benefits and beyond c. 8 health care reform
DESCRIPTION
TRANSCRIPT
Benefits and Beyond C. 8
Improving access to health care.Thomas E. Murphy

Thomas E. Murphy 210/09/09
March 23, 2010 – Patient Protection and Affordable Care Act

Thomas E. Murphy 310/09/09
What led up to this?

Thomas E. Murphy 4
U.S. offers excellent health care. It is designed to cover all Americans. Most coverage is employment based and
98% of employers with over 200 employees provide health insurance.
But – the cost is too high. Result: cost sharing increased, some small
employers abandoning coverage, and too many uninsured. And, since health care is largely tied to employment . . .
What’s wrong?
10/09/09

Thomas E. Murphy 5
Fear that “you are a pink slip away from losing health care.”
Fear of dropped coverage when sick and exclusion of pre-existing condition.
And, Unemployment is 9.6%.
10/09/09
Thomas E. Murphy 6
Continuing coverage under COBRA has been expensive.
Stimulus Law – a temporary gov’t subsidy to buy COBRA. Ended May 31, 2010.
10/09/09
Coverage after layoff? (photo:
www.medicine.net)

Thomas E. Murphy 7
Problems? Issues? Alternatives? Health Policy? Health Care
Reform? Let’s look a little
deeper!
10/09/09
What does the data show

Thomas E. Murphy 8
1996
2004
2009
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
Uninsured
Employer Coverage is down!
10/09/09

Thomas E. Murphy 9
47% of firms with 3-9 employees
72% of firms with 10-24 employees
93% of firms with over 50 employees
98% of firms with over 200 employees
10/09/09
Employer sponsored overall coverage - 59% (+180,000,000)

Thomas E. Murphy 1010/09/09
What’s Wrong?

Thomas E. Murphy 11
Our health care system**There is some overlap – for example, 27 million buy individual health policies.
10/09/09

Thomas E. Murphy 1210/09/09
U.S. Residents-No health insurance (in millions – U.S. Census)
1993 38
2004 42
2006 47.5
2007 45.4
2008 46
2009 50
Thomas E. Murphy 13
“My friend ends her own business and gets a job with Starbucks” to get health care.
Annual H.C. cost in the U.S. depends on what? (where, who, deductible)
Employee total cost sharing is around +30%.
U.S. pays more for health care:16.2% of GDP vs. 12% average for other OECD countries.
High Costs Impede Access
10/09/09
Thomas E. Murphy 14
From 2000-2010, health care premiums have increased 130% and other out-of-pocket cost sharing features have increased 115%.
10/09/09
The increasing cost shift

Thomas E. Murphy 15
Current System is too expensive because of: Inappropriate care (35%).
Medical errors: 100,000 deaths per year. Third party payer – lack of market
dynamics. No value based competition
Poor health culture (high obesity and resulting chronic diseases), poor health
education, and lack of patient compliance. Tax treatment, and other reasons . . .
Why do we cost more?
10/09/09

Thomas E. Murphy 16
Our multi-layered administrative systems cost $35 billion annually more than other OECD countries.
Our prices and salaries of health care goods and services are much higher than European countries.
We have more and quicker access to technology –such as imaging, robotic surgery, R/x.
No government subsidies or price leverage except Medicare and Medicaid.
Why do we cost more?
10/09/09

Thomas E. Murphy 17
Why do we cost more?
How to control? Cutting is not the answer
Aging Population High expenditures in
last 3 months of life 3d party long term
care system Highest compensation
for providers. High R/X marketing
and R&D costs..
10/09/09

Thomas E. Murphy 18
Malpractice and defensive medicine
Third party payer system removes the consumer from “engagement” and making informed decisions.
(PHOTOS: WWW.MEDICINE.NET)
10/09/09
More cost drivers . . .

Thomas E. Murphy 19
U.S. life expectancy, infant mortality, access to health care is below OECD leaders.
U.S. ranks last in “patient safety” among 5 top OECD countries
Research says, however, this is not result of health care system but rather culture and education. Adult obesity is over 30% and the cause of a number of chronic diseases.
10/09/09
But are we better?

Thomas E. Murphy 2010/09/09
The David, growing up in America!

Thomas E. Murphy 21
U.S. is best place to be for serious health problems.
Survival rates per 100,000 for major and acute health problems is highest.
U.S. leads world in research, innovation, and new drug therapies. (70% of innovation comes from U.S.)
U.S. has shortest wait lists by a large margin for elective procedures, and in many cases for medically necessary treatments.
But. . . The reality is . . . .
10/09/09

Thomas E. Murphy 22
Cost is the chief reason nearly 50 million are uninsured.
And why employers and government are struggling to continue health insurance.
10/09/09
What is the Problem?

Thomas E. Murphy 23
High Cost makes access difficult!
How do we reduce costs?
Need more data . . .
Could we enhance access with lower costs?
Would a quality-driven market system reduce costs?
What are the other choices?
Let’s look at more data
10/09/09

Thomas E. Murphy 24
If cost is the problem how do we best deal with it?
Can we reduce our costs and still assure high quality and efficacy?
What if we conducted a “SURGE” against costs?
10/09/09
The solutions? What data do we
need to make a policy decision?
Thomas E. Murphy 2510/09/09
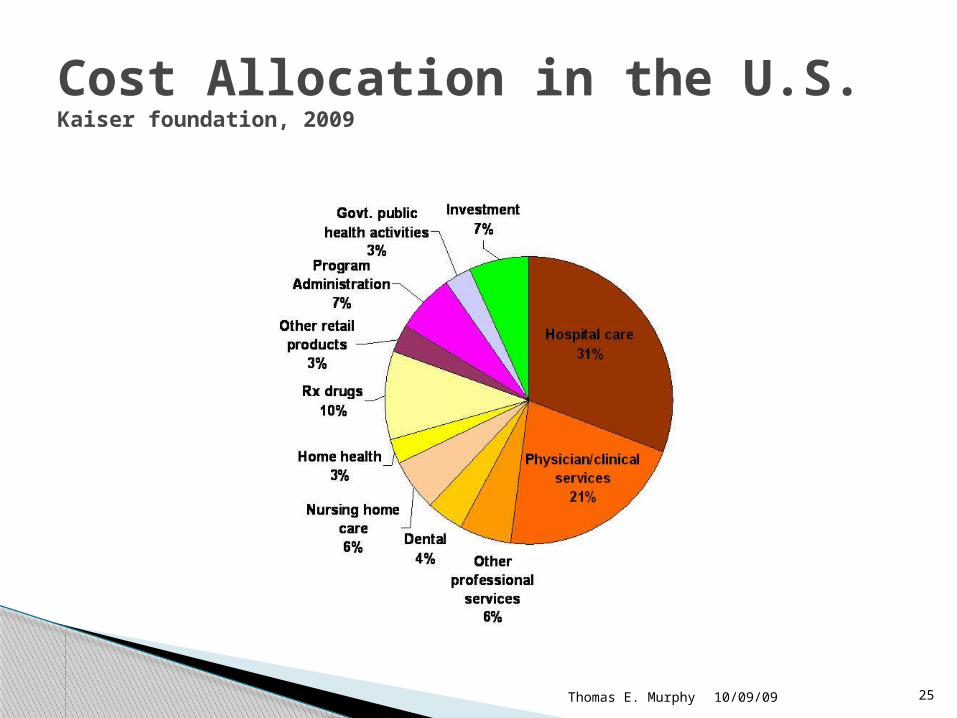
Cost Allocation in the U.S. Kaiser foundation, 2009

Thomas E. Murphy 26
Where/Type* Individual Family
Nation $2965 $6328
New York $13296
Iowa $5609
No deductible $12500
High deductible ($10,000)
$5380
*2009 Costs
10/09/09
Cost Averages* Depend On:*For state pricing see: www.healthcare.org

Thomas E. Murphy 27
The health care reform baton is being passed – 2010-2014!
Affordable Care Act of 2010 is “access reform” – it is not health care reform that in large part was driven by high numbers of uninsured and the high costs of our health care.
10/09/09
Thomas E. Murphy 28
Just less than 50% do not meet Medicaid standards, and cannot afford health care.
Some, 24.5%, however, qualify for Medicaid but choose not to enroll.
20% can afford private coverage but choose not to buy it.
Most work. 8% are business owners
Who are the 50 million uninsured?
10/09/09

Thomas E. Murphy 29
Most are uninsured for less than one year.
55% are between the ages of 18 and 35; many decide they are healthy and don’t need insurance.
7% have household incomes in excess of $75,000; 22% made over $50,000 in 2007.
Disproportionate number of black and Hispanic are uninsured.
10/09/09
Who are the Uninsured?

Thomas E. Murphy 3010/09/09
Problems – Insurance Underwriting

Thomas E. Murphy 31
Cost shifting Unreimbursed care Community rating Need old and
young, healthy and sick to pool risk.
Pre-existing condition. (HIPAA)
No guaranteed issue
Right to cancel Individual coverage
premiums based upon health status
Not much portability except for COBRA
Adverse selection State control over
insured plans
10/09/09
Health Insurance Underwriting

Thomas E. Murphy 32
When sick people are without insurance, they don’t need insurance, they need health care.
10/09/09
But remember . . . (Photo:
www.medicine.net)

Thomas E. Murphy 33
The most powerful instrument in our system that generates the utilization of health care resources and higher costs – is – the physician’s ordering pen.
10/09/09
And really remember . . .

Thomas E. Murphy 34
Insurance companies do not write prescriptions or order MRIs.
While they add costs to our system, high utilization and prices are major cost drivers in U.S.
10/09/09
And . . .

Thomas E. Murphy 3510/09/09
Range of Reform Solutions

Thomas E. Murphy 3610/09/09
A “Surge” against costs!

Thomas E. Murphy 37
Tax law change Creating quality and
value-based markets for health care (-25%)
New types of integrated care models
Improved pre-natal care education and access
Mitigate chronic disease risk factors
Electronic medical records – reduce errors
HSAs, Wellness, increase engagement
Tort Reform – reduce unnecessary care (-10-20%)
Interstate insurance competition -
Reduce administrative costs.
And more. . .
10/09/09
Surge on Costs – What might work?

Thomas E. Murphy 38
Convert Medicaid to Defined Contribution Plan.
Merge insurance markets – individual and small employer.
Pay for results not separate services
Capitation of fees (DRGs)
Change Supply Side Services
Encourage integrated care organizations.
Simplify claims processing
Assure access to Primary Care
10/09/09
Surge on Costs

Thomas E. Murphy 39
The 80/20 rule: Preventive Care
Put your resources here: Preventive and Chroniccare
10/09/09
Thomas E. Murphy 40
Change reimbursement system – reward success and pay for non-traditional services that enhance efficiency and effectiveness
Is the office visit the only way medicine can be dispensed?
Is capitation a reasonable approach vs. fee for service?
Encourage integrated health providers.
What’s this “Supply-Side” focus?
10/09/09

Thomas E. Murphy 41
What happens when providers compete on basis of quality and price? Look at what has happened to the outcomes and prices for Lasik surgery.
Wal-Mart - $4.00 for many drugs. See also, www.rx.com/
Walk in clinics in retail stores. Urgent care centers vs. hospital emergency
rooms.
Supply side emphasis?
10/09/09

Thomas E. Murphy 42
Employer paid health insurance is not taxed as ordinary income to the employee.
This is unfair to those who buy insurance on their own; the premiums are paid after tax.
If we tax employer paid premiums, employees will search for ways to find their own health plans. The plan will suit their needs and will be portable. No longer dependent upon employment.
Forgone tax revenue runs between $90-$130 billion.
What about tax change and reform?
10/09/09

Thomas E. Murphy 43
One approach is to limit the exemption from income to $5000 per year. Any higher value would be subject to income tax.
In addition, all out of pocket costs for health care would be deductible, thus encouraging purchase of more cost efficient plans.
This would not necessarily cause employers to drop sponsored care – there are competitive and productivity reasons to continue. And, employers can deduct expense.
Tax changes and health care
10/09/09

Thomas E. Murphy 44
Full deductibility of self-purchased high deductible health care plan and contributions to HSAs.
Could be offset by a refundable tax rebate? Should this be available to all or only those who purchase a plan (HDHCP) on their own?
Tax preference is based upon convenience and efficiency of employer sponsorship and lack of employee leverage and knowledge to make purchasing decisions themselves.
Tax changes and health care
10/09/09

Thomas E. Murphy 45
The view is that this change would engender fairness between those who currently participate in an employer sponsored plan and those who pay for their own insurance.
It also will provide a portable health care plan not dependent upon employment.
It should have the effect of making health care more affordable and decrease number of uninsured.
Tax changes and health care
10/09/09

Thomas E. Murphy 46
Principle of compensating differentials – more health care costs reduces other elements of compensation.
Good health care is never “free!” Someone is paying for it.
10/09/09
Tax changes – a few principles

Thomas E. Murphy 47
What do we do first?
Reduce costs? Increase access? Our health care
bridge is burdened with high costs; why would we put more people on the bridge?
10/09/09
How to prioritize – access or costs?

Thomas E. Murphy 48
Consequences of + Access?
Mandated or Public Mandated or Public
Public or mandated system must be financed- it is not free.
Underwriting savings not sufficient to finance.
Financed by taxes, fines, rationing, artificial reduction of reimbursements.
Must have a standard policy with limits on cost sharing and minimum requirements on coverage.
Providers must comply with medical protocols
Public or State option may swallow the private sector.
10/09/09

Thomas E. Murphy 49
Consequences?
Costs will increase! Increased Gov’t. Employment (HHS HQ)
Must rely on community ratings
Limited underwriting and premium differentiation.
Impact on quality and consumer satisfaction?
Will a dual system arise as it has in some EU contries?
Non-profit insurance system
10/09/09

Thomas E. Murphy 50
Free medical education?
Give subsidies to purchase – how much and for what?
Arbitrarily imposed price controls on medicine and insurance providers.
10/09/09
Consequences . . .

Thomas E. Murphy 5110/09/09
New quality based market?

Thomas E. Murphy 52
It’s a leap, but we can do this!
10/09/09

Thomas E. Murphy 53
A quality and value based competition model would be a sound basis for reforming health care in the U.S. It could be a dynamic choice to make health care affordable!
10/09/09
Murphy says:

Thomas E. Murphy 5410/09/09
A Measured Approach to Reform
04/08/2023Thomas E. Murphy 55
Allow competition to drive quality improvements and make service more affordable– as it has done in other industries.
Centerpiece: clinical outcomes data!
Data is the key!
Thomas E. Murphy 56
Reducing the costs of health care and making it more affordable through market changes are aimed at the core cause of the health care crisis in the U.S.
10/09/09
A Focused Approach

04/08/2023Thomas E. Murphy 57
Quality, value, and cost are not rewarded.
Competition should be structured so that it is quality and value based; this will lead to lower costs.
This would be REAL health care reform! (See: “My View” at this link)
See also the Mayo Clinic Health Policy Center’s Recommendations: ◦ Create Value◦ Coordinate Care◦ Reform payment
system◦ Health Insurance for
all.
More specifically. . .

04/08/2023Thomas E. Murphy 58
Competition drives improvements in quality and cost.
Rapid innovation is diffused through the industry.
Excellent competitors grow, weaker rivals exit the market.
Quality improves, prices fall, value increases, and the market accommodates more consumers
Traditional Competitive Model
04/08/2023Thomas E. Murphy 59
Health care must be a patient centered system
Currently, it serves others – TPAs, Providers, Sponsors, Patients, Unions, Government.
Competition in health care?

04/08/2023Thomas E. Murphy 60
Also, the scope of health care is too narrow: it focuses on a disease, illness, or injury.
It should focus on the full cycle of care for a medical condition.
There is very little integration of care relating to this condition.
The system is structured around medical specialties –who are like “free agents” – performing their function and billing accordingly.
Condition vs. Disease

Thomas E. Murphy 61
Would reward value
No government or sponsor imposed “solutions.”
Providers would arrive at solutions to successfully compete in this new market
10/09/09
A value-based market model:

Thomas E. Murphy 62
How many cardiac bypass surgeries?
What results? How many post
surgical infections? What were length
of stay and charges?
Complications Re-admissions
10/09/09
The centerpiece – outcomes data!

04/08/2023Thomas E. Murphy 63
Published patient outcomes per unit of cost at the medical condition level.
We currently pay for services rendered – appropriate or not and in some few cases for the provider’s adherence to certain medical protocols.
Outcomes should be but are not considered. We have the ability to review clinical
outcomes data NOW! – but we don’t
How should we measure?
Thomas E. Murphy 6410/09/09
Who is doing the best job – give them our business!
Thomas E. Murphy 65
We have no real quality records of providers.
We have no access to charges or prices.
A third party selects providers and pays them.
We don’t compare.
10/09/09
Health consumers-is this a market?
04/08/2023Thomas E. Murphy 67
Current vs. Future Model

04/08/2023Thomas E. Murphy 70
Utilization review adds administrative costs to the system without sufficient returns.
Capitation can lead to rationing to mitigate financial risk.
Malpractice litigation leads to “defensive” and inappropriate care.
The more procedures that are ordered the higher reimbursement level for the providers.
The only risk free instrument is the stethoscope – other procedures carry risk
Limit or unnecessarily add services
04/08/2023Thomas E. Murphy 71
It should occur at medical condition level – where we measure and evaluate the full cycle of care – diagnosing, prevention, monitoring, treatment, and ongoing management of the condition.
Value can be created by directing our employees and participants to those providers with the best clinical outcomes.
Competition is at wrong level

04/08/2023Thomas E. Murphy 72
Some physicians do a far better job than others.
The same for hospitals
Typically the best provide services at lower costs – “they get it right the first time!”
Health Care is not a commodity!

04/08/2023Thomas E. Murphy 74
Absolutely necessary for patients and sponsors – but not available.
Often can lead to important process improvements.
Is critical to create informed and engaged consumers and payers of health care.
See the Cincinnati and other experiences where payers used clinical outcomes data to direct their participants to the “best providers.” Costs went down!
The importance of outcomes datahttp://onlinelibrary.wiley.com/doi/10.1002/hrm.3930340407/abstract

04/08/2023Thomas E. Murphy 75
Should be assisting members in finding the best value care and improving their overall health. They do not.
The “annual enrollment” undermines an objective to look at long term health approaches.
Billing is incomprehensible and providers are encouraged to under treat.
Out of network restrictions lead to poor provider choices.
New incentives for TPAs

04/08/2023Thomas E. Murphy 76
Fee for service – creates outcome problems Capitation leads to implicit rationing. Supply driven demand leads to providers
“filling up” their capacity. No competition on results means there are
no incentives for “quality outcomes.” Create a quality outcomes-based market
and the Providers – not government or insurance companies – will find the best way to deliver health care
Incentives for providers

04/08/2023Thomas E. Murphy 77
Often believe health care is a commodity They deal with inflation by simply shifting
costs to employees. Encourage HSAs but ignore the importance
of informed consumers who must make a number of important choices without the requisite data.
Employers do not realize the financial VALUE of health care as a benefit. It is often, just a cost to bear.
Employer Perspectives

04/08/2023Thomas E. Murphy 78
Competition among providers based upon results and relating to a medical condition over a cycle of care should be the focus.
The competition should not be based upon compliance with protocols, but real results.
Results based competition will lead to provider learning and sharing of medical information.
Let’s Review Some Principles

04/08/2023Thomas E. Murphy 79
Value based competition should lower costs because the best providers will “get it right the first time.”
Results are the feedback for providers and the criteria for selection by the participants.
The pursuit of quality does not end. It is “continuous.”
SOME PRINCIPLES

04/08/2023Thomas E. Murphy 80
An endless pursuit of quality by providers incented by a new health reform system – will lead to:
Fewer medical errors and more “appropriate care.”
Disease management and real integrated care
A migration from diagnosis and treatment to addressing causes.
Cost reductions and improved affordability.
SOME PRINCIPLES

04/08/2023Thomas E. Murphy 81
Needed Data
04/08/2023Thomas E. Murphy 82
Some outcomes data shows that patients treated at certain cystic fibrosis centers have a 14 year additional life expectancy than those treated at “average centers.”
After New York city hospitals started collecting and disseminating severity adjusted mortality data for cardiac bypass surgery, deaths declined by 41%. In a 4 year period.
Data can be used to educate providers!
Outcomes vary by provider . . .

04/08/2023Thomas E. Murphy 83
It has been slow in coming.
Who should have access?
What should the data system measure?
How doe one acuity adjust?
How can change happen?
Where’s the data?Electronic Medical Records?

04/08/2023Thomas E. Murphy 84
What are barriers?
04/08/2023Thomas E. Murphy 85
TPAs focus on discounts versus patient value.
Medicare and other government systems have the wrong incentives and do not encourage patient value.
Governments so far have equated “process compliance” with “quality.”
Systems do not encourage integration of care.
Artificial and arbitrary suppression of provider fees will not create value
What are barriers?

04/08/2023Thomas E. Murphy 86
Mindsets against being held accountable for results.
Lack of management expertise in the medical provider industry.
Medical education does not focus on value driven health care.
Health care delivery is too local depriving access to best providers.
What are barriers?

04/08/2023Thomas E. Murphy 87
Physicians are often “free agents.”
Hospitals take on too many services.
The payers of health care have not insisted on accessing quality outcomes data and using it to develop their networks.
What are barriers?
04/08/2023Thomas E. Murphy 88
Providers are “pushing” back fees

04/08/2023Thomas E. Murphy 89
TPAs! Orchestrate the best care!
04/08/2023Thomas E. Murphy 90
Enable patients to make informed choices of providers. (Not restrict choice with networks)
Measure and reward providers based upon results. (Not micromanage provider activities.)
Maximize the value of care over the full cycle of a medical condition. (Not minimize costs.)
Minimize administrative tasks and costs. (Not overwhelm providers and patients with paperwork)
New Roles for TPAs

04/08/2023Thomas E. Murphy 91
Compete based upon their subscribers’ health results (not cost)
New focus:
New Roles for TPAs
Long term health-
Improved life expectancy
and quality of life

04/08/2023Thomas E. Murphy 92
United Health Group and United Resource Networks.
Cigna and Quality Networks Blue Cross and Blue Shield of Minnesota
(Disease Management) Blue Cross and Blue Shield of Mass.
(Rewards Provider Excellence: reward excellence, higher margins, gains sharing, reward accurate diagnosis)
Some examples

04/08/2023Thomas E. Murphy 93
And, very importantly . . .
To create and manage a single, comprehensive
medical record for its patients

04/08/2023Thomas E. Murphy 94
Active participation in managing personal health: healthy life style, embrace preventive care, comply with provider recommendations, make informed choices about providers and treatments.
Choose TPAs and plans based upon these values.
New Roles for Patients

04/08/2023Thomas E. Murphy 95
New Roles for Employers
New Perspective on Value Stop the mindless cost shifting
Evaluate TPAs based upon “value” not cost.
Insist on value based choices of providers
Support healthy life styles among employees
Establish long term relationship with TPAs and providers.
Hold internal benefit staff accountable for long term health and good financial returns on health care benefits
04/08/2023Thomas E. Murphy 96
First and foremost . . . No law required.
Public Policy . . . Priority:
Move to Value Based Competition!
04/08/2023Thomas E. Murphy 97
Enable More Access
Lead to real health reform
This will . . .
Enhance quality, reduce
costs, and make health care more affordable.

04/08/2023Thomas E. Murphy 98
Employer and individual mandates. Guarantee affordable health insurance for
all. Single payer, universal health care system Move to individual choice and ownership of
health insurance by making it more affordable, tax deductible or, if low income, subject to tax credits.
Then, If needed a New Delivery System?
04/08/2023Thomas E. Murphy 99
Everyone should have access to quality health care!

Thomas E. Murphy 100
Preserve what we already do well
Sustain our innovation and research.
Focus on quality, cost effectiveness, and value.
What about choice? Is this important?
We should retain employment as primary locus for health care delivery.
Portability – Yes! Should consumers
share in some of the costs of health care?
10/09/09
Values to maintain:

Thomas E. Murphy 101
People who paid nothing for health care used 30% of health care resources.
Cost sharing can enhance informed utilization and positively affect quality.
10/09/09
We need patient engagement. .
The market, by exposing clinical outcomes data will drive health care providers to improve quality and deliver value.
Failure to do so will leave them . . .

Thomas E. Murphy 102
10/09/09
Without any “customers”

Thomas E. Murphy 103
Should the sponsors tell providers how to practice medicine?
Or, should they say let me see how you are doing and we will give you our business?
10/09/09
A market that drives quality and value – See: Mayo Clinic proposal
Thomas E. Murphy 104
Without comprehensive legislation and without burdensome costs!
Can implement before January 2014!
The Market will drive providers, TPAs, and others to find the optimal utilization of health care resources!
This will lead to quality based and AFFORDABLE health care.
10/09/09
The Value Based Market
.

Thomas E. Murphy 105
10/09/09
The Path to a healthy America

04/08/2023Thomas E. Murphy 106
They are depending on us . . .