basingstoke colorectal how imaging has improved outcome in rectal cancer 4 th east- west colorectal...
TRANSCRIPT

Basingstoke Colorectal
How Imaging Has Improved Outcome In Rectal Cancer
4th East- West Colorectal Days Hungary
How Imaging Has Improved Outcome In Rectal Cancer
4th East- West Colorectal Days Hungary
Brendan Moran Brendan Moran
BasingstokeBasingstoke
OCTOBER 2008OCTOBER 2008
Brendan Moran Brendan Moran
BasingstokeBasingstoke
OCTOBER 2008OCTOBER 2008

Basingstoke Colorectal

Basingstoke Colorectal
Image and ImagingImage and Imaging
“ A picture is worth a
thousand words”
Chinese Proverb
“ A picture is worth a
thousand words”
Chinese Proverb

Basingstoke Colorectal
What does this illustrate ?What does this illustrate ?
Attempt to describe a
“revolutionary” theory
Heald, Husband, Ryall BJS 1982
Attempt to describe a
“revolutionary” theory
Heald, Husband, Ryall BJS 1982

Basingstoke Colorectal
But ?But ?
Inaccurate Drawing Not applicable to
upper rectal cancer Only 5 patients Nevertheless most
quoted paper ever in rectal cancer
Heald et al BJS 1982
Inaccurate Drawing Not applicable to
upper rectal cancer Only 5 patients Nevertheless most
quoted paper ever in rectal cancer
Heald et al BJS 1982
Basingstoke Colorectal
“The mesorectum in rectal cancer surgery -the clue to pelvic recurrence”“The mesorectum in rectal cancer surgery -the clue to pelvic recurrence”
Heald et al BJS 1982


Basingstoke Colorectal
TME EvolutionTME Evolution
Heald RJ Journal Royal Soc Med 1988

Basingstoke Colorectal
Rectal Cancer 80’s and 90’sRectal Cancer 80’s and 90’s
Surgery- TMEPre-operative RT –Sweden
Pathology -Quirke
Surgery- TMEPre-operative RT –Sweden
Pathology -Quirke
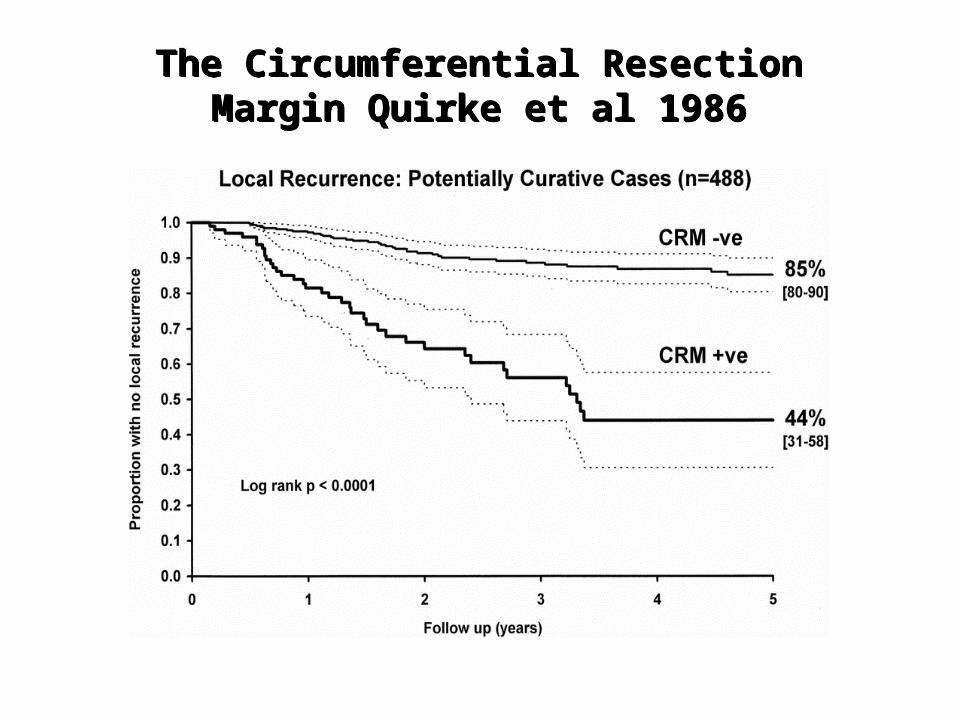
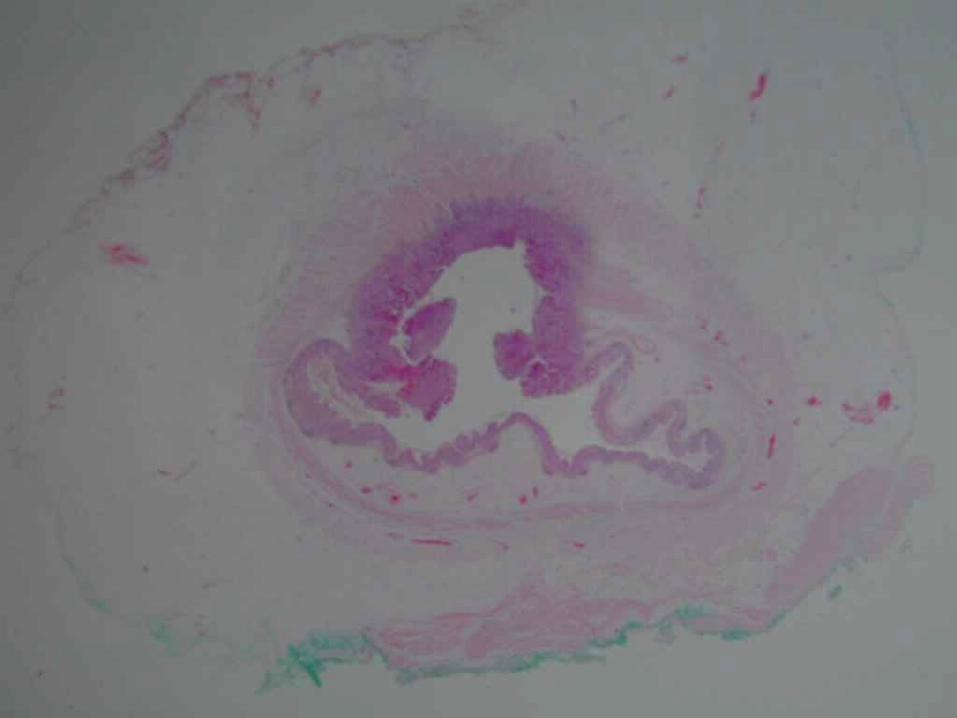
The Circumferential Resection Margin Quirke et al 1986
The Circumferential Resection Margin Quirke et al 1986

Basingstoke Colorectal
TME and RadiotherapyTME and Radiotherapy
Both aim at the circumferential margin
Both reduce the CRM involvement
Both aim at the circumferential margin
Both reduce the CRM involvement
0%
10%
20%
30%
40%
50%
0 1 2 3 4 5
Years
Loca
l rec
urre
nce
%
Norway
Netherlands
Enker
Moriya
Heald
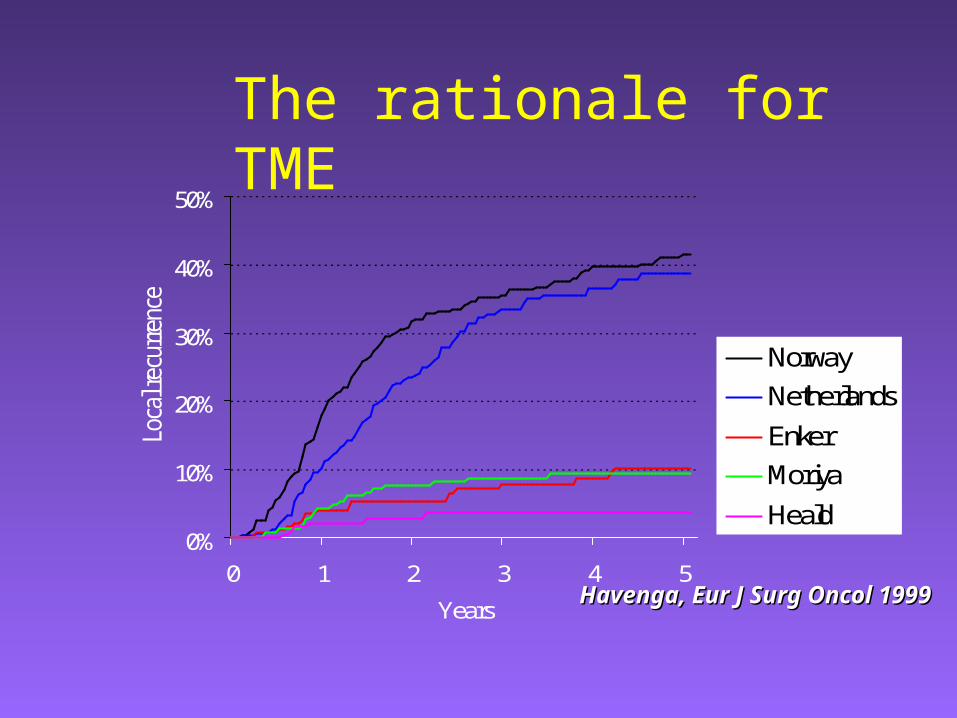
Havenga, Eur J Surg Oncol 1999Havenga, Eur J Surg Oncol 1999
The rationale for TME

Basingstoke Colorectal
Long Term Follow up Swedish Radiotherapy Study
Long Term Follow up Swedish Radiotherapy Study
The benefits are long lasting – at median follow-up 13 years [3–15]
Local recurrence rate 26% versus 9%
Folkesson et al JCO Aug 2005
The benefits are long lasting – at median follow-up 13 years [3–15]
Local recurrence rate 26% versus 9%
Folkesson et al JCO Aug 2005

Dutch TME TrialLocal Recurrence patients with macroscopically complete local resection (n=1789)
Dutch TME TrialLocal Recurrence patients with macroscopically complete local resection (n=1789)
5.8% vs 11.4% 5.8% vs 11.4% p < 0.001p < 0.001
TME alone
RT + TME
Van de Velde et al. Update at 5 yrs follow Van de Velde et al. Update at 5 yrs follow upup

Basingstoke Colorectal
Should we irradiate this patient ?
Should we irradiate this patient ?
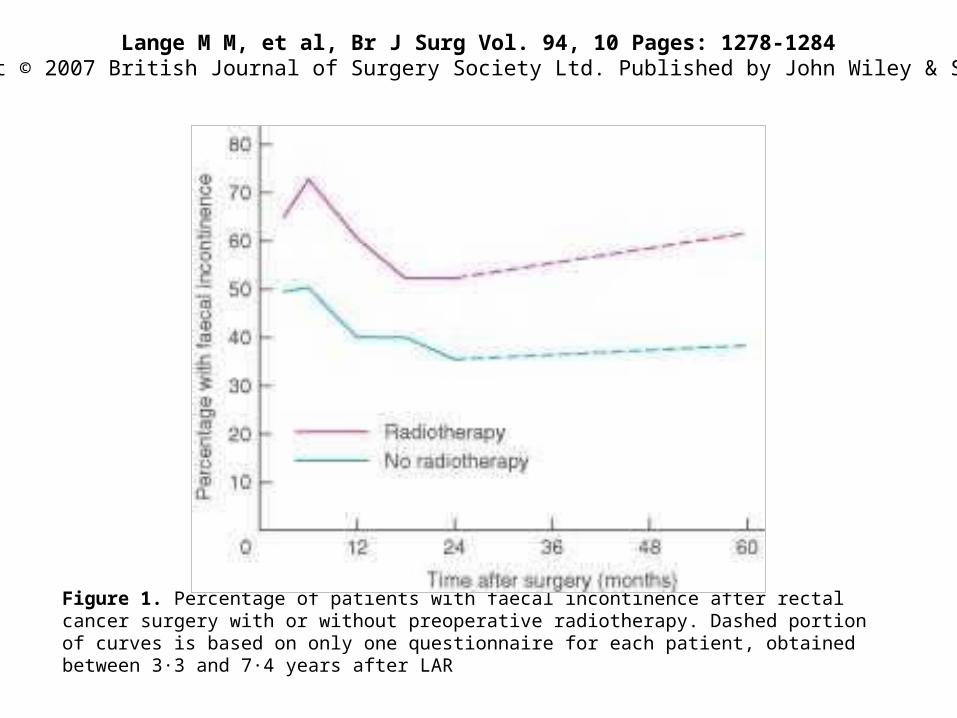
Lange M M, et al, Br J Surg Vol. 94, 10 Pages: 1278-1284Copyright © 2007 British Journal of Surgery Society Ltd. Published by John Wiley & Sons, Ltd
Figure 1. Percentage of patients with faecal incontinence after rectal cancer surgery with or without preoperative radiotherapy. Dashed portion of curves is based on only one questionnaire for each patient, obtained between 3·3 and 7·4 years after LAR

Br J Surg 2008; 95: 206-213Time after randomization (years)
Cum
ula
tive
pro
port
ion
with
out
late
bo
wel
obs
truc
tion,
tre
ated
sur
gica
lly
Late bowel obstruction treated surgically
Basingstoke Colorectal
Basingstoke Viewpoint BJS 2003
Simunovic et al. BJS 2003;90:999-1003

Basingstoke Colorectal
Selective pre-operative radiotherapy
Selective pre-operative radiotherapy
Definitely for an involved margin
Consider for a “threatened” margin – very low or very large tumour
Definitely for an involved margin
Consider for a “threatened” margin – very low or very large tumour

Basingstoke Viewpoint
Simunovic et al. BJS 2003;90:999-1003

Basingstoke Colorectal
Problems with this paper Problems with this paper
Subjective Based on large experience with
focus on optimal surgery Not reproducible
Subjective Based on large experience with
focus on optimal surgery Not reproducible
Basingstoke Colorectal
New methods of stagingNew methods of staging
Imaging techniquesImaging
techniques

Basingstoke Colorectal
Purpose of Imaging in Colorectal CancerPurpose of Imaging in Colorectal Cancer
Staging
Stage dictates outcome but especially for rectal cancer today – Stage dictates management
Staging
Stage dictates outcome but especially for rectal cancer today – Stage dictates management

Basingstoke Colorectal

Basingstoke Colorectal
Management of Rectal Cancer Today
Management of Rectal Cancer Today
No treatment Palliative therapy Local excision/TEM Radiotherapy alone Neoadjuvant therapy +Surgery Surgery alone Chemotherapy +/- some or all
No treatment Palliative therapy Local excision/TEM Radiotherapy alone Neoadjuvant therapy +Surgery Surgery alone Chemotherapy +/- some or all

Basingstoke Colorectal
Staging Rectal CancerStaging Rectal Cancer
Local staging – local extension of the tumour and particularly the margin (CRM)
Staging for systemic disease
Local staging – local extension of the tumour and particularly the margin (CRM)
Staging for systemic disease

Basingstoke Colorectal
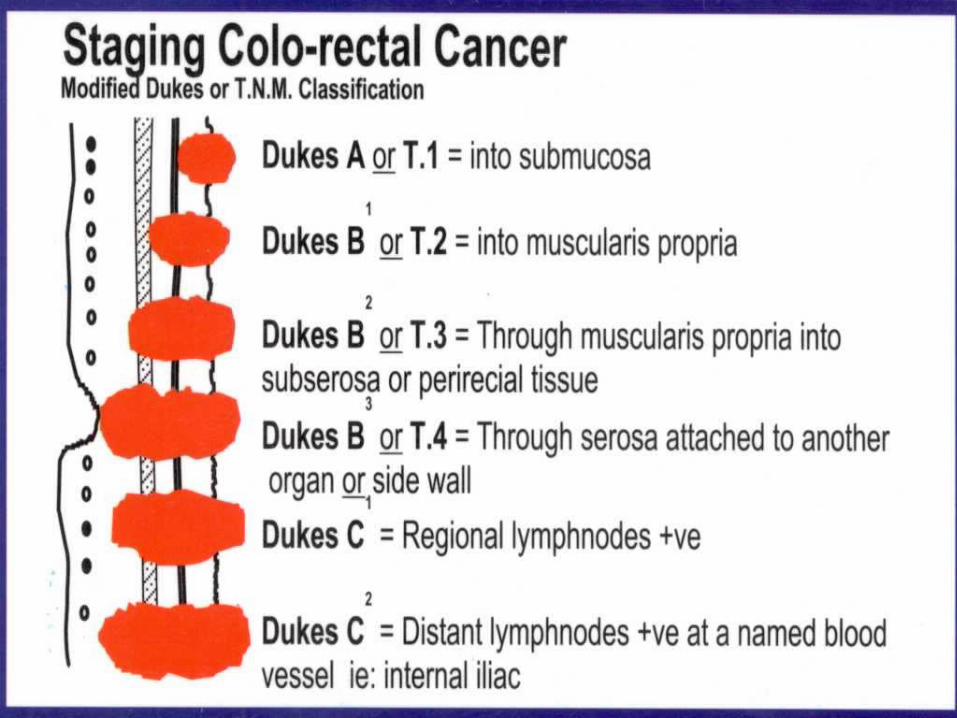
Staging Colorectal Cancer“Gold Standard”
Pathology
Staging Colorectal Cancer“Gold Standard”
Pathology
Dukes Staging
TNM
Dukes Staging
TNM

Basingstoke Colorectal
Pathology PathologyDukes Staging – Post –op pathology
TNM – Increasingly being “estimated” pre -op
Dukes Staging – Post –op pathology
TNM – Increasingly being “estimated” pre -op

Basingstoke Colorectal
Clarifying the TNM staging of rectal cancer in the context of modern imaging and neo-adjuvant
treatment: ‘y’‘u’ and ‘p’ need ‘mr’ and ‘ct’
B. Moran, G. Brown, D. Cunningham, I. Daniels, R. Heald, P. Quirke, D. Sebag-Montefiore
Colorectal Disease, OnlineEarly Articles Published article online: 10-May-2007doi: 10.1111/j.1463-1318.2007.01260.x
Basingstoke Colorectal
Staging – Moran et al Colorectal Disease 2008
Staging – Moran et al Colorectal Disease 2008
“TNM is pathology” “Imaging not equivalent”
“c” – clinical “u” – ultrasound “ct” – CT “mr” - MRI “p” – pathology “y” – after pre-op treatment
“TNM is pathology” “Imaging not equivalent”
“c” – clinical “u” – ultrasound “ct” – CT “mr” - MRI “p” – pathology “y” – after pre-op treatment
Basingstoke Colorectal
Staging – Moran et al Colorectal Disease 2008
Staging – Moran et al Colorectal Disease 2008
Thus a tumour staged by MRI as “T3N1 “should be described as
mrT3N1If given CRT eventual pathology
might beypT2N0
Thus a tumour staged by MRI as “T3N1 “should be described as
mrT3N1If given CRT eventual pathology
might beypT2N0
Basingstoke Colorectal
Local StagingLocal Staging
Depth of Tumour (“T” staging)
Mesorectal Margin
Depth of Tumour (“T” staging)
Mesorectal Margin

Basingstoke Colorectal
Imaging/ Staging Rectal Cancer Now
Imaging/ Staging Rectal Cancer Now
Finger X-ray Endoscopy US CT MRI PET
Finger X-ray Endoscopy US CT MRI PET
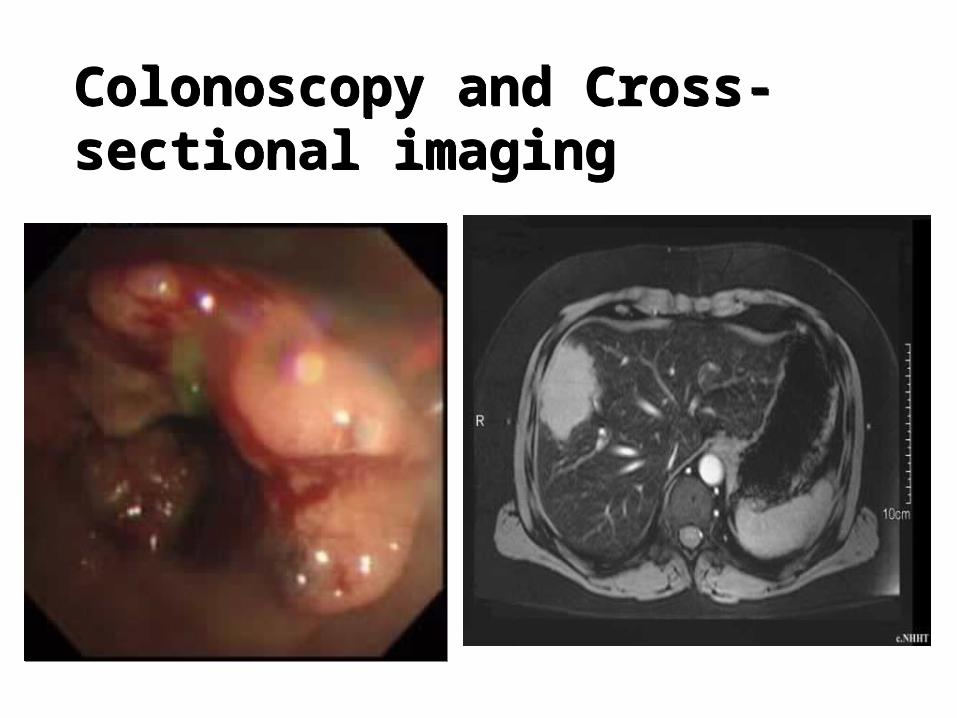
Colonoscopy and Cross-sectional imagingColonoscopy and Cross-sectional imaging

Stage Dictates TherapyStage Dictates Therapy

Basingstoke Colorectal
Local StagingLocal Staging
Finger- KeyEAUSMRI
Finger- KeyEAUSMRI

Basingstoke Colorectal
not for evaluation of mesorectal not for evaluation of mesorectal fasciafascia
EUS EUS
Superficial Rectal Superficial Rectal CancerCancerSuperficial Rectal Superficial Rectal CancerCancer

Basingstoke Colorectal
uT1uT1
intact outer hypoechoic layer (muscalaris propria)
intact outer hypoechoic layer (muscalaris propria)

Basingstoke Colorectal
uT3uN1uT3uN1

Basingstoke Colorectal
Limitations of EAUSLimitations of EAUS
Unable to view margins (CRM)
Stenotic tumours
Low painfull tumours
Unable to view margins (CRM)
Stenotic tumours
Low painfull tumours

Phased array coil/ no bowel prep




Basingstoke Colorectal
Accuracy of MRI Accuracy of MRI
Basingstoke Colorectal
The M.E.R.C.U.R.Y. Study
Magnetic REsonance Imaging andRectalCancerEURopean EquivalenceStudY

Basingstoke Colorectal
Aims of MERCURY

Basingstoke Colorectal
Diagnostic Accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer:prospective observational Study
MERCURY Study Group
Accuracy
1 Depth of extramural invasion – 95% to within 0.5mm
2 Prediction of a clear CRM (>1mm)- 91%
Diagnostic Accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer:prospective observational Study
MERCURY Study Group
Accuracy
1 Depth of extramural invasion – 95% to within 0.5mm
2 Prediction of a clear CRM (>1mm)- 91%
British MedicalJournal Volume 33 14th October 2006British MedicalJournal Volume 33 14th October 2006

Basingstoke Colorectal
Imaging Focal Point of MDT to plan treatment Imaging Focal Point of MDT to plan treatment

Tailored Treatment according to Risk for Local RecurrenceTailored Treatment according to Risk for Local Recurrence
The GoodSurgery
The BadSurgery + ? ( SC
RT) The Ugly
Long course CRT
Delayed surgery
The GoodSurgery
The BadSurgery + ? ( SC
RT) The Ugly
Long course CRT
Delayed surgery

The GoodThe Good
Extramural vascular invasion
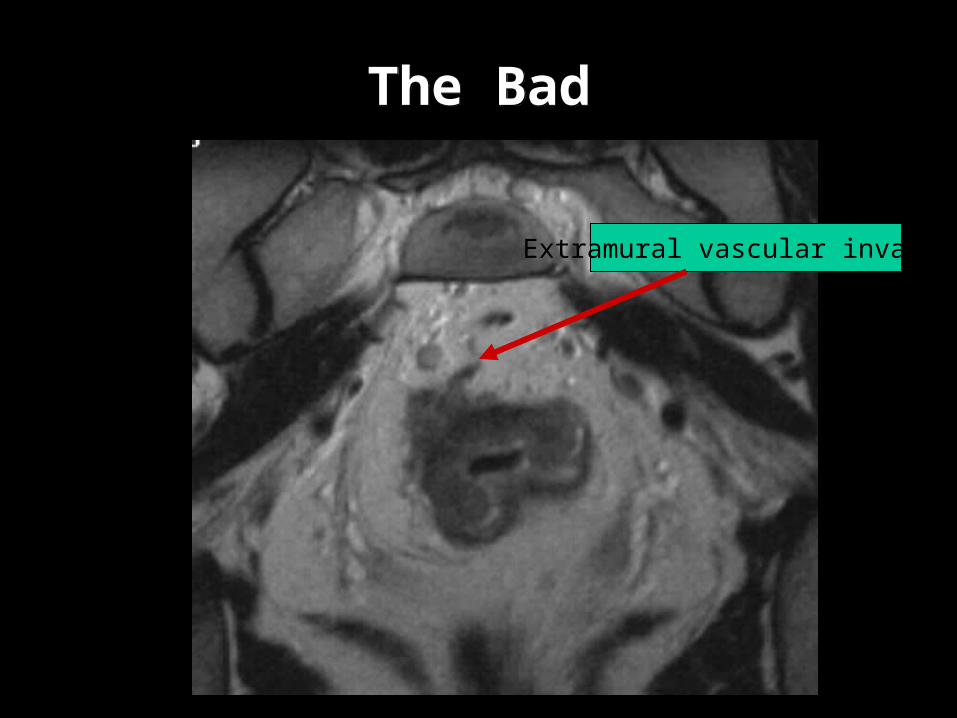
The BadThe Bad

Nodal disease and EMVINodal disease and EMVI
Tumour satellite close to CRMHeterogenous nodes

The Bad The Bad
Now 2 years old
mrT3N1 Cancer at 20 weeks

Feb 06 July 06
The UglyThe Ugly

Basingstoke Colorectal
Image and ImagingImage and Imaging
“ A picture is worth a thousand words”
Chinese Proverb
“ A picture is worth a thousand words”
Chinese Proverb

Basingstoke Colorectal
Rectal Cancer Today and 1982Rectal Cancer Today and 1982

Ongoing problems with staging/MRI
Ongoing problems with staging/MRI
MRI is not pathology
Low Rectal Cancer – staging poor- Finger better
MRI is not pathology
Low Rectal Cancer – staging poor- Finger better

Basingstoke Colorectal
Low tumours involving sphincter
Low tumours involving sphincter
Combination of PR and MRI to plan
Neoadjuvant therapy Subsequent surgery (AR or APE)
Combination of PR and MRI to plan
Neoadjuvant therapy Subsequent surgery (AR or APE)

Holm et al. (Karolinska Hospital, Stockholm)
BJS 94: 232-238, 2007
Holm et al. (Karolinska Hospital, Stockholm)
BJS 94: 232-238, 2007

Basingstoke Colorectal
Future –Optimal StagingTo Select for
Future –Optimal StagingTo Select for
TME Surgery alone
Selective neoadjuvant therapy
AR or APE
TME Surgery alone
Selective neoadjuvant therapy
AR or APE
Basingstoke Colorectal
Thank You
Thank You