benin: the challenges
DESCRIPTION
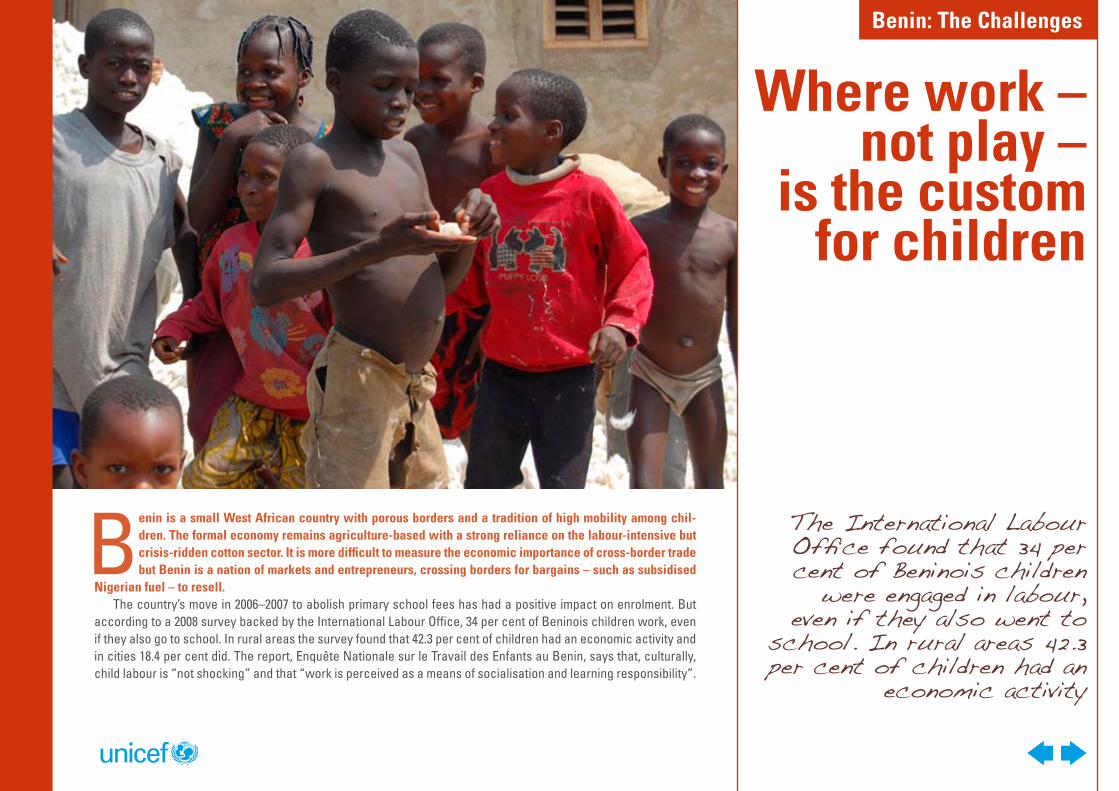
Benin is a small West African country with porous borders and a tradition of high mobility among children. The formal economy remains agriculture-based with a strong reliance on the labour-intensive but crisis-ridden cotton sector. It is more difficult to measure the economic importance of cross-border trade but Benin is a nation of markets and entrepreneurs, crossing borders for bargains – such as subsidisedNigerian fuel – to resell. The country’s move in 2006–2007 to abolish primary school fees has had a positive impact on enrolment. But according to a 2008 survey backed by the International Labour Office, 34 per cent of Beninois children work, even if they also go to school.TRANSCRIPT
The International Labour Office found that 34 per cent of Beninois children
were engaged in labour, even if they also went to
school. In rural areas 42.3 per cent of children had an
economic activity
Benin is a small West African country with porous borders and a tradition of high mobility among chil-dren. The formal economy remains agriculture-based with a strong reliance on the labour-intensive but crisis-ridden cotton sector. It is more difficult to measure the economic importance of cross-border trade but Benin is a nation of markets and entrepreneurs, crossing borders for bargains – such as subsidised
Nigerian fuel – to resell.The country’s move in 2006–2007 to abolish primary school fees has had a positive impact on enrolment. But
according to a 2008 survey backed by the International Labour Office, 34 per cent of Beninois children work, even if they also go to school. In rural areas the survey found that 42.3 per cent of children had an economic activity and in cities 18.4 per cent did. The report, Enquête Nationale sur le Travail des Enfants au Benin, says that, culturally, child labour is “not shocking” and that “work is perceived as a means of socialisation and learning responsibility”.
Where work – not play –
is the custom for children
Benin: The Challenges
In Benin, it has long been customary to send children to wealthier relatives so as to improve their prospects. UNICEF child protection expert Mary Chabi said the practice has become distorted over time and has resulted in high levels of child exploitation.
She said: “Over 600,000 children are involved in child labour with more than 67,000 of them being victims of child trafficking. Traffickers arose from a context in which it was culturally acceptable to send children away. They visit villages, asking for children and promising to take them to a better place, and they give small amounts of money to the parents.”
She said the government outlawed trafficking in 2006 and the Ministry of the Family, the police, child protection officers and special children’s magistrates are working hard to end the practice. “But in the community people are still not aware of the need to fight trafficking. If a man has about four wives and 30 children, how can he feed them? So trafficking becomes a way of supporting families.”
In the past two decades, from a very low start, Benin has made major strides to improve the health of its citizens. There have been no new cases of polio since 2009 and, in the following year, with UNICEF’s help, 97 per cent of targetted newborns received the DTP3 basic vaccination. In 2010, some 5,000 health extension workers were trained in a range of skills, including detection and prevention of malnutrition. UNICEF has supported the expansion of access to clean water but sanitation levels remain low.
As part of efforts towards the Millennium Development Goals, UNICEF programme targets up to 2013 include contributing towards reducing the under-five mortality rate to 70 per 1,000; reducing the maternal mortality ratio to 300 per 100,000 births; and pushing primary school completion rates from 64 per cent (in 2009) to 82 per cent.
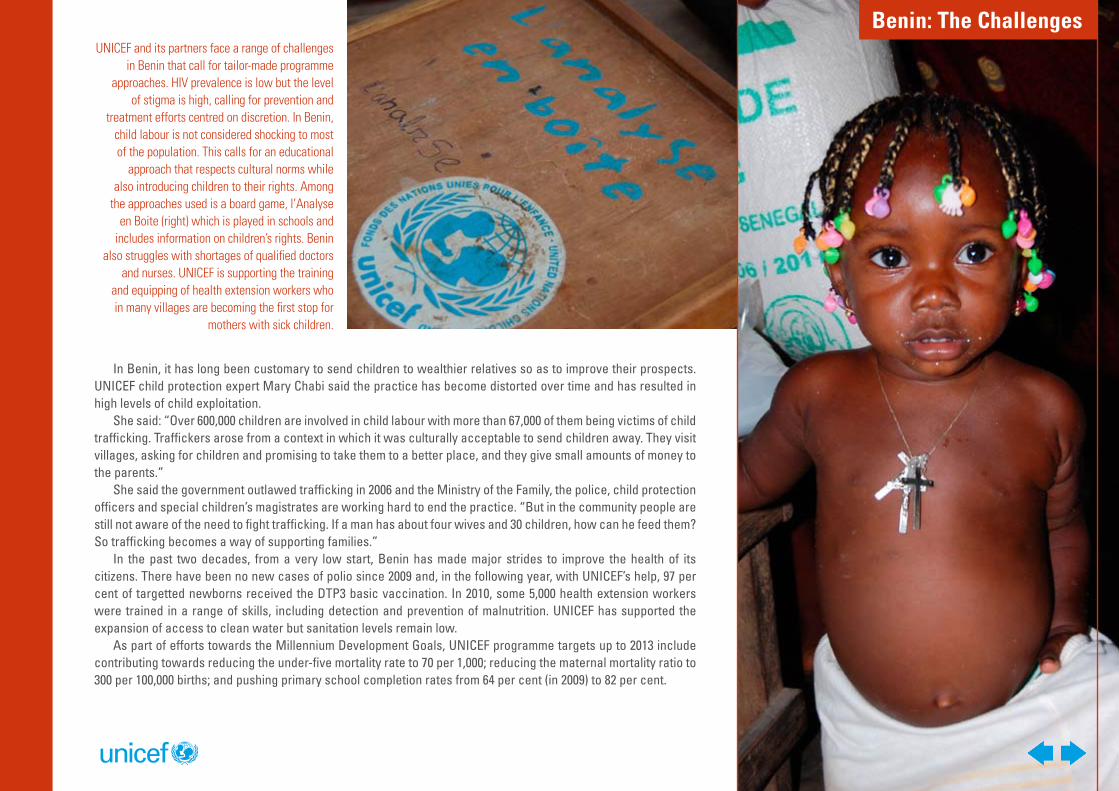
UNICEF and its partners face a range of challenges in Benin that call for tailor-made programme
approaches. HIV prevalence is low but the level of stigma is high, calling for prevention and
treatment efforts centred on discretion. In Benin, child labour is not considered shocking to most of the population. This calls for an educational
approach that respects cultural norms while also introducing children to their rights. Among
the approaches used is a board game, l’Analyse en Boite (right) which is played in schools and
includes information on children’s rights. Benin also struggles with shortages of qualified doctors
and nurses. UNICEF is supporting the training and equipping of health extension workers who in many villages are becoming the first stop for
mothers with sick children.
Benin: The Challenges
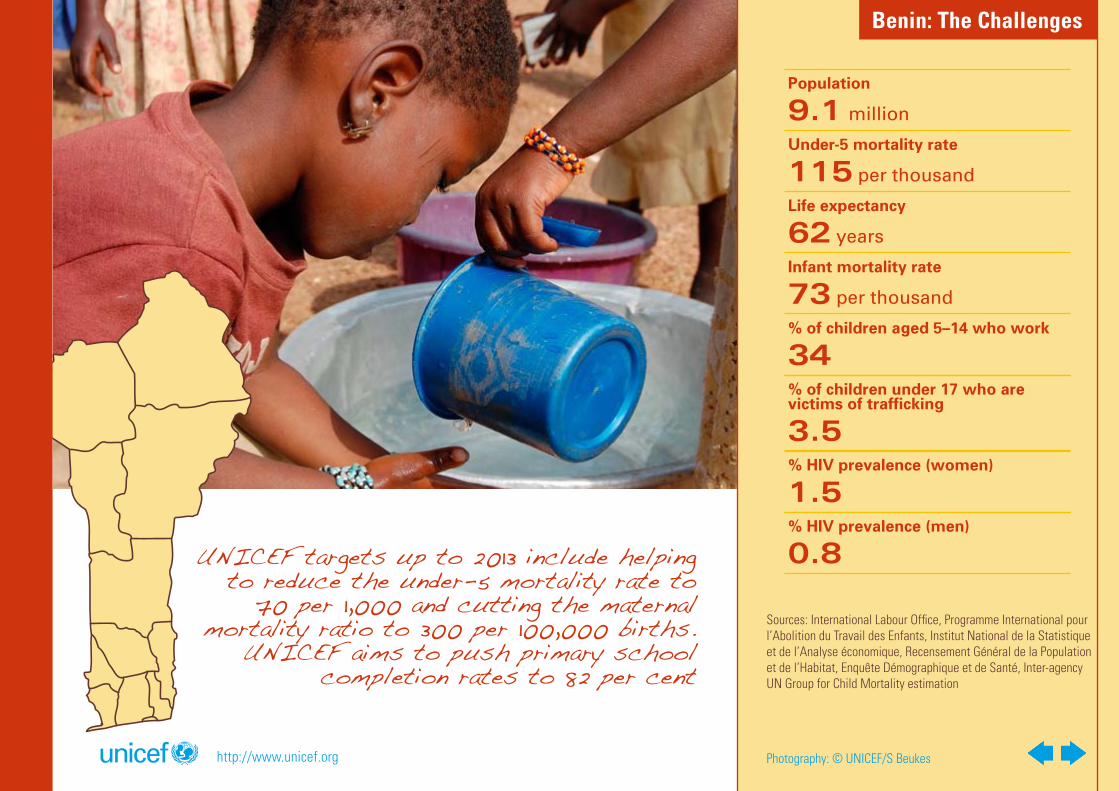
Population
9.1 million
Under-5 mortality rate
115 per thousand
Life expectancy
62 years
Infant mortality rate
73 per thousand
% of children aged 5–14 who work
34% of children under 17 who are victims of trafficking
3.5% HIV prevalence (women)
1.5% HIV prevalence (men)
0.8
Sources: International Labour Office, Programme International pour l’Abolition du Travail des Enfants, Institut National de la Statistique et de l’Analyse économique, Recensement Général de la Population et de l’Habitat, Enquête Démographique et de Santé, Inter-agency UN Group for Child Mortality estimation
Photography: © UNICEF/S Beukes
UNICEF targets up to 2013 include helping to reduce the under-5 mortality rate to
70 per 1,000 and cutting the maternal mortality ratio to 300 per 100,000 births.
UNICEF aims to push primary school completion rates to 82 per cent
http://www.unicef.org
Benin: The Challenges
Promotion of education and child
rights offers an escape from exploitation
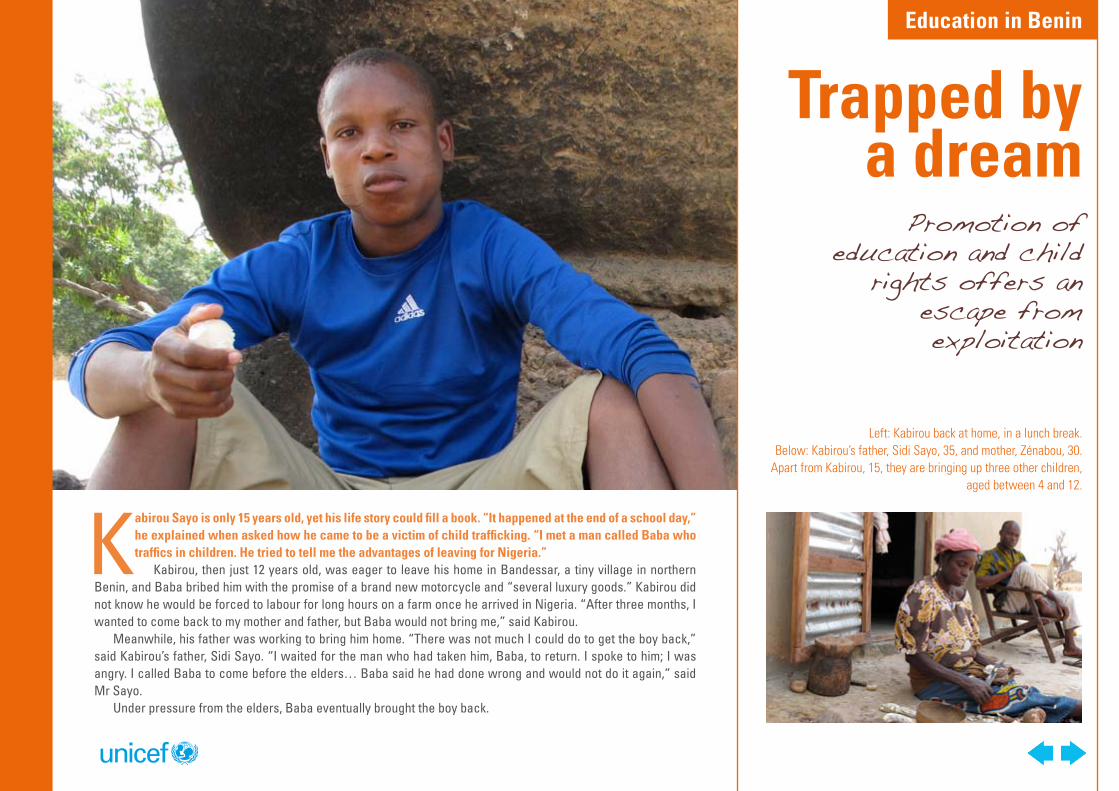
Kabirou Sayo is only 15 years old, yet his life story could fill a book. “It happened at the end of a school day,” he explained when asked how he came to be a victim of child trafficking. “I met a man called Baba who traffics in children. He tried to tell me the advantages of leaving for Nigeria.”
Kabirou, then just 12 years old, was eager to leave his home in Bandessar, a tiny village in northern Benin, and Baba bribed him with the promise of a brand new motorcycle and “several luxury goods.” Kabirou did not know he would be forced to labour for long hours on a farm once he arrived in Nigeria. “After three months, I wanted to come back to my mother and father, but Baba would not bring me,” said Kabirou.
Meanwhile, his father was working to bring him home. “There was not much I could do to get the boy back,” said Kabirou’s father, Sidi Sayo. “I waited for the man who had taken him, Baba, to return. I spoke to him; I was angry. I called Baba to come before the elders… Baba said he had done wrong and would not do it again,” said Mr Sayo.
Under pressure from the elders, Baba eventually brought the boy back.
Trapped by a dream
Left: Kabirou back at home, in a lunch break. Below: Kabirou’s father, Sidi Sayo, 35, and mother, Zénabou, 30.
Apart from Kabirou, 15, they are bringing up three other children, aged between 4 and 12.
Education in Benin
The “Analyse en Boite” game crosses Monopoly and Trivial Pursuit to challenge girls and boys to understand what they can expect of society and of their parents: to go to school, to live in a safe environment and to grow up happy and healthy. In
Djougou local authority alone, pupils in 21 primary schools play the game and competitions are organised between the top teams. The prizes are pens, copybooks and geometry sets.
“I spent two years over there,” Kabirou said.Back in Bandessar, Kabirou asked to go back to school. School is an important alternative to child labour, and
it offers children a long-term path out of poverty. Education is also a right belonging to all children, one guaranteed by the Convention on the Rights of the Child, the most endorsed human rights treaty in the world.
Djougou is one of 18 target communes where UNICEF is working to help the government increase the primary school enrolment and completion rates. But the challenges are manifold, says Abiba Orou-Tokpo, UNICEF Educa-tion Project Officer. “The cotton sector is in crisis and production has fallen. When families lack resources, they are forced to establish priorities, and education is not at the top of the list.”
The problems are not just economic, says Parfait Houssou, the head teacher at Bandessar’s primary school. “Many of our schools are short of buildings and equipment. We also suffer from a chronic lack of qualified teach-ers. The national teacher training college was closed down in 1986 and only recently re-opened. I am quite lucky to have five teachers for six classes. In many schools, children enrol and then sit there, without a teacher. The next year, they just don’t come back.”
UNICEF is working to improve education, approaching the challenges from a variety of angles, including estab-lishing partnerships with community and religious leaders; providing furniture and school supplies; and upgrading schools through the provision of latrines and safe drinking water. A special programme also aims to keep girls in school beyond primary school.
UNICEF is also distributing a board game teaching children about their rights. Based on the CRC, the ‘Analyse en boîte’ game uses elements of Monopoly and Trivial Pursuit to help children understand that they have a right to education, to protection from exploitation, and to grow up to be happy and healthy.
In Djougou, pupils in 21 primary schools play the game, and competitions are organized between the top teams. Prizes include pens, copybooks and geometry sets. While judging a play-off at Bandessar Primary School, Deputy Mayor Djibril Amadou commended the initiative. “The game teaches children their rights and prepares them for adult life. You also find that those children in Djougou’s schools who have come into contact with the game are better prepared for secondary school.”
Kabirou now attends secondary school, and is grateful for the education he receives. He says he wants to be the Education Minister of Benin when he grows up.
In the meantime, he would like to do some educating of his own. “I would like to tell Baba that if he wants to take people to Nigeria, he should choose grown up villagers, not children,” he said.
http://www.unicef.org Photography: © UNICEF/A Duval Smith
Education in Benin
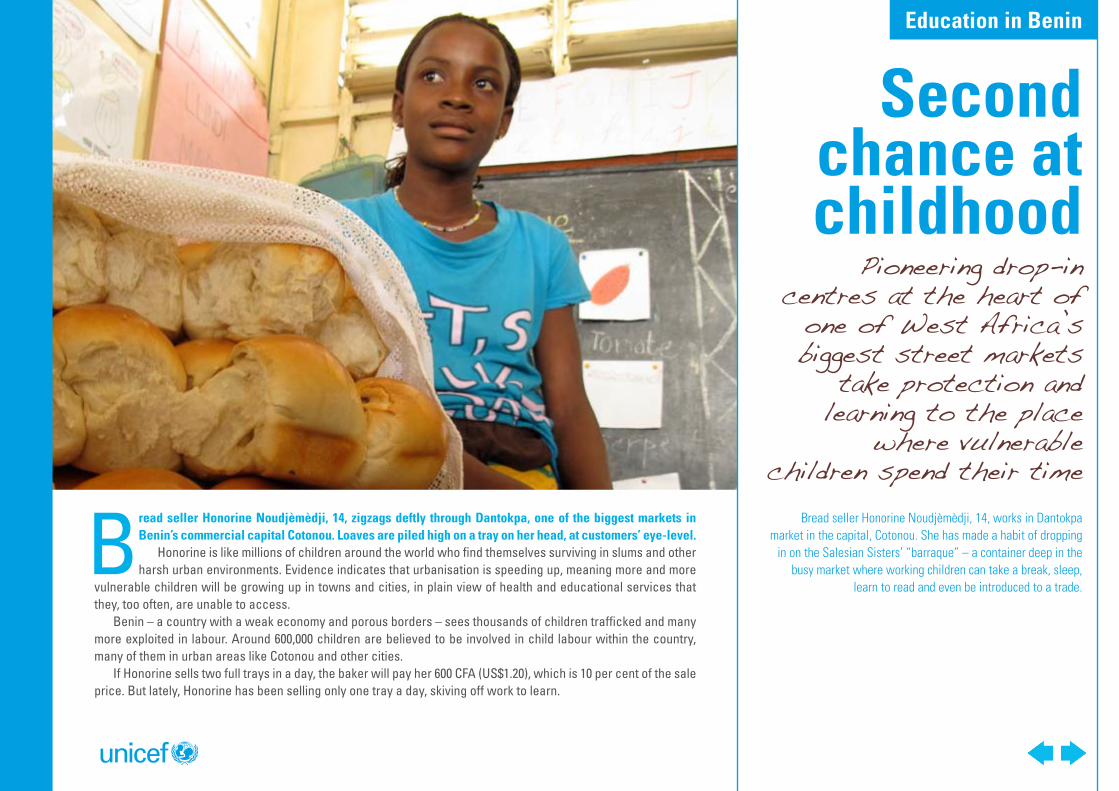
Bread seller Honorine Noudjèmèdji, 14, works in Dantokpa market in the capital, Cotonou. She has made a habit of dropping
in on the Salesian Sisters’ “barraque” – a container deep in the busy market where working children can take a break, sleep,
learn to read and even be introduced to a trade.
Pioneering drop-in centres at the heart of
one of West Africa’s biggest street markets
take protection and learning to the place
where vulnerable children spend their time
Bread seller Honorine Noudjèmèdji, 14, zigzags deftly through Dantokpa, one of the biggest markets in Benin’s commercial capital Cotonou. Loaves are piled high on a tray on her head, at customers’ eye-level.
Honorine is like millions of children around the world who find themselves surviving in slums and other harsh urban environments. Evidence indicates that urbanisation is speeding up, meaning more and more
vulnerable children will be growing up in towns and cities, in plain view of health and educational services that they, too often, are unable to access.
Benin – a country with a weak economy and porous borders – sees thousands of children trafficked and many more exploited in labour. Around 600,000 children are believed to be involved in child labour within the country, many of them in urban areas like Cotonou and other cities.
If Honorine sells two full trays in a day, the baker will pay her 600 CFA (US$1.20), which is 10 per cent of the sale price. But lately, Honorine has been selling only one tray a day, skiving off work to learn.
Second chance at childhood
Education in Benin
She goes to a “barraque” – a learning centre in a container – run by the Salesian Sisters. Honorine enters and rests her bread tray on a stool, then sits down to study near a blackboard covered in verbs. There, she is learning to read and write, and is picking up useful skills like sewing and beadwork.
“I have never been to school but I would like to,” she says. “I know of children who go to school. I don’t know what they do there, but it seems good – a bit like here. Here, I have learnt to read, to sew.”
The classes Honorine attends is one of three such drop-in havens in Benin supported by UNICEF. Children who work or live on the streets can simply wander in to learn, play or sleep. As UNICEF Child Protection Officer in Benin, Mary Chabi said it is “a second chance to return to childhood.”
Child labourers are often deprived of their rights – and many are not aware they have rights in the first place. The drop-in centre aims to change this.
“They do not know that they have a right to go to school, to food, to protection,” said Ms Chabi. “When they come to the centre, they begin to realise that they are missing a lot, that they have the right to plan their future, that they needn’t just be people who are exploited by other people in their lives.”
And parents must be educated about children’s rights as well.
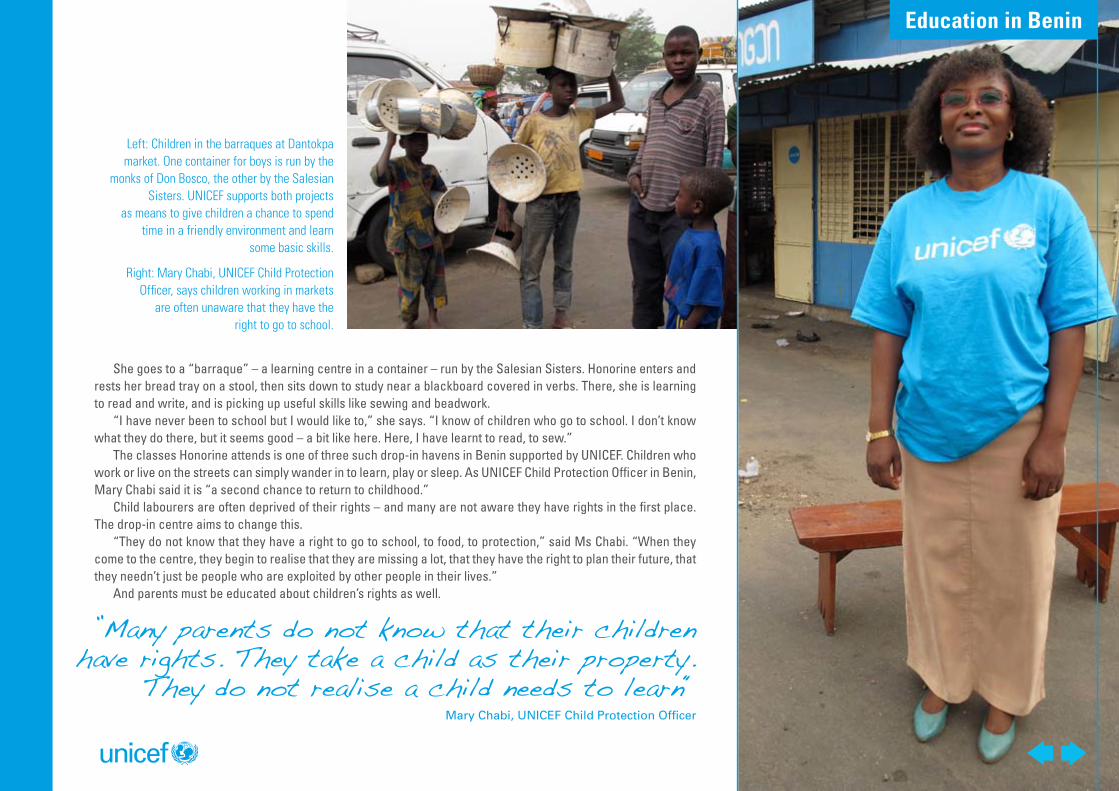
Left: Children in the barraques at Dantokpa market. One container for boys is run by the
monks of Don Bosco, the other by the Salesian Sisters. UNICEF supports both projects
as means to give children a chance to spend time in a friendly environment and learn
some basic skills.
Right: Mary Chabi, UNICEF Child Protection Officer, says children working in markets
are often unaware that they have the right to go to school.
”Many parents do not know that their children have rights. They take a child as their property.
They do not realise a child needs to learn“Mary Chabi, UNICEF Child Protection Officer
Education in Benin
“Many parents also do not know that their children have rights,” Ms Chabi continued. “They take a child as their property. They do not realise a child needs to learn.”
Outreach worker Claudine Bohissou has known Honorine for two years. “She first came with her older sister, then I did not see her for a while... Some time after that, she was accused of thieving at home and ran here to escape being beaten up by her brothers. Now she comes here most days. But she never stays long because she has to sell bread.”
Ms Bohissou has tried to convince Honorine to bring her mother to the centre. “Whenever we can, we speak to the parents, guardians or bosses, and try to convince them of the advantages of a little education or training... But there are disappointments, too. Recently, one girl who had been coming regularly just disappeared from sight. I learnt that she had been sent back to a village for marriage. She was only 12.”
As Ms Bohissou prepares for a beadwork class, an angry woman enters the centre. It is Honorine’s mother, Jeanette Olègbèyè.
It is the first time Ms Bohissou has met Honorine’s mother, and, judging from Ms Olègbèyè’s expression, she expects the girl will be marched back into the market with her tray of bread.
But Ms Olègbèyè’s anger dissolves when she is complimented on the beaded necklace and bracelet she is wearing. These were made for her by Honorine at the “barraque”.
She acknowledges: “Honorine’s behaviour has greatly improved since she started coming here... She is much more careful with her money. She also now can write ‘1, 2, 3, 4, 5’ and even further... When I ask her where she learnt those things she says ‘at that place I go to’. So I must admit it seems a good thing.”
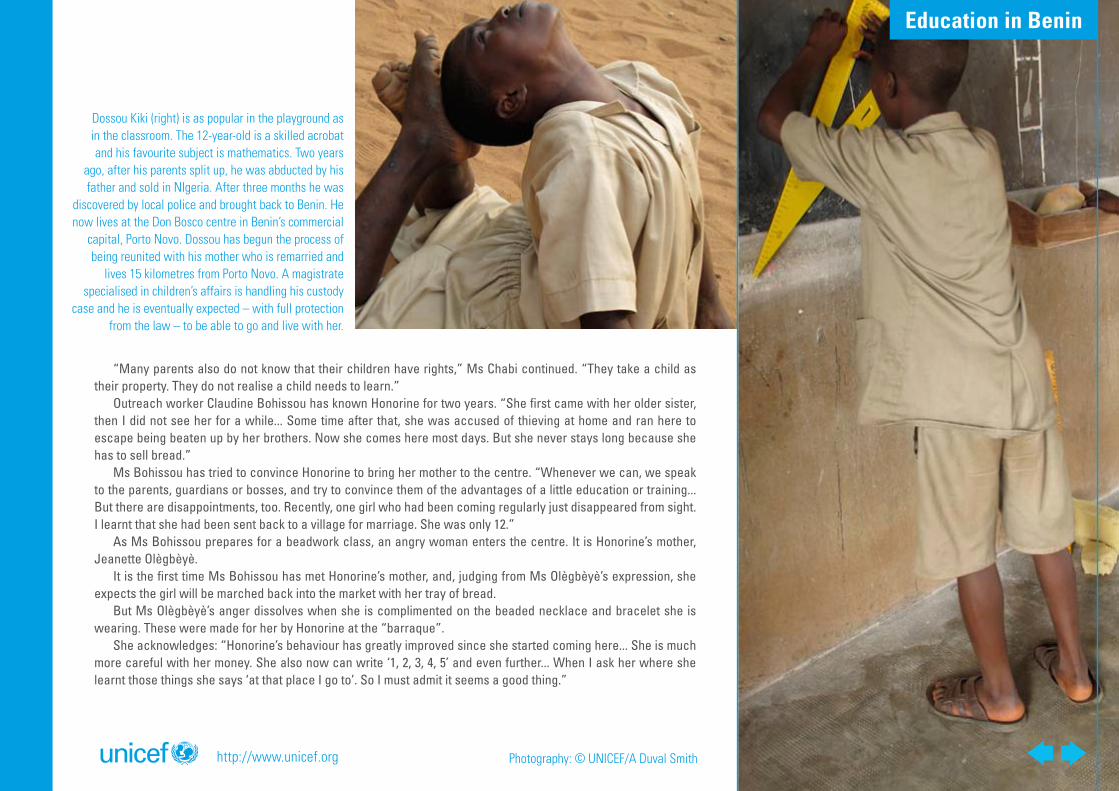
Dossou Kiki (right) is as popular in the playground as in the classroom. The 12-year-old is a skilled acrobat and his favourite subject is mathematics. Two years
ago, after his parents split up, he was abducted by his father and sold in NIgeria. After three months he was
discovered by local police and brought back to Benin. He now lives at the Don Bosco centre in Benin’s commercial
capital, Porto Novo. Dossou has begun the process of being reunited with his mother who is remarried and
lives 15 kilometres from Porto Novo. A magistrate specialised in children’s affairs is handling his custody
case and he is eventually expected – with full protection from the law – to be able to go and live with her.
http://www.unicef.org Photography: © UNICEF/A Duval Smith
Education in Benin
Stigma remains the main obstacle to
stopping HIV in its tracks. The solution
lies in confidential home visits that
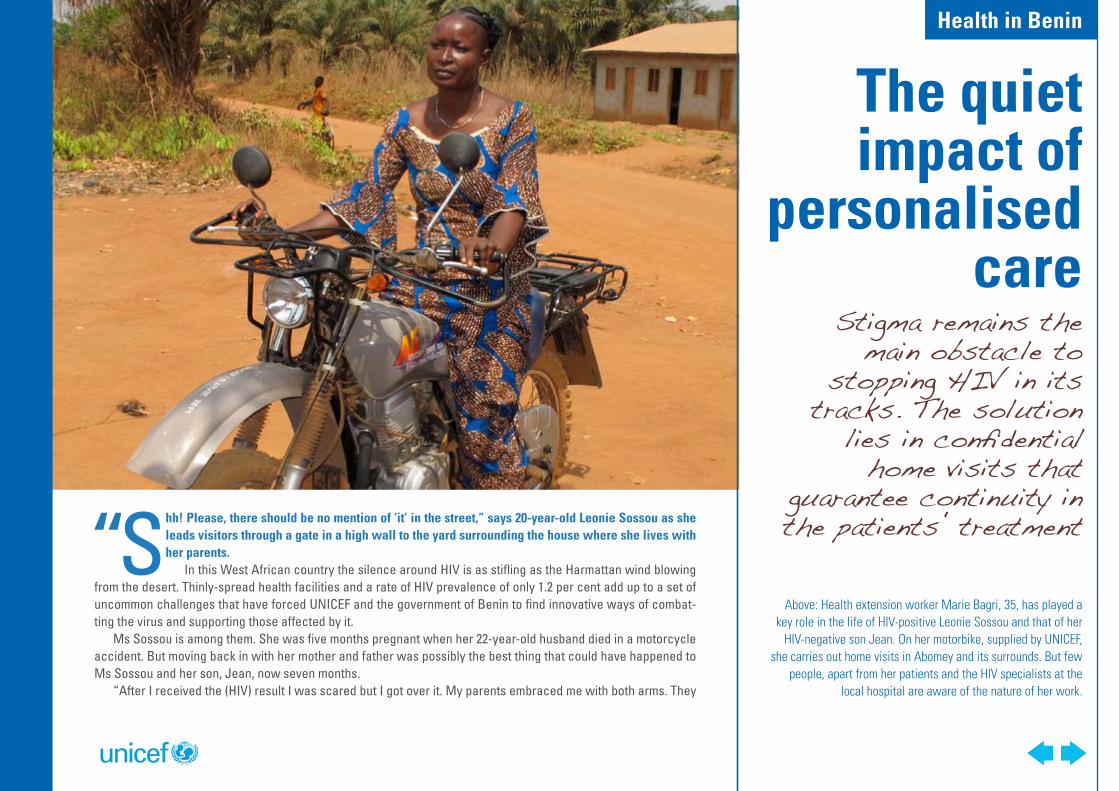
guarantee continuity in the patients‛ treatment“Shh! Please, there should be no mention of ‘it’ in the street,” says 20-year-old Leonie Sossou as she
leads visitors through a gate in a high wall to the yard surrounding the house where she lives with her parents.
In this West African country the silence around HIV is as stifling as the Harmattan wind blowing from the desert. Thinly-spread health facilities and a rate of HIV prevalence of only 1.2 per cent add up to a set of uncommon challenges that have forced UNICEF and the government of Benin to find innovative ways of combat-ting the virus and supporting those affected by it.
Ms Sossou is among them. She was five months pregnant when her 22-year-old husband died in a motorcycle accident. But moving back in with her mother and father was possibly the best thing that could have happened to Ms Sossou and her son, Jean, now seven months.
“After I received the (HIV) result I was scared but I got over it. My parents embraced me with both arms. They
The quiet impact of
personalised care
Above: Health extension worker Marie Bagri, 35, has played a key role in the life of HIV-positive Leonie Sossou and that of her
HIV-negative son Jean. On her motorbike, supplied by UNICEF, she carries out home visits in Abomey and its surrounds. But few
people, apart from her patients and the HIV specialists at the local hospital are aware of the nature of her work.
Health in Benin
said I was not to worry and so I started taking the tablets. By the grace of God everything was fine,” says the young mother as she sits with her son under a shady tree in the yard.
Ms Sossou received a Prevention of Mother-To-Child Transmission (PMTCT) course of anti-retrovirals during labour. Jean was born HIV-negative and was exclusively breastfed during his first six months. He will be tested for HIV again at nine months but the family’s rigorous adherence to medical advice suggests that the outcome will be good. Ms Sossou is also in good health and taking anti-retrovirals.
A key player in the past year of Ms Sossou’s life and that of her healthy son has been a 35-year-old local woman, Marie Bagri. With the looks and bearing of a model, she cuts an unlikely figure as she vrooms down dusty roads on her rugged health extension worker’s Yamaha motorbike.
Ms Bagri, whose salary is paid by UNICEF, says that discretion is a key part of her job: “With Leonie it has been easy. The neighbours think I am a family friend. With others it is more complicated. Once you have been to see them once or twice they will tell you not to go back to their place. Some do not even want their husbands to know. And if they live in polygamous households they do not want the other wives to know that they are HIV-positive. You have to arrange secret meetings.”
Ms Sossou is able to travel to a nearby clinic for check-ups and to collect her medication. But in distant rural areas, the medical supervision needed by an HIV-positive mother-to-be or her baby, once born, present a deeper challenge.
At a nearby clinic, laboratory engineer Sophie Tafeti holds up a small white card with five black circles, each containing a spot of blood. The so-called Dried Blood Spot test, introduced in Benin in 2010, is a further weapon in the arsenal used by health workers operating in this hot and hostile climate of secrecy and stigma.
She says: “The Dried Blood Spot kit allows a midwife to collect a sample, far away, without fuss. UNICEF pays for regular collections of the cards and they are brought here for analysis. The system means we can test more children, further away, more economically, and the samples do not get spoilt by the heat as they would if they were in test tubes. This approach is also discreet because midwives can take the sample during routine visits.”
In such a hushed atmosphere HIV prevention also presents particular challenges, says UNICEF HIV/AIDS spe-cialist Tharcienne Ndihokubwayo: “Benin has a low prevalence of HIV but high rates among certain groups, such as sex workers – over 20 per cent – and truck drivers (five per cent). These are groups that could spread the virus
Four hundred primary schools in 18 local authorities hold regular contests of “Stop Sida”, a board game similar to Monopoly in which the “chance” cards include one featuring a condom
and another showing a menacing-looking syringe.
”Some women do not even want their husbands to know they are HIV-positive.
You have to arrange secret meetings‟ Marie Bagri, HIV health extension worker
Watch the video on HIV in Benin on http://www.unicef.org/aids/benin_61951.html
Health in Benin
to the broader population. At the same time, in some villages, people are not informed or, if they are, they believe HIV does not concern them.”
Given concern about the possible future spread of HIV, the government has put the issue high on the agenda and UNICEF has taken HIV prevention to schools. Four hundred primary schools in 18 local authorities hold regular contests of “Stop Sida”, a board game similar to Monopoly in which the “chance” cards include one featuring a condom and another showing a menacing-looking syringe.
At a primary school at Zado-Gagbé in Zogbodomey town, principal Maxime Gnacadja, 52, says his 380 pupils adore the game. “Parents do not talk about HIV. It’s seen as something shameful. But through the game, the children learn what behaviour to adopt to avoid catching AIDS. You hear them shouting ‘don’t do that or you’ll catch AIDS!’ They also learn teamwork, they learn how to negotiate and how to manage money.”
The game came too late for Ms Sossou, living her status in secret and nursing Jean under the shady tree. But her mother, Eleonore, a retired market trader, is very clear about the fact that what her daughter and grandson need now is love in a supportive environment.
“Everyone in the close family knows Leonie’s status but more distant relatives do not know. This boy is my grandchild and Jean may be my daughter’s only child. Nothing else matters,” she insists.
But by now, Ms Sossou has shed a tear. Will she one day be able to marry? Will she remain healthy herself? They are questions that are impossible to answer – and even to ask – in the climate of silence beyond the walls of the family home.Names have been changed.
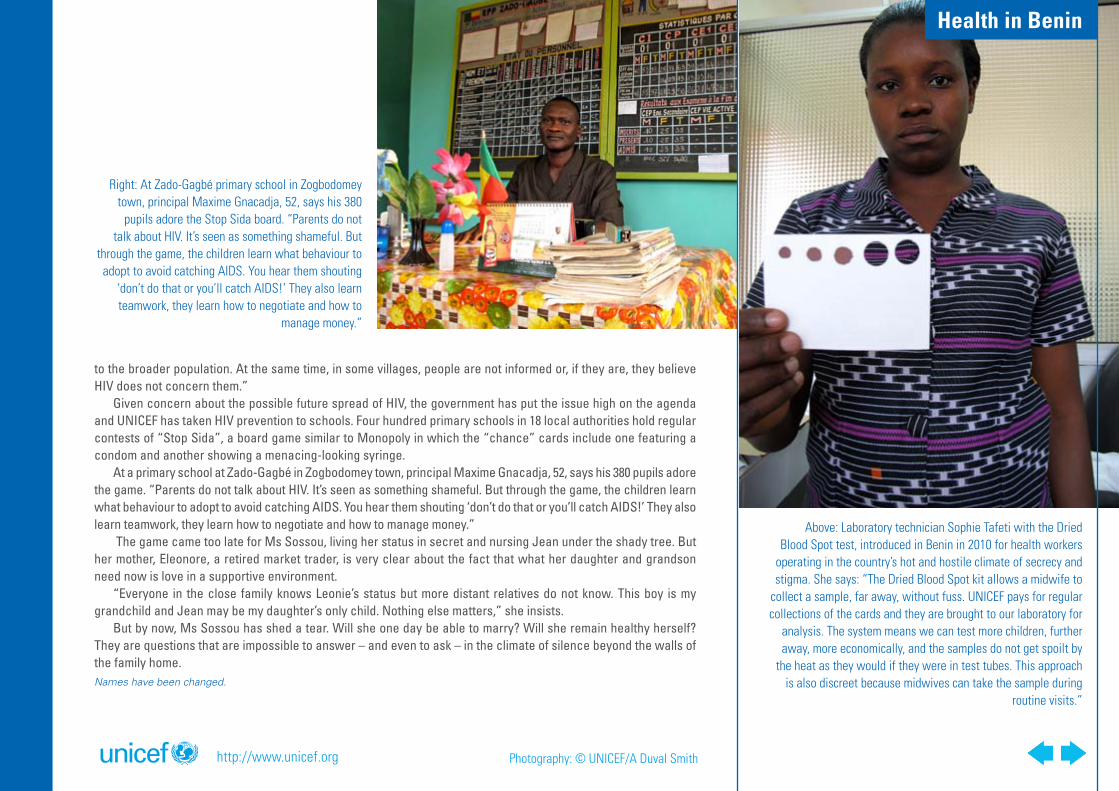
Right: At Zado-Gagbé primary school in Zogbodomey town, principal Maxime Gnacadja, 52, says his 380
pupils adore the Stop Sida board. “Parents do not talk about HIV. It’s seen as something shameful. But
through the game, the children learn what behaviour to adopt to avoid catching AIDS. You hear them shouting
‘don’t do that or you’ll catch AIDS!’ They also learn teamwork, they learn how to negotiate and how to
manage money.”
Above: Laboratory technician Sophie Tafeti with the Dried Blood Spot test, introduced in Benin in 2010 for health workers
operating in the country’s hot and hostile climate of secrecy and stigma. She says: “The Dried Blood Spot kit allows a midwife to
collect a sample, far away, without fuss. UNICEF pays for regular collections of the cards and they are brought to our laboratory for
analysis. The system means we can test more children, further away, more economically, and the samples do not get spoilt by
the heat as they would if they were in test tubes. This approach is also discreet because midwives can take the sample during
routine visits.”
http://www.unicef.org Photography: © UNICEF/A Duval Smith
Health in Benin
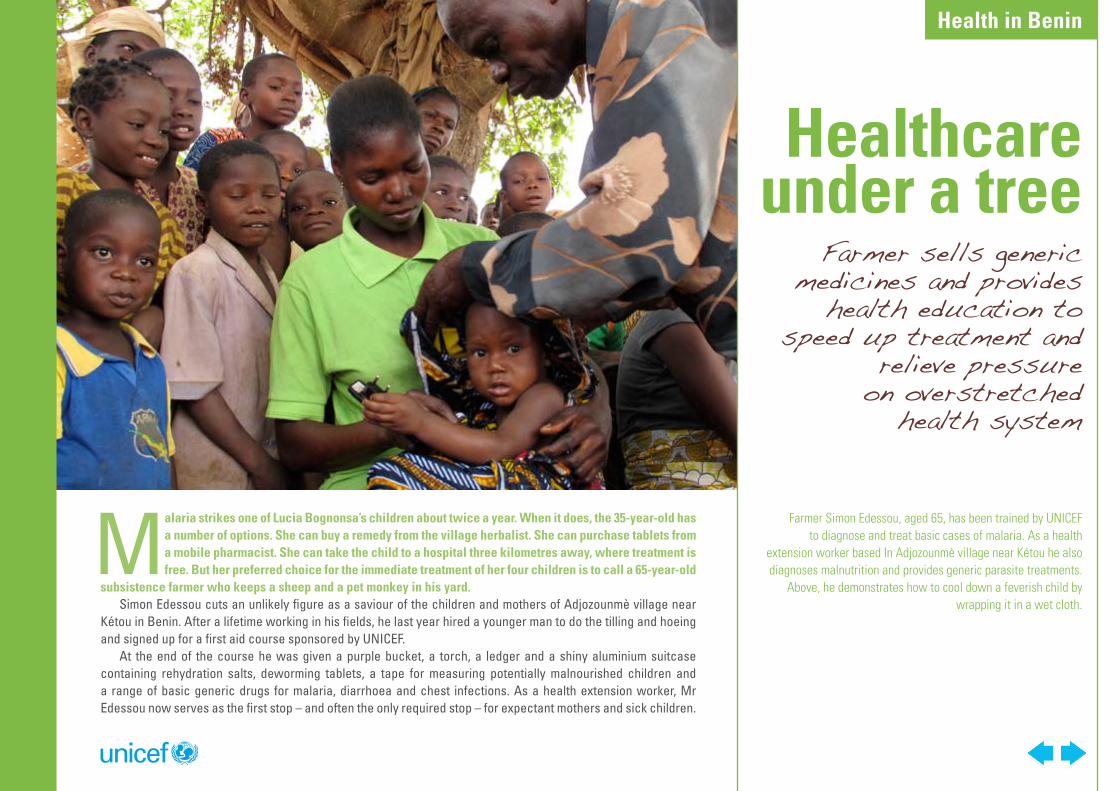
Malaria strikes one of Lucia Bognonsa’s children about twice a year. When it does, the 35-year-old has a number of options. She can buy a remedy from the village herbalist. She can purchase tablets from a mobile pharmacist. She can take the child to a hospital three kilometres away, where treatment is free. But her preferred choice for the immediate treatment of her four children is to call a 65-year-old
subsistence farmer who keeps a sheep and a pet monkey in his yard.Simon Edessou cuts an unlikely figure as a saviour of the children and mothers of Adjozounmè village near
Kétou in Benin. After a lifetime working in his fields, he last year hired a younger man to do the tilling and hoeing and signed up for a first aid course sponsored by UNICEF.
At the end of the course he was given a purple bucket, a torch, a ledger and a shiny aluminium suitcase containing rehydration salts, deworming tablets, a tape for measuring potentially malnourished children and a range of basic generic drugs for malaria, diarrhoea and chest infections. As a health extension worker, Mr Edessou now serves as the first stop – and often the only required stop – for expectant mothers and sick children.
Healthcare under a tree
Farmer Simon Edessou, aged 65, has been trained by UNICEF to diagnose and treat basic cases of malaria. As a health
extension worker based In Adjozounmè village near Kétou he also diagnoses malnutrition and provides generic parasite treatments.
Above, he demonstrates how to cool down a feverish child by wrapping it in a wet cloth.
Farmer sells generic medicines and provides
health education to speed up treatment and
relieve pressure on overstretched
health system
Health in Benin
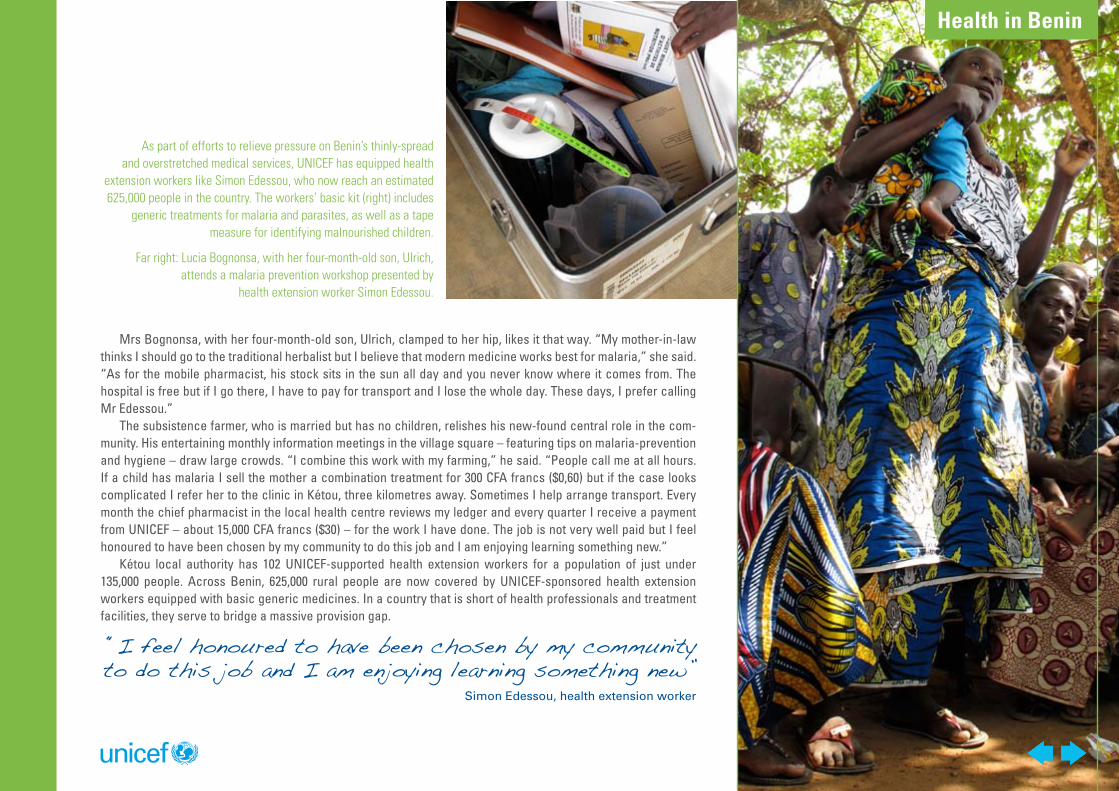
Mrs Bognonsa, with her four-month-old son, Ulrich, clamped to her hip, likes it that way. “My mother-in-law thinks I should go to the traditional herbalist but I believe that modern medicine works best for malaria,” she said. “As for the mobile pharmacist, his stock sits in the sun all day and you never know where it comes from. The hospital is free but if I go there, I have to pay for transport and I lose the whole day. These days, I prefer calling Mr Edessou.”
The subsistence farmer, who is married but has no children, relishes his new-found central role in the com-munity. His entertaining monthly information meetings in the village square – featuring tips on malaria-prevention and hygiene – draw large crowds. “I combine this work with my farming,” he said. “People call me at all hours. If a child has malaria I sell the mother a combination treatment for 300 CFA francs ($0,60) but if the case looks complicated I refer her to the clinic in Kétou, three kilometres away. Sometimes I help arrange transport. Every month the chief pharmacist in the local health centre reviews my ledger and every quarter I receive a payment from UNICEF – about 15,000 CFA francs ($30) – for the work I have done. The job is not very well paid but I feel honoured to have been chosen by my community to do this job and I am enjoying learning something new.”
Kétou local authority has 102 UNICEF-supported health extension workers for a population of just under 135,000 people. Across Benin, 625,000 rural people are now covered by UNICEF-sponsored health extension workers equipped with basic generic medicines. In a country that is short of health professionals and treatment facilities, they serve to bridge a massive provision gap.
As part of efforts to relieve pressure on Benin’s thinly-spread and overstretched medical services, UNICEF has equipped health
extension workers like Simon Edessou, who now reach an estimated 625,000 people in the country. The workers’ basic kit (right) includes
generic treatments for malaria and parasites, as well as a tape measure for identifying malnourished children.
Far right: Lucia Bognonsa, with her four-month-old son, Ulrich, attends a malaria prevention workshop presented by
health extension worker Simon Edessou.
“I feel honoured to have been chosen by my community to do this job and I am enjoying learning something new”
Simon Edessou, health extension worker
Health in Benin
UNICEF community health expert Ange Meizou says the network of extension workers – currently in four of Benin’s health districts – is intended to be expanded and gradually incorporated into the country’s health system.
“We started in March 2011 by giving each extension worker a basic kit and set of medicines. The sale of the medicines is intended to fund the purchase of new stocks. For the first 18 months, UNICEF is covering the exten-sion workers’ incentive payments. At the end of 2012, according to the contracts we have signed with health districts and local authorities, the responsibility for the incentive payments will switch to local authorities,” said Mr Meizou, aged 50, who is based in the commercial capital, Cotonou.
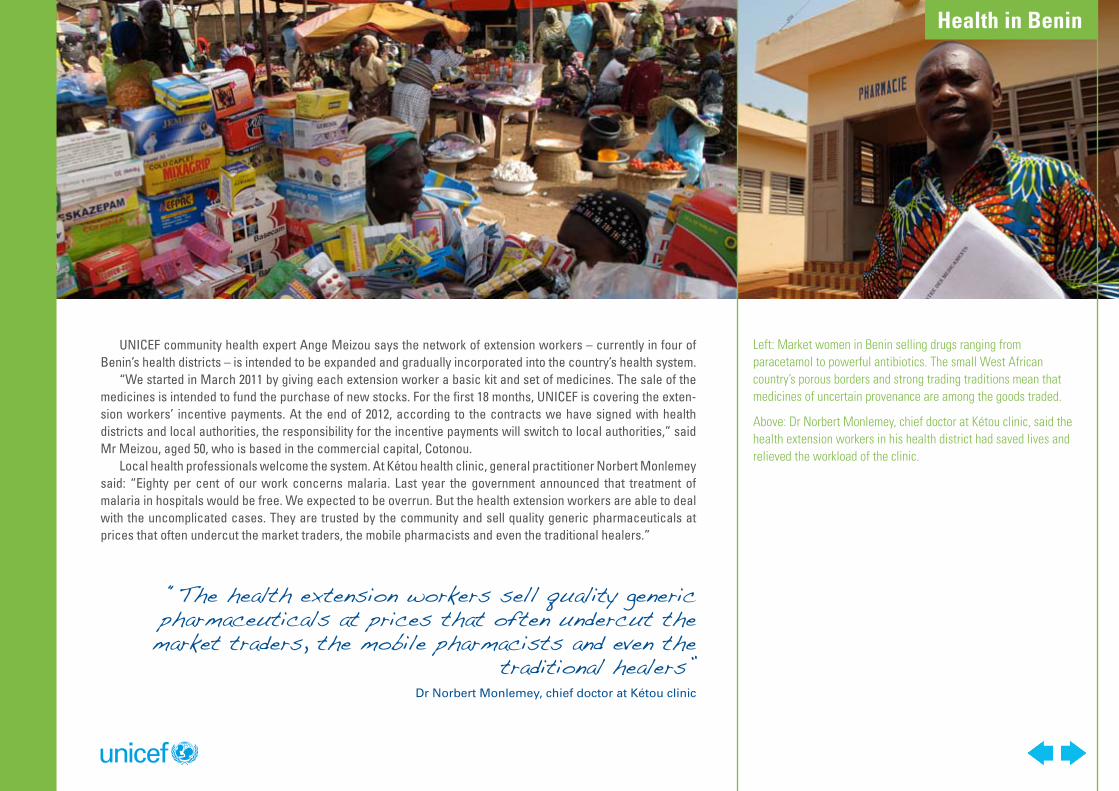
Local health professionals welcome the system. At Kétou health clinic, general practitioner Norbert Monlemey said: “Eighty per cent of our work concerns malaria. Last year the government announced that treatment of malaria in hospitals would be free. We expected to be overrun. But the health extension workers are able to deal with the uncomplicated cases. They are trusted by the community and sell quality generic pharmaceuticals at prices that often undercut the market traders, the mobile pharmacists and even the traditional healers.”
Left: Market women in Benin selling drugs ranging from paracetamol to powerful antibiotics. The small West African country’s porous borders and strong trading traditions mean that medicines of uncertain provenance are among the goods traded.
Above: Dr Norbert Monlemey, chief doctor at Kétou clinic, said the health extension workers in his health district had saved lives and relieved the workload of the clinic.
“The health extension workers sell quality generic pharmaceuticals at prices that often undercut the market traders, the mobile pharmacists and even the
traditional healers”Dr Norbert Monlemey, chief doctor at Kétou clinic
Health in Benin
Dr Monlemey believes the system is not only freeing up hospital facilities but is also saving lives. “We used to admit many children suffering from severe anaemia. The mother would say ‘I treated my child at home’ and we would have to work out what had been given to them. Often it would transpire that the child had severe malaria. Now we are seeing fewer of these serious cases and also far fewer children in early stages of malaria.
“In terms of prevention the extension workers are helpful, too, because they act as an early-warning net-work. At monthly meetings we look at their ledgers and are able to gain a good idea of potential hotspots for malnutrition.”
He said Kétou’s mayor, himself a doctor, had played a supportive role by encouraging the recruitment of health extension workers and spreading the word about their services. “One of the reasons people turn to mobile phar-macists, even though their drugs are of uncertain provenance and they have no medical expertise, is that they offer credit. But increasingly, villagers are becoming aware of the many advantages of calling the health exten-sion workers: Their prices are fair, they are selected by the community and they live there – which means they are trusted – and they do not just prescribe pills to repress symptoms; they have enough training to know when they need to refer cases to us.”
Mrs Bognonsa said she had only praise for Mr Edessou. “I remember when my eldest son, Justin, who is now four years old, started coughing and became ill with a fever. It was three years ago. We waited in the hopes that he would improve but he only got worse. In the end my husband and I took him to the hospital and he ended up spending 30 days there. We feared the worst. If we had had Mr Edessou among us then, I would have immediately taken the boy to see him and I am sure the illness would have been cured much more quickly,” she said.
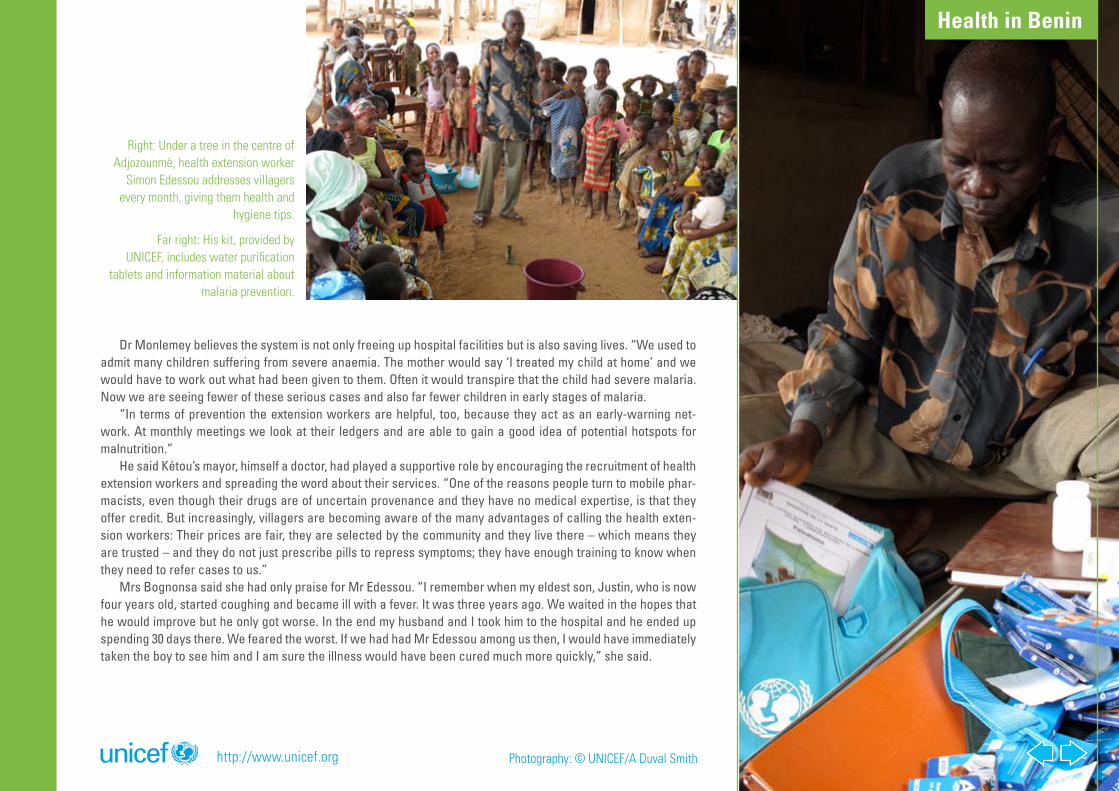
Right: Under a tree in the centre of Adjozounmè, health extension worker
Simon Edessou addresses villagers every month, giving them health and
hygiene tips.
Far right: His kit, provided by UNICEF, includes water purification
tablets and information material about malaria prevention.
http://www.unicef.org Photography: © UNICEF/A Duval Smith
Health in Benin