bcsls hematology telehealth broadcast case 2 june 16, 2005 kin cheng [email protected]
TRANSCRIPT


CASE 2
• 60 yr old oriental male• One week prior to admission:
–headache, vomiting, dizziness• In Emergency:
–Uncooperative–Combative with staff–“Code White” was called

Lab Findings
• WBC: 9.0 G/L
• RBC: 2.3 T/L
• Hgb: 71 g/L
• MCV: 91 fL
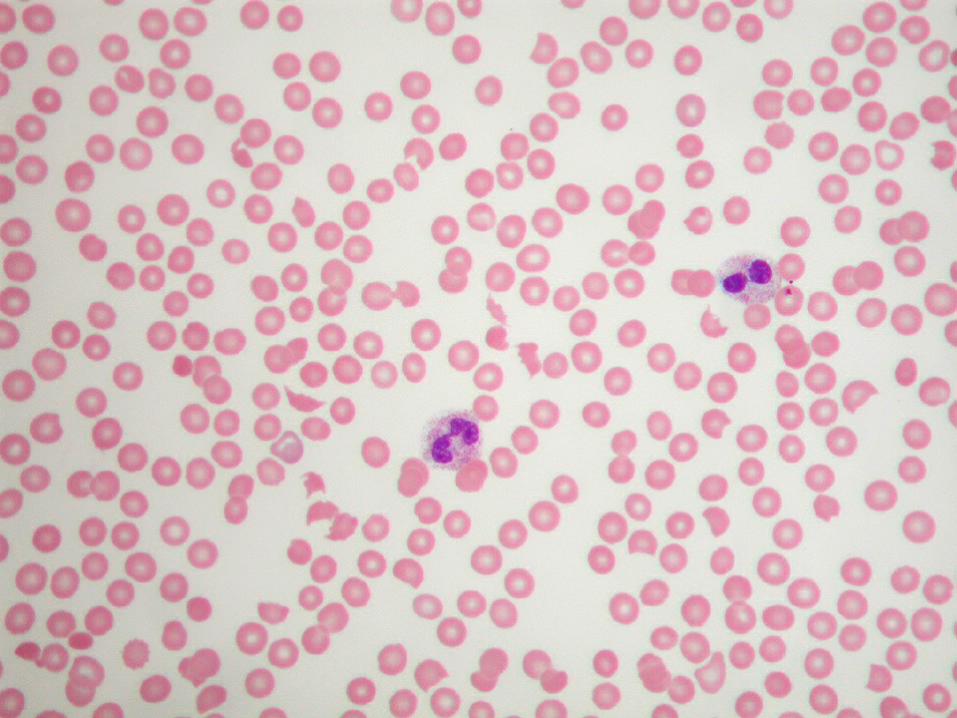
• Platelets: Less than 10 G/L with giant platelet forms
Lab Results
• INR: 1.0 aPTT: 30.0 sec
• Direct Coombs: Negative
• Total bilirubin: 46 mmol/L
• Haptoglobin: <0.1g/L
• Liver enzymes: Normal


Thrombotic Thromboctopenic Purpura (TTP)
• First described in 1926: in a 16 yr female:
–Petechiae, pallor
–Paralysis, coma
–Death– Microvascular hyaline thrombi in
terminal arterioles and capillaries

TTP HISTORY
• 1966: Pentad of TTP symptoms established
– Fever
– MAHA
– Thrombocytopenia
– Neurologic symptoms
– Renal dysfunction

TTP History
• 1982: Research on large vWf multimers
– 4 TTP patients with large multimers
– Ability to agglutinate platelets
• 1991: Plasma exchange: decreased mortality rate by 25%
• 1996: discovered vWf multimers cleaving protein
• 2004: Role of ADAMTS-13 protein

vWf
• Multimers
• Made in megakaryocytes and endothelial cells
• Stored in platelet alpha granules and Weibel-Palade bodies of endothelial cells
• Ultralarge molecule cleaved to smaller subunits by protease ADAMTS-13
• ULVWF : super adhersive to platelets

ADAMTS-13 and ULVWF
Weibel-Palade Body
ULVWF Multimers
ADAMTS-13
Endothelial Cell
Cleaved vWF Multimers

TTP and ULVWF
Weibel-Palade Body
ULVWF Multimers
ADAMTS-13
Endothelial Cell
Agglutinated platelets

Factors influencing platelet thrombi formation in TTP
• Absence or decreased level of ADAMTS-13 results in formation of ULVWF
• Level of ADAMTS-13: <5 % of normal
• Role of anchoring protein, P-selectin
• Increased fluid shear environment

ADAMTS-13
• “A Disintegrin-like And Metalloprotease with ThromboSpondin type 1 motif.”
• Normal adults: 50 – 178%
• <5% of activity found in acquired TTP patients
• Genetic: 9q34
• Antibody to ADAMTS-13

Clinical Picture of TTP
• Frequency: 3.7 per million
• Median age: 35 (neonate to 90 yrs)
• Microvascular thrombi: MAHA
• Pentad of symptom:– Fever, neurologic symptoms, renal failure,
thrombocytopenia, anemia with schistocytes
• Normal coagulation
• Increased LDH
Acute Idiopathic TTP
• Acquired
• Autoantibody to ADAMTS-13 found
• Clinical relapse not uncommon
• ULVWF multimers present

Differential Diagnosis of TTP
• Childhood HUS• Pregnancy-associated microangiopathy• Transplant-associated thrombocytopenia
pupura• Drug-induced purpura• HELLP• Malignancies• Autoimmune diseases, SLE, APLS

HUS vs TTP
• Patients: 4-5 years old
• Causative agent: E. coli 0157:H7
• Bloody diarrhea
• Shiga-toxin binds to glycolipid surface of endothelial cells, influenced by cytokines
• Toxin binding induces platelet clumping
• Acute renal failure
Pregnancy & TTP
• Risk in near term and post-partum
• Accounts for 10% of all TTP in one study
• Decreased ADAMTS-13 activity and increased plasma vWF in 2nd / 3rd trimesters
• Difficult to distinguish TTP / HELLP syndrome

TTP and drugs
• Quinine
• Penicillin
• Anti-platelet agents: ticlopidine, clopidogrel
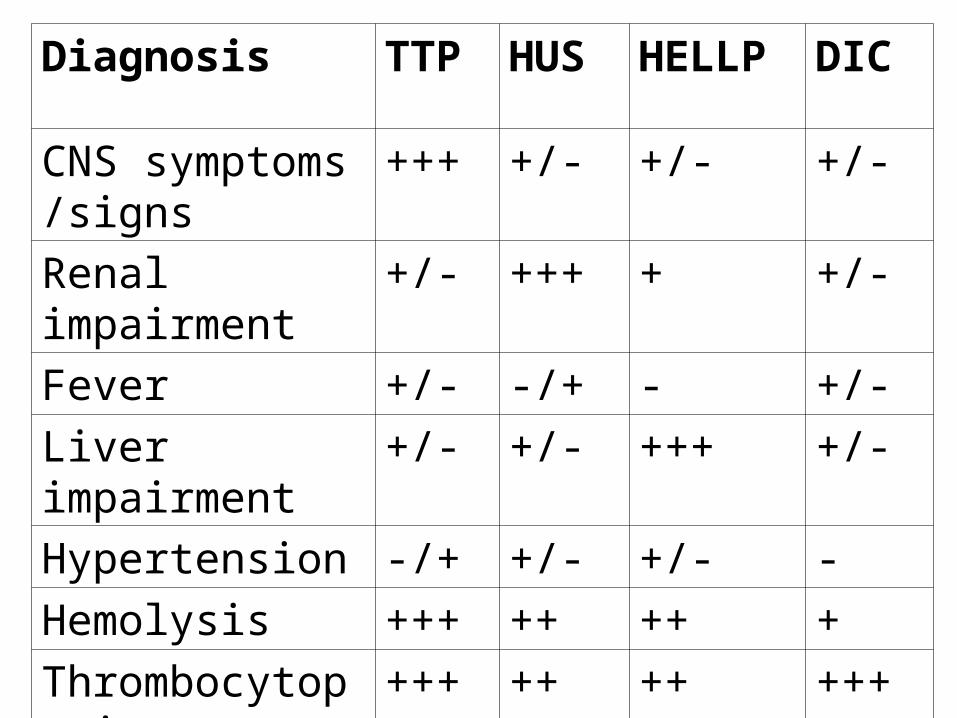
Diagnosis TTP HUS HELLP DIC
CNS symptoms /signs
+++ +/- +/- +/-
Renal impairment +/- +++ + +/-
Fever +/- -/+ - +/-
Liver impairment +/- +/- +++ +/-
Hypertension -/+ +/- +/- -
Hemolysis +++ ++ ++ +
Thrombocytopenia
+++ ++ ++ +++
Coagulopathy - - +/- +++

Treatment
Plasma exchange– Remove antibody– Restores ADAMTS-13– Improves mortality rate to 10 – 20%– Daily for 1-2 weeks
• Hemodialysis if kidney fails
• Plasma infusion if exchange not available
• Corticosteriod for non-responders

Remission
• Some patients have relapsed episodes
• Some good responders
• Reflects diversity of TTP

Summary
• Lab diagnosis of TTP:– Thrombocytopenia– Microangiopathic anemia:
• Schistocytes– Increased LDH: Due to tissue necrosis– Rule out other causes of MAHA
• Treatment: Urgent: plasma exchange