations) are summarised in Table
2.4.
These eight studies comprised two studies which didn‘t include a comparison group
and six studies that compared DVD manikin kits with Traditional programs, (one in
nursing students and five in various lay populations). Five out of the eight evaluated BLS
skill immediately post training. Sample sizes ranged from 59 (Bjorshol, Lindner, Soreide,
Moen, & Sunde, 2009) to 282 (Cason et al., 2009). Four studies were Randomised
Controlled Trials (Cason et al., 2009; Chung et al., 2010; Mancini et al., 2009; Roppolo et
al., 2007), and the two studies which did not include a comparison group (Bjorshol et al.,
2009; Nielson et. al., 2010), as well as the Jones, Handley, Whitfield, Newcombe, and
Chamberlain.(2007) study, performed a pre-test.
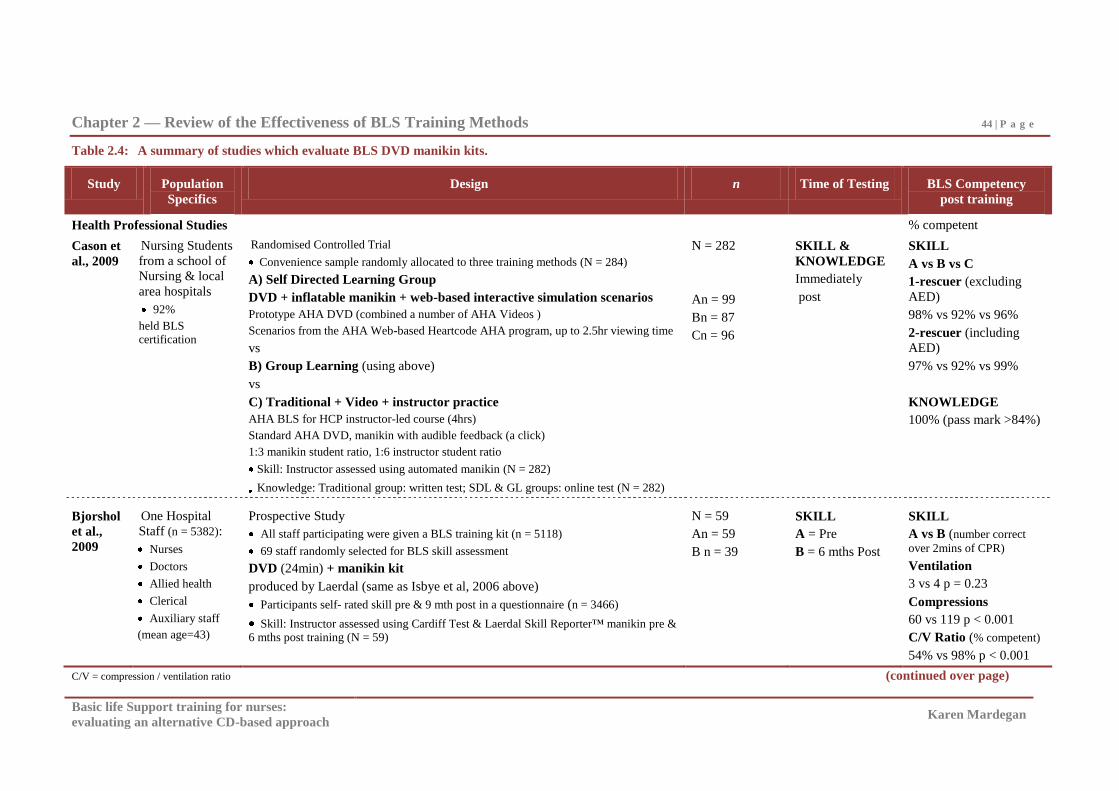
Chapter 2 — Review of the Effectiveness of BLS Training Methods 44 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.4: A summary of studies which evaluate BLS DVD manikin kits.
Study Population
Specifics
Design n Time of Testing BLS Competency
post training
Health Professional Studies % competent
Cason et
al., 2009
Nursing Students
from a school of
Nursing & local
area hospitals
92%
held BLS certification
Randomised Controlled Trial
Convenience sample randomly allocated to three training methods (N = 284)
A) Self Directed Learning Group
DVD + inflatable manikin + web-based interactive simulation scenarios
Prototype AHA DVD (combined a number of AHA Videos )
Scenarios from the AHA Web-based Heartcode AHA program, up to 2.5hr viewing time
vs
B) Group Learning (using above)
vs
C) Traditional + Video + instructor practice
AHA BLS for HCP instructor-led course (4hrs)
Standard AHA DVD, manikin with audible feedback (a click)
1:3 manikin student ratio, 1:6 instructor student ratio
Skill: Instructor assessed using automated manikin (N = 282)
Knowledge: Traditional group: written test; SDL & GL groups: online test (N = 282)
N = 282
An = 99
Bn = 87
Cn = 96
SKILL &
KNOWLEDGE
Immediately
post
SKILL
A vs B vs C
1-rescuer (excluding
AED)
98% vs 92% vs 96%
2-rescuer (including
AED)
97% vs 92% vs 99%
KNOWLEDGE
100% (pass mark >84%)
Bjorshol
et al.,
2009
One Hospital
Staff (n = 5382):
Nurses
Doctors
Allied health
Clerical
Auxiliary staff
(mean age=43)
Prospective Study
All staff participating were given a BLS training kit (n = 5118)
69 staff randomly selected for BLS skill assessment
DVD (24min) + manikin kit
produced by Laerdal (same as Isbye et al, 2006 above)
Participants self- rated skill pre & 9 mth post in a questionnaire (n = 3466)
Skill: Instructor assessed using Cardiff Test & Laerdal Skill Reporter™ manikin pre & 6 mths post training (N = 59)
N = 59
An = 59
B n = 39
SKILL
A = Pre
B = 6 mths Post
SKILL
A vs B (number correct
over 2mins of CPR)
Ventilation
3 vs 4 p = 0.23
Compressions
60 vs 119 p < 0.001
C/V Ratio (% competent)
54% vs 98% p < 0.001
C/V = compression / ventilation ratio (continued over page)
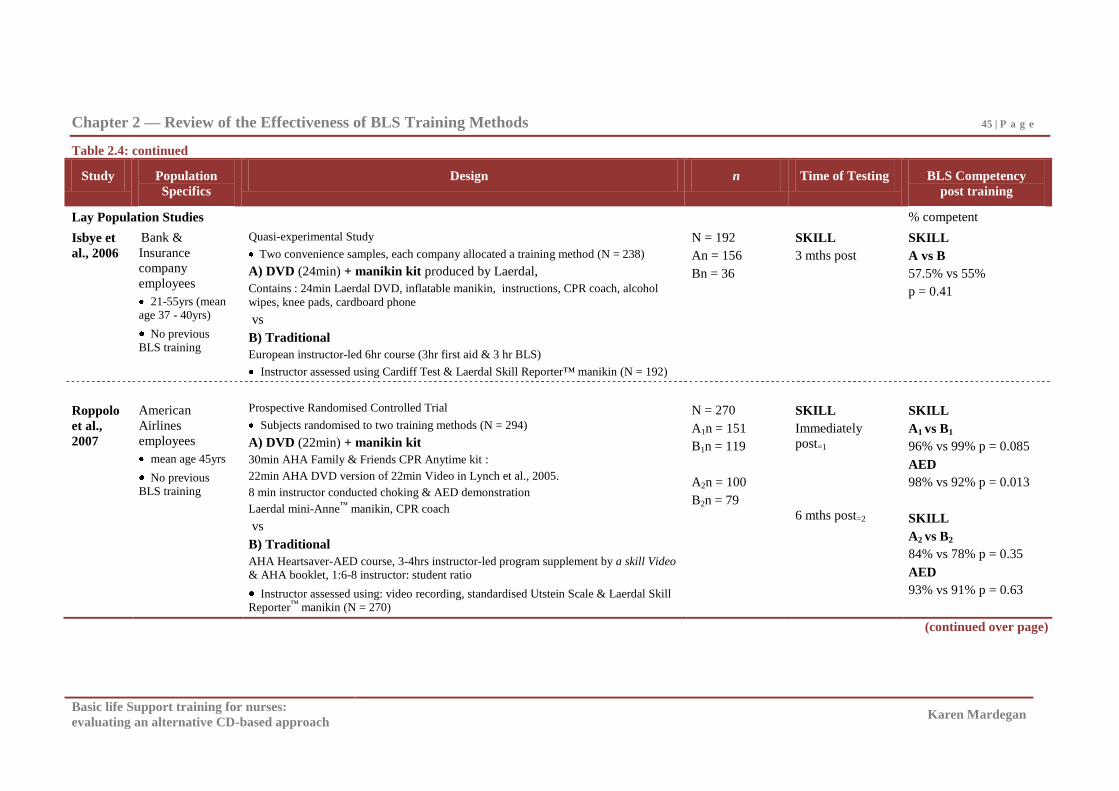
Chapter 2 — Review of the Effectiveness of BLS Training Methods 45 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.4: continued
Study Population
Specifics
Design n Time of Testing BLS Competency
post training
Lay Population Studies % competent
Isbye et
al., 2006
Bank &
Insurance
company
employees
21-55yrs (mean age 37 - 40yrs)
No previous BLS training
Quasi-experimental Study
Two convenience samples, each company allocated a training method (N = 238)
A) DVD (24min) + manikin kit produced by Laerdal,
Contains : 24min Laerdal DVD, inflatable manikin, instructions, CPR coach, alcohol
wipes, knee pads, cardboard phone
vs
B) Traditional
European instructor-led 6hr course (3hr first aid & 3 hr BLS)
Instructor assessed using Cardiff Test & Laerdal Skill Reporter™ manikin (N = 192)
N = 192
An = 156
Bn = 36
SKILL
3 mths post
SKILL
A vs B
57.5% vs 55%
p = 0.41
Roppolo
et al.,
2007
American
Airlines
employees
mean age 45yrs
No previous BLS training
Prospective Randomised Controlled Trial
Subjects randomised to two training methods (N = 294)
A) DVD (22min) + manikin kit
30min AHA Family & Friends CPR Anytime kit :
22min AHA DVD version of 22min Video in Lynch et al., 2005.
8 min instructor conducted choking & AED demonstration
Laerdal mini-Anne™ manikin, CPR coach
vs
B) Traditional
AHA Heartsaver-AED course, 3-4hrs instructor-led program supplement by a skill Video & AHA booklet, 1:6-8 instructor: student ratio
Instructor assessed using: video recording, standardised Utstein Scale & Laerdal Skill Reporter™ manikin (N = 270)
N = 270
A1n = 151
B1n = 119
A2n = 100
B2n = 79
SKILL
Immediately
post=1
6 mths post=2
SKILL
A1 vs B1
96% vs 99% p = 0.085
AED
98% vs 92% p = 0.013
SKILL
A2 vs B2
84% vs 78% p = 0.35
AED
93% vs 91% p = 0.63
(continued over page)
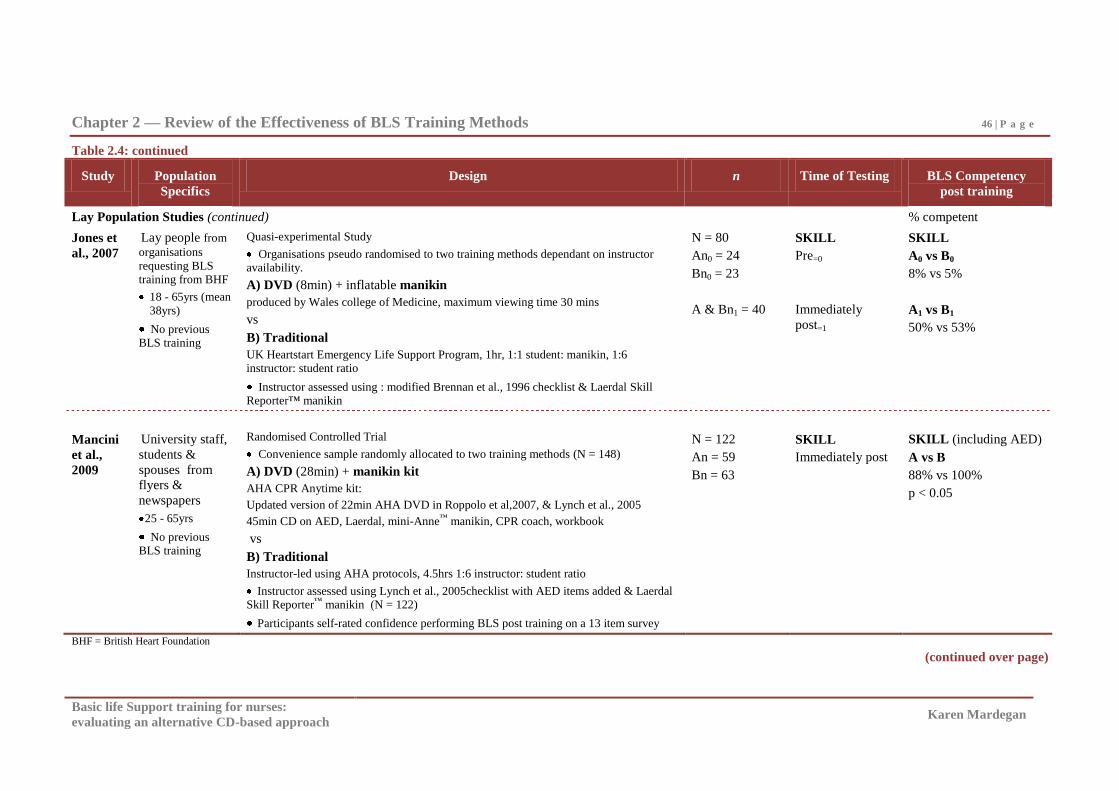
Chapter 2 — Review of the Effectiveness of BLS Training Methods 46 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.4: continued
Study Population
Specifics
Design n Time of Testing BLS Competency
post training
Lay Population Studies (continued) % competent
Jones et
al., 2007
Lay people from
organisations
requesting BLS training from BHF
18 - 65yrs (mean
38yrs)
No previous BLS training
Quasi-experimental Study
Organisations pseudo randomised to two training methods dependant on instructor availability.
A) DVD (8min) + inflatable manikin
produced by Wales college of Medicine, maximum viewing time 30 mins
vs
B) Traditional
UK Heartstart Emergency Life Support Program, 1hr, 1:1 student: manikin, 1:6 instructor: student ratio
Instructor assessed using : modified Brennan et al., 1996 checklist & Laerdal Skill Reporter™ manikin
N = 80
An0 = 24
Bn0 = 23
A & Bn1 = 40
SKILL
Pre=0
Immediately
post=1
SKILL
A0 vs B0
8% vs 5%
A1 vs B1
50% vs 53%
Mancini
et al.,
2009
University staff,
students &
spouses from
flyers &
newspapers
25 - 65yrs
No previous BLS training
Randomised Controlled Trial
Convenience sample randomly allocated to two training methods (N = 148)
A) DVD (28min) + manikin kit
AHA CPR Anytime kit:
Updated version of 22min AHA DVD in Roppolo et al,2007, & Lynch et al., 2005
45min CD on AED, Laerdal, mini-Anne™ manikin, CPR coach, workbook
vs
B) Traditional
Instructor-led using AHA protocols, 4.5hrs 1:6 instructor: student ratio
Instructor assessed using Lynch et al., 2005checklist with AED items added & Laerdal Skill Reporter™ manikin (N = 122)
Participants self-rated confidence performing BLS post training on a 13 item survey
N = 122
An = 59
Bn = 63
SKILL
Immediately post
SKILL (including AED)
A vs B
88% vs 100%
p < 0.05
BHF = British Heart Foundation
(continued over page)
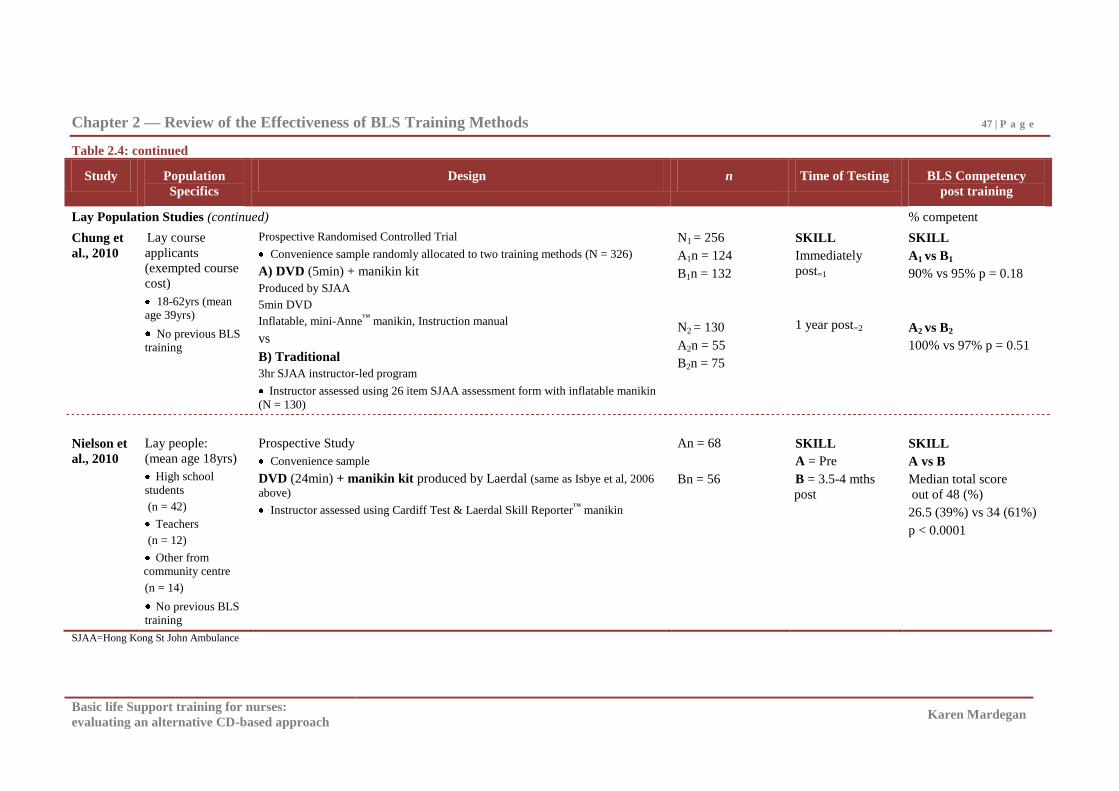
Chapter 2 — Review of the Effectiveness of BLS Training Methods 47 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.4: continued
Study Population
Specifics
Design n Time of Testing BLS Competency
post training
Lay Population Studies (continued) % competent
Chung et
al., 2010
Lay course
applicants
(exempted course
cost)
18-62yrs (mean age 39yrs)
No previous BLS training
Prospective Randomised Controlled Trial
Convenience sample randomly allocated to two training methods (N = 326)
A) DVD (5min) + manikin kit
Produced by SJAA
5min DVD
Inflatable, mini-Anne™ manikin, Instruction manual
vs
B) Traditional
3hr SJAA instructor-led program
Instructor assessed using 26 item SJAA assessment form with inflatable manikin
(N = 130)
N1 = 256
A1n = 124
B1n = 132
N2 = 130
A2n = 55
B2n = 75
SKILL
Immediately
post=1
1 year post=2
SKILL
A1 vs B1
90% vs 95% p = 0.18
A2 vs B2
100% vs 97% p = 0.51
Nielson et
al., 2010
Lay people:
(mean age 18yrs)
High school
students
(n = 42)
Teachers
(n = 12)
Other from community centre
(n = 14)
No previous BLS training
Prospective Study
Convenience sample
DVD (24min) + manikin kit produced by Laerdal (same as Isbye et al, 2006
above)
Instructor assessed using Cardiff Test & Laerdal Skill Reporter™ manikin
An = 68
Bn = 56
SKILL
A = Pre
B = 3.5-4 mths
post
SKILL
A vs B
Median total score
out of 48 (%)
26.5 (39%) vs 34 (61%)
p < 0.0001
SJAA=Hong Kong St John Ambulance
Chapter 2 — Review of the Effectiveness of BLS Training Methods 48 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
In contrast to the BLS Video manikin kit studies, BLS DVD manikin kits produced
comparable, not significantly better, BLS skill competency to Traditional training
methods immediately post training in health professionals (Cason et al., 2009) and the
majority of lay studies (Chung et al., 2010; Jones et al., 2007; Roppolo et al., 2007 [see
Table 2.4]). The high competency rates of health professionals seen in Video manikin
studies (Done & Parr, 2002; Todd et al., 1998) are also seen with DVD manikin kit
studies immediately and up to 6 months post training (Bjorshol et al., 2009; Cason et al.,
2009). Furthermore, three of the four studies which evaluated BLS skill immediately post
training in the lay population (Chung et al., 2010; Mancini et al., 2009; Roppolo et al.,
2007) reported skill competency rates of 88% to 96% which are comparable to the
Braslow et al. (1997) study and demonstrate better competency than seen in other Video
manikin kit studies (Batcheller et al., 2000; Lynch et al., 2005; Todd et al., 1999). Skill
decline post training in DVD manikin kits and Traditional methods in the lay population
is also apparent. Most (Isbye et al., 2006; Nielson et al., 2010; Roppolo et al., 2007) but
not all studies (Chung et al., 2010) suggest comparable skill retention issues for lay
people with Video, DVD and Traditional methods (see Table 2.1, Table 2.2;and Table
2.3).
It is also of interest that a 5 min DVD in the Chung et al. (2010) study produced
similarly high competency rates ranging from 90-100% immediately and one year post
training in lay people to the skill levels seen with two earlier 5-10 minute BLS Videos
(Bobrow et al., 2011; Done & Parr, 2002). In contrast, the 5 min DVD in the Jones et al.
(2007) study reported competency rates immediately post training of only 50%. Though
variable, these finding do suggest that there is a potential for the length and content of
BLS Videos and DVDs to be reduced.
The inclusion of an AHA BLS skill DVD in the Traditional program evaluated in
the Cason et al. (2009) DVD study produced high skill competence immediately post
training in health professionals. This is consistent with the improved skill outcomes in
lay people seen in the Riegel et al. (2006) and Christenson et al. (2007) studies (see Table
2.3) when Traditional instructor-led BLS programs that include a BLS skill Video were
evaluated. The potential for BLS skill DVDs to improve skill retention in health
professionals undertaking Traditional instructor-led programs, as seen in the lay studies
(Christenson et al., 2007; Riegel et al., 2006) needs further evaluation. However these
Chapter 2 — Review of the Effectiveness of BLS Training Methods 49 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
findings (Cason et al., 2009) provide additional support for skill DVDs to be included in
Traditional instructor-led BLS programs.
The evaluation of BLS knowledge (Cason et al., 2009), and self-rated BLS skill
(Bjorshol et al., 2009) post DVD manikin kit in health professionals is emerging in the
literature. Cason et al. (2009) reported 100% of participants achieving greater than 85%,
which is a little higher than Video and Traditional BLS training outcomes for knowledge
which were 70% in lay (Todd et al., 1999) and 74% in health professionals (Todd et al.,
1998). The self-rated skill of health professionals also appears to improve post DVD
manikin kit training (Bjorshol et al., 2009) and confidence to perform BLS post training
with these kits in lay people is suggested to be equivalent to Traditional training methods
(Mancini et al., 2009). However, studies which evaluate rating of BLS DVD training
programs from the participants‘ perspective have not been found.
These DVD manikin kit studies have reported improved skill competency in lay
people and sustained high levels of skill competency in health professionals. That DVD
manikin kits were comparable but not significantly better for BLS skill competency than
the Traditional training programs evaluated immediately post training (see Table 2.4),
possibly suggests that there has been an improvement in Traditional program outcomes
over time. However, as Video and DVD manikin kit BLS training does not appear to
consistently produce good retention of skill, the need for continued exploration to identify
modes of training that can improve the outcomes seen with Video, DVD and Traditional
methods appears to continue to be needed.
The consistency of the findings between the Video and DVD manikin studies and
DVDs similar outcomes to Traditional training, once again, raises further interest into the
relationship between and role of each of the four principles of training design and
delivery, and the potential for the DVD manikin kit method if feedback could be included
in this design. In view of the findings of both the BLS Video and DVD literature, it is
expected that expanded use of, and further research into, the effectiveness of BLS DVDs,
will continue. The positive findings reported to date for health professional and lay
people in the BLS Video and DVD studies supports DVD as a possible alternative to
Traditional BLS training methods, and as such the use and evaluation of DVD manikin
kits to facilitate BLS training in large organisations are beginning to be reported (Bjorshol
Chapter 2 — Review of the Effectiveness of BLS Training Methods 50 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
et al., 2009). Methods that consistently improve skill retention are of relevance, as is the
potential for further improvement if manikin feedback was added into this design.
CD basic life support training programs.
Along with the videotape, computer programs viewed on personal computers (PC)
and distributed on floppy disc technology began to emerge in the 1970s. CD technology,
released in the 1980s, replaced the floppy disc. In contrast to Video or DVD programs, a
CD program is viewed on a computer and combines written and verbal instruction with
graphics, as well as video vignettes. There is usually a menu so viewers can navigate
through the content, moving from section to section at will, and revising sections as
needed. A notebook function (for additional information), and a self-testing facility is
also usually available. CD training programs are therefore able to address the training and
delivery principles of ‗relevant information, and demonstration‘. Practice and feedback
are possible only if a manikin with either human or manikin feedback is also included
within the training program design.
The CD, along with Video/DVD BLS training methods was developed as an
alternative to Traditional instructor-led approaches. In common with the Video, and
DVD literature above, enquiry began with BLS CD product reviews and pilot studies
(Doyle, 2002). The six studies that have subsequently investigated BLS CD programs
have primarily evaluated the training of health professionals. These studies are
summarised in Table 2.5.
Our ability to draw meaningful conclusions from the six studies in Table 2.5 is
questionable. Although three of the six studies were RCT, none of the six study designs
included a pre-test, (apart from the knowledge component of the Moule [2002] study).
Four of the six studies evaluated BLS CD programs with health professionals, (three with
nurses and one with medical students). One of the six evaluated an integrated computer
manikin system with health professionals (Fabius, Grissom, & Fuentes, 1994), and one
study evaluated a lay population using a BLS CD program.
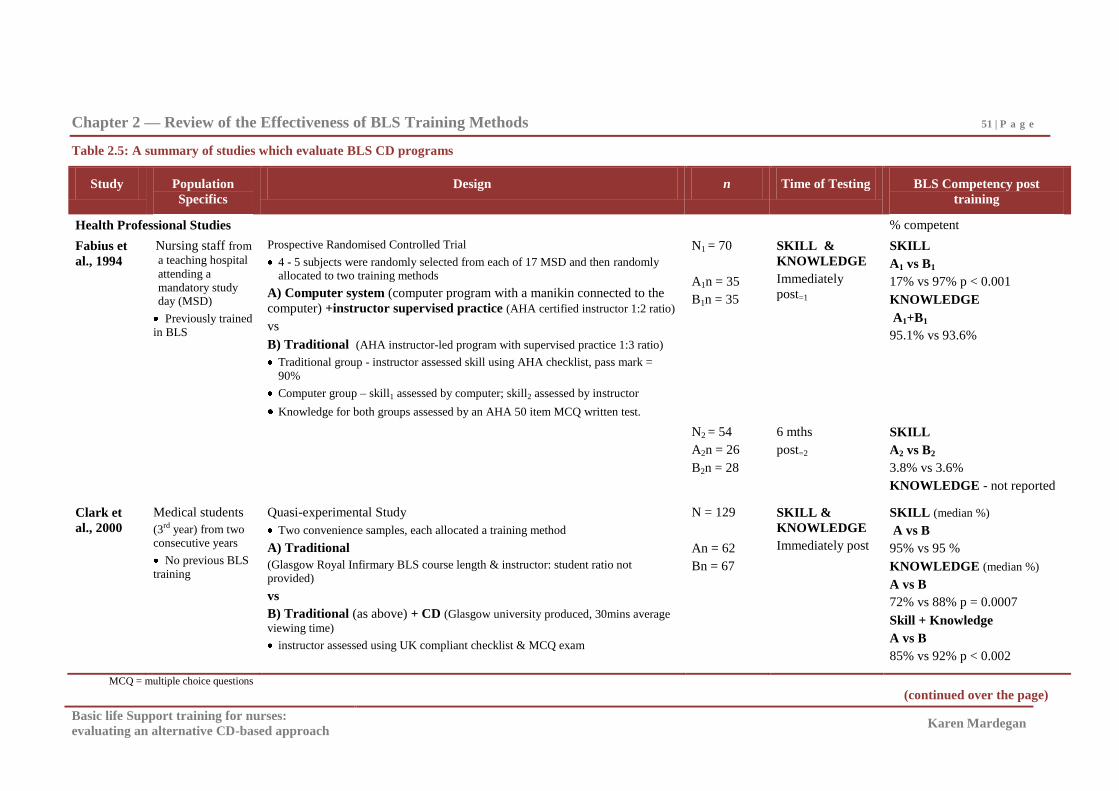
Chapter 2 — Review of the Effectiveness of BLS Training Methods 51 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.5: A summary of studies which evaluate BLS CD programs
Study Population
Specifics
Design n Time of Testing BLS Competency post
training
Health Professional Studies % competent
Fabius et
al., 1994
Nursing staff from
a teaching hospital
attending a
mandatory study day (MSD)
Previously trained
in BLS
Prospective Randomised Controlled Trial
4 - 5 subjects were randomly selected from each of 17 MSD and then randomly allocated to two training methods
A) Computer system (computer program with a manikin connected to the
computer) +instructor supervised practice (AHA certified instructor 1:2 ratio)
vs
B) Traditional (AHA instructor-led program with supervised practice 1:3 ratio)
Traditional group - instructor assessed skill using AHA checklist, pass mark =
90%
Computer group – skill1 assessed by computer; skill2 assessed by instructor
Knowledge for both groups assessed by an AHA 50 item MCQ written test.
N1 = 70
A1n = 35
B1n = 35
SKILL &
KNOWLEDGE
Immediately
post=1
SKILL
A1 vs B1
17% vs 97% p < 0.001
KNOWLEDGE
A1+B1
95.1% vs 93.6%
N2 = 54
A2n = 26
B2n = 28
6 mths
post=2
SKILL
A2 vs B2
3.8% vs 3.6%
KNOWLEDGE - not reported
Clark et
al., 2000
Medical students
(3rd year) from two consecutive years
No previous BLS
training
Quasi-experimental Study
Two convenience samples, each allocated a training method
A) Traditional
(Glasgow Royal Infirmary BLS course length & instructor: student ratio not
provided)
vs
B) Traditional (as above) + CD (Glasgow university produced, 30mins average
viewing time)
instructor assessed using UK compliant checklist & MCQ exam
N = 129
An = 62
Bn = 67
SKILL &
KNOWLEDGE
Immediately post
SKILL (median %)
A vs B
95% vs 95 %
KNOWLEDGE (median %)
A vs B
72% vs 88% p = 0.0007
Skill + Knowledge
A vs B
85% vs 92% p < 0.002
MCQ = multiple choice questions
(continued over the page)
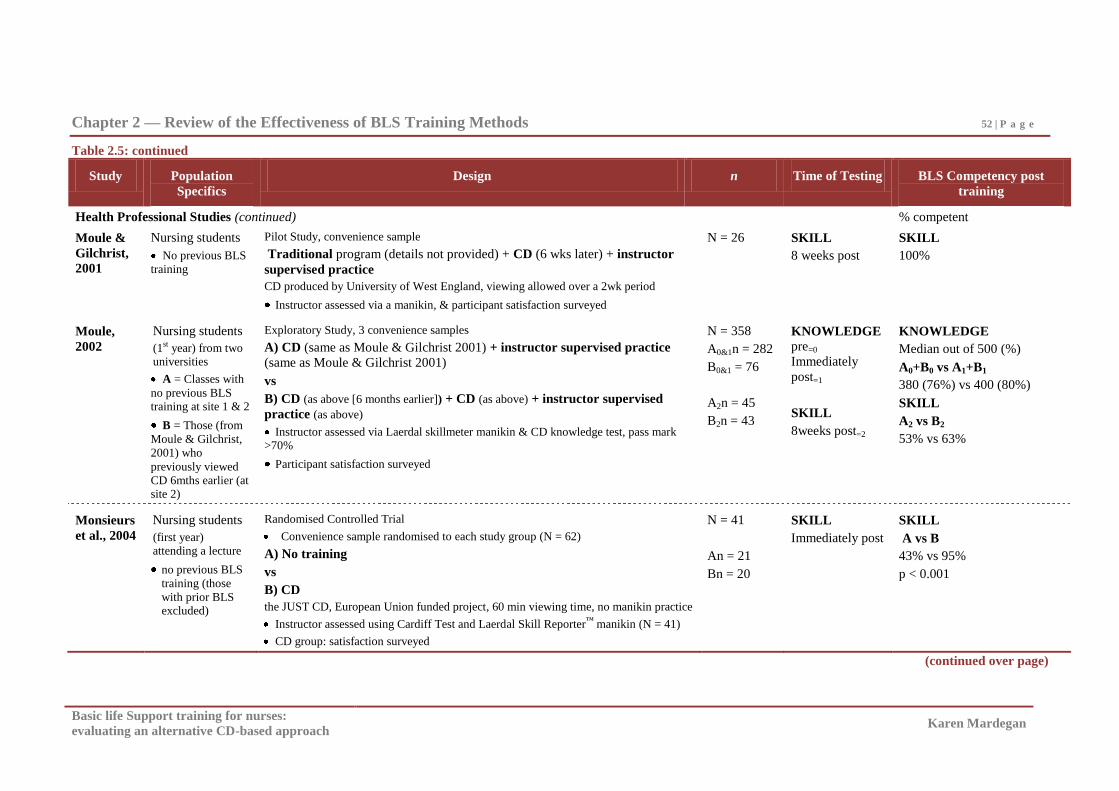
Chapter 2 — Review of the Effectiveness of BLS Training Methods 52 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.5: continued
Study Population
Specifics
Design n Time of Testing BLS Competency post
training
Health Professional Studies (continued) % competent
Moule &
Gilchrist,
2001
Nursing students
No previous BLS
training
Pilot Study, convenience sample
Traditional program (details not provided) + CD (6 wks later) + instructor
supervised practice
CD produced by University of West England, viewing allowed over a 2wk period
Instructor assessed via a manikin, & participant satisfaction surveyed
N = 26 SKILL
8 weeks post
SKILL
100%
Moule,
2002
Nursing students
(1st year) from two universities
A = Classes with
no previous BLS training at site 1 & 2
B = Those (from
Moule & Gilchrist,
2001) who
previously viewed
CD 6mths earlier (at site 2)
Exploratory Study, 3 convenience samples
A) CD (same as Moule & Gilchrist 2001) + instructor supervised practice
(same as Moule & Gilchrist 2001)
vs
B) CD (as above [6 months earlier]) + CD (as above) + instructor supervised
practice (as above)
Instructor assessed via Laerdal skillmeter manikin & CD knowledge test, pass mark >70%
Participant satisfaction surveyed
N = 358
A0&1n = 282
B0&1 = 76
A2n = 45
B2n = 43
KNOWLEDGE
pre=0
Immediately
post=1
SKILL
8weeks post=2
KNOWLEDGE
Median out of 500 (%)
A0+B0 vs A1+B1
380 (76%) vs 400 (80%)
SKILL
A2 vs B2
53% vs 63%
Monsieurs
et al., 2004
Nursing students
(first year) attending a lecture
no previous BLS
training (those
with prior BLS excluded)
Randomised Controlled Trial
Convenience sample randomised to each study group (N = 62)
A) No training
vs
B) CD
the JUST CD, European Union funded project, 60 min viewing time, no manikin practice
Instructor assessed using Cardiff Test and Laerdal Skill Reporter™ manikin (N = 41)
CD group: satisfaction surveyed
N = 41
An = 21
Bn = 20
SKILL
Immediately post
SKILL
A vs B
43% vs 95%
p < 0.001
(continued over page)
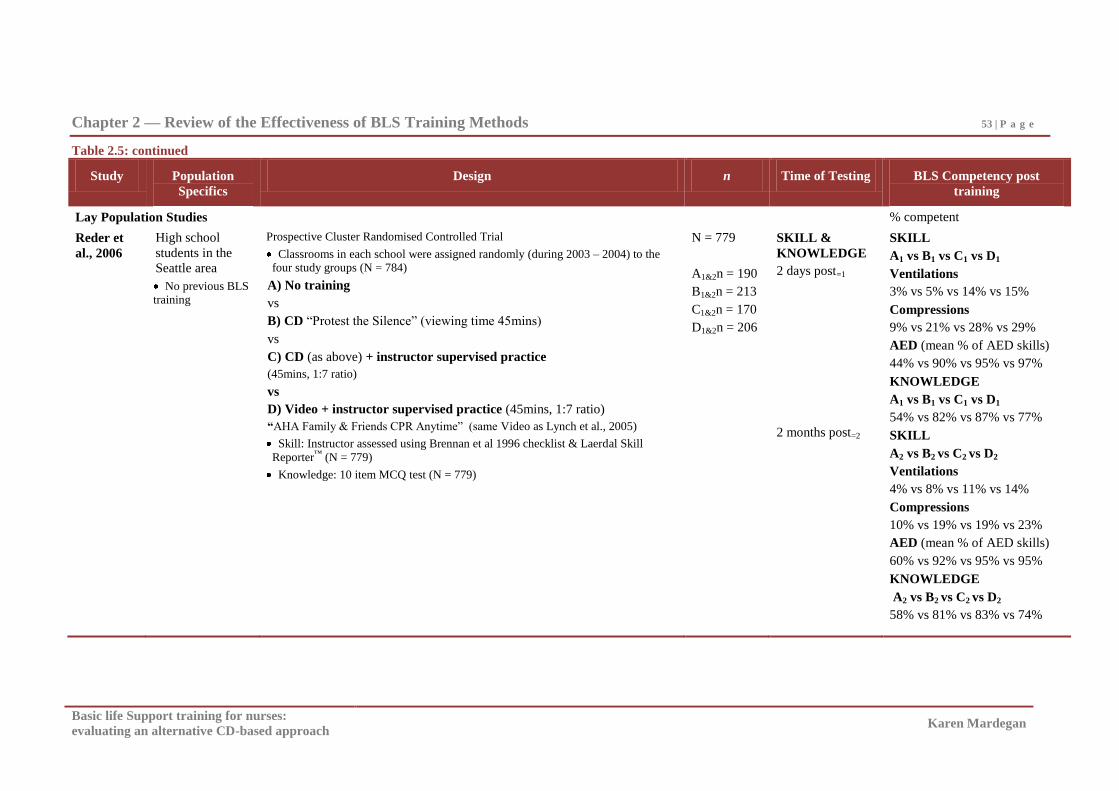
Chapter 2 — Review of the Effectiveness of BLS Training Methods 53 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.5: continued
Study Population
Specifics
Design n Time of Testing BLS Competency post
training
Lay Population Studies % competent
Reder et
al., 2006
High school
students in the
Seattle area
No previous BLS training
Prospective Cluster Randomised Controlled Trial
Classrooms in each school were assigned randomly (during 2003 – 2004) to the four study groups (N = 784)
A) No training
vs
B) CD ―Protest the Silence‖ (viewing time 45mins)
vs
C) CD (as above) + instructor supervised practice
(45mins, 1:7 ratio)
vs
D) Video + instructor supervised practice (45mins, 1:7 ratio)
―AHA Family & Friends CPR Anytime‖ (same Video as Lynch et al., 2005)
Skill: Instructor assessed using Brennan et al 1996 checklist & Laerdal Skill
Reporter™ (N = 779)
Knowledge: 10 item MCQ test (N = 779)
N = 779
A1&2n = 190
B1&2n = 213
C1&2n = 170
D1&2n = 206
SKILL &
KNOWLEDGE
2 days post=1
2 months post=2
SKILL
A1 vs B1 vs C1 vs D1
Ventilations
3% vs 5% vs 14% vs 15%
Compressions
9% vs 21% vs 28% vs 29%
AED (mean % of AED skills)
44% vs 90% vs 95% vs 97%
KNOWLEDGE
A1 vs B1 vs C1 vs D1
54% vs 82% vs 87% vs 77%
SKILL
A2 vs B2 vs C2 vs D2
Ventilations
4% vs 8% vs 11% vs 14%
Compressions
10% vs 19% vs 19% vs 23%
AED (mean % of AED skills)
60% vs 92% vs 95% vs 95%
KNOWLEDGE
A2 vs B2 vs C2 vs D2
58% vs 81% vs 83% vs 74%
Chapter 2 — Review of the Effectiveness of BLS Training Methods 54 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Of the four studies that evaluated CD programs in health professionals only one
randomly assigned participants (Monsieurs et al., 2004). Sample sizes in these four
studies ranged from 26 - 62 (Monsieurs et al., 2004; Moule & Gilchrist, 2001) to 137 -
358 (Clark et. al., 2000; Moule, 2002). Three of the four either evaluated the CD as an
adjunct to Traditional instructor-led training or provided an instructor supervised practice
following viewing of the CD (Clark et al., 2000; Moule, 2002; Moule & Gilchrist, 2001).
The additional health professional RCT study in Table 2.5 conducted by Fabius, Grissom
and Fuentes in 1994 (n = 70) randomised nurses into an integrated computer manikin
system, which no longer seems to be in production, but included both BLS training and
assessment by the computer system and as such is different to all the other programs
evaluated where skill competence is instructor determined. The only lay study located
was a cluster randomised controlled trail (n = 779) which evaluated CD and Video (with
and without instructor supervised practice), but not Traditional training, in high school
children (Reder et al., 2006). Independent evaluation of the effectiveness of CD training
is therefore limited by the small number and these study designs which do not include a
comparison with other training methods, include instructor-led practice or evaluate the
CD program as an adjunct to Traditional training.
For the health professional studies which evaluated the CD as an adjunct to
Traditional instructor-led training or provided an instructor supervised practice following
viewing of the CD, skill competence was reasonably high in the Traditional and
Traditional plus CD programs. Ninety five percent to 100% competence immediately
post and eight weeks post CD training was reported in the Clark et al. (2000) and pilot
Moule and Gilchrist (2001) CD studies, whereas competence ranging from 53% to 63%
eight weeks post training was reported in the Moule (2002) study. The lower skill
competence in the Moule (2002) study suggests that skill decline post training may be a
potential problem with this instructor-led practice plus CD design but further enquiry is
necessary before conclusions can be reached. If this is the case, it would be inconsistent
with the suggested benefit of BLS skill Videos in Traditional programs noted in the
Riegel et al. (2006) and Christenson et al. (2007) studies in Table 2.3. It is also
noteworthy that the computer manikin system plus human instructor practice in the
Fabius et al. study (1994) reported very low (17%) competence immediately post training.
This suggests that provision of an instructor-led practice is not a guarantee of adequate
Chapter 2 — Review of the Effectiveness of BLS Training Methods 55 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
skill development in health professionals and lay people (Fabius et al., 1994; Reder et al.,
2006). The Monsieurs et al. (2004) study evaluated CD with no practice in health
professionals and reported high (95%) skill competence immediately post training. This
is consistent with the findings reported in the Bobrow et al, (2011) Video (no manikin
practice) study in lay people (see Table 2.3). As elaborated earlier, these findings further
support the notion that practice may not be essential and therefore brings into question the
role of practice in CD and Video designs.
It is also important to note that for the high school students in the Reder et al.
(2006) RCT who receive the CD plus instructor-led practice, skill competence was very
poor (with 14% of ventilations and 28% of compressions performed competently) two
days post training. This result is however comparable to the outcomes for the CD alone
and Video plus instructor practice groups in the Reder et al. (2006) study, and
inconsistent with the Bobrow et al. (2011) RCT in Video (with and without practice)
programs evaluated in lay adults. There is therefore potential difference in skill between
high school children and mature adults. These conflicting findings in these two
randomised trials illustrate the need for additional studies evaluating CD programs in the
lay population.
Interestingly, CD programs which have included instructor practice and feedback
have not consistently produced adequate skill acquisition (Fabius et al., 1994; Moule,
2002; Reder et al., 2006). Therefore, the quality of the human instructor supervised
practice and feedback appears to be an important factor in the ultimate outcomes
achieved.
The three health professional studies (Clark et al., 2000; Fabius et al., 1994; Moule,
2002) and the one lay study (Reder et al., 2006) that evaluated BLS knowledge found
knowledge competence levels of between 80-95% immediately post CD training.
Knowledge retention was only reported in one study (Reder et al., 2006) and it suggests
minimal decline (81 - 83% competence) at two months post training in lay people.
Furthermore, from the limited number of studies available, knowledge competency
immediately post training in those who received CD training appears comparable to DVD
studies (Cason et al., 2006 see Table 2.4) and consistently higher than in Video and
Chapter 2 — Review of the Effectiveness of BLS Training Methods 56 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Traditional programs (Clark et al., 2000; Fabius et al., 1994; Reder et al., 2006; Todd et
al., 1998, 1999 [see Table 2.2 and Table 2.5]).
In summary, enquiry into the value of BLS CD training is limited. Although the
studies presented above have shown potential advantages in knowledge attainment
(Moule, 2002; Reder et al., 2006), the majority of studies have evaluated nursing students,
and limited the use of the CD. These studies have used the CD as either an adjunct to
Traditional instructor training (Clark, 2000; Fabius et al., 1994; Moule, 2002; Moule &
Gilchrist, 2001), a comparison with no training (Monsieurs et al., 2004), or used it
without concurrent manikin ‗practice‘ (Monsieurs et al., 2004; Reder et al., 2006). None
of the studies have compared Traditional BLS training with a BLS CD program where a
manikin is provided for unsupervised independent practice (similar to the Video/DVD
manikin kit design discussed above). Additionally, more extensive evaluation of initial
BLS skill and knowledge acquisition and retention of skill and knowledge in both the
health professional and lay population are needed for BLS CD programs to reliably
determine the relative benefits of this method of BLS training.
Basic life support training available through the Internet.
With the development of the Internet, the option to access BLS training through
DVD and CD packages via the Internet or an organisation‘s intranet is now available.
Mullner (2002) outlines the merits of placing BLS and ACLS simulations on the web to
enhance exposure of both lay and health professionals to BLS and ACLS information and
scenarios. Three types of BLS training provided through the Internet are beginning to be
evaluated. BLS training programs, BLS animations, and virtual world BLS team training.
BLS training programs compiled within a website include a combination of video, text,
animations and illustrations co-ordinated similarly to CD BLS training programs. BLS
animations are similar to the Video/DVD training programs in that they provide a
―perfect‖ run through of the BLS sequence for viewers. Simulated characters
demonstrate the sequence rather than demonstration by human instructors displayed on
Video and DVD training programs. Virtual world BLS training is essentially a virtual
computer game that has been constructed around the concepts of BLS and resuscitation
scenarios. These applications provide team and scenario practice in BLS using simulated
characters. It appears to be used primarily for those who have already received training in
Chapter 2 — Review of the Effectiveness of BLS Training Methods 57 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
the BLS procedure. Nine of the studies which have evaluated BLS training programs,
animations and virtual world training provided through the Internet have been
summarised in Table 2.6.
Internet BLS training programs.
Five Internet BLS training programs are described in Table 2.6, (three in health
professionals and two in lay people). Two included a pre-test, one for the skill (Sarac &
Ok, 2010) and one for the knowledge (Moule et al., 20008a) component. Three of these
five studies were RCT (Kardong-Edgren et al., 2010; Roppolo et al., 2011; Sarac & Ok,
2010) and apart from the larger study by Kardong-Edgren et al. (2010) in nursing students
(n = 595), sample sizes were less than 200 (Moule et al., 2008a; Roppolo et al., 2011;
Sarac & Ok, 2010; Teague & Riley, 2006). These studies compared the Internet BLS
training program with Traditional programs (Kardong-Edgren et al., 2010; Moule et al.,
2008a; Roppolo et al., 2011; Sarac & Ok, 2010) or a no training group control (Teague &
Riley, 2006).
The BLS Internet programs presented in Table 2.6, produced very low (22% to
53%) skill competence in both Internet and Traditional training methods immediately post
training in health professionals, even when an AHA BLS skill Video and instructor
practice was included as part of the Traditional AHA program (Kardong-Edgren et al.,
2010). The addition of a Voice Activated Manikin (VAM), which provides real-time
manikin feedback, as part of the Internet program (Kardong-Edgren et al., 2010) appears
to result in competence immediately post training that was statistically better than the
Traditional program but still well below skill mastery levels (Kardong-Edgren et al.,
2010). Very low skill competence was also reported when no manikin practice was
provided with Internet programs in high school students (Teague & Riley, 2006).
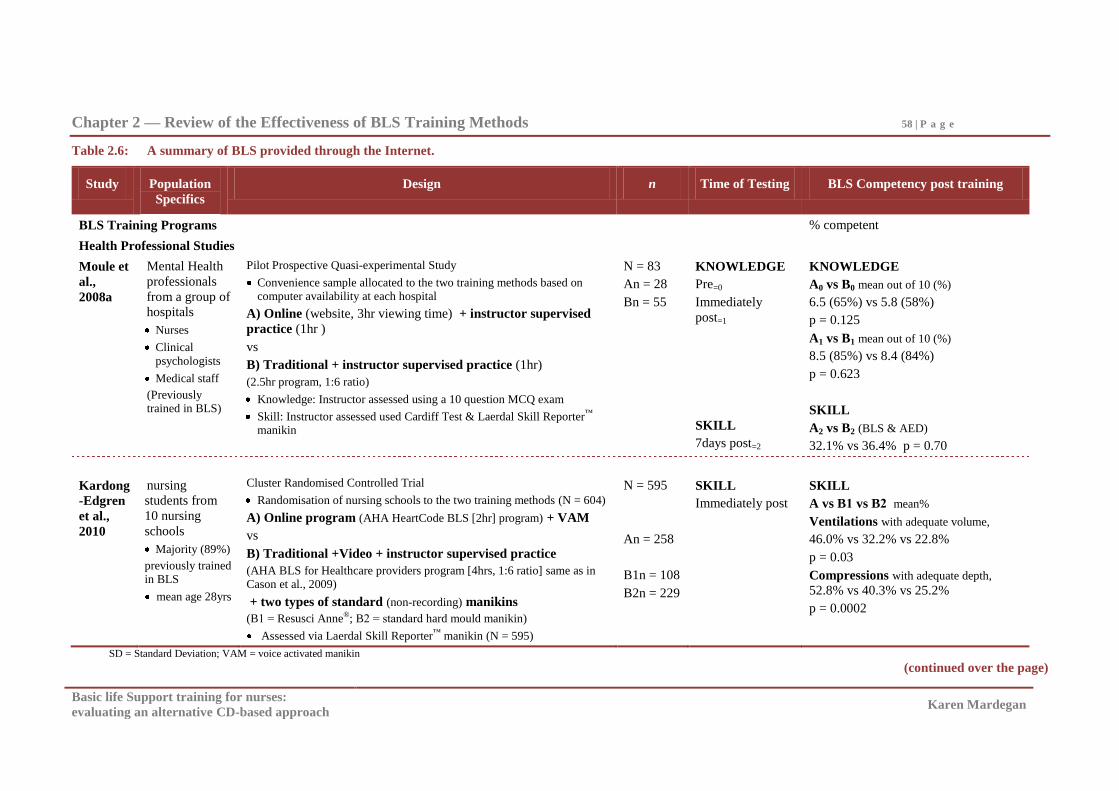
Chapter 2 — Review of the Effectiveness of BLS Training Methods 58 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.6: A summary of BLS provided through the Internet.
Study Population
Specifics
Design n Time of Testing BLS Competency post training
BLS Training Programs % competent
Health Professional Studies
Moule et
al.,
2008a
Mental Health
professionals
from a group of
hospitals
Nurses
Clinical
psychologists
Medical staff
(Previously trained in BLS)
Pilot Prospective Quasi-experimental Study
Convenience sample allocated to the two training methods based on computer availability at each hospital
A) Online (website, 3hr viewing time) + instructor supervised
practice (1hr )
vs
B) Traditional + instructor supervised practice (1hr)
(2.5hr program, 1:6 ratio)
Knowledge: Instructor assessed using a 10 question MCQ exam
Skill: Instructor assessed used Cardiff Test & Laerdal Skill Reporter™ manikin
N = 83
An = 28
Bn = 55
KNOWLEDGE
Pre=0
Immediately
post=1
SKILL
7days post=2
KNOWLEDGE
A0 vs B0 mean out of 10 (%)
6.5 (65%) vs 5.8 (58%)
p = 0.125
A1 vs B1 mean out of 10 (%)
8.5 (85%) vs 8.4 (84%)
p = 0.623
SKILL
A2 vs B2 (BLS & AED)
32.1% vs 36.4% p = 0.70
Kardong
-Edgren
et al.,
2010
nursing
students from
10 nursing
schools
Majority (89%)
previously trained
in BLS
mean age 28yrs
Cluster Randomised Controlled Trial
Randomisation of nursing schools to the two training methods (N = 604)
A) Online program (AHA HeartCode BLS [2hr] program) + VAM
vs
B) Traditional +Video + instructor supervised practice
(AHA BLS for Healthcare providers program [4hrs, 1:6 ratio] same as in
Cason et al., 2009)
+ two types of standard (non-recording) manikins
(B1 = Resusci Anne®; B2 = standard hard mould manikin)
Assessed via Laerdal Skill Reporter™ manikin (N = 595)
N = 595
An = 258
B1n = 108
B2n = 229
SKILL
Immediately post
SKILL
A vs B1 vs B2 mean%
Ventilations with adequate volume,
46.0% vs 32.2% vs 22.8%
p = 0.03
Compressions with adequate depth,
52.8% vs 40.3% vs 25.2%
p = 0.0002
SD = Standard Deviation; VAM = voice activated manikin
(continued over the page)
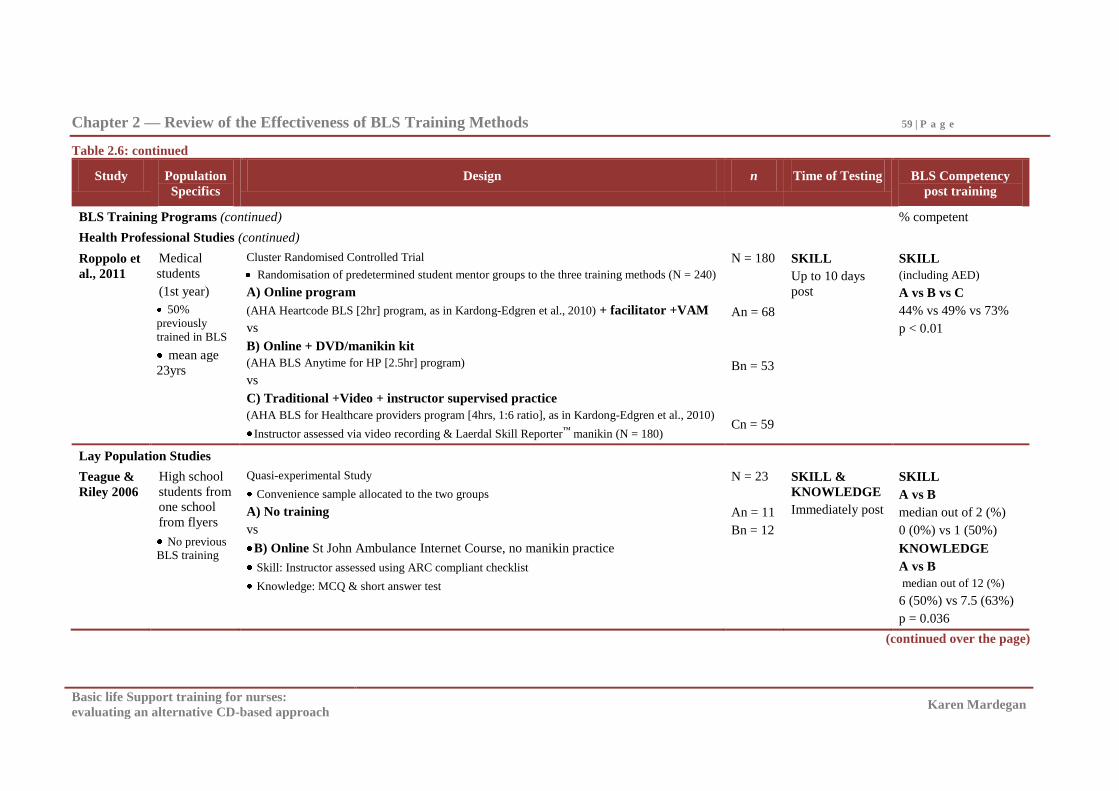
Chapter 2 — Review of the Effectiveness of BLS Training Methods 59 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.6: continued
Study Population
Specifics
Design n Time of Testing BLS Competency
post training
BLS Training Programs (continued) % competent
Health Professional Studies (continued)
Roppolo et
al., 2011
Medical
students
(1st year)
50%
previously
trained in BLS
mean age
23yrs
Cluster Randomised Controlled Trial
Randomisation of predetermined student mentor groups to the three training methods (N = 240)
A) Online program
(AHA Heartcode BLS [2hr] program, as in Kardong-Edgren et al., 2010) + facilitator +VAM
vs
B) Online + DVD/manikin kit
(AHA BLS Anytime for HP [2.5hr] program)
vs
C) Traditional +Video + instructor supervised practice
(AHA BLS for Healthcare providers program [4hrs, 1:6 ratio], as in Kardong-Edgren et al., 2010)
Instructor assessed via video recording & Laerdal Skill Reporter™ manikin (N = 180)
N = 180
An = 68
Bn = 53
Cn = 59
SKILL
Up to 10 days
post
SKILL
(including AED)
A vs B vs C
44% vs 49% vs 73%
p < 0.01
Lay Population Studies
Teague &
Riley 2006
High school
students from
one school
from flyers
No previous BLS training
Quasi-experimental Study
Convenience sample allocated to the two groups
A) No training
vs
B) Online St John Ambulance Internet Course, no manikin practice
Skill: Instructor assessed using ARC compliant checklist
Knowledge: MCQ & short answer test
N = 23
An = 11
Bn = 12
SKILL &
KNOWLEDGE
Immediately post
SKILL
A vs B
median out of 2 (%)
0 (0%) vs 1 (50%)
KNOWLEDGE
A vs B
median out of 12 (%)
6 (50%) vs 7.5 (63%)
p = 0.036
(continued over the page)
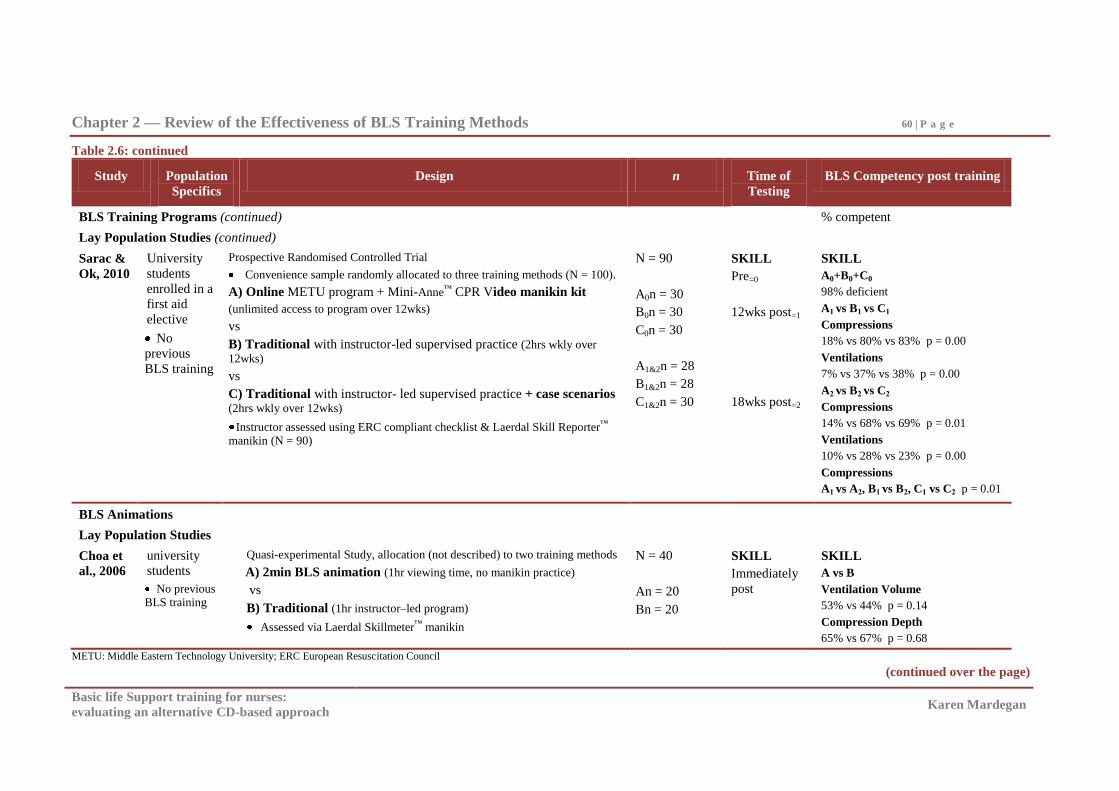
Chapter 2 — Review of the Effectiveness of BLS Training Methods 60 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.6: continued
Study Population
Specifics
Design n Time of
Testing
BLS Competency post training
BLS Training Programs (continued) % competent
Lay Population Studies (continued)
Sarac &
Ok, 2010
University
students
enrolled in a
first aid
elective
No
previous
BLS training
Prospective Randomised Controlled Trial
Convenience sample randomly allocated to three training methods (N = 100).
A) Online METU program + Mini-Anne™ CPR Video manikin kit
(unlimited access to program over 12wks)
vs
B) Traditional with instructor-led supervised practice (2hrs wkly over
12wks)
vs
C) Traditional with instructor- led supervised practice + case scenarios (2hrs wkly over 12wks)
Instructor assessed using ERC compliant checklist & Laerdal Skill Reporter™ manikin (N = 90)
N = 90
A0n = 30
B0n = 30
C0n = 30
A1&2n = 28
B1&2n = 28
C1&2n = 30
SKILL
Pre=0
12wks post=1
18wks post=2
SKILL
A0+B0+C0
98% deficient
A1 vs B1 vs C1
Compressions
18% vs 80% vs 83% p = 0.00
Ventilations
7% vs 37% vs 38% p = 0.00
A2 vs B2 vs C2
Compressions
14% vs 68% vs 69% p = 0.01
Ventilations
10% vs 28% vs 23% p = 0.00
Compressions
A1 vs A2, B1 vs B2, C1 vs C2 p = 0.01
BLS Animations
Lay Population Studies
Choa et
al., 2006
university
students
No previous BLS training
Quasi-experimental Study, allocation (not described) to two training methods
A) 2min BLS animation (1hr viewing time, no manikin practice)
vs
B) Traditional (1hr instructor–led program)
Assessed via Laerdal Skillmeter™ manikin
N = 40
An = 20
Bn = 20
SKILL
Immediately
post
SKILL
A vs B
Ventilation Volume
53% vs 44% p = 0.14
Compression Depth
65% vs 67% p = 0.68
METU: Middle Eastern Technology University; ERC European Resuscitation Council
(continued over the page)
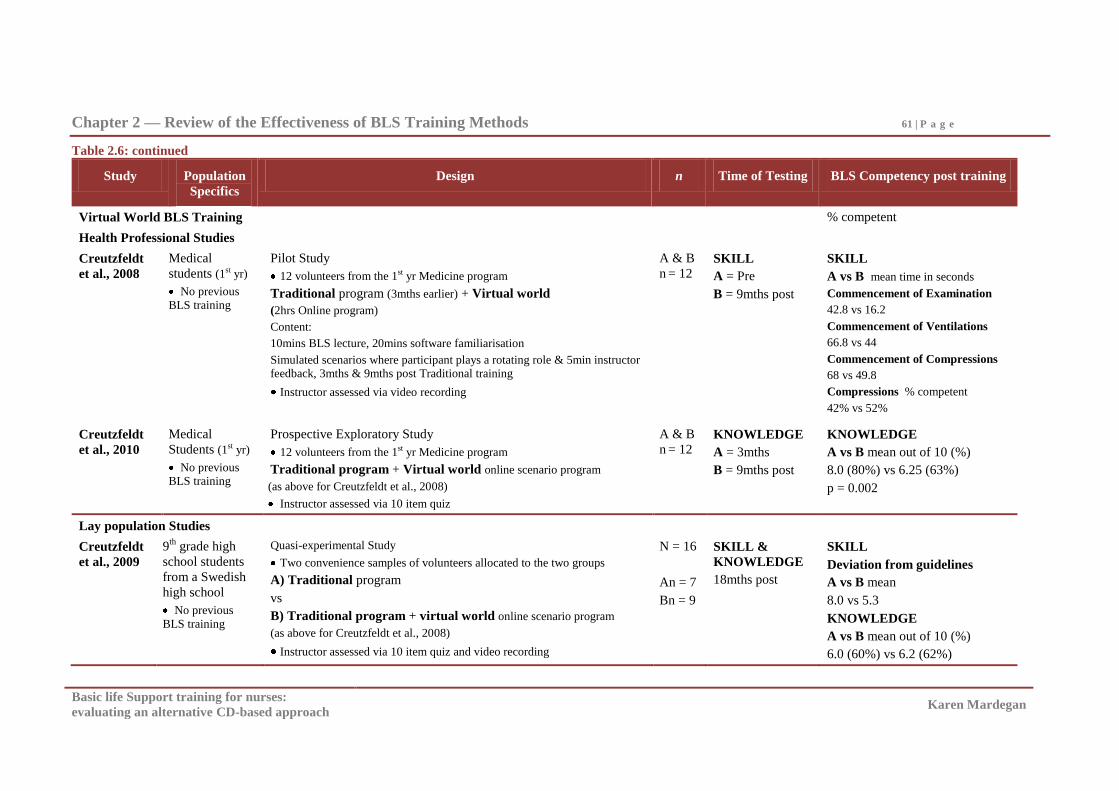
Chapter 2 — Review of the Effectiveness of BLS Training Methods 61 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.6: continued
Study Population
Specifics
Design n Time of Testing BLS Competency post training
Virtual World BLS Training % competent
Health Professional Studies
Creutzfeldt
et al., 2008
Medical
students (1st yr)
No previous
BLS training
Pilot Study
12 volunteers from the 1st yr Medicine program
Traditional program (3mths earlier) + Virtual world
(2hrs Online program)
Content:
10mins BLS lecture, 20mins software familiarisation
Simulated scenarios where participant plays a rotating role & 5min instructor feedback, 3mths & 9mths post Traditional training
Instructor assessed via video recording
A & B
n = 12
SKILL
A = Pre
B = 9mths post
SKILL
A vs B mean time in seconds
Commencement of Examination
42.8 vs 16.2
Commencement of Ventilations
66.8 vs 44
Commencement of Compressions
68 vs 49.8
Compressions % competent
42% vs 52%
Creutzfeldt
et al., 2010
Medical
Students (1st yr)
No previous BLS training
Prospective Exploratory Study
12 volunteers from the 1st yr Medicine program
Traditional program + Virtual world online scenario program
(as above for Creutzfeldt et al., 2008)
Instructor assessed via 10 item quiz
A & B
n = 12
KNOWLEDGE
A = 3mths
B = 9mths post
KNOWLEDGE
A vs B mean out of 10 (%)
8.0 (80%) vs 6.25 (63%)
p = 0.002
Lay population Studies
Creutzfeldt
et al., 2009
9th
grade high
school students
from a Swedish
high school
No previous
BLS training
Quasi-experimental Study
Two convenience samples of volunteers allocated to the two groups
A) Traditional program
vs
B) Traditional program + virtual world online scenario program
(as above for Creutzfeldt et al., 2008)
Instructor assessed via 10 item quiz and video recording
N = 16
An = 7
Bn = 9
SKILL &
KNOWLEDGE
18mths post
SKILL
Deviation from guidelines
A vs B mean
8.0 vs 5.3
KNOWLEDGE
A vs B mean out of 10 (%)
6.0 (60%) vs 6.2 (62%)
Chapter 2 — Review of the Effectiveness of BLS Training Methods 62 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
In health professionals seven days post training, an Internet program (that included
instructor-led manikin practice) produced very low skill competence as did a Traditional
instructor-led program (32% vs 36%, Moule et al., 2008a). Skill competence for health
professionals 10 days post training was 44% for an Internet program and 73% for a
Traditional program (Roppolo et al., 2011). For university students 12 weeks post
training, 18% competence for compressions and seven percent for ventilations for the
Internet program was reported compared with 80% and 37% for the Traditional program
(Sarac & Ok, 2010). These differences between the Internet and Traditional programs 10
days and 12 weeks post training in health professional and lay people were statistically
significant. Therefore skill competence at 10 days post training in medical students
(Roppolo et al., 2011) and 12 weeks post training in one study of university students
(Sarac & Ok, 2010) was significantly better with a standard Traditional program (Sarac &
Ok, 2010) and a Traditional AHA program which includes a skill Video (Roppolo et al.,
2011) compared to Internet programs which either included a Video manikin kit (Sarac &
Ok, 2010) or the AHA Internet program plus a facilitator and a VAM manikin (Roppolo
et al., 2011). Furthermore there was significant skill decline between 12 and 18 weeks
post training in both the Internet and Traditional programs in university students (Sarac &
Ok. 2010).
BLS knowledge competence following Internet BLS programs have been evaluated
in one health professional and one lay study of high school students, immediately post
training (Moule et al., 2008a; Teague & Riley, 2006). In contrast to BLS skill,
comparably high BLS knowledge (85%) in health professionals and (63%) in high school
students was reported immediately post Internet training. Studies reporting on retention
of knowledge following Internet BLS programs have not been found. High BLS
knowledge competence immediately post training is consistent with CD and DVD studies
(Cason et al., 2006; Clark et al., 2000; Fabius et al., 1994; Moule, 2002; Reder et al.,
2006) and higher than in Video and the Traditional programs evaluated in these studies
(Clark et al., 2000; Fabius et al., 1994; Reder, et al., 2006; Todd et al., 1998, 1999 [see
Table 2.2 and Table 2.5]).
These studies of BLS Internet programs therefore appear to suggest that skill
competence with Internet BLS programs are low immediately and seven days to 12 weeks
post training (Moule et al., 2008a; Roppolo et al., 2011; Sarac & Ok, 2010; Teague &
Chapter 2 — Review of the Effectiveness of BLS Training Methods 63 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Riley, 2006). Although the Internet program reported significantly better (but low)
competence immediately post training in nursing students (Kardong-Edgren et al., 2010),
Traditional programs appear to produce significantly better skill competence with higher
competence rates (73% - 80%) 10 days to 12 weeks post training in both health
professional and lay people (Roppolo et al., 2011; Sarac & Ok, 2010). There also appears
to be significant skill decline with both the Internet and Traditional programs evaluated.
BLS knowledge appears high immediately post training in Internet and the Traditional
programs in health professional and lay groups (Moule et al., 2008a; Teague & Riley,
2006). It is also noteworthy that additional insights into Traditional plus skill Video
programs, Video/DVD manikin kits, VAM manikins and the role of feedback can also be
drawn from these Internet studies. These are discussed below.
It is interesting that the Traditional plus Video programs in the Kardong-Edgren et
al. (2010) and Roppolo et al. (2011) studies were the same AHA program, yet skill
competence in this Traditional program in the Kardong-Edgren et al. (2010) study was
low, where as skill competence for the same program in the Roppolo et al. (2011) study
was high. Additionally, high skill competence has also been reported in other Traditional
with Video RCT studies (Christenson et al., 2007; Riegel et al., 2006) and Traditional
with CD studies (Clark et al., 2000; Moule & Gilchrist 2001), suggesting that there is
most likely some benefit in combining a skill Video/DVD or CD with Traditional
programs.
The low Video/DVD manikin kit skill competency at 10 days and 12 weeks when
used with Internet programs by medical and university students (Roppolo et al., 2010;
Sarac & Ok, 2010) is consistent with some lay (Braslow et al., 1997; Isbye et al., 2006;
Neilson et al., 2010; Todd et al., 1999) Video/DVD manikin kit studies but not all. Other
lay (Chung et al., 2010; Mancini et al., 2009; Roppolo et al., 2007) and health
professional (Bjorshol et al., 2009; Cason et al., 2009) Video /DVD manikin kit studies
found high skill competence up to a year post training. The skill decline post training
noted in the Sarac & Ok (2010) RCT in university students is also consistent with some
(Einspruch et al., 2007; Roppolo et al., 2007) but not all (Chung et al., 2010) Video and
DVD manikin kits in lay people. Therefore, there is inconsistent skill competence and
retention particularly in lay groups when Video manikin kits are combined with Internet
programs or used in isolation. The need for continued exploration to identify modes of
Chapter 2 — Review of the Effectiveness of BLS Training Methods 64 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
training that can improve the outcomes seen with Video/DVD manikin kits therefore
continue to be warranted.
Enquiry into the VAM is only very recent, however from the two studies in health
professionals in Table 2.6, it appears that when a VAM is added to the design of an
Internet program to allow for manikin practice and feedback by the manikin, there was
low (46% - 53%) but significantly better skill competence for the Internet plus VAM
design when compared with the Traditional AHA program immediately post training with
nursing students (Kardong-Edgren et al., 2010). Interestingly, at 10 days post training
medical students using the same Internet plus VAM program demonstrated similar low
competence levels (44%) to that seen immediately post training in the Kardong-Edgren et
al. (2010) study, but the Traditional AHA program (also the same as in Kardong-Edgren
et al., 2010 study), was in this case significantly better than the Internet VAM program
(Roppolo et al., 2011). Considering that the VAM skill outcome in both these studies is
comparable (44% - 53%), difference in skill competence between medical and nursing
students appear unlikely, therefore this variation in the Traditional AHA program
outcome is potentially variation in instructor delivery.
The role of feedback in BLS training is also of interest. There is low skill
competence in health professional samples (Kardong-Edgren et al., 2010; Roppolo et al.,
2010) when a VAM feedback manikin is used in conjunction with Internet programs.
There are also many instances, particularly in the CD literature where instructor feedback
has not appeared to make any difference to skill outcome (Fabius et al., 1994; Moule,
2002; Reder et al., 2006). High skill competence is also seen in some instances,
particularly in health professional samples, with the Video/DVD kit studies where there is
no feedback (Cason et al., 2009; Chung et al., 2010; Mancini et al., 2009; Roppolo et al.,
2007; Todd et al., 1998). This suggests that feedback is possibly not as crucial for BLS
training as suggested in the broader training design and delivery (Aguinis & Kraiger,
2009; Salas & Cannon-Bowers, 2001) and resuscitation literature (ARC & NZRC, 2010a;
Hazinski et al., 2010; Mancini et al., 2010). However, as this is the beginning of enquiry
in the VAM, further evaluation of the VAM in particularly lay people is needed before
definitive conclusions can be reached on VAM-provided feedback and feedback overall.
Chapter 2 — Review of the Effectiveness of BLS Training Methods 65 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS animations.
The one BLS animation study presented in Table 2.6 was with university students
(n = 40) and compared a two minute animation (where viewing time was one hour and no
manikin practice was provided) with a Traditional (one hour) instructor-led program.
Skill competence immediately post training was low for both the animation (with 53%
ventilations and 65% compressions performed competently) and Traditional groups (44%
ventilations and 67% compressions performed competently). This low but comparable
competency rate between the animation and Traditional program in Choa et al. (2006)
implies that BLS animations as a BLS training method is comparable to Traditional
instructor-led methods, and that CPR skills are not necessarily dependent on manikin
practice.
The comparable skill competence with and without manikin practice reported in the
Bobrow et al. (2011) and Reder et al., 2006 RCT studies in lay adults supports this
finding. However, skill competence is variable and more likely to be low in studies
where manikin practice is not provided (Bobrow et al., 2011; Choa et al., 2006;
Monsieurs et al., 2004; Reder et al., 2006; Teague & Riley, 2006). Additional research
into lay adults, children and health professional groups would therefore assist in clarifying
the role of manikin practice.
Virtual world BLS training.
The three virtual world BLS training programs in Table 2.6 were conducted by the
Creutzfeldt team. Two of the studies were with medical students (Creutzfeldt et al., 2008,
2010) and one was in high school students (Creutzfeldt et al., 2009). These pilot studies
(n < 16) evaluated BLS training using virtual world simulated BLS scenarios in addition
to Traditional BLS training. There was a decreased mean time to the commencement of
CPR, 10% improvement in the performance of compressions at nine months, and good
BLS knowledge (80%) at three months post virtual world scenario training, with a decline
(62%) in BLS knowledge from three to nine months post training for medical students
(Creutzfeldt et al., 2008, 2010). In the 2009 study, which compared Traditional BLS
training with and without virtual world training, less variation from resuscitation
guidelines for the virtual training group and comparable BLS knowledge 18 months post
training was reported for a high school student sample (Creutzfeldt et al., 2009). This
recent evaluation of virtual world BLS scenario training suggests the potential for modest
Chapter 2 — Review of the Effectiveness of BLS Training Methods 66 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
improvements in BLS skill and comparable outcomes in BLS knowledge to Traditional
training with this form of training.
Conclusions from BLS Internet studies.
It is envisaged that the continual development and expansion of the Internet will
foster the availability of various combinations of BLS DVD and CD training programs,
simulations and virtual-world training programs through this medium. Research into the
effectiveness of this medium as a vehicle for BLS training is beginning to be published in
both the health professional and lay populations. The current research, presented in Table
2.6, where the BLS Internet program is an adjunct to Traditional instructor training
(Creutzfeldt et al., 2008, 2009, 2010; Moule et al., 2008a), compared with no training
(Teague & Riley, 2006) or used without concurrent manikin practice (Teague & Riley,
2006) limits determination of the efficiency of the training method for both BLS skill and
knowledge attainment. However, at this time, skill competence post training with Internet
programs appear to be comparably below skill mastery levels with Traditional methods
(Kardong-Edgren et al., 2010; Moule et al., 2008a; Roppolo et al., 2011). There are,
however, potential access advantages, good BLS knowledge achieved with Internet
training programs (Moule et al., 2008a; Teague & Riley, 2006) and modest improvements
in skill with virtual world training (Creutzfeldt et al., 2008, 2009, 2010).
Furthermore, BLS skill competence and retention of skill with the BLS Video/DVD
self-instructional kits, provided with Internet program in the Sarac and Ok (2010) and
Roppolo et al. (2011) studies provided further example of where skill competence with
these kits can be low, even in health professionals. Skill competence when Video
manikin kits are combined with Internet programs or used in isolation have therefore not
consistently demonstrated high skill competence with consistently good retention
particularly in lay groups (Batcheller et al., 2000; Braslow et al., 1997; Einspruch et al.,
2007; Lynch et al., 2005; Roppolo et al., 2007; Todd et al., 1999). The need for
continued exploration to identify modes of training that can improve upon the outcomes
seen with Video/DVD manikin kits therefore continues to be needed.
The findings from the BLS animation study conducted by Choa et al. (2006) imply
that manikin practice is not essential to the development of CPR skills. This is consistent
with the Bobrow et al. (2011) Video and Monsieurs et al. (2004) and Reder et al. (2001)
Chapter 2 — Review of the Effectiveness of BLS Training Methods 67 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
CD studies and the recent evaluation of the Internet AHA program accompanied by a
VAM (Kardong-Edgren et al., 2010; Roppolo et al., 2011). This implies that ‗practice‘
and ‗feedback‘ is potentially not as crucial for BLS training as suggested in the training
design and delivery (Aguinis & Kraiger, 2009; Salas & Cannon-Bowers, 2001) and
resuscitation practice recommendations (ARC & NZRC, 2010a; Hazinski et al., 2010;
Mancini et al., 2010). However, if this is the case then how best can BLS training
programs be developed to significantly improve upon the BLS training outcomes from
Traditional programs?
The literature reviewed suggests variable but overall positive findings from
Video/DVD kits particularly with health professionals (Bjorshol et al., 2009; Cason et al.,
2009; Todd et al., 1998), a lack of comparisons available with independent CD training
formats with and without practice (see Table 2.5) and limited outcomes from VAM in
Internet studies (Kardong-Edgren et al., 2010; Roppolo et al., 2011). It is therefore
proposed that enquiry firstly needs to concentrate on comparing the effectiveness of a
CD-based manikin BLS training program with a Traditional BLS training program both
initially post training and in retention of BLS skill and knowledge using standard
manikins. This will have cost and access advantages for the user. CD programs which
are not dependent on Internet access yet can also be provided via the Internet offer
increased flexibility when compared with programs which are only available via the
Internet. The Video/DVD kits have inflatable or cardboard manikins which are a
compact low-cost form of manikin which can easily and cheaply accompany a CD
program. The VAM at this stage is a cumbersome and expensive manikin that is most
suited to large organisations. Wide spread access to BLS training that includes manikin
practice is therefore more easily achieved in both the health professional and lay
populations using standard manikins and CD rather than Internet programs. There is also
the potential for improved outcomes with the unevaluated CD standard manikin model.
The minimal evaluation of BLS CD programs generally and the lack of evaluation of CD
designs which incorporate independent manikin practice coupled with their cost and
access advantages substantiate priority being given to the development and evaluation of
CD-based training methods rather than programs exclusively available via the internet or
VAM incorporated designs.
Chapter 2 — Review of the Effectiveness of BLS Training Methods 68 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Training Design, Delivery and Outcomes
BLS training is delivered using predominately Traditional classroom approaches.
However, the presented research suggests that there is a building interest in Multimedia
approaches to training. The skill and knowledge outcomes from these approaches to
training vary within each method and also to some degree are training method dependent,
making it difficult to determine the best current method, particularly when the
development and evaluation of methods like CD programs have been so limited.
Examination of how effectively the various modes of BLS training can address the
prescribed principles of training design and delivery, and overall BLS skill and
knowledge outcomes for these modes of BLS training potentially can assist in the
drawing of conclusions from this literature.
BLS training design and delivery.
The review of the general training design and delivery literature suggests that
training programs which meet the four training and delivery principles of relevance,
demonstration, practice and feedback should produce the best training outcomes. Table
2.7 summarizes and compares the features of Traditional and Multimedia BLS
approaches to training in relation to these prescribed principles of training design and
delivery.
Table 2.7 illustrates that both the Traditional and Multimedia BLS training methods
have the capacity to comply with the four principles of training design and delivery.
However, in Traditional approaches, standardisation of the delivery of the training is
difficult to guarantee because it is dependent upon the quality of the trainers delivering
the program (see Table 2.7). Multimedia approaches are standardised self-paced
approaches which facilitate incorporation of the principles of relevant information,
demonstration and practice; however their ability to provide feedback is dependent on the
availability of an instrumented (rather than the standard) manikin (Dine et al., 2008;
Edelson et al., 2008; Kardong-Edgren et al., 2010). Multimedia approaches are also
potentially more cost-effective than Traditional methods because they do not rely on a
human instructor, and allow for unlimited use for the individual and across organisations
(Todd et al., 1999).
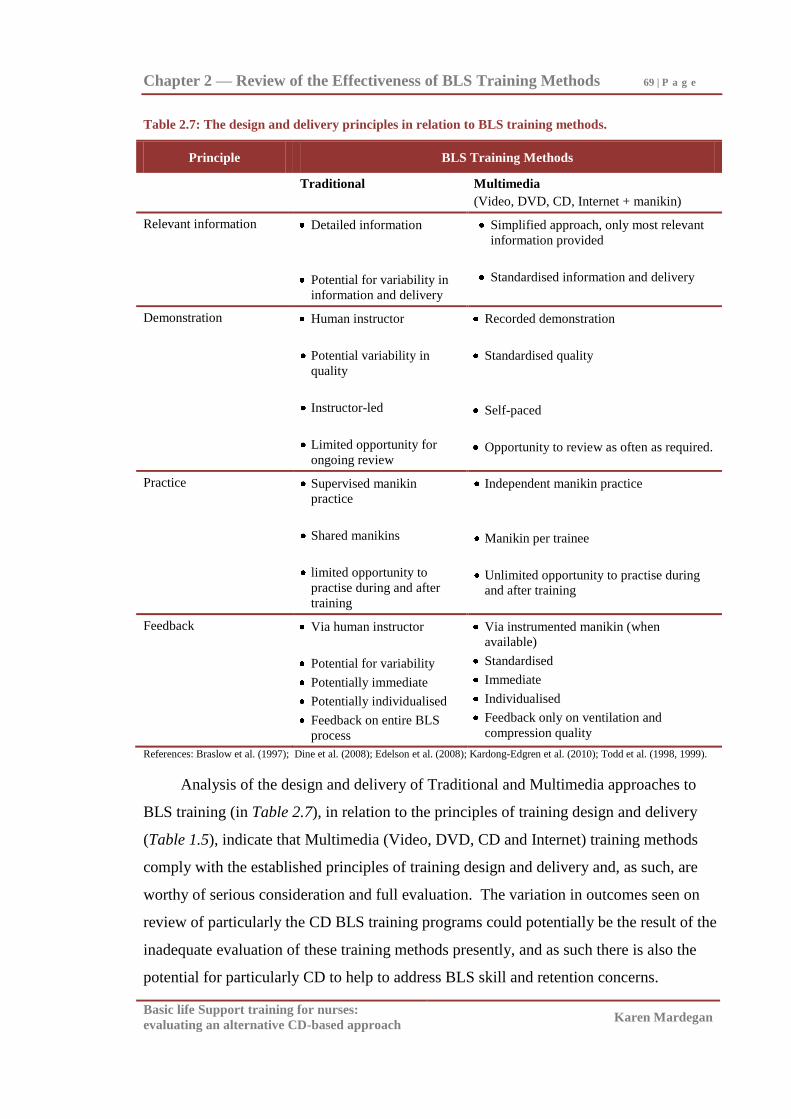
Chapter 2 — Review of the Effectiveness of BLS Training Methods 69 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.7: The design and delivery principles in relation to BLS training methods.
Principle BLS Training Methods
Traditional Multimedia
(Video, DVD, CD, Internet + manikin)
Relevant information
Detailed information
Potential for variability in
information and delivery
Simplified approach, only most relevant
information provided
Standardised information and delivery
Demonstration Human instructor
Potential variability in
quality
Instructor-led
Limited opportunity for
ongoing review
Recorded demonstration
Standardised quality
Self-paced
Opportunity to review as often as required.
Practice Supervised manikin
practice
Shared manikins
limited opportunity to
practise during and after
training
Independent manikin practice
Manikin per trainee
Unlimited opportunity to practise during
and after training
Feedback Via human instructor
Potential for variability
Potentially immediate
Potentially individualised
Feedback on entire BLS
process
Via instrumented manikin (when
available)
Standardised
Immediate
Individualised
Feedback only on ventilation and
compression quality
References: Braslow et al. (1997); Dine et al. (2008); Edelson et al. (2008); Kardong-Edgren et al. (2010); Todd et al. (1998, 1999).
Analysis of the design and delivery of Traditional and Multimedia approaches to
BLS training (in Table 2.7), in relation to the principles of training design and delivery
(Table 1.5), indicate that Multimedia (Video, DVD, CD and Internet) training methods
comply with the established principles of training design and delivery and, as such, are
worthy of serious consideration and full evaluation. The variation in outcomes seen on
review of particularly the CD BLS training programs could potentially be the result of the
inadequate evaluation of these training methods presently, and as such there is also the
potential for particularly CD to help to address BLS skill and retention concerns.
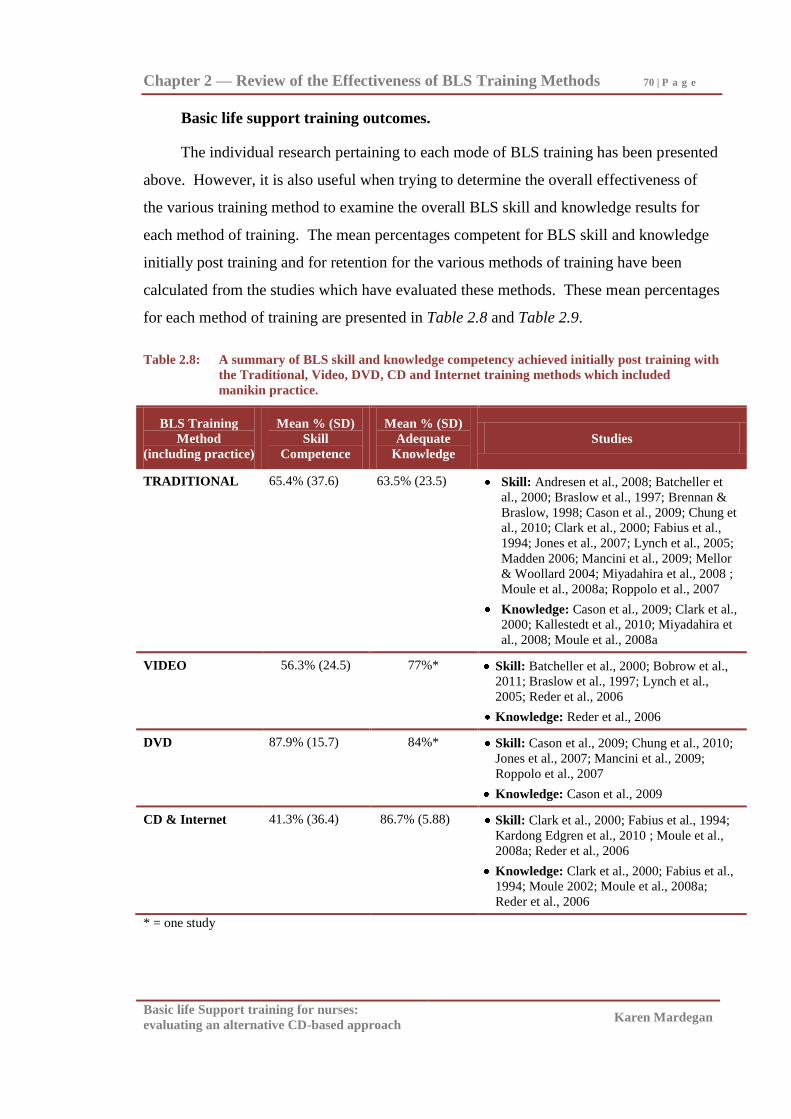
Chapter 2 — Review of the Effectiveness of BLS Training Methods 70 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Basic life support training outcomes.
The individual research pertaining to each mode of BLS training has been presented
above. However, it is also useful when trying to determine the overall effectiveness of
the various training method to examine the overall BLS skill and knowledge results for
each method of training. The mean percentages competent for BLS skill and knowledge
initially post training and for retention for the various methods of training have been
calculated from the studies which have evaluated these methods. These mean percentages
for each method of training are presented in Table 2.8 and Table 2.9.
Table 2.8: A summary of BLS skill and knowledge competency achieved initially post training with
the Traditional, Video, DVD, CD and Internet training methods which included
manikin practice.
BLS Training
Method
(including practice)
Mean % (SD)
Skill
Competence
Mean % (SD)
Adequate
Knowledge
Studies
TRADITIONAL 65.4% (37.6) 63.5% (23.5) Skill: Andresen et al., 2008; Batcheller et
al., 2000; Braslow et al., 1997; Brennan &
Braslow, 1998; Cason et al., 2009; Chung et
al., 2010; Clark et al., 2000; Fabius et al.,
1994; Jones et al., 2007; Lynch et al., 2005;
Madden 2006; Mancini et al., 2009; Mellor
& Woollard 2004; Miyadahira et al., 2008 ;
Moule et al., 2008a; Roppolo et al., 2007
Knowledge: Cason et al., 2009; Clark et al.,
2000; Kallestedt et al., 2010; Miyadahira et
al., 2008; Moule et al., 2008a
VIDEO 56.3% (24.5) 77%* Skill: Batcheller et al., 2000; Bobrow et al.,
2011; Braslow et al., 1997; Lynch et al.,
2005; Reder et al., 2006
Knowledge: Reder et al., 2006
DVD 87.9% (15.7) 84%* Skill: Cason et al., 2009; Chung et al., 2010;
Jones et al., 2007; Mancini et al., 2009;
Roppolo et al., 2007
Knowledge: Cason et al., 2009
CD & Internet 41.3% (36.4) 86.7% (5.88) Skill: Clark et al., 2000; Fabius et al., 1994;
Kardong Edgren et al., 2010 ; Moule et al.,
2008a; Reder et al., 2006
Knowledge: Clark et al., 2000; Fabius et al.,
1994; Moule 2002; Moule et al., 2008a;
Reder et al., 2006
* = one study
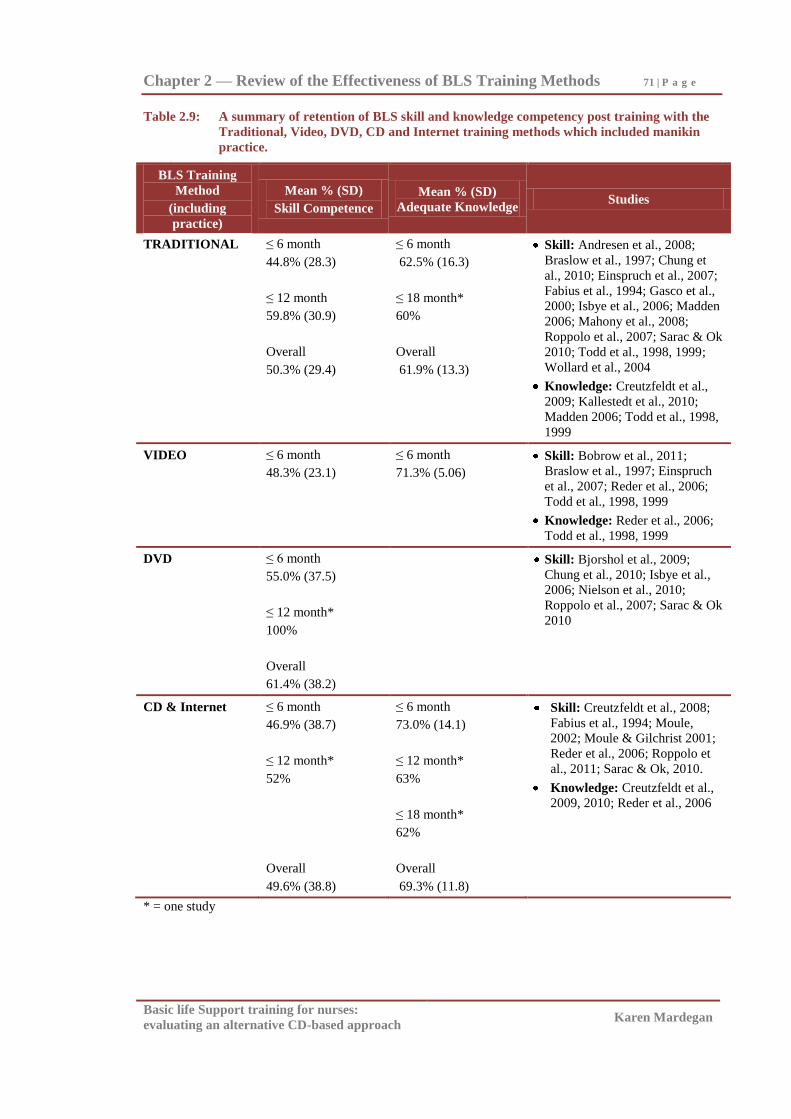
Chapter 2 — Review of the Effectiveness of BLS Training Methods 71 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 2.9: A summary of retention of BLS skill and knowledge competency post training with the
Traditional, Video, DVD, CD and Internet training methods which included manikin
practice.
BLS Training
Method
(including
practice)
Mean % (SD)
Skill Competence
Mean % (SD)
Adequate Knowledge Studies
TRADITIONAL ≤ 6 month
44.8% (28.3)
≤ 12 month
59.8% (30.9)
Overall
50.3% (29.4)
≤ 6 month
62.5% (16.3)
≤ 18 month*
60%
Overall
61.9% (13.3)
Skill: Andresen et al., 2008;
Braslow et al., 1997; Chung et
al., 2010; Einspruch et al., 2007;
Fabius et al., 1994; Gasco et al.,
2000; Isbye et al., 2006; Madden
2006; Mahony et al., 2008;
Roppolo et al., 2007; Sarac & Ok
2010; Todd et al., 1998, 1999;
Wollard et al., 2004
Knowledge: Creutzfeldt et al.,
2009; Kallestedt et al., 2010;
Madden 2006; Todd et al., 1998,
1999
VIDEO ≤ 6 month
48.3% (23.1)
≤ 6 month
71.3% (5.06)
Skill: Bobrow et al., 2011;
Braslow et al., 1997; Einspruch
et al., 2007; Reder et al., 2006;
Todd et al., 1998, 1999
Knowledge: Reder et al., 2006;
Todd et al., 1998, 1999
DVD ≤ 6 month
55.0% (37.5)
≤ 12 month*
100%
Overall
61.4% (38.2)
Skill: Bjorshol et al., 2009;
Chung et al., 2010; Isbye et al.,
2006; Nielson et al., 2010;
Roppolo et al., 2007; Sarac & Ok
2010
CD & Internet ≤ 6 month
46.9% (38.7)
≤ 12 month*
52%
Overall
49.6% (38.8)
≤ 6 month
73.0% (14.1)
≤ 12 month*
63%
≤ 18 month*
62%
Overall
69.3% (11.8)
Skill: Creutzfeldt et al., 2008;
Fabius et al., 1994; Moule,
2002; Moule & Gilchrist 2001;
Reder et al., 2006; Roppolo et
al., 2011; Sarac & Ok, 2010.
Knowledge: Creutzfeldt et al.,
2009, 2010; Reder et al., 2006
* = one study
Chapter 2 — Review of the Effectiveness of BLS Training Methods 72 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
When examining the effectiveness of these various BLS training methods the mean
percentage for BLS skill and knowledge post training with Traditional methods are 65.4%
(SD = 37.6) and 63.5% (SD = 23.5) respectively, Video is 56.3% (SD = 24.5) and 77%
(one study only), DVD is 87.9% (SD = 15.7) and 84% (one study only), and CD and
Internet programs are 41.3% (SD = 36.4) and 86.7% (SD = 5.88) respectively (see Table
2.8). This illustrates that BLS skill initially post training is well below skill mastery
standards (80%) for all training methods accept for DVD manikin kits, and DVD, CD and
Internet programs produce adequate BLS knowledge (above 80%) post training.
For retention, BLS skill and knowledge by six months with Traditional methods is
44.8% (SD = 28.3) and 62.5% (SD = 6.4) respectively, Video is 48.3% (SD = 23.1) and
71.3% (SD = 5.06), DVD is 55.0% (SD = 37.5), with no studies found which examined
knowledge, and CD and Internet programs are 46.9% (SD = 38.7) for skill and 73.0% (SD
= 14.1) for knowledge (see Table 2.9). This illustrates decay of skill and knowledge with
all BLS training methods of at least 20% for skill and 10% for knowledge competency by
six months post training (≤ 6 month overall all methods: Skill decline 22%, Knowledge
decline 12.6% [see Table 2.8 and Table 2.9]).
Video and particularly DVD programs have therefore demonstrated improved BLS
skill (DVD: mean skill competence initially post training 87.9% [see Table 2.8]) and
comparable outcomes to other methods at follow-up (≤ 6 month DVD: Skill decline =
32.9% [see Table 2.8 and Table 2.9]), which suggests partial improvement in program
effectiveness when compared to other methods for skill acquisition.
BLS knowledge initially post training and over time, in the small number of
available studies, appears to be consistently higher than skill competency rates, regardless
of training method. CD and Internet programs appear to have marginally better initial and
retention of knowledge rates when compared with Traditional and Video studies (see
Table 2.8 and Table 2.9).
It would therefore theoretically follow from this evaluation of training design and
delivery principles and overall training outcomes for the methods, that CD programs that
include independent manikin practice have the capacity to produce at least the overall
skill outcomes seen with DVD (because they are able to include more indepth information
then Video or DVD, in addition to the video footage of the BLS sequence), and improved
Chapter 2 — Review of the Effectiveness of BLS Training Methods 73 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS knowledge illustrated in the CD and Internet studies evaluated above. There is
therefore also the potential for improved skill and knowledge retention.
Summary of BLS skill, knowledge and current modes of training.
The poor BLS skills and retention of skill in the health professional and lay
populations, illustrated in the Traditional BLS training summaries Table 1.2, Table 1.3
and Table 2.1, suggest that there are limitations to the Traditional approaches to BLS
training using an instructor-led BLS presentation/demonstration/practice format. The
Videotape and its modern equivalent, the DVD and manikin model, have been heralded as
a suitable alternative to Traditional BLS training methods (Hazinski et al., 2010; Mancini
et al., 2010). However, variable BLS skill outcomes and poor retention are still a concern
with these two methods. CD programs have not been evaluated sufficiently to determine
their capabilities. However, particularly if independent manikin practice is incorporated,
there is a potential for them to improve upon the currently variable BLS skill and poor
retention of skill and knowledge reported in the literature.
The above literature review illustrates that both the development and evaluation of
Videotape and DVD BLS training programs have been far greater than the corresponding
development and evaluation of BLS CD (see Table 2.2, Table 2.3, Table 2.4, and Table
2.5). The scarcity of literature (see Table 2.5) evaluating BLS CD training programs
suggests that there may be little pressure for further evaluating BLS CD technology, if
Videotape/DVD technology is providing potential improvement at least in BLS skill
immediately following training.
However, studies evaluating and comparing Traditional BLS training approaches
with a BLS CD-based approach have not been found, either with or without a non-
integrated manikin. This suggests that the actual potential for this method of training is
still unknown. Providing the opportunity for independent manikin practice while viewing
a BLS CD could be potentially as effective, flexible and cost effective as the Video
manikin formula of Braslow and his contemporaries in Video and DVD (Batcheller et al.,
2000; Braslow et al., 1997; Chung et al., 2010; Einspruch et al., 2007; Lynch et al., 2005;
Todd et al., 1998, 1999 [see Table 2.2, Table 2.3, and Table 2.4]).
Furthermore, retention of BLS skill over time continues to be a concern regardless
of training method (Table 2.9). Video and DVD have not consistently demonstrated any
Chapter 2 — Review of the Effectiveness of BLS Training Methods 74 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
considerable improvement in retention of skill over time when compared with outcomes
from Traditionally-trained participants (Braslow et al, 1997; Einspruch et al., 2007;
Roppolo et al., 2007; Todd et al., 1999). Training methods which maximise skill
retention are required. The potential of CD-based and Internet BLS training programs
have not yet been established in the literature.
It is also noteworthy that many previous studies have evaluated BLS skills where
participants perform direct mouth-to-mouth ventilation and one-rescuer BLS. Health
professionals worldwide are currently required to be able to competently perform not only
BLS using mouth-to-mouth ventilation, but also two-rescuer BLS using ventilation
apparatus such as the one-way valve mask and bag-mask devices (ARC, 2004a;
Henderson, 1992; Hurst, West, Austin, Branson, & Beck, 2007; Kardong-Edgren et al.,
2010; Lee, Cho, Choi, & Yoon, 2008; Osterwalder & Schuhwerk, 1998; Paal, et al., 2010;
Salas, Wisor, Agazio, Branson, & Austin, 2007). Studies which evaluate participants‘
ability to perform BLS using required equipment are needed to assist understanding
particularly of health professionals‘ BLS ventilation skills and the proficiency of various
methods in teaching the use of ventilation equipment and two-rescuer BLS.
BLS knowledge has also been relatively under-evaluated (Cason et al., 2009;
Creutzfeldt et al., 2010; Khan et al., 2010; Moule & Gilchrist, 2001; Moule, 2002; Moule
et al., 2008a; Reder et al., 2006; Teague & Riley, 2006; Todd et al., 1998, 1999 [see Table
2.8 and Table 2.9]). Very few of these studies have provided comparison of acquired
knowledge across two or more BLS training methods. Where training methods have been
compared, findings appear to indicate that acquisition of BLS knowledge is comparable
across the various methods of BLS training, with the potential for improved knowledge
with CD programs (Cason et al., 2009; Reder et al., 2006; Todd et al., 1998, 1999).
Further evaluation of BLS knowledge acquisition with the various training methods is
needed to determine methods which maximise participants‘ BLS knowledge.
Participant rating of the BLS program undertaken has been evaluated in a small
number of studies, particularly BLS CD studies (Moule & Gilchrist, 2001; Moule 2002;
Monsieurs et al., 2004). The feedback from participants who have trained using
Multimedia programs is positive to date (Moule & Gilchrist, 2001; Moule 2002;
Monsieurs et al., 2004; Shindo, Goto, Shibano, Okabe, & Inaoka, 2009). Further

Chapter 2 — Review of the Effectiveness of BLS Training Methods 75 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
evaluation of participants‘ perception of the various modes of BLS training is additionally
needed to aid understanding of the relative merits of all forms of BLS training.
A further point is that the studies discussed above have not been conducted in
Australia and have also not examined whether findings for novices can be translated to
those who have previously learnt the skills, and are re-accrediting in BLS. Re-
accreditation is required for most groups of health professionals. Digital BLS programs,
like BLS CDs, could be more suited to either beginners or to those reaccrediting in BLS.
Therefore, to comprehensively evaluate the effectiveness of BLS CD studies which
compare CD-based BLS training programs where a manikin is provided for independent
practice with Traditional approaches to BLS training, in groups of varying experience,
within the Australian experience are needed.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Chapter 3
Method
Aims
Primary aim.
The primary aim of this doctoral study was:
1. To compare the BLS skill of Novice and Practising Nurses who trained via a CD-
based (unsupervised practice) BLS training program or a Traditional
(presentation/demonstration/supervised practice) program. Outcome measures were
taken at one week and at two months post-training.
Secondary aims.
The secondary aims were:
1. To compare participants‘ knowledge of BLS at one week and at two months post-
training.
2. To compare participants‘ rating (in terms of satisfaction with training program
content, structure and assessment) of the CD and Traditional BLS training program
undertaken.
Hypothesis.
It was hypothesised that the CD-based BLS training program would result in a
higher rate of overall BLS skill competence and knowledge than would the Traditional
BLS instruction program among both Novice and Practising Nurses.
Research Design
The project undertaken was a quasi-experimental study which compared two modes
of BLS training in two cohorts: a Novice sample of 187 nursing students and an
experienced sample of 107 Practising Nurses undertaking reaccreditation. Engaging a
range of participant expertise from novice to practising professional was thought to

Chapter 3 — Method 77 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
promote relevance for the participant, assist participation and broaden the evaluation
capacity of the study. The two training groups were a BLS CD training program which
included a manikin for unsupervised practice and a Traditional BLS (presentation
demonstration/supervised practice) program. Participants within the two groups were
allocated to the two modes of training.
There was no pre-test, but two post-tests, one conducted one week after training to
determine skill and knowledge acquisition, and the second post-test conducted two
months after training to assess skill and knowledge retention. BLS skill competence was
determined using an assessor-graded BLS skills assessment form and automated manikin.
BLS knowledge was established through answers given to BLS knowledge questions
contained within a questionnaire. Participants‘ ratings of the CD and Traditional BLS
training program (content, structure, assessment, and overall quality and satisfaction)
were assessed via responses to a program evaluation form at one week post-training (see
Figure 3.1).
The post-test only comparative group research design of the project is similar to that
used in foundation BLS Video studies conducted by Braslow et al. (1997) and Todd et al.
(1998, 1999). This design was modelled on Campbell and Stanley‘s (1966) experimental
design number six (post–test only control group design), except the present design (and
the Braslow et al. 1997 study), did not use random allocation to groups. Additionally, the
present design incorporates a two month follow-up period to test for retention of
intervention effects. Design six was considered by Campbell and Stanley (1966) to be a
robust design with a high degree of internal validity.
The feasibility of including a pre-test into the design of this study was considered.
Pre-tests had not been routinely employed in the founding studies (Braslow et al., 1997;
Todd et al., 1998, 1999) nor in many of the studies that comprise the subsequent
comparative literature (Batcheller et al., 2000; Einspruch et al., 2007; Jones et al., 2007;
Lynch et al., 2005; Mancini et al., 2009; Roppolo et al., 2007). In the end, access
constraints and concern that this additional assessment would increase participant burden
and therefore could negatively impact on recruitment to the study led to the decision for a
pre-test not to be included in the research design.
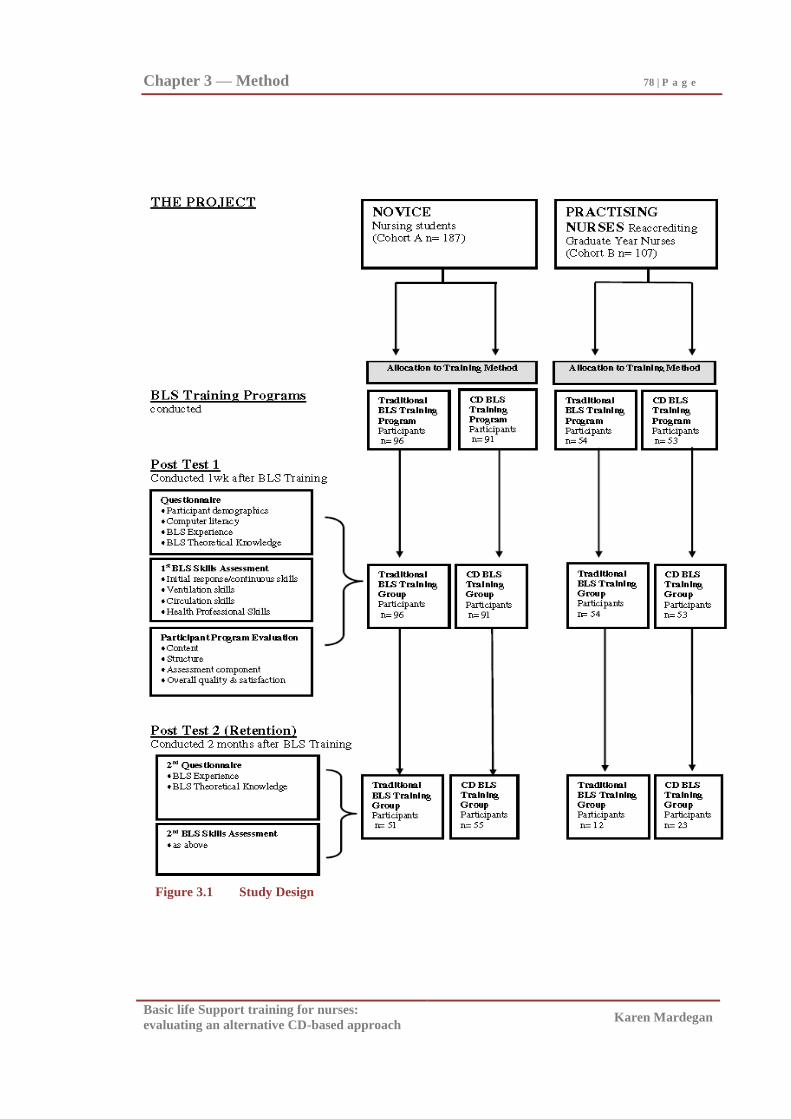
Chapter 3 — Method 78 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Figure 3.1 Study Design
Chapter 3 — Method 79 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
To test the adequacy of measures, a pilot feasibility study with a small sample of 20
novice nursing students was undertaken prior to commencing the doctoral study. The
pilot study results are described later in this chapter.
Setting.
The settings for the study were a large university which provides undergraduate
training in nursing (novice nursing student sample), and a large tertiary hospital
(reaccrediting graduate year nurse sample). The university was a multi-campus facility
with a Faculty of Health Sciences and School of Nursing where undergraduate through to
doctoral studies in nursing were offered. The hospital was a multi-campus tertiary health
service with an established reputation for teaching and research. These organisations
were deemed of sufficient size to accommodate the requirements of the study.
Sampling frame.
Three hundred and ten participants comprising 200 second year nursing students
and 110 graduate year nurses, were invited to participate in the study. In total, there were
two hundred and ninety four participants (94.8%). One hundred and eighty seven novice
nursing students comprised the Novice cohort, and 107 graduate nurses comprised the
Practising Nurses cohort (see Figure 3.1).
Participants
Recruitment of organisations.
When the design of the research program had been finalised, the Dean of the School
of Nursing from the university and the Director of Nursing and Ambulatory Services at
the hospital were approached. Permission to access participants and support for each
organisation‘s participation in the study was obtained (see Appendix A1 and Appendix A2).
As the BLS CD and BLS assessment form in the current study was the product of Austin
Health (Austin &Repatriation Medical Centre [A&RMC], 1999, 2000), permission from
the Director of Nursing and Patient Support Services at Austin Health to use these tools
was also obtained. Additionally, permission to use the questions from the Wilkinson and
Chu (1999) surveys was also granted at this time (see Appendix A3).
The research protocol of the study was then approved by the relevant Ethics
Committees of the two organisations participating in the study (Research & Graduate
Chapter 3 — Method 80 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Studies Human Research Ethics Committee of La Trobe University and the Austin Health
Human Research Ethics Committee respectively [see Appendix A1 and Appendix A2]).
The study commenced in January 2003 and was completed by December 2003.
Recruitment of participants.
Participants were approached as a group by the researcher during a scheduled
university or hospital class to participate in the study. Participation in the study included:
agreement to be allocated to a CD or Traditional instruction group, to undertake the BLS
training and to complete a questionnaire, BLS skills assessment and program evaluation
one week after the training (Post Test 1) and repeat completion of the questionnaire and
BLS skills assessment two months after the training (Post Test 2).
Once the requirements of participation were explained, and participants had an
opportunity to review the written information provided (see Appendix B1 and Appendix
B2), participants were formally invited to participate. Those who wished to take part
completed the study consent form (see Appendix B1 and Appendix B3).
Participant assignment.
A pragmatic method was used to allocate participants into the CD and Traditional
training groups. The student and graduate nurses had been arbitrarily allocated to class
groups on enrolment in their respective university and hospital programs. The co-
ordinators of the university and hospital programs randomly assigned equal numbers of
these previously determined groups to the CD-based BLS training and Traditional
(presentation /demonstration/practice) training methods. The training schedule was based
on the students‘ pre-existing university/hospital group allocations, the previously
scheduled group class timetable (which included BLS training) and the availability of the
computer lab (for CD viewing). Participant allocation to a BLS training method by the
university and hospital program co-ordinators ensured that the researcher, who assisted in
the BLS assessments, was unaware of which training method was used with which
participants.
Participant characteristics.
Two hundred and ninety four consenting second year nursing student and practising
nurses participated in the study (see Figure 3.1). From the 231 participants who
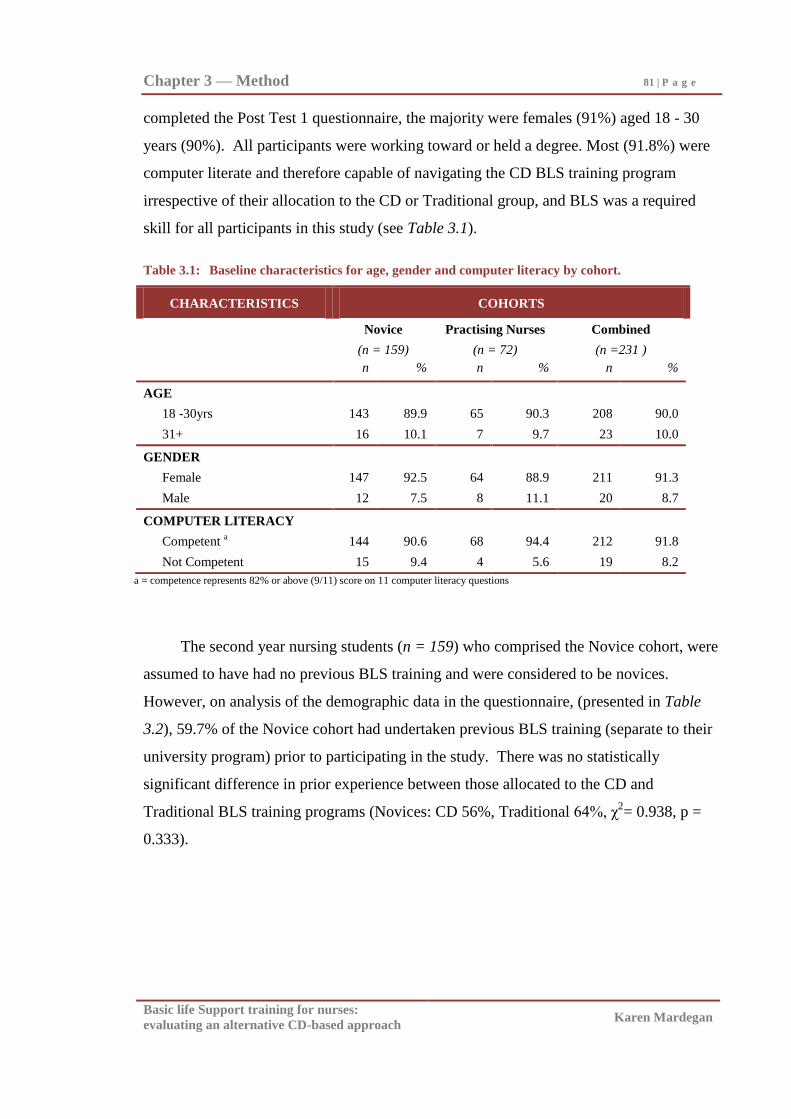
Chapter 3 — Method 81 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
completed the Post Test 1 questionnaire, the majority were females (91%) aged 18 - 30
years (90%). All participants were working toward or held a degree. Most (91.8%) were
computer literate and therefore capable of navigating the CD BLS training program
irrespective of their allocation to the CD or Traditional group, and BLS was a required
skill for all participants in this study (see Table 3.1).
Table 3.1: Baseline characteristics for age, gender and computer literacy by cohort.
CHARACTERISTICS COHORTS
Novice Practising Nurses Combined
(n = 159) (n = 72) (n =231 )
n % n % n %
AGE
18 -30yrs 143 89.9 65 90.3 208 90.0
31+ 16 10.1 7 9.7 23 10.0
GENDER
Female 147 92.5 64 88.9 211 91.3
Male 12 7.5 8 11.1 20 8.7
COMPUTER LITERACY
Competent a 144 90.6 68 94.4 212 91.8
Not Competent 15 9.4 4 5.6 19 8.2
a = competence represents 82% or above (9/11) score on 11 computer literacy questions
The second year nursing students (n = 159) who comprised the Novice cohort, were
assumed to have had no previous BLS training and were considered to be novices.
However, on analysis of the demographic data in the questionnaire, (presented in Table
3.2), 59.7% of the Novice cohort had undertaken previous BLS training (separate to their
university program) prior to participating in the study. There was no statistically
significant difference in prior experience between those allocated to the CD and
Traditional BLS training programs (Novices: CD 56%, Traditional 64%, χ2= 0.938, p =
0.333).
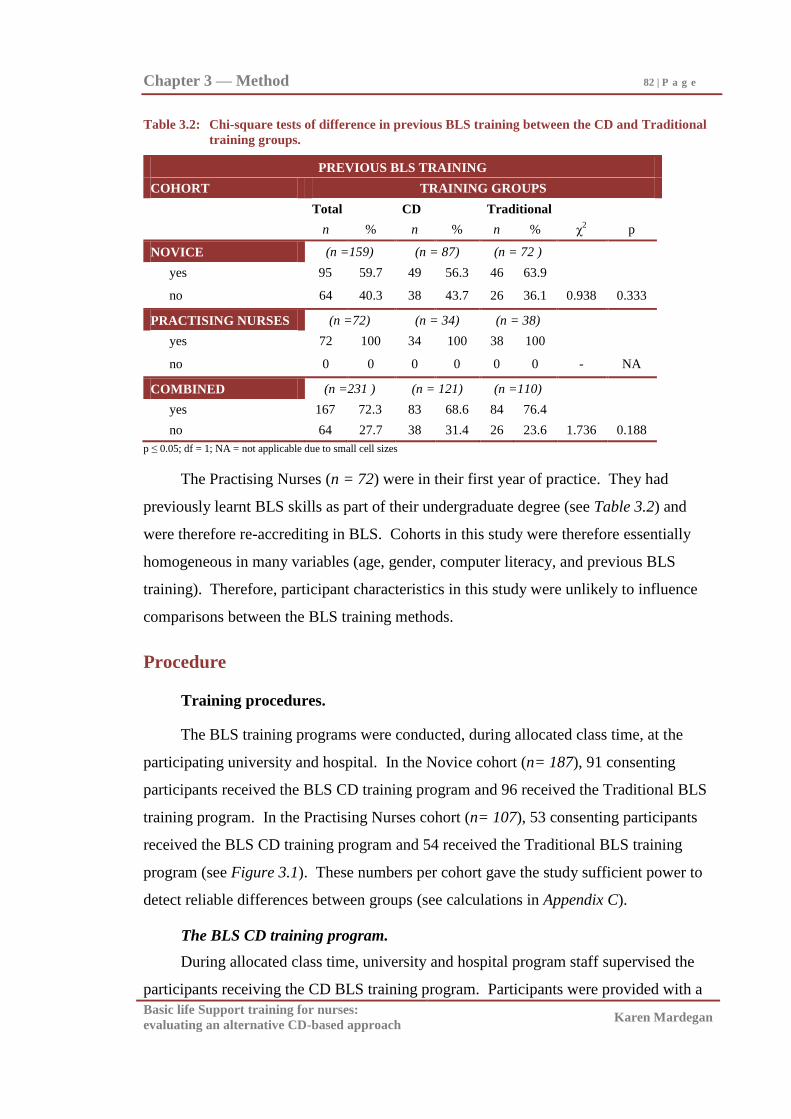
Chapter 3 — Method 82 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 3.2: Chi-square tests of difference in previous BLS training between the CD and Traditional
training groups.
PREVIOUS BLS TRAINING
COHORT TRAINING GROUPS
Total CD Traditional
n % n % n % χ2 p
NOVICE (n =159) (n = 87) (n = 72 )
yes 95 59.7 49 56.3 46 63.9
no 64 40.3 38 43.7 26 36.1 0.938 0.333
PRACTISING NURSES (n =72) (n = 34) (n = 38)
yes 72 100 34 100 38 100
no 0 0 0 0 0 0 - NA
COMBINED (n =231 ) (n = 121) (n =110)
yes 167 72.3 83 68.6 84 76.4
no 64 27.7 38 31.4 26 23.6 1.736 0.188
p ≤ 0.05; df = 1; NA = not applicable due to small cell sizes
The Practising Nurses (n = 72) were in their first year of practice. They had
previously learnt BLS skills as part of their undergraduate degree (see Table 3.2) and
were therefore re-accrediting in BLS. Cohorts in this study were therefore essentially
homogeneous in many variables (age, gender, computer literacy, and previous BLS
training). Therefore, participant characteristics in this study were unlikely to influence
comparisons between the BLS training methods.
Procedure
Training procedures.
The BLS training programs were conducted, during allocated class time, at the
participating university and hospital. In the Novice cohort (n= 187), 91 consenting
participants received the BLS CD training program and 96 received the Traditional BLS
training program. In the Practising Nurses cohort (n= 107), 53 consenting participants
received the BLS CD training program and 54 received the Traditional BLS training
program (see Figure 3.1). These numbers per cohort gave the study sufficient power to
detect reliable differences between groups (see calculations in Appendix C).
The BLS CD training program.
During allocated class time, university and hospital program staff supervised the
participants receiving the CD BLS training program. Participants were provided with a
Chapter 3 — Method 83 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
computer, the BLS CD (A&RMC, 1999) and a Laerdal Resusci Anne® manikin. The
only instruction given by the university/hospital supervising staff was to work through the
whole program practising on the manikin as they worked through each section of the CD.
Participants had the opportunity to view the CD while practising alone and in pairs (for
two-person BLS practice). Each participant documented the time spent in the training
room (Appendix G). No further access to the CD or manikin was permitted after the
training session, which ensured a controlled training time for the group.
The basic life support CD.
The BLS CD used in the study was developed in 1999 by Austin Health, a major
metropolitan hospital in Melbourne Australia. (The development team included the
current study‘s researcher, Karen Mardegan). The CD was an interactive multimedia
program which uses voice, text, animated graphic images and video in an integrated way
to provide viewers with the information traditionally covered in BLS training. The
content of the BLS CD Program was divided into nine main sections and topics. The nine
main sections covered were:
1. What is BLS?
2. What is an Emergency?
3. CPR;
4. Emergency Response Steps;
5. Anatomical Differences: infant/child/adult;
6. Emergencies in Health Care Settings;
7. Defibrillation;
8. Frequently Asked Questions; and
9. Self Check.
Although the program was suitable for the general population, the CD also covered
the broader issues required by health professionals when performing BLS, such as the use
of the one-way valve mask (e.g. concord mask), bag-mask device (e.g. air-viva),
defibrillation, and minijets for drug administration. The CD program was structured so
Chapter 3 — Method 84 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
that BLS beginners could complete each section in a recommended order. Viewers
wishing to revise specific topics could also move around quickly using the section map.
The two sections of CPR and Emergency Response Steps provided the complete
instruction on how to perform BLS. The later sections build on this knowledge by
introducing adjustments required for children and instruction on the equipment used by
health professionals.
In the CPR section of the CD program, viewers were trained in how to perform
CPR. This was achieved by a combination of text, and short video sequences with voice-
over to illustrate hand position, compression and ventilation techniques. This was
followed by a longer video sequence with voice-over which illustrates the technique of
CPR in its entirety. In the emergency response step section, viewers were then instructed
on the whole BLS sequence commencing with checking for Danger, then for Response,
Airway, Breathing and Circulation. The training of this information was also achieved by
a combination of text, diagrams and video sequences with voice-over.
The BLS CD was designed to teach the viewer BLS without manikin practice. It
therefore did not prompt the viewer to practise on a manikin while working through the
CD program. Practice has however been recommended in training design and delivery
and resuscitation practice literature (Aguinis & Kraiger, 2009; ARC & NZRC, 2010a;
Hazinski et al., 2010; Mancini et al., 2010; Salas & Cannon-Bowers, 2001). A number of
studies which have examined BLS instruction with and without manikin practice have
also found that when the opportunity for manikin practice was not provided as part of
BLS training programs, adequate BLS skill levels were not acquired (Choa et al., 2006;
Reder et al., 2006; Teague & Riley, 2006). Therefore, as it appears useful to provide
manikin practice in all forms of BLS training, this study‘s CD group had access to both
the CD and a BLS Laerdal Resusci Anne® manikin for unsupervised practice.
In contrast to Traditional BLS training, the CD program focused only on the critical
elements of BLS training for lay people and health professionals. Therefore, more time
for hands-on practice and performance of BLS skills was available. In Traditional
classroom courses trainees often share a manikin and have minimal practice time. With
the CD-based program a trainee can practise on their own manikin while working through
the CD and in pairs for two-person BLS practice.
Chapter 3 — Method 85 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Traditional BLS program.
The Traditional BLS program comprised the BLS teaching program used by the
respective participating organisations at the time of the data collection. These two
Traditional programs were therefore not standardised across the two cohorts and there
may have therefore been some instructor delivery differences from within each cohort and
across the cohorts. However, BLS certified instructors (from the participating university
and hospital) delivered the Traditional program during allotted class time. This ensured
that the researcher and supervisors of the research study had no involvement in the
delivery of the Traditional program. The training consisted of a BLS presentation and a
practical demonstration of BLS followed by instructor-supervised manikin practice. The
instructor outlined the emergency response steps, potential complications, health
professional responsibilities and the use of equipment (bag-mask device, one-way valve
mask, and artificial airway). The emergency response steps and the use of any equipment
were demonstrated by the instructor using a BLS Laerdal Resusci Anne® manikin.
Participants were then supervised practising BLS on a manikin. The participants in the
Traditional group were divided into groups of 8-10 participants per instructor. One
Laerdal Resusci Anne® manikin per 4-5 participants was available for the manikin
practice component of the program. Participants had the opportunity to practise both
alone and in pairs (for two-person BLS training).
CD and Traditional BLS program content and length.
All materials and apparatus used in the CD and Traditional programs were designed
to comply with the ARC guidelines at the time the study was conceptualised (ARC,
1997), not the most recently advocated changes to practice (ILCOR, 2000b, 2005;
Hazinski et al., 2010; Sayre et al., 2010). The BLS algorithm and compression-
ventilation ratio taught and assessed was DRABC with a ratio of 1:5 ventilation to
compressions for one operator and 2:15 for two operators (ARC, 1997; see Figure 3.2).
Practising health professionals are required to use one-way valve masks and bag-
mask devices, such as concord masks and air-vivas to administer the ventilation
component of BLS. Therefore, although many studies evaluate BLS programs using
mouth-to-mouth techniques, the training programs evaluated in this study assessed
participants‘ ability to perform BLS using the equipment required in practice by health
professionals.
Chapter 3 — Method 86 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The Novice cohort (cohort A) who were learning BLS for the first time received
two hours of BLS training time. The Practising Nurses (Cohort B) who were re-
accrediting in BLS, having some experience in BLS, received one hour of BLS training
time. These (one or two hour) training times were based on the length of the existing
Traditional programs at the two participating organisations.
Post Test procedures.
Two post tests were conducted at the participating university and hospital to
compare acquisition of BLS skills and knowledge and retention over two months. As
shown in Figure 3.1, Post Test 1, which was conducted one week after the completion of
the BLS skills training program, comprised:
1. Completion of the questionnaire (which contained participant demographic,
computer literacy, BLS experience and BLS knowledge questions),
immediately prior to the 1st BLS skills assessment.
2. Completion of the 1st assessor-conducted BLS skills assessment.
3. Completion of the program evaluation form immediately after the 1st BLS
skills assessment.
To assess BLS skills, each participant was invited into a room with a trained
assessor (who was blind to the training program completed by the participant), and a
Laerdal Skill Reporter™
Resusci Anne® manikin (Laerdal, 2002). The assessment
followed the standardised procedures used at Austin Health to assess BLS skills of health
professionals. Participants were asked to imagine that the manikin was a person who had
just collapsed, and to perform exactly as they would in real life. After one-person BLS
was demonstrated, the assessor joined the participant in two-person BLS. After two
minutes, participants were told to cease resuscitation efforts. The assessor graded each
individual BLS skill step as competent or not competent. After the assessor had
completed the skill assessment rating, the printed readout of CPR performance from the
automated manikin used in the assessment, was obtained.
Certified Austin Health BLS assessors conducted the BLS assessments in the post
tests. A minimum of four certified assessors (the researcher and three research assistants)
per cohort (therefore seven assessors in total) were necessary to ensure that the number of
Chapter 3 — Method 87 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
post test skill assessments could be completed within time and access constraints. To
ensure that the inter-rater reliability of the assessors participating in the current study was
suitable high, a proportion (17%) of BLS assessments were simultaneously assessed by
the researcher and assessors. These dual assessments were performed after the training
component of the programs, at the commencement of the post test assessments. The
respective course co-ordinators for each cohort assigned participants to an assessor based
on student availability. There was 100% agreement in the competent/not competent
rating and ordinal scale grading (1=not competent to 5 = outstanding competence) of the
dual assessments (see Appendix D). Assessor inter-rater reliability was therefore judged
to be suitably high.
One hundred and eighty seven consenting participants from the Novice cohort, (91
from the CD and 96 from the Traditional BLS training group), attended Post Test 1. One
hundred and seven consenting participants in the Practising Nurses cohort, (53 from the
CD and 54 from the Traditional BLS training groups), attended Post Test 1 (see Figure
3.1). There was a longer latency between training and Post Test 1 for the CD versus the
Traditional groups (Combined: CD Group M = 6.34 days, SD = 3.19; Traditional Group
M= 5.06, SD = 1.25) which was statistically significant (t(286) = 5.74, p < 0.001 [see
Appendix E]), however in practical terms the difference between five and seven days was
judged to be not so large as to impact on recall at the post-test assessments.
At Post Test 2, which was conducted two months after the completion of the BLS
skills training program, participants were required to:
1. Complete a shortened questionnaire (containing only the BLS experience and BLS
knowledge questions), immediately prior to the 2nd
BLS skills assessment.
2. Complete the 2nd
assessor conducted BLS skills assessment.
Based on feedback from the pilot study (presented later in this chapter), the
background questions which were essentially stable over time (demographics and
computer literacy sections), were removed from the questionnaire when administered at
Post Test 2 so as to reduce the time required to complete the questionnaire (see Appendix
F1 and Appendix F2). The BLS experience and knowledge sections of the questionnaire
were re-administered at Post Test 2 to track any changes in BLS experience and
knowledge over time.
Chapter 3 — Method 88 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Within the Novice cohort (n=106), 55 participants from the CD and 51 from the
Traditional BLS training group attended Post Test 2 (60% of CD and 53% of Traditional
Post Test 1 cohorts respectively). Within the Practising Nurses cohort (n= 35), only 23
from the CD and 12 from the Traditional BLS training groups attended Post Test 2 (43%
of CD and 22% of Traditional Post Test 1 cohorts respectively, see Figure 3.1). There
was no statistically significant difference in the number of days between training and Post
Test 2 for the CD and Traditional groups (Combined: CD M = 59.08 days, SD = 2.88,
Traditional M = 59.07 days, SD = 1.86, t(133) = 1.32, p > 0.180 [see Appendix E]).
Measures
There were four measurement tools used for the post tests. These were in order of
administration:
(a) BLS knowledge and participant characteristics were measured via a
questionnaire,
(b) Overall BLS skill competence was measured by an assessor using a BLS
assessment form,
(c) Specific CPR skills, were measured in conjunction with the assessor rating
using an automated manikin, and
(d) Program evaluation forms measured participants‘ rating of the BLS training
program undertaken (see Figure 3.1).
Questionnaire.
The questionnaire used in Post Test 1 and 2 has been included as Appendix H. It
was constructed by the researcher and contains four sections: demographic, computer
literacy, BLS experience and BLS knowledge. The demographic and computer literacy
sections of the questionnaire were drawn from the surveys designed by Wilkinson and
Chu (1999) for CD-based and face- to-face delivery of education. The questions in the
BLS experience and knowledge sections of the questionnaire were based on those in
founding BLS Video studies (Braslow et al., 1997; Todd et al., 1998, 1999) and the
content of the Traditional and CD programs in the current study. The resultant
questionnaire was a broadly focused tool aimed at capturing participant characteristics
Chapter 3 — Method 89 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
(age, gender, educational level, employment), computer literacy, BLS experience and
BLS knowledge.
Demographic and computer literacy sections of the questionnaire.
The demographic and computer literacy sections of the Wilkinson and Chu (1999)
surveys were the same for the CD-based and face-to-face program surveys. These
included six questions on the demographics of age, gender, highest educational level,
study status, current employment and employment type; three questions on current need
for BLS skills; and 15 questions on computer literacy issues such as access, frequency of
use and experience, and a single question on preferred education mode (face to face
lectures, paper based self-directed learning packages, packages on CD [see Appendix F1]).
The questions in the demographic and computer literacy sections of the
questionnaire which have been analysed and presented as part of the thesis are: the
question on Age group which was divided into five categories (18 - 20, 21 - 30, 31 - 40,
41 - 50, 51 and above years of age); and gender (male or female). Participants were
asked to tick the most appropriate box for both these questions (see Appendix F1).
The computer literacy questions (see Appendix F1) required participants to tick the
most appropriate box for: the frequency of computer use (not at all, occasionally [less
than once a week], once a week, variable number of times per week, once a day, all the
time); access to a computer at home and 11 computer usage experience questions
(yes/no). The computer usage questions were: computer experience, beginning
exploration of computers, can use one computer program for general purpose, can use one
computer program proficiently, can use two or more programs for general purpose, can
use two or more programs proficiently, can transfer data, can use internet for general
purpose, can use internet proficiently, can design computer applications and expertise in
computer application design. Responses to 11 computer usage experience questions were
summed to obtain an overall computer literacy score out of eleven (see Appendix F1).
The remaining demographic (and computer literacy sections of the questionnaire
questions), which were not analysed as part of this thesis, were either defined by the
recruitment process (i.e. education level, current studies/employment, and BLS required
for employment/studies), or did not identify any differences between the groups (i.e.
Chapter 3 — Method 90 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
whether they were living with a person at high risk of needing BLS, and performance of
BLS in an emergency).
BLS experience and knowledge sections of the questionnaire.
BLS experience questions.
The eight questions in the BLS experience section which have been analysed and
presented as part of the thesis include: previous BLS training (yes/no) response from
participants; and the BLS skill post training question which required participants to rate
their skill on a five point ordinal scale (very low, low, neutral, high and very high [see
Appendix F1]). These participant gradings were analysed to determine if there was
significant difference in participants‘ rating of their BLS skill post training.
The remaining questions in the BLS experience section of the questionnaire were
not presented as part of this thesis because they were not central to the aims of the current
study and did not identify any differences between the groups (i.e. performance of BLS in
an emergency during and after project, confidence to perform BLS in an emergency, and
practice prior to assessment). They are however available in Appendix F1.
BLS knowledge questions.
As the BLS knowledge questions in the Todd et al. (1998, 1999) studies were not
specified, therefore the six BLS knowledge questions were derived by the researcher
from the content covered in the Traditional and CD programs in the current study (see
Appendix D1). The content validity of the developed questions were supported by an
independent BLS training expert and the six BLS skill assessors who agreed that all
important areas of knowledge were addressed by the set of questions developed. The six
BLS knowledge questions were: the defining of respiratory and cardiac arrest, causes of
these, the potential complications of CPR and the most common drugs administered in
arrests (see Appendix F1). Participants were required to provide written answers to all six
BLS knowledge questions. These participant answers were matched against the correct
answer (see Appendix F3). Replies were graded as correct or incorrect by the researcher
and summed to give an overall BLS knowledge score out of six (see Appendix F3).
Internal consistency of the questionnaire.
No validity and reliability information was provided by Wilkinson and Chu (1999)
in respect to their surveys, so the internal consistency for the demographic and computer
Chapter 3 — Method 91 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
literacy questions was unknown. The Cronbach‘s alpha test of scale internal consistency
for the BLS experience questions was reported by the Todd team as α = 0.77 (Todd et al.,
1998). This suggests adequate internal consistency for the BLS experience questions.
Considering that the questionnaire was constructed from the tools used in other
studies (Braslow et al., 1997; Todd et al., 1998, 1999; Wilkinson & Chu, 1999) and that
these tools were not fully validated, it was deemed necessary to evaluate all the tools
compiled for the current project prior to embarking on the current study. To do so a pilot
feasibility study was conducted. Results from this pilot study are presented in the later
part of this chapter.
BLS assessment form.
The BLS skill assessment form used in the current study was the standard form used to
assess health professionals at Austin Health (A&RMC, 2000) at the time of the data
collection (see Figure 3.2). The broad categories of Danger, Response, Airway,
Breathing, and Circulation (DRABC) and the specific skills within these categories were
listed in the form. The BLS skill steps illustrated in the form were consistent with ARC
guidelines at the time of the data collection (ARC, 1997), and therefore similar to those
described in previous key studies in this area (Braslow et al., 1997; Brennan et al., 1996;
Todd et al., 1998, 1999), with the addition of extra health-professional-related skill steps,
e.g. features and demonstration of the use of the one-way valve mask (i.e. concord),
demonstration of use of the bag-mask device (i.e. air-viva), insertion of a guedel airway
(see Figure 3.2), which are the pieces of equipment required for health professional
practice in Australia.
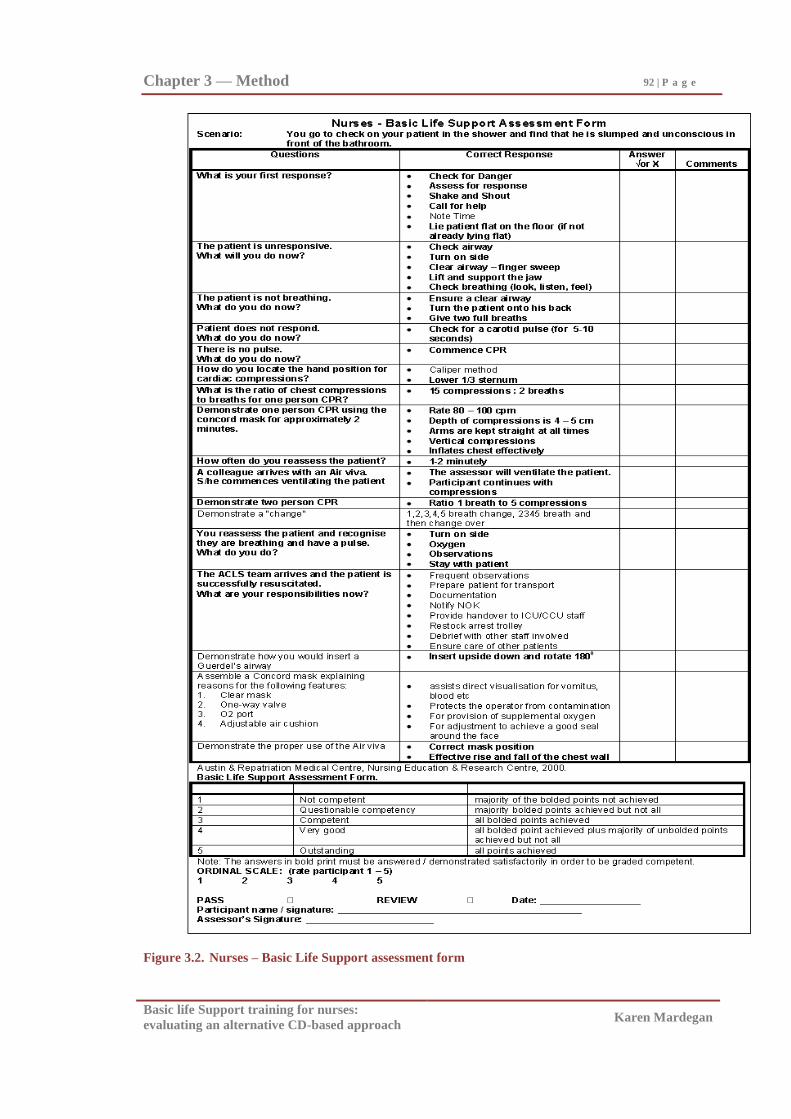
Chapter 3 — Method 92 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Figure 3.2. Nurses – Basic Life Support assessment form
Chapter 3 — Method 93 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The bolded skills in the assessment form were the skills considered mandatory for
competent performance of BLS (Austin & Repatriation Medical Centre [A&RMC], 2000;
see Figure 3.2). Non-mandatory (unbolded in Figure 3.2) skills were considered
desirable but not essential to the competent performance of BLS. Participants who
demonstrated all bolded (mandatory) skills correctly were graded by an assessor as
achieving overall BLS skill competence. Overall BLS skill competence was then rated on
a five point ordinal scale (5 outstanding = all bolded and all unbolded skills correct; 4
very good = all bolded skills and the majority of unbolded skills correct; 3 competent =
all bolded skills correct but not the majority of unbolded skills correct; 2 = questionable
competence = majority of bolded skills not achieved but the majority of unbolded skills
correct; 1 not competent = majority of bolded and majority of unbolded skills not correct).
This ordinal scale which replicated the grading scale in the Brennan et al. (1996) BLS
assessment tool, was added to the assessment form used in the current study by the
researcher to allow for a finer grading of overall competence. Participants who rated 3 or
above (therefore all mandatory skills correct) on this five point scale achieved overall
skill competence in the BLS skills assessment (see Figure 3.2).
Laerdal Skill Reporter™
Resusci Anne®.
The Laerdal Skill Reporter™
Resusci Anne® (automated) manikin was used as an
independent measure of CPR skills. It recorded the average frequency and depth of chest
compressions and the average frequency and volume of ventilation during CPR. In
addition the manikin also documented the compression/ventilation ratio and any improper
hand positioning during compressions i.e. wrong hand position, hand position too low and
incomplete release. A printed readout of (one-operator) CPR performance was obtained
from this automated manikin, after the assessor had completed the assessment rating on
the BLS assessment form.
Program evaluation forms.
Two program evaluation forms were compiled, one specifically for those who
undertook the Traditional BLS program and another form for those who undertook the
CD BLS training program. The program evaluation questions were drawn from the
Wilkinson and Chu (1999) staff education surveys for ―face to face‖ and ―CD-based‖
programs.
Chapter 3 — Method 94 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Questions common to both program evaluation forms.
The questions which were common to both the Traditional BLS program and CD
BLS program evaluation forms were questions on participant views about the program
content, structure, assessment component and overall quality and satisfaction (see
Appendix H).
The content section included eight questions relating to whether the content of the
respective programs was considered to be up-to-date, relevant, of an appropriate breadth,
and complexity, and that simulations and scenarios were useful. The structure section
contained six questions about the organisation and structure of the topics as well as the
sequencing of the information. Two questions relating to the overall quality and
participant satisfaction with the program and two questions related to the assessment
components (i.e. format and appropriateness of the practical assessment) were also asked
of both groups (see Appendix H). The questions in these sections of the evaluation forms
required a five point ordinal scale grading (strongly disagree, disagree, neutral, agree,
strongly agree) from participants, which was consistent with that used in comparable
studies (Moule et. al., 2001; Moule & Gilchrist, 2001; Moule, 2002). For some analyses,
the strongly agree/agree and disagree/strongly disagree/ neutral responses were grouped
into two categories, so that a dichotomous rating per question was able to be obtained (see
Appendix H).
Additional questions.
The Traditional and CD program evaluation forms each contained five additional
unique questions. For the Traditional program, evaluation form, the additional questions
were related to the content, pace and usefulness of the instructor-supervised manikin
practice (see Appendix H1). For the CD program, the additional questions related to the
adequacy of access and viewing time, comparison between CD and face to face program
quality and effectiveness, and the potential need for additional support with CD programs
(see Appendix H2). These additional questions in the program evaluation forms were not
central to the study aims because they did not enable comparison across training methods.
Therefore they were not reported in the current study, but are available in Appendix H.
Chapter 3 — Method 95 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Internal consistency of the program evaluation tools.
Cronbach‘s alpha test of scale internal consistency was calculated for the CD and
Traditional groups‘ program evaluation forms. Good internal consistency was
demonstrated (CD program evaluation form α = 0.905 and Traditional program evaluation
form α = 0.954, see Appendix H3). To assist further evaluation of all the tools compiled
for the current project, including the program evaluation forms, a pilot study (presented in
the later part of this chapter) was conducted prior to embarking on the main study.
Data Analysis
The data generated from this quantitative study were entered into a computer
database and then analysed using the Statistical Package for the Social Sciences (SPSS)
15.0 for Windows Graduate Pack. To reduce errors the data were entered twice and
compared. Using this approach, four errors in data entry were identified and corrected.
Data analysis was performed on the Traditional and CD group data within the
Novice cohort, Practising Nurses cohort, and the cohorts combined to provide a
comprehensive set of findings. Exploration of the data associated with the main study
variables indicated that the data generally was not normally distributed, and therefore it
was decided not to use the planned parametric tests for identifying group differences (t
test, F test). Consequently, the main analysis performed was to identify associations
between categorical variables using the chi-square test.
Sample size calculation and power analysis.
Sample size calculations for the study were determined by applying Cohen‘s
procedures (Cohen, 1988), and on the basis of being comparable to those used in similar
studies where statistically significant effects have been demonstrated (Braslow et al.,
1997; Todd et al., 1998, 1999). Sample size calculations were conducted based on a
power of 0.8 (Cohen, 1988) with an effect size of 0.6, and setting alpha at 0.05. This
corresponds to a total sample size of 88 for each cohort or 44 per group within cohorts.
To achieve 44 per group at the data analysis stage, it was necessary to recruit at least 50
per group initially (i.e. a total of at least 100 per cohort to allow for drop outs, unusable
data etc [see Appendix C]). These participant numbers were achieved on recruitment to
the study (see Figure 3.1). The effect size of 0.6 was based on the related studies at the
Chapter 3 — Method 96 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
time the project was planned (Batcheller et al., 2000; Braslow et al., 1997; Todd et al.,
1998, 1999) which found significant difference between training methods at comparative
sample sizes. More recent studies (Cason et al., 2009; Choa et al., 2006; Chung et al.,
2010; Isbye et al., 2006; Jones et al., 2007; Kardong-Edgren et al., 2010; Moule et al.,
2008a; Reder et al., 2006; Roppolo et al., 2007) have not been able to replicate this
statistical difference suggesting that the chosen effect size of 0.6 may in hindsight have
been too high, and the sample sizes needed to be greater.
Questionnaire.
The questionnaire responses for the two groups within each cohort were compared.
Frequencies, percentages and chi-square analyses were performed. This allowed for a test
of statistical difference for each question and each section of the questionnaire
(demographics, computer literacy, BLS experience, BLS knowledge sections). Analysis
of participants‘ age, gender, computer literacy, previous BLS training, and participant
rating of BLS skill post training, which was related to overall BLS skill, were analysed
because they were relevant to the key aims of this study.
Age group.
Age group was divided into categories and coded (1 = 18 - 20, 2 = 21 - 30, 3 = 31 -
40, 4 = 41 - 50, 5 = 51 and above years of age). Preliminary descriptive analysis was
performed, and age categories were collapsed to two groups, 18 - 30 and above 31 years
to produce more adequate cell sizes. These categories were compared by performing a
chi-square analysis to determine if there was significant difference in participants‘ age
between the groups, and cohorts.
Gender and previous BLS training.
The questions on gender (female/male) and previous BLS training responses were
coded 1 = yes and 0 = no (see Appendix F1). Frequencies, percentages and chi-square
analyses were performed to identify any significant difference between the training
groups for these measures.
Overall computer literacy.
To determine the overall level of computer literacy in the groups and any significant
differences between them an overall score was calculated from summing the 11 computer
usage experience questions (1= yes and 0 = no, see Appendix F1). Overall computer
Chapter 3 — Method 97 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
literacy was set at 82% (a score of 9/11 or above), reflecting generally proficient
computer skill. The last two questions on ability to design computer programs was an
advanced computer skill well above the level of computer literacy required to navigate the
CD BLS program (see Appendix F1). The scores were coded 1 = ≥ 9/11, 0 = ≤ 8/11, and
frequencies, percentages and chi-square analysis was performed to determine if there was
significant difference in computer literacy across the groups and cohorts.
Participants’ self-rating of BLS skill post training.
Participants‘ ratings (on an ordinal scale from very low to very high) of their BLS
skill post training (in the BLS experience section of the questionnaire) were analysed and
found to be not normally distributed, which prohibited parametric (t-test) analysis of
responses. Consequently responses were coded as 1 if participant‘s rated their skill as
very high or high and 0 if they rated their skill as very low, low or neutral. Frequencies,
percentages, and chi-square analyses were applied to these gradings to provide an
indication of program effectiveness, and determine if there were significant differences
between the CD and Traditional groups in participants‘ rating of their BLS skills post
training.
BLS Knowledge.
The BLS knowledge data and the BLS skill data have been analysed similarly.
Overall BLS knowledge.
The six BLS knowledge questions were graded as correct (coded 1) or incorrect
(coded 0). An overall score out of 6 was calculated. Participants were coded as 1
(adequate knowledge) if they scored 66% (4/6) or above and 0 (inadequate knowledge) if
they scored below 66%. To determine program effectiveness and identify any significant
difference in overall BLS knowledge between the CD and Traditional groups, chi-square
analyses on group frequencies were applied for Post Test 1 and Post Test 2, for each of
the Novice, Practising Nurses, and the Combined cohorts.
BLS knowledge of each question.
Frequencies, percentages, and chi-square tests were also calculated on the
correct/incorrect grading for each of the six BLS knowledge questions to identify any
significant differences between the groups and cohorts for each specific question. As
small cell sizes limited the ability to statistically analyse many BLS questions, only the
Chapter 3 — Method 98 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Combined Novice and Practising Nurses cohort results for each knowledge question were
presented in the results chapter. There was a potential for a type 1 error in the analysis of
the number of BLS knowledge questions. Bonferroni adjustment was therefore
calculated, and a consistent p value of 0.001 was applied.
Retention of BLS knowledge.
Retention of overall BLS knowledge was determined by coding each participant as
1 if their overall score at Post Test 2 was the same as or better than at Post Test 1, and 0 if
their overall score at Post Test 2 was below their Post Test 1 score. Percentages,
frequencies and chi-square analyses of difference were calculated for the Novice,
Practising nurses and the Combined cohorts to determine retention of overall BLS
knowledge and therefore an indication of program effectiveness.
Approximately 1% of questions in the questionnaire were not answered by
participants. There are a number of established techniques for managing missing
responses e.g. listwise deletion, pairwise deletion, mean imputation, full analysis (Pallant,
2007). As there are a number of possible explanations for a question not being answered
(e.g. answer unknown, question accidentally overlooked), and only a small number of
responses were missing in the questionnaire data, these missing responses were replaced
with the mean response for that question.
BLS skills assessment form.
Overall BLS skill competence.
The mandatory (bolded) skills in the BLS assessment form were analysed to
determine BLS skill competence. Firstly, an overall BLS skill score (out of a maximum
of 32 mandatory BLS skills) were calculated for each participant for Post Test 1 and Post
Test 2 from the assessor grading of each individual skill on the assessment form (coded 1
= competent, 0 = not competent). Overall BLS skill competence was set at 100%
performance on mandatory skills (a score of 32/32). To determine program effectiveness
and identify any significant difference for overall BLS skill competence between the CD
and Traditional groups‘ frequencies, and chi-square analyses were applied for Post Test 1
and Post Test 2 for the Novice, Practising Nurses and the Combined cohorts.
Chapter 3 — Method 99 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS skill categories and specific BLS skills.
Frequencies, percentages, and chi-square tests were also calculated on the
competent/not competent grading for each BLS skill within the BLS procedure. Both
mandatory and non-mandatory BLS skills were included in this analysis. The specific
skills were grouped under the headings of initial response steps, ventilation, circulation
and Health Professional skills. Where cell sizes allowed (> 5), overall frequencies, and
chi-square analyses were calculated to identify any significant differences between the
groups and cohorts for these skill categories and each specific skill. As small cell sizes
limited the ability to statistically analyse many of the skill categories and specific BLS
skill steps, only the Combined Novice and Practising Nurses cohort results for the BLS
skill categories and specific skills were presented. Bonferroni adjustment was calculated
to control for type 1 error in these measures and a p value of 0.001 was applied.
Retention of BLS skill level and competence.
Frequencies and chi-square analyses of difference were calculated for the Novice,
Practising Nurses and Combined cohorts, to determine retention of overall BLS skill level
and therefore an indication of program effectiveness.
To determine retention of overall BLS skill competence, those who were competent
at both Post Test 1 and Post Test 2, and those who were competent at Post Test 1 but not
competent at Post Test 2 were then compared by performing a chi-square analyses to
determine if there were significant differences in retention of overall BLS skill
competence over time. Those who were not competent at Post Test 1 (and consequently
received additional teaching) were excluded from the analysis of retention of skill
competence. Results are presented for each of the Novice, Practising Nurses and the
Combined cohorts. There were small cell sizes (< 5) in the retention data for the
Practising Nurses cohort, so retention results were interpreted with caution.
Laerdal Skill Reporter™
Resusci Anne® Printout.
Although it was the original intention to include the data received from the
automated manikin, it became apparent that a number of factors had compromised the
validity of this data. On many occasions the manikins did not consistently produce a
read-out or produced a read-out that did not correspond to the assessors‘ observations and
therefore implied inadequate sensitivity of the manikin. These limitations in the manikin
Chapter 3 — Method 100 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
data resulted in only a small amount of data being available for analysis which was not
convincingly representative of the population‘s CPR performance. On this basis it was
decided not to use this data in any of the analyses.
Program evaluation forms.
Participants‘ ratings of their BLS training program in the program evaluation form,
were found to be not normally distributed. This prohibited parametric (t-test) analysis of
responses. Consequently, for the questions that were common to both the CD and
Traditional program evaluation forms (i.e. content, structure, assessment and overall
quality and satisfaction questions), participants‘ ratings were coded as 1 if participants
strongly agreed/agreed and 0 if they strongly disagree/disagreed/neutral with these
questions. Each question, each group of questions, and replies overall were summed and
compared by performing chi-square analyses to determine significant differences in
participants‘ rating of their BLS training program between the groups and cohorts. As
some small cell sizes (< 5) limited the ability to statistically analyse many responses
(particularly the Practising Nurses cohort), only the Combined Novice and Practising
Nurses cohort replies for the specific and grouped questions were presented. Bonferroni
adjustment was applied to control for type 1 error in these measures and a p value of
0.001 was applied. Any unanswered questions (< 1%) were treated as missing responses
and replaced with the mean response, as previously described. The additional questions
in the program evaluation forms which were not common to both program evaluation
forms were not addressed in this study (see Appendix H).
Ethical Considerations
There was an ethical responsibility to ensure that participants met their respective
(university/hospital) program requirement and corresponding patient care requirement of
BLS accreditation. Those who chose to participate in the project met the university /
hospital program requirement of BLS accreditation by virtue of their study participation.
Those who chose not to participate in the study (Novices n = 13, Practising nurses n = 3)
completed the standard BLS training (Traditional method) and were assessed as per
program requirements along with study participants. Those in either instructional method
who were not competent at the BLS assessment in the week immediately following
Chapter 3 — Method 101 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
training (Post Test 1) were given further instruction using the Traditional method and
reassessed, to ensure that every participant demonstrated adequate BLS skills and met the
university/hospital program requirement. Record of participants‘ BLS competence was
provided to the university / hospital on successful completion of the BLS assessment.
These strategies ensured that withdrawal from the study at any time was possible without
fear of negative consequence. The additional strategies (i.e. coding of participant names,
secure data storage, and anonymity on publication) necessary to ensure maintenance of
participant confidentiality during and following completion of the study have been
outlined in Appendix A4.
Trialing of Materials
Prior to embarking on the main study, it was judged useful to conduct a pilot
feasibility study for a number of reasons. Firstly, BLS is a life saving skill and the
available literature on the effectiveness of CD BLS training programs is limited. If the
pilot study, demonstrated that the BLS CD training program was not able to produce
adequate BLS skills, then it would be unethical to embark on a larger scale study,
especially when those partaking in the study require this skill to safely perform their work
role.
Second, the questionnaire and program evaluations planned to be used in the study
were compiled primarily from surveys developed for a study proposed but not conducted
by Wilkinson and Chu (1999). The BLS assessment form which had been widely used to
assess staff at the participating hospital had not been previously used for research
purposes. The tools were therefore considered to be lacking validation. A pilot study
provided the opportunity to initially evaluate and validate test procedures and tools prior
to use in the main study.
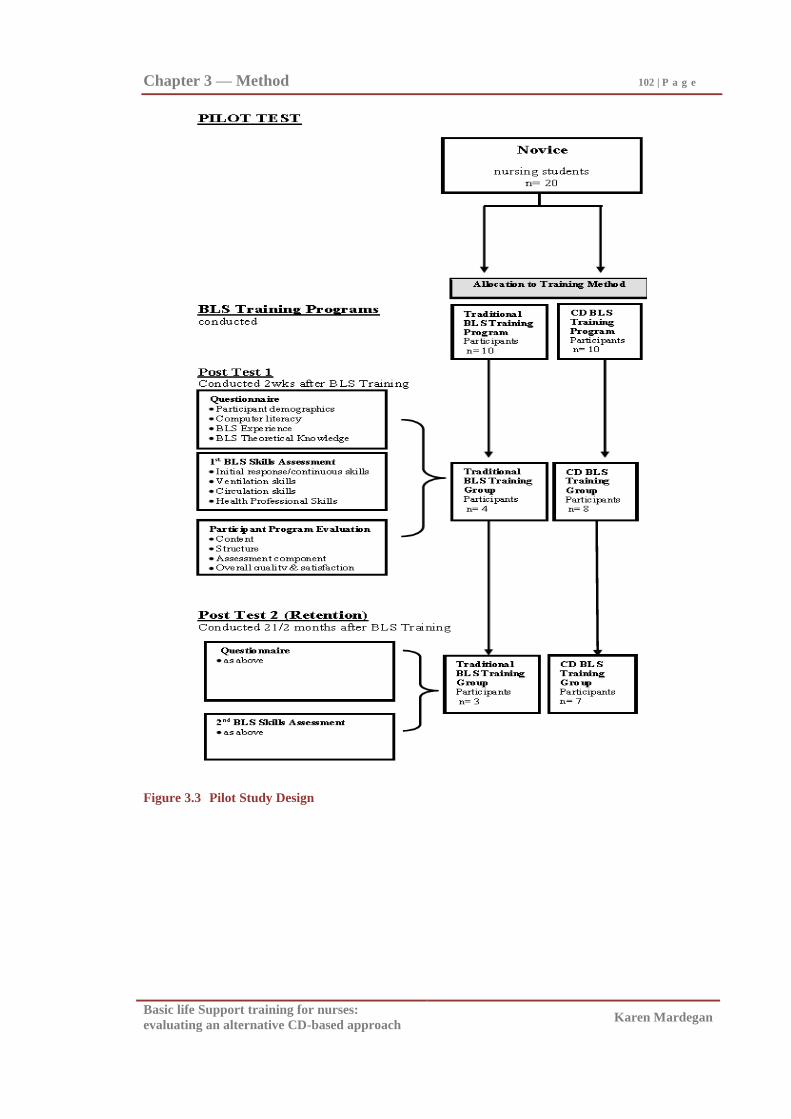
Chapter 3 — Method 102 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Figure 3.3 Pilot Study Design
Chapter 3 — Method 103 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Design of pilot study.
The pilot study compared two modes of BLS training in a small novice sample of
twenty nursing students, using a similar design and novice cohort as the main study.
There was no-pre-test, but two post-tests, one conducted two weeks after training, and the
second post-test conducted ten weeks after training. The two training groups were a BLS
CD training program which included a manikin for unsupervised practice and a
Traditional BLS (presentation demonstration/practice) program. Key outcome measures
were as planned for the main study. The research design of this pilot study, described
above, has been summarised in Figure 3.3. The pilot study procedures have been
outlined in Appendix I. It commenced in March 2002 and was completed by July 2002.
Pilot study results.
Measures.
The BLS assessment form, questionnaire and program evaluation questions used in
the pilot study were completed correctly and questions answered appropriately, which
implied that the forms were clear and understood by participants. Based on feedback
from the pilot study, the background questions (demographics and computer literacy
sections) in the questionnaire were removed when administered for the second time in the
main study, to reduce the time required to complete the questionnaire in the main study
(see Appendix F1 and Appendix F2). Removal of these questions in the Post Test 2
questionnaire in the main study was deemed reasonable because the information relevant
to these particular questions would not change over the short time period involved.
On analysis of the Laerdal Skill Reporter™
Resusci Anne® manikin recordings,
(which were taken in conjunction with the BLS assessors grading) of participant CPR
performance, many of the printouts were incomplete or produced results which appeared
incorrect, when compared with the human-assessor grading. This suggested that the skill
recording manikins were potentially inaccurate. However, the manikins used in the pilot
were the most sophisticated performance recording manikins available at the time of the
data collection. It was therefore decided that the manikins would still be used as planned
in the main study, despite these accuracy concerns having been raised.
Chapter 3 — Method 104 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS competence.
Twelve second year nursing students attended the pilot post test assessments (see
Figure 3.3). On testing of the training programs and assessment procedure, 75% of the
Pilot CD BLS group and 50.0% of the Pilot Traditional BLS group demonstrated
competent BLS skills at 2 weeks post training.
The degree of BLS skill competence of participants implies that both training
programs were potentially able to produce BLS skills in the majority of trainees. This
outcome was also comparable with the outcomes of other Traditional BLS training
programs which typically produced from 45% - 74% competent trainees (Gasco et al.,
2000; Kallestedt et al., 2010; Woollard et al., 2004). It therefore appeared feasible to
attempt to train nurses in BLS via a CD BLS training method, thus justifying
investigation of training technique differences via the planned larger main study.
Implications of the pilot study.
The pilot study provided information on the utility of the BLS training methods and
measures. It also provided an indication of the potential utility of CD BLS training.
When the CD BLS training method was evaluated in the 12 second year nursing students
who attended the pilot post test assessments, the small sample sizes precluded statistical
analysis. Nevertheless, overall judgments on the feasibility and required adjustments to
the proposed method, measures and training programs were possible from the pilot study.
Only minor adjustments to the planned procedure were required. Presentation of the
findings of the main study now follows.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Chapter 4
Results
The results from this study which evaluated a CD-based and Traditional BLS
training program in Novice and Practising Nurses will now be presented. The primary
aim of this study was to compare the BLS skill of Novice and Practising Nurses in the
two groups at one week and again at two months post training. The secondary aims were
to evaluate participants‘ BLS knowledge and participants‘ rating of the CD and
Traditional BLS training programs undertaken.
Therefore firstly, overall effectiveness of the BLS training (regardless of training
method), in Novice and Practising Nurses will be presented. Then the results from the
comparison of the CD and Traditional training in respect to BLS skill competence and
adequacy of BLS knowledge at one week, and two months, post training are presented.
This is followed by the presentation of skill and knowledge retention results, and
participants‘ self-rating of their BLS skill post training. Finally are presented the
participants‘ evaluative rating of the CD and Traditional training programs. As the main
statistical test used in the results following was a non-parametric one (chi-square test),
descriptive statistics for each group‘s scores on the main study variables are not presented
here but are included in Appendix J.
The Effectiveness of the BLS Training for Novice and Practising Nurses
Firstly, to gain an understanding of the effectiveness of BLS training by experience
level, the percentage competent in terms of adequate BLS skill and knowledge for the
Novice, Practising Nurses and Combined cohorts are described in Table 4.1. When
applying the skill mastery and program effectiveness standard of at least 80% competence
following training (Fabius et al., 1994; Frieson & Stotts, 1984; Marzooq & Lyneham,
2009; Morrison et. al.,1996; Wayne et al., 2005, 2006), the low BLS skill and knowledge
competency rates presented in Table 4.1 illustrate overall low training effectiveness and
poor retention.
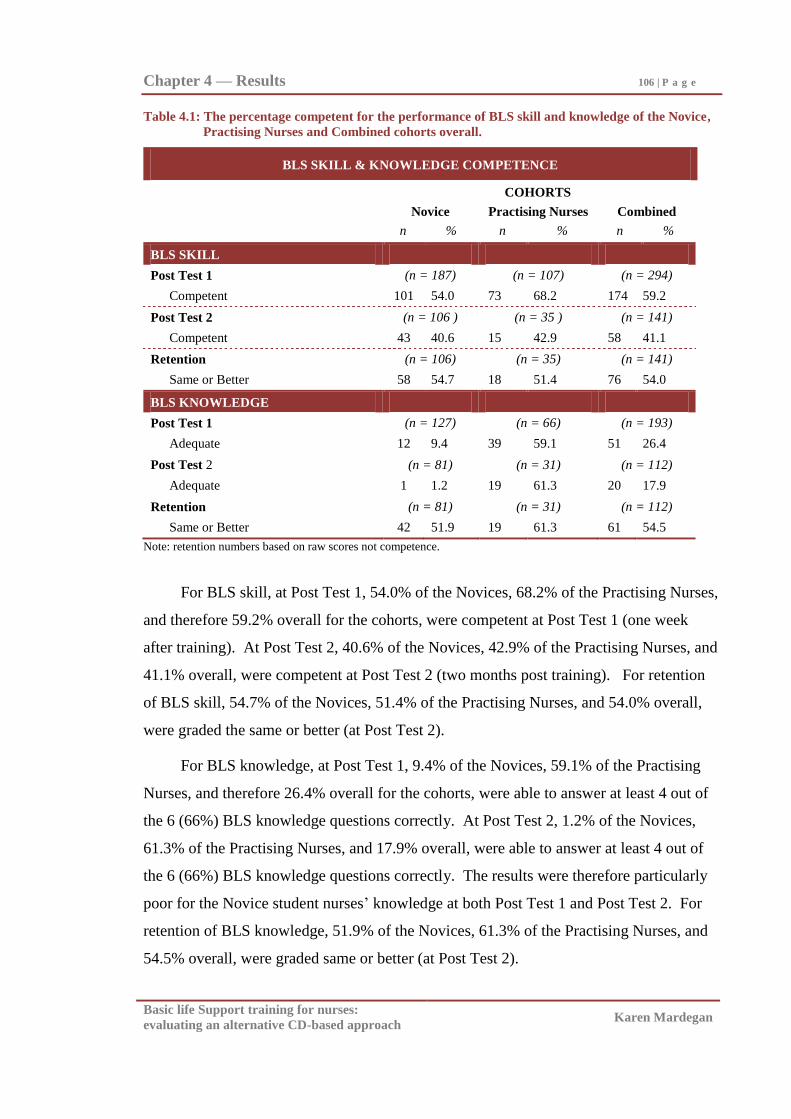
Chapter 4 — Results 106 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.1: The percentage competent for the performance of BLS skill and knowledge of the Novice,
Practising Nurses and Combined cohorts overall.
BLS SKILL & KNOWLEDGE COMPETENCE
COHORTS
Novice Practising Nurses Combined
n % n % n %
BLS SKILL
Post Test 1 (n = 187) (n = 107) (n = 294)
Competent 101 54.0 73 68.2 174 59.2
Post Test 2 (n = 106 ) (n = 35 ) (n = 141)
Competent 43 40.6 15 42.9 58 41.1
Retention (n = 106) (n = 35) (n = 141)
Same or Better 58 54.7 18 51.4 76 54.0
BLS KNOWLEDGE
Post Test 1 (n = 127) (n = 66) (n = 193)
Adequate 12 9.4 39 59.1 51 26.4
Post Test 2 (n = 81) (n = 31) (n = 112)
Adequate 1 1.2 19 61.3 20 17.9
Retention (n = 81) (n = 31) (n = 112)
Same or Better 42 51.9 19 61.3 61 54.5
Note: retention numbers based on raw scores not competence.
For BLS skill, at Post Test 1, 54.0% of the Novices, 68.2% of the Practising Nurses,
and therefore 59.2% overall for the cohorts, were competent at Post Test 1 (one week
after training). At Post Test 2, 40.6% of the Novices, 42.9% of the Practising Nurses, and
41.1% overall, were competent at Post Test 2 (two months post training). For retention
of BLS skill, 54.7% of the Novices, 51.4% of the Practising Nurses, and 54.0% overall,
were graded the same or better (at Post Test 2).
For BLS knowledge, at Post Test 1, 9.4% of the Novices, 59.1% of the Practising
Nurses, and therefore 26.4% overall for the cohorts, were able to answer at least 4 out of
the 6 (66%) BLS knowledge questions correctly. At Post Test 2, 1.2% of the Novices,
61.3% of the Practising Nurses, and 17.9% overall, were able to answer at least 4 out of
the 6 (66%) BLS knowledge questions correctly. The results were therefore particularly
poor for the Novice student nurses‘ knowledge at both Post Test 1 and Post Test 2. For
retention of BLS knowledge, 51.9% of the Novices, 61.3% of the Practising Nurses, and
54.5% overall, were graded same or better (at Post Test 2).
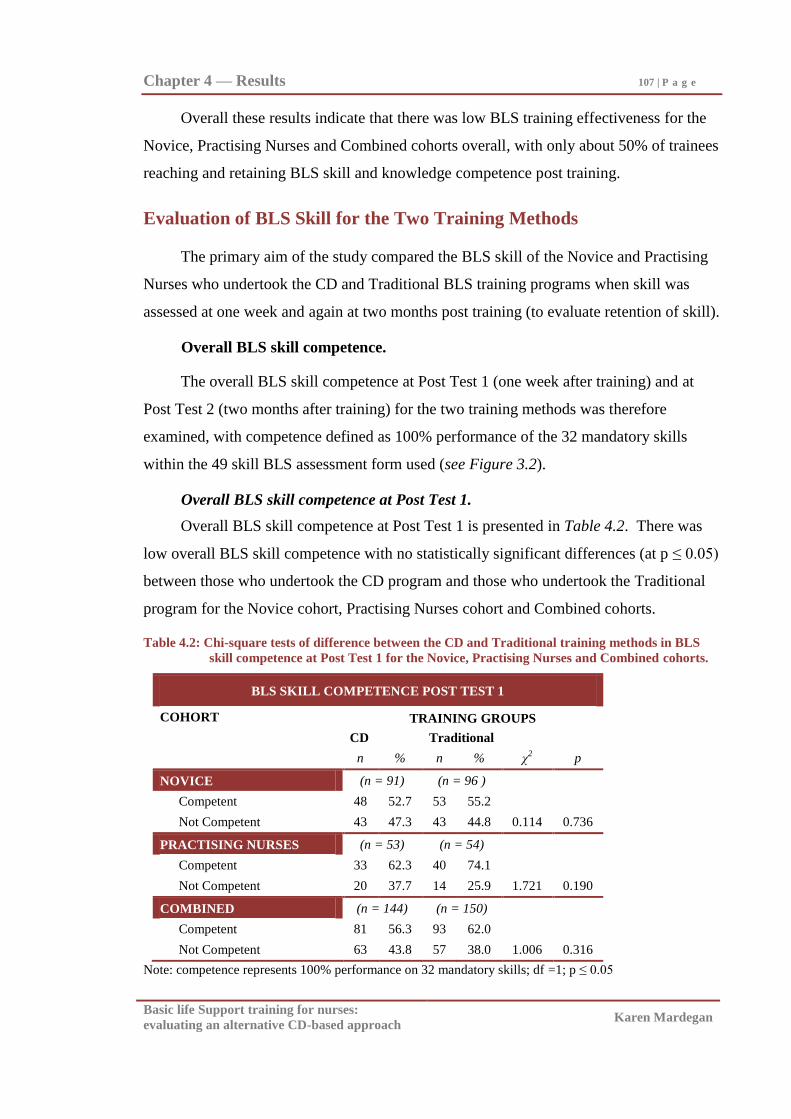
Chapter 4 — Results 107 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Overall these results indicate that there was low BLS training effectiveness for the
Novice, Practising Nurses and Combined cohorts overall, with only about 50% of trainees
reaching and retaining BLS skill and knowledge competence post training.
Evaluation of BLS Skill for the Two Training Methods
The primary aim of the study compared the BLS skill of the Novice and Practising
Nurses who undertook the CD and Traditional BLS training programs when skill was
assessed at one week and again at two months post training (to evaluate retention of skill).
Overall BLS skill competence.
The overall BLS skill competence at Post Test 1 (one week after training) and at
Post Test 2 (two months after training) for the two training methods was therefore
examined, with competence defined as 100% performance of the 32 mandatory skills
within the 49 skill BLS assessment form used (see Figure 3.2).
Overall BLS skill competence at Post Test 1.
Overall BLS skill competence at Post Test 1 is presented in Table 4.2. There was
low overall BLS skill competence with no statistically significant differences (at p ≤ 0.05)
between those who undertook the CD program and those who undertook the Traditional
program for the Novice cohort, Practising Nurses cohort and Combined cohorts.
Table 4.2: Chi-square tests of difference between the CD and Traditional training methods in BLS
skill competence at Post Test 1 for the Novice, Practising Nurses and Combined cohorts.
BLS SKILL COMPETENCE POST TEST 1
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 91) (n = 96 )
Competent 48 52.7 53 55.2
Not Competent 43 47.3 43 44.8 0.114 0.736
PRACTISING NURSES (n = 53) (n = 54)
Competent 33 62.3 40 74.1
Not Competent 20 37.7 14 25.9 1.721 0.190
COMBINED (n = 144) (n = 150)
Competent 81 56.3 93 62.0
Not Competent 63 43.8 57 38.0 1.006 0.316
Note: competence represents 100% performance on 32 mandatory skills; df =1; p ≤ 0.05
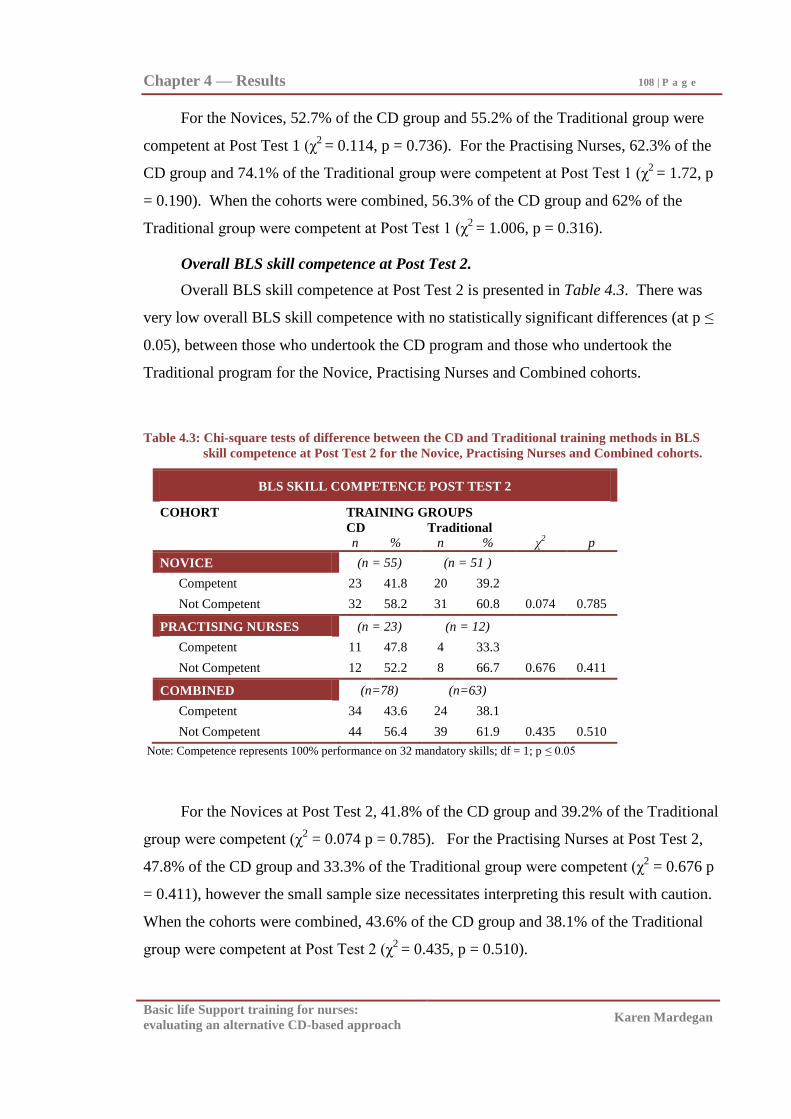
Chapter 4 — Results 108 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
For the Novices, 52.7% of the CD group and 55.2% of the Traditional group were
competent at Post Test 1 (χ2
= 0.114, p = 0.736). For the Practising Nurses, 62.3% of the
CD group and 74.1% of the Traditional group were competent at Post Test 1 (χ2
= 1.72, p
= 0.190). When the cohorts were combined, 56.3% of the CD group and 62% of the
Traditional group were competent at Post Test 1 (χ2
= 1.006, p = 0.316).
Overall BLS skill competence at Post Test 2.
Overall BLS skill competence at Post Test 2 is presented in Table 4.3. There was
very low overall BLS skill competence with no statistically significant differences (at p ≤
0.05), between those who undertook the CD program and those who undertook the
Traditional program for the Novice, Practising Nurses and Combined cohorts.
Table 4.3: Chi-square tests of difference between the CD and Traditional training methods in BLS
skill competence at Post Test 2 for the Novice, Practising Nurses and Combined cohorts.
BLS SKILL COMPETENCE POST TEST 2
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 55) (n = 51 )
Competent 23 41.8 20 39.2
Not Competent 32 58.2 31 60.8 0.074 0.785
PRACTISING NURSES (n = 23) (n = 12)
Competent 11 47.8 4 33.3
Not Competent 12 52.2 8 66.7 0.676 0.411
COMBINED (n=78) (n=63)
Competent 34 43.6 24 38.1
Not Competent 44 56.4 39 61.9 0.435 0.510
Note: Competence represents 100% performance on 32 mandatory skills; df = 1; p ≤ 0.05
For the Novices at Post Test 2, 41.8% of the CD group and 39.2% of the Traditional
group were competent (χ2 = 0.074 p = 0.785). For the Practising Nurses at Post Test 2,
47.8% of the CD group and 33.3% of the Traditional group were competent (χ2 = 0.676 p
= 0.411), however the small sample size necessitates interpreting this result with caution.
When the cohorts were combined, 43.6% of the CD group and 38.1% of the Traditional
group were competent at Post Test 2 (χ2
= 0.435, p = 0.510).
Chapter 4 — Results 109 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Evaluation of competence in BLS skill categories and specific BLS skills.
Each of the specific 32 mandatory and 17 non-mandatory skills within the BLS
procedure were then grouped into initial response skills, ventilation skills, circulation
skills and health professional skills. Competence for these skill categories were the sum
of the correct performance of each specific skill within each category. The results of the
combined cohort of Novices and Practising nurses for the mandatory and non-mandatory
skills within these four skill categories and each specific skill within these categories at
Post Test 1 and Post Test 2 are presented next for the training groups. (Small cell counts
in the Practising Nurses cohort prohibited statistical analysis and therefore presentation of
the cohorts separately).
Competence in BLS skill categories at Post Test 1.
Competence in the four BLS skill categories at Post Test 1 are presented in Table
4.4. A higher proportion of the sample achieved competence for the skill categories, than
seen in the overall BLS competency scores (Table 4.2), due to both mandatory and non-
mandatory scores being combined to form these categories. However, once again no
statistically significant differences were found at p ≤ 0.001, between those who undertook
the CD program and those who undertook the Traditional program in any of the four BLS
skill categories and overall at Post Test 1 for the Combined Novice and Practising Nurses
cohort.
For initial response skills, when the Novice and Practising Nurses were combined,
92.4% of the CD group and 94.7% of the Traditional group were competent at Post Test 1
(χ2
= 0.646, p = 0.422). For ventilation skills, 94.4% of the CD group and 95.3% of the
Traditional group were competent at Post Test 1 (χ2
= 0.120, p = 0.729). For circulation
skills, 93.1% of the CD group and 95.3% of the Traditional group were competent at Post
Test 1 (χ2
= 0.700, p = 0.403). For Health Professional skills, 79.2% of the CD group and
78.7% of the Traditional group were competent at Post Test 1 (χ2
= 0.011, p = 0.916).
Overall for these four BLS skill categories, 89.6% of the CD group and 90.7% of the
Traditional group were competent at Post Test 1 (χ2
= 0.097, p = 0.755 [see Table 4.4]).
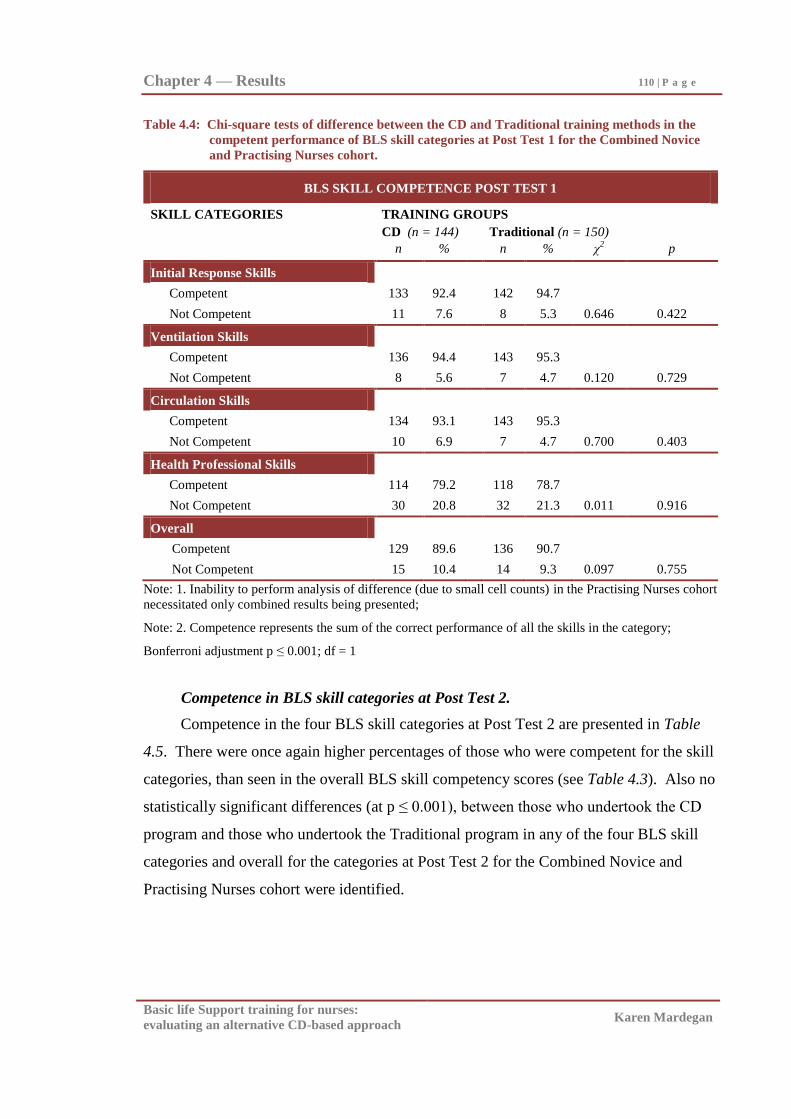
Chapter 4 — Results 110 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.4: Chi-square tests of difference between the CD and Traditional training methods in the
competent performance of BLS skill categories at Post Test 1 for the Combined Novice
and Practising Nurses cohort.
BLS SKILL COMPETENCE POST TEST 1
SKILL CATEGORIES TRAINING GROUPS
CD (n = 144) Traditional (n = 150)
n % n % χ2 p
Initial Response Skills
Competent 133 92.4 142 94.7
Not Competent 11 7.6 8 5.3 0.646 0.422
Ventilation Skills
Competent 136 94.4 143 95.3
Not Competent 8 5.6 7 4.7 0.120 0.729
Circulation Skills
Competent 134 93.1 143 95.3
Not Competent 10 6.9 7 4.7 0.700 0.403
Health Professional Skills
Competent 114 79.2 118 78.7
Not Competent 30 20.8 32 21.3 0.011 0.916
Overall
Competent 129 89.6 136 90.7
Not Competent 15 10.4 14 9.3 0.097 0.755
Note: 1. Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort
necessitated only combined results being presented;
Note: 2. Competence represents the sum of the correct performance of all the skills in the category;
Bonferroni adjustment p ≤ 0.001; df = 1
Competence in BLS skill categories at Post Test 2.
Competence in the four BLS skill categories at Post Test 2 are presented in Table
4.5. There were once again higher percentages of those who were competent for the skill
categories, than seen in the overall BLS skill competency scores (see Table 4.3). Also no
statistically significant differences (at p ≤ 0.001), between those who undertook the CD
program and those who undertook the Traditional program in any of the four BLS skill
categories and overall for the categories at Post Test 2 for the Combined Novice and
Practising Nurses cohort were identified.
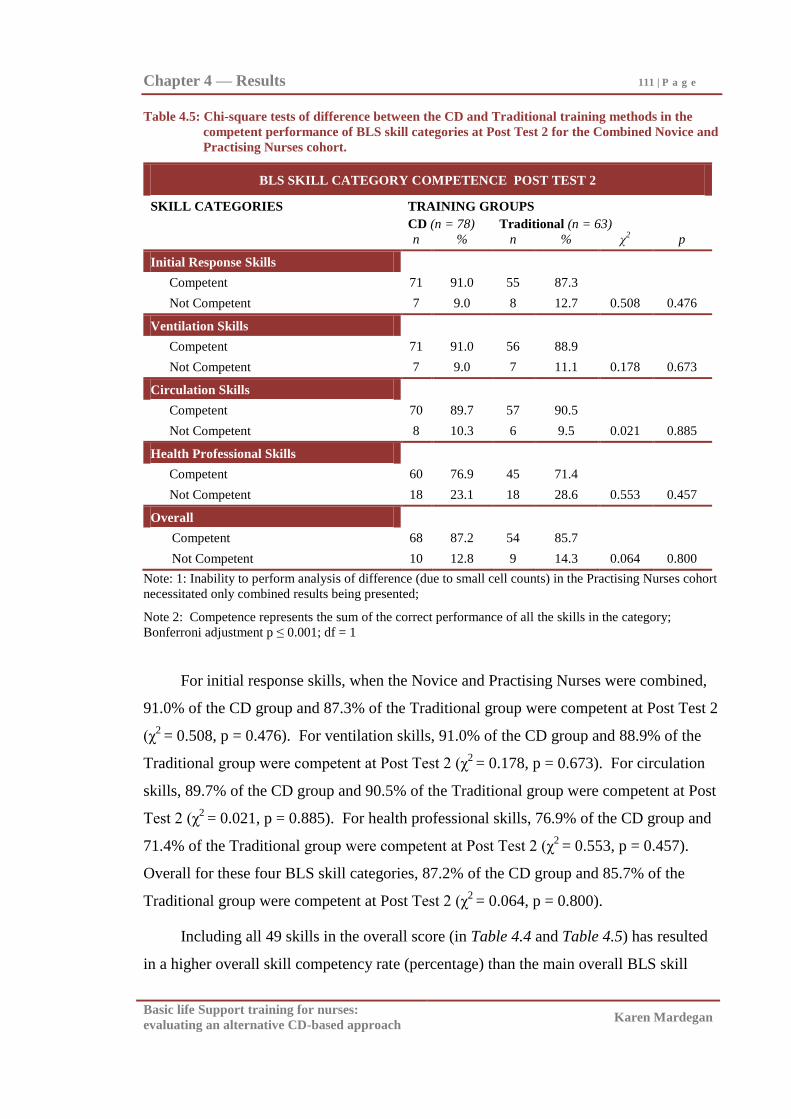
Chapter 4 — Results 111 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.5: Chi-square tests of difference between the CD and Traditional training methods in the
competent performance of BLS skill categories at Post Test 2 for the Combined Novice and
Practising Nurses cohort.
BLS SKILL CATEGORY COMPETENCE POST TEST 2
SKILL CATEGORIES TRAINING GROUPS
CD (n = 78) Traditional (n = 63)
n % n % χ2 p
Initial Response Skills
Competent 71 91.0 55 87.3
Not Competent 7 9.0 8 12.7 0.508 0.476
Ventilation Skills
Competent 71 91.0 56 88.9
Not Competent 7 9.0 7 11.1 0.178 0.673
Circulation Skills
Competent 70 89.7 57 90.5
Not Competent 8 10.3 6 9.5 0.021 0.885
Health Professional Skills
Competent 60 76.9 45 71.4
Not Competent 18 23.1 18 28.6 0.553 0.457
Overall
Competent 68 87.2 54 85.7
Not Competent 10 12.8 9 14.3 0.064 0.800
Note: 1: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort
necessitated only combined results being presented;
Note 2: Competence represents the sum of the correct performance of all the skills in the category;
Bonferroni adjustment p ≤ 0.001; df = 1
For initial response skills, when the Novice and Practising Nurses were combined,
91.0% of the CD group and 87.3% of the Traditional group were competent at Post Test 2
(χ2
= 0.508, p = 0.476). For ventilation skills, 91.0% of the CD group and 88.9% of the
Traditional group were competent at Post Test 2 (χ2
= 0.178, p = 0.673). For circulation
skills, 89.7% of the CD group and 90.5% of the Traditional group were competent at Post
Test 2 (χ2
= 0.021, p = 0.885). For health professional skills, 76.9% of the CD group and
71.4% of the Traditional group were competent at Post Test 2 (χ2
= 0.553, p = 0.457).
Overall for these four BLS skill categories, 87.2% of the CD group and 85.7% of the
Traditional group were competent at Post Test 2 (χ2
= 0.064, p = 0.800).
Including all 49 skills in the overall score (in Table 4.4 and Table 4.5) has resulted
in a higher overall skill competency rate (percentage) than the main overall BLS skill
Chapter 4 — Results 112 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
competence results presented in Table 4.2 and Table 4.3. This is explained by only
mandatory skills being included in the study‘s main overall skill competency results
(presented in Table 4.2 and Table 4.3). Both approaches to analysis of the data have
demonstrated no overall significant differences in BLS skill competence between the
groups (see Table 4.2, Table 4.3, Table 4.4, and Table 4.5).
Specific BLS Skills Competence at Post Test 1 and Post Test 2.
Every specific skill within each of the four BLS skill categories was also examined.
Results are presented in Appendix K. There were generally higher competency ratings for
most of the specific skills, than seen in the overall BLS competency scores (see Table 4.2
and Table 4.3), due to the lack of consistency across participants in the skill errors made,
and very few statistically significant differences (at p ≤ 0.001), in the performance of
specific skills within these four BLS categories between the two groups at Post Test 1 and
Post Test 2 (see Appendix K).
For the Combined Novice and Practising Nurses, there was no statistically
significant difference between the CD and Traditional groups in the majority of specific
initial response skills, ventilation skills, circulation skills, and health professional skills at
Post Test 1 and Post Test 2 (see Appendix K). Generally, specific skill competency
ranged from 80% to 100% correct performance for the Cohorts (see Appendix K).
However, the specific skills of noting the time, and post arrest management
responsibilities (within the Health Professional skill category, [see Table K4.1 and Table
K4.2]) were lower than skill mastery standards (80%) for the Cohorts.
The skill of calling for help (within the initial response skill category) was
performed in the Combined Novice and Practising Nurses statistically significantly more
correctly by the Traditional group in Post Test 1. This statistically significant difference
in the group‘s ability to call for help was not evident at Post Test 2. Furthermore,
competent performance of this skill was also below skill mastery standards for the
Cohorts (see Table K4.1, and Table K4.2).
Additionally, the skill of correctly using a bag-mask device (within the health
professionals skill category) was performed, in the Combined Novice and Practising
nurses, statistically significantly more correctly by the CD group in Post Test 2. This
statistically significant difference in the group‘s ability to correctly use a bag-mask device
Chapter 4 — Results 113 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
also approached statistical significance (p = 0.003) at Post Test 1 suggesting that the CD
group were more competent at using a bag-mask device (see Table K4.1, and Table K4.2).
Competent performance of this skill was within skill mastery standards (80%) for the
Cohorts (see Table K4.1, and Table K4.2).
Retention of BLS skill level and BLS skill competence.
Retention of BLS skill was examined by determining both the retention of BLS skill
level (overall score out of the 32 mandatory skills at Post Test 2 being the same or better
than at Post Test1), and the retention of skill competence (100% performance on
mandatory skills at both Post Test 1 and Post Test 2). Results for the retention of BLS
skill level and skill competence are presented in Table 4.6 and Table 4.7. There was low
retention of overall BLS skill level and low retention of overall skill competence with no
statistically significant differences, (at p ≤ 0.05), between those who undertook the CD
program and those who undertook the Traditional program for the Novice, Practising
Nurses and Combined cohorts.
Retention of BLS skill level.
In Table 4.6, for the Novices who attended both Post Tests, 58.2% of the CD group
and 51.0% of the Traditional group retained their overall skill level at Post Test 2 (χ2 =
0.554, p = 0.457). For the Practising Nurses who attended both Post Tests, 52.2% of the
CD group and 50.0% of the Traditional group retained their overall skill level at Post Test
2 (χ2 = 0.015, p = 0.903). When the cohorts were combined, 56.4% of the CD group and
50.8% of the Traditional group retained their overall skill level at Post Test 2, with no
statistically significant difference between the training groups (χ2
= 0.442, p = 0.506).
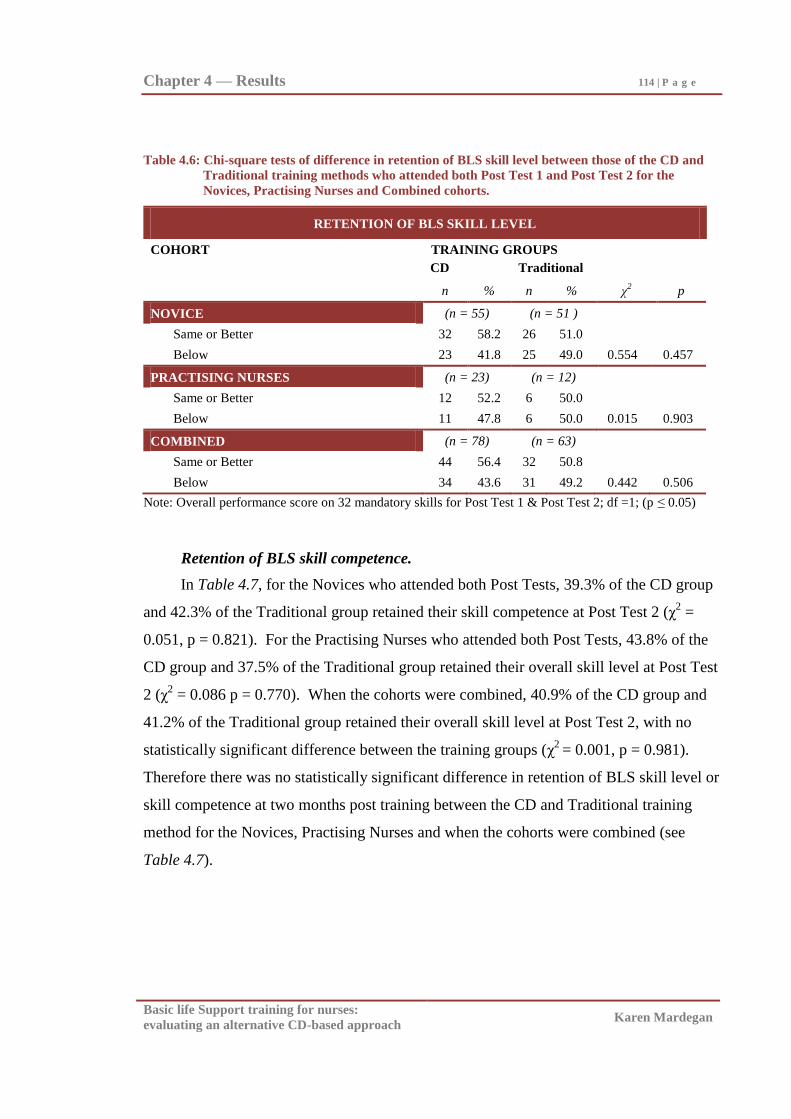
Chapter 4 — Results 114 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.6: Chi-square tests of difference in retention of BLS skill level between those of the CD and
Traditional training methods who attended both Post Test 1 and Post Test 2 for the
Novices, Practising Nurses and Combined cohorts.
RETENTION OF BLS SKILL LEVEL
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 55) (n = 51 )
Same or Better 32 58.2 26 51.0
Below 23 41.8 25 49.0 0.554 0.457
PRACTISING NURSES (n = 23) (n = 12)
Same or Better 12 52.2 6 50.0
Below 11 47.8 6 50.0 0.015 0.903
COMBINED (n = 78) (n = 63)
Same or Better 44 56.4 32 50.8
Below 34 43.6 31 49.2 0.442 0.506
Note: Overall performance score on 32 mandatory skills for Post Test 1 & Post Test 2; df =1; (p ≤ 0.05)
Retention of BLS skill competence.
In Table 4.7, for the Novices who attended both Post Tests, 39.3% of the CD group
and 42.3% of the Traditional group retained their skill competence at Post Test 2 (χ2 =
0.051, p = 0.821). For the Practising Nurses who attended both Post Tests, 43.8% of the
CD group and 37.5% of the Traditional group retained their overall skill level at Post Test
2 (χ2 = 0.086 p = 0.770). When the cohorts were combined, 40.9% of the CD group and
41.2% of the Traditional group retained their overall skill level at Post Test 2, with no
statistically significant difference between the training groups (χ2
= 0.001, p = 0.981).
Therefore there was no statistically significant difference in retention of BLS skill level or
skill competence at two months post training between the CD and Traditional training
method for the Novices, Practising Nurses and when the cohorts were combined (see
Table 4.7).
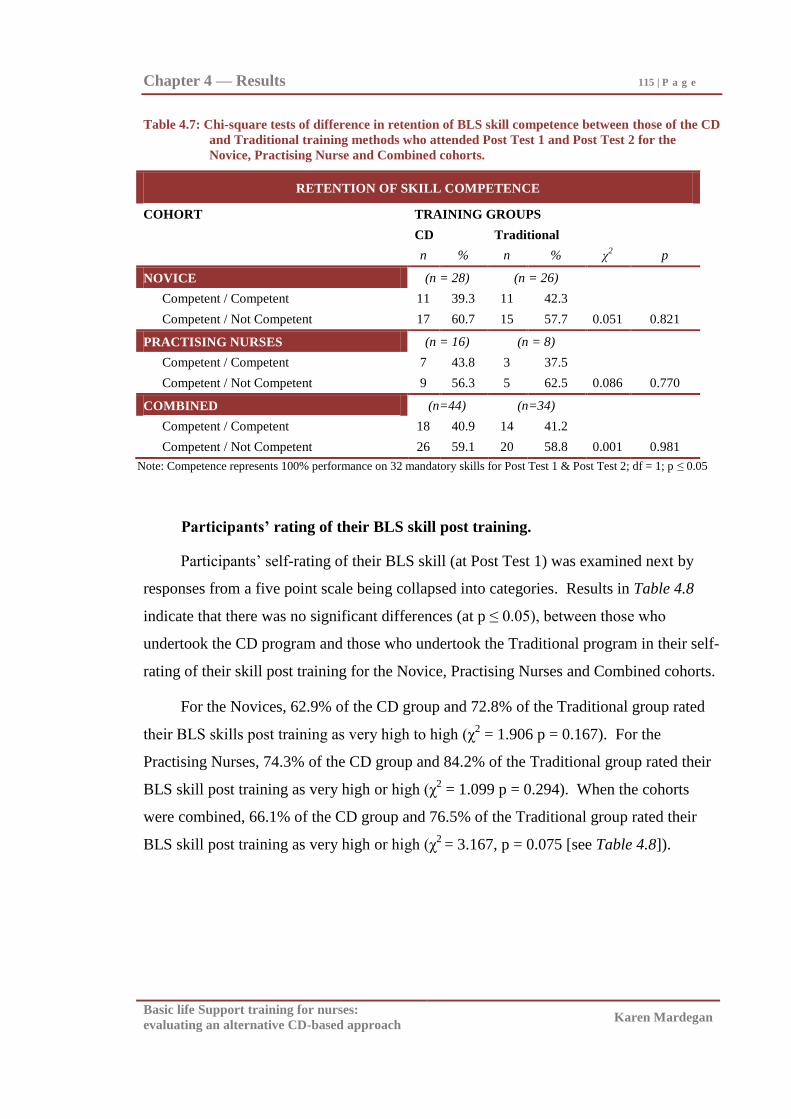
Chapter 4 — Results 115 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.7: Chi-square tests of difference in retention of BLS skill competence between those of the CD
and Traditional training methods who attended Post Test 1 and Post Test 2 for the
Novice, Practising Nurse and Combined cohorts.
RETENTION OF SKILL COMPETENCE
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 28) (n = 26)
Competent / Competent 11 39.3 11 42.3
Competent / Not Competent 17 60.7 15 57.7 0.051 0.821
PRACTISING NURSES (n = 16) (n = 8)
Competent / Competent 7 43.8 3 37.5
Competent / Not Competent 9 56.3 5 62.5 0.086 0.770
COMBINED (n=44) (n=34)
Competent / Competent 18 40.9 14 41.2
Competent / Not Competent 26 59.1 20 58.8 0.001 0.981
Note: Competence represents 100% performance on 32 mandatory skills for Post Test 1 & Post Test 2; df = 1; p ≤ 0.05
Participants’ rating of their BLS skill post training.
Participants‘ self-rating of their BLS skill (at Post Test 1) was examined next by
responses from a five point scale being collapsed into categories. Results in Table 4.8
indicate that there was no significant differences (at p ≤ 0.05), between those who
undertook the CD program and those who undertook the Traditional program in their self-
rating of their skill post training for the Novice, Practising Nurses and Combined cohorts.
For the Novices, 62.9% of the CD group and 72.8% of the Traditional group rated
their BLS skills post training as very high to high (χ2 = 1.906 p = 0.167). For the
Practising Nurses, 74.3% of the CD group and 84.2% of the Traditional group rated their
BLS skill post training as very high or high (χ2 = 1.099 p = 0.294). When the cohorts
were combined, 66.1% of the CD group and 76.5% of the Traditional group rated their
BLS skill post training as very high or high (χ2
= 3.167, p = 0.075 [see Table 4.8]).
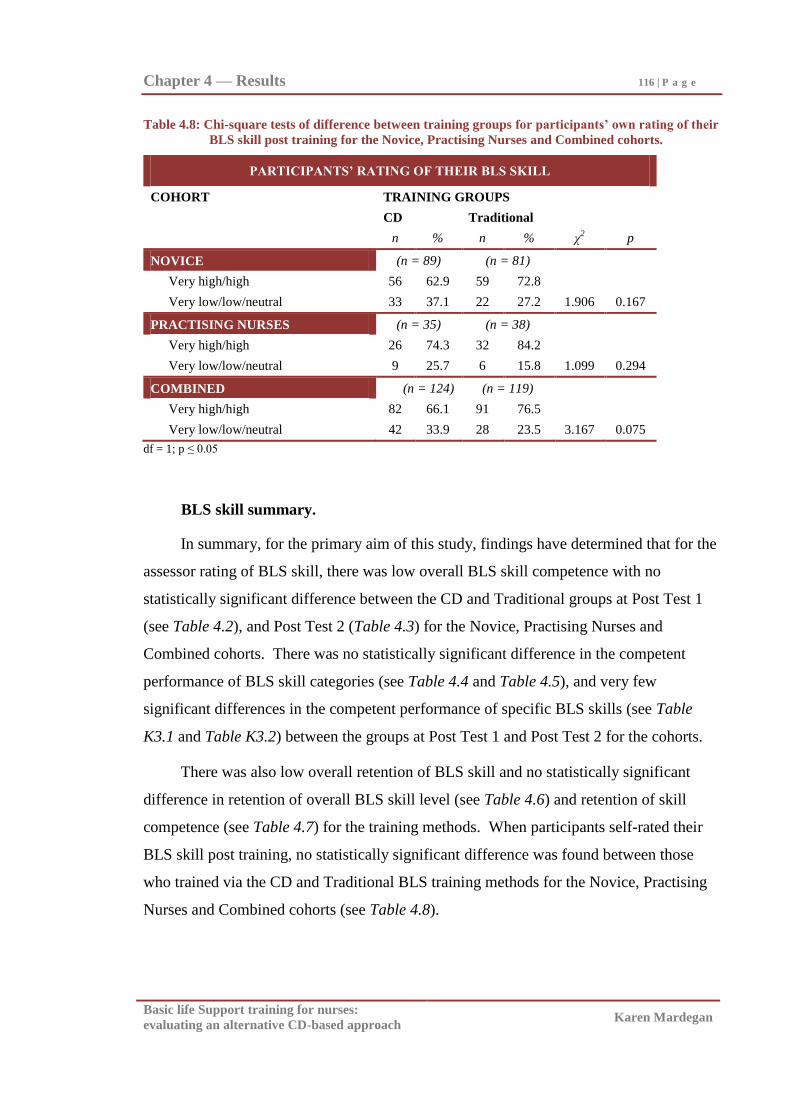
Chapter 4 — Results 116 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.8: Chi-square tests of difference between training groups for participants’ own rating of their
BLS skill post training for the Novice, Practising Nurses and Combined cohorts.
PARTICIPANTS’ RATING OF THEIR BLS SKILL
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 89) (n = 81)
Very high/high 56 62.9 59 72.8
Very low/low/neutral 33 37.1 22 27.2 1.906 0.167
PRACTISING NURSES (n = 35) (n = 38)
Very high/high 26 74.3 32 84.2
Very low/low/neutral 9 25.7 6 15.8 1.099 0.294
COMBINED (n = 124) (n = 119)
Very high/high 82 66.1 91 76.5
Very low/low/neutral 42 33.9 28 23.5 3.167 0.075
df = 1; p ≤ 0.05
BLS skill summary.
In summary, for the primary aim of this study, findings have determined that for the
assessor rating of BLS skill, there was low overall BLS skill competence with no
statistically significant difference between the CD and Traditional groups at Post Test 1
(see Table 4.2), and Post Test 2 (Table 4.3) for the Novice, Practising Nurses and
Combined cohorts. There was no statistically significant difference in the competent
performance of BLS skill categories (see Table 4.4 and Table 4.5), and very few
significant differences in the competent performance of specific BLS skills (see Table
K3.1 and Table K3.2) between the groups at Post Test 1 and Post Test 2 for the cohorts.
There was also low overall retention of BLS skill and no statistically significant
difference in retention of overall BLS skill level (see Table 4.6) and retention of skill
competence (see Table 4.7) for the training methods. When participants self-rated their
BLS skill post training, no statistically significant difference was found between those
who trained via the CD and Traditional BLS training methods for the Novice, Practising
Nurses and Combined cohorts (see Table 4.8).
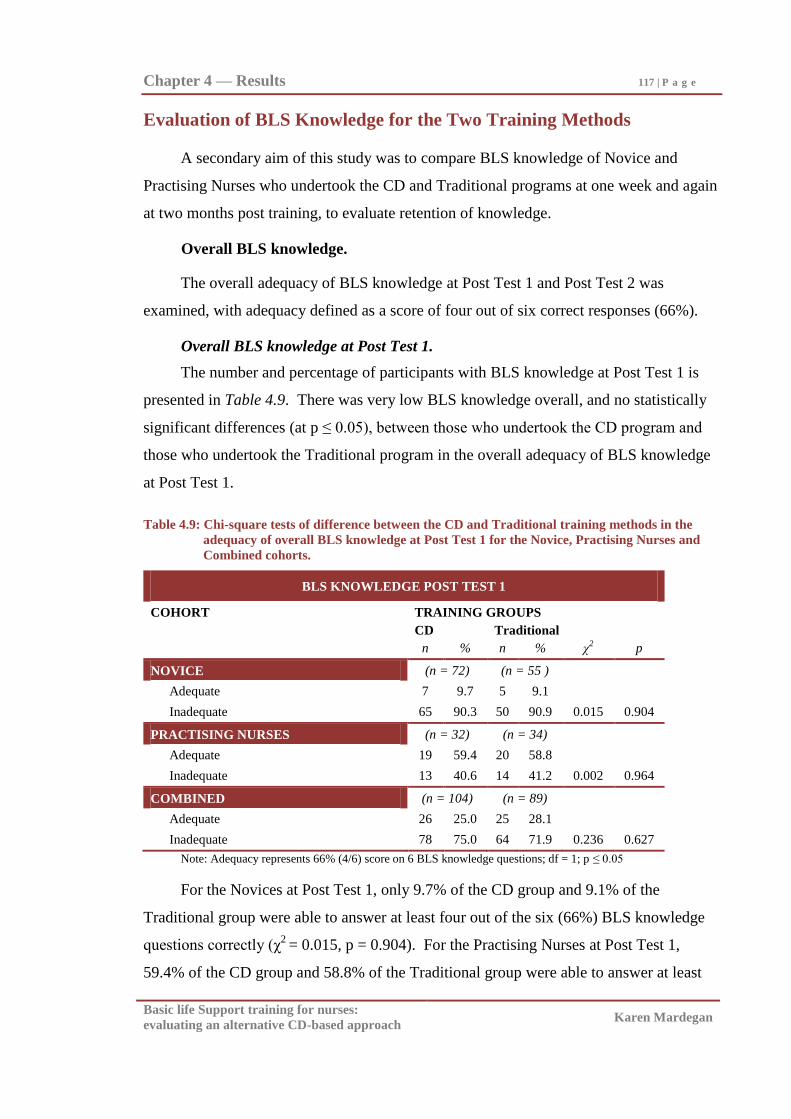
Chapter 4 — Results 117 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Evaluation of BLS Knowledge for the Two Training Methods
A secondary aim of this study was to compare BLS knowledge of Novice and
Practising Nurses who undertook the CD and Traditional programs at one week and again
at two months post training, to evaluate retention of knowledge.
Overall BLS knowledge.
The overall adequacy of BLS knowledge at Post Test 1 and Post Test 2 was
examined, with adequacy defined as a score of four out of six correct responses (66%).
Overall BLS knowledge at Post Test 1.
The number and percentage of participants with BLS knowledge at Post Test 1 is
presented in Table 4.9. There was very low BLS knowledge overall, and no statistically
significant differences (at p ≤ 0.05), between those who undertook the CD program and
those who undertook the Traditional program in the overall adequacy of BLS knowledge
at Post Test 1.
Table 4.9: Chi-square tests of difference between the CD and Traditional training methods in the
adequacy of overall BLS knowledge at Post Test 1 for the Novice, Practising Nurses and
Combined cohorts.
BLS KNOWLEDGE POST TEST 1
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 72) (n = 55 )
Adequate 7 9.7 5 9.1
Inadequate 65 90.3 50 90.9 0.015 0.904
PRACTISING NURSES (n = 32) (n = 34)
Adequate 19 59.4 20 58.8
Inadequate 13 40.6 14 41.2 0.002 0.964
COMBINED (n = 104) (n = 89)
Adequate 26 25.0 25 28.1
Inadequate 78 75.0 64 71.9 0.236 0.627
Note: Adequacy represents 66% (4/6) score on 6 BLS knowledge questions; df = 1; p ≤ 0.05
For the Novices at Post Test 1, only 9.7% of the CD group and 9.1% of the
Traditional group were able to answer at least four out of the six (66%) BLS knowledge
questions correctly (χ2
= 0.015, p = 0.904). For the Practising Nurses at Post Test 1,
59.4% of the CD group and 58.8% of the Traditional group were able to answer at least
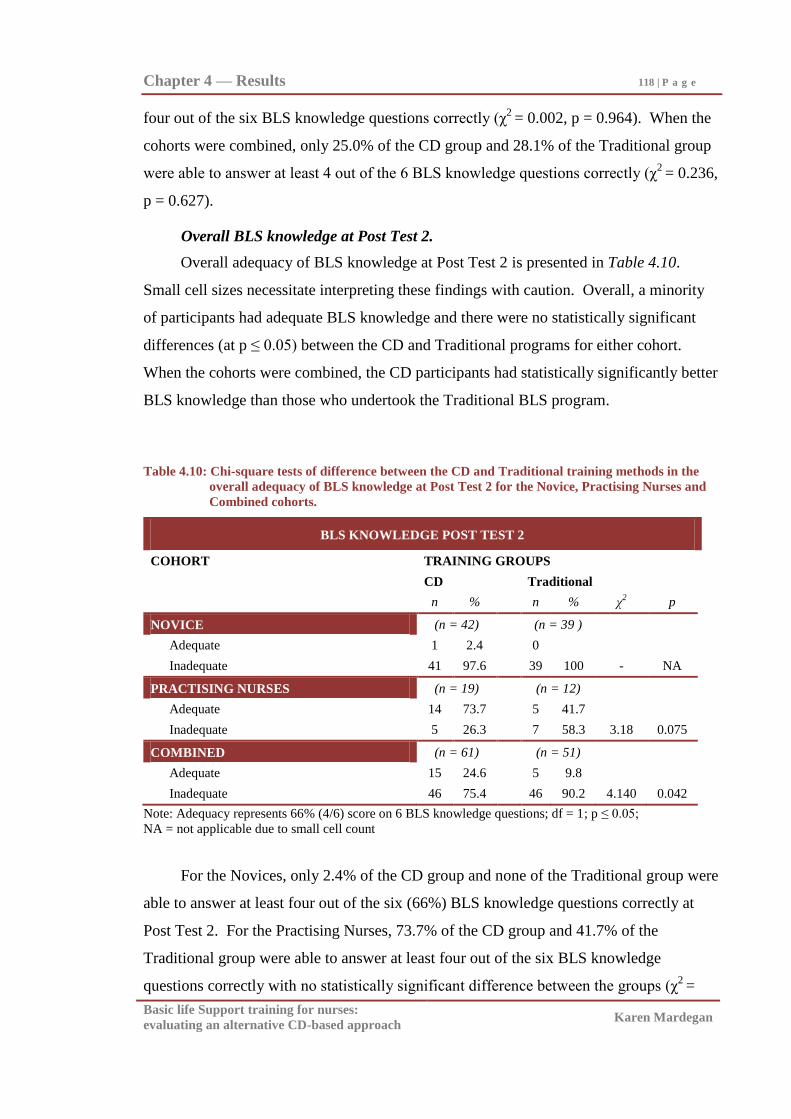
Chapter 4 — Results 118 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
four out of the six BLS knowledge questions correctly (χ2
= 0.002, p = 0.964). When the
cohorts were combined, only 25.0% of the CD group and 28.1% of the Traditional group
were able to answer at least 4 out of the 6 BLS knowledge questions correctly (χ2
= 0.236,
p = 0.627).
Overall BLS knowledge at Post Test 2.
Overall adequacy of BLS knowledge at Post Test 2 is presented in Table 4.10.
Small cell sizes necessitate interpreting these findings with caution. Overall, a minority
of participants had adequate BLS knowledge and there were no statistically significant
differences (at p ≤ 0.05) between the CD and Traditional programs for either cohort.
When the cohorts were combined, the CD participants had statistically significantly better
BLS knowledge than those who undertook the Traditional BLS program.
Table 4.10: Chi-square tests of difference between the CD and Traditional training methods in the
overall adequacy of BLS knowledge at Post Test 2 for the Novice, Practising Nurses and
Combined cohorts.
BLS KNOWLEDGE POST TEST 2
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 42) (n = 39 )
Adequate 1 2.4 0
Inadequate 41 97.6 39 100 - NA
PRACTISING NURSES (n = 19) (n = 12)
Adequate 14 73.7 5 41.7
Inadequate 5 26.3 7 58.3 3.18 0.075
COMBINED (n = 61) (n = 51)
Adequate 15 24.6 5 9.8
Inadequate 46 75.4 46 90.2 4.140 0.042
Note: Adequacy represents 66% (4/6) score on 6 BLS knowledge questions; df = 1; p ≤ 0.05;
NA = not applicable due to small cell count
For the Novices, only 2.4% of the CD group and none of the Traditional group were
able to answer at least four out of the six (66%) BLS knowledge questions correctly at
Post Test 2. For the Practising Nurses, 73.7% of the CD group and 41.7% of the
Traditional group were able to answer at least four out of the six BLS knowledge
questions correctly with no statistically significant difference between the groups (χ2
=
Chapter 4 — Results 119 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
3.18, p = 0.075). When the cohorts were combined, 24.6% of the CD group and 9.8% of
the Traditional group were able to answer at least four out of the six BLS knowledge
questions correctly at Post Test 2 with a statistically significantly better overall BLS
knowledge for the CD groups in these small samples (χ2
= 4.140, p = 0.042).
Specific BLS knowledge questions at Post Test 1 and Post Test 2.
Responses to each of the six BLS knowledge questions (define respiratory and
cardiac arrest; causes of cardiac and respiratory arrest; complications of CPR; and the
most common drugs used in arrest) at Post Test 1 and Post Test 2 were examined. Due to
small cell counts in both the Novice and Practising Nurses cohorts only the results from
the combined cohort of Novices and Practising nurses responses are presented in
Appendix L. There were no statistically significant differences (at p ≤ 0.001) between the
CD and Traditional groups for each of these specific knowledge questions at both Post
Test 1 and Post Test 2 (see Appendix L). Furthermore the percentage of participants who
answered the questions correctly was very low, (well below mastery standards), at both
Post Test 1 and Post Test 2 (see Appendix L).
Retention of BLS knowledge for the two training methods.
Retention of BLS knowledge for the CD and Traditional groups was analysed by
comparing the overall knowledge score of each participant who attended Post Test 1 and
Post Test 2. Those whose overall score remained the same or better were considered to
have retained their overall BLS knowledge level (see Table 4.11). There was low
retention of BLS knowledge with no statistically significant difference between those in
the two training methods for the Novice, Practising Nurses and Combined cohorts (at p ≤
0.05).
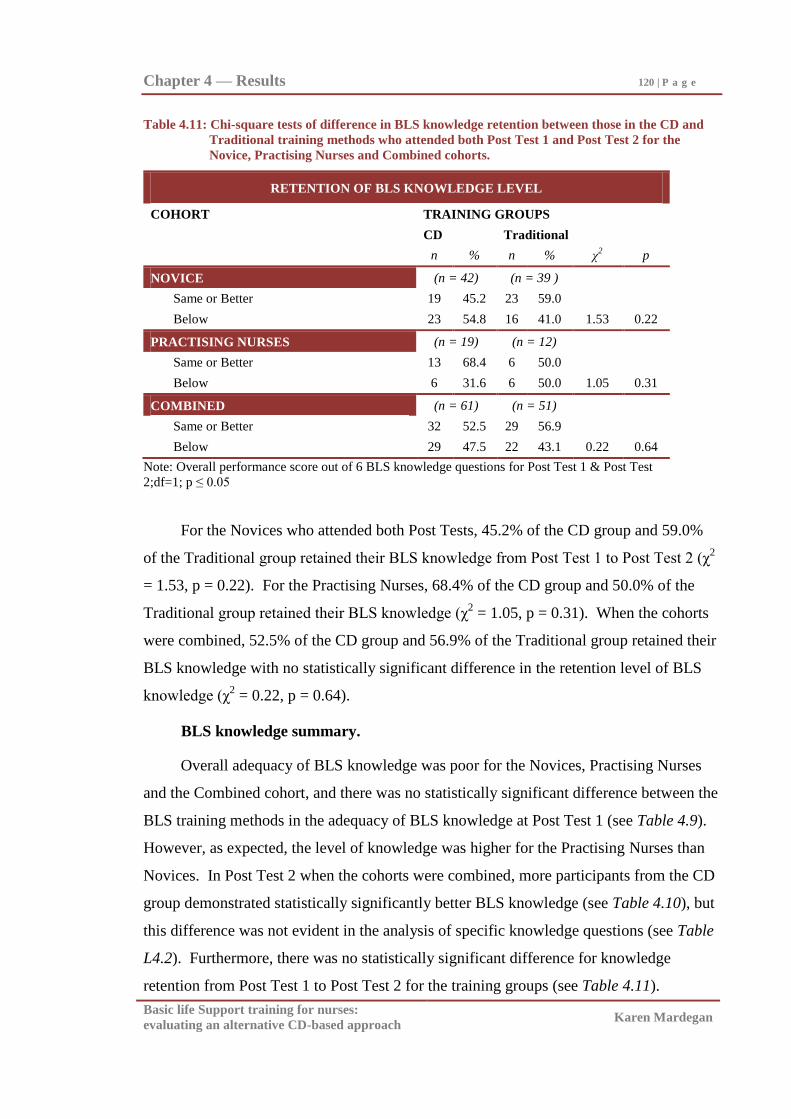
Chapter 4 — Results 120 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.11: Chi-square tests of difference in BLS knowledge retention between those in the CD and
Traditional training methods who attended both Post Test 1 and Post Test 2 for the
Novice, Practising Nurses and Combined cohorts.
RETENTION OF BLS KNOWLEDGE LEVEL
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 42) (n = 39 )
Same or Better 19 45.2 23 59.0
Below 23 54.8 16 41.0 1.53 0.22
PRACTISING NURSES (n = 19) (n = 12)
Same or Better 13 68.4 6 50.0
Below 6 31.6 6 50.0 1.05 0.31
COMBINED (n = 61) (n = 51)
Same or Better 32 52.5 29 56.9
Below 29 47.5 22 43.1 0.22 0.64
Note: Overall performance score out of 6 BLS knowledge questions for Post Test 1 & Post Test
2;df=1; p ≤ 0.05
For the Novices who attended both Post Tests, 45.2% of the CD group and 59.0%
of the Traditional group retained their BLS knowledge from Post Test 1 to Post Test 2 (χ2
= 1.53, p = 0.22). For the Practising Nurses, 68.4% of the CD group and 50.0% of the
Traditional group retained their BLS knowledge (χ2 = 1.05, p = 0.31). When the cohorts
were combined, 52.5% of the CD group and 56.9% of the Traditional group retained their
BLS knowledge with no statistically significant difference in the retention level of BLS
knowledge (χ2 = 0.22, p = 0.64).
BLS knowledge summary.
Overall adequacy of BLS knowledge was poor for the Novices, Practising Nurses
and the Combined cohort, and there was no statistically significant difference between the
BLS training methods in the adequacy of BLS knowledge at Post Test 1 (see Table 4.9).
However, as expected, the level of knowledge was higher for the Practising Nurses than
Novices. In Post Test 2 when the cohorts were combined, more participants from the CD
group demonstrated statistically significantly better BLS knowledge (see Table 4.10), but
this difference was not evident in the analysis of specific knowledge questions (see Table
L4.2). Furthermore, there was no statistically significant difference for knowledge
retention from Post Test 1 to Post Test 2 for the training groups (see Table 4.11).
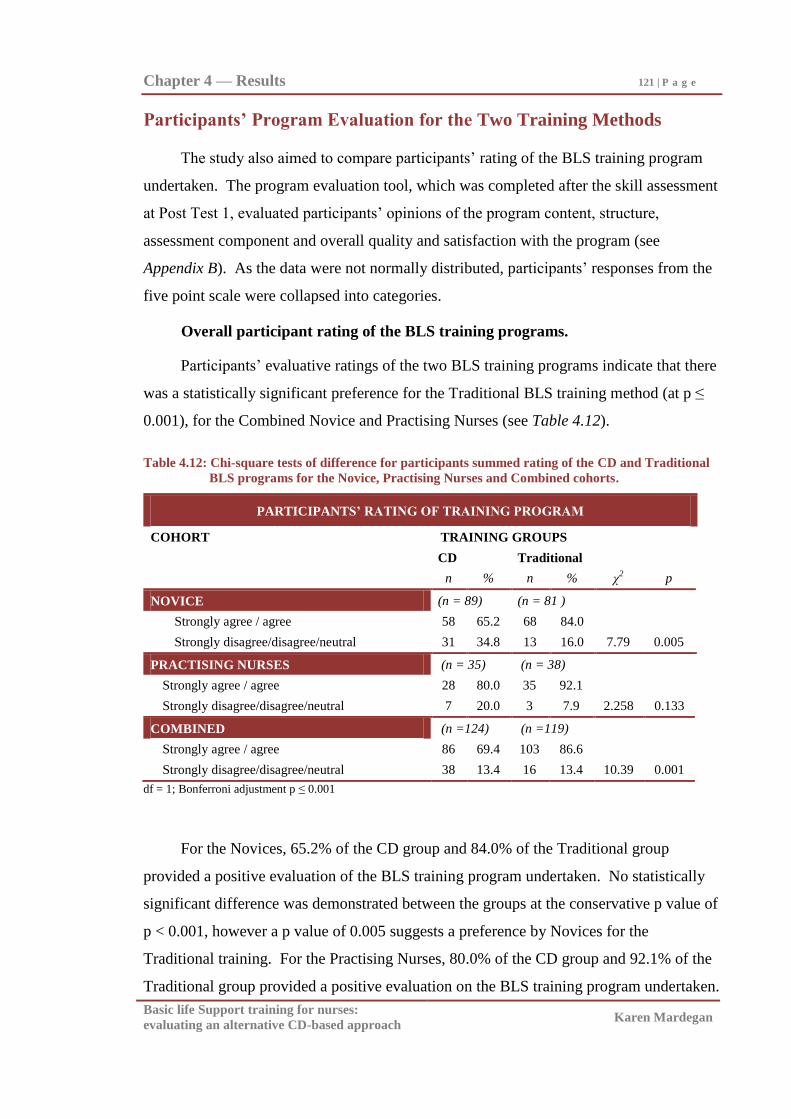
Chapter 4 — Results 121 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Participants’ Program Evaluation for the Two Training Methods
The study also aimed to compare participants‘ rating of the BLS training program
undertaken. The program evaluation tool, which was completed after the skill assessment
at Post Test 1, evaluated participants‘ opinions of the program content, structure,
assessment component and overall quality and satisfaction with the program (see
Appendix B). As the data were not normally distributed, participants‘ responses from the
five point scale were collapsed into categories.
Overall participant rating of the BLS training programs.
Participants‘ evaluative ratings of the two BLS training programs indicate that there
was a statistically significant preference for the Traditional BLS training method (at p ≤
0.001), for the Combined Novice and Practising Nurses (see Table 4.12).
Table 4.12: Chi-square tests of difference for participants summed rating of the CD and Traditional
BLS programs for the Novice, Practising Nurses and Combined cohorts.
PARTICIPANTS’ RATING OF TRAINING PROGRAM
COHORT TRAINING GROUPS
CD Traditional
n % n % χ2 p
NOVICE (n = 89) (n = 81 )
Strongly agree / agree 58 65.2 68 84.0
Strongly disagree/disagree/neutral 31 34.8 13 16.0 7.79 0.005
PRACTISING NURSES (n = 35) (n = 38)
Strongly agree / agree 28 80.0 35 92.1
Strongly disagree/disagree/neutral 7 20.0 3 7.9 2.258 0.133
COMBINED (n =124) (n =119)
Strongly agree / agree 86 69.4 103 86.6
Strongly disagree/disagree/neutral 38 13.4 16 13.4 10.39 0.001
df = 1; Bonferroni adjustment p ≤ 0.001
For the Novices, 65.2% of the CD group and 84.0% of the Traditional group
provided a positive evaluation of the BLS training program undertaken. No statistically
significant difference was demonstrated between the groups at the conservative p value of
p < 0.001, however a p value of 0.005 suggests a preference by Novices for the
Traditional training. For the Practising Nurses, 80.0% of the CD group and 92.1% of the
Traditional group provided a positive evaluation on the BLS training program undertaken.
Chapter 4 — Results 122 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
However cell sizes were too small for reliable statistical analysis. When the cohorts were
combined, 69.4% of the CD group and 86.6% of the Traditional group provided a positive
evaluation on the BLS training program undertaken, with a statistically significantly
higher rating overall for the Traditional program (χ2
= 10.39, p = 0.001).
Participant rating of program components and specific questions.
Each specific question in the program evaluation was then grouped under the
program components of: content, structure, assessment, and overall quality and
satisfaction, and the positive responses were summed. Due to small cell counts in the
Practising Nurses cohort, only the results for the combined cohort of Novices and
Practising nurses rating for these four program components and for each specific question
within these components are presented next.
Participant rating of program components.
There were statistically significantly higher ratings for the Traditional program (at p
≤ 0.001), in the overall rating of the programs‘ content and structure. However, there
were no statistically significant differences between the groups in the assessment
component and overall quality and satisfaction with the training programs between the
Combined Novice and Practising Nurses in the two training programs, although results
approached significance. Furthermore, the overall rating for each of the four components
was high, suggesting general satisfaction with the programs (see Table 4.13).
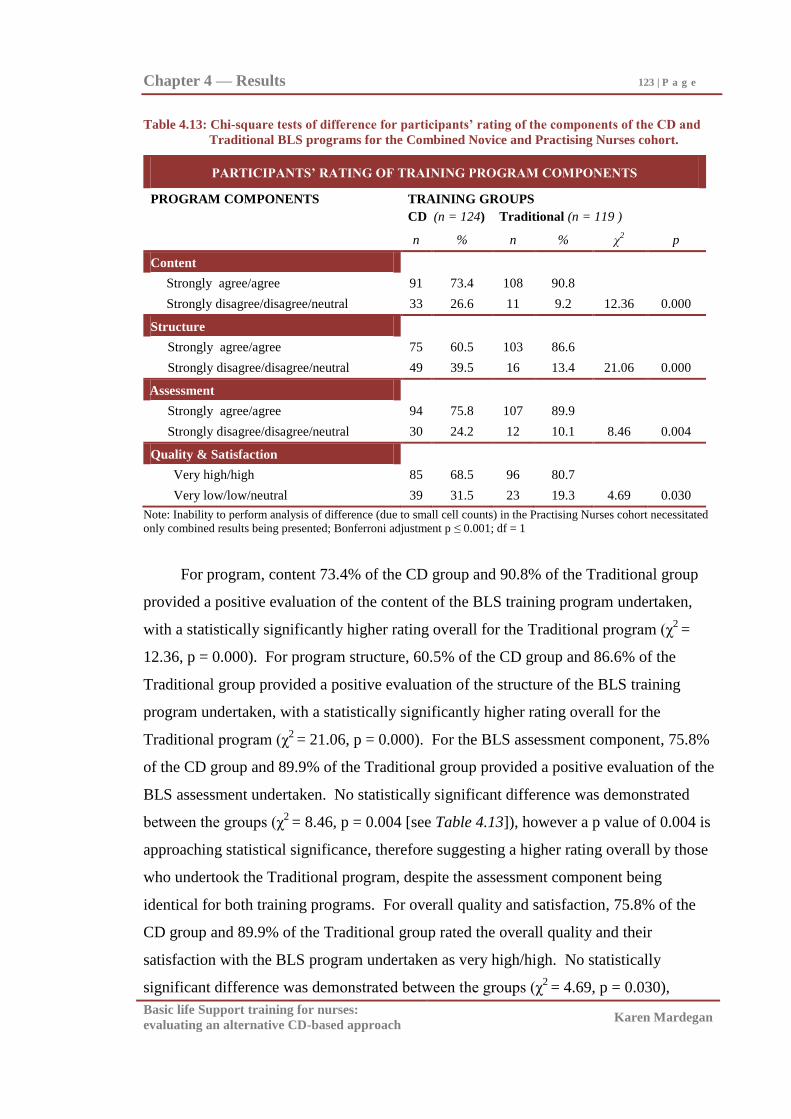
Chapter 4 — Results 123 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table 4.13: Chi-square tests of difference for participants’ rating of the components of the CD and
Traditional BLS programs for the Combined Novice and Practising Nurses cohort.
PARTICIPANTS’ RATING OF TRAINING PROGRAM COMPONENTS
PROGRAM COMPONENTS TRAINING GROUPS
CD (n = 124) Traditional (n = 119 )
n % n % χ2 p
Content
Strongly agree/agree 91 73.4 108 90.8
Strongly disagree/disagree/neutral 33 26.6 11 9.2 12.36 0.000
Structure
Strongly agree/agree 75 60.5 103 86.6
Strongly disagree/disagree/neutral 49 39.5 16 13.4 21.06 0.000
Assessment
Strongly agree/agree 94 75.8 107 89.9
Strongly disagree/disagree/neutral 30 24.2 12 10.1 8.46 0.004
Quality & Satisfaction
Very high/high 85 68.5 96 80.7
Very low/low/neutral 39 31.5 23 19.3 4.69 0.030
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; Bonferroni adjustment p ≤ 0.001; df = 1
For program, content 73.4% of the CD group and 90.8% of the Traditional group
provided a positive evaluation of the content of the BLS training program undertaken,
with a statistically significantly higher rating overall for the Traditional program (χ2
=
12.36, p = 0.000). For program structure, 60.5% of the CD group and 86.6% of the
Traditional group provided a positive evaluation of the structure of the BLS training
program undertaken, with a statistically significantly higher rating overall for the
Traditional program (χ2
= 21.06, p = 0.000). For the BLS assessment component, 75.8%
of the CD group and 89.9% of the Traditional group provided a positive evaluation of the
BLS assessment undertaken. No statistically significant difference was demonstrated
between the groups (χ2
= 8.46, p = 0.004 [see Table 4.13]), however a p value of 0.004 is
approaching statistical significance, therefore suggesting a higher rating overall by those
who undertook the Traditional program, despite the assessment component being
identical for both training programs. For overall quality and satisfaction, 75.8% of the
CD group and 89.9% of the Traditional group rated the overall quality and their
satisfaction with the BLS program undertaken as very high/high. No statistically
significant difference was demonstrated between the groups (χ2
= 4.69, p = 0.030),
Chapter 4 — Results 124 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
however, once again, a p value of 0.030 is approaching a commonly accepted level of
statistical significance (0.01 ≤ p ≤ 0.05), therefore suggesting a higher rating overall by
those who undertook the Traditional program.
Participant rating of specific program evaluation questions.
Every specific question within each of the four program components was also
examined. Results are presented in Appendix M. Many specific questions identified
statistically significant differences (at p ≤ 0.001), in program rating between the groups,
but this finding needs to be interpreted with caution due to the large number of tests
applied (see Appendix M).
For the Combined Novice and Practising Nurses, a higher proportion of the
Traditional group positively evaluated the questions on: content appropriateness, content
and simulation usefulness for knowledge and skill development, and complexity of the
content (within the program content component [see Table M4.1]), the appropriateness of
sequencing and structure for skill acquisition, maintenance of learning focus, and
facilitating mastery learning (in program structure [see Table M4.2]), and the usefulness
in reinforcement of skills (in the assessment component [see Table M4.3]).
However, there were no statistically significant differences between the CD and
Traditional groups ratings of the specific program content questions (breadth of content,
content up-to-date, content relevance to clinical practice, and appropriateness of the
content of simulations/scenarios [see Table M4.1]), the program structure question
(organisation of the topic [see Table M4.2]), the assessment component question
(appropriateness of the assessment content [see Table M4.3]), and the program quality
and satisfaction questions (quality of the program, and satisfaction with the program [see
Table M4.4]).
Participants’ program evaluation summary.
These results indicate that a higher proportion of participants in the Traditional
program positively evaluated the BLS program compared with those in the CD program
(χ2 = 10.39, p = 0.001, [see Table 4.12]). Results for the four program components
indicate that Traditional program participants‘ statistically significantly more strongly
agreed with the program‘s content and structure. There was however no statistically
Chapter 4 — Results 125 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
significant difference in overall rating of quality and satisfaction with the programs, nor
with the assessment process for the groups (see Table 4.13).
Summary of Results
Overall results of this project indicate that there was low BLS skill and knowledge
levels, which did not meet skill mastery and program effectiveness standards (80%). No
statistically significant difference between the CD and Traditional methods of BLS
training for Novices, Practising Nurses, and for the Combined group when study
participants were assessed at one week and at two months post training were found.
However there was marginally better overall adequacy of BLS knowledge at Post Test 2
for the CD group in the Combined cohort. There were also low levels of skill and
knowledge retention with no statistically significant differences between the groups.
Additionally, there were also no statistically significant differences between the CD and
Traditional participants‘ rating of their skill post training. Findings therefore indicate that
the CD BLS training method was equivalent to the Traditional method of BLS training
for the Novice, Practising Nurses and Combined cohorts, and that neither method was
overly effective.
Participants‘ evaluative rating of their respective programs, and particularly
program content and structure, suggests that the Traditional approach to BLS training was
preferred by participants. However this expressed preference has not resulted in the
Traditional method being more effective in overall BLS skill, BLS knowledge and
retention of skill and knowledge in Novices, Practising Nurses nor when the cohorts were
combined.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Chapter 5
Discussion and Conclusions
The primary aim of this study was to compare the BLS skill of Novice and
Practising Nurses who trained via a CD-based BLS training program with those who
undertook a Traditional BLS program at one week and again at two months post training.
The secondary aims were to evaluate participants‘ BLS knowledge and participants‘
rating of the CD and Traditional BLS training programs undertaken.
There was low overall BLS skill and knowledge for Novices and Practising Nurses,
and a lack of statistically significant difference between the CD and Traditional training
methods at one week, and at two months. There was also a participant preference for the
Traditional training method. These are important findings that potentially have
implications for the future direction of BLS practice and research. Therefore how these
findings relate to comparative literature, the methodological issues encountered during the
study, and the resulting implications for BLS practice and future research will be
discussed below.
Comparison with Existing Research on BLS Training
To determine the overall contribution of this study‘s findings, it is firstly necessary
to compare the outcomes of the current study with those of comparative BLS CD
literature. However, this is not possible because previous studies have not directly
compared CD BLS training programs with Traditional programs (Clark et al., 2000;
Doyle, 2002; Moule, 2002; Moule & Gilchrist, 2001; Monsieurs et al., 2004). Under
these circumstances, it is therefore relevant to compare the findings of the current project
with previous research that compares Multimedia (Video, DVD and Internet) programs
that included manikin practice, with a Traditional BLS program.
The majority of previous research examining Multimedia BLS training programs
with manikin practice have demonstrated, (along with the current study in Novice and
Practising Nurses), that Multimedia BLS training programs produce overall BLS skill
outcomes that are statistically equivalent to the Traditional training method, both initially
Chapter 5 — Discussion and Conclusions 127 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
post training and over time, for health professionals (Cason et al., 2009; Moule et al.,
2008a), and lay people (Choa et al., 2006; Chung et al., 2010; Creutzfeldt et al., 2009;
Einspruch et al., 2007; Isbye et al., 2006; Jones et al., 2007; Mancini et al., 2009; Roppolo
et al., 2007). It is only in the early BLS Video studies and three later studies in DVD and
Internet programs (Lynch et al., 2005; Kardong-Edgren et al., 2010; Roppolo et al., 2011)
where significantly better skill has been demonstrated post Multimedia training. The
notable skill decline in Novice and Practising Nurses in the current study is also
consistent with other Multimedia programs in health professional (Fabius et al., 1994) and
lay (Einspruch et al., 2007; Reder et al., 2006; Roppolo et al., 2007; Sarac & Ok, 2010)
studies. Furthermore, participant‘s self-rating of skill post training with Multimedia
training programs, likewise to the current study have also reported no significant
difference in self-rating of skill between the training methods (Batchellor et al., 2000;
Braslow et al., 1997; Liberman et al., 2000; Todd et al., 1998, 1999).
Similarly with BLS knowledge, knowledge outcomes that are statistically
equivalent to Traditional programs, initially and over time, are reported in the current
study and other Multimedia studies in health professionals (Cason et al., 2009; Moule et
al., 2008a; Todd et al., 1998) and lay people (Creutzfeldt et al., 2009; Todd et al., 1999).
Studies evaluating knowledge retention using Multimedia designs have not been found,
but in the current study there was also knowledge decline by two months post training in
the Novice and Practising Nurses.
The BLS skill mastery standard post training is 80% (Marzooq & Lyneham, 2009).
Yet the majority of health professional (Fabius et al., 1994; Kardong-Edgren et al., 2010;
Moule et al., 2008a; Roppolo et al., 2011) and lay (Batcheller et al., 2000; Choa et al.,
2006; Lynch et al., 2005; Jones et al., 2007; Reder et al., 2006; Teague & Riley, 2006)
studies report skill competence below 80% initially post training and subsequently over
time. This suggests that the current study findings in Novice and Practising Nurses are
consistent with the majority of comparative literature, and that there is low overall skill
training effectiveness across available BLS training methods. The small number of health
professional DVD and CD studies (Cason et al., 2009: Monsieurs et al., 2004), and lay
Video/DVD studies (Braslow et al., 1997; Chung et al., 2010; Mancini et al., 2009;
Roppolo et al., 2007), that report high skill competence above 80% initially post training
suggest that there are potential benefits particularly with the DVD manikin design.
Chapter 5 — Discussion and Conclusions 128 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
However, skill retention continues to be a problem with all methods of training in both
health professional (Fabius et al., 1994) and lay groups (Braslow et al., 1997; Einspruch
et al., 2007; Isbye et al., 2006; Reder et al., 2006; Sarac &Ok, 2010).
Knowledge immediately post training in the literature is generally higher in health
professional (Cason et al., 2009; Fabius et al., 1994, Moule et al., 2008a) and lay people
(Reder et al., 2006), than those achieved particularly in the novice nurse students, in the
current study. Furthermore, retention of knowledge is also generally below 80% by two
months (Todd et al., 1998, 1999) suggesting that overall BLS training program designs
along with the current studies CD design are not significantly better than Traditional
training methods. BLS training programs which meet overall industry standards of
competence post training and over time are therefore still needed.
Specific BLS skills.
In the literature, the specific skills within the BLS procedure where participants in
either the Multimedia (CD, DVD/Video or Internet) or the Traditional training program
have demonstrated statistically significant difference in skill competence varies between
the studies, and observed differences are associated usually with only a small number of
particular skills within the overall BLS skill procedure. Statistically significant difference
in ventilation and compression skills are the more commonly noted areas of skill
difference in health professional and lay studies (Braslow et al., 1997; Einspruch et al.,
2007; Creutzfeldt et al., 2009; Jones et al., 2007; Kardong-Edgren et al., 2010; Lynch et
al., 2005; Mancini et al., 2009; Moule et al., 2008a; Sarac & Ok, 2010; Todd et al., 1999).
However this is contrary to the findings of the current study in both Novice and Practising
Nurses where significant difference between the groups in ventilation and circulation
skills were not found. In all these studies (including the current study), differences in the
performance of specific skills is therefore possibly a reflection of the strength/weakness
of that particular training program rather than a reflection of reliable superiority of the
type of training method (Traditional, CD, DVD/Video or Internet), or possibly error due
to the relatively large number of statistical tests performed.
Participants’ evaluation of the training programs.
Most previous studies have not evaluated the participants‘ view of the BLS
programs undertaken. In those that have, no statistically significant difference in
Chapter 5 — Discussion and Conclusions 129 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
satisfaction has been noted (Liberman et al., 2000; Monsieurs et al., 2004; Moule &
Gilchrist, 2001; Moule, 2002). The current study participants preferred the traditional
training. Why there was this reduced overall rating of the CD program by the Novice and
Practising Nurses in the current study is unclear, particularly as there was no significant
difference in BLS skill and knowledge performance. The generally increased exposure to
the internet and computers would also suggest that acceptance of flexible modes of
training delivery has somewhat progressed (Smith, Robertson, & Wakefield, 2002) since
this study was conducted some seven years ago, which brings into question the external
validity of this finding, across time.
Current study findings therefore suggest that CD-based BLS training which
includes independent manikin practice will be generally equivalent to other contemporary
BLS training methods, both when used with health professionals and lay people. The
lack of significant superiority of the CD-based BLS training method, and the documented
poor outcomes with Multimedia and Traditional BLS programs suggest the need for
continued efforts to develop and evaluate BLS training programs that can achieve
consistently high rates of competence along with acceptable retention over time.
Methodological Issues
There were a number of methodological issues (both strengths and limitations of the
study), which need to be considered when interpreting these findings. These issues
predominately concern aspects of the research design and materials used in the current
study.
Research design.
The research design issues which need to be taken into consideration include the
chosen effect size, participants‘ age, experience and allocation to groups, testing
regimens, post-test attendance, and some aspects of the particular BLS training programs
employed. These are discussed in detail below.
Selection of effect size.
The effect size of 0.6 selected for the study (see Appendix C), was based on the
related studies at the time the study was planned (Batcheller et al., 2000; Braslow et al.,
1997; Todd et al., 1998, 1999). These studies found significant difference between
Chapter 5 — Discussion and Conclusions 130 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
training methods. However, more recent studies have not been able to replicate this
statistical difference (Cason et al., 2009; Choa et al., 2006; Chung et al., 2010; Isbye et
al., 2006; Jones et al., 2007; Kardong-Edgren et al., 2010; Moule et al., 2008a; Reder et
al., 2006; Roppolo et al., 2007). Therefore the chosen effect size of 0.6 may in hindsight
have been too high. It would probably have been more reasonable to work from an effect
size of 0.2. This is a consideration for future research, as recruitment of around 400
participants would be required.
Study participants.
The majority of participants in both the Novice and Practising Nurses cohorts of this
study were aged between 18 - 30 years, and almost two-thirds of the Novice cohort had
also undertaken some form of BLS training previously. This was unexpected because
BLS assessment had not been offered in earlier years of the undergraduate university
program. It would have been preferable to have been able to access Novices with no
previous training from within student health professional groups, but doing so proved to
be difficult in this study, and has been noted in equivalent studies (Kardong-Edgren et al.,
2010; Roppolo et al., 2011). Most likely the lack of BLS training naivete arises from the
availability of BLS training for lay people and this group‘s natural interest in a skill that
will be required once they graduate. It is important to note also that the Practising Nurses
who had all learnt the skill before, were Graduate Nurses in their first year of practice,
and thus generally relatively junior. These factors resulted in the two cohorts
subsequently being relatively similar in terms of age and experience. This justified
combining, on occasions, Novice and Practising Nurses‘ results. Obviously, nurses with
many years of experience may have performed differently from the first-year graduate
students in the practising nurses group. Caution when applying current findings to all
nurses, the general public or the older population is therefore necessary.
As described in the method chapter, participants were allocated to training groups
based on previously determined university / hospital groupings. CD or Traditional
training method allocation was randomly assigned by the course co-ordinators of the
university / hospital program. Participants being recruited from within these formal
programs resulted in access constraints which ultimately prevented the possibility of
random allocation to training groups. Were random allocation possible, this would have
Chapter 5 — Discussion and Conclusions 131 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
strengthened the design and reduced the risk to bias allocation in the current study. The
design of future studies would be strengthen by random allocation to groups and training
methods where this is possible in the applied setting.
Testing regimens.
In the current study participants‘ BLS (skill and knowledge) competence was
assessed one week (Post Test 1) and again at two months post training (Post Test 2), but
not at pre-test. Post intervention testing is the norm in comparative studies of BLS
training methods (Batcheller et al., 2000; Braslow et al., 1997; Choa et al., 2006;
Creutzfeldt et al., 2009; Isbye et al., 2006; Lynch et al., 2005; Mancini et al., 2009; Moule
et al., 2008a; Roppolo et al., 2007; Thoren et al., 2007; Todd et al., 1998, 1999).
However, conducting a pre-test as well as the two post tests would have allowed for
assessment of prior skill levels, and if there were between group differences, for these to
be controlled statistically when comparing post-training competences (Campbell &
Stanley, 1966).
A potential design advantage for the current study was that the Post Test 1
assessment was one week post training, rather than the immediate assessment post
training seen in many other studies (Batcheller et al., 2000; Braslow et al., 1997; Choa et
al., 2006; Lynch et al., 2005; Mancini et al., 2009; Moule et al., 2008a; Roppolo et al.,
2007). Assessment conducted immediately post training evaluates immediate recall
rather than consolidated skill and knowledge and therefore has the potential for artificially
enhanced competency rates to be recorded.
To assess the stability of skill and knowledge over time, the study used the
relatively short skill and knowledge retention interval of two months (Post Test 2). This
limits insight into the patterns of BLS skill and knowledge decay beyond this point.
While there is always a concern with the practicability of obtaining extended access to
participants, follow up post testing beyond two months, where possible, would provide an
improved understanding of BLS skill and knowledge decay over time. The considerable
decay of skill and knowledge over only eight weeks in the current study supports the
necessity for evaluation of retention beyond two months. It is also unknown how
consistently decay persists over longer periods such as six months or twelve months,
especially when refresher training is usually mandated.
Chapter 5 — Discussion and Conclusions 132 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Post Test attendance.
The challenges involved in maintaining participation rates at post testing are evident
in the current study. Only 45% of participants overall took part in the two month post
training test. Decline in participation was particularly noted in the Traditional group of
Practising Nurses where only 12 of the original 54 participants (22.2%) returned for the
Post Test 2 assessment. This reduced attendance in Post Test 2 resulted in small cell
counts (< 5) limiting analysis possibilities for the Practising Nurses cohort in particular.
There is also concern that those who attended the Post Test 2 assessment are not reflective
of the whole cohort thus raising the possibility that those who dropped out were more
likely to have lower competence.
Reduced participation in subsequent testing post training has been noted in other
studies (Christenson et al., 2007; Creutzfeldt et al., 2009; Einspruch et al., 2007; Reder et
al., 2006; Roppolo et al., 2007). The reasons for the attrition is unknown, but participant
time constraints, the repetitive nature of post testing, the unappreciated benefit (of further
practice) and the potential over-estimation of skill noted in health professionals (Bjorshol,
1996; Grzeskowiak, 2006; Josipovic et al., 2009; Marzooq & Lyncham, 2009) are thought
to have negatively influenced post test attendance. Strategies to promote attendance at
post testing, such as providing incentives, may have promoted sustained participation and
therefore strengthened the validity of results from the current study. Such strategies are
worthy of consideration when designing subsequent studies which intend evaluating
retention of BLS skill and knowledge.
BLS training programs.
The BLS CD training program.
Although the CD used in the program was comparable to that of similar
technologies at the time of data collection, a number of limitations of the CD are
noteworthy. Firstly, the CD was not designed to have a manikin accompanying it.
Therefore, the project facilitator asked participants to practise on the provided manikin
while viewing the program, but participants were not prompted by the CD program to
practise while working through the CD. Despite this, the findings still indicated that the
method was comparable in effectiveness to Traditional training. However, if the CD was
designed to prompt the viewer to practise at points through the program, then potentially
Chapter 5 — Discussion and Conclusions 133 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
the results could have been more positive for the CD group. Some BLS Video and DVD
manikin kit studies have used prompting to good effect (Batcheller et al., 2000; Bjorshol
et al., 2009; Braslow et al., 1997; Cason et al., 2009; Chung et al., 2010; Mancini et al.,
2009; Nielsen et al., 2010; Roppolo et al., 2007; Todd et al., 1998, 1999). Practice has
also been considered essential to skill mastery in the training design and delivery
literature (Salas & Kosarzycki, 2003; Tannenbaum & Yakl, 1992).
The CD used in this project was produced in 1999, prior to the 2000, 2005, and
2010 ILCOR resuscitation guidelines. Currency of content and the expansion of the
capacity of current CD and computer capabilities generally over the last ten years also
suggest that development of a CD-based program which incorporates independent
manikin practice could potentially produce improved results.
Traditional BLS program.
Although a number of limitations have been identified for the BLS CD used in the
study, there are also potential limitations to the Traditional training programs used in this
study. The Traditional programs were the usual training programs then current within the
respective organisations. These programs were therefore not as highly standardised as are
some contemporary public programs such as St John or Red Cross BLS courses in
Australia. The training exposure was also not identical for both Traditional groups
because the Traditional program run for the 2nd
year nursing students was designed by the
university as a detailed (two hour) program for Novice students of the health professions,
whereas the program run for the Practising Nurses was designed by the participating
hospital as a condensed (one hour) program for practising health professionals who had
been previously accredited in BLS. Having noted this, instructors in both the project‘s
Traditional BLS programs were accredited by their respective organisations. It may have
been better to use a standardised course for both cohorts rather than courses currently
used in practice at the respective organisations. However, doing so would have prevented
the inclusion of health professional skill steps being taught and assessed (i.e. mouth-mask
ventilation, bag-mask ventilation, responsibilities post arrest etc).
Training program access.
Length of access to the CD program is also an area of design which varies between
studies. In the current project, the Novice nurse students were given two hours of BLS
Chapter 5 — Discussion and Conclusions 134 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
instruction via either the CD or Traditional program. The Practising Nurses in both the
CD and Traditional groups were given only one hour to complete the CD or Traditional
program, because the review of skills was thought to require less time than when initially
learning the skill. This design allows for direct comparison between the groups of each
cohort. However, some studies have allowed the Multimedia program participants
unlimited viewing time (Clarke et al., 2000; Fabius et al., 1994; Isbye et al., 2006), which
potentially would produce improved results for the CD participants. This flexibility
would however have compromised the direct comparability of the CD and Traditional
groups in the current study, so therefore was not incorporated into the design.
Measures.
There were a number of aspects to the measures used in the current study which
need to be also considered when discussing the overall findings of this study. The
measures used included: a questionnaire which obtained participant characteristics and
assessed BLS knowledge; a BLS skill assessment form; an automated BLS manikin; and
participant program evaluation forms.
Questionnaire and program evaluation.
The questionnaire and program evaluations had not been evaluated by the original
designers (Wilkinson & Chu, 1999) prior to their being used in the current project. These
tools were however used because they were designed to evaluate the CD used in the
project and Traditional BLS training. When analysing the participants‘ program
evaluations, comparison of the Traditional and CD group data was difficult because the
program evaluation forms given to the two groups were not identical. Questions which
were asked only of one group were therefore not included in the results. Tools should
promote comparability between the groups studied. In future projects, questionnaires/
program evaluations should be the same for all groups. If extra questions are required for
only one of the groups, these questions should be in a separate section so that
comparisons (data analysis) of the groups can be performed without difficulty.
BLS assessment form.
The BLS assessment form was drawn from that used to assess health professionals
at Austin Health (A&RMC, 2000) at the time of the data collection. This BLS assessment
form was designed to be used by an assessor as the sole form of assessment. It was not
Chapter 5 — Discussion and Conclusions 135 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
designed to be used in conjunction with the printout from an automated manikin.
Therefore unlike many studies reviewed in chapter two, the data collected in the current
study contained both assessor and manikin gradings for ventilation and compression
effectiveness. This is potentially a design advantage for the current study because
comparison of both the assessor and manikin ratings for compressions and ventilations
would have been possible if manikin recordings had been more reliable.
Furthermore, as previously outlined, this BLS assessment form determined
competence from the 100% correct performance of 32 (mandatory skills) out of a total of
49 skill steps. This is a very large number of skill steps and a very high standard of
competence in comparison to other BLS assessment forms which range from five to 18
skills (Braslow et al., 1997; Jones et al., 2007; Lynch et al., 2005; Madden, 2006;
Roppolo et al., 2007; Todd et al., 1998), or determine competence via a pre-determined
pass mark (e.g. 80%) or mean (Bobrow et al., 2011; Braslow et al., 1997; Fabius et al.,
1994; Teague & Riley, 2006; Todd et al., 1998).
The Madden (2006) study in nursing students where no participant was deemed
competent, yet 83% performed 15 out of the 18 skills in the assessment form correctly,
suggests that the number of skills assessed in the assessment form and how competence is
determined by the tool will ultimately determine the proportion of participants who are
deemed competent. There is therefore the possibility that the adoption of this 32
mandatory skill assessment form as determination of BLS competence in the current
study has set a higher than usual standard for achieving BLS competence. However, for a
potentially life-saving emergency service skill the researchers judged such a standard
appropriately justified.
To remove potential bias to any training group being evaluated, and standardise the
determination of skill competence, researchers should, where possible, use standardised
BLS assessment forms prescribed by their resuscitation council such as the Resuscitation
Council UK ―CPR assessment form‖ (Resuscitation Council (UK), or a standardised BLS
assessment method such as the Cardiff Assessment of Response and Evaluation (CARE)
Test (Donnelly et al., 1998, 2000; Lester et al., 1997; Whitfield et al., 2003). A small
number of studies have chosen this path to improve the comparability of results obtained
when evaluating various methods of BLS training (Bjorshol et al., 2009; Isbye et al.,
Chapter 5 — Discussion and Conclusions 136 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
2006; Mellor & Woollard, 2010; Monsieurs et al., 2004; Moule et al., 2008a; Nielson et
al., 2010; Woollard et al., 2004). Potentially this would have been desirable in the current
study to eliminate any potential comparability issues with comparative literature.
BLS assessor reliability.
In BLS assessments, assessor reliability is a further potential area for bias (Jensen et
al., 2008; Kaye & Mancini, 1998; Lynch et. al., 2008; Makinen et al., 2007b; Ringsted et
al., 2007; Van Berkom & Noordergraaf, 2008). However this was controlled for in the
current study by engaging expert accredited BLS assessors. Assessor reliability was
assessed by having a proportion (17%) of BLS assessments being simultaneously
assessed by the researcher and assessors. One hundred percent agreement in the
competent/not competent rating and ordinal scale grading (1 = not competent to 5 =
outstanding competence) of the dual assessments conducted confirms the inter-rater
reliability of these accredited BLS assessors (see Appendix D).
Automated manikin.
Akin to the issues raised concerning the currency of the CD and Traditional
programs, is the issue of the manikin used for the current project. A number of past
studies have used both assessor and manikin ratings to evaluate the BLS procedure (see
for example Braslow et al.,1997; Donnelly et al., 1998; Nielson et al., 2010; Todd et al.,
1998, 1999; Whitfield et al., 2003), and this was also the intention for this study.
However, during the conducting of the BLS assessments it was noted that the manikin
printout for ventilation volume, compression depth and ventilation:compression ratio for
some participants were either not recorded by the manikin or very low or ―impossible‖
readings were recorded. For example readings such as 2:44, 1:15 for ventilation:
compression ratios were recorded by the manikin that was not substantiated by the human
assessor‘s rating. These limitations in the manikin data resulted in only a small amount of
data being available for analysis. A decision not to include manikin data in the results of
this project was therefore reached.
The accuracy of ventilation rate and volumes, and compression depth recorded by
automated manikins has also been reported to be variable in the literature (Oh et al.,
2008). In the Oh et al. (2008) study which employed the Laerdal PC Skill Reporter™
Resusci Anne® manikin, the researchers omitted reporting ventilation volume outcomes in
the study results because the manikin did not provide accurate ventilation volumes when
Chapter 5 — Discussion and Conclusions 137 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
chest compressions and ventilation were simultaneously performed. Furthermore, in the
Oh et al. (2008) study, compression depths recorded by the manikin were significantly
below recommended ARC standard which could possibly also imply recording anomalies
consistent with those encountered in the current study.
These accuracy concerns did not however arise in the Lynch et al. (2008) study
where high degrees of accuracy in ventilation skills (rate and volume) between the
manikin and assessor were found. Interestingly, the Lynch et al. (2008) and Oh et al.
(2008) studies both employed the Laerdal PC Skill Reporter™
manikin, (a more
sophisticated manikin then the Laerdal Skill Reporter™
, 2002 model used in the current
project which provided only print out data).
This variability could be possibly explained by many recording manikins containing
both CPR sensing function and a metal chest which allowed for defibrillation practice.
The metal chest appeared to make the chest wall of the manikin much stiffer and different
from human chest resistance (Nysaether, Dorph, Rafoss, & Steen, 2008; Tsitlik et al.,
1983). These differences between various models of manikins and human chests have
been noted in the literature (see for example Baubin, Gilly, Posch, Schinnerl, & Kroesen,
1995; Noordergraaf, Gelder, Kesteren, Diets, & Savelkoul, 1997; Tsitlik et. al., 1983;
Wenzel, Lehmkuhl, Kubilis, Idris, & Pichlmayr, 1997) and sheds light on the manikin‘s
inability in the current project to consistently record readings. It has been suggested in
the literature that manikins need to become considerably more sophisticated in their
force-depth profiles before they adequately reflect the human chest (Arbogast et al., 2009;
Nysaether et al., 2008). Until this occurs, disparity between training and adequate
performance at events will continue and CPR technique targets will continue to be
difficult to correlate with performance of BLS on victims (Arbogast et al., 2009;
Nysaether et al., 2008).
In the some recent models of automated manikins, which supersede both the
Laerdal Skill Reporter™
and the Laerdal PC Skill Reporter™
manikins, the metal chest
required for defibrillation practice has been removed from some of the models which
allow for CPR sensing. According to the manufacturers, this is in response to difficulties
with the CPR sensing functions in models which contain the metal chest and an economic
strategy that has allowed for increased diversity in the models of manikins now available.
Chapter 5 — Discussion and Conclusions 138 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Whether this change will produce improved accuracy in manikin recordings of ventilation
and compression skills will need to be seen. Considering the relatively small number of
studies which have investigated manikin/assessor rating of CPR performance and the
discrepancies identified between these study outcomes, further research into the accuracy
and comparability of manikin and assessor ratings are needed.
A number of methodological issues in the current study‘s findings have been
discussed. The limitations are predominately around currency of practice assessments
due to the dynamic nature of resuscitation practice and research. Currency issues must be
noted but changes to practice are inevitable over time. What is of importance is that the
CD used in this project was current during the data collection of this project and the
groups were comparable. The main findings therefore remain essentially sound and
relevant to current training practice.
Furthermore, endeavouring to evaluate this method of BLS CD-manikin training,
which does not appear to have been evaluated previously, is of merit considering the
identified failings of current methods and the large number of both health professionals
and lay people requiring training. Few studies have also extended their enquiry to include
evaluation of participants‘ BLS knowledge post training, and trainees‘ perception of this
form of training. These study findings therefore extend our understanding of the BLS
training experience and outcomes.
Implications for Practice
The implications for practice from this study‘s findings and the evaluation of the
available literature are threefold. Firstly, as BLS is a life saving skill, it is concerning that
post training skill deficits in both health professional and lay people continue. Skills are
too often below the training industry 80% mastery standard. Health professionals have a
duty to continue to foster an improvement in this unsatisfactory situation. As such, re-
design and development of innovative BLS programs which consistently improve upon
BLS skill and knowledge training outcomes continue to be needed.
Secondly, the lack of retention of BLS skill and knowledge over time suggests the
continued need for frequent practice and evaluation of skill on a regular basis. For this to
be feasible, training and practice methods need to be efficient and convenient.
Chapter 5 — Discussion and Conclusions 139 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Thirdly, there are a number of gaps in the literature with all the BLS training
methods evaluated suggesting that the potential of available methods is still not
completely understood. This prompts the recommendation for continued research, which
is guided by the skills training literature (summarised in chapter two).
BLS training.
The best way or ways to maximise resuscitation performance through education and
training is yet to be found. The challenge that lies ahead is to identify the optimal way to
use available teaching technologies to maximise training and performance outcomes.
A suggested future approach to BLS training.
The low program effectiveness seen in the current study in Novices and Practising Nurses
and in corresponding literature suggests that all current BLS program outcomes need to
be monitored to ensure that programs consistently achieve high training effectiveness.
For programs where this is occurring, research needs to establish whether these programs
are suitable for both health professionals and lay people or whether in fact separate
programs are needed for these groups. Once researchers have established the validity of
various training programs health services managers and decision makers within
accrediting bodies need to take research findings into consideration when making
decisions about which training programs are offered to whom. For internationalisation,
standardisation of these courses across countries is recommended as a means to
maintaining an improved high standard of post training competence. This standardised
framework needs to extend to include an instructor training program so that accredited
instructors uniformly delivery the program. Overall monitoring of the standardised
program by an authority body such as a resuscitation council would also be a necessary
component of the standardised framework to maintain outcomes. The AHA has
attempted to establish a standardised framework like the one that is being suggested (i.e.
Heartsaver AED and AHA BLS for Healthcare providers programs), but BLS skill
competence post training is variable with particularly low competence reported with the
AHA BLS for Healthcare providers program (Cason et al., 2009; Kardong-Edgren et al.,
2010; Mancini et al., 2009; Roppolo et al., 2007, 2011). This highlights the importance of
the development of programs that consistently achieve high skill competence prior to
widespread standardisation.
Chapter 5 — Discussion and Conclusions 140 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The potential of CD BLS programs.
As the identification of an effective training program using the CD medium
continues to be elusive, innovative methods of training which have the capacity to
improve upon the training effectiveness and efficiency of currently available methods
need to continue to be sought (ILCOR, 2005; Hazinski et al., 2010; Mancini et al., 2010).
Effective training must improve depressed outcomes and inadequate retention of skill, as
well as more efficiently meet the needs of the large number of both health professional
and lay people who require proficiency in BLS skill.
The CD evaluated in the current study was developed ten years ago. It is thus ―old
technology‖ that was not designed to have a manikin available for independent practice.
Yet the study‘s findings still indicate that a CD-based BLS program which allows for
manikin practice can produce comparative BLS training results to Traditional methods in
Novices and Practising Nurses. It is therefore possible that developing a CD-based BLS
program which includes the Video/DVD kit within the CD could improve BLS training
outcomes. This kind of tool would take advantage of the design of the Video/DVD kit
programs which utilise the simplified approach to training currently advocated (ILCOR,
2005, Mancini et al., 2010). An accompanying section of the CD could allow for the
inclusion of additional information (i.e. AED, bag-mask maintenance and use)
particularly but not exclusively relevant to health professionals. The development of such
a CD/DVD-manikin program would prompt participants throughout the CD to engage in
independent manikin practice while viewing the CD. This program approach would take
advantage of the improved initial BLS skill outcomes seen with DVD programs (Bjorshol
et al., 2009; Cason et al., 2009; Chung et al., 2010; Mancini et al., 2009; Nielsen et al.,
2010; Roppolo et al., 2007). It could also provide potential benefits in BLS knowledge
outcomes, as seen in the Practising Nurse cohort of the current study, and some CD and
Internet programs (Creutzfeldt et al., 2009; Fabius et al., 1994; Moule et al., 2008a;
Moule & Gilchrist, 2002; Reder et al., 2006; Teague & Riley, 2006). The development of
a program of this nature could potentially improve upon results obtained from currently
available training methods, and be relatively easily distributed widely through retail and
internet access.
Multimedia approaches to training allow for a greater breadth of audience to be
reached relatively cheaply. This reduces the need for small group training at set times as
Chapter 5 — Discussion and Conclusions 141 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
occurs with Traditional methods. The large numbers of health professional and lay
people who need to be trained and reaccredited yearly world-wide are therefore an
incentive for continued exploration into Multimedia approaches to training. Redesign of
CD-based BLS training programs as outlined above could potentially assist in this
endeavour.
Frequent practice.
As BLS skill appears to decline rapidly regardless of training method, frequent
practice, regular assessment to identify when further training is advocated, and close
monitoring of training programs must be vigilantly pursued by training organisations and
health-care facilities to ensure that this life-saving skill is performed consistently to a high
standard of practice (Hazinski et al., 2010; Mancini et al., 2010; Oermann, Kardong-
Edgren, & Odom-Maryon, 2011). The current study and review of available literature,
seems to indicate that methods which consistently improve BLS skill retention remain
elusive. Frequent practice is thought to assist with retention of skill (ARC & NZRC,
2010a; Hazinski et al., 2010; Mancini et al., 2010; Oermann et al., 2011). Multimedia-
manikin programs, which can be accessed at a time of the trainee‘s choosing, facilitate the
feasibility of frequent manikin practice. Timely, individualised feedback when it is
possible to practise on automated manikins, also should enhance the value of frequent
practice (Bohn et al., 2011; Kardong-Edgren et al., 2010; Roppolo et al., 2011; Skorning
et al., 2010; Spooner et al., 2007; Sutton et al., 2007; Wik, Myklebust, Austad, & Steen,
2002; Wik et al., 2001). This is especially relevant as the sophistication of feedback
devices improve and may also be of benefit in Multimedia-manikin kits.
BLS manikin training kits and automated manikins, which allow for practice during
training, ongoing follow-up practice and feedback, should therefore be promoted for
individuals and organisations as a feasible way of encouraging regular updating of BLS
skills. However to ensure compliance, the importance of regular practice needs to be
emphasised in training programs, and convenient ways to facilitate regular practice needs
to be provided for those who require the skill.
Recommendations for Further Research
Evaluation of CD-based and Traditional BLS training methods in the current study
and review of the BLS training literature suggests that most Multimedia approaches
Chapter 5 — Discussion and Conclusions 142 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
(including CD) are only as effective as Traditional training methods, and that most
methods have limited effectiveness. Additionally, methods which consistently improve
BLS skill retention particularly remain difficult to identify. Further exploration and
evaluation into alternative BLS training methods therefore continues to be required, with
priority being given to the review of methods which are thought to potentially improve on
retention rates and provide guidance as to how often reaccreditation should be
undertaken. Future research therefore needs to be innovative, inclusive, and cover areas
sparsely or not researched previously.
A systematic approach.
Identification of the best way to utilise current teaching approaches to improve BLS
training outcomes and skill retention is a priority. Generally, research of Multimedia BLS
training methods have concentrated on initial training outcomes in the lay population.
Research which systematically evaluates CD, DVD, and Internet BLS programs are
needed particularly for the health professional group.
The most conclusive way of conducting a systematic controlled evaluation would be
a study that includes all current Multimedia approaches, as well as programs which are
multi-model, with the Traditional program as a control. In order for there to be improved
understanding of the effect sizes involved, further research could usefully include
assessment of skill and knowledge at three points: pre-training; initial post testing; and
follow up assessment at set points post training (e.g. 3 months, 6 months).
To ensure that the research is relevant to current practices, it should also include the
evaluating of ventilation apparatus (such as one-way valve masks and bag-mask systems),
and AEDs which are relatively recent additions to the BLS procedure (ILCOR, 2005b,
2005d). Trainees‘ self-rating of their skill and evaluation of their perceptions of the
various training methods, which have also been omitted in much of the literature would
further enhance a broader understanding of the relative benefits and most effective
methods of training. If in this research low program effectiveness and poor retention is
identified then the study should be extended to investigate the skill decrement in the study
participants.
Chapter 5 — Discussion and Conclusions 143 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
CD training methods.
Specifically, the limited amount of research into the effectiveness of CD-based BLS
training programs highlights the need to extend understanding of the capabilities of the
CD training method. Developing and evaluating a combined CD-DVD program as
discussed above would particularly exploit potential solutions implied from the current
findings and recent DVD outcomes.
The findings of the current project relate to students of nursing and practising nurses
with an average of only one year experience post graduation. Therefore research which
evaluates CD-based BLS programs for nurses with extensive experience (i.e. greater than
five years experience post graduation), as well as other health professionals and various
lay populations utilising comparable methodologies are also needed.
DVD-manikin systems and Internet programs.
The growing body of evidence which supports BLS DVD training programs that
incorporate a manikin for independent practice for initial BLS skill acquisition in
particularly but not exclusively health professionals (Bjorshol et al., 2009; Cason et al.,
2009; Chung et al., 2010; Lynch et al., 2005; Roppolo et al., 2007) should inspire
continued enquiry into the DVD-manikin method. The potential for extending DVD and
other Multimedia program outcomes with automated manikins, such as the VAM, in these
kits is also of interest (Kardong-Edgren et al., 2010; Roppolo et al., 2011) and needs
further evaluation. Studies which evaluate pre and post BLS knowledge as well as skill
levels, and retention of skill and knowledge in various health professional populations are
also notably absent currently in the DVD literature.
Furthermore, evaluation of Internet programs, animations and virtual world training,
are only most recently beginning to emerge. Understanding of the capacity of website
Internet programs, along with the capacity of CD and DVD programs distributed through
the Internet needs to be fully evaluated. Skill and knowledge acquisition in both health
professional and lay people initially post training and over time are needed to determine
the value of Internet programs within the overall approach to improving BLS training
outcomes.
Chapter 5 — Discussion and Conclusions 144 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Future directions.
The mechanisms behind sub-optimal BLS performance.
The literature and the current project outcomes suggest that low program efficiency
and suboptimal BLS skill and knowledge are a concern with all current training methods.
However, there is a lack of investigation into the mechanisms behind this observed skill
decrement. Future research therefore needs not only to pursue innovative methods of
training but also needs to seek to provide explanation for the identified sub-optimal
performance of BLS in both health professionals and lay populations. Particularly
important to understand are the reasons for the decrement in skill over time.
It was outside the scope of this project to further investigate the identified low
program effectiveness of the evaluated BLS CD-based and Traditional programs.
However, in view of this study‘s findings and the BLS performance literature, future
studies which evaluate BLS training methods should extend the design of projects to
include the provision for extensive evaluation of the identified BLS performance of each
participant. This could be achieved by interviewing or surveying study participants post
evaluation of the training program.
Psychological factors on BLS performance.
It has also been outside the scope of this project to evaluate, in any detail,
psychological and social environment influences on BLS performance, particularly
declining performance over time post-training. Future work to improve the quality of
BLS training and its outcomes should consider both the psychological and BLS training
literature. A considerable body of research has accumulated in the psychological
literature about: learning styles; the comprehensibility of instructions; optimisation of
practice; age-related and attention constraints on learning and memory; its correlation
with skill mastery; and the influences of factors such as interest, motivation, and attitudes
on learning and behavioural intentions (Dwyer & Williams, 2002; Finn, 2010; Lynch &
Einspruch, 2010; Marteau et al., 1989; Makinen, Niemi-Murola, Kaila, & Castren, 2009;
Spader, 2008). An example of this literature is Hopstock‘s (2008) evaluation of hospital
staff which found that BLS training that is based on adult learning models increases
participant‘s motivation to seek training and retain skills. It is therefore plausible that
Chapter 5 — Discussion and Conclusions 145 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
applying this psychological research to BLS training may greatly inform and potentially
enhance the effectiveness of BLS training methods in the future.
Potential expansion of BLS training.
The BLS procedure is considered to be not only a practical rehearsal for the
management of cardiac arrest, but also a valuable approach to the assessment of any
medical emergency (Maclaren, 2010). Recent literature suggests that BLS skill training
and assessment could potentially expand to include management of the deteriorating
patient and therefore the prevention of arrests (Van Berkon & Noordergraaf, 2008). BLS
training and assessment within these broader boundaries would therefore start with a
critically ill patient, perhaps still talking, breathing and with a pulse, deteriorating to a
patient in need of full resuscitation. The virtual world training programs discussed in
chapter two points to early enquiry in this area (Creutzfeldt et al., 2008, 2009, 2010).
Future research could potentially evaluate health professionals‘ skills in overall
resuscitation management which includes both the deteriorating and arrested patient.
Modern automated manikins, feedback devices and simulation centres are making this
type of training and therefore research more feasible (Edelson et al., 2008; Moule,
Wilford, Sales, & Lockyer, 2008b; Van Berkom et al., 2008; Van Berkom &
Noordergraaf, 2008; Wang et al., 2008). But such expansion, while it is an exciting
prospect, would best be based on a more complete understanding of how to deliver BLS
training that reliably leads to both high-level mastery immediately post training and
acceptable retention of BLS skill and knowledge over time.
Conclusion
A CD-based BLS program has been shown to be comparable to a more resource-
intensive Traditional BLS training program in Novice and Practising Nurses. However,
competence generally is less than optimal and suggests the need for renewed efforts to
develop and evaluate BLS training programs that can achieve high rates of competence
with acceptable retention over time.
What we therefore know from the current findings and the corresponding literature
is that we are yet to identify the best way or ways to maximise resuscitation performance
through education and training in both health professionals and lay people. The challenge
Chapter 5 — Discussion and Conclusions 146 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
that lies ahead is to identify through research the optimal way to use available teaching
technologies to improve BLS training outcomes and skill retention. When identified, this
approach needs to be standardised across countries and monitored by an authoritative
body to ensure maintenance of the prescribed standard.
A potential for improved initial skill outcomes with the Video/DVD manikin
approach, and potentially improved BLS knowledge with CD and Internet programs
suggests combining the methods as a possible step forward. Further research which
evaluates all Multimedia approaches, in particularly the CD and DVD, more thoroughly
in both the lay and health professional groups, pre, post training and at varied intervals
over-time, continues to be required to validate the findings of this project and to
determine training approaches that reliably improve upon these currently available
methods.
The increased availability and promotion of frequent manikin practice which, where
possible, includes feedback is also important as part of a potential overall solution. The
greater breadth of audience that can be reached relatively cheaply, and the large numbers
of health professional and lay people who need to be trained and reaccredited yearly
world-wide is an ongoing incentive to continued exploration of Multimedia approaches to
training.
BLS is a life saving skill, and as such, patient outcomes are dependent on the
quality of the BLS skills delivered. Consequently, having trainees develop adequate BLS
skills, and retain these skills is of on-going importance. Expanded enquiry into BLS
training, skill and knowledge outcomes is therefore well warranted from a public health
perspective.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
References
Aguinis, H., & Kraiger, K. (2009). Benefits of training and development for individuals
and teams, organisations, and society. Annual Review of Psychology, 60, 451-474.
doi: 10.1146/annurev.psych.60.110707.163505
Aldossary, A., Yassin, A., & Kurashi, N.Y. (2007). The effects of cardiopulmonary
resuscitation training to mobile patrols' knowledge, attitude, and practice, Dammam
area, Kingdom of Saudi Arabia. The Middle East Journal of Emergency Medicine,
7(1), 24-27. Retrieved from http://www.hmc.org.qa/mejem/
Andresen, D., Arntz, H. R., Grafling, W., Hoffmann, S., Hofmann, D., & Kraemer, R.
(2008). Public access resuscitation program including defibrillator training for
laypersons: a randomized trial to evaluate the impact of training course duration.
Resuscitation, 76(3), 419-424. doi: 10.1016/j.resuscitation.2007.08.019
Anonymous. (2005). Bystander CPR: a new video-based training program delivers the
right message to the right people. Journal of Emergency Medical Services, 30(12),
18-19. Retrieved from http://www.jems.com/
Anthonypillai, F. (1992). Retention of advanced cardiopulmonary resuscitation
knowledge by intensive care trained nurses. Intensive & Critical Care Nursing, 8(3),
180-184. doi:10.1016/0964-3397(92)90025-F
Arbogast, K. B., Nishisaki, A., Balasubramanian, S., Nysaether, J., Niles, D., Sutton,
R. M., . . . Nadkarni, V. M. (2009). Expert clinical assessment of thorax stiffness of
infants and children during chest compressions. Resuscitation, 80(10), 1187-1191.
doi: 0.1016/j.resuscitation.2009.07.005
Arthur, W., Bennett, W., Edens, P. S., & Bell, S. T. (2003). Effectiveness of Training in
organisations: a meta-analysis of design and evaluation features. Journal of Applied
Psychology, 88(2), 234-245. doi: 10.1037/0021-9010.88.2.234
Austin & Repatriation Medical Centre (A&RMC). (2000). Basic life support assessment
form. Melbourne, Australia: Nursing Education & Research Centre, A& RMC.
References 148 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Austin & Repatriation Medical Centre (A&RMC). (1999). Basic life support [CD].
Melbourne, Australia: HealthQuest International, (a division of the A&RMC).
Australian College of Critical Care Nurses, & Australian Resuscitation Council (ARC).
(2008). Resuscitation standards for clinical practice and education provision: a
resource for health professionals – A joint statement. Melbourne, Australia:
Australian Resuscitation Council, March 2008. Retrieved from
http://www.resus.org.au/
Australian Resuscitation Council (ARC). (1997) Guideline 7 – Cardiopulmonary
resuscitation: Revised policy statement. Melbourne, Australia: Australian
Resuscitation Council, November 1997. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC). (2002) Guideline 7 – Cardiopulmonary
resuscitation: Revised policy statement. Melbourne, Australia: Australian
Resuscitation Council, June 2002. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC). (2004a) Guideline 11.1.1– Protective devices
for rescue breathing: Policy statement. Melbourne, Australia: Australian
Resuscitation Council, November 2004. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC). (2004b) Guideline 10.1.3– Public access
defibrillation (PAD): Policy statement. Melbourne, Australia: Australian
Resuscitation Council, November 2004. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC). (2006). Cardiopulmonary resuscitation:
Australian Resuscitation Council guideline 2006. Emergency Medicine Australasia,
18, 332-334. doi: 10.1111/j.1742-6723.2006.00888.x
Australian Resuscitation Council (ARC). (2007a) Guideline 9.1.1 Cardiopulmonary
resuscitation training. Melbourne, Australia: Australian Resuscitation Council,
February 2007. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC). (2007b) Guideline 11.1.1– CPR for advanced
life support providers. Melbourne, Australia: Australian Resuscitation Council, May
2007. Retrieved from http://www.resus.org.au/
References 149 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Australian Resuscitation Council (ARC), & Resuscitation Council (RC) UK. (2007).
Immediate life support course, Melbourne, Australia: Royal Australasian College of
Surgeons. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010a) Guideline 10.1 – Basic life support (BLS) training. Melbourne, Australia:
Australian and New Zealand Committee on Resuscitation, December 2010. Retrieved
from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010b) Guideline 8 – Cardiopulmonary resuscitation. Melbourne, Australia:
Australian and New Zealand Committee on Resuscitation, December 2010. Retrieved
from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010c) Guideline 11.1.1 – Cardiopulmonary resuscitation for advanced life support
providers. Melbourne, Australia: Australian and New Zealand Committee on
Resuscitation, December 2010. Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010d) Guideline 11.1 – Introduction to advanced life support. Melbourne,
Australia: Australian and New Zealand Committee on Resuscitation, December 2010.
Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010e) Guideline 1.4 –Principles and format for developing guidelines. Melbourne,
Australia: Australian and New Zealand Committee on Resuscitation, December 2010.
Retrieved from http://www.resus.org.au/
Australian Resuscitation Council (ARC), & New Zealand Resuscitation Council (NZRC).
(2010f) Guideline 1.3 –Process for developing resuscitation guidelines. Melbourne,
Australia: Australian and New Zealand Committee on Resuscitation, December 2010.
Retrieved from http://www.resus.org.au/
Baessler, C. (2000). Are educational interventions enough for retention of
cardiopulmonary resuscitation techniques? Critical Care Medicine, 28(9), 3363-
3364. doi: 10.1097/00003246-200009000-00050
References 150 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Batcheller, A. M., Brennan, R. T., Braslow, A., Urrutia, A., & Kaye, W. (2000).
Cardiopulmonary resuscitation of subjects over forty is better following half-hour
video self-instruction compared to traditional four-hour classroom training.
Resuscitation, 43(2), 101-110. doi:10.1016/S0300-9572(99)00132-X
Baubin, M. A., Gilly, H., Posch, A., Schinneri, A., & Kroesen, G. A. (1995).
Compression characteristics of CPR manikins. Resuscitation, 30(2), 117-126.
doi:10.1016/0300-9572(95)00874-S
Betz, A. E., Callaway, C. W., Hostler, D., Rittenberger, J. C. (2008). Work of CPR during
two different compression to ventilation ratios with real-time feedback.
Resuscitation, 79(2), 230-233. doi:10.1016/j.resuscitation.2008.06.016
Bjorshol, C. A. (1996). Cardiopulmonary resuscitation skills. A survey among health and
rescue personnel outside hospital [English abstract]. Tidsskrift for Den Norske
Laegeforening, 166(4), 508-511. Retrieved from http://tidsskriftet.no/
Bjorshol, C.A., Lindner, T.W., Soreide, E., Moen, L., & Sunde, K. (2009). Hospital
employees improve basic life support skills and confidence with a personal
resuscitation manikin and a 24-min video instruction. Resuscitation, 80(8), 898-902.
doi:10.1016/j.resuscitation.2009.06.009
Block, J. H. (1971). Mastery learning: theory and practice, New York, NY: Holt,
Rinehart and Winston.
Bobrow, B. J., Vadeboncoeur, T. F., Spaite, D. W., Potts, J., Denninghoff, K., Chikani,
V., . . . Abella, B. S. (2011). The effectiveness of ultrabrief and brief educational
videos for training lay responders in hands-only cardiopulmonary resuscitation:
Implications for the future of citizen cardiopulmonary resuscitation training.
Circulation: Cardiovascular Quality & Outcomes, 4(2), 220-128. doi:
10.1161/CIRCOUTCOMES.110.95935
Bohn, A., & Gude, P. (2008). Feedback during cardiopulmonary resuscitation. Current
Opinion in Anaesthesiology, 21 (2), 200-203. doi: 10.1097/ACO.0b013e3282f63f12
Bohn, A., Weber, T. P., Wecker, S., Harding, U., Osada, N., Van Aken, H., & Lukas, R.
P. (2011). The addition of voice prompts to audiovisual feedback and debriefing does
not modify CPR quality or outcomes in out of hospital cardiac arrest – A prospective,
References 151 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
randomized trial. Resuscitation, 82(3), 257-262.
doi:10.1016/j.resuscitation.2010.11.006
Bolle, S.R., Scholl, J., & Gilbert, M. (2009). Can video mobile phones improve CPR
quality when used for dispatcher assistance during simulated cardiac arrest? Acta
Anaesthesiologica Scandinavica, 53(1), 116-120. doi: 10.1111/j.1399-
6576.2008.01779.x
Braslow, A., Brennan, R. T., Newman, M. M. Bircher, N. G., Batcheller, A. M., & Kaye,
W. (1997). CPR training without an instructor: development and evaluation of a
video self-instructional system for effective performance of cardiopulmonary
resuscitation. Resuscitation, 34(3), 207-220. doi:10.1016/S0300-9572(97)01096-4
Braun, O. (2002). Maximising skills retention- current educational theory supports online
CPR training. Occupational Health & Safety, 71(12), 40-43. Retrieved from
http://ohsonline.com/
Brennan, R. T., & Braslow, A. (1998). Are we training the right people yet? A survey of
participants in public cardiopulmonary resuscitation classes. Resuscitation, 37(1), 21-
25. doi:10.1016/S0300-9572(98)00026-4
Brennan, R. T., Braslow, A., Batcheller, A. M., & Kaye, W. (1996). A reliable and valid
method for evaluating cardiopulmonary resuscitation training outcomes.
Resuscitation, 32(2), 85-93. doi:10.1016/0300-9572(96)00967-7
Broomfield, R. (1996). A quasi-experimental research to investigate the retention of basic
cardiopulmonary resuscitation skills and knowledge by qualified nurses following a
course in professional development. Journal of Advanced Nursing, 23(5), 1016-1023.
Retrieved from www.journalofadvancednursing.com/
Campbell, D. T., & Stanley, J. C. (1966). Experimental and quasi-experimental designs
for research. Chicago, IL: Rand McNaly College Publishing Co.
Campbell, J.P. (1971). Personnel training and development. Annual Review of
Psychology, 22, 565-602. doi: 10.1146/annurev.ps.22.020171.003025
Cason, C. L., Kardong-Edgren, S., Cazzell, M., Behan, D., & Mancini, M. E. (2009).
Innovations in basic life support education for healthcare providers: improving
References 152 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
competence in cardiopulmonary resuscitation through self-directed learning. Journal
for nurses in staff development (JNSD): official journal of the National Nursing Staff
Development Organization. 25 (3), E1-E13. doi: 10.1097/NND.0b013e3181a56f92
Cazzell, M.A. (2008). The effects of different CPR training upon the adequacy of the
chest compressions. Southern Online Journal of Nursing Research, 8, (2), 413.
Retrieved from www.snrs.org/
Chamberlain, D. A., & Hazinski, M. F. (2003). ILCOR Advisory Statement: Education in
Resuscitation an ILCOR symposium. Circulation, 108(20), 2575-2594.
doi:10.1161/01.CIR.0000099898.11954.3B
Choa, M., Cho, J., Choi, Y. H., Kim, S., Sung, J. M., & Chung, H. S. (2009). Animation-
assisted CPRII program as a reminder tool in achieving effective one-person-CPR
performance. Resuscitation, 80(6), 680-684. doi:10.1016/j.resuscitation.2009.03.019
Choa, M., Park, I., Chung, H. S., Yoo, S. K., Shim, H., & Kim, S. (2008). The
effectiveness of cardiopulmonary resuscitation instruction: Animation versus
dispatcher through a cellular phone. Resuscitation, 77(1), 87-94.
doi:10.1016/j.resuscitation.2007.10.023
Choa, M. H., Park, I. C., Yoon, Y. S., Kim, S. H., & Yoo, S. K. (2006). Internet-based
animation for instruction in cardiopulmonary resuscitation. Journal of Telemedicine
& Telecare, 12(Suppl 3), 31-33. doi:10.1258/135763306779380075
Christenson, J., Nafziger, S., Compton, S., Vijayaraghavan, K., Slater, B., Ledingham, R.,
. . . McBurnie, M. A. (2007). The effect of time on CPR and automated external
defibrillator skills in the Public Access Defibrillation Trial. Resuscitation, 74(1), 52-
62. doi:10.1016/j.resuscitation.2006.11.005
Chung, C. H., Siu, A. Y. C., Po, L. L. K., Lam, C. Y., & Wong, P. C. Y. (2010).
Comparing the effectiveness of video self-instruction versus traditional classroom
instruction targeted at cardiopulmonary resuscitation skills for laypersons: A
prospective randomised controlled trial. Hong Kong Medical Journal, 16(3), 165-
170. Retrieved from http://www.hkmj.org/
Clark, L. J. R., Watson, J., Cobbe, S. M., Reeve, W., Swann, I. J. & Macfarlene, P. W.
(2000). CPR ‗98‘ A practical multimedia computer-based guide to cardiopulmonary
References 153 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
resuscitation for medical students. Resuscitation, 44(2), 109-117. doi:10.1016/S0300-
9572(99)00171-9
Cohen J. (1988). Statistical Power Analysis for Behavioural Sciences, (2nd
ed.). New
York, NY: Academic Press.
Cook, R. J., Pedley, D. K., & Thakore, S. (2006). A structured competency based training
programme for junior trainees in emergency medicine: the "Dundee Model".
Emergency Medicine Journal, 23(1), 18-22. doi:10.1136/emj.2005.025072
Cooper, J. A., & Cooper, J. M. (2008). New strategies for cardiopulmonary resuscitation.
Current Treatment Options in Cardiovascular Medicine, 10(1), 49-58. doi:
10.1007/s11936-008-0006-0
Covell, C. L. (2006). BCLS certification of the nursing staff: an evidence-based approach.
Journal of Nursing Care Quality, 21(1), 63-69. Retrieved from
http://journals.lww.com/jncqjournal/pages/currenttoc.aspx
Cowie, D. A., & Story, D. A. (2000). Knowledge of cardiopulmonary resuscitation
protocols and level of anaesthetic training. Anaesthesia and Intensive Care, 28, 687-
691. Retrieved from www.aaic.net.au/
Creutzfeldt, J., Hedman, L., Medin, C., Wallin, C.J., & Fellander-Tsai, L.(2008). Effects
of repeated CPR training in virtual worlds on medical students' performance. Studies
in Health Technology & Informatics, 132, 89-94. Retrieved from
http://www.booksonline.iospress.nl/Content/View.aspx?piid=64
Creutzfeldt, J., Hedman, L., Medin, C., Stengard, K., & Fellander-Tsai, L. (2009).
Retention of knowledge after repeated virtual world CPR training in high school
students. Studies in Health Technology & Informatics, 142, 59-61. doi: 10.3233/978-
1-58603-964-6-59
Creutzfeldt, J., Hedman, L., Medin, C., Heinrichs, W. L., & Fellander-Tsai, L. (2010).
Exploring virtual worlds for scenario-based repeated team training of
cardiopulmonary resuscitation in medical students Journal of Medical Internet
Research, 12(3), E38. doi: 10.2196/jmir.1426
References 154 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Cummins, R. O., & Hazinski, M. F. (1999). Cardiopulmonary resuscitation techniques
and instruction: when does evidence justify revision? Annals of Emergency Medicine,
34(6), 780-784. doi:10.1016/S0196-0644(99)70105-8
Cummins, R. O., & Hazinski, M. F. (2000). The most important changes in the
international ECC and CPR guidelines 2000. Resuscitation, 46(1-3), 431-437.
doi:10.1016/S0300-9572(00)00301-4
Dent, T. H., & Gillard, J. H. (1993). Cardiopulmonary resuscitation: effectiveness,
training and survival. Journal of the Royal College of Physicians of London, 27(4),
354-355. Retrieved from http://www.rcplondon.ac.uk/resources/clinical-medicine-
journal
Devlin, M. (1999). An evaluative study of the basic life support skills of nurses in an
independent hospital. Journal of Clinical Nursing, 8(2), 201-205. doi:
10.1046/j.1365-2702.1999.00247.x
Dine, C. J., Gersh, R. E., Leary, M., Riegel, B. J., Bellini, L. M., & Abella, B. S. (2008).
Improving cardiopulmonary resuscitation quality and resuscitation training by
combining audiovisual feedback and debriefing Critical Care Medicine. 36(10),
2817-22. doi: 10.1097/CCM.0b013e318186fe37
Done, M. L., & Parr, M. (2002). Teaching basic life support skills using self-directed
learning, a self-instructional video, access to practice manikins and learning in pairs.
Resuscitation, 52(3), 287–291. doi:10.1016/S0300-9572(01)00449-X
Donnelly, P., Assar, D., & Lester, C. (2000). A comparison of manikin CPR performance
by lay persons trained in three variations of basic life support guidelines.
Resuscitation, 45(3), 195-199. doi:10.1016/S0300-9572(00)00186-6
Donnelly, P. D., Lester, C. A., Morgan, C. L., & Assar, D. (1998). Evaluating CPR
performance in basic life support: The VIDRAP protocol. Resuscitation, 36(1), 51-
57. doi:10.1016/S0300-9572(97)00092-0
Doyle, D. J. (2002). CD-ROM Review: ACLS HeartCode. Canadian Journal of
Anesthesia, 49(9), 997-999. doi: 10.1007/BF03016891.

References 155 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Dwyer, T., & Williams, M. L. (2002). Nurses‘ behaviour regarding CPR and the theories
of reasoned action and planned behaviour. Resuscitation, 52(1), 85-90.
doi:10.1016/S0300-9572(01)00445-2
Edelson, D. P., Litzinger, B., Arora, V., Walsh, D., Kim, S., Lauderdale, D. S., . . .
Abella, B. S. (2008). Improving in-hospital cardiac arrest process and outcomes with
performance debriefing. Archives of Internal Medicine, 168(10), 1063-1069.
Retrieved from http://WWW.ARCHINTERNMED.COM
Einspruch, E. L., Lynch, B., Aufderheide, T. P., Nichol, G., & Becker, L. (2007).
Retention of CPR skills learned in a traditional AHA Heartsaver course
versus 30-min video self-training: A controlled randomized study. Resuscitation,
74(3), 476-486. doi:10.1016/j.resuscitation.2007.01.030
Fabius, B. D., Grissom, L. E., & Fuentes, A. (1994). Recertification in Cardiopulmonary
Resuscitation: a comparison of two teaching methods. Journal of Nursing Staff
Development, 10(5), 262-268. Retrieved from http://journals.lww.com/jnsdonline/
Farah, R., Stiner, E., Zohar, Z., Zveibil, F., & Eisenman, A. (2007). Cardiopulmonary
resuscitation surprise drills for assessing, improving and maintaining
cardiopulmonary resuscitation skills of hospital personnel. European Journal of
Emergency Medicine, 14(6), 332-336. doi: 10.1097/MEJ.0b013e328285d6d6
Finn, J. (2010). E-learning in resuscitation training - students say they like it, but is there
evidence that it works? Comment on: Resuscitation, 81(7), 877-881.
doi:10.1016/j.resuscitation.2010.03.019; Source: Resuscitation. 81(7), 790-791.
doi:10.1016/j.resuscitation.2010.05.010
Friesen, L. & Stotts, N. A. (1984). Retention of basic cardiac life support content: The
effect of two teaching methods. Journal of Nursing Education, 23(5), 184–191.
Retrieved from http://www.slackjournals.com/jne
Frkovic, V., Sustic, A., Zeidler, F., Protic, A., & Desa, K. (2008). A brief re-education in
cardiopulmonary resuscitation after six months-the benefit from timely repetition.
Signa Vitae, 3(2), 24-28. Retrieved from http://www.signavitae.com/
References 156 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Gabbott, D., Smith, G., Mitchell, S., Colquhoun, M., Nolan, J., Soar, J., . . . Spearpoint,
K. (2005). Cardiopulmonary resuscitation standards for clinical practice and training
in the UK. Resuscitation, 64(1), 13-19. doi:10.1016/j.resuscitation.2004.11.001
Garvey, J. (1999). Skill decay in basic life support. Resuscitation, 37(2), S21.
doi:10.1016/S0300-9572(98)00061-6
Gasco, C., Avellanal, M., & Sanchez, M. (2000). Cardiopulmonary resuscitation training
for students of odontology: skills acquisition after two periods of learning.
Resuscitation, 45(3), 189-194. doi:10.1016/S0300-9572(00)00178-7
Gee, K. (1993). Cardiopulmonary resuscitation: basic life support skills…part 2. British
Journal of Nursing, 2(2), 138-141.Retrieved from
http://www.britishjournalofnursing.com/
Goldstein, I. L. (1980). Training in work organisations. Annual Review of Psychology, 31,
229-272. doi: 10.1146/annurev.ps.31.020180.001305
Goodwin, A. P. (1992). Cardiopulmonary resuscitation training revisited. Journal of the
Royal Society of Medicine, 85(8):452-453. Retrieved from
http://www.jrsm.rsmjournals.com/
Greig, M., Elliott, D., Parboteeah, S., & Wilks, L. (1996). Basic life support skill
acquisition and retention in student nurses undertaking a pre-registration diploma in
higher education nursing course. Nurse Education Today, 16(1), 28-31.
doi:10.1016/S0260-6917(96)80089-X
Grzeskowiak, M. (2006). The effects of teaching basic cardiopulmonary resuscitation - A
comparison between first and sixth year medical students. Resuscitation, 68(3), 391-
397. doi:10.1016/j.resuscitation.2005.07.017
Hagemann, I. S. (2007). A careful look at community CPR training. Missouri Medicine,
104(6), 481-484. Retrieved from
http://www.msma.org/mx/hm.asp?id=MissouriMedicine
Hagyard-Wiebe, T. (2007). Should critical care nurses be ACLS-trained? Dynamics, 18
(4), 28-31. Retrieved from http://www.caccn.ca/en/publications/dynamics/index.html
References 157 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Hamasu, S., Morimoto, T., Kuramoto, N., Horiguchi, M., Iwami, T., Nishiyama, C., . . .
Hiraide, A. (2009). Effects of BLS training on factors associated with attitude toward
CPR in college students. Resuscitation, 80(3), 359-364.
doi:10.1016/j.resuscitation.2008.11.023
Hamilton, R. (2005). Nurses‘ knowledge and skill retention following cardiopulmonary
resuscitation training: a review of the literature. Journal of Advanced Nursing, 51(3),
288-297. Retrieved from http://www.journalofadvancednursing.com/
Handley, A. J. (1997). Basic Life Support. British Journal of Anaesthesia, 79, 151-158.
doi:10.1093/bja/79.2.151
Handley, A. J., Monsieurs, K. G., & Bossaert, L. L. (2001). European Resuscitation
Council guidelines 2000 for adult basic life support. Resuscitation, 48(3), 199-205.
doi:10.1016/S0300-9572(00)00377-4
Harris, P., Nagy, S., & Vardaxis, N. (Ed.) (2006). Mosby’s Dictionary of Medicine,
Nursing & Health Professions [Australian & New Zealand Edition]. Sydney,
Australia: Mosby Elsevier Australia.
Hazinski, M. F. Co-Chair, Nolan, J. P. Co-Chair, Billi, J. E., Bottiger, B. W., Bossaert, L.,
de Caen, A. R., . . . Zideman, D. (2010). Part 1: Executive summary: 2010
International Consensus on cardiopulmonary resuscitation and emergency
cardiovascular care science with treatment recommendations. Circulation, 122(16),
S250-S275, October 19, 2010. doi: 10.1161/CIRCULATIONAHA.110.970889
Hekelman, F. P., Phillips, J. A., & Bierer, L. A. (1990). An interactive videodisk training
program in basic cardiac life support: implications for staff development. Journal of
Continuing Education in Nursing, 21(6), 245-247. Retrieved from
http://www.jcenonline.com/
Henderson, B. N. II. (1992). Alternative methods of ventilation during CPR training of
the dental team using a bag-mask technique. Texas Dental Journal, 109(3), 7-10.
Retrieved from http://www.tda.org/
References 158 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Higdon, T. A., Heidenreich, J. W., Kern, K. B., Sanders, A. B., Berg, R. A., Hilwig, R.
W., . . . Ewy, G. A. (2006). Single rescuer cardiopulmonary resuscitation: can anyone
perform to the guidelines 2000 recommendations? Resuscitation, 71(1), 34-39.
doi:10.1016/j.resuscitation.2006.02.020
Hopstock, L.A. (2008). Motivation and adult learning: a survey among hospital personnel
attending a CPR course. Resuscitation,76(3), 425-430.
doi:10.1016/j.resuscitation.2007.09.011
Hurst, V., West, S., Austin, P., Branson, R., & Beck, G. (2007). Comparison of
ventilation and chest compression performance by bystanders using the impact model
730 ventilator and a conventional bag valve with mask in a model of adult
cardiopulmonary arrest. Resuscitation, 73(1), 123-130.
doi:10.1016/j.resuscitation.2006.07.027
International guidelines 2000 for CPR and ECC (ILCOR): Part 1 - A consensus on
science. (2000a). Resuscitation, 46(1-3), 3-15. doi:10.1016/S0300-9572(00)00269-0
International guidelines 2000 for CPR and ECC (ILCOR): Part 3: adult basic life support.
(2000b). Resuscitation, 46(1-3), 29-71. doi:10.1016/S0300-9572(00)00271-9
International Liaison Committee on Resuscitation (ILCOR) (2005a). International
collaboration in resuscitation medicine. Resuscitation, 67(2-3), 163-165.
doi:10.1016/j.resuscitation.2005.09.009
International Liaison Committee on Resuscitation (ILCOR) (2005b). International
consensus on cardiopulmonary resuscitation (CPR) and emergency cardiovascular
care (ECC) science with treatment recommendations, Part 1: Introduction.
Resuscitation, 67(2-3), 181-186. doi:10.1016/j.resuscitation.2005.09.010
International Liaison Committee on Resuscitation (ILCOR) (2005c). International
consensus on cardiopulmonary resuscitation (CPR) and emergency cardiovascular
care (ECC) science with treatment recommendations, Part 2: Adult basic life support.
Resuscitation, 67(2-3), 187-201. doi:10.1016/j.resuscitation.2005.09.016
References 159 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
International Liaison Committee on Resuscitation (ILCOR) (2005d). International
consensus on cardiopulmonary resuscitation (CPR) and emergency cardiovascular
care (ECC) science with treatment recommendations, Part 3: Defibrillation.
Resuscitation, 67(2-3), 203-211. doi:10.1016/j.resuscitation.2005.09.017
International Liaison Committee on Resuscitation (ILCOR) (2005e). International
consensus on cardiopulmonary resuscitation (CPR) and emergency cardiovascular
care (ECC) science with treatment recommendations, Part 8: Interdisciplinary topics.
Resuscitation, 67(2-3), 305-314.doi:10.1016/j.resuscitation.2005.09.021
International Liaison Committee on Resuscitation (ILCOR) (2005f). Past and present:
Compiled by the founding members of the international liaison committee on
resuscitation. Resuscitation, 67(2-3), 157-161.
doi:10.1016/j.resuscitation.2005.05.011
International Liaison Committee on Resuscitation (ILCOR) (2005g). The evidence
process for the 2005 International consensus on cardiopulmonary resuscitation (CPR)
and emergency cardiovascular care (ECC) science with treatment recommendations.
Resuscitation, 67(2-3), 167-170. doi:10.1016/j.resuscitation.2005.09.007
Isbye, D. L., Rasmussen, L. S., Lippert, F. K., Rudolph, S. F., & Ringsted, C. V. (2006).
Laypersons may learn basic life support in 24 min using a personal resuscitation
manikin. Resuscitation, 69(3), 435-442. doi:10.1016/j.resuscitation.2005.10.027
Issenberg, S. B. (2002). Clinical skills training – Training makes perfect. Medical
Education, 36, (3), 210-211. doi: 10.1046/j.1365-2923.2002.01157.x
Jones, I., Handley, A. .J., Whitfield, R., Newcombe, R., & Chamberlain, D. (2007). A
preliminary feasibility study of a short DVD-based distance-learning package for
basic life support. Resuscitation,.75(2), 350-356.
doi:10.1016/j.resuscitation.2007.04.030
Josipovic, P., Webb, M., & McGrath, I. (2009). Basic life support knowledge of
undergraduate nursing and chiropractic students. Australian Journal of Advanced
Nursing, 26(4), 58-63. Retrieved from http://www.ajan.com.au/ajan_27.html
References 160 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Kakora-Shiner, N. (2009). Using ward-based simulation in cardiopulmonary training.
Nursing Standard, 23(38), 42-47. Retrieved from
http://nursingstandard.rcnpublishing.co.uk/
Kallestedt, M. L. S., Rosenblad, A., Leppert, J., Herlitz, J., & Enlund, M. (2010). Hospital
employees' theoretical knowledge on what to do in an in-hospital cardiac arrest
Scandinavian Journal of Trauma, Resuscitation & Emergency Medicine, 18, 43-50.
Retrieved from http://www.sjtrem.com/
Kardong-Edgren, S., Oermann, M., Odom-Maryon, T., & Ha, Y. (2010). Comparison of
two instructional modalities for nursing student CPR skill acquisition. Resuscitation,
81(8), 1019-1024. doi:10.1016/j.resuscitation.2010.04.022
Kaye, W., & Mancini, M. E. (1998). Teaching adult resuscitation in the United States:
Time for a rethink. Resuscitation, 37(3), 177-187. doi:10.1016/S0300-
9572(98)00052-5
Khan, J.A., Shafquat, A., & Kundi, A. (2010). Basic life support skills: Assessment and
education of spouse and first degree relatives of patients with coronary disease.
Journal of the College of Physicians and Surgeons Pakistan, 20(5), 299-302.
Retrieved from http://www.cpsp.edu.pk/
Kirves, H., Skrifvars, M. B., Vahakuopus, M., Ekstrom, K., Martikainen, M., & Castren,
M. (2007). Adherence to resuscitation guidelines during prehospital care of cardiac
arrest patients. European Journal of Emergency Medicine, 14(2), 75-81. Retrieved
from http://www.eusem.org/journal/
Kobayashi, M., Fujiwara, A., Morita, H., Nishimoto, Y., Mishima, T., Nitta, M., . . . Sato,
K. (2008). A manikin-based observational study on cardiopulmonary resuscitation
skills at the Osaka Senri medical rally. Resuscitation, 78(3), 333-339.
doi:10.1016/j.resuscitation.2008.03.230
Krahn, R.E. (2011). Basic life support: A call for re-evaluation by nurse educators.
Nursing Education Perspectives, 32(2), 128. doi: 10.5480/1536-5026-32.2.128
Laerdal. (2002). Resusci Anne®
Modular System – Directions for use. Stavanger, Norway:
Laerdal Medical.
References 161 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Latham, G. P. (1988). Human resource training and development. Annual Review of
Psychology, 39, 545-582. doi: 10.1146/annurev.ps.39.020188.002553
Leary, M., & Abella, B. S. (2008). The challenge of CPR quality: Improvement in the real
world. Resuscitation, 77(1), 1-3. doi:10.1016/j.resuscitation.2008.02.005
Lee, H. M., Cho, K. H., Choi, Y. H., & Yoon, S. Y. (2008). Can you deliver accurate tidal
volume by manual resuscitator? Emergency Medicine Journal. 25(10), 632-634.
doi:10.1136/emj.2007.053678
Lester, C. A., Morgan, C. L., Donnelly, P. D., & Assar, D. (1997). Assessing with CARE:
an innovative method of testing the approach and casualty assessment components of
basic life support, using video recording. Resuscitation, 34(1), 43-49.
doi:10.1016/S0300-9572(96)01046-5
Lewis, D. (1997). CPR for Windows. Computers in Nursing, 15(6), 281-288. Retrieved
from http://journals.lww.com/cinjournal/pages/default.aspx
Lewis, F. H., Kee, C. C., & Minick, M. P. (1993). Revisiting CPR knowledge and skills
among registered nurses. The Journal of Continuing Education in Nursing. 24(4),
174–179. Retrieved from http://www.slackjournals.com/jcen
Liberman, M., Golberg, N., Mulder, D., & Sampalis, J. (2000). Teaching
cardiopulmonary resuscitation to CEGEP students in Quebec—a pilot project,
Resuscitation, 47(3), 249–257. doi:10.1016/S0300-9572(00)00236-7
Livingston. S. A., & Zieky, M. J. (1982). Passing Scores: A Manual for Setting Standards
of Performance on Educational and Occupational Tests, Princeton, NJ: Educational
Training Service. Retrieved from http://www.ets.org/
Lorem, T., Steen, P. A., & Wik, L. (2010). High school students as ambassadors of CPR:
A model for reaching the most appropriate target population? Resuscitation,81(1),
78-81. doi:10.1016/j.resuscitation.2009.09.030
Lüscher, F., Hunziker, S., Gaillard, V., Tschan, F., Semmer, N., Hunziker, P., &, Marsch,
S. (2010). Proficiency in cardiopulmonary resuscitation of medical students at
graduation: a simulator based comparison with general practitioners. Swiss Medical
Weekly, 140(3/4), 57 – 61. Retrieved from http://www.smw.ch
References 162 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Lynch, B., & Einspruch, E. L. (2010). With or without an instructor, brief exposure to
CPR training produces significant attitude change. Resuscitation, 81(5), 568-575.
doi:10.1016/j.resuscitation.2009.12.022
Lynch, B., Einspruch, E., Nichol, G., Becker, L. Aufderheide, T., & Idris, A. (2005).
Effectiveness of a 30-minute CPR self-instruction program for lay responders: a
controlled randomized study. Resuscitation, 67(1), 31–43.
doi:10.1016/j.resuscitation.2005.04.017
Lynch, B., Einspruch, E. L., Nichol, G., & Aufderheide, T. P. (2008). Assessment of BLS
skills: Optimizing use of instructor and manikin measures. Resuscitation, 76(2), 233-
243. doi:10.1016/j.resuscitation.2007.07.018
Maclaren, H. (2010). Why do we practice CPR?. British Journal of General Practice.
60(571), 130-131. doi: 10.3399/bjgp10483210
Madden C. (2006). Undergraduate nursing students‘ acquisition and retention of CPR
knowledge and skills. Nurse Education Today, 26(3), 218-227.
doi:10.1016/j.nedt.2005.10.003
Mahony, P. H., Griffiths, R. F., Larsen, P., & Powell, D. (2008). Retention of knowledge
and skills in first aid and resuscitation by airline cabin crew. Resuscitation, 76(3),
413-418. doi:10.1016/j.resuscitation.2007.08.017
Makinen, M., Aune, S., Niemi-Mrola, L., Herlitz, J., Varpula, T., Nurmi, J., . . . Castren,
M. for the ECCE Study Group. (2007a). Assessment of CPR-D skills of nurses in
Goteborg, Sweden and Espoo, Finland: Teaching leadership makes a difference.
Resuscitation, 72(2), 264-269. doi:10.1016/j.resuscitation.2006.06.032
Makinen, M., Axelsson, A., Castren, M., Nurmi, J., Lankinen, I., & Niemi-Murola L.
(2010). Assessment of CPR-D skills of nursing students in two institutions: reality
versus recommendations in the guidelines. European Journal of Emergency
Medicine, 17(4), 237-239. Retrieved from http://www.eusem.org/journal/
Makinen, M., Niemi-Murola, L., Makela, M., & Castren, M. for the ECCE Study Group.
(2007b). Methods of assessing cardiopulmonary resuscitation skills: A systematic
review. European Journal of Emergency Medicine, 14(2), 108-114. Retrieved from
http://www.eusem.org/journal/
References 163 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Makinen, M., Niemi-Murola, L., Kaila, M., & Castren, M. (2009). Nurses' attitudes
towards resuscitation and national resuscitation guidelines: Nurses hesitate to start
CPR-D. Resuscitation, 80(12), 1399-1404. doi:10.1016/j.resuscitation.2009.08.025
Mancini, M. E., & Kaye, W. (1985). The effect of time since training on house officers‘
retention of cardiopulmonary resuscitation skills. American Journal of Emergency
Medicine, 3(1), 31-32. doi:10.1016/0735-6757(85)90008-7
Mancini, M. E., Cazzell, M., Kardong-Edgren, S., & Cason, C. L. (2009). Improving
workplace safety training using a self-directed CPR-AED learning program. AAOHN
Journal, 57(4), 159-67; quiz 168-9. Retrieved from http://www.aaohnjournal.com/
Mancini, M. E. Co-Chair, Soar, J. Co-Chair, Bhanji, F., Billi, J. E., Dennett, J., Finn, J., . .
Morley, P. T. Education, Implementation, and Teams Chapter Collaborators. (2010).
Part 12: Education, Implementation, and Teams 2010 International consensus on
cardiopulmonary resuscitation and emergency cardiovascular care science with
treatment recommendations. Circulation, 122(16), S539-S581. doi:
10.1161/CIRCULATIONAHA.110.971143
Marteau, T. M., Johnston, M., Wynne, G., & Evans, T. R. (1989). Cognitive factors in the
explanation of the mismatch between confidence and competence in performing
basic life support. Psychology and Health, 3(3),173-182.
doi:10.1080/08870448908400377
Marzooq, H., & Lyneham, J. (2009). Cardiopulmonary resuscitation knowledge among
nurses working in Bahrain. International Journal of Nursing Practice, 15(4), 294-
302. doi: 10.1111/j.1440-172X.2009.01752.x
McClelland, H. (2007). Research review. Comments on:Makinen, M., Aune, S., Niemi-
Murola, L., Herlitz, J., Varpula, T., Nurmi, J. . . . Castren, M. for the ECCE Study
Group. (2007) "Assessment of CPR-D skills of nurses in Goteborg, Sweden and
Espoo, Finland: Teaching leadership makes a difference." Resuscitation, 72, 264-269.
doi:10.1016/j.resuscitation.2006.06.032. Source: Accident and Emergency Nursing,
15(2), 112-113. doi:10.1016/j.aaen.2007.02.001
References 164 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Mellor, R., & Woollard, M. (2010). Skill acquisition by health care workers in the
Resuscitation Council (UK) 2005 guidelines for adult basic life support. International
Emergency Nursing, 18(2), 61-66. doi:10.1016/j.ienj.2009.08.003
Miyadahira, A. M. (2001). Motor capacities involved in the psychomotor skills of the
cardiopulmonary resuscitation technique: recommendations for the teaching-learning
process [English Abstract]. Revista Da Escola de Enfermagem Da Usp, 35(4):366-
73. Retrieved from http://www.ee.usp.br/reeusp/
Miyadahira, A. M. K., Quilici, A. P., Martins, C. C., de Araújo, & G. L., Pelliciotti, J. S.
S. (2008). Cardiopulmonary resuscitation with semi-automated external defibrillator:
assessment of the teaching-learning process [Portuguese & English]. Revista da
Escola de Enfermagem da USP, 42 (3): 532-8. Retrieved from
http://www.ee.usp.br/reeusp/
Monsieurs, K. G., Vogels, C., Bossaert, L. L., Meert, P., Manganas, A., Tsiknakis, M., . . .
Giorgini, F. (2004). Learning effect of a novel interactive basic life support CD: the
JUST system. Resuscitation, 62(2), 159-165. doi:10.1016/j.resuscitation.2004.02.014
Morley, P. T. Co-Chair, Atkins, D. L. Co-Chair, Billi, J. E., Bossaert, L., Callaway, C.
W., de Caen, A. R., . . . Zideman, D. (2010). Part 3: Evidence Evaluation Process
2010 International consensus on cardiopulmonary resuscitation and emergency
cardiovascular care science with treatment recommendations. Circulation, 122(16),
S283-S290. doi: 10.1161/CIRCULATIONAHA.110.970947
Morrison, H., McNally, H., Wylie, C., McFaul, P., & Thompson, W. (1996). The passing
score in the objective structured clinical examination. Medical Education, 30(5), 345-
348. doi: 10.1111/j.1365-2923.1996.tb00845.x
Moser, D. K., & Coleman, S. (1992). Recommendations for improving cardiopulmonary
resuscitation skills retention. Heart & Lung, 21(4), 372-380. Retrieved from
http://www.heartandlung.org/
Moser, D., & Hurley, M. L. (2007). CPR: one nurse's wake-up call. RN, 70(4), 31-33.
Retrieved from http://www.rnweb.com
References 165 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Moule, P. (2002). Evaluation of the basic life support CD-ROM: its effectiveness as
learning tool and user experiences. Journal of Educational Technology & Society,
5(3), 163-174. Retrieved from http://www.ifets.info/
Moule, P., Albarran, J. W., Bessant, E., Brownfield, C., & Pollock, J. (2008a). A non-
randomized comparison of e-learning and classroom delivery of basic life support
with automated external defibrillator use: A pilot study. International Journal of
Nursing Practice, 14(6), 427-434. doi:10.1111/j.1440-172X.2008.00716.x
Moule, P., Gilbert, P., & Chalk, V. (2001). A multimedia approach to teaching basic life
support – the development of a CD-ROM. Nurse Education in Practice, 1(2), 73-79.
doi:10.1054/nepr.2001.0013
Moule, P., & Gilchrist, M. (2001). An evaluation of a basic life support CD-ROM. Health
Informatics Journal, 7(1), 29-36. doi: 10.1177/146045820100700106
Moule, P., Wilford, A., Sales, R., & Lockyer, L. (2008b). Student experiences and mentor
views of the use of simulation for learning. Nurse Education Today, 28(7), 790-797.
doi:10.1016/j.nedt.2008.03.007
Nielsen, A., Henriksen, M., Isbye, D., Lippert, F., & Rasmussen, L. (2010). Acquisition
and retention of basic life support skills in an untrained population using a personal
resuscitation manikin and video self-instruction (VSI). Resuscitation, 81 (9), 1156-
1160. doi:10.1016/j.resuscitation.2010.06.003
Nikandish, R., Jamshidi, H., Musavifard, R., Zebardast, T., & Habibi, N. (2007). Basic
cardiopulmonary resuscitation skills of nurses at a teaching hospital in Southeast Iran
in 2006 [letter to the editor]. Resuscitation, 73, 321-322. doi:
10.1016/j.resuscitation.2006.12.016
Niles, D., Sutton, R. M., Donoghue, A., Kalsi, M. S., Roberts, K., Boyle L., Nishisaki,
A., Arbogast, K. B., Helfaer, M., & Nadkarni, V. (2009). "Rolling Refreshers": A
novel approach to maintain CPR psychomotor skill competence. Resuscitation, 80(8),
909-912. doi:10.1016/j.resuscitation.2009.04.021
Nolan, J.P. (2008). Basic life support. Current Opinion in Anaesthesiology, 21(2), 194-
199. doi: 10.1097/ACO.0b013e3282f49cb4
References 166 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Noordergraaf, G. J. Sabbe, M., Diets, R. F. Noordergraaf, A., & Van Hemelrijck, J.
(1999). Training needs and qualifications of anaesthesiologists not exposed to ALS.
Resuscitation, 40(3), 147-160. doi:10.1016/S0300-9572(99)00020-9
Noordergraaf, G. J., Van Gelder, J. M., Van Kesteren, R. G., Diets, R. F., & Savelkoul, T.
J. (1997). Learning cardiopulmonary resuscitation skills: Does the type of mannequin
make a difference. European Journal of Emergency Medicine, 4(4), 204-209.
Retrieved from http://www.eusem.org/journal/
Nysaether, J. B., Dorph, E., Rafoss, I., & Steen, P. A. (2008). Manikins with human-like
chest properties: A new tool for chest compression research. IEEE Transactions on
Biomedical Engineering, 55(11), 2643-2650. doi: 10.1109/TBME.2008.2001289
Oermann, M. H., Kardong-Edgren, S. E., & Odom-Maryon, T. (2011). Effects of monthly
practice on nursing students' CPR psychomotor skill performance. Resuscitation, 82
(4), 447-453. doi:10.1016/j.resuscitation.2010.11.022
Oh, J. H., Lee, S. J., Kim, S. E., Lee, K. J., Choe, J. W., & Kim, C. W. (2008). Effects of
audio tone guidance on performance of CPR in simulated cardiac arrest with an
advanced airway. Resuscitation, 79(2), 273-277.
doi:10.1016/j.resuscitation.2008.06.022
O'Steen, D. S., Kee, C. C., & Minick, M. P. (1996). The retention of advanced cardiac life
support knowledge among registered nurses. Journal of Nursing Staff Development,
12(2), 66–72. Retrieved from http://journals.lww.com/jnsdonline/
Osterwalder, J. J., & Schuhwerk, W. (1998). Effectiveness of mask ventilation in a
training manikin. A comparison between the Oxylator EM100 and the bag-valve
device. Resuscitation, 36(1), 23-27. doi:10.1016/S0300-9572(97)00091-9
Paal, P., Falk, M., Gruber, E., Beikircher, W., Ellerton, J., Kainz, H., . . . Brugger, H.
(2010). Effects of training time and feedback on ventilation skills in lay rescuers.
Emergency Medicine Journal, 27(4), 313-316. doi: 10.1136/emj.2008.069476
Pallant, J. (2007). SPSS survival manual, (3rd
ed.). Sydney, Australia: Allen & Unwin.
References 167 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Plank, C. H., & Steinke, K. R. (1989). Effect of two teaching methods on CPR retention.
Journal of Nursing Staff Development, 5(3), 145–147. Retrieved from
http://journals.lww.com/jnsdonline/
Preusch, M. R., Bea, F., Roggenbach, J., Katus, H. A., Junger, J., & Nikendei, C. (2010).
Resuscitation Guidelines 2005: Does experienced nursing staff need training and how
effective is it? American Journal of Emergency Medicine, 28(4), 477-484.
doi:10.1016/j.ajem.2009.01.040
Publication Manual of the American Psychological Association. (2010). (6th
ed.).
Washington D.C., USA: American Psychological Association.
Quinn, T., & Ord, L. (1996a). Cardiopulmonary resuscitation: knowledge for practice.
Nursing Times, 92(45), S1-4. Retrieved from
http://www.nursingtimes.net/publication-index/
Quinn, T., & Ord, L. (1996b). Cardiopulmonary resuscitation: knowledge for practice.
Nursing Times, 92(46), S5-8. Retrieved from
http://www.nursingtimes.net/publication-index/
Ranse, J., & Arbon, P. (2008). Graduate nurses' lived experience of in-hospital
resuscitation: A hermeneutic phenomenological approach. Australian Critical Care,
21 (1), 38-47. doi: 10.1016/j.aucc.2007.12.001
Rea, T. D., Stickney, R. E., Doherty, A., & Lank, P. (2010). Performance of chest
compressions by laypersons during the Public Access Defibrillation (PAD)Trial.
Resuscitation, 81(3), 293-296. doi:10.1016/j.resuscitation.2009.12.002
Reder, S., Cummings, P., & Quan, L. (2006). Comparison of three instructional methods
for teaching cardiopulmonary resuscitation and use of an automatic external
defibrillator to high school students. Resuscitation, 69(3), 443-453.
doi:10.1016/j.resuscitation.2005.08.020
Resuscitation Council (UK), 2006. Immediate Life Support Provider Course general
information. Retrieved from http://www.resus.org.uk
Reynolds, E. (2010). Basic life support. Nursing standard, 24(18), 59. Retrieved from
http://www.nursing-standard.co.uk/
References 168 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Richman, P. B., Bobrow, B. J., Clark, L., Noelck, N., & Sanders, A. B. (2007). Ability of
citizens in a senior living community to perform lifesaving cardiac skills and
appropriately utilize AEDs. Journal of Emergency Medicine,33(4), 395-399.
doi:10.1016/j.jemermed.2007.02.020
Riegel, B., Nafziger, S. D., McBurnie, M. A., Powell, J., Ledingham, R., Shehra, R., . . .
Henry, M. C. (2006). How well are cardiopulmonary resuscitation and automated
external defibrillator skills retained over time? Results from the Public Access
Defibrillation (PAD) Trial. Academic Emergency Medicine, 13(3), 254-263. doi:
10.1197/j.aem.2005.10.010
Ringsted, C., Lippert, F., Hesselfeldt, R., Rasmussen, M. B., Mogensen, S. S., Frost, T., . .
. Van der Vleuten, C. (2007). Assessment of advanced life support competence when
combining different test methods: Reliability and validity. Resuscitation, 75(1), 153-
160. doi:10.1016/j.resuscitation.2007.03.003
Rolfe, I. E., & Sanson-Fisher, R. W. (2002). Translating learning principles into practice:
A new strategy for learning clinical skills Medical Education, 36(4), 345-352. doi:
10.1046/j.1365-2923.2002.01170.x
Roppolo, L. P., Heymann, R., Pepe, P., Wagner, J., Commons, B., Miller, R., . . . Idris, A.
H. (2011). A randomized controlled trial comparing traditional training in
cardiopulmonary resuscitation (CPR) to self-directed CPR learning in first year
medical students: The two-person CPR study. Resuscitation, 82(3), 319-325.
doi:10.1016/j.resuscitation.2010.10.025
Roppolo, L. P., Pepe, P. E., Campbell, L., Ohman, K., Kulkarni, H., Miller, R., . . . Idris,
A. H. (2007). Prospective, randomized trial of the effectiveness and retention of 30-
min layperson training for cardiopulmonary resuscitation and automated external
defibrillators: The American Airlines study. Resuscitation, 74(2), 276-285.
doi:10.1016/j.resuscitation.2006.12.017
Roppolo, L. P., Wigginton, J. G., & Pepe, P. E. (2009). Revolving back to the basics in
cardiopulmonary resuscitation. Minerva Anestesiologica, 75(5), 301-305. Retrieved
from http://www.minervamedica.it/en/journals/minerva-anestesiologica/
References 169 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Salas, E., & Cannon-Bowers, J. A. (2001). The science of training: a decade of progress.
Annual Review of Psychology, 52, 471-499. doi: 10.1146/annurev.psych.52.1.471
Salas, E., & Kosarzycki, M. P. (2003). Why don‘t organisations pay attention to (and use)
findings from the science of training? Human Resource Development Quarterly,
14(4), 487-491. doi: 10.1002/hrdq.1081.
Salas, N., Wisor, B., Agazio, J., Branson, R., & Austin, P. N. (2007). Comparison of
ventilation and cardiac compressions using the Impact Model 730 automatic transport
ventilator compared to a conventional bag valve with a facemask in a model of adult
cardiopulmonary arrest. Resuscitation, 74(1), 94-101.
doi:10.1016/j.resuscitation.2006.01.023
Salmoni, A. W., Schmidt, R. A., & Walter, C. B. (1984). Knowledge of results and motor
learning: a review and critical reappraisal. Psychological Bulletin, 95(3), 355–386.
doi:10.1037/0033-2909.95.3.355
Salvucci, A. Jr. (2008). Literature review: feedback, debriefing effects on CPR. EMS
Magazine, 37(11), 22. Retrieved from http://www.emsresponder.com
Sarac, L., & Ok, A. (2010). The effects of different instructional methods on students'
acquisition and retention of cardiopulmonary resuscitation skills. Resuscitation,
81(5), 555-561, May 2010. doi:10.1016/j.resuscitation.2009.08.030
Sayre, M. R. Co-Chair, Koster, R. W. Co-Chair, Botha, M., Cave, D. M., Cudnik, M. T.,
Handley, A. J., . . . Travers, A. H., on behalf of the adult basic life support chapter
collaborators. (2010). Part 5: Adult Basic Life Support 2010 International consensus
on cardiopulmonary resuscitation and emergency cardiovascular care science with
treatment recommendations. Circulation, 122(16), S298-S324. doi:
10.1161/CIRCULATIONAHA.110.970996
Schellhammer, F. (2003). Do radiologists want/need training in cardiopulmonary
resuscitation. Acta Radiologica, 44(1), 56-58. doi: 10.1034/j.1600-
0455.2003.00005.x
References 170 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Schluger, J., Hayes, J. G., Turino, G. M., Fischman, S., & Fox, A. C. (1987). The
effectiveness of film and videotape cardiopulmonary resuscitation to the lay public.
New York State Journal of Medicine, 87(7), 382-385. Retrieved from
http://www.unboundmedicine.com/medline/ebm/journal/New_York_state_journal_of
_medicine
Seethala, R. R., Esposito, E. C., & Abella, B. S. (2010). Approaches to improving cardiac
arrest resuscitation performance. Current Opinion in Critical Care, 16(3), 196-202.
doi:10.1097/MCC.0b013e328338c121
Semeraro, F., Signore, L., & Cerchiari, E. L. (2006). Retention of CPR performance in
anaesthetists. Resuscitation, 68(1), 101-108. doi:10.1016/j.resuscitation.2005.06.011
Shindo, M., Goto, T., Shibano, K., Okabe, K., & Inaoka, K. (2009). Self-study supporting
CD-ROM materials to promote cardiopulmonary resuscitation training in school
situation [English abstract]. Medical Journal of Minami Osaka Hospital, 57(1), 19-
23. Retrieved from http://sciencelinks.jp/j-east/journal/M.php
Sitzmann, T., Kraiger, K., Stewart, D., & Wisher, R. (2006). The comparative
effectiveness of web-based and classroom instruction: a meta-analysis. Personnel
Psychology, 59(3), 623-664. doi: 10.1111/j.1744-6570.2006.00049.x
Skorning, M., Beckers, S. K., Brokmann, J. C., Rortgen, D., Bergrath, S., Veiser, T., . . .
Rossaint, R. (2010). New visual feedback device improves performance of chest
compressions by professionals in simulated cardiac arrest. Resuscitation, 81(1), 53-
58. doi:10.1016/j.resuscitation.2009.10.005
Smith, M. A. (2005). Cardiopulmonary resuscitation. Critical Care Nursing Clinics of
North America, 17(1), xv – xvi. doi:10.1016/j.ccell.2004.10.001
Smith, K. K., Gilcreast, D., & Pierce, K. (2008). Evaluation of staff's retention of ACLS
and BLS skills. Resuscitation, 78(1), 59-65. doi:10.1016/j.resuscitation.2008.02.007
Smith, P. J., Robertson, I., & Wakefield, L. (2002). Developing preparedness for flexible
delivery of training in enterprises. Journal of Workplace Learning, 14(5/6), 222 –
232. doi: 10.1108/13665620210441180
References 171 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Spader, C. (2008). Timing is everything: in-hospital defibrillation often is not started soon
enough, making the need for better systems painfully apparent. Nursing Spectrum –
Florida Edition, 18(6), 28-29. Retrieved from
http://www.helpatnursingspectrum.com/
Spooner, B. B., Fallaha, J. F., Kocierz, L., Smith, C. M., Smith, S. C. L., & Perkins, G. D.
(2007). An evaluation of objective feedback in basic life support (BLS) training.
Resuscitation, 73(3), 417-424. doi:10.1016/j.resuscitation.2006.10.017
Stromsoe, A., Andersson, B., Ekstrom, L., Herlitz, J., Axelsson, A., Goransson, KE., . . .
Holmberg, S. (2010). Education in cardiopulmonary resuscitation in Sweden and its
clinical consequences. Resuscitation, 81(2), 211-6.
doi:10.1016/j.resuscitation.2009.10.014
Sutton, R. M., Donoghue, A., Myklebust, H., Srikantan, S., Byrne, A., Priest, M., . . .
Nadkarni, V. (2007). The voice advisory manikin (VAM): An innovative approach to
paediatric lay provider basic life support skill education. Resuscitation, 75(1), 161-
168. doi:10.1016/j.resuscitation.2007.02.007
Swiger, F. (2001). KISS (Keep it simple, stupid) - - to save a life. Occupational Health &
Safety, 70(7):60-62, 64, 66-67. Retrieved from http://ohsonline.com/
Tan, E. C. T. H., Hekkert, K. D., Van Vugt, A. B., & Biert, J. (2009). Medical education
in first aid and basic life support in the Netherlands. Medical Teacher, 31(5), 465.
doi:10.1080/01421590903051315
Tannenbaum, S. I., & Yukl, G. (1992). Training and development in work organisations.
Annual Review of Psychology, 43, 399-441. doi:
10.1146/annurev.ps.43.020192.002151
Taylor, J. (2008). Why mandatory training needs resuscitating. Nursing Times, 104(10),
16-7, 10 March 2008. Retrieved from http://www.nursingtimes.net/publication-index/
Teague, G., & Riley, R. H. (2006). Online resuscitation training. Does it improve high
school students‘ ability to perform cardiopulmonary resuscitation in a simulated
environment. Resuscitation, 71(3), 352-357. doi:10.1016/j.resuscitation.2006.05.007
References 172 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Thoren, A., Axelsson, A., & Herlitz, J. (2007). DVD-based or instructor led CPR
education – A comparison. Resuscitation, 72(2), 333-336.
doi:10.1016/j.resuscitation.2006.09.013
Todd, K. H., Braslow, A., Brennan, R. T., Lowery, D. W., Cox, R. J., Lipscomb, L. E., &
Kellermann, A. L. (1998). Randomized, controlled trial of video self-instruction
versus traditional CPR training. Annals of Emergency Medicine, 31(3), 364 – 369.
doi:10.1016/S0196-0644(98)70348-8
Todd, K. H., Heron, S. L., Thompson, M., Dennis, R., O‘Connor, J., & Kellermann, A. L.
(1999). Simple CPR: A randomized, controlled trial of video self-instructional
cardiopulmonary resuscitation training in an African American church congregation.
Annals of Emergency Medicine, 34(6), 730–737. doi:10.1016/S0196-0644(99)70098-
3
Tsitlik, J. E., Weisfeldt, M. L., Chandra, N., Effron, M. B., Halperin, H. R., & Levin, H.
R. (1983). Elastic properties of the human chest during cardiopulmonary
resuscitation. Critical Care Medicine, 11(9), 685-691. Retrieved from
http://journals.lww.com/ccmjournal/pages/default.aspx
Turley, A. J., Bone, G., Garcia, L., & Gedney, J. (2005). Cardiopulmonary resuscitation
training: In need of some critical care? British Journal of Anaesthesia, 95(5), 721.
doi:10.1093/bja/aei610
Vaillancourt, C., Grimshaw, J., Brehaut, J. C., Osmond, M., Charette, M. L., Wells, G. A.,
& Stiell, I. G. (2008). A survey of attitudes and factors associated with successful
cardiopulmonary resuscitation (CPR) knowledge transfer in an older population most
likely to witness cardiac arrest: Design and methodology. BMC Emergency Medicine,
8, 13-23. Retrieved from http://www.biomedcentral.com/
Van Berkom, P., & Noordergraaf, G. J. (2008). Integrated resuscitation simulators should
retain "basic" options. Comment on: Resuscitation, 73(2):202-211.
doi:10.1016/j.resuscitation.2007.01.005; Source: Resuscitation, 76(3), 485-6. doi:
10.1016/j.resuscitation.2007.08.007
References 173 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Van Berkom, P. F. J., Noordergraaf, G. J., Scheffer, G. J., & Noordergraaf, A. (2008).
Does use of the CPREzy (TM) involve more work than CPR without feedback?
Resuscitation, 78(1), 66-70. doi:10.1016/j.resuscitation.2008.01.024
Van der Heide, P. A., van Toledo-Eppinga, L., van der Heide, M., & van der Lee, J. H.
(2006). Assessment of neonatal resuscitation skills: a reliable and valid scoring
system. Resuscitation, 71(2), 212-221. doi:10.1016/j.resuscitation.2006.04.009
Verplancke, T., De Paepe, P., Calle, P. A., De Regge, M., Van Maele, G., & Monsieurs,
K. G. (2008). Determinants of the quality of basic life support by hospital nurses.
Resuscitation, 77(1), 75-80. doi:10.1016/j.resuscitation.2007.10.006
Wang, E. E., Quinones, J., Fitch, M. T., Dooley-Hash, S., Griswold-Theodorson, S.,
Medzon, R., . . . Clay, L. (2008). Developing technical expertise in emergency
medicine: The role of simulation in procedural skill acquisition. Academic
Emergency Medicine, 15(11), 1046-1057. doi: 10.1111/j.1553-2712.2008.00218.x
Wayne, D. B., Butter, J., Siddall, V. J., Fudala, M. J., Wade, L. D., Feinglass, J. &
McGaghie, W. C. (2006). Mastery learning of advanced cardiac life support skills by
internal medicine residents using simulation technology and deliberate practice.
Journal of General Internal Medicine, 21(3), 251-256. doi: 10.1111/j.1525-
1497.2006.00341.x
Wayne, D. B., Fudala, M. J., Butter, J., Siddell, V. J., Feinglass, J., Wade, L. D., &
McGaghie, W. C. (2005). Comparison of two standard-setting methods for advanced
cardiac life support training. Acedemic Medicine, 80(10), S63-S66. Retrieved from
http://journals.lww.com/academicmedicine/pages/default.aspx
Wenzel, V., Lehmkuhl, P., Kubilis, P. S., Idris, A. H., & Pichlmayr, I. (1997). Poor
correlation of mouth-to-mouth ventilation skills after basic life support training and 6
months later. Resuscitation, 35(2), 129–134. doi:10.1016/S0300-9572(97)00044-0
West, H. (2000). Basic infant life support: retention of knowledge and skill. Paediatric
Nursing, 12, 34–37.Retrieved from
http://nursingchildrenandyoungpeople.rcnpublishing.co.uk/
Wexley, K. N. (1984). Personnel training. Annual Review of Psychology, 35, 519-551.
doi: 10.1146/annurev.ps.35.020184.002511
References 174 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Whitcomb, J. J., & Blackman, V. S. (2007). Cardiopulmonary resuscitation: How far have
we come? Dimensions of Critical Care Nursing, 26 (1): 1-8. Retrieved from
http://journals.lww.com/dccnjournal/pages/default.aspx
White, R. D. (2006). 2005 American Heart Association guidelines for cardiopulmonary
resuscitation: Physiological and educational rationale for changes. Mayo Clinic
Proceedings, 81(6), 736-740. doi:10.4065/81.6.736
Whitfield, R. H., Newcombe, R. G., & Woollard, M. (2003). Reliability of the Cardiff test
of basic life support and automated external defibrillation version 3.1. Resuscitation,
59(3), 291-314. doi:10.1016/S0300-9572(03)00246-6
Wik, L., Myklebust, H., Auestad, B. H., & Steen, P. A. (2002). Retention of basic life
support skills six months after training with an automated voice advisory manikin
system without instructor involvement. Resuscitation, 52(3), 273-279.
doi:10.1016/S0300-9572(01)00476-2
Wik, L., Thowsen, J., & Steen, P. A. (2001). An automated voice advisory manikin
system for training in basic life support without an instructor. A novel approach to
CPR training. Resuscitation, 50(2), 167–172. doi:10.1016/S0300-9572(01)00331-8
Wilkinson, J., & Chu, S. (1999). Development of an effective model for delivery of
continuing professional education programs for Division 1 Registered Nurses on the
staff of the Austin and Repatriation Medical Centre. [Unpublished Research
Proposal]. Melbourne, Australia: Nursing Education & Research Centre, Austin &
Repatriation Medical Centre.
Wilson, J. (1994). CPR training based on practice that ensures reliable performance?
Occupational Health & Safety, 63(10), 152-156, October 1994. Retrieved from
http://ohsonline.com/
Woollard, M., Whitfield, R., Smith, A., Colquhoun, M., Newcombe, R.G., Vetter, N., &
Chamberlain, D. (2004). Skill acquisition and retention in automated external
defibrillator (AED) use and CPR by lay responders: a prospective study.
Resuscitation, 60(1), 17–28. doi:10.1016/j.resuscitation.2003.09.006

References 175 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Woollard, M., Whitfield, R., Newcombe, R. G., Colquhoun, M., Vetter, N., &
Chamberlain, D. (2006). Optimal refresher training intervals for AED and CPR
skills: a randomized controlled trail. Resuscitation, 71(2), 237-247.
doi:10.1016/j.resuscitation.2006.04.005
Zaheer, H., & Haque, Z. (2009). Awareness about BLS (CPR) among medical students:
Status and requirements. Journal of the Pakistan Medical Association, 59(1), 57-59.
Retrieved from http://www.jpma.org.pk/
References 176 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Website Addresses
Australian Red Cross: http://www.redcross.org.au/default.asp
Australian Resuscitation Council: http://www.resus.org.au/
American Heart Association website: http://www.americanheart.org
Community Services & Health Industry Skill Council:
http://www.cshisc.com.au/index.php
European Resuscitation Council (UK): www.resus.org.uk
ILCOR: http://www.erc.edu/index.php/ilcor/en/
Resuscitation Council (UK): http://www.resus.org.uk
Surf Life Saving Australia: http://www.sls.com.au/getinvolved/first-aid
St John Ambulance Australia: http://www.stjohnvic.com.au/
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix A1
La Trobe University Human Ethics Approval
Appendices 178 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan

Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix A2
Austin & Repat Medical Centre Human Research Ethics
Committee Approval
Appendices 180 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendices 181 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix A3
Permission to use Austin & Repat Medical Centre BLS CD
and BLS Assessment Form

Appendices 183 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix A4
Ethical considerations

Appendices 185 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Ethical Considerations
Participant confidentiality.
The data record forms (BLS training time allocation, questionnaire, BLS assessment, and
program evaluation forms), and electronic copies did not identify individual participants. Each
participant was allocated a number, which they recorded on the forms used. All data was kept
separately from the list of names and code numbers, which was kept in a locked cabinet in the
supervisor‘s office in the School of Public Health. Participants were assured that they would not
be identified in any report or publication arising from the study. No information capable of
identifying a particular individual will be published or reported in any other form.
As successful completion of a BLS assessment was a course requirement, a copy of the
BLS assessment form, with the inclusion of the participant‘s name, was provided to the university
/ hospital, to be retained in the participant‘s personnel/student file retained by the institution.
Participation numbers allocated in the study were removed on the copy provided for the
participant‘s file. No other information relating to their participation appeared in this confidential
file. The above measures ensured individual‘s confidentiality.
During project.
Data record forms were stored in a locked filing cabinet located within the School of Public
Health. Only the supervisor and researcher had access to the cabinet. However, during analysis
and write up of the study, data needed to be kept at the researcher‘s home. In this circumstance
the researcher ensured that the data record forms were secured within a locked filing cabinet and
computer records were kept in a password protected computer to which only the researcher has
access. Personal identifying information did not appear on data sheets or electronic copies and
codes linking individuals to data were stored separately in a locked cabinet.
Following completion of project.
On completion of the study, all data will be kept securely at the university for seven years.
Authorised persons within the university or hospital may inspect participant‘s records for
purposes of data audit (e.g. Ethics committee, regulatory bodies). After seven years the data
record sheets will be destroyed, computer records deleted and any other paper records destroyed.

Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix B1
Participant information and consent form

Appendices 187 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
La Trobe University Participant Information & Consent Form
Project Title:
An Alternative Approach to the Delivery of Education for Health Professionals1.
Senior Investigator: Dr Jane Pierson
School of Public Health
La Trobe University
Researcher: Karen Mardegan
Professional Doctorate Student
School of Public Health
La Trobe University
What is the Research Project about?
As part of my professional doctorate studies at La Trobe University, I am conducting a research study that
aims to evaluate the effectiveness of the compact disc (an electronic data storage device) as a nursing
education delivery method. In order to evaluate the CD approach, the project will compare Traditional
lecture/demonstration Basic Life Support (BLS) training with a newly developed BLS training CD
produced by the Austin & Repatriation Medical Centre (A&RMC). It is hoped that this project will
demonstrate that educational CDs can at the very least support Traditional educational delivery methods if
not supersede them.
Why am I being asked to be in this research project?
Basic Life Support (BLS) skills training and assessment is currently a required component of the A&RMC
Graduate Nurse Year program. However, participation in this research study is entirely voluntary. If you
chose not to participate, you will still be able to complete the BLS skills training and required assessment
during allocated class time, and you will therefore not be disadvantaged or inconvenienced in any way if
you choose not to participate in, or to withdraw from, the study.
What do I need to do to be in this research project?
Participants in the study will be randomly assigned to one of two BLS skills training programs (Traditional
or CD). The Traditional program (which runs in class time), consists of a practise/demonstration tutorial,
and takes two hours in total. These sessions will be held in allocated classrooms at the A&RMC. The CD
program provides participants with access to the BLS CD and a Resusci Anne® Manikin. Participants in the
CD program will attend viewing sessions totalling two hours. These sessions will be held in the computer
lab at the Austin or Repatriation campus. The two hours is equivalent to the current time commitment
required in the BLS component of graduate nurse year program.
On completion of one of the BLS skills training sessions, study participants will be required to:
complete an Adult BLS assessment one week & two months after the program, and
complete a questionnaire prior to each BLS assessment & a program evaluation form at the time of the one
week assessment.
1 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.

Appendices 188 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The questionnaire you will be asked to complete contains questions relating to: age group, gender, computer
literacy, education, previous BLS experience, previous BLS emergency experience, knowledge, and
motivation to learn BLS. The program evaluation form has a series of questions that seek the participant‘s
opinions about the training program.
The BLS assessments will take 15 mins to complete each time and 10 minutes will also be required each
time to complete the questionnaire. A further 10 minutes will be needed to complete the program
evaluation form at the time of the one week assessment. The assessments will be conducted at a pre-
arranged time in the allocated classrooms at the A&RMC during study days or in the clinical area. Any
participant who is judged not competent in the first BLS assessment will require a further training session,
conducted by the student researcher. The time and place of this session will be negotiated with the
Graduate Nurse Year Co-ordinator. The BLS training and assessments completed as part of the study will
also fulfil the BLS training /assessment requirements of the graduate nurse year program
What will be done to make sure the information is confidential?
Information contributed by individuals will remain confidential and will be reported and published only as
group data. All information collected will remain confidential and will be stored as is required in a locked
cupboard at the university for seven years. Participant records may be inspected only for purposes of data
audit by authorised persons within the institution (e.g.; Ethics Committee) or outside (e.g.: sponsors or
regulatory bodies).
The results of this project will appear in a thesis to be written by Ms Karen Mardegan, in journal
publications and in presentations at conferences, but you will not be able to be identified in any of these
reports.
Who should I contact if I have any questions or concerns?
If you have any questions about the study, please contact senior investigator Dr Jane Pierson on 94793577.
If you have any complaints or queries that the investigators have been unable to answer, or wish to contact
someone, independent of the study, about ethical issues or your rights, you may contact either the Secretary
of the Faculty Human Ethics Committee, Faculty of Health Sciences, La Trobe University, Bundoora,
Victoria 3083, Ph. 94793573 or Mr. Stephen Duns, Chairman of the Austin & Repatriation Medical Centre
Human Research Ethics Committee, Phone 5425 5475.‖
Appendices 189 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
I, ………………………………………………….., have read and understood the information above, and
any questions have been answered to my satisfaction. I agree to participate in this project, realising that I
may withdraw at any time. I agree that research data collected during the project may be included in a
thesis, presented at conferences and published in journals, on condition that my name is not used.
My agreement is based on the understanding that the study involves:
Participating in a Basic Life Support (BLS) Program
Completing BLS assessments one week & two months after the program, and
Completing a questionnaire prior to each assessment & a program evaluation form at the one week
assessment.
Completing an additional training session if I do not perform competently in the first assessment.
I hereby voluntarily consent and offer to take part in this study.
NAME OF PARTICIPANT (in block letters): ………………………………………………….
Signature: …………………………………. Date / Time: ..…………………………..
NAME OF SENIOR INVESTIGATOR (in block letters): ……………………………………..
Signature: ………………………………… Date / Time: ……………………………
NAME OF RESEARCHER (in block letters): …………………………………………………
Signature: ………………………………… Date / Time: ……………………………
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix B2
Austin & Repatriation Medical Centre Participant
Information Sheet
Appendices 191 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Version: 1
Date: 29/10/02
Participant Information Sheet
Project Title:
An Alternative Approach To The Delivery Of Education For Health
Professionals2.
Principal Investigator:
Karen Mardegan, Professional Doctorate Student, School of Public Health, La Trobe
University
Supervisor:
Dr Jane Pierson, School of Public Health, La Trobe University
What is the Research Project about?
You are invited to participate in a research study that aims to evaluate the effectiveness of the
compact disc (an electronic data storage device) as a nursing education delivery method. Karen
Mardegan is conducting the study as part of her Doctoral studies at La Trobe University. In order
to evaluate the compact disc (CD) approach, the project will compare Traditional
lecture/demonstration Basic Life Support (BLS) training with a newly developed BLS training
CD produced by the Austin & Repatriation Medical Centre (A&RMC). It is hoped that this
project will demonstrate that educational CDs can at the very least support Traditional educational
delivery methods if not supersede them.
2 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
Appendices 192 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Why am I being asked to be in this research project?
Basic Life Support skills training and assessment is currently a required component of the
A&RMC Graduate Nurse Year program. However, participation in this research study, (which
includes a BLS skills training component and assessment) is entirely voluntary and can be
terminated at any time without prejudice. If you chose not to participate, or terminate
participation during the course of the study you will still be able to complete the BLS skills
training and assessment requirements of the graduate nurse year program during allocated class
time, and you will therefore not be disadvantaged or inconvenienced in any way if you choose not
to participate in, or to withdraw from, the study, however your participation would be appreciated.
What do I need to do to be in this research project?
Participants in the study will be randomly assigned to one of two BLS skills training programs
(Traditional or CD). Random assignment is like tossing of a coin, heads go to one group and tails
to the other. The Traditional program (which runs in class time), consists of a
practise/demonstration tutorial, and takes two hours in total. These sessions will be held in
allocated classrooms at the A&RMC. The CD program provides participants with access to the
BLS CD and a Resusci Anne® Manikin. Participants in the CD program will attend viewing
sessions totalling two hours, in class time and will not do the Traditional alternative. The CD
sessions will be held in the computer lab at the Austin or Repatriation campus. The two hours is
equivalent to the current time commitment required in the BLS component of the graduate nurse
year program.
On completion of one of the BLS skills training sessions, study participants will be required to:
complete an Adult BLS assessment one week & two months after the program, and
complete a questionnaire prior to each BLS assessment & a program evaluation form at the
time of the one week assessment.
The questionnaire you will be asked to complete contains questions relating to: age group, gender,
computer literacy, education, previous BLS experience, previous BLS emergency experience, BLS
knowledge, and motivation to learn BLS. The program evaluation form has a series of questions
that seek the participant‘s opinions about the training program.
The BLS assessments will take 15 mins to complete each time and 10 minutes will also be
required each time to complete the questionnaire. A further 10 minutes will be needed to
complete the program evaluation form at the time of the one week assessment. The assessments
will be conducted at a pre-arranged time in the allocated classrooms at the A&RMC during study
days or in the clinical area. Any participant who is judged not competent in the first BLS
assessment will be given a further training session and assessment. The BLS training and
assessments completed as part of the study will also fulfill the BLS training/assessment
requirements of the graduate nurse year program.
What will be done to make sure the information is confidential?
Information contributed by individuals will be confidential and will be reported and published
only as group data, so that no data capable of identifying a particular individual will be published.
All information collected will remain confidential and will be stored as is required in a locked
cupboard at the university for seven years. Participant records may be inspected only for purposes
of data audit by authorised persons within the institution (e.g.; Ethics Committee) or outside (e.g.:
sponsors or regulatory bodies).
The results of this project will appear in a thesis to be written by Ms Karen Mardegan, in journal
publications and in presentations at conferences, but you will not be able to be identified in any of
these reports.

Appendices 193 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Who should I contact if I have any questions or concerns?
You are welcome to ask the researcher, Ms Mardegan any questions you have about the study. If
you have any questions about the study which Ms Mardegan has not answered, please telephone
Ms Mardegan‘s research supervisor, Dr Jane Pierson, on 94793577 or write to her at the School of
Public Health, La Trobe University, Vic 3086.
If you have any complaints or queries that the researcher and supervisor have been unable to
answer, or wish to contact someone, independent of the study, about any complaints, ethical
issues or your rights, you may contact Mr Stephen Duns, Chairman of the Austin & Repatriation
Medical Centre Human Research Ethics Committee, Phone 5425 5475.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix B3
Austin & Repatriation Medical Centre Participant Consent
Form
Appendices 195 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Consent Form to Participate in Research
Project Title:
An Alternative Approach To The Delivery Of Education For Health Professionals3.
I, ..........................................................., have been invited to participate in the above study, which is being conducted
under the direction of (Principal Investigator) Karen Mardegan.
I understand that while the study will be under her supervision, other relevant and appropriate persons may assist or act
on her behalf.
My agreement is based on the understanding that the study involves:
completion of a BLS skills training program
completion of an Adult BLS assessment one week & two months after the completion of the training program
completion of a questionnaire prior to each BLS assessment & a program evaluation form at the time of the one week
assessment.
completing an additional training session and assessment if I do not perform competently in the first assessment.
Is this a drug trial? No
The study may involve the following risks, inconvenience and discomforts, which have been explained to me:
Time required to complete the study‘s second assessment, questionnaire, and the program evaluation form, which are
additional to those study requirements of training and assessment that are also requirements of the graduate nurse training
program.
I have received and read the attached ‗Participant Information Sheet‘ and understand the general purposes, methods and
demands of the study. All of my questions have been answered to my satisfaction. I understand that the study may not be
of direct benefit to me.
I can withdraw or be withdrawn by the Principal Investigator from this study at any time, without prejudice.
I consent to the publishing of results from this study provided my identity is not revealed.
I hereby voluntarily consent and offer to take part in this study.
Signature (Participant) Date: Time:
Witness to signature Date: Time:
Signature (Investigator) Date: Time:
One copy to be given to participant, one copy filed in participant’s personnel file
3 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
Version: 1
Date: 29/10/02
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix C
Calculation of Power
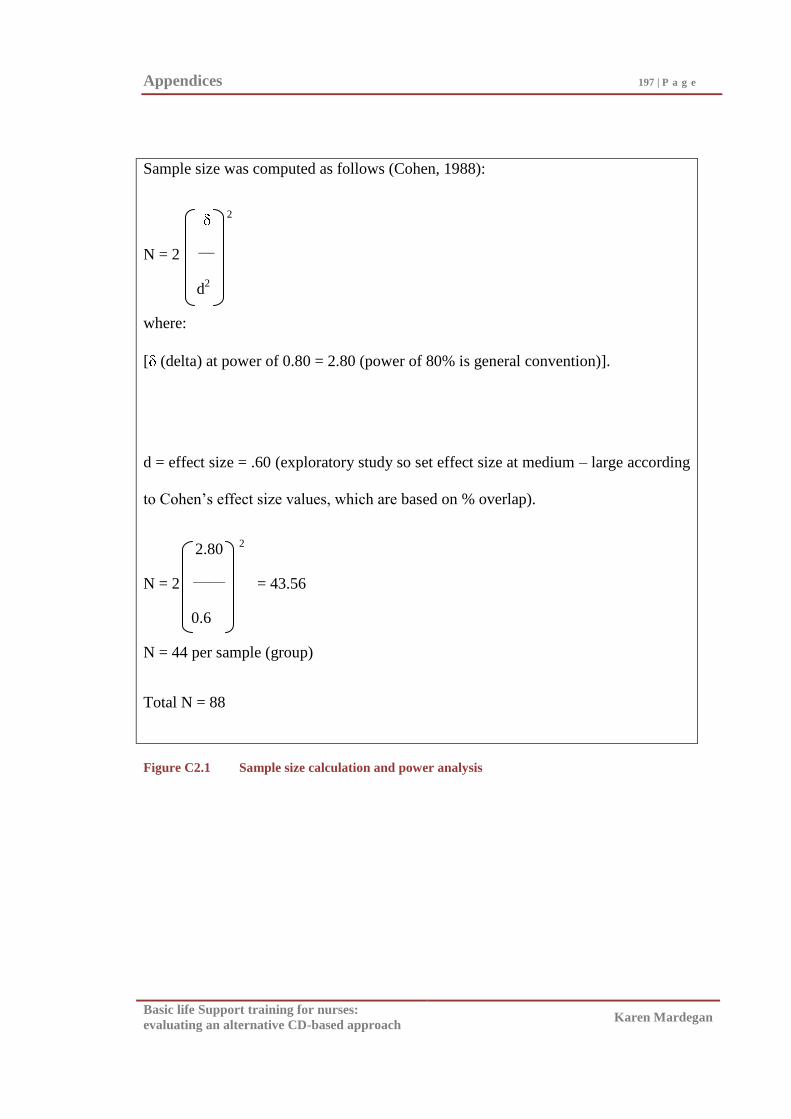
Appendices 197 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Sample size was computed as follows (Cohen, 1988):
2
N = 2 ___
d
2
where:
[ (delta) at power of 0.80 = 2.80 (power of 80% is general convention)].
d = effect size = .60 (exploratory study so set effect size at medium – large according
to Cohen‘s effect size values, which are based on % overlap).
2.80 2
N = 2 ______
= 43.56
0.6
N = 44 per sample (group)
Total N = 88
Figure C2.1 Sample size calculation and power analysis
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix D1
Inter-rater Reliability for Competent/Not Competent Results
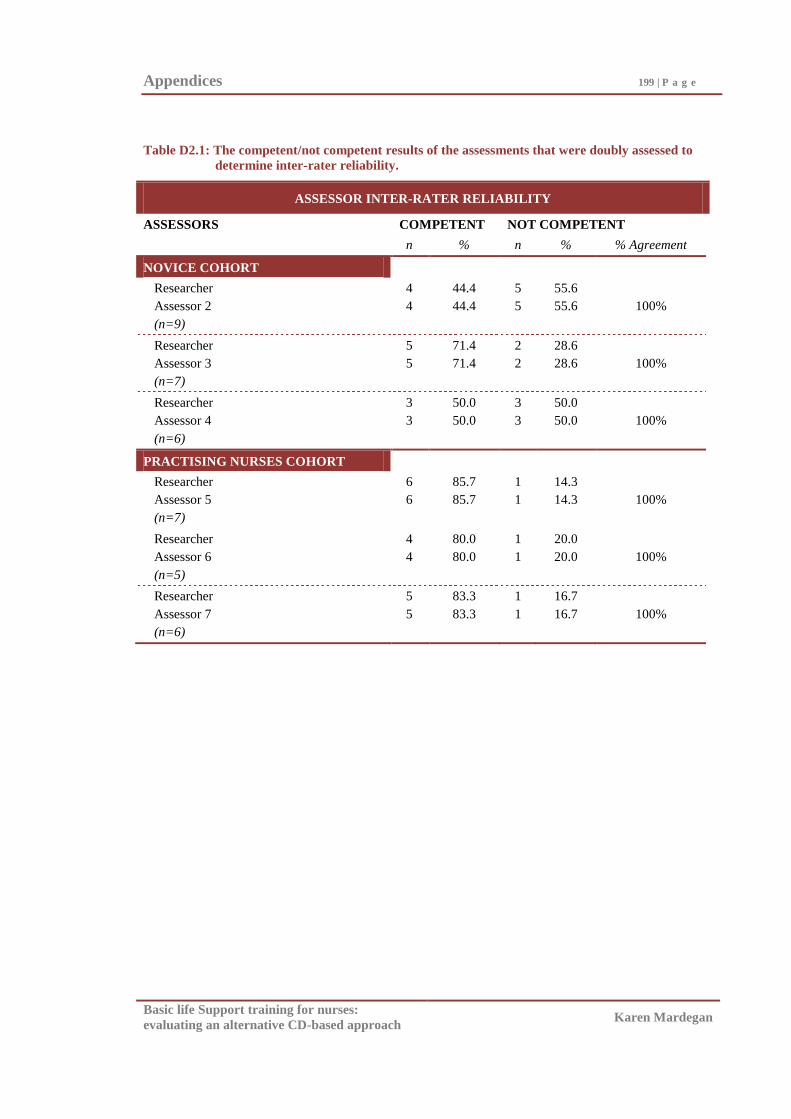
Appendices 199 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table D2.1: The competent/not competent results of the assessments that were doubly assessed to
determine inter-rater reliability.
ASSESSOR INTER-RATER RELIABILITY
ASSESSORS COMPETENT NOT COMPETENT
n % n % % Agreement
NOVICE COHORT
Researcher
Assessor 2
(n=9)
4
4
44.4
44.4
5
5
55.6
55.6
100%
Researcher
Assessor 3
(n=7)
5
5
71.4
71.4
2
2
28.6
28.6
100%
Researcher
Assessor 4
(n=6)
3
3
50.0
50.0
3
3
50.0
50.0
100%
PRACTISING NURSES COHORT
Researcher
Assessor 5
(n=7)
6
6
85.7
85.7
1
1
14.3
14.3
100%
Researcher
Assessor 6
(n=5)
4
4
80.0
80.0
1
1
20.0
20.0
100%
Researcher
Assessor 7
(n=6)
5
5
83.3
83.3
1
1
16.7
16.7
100%
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix D2
Inter-rater Reliability for Ordinal Scale Rating
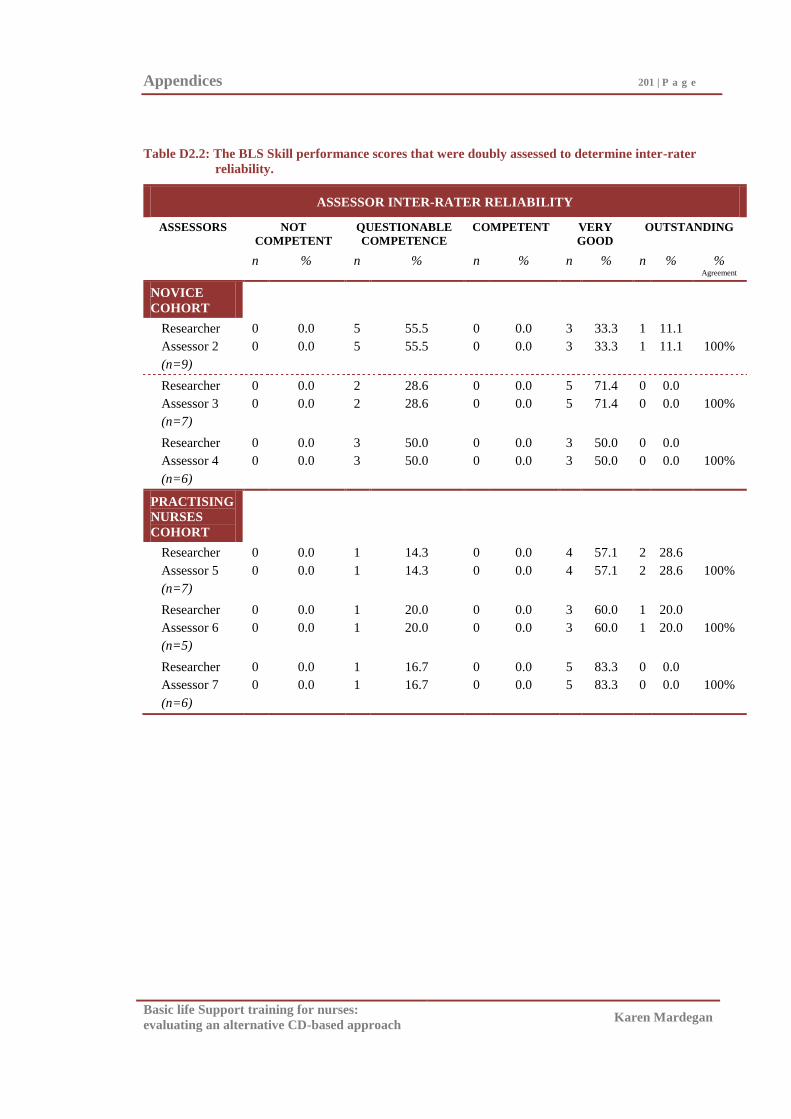
Appendices 201 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table D2.2: The BLS Skill performance scores that were doubly assessed to determine inter-rater
reliability.
ASSESSOR INTER-RATER RELIABILITY
ASSESSORS NOT
COMPETENT
QUESTIONABLE
COMPETENCE
COMPETENT VERY
GOOD
OUTSTANDING
n % n % n % n % n % % Agreement
NOVICE
COHORT
Researcher
Assessor 2
(n=9)
0
0
0.0
0.0
5
5
55.5
55.5
0
0
0.0
0.0
3
3
33.3
33.3
1
1
11.1
11.1
100%
Researcher
Assessor 3
(n=7)
0
0
0.0
0.0
2
2
28.6
28.6
0
0
0.0
0.0
5
5
71.4
71.4
0
0
0.0
0.0
100%
Researcher
Assessor 4
(n=6)
0
0
0.0
0.0
3
3
50.0
50.0
0
0
0.0
0.0
3
3
50.0
50.0
0
0
0.0
0.0
100%
PRACTISING
NURSES
COHORT
Researcher
Assessor 5
(n=7)
0
0
0.0
0.0
1
1
14.3
14.3
0
0
0.0
0.0
4
4
57.1
57.1
2
2
28.6
28.6
100%
Researcher
Assessor 6
(n=5)
0
0
0.0
0.0
1
1
20.0
20.0
0
0
0.0
0.0
3
3
60.0
60.0
1
1
20.0
20.0
100%
Researcher
Assessor 7
(n=6)
0
0
0.0
0.0
1
1
16.7
16.7
0
0
0.0
0.0
5
5
83.3
83.3
0
0
0.0
0.0
100%
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix E
Days Between Training & Testing
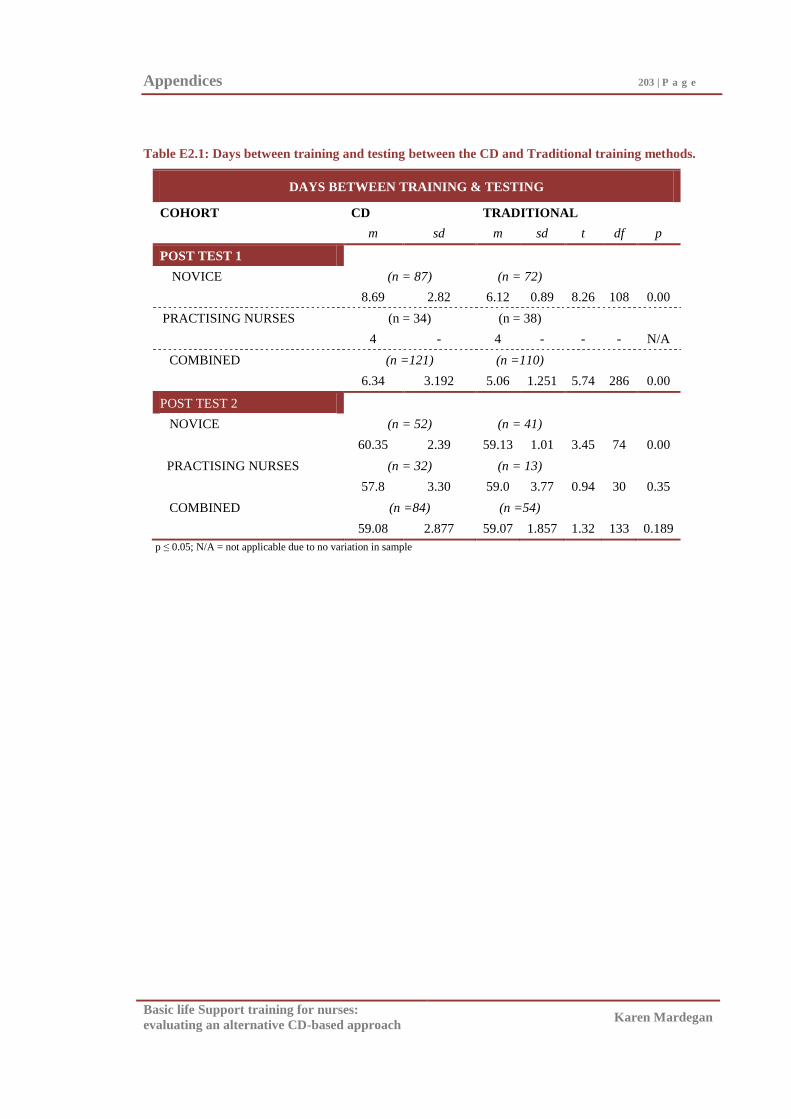
Appendices 203 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table E2.1: Days between training and testing between the CD and Traditional training methods.
DAYS BETWEEN TRAINING & TESTING
COHORT CD TRADITIONAL
m sd m sd t df p
POST TEST 1
NOVICE (n = 87) (n = 72)
8.69 2.82 6.12 0.89 8.26 108 0.00
PRACTISING NURSES (n = 34) (n = 38)
4 - 4 - - - N/A
COMBINED (n =121) (n =110)
6.34 3.192 5.06 1.251 5.74 286 0.00
POST TEST 2
NOVICE (n = 52) (n = 41)
60.35 2.39 59.13 1.01 3.45 74 0.00
PRACTISING NURSES (n = 32) (n = 13)
57.8 3.30 59.0 3.77 0.94 30 0.35
COMBINED (n =84) (n =54)
59.08 2.877 59.07 1.857 1.32 133 0.189
p ≤ 0.05; N/A = not applicable due to no variation in sample
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix F1
Questionnaire
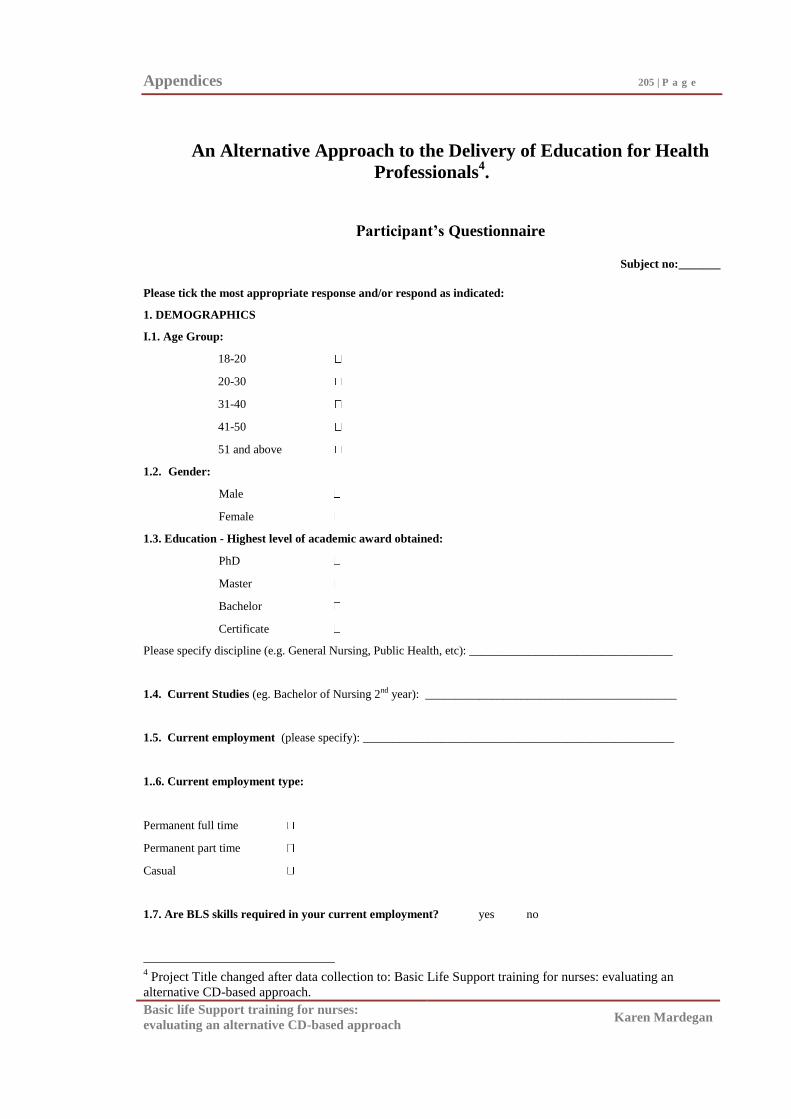
Appendices 205 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
An Alternative Approach to the Delivery of Education for Health
Professionals4.
Participant’s Questionnaire
Subject no:_______
Please tick the most appropriate response and/or respond as indicated:
1. DEMOGRAPHICS
I.1. Age Group:
18-20
20-30
31-40
41-50
51 and above
1.2. Gender:
Male
Female
1.3. Education - Highest level of academic award obtained:
PhD
Master
Bachelor
Certificate
Please specify discipline (e.g. General Nursing, Public Health, etc): __________________________________
1.4. Current Studies (eg. Bachelor of Nursing 2nd year): __________________________________________
1.5. Current employment (please specify): ____________________________________________________
1..6. Current employment type:
Permanent full time
Permanent part time
Casual
1.7. Are BLS skills required in your current employment? yes no
4 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
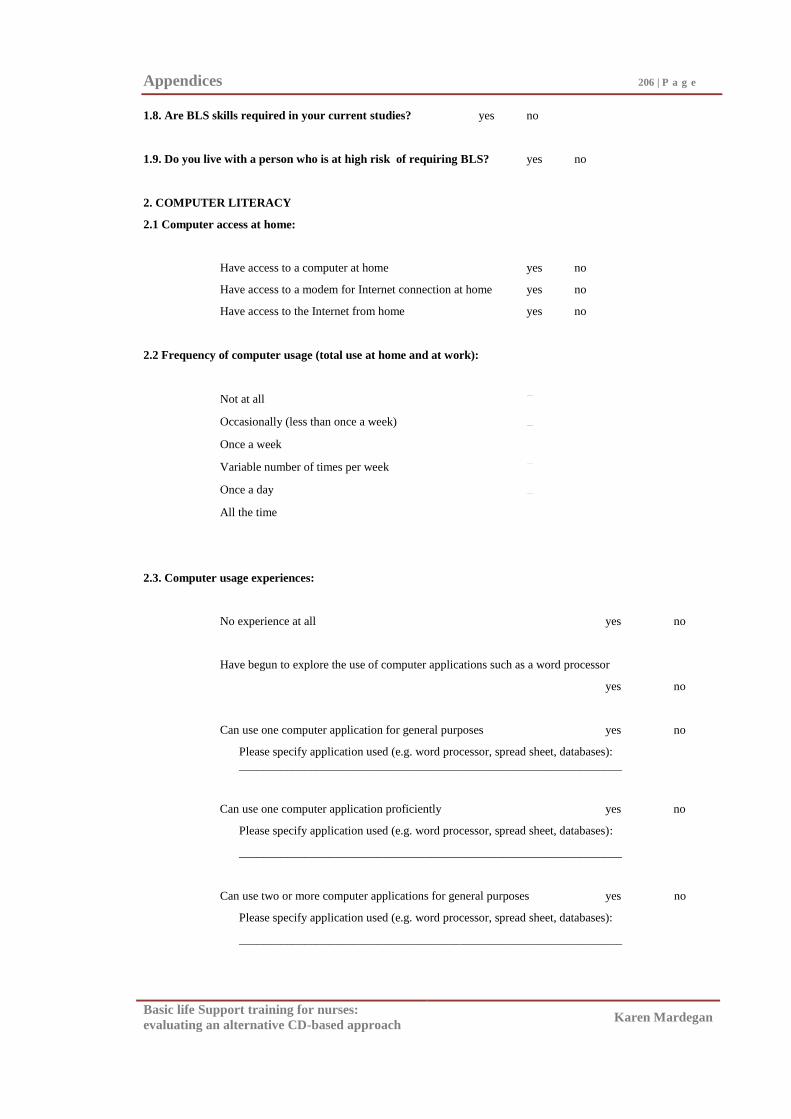
Appendices 206 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
1.8. Are BLS skills required in your current studies? yes no
1.9. Do you live with a person who is at high risk of requiring BLS? yes no
2. COMPUTER LITERACY
2.1 Computer access at home:
Have access to a computer at home yes no
Have access to a modem for Internet connection at home yes no
Have access to the Internet from home yes no
2.2 Frequency of computer usage (total use at home and at work):
Not at all
Occasionally (less than once a week)
Once a week
Variable number of times per week
Once a day
All the time
2.3. Computer usage experiences:
No experience at all yes no
Have begun to explore the use of computer applications such as a word processor
yes no
Can use one computer application for general purposes yes no
Please specify application used (e.g. word processor, spread sheet, databases):
________________________________________________________________
Can use one computer application proficiently yes no
Please specify application used (e.g. word processor, spread sheet, databases):
________________________________________________________________
Can use two or more computer applications for general purposes yes no
Please specify application used (e.g. word processor, spread sheet, databases):
________________________________________________________________
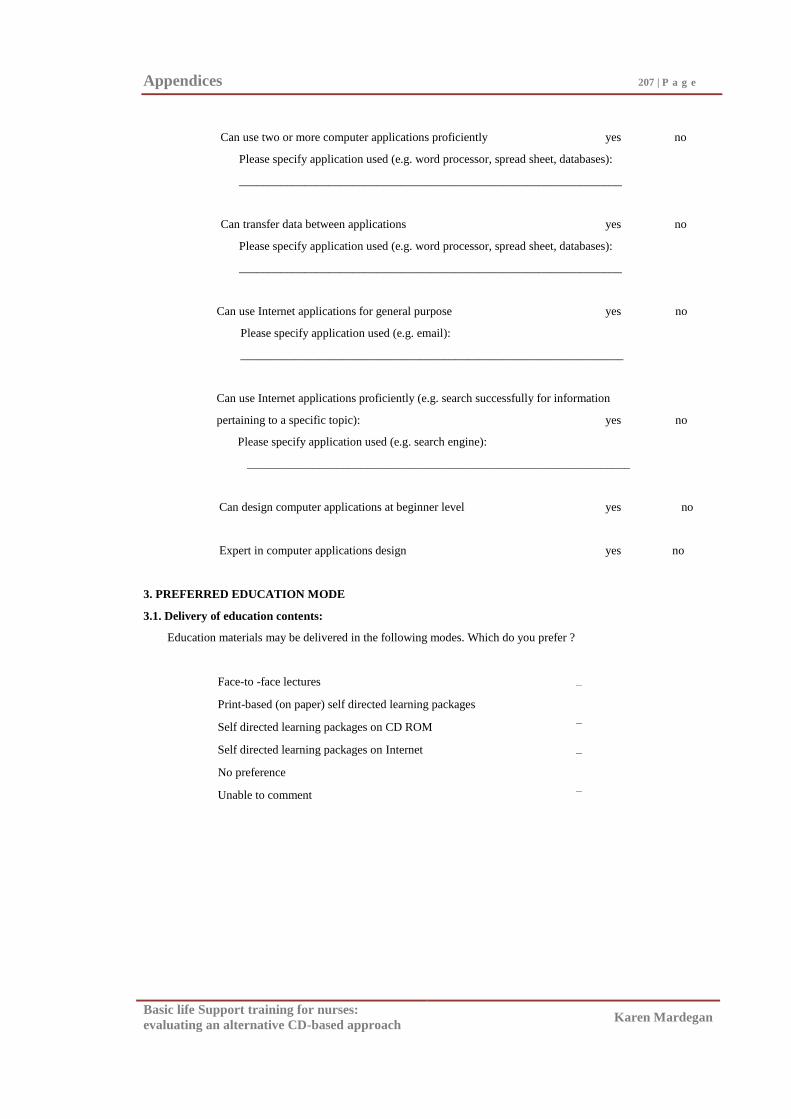
Appendices 207 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Can use two or more computer applications proficiently yes no
Please specify application used (e.g. word processor, spread sheet, databases):
________________________________________________________________
Can transfer data between applications yes no
Please specify application used (e.g. word processor, spread sheet, databases):
________________________________________________________________
Can use Internet applications for general purpose yes no
Please specify application used (e.g. email):
________________________________________________________________
Can use Internet applications proficiently (e.g. search successfully for information
pertaining to a specific topic): yes no
Please specify application used (e.g. search engine):
________________________________________________________________
Can design computer applications at beginner level yes no
Expert in computer applications design yes no
3. PREFERRED EDUCATION MODE
3.1. Delivery of education contents:
Education materials may be delivered in the following modes. Which do you prefer ?
Face-to -face lectures
Print-based (on paper) self directed learning packages
Self directed learning packages on CD ROM
Self directed learning packages on Internet
No preference
Unable to comment
Appendices 208 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
4.0 BASIC LIFE SUPORT (BLS) EXPERIENCE
4.1. Have you had previous BLS education? yes no
If so please specify name of program and date: ____________________________________________
4.2. Have you ever performed BLS in an emergency situation? yes no
If yes please state when and where: ______________________________________________________
4.3. Was this emergency situation during or after participating in this research project?
yes no
If yes please state when and where: ______________________________________________________
4.4. How would you rate your BLS skills prior to participating
in this program (1 = not competent 5 = outstanding) 1 2 3 4 5
4..5. How would you rate your BLS skills after completing the
program (1 = not competent 5 = outstanding) 1 2 3 4 5
4.6. Prior to participating in the program, if you were
required to perform BLS in an emergency:
Do you think you would have been able to? yes no
How confident do you think you would have felt?
(1 = not confident 5 = very confident) 1 2 3 4 5
4.7. Following completion of the program, if you were
now required to perform BLS in an emergency:
Do you think you could? yes no
How confident do you feel?
(1 = not confident 5 = very confident) 1 2 3 4 5
4.8 Have you practised in preparation for the assessment today yes no
(other than in the training sessions)?
5.0. BASIC LIFE SUPPORT KNOWEDGE
5.1. Define Respiratory Arrest: ________________________________________________________________________________________________
Appendices 209 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
5.2. List four (4) Causes of Respiratory Arrest:
5.3. Define Cardiopulmonary Arrest:
____________________________________________________________________________________________
5.4. List four (4) causes of Cardiac Arrest:
5.5. List 5 potential complications of performing cardiopulmonary resuscitation:
5.6. What are the three main drugs most commonly used in cardiac arrest situations?
THANK YOU FOR YOUR PARTICIPATION !
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix F2
2nd
Questionnaire
Appendices 211 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
An Alternative Approach to the Delivery of Education for Health
Professionals5.
Participants 2
nd Questionnaire
Subject no:_______
1.0 BASIC LIFE SUPORT (BLS) EXPERIENCE
1.1. Have you had previous BLS education? yes no
If so please specify name of program and date: ____________________________________________
1.2. Have you ever performed BLS in an emergency situation? yes no
If yes please state when and where: ______________________________________________________
1.3. Was this emergency situation during or after participating
in this research project? yes no
If yes please state when and where: ______________________________________________________
1.4. How would you rate your BLS skills prior to participating
in this program (1 = not competent 5 = outstanding) 1 2 3 4 5
1..5. How would you rate your BLS skills after completing the
program (1 = not competent 5 = outstanding) 1 2 3 4 5
1.6. Prior to participating in the program, if you were
required to perform BLS in an emergency:
Do you think you would have been able to? yes no
How confident do you think you would have felt?
(1 = not confident 5 = very confident) 1 2 3 4 5
5 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
Appendices 212 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
1.7. Following completion of the program, if you were
now required to perform BLS in an emergency:
Do you think you could? yes no
How confident do you feel?
(1 = not confident 5 = very confident) 1 2 3 4 5
1.8. Have you practised in preparation for the assessment today yes no
(other than in the training sessions)?
2.0. BASIC LIFE SUPPORT KNOWEDGE
2.1. Define Respiratory Arrest:
________________________________________________________________________________________________
2.2. List four (4) Causes of Respiratory Arrest:
2.3. Define Cardiopulmonary Arrest:
____________________________________________________________________________________________
2.4. List four (4) causes of Cardiac Arrest:
2.5. List 5 potential complications of performing cardiopulmonary resuscitation:
Appendices 213 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
2.6. What are the three main drugs most commonly used in cardiac arrest situations?
THANK YOU FOR YOUR PARTICIPATION
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix F3
Answers to BLS Knowledge Questions
Appendices 215 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Define Respiratory Arrest: Absence of breathing, no breathing.
List four (4) causes of Respiratory Arrest: (any combination)
Obstruction, foreign body, blockage of airway, anaphylaxis
Respiratory disease (ie asthma, bronchospasm, epiglottis)
Drug overdose
Trauma to chest, cardiac arrest
Define Cardiopumonary Arrest: Absence of breathing (no breathing) and no pulse.
List four (4) causes of Cardiac Arrest: (any combination)
Arrhythmias / abnormal heart rhythm, or Ventricular Tachycardia,
Ventricular Fibrillation, Asystole, Pulseless Electrical Activity
Chest trauma, drug overdose, respiratory arrest
Cardiac disease (AMI, heart failure), electrolyte imbalance (K+, Mg
+ or Ca
++)
Electric shock, electrocution
List five (5) potential complications of performing cardiopulmonary resuscitation:
(any combination)
Broken teeth, fractured liver, spleen, ribs, sternum, bruising
Pneumothorax
Aspiration, aspiration pneumonia,
Gastric distention, regurgitation
CPR not performed correctly/adequately
What are the three most common drugs used in cardiac arrest situations:
Adrenaline
Atropine
Lignocaine
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix G
Training Time
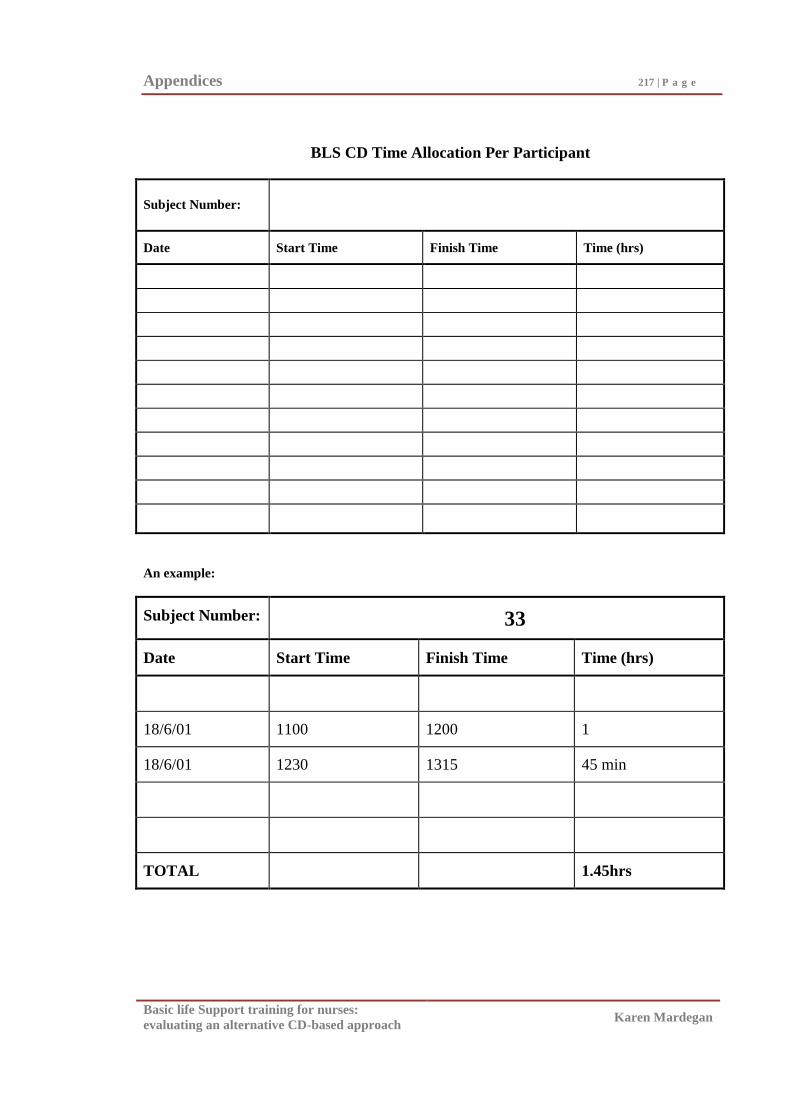
Appendices 217 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS CD Time Allocation Per Participant
Subject Number:
Date Start Time Finish Time Time (hrs)
An example:
Subject Number: 33
Date Start Time Finish Time Time (hrs)
18/6/01 1100 1200 1
18/6/01 1230 1315 45 min
TOTAL 1.45hrs

Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix H1
Traditional Program Evaluation Form
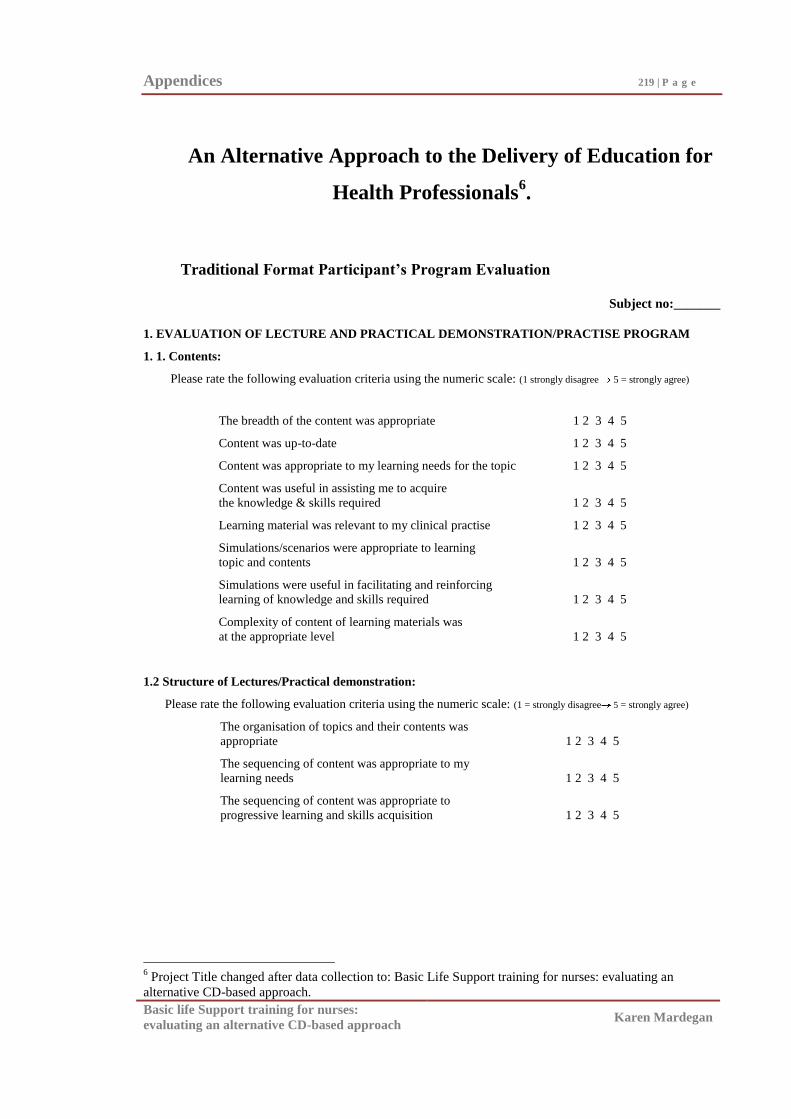
Appendices 219 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
An Alternative Approach to the Delivery of Education for
Health Professionals6.
Traditional Format Participant’s Program Evaluation
Subject no:_______
1. EVALUATION OF LECTURE AND PRACTICAL DEMONSTRATION/PRACTISE PROGRAM
1. 1. Contents:
Please rate the following evaluation criteria using the numeric scale: (1 strongly disagree 5 = strongly agree)
The breadth of the content was appropriate 1 2 3 4 5
Content was up-to-date 1 2 3 4 5
Content was appropriate to my learning needs for the topic 1 2 3 4 5
Content was useful in assisting me to acquire
the knowledge & skills required 1 2 3 4 5
Learning material was relevant to my clinical practise 1 2 3 4 5
Simulations/scenarios were appropriate to learning
topic and contents 1 2 3 4 5
Simulations were useful in facilitating and reinforcing
learning of knowledge and skills required 1 2 3 4 5
Complexity of content of learning materials was
at the appropriate level 1 2 3 4 5
1.2 Structure of Lectures/Practical demonstration:
Please rate the following evaluation criteria using the numeric scale: (1 = strongly disagree 5 = strongly agree)
The organisation of topics and their contents was
appropriate 1 2 3 4 5
The sequencing of content was appropriate to my
learning needs 1 2 3 4 5
The sequencing of content was appropriate to
progressive learning and skills acquisition 1 2 3 4 5
6 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
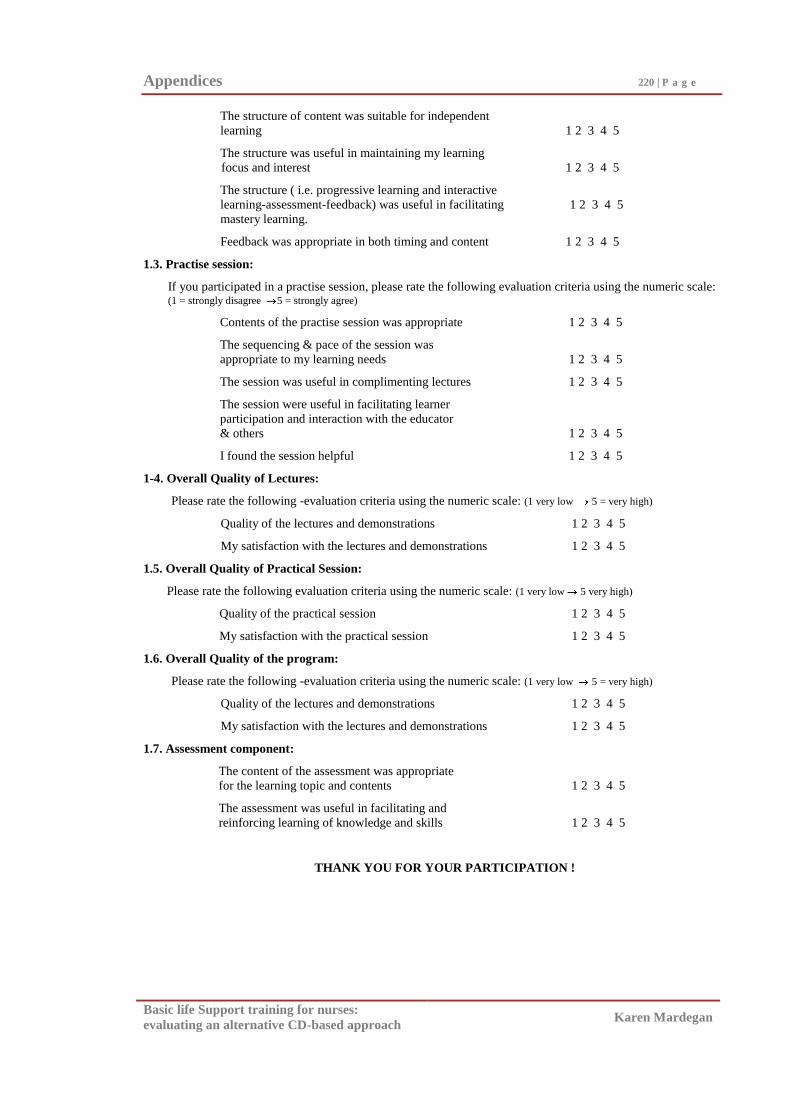
Appendices 220 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
The structure of content was suitable for independent
learning 1 2 3 4 5
The structure was useful in maintaining my learning
focus and interest 1 2 3 4 5
The structure ( i.e. progressive learning and interactive
learning-assessment-feedback) was useful in facilitating 1 2 3 4 5
mastery learning.
Feedback was appropriate in both timing and content 1 2 3 4 5
1.3. Practise session:
If you participated in a practise session, please rate the following evaluation criteria using the numeric scale: (1 = strongly disagree 5 = strongly agree)
Contents of the practise session was appropriate 1 2 3 4 5
The sequencing & pace of the session was
appropriate to my learning needs 1 2 3 4 5
The session was useful in complimenting lectures 1 2 3 4 5
The session were useful in facilitating learner
participation and interaction with the educator
& others 1 2 3 4 5
I found the session helpful 1 2 3 4 5
1-4. Overall Quality of Lectures:
Please rate the following -evaluation criteria using the numeric scale: (1 very low 5 = very high)
Quality of the lectures and demonstrations 1 2 3 4 5
My satisfaction with the lectures and demonstrations 1 2 3 4 5
1.5. Overall Quality of Practical Session:
Please rate the following evaluation criteria using the numeric scale: (1 very low 5 very high)
Quality of the practical session 1 2 3 4 5
My satisfaction with the practical session 1 2 3 4 5
1.6. Overall Quality of the program:
Please rate the following -evaluation criteria using the numeric scale: (1 very low 5 = very high)
Quality of the lectures and demonstrations 1 2 3 4 5
My satisfaction with the lectures and demonstrations 1 2 3 4 5
1.7. Assessment component:
The content of the assessment was appropriate
for the learning topic and contents 1 2 3 4 5
The assessment was useful in facilitating and
reinforcing learning of knowledge and skills 1 2 3 4 5
THANK YOU FOR YOUR PARTICIPATION !
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix H2
CD Program Evaluation Form
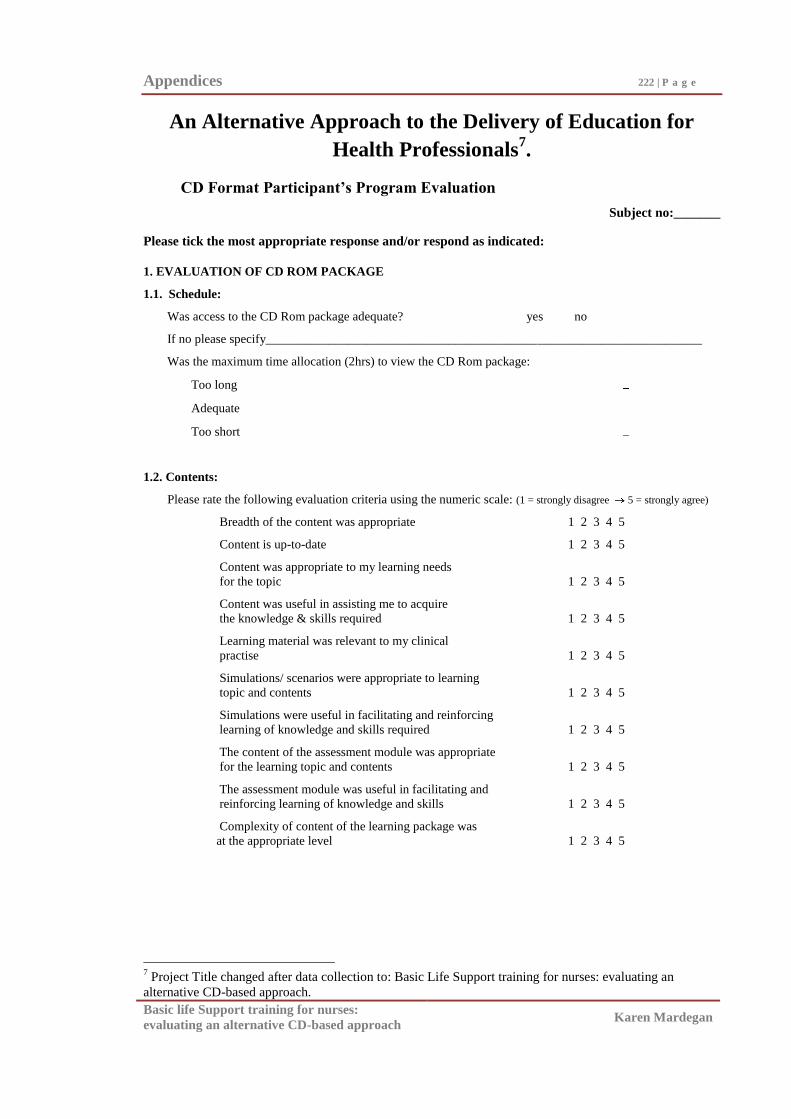
Appendices 222 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
An Alternative Approach to the Delivery of Education for
Health Professionals7.
CD Format Participant’s Program Evaluation
Subject no:_______
Please tick the most appropriate response and/or respond as indicated:
1. EVALUATION OF CD ROM PACKAGE
1.1. Schedule:
Was access to the CD Rom package adequate? yes no
If no please specify_____________________________________________________________________
Was the maximum time allocation (2hrs) to view the CD Rom package:
Too long
Adequate
Too short
1.2. Contents:
Please rate the following evaluation criteria using the numeric scale: (1 = strongly disagree 5 = strongly agree)
Breadth of the content was appropriate 1 2 3 4 5
Content is up-to-date 1 2 3 4 5
Content was appropriate to my learning needs
for the topic 1 2 3 4 5
Content was useful in assisting me to acquire
the knowledge & skills required 1 2 3 4 5
Learning material was relevant to my clinical
practise 1 2 3 4 5
Simulations/ scenarios were appropriate to learning
topic and contents 1 2 3 4 5
Simulations were useful in facilitating and reinforcing
learning of knowledge and skills required 1 2 3 4 5
The content of the assessment module was appropriate
for the learning topic and contents 1 2 3 4 5
The assessment module was useful in facilitating and
reinforcing learning of knowledge and skills 1 2 3 4 5
Complexity of content of the learning package was
at the appropriate level 1 2 3 4 5
7 Project Title changed after data collection to: Basic Life Support training for nurses: evaluating an
alternative CD-based approach.
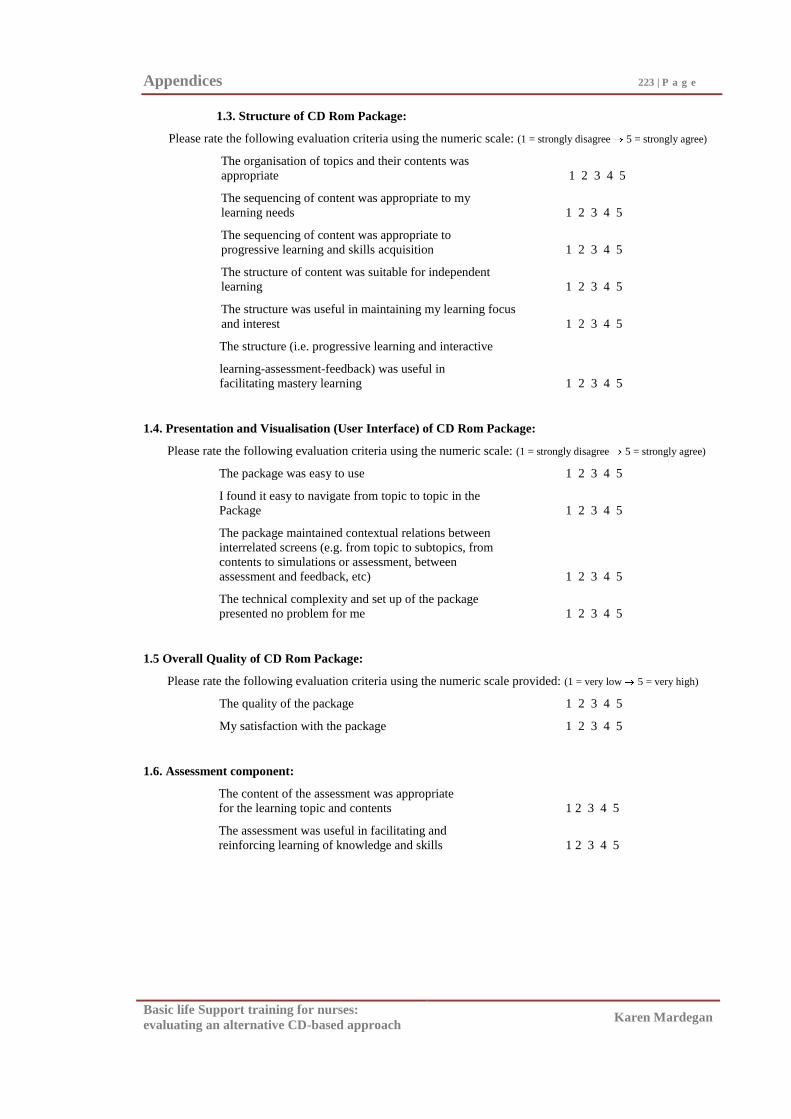
Appendices 223 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
1.3. Structure of CD Rom Package:
Please rate the following evaluation criteria using the numeric scale: (1 = strongly disagree 5 = strongly agree)
The organisation of topics and their contents was
appropriate 1 2 3 4 5
The sequencing of content was appropriate to my
learning needs 1 2 3 4 5
The sequencing of content was appropriate to
progressive learning and skills acquisition 1 2 3 4 5
The structure of content was suitable for independent
learning 1 2 3 4 5
The structure was useful in maintaining my learning focus
and interest 1 2 3 4 5
The structure (i.e. progressive learning and interactive
learning-assessment-feedback) was useful in
facilitating mastery learning 1 2 3 4 5
1.4. Presentation and Visualisation (User Interface) of CD Rom Package:
Please rate the following evaluation criteria using the numeric scale: (1 = strongly disagree 5 = strongly agree)
The package was easy to use 1 2 3 4 5
I found it easy to navigate from topic to topic in the
Package 1 2 3 4 5
The package maintained contextual relations between
interrelated screens (e.g. from topic to subtopics, from
contents to simulations or assessment, between
assessment and feedback, etc) 1 2 3 4 5
The technical complexity and set up of the package
presented no problem for me 1 2 3 4 5
1.5 Overall Quality of CD Rom Package:
Please rate the following evaluation criteria using the numeric scale provided: (1 = very low 5 = very high)
The quality of the package 1 2 3 4 5
My satisfaction with the package 1 2 3 4 5
1.6. Assessment component:
The content of the assessment was appropriate
for the learning topic and contents 1 2 3 4 5
The assessment was useful in facilitating and
reinforcing learning of knowledge and skills 1 2 3 4 5
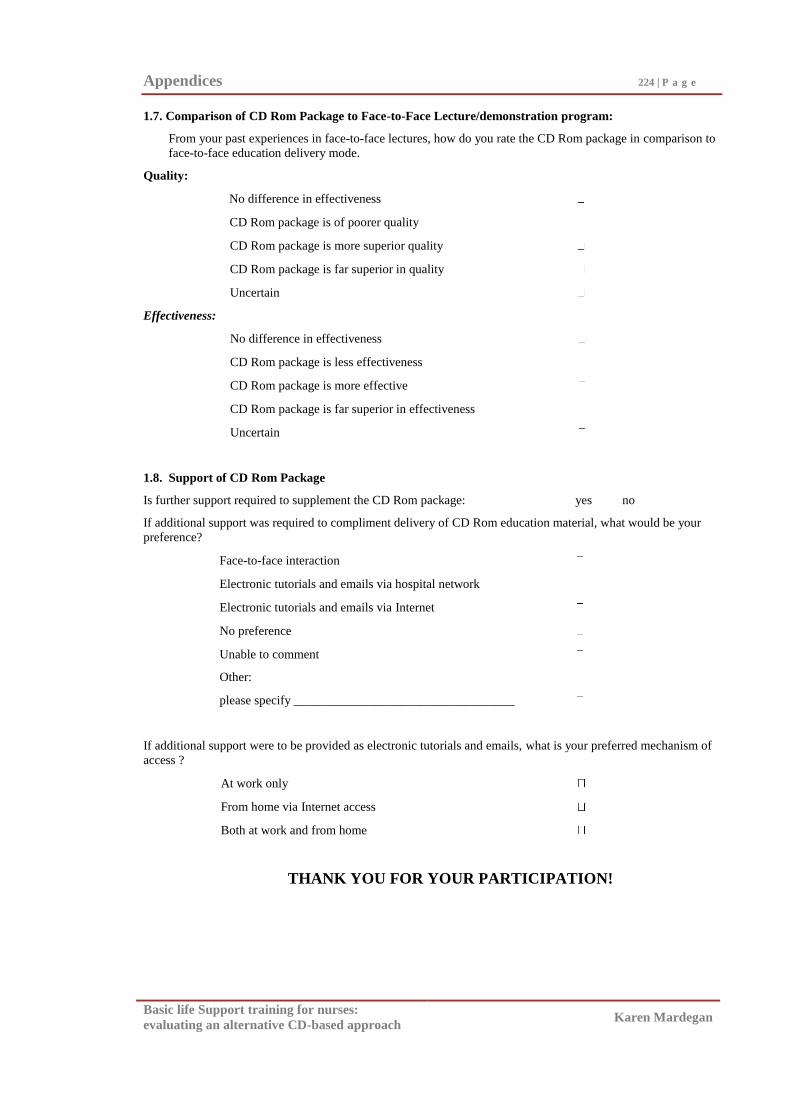
Appendices 224 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
1.7. Comparison of CD Rom Package to Face-to-Face Lecture/demonstration program:
From your past experiences in face-to-face lectures, how do you rate the CD Rom package in comparison to
face-to-face education delivery mode.
Quality:
No difference in effectiveness
CD Rom package is of poorer quality
CD Rom package is more superior quality
CD Rom package is far superior in quality
Uncertain
Effectiveness:
No difference in effectiveness
CD Rom package is less effectiveness
CD Rom package is more effective
CD Rom package is far superior in effectiveness
Uncertain
1.8. Support of CD Rom Package
Is further support required to supplement the CD Rom package: yes no
If additional support was required to compliment delivery of CD Rom education material, what would be your
preference?
Face-to-face interaction
Electronic tutorials and emails via hospital network
Electronic tutorials and emails via Internet
No preference
Unable to comment
Other:
please specify ___________________________________
If additional support were to be provided as electronic tutorials and emails, what is your preferred mechanism of
access ?
At work only
From home via Internet access
Both at work and from home
THANK YOU FOR YOUR PARTICIPATION!
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix H3
Internal Consistency of the Program Evaluation forms.
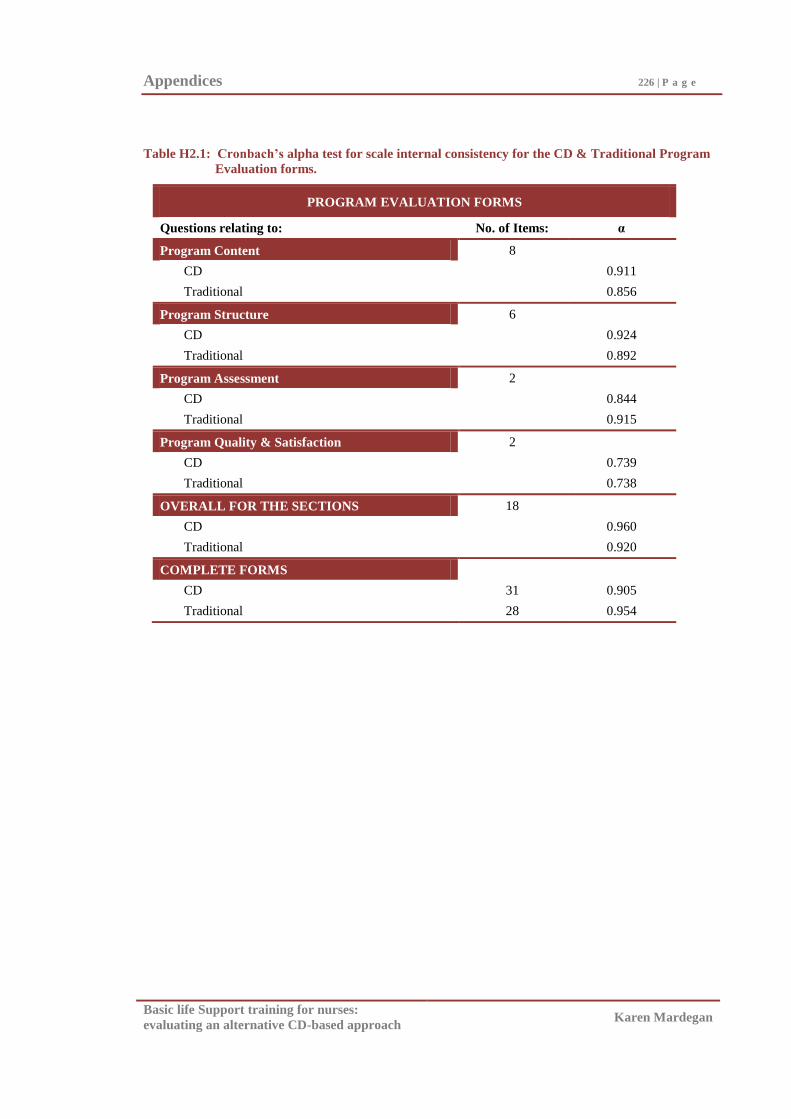
Appendices 226 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table H2.1: Cronbach’s alpha test for scale internal consistency for the CD & Traditional Program
Evaluation forms.
PROGRAM EVALUATION FORMS
Questions relating to: No. of Items: α
Program Content 8
CD 0.911
Traditional 0.856
Program Structure 6
CD 0.924
Traditional 0.892
Program Assessment 2
CD 0.844
Traditional 0.915
Program Quality & Satisfaction 2
CD 0.739
Traditional 0.738
OVERALL FOR THE SECTIONS 18
CD 0.960
Traditional 0.920
COMPLETE FORMS
CD 31 0.905
Traditional 28 0.954
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix I
Pilot Study Procedure
Appendices 228 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Participants
Second year nursing students (n=20) from a major university in Melbourne
Australia who had no previous BLS training (novices) participated in the pilot study.
There were no exclusion criteria but demographic data were collected allowing for
description of the participants and identification of any previous BLS training undertaken
(see Appendix F1).
Recruitment.
Once permissions to conduct the study and access the participants had been
obtained, as in the main study, the principal investigator approached two hundred 2nd
year
nursing students as a group during a scheduled session and invited them to participate.
Those who wished to take part completed the study consent form (see Appendix B1).
Twenty 2nd
year nursing students, (from the same population as Novice cohort A in the
main study) were recruited into the pilot study (see Figure 3.1).
Participant assignment.
Consistent with the main study, a rational method was used to allocate participants
into the Traditional and CD training groups. Ten were assigned, based on their pre-
existing university grouping, to each of the two training groups and attended training (the
university requirement). Only eight of the ten who consented to participate (80%) from
the BLS CD group and four of the ten (40%) for the Traditional BLS program group
actually attended Post Test 1, and only seven of the 10 who consented to participate
(70%) from the BLS CD group, and three of the ten (30%) for the Traditional BLS
program group attended Post Test 2 (see Figure 3.3). This high attrition rate was thought
to be due to the assessments not being part of the university program and it being
conducted outside class time. To avert this problem in the main study, the BLS
assessments were included as a university program requirement which assisted
recruitment and participation.
BLS training program and post tests.
The BLS training and post test procedures were the same as for the main study.
There were minor differences in assessment timing due to scheduling arrangements and
availability of participants in the pilot and main study. The pilot study group attended
Appendices 229 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Post Test 1 at two weeks and Post Test 2 at 10 weeks post training, where as in the main
study, the post tests were conducted at one week and then again at eight weeks after
training.
Training methods and measures.
The intervention (CD and Traditional BLS training programs) and the measures
(questionnaire, BLS assessment form/automated manikin, and program evaluations) were
as described above for the main study. Pilot participants, as with Novice Cohort A
participants in the main study, being beginners (novice learners), received two hours of
viewing/practice (CD Group) or presentation-demonstration/practise (Traditional Group)
instruction time. Completion of a BLS training program (which did not include a BLS
skill assessment) was a compulsory university course requirement for nursing students in
the pilot study. Therefore (in contrast to the main study), completion of the questionnaire,
BLS assessment and program evaluations for the pilot study was conducted outside class
time, and the questionnaire, which was condensed for post test 2 in the main study, was
completed in its entirety before both the first and second BLS post tests in the pilot study.
The small numbers involved in the pilot study allowed for BLS assessments to be
performed solely by the researcher, who was an accredited BLS instructor. Analysis of
assessor reliability was therefore not required in the pilot study. The results and
implications of this pilot study to the main study have been presented in the body of this
thesis.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix J1
Descriptive Statistics for BLS Skill
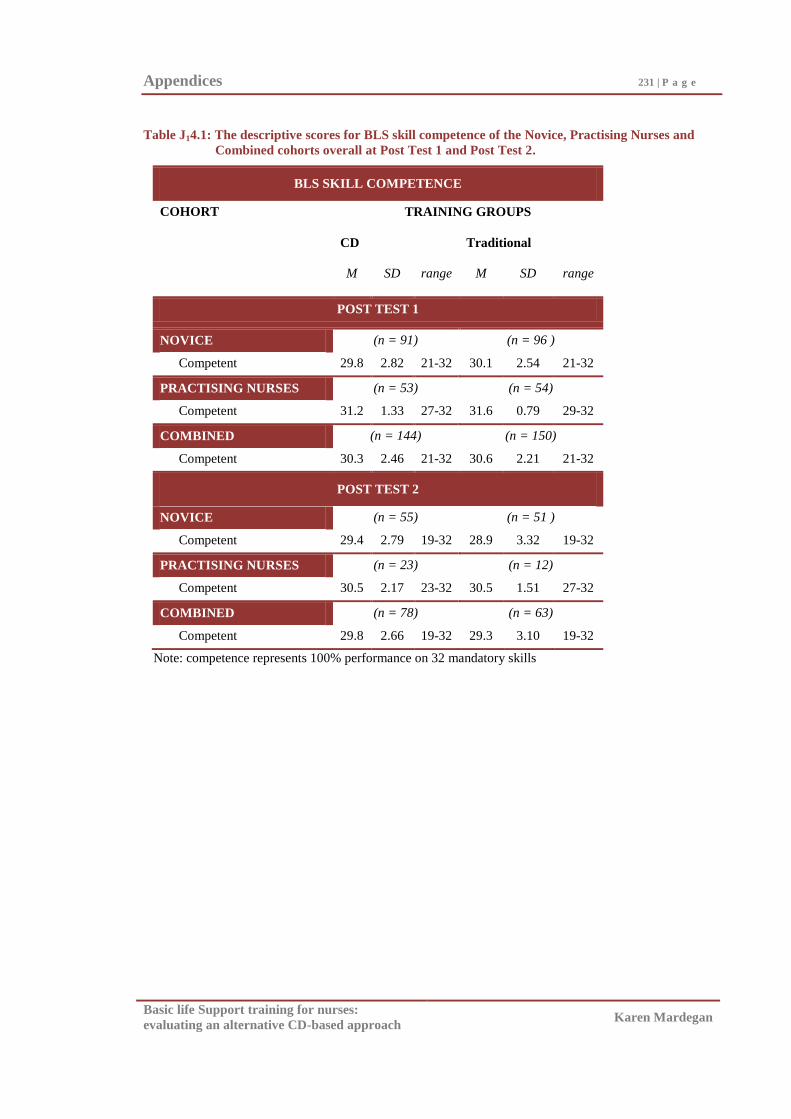
Appendices 231 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table J14.1: The descriptive scores for BLS skill competence of the Novice, Practising Nurses and
Combined cohorts overall at Post Test 1 and Post Test 2.
BLS SKILL COMPETENCE
COHORT TRAINING GROUPS
CD Traditional
M SD range M SD range
POST TEST 1
NOVICE (n = 91) (n = 96 )
Competent 29.8 2.82 21-32 30.1 2.54 21-32
PRACTISING NURSES (n = 53) (n = 54)
Competent 31.2 1.33 27-32 31.6 0.79 29-32
COMBINED (n = 144) (n = 150)
Competent 30.3 2.46 21-32 30.6 2.21 21-32
POST TEST 2
NOVICE (n = 55) (n = 51 )
Competent 29.4 2.79 19-32 28.9 3.32 19-32
PRACTISING NURSES (n = 23) (n = 12)
Competent 30.5 2.17 23-32 30.5 1.51 27-32
COMBINED (n = 78) (n = 63)
Competent 29.8 2.66 19-32 29.3 3.10 19-32
Note: competence represents 100% performance on 32 mandatory skills
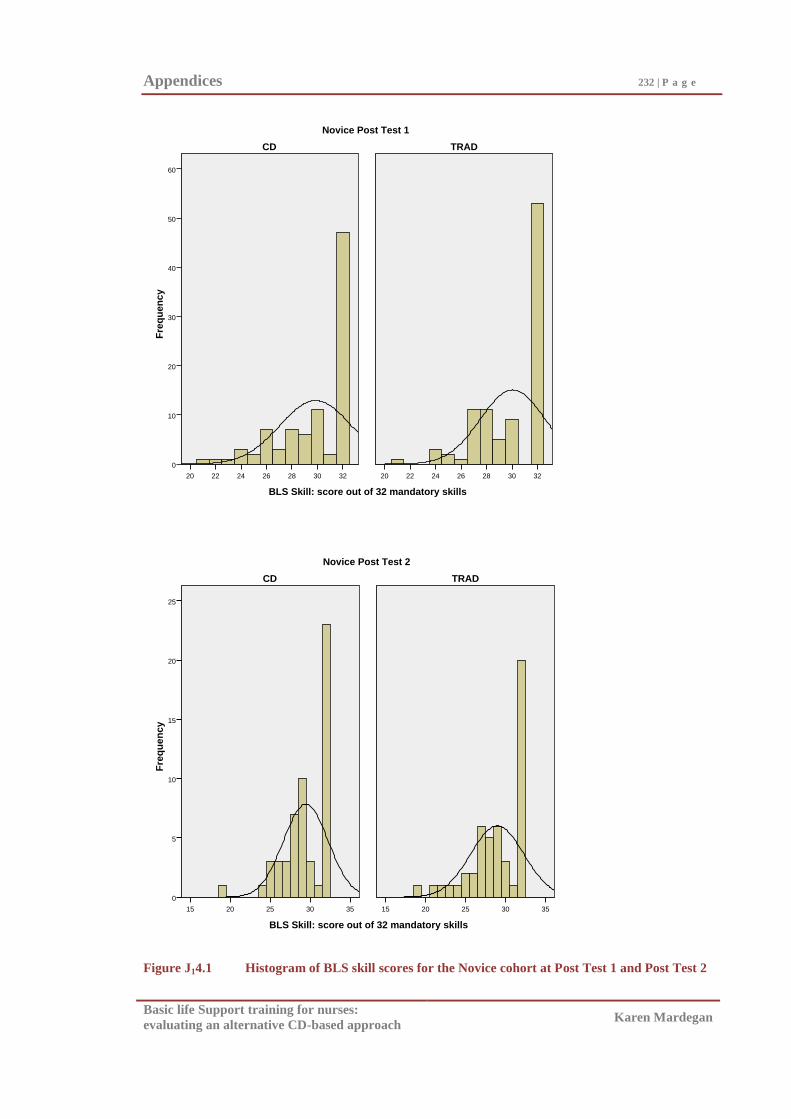
Appendices 232 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Skill: score out of 32 mandatory skills
32302826242220
Fre
qu
en
cy
60
50
40
30
20
10
0
32302826242220
Novice Post Test 1
TRADCD
BLS Skill: score out of 32 mandatory skills
3530252015
Fre
qu
en
cy
25
20
15
10
5
0
3530252015
Novice Post Test 2
TRADCD
Figure J14.1 Histogram of BLS skill scores for the Novice cohort at Post Test 1 and Post Test 2
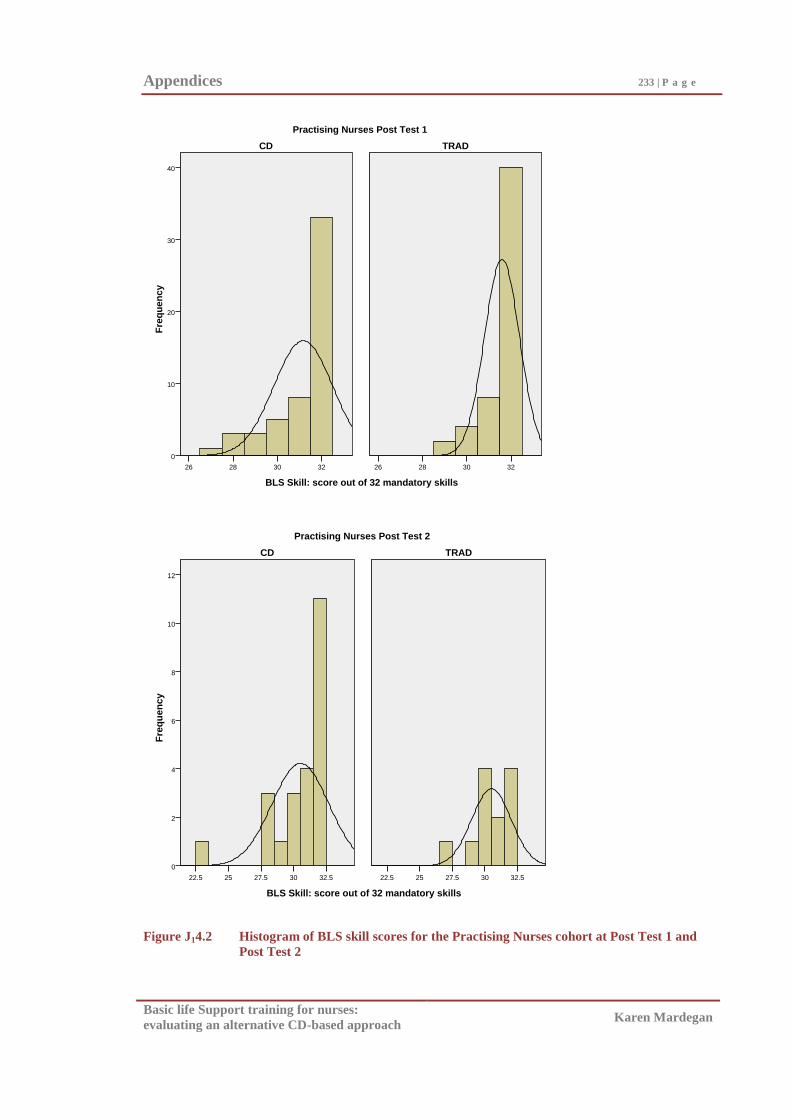
Appendices 233 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Skill: score out of 32 mandatory skills
32302826
Fre
qu
en
cy
40
30
20
10
0
32302826
Practising Nurses Post Test 1
TRADCD
BLS Skill: score out of 32 mandatory skills
32.53027.52522.5
Fre
qu
en
cy
12
10
8
6
4
2
0
32.53027.52522.5
Practising Nurses Post Test 2
TRADCD
Figure J14.2 Histogram of BLS skill scores for the Practising Nurses cohort at Post Test 1 and
Post Test 2
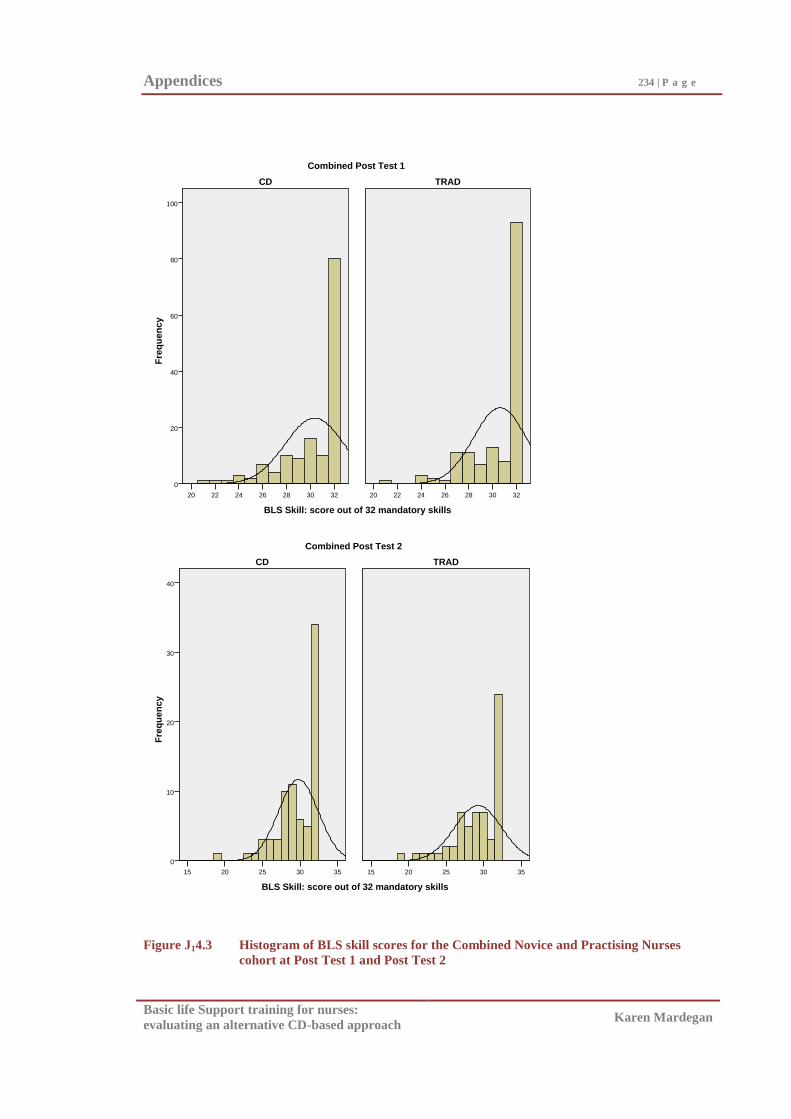
Appendices 234 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Skill: score out of 32 mandatory skills
32302826242220
Fre
qu
en
cy
100
80
60
40
20
0
32302826242220
Combined Post Test 1
TRADCD
BLS Skill: score out of 32 mandatory skills
3530252015
Fre
qu
en
cy
40
30
20
10
0
3530252015
Combined Post Test 2
TRADCD
Figure J14.3 Histogram of BLS skill scores for the Combined Novice and Practising Nurses
cohort at Post Test 1 and Post Test 2
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix J2
Descriptive Statistics for BLS Knowledge
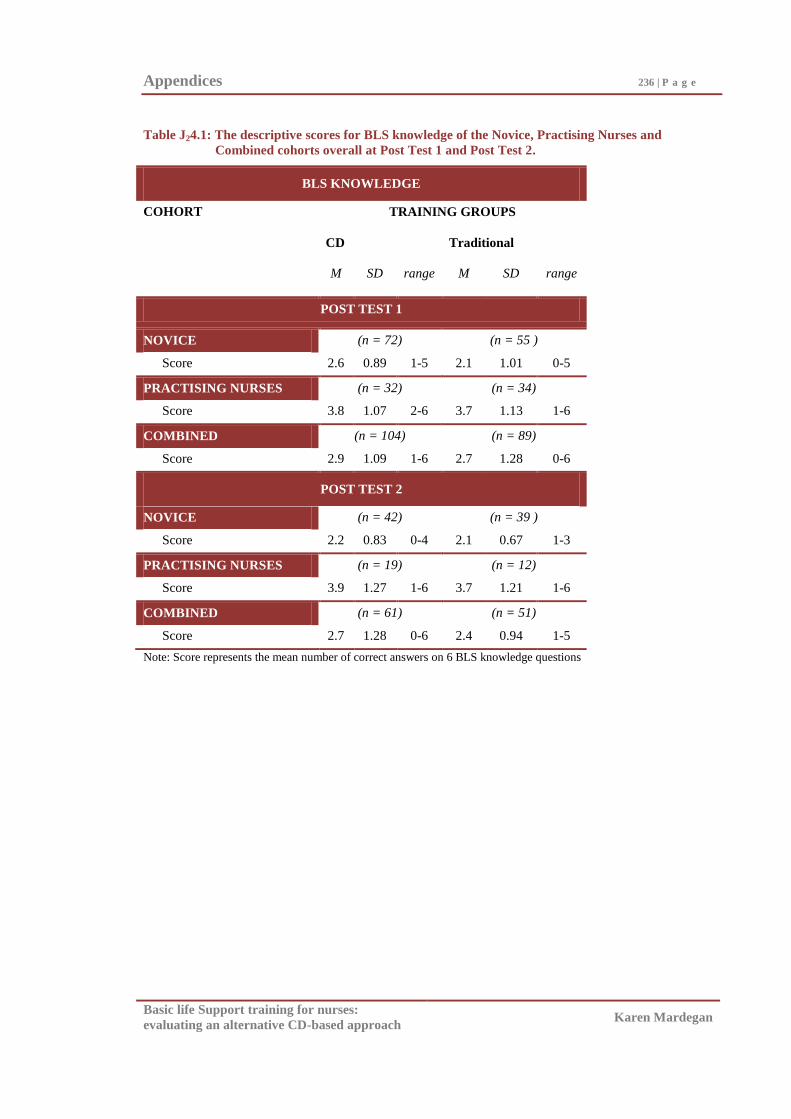
Appendices 236 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table J24.1: The descriptive scores for BLS knowledge of the Novice, Practising Nurses and
Combined cohorts overall at Post Test 1 and Post Test 2.
BLS KNOWLEDGE
COHORT TRAINING GROUPS
CD Traditional
M SD range M SD range
POST TEST 1
NOVICE (n = 72) (n = 55 )
Score 2.6 0.89 1-5 2.1 1.01 0-5
PRACTISING NURSES (n = 32) (n = 34)
Score 3.8 1.07 2-6 3.7 1.13 1-6
COMBINED (n = 104) (n = 89)
Score 2.9 1.09 1-6 2.7 1.28 0-6
POST TEST 2
NOVICE (n = 42) (n = 39 )
Score 2.2 0.83 0-4 2.1 0.67 1-3
PRACTISING NURSES (n = 19) (n = 12)
Score 3.9 1.27 1-6 3.7 1.21 1-6
COMBINED (n = 61) (n = 51)
Score 2.7 1.28 0-6 2.4 0.94 1-5
Note: Score represents the mean number of correct answers on 6 BLS knowledge questions
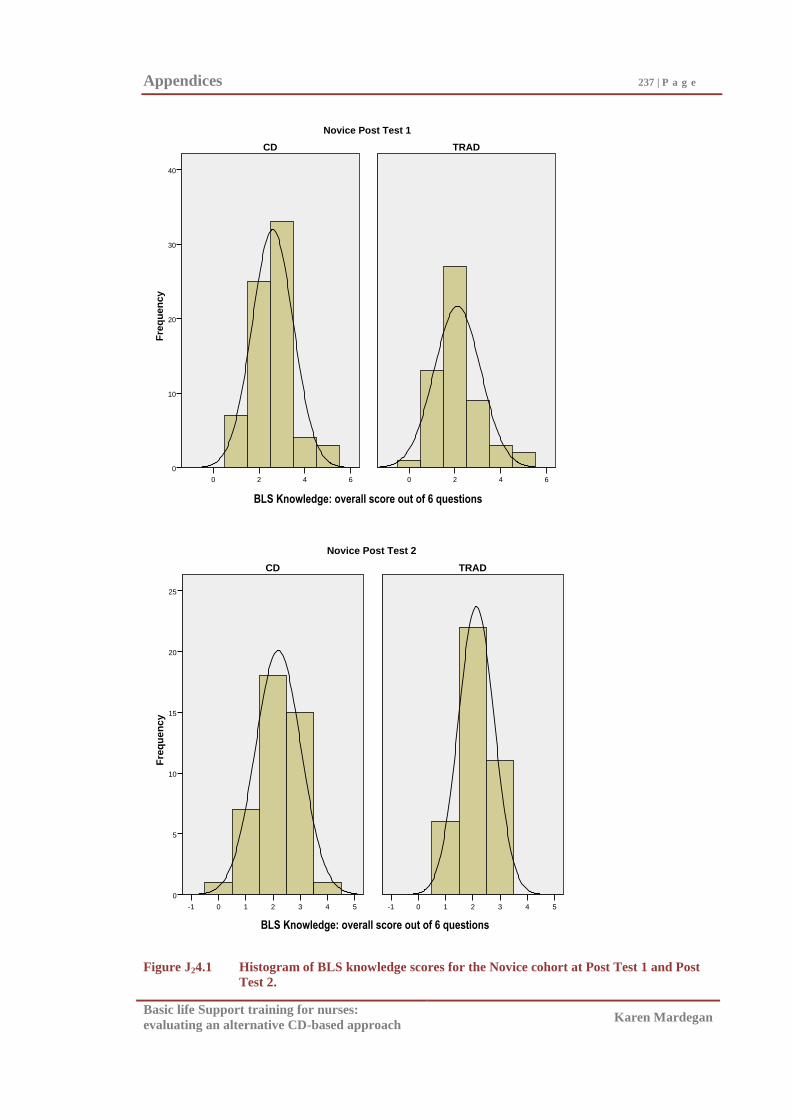
Appendices 237 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Knowledge: overall score out of 6 questions
6420
Fre
qu
en
cy
40
30
20
10
0
6420
Novice Post Test 1
TRADCD
BLS Knowledge: overall score out of 6 question
543210-1
Fre
qu
en
cy
25
20
15
10
5
0
543210-1
Novice Post Test 2
TRADCD
Figure J24.1 Histogram of BLS knowledge scores for the Novice cohort at Post Test 1 and Post
Test 2.
BLS Knowledge: overall score out of 6 questions
BLS Knowledge: overall score out of 6 questions
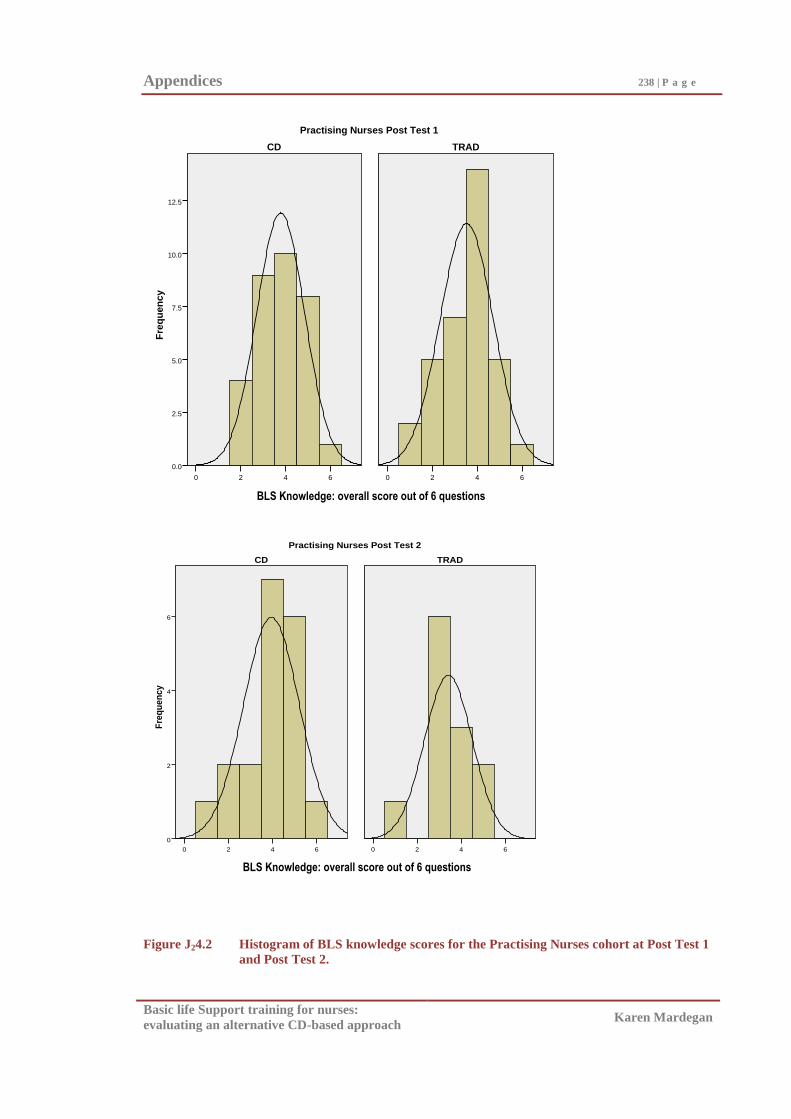
Appendices 238 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Knowledge: overall score out of 6 questions
6420
Fre
qu
en
cy
12.5
10.0
7.5
5.0
2.5
0.0
6420
Practising Nurses Post Test 1
TRADCD
BLS Knowledge: overall score out of 6
6420
Fre
qu
en
cy
6
4
2
0
6420
Practising Nurses Post Test 2
TRADCD
Figure J24.2 Histogram of BLS knowledge scores for the Practising Nurses cohort at Post Test 1
and Post Test 2.
BLS Knowledge: overall score out of 6 questions
BLS Knowledge: overall score out of 6 questions
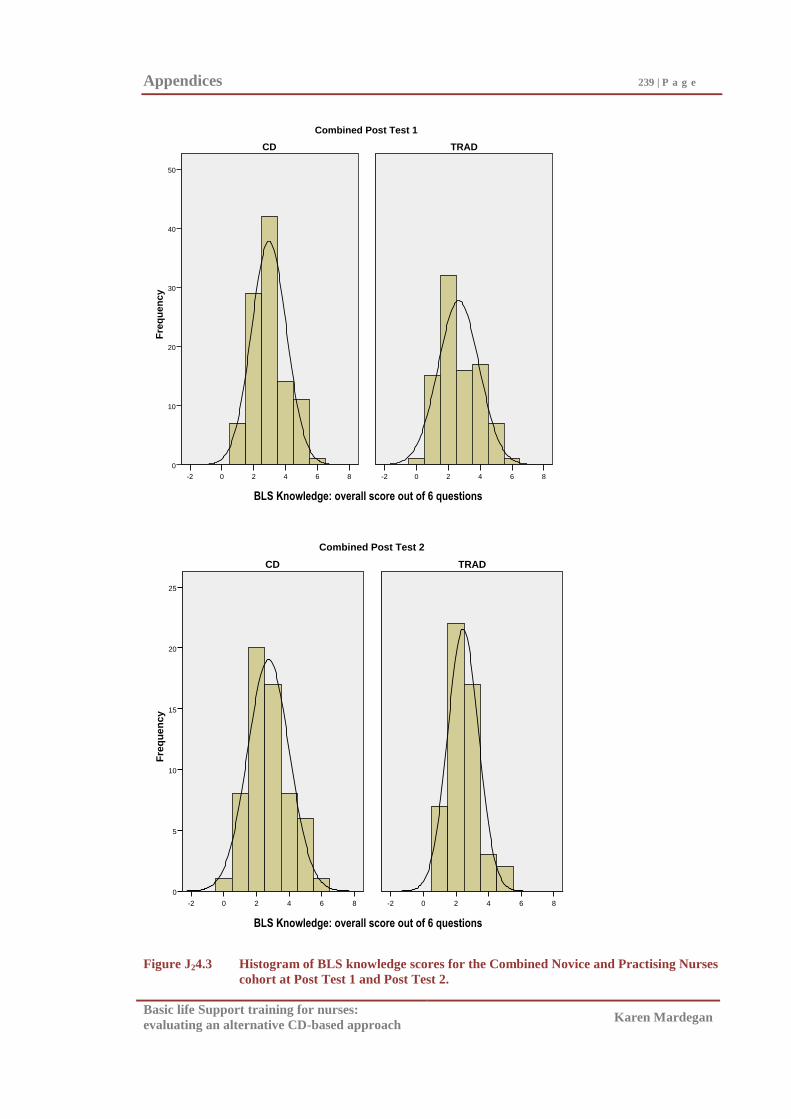
Appendices 239 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
BLS Knowledge overall score out of 6 questions
86420-2
Fre
qu
en
cy
50
40
30
20
10
0
86420-2
Combined Post Test 1
TRADCD
BLS Knowledge overall score out of 6
86420-2
Fre
qu
en
cy
25
20
15
10
5
0
86420-2
Combined Post Test 2
TRADCD
Figure J24.3 Histogram of BLS knowledge scores for the Combined Novice and Practising Nurses
cohort at Post Test 1 and Post Test 2.
BLS Knowledge: overall score out of 6 questions
BLS Knowledge: overall score out of 6 questions
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix J3
Descriptive Statistics for Participants‘ Rating of the BLS
Training Programs
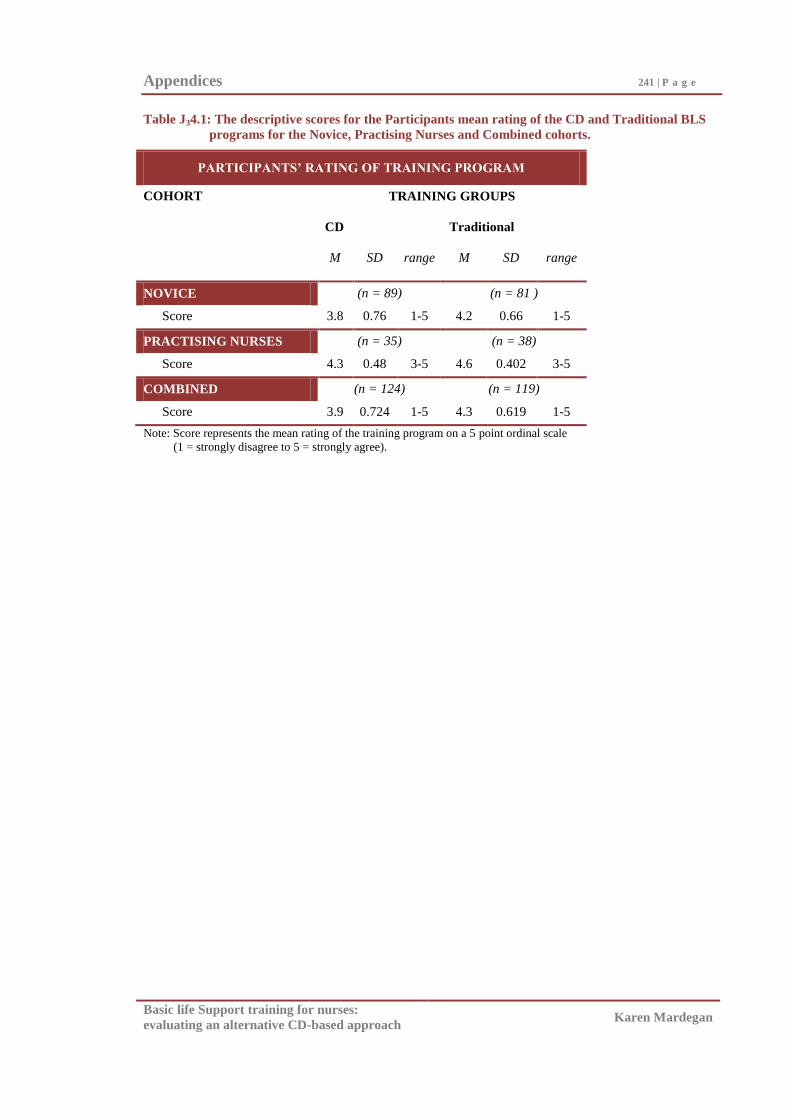
Appendices 241 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table J34.1: The descriptive scores for the Participants mean rating of the CD and Traditional BLS
programs for the Novice, Practising Nurses and Combined cohorts.
PARTICIPANTS’ RATING OF TRAINING PROGRAM
COHORT TRAINING GROUPS
CD Traditional
M SD range M SD range
NOVICE (n = 89) (n = 81 )
Score 3.8 0.76 1-5 4.2 0.66 1-5
PRACTISING NURSES (n = 35) (n = 38)
Score 4.3 0.48 3-5 4.6 0.402 3-5
COMBINED (n = 124) (n = 119)
Score 3.9 0.724 1-5 4.3 0.619 1-5
Note: Score represents the mean rating of the training program on a 5 point ordinal scale
(1 = strongly disagree to 5 = strongly agree).
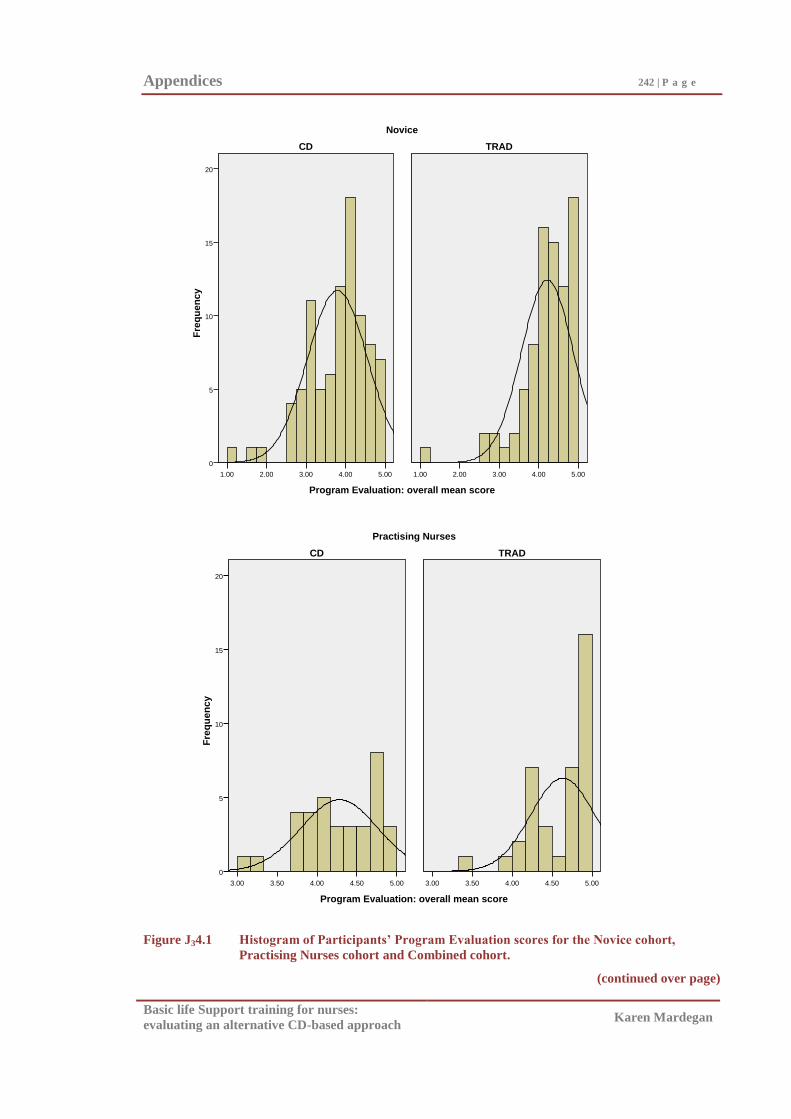
Appendices 242 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Program Evaluation: overall mean score
5.004.003.002.001.00
Fre
qu
en
cy
20
15
10
5
0
5.004.003.002.001.00
Novice
TRADCD
Program Evaluation: overall mean score
5.004.504.003.503.00
Fre
qu
en
cy
20
15
10
5
0
5.004.504.003.503.00
Practising Nurses
TRADCD
Figure J34.1 Histogram of Participants’ Program Evaluation scores for the Novice cohort,
Practising Nurses cohort and Combined cohort.
(continued over page)
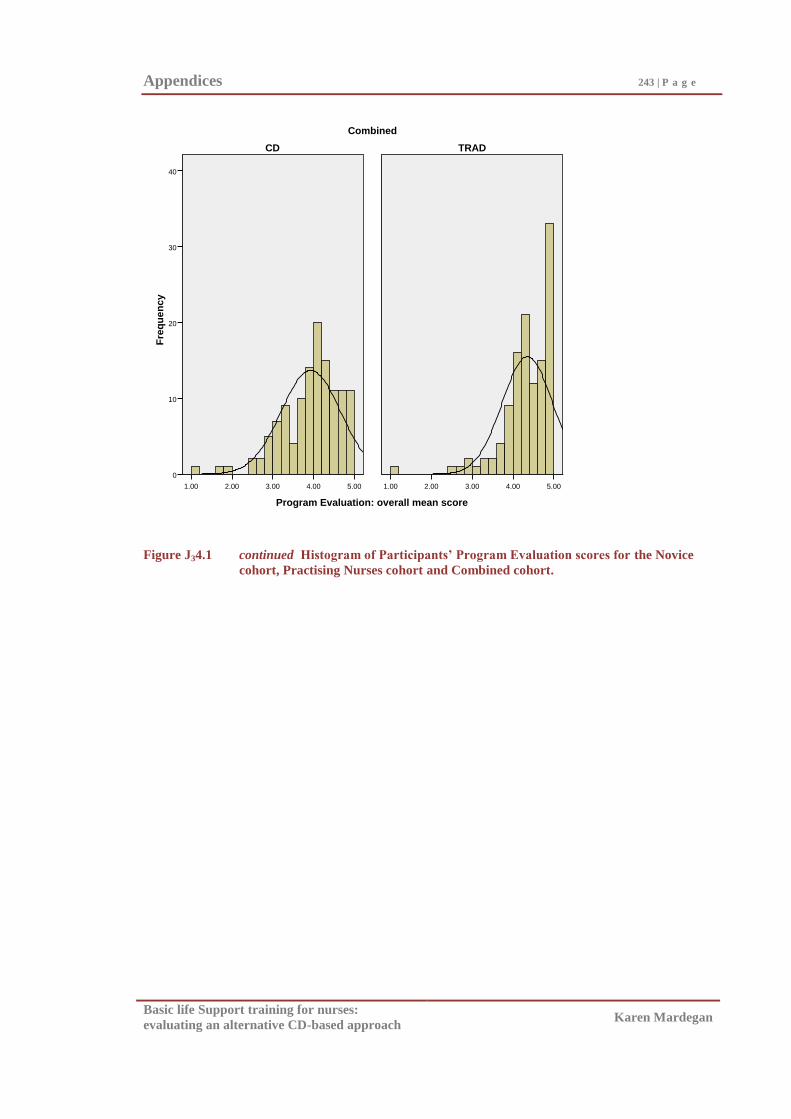
Appendices 243 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Program Evaluation: overall mean score
5.004.003.002.001.00
Fre
qu
en
cy
40
30
20
10
0
5.004.003.002.001.00
Combined
TRADCD
Figure J34.1 continued Histogram of Participants’ Program Evaluation scores for the Novice
cohort, Practising Nurses cohort and Combined cohort.
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix K
BLS Skill: Specific Skills Results
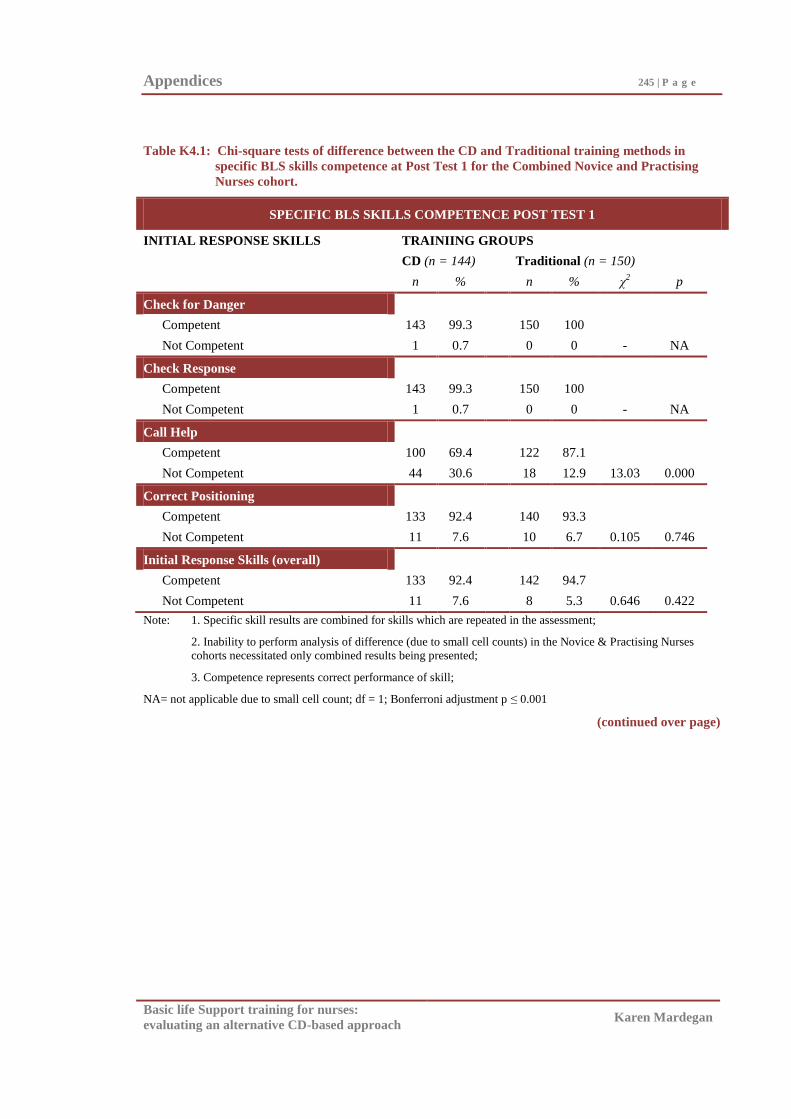
Appendices 245 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.1: Chi-square tests of difference between the CD and Traditional training methods in
specific BLS skills competence at Post Test 1 for the Combined Novice and Practising
Nurses cohort.
SPECIFIC BLS SKILLS COMPETENCE POST TEST 1
INITIAL RESPONSE SKILLS TRAINIING GROUPS
CD (n = 144) Traditional (n = 150)
n % n % χ2 p
Check for Danger
Competent 143 99.3 150 100
Not Competent 1 0.7 0 0 - NA
Check Response
Competent 143 99.3 150 100
Not Competent 1 0.7 0 0 - NA
Call Help
Competent 100 69.4 122 87.1
Not Competent 44 30.6 18 12.9 13.03 0.000
Correct Positioning
Competent 133 92.4 140 93.3
Not Competent 11 7.6 10 6.7 0.105 0.746
Initial Response Skills (overall)
Competent 133 92.4 142 94.7
Not Competent 11 7.6 8 5.3 0.646 0.422
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
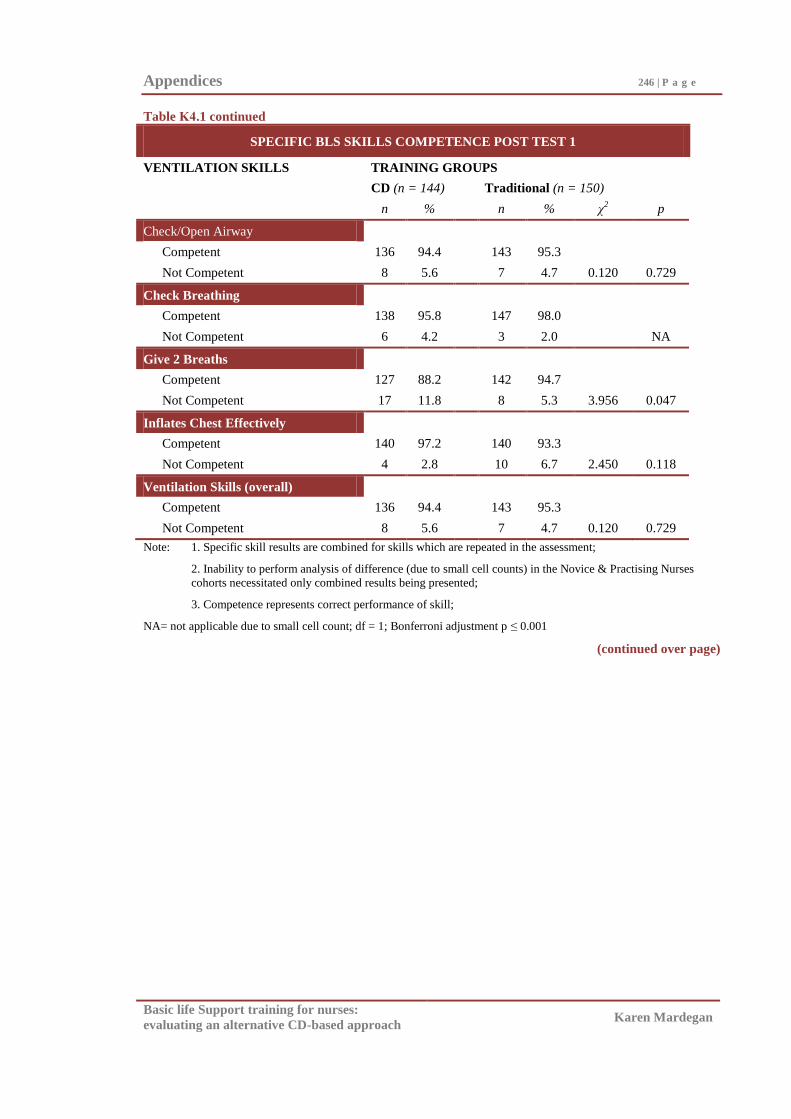
Appendices 246 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.1 continued
SPECIFIC BLS SKILLS COMPETENCE POST TEST 1
VENTILATION SKILLS TRAINING GROUPS
CD (n = 144) Traditional (n = 150)
n % n % χ2 p
Check/Open Airway
Competent 136 94.4 143 95.3
Not Competent 8 5.6 7 4.7 0.120 0.729
Check Breathing
Competent 138 95.8 147 98.0
Not Competent 6 4.2 3 2.0 NA
Give 2 Breaths
Competent 127 88.2 142 94.7
Not Competent 17 11.8 8 5.3 3.956 0.047
Inflates Chest Effectively
Competent 140 97.2 140 93.3
Not Competent 4 2.8 10 6.7 2.450 0.118
Ventilation Skills (overall)
Competent 136 94.4 143 95.3
Not Competent 8 5.6 7 4.7 0.120 0.729
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
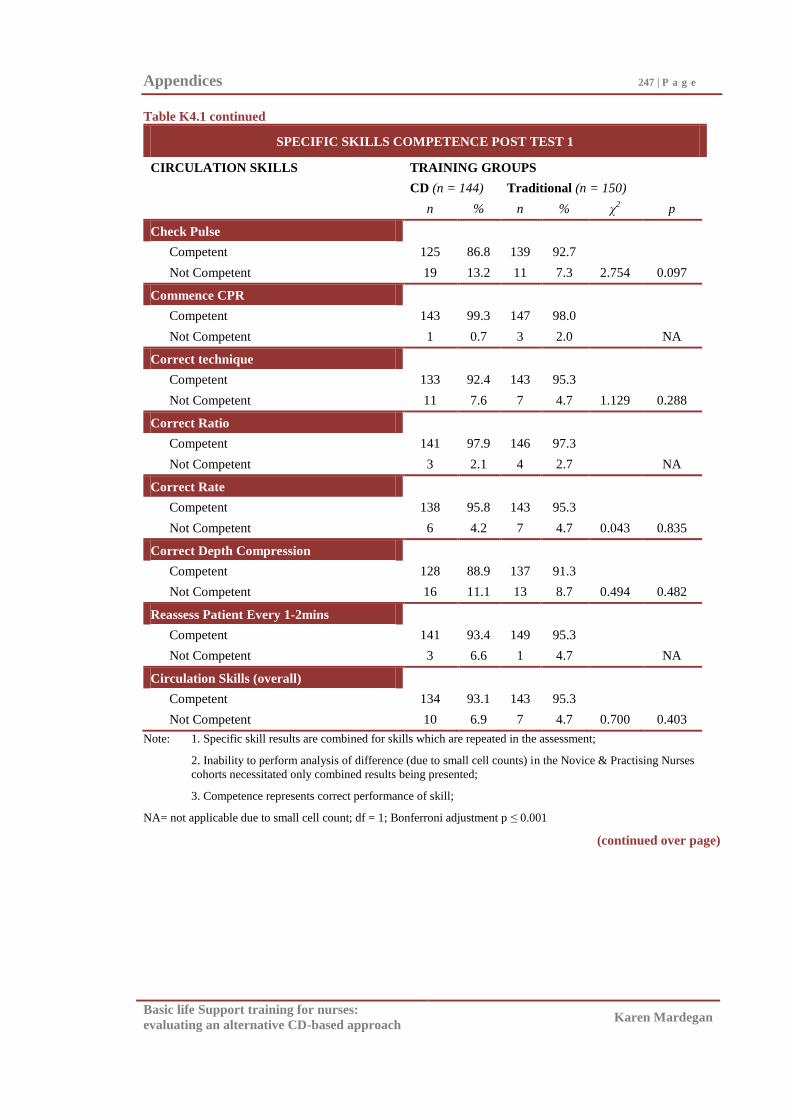
Appendices 247 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.1 continued
SPECIFIC SKILLS COMPETENCE POST TEST 1
CIRCULATION SKILLS TRAINING GROUPS
CD (n = 144) Traditional (n = 150)
n % n % χ2 p
Check Pulse
Competent 125 86.8 139 92.7
Not Competent 19 13.2 11 7.3 2.754 0.097
Commence CPR
Competent 143 99.3 147 98.0
Not Competent 1 0.7 3 2.0 NA
Correct technique
Competent 133 92.4 143 95.3
Not Competent 11 7.6 7 4.7 1.129 0.288
Correct Ratio
Competent 141 97.9 146 97.3
Not Competent 3 2.1 4 2.7 NA
Correct Rate
Competent 138 95.8 143 95.3
Not Competent 6 4.2 7 4.7 0.043 0.835
Correct Depth Compression
Competent 128 88.9 137 91.3
Not Competent 16 11.1 13 8.7 0.494 0.482
Reassess Patient Every 1-2mins
Competent 141 93.4 149 95.3
Not Competent 3 6.6 1 4.7 NA
Circulation Skills (overall)
Competent 134 93.1 143 95.3
Not Competent 10 6.9 7 4.7 0.700 0.403
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
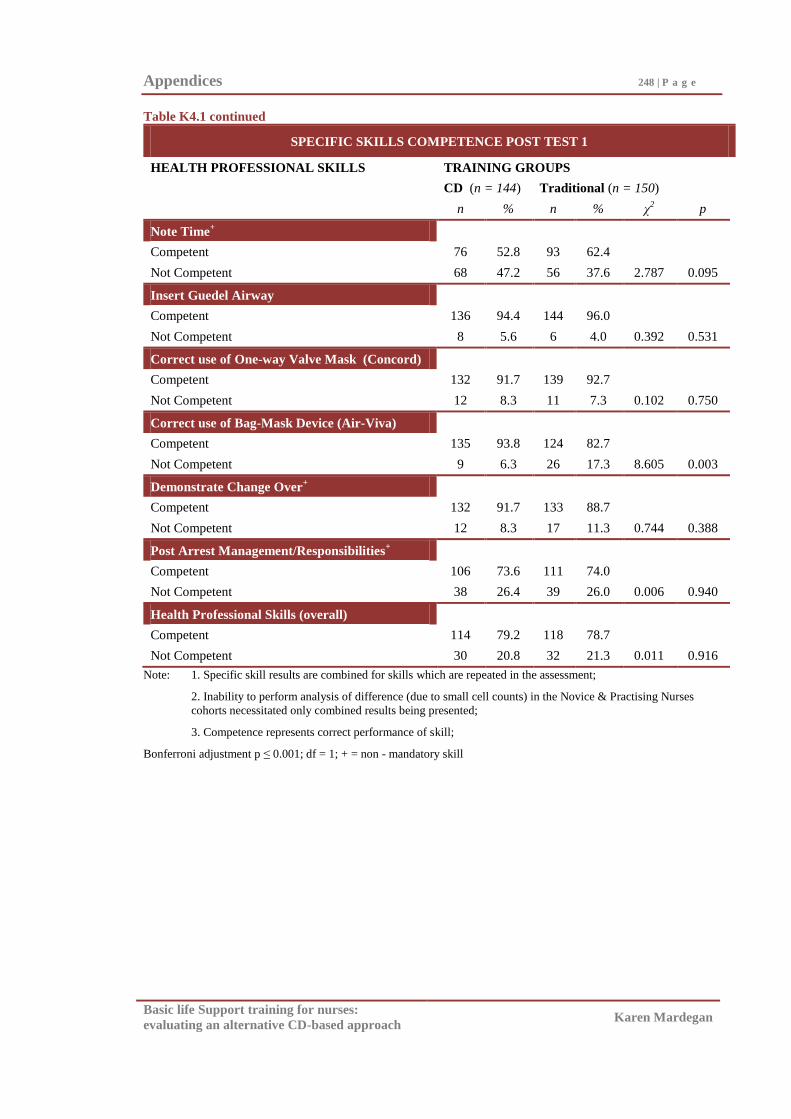
Appendices 248 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.1 continued
SPECIFIC SKILLS COMPETENCE POST TEST 1
HEALTH PROFESSIONAL SKILLS TRAINING GROUPS
CD (n = 144) Traditional (n = 150)
n % n % χ2 p
Note Time+
Competent 76 52.8 93 62.4
Not Competent 68 47.2 56 37.6 2.787 0.095
Insert Guedel Airway
Competent 136 94.4 144 96.0
Not Competent 8 5.6 6 4.0 0.392 0.531
Correct use of One-way Valve Mask (Concord)
Competent 132 91.7 139 92.7
Not Competent 12 8.3 11 7.3 0.102 0.750
Correct use of Bag-Mask Device (Air-Viva)
Competent 135 93.8 124 82.7
Not Competent 9 6.3 26 17.3 8.605 0.003
Demonstrate Change Over+
Competent 132 91.7 133 88.7
Not Competent 12 8.3 17 11.3 0.744 0.388
Post Arrest Management/Responsibilities+
Competent 106 73.6 111 74.0
Not Competent 38 26.4 39 26.0 0.006 0.940
Health Professional Skills (overall)
Competent 114 79.2 118 78.7
Not Competent 30 20.8 32 21.3 0.011 0.916
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
Bonferroni adjustment p ≤ 0.001; df = 1; + = non - mandatory skill
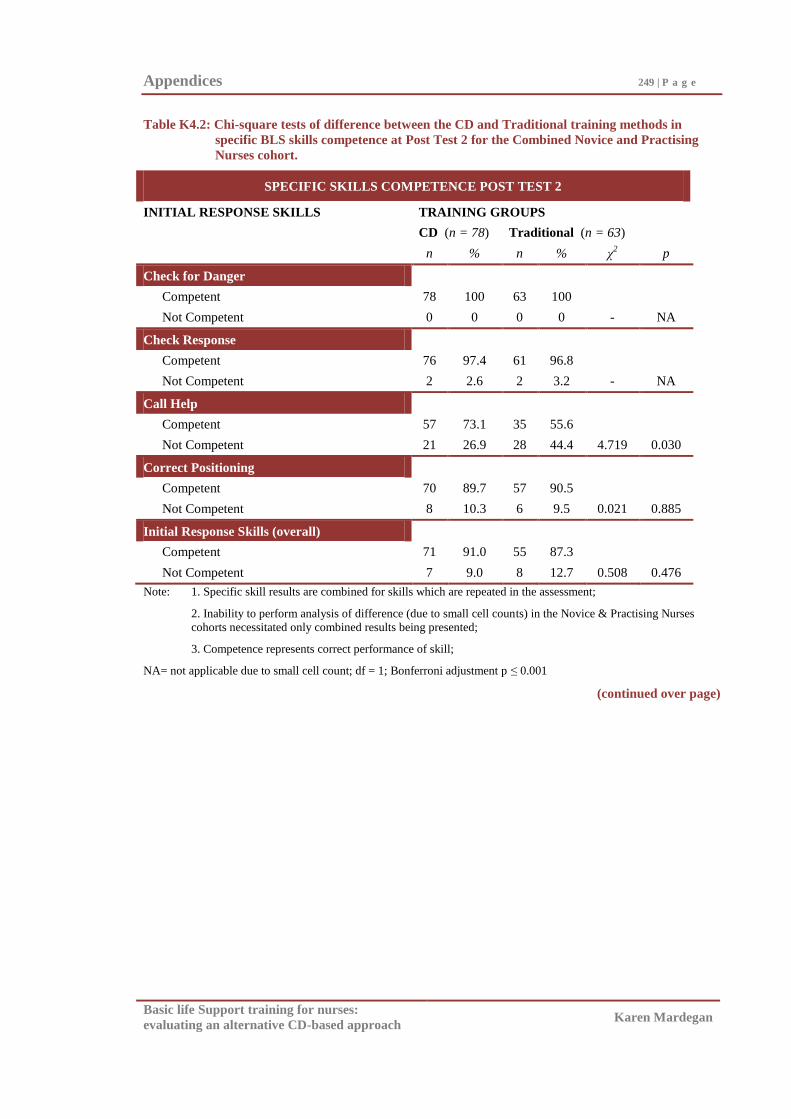
Appendices 249 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.2: Chi-square tests of difference between the CD and Traditional training methods in
specific BLS skills competence at Post Test 2 for the Combined Novice and Practising
Nurses cohort.
SPECIFIC SKILLS COMPETENCE POST TEST 2
INITIAL RESPONSE SKILLS TRAINING GROUPS
CD (n = 78) Traditional (n = 63)
n % n % χ2 p
Check for Danger
Competent 78 100 63 100
Not Competent 0 0 0 0 - NA
Check Response
Competent 76 97.4 61 96.8
Not Competent 2 2.6 2 3.2 - NA
Call Help
Competent 57 73.1 35 55.6
Not Competent 21 26.9 28 44.4 4.719 0.030
Correct Positioning
Competent 70 89.7 57 90.5
Not Competent 8 10.3 6 9.5 0.021 0.885
Initial Response Skills (overall)
Competent 71 91.0 55 87.3
Not Competent 7 9.0 8 12.7 0.508 0.476
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
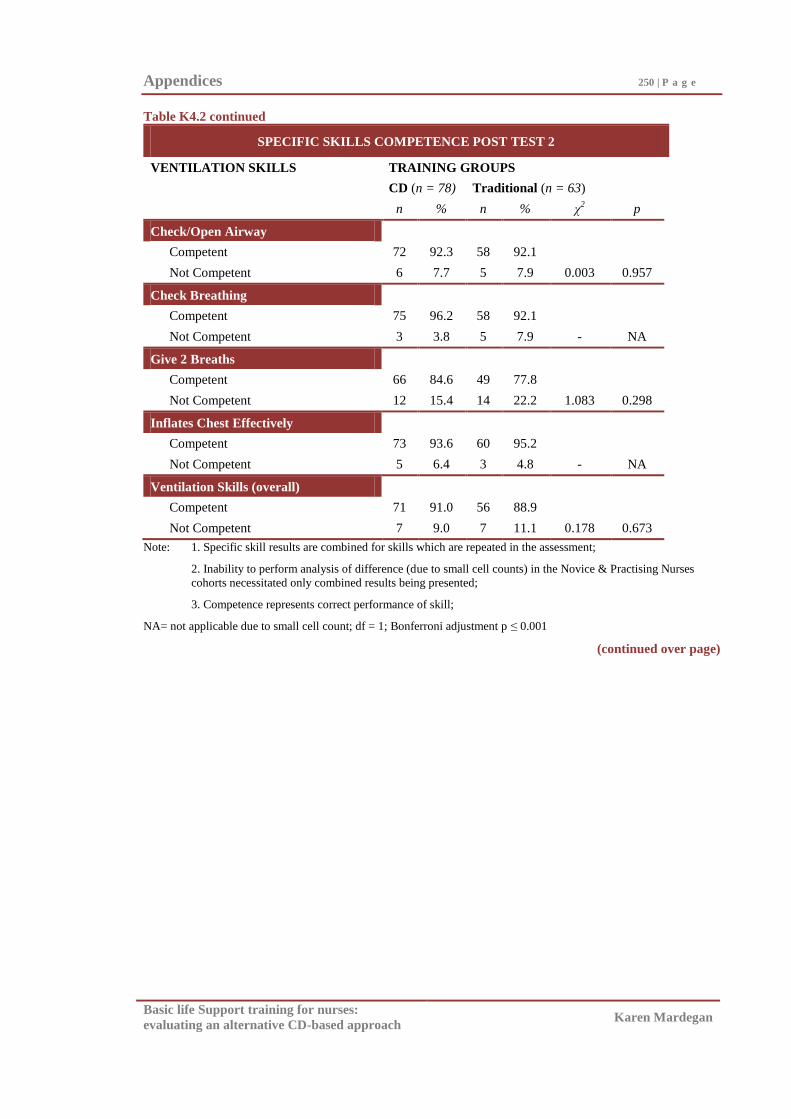
Appendices 250 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.2 continued
SPECIFIC SKILLS COMPETENCE POST TEST 2
VENTILATION SKILLS TRAINING GROUPS
CD (n = 78) Traditional (n = 63)
n % n % χ2 p
Check/Open Airway
Competent 72 92.3 58 92.1
Not Competent 6 7.7 5 7.9 0.003 0.957
Check Breathing
Competent 75 96.2 58 92.1
Not Competent 3 3.8 5 7.9 - NA
Give 2 Breaths
Competent 66 84.6 49 77.8
Not Competent 12 15.4 14 22.2 1.083 0.298
Inflates Chest Effectively
Competent 73 93.6 60 95.2
Not Competent 5 6.4 3 4.8 - NA
Ventilation Skills (overall)
Competent 71 91.0 56 88.9
Not Competent 7 9.0 7 11.1 0.178 0.673
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
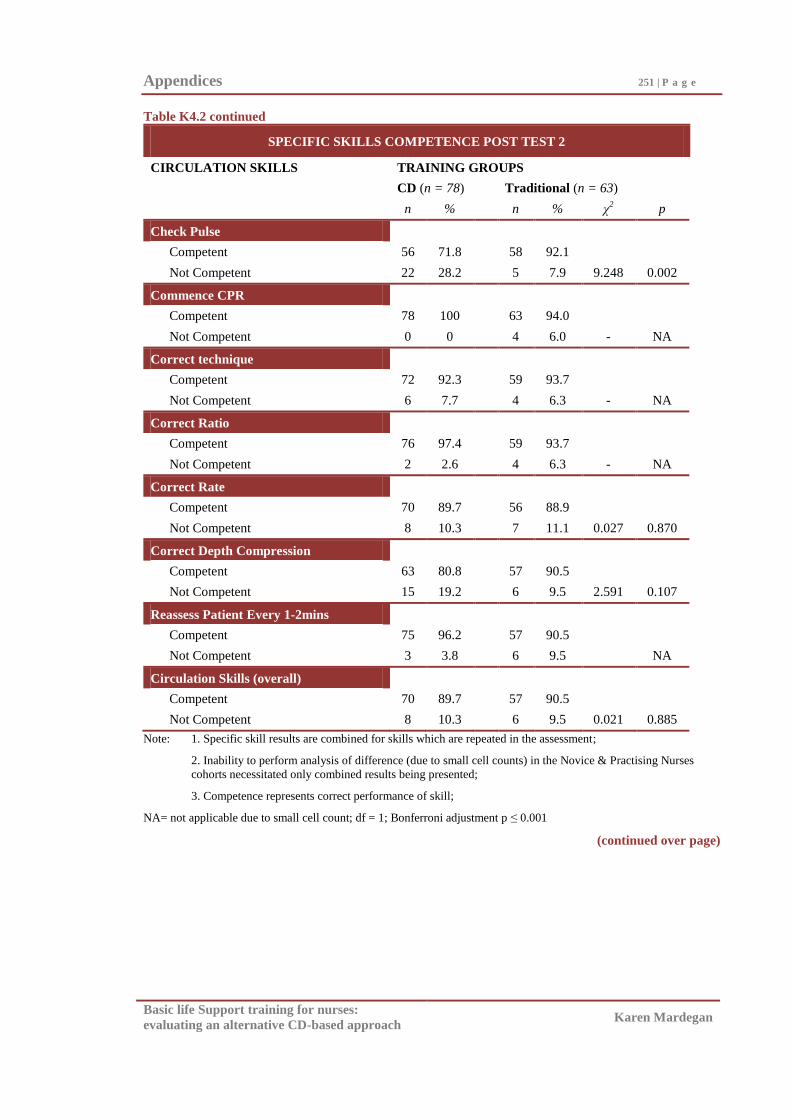
Appendices 251 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.2 continued
SPECIFIC SKILLS COMPETENCE POST TEST 2
CIRCULATION SKILLS TRAINING GROUPS
CD (n = 78) Traditional (n = 63)
n % n % χ2 p
Check Pulse
Competent 56 71.8 58 92.1
Not Competent 22 28.2 5 7.9 9.248 0.002
Commence CPR
Competent 78 100 63 94.0
Not Competent 0 0 4 6.0 - NA
Correct technique
Competent 72 92.3 59 93.7
Not Competent 6 7.7 4 6.3 - NA
Correct Ratio
Competent 76 97.4 59 93.7
Not Competent 2 2.6 4 6.3 - NA
Correct Rate
Competent 70 89.7 56 88.9
Not Competent 8 10.3 7 11.1 0.027 0.870
Correct Depth Compression
Competent 63 80.8 57 90.5
Not Competent 15 19.2 6 9.5 2.591 0.107
Reassess Patient Every 1-2mins
Competent 75 96.2 57 90.5
Not Competent 3 3.8 6 9.5 NA
Circulation Skills (overall)
Competent 70 89.7 57 90.5
Not Competent 8 10.3 6 9.5 0.021 0.885
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
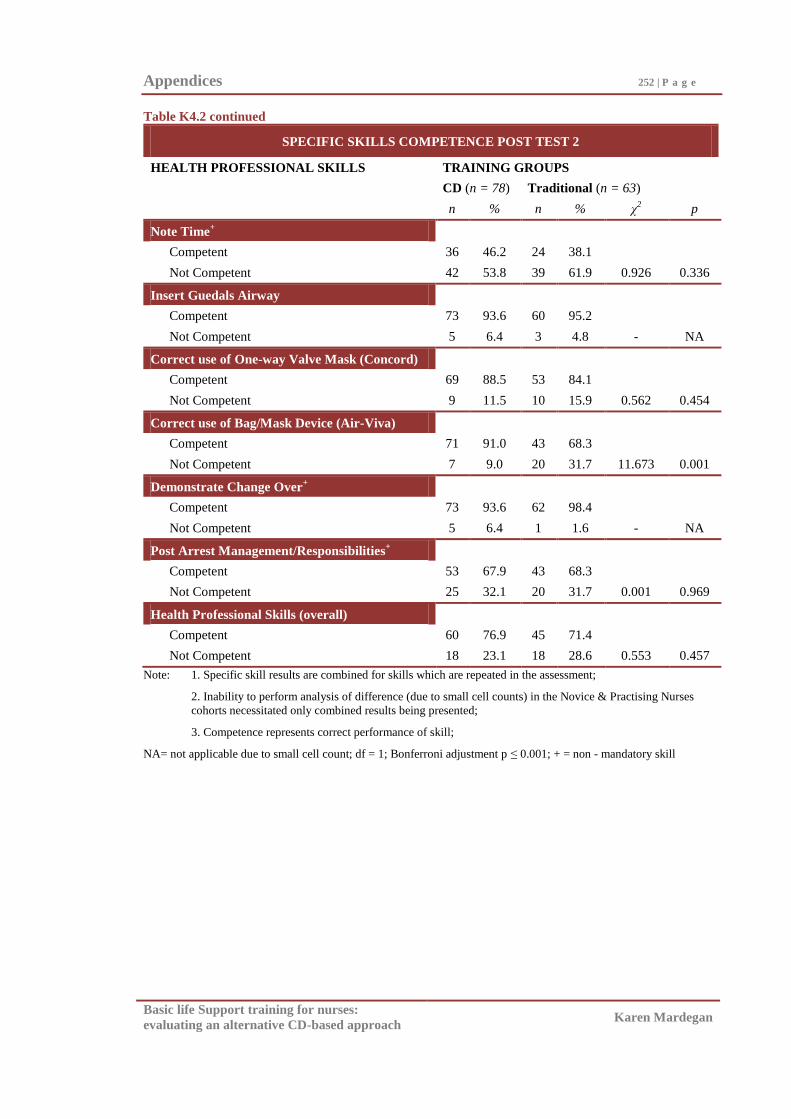
Appendices 252 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table K4.2 continued
SPECIFIC SKILLS COMPETENCE POST TEST 2
HEALTH PROFESSIONAL SKILLS TRAINING GROUPS
CD (n = 78) Traditional (n = 63)
n % n % χ2 p
Note Time+
Competent 36 46.2 24 38.1
Not Competent 42 53.8 39 61.9 0.926 0.336
Insert Guedals Airway
Competent 73 93.6 60 95.2
Not Competent 5 6.4 3 4.8 - NA
Correct use of One-way Valve Mask (Concord)
Competent 69 88.5 53 84.1
Not Competent 9 11.5 10 15.9 0.562 0.454
Correct use of Bag/Mask Device (Air-Viva)
Competent 71 91.0 43 68.3
Not Competent 7 9.0 20 31.7 11.673 0.001
Demonstrate Change Over+
Competent 73 93.6 62 98.4
Not Competent 5 6.4 1 1.6 - NA
Post Arrest Management/Responsibilities+
Competent 53 67.9 43 68.3
Not Competent 25 32.1 20 31.7 0.001 0.969
Health Professional Skills (overall)
Competent 60 76.9 45 71.4
Not Competent 18 23.1 18 28.6 0.553 0.457
Note: 1. Specific skill results are combined for skills which are repeated in the assessment;
2. Inability to perform analysis of difference (due to small cell counts) in the Novice & Practising Nurses
cohorts necessitated only combined results being presented;
3. Competence represents correct performance of skill;
NA= not applicable due to small cell count; df = 1; Bonferroni adjustment p ≤ 0.001; + = non - mandatory skill
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix L
BLS Knowledge: Specific Questions Results
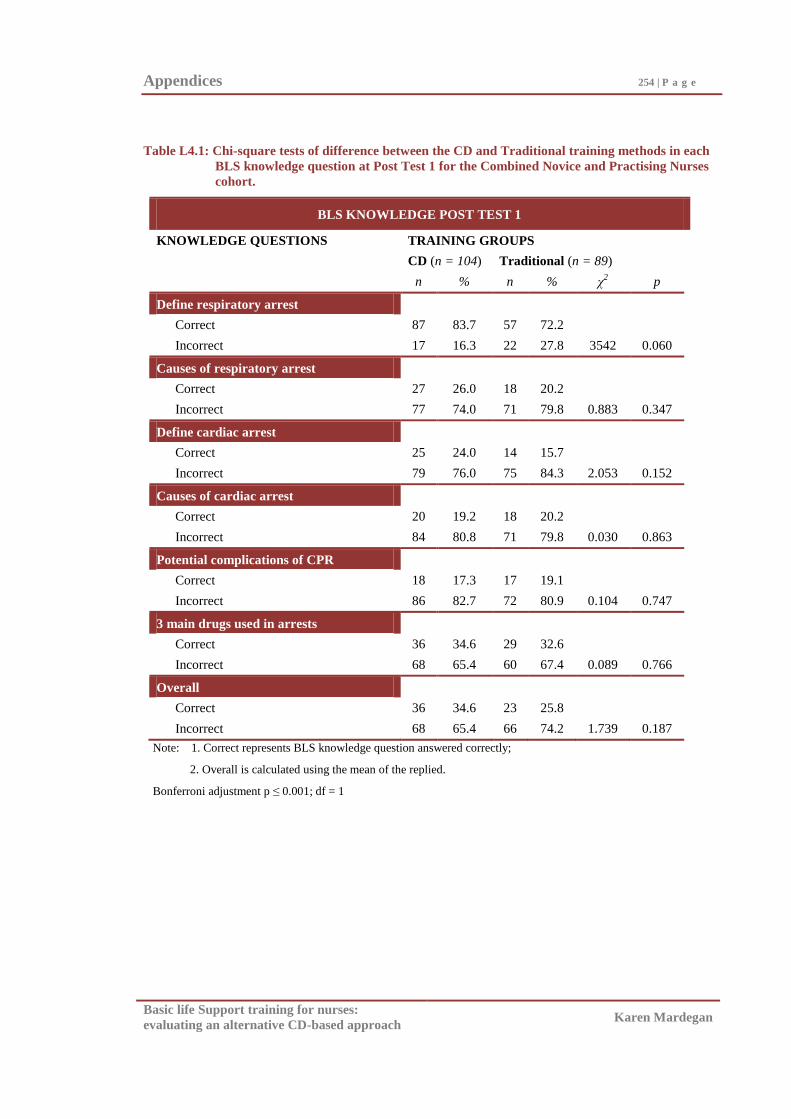
Appendices 254 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table L4.1: Chi-square tests of difference between the CD and Traditional training methods in each
BLS knowledge question at Post Test 1 for the Combined Novice and Practising Nurses
cohort.
BLS KNOWLEDGE POST TEST 1
KNOWLEDGE QUESTIONS TRAINING GROUPS
CD (n = 104) Traditional (n = 89)
n % n % χ2 p
Define respiratory arrest
Correct 87 83.7 57 72.2
Incorrect 17 16.3 22 27.8 3542 0.060
Causes of respiratory arrest
Correct 27 26.0 18 20.2
Incorrect 77 74.0 71 79.8 0.883 0.347
Define cardiac arrest
Correct 25 24.0 14 15.7
Incorrect 79 76.0 75 84.3 2.053 0.152
Causes of cardiac arrest
Correct 20 19.2 18 20.2
Incorrect 84 80.8 71 79.8 0.030 0.863
Potential complications of CPR
Correct 18 17.3 17 19.1
Incorrect 86 82.7 72 80.9 0.104 0.747
3 main drugs used in arrests
Correct 36 34.6 29 32.6
Incorrect 68 65.4 60 67.4 0.089 0.766
Overall
Correct 36 34.6 23 25.8
Incorrect 68 65.4 66 74.2 1.739 0.187
Note: 1. Correct represents BLS knowledge question answered correctly;
2. Overall is calculated using the mean of the replied.
Bonferroni adjustment p ≤ 0.001; df = 1
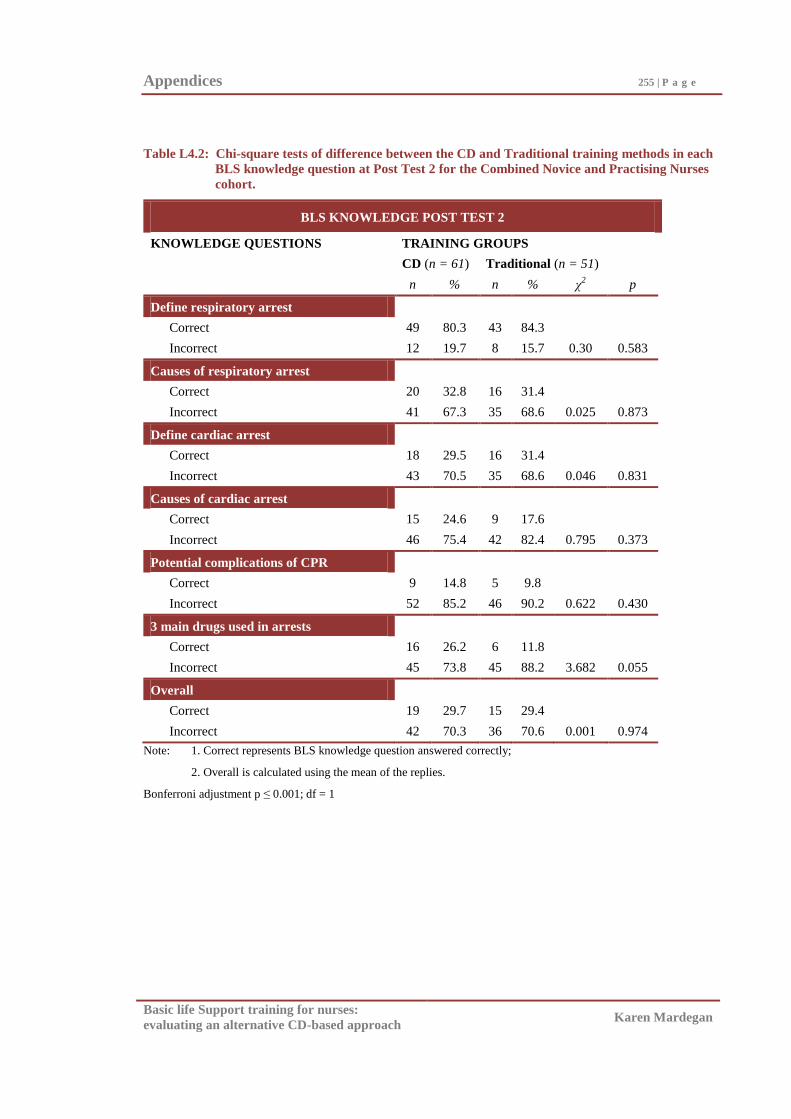
Appendices 255 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table L4.2: Chi-square tests of difference between the CD and Traditional training methods in each
BLS knowledge question at Post Test 2 for the Combined Novice and Practising Nurses
cohort.
BLS KNOWLEDGE POST TEST 2
KNOWLEDGE QUESTIONS TRAINING GROUPS
CD (n = 61) Traditional (n = 51)
n % n % χ2 p
Define respiratory arrest
Correct 49 80.3 43 84.3
Incorrect 12 19.7 8 15.7 0.30 0.583
Causes of respiratory arrest
Correct 20 32.8 16 31.4
Incorrect 41 67.3 35 68.6 0.025 0.873
Define cardiac arrest
Correct 18 29.5 16 31.4
Incorrect 43 70.5 35 68.6 0.046 0.831
Causes of cardiac arrest
Correct 15 24.6 9 17.6
Incorrect 46 75.4 42 82.4 0.795 0.373
Potential complications of CPR
Correct 9 14.8 5 9.8
Incorrect 52 85.2 46 90.2 0.622 0.430
3 main drugs used in arrests
Correct 16 26.2 6 11.8
Incorrect 45 73.8 45 88.2 3.682 0.055
Overall
Correct 19 29.7 15 29.4
Incorrect 42 70.3 36 70.6 0.001 0.974
Note: 1. Correct represents BLS knowledge question answered correctly;
2. Overall is calculated using the mean of the replies.
Bonferroni adjustment p ≤ 0.001; df = 1
Basic life support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Appendix M
Participants‘ Rating of the BLS Training Programs:
Specific Questions Results
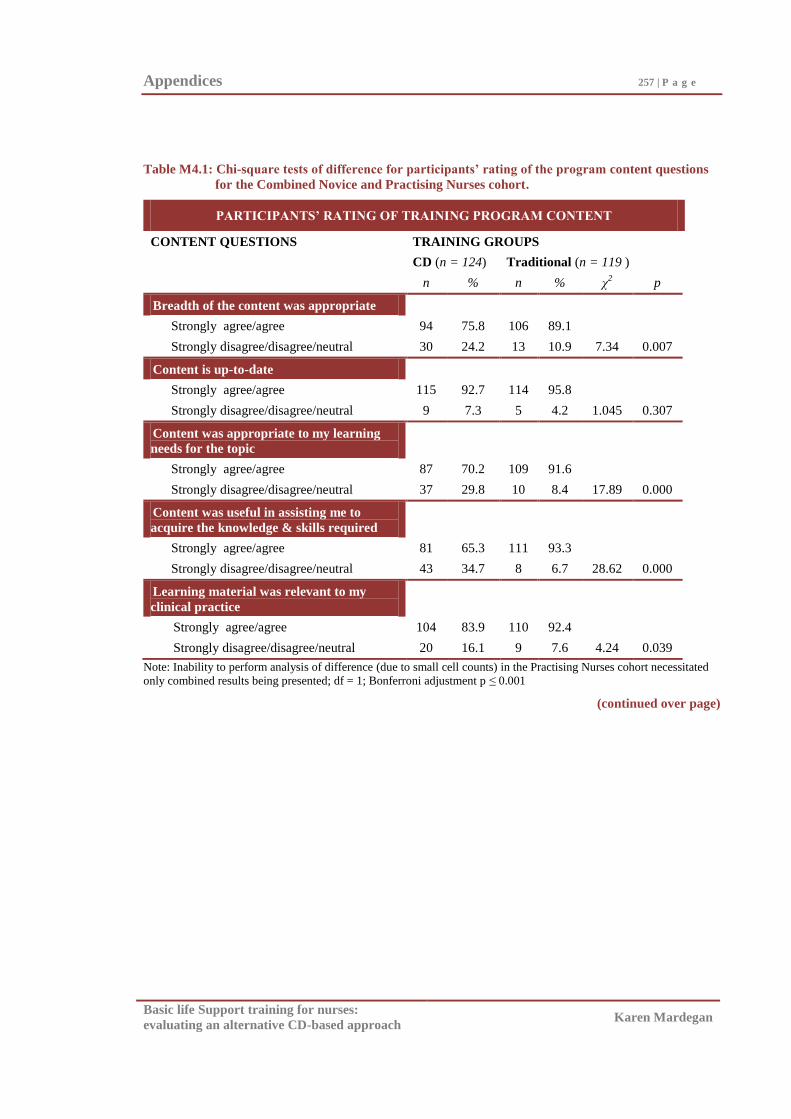
Appendices 257 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table M4.1: Chi-square tests of difference for participants’ rating of the program content questions
for the Combined Novice and Practising Nurses cohort.
PARTICIPANTS’ RATING OF TRAINING PROGRAM CONTENT
CONTENT QUESTIONS TRAINING GROUPS
CD (n = 124) Traditional (n = 119 )
n % n % χ2 p
Breadth of the content was appropriate
Strongly agree/agree 94 75.8 106 89.1
Strongly disagree/disagree/neutral 30 24.2 13 10.9 7.34 0.007
Content is up-to-date
Strongly agree/agree 115 92.7 114 95.8
Strongly disagree/disagree/neutral 9 7.3 5 4.2 1.045 0.307
Content was appropriate to my learning
needs for the topic
Strongly agree/agree 87 70.2 109 91.6
Strongly disagree/disagree/neutral 37 29.8 10 8.4 17.89 0.000
Content was useful in assisting me to
acquire the knowledge & skills required
Strongly agree/agree 81 65.3 111 93.3
Strongly disagree/disagree/neutral 43 34.7 8 6.7 28.62 0.000
Learning material was relevant to my
clinical practice
Strongly agree/agree 104 83.9 110 92.4
Strongly disagree/disagree/neutral 20 16.1 9 7.6 4.24 0.039
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; df = 1; Bonferroni adjustment p ≤ 0.001
(continued over page)
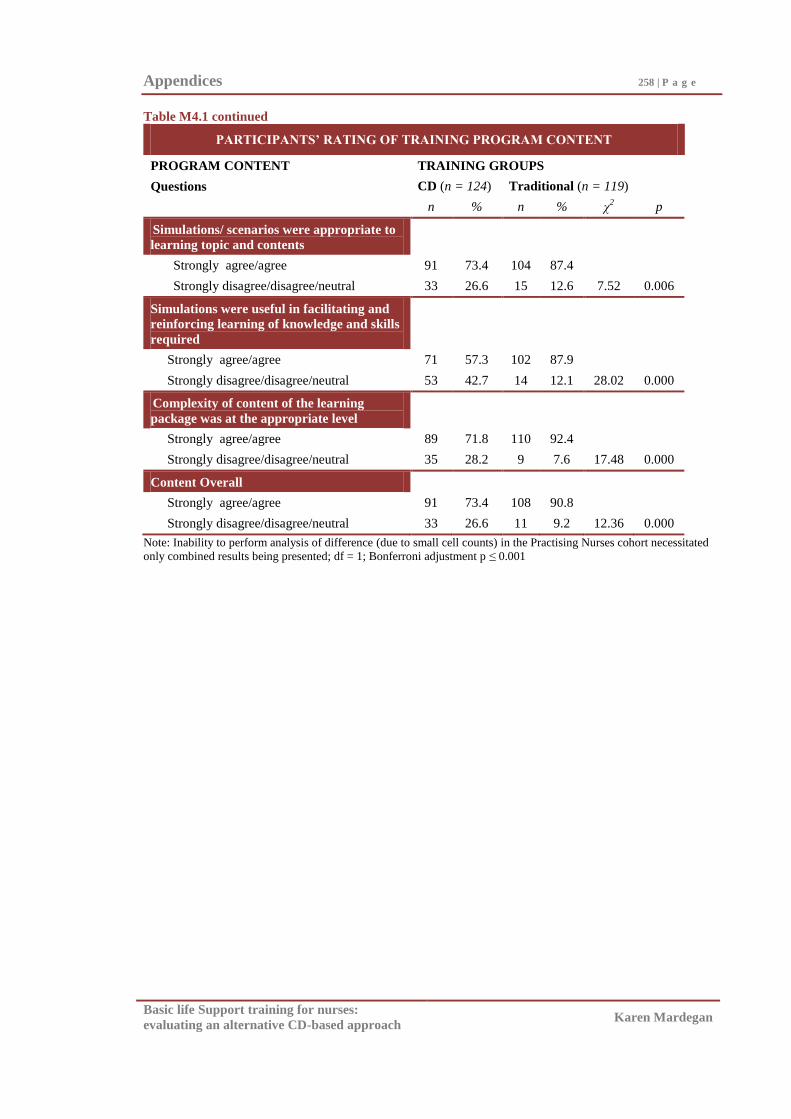
Appendices 258 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table M4.1 continued
PARTICIPANTS’ RATING OF TRAINING PROGRAM CONTENT
PROGRAM CONTENT TRAINING GROUPS
Questions CD (n = 124) Traditional (n = 119)
n % n % χ2 p
Simulations/ scenarios were appropriate to
learning topic and contents
Strongly agree/agree 91 73.4 104 87.4
Strongly disagree/disagree/neutral 33 26.6 15 12.6 7.52 0.006
Simulations were useful in facilitating and
reinforcing learning of knowledge and skills
required
Strongly agree/agree 71 57.3 102 87.9
Strongly disagree/disagree/neutral 53 42.7 14 12.1 28.02 0.000
Complexity of content of the learning
package was at the appropriate level
Strongly agree/agree 89 71.8 110 92.4
Strongly disagree/disagree/neutral 35 28.2 9 7.6 17.48 0.000
Content Overall
Strongly agree/agree 91 73.4 108 90.8
Strongly disagree/disagree/neutral 33 26.6 11 9.2 12.36 0.000
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; df = 1; Bonferroni adjustment p ≤ 0.001
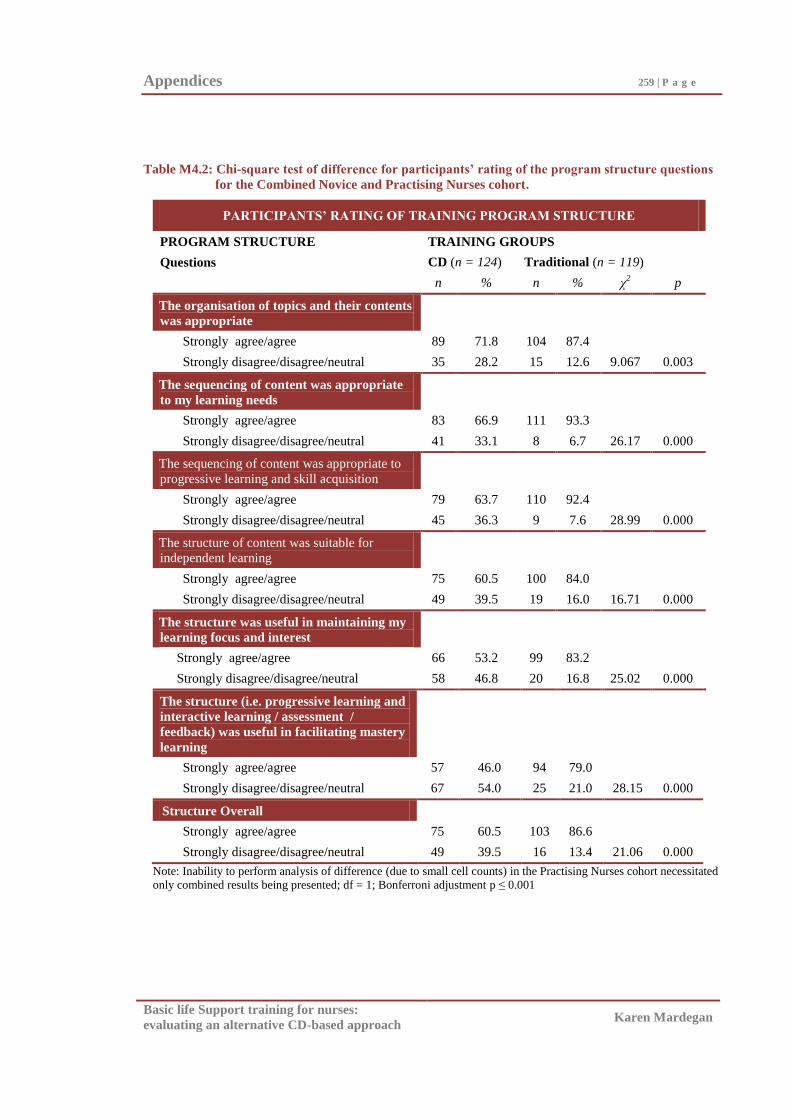
Appendices 259 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table M4.2: Chi-square test of difference for participants’ rating of the program structure questions
for the Combined Novice and Practising Nurses cohort.
PARTICIPANTS’ RATING OF TRAINING PROGRAM STRUCTURE
PROGRAM STRUCTURE TRAINING GROUPS
Questions CD (n = 124) Traditional (n = 119)
n % n % χ2 p
The organisation of topics and their contents
was appropriate
Strongly agree/agree 89 71.8 104 87.4
Strongly disagree/disagree/neutral 35 28.2 15 12.6 9.067 0.003
The sequencing of content was appropriate
to my learning needs
Strongly agree/agree 83 66.9 111 93.3
Strongly disagree/disagree/neutral 41 33.1 8 6.7 26.17 0.000
The sequencing of content was appropriate to
progressive learning and skill acquisition
Strongly agree/agree 79 63.7 110 92.4
Strongly disagree/disagree/neutral 45 36.3 9 7.6 28.99 0.000
The structure of content was suitable for
independent learning
Strongly agree/agree 75 60.5 100 84.0
Strongly disagree/disagree/neutral 49 39.5 19 16.0 16.71 0.000
The structure was useful in maintaining my
learning focus and interest
Strongly agree/agree 66 53.2 99 83.2
Strongly disagree/disagree/neutral 58 46.8 20 16.8 25.02 0.000
The structure (i.e. progressive learning and
interactive learning / assessment /
feedback) was useful in facilitating mastery
learning
Strongly agree/agree 57 46.0 94 79.0
Strongly disagree/disagree/neutral 67 54.0 25 21.0 28.15 0.000
Structure Overall
Strongly agree/agree 75 60.5 103 86.6
Strongly disagree/disagree/neutral 49 39.5 16 13.4 21.06 0.000
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; df = 1; Bonferroni adjustment p ≤ 0.001
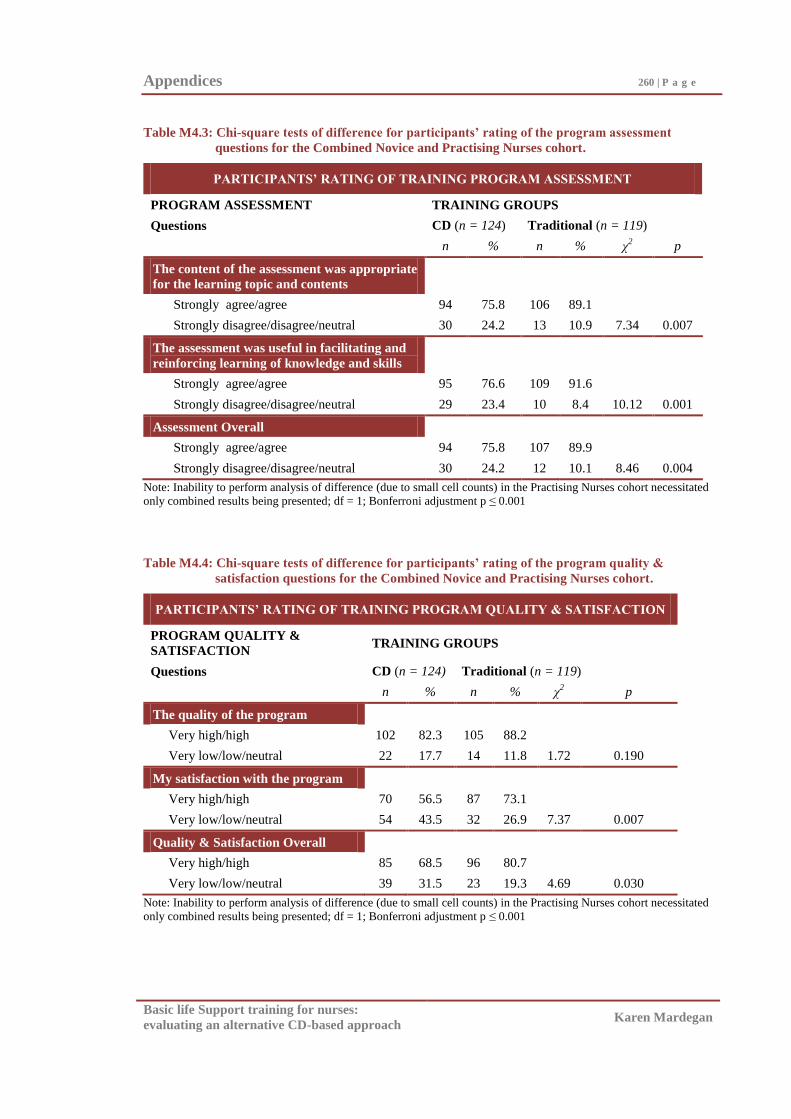
Appendices 260 | P a g e
Basic life Support training for nurses:
evaluating an alternative CD-based approach Karen Mardegan
Table M4.3: Chi-square tests of difference for participants’ rating of the program assessment
questions for the Combined Novice and Practising Nurses cohort.
PARTICIPANTS’ RATING OF TRAINING PROGRAM ASSESSMENT
PROGRAM ASSESSMENT TRAINING GROUPS
Questions CD (n = 124) Traditional (n = 119)
n % n % χ2 p
The content of the assessment was appropriate
for the learning topic and contents
Strongly agree/agree 94 75.8 106 89.1
Strongly disagree/disagree/neutral 30 24.2 13 10.9 7.34 0.007
The assessment was useful in facilitating and
reinforcing learning of knowledge and skills
Strongly agree/agree 95 76.6 109 91.6
Strongly disagree/disagree/neutral 29 23.4 10 8.4 10.12 0.001
Assessment Overall
Strongly agree/agree 94 75.8 107 89.9
Strongly disagree/disagree/neutral 30 24.2 12 10.1 8.46 0.004
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; df = 1; Bonferroni adjustment p ≤ 0.001
Table M4.4: Chi-square tests of difference for participants’ rating of the program quality &
satisfaction questions for the Combined Novice and Practising Nurses cohort.
PARTICIPANTS’ RATING OF TRAINING PROGRAM QUALITY & SATISFACTION
PROGRAM QUALITY &
SATISFACTION TRAINING GROUPS
Questions CD (n = 124) Traditional (n = 119)
n % n % χ2 p
The quality of the program
Very high/high 102 82.3 105 88.2
Very low/low/neutral 22 17.7 14 11.8 1.72 0.190
My satisfaction with the program
Very high/high 70 56.5 87 73.1
Very low/low/neutral 54 43.5 32 26.9 7.37 0.007
Quality & Satisfaction Overall
Very high/high 85 68.5 96 80.7
Very low/low/neutral 39 31.5 23 19.3 4.69 0.030
Note: Inability to perform analysis of difference (due to small cell counts) in the Practising Nurses cohort necessitated
only combined results being presented; df = 1; Bonferroni adjustment p ≤ 0.001