“believe it or not…” high dose insulin rescue therapy in calcium channel blocker overdose...
TRANSCRIPT

“Believe it or Not…”High Dose Insulin Rescue Therapy in Calcium Channel Blocker Overdose
Stefan Da Silva
CCFP-EM
Emergency Medicine Grand Rounds 2007

Outline
• Case (part I)
• Epidemiology
• Signs and Symptoms of CCB
• Pharmacokinetics
• Pathophysiology
• Treatment (will not cover the usual tx)
• Evidence/Studies
• Case (part II)
• Conclusion

Believe it or Not
• “Cup of Joe”
– Up until 1913 US Navy sailors received daily ration of rum
– That year US Secretary Joseph (Joe) Daniels prohibited any alcohol on Navy ships leaving coffee as the “strongest” drink on board.
– Disgruntled sailors began to call a cup of coffee a “cup of Joe”

Case
• 55 yr old male pharmacist presented to PLC July 10th 2006.– Brought by EMS after ingesting 20 tabs of Verapamil
240mg SR in suicide attempt.
– On scene vitals: 60HR, 65/40
– ED vitals: 65HR, 70/40, 91% on 4L
– Labs: Creatinine of 206 (remainder unremarkable)
– ECG: sinus rhythm as reported by cardiologist• PR 0.12, QTc: 453.

Epidemiology
• American Association of Poison Control Centers: Toxic Exposure Surveillance System (TESS)
– 9585 reported CCB “exposures” in 2002
– Approx 50% treated in health care facilities
– Moderate toxicity reported in 1142 cases
– Major toxicity in 339 cases
– Death in 57 cases (68 deaths 2003)
– Associated with the highest number of fatalities among cardiovascular drugs.
Signs and Symptoms
• Cardio: hypoTN, brady, blocks, arrythmias
• Pulm: resp depression, apnea, pulm edema, ARDS,
• GI: N + V, ischemic gut (rare)
• Neuro: lethargy, confusion, slurred speech, coma
• Metabolic: acidosis, hypergylcemia, hyperkalemia
• Derm: flushing, sweating, peripheral cyanosis.
Pathophysiology
– Act on L-type calcium channels
– “Block” calcium channels in myocardial cells, vascular smooth mm, and beta-islet cells of pancreas (Watson et al. Am J Emerg Med. 2003).

Pathophysiology
• Blockage of L-type channels in cardiac mm negative inotropy (contractility)
• Blockage of L-type channels in pacemaker cells negative chronotropy/dromotropy (heart rate and conduction)
• Blockage of L-type channels in vascular smooth muscle vasodilatation, decreased afterload.

Pathophysiology
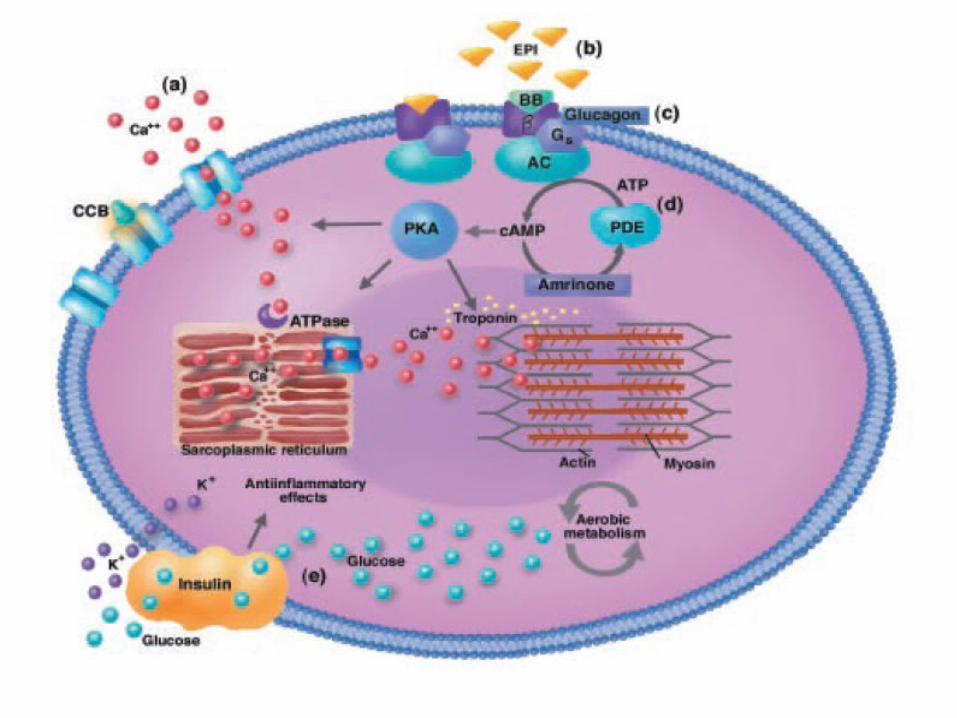
• BUT also blocks L-type channels in pancreatic beta-islet cells
– Impairs insulin release and induces a insulin resistant state which causes serum glucose levels to rise while intracellular levels fall..….


Pathophysiology
• Causes toxicity in myocardium in two ways
– 1) Impairment of conduction and contraction by blocking calcium entry through voltage-sensitive channels
– 2) Induces insulin resistance causing serum glucose levels to rise while intracellular stores fall causing cell to switch to fatty acid metabolism to make energy (Kline et al. J Cardio Pharm. 1996).
Pathophysiology
• In shock myocardial cells switch to glucose utilization as main energy substrate because more efficient.
• IF hypoinsulinemic, uptake of glucose is limited stores are used up quickly because of shock state.
• Therefore the cells have to switch back to inefficient metabolism of fatty acids further compromises cardiovascular condition.
• Lheureux et al. Critical Care. 2006.

Pathophysiology
• CCB overdose Blockage of L-type channels Decreased HR, Decreased BP “shock” state vascular smooth mm unable to “clamp” down due to blockade myocardial cells unable to increase rate because of blockade PLUS no energy substrate secondary to hypoinsulinemia Continued shock state!!

Pathophysiology
• In addition
– Lactic acidosis occurs due to hypoperfusion as well as a ketoacidotic state similar to DKA secondary to decrease in insulin production
• (Yuan et al. J Toxicol: Clin Toxicol. 1999)

Pathophysiology
• So….CCB toxicity causes problems in 2 ways
– 1) Blocks the channels in myocardial and vascular smooth mm cells
– 2) Causes hypoinsulinemia which in turn contributes to toxicity by decreasing amount of intracellular glucose for myocardial cells resulting in metabolic shift to using inefficient fatty acid.
Believe it or Not
• Burning Bright– Light bulb that was made in 1901 still burns bright
today at fire station in Livermore California.
– Proved by newspaper records and GE serial numbering.
– Standing order for any fireman who breaks the light to be transferred to another station.
– www.centennialbulb.org

Pharmacokinetics
• SR/XR tabs have prolonged toxicity due to slower absorption
– Can have delay of symptoms up to 15 hours. (Honcharik et al. J Toxicol Clin Toxicol. 1991)
• Hepatic clearance may expect decreased metabolism in hepatic dysfunction or shock states.
• Also, there may be increased drug half-life in overdose secondary to saturation of hepatic enzymes. (Buckley et al. Br J Clin Pharmacol. 1995).

Treatment
• How do we then treat this???– Supportive management (fluids, pressors,
etc)
– Conventional Treatments try to increase transmembrane calcium flow by either
• 1) increasing extracellular calcium
• 2) increasing intracellular cAMP concentration– Use of glucagon/adrenaline/milrinone

Treatment
• Thus far
– Calcium variable results
– Glucagon animal models show no improvement in survival
– Catecholamines increase BP and HR but at the expense of myocardial oxygen demand which may compromise function.

Treatment
• Hyperinsulinemia/euglycemia therapy (HIET)
• High Dose Insulin with supplemental dextrose and potassium therapy (HDIDK)
Treatment
• Rationale
– Pathophysiology mechanisms give rise to theories of use of insulin
– By overcoming hypoinsulinemia and insulin resistance through giving large amounts of insulin you could theoretically break the cycle of hemodynamic deterioration. (Lheureux et al. Critical Care. 2006)

Treatment
• Rationale con’t
– Also, it seems that insulin causes increased cellular uptake of glucose and lactate thereby decreasing acidosis and improving myocardial function and contractility. (Kline et al. Crit Care Med. 1995).
– Therefore, it appears to be helpful at a cellular metabolism level and as a result may take 30 – 45 minutes to see beneficial effect. (Lheureux et al. Crit Care Med. 2006)

Evidence
• Mainly animal studies and case reports.
• Most use anesthetized dogs that had toxicity induced with verapamil
– Most cases toxicity defined as complete AV dissociation and 50% reduction in MAP
• Case reports both pediatric and adult
– One reported death
Evidence
• 17 dogs
• 3 groups
– Saline tx, Glucagon, Insulin-glucose
– Insulin glucose group decrease glucose, decrease lactate, increase in SBP. (similar to glucagon group)
– Concluded that verapamil poisoning produced metabolic changes consistent with a diabetic human subjected to a physiologic stress
Evidence
• 24 dogs
• 4 groups: control, epi, glucagon, HIE
• Glucagon, Epi, and HIE therapy all produced similar hemodynamic responses
• However, survival rate was 100% with HIE group after 240 minutes of tx compared to 67% and 50% with epi and glucagon respectively.
• None of the glucagon group survived additional verapamil bolus of 3mg/kg and only 2 of epi group survived. All of insulin group survived.
• Concluded that HIE superior therapy to epi or glucagon based on survival.

Evidence
• 20 dogs
• 4 groups: saline, epi, glucagon, insulin+dex
• Showed increase in LV efficiency and fxn with subsequent increase in SBP with insulin treatment.
• Concluded that “treatment with insulin in verapamil shock state improves cardiac systolic and diastolic function as well as systemic hemodynamic parameters”
Believe it or Not
• Queen Victoria and childbirth– 1853
– Queen Victoria, after giving birth to seven children, became interested in the use of chloroform as an anesthetic agent as she was pregnant again
– Despite protests from advisors and medical establishment she insisted on using chloroform with her delivery which led to the practice of anesthetics during labor
– She knighted the physician administered it to her.
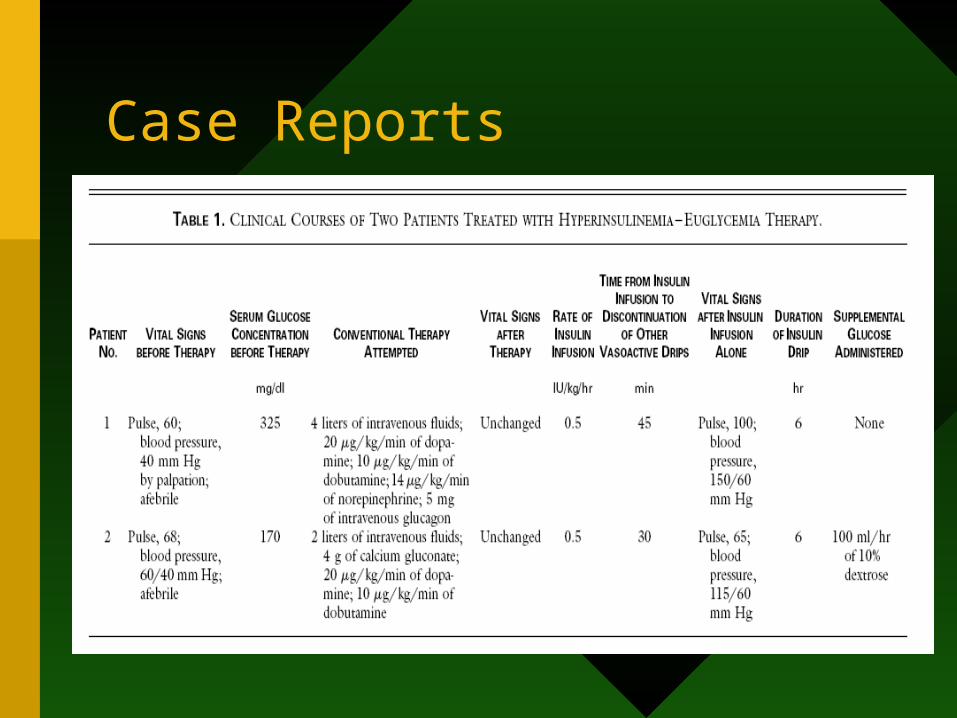
Case Reports
• Numerous case reports in literature
• None used as first-line therapy
• Only one documented death (though people may not report negative outcomes)
• Ages range from 5 months to 75 yrs.
• Variety of dosing and duration of therapy, however most consistent was 0.5 – 1.0U/kg bolus followed by infusion until hemodynamically stable (HR above 60 and SBP > 100).
• No reported adverse outcomes other than treatable hypoglycemia and hypokalemia

Case Reports
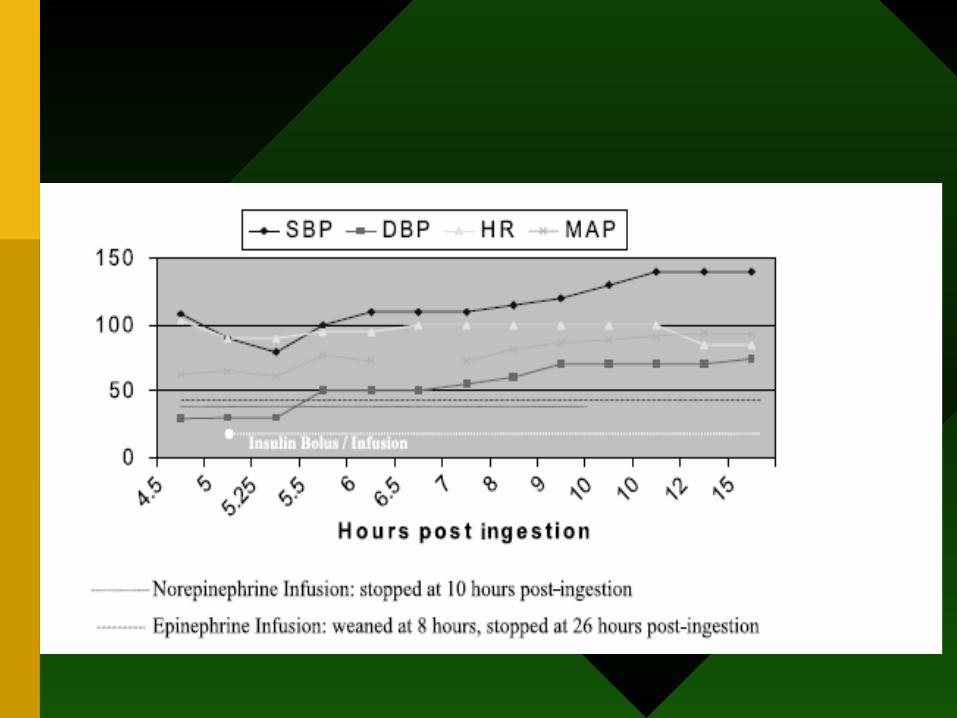
• 13 yr old female
• 25 – 30 Verapamil 120mg
• Remained hypotensive (SBP less than 100) despite dopamine, norepi
• Insulin/dextrose infusion started at 0.1 U/kg/hr plus dextrose at 0.5 g/kg/hr.
• Sustained SBP > 100 approx 45mins after infusion. Infusion stopped after 26 hrs.


Case Reports
• Journal of Toxicology. Clinical Toxicology 2001.
• 58 yr old male brought to ED hypotensive.
• Did not suspect Verapamil OD until an unspecified time later because of persistent hypotension despite vasopressor support.
• No time given re: when insulin/dextrose started nor dosing.
• Confirmed OD with verapamil blood level 48 hrs later (Verapamil 1740 ug/L and norverapamil 850 ug/L, target ranges for both are 100 – 200 ug/L).
• Pt eventually died despite all measures.

Case Reports
• Two cases
– 34 yr old female ingested 12 tabs of amlodipine SR 2.5mg each
– 48 yr old male unknown amount of Diltiazem SR
Case Reports

So now what???
• Evidence is based on animal studies and case reports.
• Pathophysiologically it seems to make sense and anecdotally seems to work.
• How and when do we use this?
Hyperinsulinemia/Euglycemia Therapy (HIET)
• Pediatric Emergency Care 2002.
• Proposed protocol for treatment
• Suggested to be used as “an adjunct to conventional therapy and should be used only after an inadequate response to fluid resuscitation, high dose calcium salts, and pressors.”
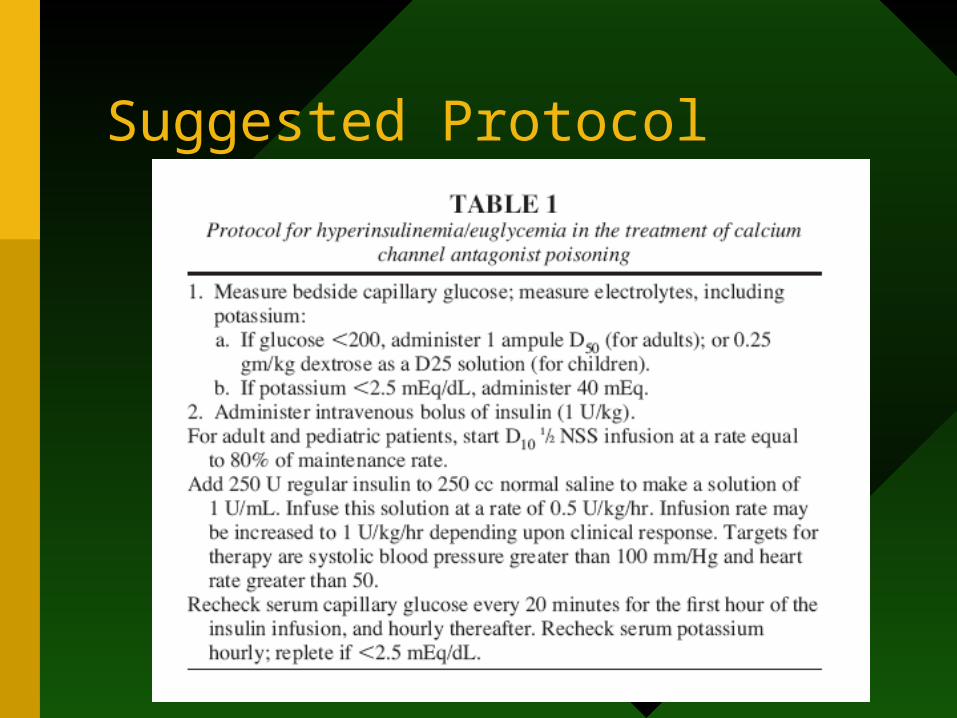
Suggested Protocol
Believe it or Not
• Just Do It
– 1989
– Nike commercial for hiking boots showed Sambucu Tribesman holding a pair of shoes and speaking in Maa, their native tongue. Subtitle read “Just do it.”
– Later, anthropology professor at Harvard revealed that actually Tribesman is saying “I don’t want these. Give me big shoes.”

Expert Advice
• 3 Questions asked via email
– When should HIET be started?
– Any new studies/research in this area?
– What starting dose?

Experts
• Dr. EW Boyer MD PhD– Associate Professor of Emergency Medicine, UMass Medical School
– Director of Toxicology, UMass Medical School
– Assistant in MedicineChildren's Hospital, Boston
– Lecturer in PediatricsHarvard Medical School
• Dr. J Kline BSc, MD, PhD – Associate Professor of Emergency Medicine, UNC-Chapel Hill
– Assistant Director of Research, UNC-Chapel Hill
– Adjunct Professor of Biology, UNC-Charlotte
– Credited with discovering the role of insulin in CCB overdose.

Dr. Boyer
• “it should be started ASAP. Personally, I don’t waste time giving calcium, and I never recommend it. I might start with dopamine or levophed (I do this in the more mildly intoxicated patients) and if that fails to have an immediate response, I start HIE, and I choose a load/drip rate based upon the serum glucose. For sicker patients, I give HIE first. I’ve treated maybe 20 patients this way—no deaths. The only documented failures that I am aware of in the literature occurred when HIE was administered late, or was done in suboptimal (e.g., less than 0.5-1.0 unit/kg bolus and drip) doses.”

Dr. Boyer
• “The reason to start it right away is that CCB poisoned patients can cook along looking better than their vital signs suggest---they’ll have good mental status, but with SBP in the 70s and a pulse in the 40s, and a FSBG of 150. They’ll have warm skin, good peripheral pulses and then they’ll die. I mean, I have had somebody die in mid-sentence. It happens with a rapidity that the uninitiated would simply not believe. Because it happens so fast, start HIE fast.”

Dr. Boyer
• “No, but we have a reference that is about to get accepted into Critical Care that outlines some diagnostic criteria.
Speaking as an attending talking to a resident now—many ER docs fear this treatment needlessly. I have had to give supplemental glucose in only about 30% of cases, and even then in concomitant beta blocker ingestion. CCB OD’s don’t need it that often, and the sick ones rarely if ever do.”

Dr. Kline
• “I believe if you suspect a severe poisoning, start AS EARLY AS POSSIBLE. Simply put, if you get the insulin receptor bound and working on the myocardium prior to severe dromotropy, you cannot then eat enough verapamil to die. But, after shock supervenes, insulin loses signal transduction to the myofilament for many reasons. Most people think my dose is obscene, but if the patient is hyperglycemic to start, I would recommend a minimum bolus of 0.5 U/Kg. The main issue is getting all insulin receptors bound and signaling. The infusion dose is less important, but >0.2 U/kg/h are required for inotropic effect in poisoned dogs.”

Case Part II
• Case was discussed with toxicologist on call
• Suggested Calcium Gluconate and if no change in hemodynamic status then Insulin 0.5 – 1.0 U/kg/hr and D50 drip
• Pt taken to ICU and placed on Calcium Gluconate drip for 24 hrs titrated from 2 gm/hr 1gm/hr 500mg/hr 250 mg/hr 125 mg/hr off
• BP 118/53 140/60
• HR: 60 75
• D/C’d to psych after 48 hrs in ICU.
So what should we do?
• Pathophysiologically it seems to make sense.
• Minimal adverse outcomes, which are easily treatable.
• Initiate HIET early because of time it takes to see effect (30 – 45min) due to having to change cell metabolism

• Discuss with toxicologist on call
• Would use the suggested Boyer protocol as it is the only one out there as of yet.

Believe it or Not
• “The Jock Strap”
– Initially used by bike riders in 1874 who were called “bicycle jockeys”.
– Used to protect themselves when they would slip and hit the crossbar when riding on the rough cobblestone streets.
– Hence the term “jock strap”
Believe it or Not
• “I’ve got a bone to pick”
– Comes from an ancient Sicilian wedding ritual where at dinner’s end the bride’s father would give the groom a bone and instruct him to pick it clean
– Signifying the groom’s authority over his new wife and that his word was final

Believe it or Not
• “It’s cold enough to freeze the balls of a brass monkey”
– Early warships piled their cannonballs in a stack next to the cannon on a brass sheet with indentations to secure the bottom layer of balls. It was nicknamed the “monkey”
– When it was too cold the brass would shrink causing the balls to fall off hence “it’s cold enough to freeze the balls of a brass monkey”.

Believe it or Not
• “7-Up”
– 1929 marketed by Charles L Grigg of St. Louis as the soda that “Takes the Ouch out of Grouch”.
– Became very popular during the Great Depression…..one of key ingredients was Lithium.
– “7” referred to seven oz bottle and “Up” to the carbonation of the soda.
Believe it or Not
• “Mind your P’s and Q’s”
– English pubs used to record patrons tabs on a blackboard behind the bar.
– Bartenders recorded consumption in pints and quarts, shorthanded to “p’s and q’s”
– Mind your P’s and Q’s originally meant to keep an eye on your tab.

Believe it or Not
• “Rx”– During Roman times healing arts and distribution of
medicine was the highest professional calling possible and could only be ordained by Jupiter
– The “R” is from the latin word “recipere” meaning to have prescribed while the small “x” was the god King Jupiter’s symbol of approval
– To the Romans it meant that the great god Jupiter himself had a hand in the medicine that was being prescribed