behavioral health issues related to all levels of...
TRANSCRIPT
S
The Rural Veterans Health Access
Program presents:
Dr. Amy Murphy Certified
Brain Injury Specialist
Behavioral Health Issues
related to all levels of TBI

S
DISCLOSURE
Purpose:
The purpose of the Traumatic Brain Injury – Medical Management of Behavioral Health Issues related to TBI webinar is to enable health care providers to better understand, identify, and treat traumatic brain injury-related behavioral health issues with new onset or existing conditions, and to develop medical management plans to improve care.
Criteria for Successful Completion:
Participants will attend the entire webinar and complete an evaluation form.
Upon completion, a CE certificate for 1.16 contact hours will be awarded.
Conflict of Interest:
There is no conflict of interest for any program planner or presenter involved with this activity.
NOTE:
This nursing CE activity is being jointly provided by the Alaska Nurses Association (AaNA), Alaska AHEC, and the State of Alaska Division of Public Health Rural Veterans Health Access Program.

Rural Veterans Health Access
Program
The Rural Veterans Health Access Program (RVHAP) is part of the Health Planning and Systems Development
Section, Division of Public Health,
Alaska Department of Health and Social Services
The RVHAP is funded by HRSA Office of Rural Health Policy: Grant number H3GRH26369

• The Rural Veterans Health Access Program (RVHAP)
deploys telehealth connectivity in selected remote SE rural
communities with no or limited health care services to
provide a Telehealth care network for behavioral health
and primary care.
• The Rural Veterans Health Access Program also provides
training to behavioral and medical health professionals on
the delivery of telehealth services using TH technology for
Behavioral Health and Primary Care related to Traumatic
Brain Injury

• Traumatic Brain Injury is one of RVHAP’s
priorities for the primary group served,
Veterans and their caregivers as well as
other rural community members with TBI
and their families and caregivers
• Provides Traumatic Brain Injury
Assessment and Treatment training to
RVHAP agencies and community health
providers including the VA and other
military health practitioners.

Tenakee SpringsOne of the remote rural Southeast Alaska communities served
by the Rural Veterans Health Access Program
http://dhss.alaska.gov/dph/HealthPlanning/Pages/veterans/default.aspx
For more information on the RVHAP or this webinar
contact the Program Director:
Susan Maley, MPH, Ph.D. [email protected], 907-
269-2084

S
Medical Management
of Behavioral Health Issues
related to all levels of TBI
Amy L. Murphy, DO
Brain Injury Medicine
Physical Medicine and Rehabilitation

S
Psychological Manifestations After Brain Injury:
Objectives
• Definitions
• Assessment
• Symptoms
• Treatment
• Discussion and Questions

S
DefinitionsNational Brain Injury Association
TBI is an insult to the brain, not of a congenital or
degenerative nature, that may produce a diminished or
altered state of consciousness which results in impairment
of cognitive abilities or physical functioning. It can also
result in the disturbance of cognitive abilities or physical
functioning. These impairments may be either temporary
or permanent and cause partial or total functional
disability or psychosocial impairment.

S
Definitions
Mild TBI
Traumatic head injury with ANY of the following:
LOC: < 30 min
GCS of 13-15
PTA: < 24 H

S
Definitions
Moderate TBI
Traumatic head injury with ANY of the following:
LOC: >30 min but <24H
GCS of 9-12
PTA: > 24 H but <1 week

S
Definitions
Severe TBI
Traumatic head injury with ANY of the following:
LOC: > 24 hours
GCS 8 or less
PTA: >1 week

S
NOTE!!!
Psychological Manifestations
• Can occur with all levels of TBI
• Some symptoms are more common with severe
injury but not golden rule
• Symptoms after TBI require more thought for
underlying process

S
Assessment• Symptoms commonly misunderstood and mismanaged
• Common scenarios post brain injury
• Complete new onset of symptoms
• Worsening of traits, now requiring treatment
• Well managed symptoms now no longer managed
• Complete shift/resolution of previous symptoms
• Treatment paradigms that are not congruent with TBI

S
Assessment• Complete history- especially risk factors, previous
behavioral health and brain injury
• Full exam- both neurologic and mental status
exam
• Overview of laboratory studies, prior radiologic
studies- especially brain
• Cognitive function
• Co-morbid physical/neurologic symptoms

S
Symptoms• Aggression: usually occurs after PTA as
patient is regaining awareness• Aggressive behavior greater concern than agitation
• More difficult to treat
• Long-term
• Safety for patient, family, staff
• Agitation: acute phase of recovery/PTA

S
Symptoms• Mood- looking at prominent symptoms
• Depressive symptoms
• Anxiety symptoms (panic attacks)
• Mania/Bipolar symptoms
• PTSD/stress response symptoms
• Hallucinations
• Unsafe behaviors/impulsivity
• Lack of insight

S
Symptoms• Personality Disorders
• Substance Abuse• Frequency
• Self medicating
• Psychosocial issues/stressors• Financial, home, family
• Legal issues/stressors• Charges pending
• Competency
S
Other Considerations• Metabolic
• Alcohol/drug withdrawal/toxicity
• Infection/systemic process
• Seizure disorder
• Endocrine dysfunction
• Cognition
• Headache
• Sleep

S
Treatment• Look for any medications/substance abuse that
worsen symptoms
• Look for physical issues that cover multiple
domains and treat first:• Sleep
• Seizures
• Migraines
• Delirium versus agitation
• Endocrine- especially testosterone

S
Treatment• Cognition first, unless mood is
overwhelming
• Then cognition second unless completely
assured
• Mood disorders after head injury respond
differently than primary mood disorders
• Hallucinations- think NOT typical psychosis

S
Treatment• Non-pharmacologic management should be used as much
as possible!
• Environment- adequate exposure to sunlight, reduced noise and distractions at night.
• Ensure that activating medications are reduced or given early
• Education staff and family
• Neurofeedback, EMDR, supportive counseling, neuropsychology
• If environmental and behavioral interventions are maximized and need for pharmacologic intervention is necessary, use medications that can cross cover multiple symptoms

S
Treatment
Seizures

S
Medication Chemistry Pharmaco
dynamics
Kinetics US/EU Side Effects
Levetiracetam Selectively prevents
hyper-
synchronization of
epileptiform burst
firing
Hydrolysis
primarily, urine
excretion
Half life 6-8 hours US- not approved
for mono-therapy,
adjunct for general
or partial seizures
Depression,
aggression,
somnolence,
asthenia, headache
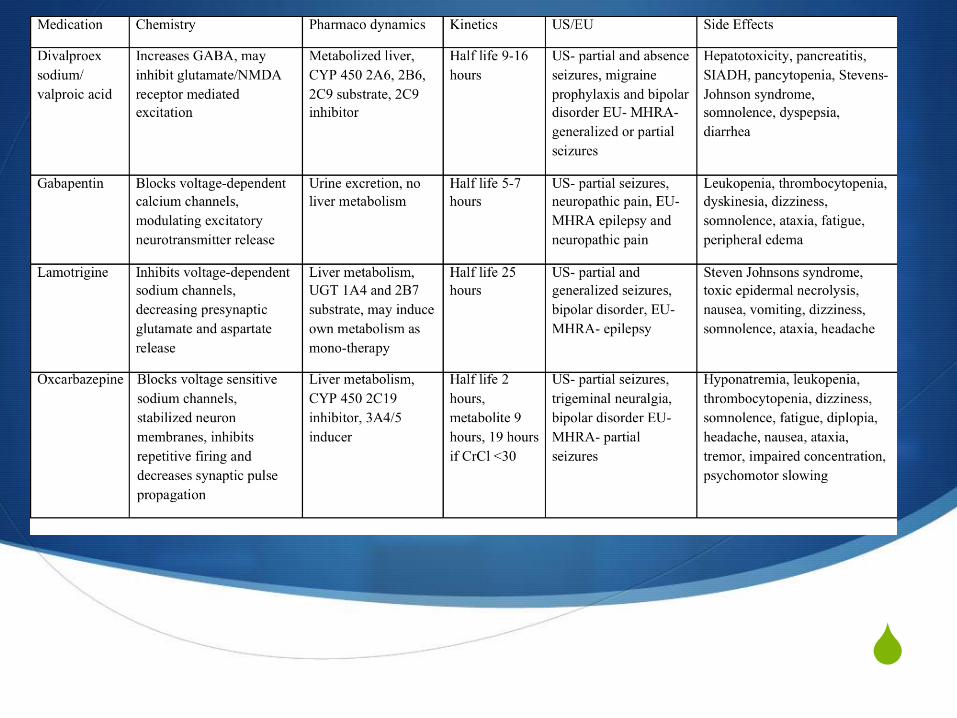
Divalproex
sodium/ valproic
acid
Increases GABA,
may inhibit
glutamate/NMDA
receptor mediated
excitation
Metabolized liver,
CYP 450 2A6, 2B6,
2C9 substrate, 2C9
inhibitor
Half life 9-16 hours US- partial and
absence seizures,
migraine
prophylaxis and
bipolar disorder
Hepatotoxicity,
pancreatitis,
SIADH,
pancytopenia,
Stevens-Johnson
syndrome,
somnolence,
dyspepsia, diarrhea,
weight gain, hair
loss, dizziness,
teratogenicity
Lamotrigine Inhibits voltage-
dependent sodium
channels,
decreasing
presynaptic
glutamate and
aspartate release
Liver metabolism,
UGT 1A4 and 2B7
substrate, may
induce own
metabolism as
mono-therapy
Half life 25 hours US- partial and
generalized
seizures, bipolar
disorder,
Steven Johnsons
syndrome, toxic
epidermal
necrolysis, nausea,
vomiting, dizziness,
somnolence, ataxia,
headache

S
Medication Chemistry Pharmaco
dynamics
Kinetics US Side Effects
Phenytoin Modulates neuronal
voltage-dependent
sodium and calcium
channels
Liver metabolism,
CYP 450 2C9
primary, 2C19
substrate, 2B6, 2C9,
2C19 and 3A4
inducer
Half life 22 hours US- status
epilepticus, seizure
disorder, seizure
prophylaxis
Cardiovascular risk
with rapid infusion,
ventricular
fibrillation, severe
hypotension,
hepatotoxicity,
nausea, vomiting,
rash, ataxia,
confusion
Carbamazepine Reduces post-
tetanic potentiation,
decreasing seizure
spread, exact
mechanism of
action in trigeminal
neuralgia and
bipolar disorder
unknown
Liver metabolism,
CYP 450 3A4
substrate, 1A2, 2B6,
2C9 and 3A4
inducer. Also
induces own
metabolism with
active metabolite,
urine excretion
Half life variable
due to
autoinduction
US- seizure
disorder, trigeminal
neuralgia, bipolar
disorder,
Fatal dermatologic
reactions including
toxic epidermal
necrolysis, Stevens
Johnsons with
increased risk for
HLA B1502 allele,
arrhythmias,
syncope, dizziness,
drowsiness, blurred
vision,
hyponatremia,
increase AST and
ALT

S
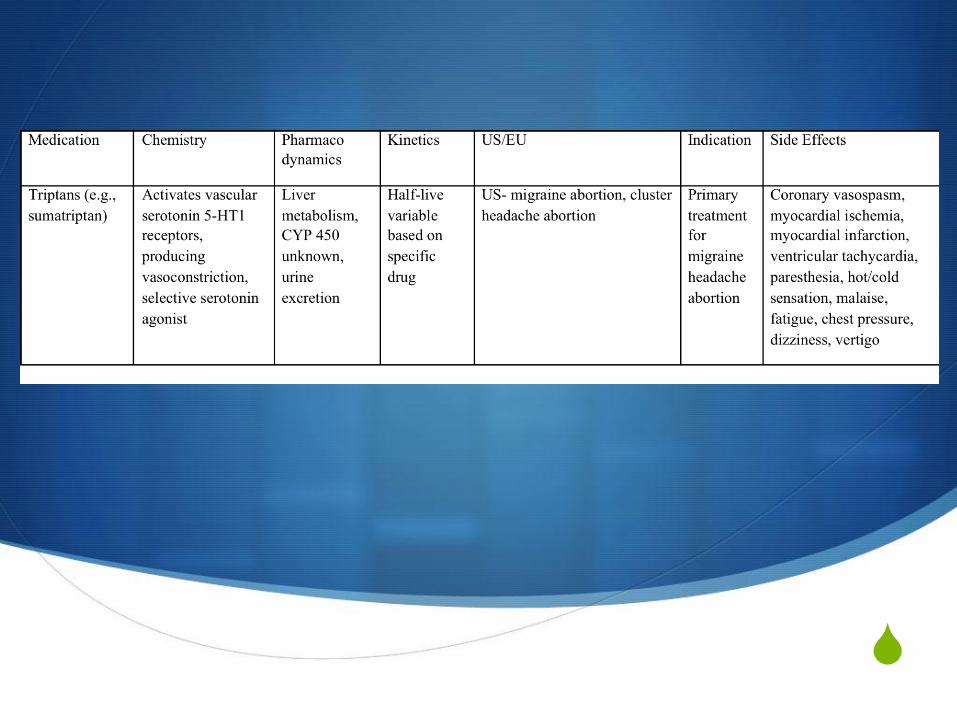
Treatment
Headaches

S

S

S
S

S
Treatment
Cognition

S

S
Treatment
Agitation/Aggression

S
Medication Chemistry Pharmaco
dynamics
Kinetics US/EU Side Effects
Haloperidol Dopamine
antagonist, D2
blocker
Metabolized liver,
CYP 450 2D6
primary, 3A4
substrate, 2D6
inhibitor
Half-life 21-24
hours
US- psychosis and
acute agitation,
Increased mortality
in elderly patients,
sedation,
extrapyramidal
side effects, tardive
dyskinesia,
neuroleptic
malignant
syndrome, QT
prolongation
Ziprasidone Dopamine D2
antagonist,
serotonin 5-HT2A
antagonist
Metabolized liver,
CYP 450 3A4
substrate
Half-life 7 hours US- schizophrenia,
bipolar disorder,
schizophrenia
associated
agitation
Same as
haloperidol plus
hyperglycemia and
serotonin
syndrome
Risperidone D2 antagonist, 5-
HT2 antagonist
Metabolized liver,
CYP 450 2D6
substrate
Half-life 20 hours
PO, 3-6 days IM
US- schizophrenia,
bipolar,dementia
associated
aggression
Same as
haloperidol plus
hyperglycemia,
priapism
Quetiapine Antagonizes D2
and 5-HT2
receptors
Metabolized liver
CYP 450 3A4
substrate
Half life 6-7 hours,
7-12 for ER
US- schizophrenia
and bipolar
disorder,
Same as
risperidone
S
Medication Chemistry Pharmaco
dynamics
Kinetics US Side Effects
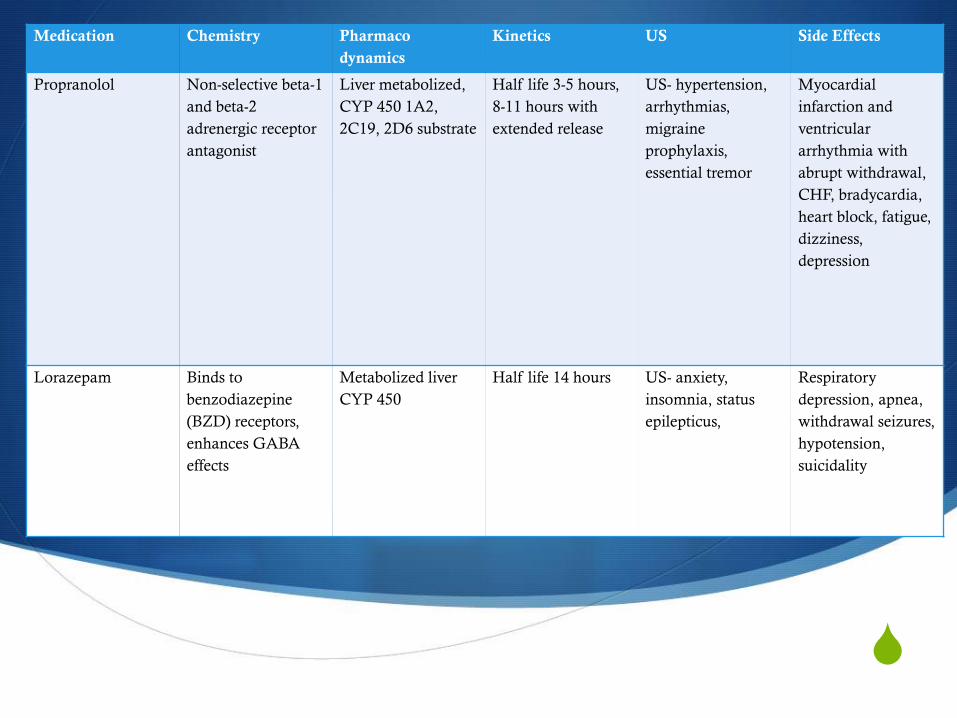
Propranolol Non-selective beta-1
and beta-2
adrenergic receptor
antagonist
Liver metabolized,
CYP 450 1A2,
2C19, 2D6 substrate
Half life 3-5 hours,
8-11 hours with
extended release
US- hypertension,
arrhythmias,
migraine
prophylaxis,
essential tremor
Myocardial
infarction and
ventricular
arrhythmia with
abrupt withdrawal,
CHF, bradycardia,
heart block, fatigue,
dizziness,
depression
Lorazepam Binds to
benzodiazepine
(BZD) receptors,
enhances GABA
effects
Metabolized liver
CYP 450
Half life 14 hours US- anxiety,
insomnia, status
epilepticus,
Respiratory
depression, apnea,
withdrawal seizures,
hypotension,
suicidality
S

S
Treatment
Mood

S

S

S
Medication Chemistry Pharmaco
dynamics
Kinetics US Side Effects
Lorazepam Binds to benzodiazepine (BZD)
receptors, enhances GABA effects
Metabolized
liver CYP 450
Half life 14
hours
US- anxiety,
insomnia, status
epilepticus,
Respiratory
depression,
apnea,
withdrawal
seizures,
hypotension,
suicidality
Tizanidine Binds to central
alpha-2
adrenergic
receptors,
increasing
presynaptic
motor neuron
inhibition,
centrally acting
muscle relaxant
Liver
metabolism,
CYP 450 1A2
substrate
Half life 2.5
hours
US- spasticity, Hepatotoxicity,
bradycardia,
hypotension,
syncope,
rebound
hypertension if
sudden
withdrawal,
xerostomia,
somnolence
Buspirone Unknown. High
affinity for
serotonin 5-
HT1A,
moderate
dopamine D2,
known to
modulate other
receptors, no
BZD
Liver
metabolism,
CYP 450 3A4
substrate
Half life 2-3
hours
US- generalized
anxiety disorder,
anxiety
disorders/sympt
oms
Dizziness,
insomnia,
lightheadedness,
nausea, tinnitus

S
Summary• Behavioral symptoms are common after all levels
of brain injury
• Understanding the root of the problem is key!
• Treatment goals
• Physical/underlying issues first
• Maximize therapies and environment
• Education for family/staff
• Maximize medications for covering multiple areas

S
S
References• Watanabe, T.K. et al. Systematic Review of Interventions for Post-traumatic Headache. PM R.
4, 129-140. (2012).
• Hou, L. et al. Risk Factors Associated with Sleep Disturbance following Traumatic Brain Injury: Clinical Findings and Questionnaire Based Study. PLoS One. 8(10), e76087. (2013)
• Giacino J, Whyte J, Bagiella E et al. Placebo-Controlled Trial of Amantadine for Severe Traumatic Brain Injury. N Eng J Med. 366(9), 819-826 (2012).
• Jha A, Weintraub A, Allshouse A et al. A Randomized Trial of Modafinil for the Treatment of Fatigue and Excessive Daytime Sleepiness in Individuals with Chronic Traumatic Brain Injury. J Head Trauma Rehabil. 23(1), 52-63 (2008).
• McNett M, Sarver W, Wilczewski P. The prevalence, treatment and outcomes of agitation among patients with brain injury admitted to acute care units. Brain Inj. 26(9), 1155-1162 (2012).
• Ferguson PL, Smith GM, Wannamaker BB et al. A population-based study of risk of epilepsy after hospitalization for traumatic brain injury. Epilepsia. 51(5), 891-898 (2010).
• Fountain N. Choosing Among Antiepileptic Drugs. Continuum Lifelong Learning Neurol. 16(3), 121-135 (2010).
• Tatum W. Antiepileptic Drugs: Adverse Effects and Drug Interactions. Continuum Lifelong Learning Neurol. 16(3), 136-158 (2010).

S
References• Perna R. Brain Injury: Benzodiazepines, Antipsychotics, and Functional Recovery. J
Head Trauma Rehabil. 21(1), 82-84 (2006).• Mysiw WJ, Bogner J, Corrigan J et al. The impact of acute care medications on
rehabilitation outcome after traumatic brain injury. Brain Injury. 20(9), 905-911 (2006).
• Willmott C, Ponsford J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: a randomised, crossover, double blind, placebo controlled inpatient trial. J Neurol Neurosurg Psychiatry. 80, 552-557 (2009).
• Erickson JC, Neely ET, Theeler BJ. Posttraumatic Headache. Continuum Lifelong Learning Neurol. 16(6), 55-78 (2010).
• Rizzoli P. Acute and Preventive Treatment of Migraine. Continuum Lifelong Learning Neurol. 18(4), 764-782 (2012).
• Kaniecki R. Tension-type headache. Continuum Lifelong Learning Neurol. 18(4), 823-834 (2012).
• Wagner A, McCullough E, Niyonkuru C et al. Acute Serum Hormone Levels: Characterization and Prognosis after Severe Traumatic Brain Injury. J Neurotrauma. 28, 871-888 (2011).